MINERVA ANESTESIOLOGICA - Siaarti · P. Di Marco (Roma, Italy) J. T ... Pediatric Anesthesia...
124
EDITORIAL BOARD EDITOR IN CHIEF F. Cavaliere Roma, Italy General Critical Care Associate Editor G. M. Albaiceta (Oviedo, Spain) Section Editor G. Biancofiore (Pisa, Italy) E. De Robertis (Napoli, Italy) Circulation Critical Care Section Editor S. Scolletta (Siena, Italy) E. Bignami (Milano, Italy), Respiration Critical Care Section Editor S. Grasso (Bari, Italy) P. Terragni (Sassari, Italy), Neurocritical Care Section Editor F. S. Taccone (Brussels, Belgium) Section Editor A. Giannini (Milano, Italy) Section Editor M. Allegri (Parma, Italy) F. Coluzzi (Roma, Italy) ETHICS PAIN Section Editor B. M. Cesana (Brescia, Italy) MEDICAL STATISTIC General Anesthesia Associate Editor M. Rossi (Roma, Italy) Section Editor E. Cohen (New York, USA) P. Di Marco (Roma, Italy) J. T. Knape (Utrecht, The Netherlands) O. Langeron (Paris, France) P. M. Spieth (Dresden, Germany) Pediatric Anesthesia Section Editor M. Piastra (Roma, Italy) Obstetric Anesthesia Section Editor E. Calderini (Milano, Italy) Regional Anesthesia Section Editor A. Apan (Giresun, Turkey) M. Carassiti (Roma, Italy) CRITICAL CARE ANESTHESIA MANAGING EDITOR A. Oliaro Torino, Italy MINERVA ANESTESIOLOGICA ITALIAN JOURNAL OF ANESTHESIOLOGY AND ANALGESIA MONTHLY JOURNAL FOUNDED IN 1935 BY A. M. DOGLIOTTI OFFICIAL JOURNAL OF ITALIAN SOCIETY OF ANESTHESIOLOGY, ANALGESIA, RESUSCITATION AND INTENSIVE CARE (S.I.A.A.R.T.I.) Vol. 82 - No. 3 MINERVA ANESTESIOLOGICA V
Transcript of MINERVA ANESTESIOLOGICA - Siaarti · P. Di Marco (Roma, Italy) J. T ... Pediatric Anesthesia...

EDITORIAL BOARD
EDITOR IN CHIEFF. CavaliereRoma, Italy
General Critical CareAssociate Editor
G. M. Albaiceta (Oviedo, Spain)Section Editor
G. Biancofiore (Pisa, Italy)E. De Robertis (Napoli, Italy)
Circulation Critical CareSection Editor
S. Scolletta (Siena, Italy)E. Bignami (Milano, Italy),
Respiration Critical CareSection Editor
S. Grasso (Bari, Italy)P. Terragni (Sassari, Italy),
Neurocritical CareSection Editor
F. S. Taccone (Brussels, Belgium)
Section EditorA. Giannini (Milano, Italy)
Section EditorM. Allegri (Parma, Italy)F. Coluzzi (Roma, Italy)
ETHICS PAIN
Section EditorB. M. Cesana (Brescia, Italy)
MEDICAL STATISTIC
General AnesthesiaAssociate Editor
M. Rossi (Roma, Italy)Section Editor
E. Cohen (New York, USA)P. Di Marco (Roma, Italy)
J. T. Knape (Utrecht, The Netherlands)O. Langeron (Paris, France)
P. M. Spieth (Dresden, Germany)
Pediatric AnesthesiaSection Editor
M. Piastra (Roma, Italy)
Obstetric AnesthesiaSection Editor
E. Calderini (Milano, Italy)
Regional AnesthesiaSection Editor
A. Apan (Giresun, Turkey)M. Carassiti (Roma, Italy)
CRITICAL CARE ANESTHESIA
MANAGING EDITORA. Oliaro
Torino, Italy
MINERVA ANESTESIOLOGICAITALIAN JOURNAL OF ANESTHESIOLOGY AND ANALGESIA
MONTHLY JOURNAL FOUNDED IN 1935 BY A. M. DOGLIOTTIOFFICIAL JOURNAL OF ITALIAN SOCIETY OF ANESTHESIOLOGY, ANALGESIA,
RESUSCITATION AND INTENSIVE CARE (S.I.A.A.R.T.I.)
