Module 2 Exchange and transport 1.2.8 Control of the cardiac cycle.

West Virginia OEMS
Class 3 Inter-Facility Transport
(C3-IFT)
Course
Module 5
Cardiac Assessment
Basic ECG

OVERVIEW
• Cardiac Anatomy/Assessment
– Electrical conduction/cardiac cycle
– Blood flow through the heart
– Cardiac output/contraction
• Preparing for the ECG
– Remember the basics
– 12 Lead ECG acquisition• Positioning the patient
• Lead placement

OVERVIEW
• 12 Lead ECG Assessment
– Coronary Artery flow
– Ischemia/Infarct localization
• General Management
– Angina/Ischemia
– Myocardial Infarction (MI)
– Congestive Heart Failure (CHF)
Cardiac Terminology
• Systole– the squeeze phase of the contraction
• Systemic arteries are perfused
• Diastole– the relaxing phase of the contraction
• Coronary arteries are perfused
• Cardiac Cycle– one complete contraction of the heart
• Cardiac Output– volume of blood circulated in one minute
The Electrical Conduction
System• SA Node
• AV Node
• Bundle of His
• Left and Right Bundle
Branches
• Purkinje Fibers
• 60-100 / min
• 40-60 / min
• 20-40 / min
The Cardiac Cycle
• P wave
• QRS complex
• T wave
• Depolarization of the
atria
• Depolarization of the
ventricles
• Repolarization of the
ventricles

The Cardiac Cycle

The Cardiac Cycle
• P-R Interval
– 0.12 - .020 seconds
• QRS width
– < 0.12 seconds
Blood Flow Through The Heart
• Inferior and Superior Vena Cava
• Right Atrium
• Tricuspid Valve
• Right Ventricle
• Semilunar Valve
• Pulmonary Artery
• Lungs
Blood Flow Through The Heart
• Pulmonary Vein
• Left Atrium
• Bicuspid/Mitral Valve
• Left Ventricle
• Semilunar Valve
• Aorta
• Systemic Circulation


What are the basic heart sounds?
• S 1
– First sound: “lub” occurs during ventricular
contraction when the tricuspid and mitral
valves are closing. (Systolic)
• S 2
– Second sound: “dub” occurs during
ventricular relaxation when the pulmonic and
aortic valves are closing. (Diastolic)

Physiology

Heart sounds
• Ventricles begin filling with blood
• Ventricular pressure rises until > than atrial pressure
• Ventricles contract
• Mitral and tricuspid valves snap shut
– S1 ("lub")
• S1 signifies the beginning of systole

Heart sounds
• Ventricular pressure drops below arterial pressure in Aorta and PA
• Aortic and pulmonic valves snap shut
– S2 ("dub")
• S2 signifies the beginning of diastole
• Atrial pressure > ventricular pressure
• Mitral and tricuspid valves open
• Blood flows from atria to ventricles
What is the Significance to a 12
Lead?• Why is blood flow important?
– Anatomically, depending upon the area of the heart effected, we can predict either symptoms or a diagnosis based on clinical presentation. (LV failure, RV infarct)
• Why are heart sounds important?– We may never be good at abnormal heart sounds, but
if we know what is normal we can determine when an abnormal sound is present. (S3, S4, murmurs, clicks) They may indicate HTN, cardiac defect, CAD, etc.

Cardiac output
• The volume of blood pumped by the ventricles in a given unit of time
• Typically measured and expressed in terms of liters of blood pumped per minute
– Normal is 4-8 liters/min
• Cardiac output is the product of stroke volume (or how much blood the ventricles eject with each beat), and heart rate (how fast the heart beats)
»CO=SV x HR
Cardiac Output
• Also dependent upon• Preload
– volume in ventricle at end of diastole
– Volume of blood returning to the heart
• Afterload
– resistance against which left ventricle must pump (SVR)
• Contractility
Problems with Cardiac Output
• Hypovolemia• Hemorrhagic
• Burns, Emesis, etc.
– Relative Hypovolemia• Neurogenic shock
• Sepsis
• Heart Rate
– Tachycardia
– Bradycardia
Problems with Cardiac Output
– Arrhythmias– A-fib
– Heart blocks
– SVT
– WPW
– Mitral Stenosis or insufficiency
– Cardiac Tamponade
– Constrictive Pericarditis
– Restrictive Cardiomyopathy
Problems with Cardiac Output
• Pump Issues
– Coronary Circulation• Angina Pectoris
• Myocardial Infarction
– Congestive Heart Failure (CHF)– Left or Right sided failure
– Trauma• Direct
• Indirect
Contractility
• Refers to the strength of cardiac muscle contractions
• Contractility has both active and passive components– Active contractility refers to the increase in contraction
strength that derives from stimulation of the sympathetic nerves to the heart.
– Passive contractility refers to the rise in contraction strength that is the result of changing the length of the cardiac muscle fibers (the so-called "Frank-Starling mechanism").

