MODULE BASIS OF PRECLINICAL STUDIESjulivan/MF rudens semestras/Basis of... · MODULE BASIS OF...
46
1 Lithuanian University of Health Sciences Faculty of Medicine Second year Autumn semester MODULE BASIS OF PRECLINICAL STUDIES Part Biochemistry Practicals Kaunas 2012 September-October
Transcript of MODULE BASIS OF PRECLINICAL STUDIESjulivan/MF rudens semestras/Basis of... · MODULE BASIS OF...
1
Lithuanian University of Health Sciences Faculty of Medicine
Second year Autumn semester
MODULE BASIS OF PRECLINICAL STUDIES
Part Biochemistry
Practicals
Kaunas 2012 September-October

2
ESSENTIAL INFORMATION
All laboratory works take place in Laboratory Building of LUHS, Eiveniu str.4
Biochemistry lab-room 235 (2nd floor)
Course organizer prof.L.Ivanoviene room 209
3
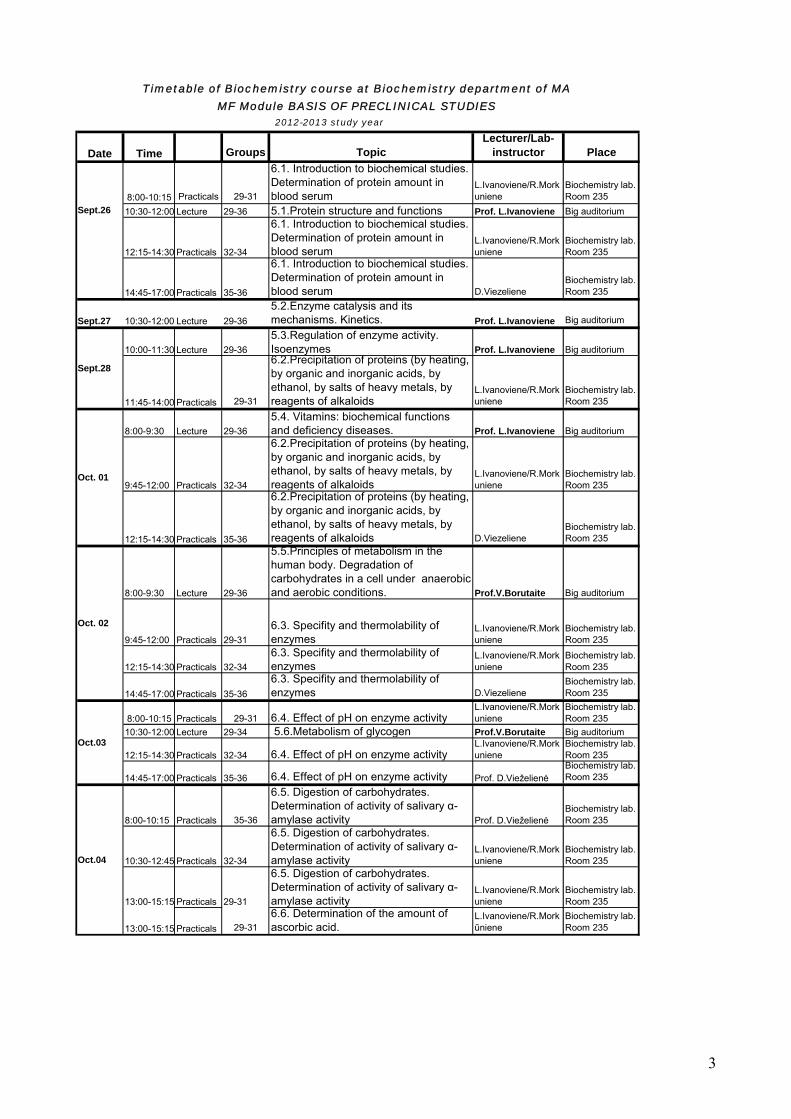
2012-2013 study year
Date Time Groups TopicLecturer/Lab-
instructor Place
8:00-10:15 Practicals 29-31
6.1. Introduction to biochemical studies. Determination of protein amount in blood serum
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
10:30-12:00 Lecture 29-36 5.1.Protein structure and functions Prof. L.Ivanoviene Big auditorium
12:15-14:30 Practicals 32-34
6.1. Introduction to biochemical studies. Determination of protein amount in blood serum
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
14:45-17:00 Practicals 35-36
6.1. Introduction to biochemical studies. Determination of protein amount in blood serum D.Viezeliene
Biochemistry lab. Room 235
Sept.27 10:30-12:00 Lecture 29-36
5.2.Enzyme catalysis and its mechanisms. Kinetics. Prof. L.Ivanoviene Big auditorium
10:00-11:30 Lecture 29-36
5.3.Regulation of enzyme activity. Isoenzymes Prof. L.Ivanoviene Big auditorium
11:45-14:00 Practicals 29-31
6.2.Precipitation of proteins (by heating, by organic and inorganic acids, by ethanol, by salts of heavy metals, by reagents of alkaloids
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
8:00-9:30 Lecture 29-36
5.4. Vitamins: biochemical functions and deficiency diseases. Prof. L.Ivanoviene Big auditorium
9:45-12:00 Practicals 32-34
6.2.Precipitation of proteins (by heating, by organic and inorganic acids, by ethanol, by salts of heavy metals, by reagents of alkaloids
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
12:15-14:30 Practicals 35-36
6.2.Precipitation of proteins (by heating, by organic and inorganic acids, by ethanol, by salts of heavy metals, by reagents of alkaloids D.Viezeliene
Biochemistry lab. Room 235
8:00-9:30 Lecture 29-36
5.5.Principles of metabolism in the human body. Degradation of carbohydrates in a cell under anaerobic and aerobic conditions. Prof.V.Borutaite Big auditorium
9:45-12:00 Practicals 29-31
6.3. Specifity and thermolability of enzymes
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
12:15-14:30 Practicals 32-34
6.3. Specifity and thermolability of enzymes
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
14:45-17:00 Practicals 35-36
6.3. Specifity and thermolability of enzymes D.Viezeliene
Biochemistry lab. Room 235
8:00-10:15 Practicals 29-31 6.4. Effect of pH on enzyme activityL.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
10:30-12:00 Lecture 29-34 5.6.Metabolism of glycogen Prof.V.Borutaite Big auditorium
12:15-14:30 Practicals 32-34 6.4. Effect of pH on enzyme activityL.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
14:45-17:00 Practicals 35-36 6.4. Effect of pH on enzyme activity Prof. D.VieželienėBiochemistry lab. Room 235
8:00-10:15 Practicals 35-36
6.5. Digestion of carbohydrates. Determination of activity of salivary α-amylase activity Prof. D.Vieželienė
Biochemistry lab. Room 235
10:30-12:45 Practicals 32-34
6.5. Digestion of carbohydrates. Determination of activity of salivary α-amylase activity
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
13:00-15:15 Practicals 29-31
6.5. Digestion of carbohydrates. Determination of activity of salivary α-amylase activity
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
13:00-15:15 Practicals 29-31
6.6. Determination of the amount of ascorbic acid.
L.Ivanoviene/R.Morkūniene
Biochemistry lab. Room 235
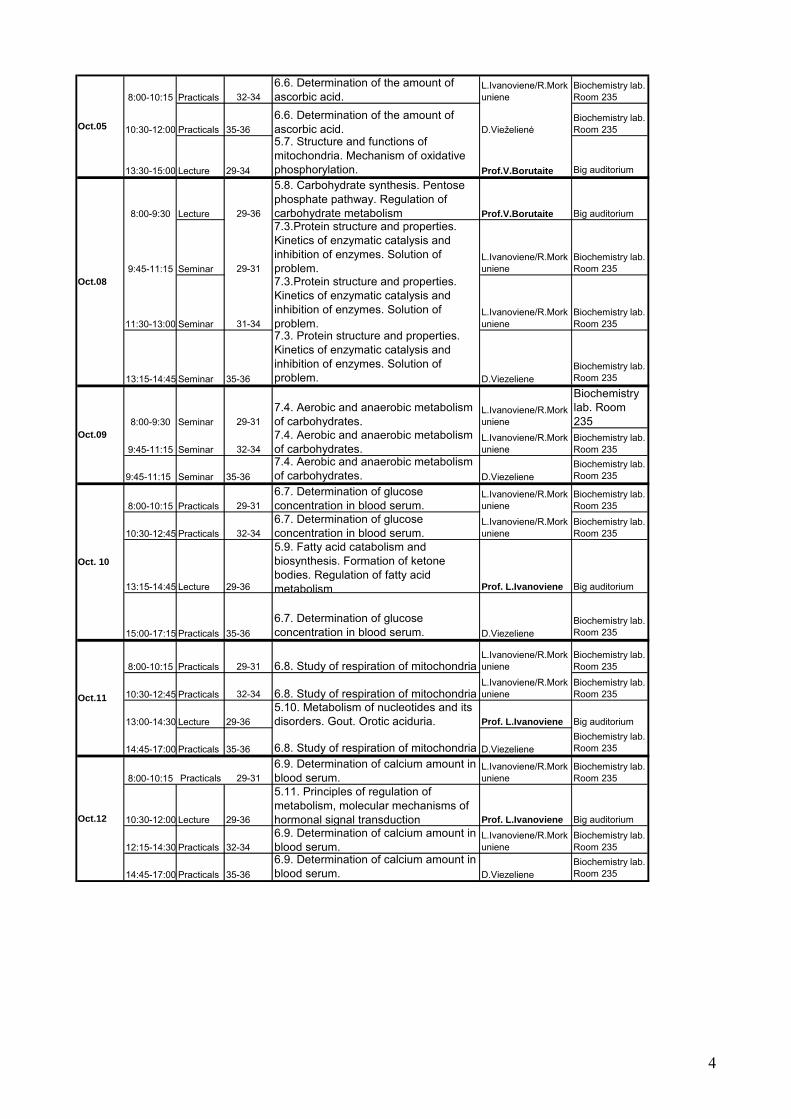
Timetable of Biochemistry course at Biochemistry department of MA
MF Module BASIS OF PRECLINICAL STUDIES
Sept.28
Sept.26
Oct. 01
Oct. 02
Oct.03
Oct.04
4
8:00-10:15 Practicals 32-34
6.6. Determination of the amount of ascorbic acid.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
10:30-12:00 Practicals 35-36
6.6. Determination of the amount of ascorbic acid. D.Vieželienė
Biochemistry lab. Room 235
13:30-15:00 Lecture 29-34
5.7. Structure and functions of mitochondria. Mechanism of oxidative phosphorylation. Prof.V.Borutaite Big auditorium
8:00-9:30 Lecture 29-36
5.8. Carbohydrate synthesis. Pentose phosphate pathway. Regulation of carbohydrate metabolism Prof.V.Borutaite Big auditorium
9:45-11:15 Seminar 29-31
7.3.Protein structure and properties. Kinetics of enzymatic catalysis and inhibition of enzymes. Solution of problem.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
11:30-13:00 Seminar 31-34
7.3.Protein structure and properties. Kinetics of enzymatic catalysis and inhibition of enzymes. Solution of problem.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
13:15-14:45 Seminar 35-36
7.3. Protein structure and properties. Kinetics of enzymatic catalysis and inhibition of enzymes. Solution of problem. D.Viezeliene
Biochemistry lab. Room 235
8:00-9:30 Seminar 29-31
7.4. Aerobic and anaerobic metabolism of carbohydrates.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
9:45-11:15 Seminar 32-34
7.4. Aerobic and anaerobic metabolism of carbohydrates.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
9:45-11:15 Seminar 35-36
7.4. Aerobic and anaerobic metabolism of carbohydrates. D.Viezeliene
Biochemistry lab. Room 235
8:00-10:15 Practicals 29-31
6.7. Determination of glucose concentration in blood serum.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
10:30-12:45 Practicals 32-34
6.7. Determination of glucose concentration in blood serum.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
13:15-14:45 Lecture 29-36
5.9. Fatty acid catabolism and biosynthesis. Formation of ketone bodies. Regulation of fatty acid metabolism Prof. L.Ivanoviene Big auditorium
15:00-17:15 Practicals 35-36
6.7. Determination of glucose concentration in blood serum. D.Viezeliene
Biochemistry lab. Room 235
8:00-10:15 Practicals 29-31 6.8. Study of respiration of mitochondria L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
10:30-12:45 Practicals 32-34 6.8. Study of respiration of mitochondria L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
13:00-14:30 Lecture 29-36
5.10. Metabolism of nucleotides and its disorders. Gout. Orotic aciduria. Prof. L.Ivanoviene Big auditorium
14:45-17:00 Practicals 35-36 6.8. Study of respiration of mitochondria D.ViezelieneBiochemistry lab. Room 235
8:00-10:15 Practicals 29-31
6.9. Determination of calcium amount in blood serum.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
10:30-12:00 Lecture 29-36
5.11. Principles of regulation of metabolism, molecular mechanisms of hormonal signal transduction Prof. L.Ivanoviene Big auditorium
12:15-14:30 Practicals 32-34
6.9. Determination of calcium amount in blood serum.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
14:45-17:00 Practicals 35-36
6.9. Determination of calcium amount in blood serum. D.Viezeliene
Biochemistry lab. Room 235
Oct.12
Oct.11
Oct. 10
Oct.09
Oct.05
Oct.08

