
MKBC Theatres & ICU Reconfiguration and Upgrade · MKBC Theatres & ICU Reconfiguration and Upgrade...
130
MKBC Theatres & ICU Reconfiguration and Upgrade Outline Business Case
Transcript of MKBC Theatres & ICU Reconfiguration and Upgrade · MKBC Theatres & ICU Reconfiguration and Upgrade...
MKBC Theatres & ICU Reconfiguration and Upgrade
Outline Business Case

2
Document Control
Document Name MKBC Theatres & ICU Reconfiguration and Upgrade Outline Business Case
Document Version 0.8
Author Kevin Gauld
E-mail [email protected]
Phone number 0845 287 8500
Control Status DRAFT
Document Control
Version Date Reason for issue Issued To Issued By
0.0 15th January 2013 Layout/ Content agreement CL/ RS KG
0.1 28th January Inclusion of all OBC sections CL/ RS KG
0.2 21st February Inclusive of FMcD comment and exemplars
CL/ RS KG
0.3 25th March Further drafting CL/ RS KG
0.4 26th March Further drafting CL/ RS/ BMcW KG
0.5 28th March Further drafting post 28th March OBC Meeting
CL/ RS/ BMcW/ NR/ GM KG
0.6 24th April Further drafting from team CL/ RS/ BMcW/ FMcD KG
0.7 10th June Gateway Review Gateway Review Team KG
0.8 17th June NHSL CIG review NHSL CIG KG

3
Contents
1 Executive Summary
1.1 Introduction
1.2 Strategic Context
1.3 Option Appraisal Process
1.4 Commercial/ Financial Position
1.5 Conclusion and Recommendation
2 Strategic Case
2.1 Strategic Context
2.2 Organisational Overview
2.3 Business Strategy and Aims
2.4 Other Organisational Strategies
2.5 Investment Objectives
2.6 Existing Arrangements
2.7 Business Needs – Current and Future
2.8 Desired Scope/ Service Requirements
2.9 Benefits Criteria
2.10 Strategic Risks
2.11 Constraints and Dependencies
3 Economic Case
3.1 Introduction
3.2 Critical Success Factors
3.3 Main Business Options
3.4 Preferred Way Forward
3.5 The Short Listed Options
3.6 NPC/ NPV Findings
3.7 Benefits Appraisal
3.8 Risk Assessment
4
3.9 Preferred Option
3.10 Sensitivity Analysis
4 The Commercial Case
4.1 Introduction
4.2 Potential Scope and Service
4.3 Potential Risk Allocation
4.4 Potential Charging Mechanisms
4.5 Potential Key Contractual Arrangements
4.6 Potential Personnel Implications
4.7 Potential Implementation Timescales
4.8 Potential Accountancy Treatment
5 The Financial Case
5.1 Introduction
5.2 Potential Capital/ Funding Requirement
5.3 Revenue Impact
5.4 Potential Impact on Balance Sheet
5.5 Stakeholder Support
5.6 Overall Affordability
6 The Management Case
6.1 Introduction
6.2 Procurement Strategy
6.3 Project Management
6.4 Change Management
6.5 Benefits Realisation
6.6 Risk Management
6.7 Post Project Evaluation
7 Conclusion
7.1 Summary
5
Appendix:
01: Design Statement
02: A&DS/ HFS Letter of Support [will be included in SGHSCD submission]
03: AEDET Workshop
04: Risk Register
05: SWOT Analysis
06: Schedule of Accommodation
07: Letter of Financial Support [will be included in SGHSCD submission]
08: PSCP Stage 1B Programme
09: Schedule of Derogations

6
Glossary of Terms
7
1 Executive Summary
8
1.1 Introduction
This Outline Business Case (OBC) sets out the strategy for the refurbishment and upgrade of
the Theatres and ICU at Monklands District General Hospital.
The completion of the work described in this business case will address potential
environmental risks identified within the theatre and intensive care departments of Monklands
District General Hospital, as well as creating a safer environment for patients in keeping with
21st century standards, and dramatically improving the working environment for staff. These
benefits are entirely in accord with the ambitions of ‘A Healthier Future’.
1.2 Strategic Context
Monklands District General Hospital was constructed in 1974 and the theatre areas and ICU
are typical of the age of the building.
Different elements of the Theatre/ ICU department have been upgraded at several stages in
the past, with theatres 4, 7 and Recovery having improvement works delivered more recently
however the entire department has not received a co-ordinated overall refurbishment in the
recent past.
During 2009/10 Health Facilities Scotland (HFS), as part of a Scottish Government funded
project, surveyed theatre suites and associated ventilation plant in all Scottish acute hospitals.
Using Scottish Health Technical Memorandum (SHTM) 03-01 – “Ventilation for healthcare
premises” a benchmark was created to determine performance and compliance of the
ventilation plant. Subsequently the outcome of the HFS report advised the Board that the
condition of the Theatre ventilation plant was poor.
In the review of works required to ensure the Air Handling Units’ compliance with the SHTM, it
was noted in reports provided by Capita Symonds in April and July 2012 that the disruption
caused in carrying out any replacement work would be major. The reports also noted that:
The current plant room does not lend itself to replacement with removal being very
difficult due to close proximity of plant, ductwork or building fabric.
Power supply to each theatre to be upgraded and fitted with both UPS and IPS system
along with general upgrade work to general and emergency escape lighting which is
currently non- compliant
Issues with fire compartmentation and escape signage identified in several theatres
9
The overall recommendation from the Capita Symonds reports notes that due to the severe
disruption required to the theatre area in order to replace the AHUs initially, and several non-
compliances identified in the theatres regarding ventilation ductwork, fire compartmentation,
and fabric and architectural items, that a programmed theatre upgrade works package be
implemented at Monklands District General Hospital.
NHS Lanarkshire’s quality vision is to achieve transformational improvement in the provision
of safe, person centred and effective care for our patients and for our patients to be confident
that this is what they will receive, no matter where and when they access our services.
To achieve our quality vision, we are committed to transforming the quality of health care in
Lanarkshire through investment in and continuous reliable implementation of patient safety
processes. Through this we aim to:
be the safest health and care system in Scotland
have no avoidable deaths
reduce avoidable harm
deliver care in partnership with patients that is responsive to their needs
meet the highest standards of evidence based best practice
be an employer of choice
develop a culture of learning and improvement, characterised by our values of
Fairness, Respect, Quality and Working Together
The successful completion of the refurbishment and upgrade works will address the
immediate concerns with the plant and fabric of the current facilities, which in turn will allow
solid progress to be made towards both NHSL’s and SGHSCD’s vision for patient care.
1.3 Option Appraisal Process
A detailed process to determine a long list of possible options, assessment of these, and the
development of a short list of options for the refurbishment and upgrade of the Theatres and
ICU has been undertaken.
Following a non-financial benefits appraisal workshop and further financial appraisal, a
preferred option to meet service objectives has been identified. This full process is set out in
detail within this OBC.
The preferred option for the Theatres and ICU has been identified as the full refurbishment of
the existing seven theatres and the construction of a 10 bed ICU adjacent to the existing
theatre suite.
10
Sensitivity testing has been carried out from both a non-financial and financial perspective to
confirm that the identified option does not change under different scenarios and this has been
clearly shown to be the case.
1.4 Commercial/ Financial Position
The refurbishment and upgrade will be delivered through the Frameworks Scotland 2
procurement route and this OBC has been developed in accordance with those requirements
and also the Scottish Capital Investment Manual.
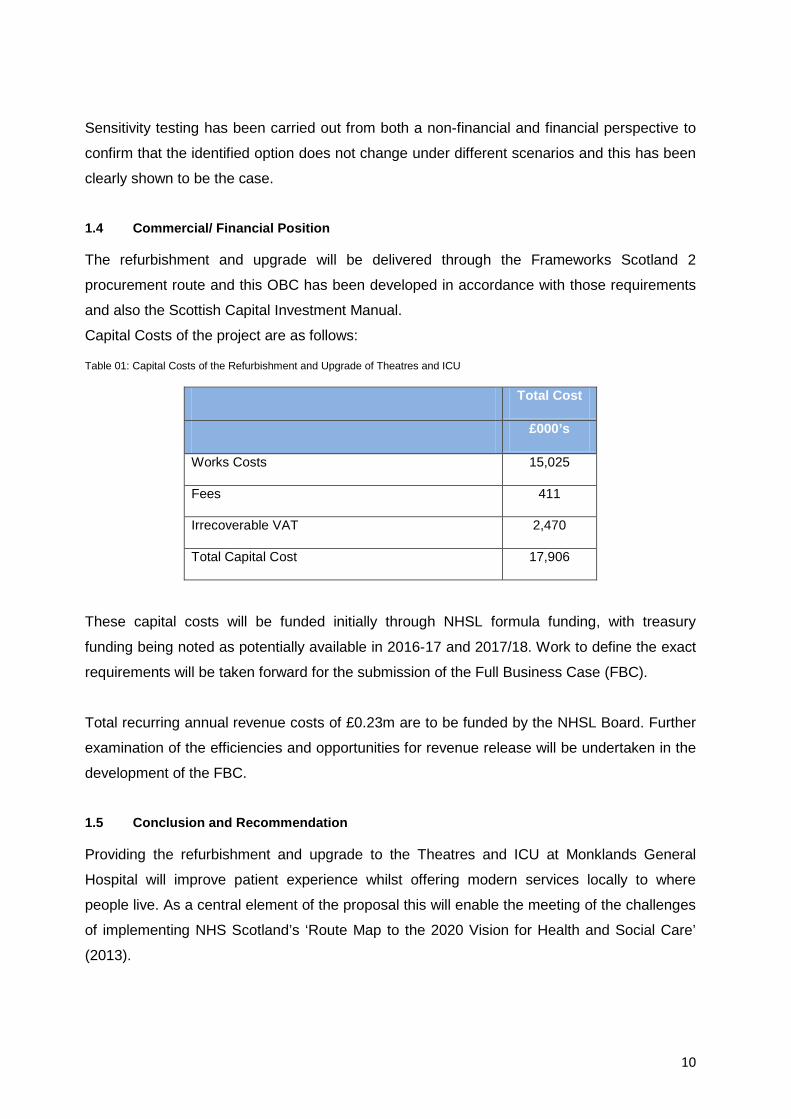
Capital Costs of the project are as follows:
Table 01: Capital Costs of the Refurbishment and Upgrade of Theatres and ICU
Total Cost
£000’s
Works Costs 15,025
Fees 411
Irrecoverable VAT 2,470
Total Capital Cost 17,906
These capital costs will be funded initially through NHSL formula funding, with treasury
funding being noted as potentially available in 2016-17 and 2017/18. Work to define the exact
requirements will be taken forward for the submission of the Full Business Case (FBC).
Total recurring annual revenue costs of £0.23m are to be funded by the NHSL Board. Further
examination of the efficiencies and opportunities for revenue release will be undertaken in the
development of the FBC.
1.5 Conclusion and Recommendation
Providing the refurbishment and upgrade to the Theatres and ICU at Monklands General
Hospital will improve patient experience whilst offering modern services locally to where
people live. As a central element of the proposal this will enable the meeting of the challenges
of implementing NHS Scotland’s ‘Route Map to the 2020 Vision for Health and Social Care’
(2013).
11
The Preferred Option, to refurbish the existing seven theatres alongside the construction of a
new build 10 bed ICU represents the best investment to provide the required services going
forward. It is the best value option, as has been demonstrated throughout this document, and
would fulfil the drivers identified in this OBC. These new facilities would provide a 21st century
environment that would meet the needs and aspirations of the patients within NHS
Lanarkshire.
Approval of this OBC will ensure that the project can move at pace towards the development
of the Full Business Case for this critical project.
12
2 Strategic Case
2.1 Strategic Context
The Scottish Government published their 2020 Vision in September 2011 which sets out the
actions required to achieve sustainable quality in Scotland’s Healthcare system. This strategic
narrative, set out by the Cabinet Secretary for Health and Wellbeing, provides the context for
taking forward the implementation of the Quality Strategy, published in May 2010, and the
actions required to improve efficiency and achieve financial sustainability. The vision is shown
in the box below.
Our ‘2020 Vision’
Our vision is that by 2020 everyone is able to live longer healthier lives at home, or in a homely
setting.
We will have a healthcare system where we have integrated health and social care, a focus on
prevention, anticipation and supported self management. When hospital treatment is required, and
cannot be provided in a community setting, day case treatment will be the norm. Whatever the
setting, care will be provided to the highest standards of quality and safety, with the person at the
centre of all decisions. There will be a focus on ensuring that people get back into their home or
community environment as soon as appropriate, with minimal risk of re-admission.
Source: Scottish Government, September 2011
In response to this vision NHSL has developed and published a framework for Strategic
Health Planning: ‘A Healthier Future 2012-2020’ to support future strategic health planning
and to facilitate definition of the actions required to achieve the Scottish Government’s 2020
Vision. This strategic framework will support NHSL to achieve the implementation of the 2020
vision and ensure that service change and developments are based upon the three Quality
ambitions of Patient Centred, Safe and Effective and enable improved efficiency and financial
sustainability within the Board.
NHS Lanarkshire’s quality vision is to achieve transformational improvement in the provision
of safe, person centred and effective care for our patients and for our patients to be confident
that this is what they will receive, no matter where and when they access our services.

13
We know that following an intensive review by Healthcare Improvement Scotland of NHS
Lanarkshire’s acute adult patient services in 2013 serious failings and unacceptable practice
were identified. We also know that UK and international evidence shows that up to 25 per
cent of patients experience a safety incident while in hospital. We do not believe this is
acceptable for our patients.
To achieve our quality vision, we are committed to transforming the quality of health care in
Lanarkshire through investment in and continuous reliable implementation of patient safety
processes. Through this we aim to:
be the safest health and care system in Scotland
have no avoidable deaths
reduce avoidable harm
deliver care in partnership with patients that is responsive to their needs
meet the highest standards of evidence based best practice
be an employer of choice
develop a culture of learning and improvement, characterised by our values of
Fairness, Respect, Quality and Working Together
The completion of the work described in this business case will address potential
environmental risks identified within the theatre and intensive care departments of Monklands
District General Hospital as well as creating a safer environment for patients in keeping with
21st century standards, the working environment for staff will be dramatically improved. These
benefits are entirely in accord with the ambitions of ‘A Healthier Future’.
14
2.2 Organisational Overview
NHSL serves a population of 600,000. The NHS Board is conterminous with North and South
Lanarkshire Councils. The legal entity is the Lanarkshire NHS Board. Within this, operational
delivery of all clinical services is organised around an Acute Services Division and two Health
and Social Care Partnerships (from 1st April 2015) – one for North Lanarkshire and one for
South Lanarkshire.
The principal role of the NHS Board is the protection and improvement of the health of the
resident population, and the delivery of high-quality, patient-focused services. Specifically, the
key functions of the NHS Board, for which it is accountable to the Scottish Government Health
& Social Care Directorates, on behalf of the Cabinet Secretary for Health and Wellbeing are:
Set the strategic direction of the organisation within the overall policies and priorities of
the Scottish Government and the National Health Service in Scotland
Define its annual and longer term objectives, and agree plans to achieve them
To oversee the delivery of planned results by monitoring performance against
objectives and ensuring corrective action is taken when necessary
To ensure effective financial stewardship through value for money, financial control
and financial planning and strategy
To ensure that high standards of Corporate Governance and personal behaviour are
maintained in the conduct of the business of the whole organisation
To ensure there is effective dialogue between the NHS Board, other agencies,
particularly North and South Lanarkshire Councils, and communities, on its plans and
performance, and that these are responsive to the communities’ assessed needs
The document which sets out how the NHS Board is expected to ensure the discharge of
these responsibilities is the Local Delivery Plan (LDP), constructed around the HEAT targets,
issued to the service each year by the Scottish Government Health and Social Care
Directorates (SGHSCD).
NHSL employs approximately 12, 000 staff and provides services in over 100 properties of
varying sizes. It has 3 District General Hospitals – at Wishaw, Hairmyres (East Kilbride) and
Monklands Hospital. The hospitals at Wishaw and Hairmyres were procured through the PFI
process and both opened in 2001 – the first PFI District General Hospitals in Scotland.
15
The Board has an annual expenditure of £1,074m in the provision of all health services in
Lanarkshire. The NHS Board comprising of Executive and Non Executive Directors meets
monthly in public and has established a rigorous approach to performance management
across a wide range of indicators with detailed reports provided either monthly or more
frequently as appropriate.
Included in the Non Executive membership of the Board are the leaders of both North and
South Lanarkshire Councils. This is a clear demonstration at the highest level of the
commitment to integrated working between health and local authorities to improve the health
and well-being of the people of Lanarkshire.
16
2.3 Business Strategy and Aims
The Scottish Government’s requirement to take forward the Quality Agenda through the 2020
Vision, the need to achieve financial sustainability and the need for improving the efficiency of
service delivery are all key drivers for NHS Boards to implement. ‘A Healthier Future 2012-
2020’ is flexible and has been developed to ensure that service changes and developments
can be assessed against a framework of strategic priorities. This will assist with prioritisation
and the approach to implementation.
This strategic framework will ensure that all service change and developments are assessed
against a clear criteria developed and will also ensure that all proposed actions move towards
the clear objectives of the 2020 vision. It is not a plan of specific service changes but a
framework against which service changes can be clearly and openly tested before
implementation. To undertake future changes without such assessment against the criteria
will not be acceptable.
The framework sets out the aims of NHSL for the period 2012-2020 and highlights the
intention of the Board to deliver the best quality of services to its patients.
The development of the framework for strategic health planning highlights a number of key
strategies and documents which set out plans and actions for developing services that
underpin the Board’s desire to improve patient care and offer improved access to services.
These plans will improve and develop clinical services within NHSL to reflect national
strategies and priorities. In particular, the strategies include:
Diagram 01: Strategies
17
These are underpinned by other strategies and plans but are specifically linked to a detailed
workforce development plan, the property strategy and a five-year financial plan.
The specific detail of individual actions within plans which require to be implemented in
2014/15 is consolidated within the Board’s Local Delivery Plan (LDP) which sets out key
organisational objectives and provides a mechanism to record progress in achieving and
complying with HEAT targets.
The method of service delivery is always evolving and the key to successful investment in
property is the ability to design facilities which meet our existing needs but can be flexible to
change to meet our future needs within the confines of a defined space. Investment should
also provide the opportunity for property to be enhanced in future if services needs and
resources demand this.
NHSL is responsible for the assessment of healthcare needs and for ensuring that a full range
of services are in place to meet these needs. This is undertaken against a background of
challenges and competing priorities.
18
2.4 Other Organisational Strategies
We are translating our action plan for the Healthcare Improvement Scotland Rapid Review
into a three year quality strategy, Transforming Patient Safety and Quality of Care in NHS
Lanarkshire, Healthcare Quality Assurance and Improvement Strategy 2014-17, to support the
on-going implementation of ‘A Healthier Future’ (NHS Lanarkshire’s strategic framework
taking forward the 2020 Vision) and to deliver against our quality vision. This will be a NHS
Lanarkshire wide strategy which will ensure that the initiatives and improvements commenced
in the acute hospitals are applied across all of our services.
The provision of a safe and effective healthcare environment for the provision of patient care
is an essential part of this transformational quality strategy, and is articulate with the Property
and Asset Management Strategy 2014 (PAMS).
The work of clinicians and support staff in operating theatres and intensive care can be
intense and demanding. The current facilities within Monklands do not meet the standards set
for a modern healthcare facility. The benefits to be achieved by this programme of works are
significant and will also support then ambition of NHS Lanarkshire to be an employer of choice
through providing a 21st century working environment for our staff.
19
2.5 Investment Objectives
The proposed investment has a number of key objectives which can be presented in the broad
categories of:
Diagram 02: Key Objectives
At an overarching level the proposed investment will:
Strategic/ Service:
Enable NHSL to achieve the objectives set out in the Scottish Government’s 2020
vision
Enable NHSL to achieve it’s the objectives set out in ‘A Healthier Future 2012-2020’
Design:
Achieve a high design quality in accordance with the Board’s Design Action Plan and
guidance available from HFS, A+DS and CABE
Meet statutory requirements and obligations for public buildings e.g. with regards to
DDA, HEI, HAI
Follow NHS Technical Guidance where appropriate
Work towards a BREEAM Healthcare rating of ‘Good’ under the HFS BREEAM
Pragmatic scheme
Improve flexibility through increased standardisation
20
Sustainability:
Deliver more energy efficient facilities within the NHSL estate contributing to a
reduction in whole life costs
Deliver facilities that provide value for money within the affordability caps set
Ensure ongoing financial sustainability in provision of services
Patient Experience:
Improved service coordination
Improved physical environment
Quality Strategy
The investment objectives have been designed to ensure that the Scottish Government 2020
vision is taken forward effectively and that the three quality ambitions are achieved. The
achievement of the three quality ambitions will ensure:
Person Centred
Implement service models which support the services’ strategic objectives by
optimising the quality of seamless care delivered for patients in Lanarkshire
Ensure that care is structured around the needs of patients and delivered through an
integrated (inpatient and community) pathway as agreed with the NHSL Strategic
Programmes
Embed integrated health and social care models of care to provide well co-ordinated,
flexible and responsive services to patients and their carers
Safe
To provide a physical environment that complies with modern standards of healthcare
and that promotes the safety, dignity, and privacy of all patients in purpose-built
facilities that significantly improve the patient experience
To create an environment which supports the improvement of HEI standards
Effective
To provide a therapeutic environment which allows the delivery of more appropriate
care that benefits patients and provides staff with improved conditions to deliver clinical
care
21
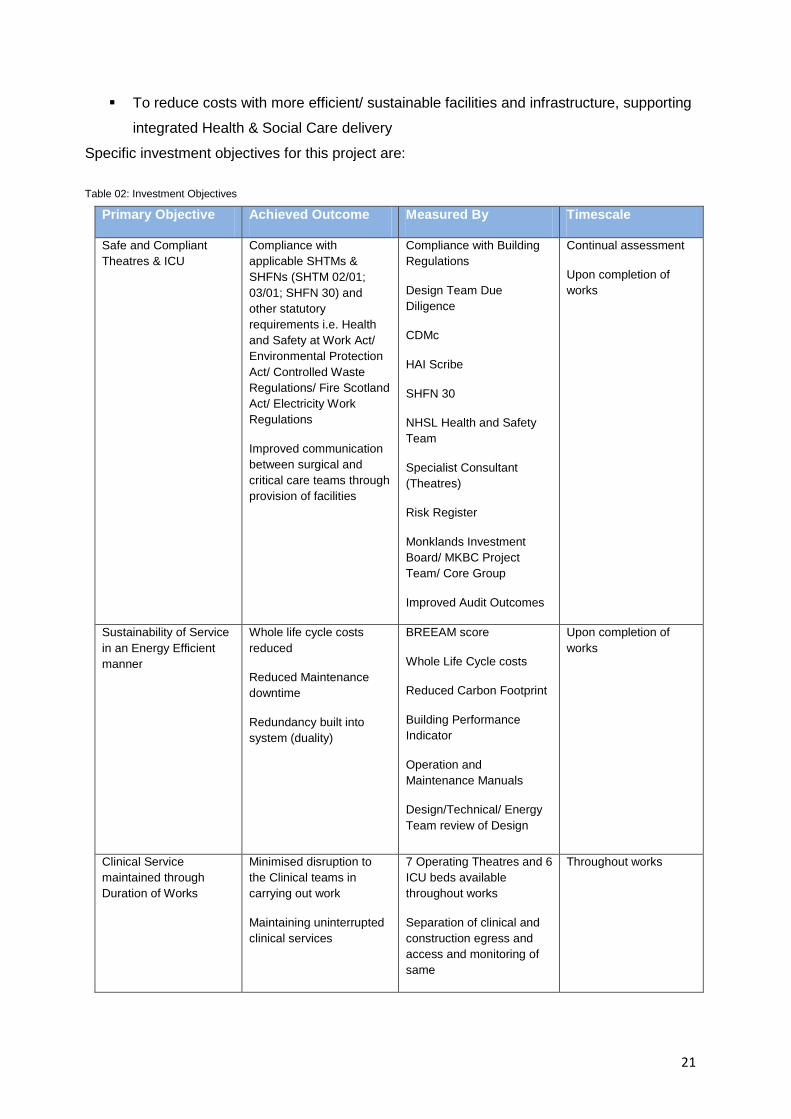
To reduce costs with more efficient/ sustainable facilities and infrastructure, supporting
integrated Health & Social Care delivery
Specific investment objectives for this project are:
Table 02: Investment Objectives
Primary Objective Achieved Outcome Measured By Timescale
Safe and Compliant Theatres & ICU
Compliance with applicable SHTMs & SHFNs (SHTM 02/01; 03/01; SHFN 30) and other statutory requirements i.e. Health and Safety at Work Act/ Environmental Protection Act/ Controlled Waste Regulations/ Fire Scotland Act/ Electricity Work Regulations
Improved communication between surgical and critical care teams through provision of facilities
Compliance with Building Regulations
Design Team Due Diligence
CDMc
HAI Scribe
SHFN 30
NHSL Health and Safety Team
Specialist Consultant (Theatres)
Risk Register
Monklands Investment Board/ MKBC Project Team/ Core Group
Improved Audit Outcomes
Continual assessment
Upon completion of works
Sustainability of Service in an Energy Efficient manner
Whole life cycle costs reduced
Reduced Maintenance downtime
Redundancy built into system (duality)
BREEAM score
Whole Life Cycle costs
Reduced Carbon Footprint
Building Performance Indicator
Operation and Maintenance Manuals
Design/Technical/ Energy Team review of Design
Upon completion of works
Clinical Service maintained through Duration of Works
Minimised disruption to the Clinical teams in carrying out work
Maintaining uninterrupted clinical services
7 Operating Theatres and 6 ICU beds available throughout works
Separation of clinical and construction egress and access and monitoring of same
Throughout works

22
Efficiency within the department leading to best practice and improved service delivery
Improved Patient flow from pre operative to post operative
Better bed space size
Better decontamination leads to improved productivity in endoscopy
More flexible usage of clinical spaces
Each theatre has anaesthetic room
Doubling number of laminar flow theatres
Reduced HAI Risk
Segregated paediatrics
Reduced length of stay
Improved turnover times in theatre
Design team review
On completion of works
Providing better working environment
Improved changing facilities
Improved catering facilities
Improved space utilisation and functional suitability through increased Theatre and ICU space
Improved Training facilities
Improved control over temperature and air circulation
Improved storage
Improved patient safety
Design Team Due Diligence
Compliance with Building Regulations
CDM
HAI Scribe
NHSL Health and Safety Team
Specialist Consultant (Theatres)
Risk Register
Monklands Investment Board/ MKBC Project Team / Core Group
Less down time through on- site training facilities and higher quality training environment
On completion of works
Improved facilities for carers and relatives
Segregated relative waiting and confidential interview rooms
Relative experience surveys
Ongoing
This investment will undoubtedly facilitate the modernisation of healthcare delivery at
Monklands District General Hospital. It is generally accepted that well designed health
buildings are conducive to the maintenance of good physical and mental health, and have a
23
positive effect on staff performance and retention. Such facilities should also improve the
efficiency of operational relationships and provide better value for money in terms of whole-life
costs. The objectives identified in this OBC are set within this context.
Design/ Quality Objectives
NHSL is committed to the integration of design quality throughout the project. A Design
Statement has been prepared through consultation and workshops with the key project
stakeholders.
The design statement sets out in detail the specific objectives to be achieved and sets out a
series of key, non-negotiable performance criteria related to patients, staff and visitors. It
defines benchmarks for how the design will help to deliver these objectives.
The design statement is the key briefing document for the Technical Team and has been used
to inform the more detailed briefing documents such as the Schedules of Accommodation, key
adjacencies and the room data sheets as the design progresses into Stage D. The design
statement is attached as Appendix 01.
A design submission for the project was made to HFS and A+DS in line with the NHS
Scotland Design Assessment process at this Outline Business Case stage on 19th March
2014. The project team is currently engaged in an open dialogue with the HFS team in order
to achieve a supported status for the scheme.
NHS Lanarkshire is committed to developing excellence in building design and providing fit for
purpose facilities for the patients they serve in Lanarkshire.
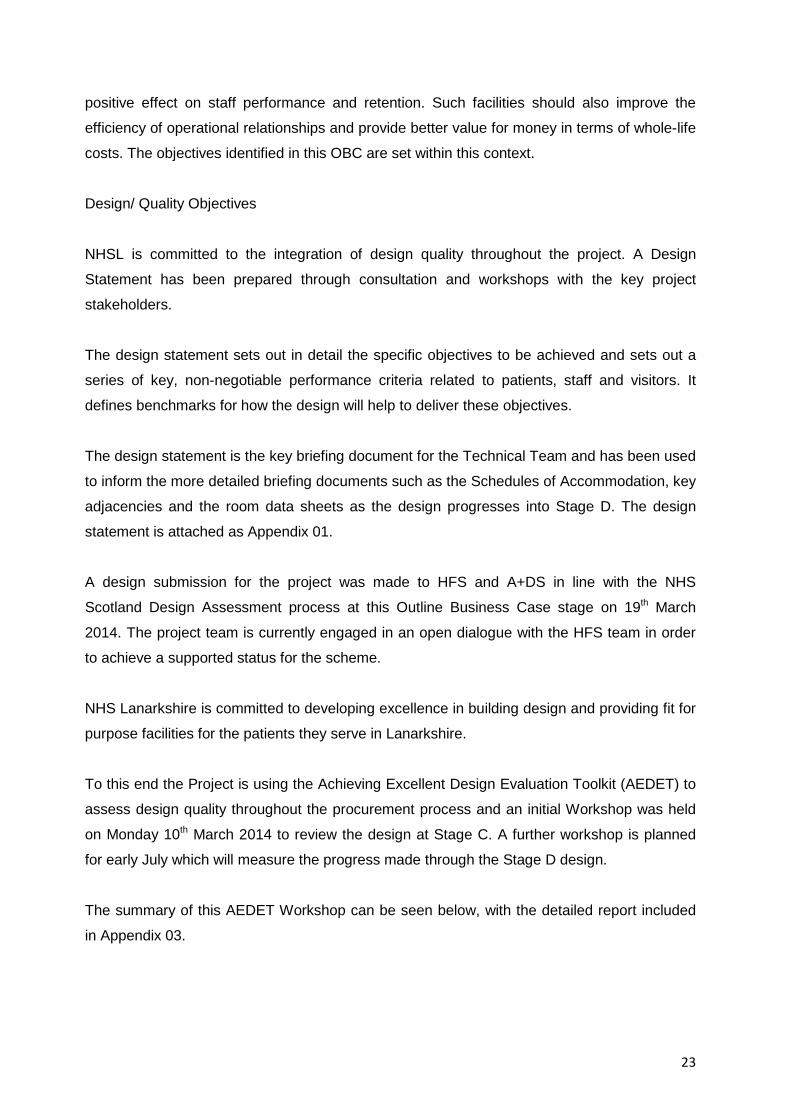
To this end the Project is using the Achieving Excellent Design Evaluation Toolkit (AEDET) to
assess design quality throughout the procurement process and an initial Workshop was held
on Monday 10th March 2014 to review the design at Stage C. A further workshop is planned
for early July which will measure the progress made through the Stage D design.
The summary of this AEDET Workshop can be seen below, with the detailed report included
in Appendix 03.
24
Diagram 03: AEDET Summary
There will be further AEDET reviews throughout the project ensuring that every category
scores higher than 4.0.
Sustainability Objective
NHS Lanarkshire is committed to developing sustainable, fit for purpose facilities for the
communities served in Lanarkshire and to that end a BREEAM Assessor was appointed early
in the planning and design process. It has been agreed with SGHSCD that the new BREEAM
Pragmatic Scheme being undertaken by Health Facilities Scotland will apply to the Project.
The design team is acutely aware of client requirements, and working in collaboration with
both NHSL and HFS throughout the process of design development, has considered all
aspects of the design throughout the life of the proposed works in order to achieve the
maximum value for money and energy efficiency that can be driven through BREEAM.
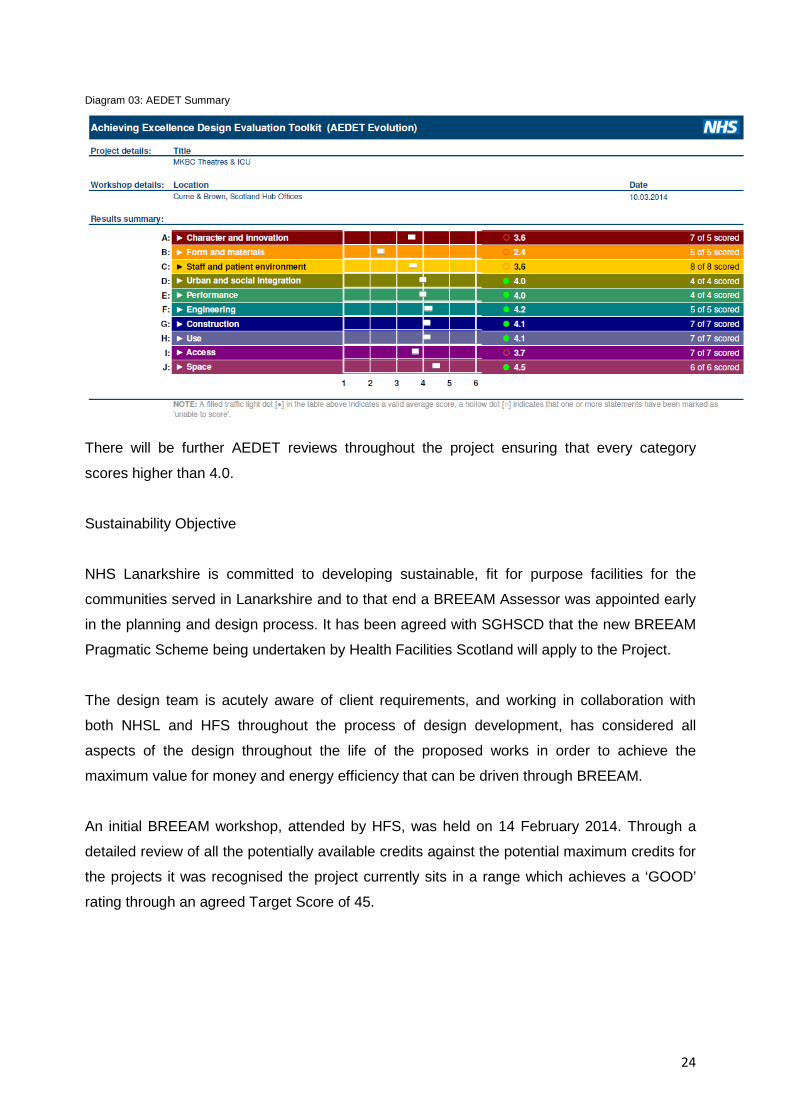
An initial BREEAM workshop, attended by HFS, was held on 14 February 2014. Through a
detailed review of all the potentially available credits against the potential maximum credits for
the projects it was recognised the project currently sits in a range which achieves a ‘GOOD’
rating through an agreed Target Score of 45.
25
Diagram 04: Current BREEAM Target Score
As noted previously, early engagement has been undertaken with HFS as part of the NDAP
submission for the project. An element of ongoing discussion is to ensure that the highest
possible score is achieved under the BREEAM Pragmatic route, with a practical view being
taken as to which credits are most suitable/ cost effective for the proposed works.
26
2.6 Existing Arrangements
2.6.1 Building and Fabric
Monklands District General Hospital opened in 1974 and the theatre areas are typical of the
age of the building with construction comprising of concrete floor slabs, brickwork walls and
metal stud/ plasterboard partitions, ‘waffle’ concrete soffits/ slab above ceiling voids. Corridor
and circulation areas have dated perforated steel ceiling panels spanning the width of the
corridor. Different elements of the Theatre/ ICU department have been upgraded at several
stages in the past, with theatres 4, 7 and Recovery having improvement works delivered more
recently however the entire department has not received a co-ordinated overall refurbishment
in the recent past. Alterations have been made to the original layout - some of which have
enhanced and some which have detracted from the original systems - and in some cases
these have not been fully integrated with the relevant Hospital systems or design. The central
core area is located between the two circulation corridors adjacent to the north and south
theatres and a large proportion of the core area is taken up with the TSSU.
The existing AHUs serving the Theatre and associated areas are the original units, in excess
of 35 years old and are now beyond the end of their economical lifespan.
The Theatres are served by packaged Air Handling Units located in the first floor plantroom.
These units provide conditioned supply air to the theatres. Conditioned supply air is introduced
into the theatre space via high level linear diffusers The primary supply air is drawn from a
brick built plenum chamber, which is common to all surgical unit AHU’s located in the
plantroom. Due to the age of the AHUs, spare parts are difficult to obtain and any AHU
breakdown has the potential to cause significant business continuity issues.
During 2009/10 Health Facilities Scotland (HFS), as part of a Scottish Government-funded
project, surveyed theatre suites and associated ventilation plant in all Scottish acute hospitals.
The Monklands District Hospital theatre suite was surveyed on 12th January 2010.
Using Scottish Health Technical Memorandum (SHTM) 03-01 – “Ventilation for healthcare
premises” (awaiting publication at that time) a benchmark was created to determine
performance and compliance of the ventilation plant. Subsequently the outcome of the HFS
report advised the Board that the condition of the Theatre ventilation plant was poor.
27
NHS Lanarkshire placed the Theatre ventilation risk onto the Monklands Business Continuity
Risk register, and put in place interim control measures with Maintenance Services and
Infection Control to ensure that any risk exposure to patients was monitored.
In the review of works required to ensure the AHUs compliance with the SHTM, it was noted in
subsequent Capita Symonds reports of April and July 2012 that the disruption caused in
carrying out any replacement work would be major. The reports also noted that:
The current plant room does not lend itself to replacement with removal being very
difficult due to close proximity of plant, ductwork or building fabric.
Power supply to each theatre to be upgraded and fitted with both UPS and IPS system
along with general upgrade work to general and emergency escape lighting which is
currently non- compliant
Issues with fire compartmentation and escape signage identified in several theatres
The overall recommendation from the Capita Symonds reports notes that due to the severe
disruption required to the theatre area in order to replace the AHUs initially, and several non-
compliances identified in the theatres regarding ventilation ductwork, fire compartmentation,
and fabric and architectural items, that a programmed theatre upgrade works package be
implemented at Monklands District General Hospital.
2.6.2 Theatres:
The existing theatres currently provide a range of services to patients undergoing both major
and minor surgery, including two centralised services in Urology and Ear, Nose and Throat
Maxillofacial.
Since the construction of the theatres there have been many developments in associated
technologies such as laparoscopic and lasers which has led to additional items of equipment
being added to the existing space. This has impacted the theatres whereby they are no longer
of a suitable size to manage all of the required equipment, hindering flow and productivity
through the area. There has also been an impact on certain procedures e.g. certain
anaesthetic blocks due to the rooms being of inadequate size to accommodate the patient,
staff and equipment in the same space.
The flow of patients is also problematic as both male and female pre and post operative
patients are located in the same area, segregated only by a small partition which brings with it
issues around patient privacy and dignity. Similar issues exist with paediatric patients as there
is no current area where they can be segregated from adult patients.