Vol. 82 - No. 3 MINERVA ANESTESIOLOGICA V

This journal is PEER REVIEWED and is quoted in:
Current Contents, SciSearch, PubMed/MEDLINE, EMBASE, Scopus
G E N E R A L I N F O R M A T I O N
Subscribers: Payment to be made in Italy: a) by check; b) by bank transfer to: Edizioni Minerva Medica, INTESA SANPAOLO Branch no. 18 Torino. IBAN: IT45 K030 6909 2191 0000 0002 917 c) through postal account no. 00279109 in the name of Edizioni Minerva Medica, Corso Bramante 83-85, 10126 Torino; d) by credit card Diners Club International, Master Card, VISA, American Express. Foreign countries: a) by check; b) by bank transfer to: Edizioni Minerva Medica, INTESA SANPAOLO Branch no. 18 Torino. IBAN: IT45 K030 6909 2191 0000 0002 917; BIC: BCITITMM c) by credit card Diners Club International, Master Card, VISA, American Express. Members: for payment please contact the Administrative Secretariat SIAARTI.Notification of changes to mailing addresses, e-mail addresses or any other subscription information must be received in good time. Notification can be made by sending the new and old information by mail, fax or e-mail or directly through the website www.minerva-medica.it at the section “Your subscriptions - Contact subscriptions department”.Complaints regarding missing issues must be made within six months of the issue’s publication date.Prices for back issues and years are available upon request.© Edizioni Minerva Medica - Torino 2016. All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, without the prior permission of the copyright owner.Monthly publication. Authorized by Turin Court no. 281 of 24-1-1953.
Published byEdizioni Minerva Medica - Corso Bramante 83-85 - I-10126 Turin (Italy)
Tel. +39 (011) 678282 - Fax +39 (011) 674502 Website: www.minervamedica.it
Editorial office: [email protected] - Subscriptions: [email protected]: [email protected]
Presidential Office: Antonio Corcione, UOC Anestesia e TIPO, Azienda Ospedaliera dei Colli, V. Monaldi, Via Leonardo Bianchi 1, 80131 Naples, Italy - Tel. 081 7065214. E-mail: [email protected]
Technical Secretariat: S.I.A.A.R.T.I., Viale dell’Università 11, 00185 Rome, Italy - Tel. 06 4452816
E-mail: [email protected] - Website: www.siaarti.it
Administrative Secretariat S.I.A.A.R.T.I. - Edizioni Minerva Medica - Corso Bramante 83-85 - 10126 Turin, Italy - Tel. +39 (011) 678282 - Fax +39 (011) 674502 - E-mail: [email protected]
ITALY
Individual: Print € 130,00 Print+Online € 135,00 Online € 140,00
Institutional: Print € 180,00
Online Small € 350,00 Medium € 407,00 Large € 429,00
Print+Online Small € 367,00 Medium € 420,00 Large € 446,00
EUROPEAN UNION
Individual: Print € 225,00 Print+Online € 235,00 Online € 245,00
Institutional: Print € 300,00
Online Small € 351,00 Medium € 409,00 Large € 429,00
Print+Online Small € 378,00 Medium € 430,00 Large € 456,00
OUTSIDE THEEUROPEAN UNION
Individual: Print € 250,00 Print+Online € 260,00 Online € 270,00
Institutional: Print € 335,00
Online Small € 383,00 Medium € 446,00 Large € 462,00
Print+Online Small € 404,00 Medium € 467,00 Large € 483,00
ANNUAL SUBSCRIPTIONS
VI MINERVA ANESTESIOLOGICA March 2016
Impact factor: 2,134
This Journal complies with the Code of Self-Discipline of Medical/Scientific Publishers associated with FARMAMEDIA and may accept advertisingThis Journal is associated with

I N S T R U C T I O N S T O A U T H O R S
Minerva Anestesiologica is the journal of the Italian National Society of Anaesthesia, Analgesia, Resuscitation, and Intensive Care (SIAARTI). Minerva Anestesiologica publishes scientific papers on Anesthesiology, Intensive care, Analgesia, Perioperative Medicine and related fields. Manuscripts are expected to comply with the instructions to authors which conform to the Uniform Requirements for Manuscripts Submitted to Biomedical Editors by the International Committee of Medical Journal Editors (http://www.icmje.org/).Articles not conforming to international standards will not be con-sidered for acceptance. Submission of manuscriptsPapers should be submitted directly to the online Editorial Office at the Edizioni Minerva Medica website:www.minervamedicaonlinesubmission.it Duplicate or multiple publicationSubmission of the manuscript means that the paper is original and has not yet been totally or partially published, is not currently under evaluation elsewhere, and, if accepted, will not be published else-where either wholly or in part. Splitting the data concerning one study in more than one publi-cation could be acceptable if authors justify the choice with good reasons both in the cover letter and in the manuscript. Authors should state the new scientific contribution of their manuscript as compared to any previously published article derived from the same study. Relevant previously published articles should be included in the cover letter of the currently submitted article.Permissions to reproduce