
Minimally Invasive Surgery Task Decomposition - Etymology of Endoscopic Suturing
32
Minimally Invasive Surgery Task Decomposition - Etymology of Endoscopic Suturing Jacob Rosen* Ph.D., Lily Chang** MD, Jeff Brown ***, Andy Isch** MD Blake Hannaford* Ph.D., Mika Sinanan** MD Ph.D., Richard Satava** MD * Department of Electrical Engineering ** Department of Surgery *** Department of Bioengineering University of Washington Seattle, Washington
description
Minimally Invasive Surgery Task Decomposition - Etymology of Endoscopic Suturing. Jacob Rosen* Ph.D., Lily Chang** MD, Jeff Brown ***, Andy Isch** MD Blake Hannaford* Ph.D., Mika Sinanan** MD Ph.D., Richard Satava** MD * Department of Electrical Engineering ** Department of Surgery - PowerPoint PPT Presentation
Transcript of Minimally Invasive Surgery Task Decomposition - Etymology of Endoscopic Suturing

Minimally Invasive Surgery Task Decomposition -
Etymology of Endoscopic Suturing
Jacob Rosen* Ph.D.,
Lily Chang** MD, Jeff Brown ***, Andy Isch** MD
Blake Hannaford* Ph.D., Mika Sinanan** MD Ph.D., Richard Satava** MD
* Department of Electrical Engineering
** Department of Surgery
*** Department of Bioengineering
University of Washington
Seattle, Washington

Surgery - The Big Picture
Surgeon
Virtual Reality
Tool Tissue
Reality
Robot(master-slave)
HapticDevice TissueTool
Human - Machine Interface
Evaluation of Surgical Skill

Surgery - The Hidden Language Metaphor
Surgeon
HMI
Resident
Robot / Tool
Target Patient
Tool
Operator
LanguageLanguage

Surgery - The Hidden Language Elements
Human Language Surgical Language Markov Model
Book Operation Multiple Models
Chapter Step of the Operation Single Model
Words Tool/Tissue Interaction State
Pronunciation Force / Torque Observation
Research Aim
Create new quantitative knowledge of the forces and torques (F/T) applied by surgeons to their instruments and the positions and orientations (P/O) of the endoscopic tools during minimally invasive surgery
Develop and evaluate an objective surgical skill scale based multi finite state models (Markov Model) incorporating information regarding the kinematics and the dynamics of the endoscopic tools

Instrumented Endoscopic Grasper

Blue DRAGON

Blue DRAGON

Blue DRAGON - Graphical User Interface

Experimental System
PC (A/D)
VCR(PIP Mode)
Video
Blue DRAGONLeft
Contact
R
FMMMFFF
gzyx
gzyxzyx
,,,,
,,,,,,
Blue DRAGONRight
Endoscope
GUI
Mixer
Data
13 (Channels) * 2 (Dragons) = 26 Channels