The Basics of ECG
Interpretation• Are there P waves?
• What is the P-R interval and is it constant?
• What is the QRS width?
• What is the rhythm? Regular or Irregular.
• What is the rate?

12 Lead ECG Acquisition
• Positioning of the patient
– Supine (1st choice), Fowler’s for the acute pt.
– Dry diaphoretic skin
– Shave if necessary
• Lead placement
– Limb leads
– Precordial leads

Limb Leads
• RA- (white) right arm
• LA- (black) left arm
• LL- (red) left leg
• RL- (green) right leg
– LIMB LEADS MUST GO ON THE LIMBS
WHEN ECG IS USED FOR DIAGNOSTIC
PURPOSES.

Precordial Leads
• V1- 4th ICS, right of the sternum.
• V2- 4th ICS, left of the sternum.
• V3- between V2 and V4.
• V4- 5th ICS, midclavicular line.
• V5- 5th ICS, anterior axillary line.
• V6- 5th ICS, midaxillary line.
– V4, V5 and V6 are in a straight line…

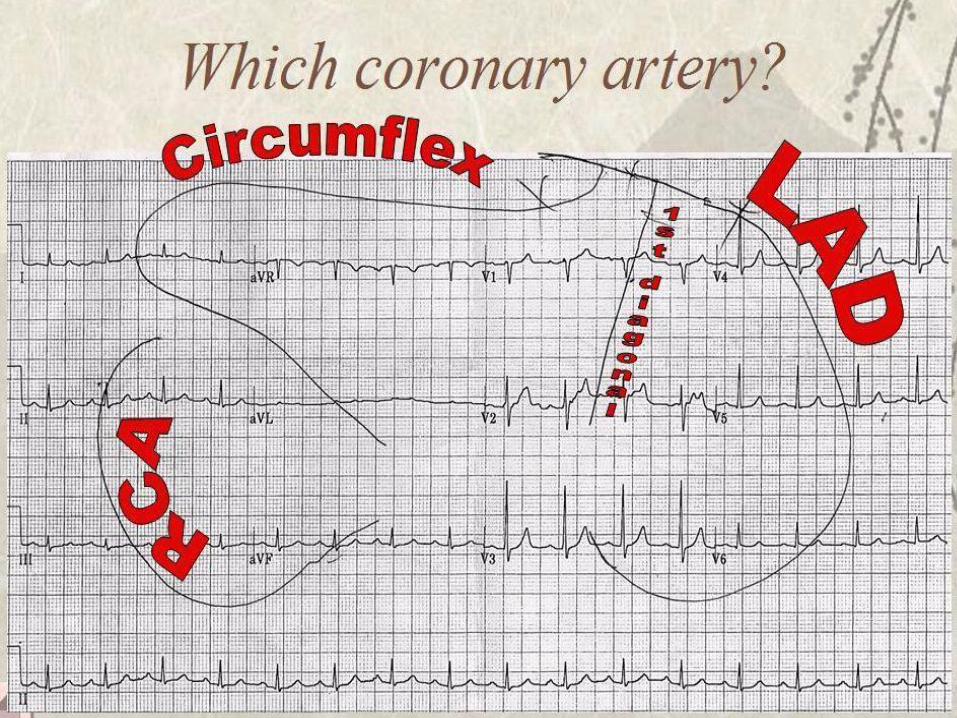
Coronary Artery Perfusion and MI
Localization
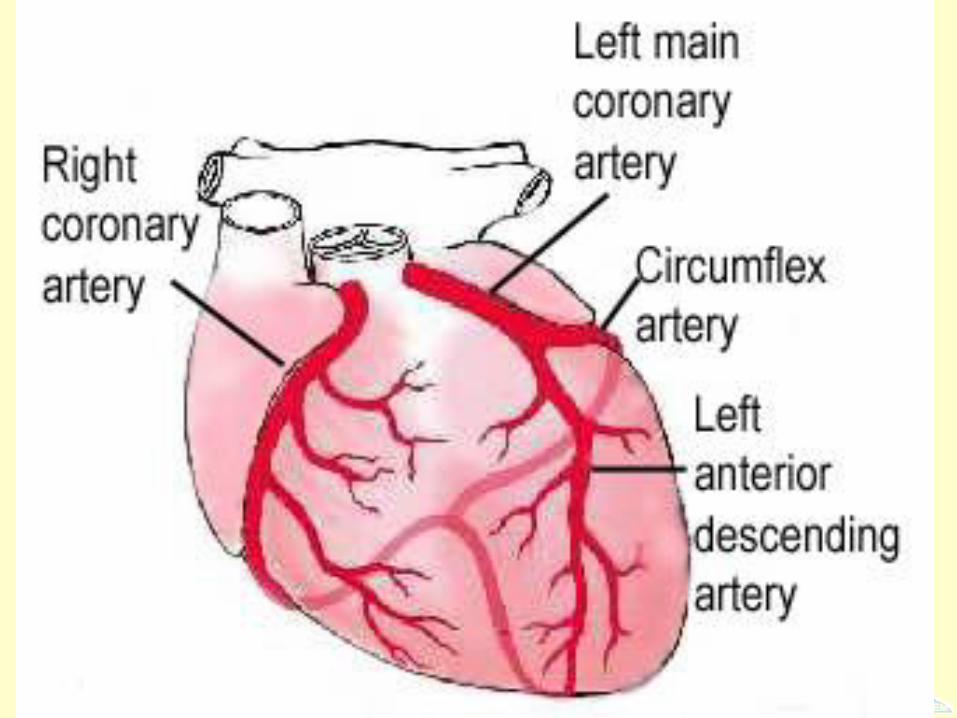