28
To compound matters the existing operating theatres are also fully utilised, leaving very limited
opportunity for planned maintenance. Loss of any operating rooms through AHU failure would
have a considerable impact on NHS Lanarkshire’s ability to provide surgical care. This would
result in cancellation of operations, an increase in waiting times and provide a potential risk to
patients.
2.6.3 ICU
2.6.3.1 Critical Care Needs Assessment:
NHSL undertook a comprehensive needs assessment in 2011, the data from which
demonstrated an inadequacy of Level 3 beds and Level 1 beds, with a satisfactory availability
of Level 2 beds.
Critical Care beds are defined as Level 1, 2 or 3. The following is the standard UK definition
for the category of patient housed in these beds:
Diagram 05: Critical Care Bed definition
The current situation in Monklands displays a disparate scattering of critical care throughout
the hospital:
Stand alone 6 bedded ICU (Level 3) situated next to the theatre complex on the
ground floor.
Stand alone 8 bedded surgical HDU within the surgical tower on the 2nd floor. Funded
for 8 HDU surgical patients from all disciplines within the surgical directorate (Level 2).
4 General medical HDU beds within ward 18 on the medical tower (Level 2). This ward
also has 6 CCU beds and step down cardiology beds.
Level 1: Patients at risk of their condition deteriorating, or those relocated from higher levels of care whose needs can be met on an acute ward with additional advice and support from the critical care team Level 2: Patients requiring more detailed observation or intervention including support for a single failing organ or postoperative care, and those stepping down from higher levels of care Level 3: Patients requiring advanced respiratory support alone, or basic respiratory support, together with support of at least two organ systems. This level includes all complex patients requiring support for multi-organ failure
29
2 renal HDU beds within ward 1 Renal Unit (Level 2). This ward lies separate to the
main hospital on the ground floor linked by a glass corridor.
Analysis of the 2011 study revealed that 50% of patients within surgical HDU actually required
Level 1 care. Simply translated this means that 4 out of the 8 beds effectively operate at Level
1.
Since the needs assessment was carried out, further pressure on the availability of surgical
HDU beds has arisen due to the increase in major operating on the site, particularly within
Urology.
2.6.3.2 Planned Redevelopment:
For the short to medium term, restructuring of beds within the surgical tower at Monklands, in
particular ward 4a (Emergency Surgical Receiving Unit), ward 4 (General Surgery), ward 5
(Surgical HDU), ward 6 (Urology) and ward 7 (General Surgery) has started and ongoing
discussions are underway to address the following patient centred, safe and effective
developments:
Introduction of a 4 bedded surgical GP assessment bay within the ESRU (Ward 4a)
open 08.00 – 18.00 Monday to Friday
The need for more beds providing heightened level of care post- operatively due to the
nature and volume of major surgery on the site
The launch of an enhanced recovery programme to improve the perioperative quality
of care
The requirement to expand the same day admission unit
The expansion of in- patient Urology bed numbers
2.6.3.3 Hospital Wide Operational Impact:
The CCNA suggests that a number of Level 1 beds are needed on the site and the Enhanced
Recovery Programme as applied to major urology and colorectal cases requires support. For
the surgical directorate, up to 8 Level 1 beds would satisfy these demands. If 4 of the current
Level 2 surgical HDU beds were relocated to a combined ICU/ HDU this would theoretically
leave nurse staffing for 4 Level 2 beds on ward 5. This resource would provide the basis for
safe staffing of Level 1 beds in the surgical tower.
As outlined above, existing preliminary plans to redevelop and re- designate beds within the
surgical tower would allow the development of a Level 1 surgical HDU which could house
appropriate post- operative and emergency non- operative surgical cases. The overall impact
30
is freeing up of beds within the surgical tower proportionate to the number of additional beds
provided within a combined ICU/ HDU.
Through progression of this OBC an opportunity would arise to improve the standard of critical
care delivered on the Monklands site. As part of the essential theatre refurbishment the first
major phase of the project would involve the relocation of the current Intensive Care Unit to a
10 bed ICU in a standalone building next to the current geographical locus providing the
ongoing benefits of a ground floor placement and proximity to the main operating theatre
complex.
A larger 10 bedded combined ICU/ HDU will afford greater flexibility, greater workforce
efficiencies, greater business continuity options, greater training potential and ultimately better
patient care in line with the quality ambitions of the Scottish Government Healthcare Quality
Strategy.
31
2.7 Business Needs – Current & Future
Current Business Needs
The current situation with the 7 operating theatre facilities on the Monklands site is such that
scheduled cases are planned across a 6 day working week with evenings and weekends held
open for emergency cases.
The ICU service is adjacent to the theatre complex. The current service provision is 5 beds in
this area. This area is undersized in relation to the healthcare standard Scottish Health
Planning Note 27, which consequently has an impact on its operational functionality
As part of a Scottish Government-funded project Health Facilities Scotland surveyed theatre
suites and associated ventilation plant in Scottish acute hospitals in 2010. As part of that
initiative the plant serving the Monklands District Hospital theatre suites was surveyed on 12th
January 2010.
Using Scottish Health Technical Memorandum (SHTM) 03-01 – “Ventilation for healthcare
premises” a benchmark was created to determine performance and compliance of the
ventilation plant. The subsequent outcome of this report advised the Board in February 2011,
that the condition of the Theatre ventilation plant was scored as poor.
The exposure to patients and staff is further compounded through non-compliance with other
healthcare technical memorandum and healthcare standards such as Firecode, Fabric
condition and CIBSE lighting standards. However the standards of Infection Control (Scottish
Health Facilities Note (SHFN) 30) are compromised as perioperative infection, staff safety due
to the non-compliant size of the theatres and fabric condition have increased the risk rating in
conjunction with the ventilation issues to that of ‘High’.
NHS Lanarkshire placed the Theatre refurbishment onto the Monklands Business Continuity
Risk register and subsequently put in place interim control measures of additional
environmental monitoring through Maintenance Services and Infection Control to ensure that
any risk is minimised.
Future Business Needs
The number of Theatres remains the same under the refurbishment scheme as the physical
footprint available will not permit expansion, however they will be significantly improved with
regards to current healthcare guidance post works completion.
32
It is also acknowledged that providing additional theatres within the envelope would also result
in smaller theatres and thus non- compliance with the healthcare standards once again.
To accommodate any expansion in theatre/ patient activity, the existing Day Surgery provision
on site will be used to take up any future increase.
ICU will be expanded into a combined ICU/HDU with the capacity of 10 beds ensuring
compliance with healthcare guidance.
The areas that require improvement to ensure that the service and the facilities comply with
legislation and healthcare guidance are as follows:
Functional suitability
Space utilisation
Physical Condition
Quality of patient care
Ventilation
HEI
Control of Infection
Fire Safety
Energy use
33
2.8 Desired Scope/ Service Requirements
The Theatre suite in Monklands Hospital is now over 30 years old and no longer meets the
requirements for patient management in the 21st century. The physical infrastructure
including; air handling systems, size of theatres and anaesthetic facilities does not meet
current standards. Moreover, the current environment limits both the efficiency of theatre and
the type of surgery that can be carried out.
The theatre suite has always achieved compliance with Health Environment Inspections (HEI)
guidelines and Patient Safety Requirements. However, there are now regular issues with the
theatre environment that are cause for concern both in the short and longer term.
Maintenance of the theatre infrastructure is now proving more challenging and structural
issues are becoming more frequent with a high risk of treatment delays and list cancellations.
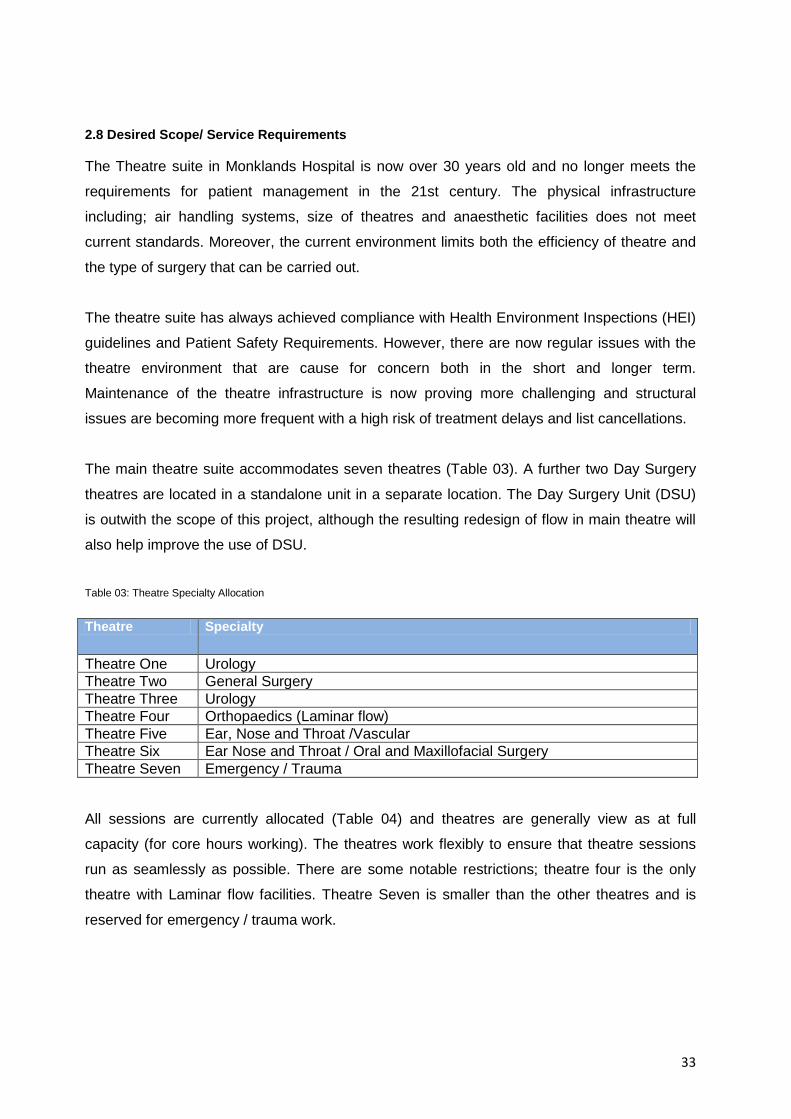
The main theatre suite accommodates seven theatres (Table 03). A further two Day Surgery
theatres are located in a standalone unit in a separate location. The Day Surgery Unit (DSU)
is outwith the scope of this project, although the resulting redesign of flow in main theatre will
also help improve the use of DSU.
Table 03: Theatre Specialty Allocation
Theatre Specialty
Theatre One Urology Theatre Two General Surgery Theatre Three Urology Theatre Four Orthopaedics (Laminar flow) Theatre Five Ear, Nose and Throat /Vascular Theatre Six Ear Nose and Throat / Oral and Maxillofacial Surgery Theatre Seven Emergency / Trauma
All sessions are currently allocated (Table 04) and theatres are generally view as at full
capacity (for core hours working). The theatres work flexibly to ensure that theatre sessions
run as seamlessly as possible. There are some notable restrictions; theatre four is the only
theatre with Laminar flow facilities. Theatre Seven is smaller than the other theatres and is
reserved for emergency / trauma work.
34
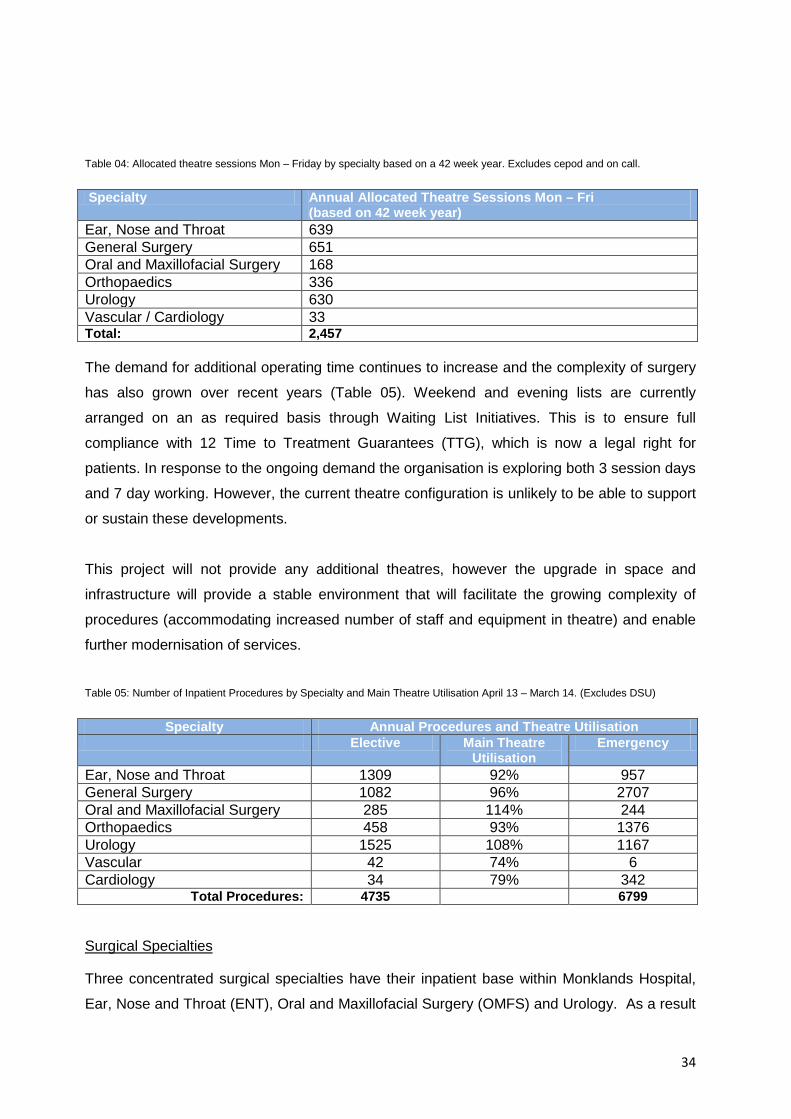
Table 04: Allocated theatre sessions Mon – Friday by specialty based on a 42 week year. Excludes cepod and on call.
Specialty Annual Allocated Theatre Sessions Mon – Fri (based on 42 week year)
Ear, Nose and Throat 639 General Surgery 651 Oral and Maxillofacial Surgery 168 Orthopaedics 336 Urology 630 Vascular / Cardiology 33 Total: 2,457 The demand for additional operating time continues to increase and the complexity of surgery
has also grown over recent years (Table 05). Weekend and evening lists are currently
arranged on an as required basis through Waiting List Initiatives. This is to ensure full
compliance with 12 Time to Treatment Guarantees (TTG), which is now a legal right for
patients. In response to the ongoing demand the organisation is exploring both 3 session days
and 7 day working. However, the current theatre configuration is unlikely to be able to support
or sustain these developments.
This project will not provide any additional theatres, however the upgrade in space and
infrastructure will provide a stable environment that will facilitate the growing complexity of
procedures (accommodating increased number of staff and equipment in theatre) and enable
further modernisation of services.
Table 05: Number of Inpatient Procedures by Specialty and Main Theatre Utilisation April 13 – March 14. (Excludes DSU)
Specialty Annual Procedures and Theatre Utilisation Elective Main Theatre
Utilisation Emergency
Ear, Nose and Throat 1309 92% 957 General Surgery 1082 96% 2707 Oral and Maxillofacial Surgery 285 114% 244 Orthopaedics 458 93% 1376 Urology 1525 108% 1167 Vascular 42 74% 6 Cardiology 34 79% 342
Total Procedures: 4735 6799
Surgical Specialties
Three concentrated surgical specialties have their inpatient base within Monklands Hospital,
Ear, Nose and Throat (ENT), Oral and Maxillofacial Surgery (OMFS) and Urology. As a result
35
all inpatient surgery, for these specialties, is restricted to Monklands Hospital. In addition,
Urology and ENT are high volume specialties and consequently place a high demand on
theatre time. This is an important consideration as these services cannot be easily relocated
either within Lanarkshire or externally.
Urology surgical procedures range in complexity from minor surgery to complex corrective or
cancer surgery. The service has seen a major increase in cancer surgery and the incidences
of Urology cancer is predicted to increase significantly over the next three years. This includes
prostate (49%), Kidney (21%), bladder (13%) and testicular cancer (6%). This has
implications not only in terms of the volume of surgery but also in complexity and developing
surgical techniques.
The wide spread move to laparoscopic surgery has placed considerable demand on theatre
time with many Urology procedures now require anything from one to three sessions per
patient. The demographic makeup of urology referrals is an indicator for future demand with
74% of patients in the over 50 year age group. Unfortunately, these patients often have other
health issues and specific anaesthetic requirements placing additional pressure on ITU /HDU
facilities post operatively.
In contrast to Urology, Ear, Nose and Throat (ENT) patients span a wide range of ages and
Paediatric surgery is a main feature of the ENT workload. This creates additional challenges in
achieving appropriate segregation of operating lists and recovery space within the theatre suit
to comply with paediatric guidelines. The redesign of patient flow and space included in the
project proposals will resolve these issues.
One of the main issues for ENT is patient volume with a high number of routine procedures. It
is planned to reflow a proportion of ENT procedures to DSU. However, this requires a number
of elements to be put in place relating to organisation, flow and recovery space which will be
influenced by this project. In addition, 15% of referrals for patients with ear problems convert
to surgery. This is intricate surgery (including Myringoplasty and Stapedectomy) with these
procedures often taking one session and requiring the continued use of a microscope during
surgery. This has been noted as an issue during works, as excessive vibration can disturb
these procedures.
Three ENT consultants also make up part of the NHS Lanarkshire Head and Neck service.
This forms the bulk of major and complex surgery in ENT including; Thyroidectomy and
36
Laryngectomy. NHS Lanarkshire has the third highest incidence of Head and Neck Cancer in
Scotland, therefore, this type of surgery will continues to increase.
Oral and Maxillofacial Surgery (OMFS) is the third concentrated specialty on the Monklands
site. This is a much smaller specialty in terms of numbers but treats a high proportion of facial
trauma including; fractures to the malar, maxilla and mandible.
OMFS makes up the remaining part of the Head and Neck service performing complex
surgery on floor of mouth cancer including facial reconstruction. The remaining elective
procedures focus on Orthognathic surgery. The procedures undertaken in both types of
surgery require one to three sessions per patient.
The Orthopaedic department provides a range of joint surgery including knee and hip
replacements as well as revisions. This type of surgery is currently restricted within Monklands
Hospital as only theatre four contains a laminar flow system. It is proposed that this will be
expanded to a second theatre as a result of this project.
Trauma also forms a major part of the orthopaedic workload. Monday to Friday there are 5
morning theatre sessions dedicated to trauma. During their on call week the orthopaedic
surgeons elective lists are backfilled to further increase capacity.
General surgery includes a range of sub specialties including colorectal surgery and breast
surgery. The increase in colorectal cancer and resulting increase in complex bowel surgery
has been an ongoing issue in accessing theatre space.
As with other specialties there has been a move to laparoscopic surgery for Gallbladder
surgery and Hernia. The benefits in this type of surgery are well known for patients and
include a quicker recovery and reduced length of stay in hospital. However, in theatre terms
these procedures take longer, demanding more theatre time and require additional equipment
and staff in theatre.
Trauma and Emergency access is required by all surgical specialties within Monklands
Hospital. Theatre 7 accommodates emergency surgery 24 hours a day, 7 days per week.
Monday to Friday the morning sessions of the emergency lists are given to orthopaedic
trauma. In addition, each surgeon gives up a session of their allocated theatre time on a
rotational basis to provide a daily morning CEPOD list.
Critical Care
37
As part of the refurbishment of theatre the first major phase requires the relocation of the
current intensive care unit (ICU). It has been agreed that a ten bedded unit will replace the
current 6 bedded ICU and 8 bedded High Dependency Unit (HDU) (Table 06). This will move
to a combined unit staffed to enable flexing up and down between levels of care depending on
site demand. The location of the replacement unit has been identified and construction can
take place with minimal disruption to the existing facilities.
Critical Care Needs Assessment
NHS Lanarkshire undertook a comprehensive needs assessment in 2011. This demonstrated
a shortfall in Level 3 and Level 1 beds. However, an over provision of Level 2 beds were also
identified with 50% of patients within the surgical HDU requiring only Level 1 care. This was
further confirmed by local audit including the day of care audit. Therefore, based on the
introduction of a minimum of 4 level 1 beds the number of HDU beds could be reduced to 4.
ICU beds are staffed to 5 beds for the most part of the year increasing to 6 beds over winter
when demand increases. Establishing a joint unit builds in flexibility around the provision of
both ICU and HDU beds in response to demand.
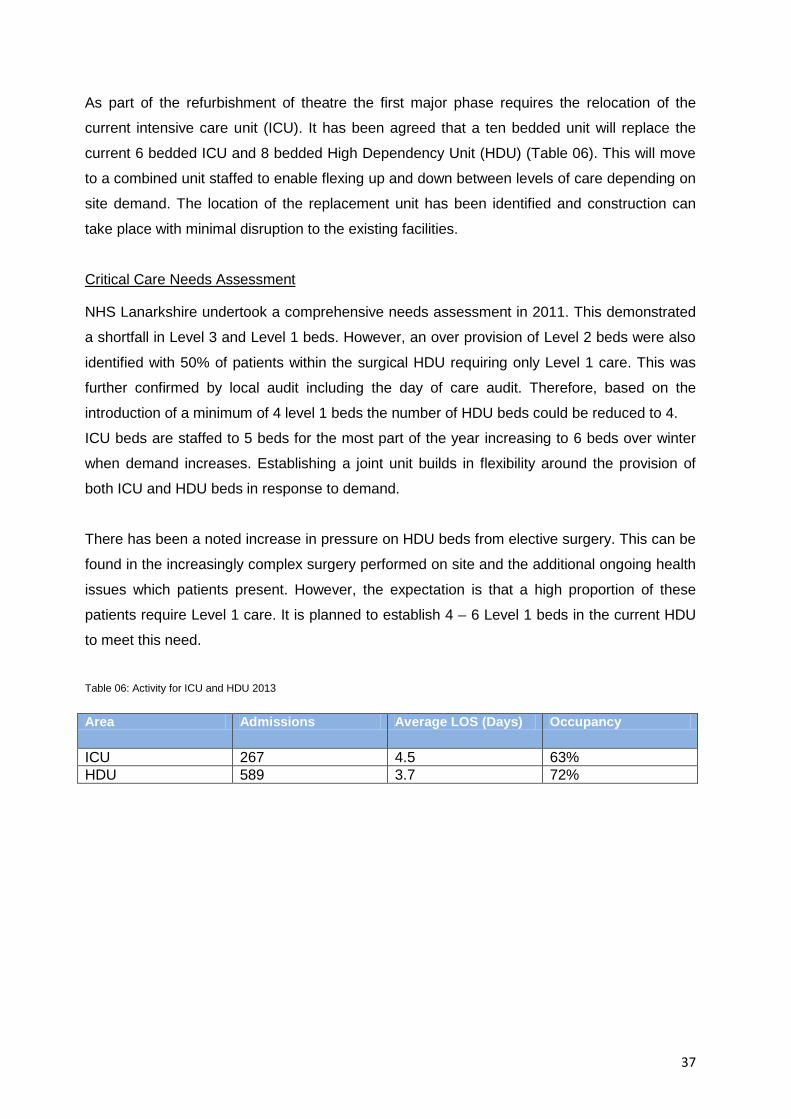
There has been a noted increase in pressure on HDU beds from elective surgery. This can be
found in the increasingly complex surgery performed on site and the additional ongoing health
issues which patients present. However, the expectation is that a high proportion of these
patients require Level 1 care. It is planned to establish 4 – 6 Level 1 beds in the current HDU
to meet this need.
Table 06: Activity for ICU and HDU 2013
Area Admissions Average LOS (Days) Occupancy
ICU 267 4.5 63% HDU 589 3.7 72%