5
8:00-9:30 Seminar 29-31
7.5. Analysis of metabolism of fats and fatty acid using the maps of metabolic pathways. Biochemical aspects of obesity.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
9:45-11:15 Seminar 32-34
7.5. Analysis of metabolism of fats and fatty acid using the maps of metabolic pathways. Biochemical aspects of obesity.
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
11:30-13:00 Seminar 35-36
7.5. Analysis of metabolism of fats and fatty acid using the maps of metabolic pathways. Biochemical aspects of obesity. D.Viezeliene
Biochemistry lab. Room 235
8:00-9:30 Seminar 29-31
7.6. Signal transduction: second messengers, their formation, inactivation and significance in regulation of metabolism
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
9:45-11:15 Seminar 32-34
7.6. Signal transduction: second messengers, their formation, inactivation and significance in regulation of metabolism
L.Ivanoviene/R.Morkuniene
Biochemistry lab. Room 235
11:30-13:00 Seminar 35-36
7.6. Signal transduction: second messengers, their formation, inactivation and significance in regulation of metabolism D.Viezeliene
Biochemistry lab. Room 235
11:15-13:30 EXAMINATION Big auditoriumOct.19
Oct.15
Oct.16
6
SAFETY NOTES OF WORK IN BIOCHEMISTRY LABORATORY
This document must be read before your first practical.
1. Department policy 1.1 It is overriding policy of the University and Department of Biochemistry that experimental
work, whether associated with teaching or research, be done efficiently and safely. Safety begins with the individual’s personal responsibility. However, in addition, each member of the academic staff and each technician have a statutory duty to take reasonable care for persons under his/her supervision.
1.2 Students have a statutory obligation to protect themselves and others from hazards resulting from their acts or omissions in the laboratory.
1.3 Only the students of groups scheduled are permitted to be in the laboratory. Visitors or intruders should be asked to leave.
2. General 2.1. Smoking, eating and drinking are not permitted on the laboratory. 2.2. Outdoor clothing must be left in a cloakroom. Bags must be placed on side podia provided
for the purpose and not allowed to obstruct gangways or bench tops. 2.3. Suitable laboratory coats must be worn in the laboratory and removed after leaving. Safety
spectacles must be worn when carrying out any procedure where may be slightest risk of eye injury; gloves of the appropriate type must be worn when necessary. Long hair must be restrained e.g. by means of a cap, ribbon or headband.
2.4. The notes for each practical should be read before coming to the practical and note taken of any safety matters. Students are NOT permitted to do any experimental work unless a supervisor (demonstrator or a member of staff) is present.
2.5. The use of unfamiliar equipment and the handling of potentially hazardous materials will be explained to students. If a student, for some reason, misses the appropriate explanation, then it is the student’s responsibility to bring the lack of knowledge to the attention of the Chief Technician, so that appropriate arrangements can be made to remedy the situation.
2.6. Glassware and plastic ware that is being used should be labeled with felt-tip pen; this avoids confusion and will help the laboratory staff.
3. Substances and procedures hazardous to health 3.1. Where a potential hazard exists in a particular practical, this will be discussed in the talk
before the practical and details of safe working methods will be highlighted in the practical notes.
3.2. Students must NOT use unfamiliar equipment or procedures without them having been given instruction. All safety instructions given in the preliminary talk and practical notes must be adhered to.
3.3. Mouth pipetting is forbidden for acids, bases and hazardous fluids. 3.4. All hazardous materials are deposited in a fume cupboard. 3.5. Never use toxic substances without taking the proper precautions and making arrangements
for safe working. Use volatile solvents in a fume cupboard. 3.6. Broken glassware must be placed in one of the special bins provided in the laboratory. 3.7. Used plastic pipette tips must be placed in the appropriate labeled container on the bench.
4. Waste 4.1. Bench should be left waste-free and tidy at the end of each practical – this reduces potential
for accidents and spillages and is of considerable help to the laboratory staff.
7
4.1.Laboratory equipment must be left clean after the practical. The supervisor of the chief technician instructs about the place of test-tube or flask washing.
5. Accidents 5.1. All accidents and spillages, including any personal injuries and damage caused to
equipment, must be reported as soon as practicable to the supervisor, the chief technician or other technicians.
5.2. Concentrated acid or alkali on the skin: a) flood the splashed surface thoroughly with water and continue until satisfied that no chemical remains in contact with the skin. Soap will help to remove chemical which are insoluble in water; b) remove all contaminated clothing take care not to contaminate yourself in the process.
5.3. Splashes in the eye. Eye protection should be worn for any work where there is a potential hazard but if accident occurs: a) flood the eye thoroughly but gently with water; b) seek medical advice for all eye injuries from chemicals.
5.4. Burns and scalds. Cool affected area by immersing in cold water. Seed is essential. Continue for at least 5 minutes or until pain is relieved.
5.5. Spillages must be cleared up immediately and the area decontaminated; they must NOT be left as a hazard to others.
5.6. A first aid box is located in the preparatory room. Consult a demonstrator or technicians if you need items from the first aid box.
8
INSTRUCTION ABOUT YOUR RESULTS RECORDING AND PRESENTATION
Students should bring their own notebook or loose-leaf book along to the practical. The description of each practical should be organized in the following order:
1. Title of the practical. 2. Objectives of a practical. 3. Principles of the procedure. 4. Equipment and materials 5. Data of measurement and calculations. Graphs are often an essential part of data analysis.
They are best plotted as you go along wherever possible. Remember to label axes clearly. 6. Interpretation and conclusions. Conclusions have to correspond to the objectives of
practical.