previously published materialMaterial (such as illustrations) taken from other publications must be accompanied by the publisher’s permission.CopyrightThe Authors agree to transfer the ownership of copyright to Minerva Anestesiologica in the event the manuscript is published. Ethics committee approvalAll articles dealing with original human or animal data must include a statement on ethics approval at the beginning of the methods sec-tion, clearly indicating that the study has been approved by the ethics committee. This paragraph must contain the following informa-tion: the identification details of the ethics committee; the protocol number that was attributed by the ethics committee and the date of approval by the ethics committee.The journal adheres to the principles set forth in the Helsinki Declaration (http://www.wma.net/en/30publications/10policies/b3/index.html) and states that all reported research concern-ing human beings should be conducted in accordance with such principles. The journal also adheres to the International Guiding Principles for Biomedical Research Involving Animals (http://www.cioms.ch/publications/guidelines/1985_texts_of_guidelines.html) recommended by the WHO and requires that all research on animals be conducted in accordance with these principles. Patient consentAuthors should include at the beginning of the methods section of their manuscript a statement clearly indicating that patients have given their informed consent for participation in the research study.Every precaution must be taken to protect the privacy of patients.Conflicts of interestAuthors must disclose possible conflicts of interest including finan-cial agreements or consultant relationships with organizations involved in the research. All conflicts of interest must be declared both in the authors’ statement form and in the manuscript file. If there is no conflict of interest, this should also be explicitly stated as none declared. All sources of funding should be acknowledged in the manuscript. AuthorshipAll persons and organizations that have participated to the study must be listed among the Authors or in the acknowledgements. Authors must meet the criteria for authorship established by the Uniform Requirements for Manuscripts Submitted to Biomedical Editors by the International Committee of Medical Journal Editors (http://www.icmje.org/).
Authors’ statementPapers must be accompanied by the authors’ statement (http://www.minervamedica.it/en/journals/minerva-anestesiologica/index.php) relative to copyright, originality, authorship, ethics and conflicts of interest, signed by all authors.Disclaimer The Publisher, Editors, and Editorial Board cannot be held respon-sible for the opinions and contents of publications contained in this journal.
The authors implicitly agree to their paper being peer-reviewed. All manuscripts will be reviewed by Editorial Board members who reserve the right to reject the manuscript without entering the review process in the case that the topic, the format or ethical aspects are inappropriate. In addition, the Editorial Board admits for submis-sion manuscripts previously submitted for publication to another journal but rejected with reviewers’ comments. In such cases, authors are requested to submit the scientific comments of the other journal and their point-by-point reply to the reviewers’ comments in the manuscript file. This will help to speed up the peer review process.Once accepted, all manuscripts are subjected to copy editing. If modifications to the manuscript are requested, the corresponding author should send to the online Editorial Office the revised manu-script under two separate files, one file containing the revised clean version and another containing both a letter with point-by-point responses to the reviewers’ comments and the revised version with corrections highlighted.Correction of proofs should be limited to typographical errors. Substantial changes in content (changes of title and authorship, new results and corrected values, changes in figures and tables) are subject to editorial review. Changes that do not conform to the journal’s style are not accepted. Corrected proofs must be sent back within 3 working days to the online Editorial Office of Minerva Anestesiologica. In case of delay, the editorial staff of the journal may correct the proofs on the basis of the original manuscript.Publication of manuscripts is free of charge. Colour figures and excessive alterations to proofs will be charged to the authors. Authors will receive instructions on how to order reprints and a copy of the manuscript in PDF.For further information about publication terms please contact the Editorial Office of Minerva Anestesiologica, Edizioni Minerva Medica, Corso Bramante 83-85, 10126 Torino, Italy - Phone +39-011-678282 - Fax +39-011-674502 - E-mail: [email protected].