38
2.9 Benefits Criteria
This section describes the main benefits and outcomes associated with the project and how
these will be measured. The table below summarises the benefits identified and carried into
the appraisal of the project options:
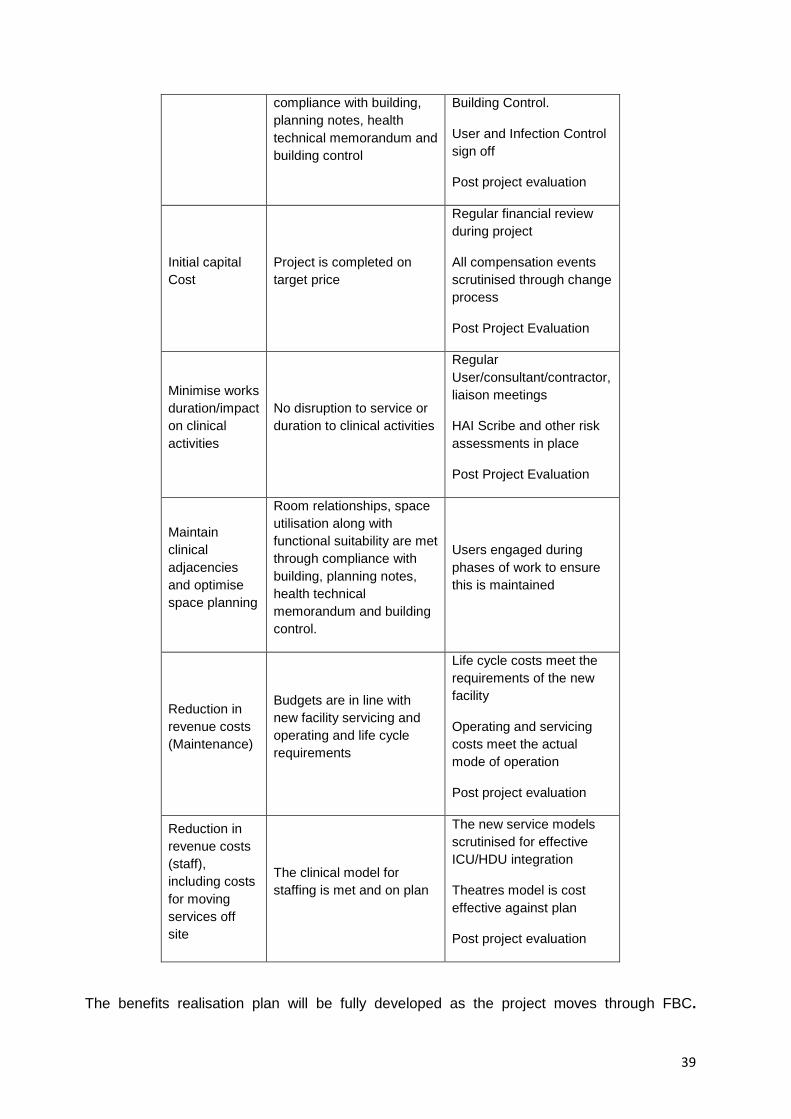
Table 07: Benefits Criteria
Benefit Outcomes Measure
Mitigation of fire safety compliance risk
Firecode and building control requirements are improved and compliance achieved against standards
Commissioned and signed off by building control and Fire safety advisors.
Post Project Evaluation
Mitigation of AHU failure risk
Air handling units and ventilation systems refurbished to compliant standards
Commissioned and signed off by Consulting Engineers, Architects and Building Control.
Infection Control confirmation that works are satisfactory
Post project evaluation
Mitigation of infection control risk, due to building fabric
All fabric replaced/upgraded in line with SHFN 30, HAI Scribe and healthcare compliant supplied materials
Commissioned and signed off by Consulting Engineers, Architects and Building Control.
Infection Control confirmation that works are satisfactory
Post project evaluation
Mitigation of risk to clinical continuity
Room relationships and space utilisation along with functional suitability are met through compliance with building, planning notes and building control
Commissioned and signed off by Consulting Engineers, Architects and Building Control.
User sign off
Post project evaluation
Mitigation of risk to patient safety
Room relationships, space utilisation and HAI/Quality along with functional suitability are met through
Commissioned and signed off by Consulting Engineers, Architects and
39
compliance with building, planning notes, health technical memorandum and building control
Building Control.
User and Infection Control sign off
Post project evaluation
Initial capital Cost
Project is completed on target price
Regular financial review during project
All compensation events scrutinised through change process
Post Project Evaluation
Minimise works duration/impact on clinical activities
No disruption to service or duration to clinical activities
Regular User/consultant/contractor, liaison meetings
HAI Scribe and other risk assessments in place
Post Project Evaluation
Maintain clinical adjacencies and optimise space planning
Room relationships, space utilisation along with functional suitability are met through compliance with building, planning notes, health technical memorandum and building control.
Users engaged during phases of work to ensure this is maintained
Reduction in revenue costs (Maintenance)
Budgets are in line with new facility servicing and operating and life cycle requirements
Life cycle costs meet the requirements of the new facility
Operating and servicing costs meet the actual mode of operation
Post project evaluation
Reduction in revenue costs (staff), including costs for moving services off site
The clinical model for staffing is met and on plan
The new service models scrutinised for effective ICU/HDU integration
Theatres model is cost effective against plan
Post project evaluation
The benefits realisation plan will be fully developed as the project moves through FBC.
40
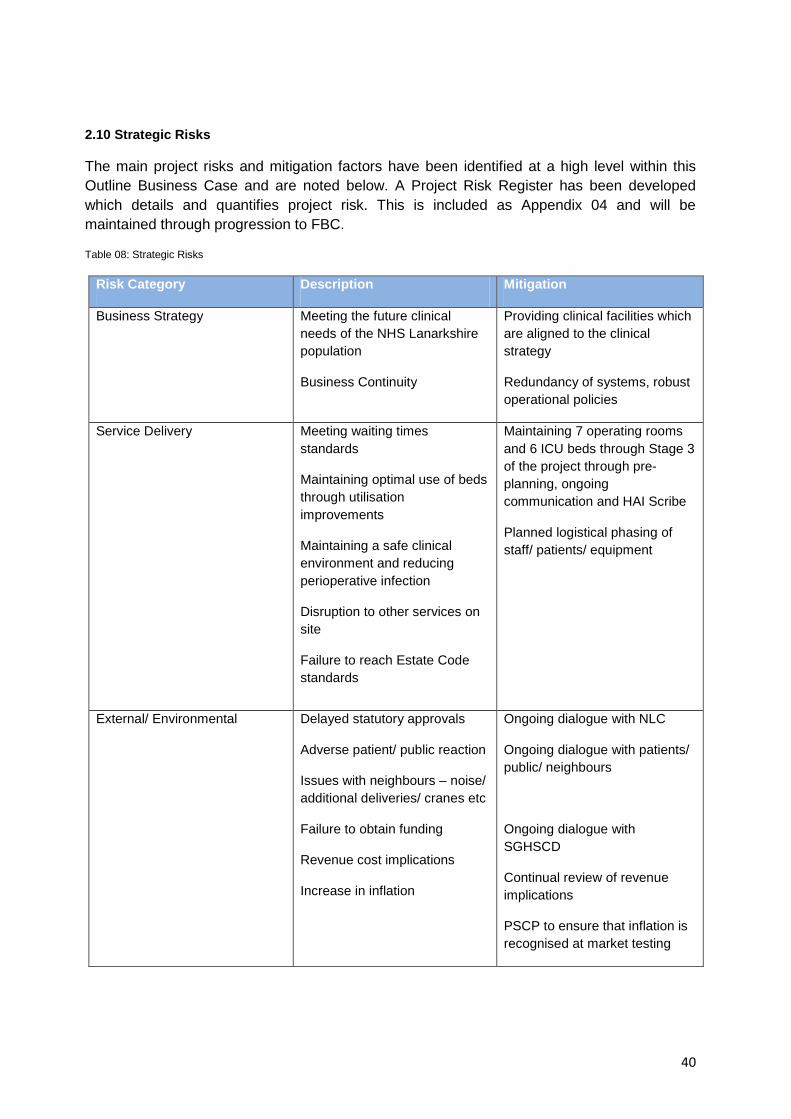
2.10 Strategic Risks
The main project risks and mitigation factors have been identified at a high level within this Outline Business Case and are noted below. A Project Risk Register has been developed which details and quantifies project risk. This is included as Appendix 04 and will be maintained through progression to FBC.
Table 08: Strategic Risks
Risk Category Description Mitigation
Business Strategy Meeting the future clinical needs of the NHS Lanarkshire population
Business Continuity
Providing clinical facilities which are aligned to the clinical strategy
Redundancy of systems, robust operational policies
Service Delivery Meeting waiting times standards
Maintaining optimal use of beds through utilisation improvements
Maintaining a safe clinical environment and reducing perioperative infection
Disruption to other services on site
Failure to reach Estate Code standards
Maintaining 7 operating rooms and 6 ICU beds through Stage 3 of the project through pre- planning, ongoing communication and HAI Scribe
Planned logistical phasing of staff/ patients/ equipment
External/ Environmental Delayed statutory approvals
Adverse patient/ public reaction
Issues with neighbours – noise/ additional deliveries/ cranes etc
Failure to obtain funding
Revenue cost implications
Increase in inflation
Ongoing dialogue with NLC
Ongoing dialogue with patients/ public/ neighbours
Ongoing dialogue with SGHSCD
Continual review of revenue implications
PSCP to ensure that inflation is recognised at market testing
41
This OBC details the development of risks into a formal risk register capturing individual risks within each category. The format of the risk register follows the guidance set in the Scottish Capital Investment Manual (SCIM) and has been formatted as per the guidance provided in the NHS Health Improvement Standards (NHSHIS). An initial project risk register was established at a Core Team Risk Workshop held on 14/02 2014. This Workshop was run by the PSC PM and was attended by a wide audience comprising workgroup representatives from the core team, Clinical staff, and the PSCP and their design team, which fed Risks from each sub group into the Master Register.
The risk register continues to be reviewed and updated. The latest Risk Register is attached as Appendix 04.
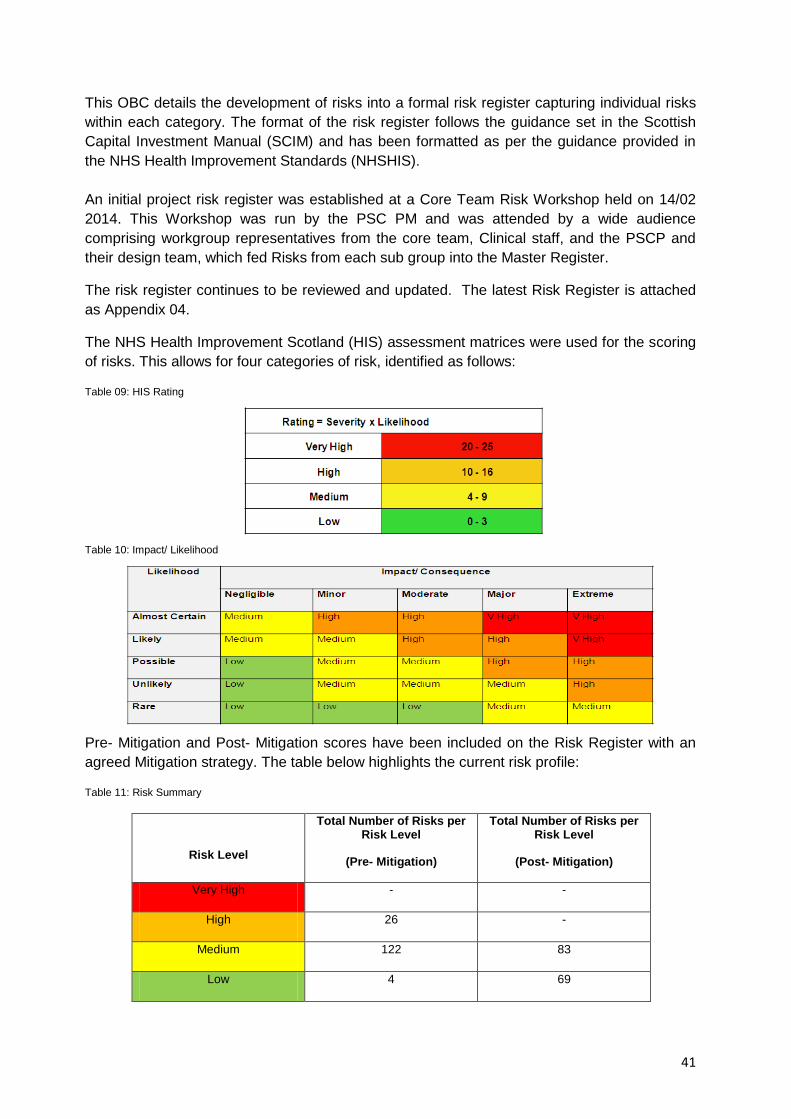
The NHS Health Improvement Scotland (HIS) assessment matrices were used for the scoring of risks. This allows for four categories of risk, identified as follows:
Table 09: HIS Rating
Table 10: Impact/ Likelihood
Pre- Mitigation and Post- Mitigation scores have been included on the Risk Register with an agreed Mitigation strategy. The table below highlights the current risk profile:
Table 11: Risk Summary
Risk Level
Total Number of Risks per Risk Level
(Pre- Mitigation)
Total Number of Risks per Risk Level
(Post- Mitigation)
Very High - -
High 26 -
Medium 122 83
Low 4 69
42
Further details on the approach to Risk Management moving forward towards FBC are documented within Section 3.8 Risk Assessment and Section 6.6 Risk Management.
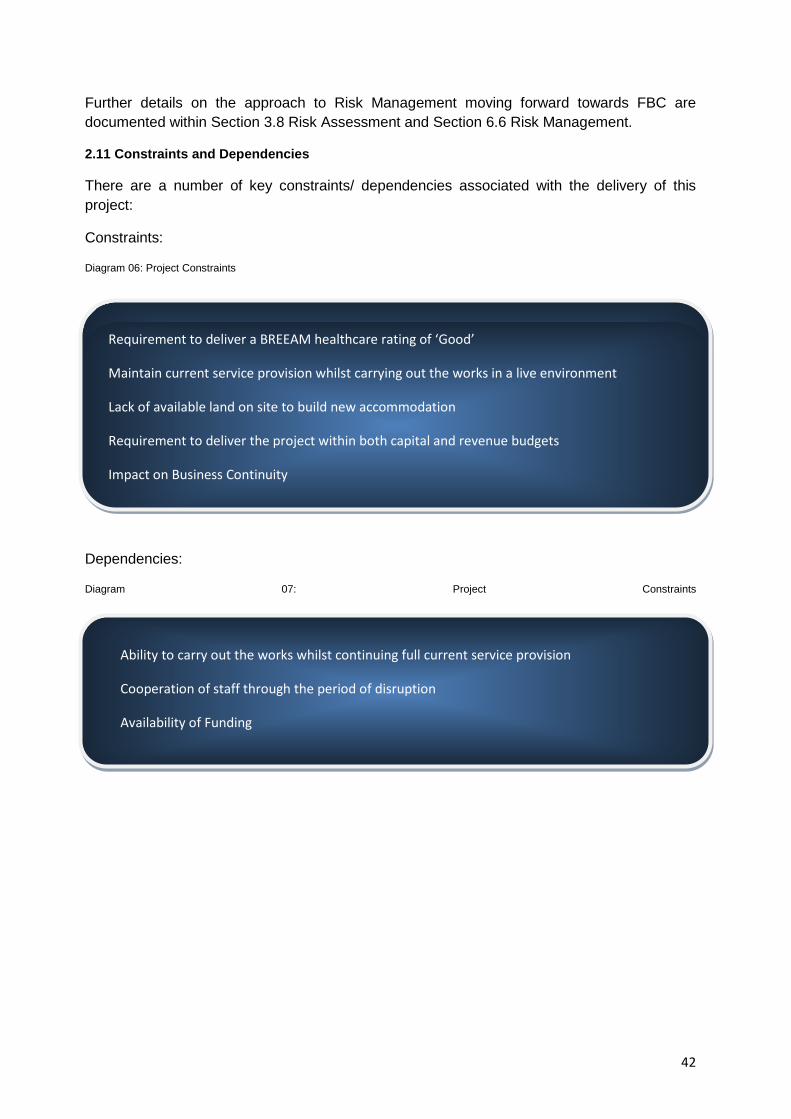
2.11 Constraints and Dependencies
There are a number of key constraints/ dependencies associated with the delivery of this project:
Constraints:
Diagram 06: Project Constraints
Dependencies:
Diagram 07: Project Constraints
Requirement to deliver a BREEAM healthcare rating of ‘Good’
Maintain current service provision whilst carrying out the works in a live environment
Lack of available land on site to build new accommodation
Requirement to deliver the project within both capital and revenue budgets
Impact on Business Continuity
Ability to carry out the works whilst continuing full current service provision
Cooperation of staff through the period of disruption
Availability of Funding

