Modeling psychiatric disorders at the cellular and network …...Although psychiatric disorders such...
15
EXPERT REVIEW Modeling psychiatric disorders at the cellular and network levels KJ Brennand, A Simone, N Tran and FH Gage Laboratory of Genetics, Salk Institute for Biological Studies, La Jolla, CA, USA Although psychiatric disorders such as autism spectrum disorders, schizophrenia and bipolar disorder affect a number of brain regions and produce a complex array of clinical symptoms, basic phenotypes likely exist at the level of single neurons and simple networks. Being highly heritable, it is hypothesized that these disorders are amenable to cell-based studies in vitro. Using induced pluripotent stem cell-derived neurons and/or induced neurons from fibroblasts, limitless numbers of live human neurons can now be generated from patients with a genetic background permissive to the disease state. We predict that cell-based studies will ultimately contribute to our understanding of the initiation, progression and treatment of these psychiatric disorders. Molecular Psychiatry advance online publication, 3 April 2012; doi:10.1038/mp.2012.20 Keywords: autism spectrum disorders; bipolar disorder; neurons; schizophrenia; stem cells Introduction Autism spectrum disorders (ASDs), schizophrenia (SCZD) and bipolar disorder (BD) combine to affect nearly 1 in 30 adults throughout the global popula- tion. 1 While these psychiatric disorders are character- ized by markedly different clinical phenotypes, recent genetic studies have suggested that they may share common underlying molecular causes. ASD, SCZD and BD are believed to be developmental in origin, resulting from events that occur in fetal development or early childhood. The molecular mechanism of these disorders is difficult to study in patients or animal models because of the complex genetic etiologies and varying environmental effects contri- buting to disease. Cell-based models produce live human neurons with genetic backgrounds permissive to the disease state. Temporal analysis of disease initiation and progression can be studied in the cell type relevant to disease. Human cell-based models can be ideal experimental paradigms with which to investigate disease mechanisms; for example, studies of amyo- trophic lateral sclerosis have revealed a non-cell autonomous contribution of glial cells to this neuronal disease. 2,3 In order to be studied using an in vitro model, a given disease must (1) be highly genetic, ensuring that cultured cells are afflicted by disease in the absence of any potentially unresolved environ- mental factors and (2) affect a cell type that can survive and, ideally, be robustly expanded when cultured in vitro. With respect to the first criterion, twin studies have calculated the heritability of ASD, SCZD and BD to be between 70 and 90%. 4–6 Our hypothesis is that this genetic predisposition to psychiatric illness is sufficient that cultured neurons will consistently undergo disease initiation and progression. Regarding the second criterion, while mature neurons are post- mitotic and cannot be expanded in culture, conditions for the survival of human neurons are well described, 7 and robust quantities of neurons for study can be generated through the growth and subsequent differ- entiation of proliferative neural progenitor cells. The ability to compare cellular and network proper- ties of live human neurons in vitro represents an important new approach with which to study psy- chiatric disease because live human neurons from patients or controls are exceedingly rare. Recently, three new sources of live human neurons have been reported: primary olfactory neural precursors, neurons differentiated from human-derived induced pluripo- tent stem cells (hiPSC neurons) and induced neurons (iNeurons) generated from primary patient fibroblasts. Although olfactory neural precursors are capable of self-renewal and differentiation to mature neurons, 8,9 olfactory neural precursors cannot yield cells from the neural lineages specifically implicated in psychiatric disorders, such as GABAergic or dopaminergic neurons. Because we believe it is critical that the relevant cell type affected in the disease state be studied, we will therefore focus on in vitro models of psychiatric disease utilizing hiPSC neurons and iNeurons (Figure 1). While generally considered to be whole-brain disorders, we suggest that ASD, SCZD and BD can be broken down to component aberrations at the Received 18 November 2011; revised 26 January 2012; accepted 16 February 2012 Correspondence: FH Gage, PhD, Laboratory of Genetics, Salk Institute for Biological Studies, 10010 North Torrey Pines Road, La Jolla, CA 92037, USA. E-mail: [email protected] Molecular Psychiatry (2012), 1–15 & 2012 Macmillan Publishers Limited All rights reserved 1359-4184/12 www.nature.com/mp
Transcript of Modeling psychiatric disorders at the cellular and network …...Although psychiatric disorders such...

EXPERT REVIEW
Modeling psychiatric disorders at the cellular andnetwork levelsKJ Brennand, A Simone, N Tran and FH Gage
Laboratory of Genetics, Salk Institute for Biological Studies, La Jolla, CA, USA
Although psychiatric disorders such as autism spectrum disorders, schizophrenia and bipolardisorder affect a number of brain regions and produce a complex array of clinical symptoms,basic phenotypes likely exist at the level of single neurons and simple networks. Being highlyheritable, it is hypothesized that these disorders are amenable to cell-based studies in vitro.Using induced pluripotent stem cell-derived neurons and/or induced neurons from fibroblasts,limitless numbers of live human neurons can now be generated from patients with a geneticbackground permissive to the disease state. We predict that cell-based studies will ultimatelycontribute to our understanding of the initiation, progression and treatment of thesepsychiatric disorders.Molecular Psychiatry advance online publication, 3 April 2012; doi:10.1038/mp.2012.20
Keywords: autism spectrum disorders; bipolar disorder; neurons; schizophrenia; stem cells
Introduction
Autism spectrum disorders (ASDs), schizophrenia(SCZD) and bipolar disorder (BD) combine to affectnearly 1 in 30 adults throughout the global popula-tion.1 While these psychiatric disorders are character-ized by markedly different clinical phenotypes, recentgenetic studies have suggested that they may sharecommon underlying molecular causes. ASD, SCZDand BD are believed to be developmental in origin,resulting from events that occur in fetal developmentor early childhood. The molecular mechanism ofthese disorders is difficult to study in patients oranimal models because of the complex geneticetiologies and varying environmental effects contri-buting to disease.
Cell-based models produce live human neuronswith genetic backgrounds permissive to the diseasestate. Temporal analysis of disease initiation andprogression can be studied in the cell type relevantto disease. Human cell-based models can be idealexperimental paradigms with which to investigatedisease mechanisms; for example, studies of amyo-trophic lateral sclerosis have revealed a non-cellautonomous contribution of glial cells to this neuronaldisease.2,3 In order to be studied using an in vitromodel, a given disease must (1) be highly genetic,ensuring that cultured cells are afflicted by disease inthe absence of any potentially unresolved environ-mental factors and (2) affect a cell type that can survive
and, ideally, be robustly expanded when culturedin vitro. With respect to the first criterion, twin studieshave calculated the heritability of ASD, SCZD and BDto be between 70 and 90%.4–6 Our hypothesis is thatthis genetic predisposition to psychiatric illness issufficient that cultured neurons will consistentlyundergo disease initiation and progression. Regardingthe second criterion, while mature neurons are post-mitotic and cannot be expanded in culture, conditionsfor the survival of human neurons are well described,7
and robust quantities of neurons for study can begenerated through the growth and subsequent differ-entiation of proliferative neural progenitor cells.
The ability to compare cellular and network proper-ties of live human neurons in vitro represents animportant new approach with which to study psy-chiatric disease because live human neurons frompatients or controls are exceedingly rare. Recently,three new sources of live human neurons have beenreported: primary olfactory neural precursors, neuronsdifferentiated from human-derived induced pluripo-tent stem cells (hiPSC neurons) and induced neurons(iNeurons) generated from primary patient fibroblasts.Although olfactory neural precursors are capable ofself-renewal and differentiation to mature neurons,8,9
olfactory neural precursors cannot yield cells from theneural lineages specifically implicated in psychiatricdisorders, such as GABAergic or dopaminergicneurons. Because we believe it is critical that therelevant cell type affected in the disease state bestudied, we will therefore focus on in vitro models ofpsychiatric disease utilizing hiPSC neurons andiNeurons (Figure 1).
While generally considered to be whole-braindisorders, we suggest that ASD, SCZD and BD canbe broken down to component aberrations at the
Received 18 November 2011; revised 26 January 2012; accepted16 February 2012
Correspondence: FH Gage, PhD, Laboratory of Genetics, SalkInstitute for Biological Studies, 10010 North Torrey Pines Road,La Jolla, CA 92037, USA.E-mail: [email protected]
Molecular Psychiatry (2012), 1–15& 2012 Macmillan Publishers Limited All rights reserved 1359-4184/12
www.nature.com/mp

cellular and/or network levels. For example, at thecellular level, the subtle synaptic defects that arebelieved to contribute to illness can be studied withcell-based models. Furthermore, while the cyclicalbehavioral swings of BD cannot be reproduced,patterns of spontaneous and stimulated neuronalnetwork activity can be measured in vitro. Usingcell-based models, one can study ASD, SCZD and BDby observing the abnormal development of neuronsand their circuitry in vitro.
In this review, we will discuss (1) post-mortem andanimal studies demonstrating that cellular pheno-types exist at the neuronal level in these disorders(Tables 1 and 2), (2) functional magnetic resonanceimaging (fMRI) and electrophysiological evidencefrom humans and rodents suggesting that networkdefects contribute to these disorders (Tables 1 and 2)and (3) the recent findings of novel in vitro models ofpsychiatric disorders (Table 3).
Evidence for cellular phenotypes in psychiatricdisorders
Aberrant neuronal connectivity, as assessed by den-dritic arborization and synaptic density, is a char-acteristic that appears to be shared between ASD,SCZD and BD. Perturbed neuronal migration has alsobeen linked to psychiatric disorders, althoughwhether this contributes to, or functions separatelyfrom, abnormal neuronal connectivity remains to bedemonstrated.
Altered dendritic arborizationAt onset, ASD is often characterized by excessive brainvolume; MRI studies observed increased cerebral whitematter volume in 2- to 4-year-old autistic children,10–12
which has been correlated with an excess number ofneurons in the prefrontal cortex.13 Over the lifetime ofthe ASD patient, however, the brain overgrowthphenotype is typically reversed; studies of adults withASD have observed cortical thinning14,15 and reducedfrontal lobe10,16,17 and corpus callosum18 volumes.While we found few anatomical post-mortem studies
of ASD, there are reports of reduced dendritic arboriza-tion in hippocampal neurons in two cases of ASD.19 InRett syndrome (RTT), a severe and rare ASD caused bythe mutation of the MECP2 gene,20,21 post-mortemstudies report reduced neuronal cell size and dendriticarborization throughout the cortex.22 Reports of fragileX syndrome (FX), another monogenetic form of ASD,have been less conclusive: while one study reporteddifferences in dendritic arborization following in vitrodifferentiation of neurospheres derived from post-mortem human FXS brain tissue,23 a second groupfailed to observe significant differences in a similarstudy.24
Decreased whole-brain volume is consistently ob-served in SCZD,25–27 particularly in the gray matter of thefrontal cortex, temporal lobe (particularly the hippo-campus and amygdala) and the basal ganglia,27–29 andlongitudinal studies report that progressive brainvolume declines for at least 20 years after the onsetof symptoms. Post-mortem studies of brains frompatients with SCZD have not found evidence ofneuronal loss; instead, they observe smaller neuronalsomas30,31 reduced dendritic arborizations31,32 andincreased neuronal density without changes in abso-lute cell number in the cortex and hippocampus.30,33
Decreased brain volumes in the limbic system,particularly the amygdala and hippocampus, and inthe frontal cortex are associated with BD.34,35 Itremains unclear, however, whether brain volumechanges are a preexisting factor contributing to thedevelopment of BD or a consequence of prolongedillness; one recent study suggests that brain volumechanges are more tightly correlated to active psycho-sis than BD.36 Despite observations of diminishedbrain volumes and reduced neuronal density in BDpatients,37,38 we found no report of altered dendriticarborization or synaptic density in post-mortemstudies of BD patient brains.
Mouse models of a number of psychiatric disordershave been developed. For the most part, these micehave reduced expression of rare, highly penetrantgenes implicated in ASD, SCZD or BD. RTT (Mecp2null) mouse brains show a reduction in neuronal size;39
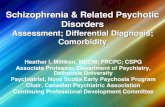
Figure 1 Cell-based modeling of psychiatric disorders. Fibroblast cells obtained from patients can be used to generate livehuman neurons with a genetic background known to produce the disease state. Fibroblasts can be reprogrammed to human-derived induced pluripotent stem cells (hiPSCs) by transient expression of OCT4, SOX2, KLF4 and cMYC and thensubsequently differentiated into mature neurons. Alternately, fibroblasts can be directly converted into a neuronal fate bytransient expression of ASCL1, BRN2, MYT1L and NEUROD.
iPSC modeling of psychiatric disordersKJ Brennand et al
2
Molecular Psychiatry