Experimental Protocol
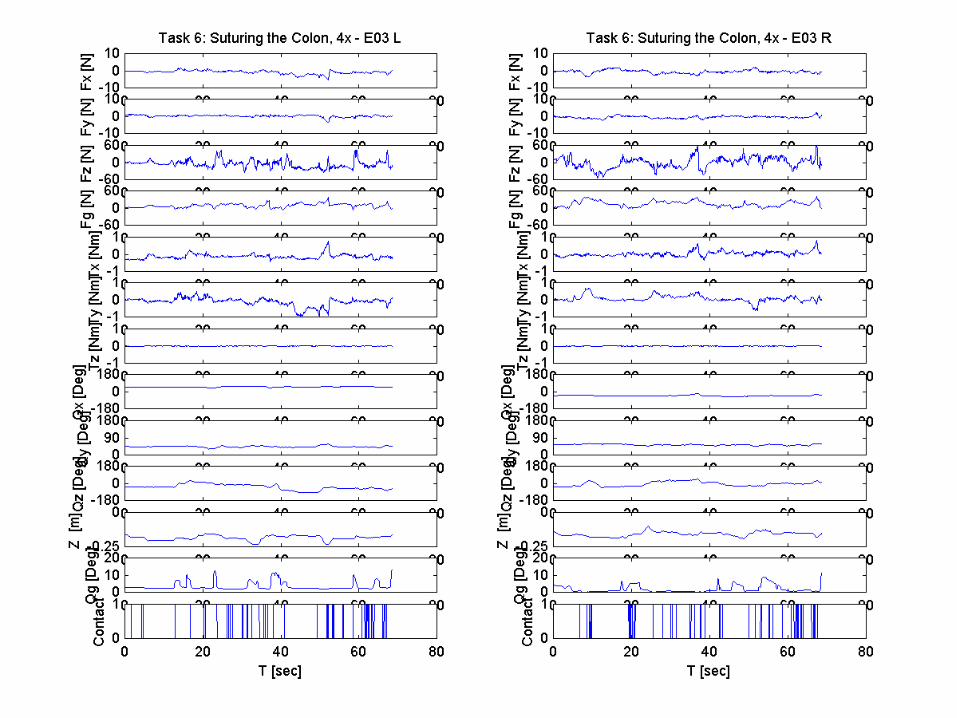
Surgical Tasks:
Task 1: Running the bowel, 10x3” (right to left) Task 2: Running the bowel, 10x3” (left to right) Task 3: Dissecting Mesenteric Vessels, 4x Task 4: Passing a Suture, 5x Task 5: Tying a Knot, 4x Task 6: Suturing the Bowel and Tying a Knot Task 7: Passing Stomach Fundus behind the Esophagus, 1x
Subjects: 5x (R1, R2, R3, R4, R5, E) - 30 Subjects
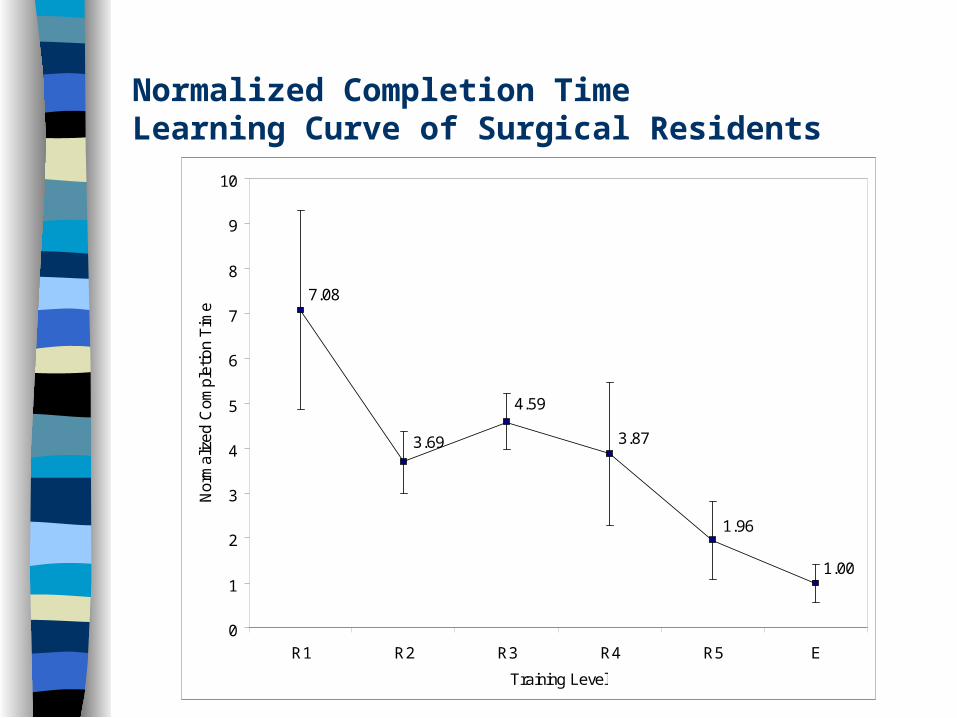
Normalized Completion TimeLearning Curve of Surgical Residents
1.00
1.96
3.87
4.59
3.69
7.08
0
1
2
3
4
5
6
7
8
9
10
R1 R2 R3 R4 R5 E
Training Level
Nor
mal
ized
Com
plet
ion
Tim
e

