Mitral Valve Prolapse MEDICINE II. General Data and HPI MM, 23 years old, female Chief Complaint:...
58
Mitral Valve Prolapse MEDICINE II
-
Upload
brett-davidson -
Category
Documents
-
view
219 -
download
0
Transcript of Mitral Valve Prolapse MEDICINE II. General Data and HPI MM, 23 years old, female Chief Complaint:...

Mitral Valve Prolapse
MEDICINE II
General Data and HPI• MM, 23 years old, female
• Chief Complaint: Palpitations
• 4 years PTA– Palpitations – irregular heart beats associated with
increased sweating and shortness of breath– Given verapamil – taken for 3 days only; subsequently
took medication intermittently for palpitations

General Data and HPI
• Few hours PTA– Experienced palpitation accompanied by
shortness of breath– Prompted consult and admission

Review of Systems
• No dizziness, nor loss of consciousness
• No coughs or colds
• No PND or orthopnea

Physical Examination• Conscious, coherent ambulatory• BP 110/70 CR: 80bpm, regular• RR: 16 cycles/min BMI: 19
• Symmetrical chest expansion, narrow A-P diameter of chest, no retractions, clear breath sound
• Adynamic precordium, AB at 5th LICS MCL no murmurs
• (+) midsystolic click followed by 2/6 crescendo-decrescendo murmur noted at the apex
Ancillary and Lab Tests
• 2D0-echo Doppler: MVP, Anterior MV leaflet with moderate MR; slightly dilated RA with no evidence of thrombus
• 12L ECG: sinus rhythm; occasional PACs
• Chest X-ray: Normal
Salient Features
• Female, 23 years old
• Palpitations
• (+) midsystolic click followed by 2/6 crescendo-decrescendo murmur noted at the apex
• BMI: 19; narrow A-P diameter of chest

Clinical Impression:
Mitral Valve Prolapse

Mitral Valve Prolapse
• Floppy-valve syndrome, Barlow’s syndrome
• Excessive connective tissue in the mitral leaflet - Elongation and thickening of the mitral valve
• Displacement of the mitral valve into the LA during systole
Mitral Valve Prolapse• Exact cause is unknown - thought to be
genetically determined collagen tissue disorder
• A frequent finding in patients with other heritable connective tissue disorders– Marfan’s Syndrome– Osteogenesis imperfecta– Ehler-Danlos Syndrome
• May occur as a sequel of ARF, Ischemic heart disease, cardiomyopathies, Ostium Secundum ASD

Mitral Valve Prolapse
• Clinical Features:– More common in females – Patients between the ages 14 and 30 years most
commonly affected– Certain body features that may be associated with
MVP:• low body weight, long arms, flat rib cage, and loose
joints • Straight back syndrome