43
3.0 The Economic Case
3.1 Introduction
In accordance with the Scottish Capital Investment Manual and the requirements of HM Treasury’s Green Book (A Guide to Appraisal in the Public Sector), this section of the OBC documents the process and provides evidence to show that the selection of the preferred option is derived from the most economically advantageous option whilst best meeting the service needs and optimising value for money.
The Economic Case sets out:
Critical Success Factors; Long Listed Options; Preferred Way Forward Short Listed Options; Economic Appraisal; Qualitative Benefits Appraisal; Risk Appraisal; Sensitivity Analysis; Preferred Option
44
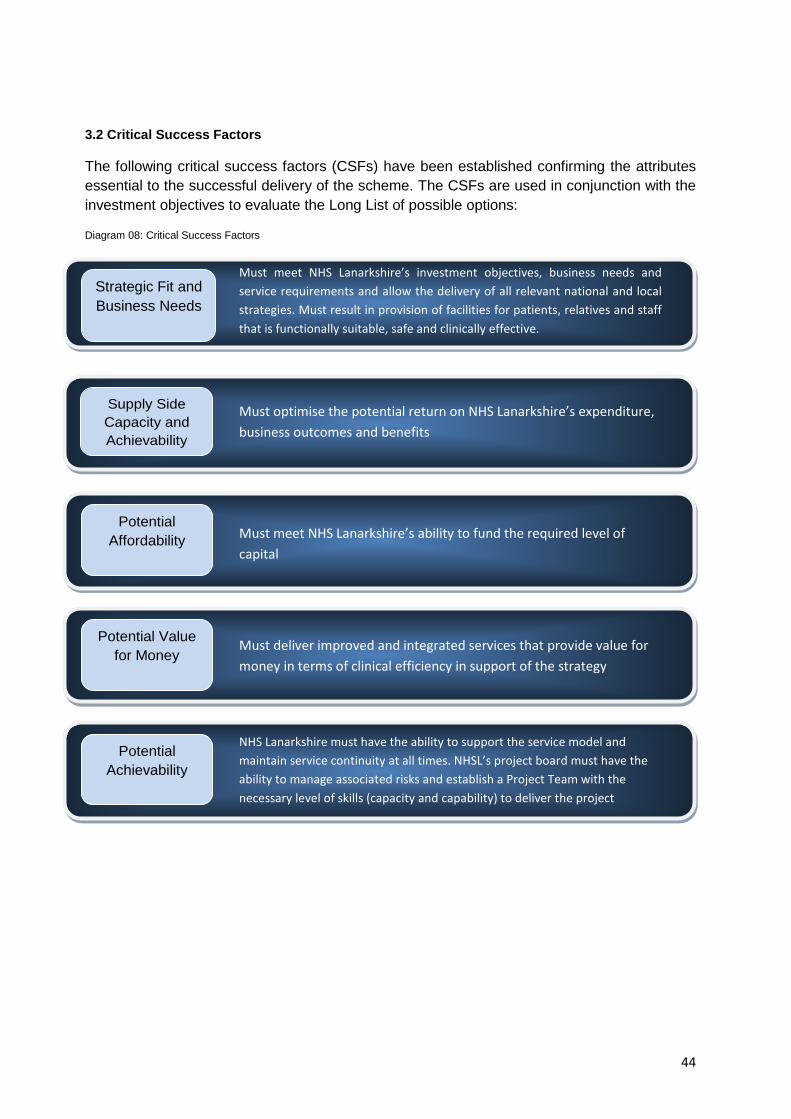
3.2 Critical Success Factors
The following critical success factors (CSFs) have been established confirming the attributes essential to the successful delivery of the scheme. The CSFs are used in conjunction with the investment objectives to evaluate the Long List of possible options:
Diagram 08: Critical Success Factors
Supply Side Capacity and Achievability
Potential Affordability
Potential Value for Money
Potential Achievability
Strategic Fit and Business Needs
Must meet NHS Lanarkshire’s investment objectives, business needs and service requirements and allow the delivery of all relevant national and local strategies. Must result in provision of facilities for patients, relatives and staff that is functionally suitable, safe and clinically effective.
Must optimise the potential return on NHS Lanarkshire’s expenditure, business outcomes and benefits
Must meet NHS Lanarkshire’s ability to fund the required level of capital
Must deliver improved and integrated services that provide value for money in terms of clinical efficiency in support of the strategy
NHS Lanarkshire must have the ability to support the service model and maintain service continuity at all times. NHSL’s project board must have the ability to manage associated risks and establish a Project Team with the necessary level of skills (capacity and capability) to deliver the project
45
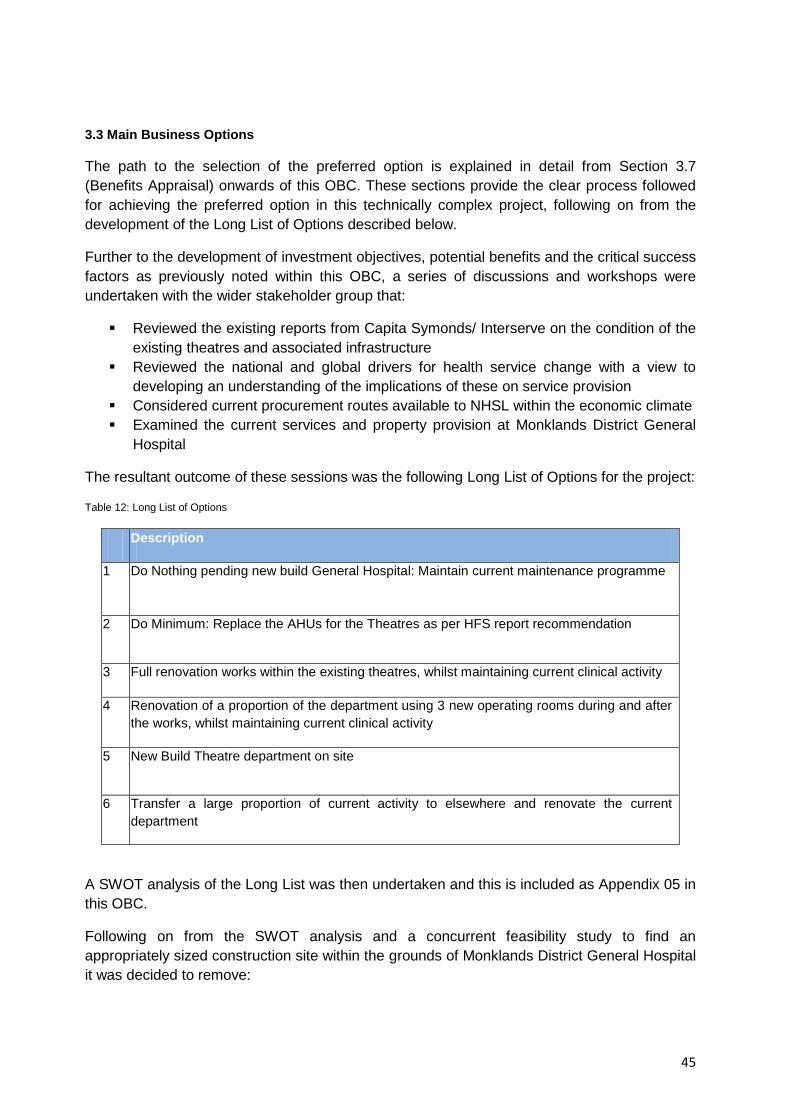
3.3 Main Business Options
The path to the selection of the preferred option is explained in detail from Section 3.7 (Benefits Appraisal) onwards of this OBC. These sections provide the clear process followed for achieving the preferred option in this technically complex project, following on from the development of the Long List of Options described below.
Further to the development of investment objectives, potential benefits and the critical success factors as previously noted within this OBC, a series of discussions and workshops were undertaken with the wider stakeholder group that:
Reviewed the existing reports from Capita Symonds/ Interserve on the condition of the existing theatres and associated infrastructure
Reviewed the national and global drivers for health service change with a view to developing an understanding of the implications of these on service provision
Considered current procurement routes available to NHSL within the economic climate Examined the current services and property provision at Monklands District General
Hospital
The resultant outcome of these sessions was the following Long List of Options for the project:
Table 12: Long List of Options
Description
1 Do Nothing pending new build General Hospital: Maintain current maintenance programme
2 Do Minimum: Replace the AHUs for the Theatres as per HFS report recommendation
3 Full renovation works within the existing theatres, whilst maintaining current clinical activity
4 Renovation of a proportion of the department using 3 new operating rooms during and after the works, whilst maintaining current clinical activity
5 New Build Theatre department on site
6 Transfer a large proportion of current activity to elsewhere and renovate the current department
A SWOT analysis of the Long List was then undertaken and this is included as Appendix 05 in this OBC.
Following on from the SWOT analysis and a concurrent feasibility study to find an appropriately sized construction site within the grounds of Monklands District General Hospital it was decided to remove:
46
Option 1 as it will not address the issues currently identified within what would be considered an appropriate timescale:
Air Handling Units (AHUs) not providing air pressure differentials to current building standards which poses a theoretical risk of cross infection between clean and dirty areas.
AHUs are now 35 years old with a heightened risk of component failure which in turn poses an operational risk to business continuity.
And:
Option 5 due to the lack of availability of space within the current site to construct a new theatre block
3.4 Preferred Way Forward
In preparing the OBC all appropriate funding and procurement options have been considered including NPD. The indicative construction costs are identified as circa £15m. As detailed in SCIM, the minimum level for considering whether projects are suitable for NPD is £20m. Consequently, the guidance contained within SCIM has been followed i.e. the default procurement route for acute construction projects not suitable for NPD is Frameworks Scotland 2.
The preferred way forward is therefore to proceed under Frameworks Scotland 2 and to investigate the Short List of Options for the project highlighted in section 3.4 of this document.
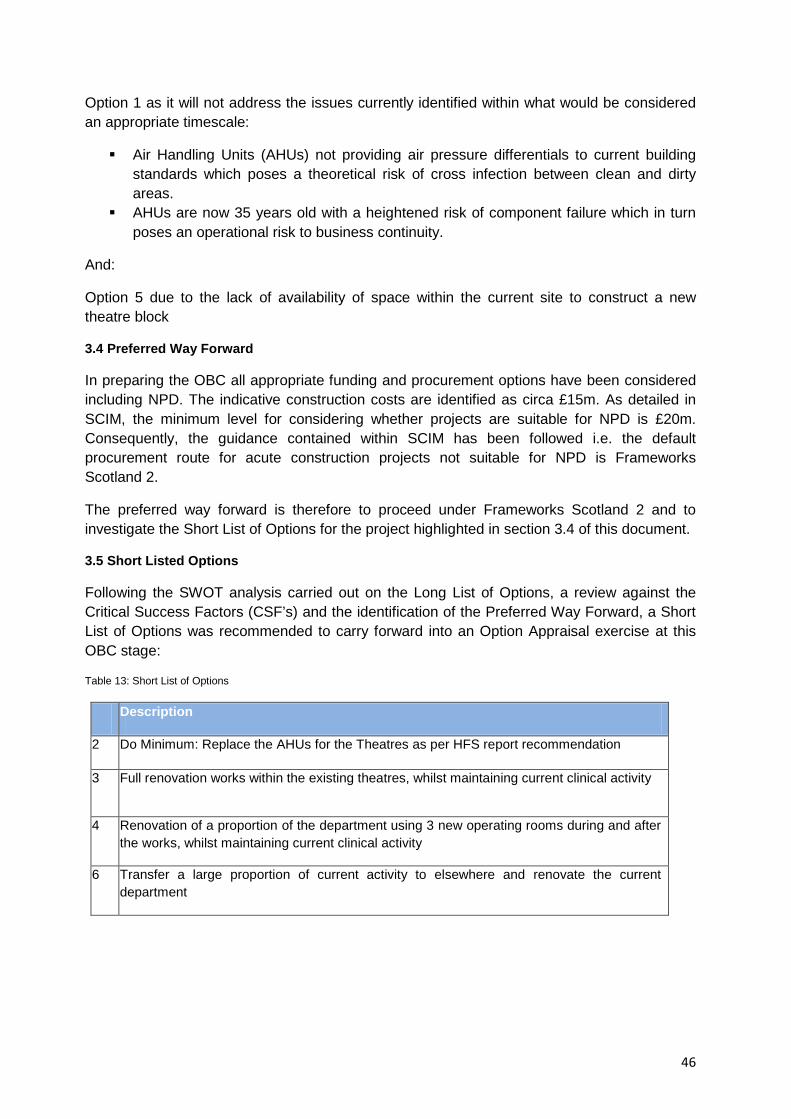
3.5 Short Listed Options
Following the SWOT analysis carried out on the Long List of Options, a review against the Critical Success Factors (CSF’s) and the identification of the Preferred Way Forward, a Short List of Options was recommended to carry forward into an Option Appraisal exercise at this OBC stage:
Table 13: Short List of Options
Description
2 Do Minimum: Replace the AHUs for the Theatres as per HFS report recommendation
3 Full renovation works within the existing theatres, whilst maintaining current clinical activity
4 Renovation of a proportion of the department using 3 new operating rooms during and after the works, whilst maintaining current clinical activity
6 Transfer a large proportion of current activity to elsewhere and renovate the current department
47
3.6 NPC/ NPV Findings
This section presents the economic appraisal of the shortlisted options and incorporates key elements of the Capital and Revenue implications of each which have been assessed over the anticipated life of the project and discounted to derive a Net Present Cost (NPC) for each viable option.
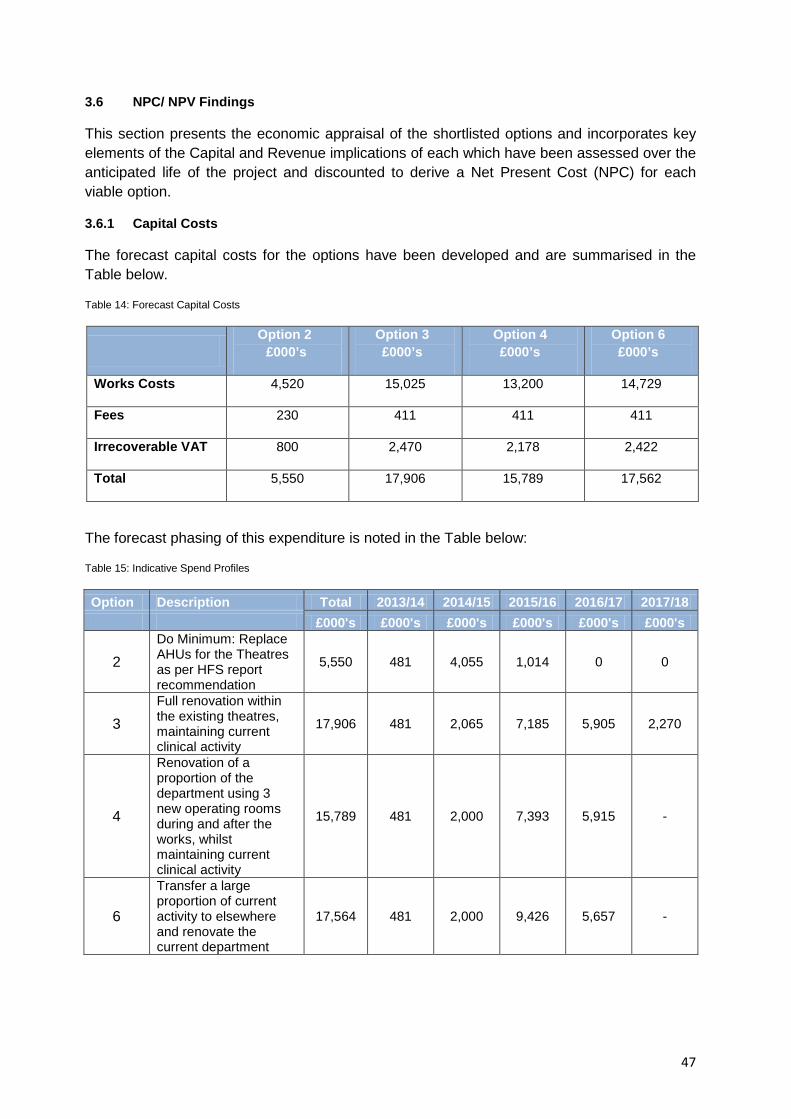
3.6.1 Capital Costs
The forecast capital costs for the options have been developed and are summarised in the Table below.
Table 14: Forecast Capital Costs
Option 2 £000’s
Option 3 £000’s
Option 4 £000’s
Option 6 £000’s
Works Costs 4,520 15,025 13,200 14,729
Fees 230 411 411 411
Irrecoverable VAT 800 2,470 2,178 2,422
Total 5,550 17,906 15,789 17,562
The forecast phasing of this expenditure is noted in the Table below:
Table 15: Indicative Spend Profiles
Option Description Total 2013/14 2014/15 2015/16 2016/17 2017/18 £000's £000's £000's £000's £000's £000's
2 Do Minimum: Replace AHUs for the Theatres as per HFS report recommendation
5,550 481 4,055 1,014 0 0
3 Full renovation within the existing theatres, maintaining current clinical activity
17,906 481 2,065 7,185 5,905 2,270
4
Renovation of a proportion of the department using 3 new operating rooms during and after the works, whilst maintaining current clinical activity
15,789 481 2,000 7,393 5,915 -
6
Transfer a large proportion of current activity to elsewhere and renovate the current department
17,564 481 2,000 9,426 5,657 -
48
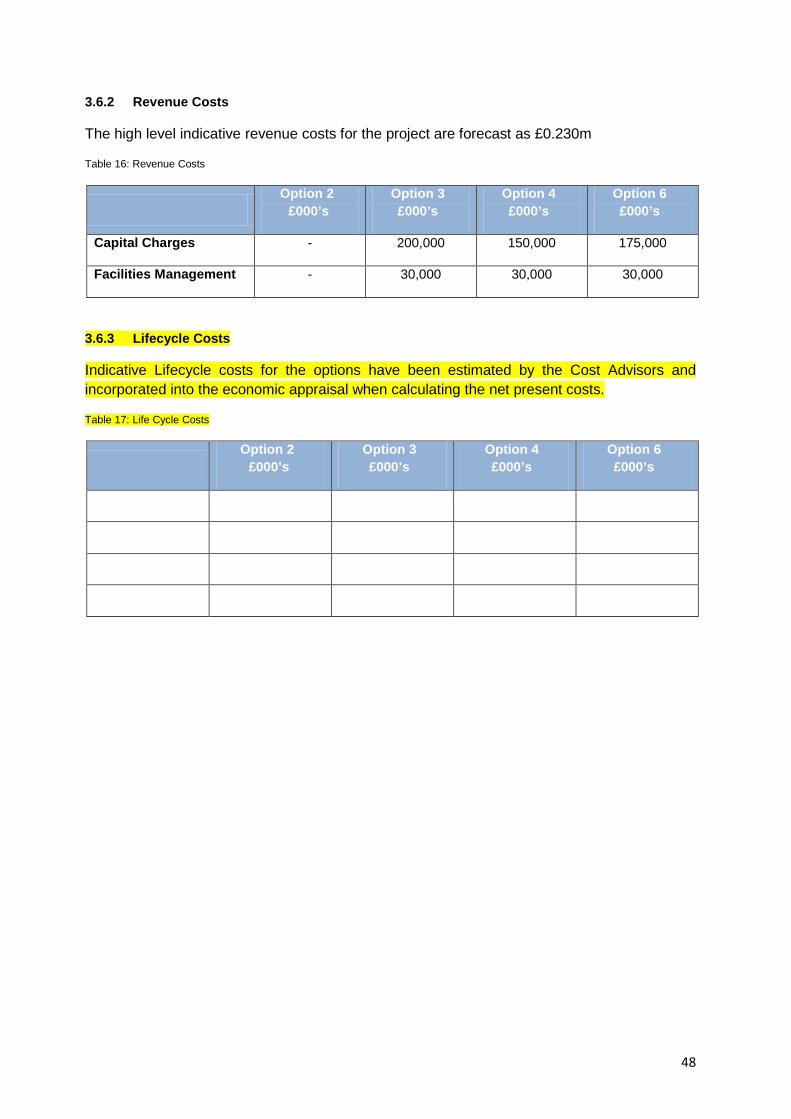
3.6.2 Revenue Costs
The high level indicative revenue costs for the project are forecast as £0.230m
Table 16: Revenue Costs
Option 2 £000’s
Option 3 £000’s
Option 4 £000’s
Option 6 £000’s
Capital Charges - 200,000 150,000 175,000
Facilities Management - 30,000 30,000 30,000
3.6.3 Lifecycle Costs
Indicative Lifecycle costs for the options have been estimated by the Cost Advisors and incorporated into the economic appraisal when calculating the net present costs.
Table 17: Life Cycle Costs
Option 2 £000’s
Option 3 £000’s
Option 4 £000’s
Option 6 £000’s
49
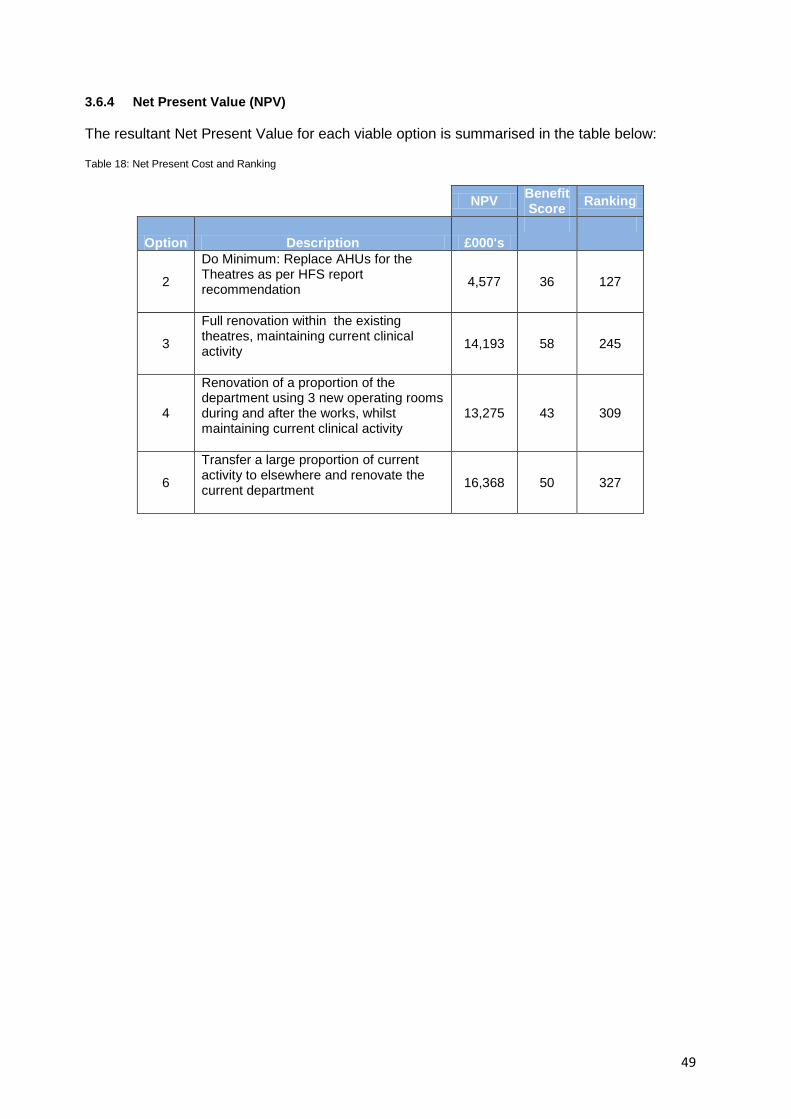
3.6.4 Net Present Value (NPV)
The resultant Net Present Value for each viable option is summarised in the table below:
Table 18: Net Present Cost and Ranking
NPV Benefit Score Ranking
Option Description £000's
2
Do Minimum: Replace AHUs for the Theatres as per HFS report recommendation
4,577 36 127
3
Full renovation within the existing theatres, maintaining current clinical activity
14,193 58 245
4
Renovation of a proportion of the department using 3 new operating rooms during and after the works, whilst maintaining current clinical activity
13,275 43 309
6
Transfer a large proportion of current activity to elsewhere and renovate the current department
16,368
50 327
50
3.7 Benefits Appraisal
A Non- Financial Benefits Appraisal Workshop was undertaken on 12th September 2012 to explore and examine the short list of options and to inform the development of the preferred option for the project. A group of stakeholders comprising clinical departmental staff, operational staff and representatives from the PSCP and their design team was present to ensure a consistency of approach and appropriate technical input was available. This Workshop took the form of a scoring exercise against the set of benefits criteria established in section 2.9 of this Outline Business Case. The Options appraised were: Diagram 09: Short List of Options
3.7.1 The Workshop
The Workshop began with an introduction to establish the outline for the session and key elements for consideration.
There was then a short presentation to refresh key project elements for the audience prior to moving to the scoring process.
Do Minimum: Replace the AHU’s for the Theatres as per HFS report
recommendation Full renovation works within the existing theatres, whilst maintaining current
clinical activity Renovation of a proportion of the department using 3 new operating rooms
during and after the works, whilst maintaining current clinical activity Transfer a large proportion of current activity to elsewhere and renovate the
current department
51
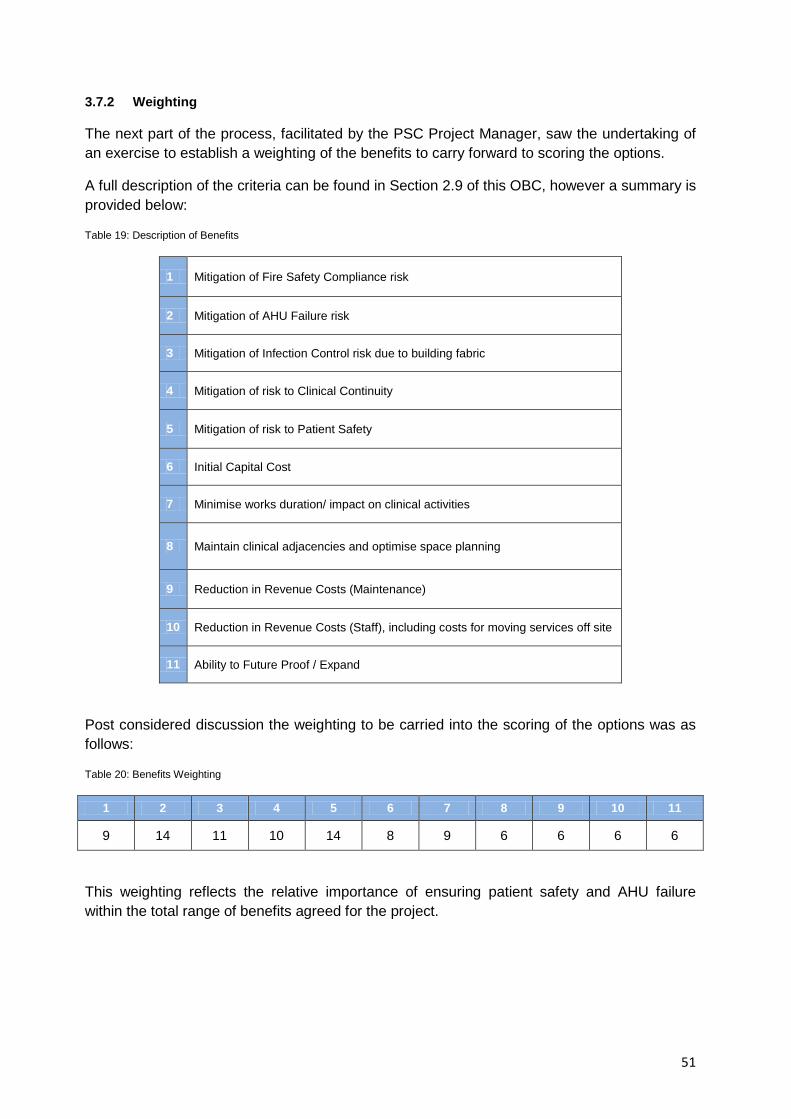
3.7.2 Weighting
The next part of the process, facilitated by the PSC Project Manager, saw the undertaking of an exercise to establish a weighting of the benefits to carry forward to scoring the options.
A full description of the criteria can be found in Section 2.9 of this OBC, however a summary is provided below:
Table 19: Description of Benefits
1 Mitigation of Fire Safety Compliance risk
2 Mitigation of AHU Failure risk
3 Mitigation of Infection Control risk due to building fabric
4 Mitigation of risk to Clinical Continuity
5 Mitigation of risk to Patient Safety
6 Initial Capital Cost
7 Minimise works duration/ impact on clinical activities
8 Maintain clinical adjacencies and optimise space planning
9 Reduction in Revenue Costs (Maintenance)
10 Reduction in Revenue Costs (Staff), including costs for moving services off site
11 Ability to Future Proof / Expand
Post considered discussion the weighting to be carried into the scoring of the options was as follows:
Table 20: Benefits Weighting
1 2 3 4 5 6 7 8 9 10 11
9 14 11 10 14 8 9 6 6 6 6
This weighting reflects the relative importance of ensuring patient safety and AHU failure within the total range of benefits agreed for the project.
52
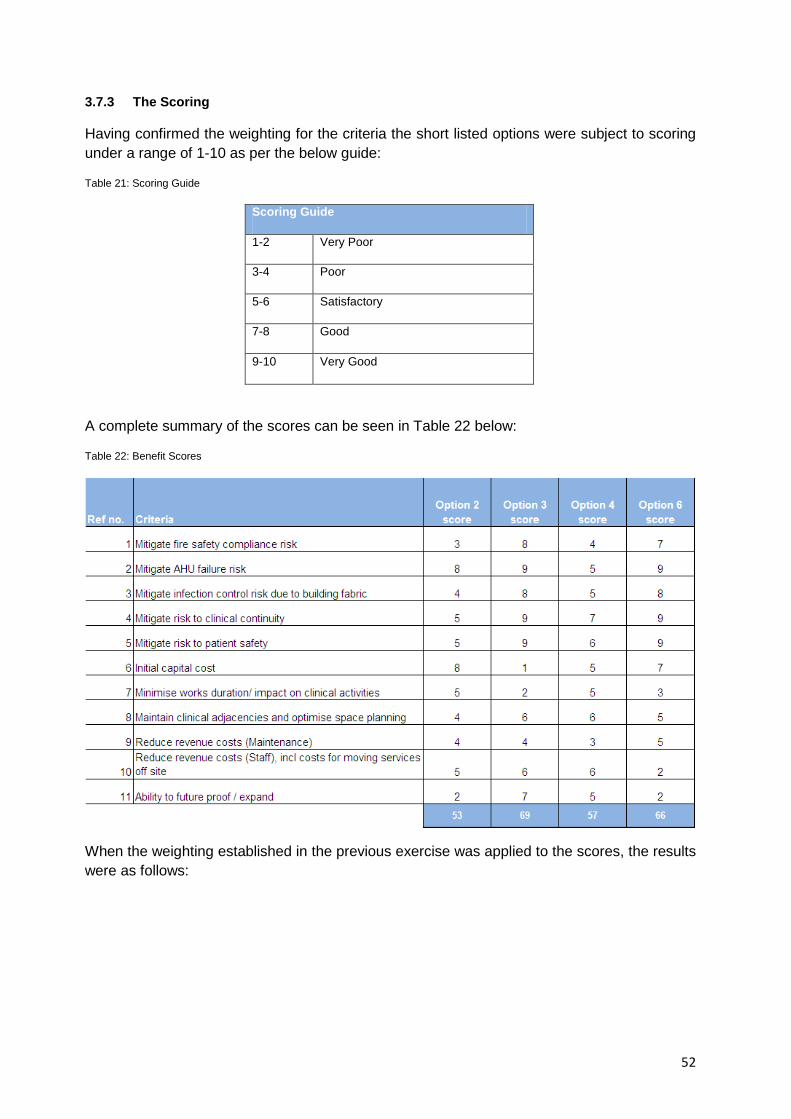
3.7.3 The Scoring
Having confirmed the weighting for the criteria the short listed options were subject to scoring under a range of 1-10 as per the below guide:
Table 21: Scoring Guide
Scoring Guide
1-2 Very Poor
3-4 Poor
5-6 Satisfactory
7-8 Good
9-10 Very Good
A complete summary of the scores can be seen in Table 22 below:
Table 22: Benefit Scores
When the weighting established in the previous exercise was applied to the scores, the results were as follows:
53
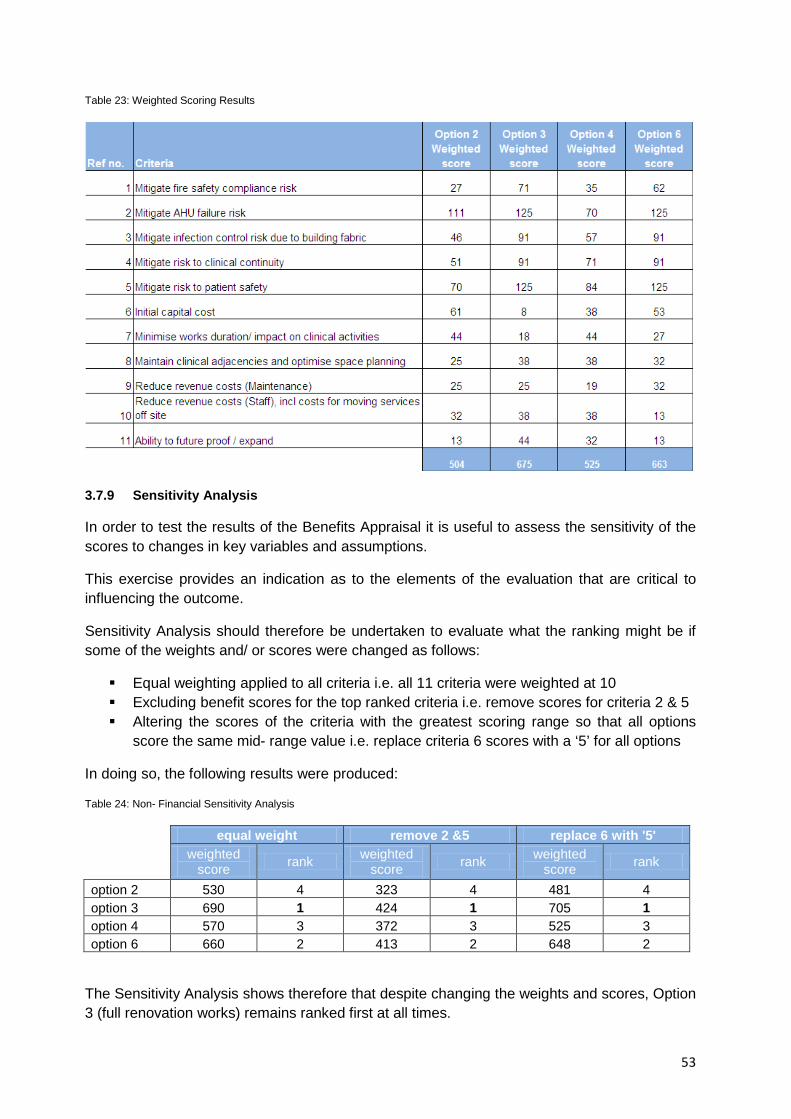
Table 23: Weighted Scoring Results
3.7.9 Sensitivity Analysis
In order to test the results of the Benefits Appraisal it is useful to assess the sensitivity of the scores to changes in key variables and assumptions.
This exercise provides an indication as to the elements of the evaluation that are critical to influencing the outcome.
Sensitivity Analysis should therefore be undertaken to evaluate what the ranking might be if some of the weights and/ or scores were changed as follows:
Equal weighting applied to all criteria i.e. all 11 criteria were weighted at 10 Excluding benefit scores for the top ranked criteria i.e. remove scores for criteria 2 & 5 Altering the scores of the criteria with the greatest scoring range so that all options
score the same mid- range value i.e. replace criteria 6 scores with a ‘5’ for all options
In doing so, the following results were produced:
Table 24: Non- Financial Sensitivity Analysis
equal weight remove 2 &5 replace 6 with '5' weighted
score rank weighted score rank weighted
score rank option 2 530 4 323 4 481 4 option 3 690 1 424 1 705 1 option 4 570 3 372 3 525 3 option 6 660 2 413 2 648 2
The Sensitivity Analysis shows therefore that despite changing the weights and scores, Option 3 (full renovation works) remains ranked first at all times.
54
3.8 Risk Assessment
A full risk analysis was undertaken to identify and assess the impact of risks during the stages of the project. An initial project risk register was established at a Risk Workshop held on 14/02/2014.
The Register will continue to be updated and reviewed throughout the course of the project. The various workgroups will feed pertinent Risks in to the Master Register on a regular basis and Board Risk will also be captured and mitigated. An update on the very high risks will be discussed at the Core Group Meetings and the Project Board will be kept informed of the highest scoring risks via their Project Board Meeting.
Further details of the approach to Risk Management moving towards Full Business Case are documented within Section 2.10 and Section 6.6 of this OBC.
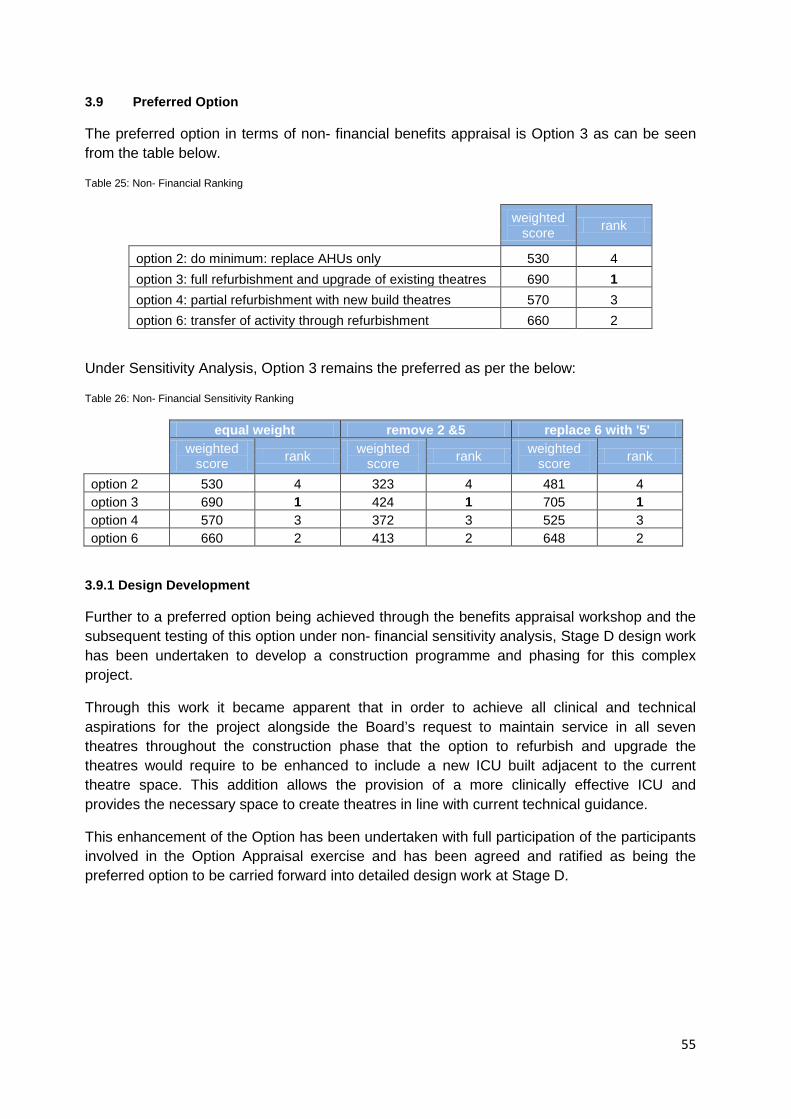
55
3.9 Preferred Option
The preferred option in terms of non- financial benefits appraisal is Option 3 as can be seen from the table below.
Table 25: Non- Financial Ranking
weighted score rank
option 2: do minimum: replace AHUs only 530 4 option 3: full refurbishment and upgrade of existing theatres 690 1 option 4: partial refurbishment with new build theatres 570 3 option 6: transfer of activity through refurbishment 660 2
Under Sensitivity Analysis, Option 3 remains the preferred as per the below:
Table 26: Non- Financial Sensitivity Ranking
equal weight remove 2 &5 replace 6 with '5' weighted
score rank weighted score rank weighted
score rank option 2 530 4 323 4 481 4 option 3 690 1 424 1 705 1 option 4 570 3 372 3 525 3 option 6 660 2 413 2 648 2
3.9.1 Design Development
Further to a preferred option being achieved through the benefits appraisal workshop and the subsequent testing of this option under non- financial sensitivity analysis, Stage D design work has been undertaken to develop a construction programme and phasing for this complex project.
Through this work it became apparent that in order to achieve all clinical and technical aspirations for the project alongside the Board’s request to maintain service in all seven theatres throughout the construction phase that the option to refurbish and upgrade the theatres would require to be enhanced to include a new ICU built adjacent to the current theatre space. This addition allows the provision of a more clinically effective ICU and provides the necessary space to create theatres in line with current technical guidance.
This enhancement of the Option has been undertaken with full participation of the participants involved in the Option Appraisal exercise and has been agreed and ratified as being the preferred option to be carried forward into detailed design work at Stage D.
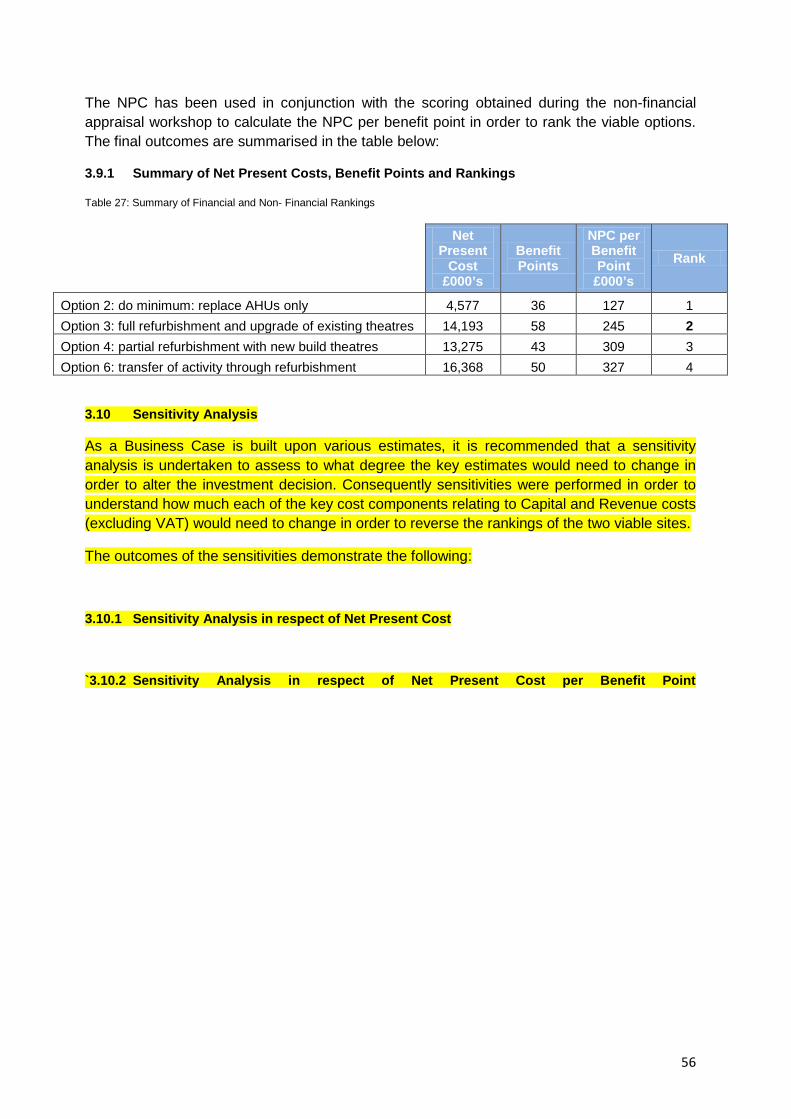
56
The NPC has been used in conjunction with the scoring obtained during the non-financial appraisal workshop to calculate the NPC per benefit point in order to rank the viable options. The final outcomes are summarised in the table below:
3.9.1 Summary of Net Present Costs, Benefit Points and Rankings
Table 27: Summary of Financial and Non- Financial Rankings
Net Present
Cost £000’s
Benefit Points
NPC per Benefit Point
£000’s Rank
Option 2: do minimum: replace AHUs only 4,577 36 127 1 Option 3: full refurbishment and upgrade of existing theatres 14,193 58 245 2 Option 4: partial refurbishment with new build theatres 13,275 43 309 3 Option 6: transfer of activity through refurbishment 16,368 50 327 4
3.10 Sensitivity Analysis
As a Business Case is built upon various estimates, it is recommended that a sensitivity analysis is undertaken to assess to what degree the key estimates would need to change in order to alter the investment decision. Consequently sensitivities were performed in order to understand how much each of the key cost components relating to Capital and Revenue costs (excluding VAT) would need to change in order to reverse the rankings of the two viable sites.
The outcomes of the sensitivities demonstrate the following:
3.10.1 Sensitivity Analysis in respect of Net Present Cost
`3.10.2 Sensitivity Analysis in respect of Net Present Cost per Benefit Point
57
4 The Commercial Case
4.1 Introduction
This section outlines the commercial transaction that the board will sign up to and will consider the following:
The scope of the services being contracted for The management and allocation of risk Potential charging mechanism Key contractual arrangements Personnel implications Implementation timescales Accountancy treatment
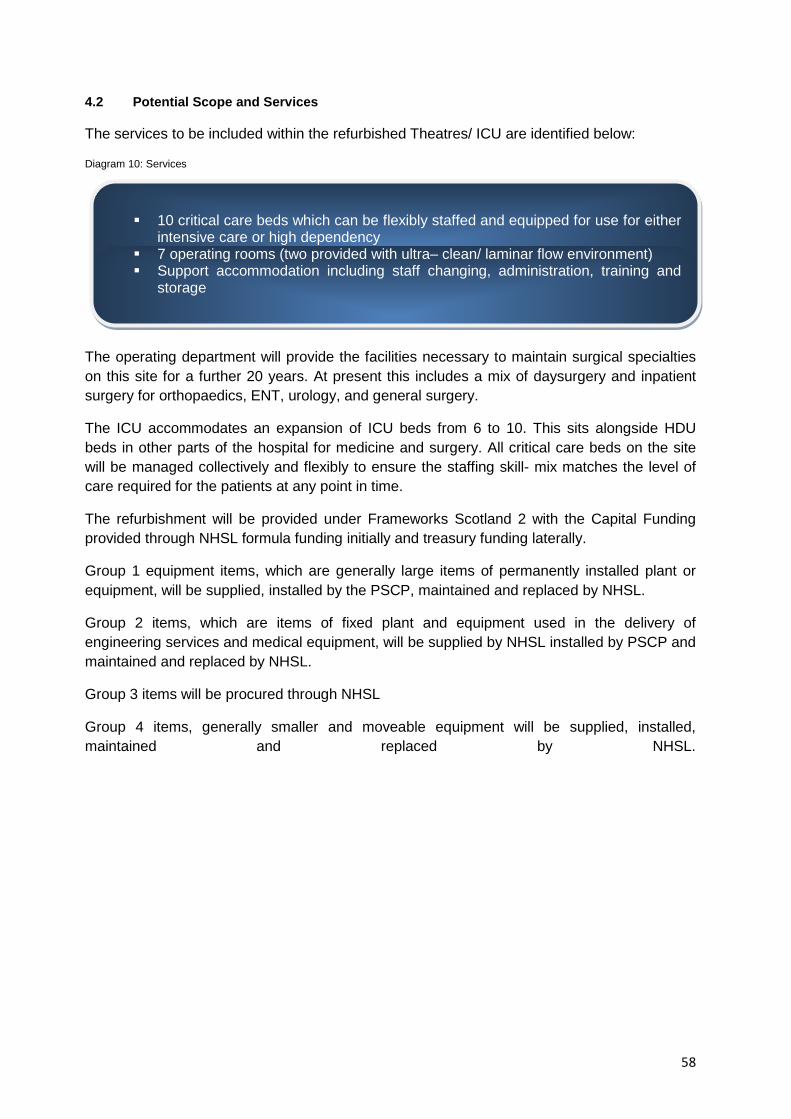
58
4.2 Potential Scope and Services
The services to be included within the refurbished Theatres/ ICU are identified below:
Diagram 10: Services
The operating department will provide the facilities necessary to maintain surgical specialties on this site for a further 20 years. At present this includes a mix of daysurgery and inpatient surgery for orthopaedics, ENT, urology, and general surgery.
The ICU accommodates an expansion of ICU beds from 6 to 10. This sits alongside HDU beds in other parts of the hospital for medicine and surgery. All critical care beds on the site will be managed collectively and flexibly to ensure the staffing skill- mix matches the level of care required for the patients at any point in time.
The refurbishment will be provided under Frameworks Scotland 2 with the Capital Funding provided through NHSL formula funding initially and treasury funding laterally.
Group 1 equipment items, which are generally large items of permanently installed plant or equipment, will be supplied, installed by the PSCP, maintained and replaced by NHSL.
Group 2 items, which are items of fixed plant and equipment used in the delivery of engineering services and medical equipment, will be supplied by NHSL installed by PSCP and maintained and replaced by NHSL.
Group 3 items will be procured through NHSL
Group 4 items, generally smaller and moveable equipment will be supplied, installed, maintained and replaced by NHSL.
10 critical care beds which can be flexibly staffed and equipped for use for either
intensive care or high dependency 7 operating rooms (two provided with ultra– clean/ laminar flow environment) Support accommodation including staff changing, administration, training and
storage
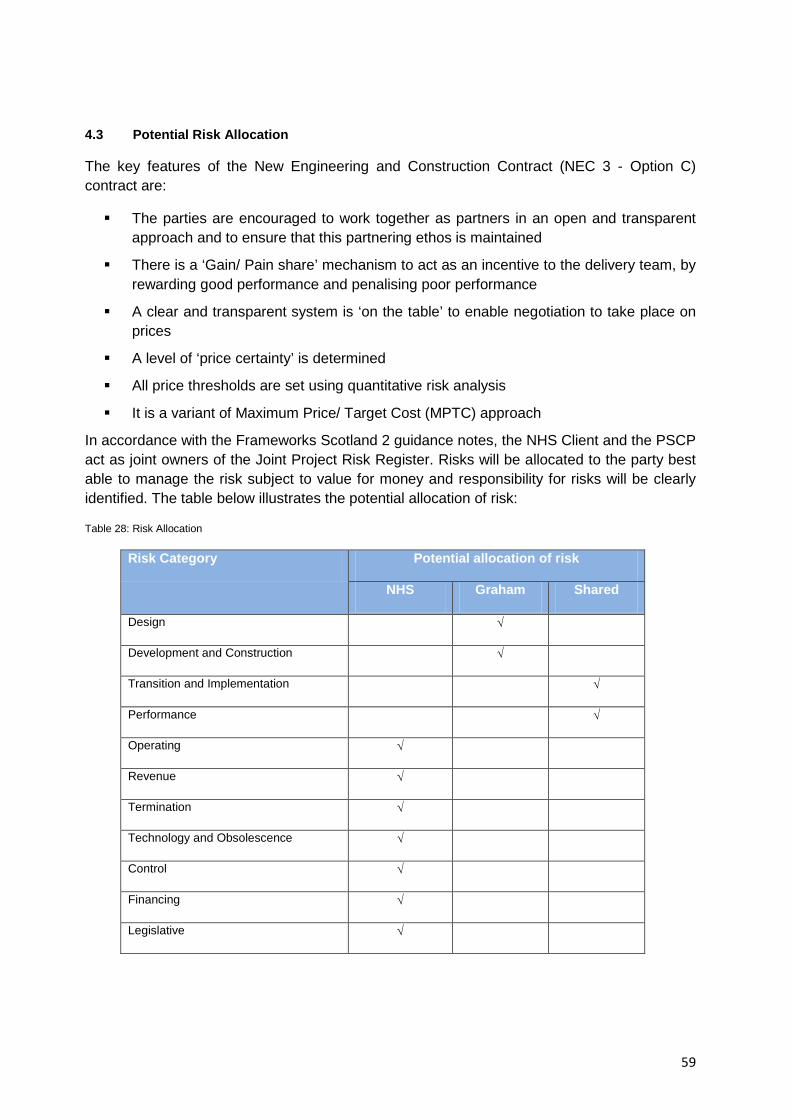
59
4.3 Potential Risk Allocation
The key features of the New Engineering and Construction Contract (NEC 3 - Option C) contract are:
The parties are encouraged to work together as partners in an open and transparent approach and to ensure that this partnering ethos is maintained
There is a ‘Gain/ Pain share’ mechanism to act as an incentive to the delivery team, by rewarding good performance and penalising poor performance
A clear and transparent system is ‘on the table’ to enable negotiation to take place on prices
A level of ‘price certainty’ is determined
All price thresholds are set using quantitative risk analysis
It is a variant of Maximum Price/ Target Cost (MPTC) approach
In accordance with the Frameworks Scotland 2 guidance notes, the NHS Client and the PSCP act as joint owners of the Joint Project Risk Register. Risks will be allocated to the party best able to manage the risk subject to value for money and responsibility for risks will be clearly identified. The table below illustrates the potential allocation of risk:
Table 28: Risk Allocation
Risk Category Potential allocation of risk
NHS Graham Shared
Design √
Development and Construction √
Transition and Implementation √
Performance √
Operating √
Revenue √
Termination √
Technology and Obsolescence √
Control √
Financing √
Legislative √
60
4.4 Agreed Charging Mechanisms
This project is being procured through HFS framework Scotland 2 with design being led by the PSCP and their design team. As such there is no concession period and so no charging mechanism applied.
The PSCP shall design & build the project and upon completion hand the building over to the client (NHSL) to manage and operate the facility.
It is worth noting that during the design & construction process cognisance shall be given to the whole life costs of the facility in order that the project achieves value for money. The PSCP is also incentivised through the use of a target cost contract NEC3 Option C for Stage 2, which promotes that the PSCP look for efficiencies when carrying out the project.
4.5 Agreed Key Contractual Arrangements
The preferred solution is being procured under Frameworks Scotland 2. This framework is founded on collaborative working and the NEC3 form of contract is used to support these principles.
Following the SGHSCD’s methodology for tendering work through the new Framework for Scotland 2, Graham Construction has been appointed as Principal Supply Chain Partner (PSCP) to work with the Board to finalise design, work up the target cost for the scheme and to construct the building.
Graham Construction has been appointed to deliver multiple works task orders for NHS Lanarkshire under the new Health Facilities Overarching Scheme Contract. The Theatres/ ICU work task order is the largest and most complex project currently being delivered under the scheme
As noted above, the mechanism for ensuring that this partnership ethos is carried through to the construction of the new facility is through the use of the NEC3 form of contract. The main principles of this procurement methodology are outlined below:
4.5.1 The Priced Contract – Stage 1B Preconstruction Activity - Designing a Solution The priced contract for the Preconstruction Activity, designing a solution is fixed priced during Stage 1B and before construction is commenced (Stage 2). During Stage 1B the PSCP must deliver a design solution for a priced contract sum NEC Option A. Once agreed the priced contract sum for this stage, my only be revised upward or downward when compensation events occur under the scheme contract. Any estimated costs included within the priced contract sum must be understood together with the potential risks to the project and how they may be removed/ managed.
The likely cost consequences and the occurrence of risks that are considered likely to occur will be discussed with a view to agreeing an appropriate contingency in either the priced

61
contract sum (if the PSCP is responsible for the risk) or in NHS Lanarkshire’s Budget (if NHS Lanarkshire is responsible for the risk).
The level of information that the PSCP requires to provide in support of the priced contract with activity schedule for monthly applications for payment will be agreed with the Cost Advisor.
The PSCP will provide a fully detailed priced activity schedule breakdown with their application for payment which will be verified by the Cost Advisor.
The objective is to work together to agree the completion of each activity as detailed within the priced contract activity schedule, any risk allowances; and the percentage fee (overheads and profit) applied to such sums.
The aim underpinning this approach is to reduce costs by understanding the risks that make it higher and managing/ removing those risks and at the same time seeking to plan the services/ works provided by the PSCP and its SCMs so that the Stage will be more effectively carried out.
4.5.2 Open Book Philosophy - Stage 2 Construction – Target Contract with Activity Schedule The target contract for construction following completion of the design, is a target price with activity schedule during Stage 2 construction NEC3 Option C. A key principle of the NEC3 Option C contract is the payment of ‘Defined Cost’ and an open book accounting philosophy. These require a robust, reliable and transparent system to record staff time and manage the invoicing process. This allows the Cost Advisor not only to identify costs but also to establish that the costs have been properly expended on the project and that they are allowable under the NEC3 Option C contract as defined under the “schedule of cost components”. Project costs must be referenced to items on the activity schedules with detail added against 5 main headings of; labour, plant, materials, sub contractors and preliminaries. Orders, deliveries, invoices for payment, external plant hires and sub-contracts also have to be cross-checked against Goods Received Notes.
The PSCP will be required to demonstrate that market testing has occurred at Stage 2 in the order of 80% of the priced contract sum.
The target price is key to the cost operation of the contract and is set during the pre-construction phase. This process concludes when the PSCP’s proposals are completed for costing and the risk register has been agreed. The target price costing is made up of the following elements:
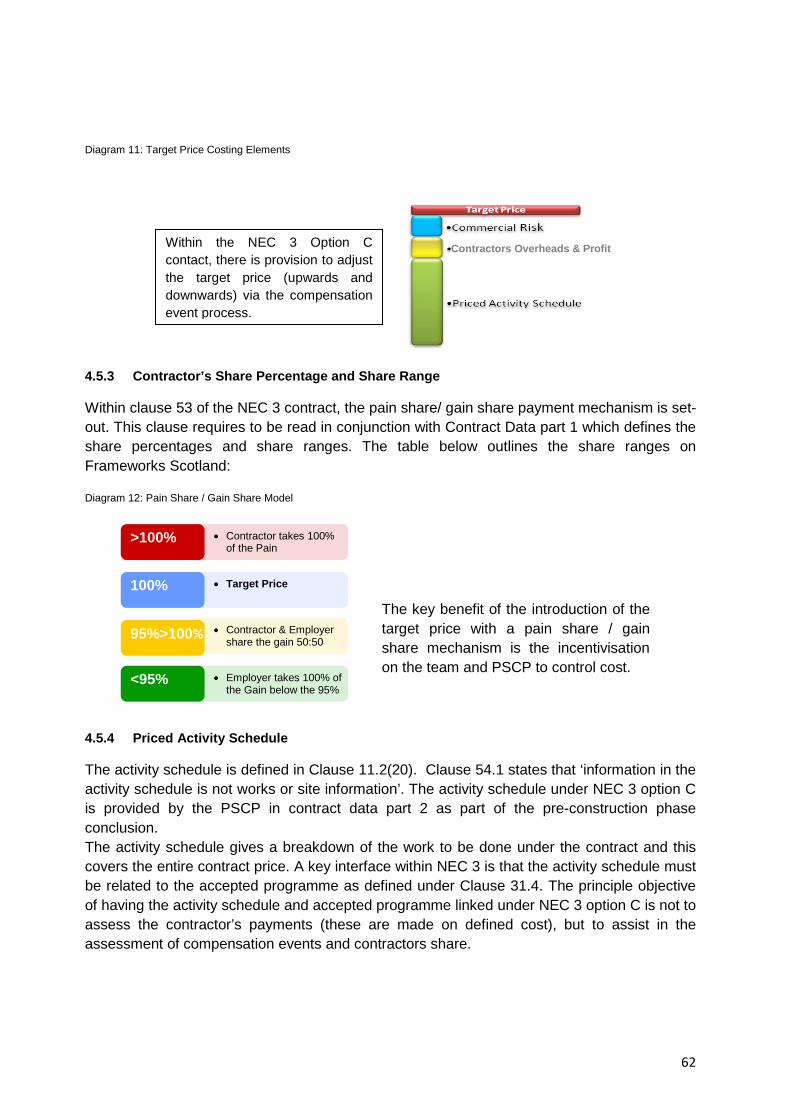
62
Diagram 11: Target Price Costing Elements
4.5.3 Contractor’s Share Percentage and Share Range Within clause 53 of the NEC 3 contract, the pain share/ gain share payment mechanism is set-out. This clause requires to be read in conjunction with Contract Data part 1 which defines the share percentages and share ranges. The table below outlines the share ranges on Frameworks Scotland: Diagram 12: Pain Share / Gain Share Model
4.5.4 Priced Activity Schedule The activity schedule is defined in Clause 11.2(20). Clause 54.1 states that ‘information in the activity schedule is not works or site information’. The activity schedule under NEC 3 option C is provided by the PSCP in contract data part 2 as part of the pre-construction phase conclusion. The activity schedule gives a breakdown of the work to be done under the contract and this covers the entire contract price. A key interface within NEC 3 is that the activity schedule must be related to the accepted programme as defined under Clause 31.4. The principle objective of having the activity schedule and accepted programme linked under NEC 3 option C is not to assess the contractor’s payments (these are made on defined cost), but to assist in the assessment of compensation events and contractors share.
>100%
100%
95%>100%
<95%
• Contractor takes 100% of the Pain
• Target Price
• Contractor & Employer share the gain 50:50
• Employer takes 100% of the Gain below the 95%
The key benefit of the introduction of the target price with a pain share / gain share mechanism is the incentivisation on the team and PSCP to control cost.
Contractors Overheads & Profit Within the NEC 3 Option C contact, there is provision to adjust the target price (upwards and downwards) via the compensation event process.
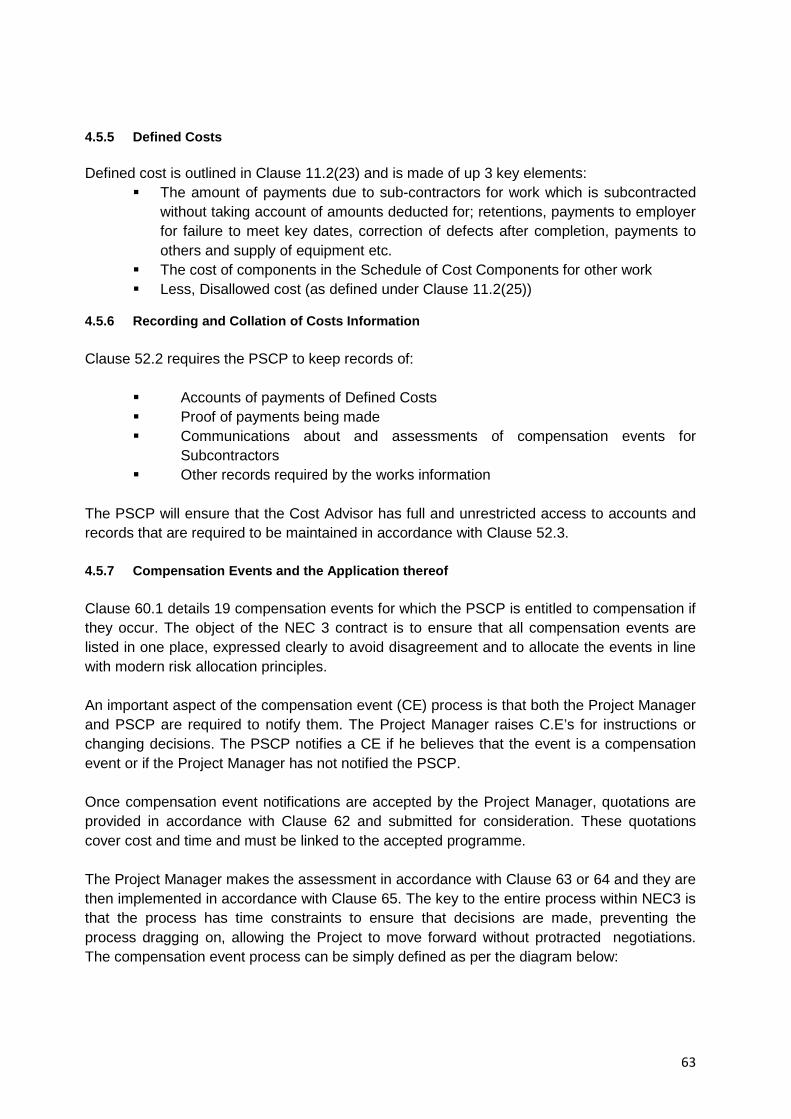
63
4.5.5 Defined Costs Defined cost is outlined in Clause 11.2(23) and is made of up 3 key elements:
The amount of payments due to sub-contractors for work which is subcontracted without taking account of amounts deducted for; retentions, payments to employer for failure to meet key dates, correction of defects after completion, payments to others and supply of equipment etc.
The cost of components in the Schedule of Cost Components for other work Less, Disallowed cost (as defined under Clause 11.2(25))
4.5.6 Recording and Collation of Costs Information Clause 52.2 requires the PSCP to keep records of:
Accounts of payments of Defined Costs Proof of payments being made Communications about and assessments of compensation events for
Subcontractors Other records required by the works information
The PSCP will ensure that the Cost Advisor has full and unrestricted access to accounts and records that are required to be maintained in accordance with Clause 52.3. 4.5.7 Compensation Events and the Application thereof Clause 60.1 details 19 compensation events for which the PSCP is entitled to compensation if they occur. The object of the NEC 3 contract is to ensure that all compensation events are listed in one place, expressed clearly to avoid disagreement and to allocate the events in line with modern risk allocation principles. An important aspect of the compensation event (CE) process is that both the Project Manager and PSCP are required to notify them. The Project Manager raises C.E’s for instructions or changing decisions. The PSCP notifies a CE if he believes that the event is a compensation event or if the Project Manager has not notified the PSCP. Once compensation event notifications are accepted by the Project Manager, quotations are provided in accordance with Clause 62 and submitted for consideration. These quotations cover cost and time and must be linked to the accepted programme. The Project Manager makes the assessment in accordance with Clause 63 or 64 and they are then implemented in accordance with Clause 65. The key to the entire process within NEC3 is that the process has time constraints to ensure that decisions are made, preventing the process dragging on, allowing the Project to move forward without protracted negotiations. The compensation event process can be simply defined as per the diagram below:

64
Diagram 13: Compensation Event Sequence

65
4.6 Potential Personnel Implications
There is no major impact for staff with regard to terms and conditions as a result of the refurbishment and new build work. Some working practices will change by the time the refurbishment is complete but this is work already in progress and not as a direct result of the project. The change in flow of both HDU and theatre patients provided by the project will not only facilitate a better patient experience and a higher standard of care but also a greatly improved working environment for staff. The Intensive Care Unit (ward 26) and surgical High Dependency Unit (ward 5) as previously noted in this OBC currently occupy two separate locations within Monklands General Hospital however they are managed as one unit with staff rotating between both. The plan to establish a combined unit will require a change in base ward for some staff. The remaining beds in the existing surgical HDU will revert to Level 1 which is already staffed by nurses with the appropriate training and skills. The proposed combined unit will comprise of 10 beds with a 6:4 split of ITU to HDU. However, the unit will be staffed to enable the beds to flex up and down between dependency levels in response to site demand. Nursing staff with the required skills are currently available to facilitate this but there is also an ongoing training programme for staff working in these areas to ensure all necessary skills are met. Within the existing units the access and discharge criteria are applied quite differently with medical staff fulfilling a gate keeping role. Consultant Intensivists manage both admissions and discharge to ITU beds. The General Surgeons currently agree access to surgical HDU but discharge is left to individual consultants with considerable input from nursing staff. Within a combined unit it is proposed that the Consultant Intensivists will assume the complete role for both ITU and HDU. This role change will provide a consistent standard of care to both Level 2 and 3 patients whilst ensuring efficient bed management. Historically within the theatre suite, staff were employed to work in either the recovery area or theatre. Over the last few years this policy has changed with nursing staff now employed as cover for the complete theatre suite. This ensures flexibility in staffing for both areas as well as the same day admission lounge which is run as part of theatres. A rotational programme is currently in place for all theatre staff and this is embedded within the staff rota therefore no staffing issues are expected as a result of the redesigned flow of patients through the theatre suite. The additional available work space will also create an improved and safer working environment for staff within ITU and Theatres. This will also further promote patient safety and there will be the opportunity to provide additional work based clinical training and education.
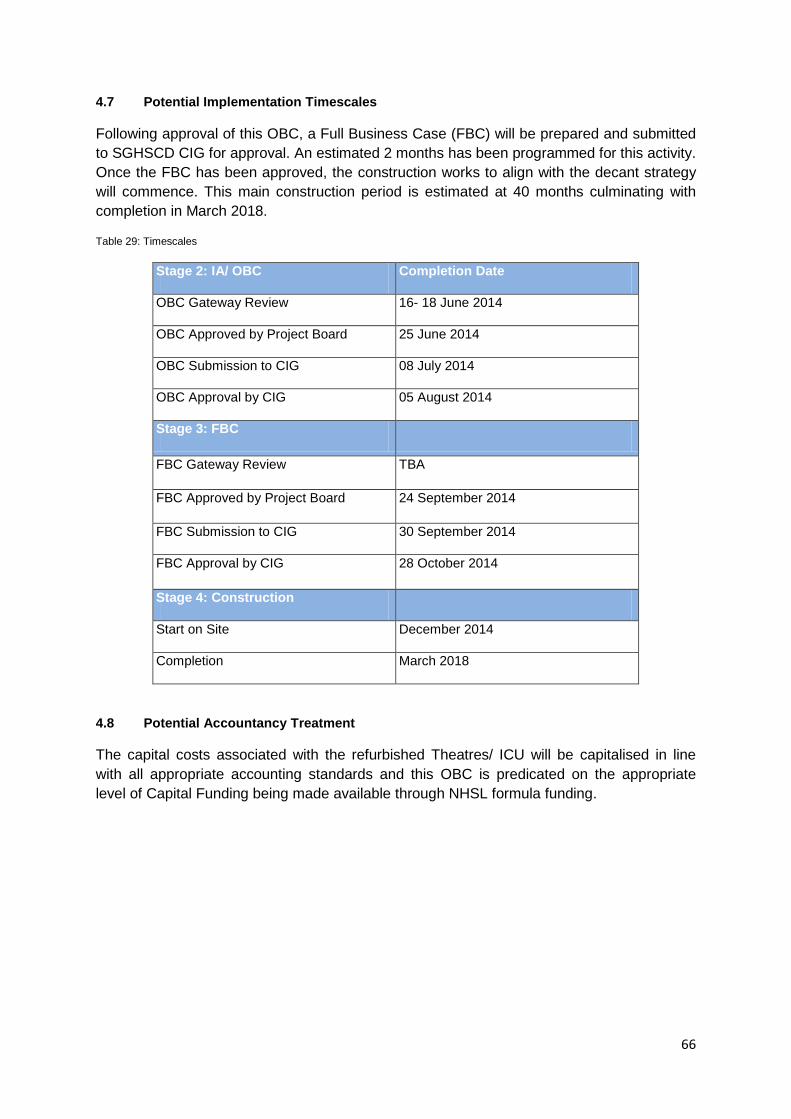
66
4.7 Potential Implementation Timescales
Following approval of this OBC, a Full Business Case (FBC) will be prepared and submitted to SGHSCD CIG for approval. An estimated 2 months has been programmed for this activity. Once the FBC has been approved, the construction works to align with the decant strategy will commence. This main construction period is estimated at 40 months culminating with completion in March 2018.
Table 29: Timescales
Stage 2: IA/ OBC Completion Date
OBC Gateway Review 16- 18 June 2014
OBC Approved by Project Board 25 June 2014
OBC Submission to CIG 08 July 2014
OBC Approval by CIG 05 August 2014
Stage 3: FBC
FBC Gateway Review TBA
FBC Approved by Project Board 24 September 2014
FBC Submission to CIG 30 September 2014
FBC Approval by CIG 28 October 2014
Stage 4: Construction
Start on Site December 2014
Completion March 2018
4.8 Potential Accountancy Treatment
The capital costs associated with the refurbished Theatres/ ICU will be capitalised in line with all appropriate accounting standards and this OBC is predicated on the appropriate level of Capital Funding being made available through NHSL formula funding.

67
5.0 The Financial Case
5.1 Introduction
The financial case for the preferred option sets out the following key features:
Potential Capital/ Funding Requirement; Potential Revenue Impact; Impact on Balance Sheet; Stakeholder Support; Overall Affordability
5.2 Potential Capital/ Funding Requirement
The potential capital costs and associated funding requirement are considered in greater detail in the following sections.
The capital costs for the preferred option are shown below and are derived from cost schedules produced by the Framework PSCP Graham Construction, in conjunction with the cost advisors Currie & Brown.
5.2.1 Capital Costs
The capital costs for the preferred option are shown below and are derived from cost schedules produced by the Framework 2 PSCP Graham Construction, in conjunction with the cost advisors Currie & Brown. The Capital Costs include contingencies and allowance for out of hours working to allow the project to be delivered while the theatres remain in use.
Table 30: Forecast Capital Costs for the Preferred Option
Total Cost
£000’s
Works Costs 15,025
Fees 411
Irrecoverable VAT 2,470
Total Capital Cost 17,906
The build costs represent the cost of construction in respect of a 7 theatre facility with a 10 bed ICU which adds 1,100m2 to the current footprint of the hospital.
The departments and areas are based on Schedule of Accommodation included as Appendix 06 in this OBC.
The estimated construction costs have been prepared by the Framework PSCP partners in conjunction with the Cost Advisors using the following assumptions and allowances:
The project is planned to commence construction in November 2014 with Clinical Service commencing in January 2018;
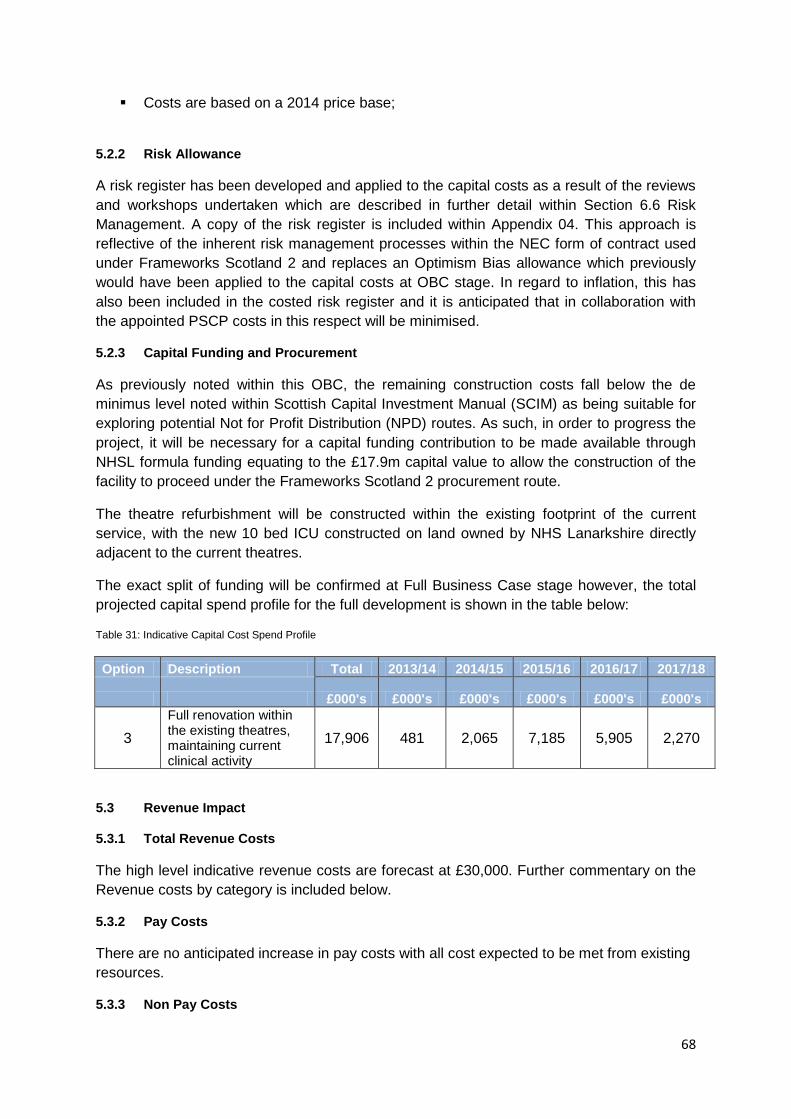
68
Costs are based on a 2014 price base;
5.2.2 Risk Allowance
A risk register has been developed and applied to the capital costs as a result of the reviews and workshops undertaken which are described in further detail within Section 6.6 Risk Management. A copy of the risk register is included within Appendix 04. This approach is reflective of the inherent risk management processes within the NEC form of contract used under Frameworks Scotland 2 and replaces an Optimism Bias allowance which previously would have been applied to the capital costs at OBC stage. In regard to inflation, this has also been included in the costed risk register and it is anticipated that in collaboration with the appointed PSCP costs in this respect will be minimised.
5.2.3 Capital Funding and Procurement
As previously noted within this OBC, the remaining construction costs fall below the de minimus level noted within Scottish Capital Investment Manual (SCIM) as being suitable for exploring potential Not for Profit Distribution (NPD) routes. As such, in order to progress the project, it will be necessary for a capital funding contribution to be made available through NHSL formula funding equating to the £17.9m capital value to allow the construction of the facility to proceed under the Frameworks Scotland 2 procurement route.
The theatre refurbishment will be constructed within the existing footprint of the current service, with the new 10 bed ICU constructed on land owned by NHS Lanarkshire directly adjacent to the current theatres.
The exact split of funding will be confirmed at Full Business Case stage however, the total projected capital spend profile for the full development is shown in the table below:
Table 31: Indicative Capital Cost Spend Profile
Option Description Total 2013/14 2014/15 2015/16 2016/17 2017/18
£000's £000's £000's £000's £000's £000's
3 Full renovation within the existing theatres, maintaining current clinical activity
17,906 481 2,065 7,185 5,905 2,270
5.3 Revenue Impact
5.3.1 Total Revenue Costs
The high level indicative revenue costs are forecast at £30,000. Further commentary on the Revenue costs by category is included below.
5.3.2 Pay Costs
There are no anticipated increase in pay costs with all cost expected to be met from existing resources.
5.3.3 Non Pay Costs

69
There will be a minor increase in facilities management costs as a result of the increase the 1,100 m2 of the footprint for the ITU. This has been estimated at £30,000, p.a.
5.3.4 Depreciation
For forecasting and appraisal purposes, the building depreciation has been calculated over 25 years. Following completion of the ICU it is anticipated that the new building will be valued by the appointed valuer at which time a building specific Assessed Life will be allocated.
5.3.5 Overall Recurring Revenue Costs
These costs represent the additional recurring revenue costs associated with the refurbishment project.
As the project will be constructed on land owned by NHS Lanarkshire, ownership and responsibility for the facilities management, support services and clinical services support will rest with NHSL.
In conformance with the guidelines issued by SGHSCD, a statement of sustainable financial support for the revenue costs associated with the preferred option is contained Appendix 07.
5.4 Potential Impact on Balance Sheet
The capital costs associated with the refurbished and upgraded theatres and ICU will be capitalised in line with all appropriate accounting standards and this OBC is predicated on the appropriate level of Capital Funding being made available.
5.4.1 Major Medical Equipment
There are no costs included within this OBC for major medical equipment. There has been some recent investment in the Monklands Theatre Equipment and this will be available after conclusion of the works.
5.4.2 Construction Costs of the Facility
As responsibility for the construction and provision of the facility at Monklands District General Hospital will be the responsibility of NHSL, the capital funding for the construction, including appropriate fees etc., will need to be made available to NHSL. On completion of the ICU, it is proposed that the new building be subjected to an initial valuation by the District Valuer. As the project will result in the construction of a new building it is anticipated that the vast majority of the construction investment will add value to NHSL’s existing estate, however any impairment value will be communicated to the SGHSCD through completion of the annual AME Impairment Return.
5.4.3 Initial Expenditure up to Stage 1B of the Project
In order to progress the design and development of the facility to the current stage it has been necessary to appoint a Principal Supply Chain Partner (PSCP), Project Managers and Cost Advisors to progress the initial designs for the facility. Pending the approval of a preferred option, NHSL has progressed these aspects of the scheme and has therefore incurred some early capital costs associated with this work. As these costs are an integral
70
part of the scheme, they have been included in the construction expenditure noted in this document.
5.5 Stakeholder Support
The development of the Theatres & ICU refurbishment is supported by the following:
Diagram 14: Supporting Parties
A Letter of support is provided within Appendix 07.
5.6 Overall Affordability
The Financial Case has highlighted the overall capital and revenue affordability of the preferred option and identifies a requirement for:
A total forecast Capital cost of £17.9m to be funded through NHSL formula funding through 2014-15 with additional Scottish Government capital being provided from 2016-17 to completion.
Total recurring annual revenue costs of £0.23m to be funded by NHSL.
Acute Division Operating management committee NHS Lanarkshire Capital Investment Group NHS Lanarkshire Monklands investment Board
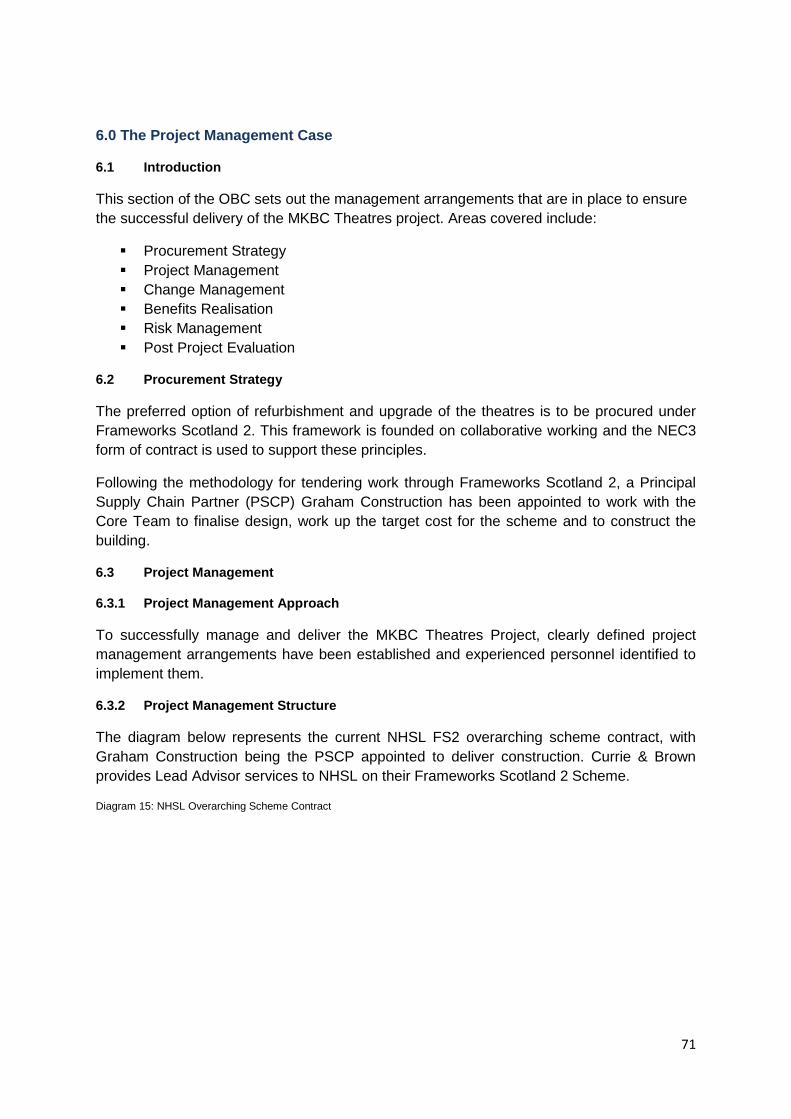
71
6.0 The Project Management Case
6.1 Introduction
This section of the OBC sets out the management arrangements that are in place to ensure the successful delivery of the MKBC Theatres project. Areas covered include:
Procurement Strategy Project Management Change Management Benefits Realisation Risk Management Post Project Evaluation
6.2 Procurement Strategy
The preferred option of refurbishment and upgrade of the theatres is to be procured under Frameworks Scotland 2. This framework is founded on collaborative working and the NEC3 form of contract is used to support these principles.
Following the methodology for tendering work through Frameworks Scotland 2, a Principal Supply Chain Partner (PSCP) Graham Construction has been appointed to work with the Core Team to finalise design, work up the target cost for the scheme and to construct the building.
6.3 Project Management
6.3.1 Project Management Approach
To successfully manage and deliver the MKBC Theatres Project, clearly defined project management arrangements have been established and experienced personnel identified to implement them.
6.3.2 Project Management Structure
The diagram below represents the current NHSL FS2 overarching scheme contract, with Graham Construction being the PSCP appointed to deliver construction. Currie & Brown provides Lead Advisor services to NHSL on their Frameworks Scotland 2 Scheme.
Diagram 15: NHSL Overarching Scheme Contract
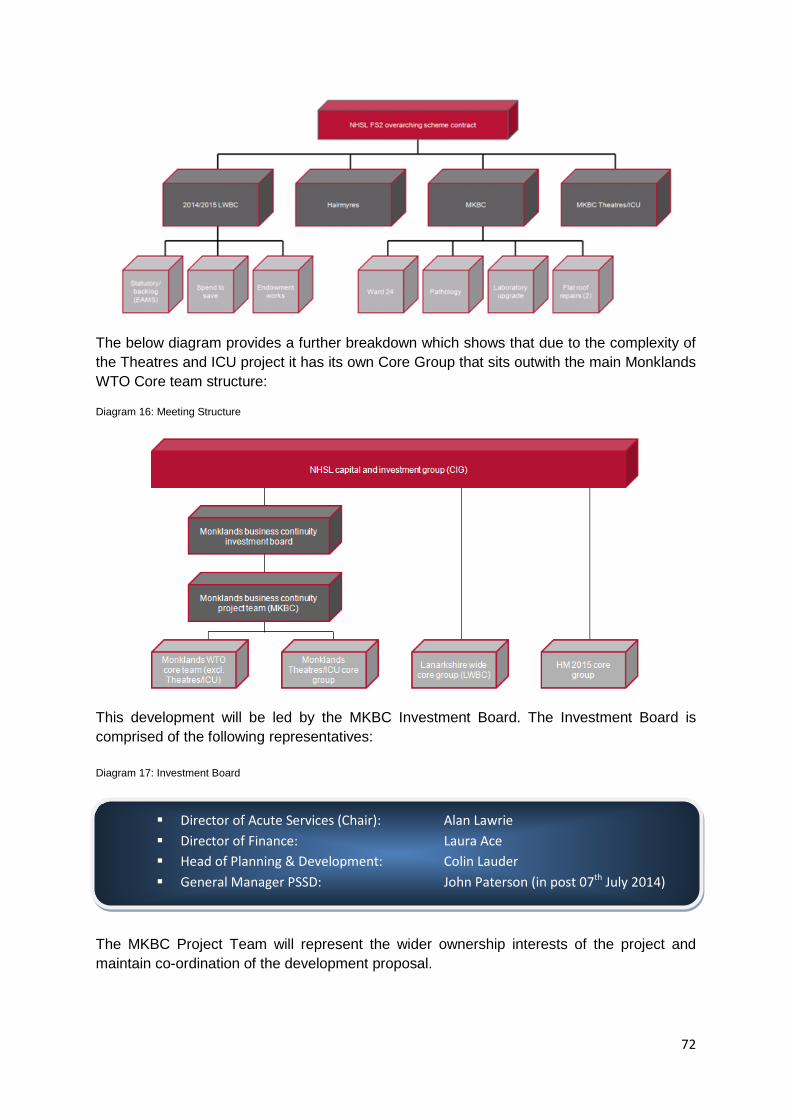
72
The below diagram provides a further breakdown which shows that due to the complexity of the Theatres and ICU project it has its own Core Group that sits outwith the main Monklands WTO Core team structure:
Diagram 16: Meeting Structure
This development will be led by the MKBC Investment Board. The Investment Board is comprised of the following representatives: Diagram 17: Investment Board The MKBC Project Team will represent the wider ownership interests of the project and maintain co-ordination of the development proposal.
Director of Acute Services (Chair): Alan Lawrie Director of Finance: Laura Ace Head of Planning & Development: Colin Lauder General Manager PSSD: John Paterson (in post 07th July 2014)
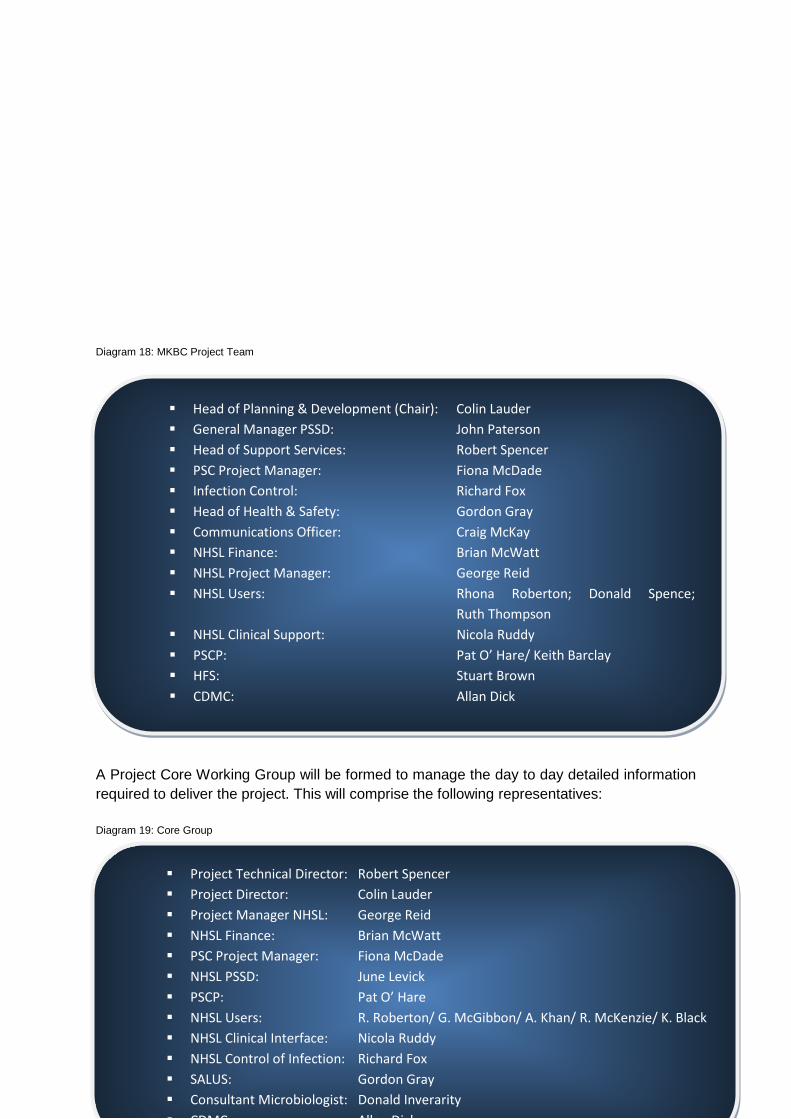
73
Diagram 18: MKBC Project Team A Project Core Working Group will be formed to manage the day to day detailed information required to deliver the project. This will comprise the following representatives: Diagram 19: Core Group
Project Technical Director: Robert Spencer Project Director: Colin Lauder Project Manager NHSL: George Reid NHSL Finance: Brian McWatt PSC Project Manager: Fiona McDade NHSL PSSD: June Levick PSCP: Pat O’ Hare NHSL Users: R. Roberton/ G. McGibbon/ A. Khan/ R. McKenzie/ K. Black NHSL Clinical Interface: Nicola Ruddy NHSL Control of Infection: Richard Fox SALUS: Gordon Gray Consultant Microbiologist: Donald Inverarity CDMC Allen Dick
Head of Planning & Development (Chair): Colin Lauder General Manager PSSD: John Paterson Head of Support Services: Robert Spencer PSC Project Manager: Fiona McDade Infection Control: Richard Fox Head of Health & Safety: Gordon Gray Communications Officer: Craig McKay NHSL Finance: Brian McWatt NHSL Project Manager: George Reid NHSL Users: Rhona Roberton; Donald Spence;
Ruth Thompson NHSL Clinical Support: Nicola Ruddy PSCP: Pat O’ Hare/ Keith Barclay HFS: Stuart Brown CDMC: Allan Dick
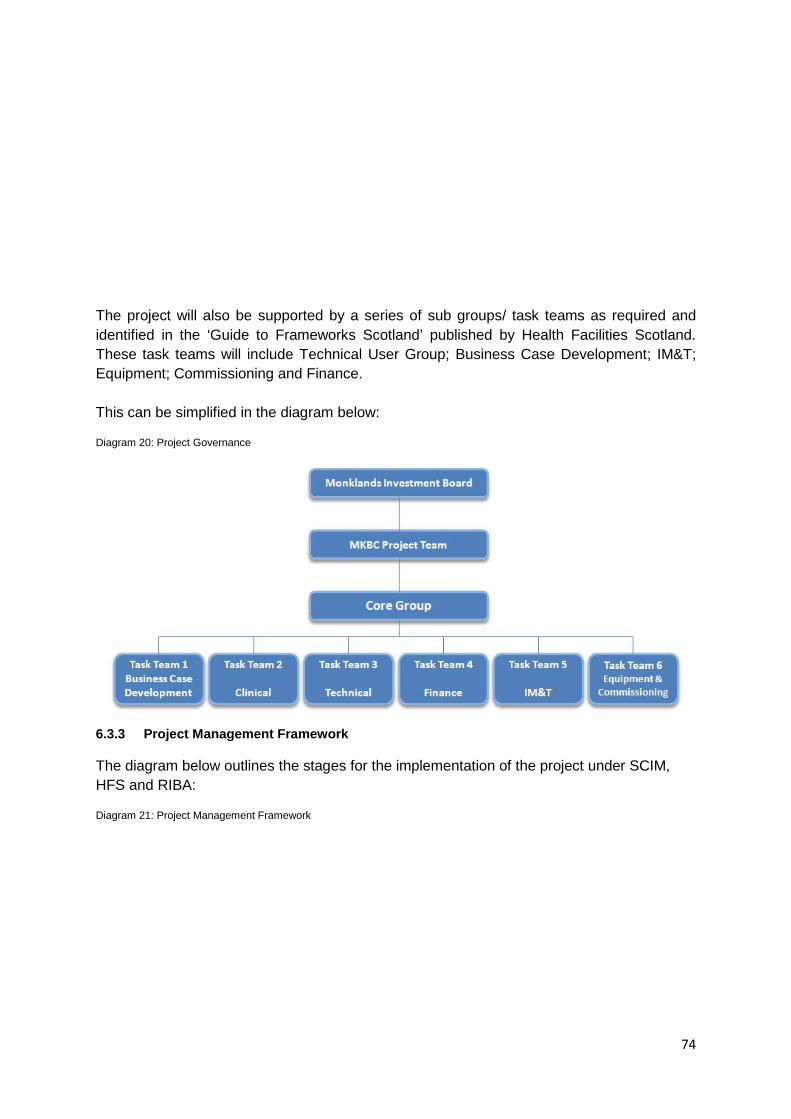
74
The project will also be supported by a series of sub groups/ task teams as required and identified in the ‘Guide to Frameworks Scotland’ published by Health Facilities Scotland. These task teams will include Technical User Group; Business Case Development; IM&T; Equipment; Commissioning and Finance. This can be simplified in the diagram below:
Diagram 20: Project Governance
6.3.3 Project Management Framework
The diagram below outlines the stages for the implementation of the project under SCIM, HFS and RIBA:
Diagram 21: Project Management Framework

75
6.3.4 Programme and Milestones
The Board anticipate that the Outline Business Case will be considered by the Scottish Government Capital Investment Group in July 2014. Should approval be granted to progress to FBC at this time, the indicative project timetable is as follows:
Table 32: Indicative Project Timetable
OBC CIG Submission 08th July 2014
OBC CIG Approval 05th August 2014
FBC CIG Submission 30th September 2014
FBC CIG Approval 28th October 2014
Construction Start on Site December 2014
Construction Completion March 2018
Post Project Evaluation +12 months from occupation
Post Occupancy Evaluation +2-5 years from occupation
The dates noted in the above table will be subject to further development/ agreement as the project progresses.
76
6.3.5 Stakeholder Consultation and Engagement
The MKBC project team has identified the key stakeholders with an interest this project as being:
Surgeons Anaesthetists Theatre and recovery nursing staff Control of infection team Managers within the acute division Managers within support services (estates and hotel services) Patient representatives.
Over the past two years a series of meetings and discussions has taken place with these stakeholders. This has included workshops to develop potential options and scoring of these options. Stakeholders are represented on the Core Group and as such have an active input into elements of the design of the proposed departments.
The design stages have been driven by the requirements of the clinical teams. Given that patients are generally unaware of their environment when in theatre or ICU, patient representatives have not yet been engaged with the design/ build process. It is intended that patient/ public input will be sought (via PPF’s) during the next stage.
6.4 Change Management
The project will utilise the processes from the Frameworks Scotland 2 procurement route which uses the NEC3 Engineering and Construction Contract with Activity Schedule.
This creates a structure and a discipline to manage change via the use of Early Warning Notices and Compensation Events and ensures change is identified early and is proactively managed by the project team.
6.5 Benefits Realisation
The main benefits for the MKBC Theatres Project are noted within section 2.9 of this OBC ‘Benefits Criteria’.
These will be reviewed as an integral part of the Post Project Evaluation work to ascertain if the benefits identified against the objectives of the business case have been met as a result of the project.
6.6 Risk Management
A Risk Register has been developed that is reflective of the Preferred Option and that includes contributions from all key stakeholders. The Risk Register will continue to be developed in accordance with SCIM guidance.
A Risk Workshop was held on 14/02/2014 and updated on 09/06/2014 in order to establish a project specific Register for this document.