Novice
Expert
Position (Path) - Raw Data
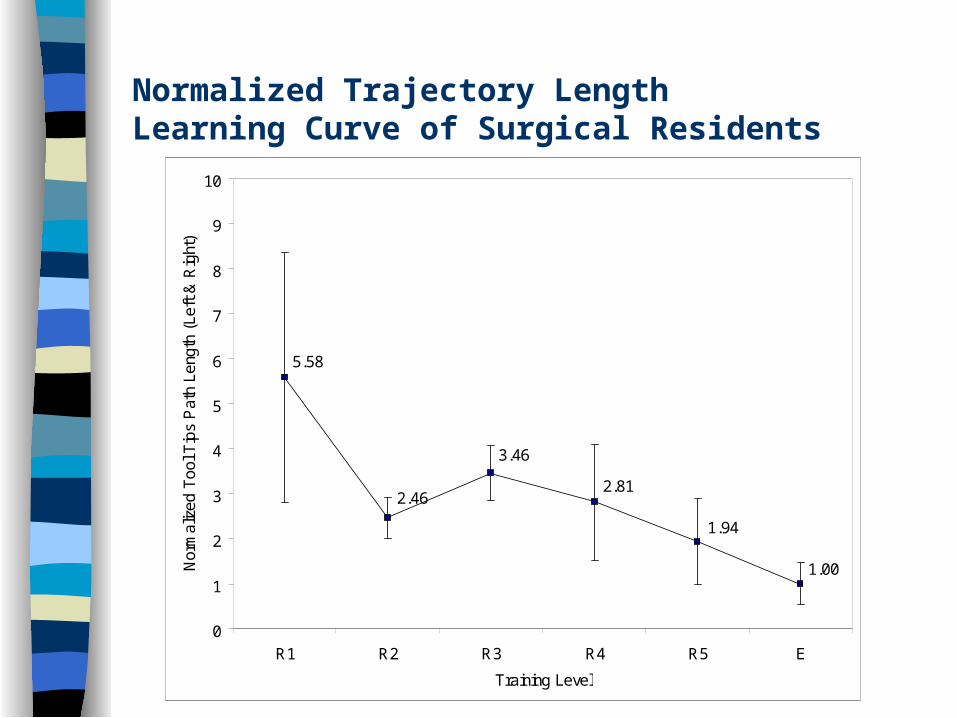
Normalized Trajectory LengthLearning Curve of Surgical Residents
1.00
1.94
2.81
3.46
2.46
5.58
0
1
2
3
4
5
6
7
8
9
10
R1 R2 R3 R4 R5 E
Training Level
Nor
mal
ized
Too
l Tip
s P
ath
Leng
th (
Left
& R
ight
)