Table
1S
um
mary
of
pu
bli
shed
cell
ula
ran
dn
etw
ork
ph
en
oty
pes
inh
um
an
SC
ZD
pati
en
ts
Dis
ease
Stu
dy
Bra
inre
gio
n/c
ell
typ
eO
bse
rvati
on
Refe
ren
ce
AS
DM
RI,
post
-m
ort
em
Cere
bru
mIn
cre
ase
dcere
bra
lw
hit
em
att
er
volu
me
inch
ild
ren
,excess
nu
mber
of
neu
ron
sin
pre
fron
tal
cort
ex
inch
ild
ren
Carp
er
et
al.
,10
Cou
rch
esn
e,1
1H
azle
tet
al.
,12
Cou
rch
esn
eet
al.
13
AS
DM
RI
Cere
bru
m,
corp
us
call
osu
mR
ed
uced
fron
tal
an
dp
ari
eta
llo
be
gra
ym
att
er
volu
me
inold
er
ch
ild
ren
an
dad
ult
s,in
cre
ase
dven
tric
ula
rvolu
me,
red
uced
corp
us
call
osu
mvolu
me
Cou
rch
esn
eet
al.
,14
Sch
mit
zet
al.
,16
Bru
net
al.
,17
Wri
gh
tet
al.
,27
Fra
zie
ran
dH
ard
en
18
AS
DP
ost
-mort
em
Hip
pocam
pu
s,cort
ex
Red
uced
den
dri
tic
arb
ori
zati
on
inh
ipp
ocam
pu
s,gre
ate
rcort
ical
pyra
mid
al
spin
ed
en
sity
corr
ela
ted
wit
hd
ecre
ase
dcogn
itiv
efu
ncti
on
,lo
ssof
vert
ical
an
dh
ori
zon
tal
org
an
izati
on
of
cort
ical
layers
Raym
on
det
al.
,19
Hu
tsle
ran
dZ
han
g,4
8
Wegie
let
al.
72
AS
DfM
RI
Cort
ex
Incre
ase
dcon
necti
vit
ybetw
een
pro
xim
al:
post
eri
or
cin
gu
late
/para
hip
pocam
pal
gyru
s,d
ecre
ase
dcon
necti
vit
ybetw
een
dis
tal:
fron
tal
lobe-p
ari
eta
llo
be,
insu
lar
cort
ices-
som
ato
sen
sory
cort
ices
of
am
ygd
ala
,fr
on
tal
cort
ex-p
ost
eri
or
cin
gu
late
d,
decre
ase
din
terh
em
isp
heri
csy
nch
ron
izati
on
Mon
ket
al.
,80
Ken
ned
yan
dC
ou
rch
esn
e,8
1
Ebis
ch
et
al.
,82
Din
stein
et
al.
,83
Ken
ned
yan
dC
ou
rch
esn
e84
AS
D(R
TT
)P
ost
-mort
em
Cort
ex,
hip
pocam
pu
sR
ed
uced
cell
size
an
dd
en
dri
tic
arb
ori
zati
on
incort
ex,
red
uced
nu
mber
of
den
dri
tic
spin
es
inh
ipp
ocam
pu
s
Bau
man
et
al.
,22
Ch
ap
leau
et
al.
49
AS
D(F
X)
Invit
roP
ost
-mort
em
neu
rosp
here
cu
ltu
re,
feta
lcort
ical
NP
Ccu
ltu
re
Neu
ron
sw
ith
few
er
an
dsh
ort
er
neu
rite
s,sm
all
er
cell
bod
yvolu
me
an
dd
ecre
ase
dgli
al
dif
fere
nti
ati
on
;n
orm
al
neu
rogen
esi
sby
feta
lN
PC
s
Cast
ren
et
al.
,23
Bh
att
ach
ary
ya
et
al.
24
AS
D(F
X)
Post
-mort
em
Cort
ical
pyra
mid
al
cell
sL
on
ger,
more
slen
der
den
dri
tic
spin
esh
ap
eIr
win
et
al.
50
SC
ZD
MR
IG
ray
matt
er
fron
tal
cort
ex,
tem
pora
llo
be,
hip
pocam
pu
s,am
ygd
ala
,basa
lgan
gli
a
Decre
ase
dvolu
me
(wh
ole
bra
in)
inearl
yp
hase
SC
ZD
Vit
aet
al.
,25
Ste
en
et
al.
,26
Th
om
pso
net
al.
,28
Ell
ison
-Wri
gh
tet
al.
29
SC
ZD
Post
-mort
em
Cort
ex,
hip
pocam
pu
sR
ed
uced
den
dri
tic
arb
ori
zati
on
,re
du
ced
som
asi
ze,
incre
ase
dn
eu
ron
al
den
sity
,d
ecre
ase
dsy
nap
tic
den
sity
Rajk
ow
ska
et
al.
,30
Kolo
meets
et
al.
,31
Bla
ck
et
al.
,32
Sele
mon
et
al.
,33
Gare
yet
al.
,51
Gla
ntz
an
dL
ew
is52,
Kolo
meets
et
al.
53
SC
ZD
fMR
IF
ron
tal/
tem
pora
llo
be
Bra
inacti
vit
yabn
orm
ali
tyin
fron
tal
an
dte
mp
ora
llo
bes
Yu
rgelu
n-T
od
det
al.
,85
Yu
rgelu
n-T
od
det
al.
86
SC
ZD
fMR
IC
ort
ex
Cort
ical
hyp
er-
acti
vit
yan
dh
yp
er-
con
necti
vit
yin
pre
fron
tal
cort
ex
at
rest
,re
du
ced
acti
vati
on
of
med
ial
pre
fron
tal
du
rin
gw
ork
ing
mem
ory
task
sin
earl
yp
hase
SC
ZD
,in
cre
ase
dfu
ncti
on
al
con
necti
vit
ybetw
een
the
ven
tral
pre
fron
tal
cort
ex
an
dp
ost
eri
or
pari
eta
lcort
ex
gre
ate
r,d
ecre
ase
dfu
ncti
on
al
con
necti
vit
ybetw
een
the
dors
al
pre
fron
tal
cort
ex
an
dp
ost
eri
or
pari
eta
lcort
ex
gre
ate
r
Wh
itfi
eld
-Gabri
eli
et
al.
,87
Tan
et
al.
88
iPSC modeling of psychiatric disordersKJ Brennand et al
3
Molecular Psychiatry

and abnormalities in dendritic arborization.39–41 Con-versely, dendritic arborization defects have not beenreported in FX (Fmr1 null) mice. Many SCZD mousemodels, including Disc1 and heterozygous-null Nrg1and Erbb4 mice, have reduced neurite outgrowthand reduced dendritic complexity.42–45 Although fewgenetic mouse models of BD have been reported,neurons from mice with a point mutation in thecircadian Clock gene display complex changes indendritic morphology,46 which can be ameliorated withlithium, a drug routinely used in the treatment of BD.46
Altered synaptic densityA number of genes implicated in ASD, SCZD and BDhave been associated with synaptic maturation andfunction.47 Post-mortem synaptic spine density has notbeen adequately explored in human patients withASD. One report found that relative to controls, spinedensities on cortical pyramidal cells were greater inASD subjects, and highest spine densities were mostcommonly found in ASD subjects with lower levels ofcognitive functioning.48 Conversely, the number ofspines in dendrites of neurons from post-mortem RTTbrains is reduced.49 In FX patients, post-mortemstudies have identified abnormalities in dendriticspine shape in cortical pyramidal cells, which tendto be both longer and more slender than controls.50
Post-mortem studies of SCZD patient brains foundreduced dendritic spine density in the cortex51,52 andhippocampus.31,53 What post-mortem analysis of ASDand SCZD has failed to resolve is whether diseaseprogression reflects developmental aberrations duringneuronal differentiation or activity-dependent atrophyof neuronal dendrites or synapses in mature neurons.33
Animal studies recapitulate these synaptic defects.Using mouse models of RTT, decreased Mecp2levels have been implicated in defects of synapticcontact formation and synaptic transmission.41,54–56
Comparably, inherited mutations of Shank3, whichalso model ASD, result in reduced dendritic synapticspine induction and maturation.57 Similar to post-mortem observations of FX patient brains, Fmr1 micehave abnormally thin and elongated dendritic spinemorphology and greater spine density.58 Fmr1, thegene affected in FX, regulates the translation ofmessages important for activity-dependent synapticmodulation.59 Although a number of animal models ofASD recapitulate defects in synaptic maturation, thedirection of the change varies depending uponthe gene under investigation, which is consistent withthe hypothesis that ASD is a spectrum of complexgenetic disorders involving impaired developmentalsynaptic maturation, stabilization, elimination orpruning. Studies of mouse models of SCZD have alsoobserved synaptic defects; there is reduced hippo-campal synaptic transmission in Disc1 mice,42,43
impaired synaptic maturation and function in Nrg1mice60–62 and fewer cortical neurons with slightlysmaller spines in mouse models of the human SCZDcopy number variant at 22q11.2.63–65 In mice withreduced Reelin (Reln) expression (putative models ofT
able
1C
on
tin
ued
Dis
ease
Stu
dy
Bra
inre
gio
n/c
ell
typ
eO
bse
rvati
on
Refe
ren
ce
SC
ZD
An
ato
mic
al
netw
ork
san
aly
sis
Cort
ex
Cort
ical
org
an
izati
on
alt
ere
d,
loss
of
netw
ork
hu
bs
infr
on
tal
cort
ex,em
erg
en
ce
of
hu
bs
ou
tsid
ecort
ex
Bass
ett
et
al.
89
SC
ZD
Post
-mort
em
,P
ET
Su
bst
an
ian
igra
,st
riatu
m,
cort
ex
Incre
ase
dD
Are
cep
tor
sen
siti
vit
y,in
cre
ase
dD
Are
cep
tor
levels
insu
bst
an
ian
igra
,corr
ela
tion
of
DA
recep
tor
exp
ress
ion
level
inte
mp
ora
lcort
ex
an
dst
riatu
mto
posi
tive
sym
pto
ms
of
SC
ZD
Ow
en
et
al.
,91
Kess
ler
et
al.
,90
SC
ZD
Ph
arm
acolo
gy
Not
dete
rmin
ed
NM
DA
an
tagon
ist
keta
min
ein
du
ces
SC
ZD
-lik
esy
mp
tom
s,M
GL
UR
2/3
agon
ists
am
eli
ora
teth
em
Kry
stal
et
al.
,92
Pati
let
al.
93
SC
ZD
Post
-mort
em
Hip
pocam
pu
s,cort
ex
Red
uced
GL
Ure
cep
tor
exp
ress
ion
Mead
or-
Wood
ruff
an
dH
ealy
94
BD
MR
IL
imbic
syst
em
(am
ygd
ala
/h
ipp
ocam
pu
s)R
ed
uced
bra
involu
me:
lim
bic
syst
em
(am
ygd
ala
,h
ipp
ocam
pu
s,fr
on
tal
cort
ex)
inad
ole
scen
tsK
arc
hem
skiy
et
al.
,34
Fra
zie
r,35
BD
Post
-mort
em
En
torh
inal
cort
ex
Decre
ase
dcell
nu
mber
an
dd
en
sity
of
GA
BA
neu
ron
sR
ajk
ow
ska
et
al.
,37
Pan
tazop
ou
los
et
al.
38
Abbre
via
tion
s:A
SD
,au
tism
spectr
um
dis
ord
er;
BD
,bip
ola
rd
isord
er;
DA
,d
op
am
ine;
GL
U,
glu
tam
ate
;F
X,
fragil
eX
syn
dro
me;
fMR
I,fu
ncti
on
al
magn
eti
cre
son
an
ce
imagin
g;
MR
I,m
agn
eti
cre
son
an
ce
imagin
g;
NP
C,
neu
ral
pro
gen
itor
cell
;R
TT
,R
ett
syn
dro
me;
SC
ZD
,sc
hiz
op
hre
nia
dis
ord
er.
iPSC modeling of psychiatric disordersKJ Brennand et al
4
Molecular Psychiatry