9
6.1. Introduction to biochemical studies. Determination of protein amount in blood serum by Biuret methods
Aim: To determine the amount of protein by biuret method and by Bradford and be able to evaluate the significance of protein amount in blood serum. Objectives: 1. Introduce the objects of the course of Biochemistry. 2. Determine the amount of proteins in blood serum by biuret and Bradford methods. 3. Learn to calculate protein amount and express it in systemic and not systemic units. 4. Be able to discuss the significance of alterations of protein amount in blood serum. 1) Biuret reaction Principle: The biuret reaction is a method that can be used to determine the amount of soluble protein in a solution. The biuret reagent (copper sulfate in a strong base) reacts with peptide bonds (at least two peptide bonds) and changes color (form a violet) when it does so. The spectrophotometer can then be used to measure the intensity of the color produced. The more protein present the darker the color.
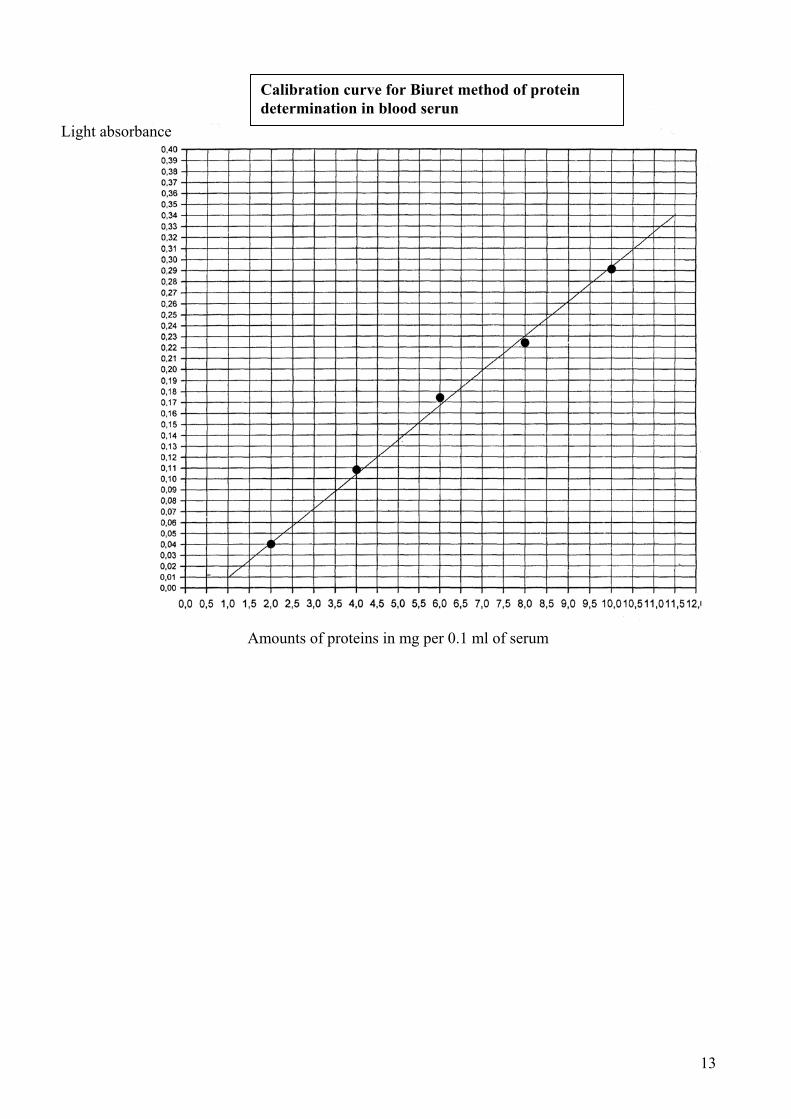
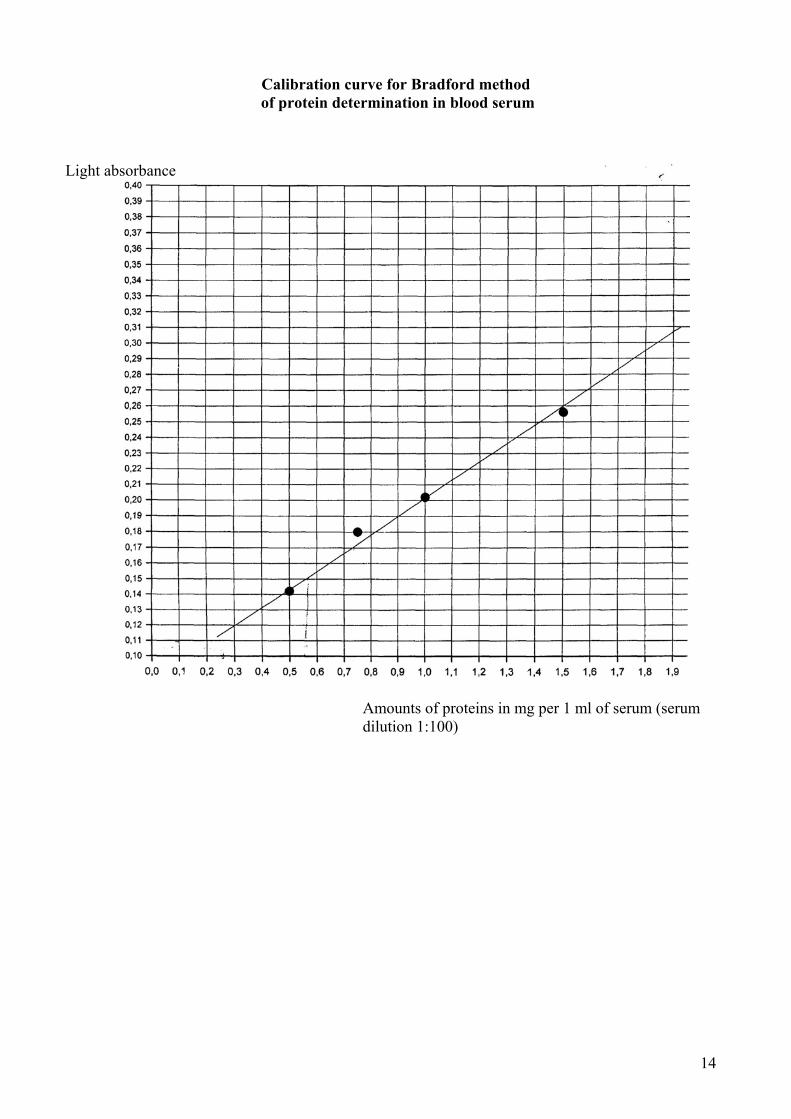
Dipeptides and free amino acids do not participate in this reaction. Procedure. 1. Take 2 test tubes. Pour 0.1 ml of serum into the tube No.1 and 0.1 ml of H2O into the tube No.2. 2. Add 5 ml of biuret reagent into each of the test tubes. Shake and set aside for 10 min. 3. The extinction of the samples is determined spectrophotometrically using sample No.2 as reference. 4. The concentration of protein is calculated from the calibration curve (page 13). For example, let us assume that the determined amount of protein is 3.5 mg per 0.1 ml of serum. It corresponds to 3.5 g per 100 ml or 35 g per liter of serum. The normal level of protein in serum is 65-85 g/l. 2) Bradford reaction Principle: Bradford assay is rapid and sensitive assay for quantification of proteins. It works by the action of Coomassie G-250 (brilliant blue) dye, which binds specific amino acid residues forming blue protein-dye complex. The intensity of blue color (protein-dye compex) is monitored at 595 nm in a spectrophotometer. The more protein presents the darker the color. Procedure: 1. Take 2 test tubes. Using automatic pipette put 0.1 ml of diluted serum (1:100) into the tube No.1 and 0.1 ml of H2O into the tube No.2. 3. Using automatic pipette add 3 ml of Bradford reagent into each of the test tubes. Shake and set aside for 10 min. 4. The absorbance of the samples is determined spectrophotometrically at 595 nm using sample No.2 as reference. (A technician will assist in registration of light absorbance). The concentration of protein is calculated from the calibration curve (page 14). 6. For example, let us assume that the determined amount of protein is 0.5 mg per 1 ml of serum
diluted 1:100. It corresponds to 50 mg per 1 ml or 50 g per liter of serum. The normal level of protein in serum is 65-85 g/l.
O = C
H - N
H - C - R
O = C
H - N
H - C - R
R - C - HC u 2 +
N - H
N - H
R - C - H
C = O
C = O