Novice
Expert
Forces - Raw Data

Novice
Expert
Torques - Raw Data
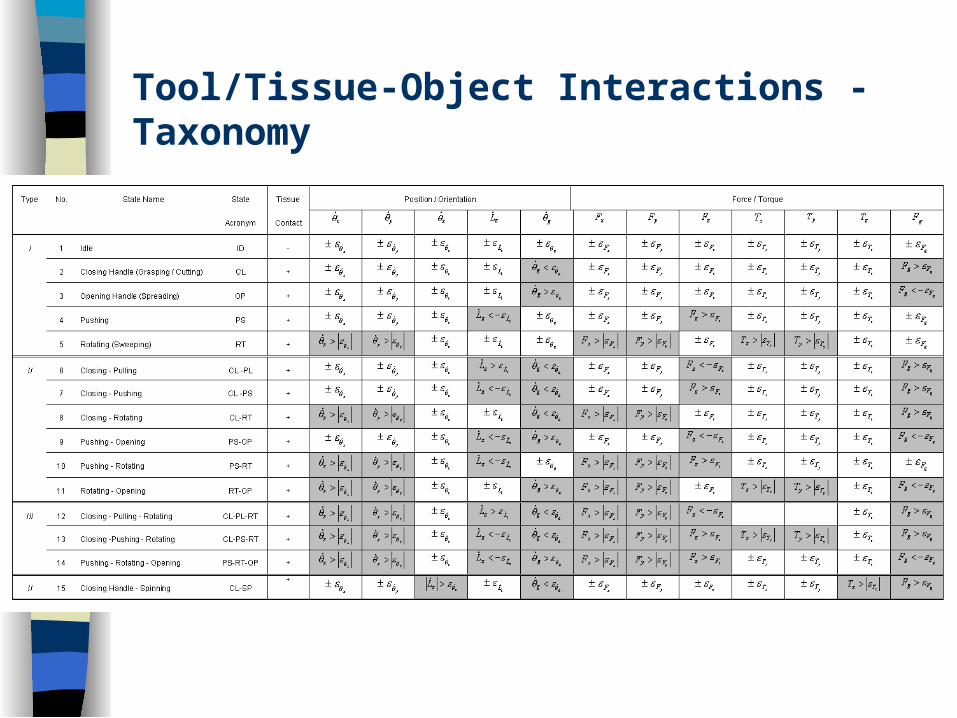
Tool/Tissue-Object Interactions - Taxonomy
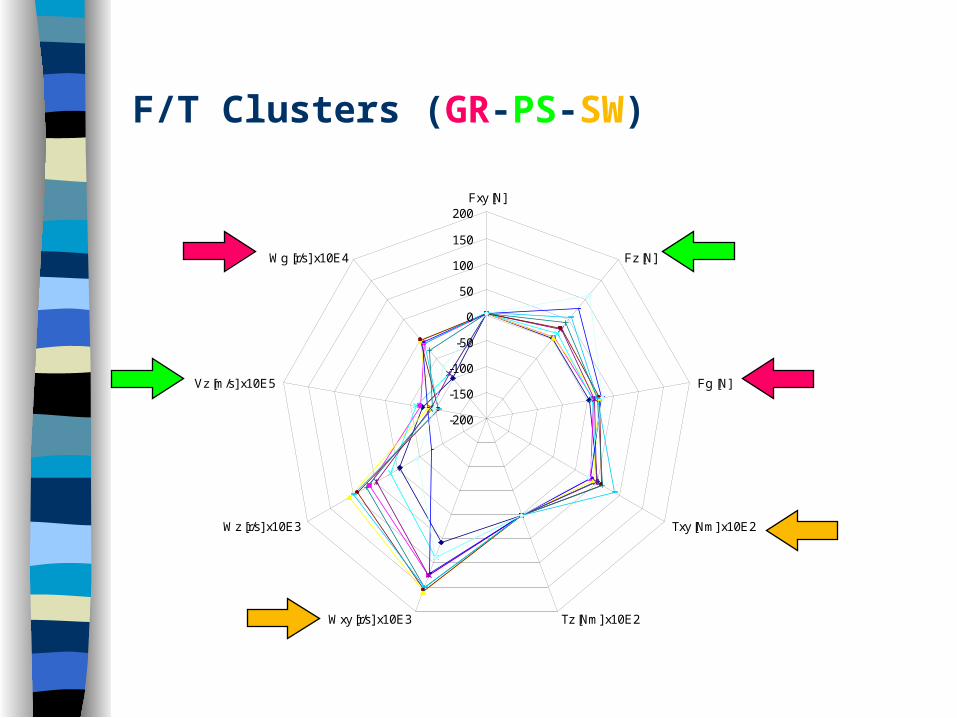
-200
-150
-100
-50
0
50
100
150
200Fxy [N]
Fz [N]
Fg [N]
Txy [Nm] x10E2
Tz [Nm] x10E2Wxy [r/s] x10E3
Wz [r/s] x10E3
Vz [m/s] x10E5
Wg [r/s] x10E4
F/T Clusters (GR-PS-SW)
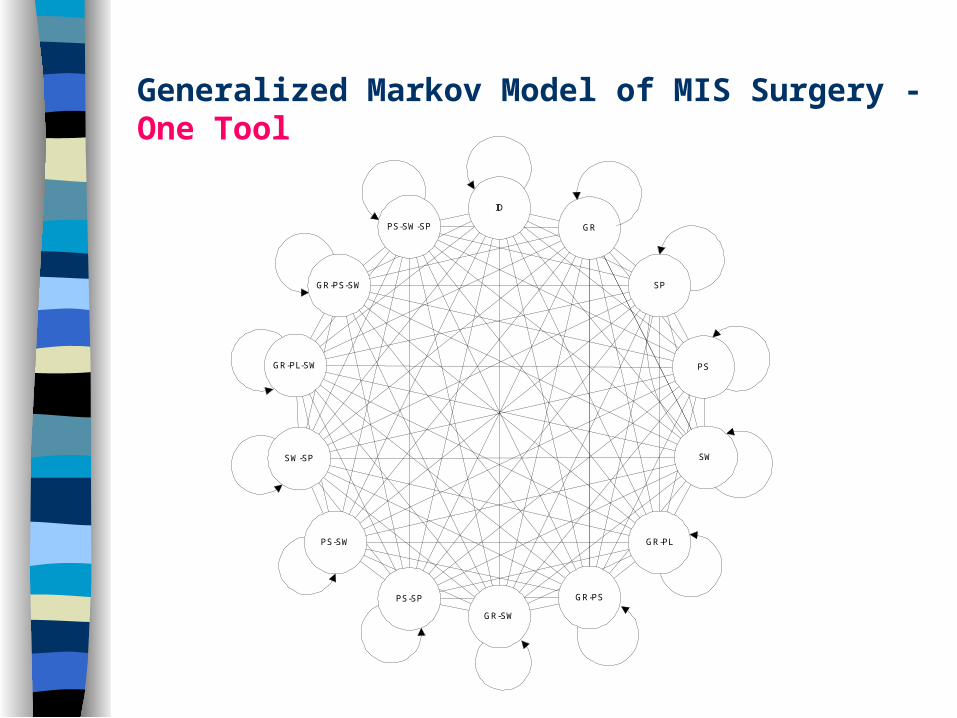
Generalized Markov Model of MIS Surgery - One Tool
GR
ID
PS-SW-SP
GR-PS-SW
GR-PL-SW
SW-SP
PS-SW
PS-SP
GR-SW
GR-PS
GR-PL
SW
PS
SP