Article types
Original papers are reports of original researches on the topics of interest to the journal and do not exceed 3000 words, 6 figures or tables, and 40 references. Papers reporting randomized control-led trials should be in accordance with the CONSORT statement (http://www. consort-statement.org).Review articles are comprehensive papers that outline current knowl-edge, usually submitted after prior consultation with the Editors and do not exceed 4000 words, 6 figures or tables, 70 references. Reviews should be in accordance with the PRISMA statement (www.prisma-statement.org).Experts’ opinion are papers reviewing the literature, usually invited by the Editor in Chief and do not exceed 3000 and 2000 words with 50 and 40 references respectively.Editorials are brief comments, commissioned by the Editor-in-Chief and express author’s opinion about published papers or topical issues and do not exceed 1000 words and 20 references.Letters to the Editor (Correspondence) are brief comments on articles published in the journal or with other topics of interest and do not exceed 500 words, 5 references and 1 figure or table.
Preparation of manuscripts
Text fileThe formats accepted are Word and RTF. The paper must contain title, authors’ details, notes, abstract, key words, text, references and

titles of tables and figures. Tables and figures should be submitted as separate files.
Title and authors’ details• Shorttitle(notexceeding100characters,spacesincluded),
with no abbreviations. • Firstnameandsurnameoftheauthors.• Affiliation(section,departmentand institution)ofeach
author.
Notes• Datesofanycongresswherethepaperhasalreadybeenpre-
sented. • Mentionofanyfundingorresearchcontractsorconflictof
interest. • Acknowledgements.• Name,address,e-mailofthecorrespondingauthor.
Abstract and key words Articles should include an abstract not exceeding 250 words. For original papers, the abstract should be structured as follows: background (status of knowledge and aim of the study), methods (experimental design, patients and interventions), results (what was found), conclusions (meaning of the study). Key words should refer to the terms from Medical Subject Headings (MeSH) of the Index Medicus. No abstracts are required for editorials or letters to the Editor.
Text
Units of measurement, symbols and abbreviations must conform to international standards. Measurements of length, height, weight and volume should be given in metric units (meter, kilogram, liter) or their decimal multiples. Temperatures must be expressed in degrees Celsius. Blood pressure must be expressed in millimeters of mer-cury. All hematological and clinicochemical measurements should be expressed in metric units using the International System of Units (IS). The use of unusual symbols or abbreviations is strongly discour-aged. The first time an abbreviation appears in the text, it should be preceded by the words for which it stands.For original papers the text must be subdivided into the following sections: introduction, materials and methods, results, discussion, conclusions. The introduction should describe the present state of knowledge on the subject and clearly state the aim of the research. The Materials and methods section should provide enough infor-mation to allow other researchers to reproduce results and should include a statistics section. Detailed statistical methodology must be described in order to enable the reader to evaluate and verify the results. Please report power analysis, randomized procedure, tests of normality, descriptive parameters, statistical tests and the probability level chosen for statistical significance. Drugs should be identified by their international non-proprietary name. If special equipment is used, then the manufacturer’s details (including town and country) should be given in parentheses. The Results section should describe the outcome of the study. Data presented in tables and graphs should not duplicate those presented in the text. Very large tables should be avoided. The Discussion should include the interpretation of the results obtained, an analysis of the limits of the study, and references to work by other authors. Conclusions should highlight the significance of the results for clinical practice and experimental research.
References
The list of references should only include works that are cited in the text and that have been published or accepted for publication (a copy of the acceptation letter can be requested) in journals cited in peer-reviewed Index Medicus journals. Websites can also be cited providing the date of access. Bibliographical entries in the text should be quoted using superscripted Arabic numerals. References must be set out in the standard format approved by the International Committee of Medical Journal Editors (www.icmje.org).Footnotes and endnotes must not be used in the preparation of references.
JournalsEach entry must specify the author’s surname and initials (list all authors when there are six or fewer; when there are seven or more, list only the first six and then “et al.”), the article’s original title, the name of the Journal (according to the abbreviations used by Index Medicus), the year of publication, the volume number and the number of the first and last pages. When citing references, please follow the rules for international standard punctuation carefully.Examples– Standard articleSutherland DE, Simmons RL, Howard RJ. Intracapsular technique of transplant nephrectomy. Surg Gynecol Obstet 1978;146:951-2.– Organization as authorInternational Committee of Medical Journal Editors. Uniform requirements for manuscripts submitted to biomedical journals. Ann Int Med 1988;108:258-65.– Issue with supplementPayne DK, Sullivan MD, Massie MJ. Women’s psychological reactions to breast cancer. Semin Oncol 1996;23(1 Suppl 2): 89-97.