10
7. Fill the Labreport pages and be ready to make explanations (page 8) Name Family name Group N Year Faculty
Labwork N 6.1.
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work …
1. Biuret method.
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
2. Bradford method
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
……………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………

11
Results and calculations.
1. Biuret method.
2. Bradford method.
Conclusion.

12
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 20-23. Control questions for practical work defense 1. How is the amount of protein determined in blood serum? What is the principle underlying these methods? 2. What physical-chemical method is used to determine the amount of protein in blood serum by the biuret and Bradford methods? What index is registered in these methods? 3. How do you calculate the amount of protein, when it is being determined by the biuret or Bradford method? What indices are needed for it? 4. How is the amount of protein in blood serum expressed, and why? What is the normal physiological amount of protein in blood serum? 5. What protein is present in blood serum in the highest quantities? What state is it, when protein, or some specific protein present in blood serum, has levels below normal?
13
Calibration curve for Biuret method of protein determination in blood serun
Amounts of proteins in mg per 0.1 ml of serum
Light absorbance
14
Calibration curve for Bradford method of protein determination in blood serum
Amounts of proteins in mg per 1 ml of serum (serum dilution 1:100)
Light absorbance

15
6.2. Precipitation of proteins (by heating, by organic and inorganic acids, by ethanol, by salts of heavy metals, by reagents of alkaloids).
Aim: To understand protein physical-chemical properties and mechanisms of protein precipitation and denaturation. Objectives 1. Ascertain the mechanisms of reversible protein precipitation. 2. Understand the mechanisms of protein denaturation under exposure to different physical and chemical factors. 3. Understand the significance of protein precipitation in medicine. A number of proteins, including most globulins, are water-soluble. The hydratation of molecules makes the solutions of these proteins stable. The stability of protein solution may be disturbed by factors inducing precipitation. The precipitation of proteins may be reversible and irreversible. Precipitation is considered as reversible if native molecular conformation of protein is preserved. In this case the functional activity of protein can be recovered after dissolving the precipitate. Reversible precipitation is induced by acetone, ethanol, and high concentration of mineral salts. Chemical modification of side chains of amino acids or spitting of peptide bonds always induces an irreversible precipitation called denaturation. Proteins may be denatured by heating, high-concentrated urea, detergents, extreme pH, many organic solvents, radiation. Denaturated protein loses its native conformation and biological activity.
1. Precipitation by heating When proteins are exposed to increasing temperature, loss of solubility or enzymatic activity occurs over a fairly narrow range. Depending upon the protein studied and the severity of the heating, these changes may or may not be reversible. Few proteins can remain biologically active above 50oC. As the temperature is increased, a number of bonds in the protein molecule are weakened. The first affected are the long range interactions that are necessary for the presence of tertiary structure. As these bonds are first weakened and are broken, the protein obtains a more flexible structure and the groups are exposed to solvent. If heating ceases at this stage the protein should be able to readily refold to the native structure. If heating continues, some of the cooperative hydrogen bonds that stabilize helical structure will begin to break. As these bonds are broken, water can interact with and form new hydrogen bonds with the amide nitrogen and carbonyl oxygen of the peptide bonds. The presence of water further weakens nearby hydrogen bonds by causing an increase in the effective dielectric constant near them. As the helical structure is broken, hydrophobic groups are exposed to the solvent.
Procedure: 1. Pour about 1 ml of 1% protein solution into each of 5 test tubes. 2. Heat the tube No.1 until the precipitate appears. 3. Add 1 drop of 1% acetic acid into the tube No.2. The precipitate appears sooner if the tube is
heated. In this case the pH value of solution corresponds to the pI value of the protein. 4. Add 0.5 ml of 10% acetic acid into the tube No.3. The precipitate will not appear even if
you heat the tube. The protein gives no precipitate, because of the positive charge of molecules in acidic solution.
5. Add 0.5 ml of 10% acetic acid into the tube No.4 and put some drops of saturated NaCl. The precipitate appears during heating the tube.
6. Add 0.5 ml of 10% NaOH into the tube No.5. The precipitate is not formed even you heat the tube. In this case the negative charge of protein molecules prevents the formation of precipitate.
16
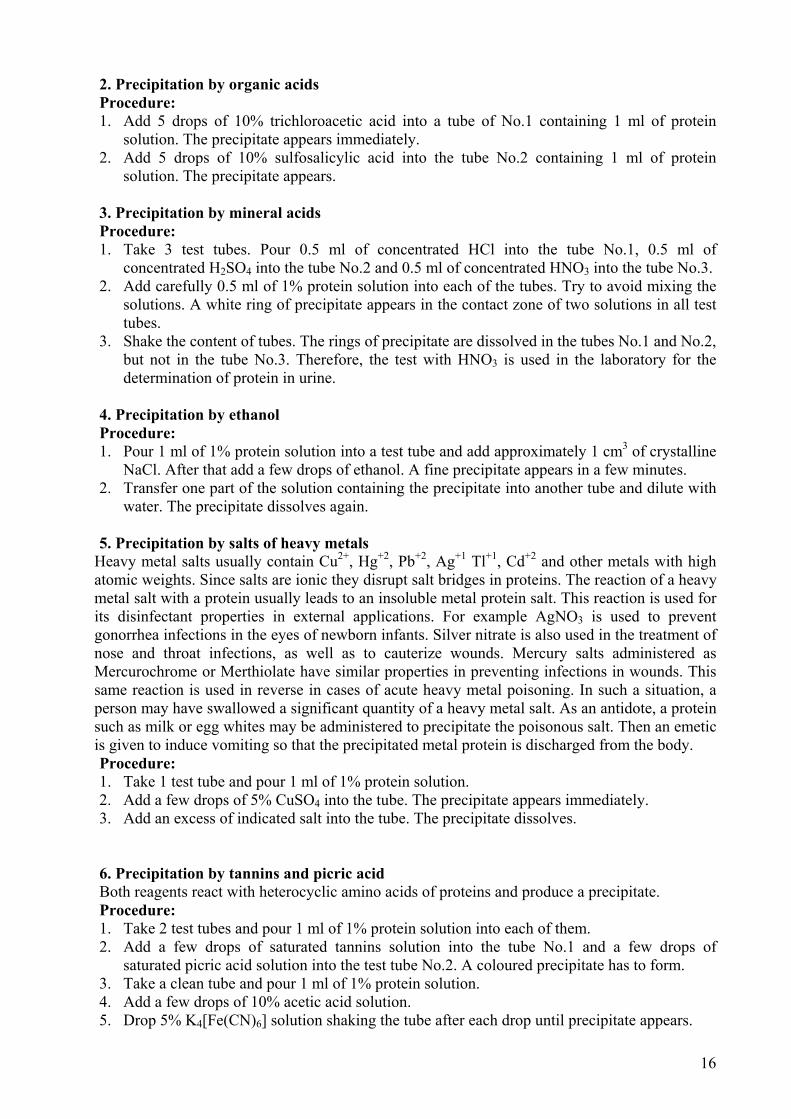
2. Precipitation by organic acids Procedure: 1. Add 5 drops of 10% trichloroacetic acid into a tube of No.1 containing 1 ml of protein
solution. The precipitate appears immediately. 2. Add 5 drops of 10% sulfosalicylic acid into the tube No.2 containing 1 ml of protein
solution. The precipitate appears. 3. Precipitation by mineral acids Procedure: 1. Take 3 test tubes. Pour 0.5 ml of concentrated HCl into the tube No.1, 0.5 ml of
concentrated H2SO4 into the tube No.2 and 0.5 ml of concentrated HNO3 into the tube No.3. 2. Add carefully 0.5 ml of 1% protein solution into each of the tubes. Try to avoid mixing the
solutions. A white ring of precipitate appears in the contact zone of two solutions in all test tubes.
3. Shake the content of tubes. The rings of precipitate are dissolved in the tubes No.1 and No.2, but not in the tube No.3. Therefore, the test with HNO3 is used in the laboratory for the determination of protein in urine.
4. Precipitation by ethanol Procedure: 1. Pour 1 ml of 1% protein solution into a test tube and add approximately 1 cm3 of crystalline
NaCl. After that add a few drops of ethanol. A fine precipitate appears in a few minutes. 2. Transfer one part of the solution containing the precipitate into another tube and dilute with
water. The precipitate dissolves again. 5. Precipitation by salts of heavy metals
Heavy metal salts usually contain Cu2+, Hg+2, Pb+2, Ag+1 Tl+1, Cd+2 and other metals with high atomic weights. Since salts are ionic they disrupt salt bridges in proteins. The reaction of a heavy metal salt with a protein usually leads to an insoluble metal protein salt. This reaction is used for its disinfectant properties in external applications. For example AgNO3 is used to prevent gonorrhea infections in the eyes of newborn infants. Silver nitrate is also used in the treatment of nose and throat infections, as well as to cauterize wounds. Mercury salts administered as Mercurochrome or Merthiolate have similar properties in preventing infections in wounds. This same reaction is used in reverse in cases of acute heavy metal poisoning. In such a situation, a person may have swallowed a significant quantity of a heavy metal salt. As an antidote, a protein such as milk or egg whites may be administered to precipitate the poisonous salt. Then an emetic is given to induce vomiting so that the precipitated metal protein is discharged from the body. Procedure: 1. Take 1 test tube and pour 1 ml of 1% protein solution. 2. Add a few drops of 5% CuSO4 into the tube. The precipitate appears immediately. 3. Add an excess of indicated salt into the tube. The precipitate dissolves. 6. Precipitation by tannins and picric acid Both reagents react with heterocyclic amino acids of proteins and produce a precipitate. Procedure: 1. Take 2 test tubes and pour 1 ml of 1% protein solution into each of them. 2. Add a few drops of saturated tannins solution into the tube No.1 and a few drops of
saturated picric acid solution into the test tube No.2. A coloured precipitate has to form. 3. Take a clean tube and pour 1 ml of 1% protein solution. 4. Add a few drops of 10% acetic acid solution. 5. Drop 5% K4[Fe(CN)6] solution shaking the tube after each drop until precipitate appears.