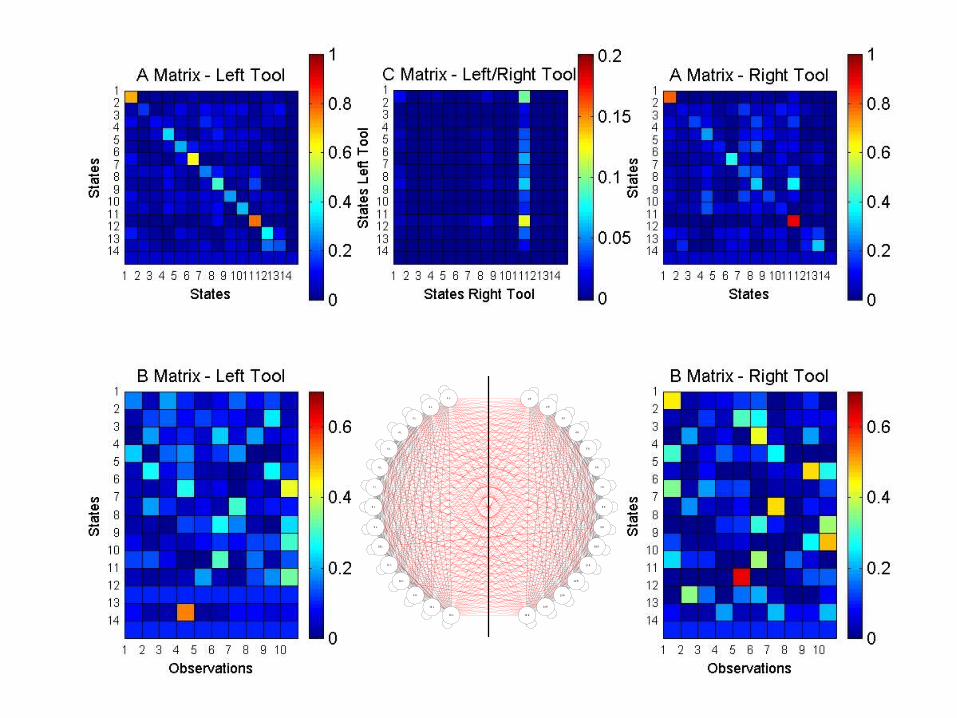
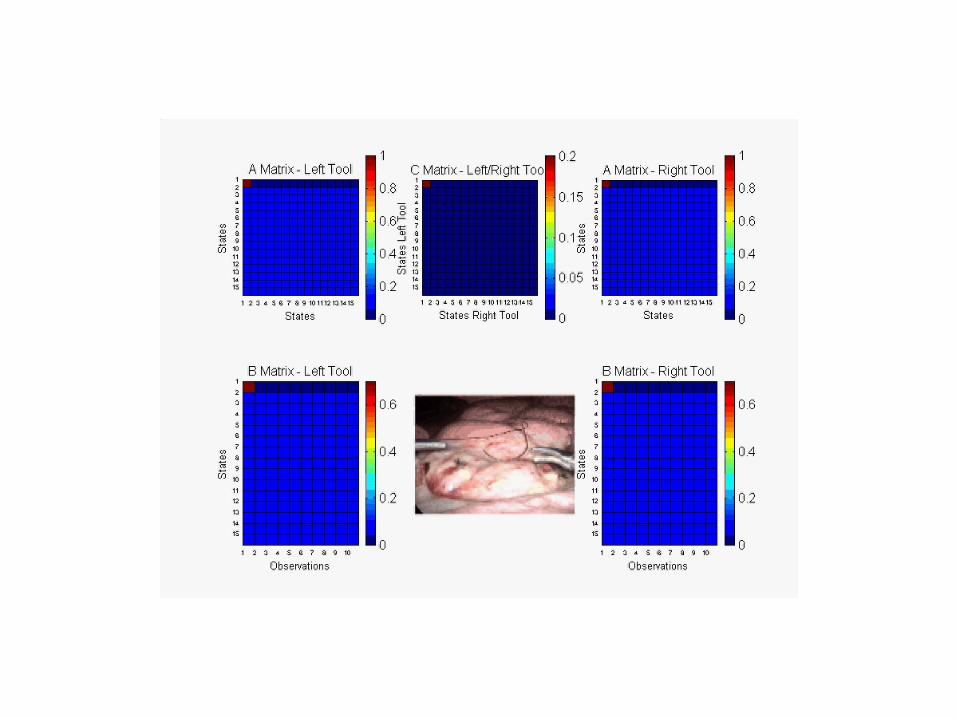
Generalized Markov Model of MIS Surgery - Two Tools
Right ToolLeft Tool1 R
2 R
3 R
4 R
5 R
6 R
8 R
9 R
10 R
11 R
12 R
13 R
14 R
15 R15 L
14 L
13 L
12 L
11 L
10 L
9 L
8 L
7 L
6 L
5 L
4 L
3 L
2 L
1 L
7 R