Books and mono graphsFor occasional publications the names of the Authors, the title, edi-tion, place, publisher and year of publication must be given.Examples– Books by one or more AuthorsRossi G. Manual of Otorhinolaryngology. Turin: Edizioni Minerva Medica; 1987. – Chapter from bookDe Meester TR. Gastroesophageal reflux disease. In: Moody FG, Carey LC, Scott Jones R, Ketly KA, Nahrwold DL, Skinner DB, editors. Surgical treatment of digestive diseases. Chicago: Year Book Medical Publishers; 1986. p. 132-58. – Congress proceedingsKimura J, Shibasaki H, editors. Recent advances in clinical neu-rophysiology. Proceedings of the 10th International Congress of EMG and Clinical Neurophysiology; 1995 Oct 15-19; Kyoto, Japan. Amsterdam: Elsevier; 1996. Titles of tables and figuresTitles of tables and legends of figures should be included both in the text file and in the file of tables and figures.File of tablesEach table should be submitted as a separate file. Formats accepted are Word and RTF. Each table must be typed correctly and prepared graphically in keeping with the page layout of the journal, numbered in Roman numerals and accompanied by the relevant title. Notes should be inserted at the foot of the table and not in the title. Tables should be referenced in the text sequentially. Tables should be self-explanatory and have a brief title and a legend if appropriate. File of figuresEach figure should be submitted as a separate file. Formats accepted: JPEG set at 300 dpi resolution preferred; other formats accepted are TIFF and PDF (high quality). Figures should be numbered in Arabic numerals and accompanied by the relevant legend. Figures should be referenced in the text sequentially.Histological photographs should always be accompanied by the magnification ratio and the staining method.If figures are in color, it should always be specified whether color or black and white reproduction is required.Authors of Original Articles are invited to submit figures for con-sideration as part of the cover design of an issue of the Journal. The Editorial Board will select from among the most interesting published Original Articles a figure they deem appropriate as a cover image for the issue in which the Original Article is published.
INSTRUCTIONS TO AUTHORS
For any fur ther in for ma tion vis it our web sitewww.minervamedica.it

271Organ donation after circulatory death in Italy? Yes we can!Nanni Costa A., Procaccio F.
274ORIGINAL ARTICLESDynamic view of postoperative pain evolution after total knee arthroplasty: a prospective observational studyGrosu I., Thienpont E., De Kock M., Scholtes J. L., Lavand’Homme P.
284Continuous vs. intermittent vancomycin therapy for Gram-positive infections not caused by methicillin-resistant Staphylococcus AureusDuszynska W., Taccone F. S., Hurkacz M., Wiela-Hojenska A., Kübler A.
294Potential neurotoxicity of anesthetic drugs in young children: who cares? A survey among European anes-thetistsWeber F., Van Beek S., Scoones G.
257EDITORIALSIt is time for anesthetists to act as perioperative physi-ciansDeflandre E., Lacroix S.
259How should pediatric anesthesia respond on the dis-cussion about neurotoxicity in daily practice?Kaufmann J., Laschat M.
262The end of an era of pharmaconutrition and immu-nonutrition trials for the critically-ill patient?Festen B., Van Zanten A. R.
265Predictive scores for postoperative pulmonary compli-cations: time to move towards clinical practiceBall L., Pelosi P.
268How genomics can improve the management of septic patientsVincent J-L.
MINERVA ANESTESIOLOGICA
Vol. 82 March 2016 No. 3
CONTENTS
Vol. 82 - No. 3 MINERVA ANESTESIOLOGICA I
OFFICIAL JOURNAL OF ITALIAN SOCIETY OF ANESTHESIOLOGY, ANALGESIA,RESUSCITATION AND INTENSIVE CARE (SIAARTI)
ITALIAN JOURNAL OF ANESTHESIOLOGY AND ANALGESIAMONTHLY JOURNAL FOUNDED IN 1935 BY A. M. DOGLIOTTI
OFFICIAL JOURNAL OF ITALIAN SOCIETY OF ANESTHESIOLOGY, ANALGESIA,RESUSCITATION AND INTENSIVE CARE (S.I.A.A.R.T.I.)