17
Name Family name Group N Year Faculty
Labwork N 6.2.
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work …
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
……………………………………………………………………………………………………
………………………………………………………………………………………………………..
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………

18
Results
1. Write the flowcharts for the test N1. Explain results obtained.
2. Write the flowcharts for the test N2. Explain results obtained.
3. Write the flowcharts for the test N3. Explain results obtained.

19
4. Write the flowcharts for the test N4. Explain results obtained.
5. Write the flowcharts for the test N5. Explain results obtained.
6. Write the flowcharts for the test N6. Explain results obtained.
20
Conclusion.
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 24-29. Control questions for practical work defense 1. What is the reason for lowered solubility of protein? 2. How is reversible precipitation of protein different from irreversible precipitation? What reagents can cause the reversible precipitation? Why? 3. Why does precipitation occur during heating of a protein solution and what happens to the structure of protein molecules? 4. What organic acids can precipitate protein from solutions? Is this process reversible or irreversible? Does the precipitate dissolve in the excess acid? 5. What mineral acids can cause irreversible precipitation of protein? Why? 6. In what mineral acid excess does protein precipitation dissolve? Why? 7. What metal ions can precipitate protein, and why? What happens with the addition of the excess ions? Explain the mechanism of it. 8. How is the metal interaction with protein applied in medicine?
9. What are alkaloid reagents, and how do they affect dissolved protein? Is the effect reversible?
21
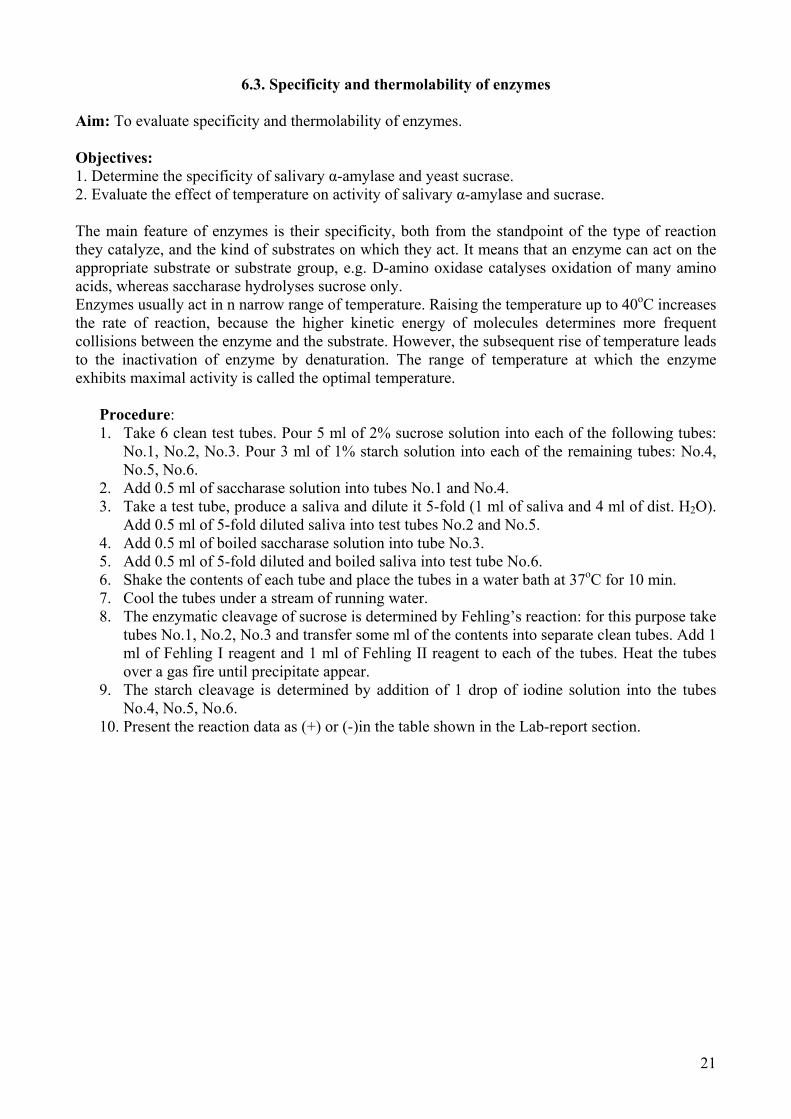
6.3. Specificity and thermolability of enzymes
Aim: To evaluate specificity and thermolability of enzymes. Objectives: 1. Determine the specificity of salivary α-amylase and yeast sucrase. 2. Evaluate the effect of temperature on activity of salivary α-amylase and sucrase. The main feature of enzymes is their specificity, both from the standpoint of the type of reaction they catalyze, and the kind of substrates on which they act. It means that an enzyme can act on the appropriate substrate or substrate group, e.g. D-amino oxidase catalyses oxidation of many amino acids, whereas saccharase hydrolyses sucrose only. Enzymes usually act in n narrow range of temperature. Raising the temperature up to 40oC increases the rate of reaction, because the higher kinetic energy of molecules determines more frequent collisions between the enzyme and the substrate. However, the subsequent rise of temperature leads to the inactivation of enzyme by denaturation. The range of temperature at which the enzyme exhibits maximal activity is called the optimal temperature.
Procedure: 1. Take 6 clean test tubes. Pour 5 ml of 2% sucrose solution into each of the following tubes:
No.1, No.2, No.3. Pour 3 ml of 1% starch solution into each of the remaining tubes: No.4, No.5, No.6.
2. Add 0.5 ml of saccharase solution into tubes No.1 and No.4. 3. Take a test tube, produce a saliva and dilute it 5-fold (1 ml of saliva and 4 ml of dist. H2O).
Add 0.5 ml of 5-fold diluted saliva into test tubes No.2 and No.5. 4. Add 0.5 ml of boiled saccharase solution into tube No.3. 5. Add 0.5 ml of 5-fold diluted and boiled saliva into test tube No.6. 6. Shake the contents of each tube and place the tubes in a water bath at 37oC for 10 min. 7. Cool the tubes under a stream of running water. 8. The enzymatic cleavage of sucrose is determined by Fehling’s reaction: for this purpose take
tubes No.1, No.2, No.3 and transfer some ml of the contents into separate clean tubes. Add 1 ml of Fehling I reagent and 1 ml of Fehling II reagent to each of the tubes. Heat the tubes over a gas fire until precipitate appear.
9. The starch cleavage is determined by addition of 1 drop of iodine solution into the tubes No.4, No.5, No.6.
10. Present the reaction data as (+) or (-)in the table shown in the Lab-report section.
22
Name Family name Group N Year Faculty
Labwork N 6.3.
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Results and calculations.
23
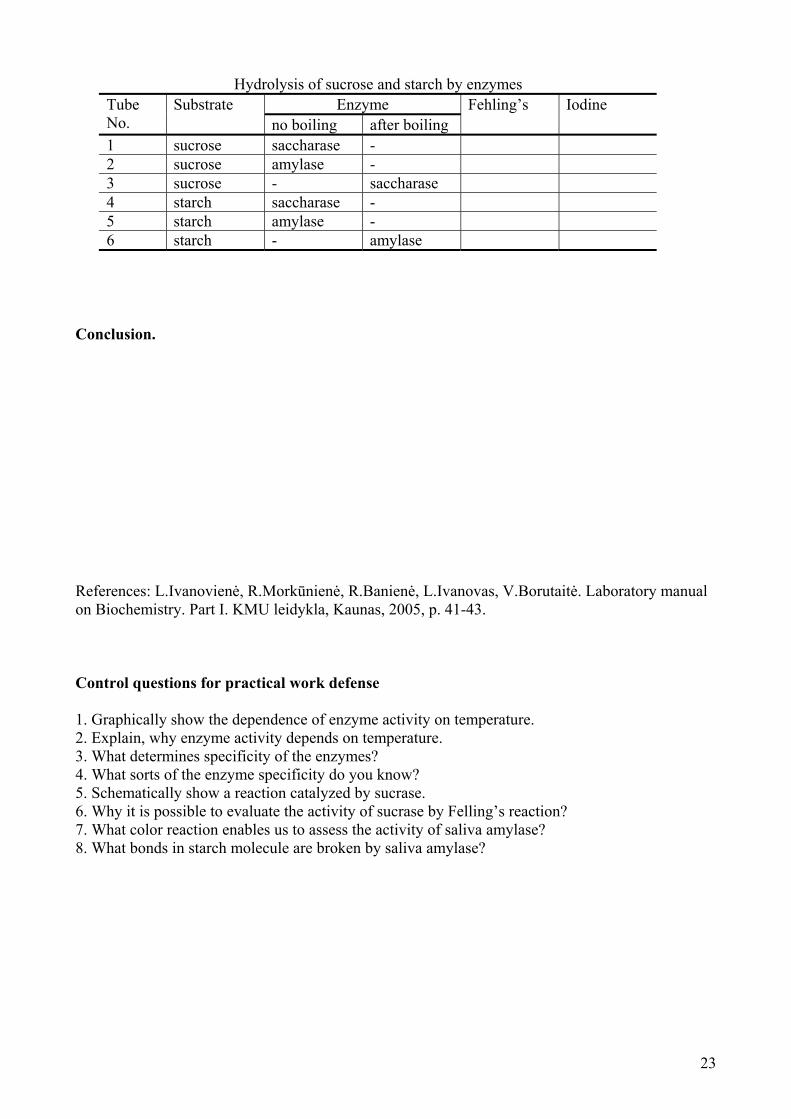
Hydrolysis of sucrose and starch by enzymes Enzyme Tube
No. Substrate
no boiling after boiling Fehling’s Iodine
1 sucrose saccharase - 2 sucrose amylase - 3 sucrose - saccharase 4 starch saccharase - 5 starch amylase - 6 starch - amylase
Conclusion.
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 41-43. Control questions for practical work defense 1. Graphically show the dependence of enzyme activity on temperature. 2. Explain, why enzyme activity depends on temperature. 3. What determines specificity of the enzymes? 4. What sorts of the enzyme specificity do you know? 5. Schematically show a reaction catalyzed by sucrase. 6. Why it is possible to evaluate the activity of sucrase by Felling’s reaction? 7. What color reaction enables us to assess the activity of saliva amylase? 8. What bonds in starch molecule are broken by saliva amylase?