Laparoscopic CholecystectomyExposure of Cystic Duct
SurgeonNon - Surgeon
GR
ID
PS-SW-SP
GR-PS-SW
GR-PL-SW
SW-SP
PS-SW
PS-SP
GR-SW
GR-PS
GR-PL
SW
PS
1 R
2 R
3 R
4 R
5 R
6 R
8 R
9 R
10 R
11 R
12 R
13 R
14 R
15 R15 L
14 L
13 L
12 L
11 L
10 L
9 L
8 L
7 L
6 L
5 L
4 L
3 L
2 L
1 L
7 R
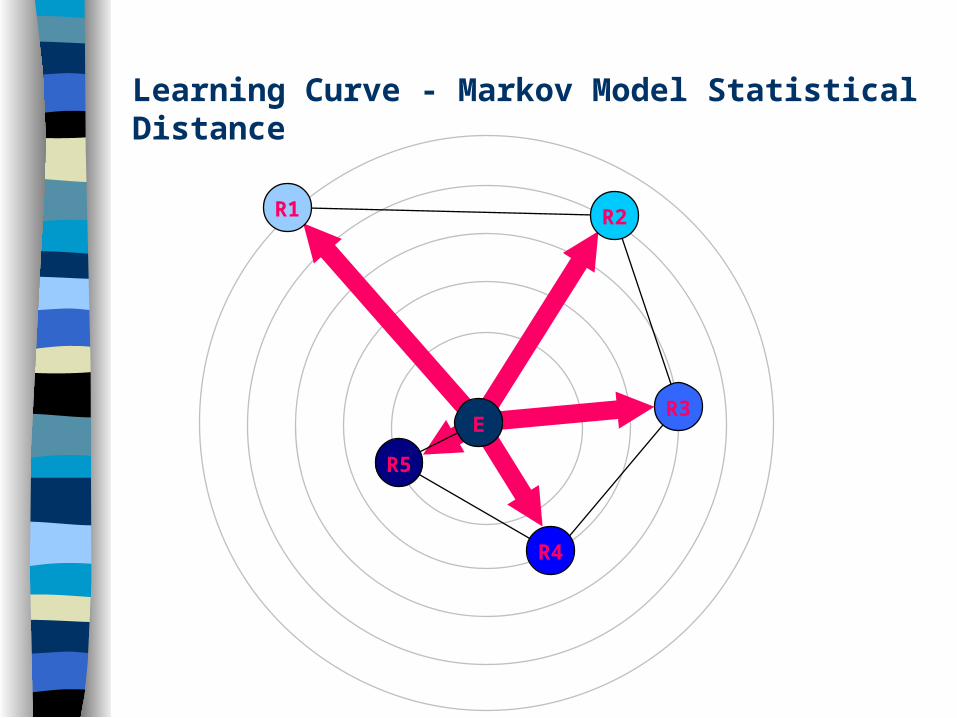
Learning Curve - Markov Model Statistical Distance
R1 R2
R3
R4
R5
E