Right Coronary Artery (RCA)
• Supplies the right ventricle and the inferior
wall of the left ventricle.
• RCA divides into the posterior descending
coronary artery, supplying parts of the
posterior wall of the left ventricle.
• Responsible for part of the blood flow to
the SA and AV nodes.

RCA
• Supplies blood to SA node in 55 % of pop.
• Supplies blood to AV node in 90 % of pop.
Left Coronary Artery
• Left Anterior Descending (LAD) Coronary
Artery.
• Left Circumflex Artery (LCA, Cx)

Left Anterior Descending (LAD)
• Major branch of left coronary, supplying
40% of left ventricular muscle mass.
• Known as “the widow-maker”.
• Supplies the anterior and septal walls of
the LV.
• Supplies the Bundle of His and both
bundle branches.
Left Circumflex
• Supplies the lateral and posterior walls of
the left ventricle.
• Less common vessel to have primary
occlusion.
• Supplies blood to SA node in 45 % of pop.
• Supplies blood to AV node in 10 % of pop.
IMPORTANCE ???
• Based on the interpretation of a 12 lead
ECG, clinical presentation and
assessment, you are able to determine:
– Where the MI is located
– What vessel is involved
– What to expect with your patient
– What you can do to help the patient

How to tell if they’re…
Having the BIG ONE !!!

PLEASE NOTE !!!!
• The following information does not include
descriptions or examples of conditions or
disease processes that may interfere with
the ability to read or interpret an ECG.
• Paramedics interested in further ECG
interpretation should consider a Critical
Care Transport (CCT) Course or a specific
12-Lead ECG program.