77
Each identified risk will be assessed, quantified, managed and a designated risk owner/ manager assigned.
The Register will be routinely reviewed and updated over the lifespan of the project to minimise the level of risk. It will be updated for each early warning during the construction phase.
The Risk Register will be an Agenda item at the Core Team Meetings, with all high priority risks subject to review and a general overview of all other risks to ensure that their impact on the project is not escalating.
The Risk Register will be a key tool in the ongoing management of the Project with a risk management strategy being employed to ensure:
Risks are identified in advance and mitigation strategies are agreed A process is in place to monitor risks and keep them up to date Agreement as to the right balance of control to mitigate against the adverse
consequences of the risk should it materialise A decision making process is implemented, supported by a framework of risk
analysis and evaluation
6.7 Post Project Evaluation
In order to assess the impact of the project, an evaluation of activity and performance must be carried out post completion. This is an essential aid to improving future project performance, achieving best value for money from public resources, improving decision making and learning lessons. The PPE shall follow the guidance as detailed in the Scottish Capital Investment Manual and will be implemented six months after completion, appraising all stages of the Project from preparation of the business case through construction to occupation and service.
A Post Occupancy Evaluation will be implemented 2-5 years after completion to appraise whether the project has delivered its anticipated improvements and benefits.
78
7. Conclusion
Providing the refurbishment and upgrade to the Theatres and ICU at Monklands General Hospital will improve patient experience whilst offering modern services locally to where people live. As a central element of the proposal this will enable the meeting of the challenges of implementing NHS Scotland’s ‘Route Map to the 2020 Vision for Health and Social Care’ (2013).
The Preferred Option, to refurbish the existing seven theatres alongside the construction of a new build 10 bed ICU represents the best investment to provide the required services going forward. It is the best value option, as has been demonstrated throughout this document, and would fulfil the drivers identified in this OBC. These new facilities would provide a 21st century environment that would meet the needs and aspirations of both staff and patients within NHS Lanarkshire.
Approval of this OBC will ensure that the project can move at pace towards the development of the Full Business Case for this critical project.

79
Appendix 01:
Design Statement

80
81
MKBC Theatres & ICU refurbishment and upgrade: Design Statement
Introduction:
This Design Statement has been created to support the development of the above new and refurbished facilities and acts as a key briefing document for the project Technical Team. It will be used to enhance the design process to ensure that the project primary objectives are delivered. The key design principles and non- negotiable performance criteria are set out below:
Key Design Principles:
Provide Services that are safely and easily accessible
Improve and maintain retention and recruitment of staff
Provide an environment that supports service delivery, clinical effectiveness and integrated service provision
Provide a quality of clinical environment that promotes the health and wellbeing of the staff and patients
Develop theatre designs that will improve surgical services, storage and support.
Provide facilities that are both sustainable and flexible to support service provision in the future
Encourage a learning environment for staff through the provision of dedicated training facilities
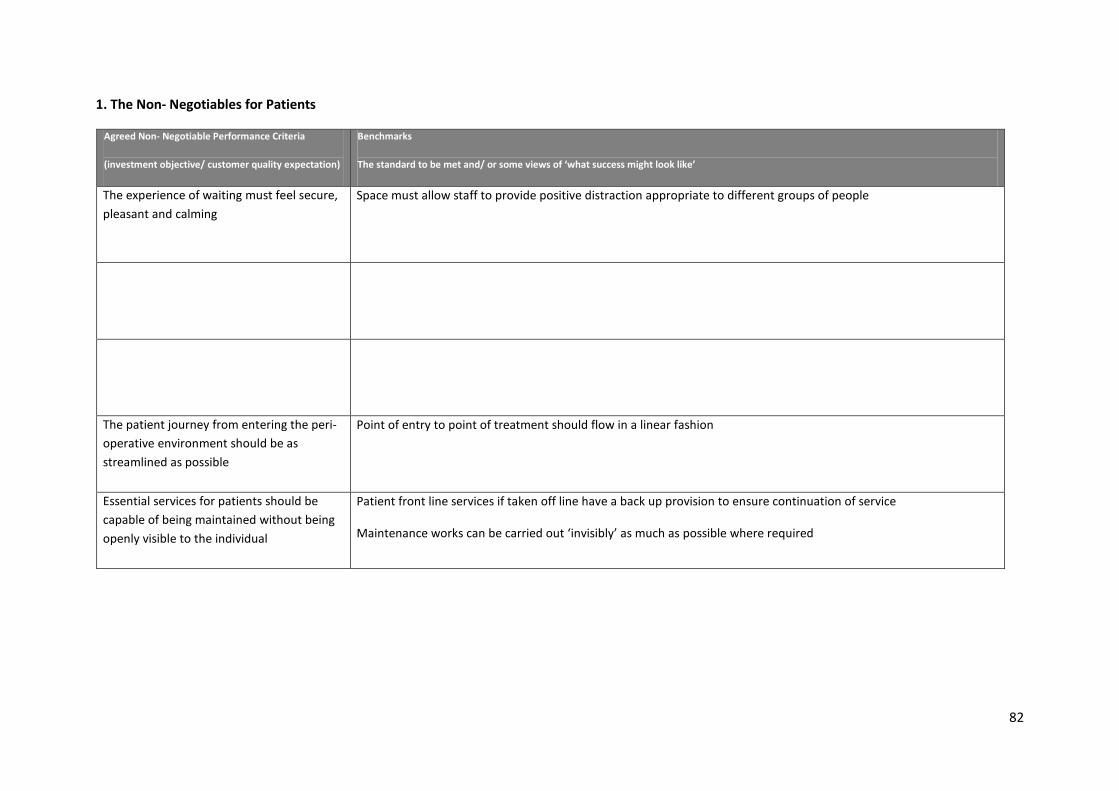
82
1. The Non- Negotiables for Patients
Agreed Non- Negotiable Performance Criteria
(investment objective/ customer quality expectation)
Benchmarks
The standard to be met and/ or some views of ‘what success might look like’
The experience of waiting must feel secure, pleasant and calming
Space must allow staff to provide positive distraction appropriate to different groups of people
The patient journey from entering the peri- operative environment should be as streamlined as possible
Point of entry to point of treatment should flow in a linear fashion
Essential services for patients should be capable of being maintained without being openly visible to the individual
Patient front line services if taken off line have a back up provision to ensure continuation of service
Maintenance works can be carried out ‘invisibly’ as much as possible where required

83
2. The Non- Negotiables for Staff
Agreed Non- Negotiable Performance Criteria
(investment objective/ customer quality expectation)
Benchmarks
The standard to be met and/ or some views of ‘what success might look like’
The development must be efficient with rooms and circulation routes configured to allow flexibility in use.
Clear definition of patient areas from back of house/ staff areas
Design to ensure optimal flexibility and efficiency
Staff must be able to rest/ debrief/ relax away from the service provision spaces with access to daylight
Staff rest space, in addition to providing for tea/ lunch prep must provide:
• Space for coming together to chat
• Space for quiet thought
• Good daylight
• Be an attractive and restful space
Ensure the most efficient use of space and that the use of shared space is optimised. Efficient space allocation and ability to respond to future service changes effectively is to be promoted.
Office space should be shared wherever possible – limit one person offices
Space should allow long term flexibility of use without fundamental physical change
Spaces should be set out logically in relation to each other and should be capable of long term flexibility
The layout of the facility must encourage and facilitate co-ordinated working and communication between disciplines on a formal and informal basis
Staff routes should encourage interaction between services rather than isolate them
Common facilities such as staff rest and meeting rooms should be provided as a shared resource
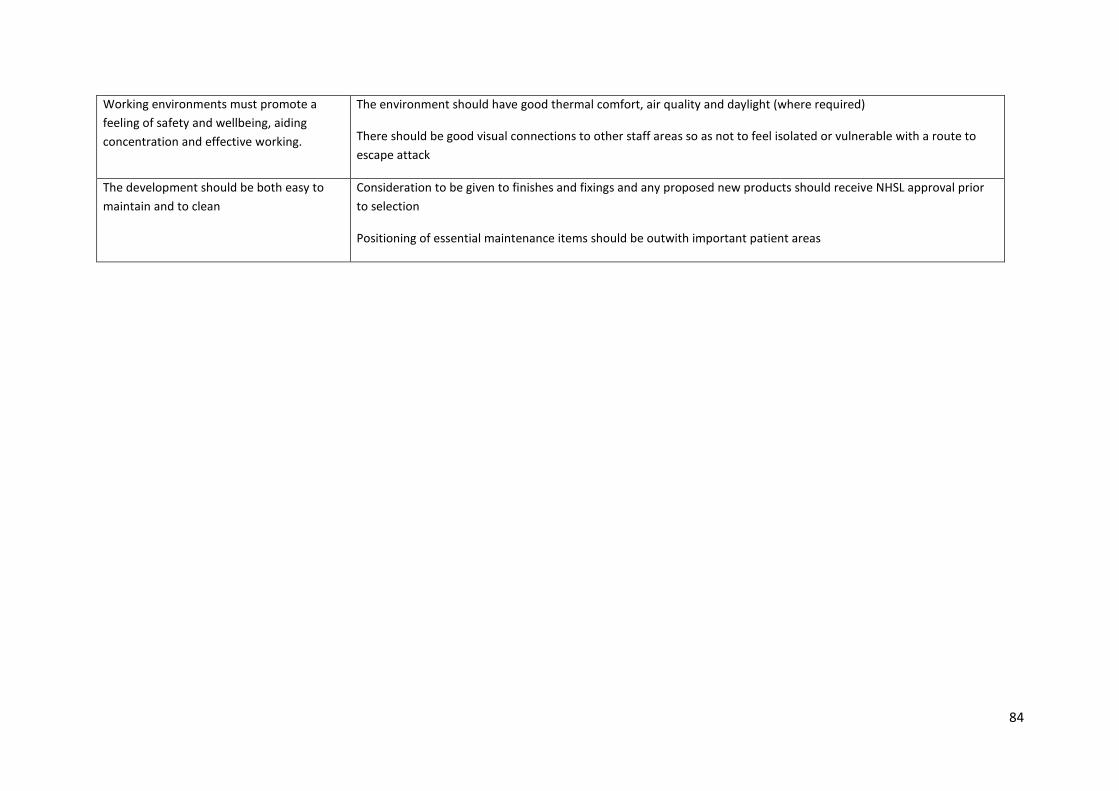
84
Working environments must promote a feeling of safety and wellbeing, aiding concentration and effective working.
The environment should have good thermal comfort, air quality and daylight (where required)
There should be good visual connections to other staff areas so as not to feel isolated or vulnerable with a route to escape attack
The development should be both easy to maintain and to clean
Consideration to be given to finishes and fixings and any proposed new products should receive NHSL approval prior to selection
Positioning of essential maintenance items should be outwith important patient areas

85
3. The Non- Negotiables for Visitors
Agreed Non- Negotiable Performance Criteria
(investment objective/ customer quality expectation)
Benchmarks
The standard to be met and/ or some views of ‘what success might look like’
Carers/ Family members accompanying patients must be able to find information and additional support to assist them
Information and signposting points available
Space should be provided to accommodate and occupy dependants while patients are being treated
Waiting areas should be attractive and restful with daylight
Carers/ Family members accompanying patients should have access to an interview room that provides a confidential environment for discussion
Interview room should be within easy access of the relative waiting area
Carers/ Family members accompanying patients should have the ability to access assistance if required
Staff should be within easy reach of Carers/ Family Members if assistance is needed
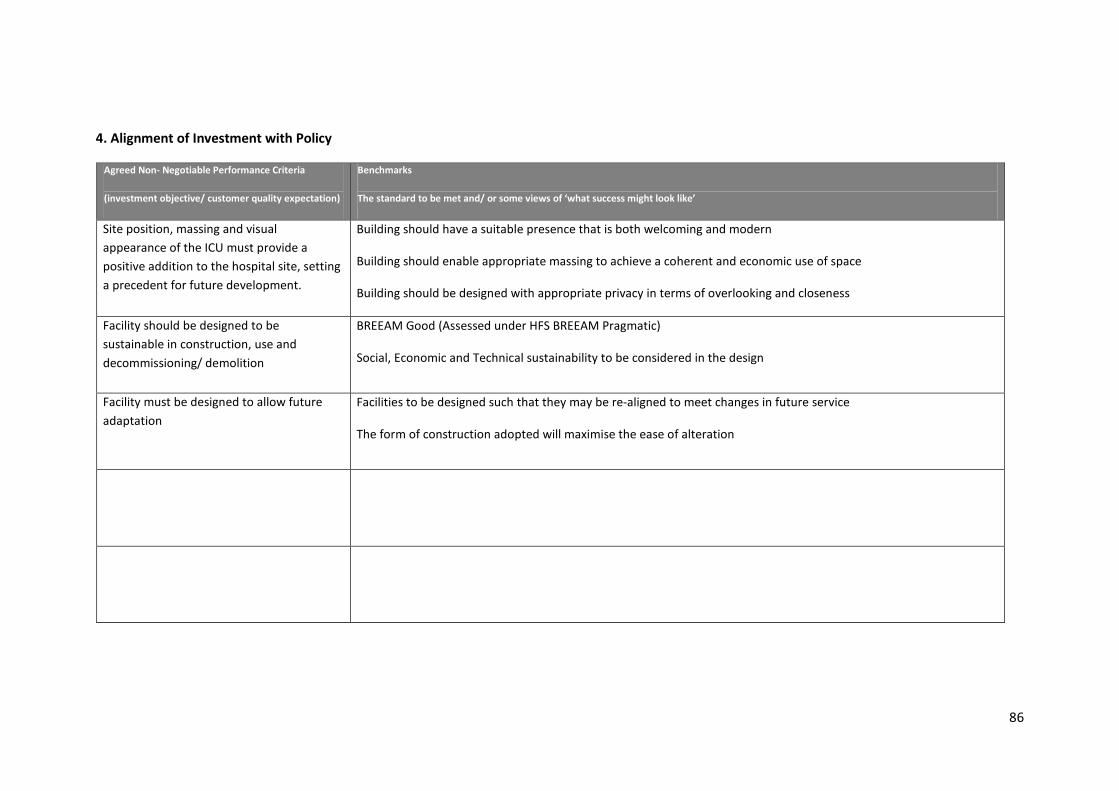
86
4. Alignment of Investment with Policy
Agreed Non- Negotiable Performance Criteria
(investment objective/ customer quality expectation)
Benchmarks
The standard to be met and/ or some views of ‘what success might look like’
Site position, massing and visual appearance of the ICU must provide a positive addition to the hospital site, setting a precedent for future development.
Building should have a suitable presence that is both welcoming and modern
Building should enable appropriate massing to achieve a coherent and economic use of space
Building should be designed with appropriate privacy in terms of overlooking and closeness
Facility should be designed to be sustainable in construction, use and decommissioning/ demolition
BREEAM Good (Assessed under HFS BREEAM Pragmatic)
Social, Economic and Technical sustainability to be considered in the design
Facility must be designed to allow future adaptation
Facilities to be designed such that they may be re-aligned to meet changes in future service
The form of construction adopted will maximise the ease of alteration
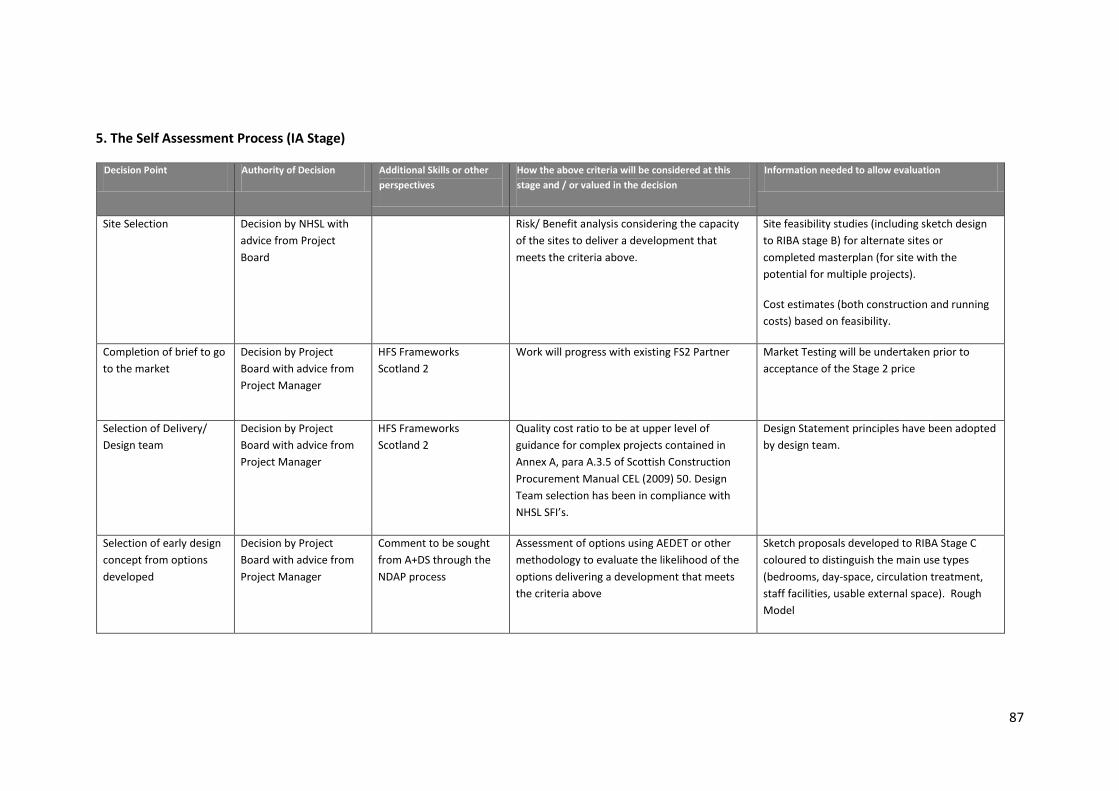
87
5. The Self Assessment Process (IA Stage)
Decision Point Authority of Decision Additional Skills or other perspectives
How the above criteria will be considered at this stage and / or valued in the decision
Information needed to allow evaluation
Site Selection Decision by NHSL with advice from Project Board
Risk/ Benefit analysis considering the capacity of the sites to deliver a development that meets the criteria above.
Site feasibility studies (including sketch design to RIBA stage B) for alternate sites or completed masterplan (for site with the potential for multiple projects).
Cost estimates (both construction and running costs) based on feasibility.
Completion of brief to go to the market
Decision by Project Board with advice from Project Manager
HFS Frameworks Scotland 2
Work will progress with existing FS2 Partner Market Testing will be undertaken prior to acceptance of the Stage 2 price
Selection of Delivery/ Design team
Decision by Project Board with advice from Project Manager
HFS Frameworks Scotland 2
Quality cost ratio to be at upper level of guidance for complex projects contained in Annex A, para A.3.5 of Scottish Construction Procurement Manual CEL (2009) 50. Design Team selection has been in compliance with NHSL SFI’s.
Design Statement principles have been adopted by design team.
Selection of early design concept from options developed
Decision by Project Board with advice from Project Manager
Comment to be sought from A+DS through the NDAP process
Assessment of options using AEDET or other methodology to evaluate the likelihood of the options delivering a development that meets the criteria above
Sketch proposals developed to RIBA Stage C coloured to distinguish the main use types (bedrooms, day-space, circulation treatment, staff facilities, usable external space). Rough Model
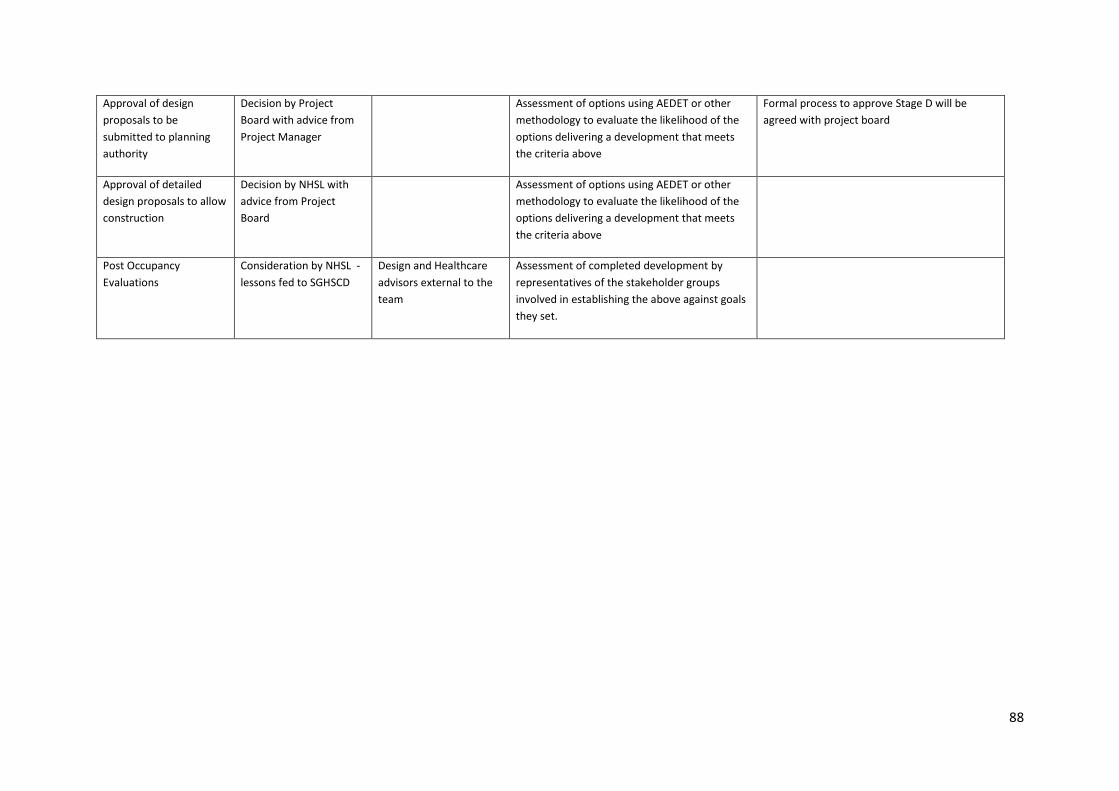
88
Approval of design proposals to be submitted to planning authority
Decision by Project Board with advice from Project Manager
Assessment of options using AEDET or other methodology to evaluate the likelihood of the options delivering a development that meets the criteria above
Formal process to approve Stage D will be agreed with project board
Approval of detailed design proposals to allow construction
Decision by NHSL with advice from Project Board
Assessment of options using AEDET or other methodology to evaluate the likelihood of the options delivering a development that meets the criteria above
Post Occupancy Evaluations
Consideration by NHSL - lessons fed to SGHSCD
Design and Healthcare advisors external to the team
Assessment of completed development by representatives of the stakeholder groups involved in establishing the above against goals they set.