Table
2S
um
mary
of
pu
bli
shed
cell
ula
ran
dn
etw
ork
ph
en
oty
pes
inro
den
tm
od
els
of
SC
ZD
Dis
ease
Gen
eB
rain
regio
n/c
ell
typ
eO
bse
rvati
on
Refe
ren
ce
AS
DC
ntn
ap
2C
ort
ex,
GA
BA
Imp
air
ed
mig
rati
on
of
cort
ical
pro
jecti
on
neu
ron
s,re
du
ced
GA
BA
erg
icn
eu
ron
s,d
ecre
ase
dn
eu
ral
syn
ch
ron
yP
en
agari
kan
oet
al.
100
AS
DS
han
k3
Hip
pocam
pal
neu
ral
cu
ltu
res
Red
uced
den
dri
tic
spin
ein
du
cti
on
/matu
rati
on
invit
roD
ura
nd
et
al.
57
AS
D(R
TT
)M
ecp
2H
ipp
ocam
pu
s,cort
ex,
cere
bell
um
,re
tin
ogen
icu
late
syn
ap
se,
NP
Cs
Red
ucti
on
inn
eu
ron
al
size,
den
dri
tic
arb
ori
zati
on
abn
orm
ali
ties,
thin
ner
cort
ical
layers
,re
du
ced
spin
ed
en
sity
,d
efe
cts
insy
nap
tic
matu
rati
on
an
dsy
nap
tic
tran
smis
sion
,im
pair
ed
exp
eri
en
ce
dep
en
den
tre
mod
eli
ng,
an
dalt
ere
dgen
eexp
ress
ion
Ch
en
et
al.
,39
Kis
hi
an
dM
ackli
s,40
Sm
rtet
al.
,41
Asa
ka
et
al.
,54
More
tti
et
al.
,55
Nels
on
et
al.
,56
Nou
tel
et
al.
,98
Dan
iet
al.
99
AS
D(F
X)
Fm
r1C
ort
ex,
neu
rosp
here
cu
ltu
reT
hin
an
delo
ngate
dd
en
dri
tic
spin
es
on
pyra
mid
al
neu
ron
s,in
cre
ase
dsp
ine
den
sity
alo
ng
ap
ical
den
dri
tes,
invit
rod
iffe
ren
tiate
dn
eu
ron
sh
ave
few
er
an
dsh
ort
er
neu
rite
san
da
small
er
cell
bod
yvolu
me
Com
ery
et
al.
,58
Cast
ren
et
al.
23
SC
ZD
Dis
c1
Cort
ex,
hip
pocam
pu
sR
ed
ucti
on
infe
tal
cort
ical
neu
ral
pro
gen
itor
pro
life
rati
on
an
dp
rem
atu
ren
eu
ral
dif
fere
nti
ati
on
,re
du
ced
cort
ical
mig
rati
on
,d
imin
ish
ed
resp
on
seto
cA
MP
-sen
siti
ve
rep
uls
ive
cu
es,
red
uced
neu
rite
ou
tgro
wth
,sy
nap
tic
tran
smis
sion
an
dalt
ere
dd
istr
ibu
tion
of
hip
pocam
pal
neu
ron
s
Mao
et
al.
,67
Kam
iya
et
al.
,74
Kvajo
et
al.
,42
Li
et
al.
43
SC
ZD
Dis
c1
kn
ockd
ow
nH
ipp
ocam
pal
ad
ult
-born
neu
ron
sA
du
ltn
ew
born
neu
ron
ssh
ow
accele
rate
dd
en
dri
tic
develo
pm
en
tan
dsy
nap
sefo
rmati
on
,d
efe
cts
inaxon
al
targ
eti
ng,
en
han
ced
excit
abil
ity
Fau
lker
et
al.
,70
Du
an
et
al.
69
SC
ZD
Nrg
1C
ort
ex,
peri
ph
era
ln
erv
es
Aberr
an
tta
ngen
tial
mig
rati
on
of
neu
ron
sd
eri
ved
from
the
ven
tral
tele
ncep
halo
n,
imp
air
ed
syn
ap
tic
matu
rati
on
an
dfu
ncti
on
,h
yp
om
yeli
nati
on
Lop
ez-B
en
dit
oet
al.
,44
Barr
os
et
al.
,60
Ch
en
et
al.
62
SC
ZD
Erb
B4
Hip
pocam
pu
s,cort
ex
Aberr
an
tn
eu
rite
ou
tgro
wth
an
dsy
nap
sem
atu
rati
on
,re
du
ced
lon
g-t
erm
pote
nti
ati
on
,su
pp
ress
ed
Src
-dep
en
den
ten
han
cem
en
tof
NM
DA
Rre
spon
ses
du
rin
gth
eta
-bu
rst
stim
ula
tion
,re
du
ced
excit
ato
ryin
pu
ton
toG
AB
Aerg
icn
eu
ron
s,P
PI
defi
cit
s
Kri
vosh
eya
et
al.
,45
Pit
ch
er
et
al.
,61
Pit
ch
er
et
al.
,101
Barr
os
et
al.
,60
Li
et
al.
,95
Ch
en
et
al.
62
SC
ZD
22q11.2
Cort
ex,
hip
pocam
pu
sF
ew
er
cort
ical
neu
ron
sw
ith
small
er
spin
es,
alt
ere
dsh
ort
-an
dlo
ng-
term
syn
ap
tic
pla
stic
ity
an
dcalc
ium
kin
eti
cs,
imp
air
ed
hip
pocam
pal-
pre
fron
tal
syn
ch
ron
y
Fen
elo
net
al.
63
Earl
set
al.
,64
Sig
urd
sson
et
al.
65
SC
ZD
Reln
Cort
ex,
hip
pocam
pu
sD
ecre
ase
dd
en
dri
tic
spin
em
atu
rati
on
,d
en
sity
an
dp
last
icit
yP
ap
pas
et
al.
66
SC
ZD
Dtn
bp
1G
AB
AD
ecre
ase
dP
PI,
red
uced
evoked
gam
ma
acti
vit
yC
arl
son
et
al.
104
BD
Clo
ck
Str
iatu
m(n
ucle
us
accu
mben
s)In
cre
ase
dle
ngth
an
dcom
ple
xit
yof
den
dri
tes,
norm
al
syn
ap
tic
den
sity
,d
ysf
un
cti
on
al
gam
ma
acti
vit
yacro
ssli
mbic
cir
cu
its,
imp
roved
by
lith
ium
treatm
en
t
Dzir
asa
et
al.
46
Abbre
via
tion
s:A
SD
,au
tism
spectr
um
dis
ord
er;
BD
,bip
ola
rd
isord
er;
FX
,fr
agil
eX
syn
dro
me;
PP
I,p
rep
uls
ein
hib
itio
n;
RT
T,
Rett
syn
dro
me;
SC
ZD
,sc
hiz
op
hre
nia
dis
ord
er.
iPSC modeling of psychiatric disordersKJ Brennand et al
5
Molecular Psychiatry

Table
3S
um
mary
of
pu
bli
shed
rep
ort
sof
hiP
SC
-base
dm
od
els
of
AS
D,
SC
ZD
an
dB
D
Dis
ease
Refe
ren
ce
Gen
eti
cm
uta
tion
Neu
ron
al
ph
en
oty
pe
hiP
SC
meth
od
Sou
rce
of
cell
sP
ati
en
tse
x;
age
at
bio
psy
(years
);avail
able
ph
en
oty
pic
info
rmati
on
RT
TC
heu
ng
et
al.
122
MeC
P2
(D3–4,
T158
M,
R306C
)D
ecre
ase
dso
ma
size
Retr
ovir
us:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
pati
en
tbio
psy
(1)
an
dC
ori
ell
GM
11270
(2),
GM
17880
(3)
(1)
Fem
ale
;6
gro
wth
an
dd
evelo
pm
en
tal
dela
y,in
abil
ity
tow
alk
wit
hou
tass
ista
nce,
ata
xia
,n
on
verb
al,
has
no
han
du
sean
dcon
stan
tre
peti
tive
han
dm
oti
on
s,so
me
trem
or,
has
had
ep
ilep
tic
seiz
ure
san
dsi
gn
ific
an
tabn
orm
al
ele
ctr
oen
cep
halo
gra
m,
teeth
gri
nd
ing,
som
esl
eep
dif
ficu
ltie
s,an
dbre
ath
hold
ing
an
dh
yp
erv
en
tila
tion
(2)
Fem
ale
;8;
norm
al
lyso
som
al
en
zym
es,
cli
nic
all
yaff
ecte
d,
cla
ssic
al
sym
pto
ms
(3)
Fem
ale
;5;ass
ista
nce
requ
ired
for
walk
ing,d
ela
yin
gro
wth
an
dd
evelo
pm
en
t,sl
eep
pro
ble
ms,
abn
orm
al
EE
Gw
ith
no
sym
pto
ms
of
seiz
ure
s,gri
nd
ing
of
teeth
,bre
ath
hold
ing,
hyp
erv
en
tila
tion
,n
on
verb
al,
lack
of
han
du
sage,
rep
eti
tive
han
dm
oti
on
s,d
iffi
cu
lty
eati
ng
an
dsl
igh
tre
flu
xes,
slig
ht
trem
or,
small
feet
RT
TM
arc
hett
oet
al.
123
MeC
P2
(1155d
el3
,Q
244X
,T
158
M,
R306C
)
Red
uced
som
asi
ze
an
dsp
ine
den
sity
,fe
wer
syn
ap
ses,
alt
ere
dcalc
ium
sign
ali
ng,
ele
ctr
op
hysi
olo
gic
al
abn
orm
ali
ties
Retr
ovir
us:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
Cori
ell
GM
11272
(1),
GM
16548
(2),
GM
17880
(3),
GM
11270
(4)
(1)
Fem
ale
;3;
norm
al
lyso
som
al
en
zym
es,
cli
nic
all
yaff
ecte
d,
cla
ssic
al
sym
pto
ms
(2)
Fem
ale
;5;
cli
nic
all
yaff
ecte
d,
slig
htl
ycu
rved
spin
e,
am
bu
lato
ry,
slig
ht
rigid
ity
an
dsp
ast
icit
y,d
ecre
asi
ng
head
cir
cu
mfe
ren
ce,
aberr
an
tsl
eep
patt
ern
s,d
ecre
ase
dh
an
du
sage,
rep
eti
tive
han
dm
oti
on
s,bre
ath
hold
ing,
non
verb
al,
con
stip
ati
on
,d
ecre
ase
dh
an
dan
dfe
et
cir
cu
lati
on
,ra
rese
lf-
inju
riou
sbeh
avio
r,sl
igh
teati
ng
pro
ble
ms
an
dre
flu
zes,
teeth
gri
nd
ing,
slig
ht
EE
Gabn
orm
ali
ties,
trem
ors
(3)
Fem
ale
;5;ass
ista
nce
requ
ired
for
walk
ing,d
ela
yin
gro
wth
an
dd
evelo
pm
en
t,sl
eep
pro
ble
ms,
abn
orm
al
EE
Gw
ith
no
sym
pto
ms
of
seiz
ure
s,gri
nd
ing
of
teeth
,bre
ath
hold
ing,
hyp
erv
en
tila
tion
,n
on
verb
al,
lack
of
han
du
sage,
rep
eti
tive
han
dm
oti
on
s,d
iffi
cu
lty
eati
ng
an
dsl
igh
tre
flu
xes,
slig
ht
trem
or,
small
feet
(4)
Fem
ale
;8;
norm
al
lyso
som
al
en
zym
es,
cli
nic
all
yaff
ecte
d,
cla
ssic
al
sym
pto
ms
RT
TA
nan
iev
et
al.
124
MeC
P2
(T158
M,
V247X
,R
306C
)D
ecre
ase
inn
ucle
ar
an
dn
eu
ron
size
Len
tivir
us:
fou
rfa
cto
rs(O
CT
4,N
AN
OG
,S
OX
2,
LIN
28),
Retr
ovir
us:
4fa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
Cori
ell
GM
17880
(1),
GM
07982
(2),
GM
11270
(3)
(1)
Fem
ale
;5;ass
ista
nce
requ
ired
for
walk
ing,d
ela
yin
gro
wth
an
dd
evelo
pm
en
t,sl
eep
pro
ble
ms,
abn
orm
al
EE
Gw
ith
no
sym
pto
ms
of
seiz
ure
s,gri
nd
ing
of
teeth
,bre
ath
hold
ing,
hyp
erv
en
tila
tion
,n
on
verb
al,
lack
of
han
du
sage,
rep
eti
tive
han
dm
oti
on
s,d
iffi
cu
lty
eati
ng
an
dsl
igh
tre
flu
xes,
slig
ht
trem
or,
small
feet
(2)
Fem
ale
;25;
cli
nic
all
yaff
ecte
d,
mic
rocep
haly
,se
vere
lyre
tard
ed
,h
an
dw
rin
gin
gst
art
ing
at
age
2,
scoli
osi
sat
age
12,
kyp
hosc
oli
osi
sat
age
25,
start
ed
tolo
sesk
ills
at
2years
old
,C
Tsc
an
at
25
show
ed
atr
op
hy,
slow
,abn
orm
al
EE
G,
no
sleep
pro
ble
ms
(3)
Fem
ale
;8;
norm
al
lyso
som
al
en
zym
es,
cli
nic
all
yaff
ecte
d,
cla
ssic
al
sym
pto
ms
iPSC modeling of psychiatric disordersKJ Brennand et al
6
Molecular Psychiatry

