
Module : Development of the Nervous System Lecture 6 Synapse formation & refinement

11/7/2016
1
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
MODULE G
SECTION 1
Nervous System
NUR 202
Instructor: Dr. Dowanda D. Pullom, RN
OBJECTIVES
• The student will:
�Understand the anatomy & physiology of the nervous system.
�Compare and contrast the etiology, clinical manifestations, collaborative care, and nursing management of tension-type, migraine, and cluster headaches.
�Differentiate the etiology, clinical manifestations, diagnostic studies, collaborative care, and nursing management of multiple sclerosis, Parkinson’s disease, and myasthenia gravis. 2
TOPICS
• ANATOMY & PHYSIOLOGY REVIEW
• Central nervous system
• Peripheral nervous system
• Neuron
• Neuroglia
• Neurotransmitter
• Myelin
• Autonomic nervous system
• HEADACHES
• MAJOR CHRONIC DISEASES
• Multiple sclerosis
• Parkinson’s disease
• Myasthenia gravis
3

11/7/2016
2
COMPONENTS OF THE
NERVOUS SYSTEM
Central Nervous
System includes
both Spinal and
Cranial Nerves
4
CELLS OF THE
NERVOUS SYSTEM: NEURON
5
1. Excitability
2. Conductivity
3. Influence
CELLS OF THE NERVOUS SYSTEM:
GLIAL (NEUROGLIA)
Provide to Neurons
• Support
• Nourishment
• Protection
6
What is the function of the Glial
Cells?

11/7/2016
3
NEUROTRANSMITTERS
7
8
Circle of Willis
9

11/7/2016
4
CRANIAL NERVES
10
CRANIAL NERVES
On Olfactory
Old Optic
Olympus Oculomotor
Towering Trochlear
Tops Trigeminal
A Abducens
French Facial
And Auditory
Vestibulocochlear
German Glossopharyngeal
Viewed Vagus
Some Spinal Accessory
Hops Hypoglossal
11
EFFECTS OF AGING
• Fall Risks
• Nutritional Risks
• Risk for Temperature,
BP Problems
12

11/7/2016
5
Assessment of Nervous System
• Past Health History
• Medications
• Surgery or other treatment
• Functional health Patterns
� Substance abuse, smoking, nutrition, blood pressure control
� Participation in recreational activities
• Seat belts, and Helmets
• Elimination
• Sleep/Rest Pattern
• Physical exam Findings
� Mental Status
� Cranial Nerve Assessment
Table 56-6 Normal physical assessment or nervous system p. 1349 13
Diagnostic Studies of Nervous
System
• Lumbar Puncture
• Computed Tomography
• Magnetic Resonance Imaging
• Cerebral Angiography
• Electroencephalography
• Electromyography and Nerve Conduction Studies
P. 1351 Table 56-8 1352-1353
Please read purpose of the tests and the nursing responsibilities
related to the test.14
LUMBAR PUNCTURE **
15
Tube # 1 Chemistries – GLUCOSE
Tube # 2 Bacteria
Tube # 3 or 4 Blood (WBC and RBC)

11/7/2016
6
Copyright © 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.
Chapter 57 Acute
Intracranial Problems
COMA
INCREASED INTRACRANIAL PRESSURE
(IICP)
NORMAL INTRACRANIAL PRESSURE
17
� DEFINED
� 3 components
� Normal limit
ICP Normal 5-
15%
Compliance :
Is the expandability of the brain
• Monro-Kelly doctrine
18
NORMAL INTRACRANIAL PRESSURE cont…
11/7/2016
7
• DEFINITION: The amount of blood in milliliters passing through
100grams of brain tissue in 1 minute.
• NORMAL RANGE: Approx. 50mL/min per 100g of brain tissue.
• AUTOREGULATION: Automatic adjustments in the diameter of the
cerebral blood vessels in order to maintain a constant blood flow
during changes in systemic BP.
CEREBRAL BLOOD FLOW
19
20
**CBF and ICP are NOT the same thing. Increased ICP causes decreased
CBF.
• The pressure needed to ensure blood flow to the brain.
• CPP = MAP − ICP
• Normal CPP 60 to 100
• CPP of less than 50 is associated with ischemia and neuronal
death
21
CPP (Cerebral Perfusion Pressure)

11/7/2016
8
Intracranial Pressure (ICP)
22Table 57-1. Calculation of Cerebral Perfusion Pressure
22
Increased Intracranial Pressure (ICP)
23
Fig. 57-2. Intracranial pressure-volume curve. (See text for descriptions of 1, 2, 3, and 4.)
Compliance :
Is the expandability of the brain
With HIGH compliance
the brain’s
autoregulation is intact
and accommodating
changes in volume
With LOW compliance
the brain’s
compensation
mechanisms start to
fail.
Compliance
23
24
Increased Intracranial Pressure (ICP)

11/7/2016
9
INCREASED
INTRACRANIAL PRESSURE:
25
Fig. 57-3. Progression of increased intracranial pressure (ICP).
25
• DEFINITION:
• LOC- A range of signs/symptoms from headache coma.
• Coma- a state of extreme unresponsiveness, in which an individual
exhibits no voluntary movement or behavior.
� SIGNIFICANCE:
� Level of consciousness is the most sensitive and reliable indicator of
the patient’s neurologic status.
� RAS (Reticular Activating System)
located in brain stem.
Damage to RAS can cause coma
ALTERED LEVEL OF CONSCIOUSNESS
(LOC) COMA
26
Personality and Behavioral Signs of
Increasing ICP
• Irritability, restlessness
• Drowsiness, indifference, decrease in physical
activity and motor skills
• Diminished physical activity
• Inability to follow commands, memory loss
• Lethargy and drowsiness
• YAWNING
27

11/7/2016
10
Late Signs of Increasing ICP• Decreased LOC
• Decreased motor response to command
• Decreased sensory response to painful stimuli
• Alterations in pupil size and reactivity
• Papilledema
• Decerebrate or decorticate posturing
• Cheyne-Stokes respirations
https://www.youtube.com/watch?v=DH2GElqrK8o
28
COMPLICATIONS OF ICP
• In adequate cerebral perfusion
• Cerebral Herniation
29
• Rise in systolic BP
• Widening Pulse Pressure
• PP= SP - DS
• Bradycardia with a full bounding
pulse and altered respirations.
30
*CUSHING’S TRIAD*
11/7/2016
11
LOCs
(in Descending Order)
↓Full consciousness
↓ Confusion: impaired decision
making
↓ Disorientation: to time and place
↓ Lethargy: sluggish speech
32
LOCs
(in Descending Order)—cont’d
↓ Obtundation: arouses with stimulation
↓ Stupor: responds only to vigorous and repeated
stimulation
↓ Coma: no motor or verbal response to noxious stimuli
↓ Persistent vegetative state: permanently lost function of
cerebral cortex
33
11/7/2016
12
� Assessment:
� Vigilant and frequent neuro-assessment is
mandatory.
� Change in affect, orientation, attention
� EEG: electroencephalogram
� Vital Signs
� Labs: CBC, CMP, PT-INR, PTT, Ammonia, Drug
Screen
� CSF for WBC, culture, protein and glucose
34
Diagnostics in Altered LOC
Neurologic Examination
• Vital signs
• Skin
• Eyes
• Motor function
• Posturing
• Reflexes
35
Coma Assessment• Glasgow Coma Scale
• Three-part assessment
• Eyes
• Verbal response
• Motor response
• Score of 15: unaltered LOC
• Score of 3: extremely decreased LOC (worst possible
score on the scale)
• LESS THAN 8 LESS THAN 8 LESS THAN 8 LESS THAN 8 –––– ComaComaComaComa----INTUBATEINTUBATEINTUBATEINTUBATE
36