CONTENTS
II MINERVA ANESTESIOLOGICA March 2016
301Comparison of blood culture and multiplex real-time PCR for the diagnosis of nosocomial sepsisDinç F., Akalin H., Özakin C., Sinirtaş M., Kebabçi N., Işçimen R., Kelebek Girgin N., Kahveci F.
310Time course of cytokines, hemodynamic and meta-bolic parameters during hyperthermic intraperitoneal chemotherapyCoccolini F., Corbella D., Finazzi P., Brambillasca P., Benigni A., Prussiani V., Ceresoli M., Manfredi R., Poiasina E., Bertoli P., Catena F., Bianchetti A., Bontempelli M., Lorini L. F., Sonzogni V., Ansaloni L.
320REVIEWSImmunonutrients in critically ill patients: an analysis of the most recent literatureAnnetta M. G., Pittiruti M., Vecchiarelli P., Silvestri D., Caricato A., Antonelli M.
332How to optimize and use predictive models for post-operative pulmonary complicationsMazo V., Sabaté S., Canet J.
343The role of genomics to identify biomarkers and sign-aling molecules during severe sepsisDouglas J. J., Russell J. A.
359EXPERTS’ OPINION“Why can’t I give you my organs after my heart has stopped beating?”An overview of the main clinical, organisational, ethical and legal issues concerning organ donation after circulatory death in ItalyGiannini A., Abelli M., Azzoni G., Biancofiore G., Citterio F., Geraci P., Latronico N., Picozzi M., Procaccio F., Riccioni L., Rigotti P., Valenza F., Vesconi S., Zamperetti N.
369LETTERS TO THE EDITORRegional blocks for breast surgery: is it enough?Huercio I., Abad-Gurumeta A., Gilsanz F.
370Regional block for breast surgery: is it enough? Authors’ replyBouzinac A.
371Extracorporeal membrane oxygenation in avalanche victim with deep hypothermia and circulatory arrestFacchetti G., Carbuglia N., Bucci V., Taraschi F., Paparoni S., Gyra A., Marinangeli F.
372Incidence and laryngoscopic grade of adult patients with Mallampati class zero airwayMiyoshi H., Kusunoki S., Nakamura R., Kawamoto M.
374TOP 50 MINERVA ANESTESIOLOGICA REVIEWERS
About the cover: the cover shows the Engström narcosis respirator model 200 projected around 1956 and produced by Gambro Engström AB. From the SIAARTI collection of medical devices at Viale dell’Università 11, Rome, Italy.
V O L U M E 8 2 · N o. 3 · M A R C H 2 0 1 6

Vol. 82 - No. 3 MiNerVa aNestesiologica 257
in this issue of Minerva Anestesiologica, grosu et al. have taken into account the evo-lution of pain after total knee arthroplasty (tKa).8 this original paper is interesting as it confirms the need for a holistic view of the patient. Indeed, the authors were interested in the patient’s pain (acute and chronic); but also, they measured the influence of pain on quality of life. This care corresponds to a method of the perioperative medicine.
As part of perioperative medicine, other ap-proaches could complement this patient’s care. Some examples are detailed hereafter. The preoperative anesthesia consultation should not only be used to identify high-risk patients (e.g. cardiac patients) but also should allow to track more efficiently “new risks” for patients. Among these, the anaesthetist can identify pa-tients with an increased likelihood of devel-oping postoperative chronic pain.9 Sessler et al. perfectly demonstrated that perioperative management conditioned patient’s outcome.7 For TKA, while the technique is not without risk, several authors have confirmed the su-periority of neuraxial anesthesia compared to general anesthesia in terms of postoperative infections, quality of life and 30-day mortal-ity.10-12 Postoperative pain should be treated quickly and adequately. Untreated acute pain is a major risk factor for chronicity of these.8, 13 However, some issues are still unresolved.14
Whether the patient will be dead or alive at the end of the operation is no longer the
matter. Intraoperative mortality has dramati-cally decreased since the early 1980s, even if variability could be observed between coun-tries.1-3 In an outstanding editorial, Grocott et al. have shown the need for anesthetists to in-tegrate the concept of perioperative medicine.4 This idea is not recent as in the late 1990s some visionary authors looked at the periop-erative medicine as the future of anesthesia.5, 6 as grocott et al. specify, many disciplines set one’s sight on perioperative medicine. How-ever, anesthetists are still the best placed to become leaders in this field. Indeed, we have an ideal combination of training, skills, knowl-edge, and experience.4