Table
3C
on
tin
ued
Dis
ease
Refe
ren
ce
Gen
eti
cm
uta
tion
Neu
ron
al
ph
en
oty
pe
hiP
SC
meth
od
Sou
rce
of
cell
sP
ati
en
tse
x;
age
at
bio
psy
(years
);avail
able
ph
en
oty
pic
info
rmati
on
Tim
oth
ysy
nd
rom
eP
asc
aet
al.
129
CA
CN
A1C
Defe
cts
incalc
ium
sign
ali
ng,
decre
ase
dexp
ress
ion
of
cort
ical
gen
es,
incre
ase
dp
rod
ucti
on
of
nore
pin
ep
hri
ne
an
dd
op
am
ine
Retr
ovir
us:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
pati
en
tbio
psy
(1)
Fem
ale
;n
ot
state
d;
not
state
d(2
)N
ot
state
d;
not
state
d;
not
state
d
FX
SU
rbach
et
al.
127
FM
R1
No
neu
ron
sgen
era
ted
Retr
ovir
us:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
Cori
ell
GM
05848
(1),
GM
07072
(2),
GM
09497
(3)
(1)
Male
;4;in
cre
ase
dear
size,elo
ngate
dfa
ce,ap
pears
pro
gn
ath
ic,
men
tal
reta
rdati
on
,u
nd
efi
ned
con
necti
ve
tiss
ue
dysp
lasi
a(2
)M
ale
;22;
9/5
0cord
blo
od
lym
ph
ocyte
ssh
ow
ed
fra(X
),m
oth
er
isan
obli
gate
carr
ier
for
fra(x
)(3
)M
ale
;28;
aff
ecte
dbro
ther,
larg
eears
,m
en
tal
reta
rdati
on
,m
acro
-orc
hid
ism
,h
yp
era
cti
ve,
20%
of
PB
Lp
osi
tive
for
fra(x
)
FX
SS
heri
dan
et
al.
128
FM
R1
Few
er
an
dsh
ort
er
neu
ral
pro
cess
es,
incre
ase
dgli
al
cell
sw
ith
more
com
pact
morp
holo
gy
Retr
ovir
us:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
Cori
ell
GM
05848
(1),
GM
05131
(2),
GM
05185
(3)
(1)
Male
;4;in
cre
ase
dear
size,elo
ngate
dfa
ce,ap
pears
pro
gn
ath
ic,
men
tal
reta
rdati
on
,u
nd
efi
ned
con
necti
ve
tiss
ue
dysp
lasi
a(2
)M
ale
;3;
aff
ecte
dbro
ther
an
du
ncle
,(3
)M
ale
;26;
46,f
ra(X
),Y
pre
sen
tin
30–50%
of
PB
L
SC
ZD
Ch
ian
get
al.
131
DIS
C1
No
neu
ron
sgen
era
ted
Ep
isom
e:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
pati
en
tbio
psy
(1)
Male
;N
A;
dia
gn
ose
dw
ith
ch
ron
icu
nd
iffe
ren
tiate
dsc
hiz
op
hre
nia
,au
dit
ory
an
dvis
ual
hall
ucin
ati
on
s,m
ult
iple
delu
sion
san
dh
ad
form
al
thou
gh
td
isord
er
(2)
Fem
ale
;N
A;
dia
gn
ose
dch
ron
icp
ara
noid
sch
izop
hre
nia
,au
dit
ory
an
dvis
ual
hall
ucin
ati
on
s,m
ult
iple
delu
sion
san
dh
ad
form
al
thou
gh
td
isord
er
SC
ZD
Bre
nn
an
det
al.
132
Sp
ora
dic
Red
uced
neu
ron
al
con
necti
vit
y,fe
wer
neu
rite
s,d
ecre
ase
dP
SD
95
an
dglu
tam
ate
recep
tor
exp
ress
ion
levels
Tetr
acycli
ne-i
nd
ucib
lele
nti
vir
us:
five
facto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
,LIN
28)
Fib
robla
st:
Cori
ell
GM
02038
(1),
GM
01792
(2),
GM
01835
(3),
GM
02497
(4)
(1)
Male
;22;
on
set
at
age
6,
com
mit
ted
suic
ide
(2)
Male
;26;
recu
rren
ces
of
agit
ati
on
,d
elu
sion
sof
pers
ecu
tion
,fe
ar
of
ass
ass
inati
on
,fa
ther
an
dsi
ster
aff
ecte
d(3
)F
em
ale
;27;
sch
izoaff
ecti
ve
dis
ord
er,
pro
ble
ms
of
dru
gabu
se,
hosp
itali
zed
,fa
ther
aff
ecte
d(4
)M
ale
;23;
para
logic
al
thin
kin
g,
spli
ttin
gof
eff
ect
from
con
ten
t,su
spic
iou
sness
,aff
ecti
ve
shie
ldin
g,
on
set
at
age
15,
hosp
itali
zed
,p
osi
tive
fam
ily
his
tory
SC
ZD
Pau
lsen
et
al.
133
Sp
ora
dic
Ele
vate
dextr
a-
mit
och
on
dri
al
oxygen
con
sum
pti
on
,in
cre
ase
dle
vels
of
reacti
ve
oxygen
specie
s
Retr
ovir
us:
fou
rfa
cto
rs(O
CT
4,
SO
X2,
KLF
4,
c-M
YC
)
Fib
robla
st:
pati
en
tbio
psy
Fem
ale
;48;
clo
zap
ine-r
esi
stan
t
Abbre
via
tion
s:A
SD
,au
tism
spectr
um
dis
ord
er;
BD
,bip
ola
rd
isord
er;
EE
G,
ele
ctr
oen
cep
halo
gra
mte
st;
FX
,fr
agil
eX
syn
dro
me;
hiP
SC
,h
um
an
-deri
ved
ind
uced
plu
rip
ote
nt
stem
cell
;N
A,
not
ap
pli
cable
;P
BL
,p
eri
ph
era
lblo
od
lym
ph
ocyte
;R
TT
,R
ett
syn
dro
me;
SC
ZD
,sc
hiz
op
hre
nia
dis
ord
er.
iPSC modeling of psychiatric disordersKJ Brennand et al
7
Molecular Psychiatry

SCZD and BD), there is decreased dendritic spinematuration and plasticity, leading to decreased spinedensity,66 whereas Clock mice, a model of mania inBD, appear to have normal synaptic density.46
Particularly with respect to SCZD, aberrations insynaptic activity have also been observed in adultneurogenesis in the hippocampus. Similar to corticalembryonic development, where downregulation ofDisc1 results in premature cell cycle exit of neuralprogenitor cells,67,68 adult-born neurons with reducedDisc1 have hastened neural development. Disc1knockdown results in accelerated dendritic develop-ment, soma hypertrophy, aberrant positioning andincreased neural excitability.69–71 It remains unknownif aberrant adult neurogenesis contributes to psychia-tric disease in humans.
Aberrant neuronal migrationIn ASD patients, defects of migration can lead to avariety of morphological outcomes, particularly hetero-topias and dysplastic changes. One recent pathologicalstudy identified a number of abnormalities andlesions in most of the ASD brains studied, includinga loss of vertical and horizontal organization of corticallayers in some patients.72 It has been hypothesizedthat altered expression of cytoskeletal proteins and lossof neuronal polarity contribute to these corticalmigration defects.73
Animal models also show phenotypes consistentwith abnormal neuronal migration: mice with re-duced Disc1 activity have reduced cortical migra-tion,74 Nrg1 mutant mice have reduced tangentialneural migration from the ventral telencephalon44,45
and Cntnap2-null mice have impaired migration ofcortical projection neurons.75 Disc1 mutant mice havealtered distribution of hippocampal mossy fiberterminals on CA3,42 and axons with Disc1 knockdownmiss CA3 altogether and project onto CA1.70 dnDISC1neurites have deficits in neurite repulsionin vitro.42 Although DISC1 is a rare SCZD allele, anunderstanding of the downstream targets or bindingpartners through which it mediates its cellulareffects may identify drug targets relevant to thebroader SCZD population. One putative downstreamtarget of DISC1 is Glycogen Synthase 3-beta (Gsk3b),67
Gsk3b functions within several central path-ways (including cAMP and Wnt) is a direct targetof lithium (a drug commonly used to treat BD)76,77
and mounting evidence indicates that Gsk3bmay be a central mediator of axon outgrowthdynamics.78 Cell-based assays will allow the studyof the effects of Gsk3b, cAMP and WNT levels onneurite outgrowths and axon migration of live humanneurons.
Evidence for network phenotypes in psychiatricdisorders
While comparable neuronal phenotypes, particularlyaberrant dendritic arborization, synaptic density andneuronal migration, are shared between ASD, SCZD
and BD, these cellular phenotypes likely result invastly different network effects in each disorder.Functional imaging facilitates the study of the abnor-mal neural circuitry behind cognitive dysfunction.
One hypothesis concerning ASD is that short-distance over-connectivity in the cortex leads to afailure of long-distance coupling.79 This hypothesispredicts that impaired long-distance connectivity inthe cortex impedes information integration acrossdiverse functional systems (emotional, sensory, auto-nomic, memory). Consistent with this prediction,fMRI studies of resting state brain activity haveobserved increased connectivity between proximalregions, such as the posterior cingulate and theparahippocampal gyrus,80 and decreased connectivitybetween the distal regions, such as the frontal cortexand the parietal lobe,81 the insular cortices and thesomatosensory cortices or amygdala,82 the frontalcortex and the posterior cingulate,80 as well asdecreased interhemispheric synchronization.83 Com-parable defects in long-distance connectivity werefound when ASD patients performed social andintrospective tasks.84 Among ASD patients, a negativecorrelation exists between functional connectivity inthese regions and severity of social and communica-tion impairment.80,82
Just as pathological studies of SCZD reporteddecreased frontal and temporal lobe volumes, earlyfMRI studies of SCZD patients revealed brain activityabnormalities in the frontal and temporal lobes.85,86
More recent studies have further shown that SCZDpatients exhibit cortical hyper-activity and hyper-connectivity of the prefrontal cortex at rest, butreduced activation of the medial prefrontal cortexduring working memory tasks.87 While functionalconnectivity of the parietal cortex to the ventralprefrontal cortex is greater in SCZD, it is reduced tothe dorsal prefrontal cortex.88 This is consistent withanatomical neuronal network maps, which reveal aloss of network ‘hubs’ in the frontal cortex, andincreased connection distance. These network aberra-tions are thought to result from neurodevelopmentalabnormalities impacting cortical organization.89
Although fMRI studies can reveal regions of thebrain with aberrant activity in the disease state, theycannot elucidate the specific neuronal cell typesaffected. Therefore, pharmacological and post-mor-tem studies have generated hypotheses concerningthe cell types affected by SCZD. Similar studies ofASD and BD have been less successful in identifyingthe specific cell types relevant to disease.
Good evidence now links aberrant neurotransmittersignaling to SCZD. Dopamine receptor antagonistsreduce the symptoms of SCZD and evidence nowlinks SCZD with increased dopamine receptor levelsand sensitivity.90,91 Comparably, glutamate-blockingdrugs such as ketamine produce symptoms generallyassociated with SCZD,92 whereas the glutamatereceptor2/3 agonist LY2140023 may ameliorate thesymptoms of SCZD.93 Post-mortem studies of SCZDbrains have found decreased glutamate receptor
iPSC modeling of psychiatric disordersKJ Brennand et al
8
Molecular Psychiatry