24
6.4. Effect of pH on enzyme activity Aim: To evaluate the dependance of enzyme activity on pH. Objectives: 1. Determine the effect of pH on activity of salivary α-amylase. 2. Ascertain why enzyme activity depends on pH. The pH has a significant influence on the rate of enzymatic reaction. Many enzymes may be characterized by a certain pH value at which the rate is maximal. This value is called the pH optimum. The shift of pH to both sides from the optimum value leads to the decrease in the rate of reaction. Optimal pH is often close to the pH of the tissue enzyme is localized, e.g. pepsin secreted in the stomach has optimal pH of about 2.0 (gastric pH is 2.0-3.0); pancreatic α-amylase secreted in the duodenum has optimal pH of about 7.0 (intestinal pH is 6.0-7.0). Procedure: Assay the pH optimum of salivary amylase.
1. Take 8 test tubes and pour the volumes of 0.2 Na2HPO4 and 0.1 M of citric acid, as indicated in the table below each of them.
2. Prepare a 250-fold diluted saliva. 3. Add 5 ml of 0.5% starch solution and 2.5 ml of 250-fold diluted saliva into each of the
tubes. The diluted saliva is added at equal time intervals beginning from the first tube. 4. Set the tubes for 15 min. After that take a few drops from the tube No.5 into a separate clean
tube and add 1 drop of iodine solution. The blue color indicates that the reaction is not completed. Repeat this test until a brown color appears.
5. Add 2 drops of iodine solution into each of the tubes and shake them. Observe in which of the tubes the starch is cleaved completely.
25
Name Family name Group N Year Faculty
Labwork N …..
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Results and calculations.
26
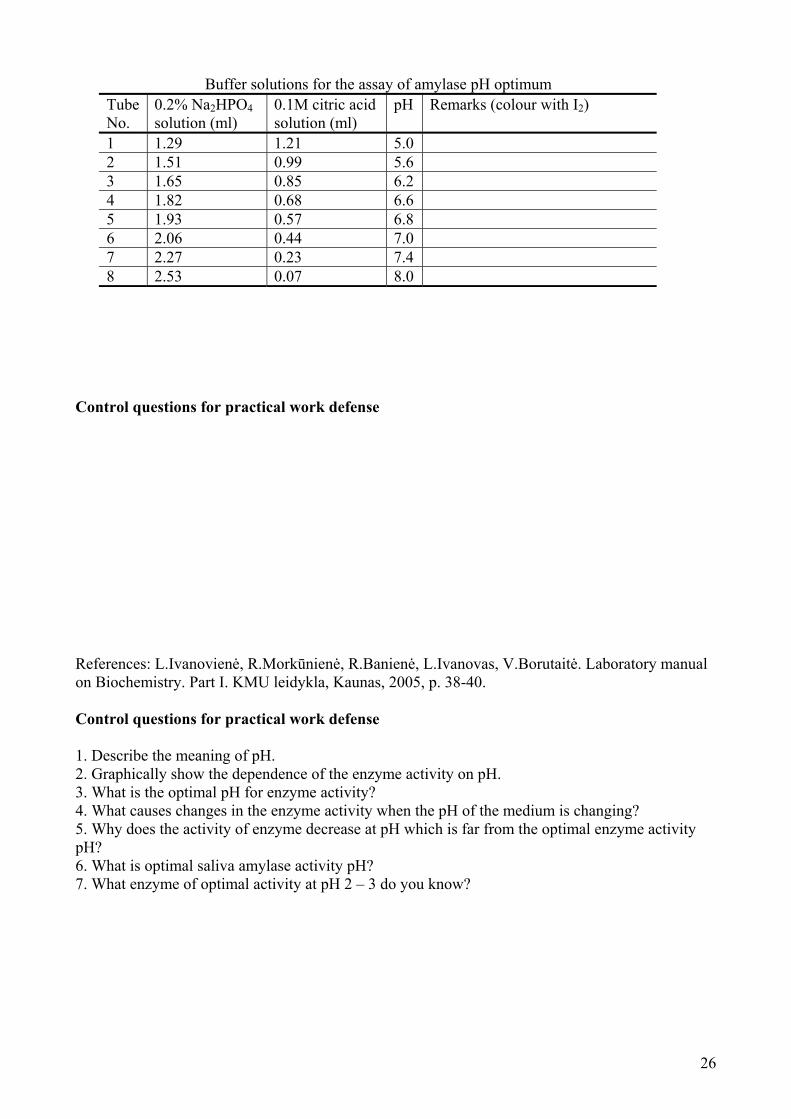
Buffer solutions for the assay of amylase pH optimum Tube No.
0.2% Na2HPO4 solution (ml)
0.1M citric acid solution (ml)
pH Remarks (colour with I2)
1 1.29 1.21 5.0 2 1.51 0.99 5.6 3 1.65 0.85 6.2 4 1.82 0.68 6.6 5 1.93 0.57 6.8 6 2.06 0.44 7.0 7 2.27 0.23 7.4 8 2.53 0.07 8.0
Control questions for practical work defense
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 38-40. Control questions for practical work defense 1. Describe the meaning of pH. 2. Graphically show the dependence of the enzyme activity on pH. 3. What is the optimal pH for enzyme activity? 4. What causes changes in the enzyme activity when the pH of the medium is changing? 5. Why does the activity of enzyme decrease at pH which is far from the optimal enzyme activity pH? 6. What is optimal saliva amylase activity pH? 7. What enzyme of optimal activity at pH 2 – 3 do you know?