11/7/2016
13
Fig. 51-1. Pediatric coma scale. 37
PE
DIA
TR
IC
Nursing Management: Increased Intracranial
Pressure (ICP)
38
Fig. 57-11. Pupillary check for size and response.
38
Fig. 51-2. Variations in pupil size with altered states of consciousness. A, Ipsilateral pupillary constriction with slight ptosis. B, Bilateral small pupils. C, Midposition, light fixed to all stimuli. D,Bilateral dilated and fixed pupils. E, Dilated pupils, left eye abducted with ptosis. F, Pinpoint pupils.
39

11/7/2016
14
Fig. 51-3. A, Flexion posturing. B, Extension posturing. 40
�ABC
� INJURY
�SKIN
�MUSCULOSKELETAL
�NUTRITIONAL
COMA CARE: PRIORITIES
41
ICP Monitoring
• Indications for ICP monitoring
• Glasgow Coma Scale of 8
• Glasgow Coma Scale <8 with
respiratory assistance
• Deteriorating neurologic condition
• Subjective judgment regarding clinical
appearance and response
42

11/7/2016
15
Methods of Measuring ICP
• Ventriculostomy
• Subarachnoid bolt (Richmond
screw)
• Fiberoptic Catheter
43
Increased Intracranial Pressure
(ICP)
44
44
Collaborative Therapy
�Elevation of head of bed to 30 degrees with head in a neutral
position
�Intubation and mechanical ventilation
�ICP monitoring
�Cerebral oxygenation monitoring (PbtO2, SjvO2)
�Maintenance of PaO2 ≥100 mm Hg
�Maintenance of fluid balance and assessment of osmolality
�Maintenance of systolic arterial pressure between 100 and
160 mm Hg
�Maintenance of CPP >60 mm Hg
�Reduction of cerebral metabolism (e.g., high-dose
barbiturates)45

11/7/2016
16
Collaborative Therapy
Drug therapy�Osmotic diuretic (mannitol)
�Hypertonic saline
�Antiseizure drugs (e.g., phenytoin [Dilantin])
�Corticosteroids (dexamethasone [Decadron]) for brain tumors,
bacterial meningitis
�Histamine (H2)-receptor antagonist (e.g., cimetidine
[Tagamet]) or proton pump inhibitor (e.g., pantoprazole
[Protonix]) to prevent GI ulcers and bleeding
46
MANNITOL
47
Oliguria, edema, ICP-Indications
Stops reabsorption of water
Mannitol
Output of urine, electrolytes-monitor
Tissue dehydration-UE
Increased urination
Circulatory overload - UE
HYPERTONIC SOLUTION
• D5NSS (5% Dextrose in normal saline solution)
•
D5 in 0.45% NaCl ( 5% Dextrose in half strength normal saline)
•D5LR (5% Dextrose in Lactated Ringer's Solution)
•
D10W ( 10% Dextrose in water)
•
D50W50 (50% Dextrose in 50 ml of water)
• 3% Saline
48

11/7/2016
17
CORTICOSTEROIDS
Side Effects:
�Cushing like syndrome (moon face, wasting of arms and legs, buffalo hump resulting from excess fat deposits.
�Weight gain
�Changes in Labs - Some People Get Cold (SPGC)
Sodium
Potassium
Glucose
Calcium
Education:
• Administer with food or milk
• Withdraw medicine slowly
• Avoid infections and large crowds
• Don’t take ASPIRIN without consulting physician first 49
BARBITURATES
• Pentobarbital {Nembutal}
• Thiopental { Pentothall}
50
Nursing Care of the Client with
Increased ICP
• Patient positioning
• Avoid activities that may increase ICP
• Eliminate or minimize environmental noise
• Suctioning issues
• Strict aseptic technique during dressing changes or sampling
of CSF is imperative to prevent infection With the ventricular
catheter in place
51

11/7/2016
18
Increased Intracranial Pressure
(ICP)
52
Fig. 57-9. A, Leveling a ventriculostomy. B, CSF is drained into a drainage system.52
• OXYGENATION
• FLUIDS
• METABOLIC DEMANDS
• OTHER INTERVENTIONS
Safety Alert
• Be alert to altered breathing patterns.
• Snoring sounds indicate obstruction and require immediate intervention.
IICP: INTERVENTIONS
53
Chapter 59 Chronic
Neurological Problems
54

11/7/2016
19
TYPES OF HEADACHES
• TENSION
• CLUSTER
• MIGRAINE
• LP/ POSTCONCUSSION
55
Headache
• Probably the most common type of pain
experienced by humans
• Majority of people have functional headaches
• Migraine or tension-type headaches
56
Pain Location for Common Headache
Syndromes
57Fig. 59-1. Location of pain for common headache syndromes.
11/7/2016
20
Tension-Type Headache
• Most common type
• Bilateral, band-like feeling of pressure around the head
• Constant, squeezing tightness
• Not aggravated by physical activity
Etiology and Pathophysiology
• Mechanism in all patients with tension-type headaches has neurovascular factors similar to those involved in migraine headaches.
58
Tension-Type Headache
Clinical Manifestations
• May involve sensitivity to light and sound
• May occur intermittently
• Can have combination of migraine and tension-
type headaches
59
Tension-Type Headache
Diagnostic Studies
• Careful history taking
• Electromyography (EMG) may be performed.
• May reveal sustained contraction of neck,
scalp, or facial muscles
• May not show increased tension even when test
is done during headache
60
11/7/2016
21
Gender Differences
MEN
• Cluster headaches are
more common than in
women (6:1).
• Exercise-induced
headaches are more
common than in women.
WOMEN
• Migraine headaches are
more common than in
men (3:1).
• Tension headaches are
more common than in
men.
61
Migraine Headache
• Recurring
• Characterized by unilateral or bilateral throbbing
pain
• Strong family history
• More common in females than males
• In United States, prevalence highest in those of
lower socioeconomic status
62
Migraine Headache
Etiology and Pathophysiology
• Evidence suggests vascular, muscular, and
biochemical factors are involved.
• Exact cause is unknown.
• Can be preceded by an aura and prodrome
• May precede by days or hours
63

11/7/2016
22
Migraine Headache
Etiology and Pathophysiology
• May be precipitated or triggered by
• Food
• Hormonal fluctuations (Post Partum)
• Head trauma
• Physical exertion
• Fatigue
• Stress
• Pharmacologic agents
64
Migraine Headache
Clinical Manifestations
• Subdivided into categories. Two most important are:
• Migraine with aura
• Migraine without aura
Signs/Symptoms
• Generalized edema
• Irritability
• Pallor
• Nausea, vomiting
• Sweating 65
Migraine Headache
Clinical Manifestations
• During headache, some patients “hibernate.”
• Seek shelter from noise, light, odors, people,
and problems
• Headache is described as steady, throbbing pain
that matches the pulse.
• Pain is usually unilateral but may switch to other
side in another episode.
66
66

11/7/2016
23
Migraine Headache
Diagnostic Studies
• No specific laboratory or radiologic tests
• Diagnosis is usually made from history.
• Neurologic and diagnostic examinations are
normal.
67
Cluster Headache
• Rare form of headache
• Characterized by repeated headaches that occur
for weeks or months at a time, followed by
periods of remission
• One of the most severe forms of head pain
68
68
Cluster Headache
Etiology and Pathophysiology
• Neither cause nor pathophysiologic mechanism is
known.
• Extracranial vasodilation
occurs in affected part of face.
• Trigeminal nerve is
implicated.
69

11/7/2016
24
Cluster Headache
Clinical Manifestations
• Sharp stabbing
• Intense pain typically lasting from a few
minutes to 3 hours
• Pain is usually located around the eye,
radiating to the temple, forehead, cheek, nose,
or gums.
• Swelling around the eye, Constriction of the
pupil
• Facial flushing or pallor70
70
Cluster Headache
Clinical Manifestations
• During the headache, patient is often agitated and
restless.
• Headaches occur with regularity.
• Usually occur at same time of day
• Typically last daily for 2 weeks to 3 months, then
into remission for months or years
� Apply 6-8 liters O2 as a first priority.
71
71
Cluster Headache
Diagnostic Studies
• Diagnosis may be based primarily on
history.
• Headache diaries are helpful.
• CT scan, MRI, or MRA may be performed
to rule out aneurysm, tumor, or infection.
72
72