expression,94 whereas among GABAergic interneur-ons, a decrease in GAD67 and calcium-bindingproteins was found. Changes in GABAergic neuronsare particularly relevant as they are thought toproduce gamma oscillations, which synchronizepyramidal neuron firing, an activity that is impairedin SCZD. Evidence in mice suggests that SCZD results,at least in part, from reduced excitatory glutamatergicinput onto GABAergic inhibitory neurons.60,95,96 Itremains unclear whether aberrant dopamine, gluta-mate or GABA signaling is the primary cause of SCZD,as aberrant activity of any neuronal cell type couldaffect neurotransmitter activity of the remaining celltypes in the disease state.
In model organisms from Drosophila to mice, genesassociated with ASD, SCZD and BD have been shownto regulate synaptic activity and plasticity. Forexample, a screen in Drosophila for genes critical inmaintaining homeostatic modulation of synaptictransmission identified the SCZD gene Dysbindin(DTNBP1). Dtnbp1 acts presynaptically, in a dose-dependent manner, to regulate adaptive neuralplasticity.97 In Mecp2 mice, although synapse forma-tion, elimination and strengthening are normal, theexperience-dependent phase of synapse remodelingis impaired98 and Mecp2 mice show altered activity-dependent neural gene expression.99 Cntnap2-nullmice, lacking a gene associated with ASD, havereduced GABAergic neurons and decreased neuronalsynchrony.100 Disc1 mice have reduced hippocampalsynaptic transmission.42,43 Nrg1 mice have impairedsynaptic maturation and function58,60–62,101 and22q11.2 mice show altered short- and long-termsynaptic plasticity as well as calcium kinetics inCA3 presynaptic terminals. Defects in synapticplasticity at the cellular level likely contributeto the network aberrations observed in psychiatricdisorders.
One characteristic network defect observed inSCZD is prepulse inhibition (PPI). PPI is a measureof sensory gating, in which a weaker prestimulus(prepulse) inhibits the reaction of an organism to asubsequent strong startling stimulus (pulse). Deficitsin PPI are observed in Nrg1 mice60,95 and are reversedby dopamine receptor antagonists.102,103 Dtnbp1 micedisplay not only decreased PPI but also reducedevoked g-activity, a second pattern seen in patientswith SCZD.104 In humans, polymorphisms in circa-dian genes such as CLOCK convey risk for BD; mutantClock mice also have dysfunctional g-activity acrosslimbic circuits, which can be improved by chroniclithium treatment.46
While PPI is attributed to glutamatergic activity,reduced g-activity indicates abnormal GABAergicneurotransmission. Therefore, although pharmacolo-gical evidence implicates dopaminergic and glutama-tergic neurons in SCZD, network analysis revealsdefects in both glutamatergic and GABAergic activityin SCZD and BD. Aberrations originating in any oneneuronal subtype would ultimately be expected toaffect activity in other types of neurons and in a
variety of brain regions. The ability to testsynaptic activity in defined populations of humanglutamatergic, GABAergic and dopaminergicneurons affected by ASD, SCZD or BD might help toelucidate the neuronal subtypes at the core of eachdisorder.
Introduction to hiPSCs and iNeurons
The transient expression of four factors (OCT3/4,KLF4, SOX2 and c-MYC) is sufficient to directlyreprogram adult somatic cells into an iPSC state.105–107
Because hiPSCs can be derived from adult patientsafter the development of disease, hiPSCs represent apotentially limitless source of human cells withwhich to study disease, even without knowing whichgenes are interacting to produce the disease state inan individual patient. Methods to efficiently differ-entiate pluripotent stem cells to neurons were devel-oped initially in studies using human embryonic stemcells.108 Through the addition of various morphogensto recapitulate the cues of embryonic development,ESCs and iPSCs can be directed to differentiate toregional identities including forebrain,109 midbrain/hindbrain110,111 and spinal cord.112,113 It is generallythought that every cell type present in vivo can bedifferentiated in vitro using hiPSCs, although meth-ods for many remain unexplored or inefficient.
An alternative approach for generating patient-specific neurons to study complex psychiatric dis-orders is now possible. Expression of four factors(ASCL1, BRN2, MYT1L and NEUROD) can convertfibroblasts into functional iNeurons in vitro.114,115 Theprocess is rapid, generating electrophysiologicallymature neurons with functional synapses within 14days, and it is efficient, yielding up to 8% neurons. Todate, methods exist to transform fibroblasts directly toglutamatergic115 and dopaminergic neurons,116 butmethods to generate GABAergic iNeurons have notyet been reported. The regional identity of eachneurotransmitter subtype remains unclear.
Both hiPSC neurons and iNeurons have thecapacity to generate vast numbers of live humanneurons for the study of psychiatric disorders.Because iNeuron generation bypasses neuronal differ-entiation and maturation, hiPSC neurons are likelythe best method by which to model developmentalfacets of disease. For example, if SCZD ultimatelyresults from abnormal synaptic maturation, it ispossible that direct reprogramming would bypassthe developmental window in which the SCZDcellular phenotype can be observed in vitro. Addi-tionally, as aberrant ASCL1, BRN2 and MYT1L haveall been linked to neurological disease,117–120 it is notunreasonable to predict that overexpression of one ormore of these key neuronal genes might affect theinitiation or progression of a psychiatric disorder invitro. Conversely, the rapid experimental timeframe ofiNeuron generation makes it an ideal system withwhich to study phenotypic effects in mature neurons.If ASD is indeed a disease of activity-dependent
iPSC modeling of psychiatric disordersKJ Brennand et al
9
Molecular Psychiatry

synaptic modulation rather than synaptic maturation,iNeurons represent a more direct cell type with whichto assay network properties. As the efficiency ofiNeuron generation increases, and spontaneous neu-ronal networks result, this method may facilitaterobust and swift network analysis of ASD, SCZD andBD neurons. It is important to note that both strategiesfacilitate novel experiments of innate neuron-specificdeficits in psychiatric disease that are not confoundedby environmental factors, such as treatment history,drug and alcohol abuse or poverty, that typicallyplague clinical studies.
Psychiatric disorders result in hiPSC neuronalphenotypes in vitro
While no reported studies have yet characterizediNeurons from patients with psychiatric disorders, anumber of groups, including ours, have now pub-lished studies of hiPSC neurons derived from patientswith ASD and SCZD. During neuronal differentiationof hiPSCs, a number of neuronal genes alreadyimplicated in ASD, SCZD and BD, such as transcrip-tion factors and chromatin modifiers like POU3F2and ZNF804A and cell adhesion genes like NRXN1and NLGN1,121 are upregulated, permitting compar-isons of expression levels in diseased and healthy livehuman neurons.
Three groups have now generated hiPSCs from atotal of seven RTT patients, representing a number ofunique point mutations and deletions in the MeCP2gene (Q244X, 1155del 32, T158 M, R306C,D3-4,R294X, V247X).122–124 None of the groups observedaltered replication or differentiation of RTT hiPSCs orneural progenitor cells. Rather, consistent withanimal and post-mortem patient studies, all threegroups reported that neuronal soma size of RTThiPSC neurons is reduced by approximately 10–20%compared with controls.122–124 Furthermore, we ob-served that RTT hiPSC neurons have reduced spinedensity, decreased neuronal spontaneous calciumsignaling and decreased spontaneous excitatory andinhibitory postsynaptic currents. The reproducibilityof these findings across three independent reportsvalidates the use of hiPSC-based models. Further-more, by demonstrating the ability to test drugs torescue synaptic deficiency in RTT neurons, thesestudies hint at future uses of hiPSC neurons for high-throughout drug screening to identify new therapeu-tic drugs for psychiatric disorders.
FX is caused by the absence of expression of thefragile X mental retardation 1 (FMR1) gene,125 whichis believed to result from transcriptional silencingduring embryonic development, owing to a CGGtriplet-repeat expansion in the 50 untranslated regionof the gene.126 Although the somatic cells of three FXpatients were successfully reprogrammed to pluripo-tency, the FMR1 gene remained inactive in all FXhiPSC lines, unlike FX embryonic stem cell lines.Consequently, the authors of this first report of FXhiPSCs concluded that ‘FX-iPSCs do not model the
differentiation-dependent silencing of the FMR1gene,’ and therefore chose not to assess their FX-hiPSC neurons for phenotypic abormalities.127 Morerecently, a second group generated hiPSCs from threepatients (including one patient common to the firstgroup) via nearly identical methods. They noted thata number of hiPSC lines had FMR1 CGG-repeatlengths that were clearly different from the originalfibroblasts, and they also failed to detect FMR1 geneexpression in the original FX fibroblasts or their FXhiPSCs.128 Despite also not observing reactivatedFMR1 expression in FX hiPSCs, this group comparedneural differentiation of FX and control hiPSCs. Theyobserved that neural cultures generated from FXhiPSCs consisted of neurons with fewer and shorterprocesses, as well as a larger number of glial cellswith more compact morphology, suggesting thatdecreased FMR1 expression levels, rather than theslow silencing of FMR1 during neuronal differentia-tion, are sufficient to produce the disease state in FX.
Timothy syndrome is caused by a mutation in theL-type calcium channel Ca(v)1.2 and is associatedwith heart arrhythmias and ASD. From two patientswith Timothy syndrome, hiPSC-derived corticalneural progenitor cells (NPCs) and neurons weregenerated. Neurons from these individuals wereshown to have aberrant calcium signaling,129 whilean earlier publication by this same group demon-strated that hiPSC-derived cardiomyocytes from thesesame patients had irregular contraction, abnormalcalcium transients and irregular electrical activity.130
Timothy syndrome hiPSC neurons underwent abnor-mal cortical differentiation, showing decreased ex-pression of cortical genes and increased production ofnorepinephrine and DA. Notably, treatment withroscovitine, a cyclin-dependent kinase inhibitor andatypical L-type-channel blocker, was sufficient toameliorate many characteristics of Timothy syndromeneurons in vitro.129
DISC1 mutations cause a rare monogenic form ofSCZD. The generation of hiPSCs from SCZD patientswith a DISC1 mutation have now been reported,131
although neurons differentiated from these hiPSCshave not yet been characterized. We predict thatDISC1–hiPSC-derived neurons will ultimately beshown to recapitulate the cellular phenotypes ob-served in dnDISC mice, just as RTT and FX-hiPSCneurons have replicated findings from mouse studies.
We recently reported neuronal phenotypes ofhiPSC neurons from four patients with complexgenetic forms of SCZD. When assayed by retrogradetransmission of rabies virus neuronal labeling, SCZD-hiPSC neurons showed reduced neuronal connectiv-ity and altered gene expression profiles.132 Whilenearly 25% of genes with altered expression had beenpreviously implicated in SCZD, we also identified anumber of new pathways that may contribute toSCZD. A second group has now reported an oxygenmetabolism phenotype associated with SCZD;133 theyobserved a twofold increase in extra-mitochondrialoxygen consumption as well as elevated levels of
iPSC modeling of psychiatric disordersKJ Brennand et al
10
Molecular Psychiatry