Therefore, a comprehensive view on the whole perioperative period is necessary. The perioperative management should start during the preoperative anaesthetic visit, follow with a “goal-directed patient-centred” intraopera-tive management and finish with postoperative care. This last one should not be limited to the recovery room, but will continue on the ward and even more after hospital discharge. There is growing evidence that our anesthesia influ-ences patient’s outcome, as surgical proce-dures do.7
E D I T O R I A L
It is time for anesthetists to act as perioperative physicians
eric DeFlaNDre 1-3 *, Simon LACROIX 3
1Cabinet Medical ASTES, Jambes, Belgium; 2University of Liege, Liege, Belgium; 3Clinique Saint-Luc of Bouge, Namur, Belgium*Corresponding author: Eric Deflandre, Chaussee de Tongres, 29, 4000 Liege-Rocourt, Belgium. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva anestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: 10888-MAStitolo breve: ANAESTHETISTS SHOULD ACT AS PERIOPERATIVE PHYSICIANSprimo autore: DEFLANDREpagine: 257-8citazione: Minerva Anestesiol 2016;82:000-000
Comment on p. 274
Minerva Anestesiologica 2016 March;82(3):257-8© 2015 EDIZIONI MINERVA MEDICAThe online version of this article is located at http://www.minervamedica.it

DeFlaNDre ANAESTHETISTS SHOULD ACT AS PERIOPERATIVE PHYSICIANS
258 MiNerVa aNestesiologica March 2016
4. Grocott MP, Pearse RM. Perioperative medicine: the fu-ture of anesthesia? Br J Anaesth 2012;108:723-6.
5. Van Aken H, Thomson D, Smith G, Zorab J. 150 years of anesthesia--a long way to perioperative medicine: the modern role of the anaesthesiologist. Eur J Anaesthesiol 1998;15:520-3.
6. rock P. the future of anesthesiology is perioperative medicine. anesthesiol clin 2000;18:495-513.
7. Sessler DI, Sigl JC, Kelley SD, Chamoun NG, Manberg PJ, Saager L, et al. Hospital stay and mortality are in-creased in patients having a “triple low” of low blood pressure, low bispectral index, and low minimum alveo-lar concentration of volatile anesthesia. anesthesiology 2012;116:1195-203.
8. Grosu I, Thienpont E, De Kock M, Scholtes JL, Lavand’homme P. Dynamic view of postoperative pain evolution after total knee arthroplasty: a prospec-tive observational study. Minerva Anestesiol 2016;82: 274-83.
9. Janssen KJ, Kalkman CJ, Grobbee DE, Bonsel GJ, Moons KG, Vergouwe Y. The risk of severe postoperative pain: modification and validation of a clinical prediction rule. Anesth Analg 2008;107:1330-9.
10. Liu J, Ma C, Elkassabany N, Fleisher LA, Neuman MD. Neuraxial anesthesia decreases postoperative systemic infection risk compared with general anesthesia in knee arthroplasty. Anesth Analg 2013;117:1010-6.
11. Memtsoudis SG, Sun X, Chiu YL, Stundner O, Liu SS, Banerjee S, et al. Perioperative comparative effective-ness of anesthetic technique in orthopedic patients. An-esthesiology 2013;118:1046-58.
12. Lirk P, Hollmann MW. Outcome after regional anesthe-sia: weighing risks and benefits. Minerva Anestesiol 2014;80:610-8.
13. Lavand’homme P. The progression from acute to chronic pain. curr opin anaesthesiol 2011;24:545-50.
14. Allegri M, Clark MR, De Andres J, Jensen TS. Acute and chronic pain: where we are and where we have to go. Minerva Anestesiol 2012;78:222-35.
15. Allegri M, De Gregori M, Niebel T, Minella C, Tinelli c, govoni s, et al. Pharmacogenetics and postoperative pain: a new approach to improve acute pain management. Minerva Anestesiol 2010;76:937-44.
16. Vetter TR, Goeddel LA, Boudreaux AM, Hunt TR, Jones KA, Pittet JF. The Perioperative Surgical Home: how can it make the case so everyone wins? BMC Anesthesiology 2013;13:6.
17. Martin J, Cheng D. Role of the anesthesiologist in the wider governance of healthcare and health economics. Can J Anaesth 2013;60:918-28.