Ischemia / Infarct Localization
• Determine baseline of ECG
• Find the J-point, move plus 0.04 seconds
– Point of Juncture (angle change) between the ending
of the QRS and the beginning of the ST
• Measure ST segment changes above or below
baseline
• What are we looking for?
– Changes of >1mm in two or more contiguous leads
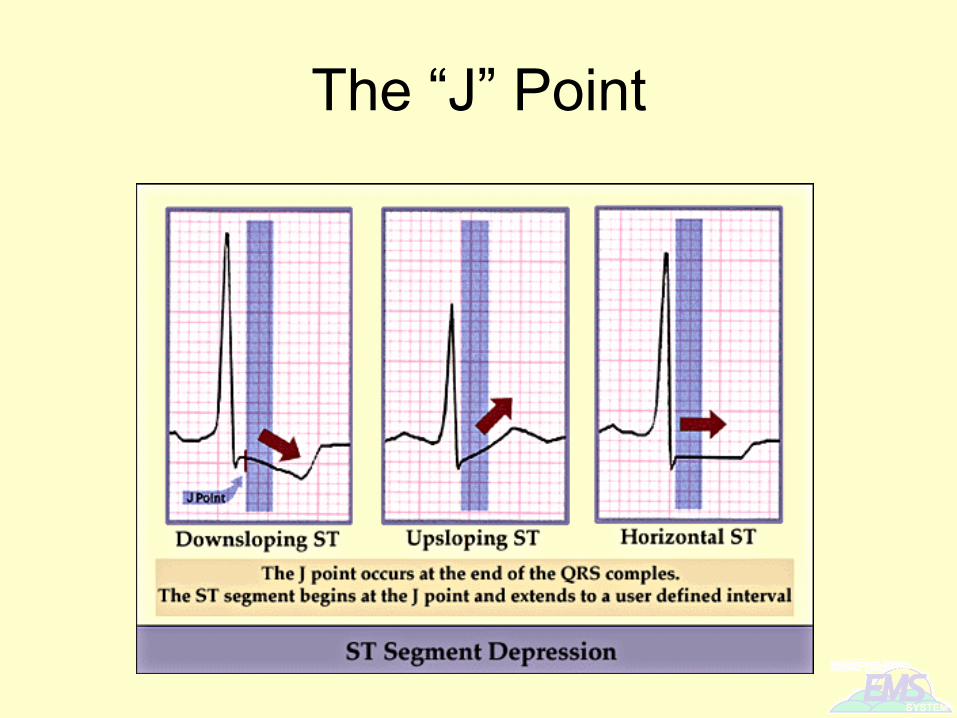
The “J” Point

• Check out this study
that tells that 29% of
Dr.’s measure at the J-
pt
and 43% measure at
the
J-pt plus 1 mm. The
results favored this pt
for measuring STEMI.Emerg Med J 2002; 19:126-128

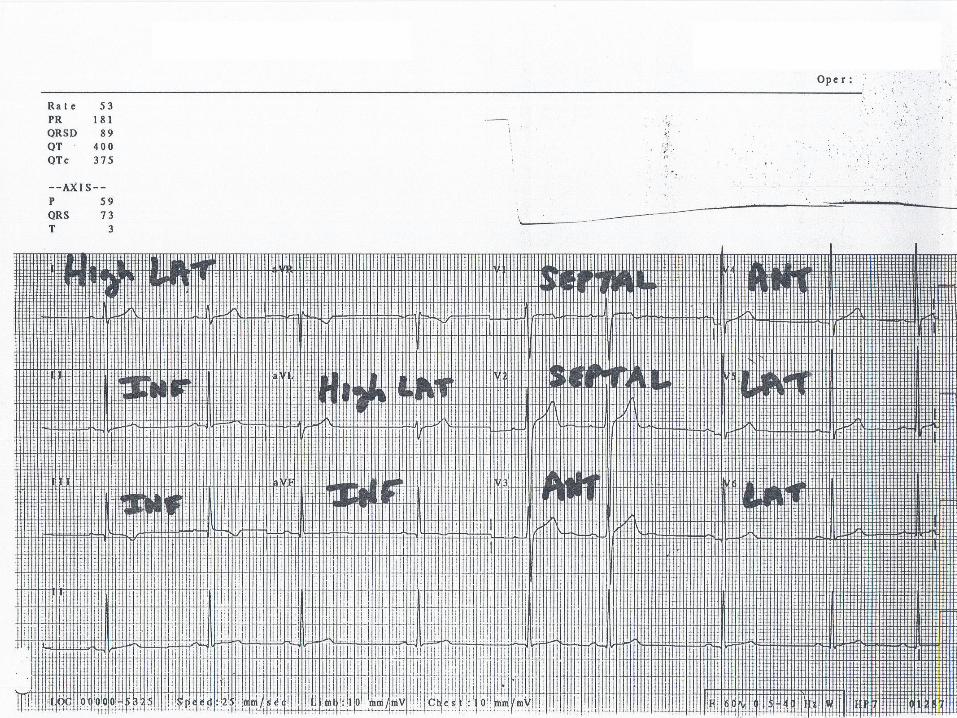
Finding an MI
• Assessing contiguous leads
• Ischemia and infarct localization
– I See All Leads (ISAL)
• What is the complex telling us?
– A look at common injury and ischemia
patterns.