reactive oxygen species in neural progenitor cellsderived from hiPSCs from one SCZD patient relativeto controls. Although a small study, this observationis consistent with animal studies134,135 and deservesattention. Oxygen metabolism defects have not beenwell demonstrated in human neurons, owing to a lackof live human cells for study. This is an excellentexample of the type of hiPSC study that can inve-stigate hypotheses not testable in human patients.
Limitations of hiPSC-based modeling
A number of major limitations currently restricthiPSC-based studies, particularly concerning thescalability of hiPSC generation, neural differentiationand phenotypic characterization of derived neuronsand neural networks. These technical limitationshave made it hard to accurately address the inherentvariability of cell-based studies, which exist in threemajor forms: (1) neuron-to-neuron (intra-patient), (2)hiPSC-to-hiPSC (intra-patient) and (3) patient-to-patient (inter-patient). To produce meaningful data,each cell-based experiment should ideally comparemultiple neuronal differentiations from multipleindependent hiPSC lines from multiple patients.Owing to cost and time constraints, such largeexperiments have not yet been completed. Conse-quently, the hiPSC studies reported to date mayultimately prove to be proof-of-concept demonstra-tions until methods to compare derived neurons fromhundred or thousands of patients and controls arerefined.
Intra-patient variability results from differencesbetween neurons and iPSCs generated from a singlepatient; it is the major constraint on signal to noise incell-based experiments. Differences between indivi-dual hiPSC neurons derived from a single patientproduce neuron-to-neuron variability. To some extent,this variability may be unavoidable, although it iscurrently exacerbated by the heterogeneity of cellularsubtypes in hiPSC neural populations; none of thereports described in this review compare pureneuronal populations of a specific subtype. At theexperimental level, neural subtype heterogeneityresults because current neuronal differentiation pro-tocols are not 100% efficient and, in contrast to thehematopoietic system, cell surface markers by whichspecific subtypes of neurons might be purified havenot been developed. It is well established thatindividual hiPSC lines vary genetically, epigeneti-cally and in terms of neural differentiation propen-sities to produce hiPSC-to-hiPSC variability. Geneticdifferences include the location and number of viralintegrations produced during the reprogrammingprocess and spontaneous mutations that have beenobserved during hiPSC generation and expansion.136
Epigenetic differences reflect the somatic cell typeused for reprogramming and the completeness of itschromatin remodeling.137 Differences in developmen-tal potential exist among human embryonic stem celllines138 and between individual hiPSC lines.139
Inter-patient variability reflects the heterogeneity inclinical outcomes between patients with ASD, SCZDor BD. Consequently, given the small sample size(typically 1–4 patients) of the current hiPSC-basedstudies discussed in this review, a major concern iswhether their findings are representative of the largerpatient population. In the short term, this has beenaddressed by recruiting patients with well-definedclinical or genetic characteristics as well as matchedhealthy controls. Ultimately, methods will have to bedeveloped to permit comparisons of thousands ofpatients.
Future directions of cell-based studies
Whole-brain disorders should be studied at the levelof component aberrations of cells and neural net-works. Neuroimaging, post-mortem anatomical andpharmacological studies of patients may be measuringconsequences of the disease state, rather than itsorigin. Cell-based studies will lead to the discernmentand characterization of the molecular causes of ASD,SCZD and BD and facilitate studies of the cellular andnetwork phenotypes that serve as neuronal predis-positions to disease. Furthermore, these studiesconfer the ability to test various neuron non-cell-autonomous effects, such as inflammation, oxidativestress, activity-dependent modulations and the influ-ence of stress hormones in psychiatric disorders.High-throughput screening of new classes of com-pounds capable of pharmacological amelioration ofneuronal and/or network phenotypes for treatment ofthese disorders is possible.
Small defects at the cellular level could ultimatelymanifest as complex psychiatric disorders with anarray of symptoms in patients. For example, ifneurons derived from psychiatric patients show adecrease in the absolute number of connectionsbetween cells, and if this phenotype is restricted toa specific subtype of neurons, this finding might hintat the central cell type relevant to the disease state.Because synaptic strength is highly modulated bysynaptic activity, a decrease in the strength ofindividual connections between neurons in psychia-tric patients could indicate aberrant synaptic activityor plasticity in patient brains. Finally, perturbedneuronal migration or axon targeting in vitro mightsuggest that mis-targeted neuronal connections,rather than decreased neuronal connectivity, iscentral to disease. Cellular phenotypes hint at theneuronal predispositions contributing to psychiatricdisorders and may help to unlock the complexities ofpsychiatric illness.
While overlapping genetic susceptibilities mightproduce a common cellular phenotype, or predis-position, to psychiatric illness, clinical outcome maybe determined by activity at the network level.Synaptic pruning (either whole brain or in specificregions) is an activity-dependent process that couldgenerate the clinical differences distinguishing ASD,SCZD and BD. Cell-based studies of neuronal and
iPSC modeling of psychiatric disordersKJ Brennand et al
11
Molecular Psychiatry

network aberrations in psychiatric disorders may leadto predictions of activity-dependent environmentalinfluences that contribute to disease progression.
Human iPSC- and iNeuron-based methods have thepotential to simplify whole-brain disorders like ASD,SCZD and BD to their cellular and network compo-nents, contributing to our understanding of theseconditions. Although many technical issues, particu-larly, concerning the scalability of hiPSC generation,neuronal differentiation and neural assays remain, webelieve that studies of neuronal networks constructedfrom defined neuronal populations are feasible. Byrecapitulating and monitoring healthy and diseasenetworks in a dish, it is likely that new methods ofin vitro modeling of psychiatric disorders willresult in new insights into the mechanism of diseaseinitiation, progression and, ultimately, treatment.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
The Gage Laboratory is partially funded by CIRMGrant RL1-00649-1, The Lookout and Mathers Foun-dation, the Helmsley Foundation as well as Sanofi-Aventis. We thank J Simon for illustrations and MLGage for editorial comments.
References
1 Association AP. Diagnostic and statistical manual of mentaldisorders: DSM-IV. 3rd ed., rev. edn, vol. 4th ed, AmericanPsychiatric Press: Washington, DC, 1994; 886, pp 69–70, 263,350–359.
2 Di Giorgio FP, Boulting GL, Bobrowicz S, Eggan KC. Humanembryonic stem cell-derived motor neurons are sensitive to thetoxic effect of glial cells carrying an ALS-causing mutation. CellStem Cell 2008; 3: 637–648.
3 Marchetto MC, Muotri AR, Mu Y, Smith AM, Cezar GG, Gage FH.Non-cell-autonomous effect of human SOD1 G37R astrocytes onmotor neurons derived from human embryonic stem cells. CellStem Cell 2008; 3: 649–657.
4 Ritvo ER, Freeman BJ, Mason-Brothers A, Mo A, Ritvo AM.Concordance for the syndrome of autism in 40 pairs of afflictedtwins. Am J Psychiatry 1985; 142: 74–77.
5 Sullivan PF, Kendler KS, Neale MC. Schizophrenia as a complextrait: evidence from a meta-analysis of twin studies. Arch GenPsychiatry 2003; 60: 1187–1192.
6 Tsuang MT, Stone WS, Faraone SV. Genes, environment andschizophrenia. Br J Psychiatry Suppl 2001; 40: s18–s24.
7 Bottenstein JE, Sato GH. Growth of a rat neuroblastoma cell linein serum-free supplemented medium. Proc Natl Acad Sci USA1979; 76: 514–517.
8 Benitez-King G, Riquelme A, Ortiz-Lopez L, Berlanga C, Rodri-guez-Verdugo MS, Romo F et al. A non-invasive method to isolatethe neuronal linage from the nasal epithelium from schizophre-nic and bipolar diseases. J Neurosci Methods 2011; 201: 35–45.
9 Matigian N, Abrahamsen G, Sutharsan R, Cook AL, Vitale AM,Nouwens A et al. Disease-specific, neurosphere-derived cells asmodels for brain disorders. Dis Model Mech 2010; 3: 785–798.
10 Carper RA, Moses P, Tigue ZD, Courchesne E. Cerebral lobes inautism: early hyperplasia and abnormal age effects. Neuroimage2002; 16: 1038–1051.
11 Courchesne E, Karns CM, Davis HR, Ziccardi R, Carper RA, TigueZD et al. Unusual brain growth patterns in early life in patients
with autistic disorder: an MRI study. Neurology 2001; 57:245–254.
12 Hazlett HC, Poe M, Gerig G, Smith RG, Provenzale J, Ross A et al.Magnetic resonance imaging and head circumference study ofbrain size in autism: birth through age 2 years. Arch GenPsychiatry 2005; 62: 1366–1376.
13 Courchesne E, Mouton P, Calhoun M, Semendeferi K, Ahrens-Barbeau C, Hallet M et al. Neuron number and size in prefrontalcortex of children with autism. JAMA 2011; 206: 2001–2010.
14 Courchesne E, Press GA, Yeung-Courchesne R. Parietal lobeabnormalities detected with MR in patients with infantile autism.AJR Am J Roentgenol 1993; 160: 387–393.
15 Hadjikhani N, Joseph RM, Snyder J, Tager-Flusberg H. Anatomi-cal differences in the mirror neuron system and social cognitionnetwork in autism. Cereb Cortex 2006; 16: 1276–1282.
16 Schmitz N, Daly E, Murphy D. Frontal anatomy and reaction timein Autism. Neurosci Lett 2007; 412: 12–17.
17 Brun CC, Nicolson R, Lepore N, Chou YY, Vidal CN, DeVito TJet al. Mapping brain abnormalities in boys with autism. HumBrain Mapp 2009; 30: 3887–3900.
18 Frazier TW, Hardan AY. A meta-analysis of the corpus callosumin autism. Biol Psychiatry 2009; 66: 935–941.
19 Raymond GV, Bauman ML, Kemper TL. Hippocampus in autism:a Golgi analysis. Acta Neuropathol 1996; 91: 117–119.
20 Amir RE, Van den Veyver IB, Wan M, Tran CQ, Francke U, ZoghbiHY. Rett syndrome is caused by mutations in X-linked MECP2,encoding methyl-CpG-binding protein 2. Nat Genet 1999; 23:185–188.
21 Van den Veyver IB, Zoghbi HY. Methyl-CpG-binding protein 2mutations in Rett syndrome. Curr Opin Genet Dev 2000; 10:275–279.
22 Bauman ML, Kemper TL, Arin DM. Pervasive neuroanatomicabnormalities of the brain in three cases of Rett’s syndrome.Neurology 1995; 45: 1581–1586.
23 Castren M, Tervonen T, Karkkainen V, Heinonen S, Castren E,Larsson K et al. Altered differentiation of neural stem cellsin fragile X syndrome. Proc Natl Acad Sci USA 2005; 102: 17834–17839.
24 Bhattacharyya A, McMillan E, Wallace K, Tubon Jr TC, CapowskiEE, Svendsen CN. Normal neurogenesis but abnormal gene
expression in human Fragile X cortical progenitor cells. Stem
Cells Dev 2008; 17: 107–117.25 Vita A, De Peri L, Silenzi C, Dieci M. Brain morphology in first-
episode schizophrenia: a meta-analysis of quantitative magnetic
resonance imaging studies. Schizophr Res 2006; 82: 75–88.26 Steen RG, Mull C, McClure R, Hamer RM, Lieberman JA. Brain
volume in first-episode schizophrenia: systematic review and
meta-analysis of magnetic resonance imaging studies. Br
J Psychiatry 2006; 188: 510–518.27 Wright IC, Rabe-Hesketh S, Woodruff PW, David AS, Murray RM,
Bullmore ET. Meta-analysis of regional brain volumes in schizo-
phrenia. Am J Psychiatry 2000; 157: 16–25.28 Thompson PM, Vidal C, Giedd JN, Gochman P, Blumenthal J,
Nicolson R et al. Mapping adolescent brain change
reveals dynamic wave of accelerated gray matter loss in very
early-onset schizophrenia. Proc Natl Acad Sci USA 2001; 98:
11650–11655.29 Ellison-Wright I, Glahn DC, Laird AR, Thelen SM, Bullmore E.
The anatomy of first-episode and chronic schizophrenia: an
anatomical likelihood estimation meta-analysis. Am J Psychiatry
2008; 165: 1015–1023.30 Rajkowska G, Selemon LD, Goldman-Rakic PS. Neuronal and
glial somal size in the prefrontal cortex: a postmortem morpho-
metric study of schizophrenia and Huntington disease. Arch Gen
Psychiatry 1998; 55: 215–224.31 Kolomeets NS, Orlovskaya DD, Rachmanova VI, Uranova NA.
Ultrastructural alterations in hippocampal mossy fiber synapses
in schizophrenia: a postmortem morphometric study. Synapse
2005; 57: 47–55.32 Black JE, Kodish IM, Grossman AW, Klintsova AY, Orlovskaya D,
Vostrikov V et al. Pathology of layer V pyramidal neurons in theprefrontal cortex of patients with schizophrenia. Am J Psychiatry2004; 161: 742–744.
iPSC modeling of psychiatric disordersKJ Brennand et al
12
Molecular Psychiatry