27
6.5. Digestion of carbohydrates.
Determination of activity of salivary α-amylase Aim: To evaluate effect of salivary α-amylase on dietary carbohydrates. Objectives: 1. Determine the activity of salivary α-amylase. 2. Evaluate effect of activators and inhibitors on activity of salivary α-amylase. Method is based on ability of minimal salivary amylase amount to cleave the certain amount of starch per time unit. The amylase activity in saliva can be expressed in ml of starch solution (0.1%) which is broken down by 1 ml of undiluted saliva during 30 min at body temperature.
Procedure: 1. Take 10 tubes and number them. Pour 1 ml of water into each tube. 2. Pour 1 ml of saliva into other clean tube and dilute it 10 folds (1 ml saliva + 9 ml water). 3. Add 1 ml of diluted saliva into tube No.1. Shake it carefully. 4. Take 1 ml of solution from tube No.1 and transfer it into tube No.2. Shake the content of
tube No.2. 5. Take 1 ml of solution from tube No.2 and transfer it into tube No.3. Shake. 6. Take 1 ml from tube No.3 and transfer it into tube No.4. In this way do the same procedure
with all subsequent tubes. The line of dilutions is formed where each preceding solution contains twice more amylase than the subsequent one (1/20; 1/40; 1/80; 1/160 and so on).
7. Add 1 ml of a particular solution into each of tubes. Shake. Type of a solution is indicated by lab-instructor. It is one of the following NaCl, CuSO4 or water.
8. Add 2 ml of starch (0.1%) solution exactly into each of tubes. Shake the content of each tube.
9. Place the thermostated box for 30 min. (T=38o) 10. Then take the tubes out and cool immediately in running water. 11. Put a few drops of iodine solution into each tube and mark the color in your reports. 12. The blue color indicates that starch is not cleaved or incompletely cleaved. Calculate the
activity if amylase. The dilution value of the first brown colored solution is taken for calculation. E.g. the fifth tube solution is brown colored. The dilution is 1/320 in this tube. That means:
1/320 ml of saliva cleaved 2 ml of starch (0.1%) 1 ml of saliva would cleave X ml of starch There X = 2*1 / (1/320) = 640
So, 1 ml of undiluted saliva has cleaved 640 ml of starch solution (0.1%) during 30 min at 38o.

28
Name Family name Group N Year Faculty
Labwork N 6.5.
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Results and calculations.

29
Fill the Data table
It contains the results of starch digestion in the presence of three types of solution
Colour with iodine Activity Tube N and Dilution
+ water + NaCl + CuSO4
with water
with NaCl
with CuSO4
Make respective calculations as indicated in the paragraph N12 of the instruction.
Conclusion.

30
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 48-53. Control questions for practical work defense 1. How can the activity of enzyme be determined? 2. Explain how you determined the activity of saliva amylase in your experiment? 3. What units of enzyme activity do you know? 4. How would you describe the enzyme inhibitors? 5. Explain why CuSO4 diminishes enzyme activity. 6. Explain the action of enzyme promoters.

31
6.6. Determination of the amount of ascorbic acid
Aims: To determine the amount of ascorbic acid in the specimen of one of biological fluids. Objectives: 1. Determine the amount of ascorbic acid by 2,6-dichlorphenolindophenol. 2. Learn to calculate the amount of ascorbic acid in the specimen. 3. Discuss the biological meaning of results. 4. Know the role of ascorbic acid in enzymatic catalysis. The normal plasma ascorbic acid concentration for man is 0.7-1.2 mg/100 ml. After administration of ascorbic acid (dose 0.5 g) normal individuals excrete 50% of this dose within 24 h.
Procedure: 1. Take a cone flask (200 ml) and pour 10 ml of urine, 100 ml H2O and 1 ml of glacial acetic
acid. 2. Titrate the obtained solution with 0.001 M 2.6-diclorphenolindophenol solution until a blue
color appears. 3. Calculate the amount of ascorbate in solution according to the utilized volume of 2.6-
dichlorphenolindophenol solution taking into account that 1 ml of 0.001 M 2.6-dichlorphenolindophenol solution corresponds to 0.088 mg of ascorbic acid.

32
Name Family name Group N Year Faculty
Labwork N …..
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Results and calculations.
33
Conclusion.
34
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 59-61. Questions for practical work defense 1. What is determination of the vitamin C amount in a sample based on, if the reagent 2.6-dichlorophenolindophenol was used? 2. How do you calculate the amount of vitamin C in urine? What is vitamin C concentration in blood plasma? 3. What is the active form of vitamin C? 4. In what cases is vitamin C partially excreted with urine? Is it accumulated in the body?

35
6.7. Determination of glucose concentration in blood serum Aim: To learn to determine and calculate glucose concentration in blood serum and interpret results of the study. Objectives: 1. Determine glucose concentration in blood serum by enzymatic method and by using CARDIO-Check analyser. 2. Calculate glucose concentration in blood and express it in systemic and nonsystemic units. 3. Evaluate alterations of glucose concentration and be able to intepret them. 4. Get acquainted with glucose tolerance test and its significance for identification of glucose consumption disorders in organism. Glucose is the main carbohydrate in blood. It is evenly distributed in plasma and erythrocytes. The determination of glucose in blood is a procedure most frequently performed in laboratory of clinical chemistry. The aim of this test is early diagnosis of diabetes mellitus. The determination must be performed on patients in fasting state. The normal glucose concentration in human plasma or serum determined by highly specific methods, ranges from 3.33 to 5.55 mmol/l. In fasting state, the concentration of glucose in arterial and capillary blood is higher than that in the venous blood. Sometimes, glucose overload test is useful for diabetes mellitus diagnosing. For this, a patient is given to drink solution of glucose (50-75g/100 ml of water) under fasting. For glucose concentration determination, blood specimens are taken from the patient every 30 min during 2 h after glucose intake. The data of glucose concentration at time points after glucose ingestion are used for plotting of a graph. The increased concentration of glucose in blood is called hyperglycemia, and decreased - hypoglycemia. When the glucose concentration in blood exceeds 9-10 mmol/L, glucose is not reabsorbed in nephrotubules and is excreted into the urine (glycosuria). This is not observed in low hyperglycemia. Principle of the enzymatic method Glucose in the sample originates, by means of the coupled reactions described below, a coloured complex that can be measured by spectrophotometry. Glucose + ½ O2 + H2O eoxydaseglu cos Gluconate + H2O2 2 H2O2 + 4-Aminoantipyrine + Phenol peroxydase Quinoneimine + 4 H2O Reagent (working solution): phosphate 100 mmol/L, glucose oxydase > 10 U/mL, peroxydase > 1 U/mL, 4-aminoantipyrine 0.4 mmol/L, pH 7.5. Standard solution: glucose 100 mg/dL (5.55 mmol/L). Procedure
1. Take 2 test tubes for a blank and sample tests. 2. Put 1 mL of the reagent into the first test tube. 3. Put 1 mL of the reagent and 10 L of the blood serum sample into the second test tube. 4. Mix thoroughly and incubate the test tubes at room temperature for 10 min. 5. Measure the absorbance (A) of the Sample at 500nm against the Blank. 6. calculate that concentration of glucose using the formula:
sampledardsdards
sample CCA
A tan
tan
A – Light absorbance at 500nm Cstandard =100mg/dL (5.55mmol/L) glucose
36
Reference values (serum and plasma): Newborn, premature 25-80 mg/dL=1.39-4.44 mmol/L Newborn, term 30-90 mg/dL=1.67-5.00 mmol/L Children, adult 70-105 mg/dL=3.89-5.83 mmol/L

37
Name Family name Group N Year Faculty
Labwork N …..
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Results and calculations.