11/7/2016
25
Headache
Other Types
• Can be first symptom of a more serious illness
• Can accompany subarachnoid hemorrhage; brain
tumors; other intracranial masses; arteritis;
vascular abnormalities; trigeminal neuralgia;
diseases of the eyes, nose, and teeth; and
systemic illness
73
73
74
As we consider drugs for headache, keep three basic principles
in mind:
• First, anti-headache drugs may be used in two ways…to abort an
attack or to prevent an attack.
• Second, not all patients with a particular type of headache
respond to the same drugs and therefore treatment must be
individualized.
• Third, several of the drugs employed to treat severe headaches
can cause physical dependence
The objective of abortive therapy is to eliminate
headache pain and suppress nausea and vomiting.
�Treatment should begin at the earliest sign of attack.
�Route: rectally, injection, inhalation.
�Drug selection depends on intensity of attack.
�Use of abortive meds should be limited to 1-2 days
per week.
Abortive Therapy

11/7/2016
26
Tension Headache
DRUG THERAPY• Aspirin
• Acetaminophen
• Nonsteroidal anti-inflammatory drugs (NSAIDS)
• Sedative
• Muscle relaxant
• Tranquilizer
Decrease Reoccurrence
�Tricyclic antidepressant (elavil, nortriptyline)
�Topiramate (topamax)
�Divalproex (depakote)
�Mirtazapine (Remeron) 76
• Used with severe migraine that has not responded to first-line
medications.
• Examples: Meperidine (Demerol),and Butorphanol (Stadol)
nasal spray.
• Disadvantages of Demerol versus Stadol:
• Adverse effects of Demerol are the 6 D’s
� Depressed respirations
� dizzy
� Drowsy
� Drug dependence
� Decreased blood pressure
� Decreased GI peristalsis & urine output
Opioid Analgesics
• Mechanism of action providing relief: unknown.
• Possible mechanism of action: act as serotonin agonists,
resulting in a vasoconstriction effect = decrease blood
flow to area and decreases painful pulsations. Also
possibly blocks inflammation.
• Therapeutic uses: drug of choice to stop an ongoing
migraine. Also used to treat cluster headaches that are
characterized by tearing, rhinnorhea, sharp on sided pain
from neck to temporal area.
• Risk of dependency…should not be taken on a daily basis
for a long time.
Ergot Alkaloids
11/7/2016
27
• Drug therapy to prevent migraines.
• Goal of therapy: to reduce the frequency and intensity
of migraine attacks.
• Indicated for patients who have not responded
adequately to abortive therapy and for patients whose
attacks are frequent or especially severe.
• Examples: beta blockers (Inderal used most often),
antiepileptic drugs (Depakote, Topramax), Tricyclic
(amitriptyline), Calcium Channel blocker (verapamil,
Calan), and estrogens (for menstrual migraines).
Preventive Therapy
Migraine Headache
Drug Therapy• NSAIDs
• Aspirin
• Caffeine-containing combination analgesics
� triptans have become the first line of therapy
� sumatriptan (Imitrex) affect selected serotonin receptors
Drug Alert
Sumatriptan (Imitrex)
• Should not be given to patients with the following:
•History or manifestations of ischemic cardiac, cerebrovascular, or peripheral vascular problems
•Uncontrolled hypertension, since it may increase blood pressure
• Excess dosage may produce tremor and decrease respirations. 80
�Therapeutic uses:
• To abort ongoing migraine attacks.
• Relieves pain, nausea, photophobia, phonophobia.
• Effects begin in 15 minutes after SC or IN, and 30-60 minutes
after PO
• 40% of patients have return of HA within 24 hours.
�Adverse effects:
• Generally well tolerated. Coronary vasospasm biggest concern.
• Sumatriptan should be avoided during pregnancy.
• Others include dizziness, malaise, vertigo, tingling, warm/hot
sensation, chest symptoms including heaviness, pressure,
tightness, angina, and injection site reaction.
Sumatriptan

11/7/2016
28
• Drug interactions:
• Do not give with any other drug causing vasoconstriction unless
discontinued for 24 hours.
• MAOI’s cause decreased metabolism of Imitrex, Zomig, and Maxalt.
Preparations:
prefilled SQ syringes
stat-dose pen
Oral/PO
Nasal spray
Sumatriptan
SUMATRIPTAN (IMITREX)
I schemic heart disease
Maoi’s may lead to MAOI toxicity
Iintial dose evaluate B/P 1 hr before and after administration
Teach to use adequate contraception during therapy
Remind to allow 1 hr between doses; no > than 2 doses in 24hrs
Evaluate EKG for changes if angina occurs
X outa migraine headache-not just to prevent headaches83
• Drug therapy to prevent migraines.
• Goal of therapy: to reduce the frequency and intensity
of migraine attacks.
• Indicated for patients who have not responded
adequately to abortive therapy and for patients whose
attacks are frequent or especially severe.
• Examples: beta blockers (Inderal used most often),
antiepileptic drugs (Depakote, Topramax), Tricyclic
(amitriptyline), Calcium Channel blocker (verapamil,
Calan), and estrogens (for menstrual migraines).
Preventive Therapy

11/7/2016
29
Beta Blocker Propranolol
BLOCKER – 5 B’s
BRADYCARDIA
BLOOD PRESSURE – TOO LOW
BRONCHIAL CONSTRICTION
BLOOD SUGAR – MASK LOW
BLOCKS (HEART) > 1ST DEGREE
85
Headache
Nursing Management
• Nursing assessment
• Health history
• Seizures, cancer, stroke, trauma, asthma or allergies, mental illness, stress, menstruation, exercise, food, bright lights, noxious stimuli
• Medications
• Surgery and other treatments
• Specific details about the headache
• Objective data
• Anxiety or apprehension
• Diaphoresis, pallor, unilateral flushing with cheek edema, conjunctivitis
86
86
Headache
Nursing Management
• Nursing diagnoses
• Acute pain
• Anxiety
• Hopelessness
87
87

11/7/2016
30
Headache
Nursing Management
• Planning
• Have decreased or no pain
• Experience increased comfort and reduced anxiety
• Demonstrate understanding of triggering events and treatment strategies
• Use positive coping strategies to deal with chronic pain.
• Experience ↑ quality of life88
88
Headache
Nursing Management
• Nursing implementation
• Daily exercise, relaxation, and socializing help
reduce recurrence.
• Suggest alternative pain management such as
relaxation, meditation, yoga, and self-hypnosis.
• Massage and heat packs.
• *Oxygen therapy for cluster headaches
89
89
Headache
Nursing Management
• Nursing implementation (cont’d)
• Patient should make a written note of
medications to prevent accidental overdose.
• Teach patient about prophylactic treatment.
• Dietary counseling for food triggers
• Avoid smoking and smoke exposure and other
environmental triggers.
90
90

11/7/2016
31
SEIZURES AND
SEIZURE DISORDER (EPILEPSY)
�DEFINITION : �Seizure: Paroxysmal, uncontrolled
electrical discharge of neurons in the brain, interrupting normal function.
�Epilepsy or seizure disorder : Is the condition in which a person has reoccurring seizures due to an underlying, chronic condition.
�PATHOLOGY : Causes can be intracranial,
extracranial, metabolic, and genetic.
RISK FACTORS
• Decreasing in children and increasing in
the elderly.
• Males are more likely to develop disorder
than females.
• Persons with traumatic brain injury and
stroke are at high risk.
Algorithm
Classification of Seizures
Fig. 59-2. Algorithm for classification of seizures.

