Moebius Syndrome With Total Anomalous Pulmonary Venous Connection
3
53 Clinical Brief Moebius Syndrome with Total Anomalous Pulmonary Venous Connection Jyoti Suvarna, Mahananda Bagnawar and C.T. Deshmukh Department of Pediatrics, Seth G S Medical College and KEM Hospital, Parel, Mumbai, Maharashtra, India. ABSTRACT. Moebius syndrome is characterized by congenital complete or partial facial nerve palsy with or without paralysis of cranial nerves and often associated with other malformations. Cardiac anomalies though known are very rare and till date only 4 cases have been reported. We present a case of Moebius syndrome with supracardiac total anomalous pulmonary venous connection which has not yet been reported in literature. [Indian J Pediatr 2006; 73 (5) : 427-429] Key words : Abducens nerve palsy; Ear external; Facies; Facial nerve, Hypoglossal nerve, Polydactyly. Moebius syndrome, a rare disorder of unknown etiology, presents with mask like facies (due to congenital complete or partial VII nerve palsy), and may be associated with squint (III nerve palsy), tongue hypoplasia (XII nerve palsy), swallowing difficulties (IX, X nerve palsy), orofacial and limb abnormalities. 1 Von Graafe first described a case of facial diplegia in 1880. Moebius in 1888 described association of facial diplegia with other malformations like multiple cranial neuropathies, mental deficiency, endocrine disorders, musculoskeletal deformities and cardiovascular defects. Handerson broadened the definition and included cases with congenital unilateral facial palsy. Cardiovascular defects though described, are rare, with only 4 cases with cardiac anomalies reported till date. 2, 3, 4, 5 Here is a case of Moebius syndrome with total anomalous pulmonary venous connection (TAPVC), which is not yet reported. CASE REPORT An eight month old female child, born of a non- consanguineous marriage, presented with facial asymmetry, cyanosis since birth, delayed milestones and failure to thrive. The child was born in a pre-term delivery (32 wks) with birth wt of 1.3 kg, without birth asphyxia. There was cyanosis, clubbing, without congestive cardiac failure. Child had dysmorphic features like malformed right ear with under developed external auditory meatus, small left ear, hypoplastic right side of the face, deviation of the angle of mouth to the left, hypoplasia of the tongue on the right, right sided microphthalmia with small palpabral fissure, right lateral rectal palsy and polydactyly of the right hand. Child had an ejection systolic murmur in the 3 rd and 4 th left intercostal space parasternally. Other systems were normal. On investigations X-ray chest showed cardiomegaly with right ventricular apex, ECG showed right ventricular hypertrophy, 2-D-Echo showed supracardiac non- obstructive total anomalous pulmonary venous connection. CT scan brain was normal. Moebius syndrome was diagnosed on the basis of right VII facial nerve palsy, right VI nerve palsy, XII cranial nerve involvement, polydactyly, ear anomalies and cyanotic congenital heart disease. Correspondence and Reprint requests : Dr. Jyoti Suvarna, B/21, Fig. 1. Shows the facial nerve palsy, inability to close the right eye Shivganga CHS, Vakola Pipeline, Mumbai-400055, Maharashtra, and flattening of the right nasolabial fold. India. E-mail: [email protected] Indian Journal of Pediatrics, Volume 73—May, 2006 427
-
Upload
thodoris-yuruba-bombadill -
Category
Documents
-
view
2 -
download
0
description
Moebius Syndrome With Total Anomalous Pulmonary Venous Connection
Transcript of Moebius Syndrome With Total Anomalous Pulmonary Venous Connection

53
Clinical Brief
Moebius Syndrome with Total Anomalous Pulmonary Venous Connection
Jyoti Suvarna, Mahananda Bagnawar and C.T. Deshmukh
Department of Pediatrics, Seth G S Medical College and KEM Hospital, Parel, Mumbai, Maharashtra, India.
ABSTRACT . Moebius syndrome is characterized by congenital complete or partial facial nerve palsy with or without paralysis of cranial nerves and often associated with other malformations. Cardiac anomalies though known are very rare and till date only 4 cases have been reported. We present a case of Moebius syndrome with supracardiac total anomalous pulmonary venous connection which has not yet been reported in literature. [Indian J Pediatr 2006; 73 (5) : 427-429]
Key words : Abducens nerve palsy; Ear external; Facies; Facial nerve, Hypoglossal nerve, Polydactyly.