Common Physical Examination Features

Midsystolic Click
• Classic auscultatory feature of MVP
• Elongated leaflet balloons into the left atrium during systole leaflet collapses into the atrium, producing a click
• Or produced by sudden tensing of• slack, elongated chordae tendinae
Mid- to Late Systolic Murmur
• Midsystolic click may be followed by a high-pitched mid- to late systolic murmur
• Crescendo-decrescendo, often heard best at the apex
• Prolapse of the mitral valve causes some regurgitation of blood into the left atrium
Mid- to Late Systolic Murmur
• Occurrence of click and murmur vary according to position
• In general, any maneuver that decreases the end-diastolic LV volume, increases the rate of ventricular contraction or decreases resistance to the LV ejection of blood causes MVP to occur earlier in systole (standing, valsalva maneuver)
Mid- to Late Systolic Murmur
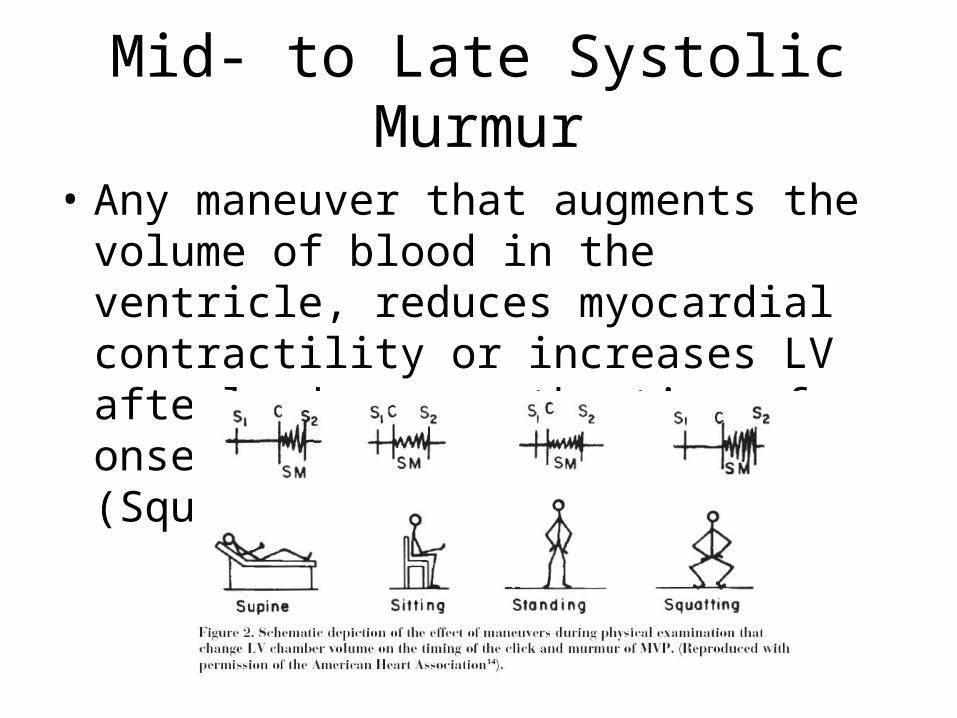
• Any maneuver that augments the volume of blood in the ventricle, reduces myocardial contractility or increases LV afterload causes the time of onset of MVP to lengthen (Squatting, supine position)

Other Findings
• Other PE findings in patients with MVP include:
– Tendency for low body weight
– Thoracic skeletal deformities – such as high-arched palate, alterations of the chest and thoracic spine

Common and Uncommon Symptoms

Common Symptoms• Fatigue – most common
– ANS- regulates heart rate and breathing. – imbalances cause inadequate blood oxygen delivery to the working muscles
during exercise
• Palpitations -harmless – In very rare cases, potentially serious heart rhythm abnormalities may
underlie palpitations which require further evaluation and treatment
• Chest pain– rarely occurs during or after exercise, and may not respond to nitorglycerin
• Anxiety, panic attacks, depression – related to imbalances of the autonomic nervous system.
• Migraine headaches– abnormal nervous system control of the tension in the blood vessels in the
brain.
Uncommon Symtoms
• Chronically cold hands and feet • Problems sleeping • Numbness and tingling of the arms or legs • Lump in throat • Difficulty swallowing • Inability to concentrate • Problems with memory or a feeling of
fogginess

Long-term Complications

Pathophysiologymyxomatous degeneration from collagen dissolution
excess mucopolysaccharides in the middle spongiosa layer of the mitral valve leaflets
stretching of the leaflets and the chordae tendineae
mitral valve prolapse


Progression or appearance of MR
Congestive Heart
Failure

Rupture of Chordae Tendineae
• MVP excessive stress on the papillary muscles dysfunction, ischemia of the papillary muscles, subjacent ventricular myocardium
• Progressive annular dilatation
• Calcification
• Stress on diseased mitral valve apparatus