Inferior Wall
• Leads II, III and aVF
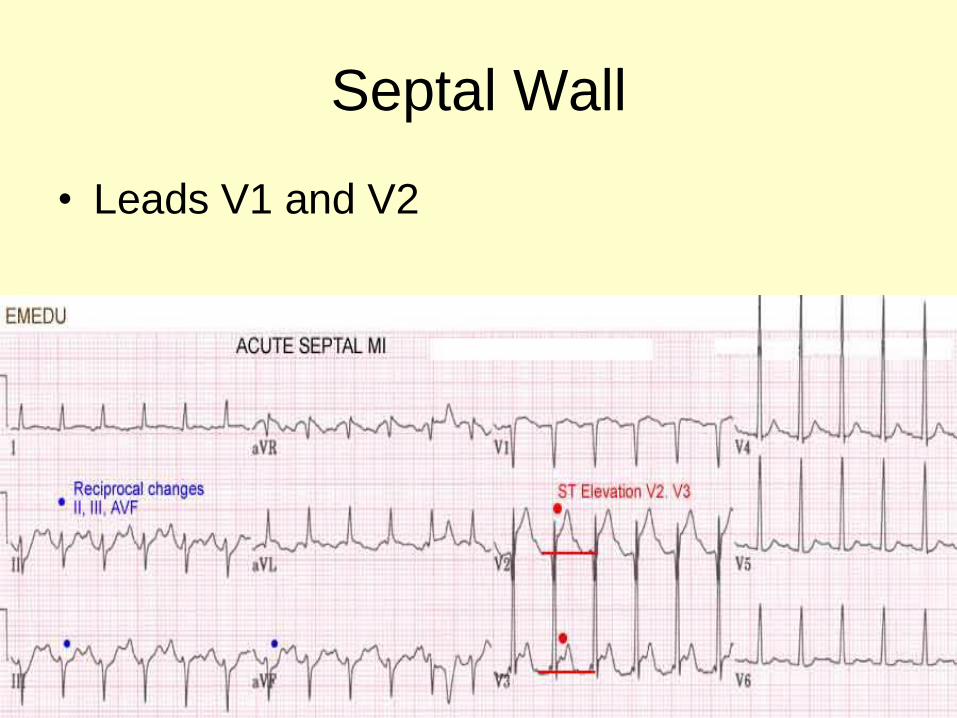
Septal Wall
• Leads V1 and V2
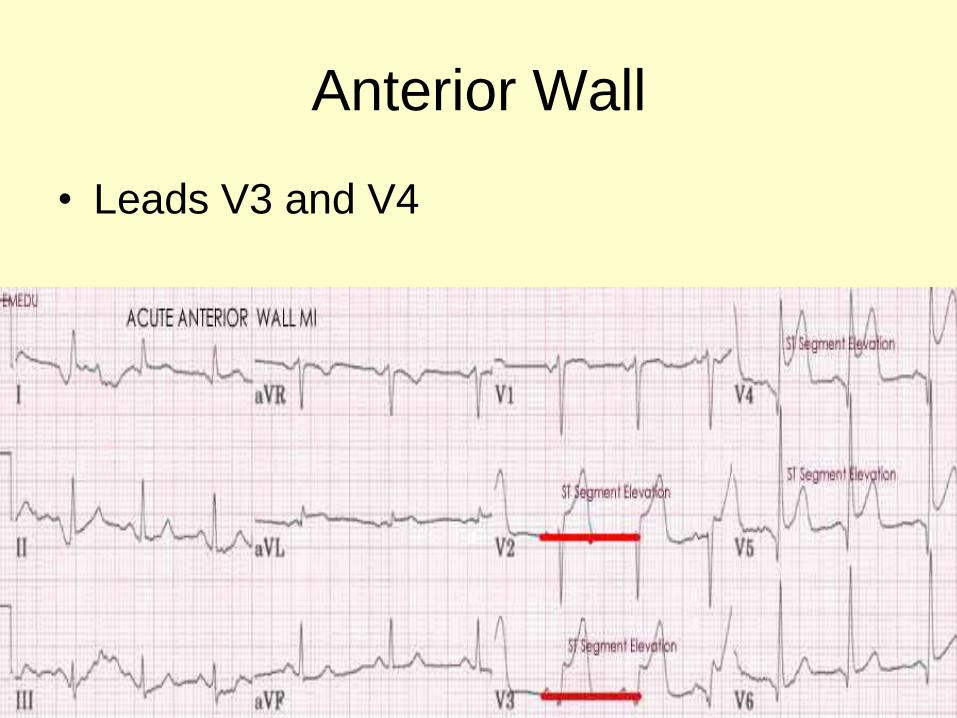
Anterior Wall
• Leads V3 and V4