Moebius syndrome, a rare disorder of unknown etiology, presents with mask like facies (due to congenital complete or partial VII nerve palsy), and may be associated with squint (III nerve palsy), tongue hypoplasia (XII nerve palsy), swallowing difficulties (IX, X nerve palsy), orofacial and limb abnormalities.1 Von Graafe first described a case of facial diplegia in 1880. Moebius in 1888 described association of facial diplegia with other malformations like multiple cranial neuropathies, mental deficiency, endocrine disorders, musculoskeletal deformities and cardiovascular defects. Handerson broadened the definition and included cases with congenital unilateral facial palsy.
Cardiovascular defects though described, are rare, with only 4 cases with cardiac anomalies reported till date.2, 3, 4,
5 Here is a case of Moebius syndrome with total anomalous pulmonary venous connection (TAPVC), which is not yet reported.
CASE REPORT
An eight month old female child, born of a non-consanguineous marriage, presented with facial asymmetry, cyanosis since birth, delayed milestones and failure to thrive. The child was born in a pre-term delivery (32 wks) with birth wt of 1.3 kg, without birth asphyxia. There was cyanosis, clubbing, without congestive cardiac failure. Child had dysmorphic features like malformed right ear with under developed external auditory meatus, small left ear, hypoplastic right side of the face, deviation
of the angle of mouth to the left, hypoplasia of the tongue on the right, right sided microphthalmia with small palpabral fissure, right lateral rectal palsy and polydactyly of the right hand. Child had an ejection systolic murmur in the 3rd and 4th left intercostal space parasternally. Other systems were normal.
On investigations X-ray chest showed cardiomegaly with right ventricular apex, ECG showed right ventricular hypertrophy, 2-D-Echo showed supracardiac non-obstructive total anomalous pulmonary venous connection. CT scan brain was normal.
Moebius syndrome was diagnosed on the basis of right VII facial nerve palsy, right VI nerve palsy, XII cranial nerve involvement, polydactyly, ear anomalies and cyanotic congenital heart disease.
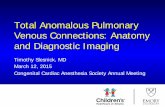
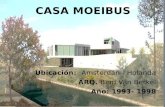
Correspondence and Reprint requests : Dr. Jyoti Suvarna, B/21, Fig. 1. Shows the facial nerve palsy, inability to close the right eyeShivganga CHS, Vakola Pipeline, Mumbai-400055, Maharashtra, and flattening of the right nasolabial fold.India. E-mail: [email protected]
Indian Journal of Pediatrics, Volume 73—May, 2006 427

54
Jyoti Suvarna et al
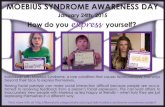
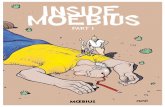
Fig. 2. Shows malformed right ear with underdeveloped external auditory meatus
DISCUSSION
Moebius syndrome with its wide spectrum of congenital malformations points to some disturbance during 4th -7th
gestational week, since hand, heart develop between 4th to 7th weeks and neuronal cellular differentiation forming cranial nerve nuclei from 4th to 5th week onwards.3
Association of all these defects supports the vascular theory of embryopathogenesis, that cranial nuclear necrosis due to an insufficient blood supply is the cause of Moebius syndrome. Bavinck and Weaver6 proposed a unifying theory to explain the findings of Moebius syndrome, Poland anomaly and Klippel-Feil defect. They suggested that the interruption of the development of
TABLE 1. Clinical Features of Moebius Syndrome
subclavian artery and its tributaries, (including the basilar, vertebral and internal thoracic arteries, which supply the brain, neck, pectoral muscles and upper limb), at or around sixth intrauterine week, is causative. Furthermore they postulated that, in Moebius syndrome, the regression of the primitive trigeminal artery supplying the hindbrain before the establishment of vertebral or basilar artery may impair the cranial nerve nuclei development.6 Facial weakness with cardiovascular anomalies gives indirect evidence for the vascular pathogenesis of Moebius anomaly (Pape and Pickering 1972). Mesodermal dysplasia of the 1st and 2nd
branchial arches and drugs like misoprostol,5
benzodiazepines7and cocaine8 have also been implicated as causes in certain studies. Although most of the cases are sporadic, all patterns of inheritance autosomal recessive, autosomal dominant, and X-linked recessive have been described1. Reciprocal translocation between chromosome 1 and 13, t (1p34; 13q13) has been described in seven members of a family over three generations with congenital facial diplegia, finger flexon deformities and mild mental retardation.9
Following guidelines, based on previous studies, are made for the diagnosis of Moebius syndrome1, 10
a. Complete or partial facial nerve paralysis is an essential feature.
b. Limb malformations (syndactyly, brachydactyly, absent digits, talipes) are often present.
c. Bilateral or unilateral cranial nerve palsies (commonly VI, XII, also IX, X) may be seen.
d. Orofacial malformations, ear deformities and musculoskeletal deformities may also be seen. (See table 1, for clinical features in detail)
Neurological manifestation: common VII Cranial nerve – 100% VI – 75% XII - 25% Mask facies (expressionless) IX , X Palsies
Other Neurological Features § Mental retardation 10-15% § Conductive hearing loss § Speech problems- disarticulations. § Autistic behaviour noticed in 30-40%. § Anosmia with hypogonadotropic hypogonadism.