33 Selemon LD, Goldman-Rakic PS. The reduced neuropil hypoth-esis: a circuit based model of schizophrenia. Biol Psychiatry1999; 45: 17–25.
34 Karchemskiy A, Garrett A, Howe M, Adleman N, Simeonova DI,Alegria D et al. Amygdalar, hippocampal, and thalamic volumesin youth at high risk for development of bipolar disorder.Psychiatry Res 2011; 194: 319–325.
35 Frazier JA, Chiu S, Breeze JL, Makris N, Lange N, Kennedy DNet al. Structural brain magnetic resonance imaging of limbic andthalamic volumes in pediatric bipolar disorder. Am J Psychiatry2005; 162: 1256–1265.
36 Edmiston EE, Wang F, Kalmar JH, Womer FY, Chepenik LG,Pittman B et al. Lateral ventricle volume and psychotic featuresin adolescents and adults with bipolar disorder. Psychiatry Res2011; 194: 400–402.
37 Rajkowska G, Halaris A, Selemon LD. Reductions in neuronaland glial density characterize the dorsolateral prefrontal cortex inbipolar disorder. Biol Psychiatry 2001; 49: 741–752.
38 Pantazopoulos H, Lange N, Baldessarini RJ, Berretta S. Parvalbu-min neurons in the entorhinal cortex of subjects diagnosedwith bipolar disorder or schizophrenia. Biol Psychiatry 2007; 61:640–652.
39 Chen RZ, Akbarian S, Tudor M, Jaenisch R. Deficiency of methyl-CpG binding protein-2 in CNS neurons results in a Rett-likephenotype in mice. Nat Genet 2001; 27: 327–331.
40 Kishi N, Macklis JD. MECP2 is progressively expressed in post-migratory neurons and is involved in neuronal maturation ratherthan cell fate decisions. Mol Cell Neurosci 2004; 27:306–321.
41 Smrt RD, Eaves-Egenes J, Barkho BZ, Santistevan NJ, Zhao C,Aimone JB et al. Mecp2 deficiency leads to delayed maturationand altered gene expression in hippocampal neurons. NeurobiolDis 2007; 27: 77–89.
42 Kvajo M, McKellar H, Arguello PA, Drew LJ, Moore H,MacDermott AB et al. A mutation in mouse Disc1 that models aschizophrenia risk allele leads to specific alterations in neuronalarchitecture and cognition. Proc Natl Acad Sci USA 2008; 105:7076–7081.
43 Li W, Zhou Y, Jentsch JD, Brown RA, Tian X, Ehninger Det al. Specific developmental disruption of disrupted-in-schizophrenia-1 function results in schizophrenia-relatedphenotypes in mice. Proc Natl Acad Sci UnSA 2007; 104:18280–18285.
44 Lopez-Bendito G, Cautinat A, Sanchez JA, Bielle F, Flames N,Garratt AN et al. Tangential neuronal migration controls axonguidance: a role for neuregulin-1 in thalamocortical axonnavigation. Cell 2006; 125: 127–142.
45 Krivosheya D, Tapia L, Levinson JN, Huang K, Kang Y, Hines Ret al. ErbB4-neuregulin signaling modulates synapse develop-ment and dendritic arborization through distinct mechanisms.J Biol Chem 2008; 283: 32944–32956.
46 Dzirasa K, Coque L, Sidor MM, Kumar S, Dancy EA, Takahashi JSet al. Lithium ameliorates nucleus accumbens phase-signalingdysfunction in a genetic mouse model of mania. J Neurosci 2010;30: 16314–16323.
47 Sudhof TC. Neuroligins and neurexins link synaptic function tocognitive disease. Nature 2008; 455: 903–911.
48 Hutsler JJ, Zhang H. Increased dendritic spine densities oncortical projection neurons in autism spectrum disorders. BrainRes 2010; 1309: 83–94.
49 Chapleau CA, Calfa GD, Lane MC, Albertson AJ, Larimore JL,Kudo S et al. Dendritic spine pathologies in hippocampalpyramidal neurons from Rett syndrome brain and after expres-sion of Rett-associated MECP2 mutations. Neurobiol Dis 2009; 35:219–233.
50 Irwin SA, Patel B, Idupulapati M, Harris JB, Crisostomo RA,Larsen BP et al. Abnormal dendritic spine characteristics in thetemporal and visual cortices of patients with fragile-X syndrome:a quantitative examination. Am J Med Genet 2001; 98: 161–167.
51 Garey LJ, Ong WY, Patel TS, Kanani M, Davis A, Mortimer AMet al. Reduced dendritic spine density on cerebral corticalpyramidal neurons in schizophrenia. J Neurol Neurosurg Psy-chiatry 1998; 65: 446–453.
52 Glantz LA, Lewis DA. Decreased dendritic spine density onprefrontal cortical pyramidal neurons in schizophrenia. ArchGen Psychiatry 2000; 57: 65–73.
53 Kolomeets NS, Orlovskaya DD, Uranova NA. Decreased numer-ical density of CA3 hippocampal mossy fiber synapses inschizophrenia. Synapse 2007; 61: 615–621.
54 Asaka Y, Jugloff DG, Zhang L, Eubanks JH, Fitzsimonds RM.Hippocampal synaptic plasticity is impaired in the Mecp2-nullmouse model of Rett syndrome. Neurobiol Dis 2006; 21: 217–227.
55 Moretti P, Levenson JM, Battaglia F, Atkinson R, Teague R,Antalffy B et al. Learning and memory and synaptic plasticity areimpaired in a mouse model of Rett syndrome. J Neurosci 2006;26: 319–327.
56 Nelson ED, Kavalali ET, Monteggia LM. MeCP2-dependenttranscriptional repression regulates excitatory neurotransmis-sion. Curr Biol 2006; 16: 710–716.
57 Durand CM, Perroy J, Loll F, Perrais D, Fagni L, Bourgeron T et al.SHANK3 mutations identified in autism lead to modification ofdendritic spine morphology via an actin-dependent mechanism.Mol Psychiatry 2011; 17: 71–84.
58 Comery TA, Harris JB, Willems PJ, Oostra BA, Irwin SA, Weiler IJet al. Abnormal dendritic spines in fragile X knockout mice:maturation and pruning deficits. Proc Natl Acad Sci USA 1997;94: 5401–5404.
59 Weiler IJ, Spangler CC, Klintsova AY, Grossman AW, Kim SH,Bertaina-Anglade V et al. Fragile X mental retardation protein isnecessary for neurotransmitter-activated protein translation atsynapses. Proc Natl Acad Sci USA 2004; 101: 17504–17509.
60 Barros CS, Calabrese B, Chamero P, Roberts AJ, Korzus E, Lloyd Ket al. Impaired maturation of dendritic spines without disorga-nization of cortical cell layers in mice lacking NRG1/ErbBsignaling in the central nervous system. Proc Natl Acad SciUSA 2009; 106: 4507–4512.
61 Pitcher GM, Beggs S, Woo RS, Mei L, Salter MW. ErbB4 is asuppressor of long-term potentiation in the adult hippocampus.Neuroreport 2008; 19: 139–143.
62 Chen YJ, Zhang M, Yin DM, Wen L, Ting A, Wang P et al. ErbB4 inparvalbumin-positive interneurons is critical for neuregulin 1regulation of long-term potentiation. Proc Natl Acad Sci USA2010; 107: 21818–21823.
63 Fenelon K, Mukai J, Xu B, Hsu PK, Drew LJ, Karayiorgou M et al.Deficiency of Dgcr8, a gene disrupted by the 22q11.2 microdele-tion, results in altered short-term plasticity in the prefrontalcortex. Proc Natl Acad Sci USA 2011; 108: 4447–4452.
64 Earls LR, Bayazitov IT, Fricke RG, Berry RB, Illingworth E,Mittleman G et al. Dysregulation of presynaptic calcium andsynaptic plasticity in a mouse model of 22q11 deletionsyndrome. J Neurosci 2010; 30: 15843–15855.
65 Sigurdsson T, Stark KL, Karayiorgou M, Gogos JA, Gordon JA.Impaired hippocampal-prefrontal synchrony in a genetic mousemodel of schizophrenia. Nature 2010; 464: 763–767.
66 Pappas GD, Kriho V, Pesold C. Reelin in the extracellular matrixand dendritic spines of the cortex and hippocampus: acomparison between wild type and heterozygous reeler mice byimmunoelectron microscopy. J Neurocytol 2001; 30: 413–425.
67 Mao Y, Ge X, Frank CL, Madison JM, Koehler AN, Doud MK et al.Disrupted in schizophrenia 1 regulates neuronal progenitorproliferation via modulation of GSK3beta/beta-catenin signaling.Cell 2009; 136: 1017–1031.
68 Singh KK, Ge X, Mao Y, Drane L, Meletis K, Samuels BA et al.Dixdc1 is a critical regulator of DISC1 and embryonic corticaldevelopment. Neuron 2010; 67: 33–48.
69 Duan X, Chang JH, Ge S, Faulkner RL, Kim JY, Kitabatake Y et al.Disrupted-In-Schizophrenia 1 regulates integration of newlygenerated neurons in the adult brain. Cell 2007; 130: 1146–1158.
70 Faulkner RL, Jang MH, Liu XB, Duan X, Sailor KA, Kim JY et al.Development of hippocampal mossy fiber synaptic outputs bynew neurons in the adult brain. Proc Natl Acad Sci USA 2008;105: 14157–14162.
71 Kim JY, Duan X, Liu CY, Jang MH, Guo JU, Pow-anpongkul N etal. DISC1 regulates new neuron development in the adult brainvia modulation of AKT-mTOR signaling through KIAA1212.Neuron 2009; 63: 761–773.
iPSC modeling of psychiatric disordersKJ Brennand et al
13
Molecular Psychiatry

