Minimal Change Disease
25
Minimal change GN
-
Upload
mohamed-elamin-awad -
Category
Health & Medicine
-
view
166 -
download
1
description
minimal change disease presentation, diagnosis and update management.
Transcript of Minimal Change Disease

Minimal change GN

Nothing in light microscopy.
Diffuse effacement of the epithelia cell foot processes
No immune deposition
2 – 8 ys & 10% in adults
NSAID & malignancies
Presentation :NS.
Renal biopsy for diagnosis

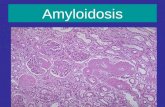
MCD1. 1- 2 cells per capillary tuft
2. Capillary lumen is open
3. Normal thickness of capillary wall

MCD
Silver stain

Electron microscopy
Ultrastructurally, the only glomerular abnormality apparent is effacement of the podocyte foot processes


SSNS

Relapsing SSNS





SRNS


MCD relapses after Cyclosporine cessation

Treatment Characterized by remission & relapse
Good response to steroids
Spontaneous remission in 5%
Respond to treatment:Primary Responder non RelapserPR infrequent RLPR frequent RLSecondary non RespondersP non-responders late RespondersNon –respondersSteroids dependent

Steroids
Corner stone in treatment
50% of children respond within the first 2/52
Almost all within 8/52
Adults 10 – 25 % & renal biopsy is mandatory for diagnosis
25% of adults need 12 – 16 weeks to completely remit.

Objectives
Speed induction of remission.
Avoid serious complications.
Prevent or minimize relapses
Avoid or minimize side effects of drugs

Symptomatic treatment
Oedema : Salt & water retention . Loop diuretics Salt free Alb
Thrombosis : Mobilization, aspirin & dipyridamole
Infections

If the proteinuria persisted beyond the first month the steroid may be boosted or the patient given a daily inj of methylpredisolone for three days.
30 % are cured by this treatment.
Infrequent & frequent relapses describe 10 – 20 % & 40 – 50 % respectively.

Cyclophosphamide :
started after steroid induced remission in a dose of 2 mg/kg/day for a total duration of 12 weeks
Longer remission if used for 12 instead of 8/52
The response has -ve correlation with HLA-DR7.

Blood count ( 3000 mm3)
The total dose is away below the gonadotoxic level of 300 mg/kg.

Chlorambucil : 0.2 mg/kg/day for a period of 2/12.
Levamisol :
Immune modulator that gives a longer remission period.
Longer use more than 6/12 is assosiated with GI manifestations, leuocopenia , psoriasis- like cutaneous lesion & leukaemia.

cyclosporine
Can induce & maintain remission but many patients relapse upon cessation of the drug.
Relapsers respond poorly to another course of the drug
Toxicity follow up & renal biopsy 18/12 from drug initiation is a better guide.

Steroid resistant cases
Due to genetic factors ( q1) or due to down regulation of glucocorticiods receptors.
Cyclosporine + prednisolone if normal GFR
Cyclophosphamide or chlorambucil in those with low GFR or non responders to the first regimen.