11/7/2016
32
Seizures Phases
�Prodromal phase
�Aural phase
� Ictal phase
�Postictal phase
Absence Seizures• Formerly called petit mal or lapses
• Brief loss of consciousness
• Minimal or no change in muscle tone
**Almost always appear in childhood
(4 to 12 years old)
PARTIAL SEIZURE

11/7/2016
33
TONIC/CLONIC PHASES
Febrile Seizures
• Transient disorder of childhood
• Affect approximately 3% to 8% of children
• Usually occur between ages 6 months and
3 years
• Rare after age 5
• Twice as frequent in males
98
Complications � Status epilepticus is state of constant seizure or
condition when seizures recur in rapid
succession without return to consciousness
between seizures.
� Neurologic emergency
� Can involve any type of seizure
� Neurons become exhausted and cease to
function.
� Permanent brain damage can result.
�Other complications.

11/7/2016
34
Diagnostic Studies
� Table 59-7 Page 1422 Collaborative Care
� Accurate, comprehensive description of seizures
with patient’s health history
� EEG
� Labs
� Radiology
� MANAGEMENT
� Goals
� Principles of drug therapy
� Care during/after seizure
� Review Care Plans
Nursing AssessmentAssessment
1.Seizure history
2.Type of seizure
3.Occurrences before, during, and after the seizure
4.Prodromal signs, such as mood changes, irritability, and
insomnia
5.Aura: Sensation that warns the client of the impending
seizure
6.Loss of motor activity or bowel and bladder function or loss
of consciousness during the seizure
7.Occurrences during the postictal state, such as headache,
loss of consciousness, sleepiness, and impaired speech or
thinking
102

11/7/2016
35
Nursing Interventions1. Note the time and duration of the seizure.
2. Assess behavior at the onset of the seizure: If the client has experienced an aura, if a change in facial expression occurred, or if a sound or cry occurred from the client
3. If the client is standing or sitting, place the client on the floor and protect the head and body.
4. Support the ABCs—airway, breathing, and circulation.
5. Administer oxygen.
6. Prepare to suction secretions.
7. Turn the client to the side to allow secretions to drain while maintaining the airway.
8. Prevent injury during the seizure.
9. Remain with the client.
10. Do not restrain the client.
103
Nursing Interventions Cont’11. Loosen restrictive clothing.
12. Note the type, character, and progression of the movements during the seizure.
13. Monitor for incontinence.
14. Administer intravenous medications as prescribed to stop the seizure.
15. Document the characteristics of the seizure.
16. Provide privacy, if possible.
17. Monitor behavior following the seizure, such as the state of consciousness, motor ability, and speech ability.
18. Instruct the client about the importance of lifelong medication and the need for follow-up determination of medication blood levels.
19. Instruct the client to avoid alcohol, excessive stress, fatigue, and strobe lights.
20. Encourage the client to contact available community resources, such as the Epilepsy Foundation of America.
21. Encourage the client to wear a Medic-Alert bracelet.
104
If the client is having a seizure,
maintain a patent airway. Do
not force the jaws open or place
anything in the client’s mouth. 105

11/7/2016
36
Antiepileptic Drugs
107
108

11/7/2016
37
Therapeutic Goal: to reduce seizures to an extent that
allows the patient to live a normal/near normal life.
�Drugs can benefit 60-70% of patients.
�Noncompliance is a nursing problem because
treatment is continuous and not curative.
�Monitoring plasma drug levels
�Withdrawing antiepileptic drugs
Antiepileptic
Antiepileptic Drugs
Classifications:
• Traditional AED’s (such as Tegretol, Dilantin)
• Newer AED’s (such as Neurontin, Lyrica, Topamax)
KEY: Neither group is superior to the other, so drugs
from both groups must be considered when selecting
appropriate pharmacological therapy.
110
Phenytoin (Dilantin): Tonic-Clonic Seizures
• Most widely used AED. Used PO and IV.
• Suppresses seizures without depressing the entire CNS.
• Absorption varies greatly among patients…dosage must be highly individualized.
• Small changes in dosage can cause disproportionately large changes in serum drug levels, thus producing toxicity.
• Half-life varies in relation to dosage (lower dose has shorter half-life of 8 hours where a higher dose can have a half-life of up to 60 hours).
• Therapeutic uses: epilepsy, digoxin induced dysrhythmias.
Traditional Antiepileptic Drugs

11/7/2016
38
• At therapeutic levels (10-20), sedation and other CNS
symptoms are mild.
• At levels above 20, toxicity can occur with nystagmus,
sedation, ataxia, diplopia, and cognitive impairment.
• Others: gingival hyperplasia, skin rash, hypotension,
dysrhythmias, gastric upset.
• Must gradually withdraw drug.
Phenytoin (Cont.)
• Regular and meticulous mouth care.
• Narrow therapeutic index.
• IV administration: give slowly, do not add to an
existing IV solution, and flush before and after with NS.
• Recommended administration: 50 mg over 1 minute
or so. Giving faster may cause cardiovascular collapse
Phenytoin (Cont.)
NURSING Interventions�Tube feedings may interfere with the absorption of the enteral
form of phenytoin and diminish the effectiveness of the medication; therefore, feedings should be scheduled as far as possible away from the time of phenytoin administration.
�Monitor therapeutic serum levels to assess for toxicity.
�Monitor for signs of toxicity.
�When administering phenytoin intravenously, dilute in normal saline because dextrose causes the medication to precipitate.
�When administering phenytoin intravenously, infuse with an inline filter and no faster than 25 to 50 mg/minute; otherwise, a decrease in blood pressure and cardiac dysrhythmias could occur.
�Assess for ataxia (staggering gait).
�Instruct the client to consult with the HCP before taking other medications to ensure compatibility with anticonvulsants.
114

11/7/2016
39
DILANTIN
Gingival hyperplasia
Use alternate birth control
Mouth care-preventative dental
Soft toothbrush, don’t stop abruptly
115
Adverse effects of PHENYTOINP Plasma level monitoring needed because of its zero order
kinetics
H Hypertrophy of gums, can be minimized by good oral hygiene
E Enzyme induction so interacts with many drugs including other antiepileptics
N Neutropenia and other hypersensitivity reactions
Y Young girls beware! Causes hirsutism, coarsening of facial features and acne
T Teratogenic, married girls beware! Causes Fetal HydantoinSyndrome
O Osteomalacia due to interference with calcium absorption
I Interference with folate absorption leads to megaloblastic anemia
N Neurological manifestations at higher doses: Ataxia, vertigo, headache and nystagmus
116
117
Phenytoin must be given slowly to
prevent hypotension and cardiac
dysrhythmias. Also, it may decrease the
effectiveness of some birth control pills
and may cause teratogenic effects, if
taken during pregnancy.

11/7/2016
40
• Used to treat tonic-clonic, and partial but not absence. Also can be used in treatment of bipolar disease and neuralgias.
• Therapeutic levels: 5-12
• Adverse effects:
• Bone marrow suppression (rare) such as aplastic anemia, leukopenia, anemia, thrombocytopenia, agranulocytosis.
• Birth defects (cleft palate, growth retardation).
• Hypo-osmolarity
• Photosensitivity, rash, SJS
Carbamazepine (Tegretol)
Stevens–Johnson Syndrome
119
Adverse effects (Cont.)
• Minimal effect of cognitive ability
• Others: visual disturbances, ataxia, vertigo, unsteadiness, HA especially in the first weeks of treatment with tolerance developing with continued use.
• Grapefruit juice can increase the peak and trough levels by 40%!
Carbamazepine (Tegretol)

11/7/2016
41
TEGRETOL
Trigeminial neuralgia, tonic clonic seizures
Evaluate for anorexia, nausea, dizziness sedation, HA, sore throat
Give with food, milk to GI distress
Review levels, maintain 4-12mcg/ml
Evaluate for anorexia-indicate toxic level
Tablet-chewable, do not swallow whole
Open & mix with food (extended capsule)
Look for other drug interactions 121
122
• Used to treat all major seizure types.
• Widely used.
• Therapeutic levels: 50-100
• GI upset is common (transient N/V) so take with food or use enteric coated formulation.
• Severe adverse effects are limited to rare cases of severe hepatotoxicity (usually first few months of therapy and in children less than 2 years old)and pancreatitis (soon after starting or years later).
Valproic Acid (Depakote,
Depakene)