Infective Endocarditis
• Infective endocarditis may also occur in patients with MR assoc w/ MVP.
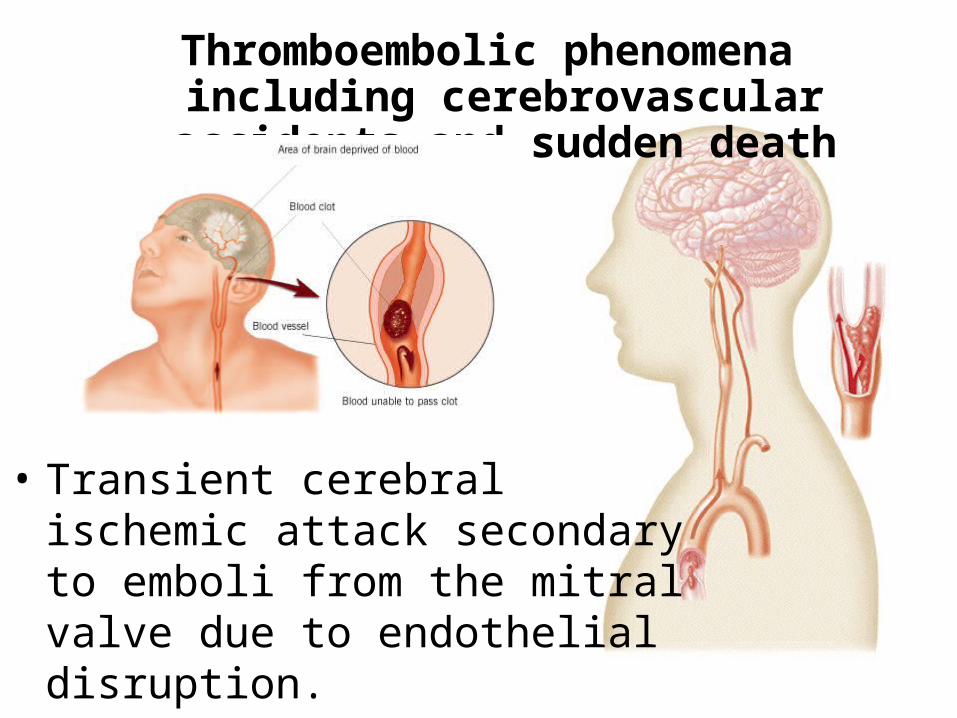
Thromboembolic phenomena including cerebrovascular accidents and sudden death
• Transient cerebral ischemic attack secondary to emboli from the mitral valve due to endothelial disruption.

Cardiac arrhythmia

Ventricular tachycardia and fibrillation
• Ventricular premature contractions• Paroxysmal supraventricular and
ventricular tachycardia• Result of regional ventricular dysfunction
related to inc stress placed on papillary muscles
Sudden death
• Rare complication• Etiology: ventricular fibrillation• Risk factors:
– Severe MR– Severe valvular deformity– LV dysfunction– Prologed QT interval– History of syncope

Population at risk

What population groups are associated with an increased predilection for MVP?
• Females > Males• Ages 14 – 30 y/o• (+) family history of MVP (autosomal
dominant), collagen tissue disorders
Increased predilection for MVP
• Elderly patients (>50 y/o)– myxomatous degeneration of the mitral valves (less commonly
affecting the TV or AV)– Usually without other clinical or pathologic manifestations of the
disease– Posterior leaflet > anterior leaflet
• Patients with elongated redundant chordae tendinae• Patients with ostium secundum ASD (20%)• Sequelae of acute RF, ischemic heart disease,
cardiomyopathies
Increased predilection to MVP
• Patients with collagen tissue disorder– Marfan syndrome (most commonly associated)– Osteogenesis imperfecta– Ehler-Danlos syndrome

Prophylactic Treatment

EndocarditisEndocarditis is a life-threatening disease, although it
is relatively uncommon. Substantial morbidity and mortality result from this
infection, despite antimicrobial therapy and enhanced ability to diagnose and treat complications. Primary prevention of endocarditis whenever possible is
therefore very important. Endocarditis usually develops in individuals with
underlying structural cardiac defects who develop bacteremia with organisms likely to cause endocarditis.
Bacteremia
• Bacteremia commonly occurs during activities of daily living such as routine tooth brushing or chewing.
• With respect to endocarditis prophylaxis, significant bacteremia is only those caused by organisms commonly associated with endocarditis and attributable to identifiable procedures.
• The procedures for which prophylaxis is recommended are those known to induce bacteremia
• Invasive procedures performed through surgically scrubbed skin are NOT likely to produce bacteremia.