Lateral Wall
• Leads V5 and V6
• Leads I and aVL (high lateral)
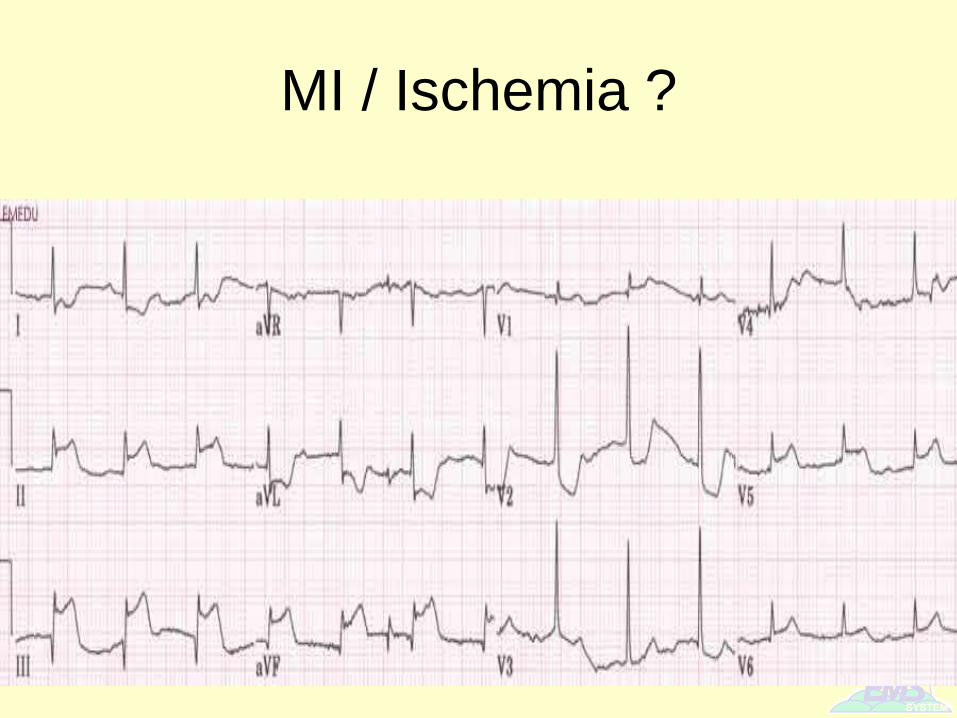
MI / Ischemia ?