11/7/2016
42
• Valproic acid is highly teratogenic.
• Hyperammonemia (if combined with Topamax).
• Will also potentiate levels of Dilantin and phenobarbital.
• Others: (not common) rash, weight gain, hair loss,
tremor, blood dyscrasias)
• Also used to treat bipolar disorder and prevention of
migraine.
Valproic Acid (Depakote,
Depakene) (Cont.)
125
Adverse effects of VALPROICV Vomiting, Nausea
A Alopecia
L Liver toxicity (Hepatoxicity)
P Pancreatitis
R Rashes & thrombocytopenia are rare
hypersensitivity reactions
O Oedema
I Ingestion
C Cell count will decrease, platelet & wbc =
Blood Dyscrasias
• One of our oldest drugs used for epilepsy.
• Therapeutic levels: 15-45
• Unfortunately, can cause significant lethargy, depression,
learning impairment.
• Largely replaced by newer drugs.
Phenobarbital (Luminal)

11/7/2016
43
Adverse effects: drowsiness (tolerance will develop),
depression, confusion and agitation in the elderly, physical
dependence.
• When phenobarbital is withdrawn, dosage should be
reduced gradually.
• If administering IV, give slowly. If done too fast, excessive
CNS depression may result.
• Monitor BP during IV infusion.
Phenobarbital (Luminal)
(Cont.)
Antiseizure Medications
128
• Better tolerated.
• Smaller risk to developing fetus.
• Examples: Trileptal, Topamax, Keppra, Lamictal,
Neurontin, Lyrica.
• Most recommended for adjunctive therapy versus
monotherapy (Trileptal/monotherapy).
Newer Antiepileptic Drugs

11/7/2016
44
• Lyrica also widely used for neuropathic pain and
fibromyalgia.
• Unlike most other anti-seizure agents, Lyrica is regulated
under the Controlled Substance Act (schedule V).
Newer Antiepileptic Drugs (Cont.)
Benzodiazepines
Benzodiazepines are used to treat absence seizures.
�Clonazepam (Klonopin)
�Clorazepate (Tranxene)
�Diazepam (Valium)
�Lorazepam (Ativan)
Side/adverse effects
a. Sedation, drowsiness, dizziness, blurred vision
b. For intravenous injection, administer slowly to prevent bradycardia.
c. Medication tolerance and drug dependency
d. Blood dyscrasias: Decreased platelet count and decreased white blood cell count
e. Hepatotoxicity
131
132
Flumazenil (Romazicon) reverses
the effects of benzodiazepines. It
should not be administered to
clients with increased intracranial
pressure or status epilepticus who
were treated with benzodiazepines
because these problems may recur
with reversal.

11/7/2016
45
DEGENERATIVE DISEASES
• CHARACTERISTICS
�MS
�Parkinson’s
�Myasthenia Gravis
133
MULTIPLE SCLEROSIS
• ETIOLOGY/PATHOPHYSIOLOGY
134
MS: MYELIN LOSS
135
� Initially, the myelin sheaths of the neurons in the brain
and spinal cord are attacked, but the nerve fiber is not
affected.
� Patient may complain of noticeable impairment of
function.
� Myelin can be replaced by glial scar tissue.
� Nerve impulses slow down without myelin.

11/7/2016
46
Risk Factors for Multiple
Sclerosis�Infection
�Smoking
�Physical injury
�Emotional stress
�Excessive fatigue
�Pregnancy
�Poor state of health
�Pathogenic agents(controversial)
136
137
Early Multiple Sclerosis
Diagnosis
138

11/7/2016
47
MRI of the Brain/MS Plaque
139
MRI of the Brain Scan
140
Chronic Multiple Sclerosis
141
141
Fig. 59-4. Chronic multiple sclerosis. Demyelination plaque (P) at gray-white junction and
adjacent partially remyelinated shadow plaque (V).

11/7/2016
48
142
Multiple Sclerosis
143
144

11/7/2016
49
Clinical Manifestations
• Common signs and symptoms include
�Motor problems
• Weakness or paralysis of limbs, trunk, and head
• Diplopia
• Scanning speech
• Spasticity of muscles
�Sensory problems
• Numbness and tingling
• Blurred vision
• Vertigo and tinnitus
• ↓ hearing
• Chronic neuropathic pain 145
Clinical Manifestations�Cerebellar problems
• Nystagmus
• Ataxia
• Dysarthria
• Dysphagia
�Cognitive problems
• Short-term memory attention
• Information processing
• Visual perception
• Word finding
�Emotional problems
• Anger
• Depression
• Euphoria
� Other Physical
�Spastic bladder, retention or flaccid bladder may occur
Diagnostic Testing
• Based primarily on history, clinical
manifestations, and presence of multiple lesions
over time measured by MRI
• Cerebral spinal fluid (CSF) analysis
• ↑ in oligoclonal immunoglobulin G
• Contains higher numbers of lymphocytes and
monocytes
147
11/7/2016
50
DRUG THERAPYThe initial treatment of MS is the use of immunomodulator drugs to modify the disease progression and prevent relapses.
β-Interferon
�Avonex*
�Betaseron*
�Rebif*
�Copaxone
�Aubagio
** Drug Alert
• Rotate injection sites with each dose.
• Assess for depression, suicidal ideation.
• Wear sunscreen and protective clothing while exposed to sun.
• Know that flu-like symptoms are common after initiation of therapy.
148
Drug Therapy for Active and
Aggressive forms of MS
�Tysabri (Natalizumab)
�Novantrone (Mitoxantrone)
149
150

11/7/2016
51
Drugs for Symptom
ManagementCholinergics� bethanechol (Urecholine)
� neostigmine (Prostigmin)
Anticholinergics� propantheline (Pro-Banthine)
� oxybutynin (Ditropan)
Muscle Relaxants� diazepam (Valium)
� baclofen (Lioresal)
� dantrolene (Dantrium)
� tizanidine (Zanaflex)
151
Anticholinergic Medications
152
Cholinergic Overdose
This is an example of a mnemonic that is commonly used in the
real world to diagnose cholinergic overdose
Diarrhoea
Urination
Miosis/muscle weakness
Bronchorrhea
Bradycardia
Emesis
Lacrimation
Salivation/sweating 153

11/7/2016
52
Nursing Assessment
Subjective data
�Health history
�Viral infections or vaccinations
�Residence in cold or temperate climates
�Physical and emotional stress
�Medications
�Elimination problems
�Weight loss, dysphagia
�Anger, depression, euphoria, isolation
�Presence of frequent UTI or incontinence154
154
Nursing Assessment
Objective Data:
�Apathy, inattentiveness
�Pressure ulcers
�Scanning speech
�Tremor
�Nystagmus
�Ataxia
�Spasticity
155
155
Nursing Assessment
Objective Data (con’t):
�Hyperreflexia
�↓ hearing
�Muscular
�Weakness
�Paresis
�Paralysis
�Foot dragging
�Dysarthria 156

11/7/2016
53
Managing Relapse of MS
The most common treatment regimen is:
� a three-to-five-day course of high-dose
�intravenous corticosteroids to reduce inflammation and end
the relapse more quickly (Solu-Medrol)
�followed with a slow taper of oral prednisone (Deltasone)
�H.P. Acthar Gel
• Given to PATIENTS who are unable to cope with the side effects of
high-dose corticosteroids,
• have been treated unsuccessfully with corticosteroids
• do not have access to intravenous therapy
• have trouble receiving medication intravenously because of
difficulty accessing the veins.157
Nursing Diagnosis, Planning and
Implementation
�Impaired physical mobility
�Impaired urinary elimination
�Interrupted family processes
�Ineffective self-health management
158
PARKINSON’S DISEASE
159