38
Conclusion.

39
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part I. KMU leidykla, Kaunas, 2005, p. 77-80. Questions for practical work evaluation 1. What method did you apply to determine the amount of glucose in blood serum? 2. What indices are needed for the calculation of the glucose amount in blood serum? 3. How did you convert the amount of glucose in blood serum which you found into SI units? 4. In what units is the amount of glucose in blood serum expressed? 5. What is the physiological normal level of glucose in blood? 6. What state is it, when there is an excess or lack of glucose in blood? At what concentration of glucose in blood does excretion of glucose with urine start (the kidney threshold for glucose)?
40
6.8. Study of respiration of mitochondria
Aim: To get acquainted with both the mechanism of oxidative phosphorylation and methods used in its study. Objectives: 1. Understand the principles of methods used in examination of mitochondria respiration. 2. Understand the mechanism of oxidative phosphorylation. 3. Discuss the principles of methods used to study the intensity of oxidative phosphorylation. Questions for practical work evaluation 1. What phenomenon the isolation of cell organoids is based on? What is biomedical meaning of the organoid isolation? 2. What is differential centrifugation? Are certain fractions of organoids isolated in pure form? 3. What is isopiknic centrifugation (e.g. centrifugation in saccharose gradient)? In what cases is it used? Give an example. 4. What organoids can not be isolated intact and why? What conditions and equipment are needed to isolate those partially degraded organoids? 5. What are the main stages of mitochondria isolation? What requirements do solutions for isolation need to meet? 6. How can the purity of mitochondria fraction be assessed? List the methods of assessment and indicate what are they based on. 7. What is mitochondrial respiration? By what method is it assessed and what equipment is used? 8. What is the control of mitochondrial respiration? How can it be assessed and what does it reflect? 9. What methods can be used to assess the efficiency of mitochondrial oxidative phosphorylation? What does the ratio P:O depend on? What is its digital meaning? 10. What is bioluminescent ATP determination based on? References: L.Ivanoviene, V.Borutaite Advanced practical course in biochemistry, Kaunas, 1993, p.3-8.

41
6.9. Determination of calcium amount in blood serum Aim: To determine calcium amount in blood serum. Objectives: 1. To determine calcium amount in blood serum. 2. Learn to calculate calcium amount in specimen of blood serum. 3. Understand the role of calcium in the human body. 4. Be able to evaluate the significance of changes of calcium amount in the body. The metabolism of calcium is closely related to that of phosphorus. More than 99% of calcium and 80% of phosphorus are present in the bones as calcium fluorophosphate apatite. The remaining calcium is present in the form of ions in various body fluids and performs a number of functions. For example, calcium ions are able to decrease neuromuscular excitability, to participate in blood coagulation, to activate some enzymes such as succinate dehydrogenase and proteinkinase. Essentially all blood calcium is present in serum, meanwhile phosphorus is mainly in cells as organic phosphate, with only a small but important amount in serum as inorganic phosphate. In serum calcium exists in 2 different forms, the nondiffusible protein-bound calcium (comprising approximately 40-50% of the total calcium), and the diffusible free calcium. The latter can be subdivided into complexed (by phosphate and bicarbonate) calcium, and ionized calcium, which is physiologically active form. Calcium homeostasis is controlled by hormones: parathyroid hormone, calcitonin, and a derivative of vitamin D3 – 1,25-dihydroxylcholecalciferol. The measurements of calcium and phosphorus play a significant role in diagnosis of some diseases. The normal level of calcium in serum is 2.25-2.8 mmol/l. Increased serum calcium level – hypercalcemia, is observed in primary hyperparathyroidism, along with decrease in the level of serum phosphorus and increased excretion of calcium and phosphorus in urine. Hypervitaminosis D, multiple myeloma, and some neoplastic diseases of bone may also be accompanied by increased concentration of serum calcium, but serum phosphorus levels in these cases (unlike the situation in hyperparathyroidism) are normal or even elevated. Hypocalcemia may be observed in hypoparathyroidism together with normal or increased serum phosphorus level, and decreased urinary calcium and phosphorus excretion. The low concentration of ionized calcium in serum in this disease may lead to an increase of neuromuscular irritability followed by tetany. Serum calcium levels may be low in nephrosis, in nephritis, and in pancreatitis. Hyperphosphatemia may be detected in the case of hypervitaminosis D, hypoparathyroidism, and renal failure, whereas hypophosphatemia – in rickets, in hyperparathyroidism, etc.
1. Determination of calcium amount in serum by oxalate precicpitation and redox titration The principle of determination involves the precipitation of Ca2+ with ammonium oxalate. The precipitate of calcium oxalate is dissolved in H2SO4 solution. The liberated oxalic acid is determined by titration with potassium permanganate: Ca2+ + (NH4)2C2O4 CaC2O4 ↓ + 2 NH+
4, CaC2O4 ↓ + H2SO4 CaSO4 + H2C2O4, 5 H2C2O4 + KMnO4 + 3 H2SO4 K2SO4 + 2 MnSO4 + 10 CO2 + 8 H2O. This method gives highly reliable results and therefore has served for many years as a reference method for serum calcium determination. It has been now largely replaced by more convenient and potentially more accurate method emplying atomic absorption spectrometry. Procedure:
42
1. Take 2 centrifuge test tubes and numerate them. Transfer 2 ml of water to the tube No.1 and 4 ml of water to the tube No.2.
2. Add 2 ml of blood serum into the tube No.1. 3. Add 1 ml of ammonium oxalate into both tubes, and shake them. Set them aside for 30 min. 4. Put the tubes into plastic holders, place them on the balance, and equilibrate them by means
of water. 5. Centrifuge for 10 min. 6. Pour out the solution from both tubes. The precipitate of calcium oxalate remains on the
bottom of tube No.1. 7. Add 4 ml of 2% NH4OH solution into both tubes. Shake them, equilibrate and centrifuge for
10 min. 8. After the last centrifugation pour out the solution from both tubes, add 2 ml of 1 N H2SO4
into both of them, mix with glass rod, and place in a boiling water bath for 2 min. 9. Titrate the hot solution with 0.01 N KMnO4 solution until a pink color appears. 10. Calculate the concentration of calcium according to the equation:
X = 0.2 x (A – B) x 50 x 0.25 (mmol/l) where A is the volume of 0.01 N KMnO4 solution used for the titration of examined sample (tube No.1), B is the volume of 0.01 N KMnO4 solution used for the titration of control sample (tube No.2).
References: L.Ivanovienė, R.Morkūnienė, R.Banienė, L.Ivanovas, V.Borutaitė. Laboratory manual on Biochemistry. Part II. KMU leidykla, Kaunas, 2005, p. 54-59. 2. Ouantitative colorimetric determination of calcium in blood plasma with Arsenazo III
Principle of the method: Calcium with Arsenazo III (1,8-Dihydroxy-3,6-disulpho-2,7-naphtalene-bis(azo)-dibenzenearsonic acid) at neutral pH, yields a blue coloured complex. The intensity of the colour formed is directly proportional to the calcium concentration in the sample. Samples: Serum or plasma Reagents: 1. Arsenazo III 2. Calcium aqueous primary standard 10mg/dl Equipment: Spectrophotometer or colorimeter measuring at 650 nm; Cuvettes 1.0 cm light path. Procedure:
1. In sample cuvette put 10 l blood serum. (second cuvette with 10 l standard solution and third for the blank test are prepared by laboratory assistant).
2. Put 1ml Arsenazo III reagent into the cuvette. Mix and incubate for 2 min at room temperature.
3. Read the absorbance (A) of the sample and Standard, against the Blank at 650nm. Solution is stable for 1 hour.
4. Calculate calcium concentration using formula
Serum and plasma calcium /)conc. Standard(10Standard)(
)(dLmg
A
sampleA
Conversion factor: mg/dL0.25= mmol/L
43
Reference values: Serum or plasma Adults 8.5-10.5 mg/dL = 2.1-2.6 mmol/L Children 10-12 mg/dL = 2.5-3 mmol/L Newborns 8-13 mg/dL = 2-3.25 mmol/L
44
Name Family name Group N Year Faculty
Labwork N …..
Title ……………………………………………………………………………………………
…………………………………………………………………………………………………
Aim……………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………..
……………………………………………………………………………………………………
Principle of the lab-work
I..………………………………………………………………………………………………………
…………………………………………………………………………………………………………
.………………………………………………………………………………………………………
…………………………………………………………………………………………………………
………………………………………………………………………………………………………..
II.
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Equipment and materials………………………………………………………………………….
………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
45
…………………………………………………………………………………………………………
…………………………………………………………………………………………………………
Results and calculations.
I.
II.
Conclusion.
46
Questions for practical work evaluation 1. What is normal concentration of calcium in blood serum? What main functions of calcium in the human body do you know? 2. What methods did you use to determine calcium concentration in blood serum? 3. Write the reactions of the redox titration method you used to determine the calcium concentration is based on. 4. According to what compound amount is the amount of calcium evaluated? How is the amount of this compound determined in the laboratory? 5. What is hypocalcaemia and what are its clinical symptoms? 6. What is hypercalcaemia and what are its clinical symptoms?