MI / Ischemia ?
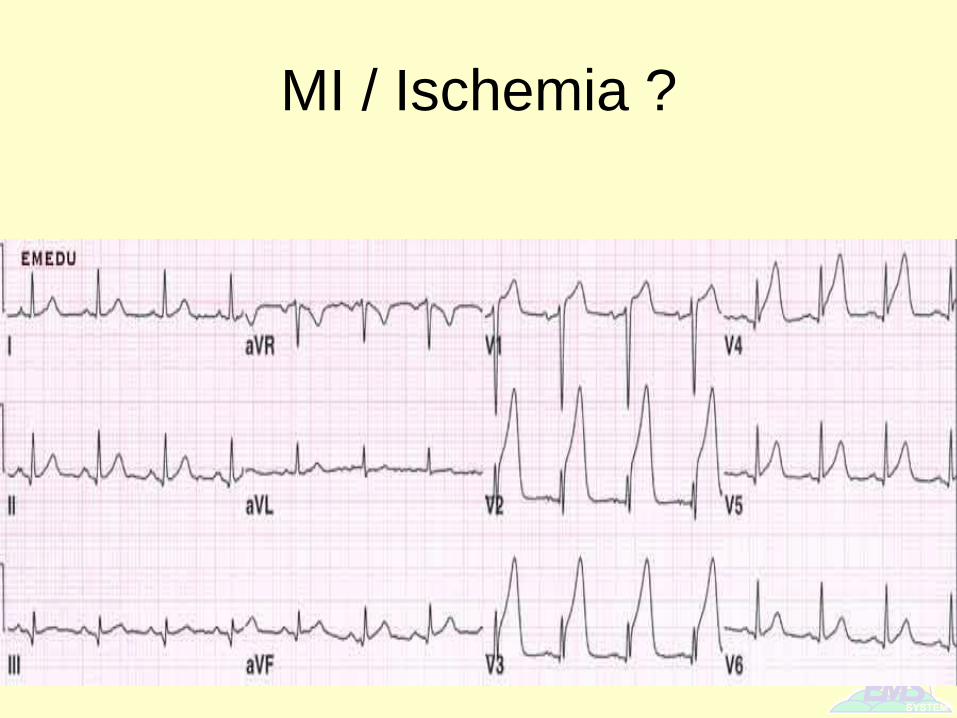
MI / Ischemia ?
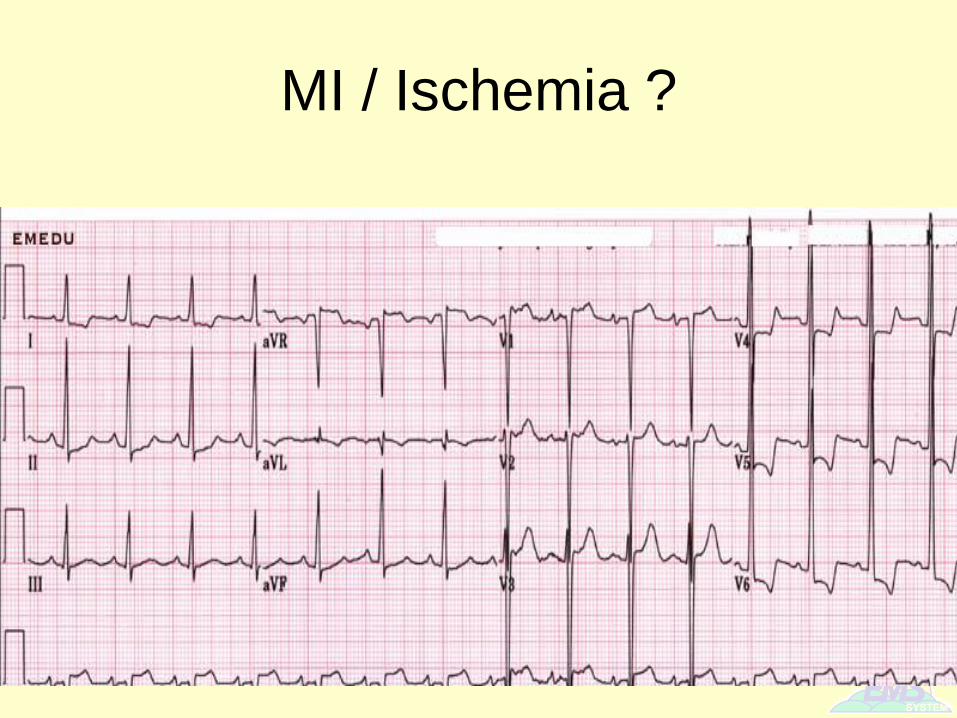
MI / Ischemia ?
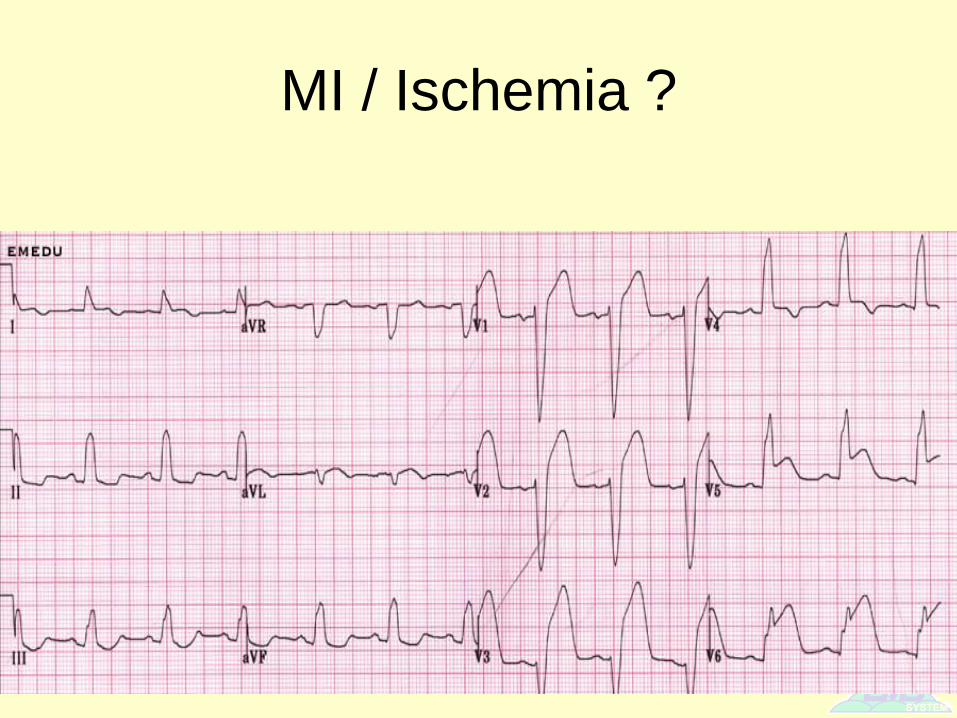
MI / Ischemia ?