11/7/2016
54
Etiology and Pathophysiology
• Diagnosis increases with age, with peak onset in the seventh decade.
• More common in men, ratio of 3:2
• Other causes of parkinsonism
• Encephalitis lethargica (type A encephalitis) has been associated with onset.
• Incidence has dwindled since 1920s.
• Symptoms have occurred after intoxication with a variety of chemicals.
160
Parkinson’s Disease (PD)
• Disease of basal ganglia
characterized by
• Slowing down in the initiation and execution
of movement
• ↑ muscle tone
• Tremor at rest
• Gait disturbance
161
162

11/7/2016
55
Clinical Manifestations
• Onset is gradual and insidious.
• Classic triad of PD
• Tremor
• Rigidity
• Bradykinesia
• Beginning stages may involve only mild tremor, slight limp, or ↓ arm swing.
• Later stages may have shuffling, propulsive gait with arms flexed, and loss of postural reflexes.
163
Clinical Manifestations
�Tremor
�So minimal initially that only the patient may
notice it
�More prominent at rest and is aggravated by
emotional stress or ↑ concentration
�Described as pill rolling because thumb and
forefinger appear to move in rotary fashion
�Benign essential tremor, which occurs during
voluntary movement, has been misdiagnosed as
Parkinson’s disease (PD). 164
Clinical Manifestations
• Rigidity
• Increased resistance to passive motion.
• Typified by a jerky quality when the joint
is moved.
Caused by sustained muscle contraction and consequently
elicits the following:
• Complaint of soreness
• Feeling tired and achy
• Pain in the head, upper body, spine, or legs
• Inhibits the alternating contraction and relaxation in
opposite muscle groups.165
165
11/7/2016
56
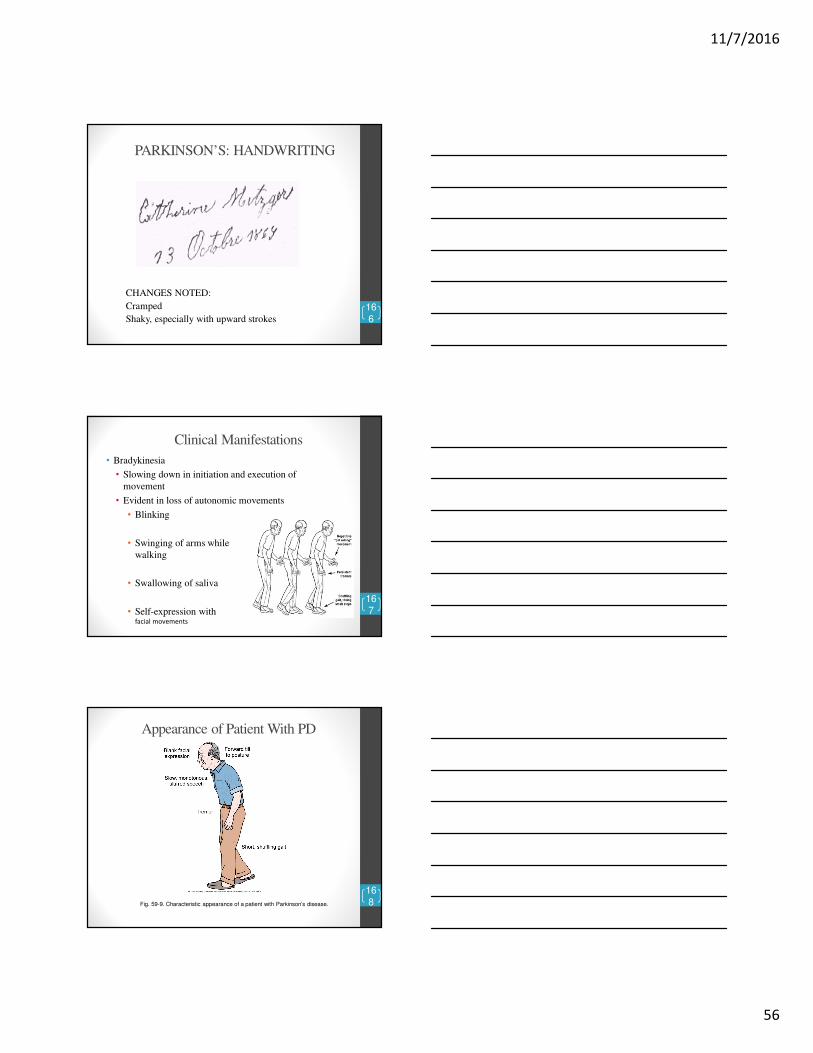
PARKINSON’S: HANDWRITING
CHANGES NOTED:
Cramped
Shaky, especially with upward strokes
166
Clinical Manifestations
• Bradykinesia
• Slowing down in initiation and execution of
movement
• Evident in loss of autonomic movements
• Blinking
• Swinging of arms while
walking
• Swallowing of saliva
• Self-expression with facial movements
167
167
Appearance of Patient With PD
168
168
Fig. 59-9. Characteristic appearance of a patient with Parkinson’s disease.
11/7/2016
57
Complications
• Non-motor symptoms
• Depression
• Anxiety
• Impotence
• Short-term memory
impairment
• Sleep disorders are common and potentially
severe.
• Effective management of sleep disturbances can
greatly improve quality of life. 169
169
• Apathy
• Fatigue
• Pain
• Constipation
Complications
• As disease progresses, complications increase
�Motor symptoms
�Weakness
�Akinesia
�Neurologic problems
�Neuropsychiatric problems
• Dementia occurs in 40% of patients.
170
Complications
• Dysphagia may result in malnutrition and
aspiration.
• General debilitation may lead to
pneumonia, UTIs, and skin breakdown.
• Orthostatic hypotension may occur.
• Could result in falls and injuries171

11/7/2016
58
NOW…
• A CLIENT IS
DIAGNOSED WITH
PARKINSON’S
DISEASE. WHAT
PROBLEMS DO
YOU ANTICIPATE?
172
Diagnostic Tests
• No specific tests
• Diagnosis based solely on history and
clinical features
• Firm diagnosis can be made when at least
two of three characteristics of the classic
triad (tremor, rigidity, and bradykinesia)
are present.
173
173
174

11/7/2016
59
Collaborative Care
Drug Therapy
• Aimed at correcting imbalances of
neurotransmitters within the CNS
• Antiparkinsonian drugs either
�Enhance or release supply of DA
�Antagonize or block the effects of overactive
cholinergic neurons in the striatum
• Levodopa with carbidopa (Sinemet) is often the
first drug used.
175
175
Collaborative Care
Drug Therapy
• Anticholinergics are also used in management.
�↓ activity of acetylcholine
• Antihistamines with anticholinergic or β-adrenergic blockers are used to manage tremors.
• Antiviral agent amantadine is effective, although exact mechanism is unknown.
• MAO-B inhibitors, selegiline, and rasagiline (Azilect) may be combined with Sinemet.
• Entacapone and tolcapone block the enzyme that breaks down levodopa in the peripheral circulation.�Prolong the effects of Sinemet 17
6
176
Collaborative Care
Drug Therapy
• Within 3 to 5 years of treatment, patients experience episodes of hypomobility.
• Treated with apomorphine (Apokyn)
�MUST NOT BE taken with an antiemetic drug
• Aricept is used to treat Parkinson’s dementia.
• Elavil may be used to treat depression. 177
177

11/7/2016
60
Nursing Interventions
1. Assess neurological status.
2. Assess ability to swallow and chew.
3. Provide high-calorie, high-protein, high-fiber soft diet with
small, frequent feedings.
4. Increase fluid intake to 2000 mL/day.
5. Monitor for constipation.
6. Promote independence along with safety measures.
7. Avoid rushing the client with activities.
8. Assist with ambulation and provide assistive devices.
9. Instruct the client to rock back and forth to initiate
movement. 178
Nursing Interventions Cont’d10. Instruct the client to wear low-heeled shoes.
11. Encourage the client to lift feet when walking and to avoid prolonged sitting.
12. Provide a firm mattress and position the client prone, without a pillow, to facilitate proper posture.
13. Instruct in proper posture by teaching the client to hold the hands behind the back to keep the spine and neck erect.
14. Promote physical therapy and rehabilitation.
15. Administer antiparkinsonian medications to increase the level of dopamine in the CNS.
16. Instruct the client to avoid foods high in vitamin B6 because they block the effects of antiparkinsonian medications.
17. Instruct the client to avoid monoamine oxidase inhibitors because they will precipitate hypertensive crisis.
179
Parkinson’s Disease• Goal of treatment: to improve the patients
ability to carry out activities of daily living.
• Drugs do not cure, but will treat symptoms
of the disorder.
• Two types of agents used for this:
• Dopaminergic agents (drugs that either
directly or indirectly activate dopamine
receptors).
• Anticholinergic Agents (drugs that block
receptors for acetylcholine).