72 Wegiel J, Kuchna I, Nowicki K, Imaki H, Marchi E, Ma SY et al.The neuropathology of autism: defects of neurogenesis andneuronal migration, and dysplastic changes. Acta Neuropathol2010; 119: 755–770.
73 Rorke LB. A perspective: the role of disordered genetic controlof neurogenesis in the pathogenesis of migration disorders.J Neuropathol Exp Neurol 1994; 53: 105–117.
74 Kamiya A, Kubo K, Tomoda T, Takaki M, Youn R, Ozeki Y et al. Aschizophrenia-associated mutation of DISC1 perturbs cerebralcortex development. Nat Cell Biol 2005; 7: 1167–1178.
75 Just MA, Cherkassky VL, Keller TA, Minshew NJ. Corticalactivation and synchronization during sentence comprehensionin high-functioning autism: evidence of underconnectivity. Brain2004; 127(Part 8): 1811–1821.
76 Ruiz i Altaba A, Melton DA. Involvement of the Xenopushomeobox gene Xhox3 in pattern formation along the anterior-posterior axis. Cell 1989; 57: 317–326.
77 O’Brien WT, Klein PS. Validating GSK3 as an in vivo targetof lithium action. Biochem Soc Trans 2009; 37(Part 5):1133–1138.
78 Kim WY, Zhou FQ, Zhou J, Yokota Y, Wang YM, Yoshimura Tet al. Essential roles for GSK-3s and GSK-3-primed substrates inneurotrophin-induced and hippocampal axon growth. Neuron2006; 52: 981–996.
79 Courchesne E, Redcay E, Morgan JT, Kennedy DP. Autism at thebeginning: microstructural and growth abnormalities underlyingthe cognitive and behavioral phenotype of autism. Dev Psycho-pathol 2005; 17: 577–597.
80 Monk CS, Peltier SJ, Wiggins JL, Weng SJ, Carrasco M, Risi S et al.Abnormalities of intrinsic functional connectivity in autismspectrum disorders. Neuroimage 2009; 47: 764–772.
81 Kennedy DP, Courchesne E. The intrinsic functional organizationof the brain is altered in autism. Neuroimage 2008; 39:1877–1885.
82 Ebisch SJ, Gallese V, Willems RM, Mantini D, Groen WB, RomaniGL et al. Altered intrinsic functional connectivity of anterior andposterior insula regions in high-functioning participantswith autism spectrum disorder. Hum Brain Mapp 2011; 32:1013–1028.
83 Dinstein I, Pierce K, Eyler L, Solso S, Malach R, Behrmann M etal. Disrupted neural synchronization in toddlers with autism.Neuron 2011; 70: 1218–1225.
84 Kennedy DP, Courchesne E. Functional abnormalities of thedefault network during self- and other-reflection in autism. SocCogn Affect Neurosci 2008; 3: 177–190.
85 Yurgelun-Todd DA, Renshaw PF, Gruber SA, Ed M, Waternaux C,Cohen BM. Proton magnetic resonance spectroscopy of thetemporal lobes in schizophrenics and normal controls. SchizophrRes 1996; 19: 55–59.
86 Yurgelun-Todd DA, Waternaux CM, Cohen BM, Gruber SA,English CD, Renshaw PF. Functional magnetic resonance imagingof schizophrenic patients and comparison subjects during wordproduction. Am J Psychiatry 1996; 153: 200–205.
87 Whitfield-Gabrieli S, Thermenos HW, Milanovic S, Tsuang MT,Faraone SV, McCarley RW et al. Hyperactivity and hyperconnec-tivity of the default network in schizophrenia and in first-degreerelatives of persons with schizophrenia. Proc Natl Acad Sci USA2009; 106: 1279–1284.
88 Tan HY, Sust S, Buckholtz JW, Mattay VS, Meyer-Lindenberg A,Egan MF et al. Dysfunctional prefrontal regional specializationand compensation in schizophrenia. Am J Psychiatry 2006; 163:1969–1977.
89 Bassett DS, Bullmore E, Verchinski BA, Mattay VS, WeinbergerDR, Meyer-Lindenberg A. Hierarchical organization of humancortical networks in health and schizophrenia. J Neurosci 2008;28: 9239–9248.
90 Kessler RM, Woodward ND, Riccardi P, Li R, Ansari MS,Anderson S et al. Dopamine D2 receptor levels in striatum,thalamus, substantia nigra, limbic regions, and cortex in schizo-phrenic subjects. Biol Psychiatry 2009; 65: 1024–1031.
91 Owen F, Cross AJ, Crow TJ, Longden A, Poulter M, Riley GJ.Increased dopamine-receptor sensitivity in schizophrenia.Lancet 1978; 2: 223–226.
92 Krystal JH, Karper LP, Seibyl JP, Freeman GK, Delaney R, BremnerJD et al. Subanesthetic effects of the noncompetitive NMDAantagonist, ketamine, in humans. Psychotomimetic, perceptual,cognitive, and neuroendocrine responses. Arch Gen Psychiatry1994; 51: 199–214.
93 Patil ST, Zhang L, Martenyi F, Lowe SL, Jackson KA, Andreev BVet al. Activation of mGlu2/3 receptors as a new approach to treatschizophrenia: a randomized Phase 2 clinical trial. Nat Med2007; 13: 1102–1107.
94 Meador-Woodruff JH, Healy DJ. Glutamate receptor expressionin schizophrenic brain. Brain Res Brain Res Rev 2000; 31:288–294.
95 Li B, Woo RS, Mei L, Malinow R. The neuregulin-1 receptorerbB4 controls glutamatergic synapse maturation and plasticity.Neuron 2007; 54: 583–597.
96 Stefansson H, Sigurdsson E, Steinthorsdottir V, Bjornsdottir S,Sigmundsson T, Ghosh S et al. Neuregulin 1 and susceptibility toschizophrenia. Am J Hum Genet 2002; 71: 877–892.
97 Dickman DK, Davis GW. The schizophrenia susceptibility genedysbindin controls synaptic homeostasis. Science (New York,NY) 2009; 326: 1127–1130.
98 Noutel J, Hong YK, Leu B, Kang E, Chen C. Experience-dependentretinogeniculate synapse remodeling is abnormal in MeCP2-deficient mice. Neuron 2011; 70: 35–42.
99 Dani VS, Chang Q, Maffei A, Turrigiano GG, Jaenisch R,Nelson SB. Reduced cortical activity due to a shift in the balancebetween excitation and inhibition in a mouse model of Rettsyndrome. Proc Natl Acad Sci USA 2005; 102: 12560–12565.
100 Penagarikano O, Abrahams BS, Herman EI, Winden KD,Gdalyahu A, Dong H et al. Absence of CNTNAP2 leads toepilepsy, neuronal migration abnormalities, and core autism-related deficits. Cell 2011; 147: 235–246.
101 Pitcher GM, Kalia LV, Ng D, Goodfellow NM, Yee KT, Lambe EKet al. Schizophrenia susceptibility pathway neuregulin 1-ErbB4suppresses Src upregulation of NMDA receptors. Nat Med 2011;17: 470–478.
102 Geyer MA, Swerdlow NR, Mansbach RS, Braff DL. Startleresponse models of sensorimotor gating and habituation deficitsin schizophrenia. Brain Res Bull 1990; 25: 485–498.
103 Caine SB, Geyer MA, Swerdlow NR. Effects of D3/D2 dopaminereceptor agonists and antagonists on prepulse inhibition ofacoustic startle in the rat. Neuropsychopharmacology 1995; 12:139–145.
104 Carlson GC, Talbot K, Halene TB, Gandal MJ, Kazi HA, SchlosserL et al. From the cover: Dysbindin-1 mutant mice implicatereduced fast-phasic inhibition as a final common diseasemechanism in schizophrenia. Proc Natl Acad Sci USA 2011;108: E962–E970.
105 Takahashi K, Yamanaka S. Induction of pluripotent stem cellsfrom mouse embryonic and adult fibroblast cultures by definedfactors. Cell 2006; 126: 663–676.
106 Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, TomodaK et al. Induction of pluripotent stem cells from adult humanfibroblasts by defined factors. Cell 2007; 131: 861–872.
107 Yu J, Vodyanik MA, Smuga-Otto K, Antosiewicz-Bourget J, FraneJL, Tian S et al. Induced pluripotent stem cell lines derivedfrom human somatic cells. Science (New York, NY) 2007; 318:1917–1920.
108 Tropepe V, Hitoshi S, Sirard C, Mak TW, Rossant J, van der KooyD. Direct neural fate specification from embryonic stem cells: aprimitive mammalian neural stem cell stage acquired through adefault mechanism. Neuron 2001; 30: 65–78.
109 Watanabe K, Kamiya D, Nishiyama A, Katayama T, Nozaki S,Kawasaki H et al. Directed differentiation of telencephalicprecursors from embryonic stem cells. Nat Neurosci 2005; 8:288–296.
110 Kawasaki H, Mizuseki K, Nishikawa S, Kaneko S, Kuwana Y,Nakanishi S et al. Induction of midbrain dopaminergic neuronsfrom ES cells by stromal cell-derived inducing activity. Neuron2000; 28: 31–40.
111 Perrier AL, Tabar V, Barberi T, Rubio ME, Bruses J, Topf N et al.Derivation of midbrain dopamine neurons from human embryo-nic stem cells. Proc Natl Acad Sci USA 2004; 101: 12543–12548.
iPSC modeling of psychiatric disordersKJ Brennand et al
14
Molecular Psychiatry

112 Li XJ, Du ZW, Zarnowska ED, Pankratz M, Hansen LO, Pearce RAet al. Specification of motoneurons from human embryonic stemcells. Nat Biotechnol 2005; 23: 215–221.
113 Wichterle H, Lieberam I, Porter JA, Jessell TM. Directeddifferentiation of embryonic stem cells into motor neurons. Cell2002; 110: 385–397.
114 Vierbuchen T, Ostermeier A, Pang ZP, Kokubu Y, Sudhof TC,Wernig M. Direct conversion of fibroblasts to functional neuronsby defined factors. Nature 2010; 463: 1035–1041.
115 Pang ZP, Yang N, Vierbuchen T, Ostermeier A, Fuentes DR, YangTQ et al. Induction of human neuronal cells by definedtranscription factors. Nature 2011; 476: 220–223.
116 Kim J, Su SC, Wang H, Cheng AW, Cassady JP, Lodato MA et al.Functional integration of dopaminergic neurons directly con-verted from mouse fibroblasts. Cell Stem Cell 2011; 9: 413–419.
117 Vrijenhoek T, Buizer-Voskamp JE, van der Stelt I, Strengman E,Sabatti C, Geurts van Kessel A et al. Recurrent CNVs disruptthree candidate genes in schizophrenia patients. Am J HumGenet 2008; 83: 504–510.
118 Riley B, Thiselton D, Maher BS, Bigdeli T, Wormley B,McMichael GO et al. Replication of association between schizo-phrenia and ZNF804A in the irish case-control study ofschizophrenia sample. Mol Psychiatry 2010; 15: 29–37.
119 Sun G, Tomita H, Shakkottai VG, Gargus JJ. Genomic organizationand promoter analysis of human KCNN3 gene. J Hum Genet 2001;46: 463–470.
120 Ide M, Yamada K, Toyota T, Iwayama Y, Ishitsuka Y, Minabe Yet al. Genetic association analyses of PHOX2B and ASCL1 inneuropsychiatric disorders: evidence for association of ASCL1with Parkinson’s disease. Hum Genet 2005; 117: 520–527.
121 Lin M, Pedrosa E, Shah A, Hrabovsky A, Maqbool S, Zheng Det al. RNA-Seq of human neurons derived from iPS cells revealscandidate long non-coding RNAs involved in neurogenesis andneuropsychiatric disorders. PLoS One 2011; 6: e23356.
122 Cheung AY, Horvath LM, Grafodatskaya D, Pasceri P, Weksberg R,Hotta A et al. Isolation of MECP2-null rett syndrome patient hiPScells and isogenic controls through X-chromosome inactivation.Hum Mol Genet 2011; 20: 2103–2115.
123 Marchetto MC, Carromeu C, Acab A, Yu D, Yeo GW, Mu Y et al.A model for neural development and treatment of rett syndromeusing human induced pluripotent stem cells. Cell 2010; 143:527–539.
124 Ananiev G, Williams EC, Li H, Chang Q. Isogenic pairs of wildtype and mutant induced pluripotent stem cell (iPSC) lines fromrett syndrome patients as in vitro disease model. PLoS One 2011;6: e25255.
125 O’Donnell WT, Warren ST. A decade of molecular studies offragile X syndrome. Annu Rev Neurosci 2002; 25: 315–338.
126 Nichol Edamura K, Pearson CE. DNA methylation and replica-tion: implications for the ‘deletion hotspot’ region of FMR1. HumGenet 2005; 118: 301–304.
127 Urbach A, Bar-Nur O, Daley GQ, Benvenisty N. Differentialmodeling of fragile X syndrome by human embryonic stemcells and induced pluripotent stem cells. Cell Stem Cell 2010; 6:407–411.
128 Sheridan SD, Theriault KM, Reis SA, Zhou F, Madison JM,Daheron L et al. Epigenetic characterization of the FMR1 gene andaberrant neurodevelopment in human induced pluripotent stemcell models of fragile x syndrome. PLoS One 2011; 6: e26203.
129 Pasca SP, Portmann T, Voineagu I, Yazawa M, Shcheglovitov A,Pasca AM et al. Using iPSC-derived neurons to uncover cellularphenotypes associated with Timothy syndrome. Nat Med 2011;17: 1657–1662.
130 Yazawa M, Hsueh B, Jia X, Pasca AM, Bernstein JA, Hallmayer Jet al. Using induced pluripotent stem cells to investigate cardiacphenotypes in Timothy syndrome. Nature 2011; 471: 230–234.
131 Chiang CH, Su Y, Wen Z, Yoritomo N, Ross CA, Margolis RL et al.Integration-free induced pluripotent stem cells derived fromschizophrenia patients with a DISC1 mutation. Mol Psychiatry2011; 16: 358–360.
132 Brennand KJ, Simone A, Jou J, Gelboin-Burkhart C, Tran N,Sangar S et al. Modelling schizophrenia using human inducedpluripotent stem cells. Nature 2011; 473: 221–225.
133 Paulsen BD, Maciel RD, Galina A, da Silveira MS, Souza CD,Drummond H et al. Altered oxygen metabolism associated toneurogenesis of induced pluripotent stem cells derived from aschizophrenic patient. Cell Transplant 2011 (e-pub ahead ofprint).
134 Meechan DW, Maynard TM, Tucker ES, LaMantia AS. Threephases of DiGeorge/22q11 deletion syndrome pathogenesisduring brain development: patterning, proliferation, and mito-chondrial functions of 22q11 genes. Int J Dev Neurosci 2011; 29:283–294.
135 Park YU, Jeong J, Lee H, Mun JY, Kim JH, Lee JS et al. Disrupted-in-schizophrenia 1 (DISC1) plays essential roles in mitochondriain collaboration with Mitofilin. Proc Natl Acad Sci USA 2010;107: 17785–17790.
136 Gore A, Li Z, Fung HL, Young JE, Agarwal S, Antosiewicz-Bourget J et al. Somatic coding mutations in human inducedpluripotent stem cells. Nature 2011; 471: 63–67.
137 Lister R, Pelizzola M, Kida YS, Hawkins RD, Nery JR,Hon G et al. Hotspots of aberrant epigenomic reprogrammingin human induced pluripotent stem cells. Nature 2011; 471:68–73.
138 Osafune K, Caron L, Borowiak M, Martinez RJ, Fitz-Gerald CS,Sato Y et al. Marked differences in differentiation propensityamong human embryonic stem cell lines. Nat Biotechnol 2008;26: 313–315.
139 Hu BY, Weick JP, Yu J, Ma LX, Zhang XQ, Thomson JA et al.Neural differentiation of human induced pluripotent stem cellsfollows developmental principles but with variable potency. ProcNatl Acad Sci USA 2010; 107: 4335–4340.
iPSC modeling of psychiatric disordersKJ Brennand et al
15
Molecular Psychiatry