Bacteremia
• Bacteremia may occur spontaneously or may complicate a focal infection – urinary tract infection– pneumonia– cellulitis
• Blood-borne bacteria may lodge on damaged or abnormal heart valves, endocardium or the endothelium near anatomic defects resulting in bacterial endocarditis or endarteritis.
Endocarditis prophylaxis recommended
• High-risk category • Prosthetic cardiac valves • Previous bacterial endocarditis • Complex cyanotic congenital heart disease
– single ventricle states– transposition of the great arteries– tetralogy of Fallot
• Surgically constructed systemic pulmonary shunts or conduits

Endocarditis prophylaxis recommended
• Moderate-risk category • Acquired valvular dysfunction (eg, rheumatic
heart disease) • Hypertrophic cardiomyopathy • Mitral valve prolapse with valvular
regurgitation and/or thickened leaflets

Endocarditis prophylaxis NOT recommended
• Negligible-risk category • Isolated secundum atrial septal defect • Surgical repair of ASD, VSD or PDA• Previous coronary artery bypass graft surgery • Mitral valve prolapse without valvular regurgitation • Physiologic, functional, or innocent heart murmurs • Previous Kawasaki disease without valvular dysfunction • Previous rheumatic fever without valvular dysfunction • Cardiac pacemakers and implanted defibrillators

Copyright ©1997 American Heart Association
Dajani, A. S. et al. Circulation 1997;96:358-366
Clinical approach to determination of the need for prophylaxis in patients with suspected mitral valve prolapse

Dental and Oral Procedures• Poor dental hygiene and periodontal or periapical infections may
produce bacteremia even in the absence of dental procedures. • The incidence and magnitude of bacteremia of oral origin are
directly proportional to the degree of oral inflammation and infection.
• Individuals who are at risk for developing bacterial endocarditis should establish and maintain the best possible oral health to reduce potential sources of bacterial seeding. Optimal oral health is maintained through regular professional care
• Pallasch TJ, Slots J. Antibiotic prophylaxis and the medically compromised patient. Periodontol 2000. 1996;10:107-138

Dental and Oral Procedures
• Prophylaxis is recommended • procedures associated with significant bleeding
from hard or soft tissues, periodontal surgery, scaling, and professional teeth cleaning.
• for tonsillectomy or adenoidectomy. • unanticipated bleeding may occur on some
occasions. – antimicrobial prophylaxis administered within 2 hours
following the procedure will provide effective prophylaxis
Respiratory Procedures
• Surgical procedures involving the respiratory mucosa may lead to bacteremia, antimicrobial prophylaxis is recommended
• a rigid bronchoscope may cause mucosal damage, whereas such damage is unlikely with a flexible bronchoscope.
• Endotracheal intubation is NOT an indication for antibiotic prophylaxis.

Gastrointestinal Procedures
The risk of endocarditis as a direct result of an endoscopic procedure is small. Transient bacteremia may occur during or immediately after
endoscopy; however, there are few reports of infective endocarditis attributable to endoscopy
Esophageal stricture dilation has been associated with bacteremia rates as high as 45%
The bacteremia rate associated with sclerotherapy of esophageal varices is approximately 31%
An obstructed biliary tree, due to benign or malignant disease, may be colonized with a variety of organisms