11/7/2016
61
Levodopa• Introduced in 1960’s
• Stimulates dopamine production or increases sensitivity of dopamine receptors.
• A “prodrug”: no effect orally until it is converted to dopamine once in the body. This process is facilitated by an enzyme decarboxylase and enhanced by pyridoxine (vitamin B6).
• Very effective (if drug not effective, diagnosis of Parkinson's disease should be questioned).
• Beneficial effects diminish over time.
• Most troubling side effect: dyskinesias.
• Full therapeutic effects may take several weeks or months (6) to develop. Patients should be informed that beneficial effects are likely to increase steadily over the first few months.
• Symptoms usually well controlled for 2 years; at end of 5 years, back to pretreatment level (one reason it is reserved for patient’s that have been treated with other agents in the initial stages of Parkinson’s).
Levodopa continues…Acute loss of effect:
• Occurs in 2 patterns:
• 1. Gradual loss – “wearing off”
developing near the end of the dosing
interval when drug levels have declined
to a sub therapeutic level. May be
minimized by shortening the dosing
interval, and giving a drug that prolongs
levodopa’s half-life (Comtan), and giving a
direct-acting dopamine agonists
(Mirapex, Requip, Parlodel).
Levodopa….2. Abrupt loss of effect
• Often referred to as the “on-off” phenomenon.
• Can occur at any time during the dosing interval.
• “Off” times may last from minutes to hours and are
likely to increase in both intensity and frequency as
treatment continues.
• The patient has and abrupt loss of effect.
• Avoiding high-protein meals may help (amino acids
compete with levodopa for intestinal absorption)
(page 185).

11/7/2016
62
Levodopa…
Drug holiday:
• Defined as a brief (i.e.10 day) interruption
of treatment.
• When holiday is successful, beneficial
effects are achieved with lower doses, and
therefore the incidence of dyskinesias and
psychosis is lowered as well.
• Drug holidays do not eliminate “off” times.
• These holidays are dangerous and must
take place in a hospital.
Levodopa….Adverse effects:
• Nausea and vomiting: common. May be helped if administered with food
(watch protein).
• Dyskinesias: in 80% of patients..Ironic. Develop just before or soon after
optimal levodopa dosage has been achieved. May be head bobbing, tics,
grimacing, or ballismus (uncoordinated swinging of the limbs and jerky
movements), choreoathetosis (irregular involuntary movements giving the
appearance of restlessness).
• CV effects: postural hypotension (especially early in treatment. May be
helped by increasing intake of salt and water, or by an alpha-adrenergic
agonists).
• Psychosis (manifested initially by hallucinations): in 20% of patients. May
be reduced by lowering dosages, but this will also decrease beneficial
effects too. Clozaril and Seroquel used to treat symptoms. Why wouldn’t
traditional antipsychotics be used???
• Others: dark sweat and urine (harmless but patients need to be told),
activation of malignant melanoma and therefore should be avoided in
patients with undiagnoses skin lesions.
Levodopa/Carbidopa
• Brand names: Sinemet and Paracopa .
• Combination of levodopa and carbidopa.
• The addition of carbidopa results in the most effective
therapy for PD..much more effective than levodopa
alone.
• Carbidopa enhances the effects of Levodopa by
increasing the amounts of dopamine available in the
brain. How?? By inhibiting peripheral conversion of
dopamine in the periphery, more levodopa will be
converted to dopamine in the brain.
• Carbidopa has no effect on its own.
• Vitamin B6 not a problem.
11/7/2016
63
Levodopa/Carbidopa
Advantages:
• Because carbidopa increases levels of dopamine in
the brain, dosages of levodopa can be reduced by
about 75%.
• Cardiovascular responses to levodopa are reduced
as well as nausea and vomiting.
• By causing direct inhibition of decarboxylase,
carbidopa eliminates concern about decreasing the
effects of levodopa by taking vitamin preparations
that contain vitamin B6.
Dopamine Agonists• Act to directly activate dopamine receptors in the brain.
• For patients with mild or moderate symptoms, these are drugs
of first choice.
• Advantages: not dependent on conversion by enzymes to be
active, don’t compete with dietary proteins, lower incidence
of response failures, and are less likely to cause disabling
dyskinesias.
• Disadvantage: cause more serious SE’s, like hallucinations,
day-time sleepiness, and postural hypotension.
• Usually reserved for younger patients, who tolerate their side
effects better than do the elderly.
• Examples: Mirapex, Requip, Permax, Parlodel.
Dopamine Agonist
Renal impairment
Extrapyramidal symptoms
Seeing things (hallucinations)
Thirsty (dry mouth)
Lethargy
Express concern of falling asleep during activity
Sickness (nausea)
Stuck up (constipation) 189

11/7/2016
64
Other agents used to treat Parkinson’s
Disease• Anticholinergic agents: Cogentin, Artane (how would these
work and what would be their side effects????). Used for
younger patients with mild symptoms. Usually avoided in the
elderly because of CNS side effects (sedation, confusion,
hallucinations).
• Antiviral agent: Symmetrel (not considered a first-line drug
because responses begin to diminish within 3-6 months).
• MAO-B inhibitor: Eldepryl (MOA remember inactivates
catecholamine's in the brain, such as dopamine).
Collaborative Care
• Surgical therapy
• Procedures aimed at relieving symptoms
• Used in patients who are usually unresponsive to drug therapy or have developed severe motor complications
• Ablation surgery
• Has been used to treat PD for over 50 years
• But has been recently replaced by deep brain stimulation (DBS) 19
1
191
Collaborative Care
• Deep brain stimulation
�Involves placing an electrode in the thalamus,
globus pallidus, or subthalamic nucleus
�Connected to a generator placed in the upper chest
�Device is programmed to a to deliver specific
current to targeted brain
location.
192
192

11/7/2016
65
Collaborative Care
• Transplantation of fetal neural tissue into the basal
ganglia provides DA-producing cells in the brains
of patients.
�Still in experimental stages
193
193
Collaborative Care
• Nutritional therapy
�Malnutrition and constipation can be serious
consequences.
�Patients with dysphagia and Bradykinesia need
food that is easily chewed and swallowed.
�Adequate roughage
194
194
NURSING CARE OF THE CLIENT
WITH PD: MOBILITY
• PROMOTE EXERCISE
• MAINTAIN SAFETY
• USE ADAPTIVE DEVICES
195