89

90
Appendix 02:
A+DS/ HFS Letter of Support
[will be included in SGHSCD submission]

91
Appendix 03:
AEDET Workshop One Summary
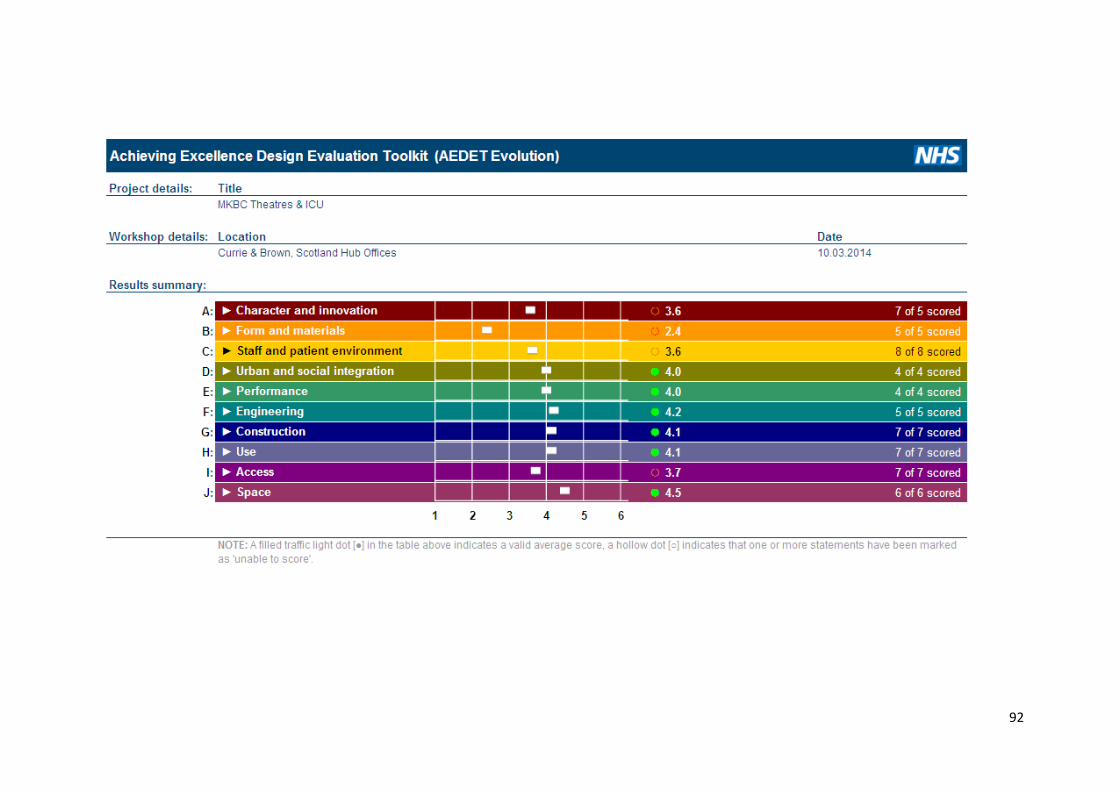
92

93
Appendix 04:
Risk Register
94

95

96
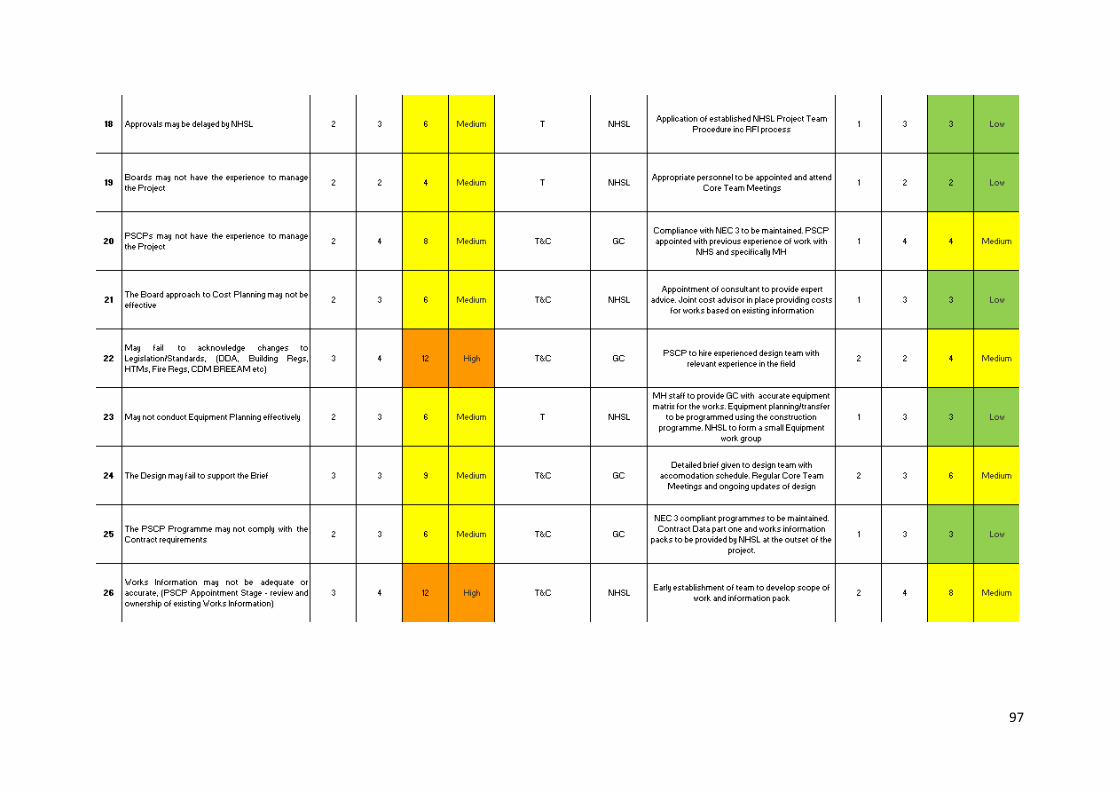
97
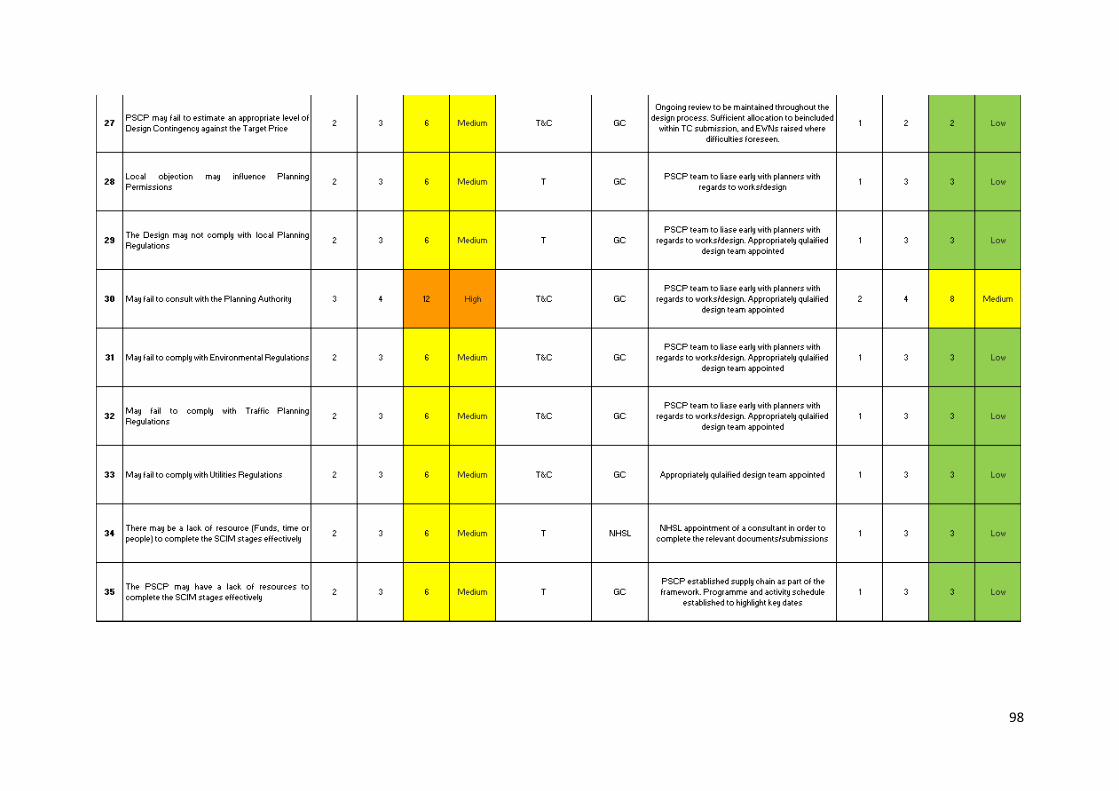
98
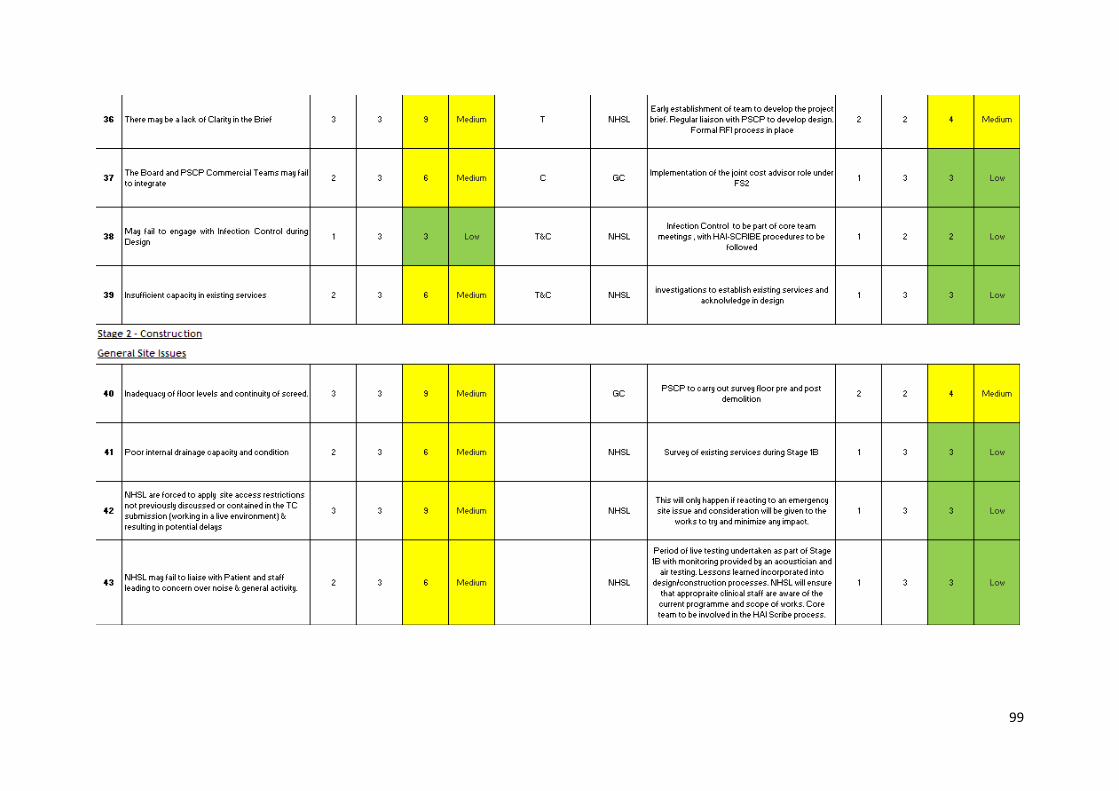
99
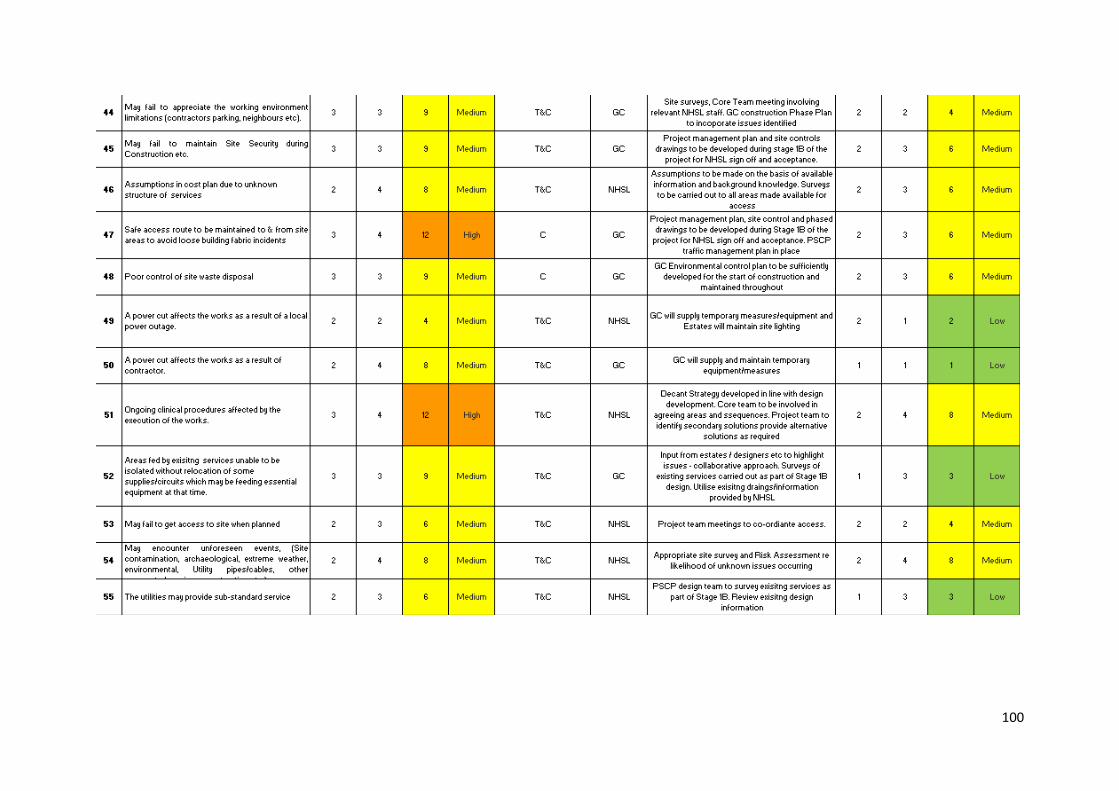
100
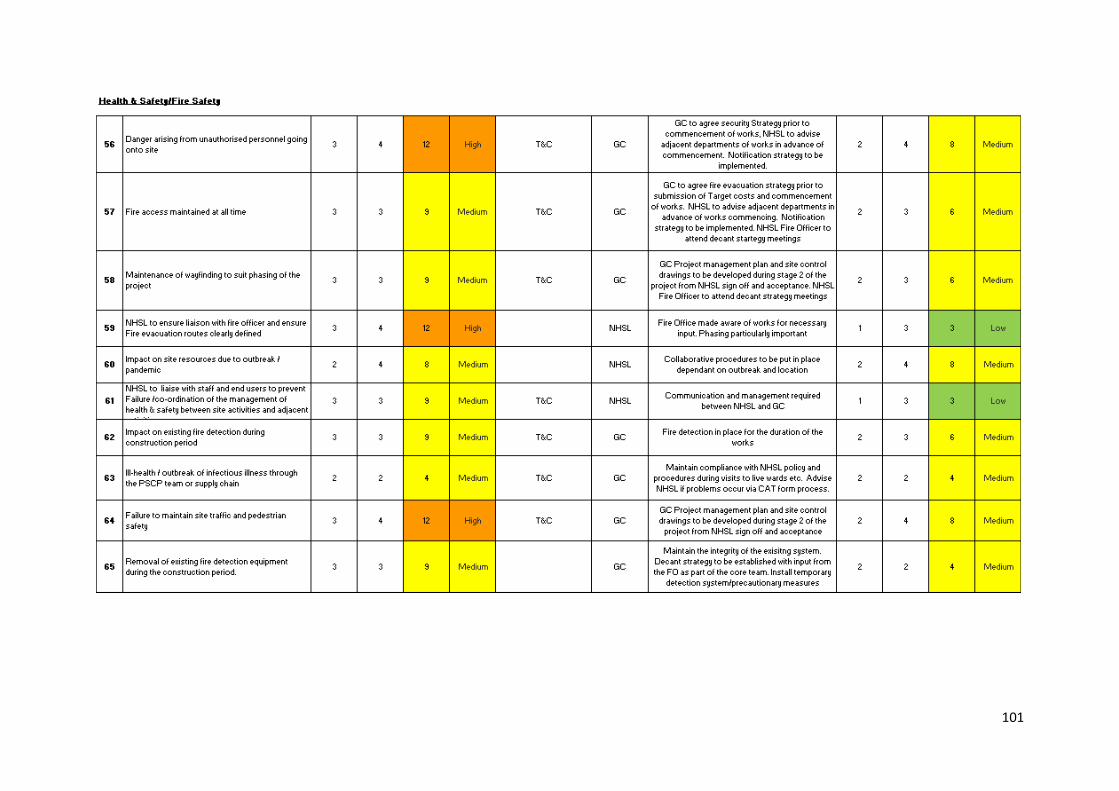
101
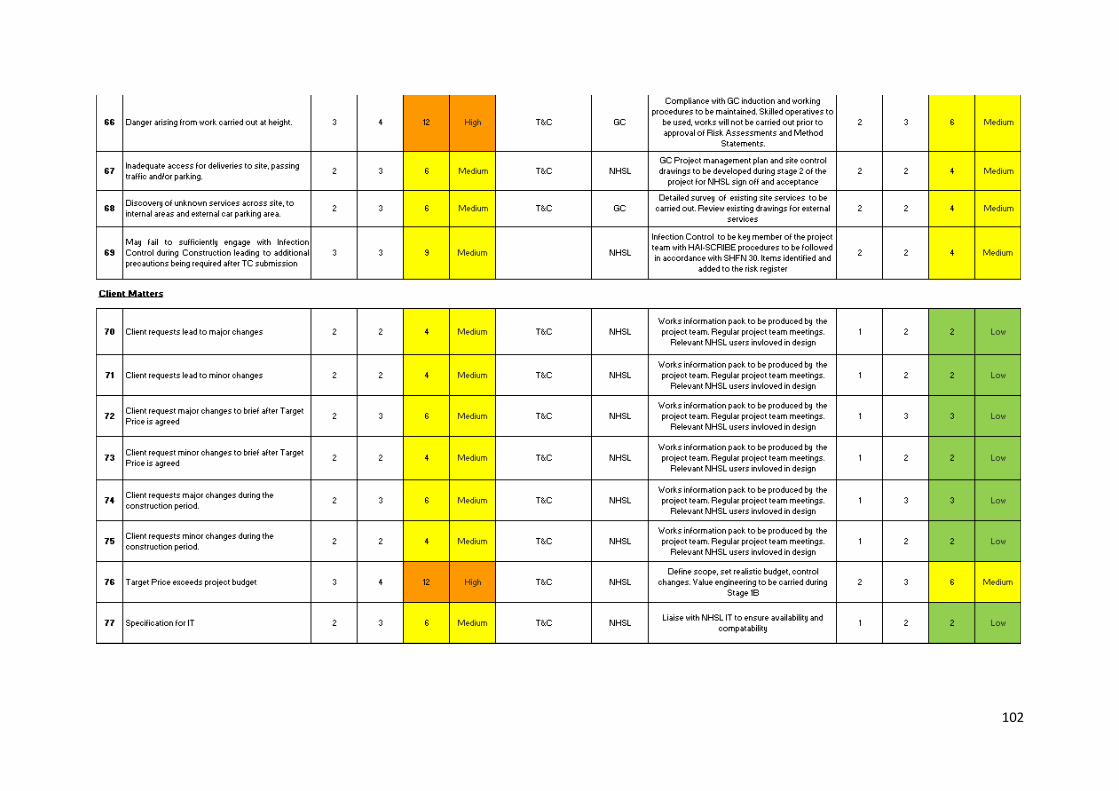
102

103
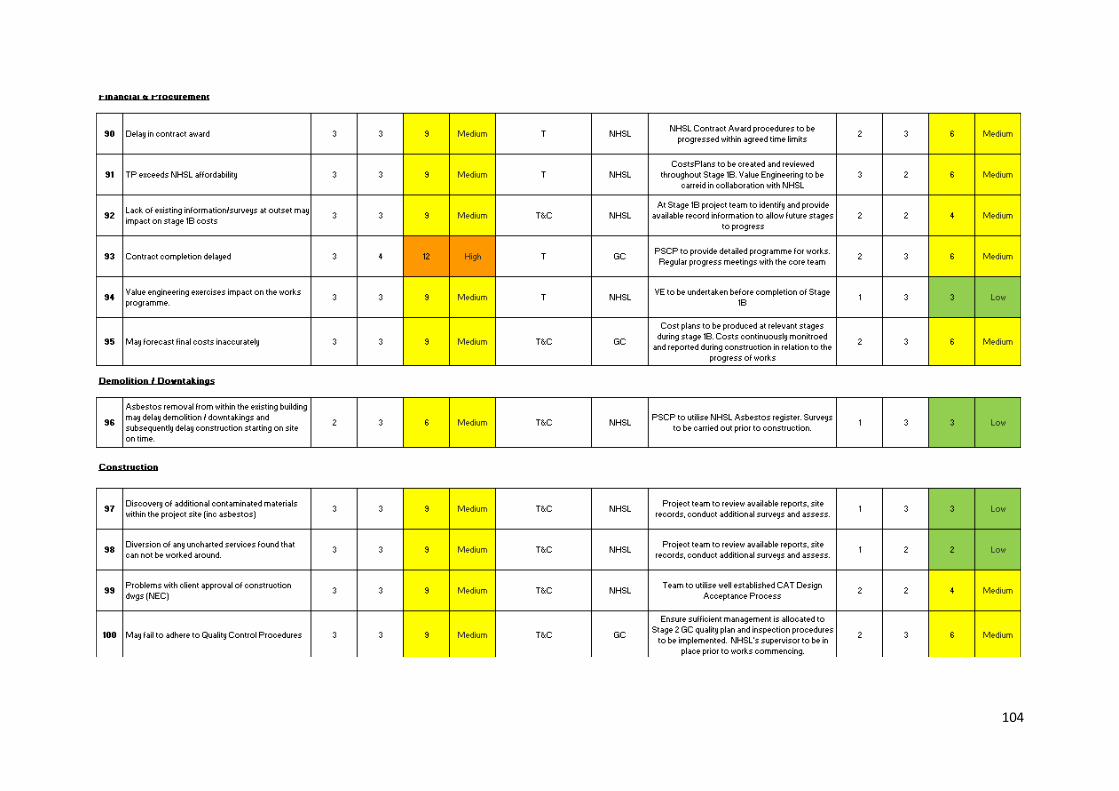
104
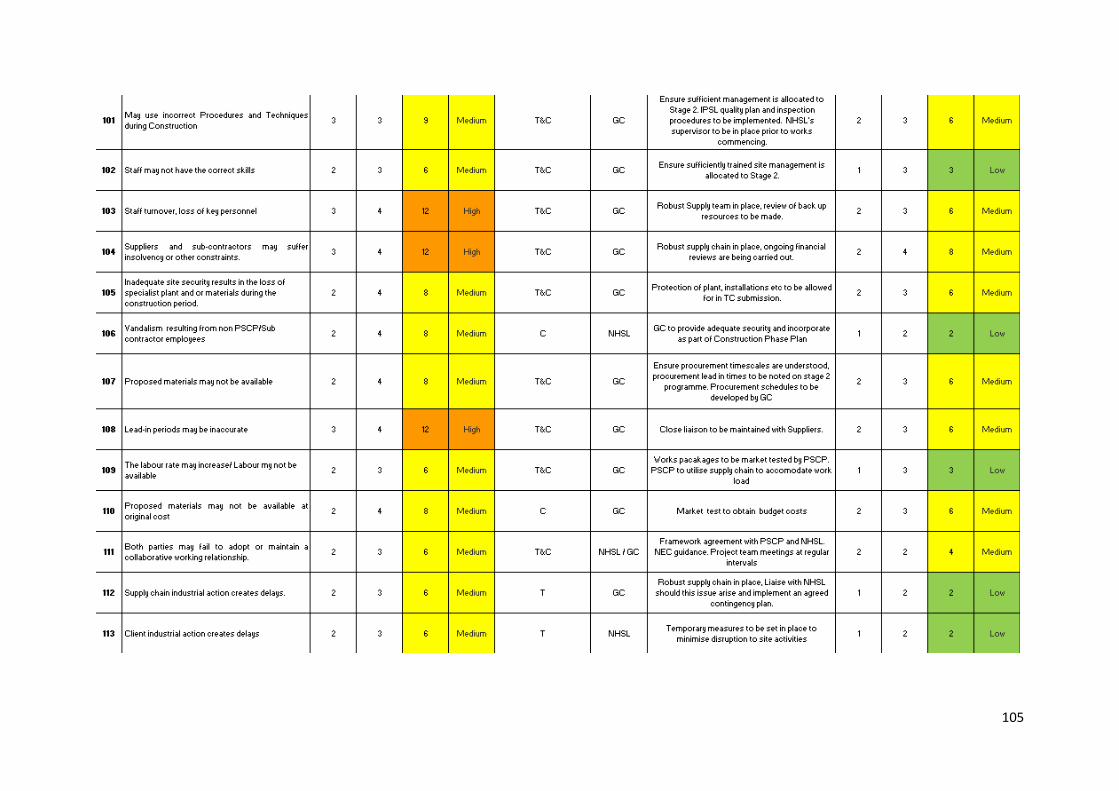
105
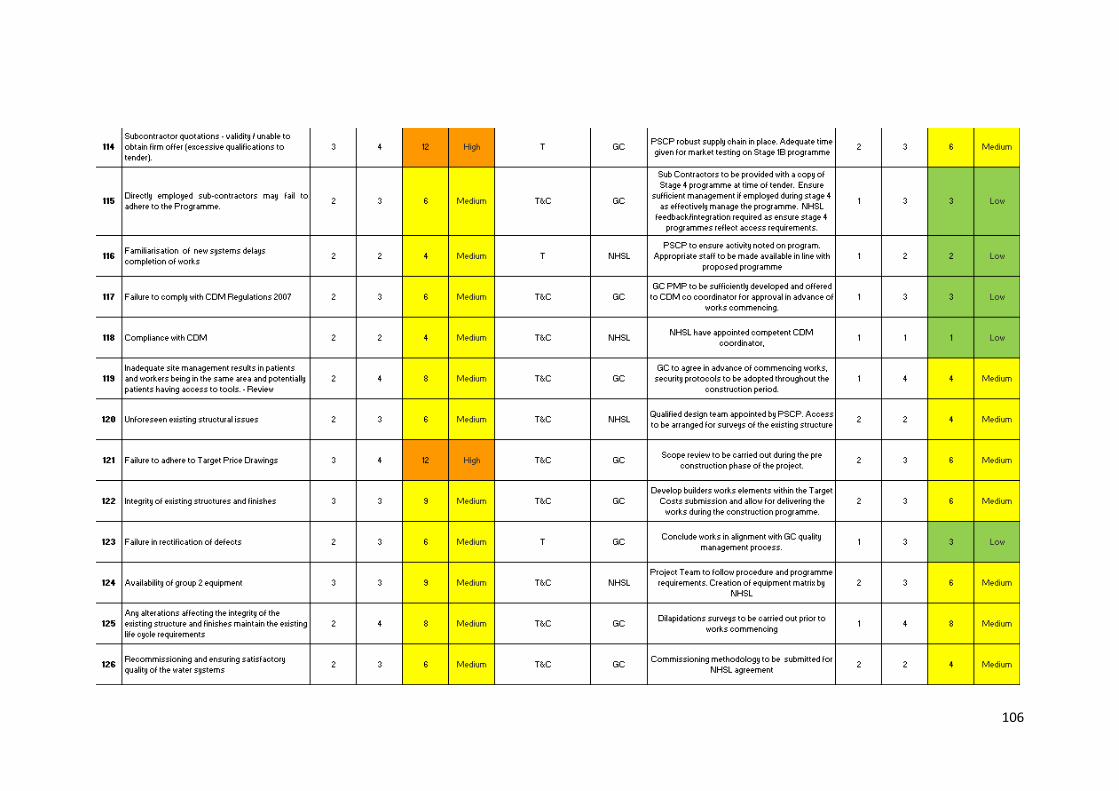
106

107
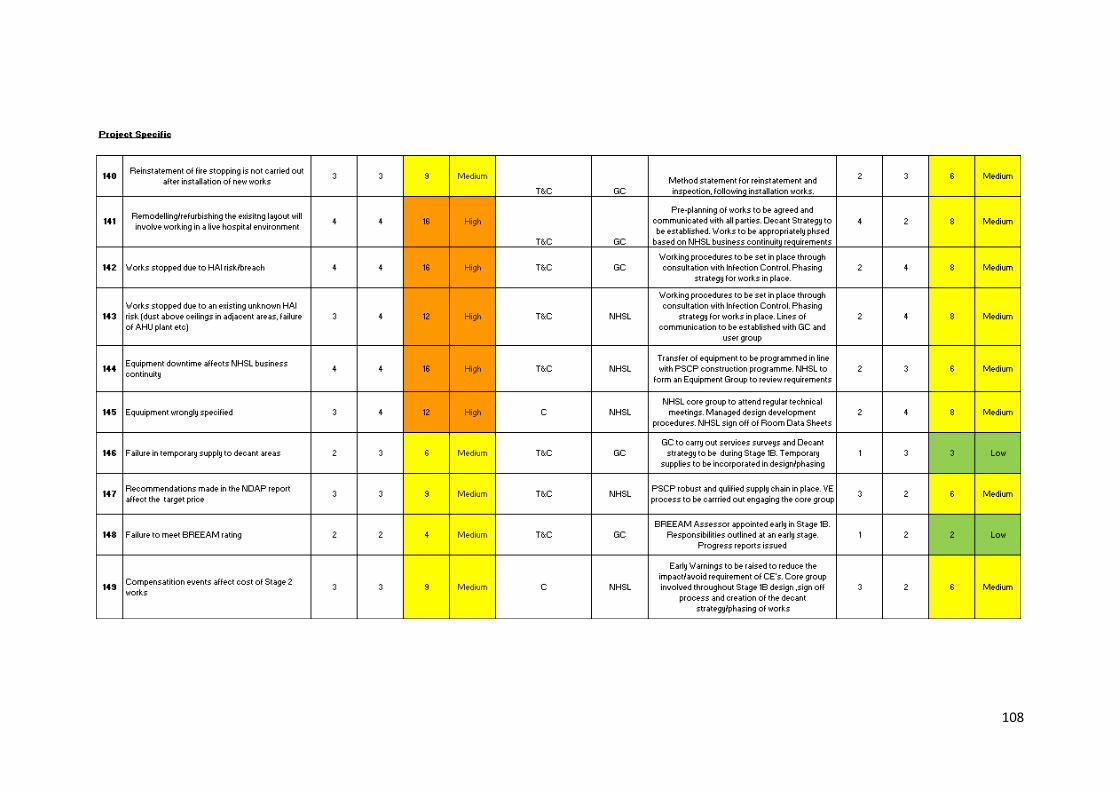
108
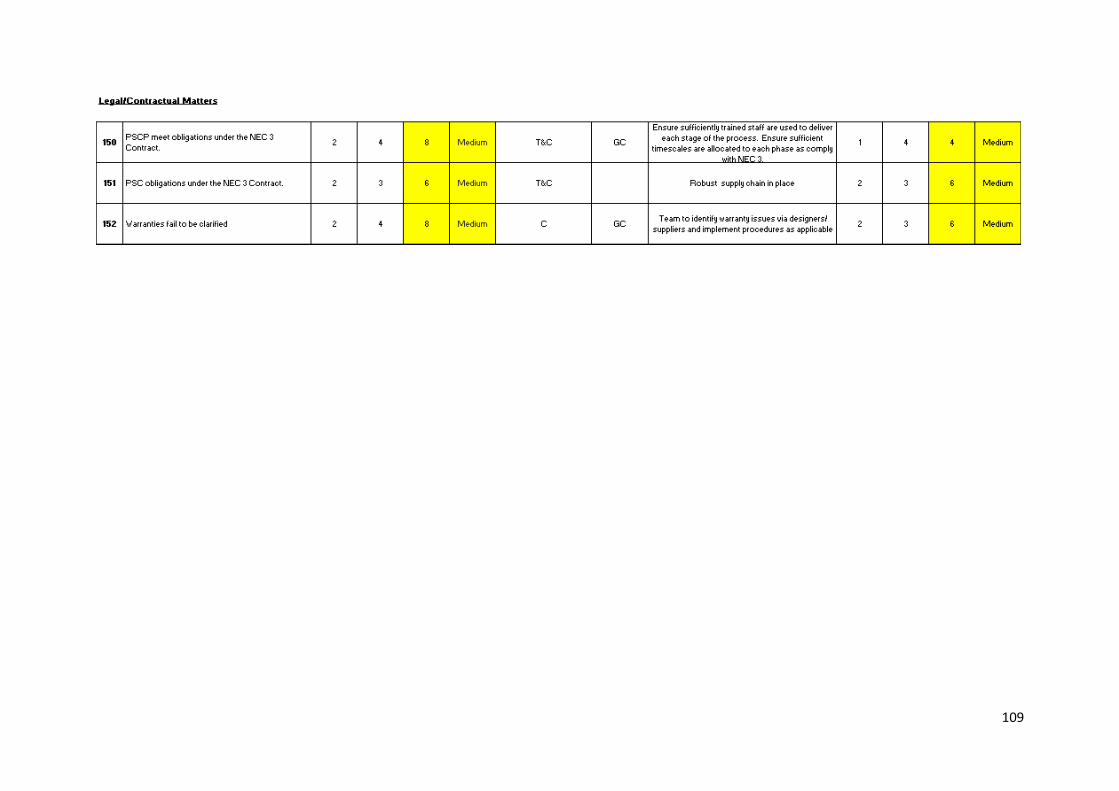
109
110
Appendix 05:
SWOT Analysis
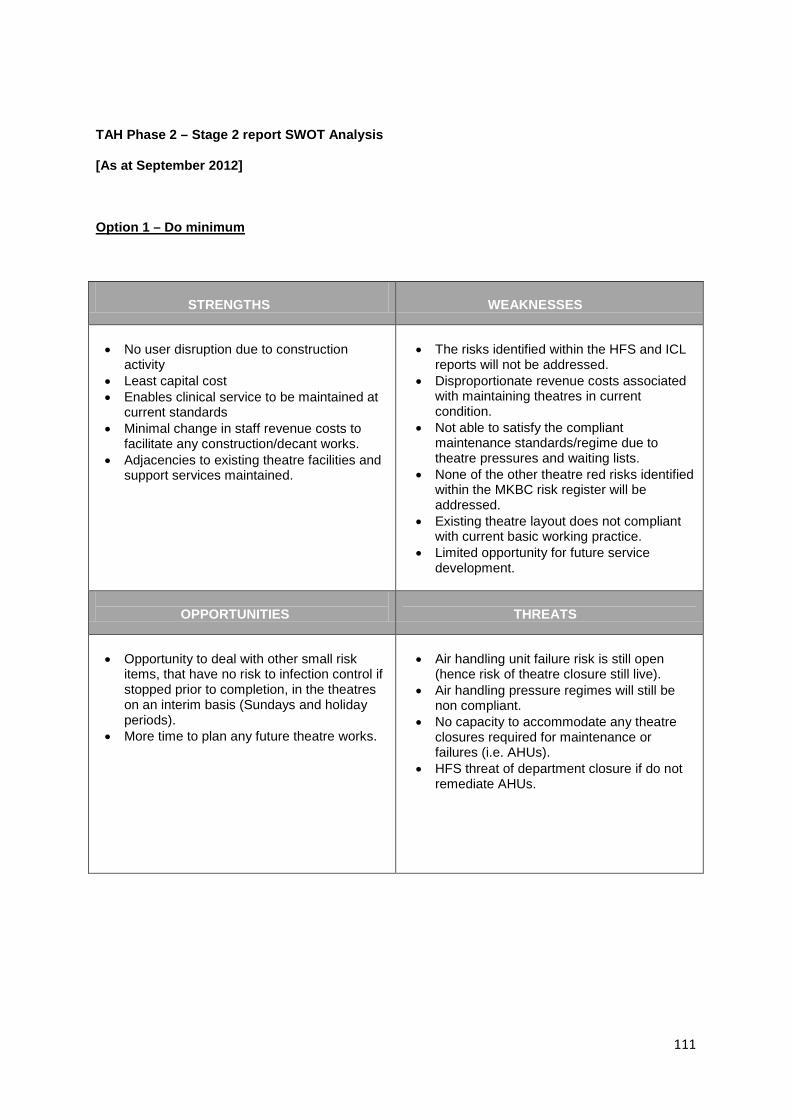
111
TAH Phase 2 – Stage 2 report SWOT Analysis
[As at September 2012]
Option 1 – Do minimum
STRENGTHS
WEAKNESSES
• No user disruption due to construction
activity • Least capital cost • Enables clinical service to be maintained at
current standards • Minimal change in staff revenue costs to
facilitate any construction/decant works. • Adjacencies to existing theatre facilities and
support services maintained.
• The risks identified within the HFS and ICL
reports will not be addressed. • Disproportionate revenue costs associated
with maintaining theatres in current condition.
• Not able to satisfy the compliant maintenance standards/regime due to theatre pressures and waiting lists.
• None of the other theatre red risks identified within the MKBC risk register will be addressed.
• Existing theatre layout does not compliant with current basic working practice.
• Limited opportunity for future service development.
OPPORTUNITIES
THREATS
• Opportunity to deal with other small risk
items, that have no risk to infection control if stopped prior to completion, in the theatres on an interim basis (Sundays and holiday periods).
• More time to plan any future theatre works.
• Air handling unit failure risk is still open
(hence risk of theatre closure still live). • Air handling pressure regimes will still be
non compliant. • No capacity to accommodate any theatre
closures required for maintenance or failures (i.e. AHUs).
• HFS threat of department closure if do not remediate AHUs.
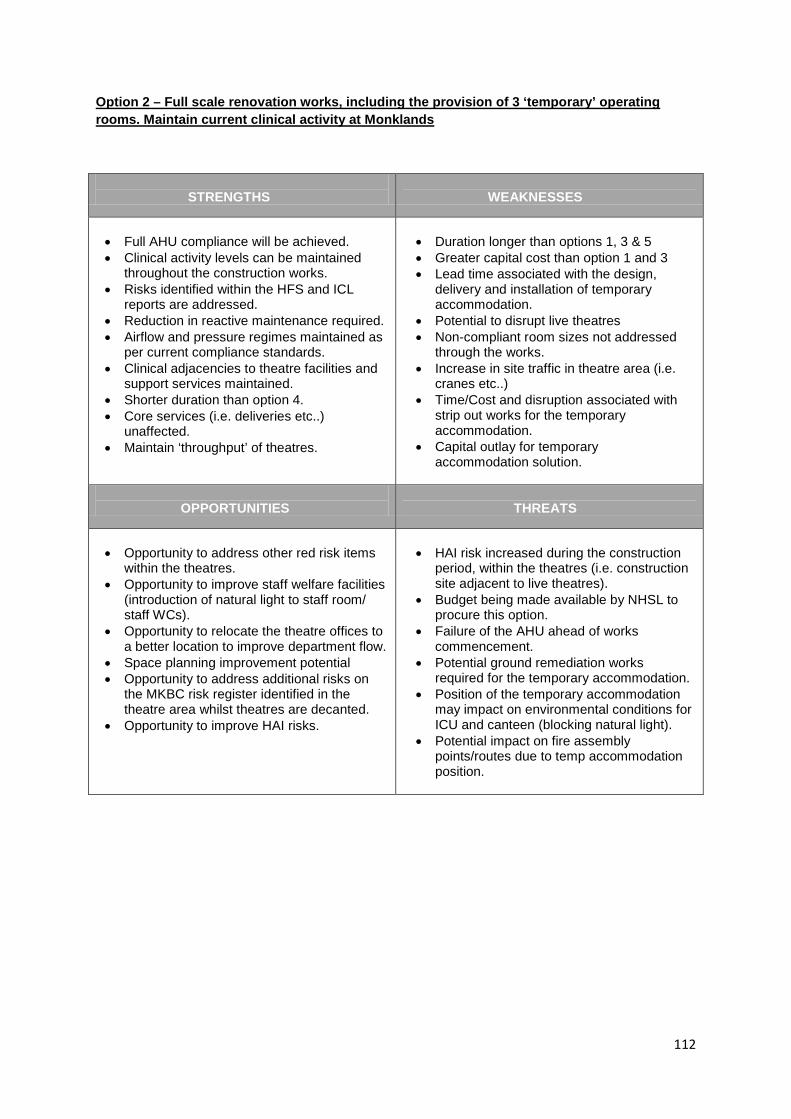
112
Option 2 – Full scale renovation works, including the provision of 3 ‘temporary’ operating rooms. Maintain current clinical activity at Monklands
STRENGTHS
WEAKNESSES
• Full AHU compliance will be achieved. • Clinical activity levels can be maintained
throughout the construction works. • Risks identified within the HFS and ICL
reports are addressed. • Reduction in reactive maintenance required. • Airflow and pressure regimes maintained as
per current compliance standards. • Clinical adjacencies to theatre facilities and
support services maintained. • Shorter duration than option 4. • Core services (i.e. deliveries etc..)
unaffected. • Maintain ‘throughput’ of theatres.
• Duration longer than options 1, 3 & 5 • Greater capital cost than option 1 and 3 • Lead time associated with the design,
delivery and installation of temporary accommodation.
• Potential to disrupt live theatres • Non-compliant room sizes not addressed
through the works. • Increase in site traffic in theatre area (i.e.
cranes etc..) • Time/Cost and disruption associated with
strip out works for the temporary accommodation.
• Capital outlay for temporary accommodation solution.
OPPORTUNITIES
THREATS
• Opportunity to address other red risk items
within the theatres. • Opportunity to improve staff welfare facilities
(introduction of natural light to staff room/ staff WCs).
• Opportunity to relocate the theatre offices to a better location to improve department flow.
• Space planning improvement potential • Opportunity to address additional risks on
the MKBC risk register identified in the theatre area whilst theatres are decanted.
• Opportunity to improve HAI risks.
• HAI risk increased during the construction
period, within the theatres (i.e. construction site adjacent to live theatres).
• Budget being made available by NHSL to procure this option.
• Failure of the AHU ahead of works commencement.
• Potential ground remediation works required for the temporary accommodation.
• Position of the temporary accommodation may impact on environmental conditions for ICU and canteen (blocking natural light).
• Potential impact on fire assembly points/routes due to temp accommodation position.