Musculoskeletal manifestations A) Limb defects - Syndactyly, brachydactyly, polydactyly - Talipus equinovarus - Arthrogryposis. - Congenital amputation
B) Aplastic, hypoplastic latissimus dorsi, serratus anterior, intercostal muscles. - Absence of pectoralis muscle usually unilateral with mammary hypoplasia. - Webbed neck, finger toes. - Absence or hypoplasia of radius, ulna metacarpals, phalanges, bilateral epicanthic folds ear deformities, arched palate bifid uvula microglossia, microstomia, micrognathia, teeth and jaw malformations, hypertelorism.
Ear Anomalies Microtia, malformed ears, malformed auditory meatus. Skin Café au lait spots, webbing of axilla, absence of subcutaneous tissue. Less common Cardiovascular anomalies, arthrogryposis multiplex congenita, Klippel Feil anomaly.
428 Indian Journal of Pediatrics, Volume 73—May, 2006

55
Moebius Syndrome with Total Anomalous Pulmonary Venous Connection
The cardiac anomalies described previously in Moebius syndrome are plain dextrocardia,2 dextrocardia with ventricular septal defect,3 transposition of great vessels,4 and ventricular septal defect.5 Our patient had supracardiac total anomalous pulmonary venous return, which has not yet been reported.
10-15% of the patients with Moebius syndrome have mild mental retardation and 30-40% may have autistic behaviour. Severe brain stem compromise, if present, can cause dysphagia, aspiration, and inability to protect the airway, may lead to death at young age. Recurrence risks to sibs of classical isolated cases is 2 %, but risks to offspring is still uncertain. Quality of life depends on degree of severity of the malformation. Treatment is predominantly management of the associated defects and essentially multidisciplinary. Special attention should be paid to problems of parental bonding and family care disturbance, due to lack of feedback from the child by smiling or visual following. Neuro psychological and intelligence testing should be done to detect learning difficulties autism and visual apraxias.
Acknowledgements
The authors thank Dr N A Kshirsagar- Dean, Seth G S Medical College and K E M Hospital for granting permission to publish this article.
REFERENCES
1. Kumar D. Moebius Syndrome. J Med Genet 1990; 27: 122-126. 2. Bosch Banyeras JM, Zuasnabar A, Puig A, Catalia M,
Cuatercasas SM. Poland Mobius syndrome associated with dextrocardia. J Med Genetics 1984; 21 : 70-71.
3. Caravella L, Rogers GL. Dextrocardia and ventricular septal defect in Moebius syndrome. Ann Ophthalmol 1978; 10 : 572575.
4. Rarogue HG Jr, Hershewe GL, Synder RD. Moebius syndrome and transposition of great vessels. Neurology 1988; 38 : 18941895.
5. Deda G, Caksen H, Atalay S. Moebius syndrome with ventricular septal defect. Indian J Pediatr 2001; 68: 455-456.
6. Bavinck JN, Weaver DD. Subclavian artery supply disruption sequence: hypothesis of vascular etiology for Poland, Klippel Feil and Moebius anomalies. Am J Med Genet 1986; 23: 903-918.
7. Courtens W, Vamos E, Hainaut M, Vergauwen P. Moebius syndrome in an infant exposed in utero to benzodiazepines. J Pediatr 1992; 121: 833-834.
8. Kankirawatana P, Tennison MB, D’Cruz O, Greenwood RS. Moebius syndrome in infant exposed to cocaine inutero. Pediatr Neurol 1993; 9: 71-72.
9. Hedges DW, Jeppson KG, Burn SC. Twenty year behavioural follow-up of a 1: 13 chromosomal translocaion and Moebius syndrome presenting with poor impulse control, exhibitionism and aggression. Compr Psychiatr 2003; 44: 462 465.
10. Baraister M. Genetics of Moebius syndrome. J Med Genet 1977; 14: 415-417.
Indian Journal of Pediatrics, Volume 73—May, 2006 429