Genitourinary Tract Procedures The genitourinary tract is second only to the oral cavity
as a portal of entry for organisms that cause endocarditis.
The rate of bacteremia following urinary tract procedures is high in the presence of urinary tract infection.
Sterilization of the urinary tract with antimicrobial therapy in patients with bacteriuria should be attempted prior to elective procedures, including lithotripsy.
A preprocedure urine culture will allow the practitioner to choose appropriate antibiotics

• Many procedures involving the urethra and prostatic bed are associated with high rates of bacteremia
• An antimicrobial regimen effective against the infective urinary pathogen, eg, enteric gram-negative bacilli, in addition to the enterococcus, should be administered before the invasive genitourinary procedures.
• antibiotic prophylaxis for normal vaginal delivery is not recommended. If an unanticipated bacteremia is suspected during vaginal delivery, intravenous antibiotics can be administered at that time
• Sugrue D, Blake S, Troy P, MacDonald D. Antibiotic prophylaxis against infective endocarditis after normal delivery: is it necessary? Br Heart J. 1980;44:499-502
Cardiac SurgeryPatients who have cardiac conditions that predispose
them to endocarditis are at risk for developing bacterial endocarditis when undergoing open heart surgery.
patients who undergo surgery for placement of prosthetic heart valves or prosthetic intravascular or intracardiac materials are also at risk for the development of bacterial endocarditis.
the morbidity and mortality of endocarditis in such patients are high, perioperative prophylactic antibiotics are recommended.
Endocarditis associated with open heart surgery is most often caused by S aureus, coagulase-negative staphylococci, or diphtheroids

Prophylaxis
• Prophylaxis at the time of cardiac surgery should be directed primarily against staphylococci and should be of short duration.
• First-generation cephalosporins are most often used, but the choice of an antibiotic should be influenced by the antibiotic susceptibility patterns at each hospital.
Prophylaxis
Prophylaxis is most effective when given perioperatively in doses that are sufficient to assure adequate antibiotic concentrations during and after the procedure.
Antibiotics should be used only during the peri-operative period.
They should be initiated shortly before a procedure and should not be continued no more than 6 to 8 hours.
In the case of delayed healing, or of a procedure that involves infected tissue, it may be necessary to provide additional doses of antibiotics
Prophylaxis
• Streptococcus viridans is the most common cause of endocarditis following: – dental or oral procedures– certain upper respiratory tract procedures– bronchoscopy with a rigid bronchoscope– surgical procedures that involve the respiratory
mucosa– esophageal procedures

Prophylaxis
• The recommended standard prophylactic regimen for all these procedures is a single dose of oral amoxicillin to be administered 1 hour before the anticipated procedure
• adult dose is 2.0 g• pediatric dose is 50 mg/kg (not to exceed adult
dose) • For individuals who are unable to take or unable to
absorb oral medications, parenteral Ampicillin sodium is recommended

Prophylaxis
• Individuals who are allergic to penicillin should be treated with alternative oral regimens. – Clindamycin hydrochloride is one alternative – Azithromycin or clarithromycin are also acceptable
alternative agents • When parenteral administration is needed in an
individual who is allergic to penicillin, clindamycin phosphate is recommended
• Durack DT. Prevention of infective endocarditis. N Engl J Med. 1995;332:38-44
Prophylaxis
• Bacterial endocarditis that occurs following genitourinary and gastrointestinal tract surgery or instrumentation is most often caused by Enterococcus faecalis
• antibiotic prophylaxis to prevent endocarditis that occurs following genitourinary or gastrointestinal procedures should be directed primarily against enterococci.

Prophylaxis
• High-risk patients– Ampicillin plus gentamicin
• High-risk patients allergic to ampicillin/amoxicillin– Vancomycin plus gentamicin
• Moderate-risk patients– Amoxicillin or ampicillin
• Moderate-risk patients allergic to ampicillin/amoxicillin– Vancomycin
• Durack DT. Prevention of infective endocarditis. N Engl J Med. 1995;332:38-44

THANK YOU!