113
Option 3 – Renovation of a proportion of the department, using 3 new operating rooms during and after the works
STRENGTHS
WEAKNESSES
• Full AHU compliance will be achieved. • Clinical activity levels can be maintained
throughout the construction works. • Risks identified within the HFS and ICL
reports are addressed. • Reduction in reactive maintenance required. • Airflow and pressure regimes maintained as
per current compliance standards. • Clinical adjacencies to theatre facilities and
support services maintained. • Shorter duration than option 4. • Core services (i.e. deliveries etc..)
unaffected. • Maintain ‘throughput’ of theatres. • No cost associated with the demolition of the
modular building (as per option 2). • Opportunity to use redundant theatres for
another purpose.
• Duration longer than options 1 & 5 • Greater capital cost than option 1 • Lead time associated with the design,
delivery and installation of temporary accommodation.
• Potential to disrupt live theatres • Non-compliant room sizes not addressed
through the works (unless theatres re-configured i.e. 7 existing theatres become 4 compliant theatres)
• Increase in site traffic in theatre area (i.e. cranes etc..)
• Capital outlay for modular accommodation solution.
OPPORTUNITIES
THREATS
• Opportunity to increase the no. of theatres to
8 no. working theatres (i.e. 3 no. theatres in modular building and convert the existing 7 theatres into 5 complaint sized theatres).
• Ability to increase the ‘throughput’ at the theatres.
• HAI risk increased during the construction
period, within the theatres (i.e. construction site adjacent to live theatres).
• Budget being made available by NHSL to procure this option.
• Failure of the AHU ahead of works commencement.
• Potential ground remediation works required for the modular accommodation.
• Position of the modular accommodation may impact on environmental conditions for ICU and canteen (blocking natural light).
• Potential impact on fire assembly points/routes due to modular accommodation position.
• If the decision was made to increase the no. of theatres (i.e. refurb all 7 existing theatres and maintain the modular accommodation) the associated facilities would require expansion also (i.e. ICU and recovery).
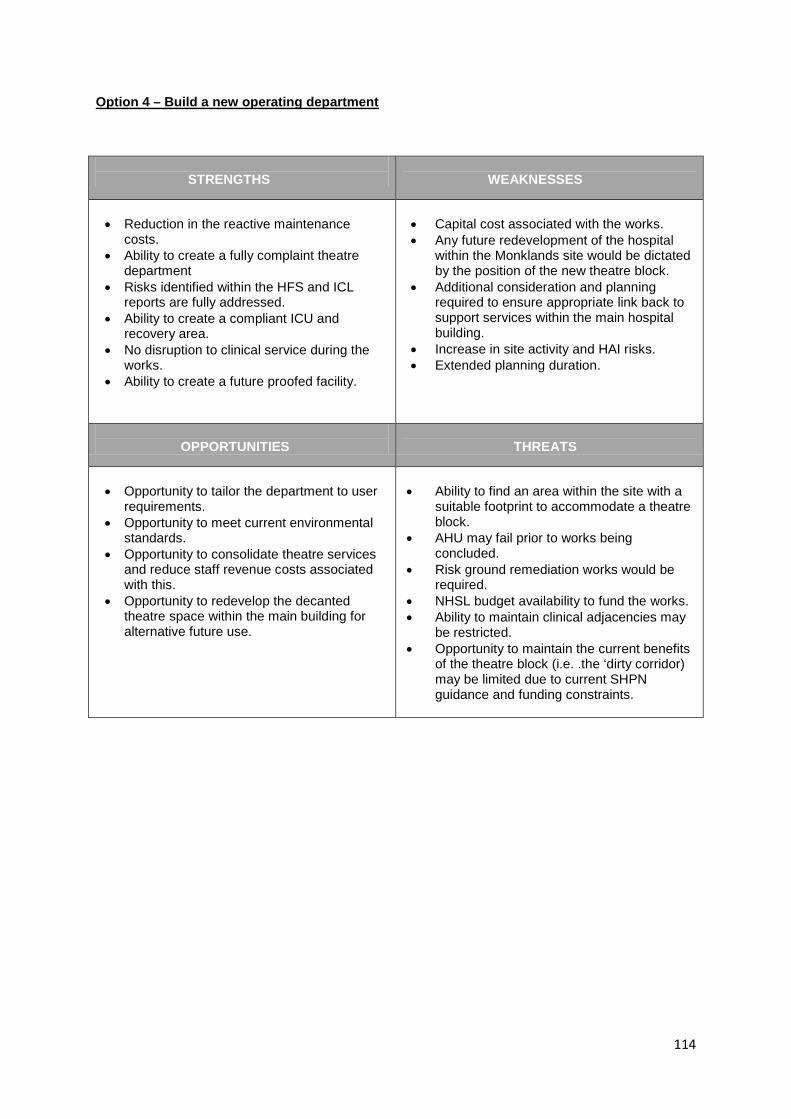
114
Option 4 – Build a new operating department
STRENGTHS
WEAKNESSES
• Reduction in the reactive maintenance
costs. • Ability to create a fully complaint theatre
department • Risks identified within the HFS and ICL
reports are fully addressed. • Ability to create a compliant ICU and
recovery area. • No disruption to clinical service during the
works. • Ability to create a future proofed facility.
• Capital cost associated with the works. • Any future redevelopment of the hospital
within the Monklands site would be dictated by the position of the new theatre block.
• Additional consideration and planning required to ensure appropriate link back to support services within the main hospital building.
• Increase in site activity and HAI risks. • Extended planning duration.
OPPORTUNITIES
THREATS
• Opportunity to tailor the department to user
requirements. • Opportunity to meet current environmental
standards. • Opportunity to consolidate theatre services
and reduce staff revenue costs associated with this.
• Opportunity to redevelop the decanted theatre space within the main building for alternative future use.
• Ability to find an area within the site with a
suitable footprint to accommodate a theatre block.
• AHU may fail prior to works being concluded.
• Risk ground remediation works would be required.
• NHSL budget availability to fund the works. • Ability to maintain clinical adjacencies may
be restricted. • Opportunity to maintain the current benefits
of the theatre block (i.e. .the ‘dirty corridor) may be limited due to current SHPN guidance and funding constraints.
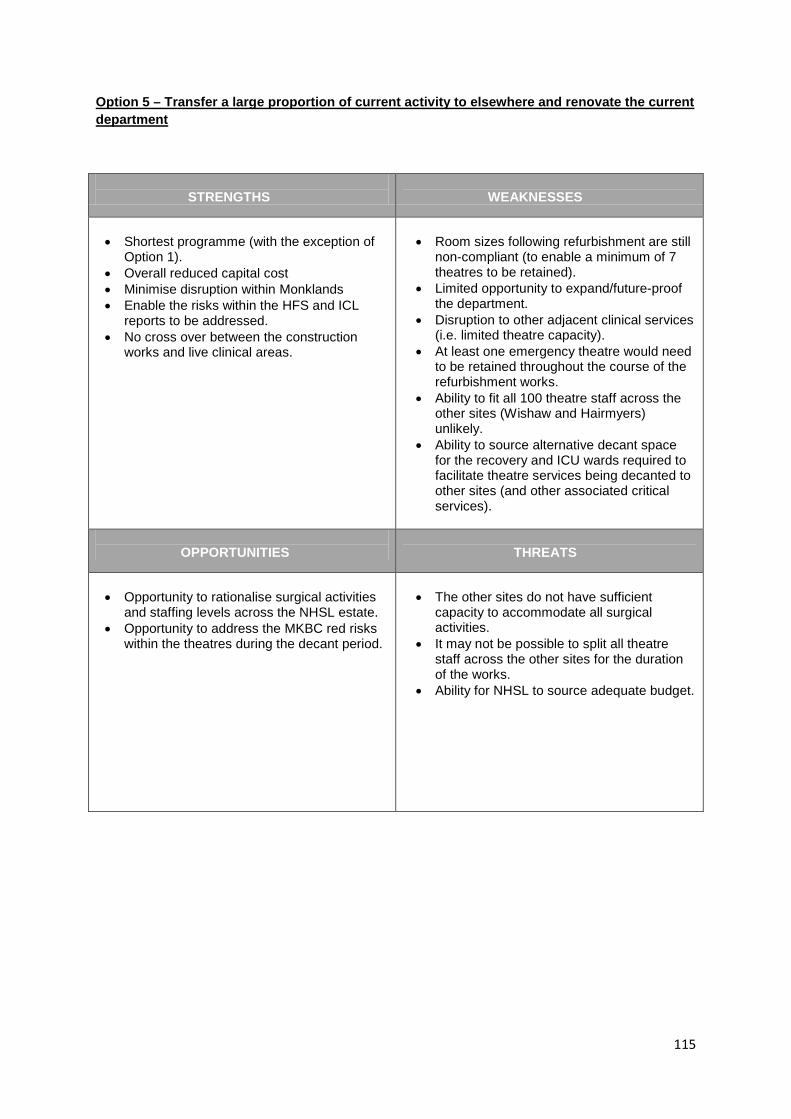
115
Option 5 – Transfer a large proportion of current activity to elsewhere and renovate the current department
STRENGTHS
WEAKNESSES
• Shortest programme (with the exception of
Option 1). • Overall reduced capital cost • Minimise disruption within Monklands • Enable the risks within the HFS and ICL
reports to be addressed. • No cross over between the construction
works and live clinical areas.
• Room sizes following refurbishment are still
non-compliant (to enable a minimum of 7 theatres to be retained).
• Limited opportunity to expand/future-proof the department.
• Disruption to other adjacent clinical services (i.e. limited theatre capacity).
• At least one emergency theatre would need to be retained throughout the course of the refurbishment works.
• Ability to fit all 100 theatre staff across the other sites (Wishaw and Hairmyers) unlikely.
• Ability to source alternative decant space for the recovery and ICU wards required to facilitate theatre services being decanted to other sites (and other associated critical services).
OPPORTUNITIES
THREATS
• Opportunity to rationalise surgical activities
and staffing levels across the NHSL estate. • Opportunity to address the MKBC red risks
within the theatres during the decant period.
• The other sites do not have sufficient
capacity to accommodate all surgical activities.
• It may not be possible to split all theatre staff across the other sites for the duration of the works.
• Ability for NHSL to source adequate budget.

116
Appendix 06:
Schedule of Accommodation
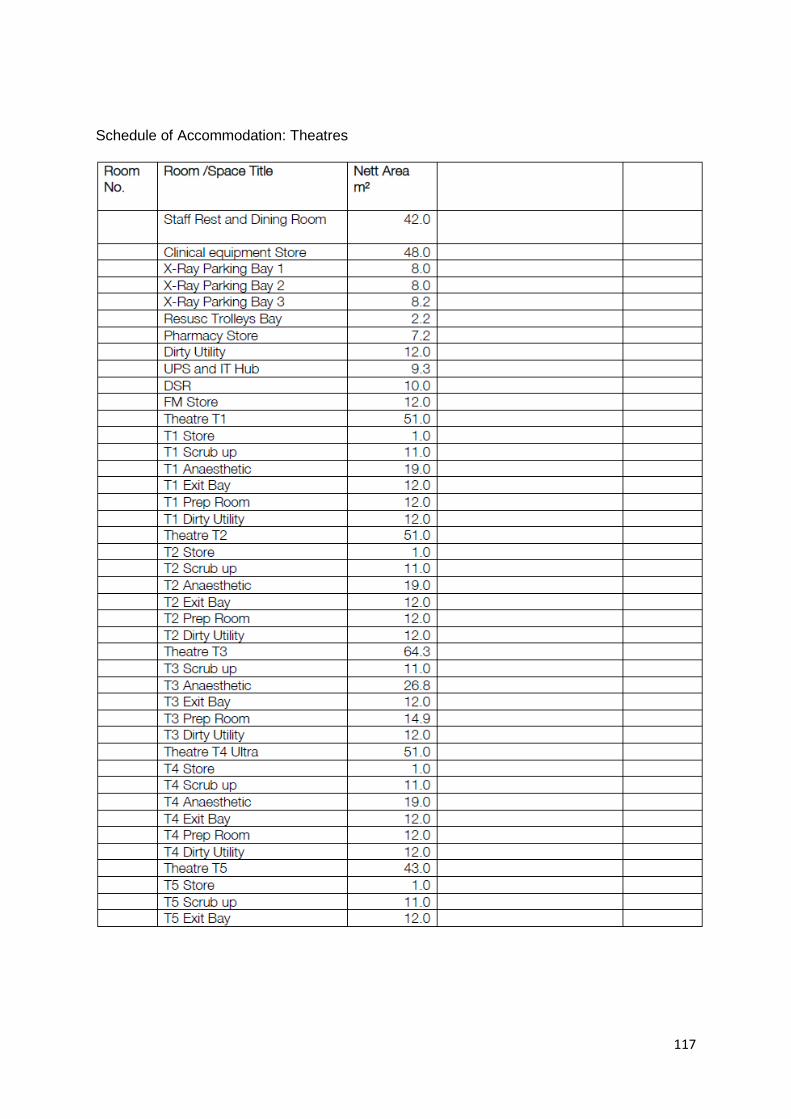
117
Schedule of Accommodation: Theatres
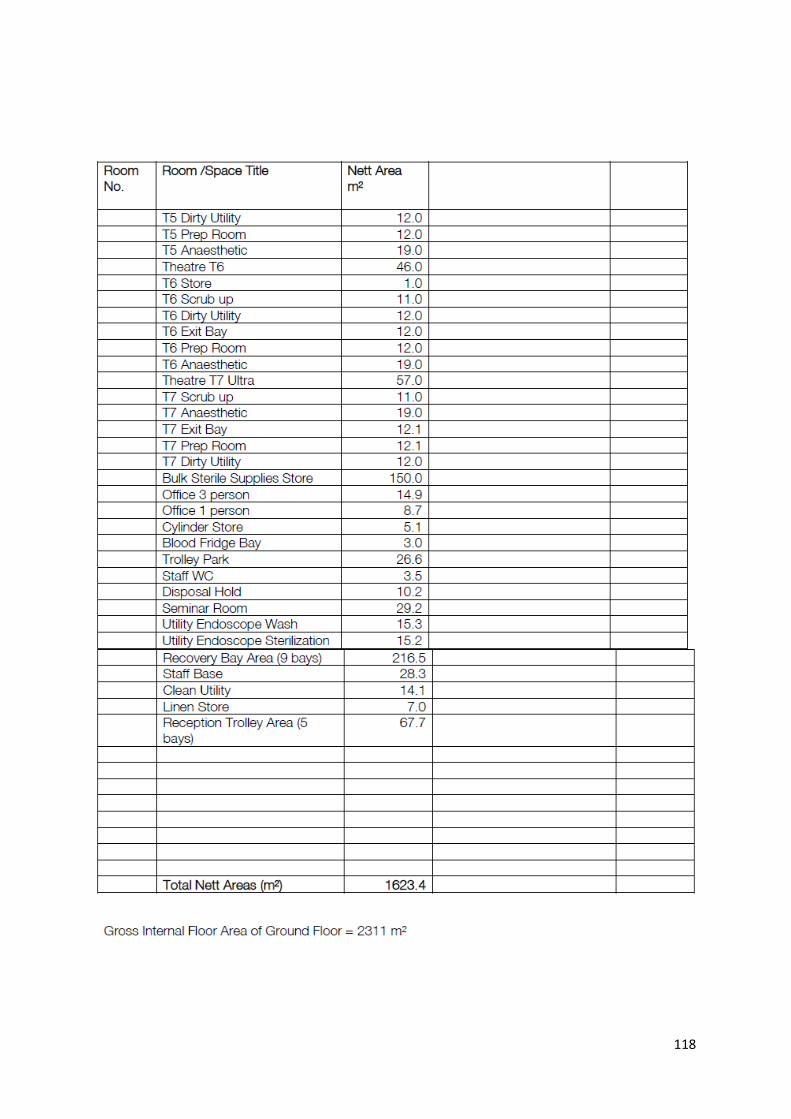
118
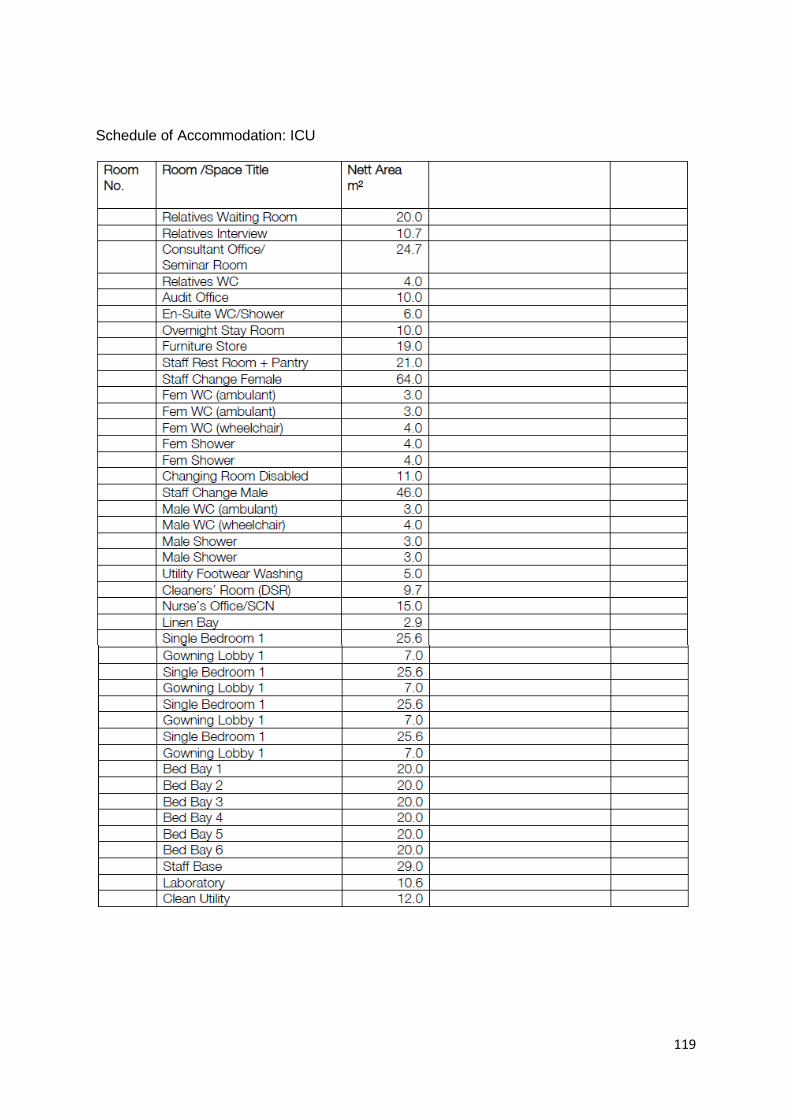
119
Schedule of Accommodation: ICU
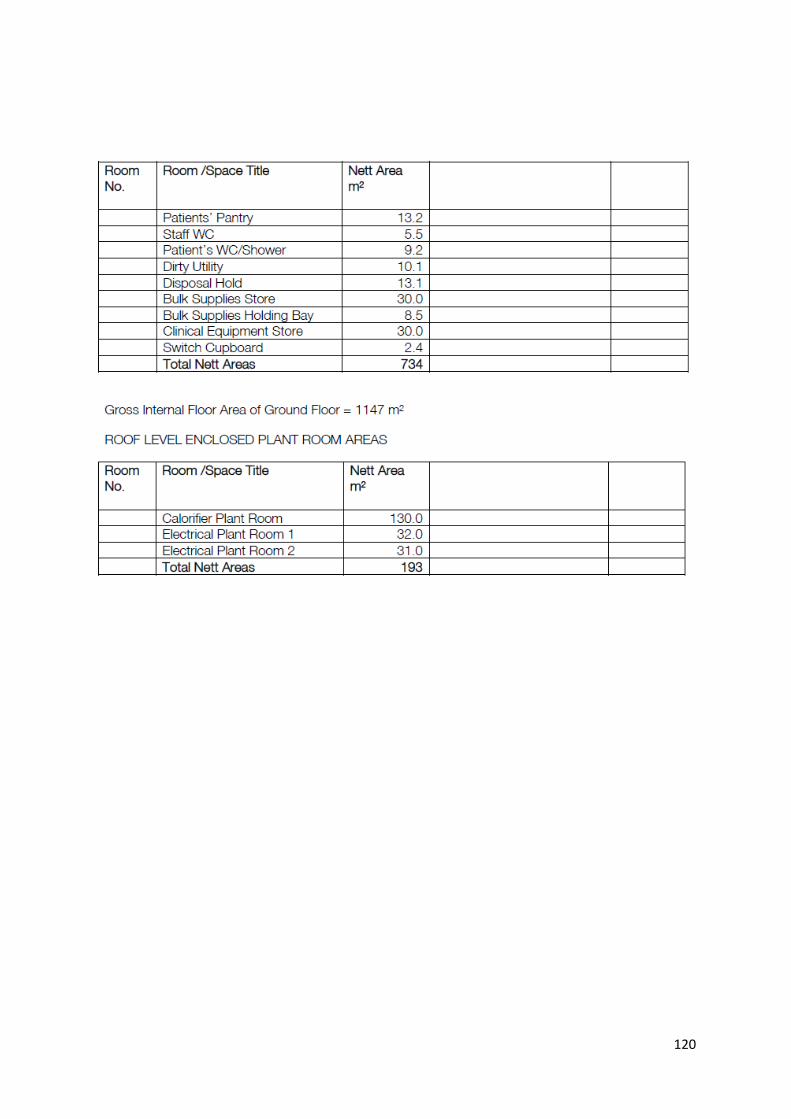
120

121
Appendix 07:
Letter of Support
[will be included in SGHSCD submission]

122
Appendix 08:
PSCP Programme
Stage 1B

123
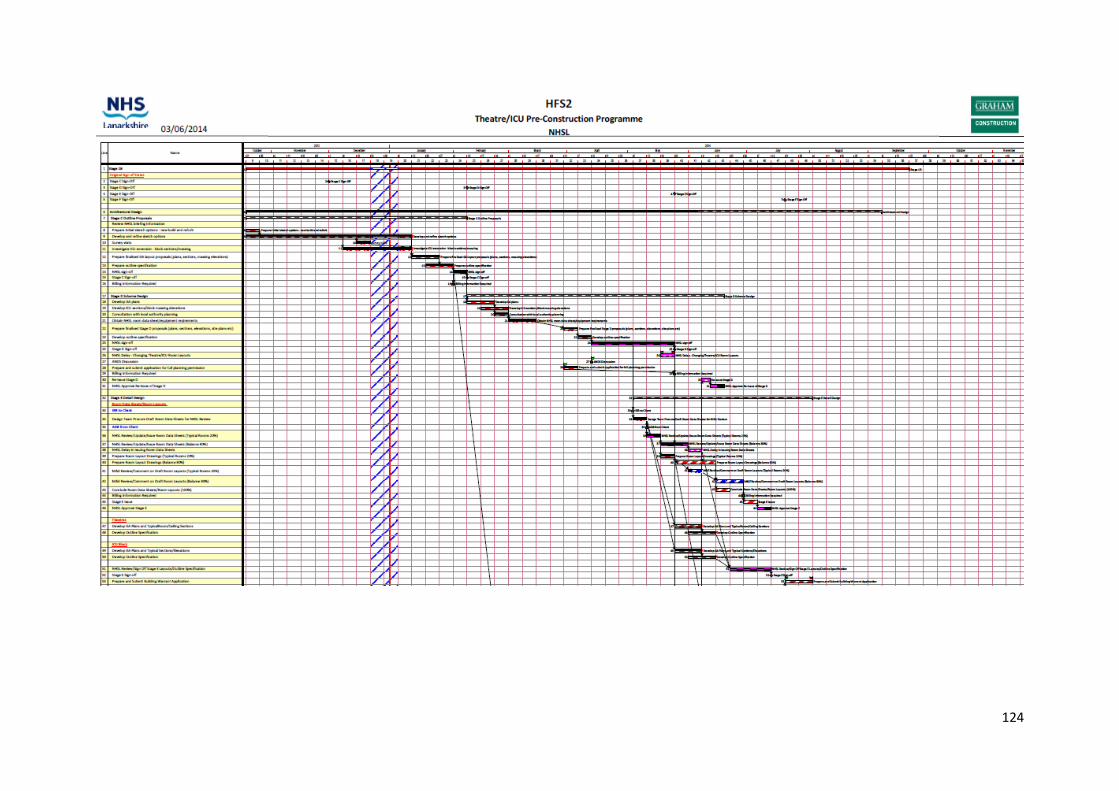
124
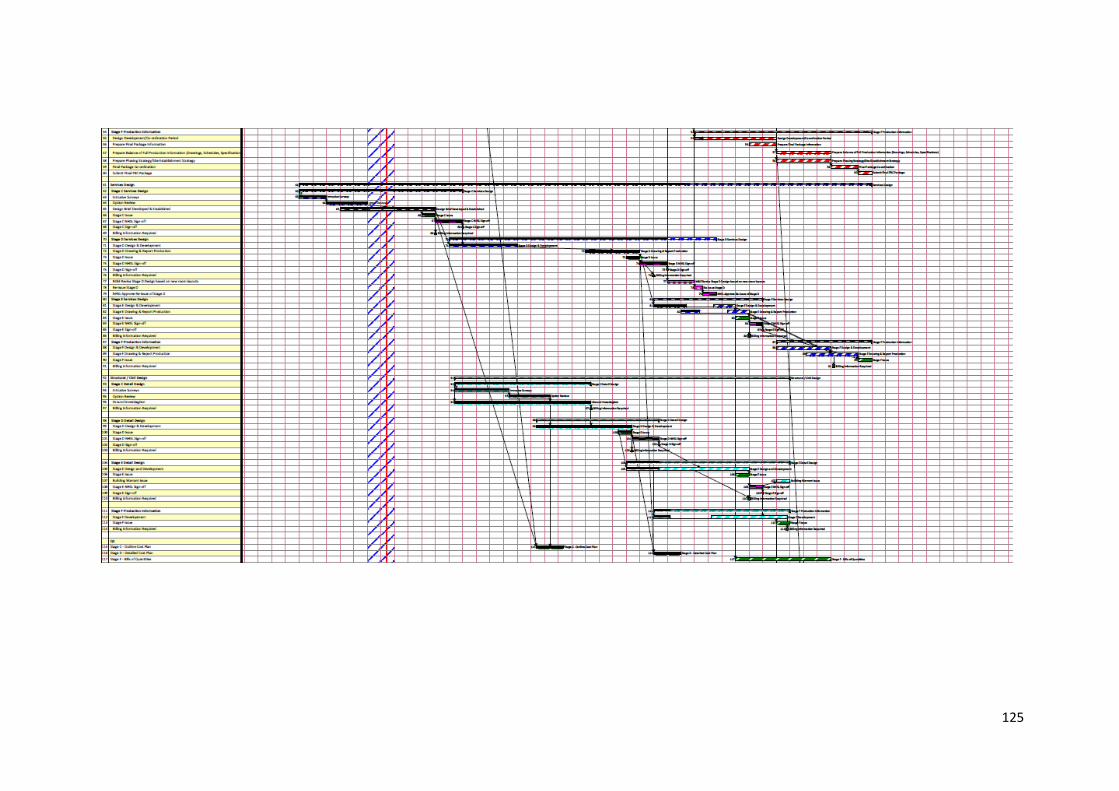
125
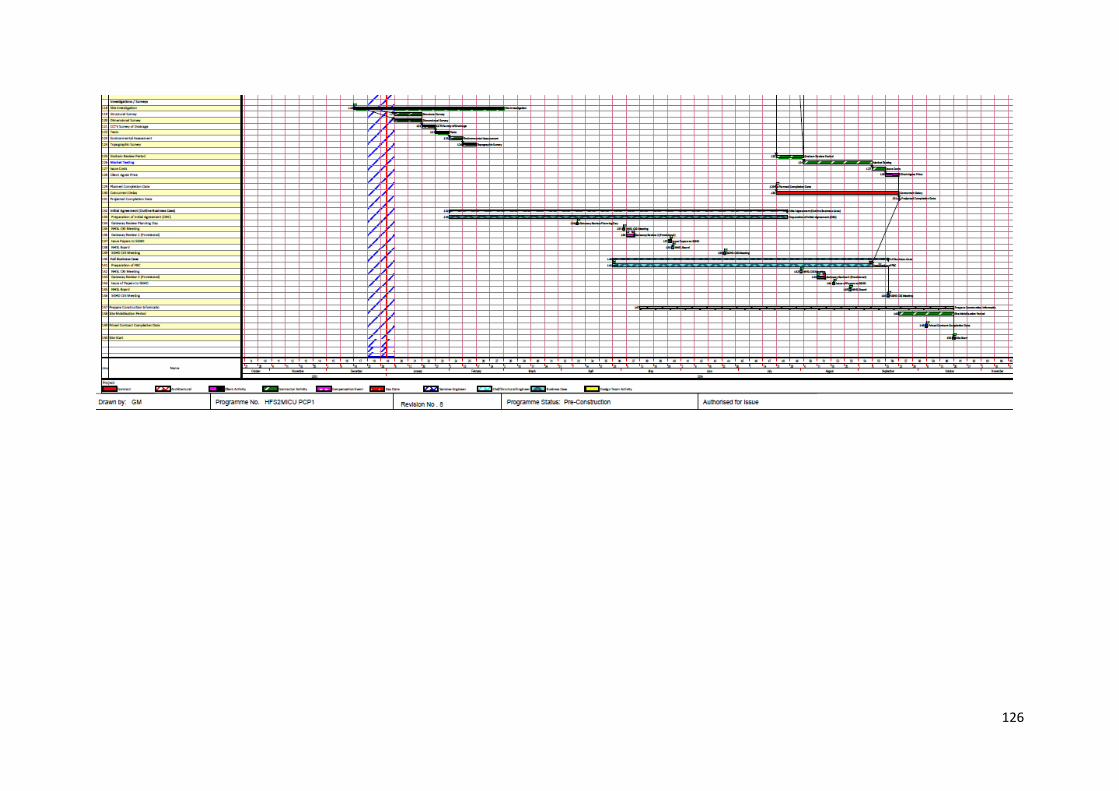
126

127
Appendix 09:
Schedule of Derogations
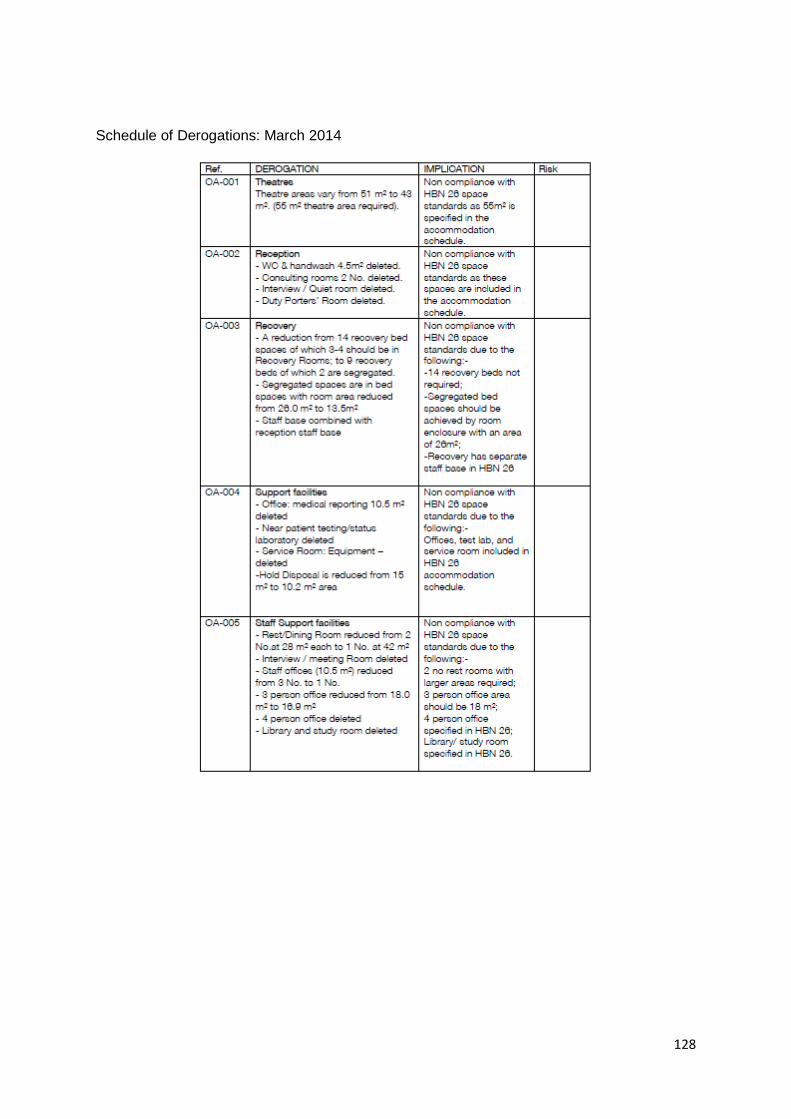
128
Schedule of Derogations: March 2014
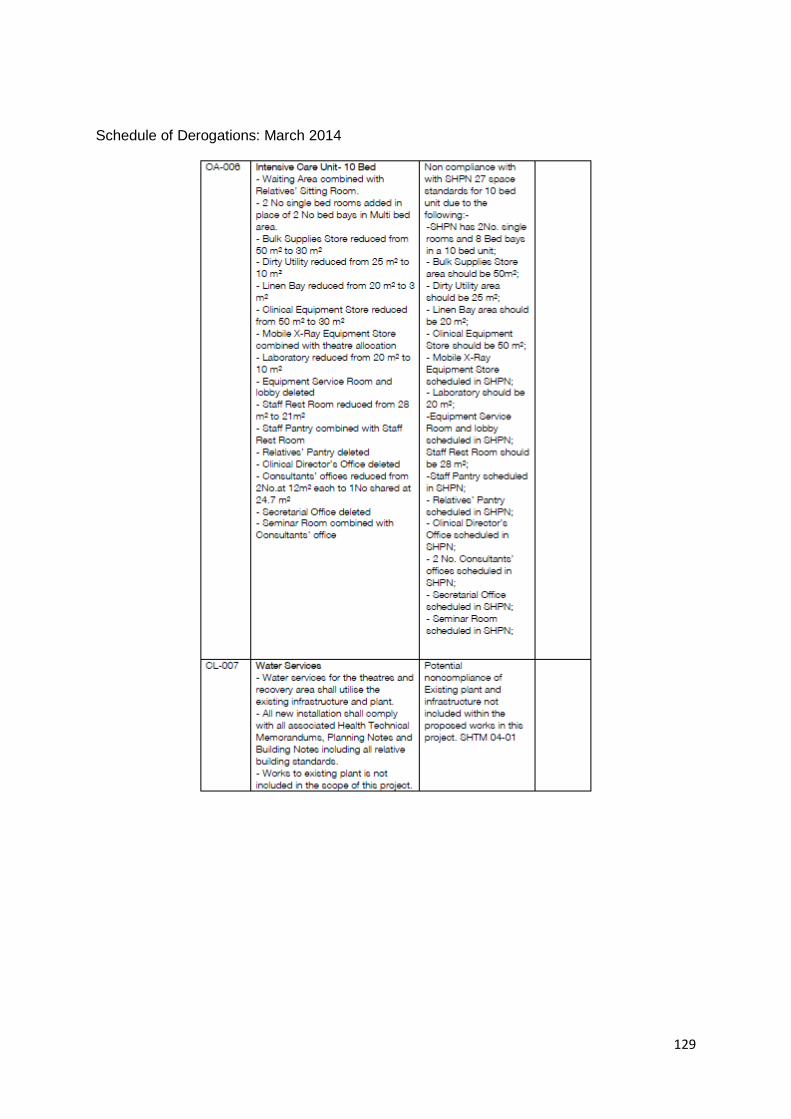
129
Schedule of Derogations: March 2014
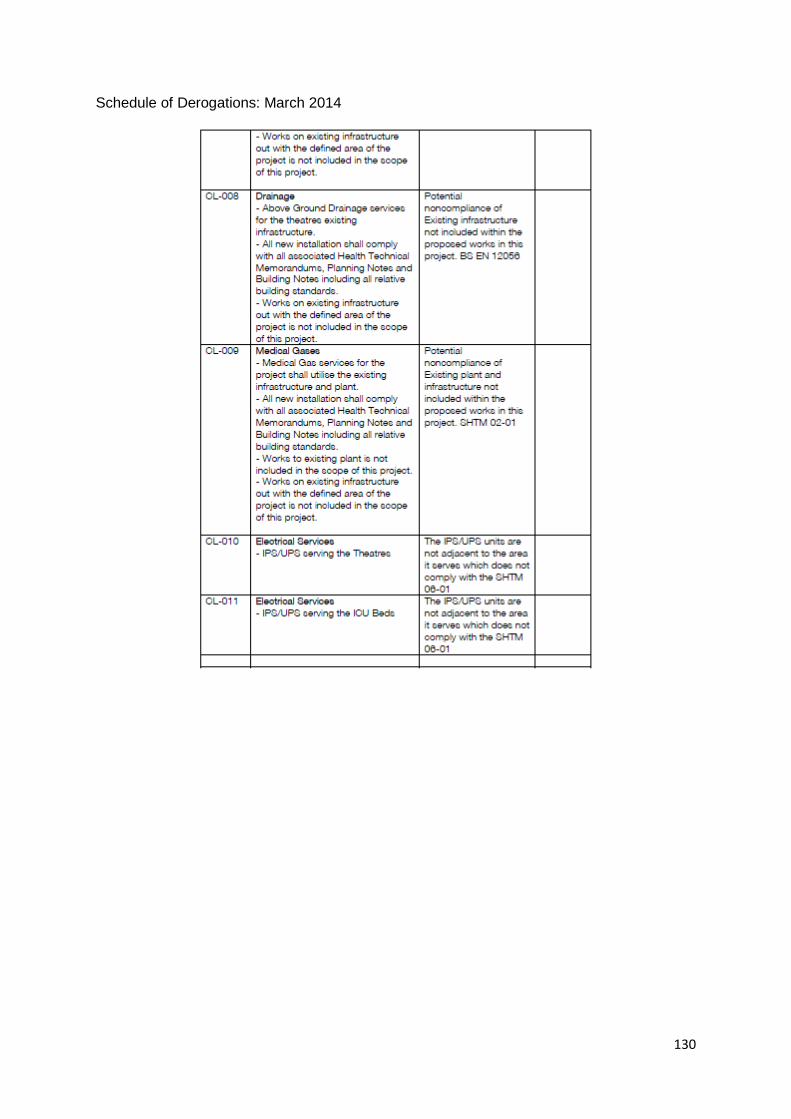
130
Schedule of Derogations: March 2014


