11/7/2016
66
NURSING CARE OF THE CLIENT
WITH PD: NUTRITION
• AID SWALLOWING
• OFFER APPROPRIATE FOODS
• USE ADAPTIVE DEVICES
196
197
MYASTHENIA GRAVIS
• DEFINITION
• INCIDENCE
• PATHOLOGY
• MANIFESTATIONS
198
11/7/2016
67
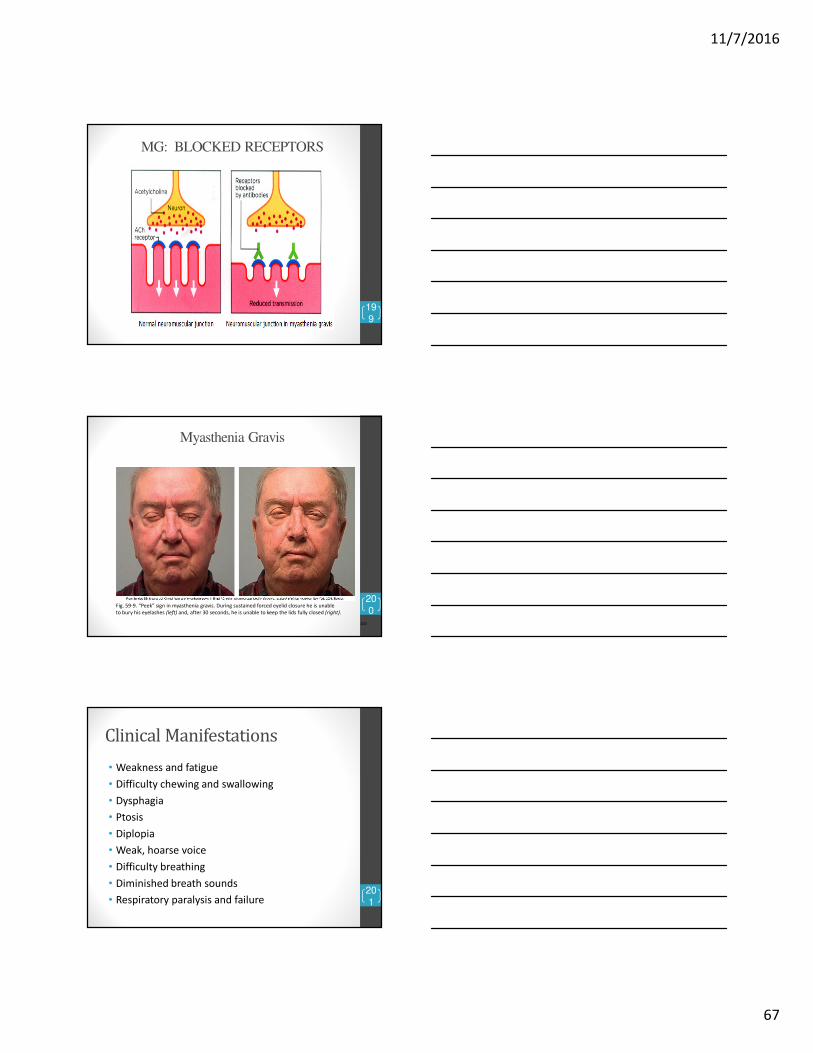
MG: BLOCKED RECEPTORS
199
Myasthenia Gravis
200
200
Fig. 59-9. “Peek” sign in myasthenia gravis. During sustained forced eyelid closure he is unable
to bury his eyelashes (left) and, after 30 seconds, he is unable to keep the lids fully closed (right).
Clinical Manifestations
• Weakness and fatigue
• Difficulty chewing and swallowing
• Dysphagia
• Ptosis
• Diplopia
• Weak, hoarse voice
• Difficulty breathing
• Diminished breath sounds
• Respiratory paralysis and failure201

11/7/2016
68
HORNER’S SYNDROME
• Unilateral:
• Ptosis
• Tearing
• Rhinitis
• Pupillary constriction202
MYASTHENIA GRAVIS
• DIAGNOSIS
• H & P
• Sustained force test
• Labs
• EMG
203
Tensilon (edrophonium chloride) Test
• The Tensilon test is an injection.
• Tensilon blocks the action of acetylcholinesterase.
• To stimulate a muscle, a nerve cell (neuron) releases
acetylcholine.
• To prevent prolonged muscle response to a single nerve signal,
acetylcholine is broken down by acetylcholinesterase after the
muscle is stimulated.
• The Tensilon test involves the IV injection of a small amount
of Tensilon.
• The needle is left in place. If no adverse reaction is observed
within 30 seconds, an additional volume is injected.
• Results are apparent within one minute.204

11/7/2016
69
205
Anticholinesterase drugs
Prostigmin
Mestinon
Mytelase
Corticosteroids
206
MYASTHENIA GRAVIS:
FOCUS ON TEACHING
• MEDICATION
• SAFETY
• LIFESTYLE ADJUSTMENTS
• CRISIS MANAGEMENT
207

11/7/2016
70
MYASTHENIA GRAVIS:
CRISIS MANAGEMENT
• MYASTHENIC CRISIS
• An acute ↑ in requirement for anticholinesterase therapy
• Symptoms
• Response
• CHOLINERGIC CRISIS
• An acute ↓ in the need for anticholinesterase medication
• Symptoms
• Response 208
Assessment of MG Crisis
�Increased pulse, respirations, and blood
pressure
�Dyspnea, anoxia, and cyanosis
�Bowel and bladder incontinence
�Decreased urine output
�Absent cough and swallow reflex
209
Cholinergic Crisis
a. Abdominal cramps
b. Nausea, vomiting, and diarrhea
c. Blurred vision
d. Pallor
e. Facial muscle twitching
f. Hypotension
g. Pupillary miosis210

11/7/2016
71
Cholinergic Overdose
This is an example of a mnemonic that is commonly used in the
real world to diagnose cholinergic overdose
Diarrhoea
Urination
Miosis/muscle weakness
Bronchorrhea
Bradycardia
Emesis
Lacrimation
Salivation/sweating211
Edrophonium test
Have atropine sulfate available
when performing the Tensilon test.
212
Nursing Interventions
1. Monitor respiratory status and ability to cough
and deep-breathe adequately.
2. Monitor for respiratory failure.
3. Maintain suctioning and emergency equipment
at the bedside.
4. Monitor vital signs.
5. Monitor speech and swallowing abilities to
prevent aspiration.
6. Encourage the client to sit up when eating.
7. Assess muscle status.
213

11/7/2016
72
Nursing Interventions8. Instruct the client to conserve strength.
9. Plan short activities that coincide with times of
maximal muscle strength.
10. Monitor for myasthenic and cholinergic crises.
11. Administer anticholinesterase medications as
prescribed.
12. Instruct the client to avoid stress, infection,
fatigue, and over-the-counter medications.
13. Instruct the client to wear a Medic-Alert
bracelet.
14. Inform the client about services from the
Myasthenia Gravis Foundation.
214
THE DIEASES MS, PD, AND MG ALL
INVOLVE MOVEMENT PROBLEMS
215
� MS: Demyelination of nerve fibers of
the brain and spinal cord
� PD: Degeneration of dopamine
producing neurons in the substantia
nigra
� MG: Reduction in the number of these
receptor sites for acetylcholine
Myasthenia Gravis• Cholinestrerase: Reversible cholinesterase inhibitors are
the mainstay of therapy.
• Prevent ACh inactivation, anticholinesterase agents can
intensify the effects of ACh released from motor
neurons, and can thereby increase muscle strength.
• Cholinesterase inhibitors do not cure MG. Rather, they
only produce symptomatic relief, and hence patients
usually need therapy lifelong.

11/7/2016
73
Myasthenia Gravis (Cont.)Most commonly used:
� Ambenonium
� Neostigmine
� Pyridostigmine
• Route: PO, IM, SQ, IV & Topical
• Side Effects:
� Causes ACh to accumulate at muscarinic junctions
�If muscarinic responses are excessive, atropine may be
given to suppress them.
�Atropine should not be employed routinely.
�Atropine can mask the early signs (eg, excessive
salivation) of overdose with anticholinesterase agents.
QUESTIONS
218














![The Nervous System [Class Number Section] [Instructor Name]](https://static.fdocuments.us/doc/165x107/5697bff71a28abf838cbe7ba/the-nervous-system-class-number-section-instructor-name.jpg)

![The Brain & Nervous System [Class Number Section] [Instructor Name]](https://static.fdocuments.us/doc/165x107/56649ccb5503460f94995142/the-brain-nervous-system-class-number-section-instructor-name.jpg)