Normalized Statistical DistanceLearning Curve of Surgical Residents
1.0000
1.9972
5.07734.5722
3.8967
8.3436
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
R1 R2 R3 R4 R5 E
Training Level
Nor
mal
ized
Sta
tistic
al D
ista
nce
(Mar
kov
Mod
els)
Subjective Score (Video Analysis) - CriteriaSuturing the Bowel and Tying a Knot
Overall performance [1-5] Economy of movement [1-5] Tissue handling [1-5] Numbers of errors [No.]
– Drop needle– Drop suture– Lose suture loop– Break suture– Needle injury to adjacent tissue– Inability to puncture bowel with needle
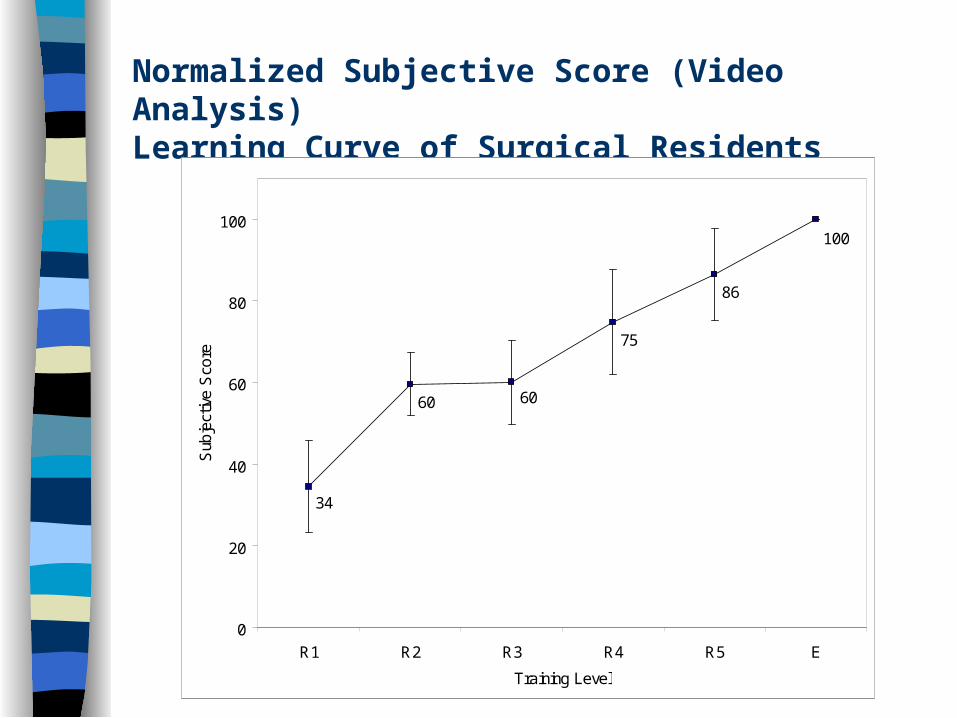
Normalized Subjective Score (Video Analysis)Learning Curve of Surgical Residents
34
60 60
75
86
100
0
20
40
60
80
100
R1 R2 R3 R4 R5 E
Training Level
Sub
ject
ive
Sco
re

Correlation Between Subjective and ObjectiveAssessment of Surgical Skill
R1 (34.4, 8.34)
R2 (59.6, 3.9)
R3 (60.0, 4.6)
R4 (74.7, 5.1)
R5 (86.5, 2.0)
E (100, 1)
R2 = 0.8623
0
1
2
3
4
5
6
7
8
9
0 20 40 60 80 100
Subjective Analysis (Video Analysis)
Ob
ject
ive
An
alys
is (
Mar
kov
Mo
del
)

Conclusions / Application
Analyzing Minimally Invasive Surgery requires a synthesis between visual and haptic information.
Differences between expert and novice surgeons can be defined in terms of: – Force / Torque / Velocity signatures – State transitions / combinations– Time spent in each state– Trajectory (tool tip) length
Good correlation (R2=0.86) between objective (Markov Model) and subjective (video analysis scoring) assessment of surgical skill
The objective methodology for surgical skill evaluation is a modality independent. It can be applied to:– In-vivo surgical conditions– Telerobotic systems
– VR haptics simulators
10Q


