Acute Coronary Syndromes
• Management discussion:
– Angina
– Myocardial Infarction
– Congestive Heart Failure
Angina Pectoris
• What is it?
– Pathophysiology is similar to MI
• chronic problem
• exertion induced
• rest improved
• treated with Nitroglycerin
• transient in nature
• When would we see this patient in BITP?
– Transfer to Cath Lab or ER-ER Transport

Myocardial Infarction (MI)
• Acute MI should always consider air transfer
first, then CCT ground second if time permits
(remember: time is muscle…)
• Treatment
– Consider presentation and MI location
– Anticipate needs of the patient
– O2, IV (prefer 2 lines), Monitor, SpO2
– NTG, Heparin drips
– Monitor for hemorrhage if thrombolytics administered
– Accurately assess, document, and manage pain

Congestive Heart Failure
• Definition
– inefficient pump
• Pathophysiology
– Input is greater than output
– Increased pressure causes backup of blood
– Where does blood back up?

CHF
• Right sided failure
– common causes• left sided failure
• MI
• cor pulmonale (pulmonary hypertension)
– systemic backup• + jugular vein distention
• gravity dependent edema (ie. pedal, sacral)
– What will lungs sound like?

CHF
• Left sided failure
– common causes
• systemic hypertension
• MI
– pulmonary backup
• pulmonary edema
CHF
• Acute Exacerbation Signs & Symptoms
– Dyspnea
– Orthopnea
– Pulmonary edema
– Pedal/Sacral edema
– JVD
– Pallor/cyanosis
– Diaphoresis

CHF
• General Treatment
– Calm & Reassure (Consider stability and need for CCT Transport)
– Position upright
– Oxygen
• NRB or BVM/PPV
• Consider intubation
– Continuous EKG, BP and O2 sat monitoring
– Nitroglycerin ???
– Morphine Sulfate ???
– Diuretics ???
– Bronchodilators ???

Questions / Comments ?







![PedsQL Quality of Life and Cardiac Module Inventories and ... · PedsQL™ Quality of Life and Cardiac Module Inventories and Conditions and Problems Questionnaire [CHSS Data Center]](https://static.fdocuments.us/doc/165x107/5afb416b7f8b9a19548f0a02/pedsql-quality-of-life-and-cardiac-module-inventories-and-quality-of-life.jpg)