18. Walder B, Maillard J, Lubbeke A. Minimal clinically im-portant difference: a novel approach to measure changes in outcome in perioperative medicine. Eur J Anaesthesiol 2015;32:77-8.
19. Hyder JA, Niconchuk J, Glance LG, Neuman MD, Cima rr, Dutton rP, et al. What can the national quality forum tell us about performance measurement in anesthesiol-ogy? Anesth Analg 2015;120:440-8.
20. Wacker J, Staender S. The role of the anesthesiologist in perioperative patient safety. curr opin anaesthesiol 2014;27:649-56.
In the future, the pharmacogenetic approach might then bring some answers.15
Anesthesia practice has profoundly im-proved in terms of safety, activities and per-spectives.3 This shows how anesthesia is able to move forward and how it tries to meet the requirements of our current society. Another change in practice will be achieved by the implementation of the Perioperative Surgical Home.16 This comprehensive reform will aim to improve the quality of care (patient-cen-tred); but it will also lead to an economy of means. For some authors, the access of anes-thetists to the wider governance of healthcare and health economics (both within the hospital and in new non-hospital structures) will have a positive economic impact.17
For all of these changes, we will never for-get to measure and implement practice quality parameters.18, 19 For the time being, we cannot manage what we do not measure. “Primum non nocere, deinde curare”: outcome quality indicators are essential. The role of the anaes-thetist in perioperative patient safety is defi-nitely inescapable.20
Anesthesia is moving outside the operative room. If anesthesia succeeds in imposing one-self in perioperative period, it will gain cred-ibility towards patient and other physicians. Conversely, if we spoil this opportunity, others will jump at it.
References
1. Lienhart A, Auroy Y, Pequignot F, Benhamou D, Warsza-wski J, Bovet M, et al. Survey of anesthesia-related mortality in France. Anesthesiology 2006;105:1087- 97.
2. Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, spies c, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet 2012;380:1059-65.
3. Clergue F. The challenges of anesthesia for the next decade: the Sir Robert Macintosh Lecture 2014. Eur J anaesthesiol 2015;32:223-9.
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: September 17, 2015. - Manuscript accepted: September 16, 2015. - Manuscript received: August 21, 2015.(Cite this article as: Deflandre E, Lacroix S. It is time for anesthetists to act as perioperative physicians. Minerva Anestesiol 2016;82:257-8)

Vol. 82 - No. 3 MiNerVa aNestesiologica 259
are the threat to baby brains” 2 certainly fueled the emotional component of the debate. the impact of this topic in pediatric anesthesia is very noticeable during daily practice and will undoubtedly remain prevalent in the future. apart from the increasing anxiety of parents and other medical specialties, it must be as-sumed that lawsuits concerning disabled pre-mature children will increasingly focus on the anesthetic care.
in this issue of Minerva Anestesiologica, a survey by Frank Weber et al. tackles the im-pact the discussion about neurotoxicity has on pediatric anesthesiologists.3 they focused on the thoughts of the colleagues and if they have changed their daily practice as a conse-quence. By contacting the participants in the aPricot trial (www.esahq.org/apricot), they reached a large, selected group of scien-tifically interested pediatric anesthesiologists from all over europe. this study is able to add valuable information to assess the influence of the current knowledge and discussion about neurotoxicity on the daily routine of pediatric anesthesia specialists in europe.
surprisingly, only half of the participants (mostly specialists in anesthesia) felt them-selves well informed about the issue of neu-rotoxicity in pediatric anesthesia. two thirds of the participants reported that neurotoxicity affected their daily practice, in most of the
the current discussion of the impact of nar-cotics on the neurological development
of neonates and small children is a result of animal studies. invariably, the exposure to an-esthetic agents in these studies was not consis-tent with routine clinical practice and the ex-perimental setup a consequence of the desire and need to obtain a significant result in order to ensure publication.
only fragmented and contradictory evidence is available for humans, however, various sci-entific publications call for a “heightened level of concern” on this issue.1 Furthermore, the non-scientific media has processed this topic providing various articles and editorials with alarming headlines such as “Does anesthesia make your child stupid?”. Both the academic and lay press create the impression of this be-ing a statement rather than a question. a re-cent alternative view editorial highlighted that maintaining homeostasis (avoiding arterial hy-potension, hypocapnia, hyponatremia and hy-poglycemia) may be even more important for the neurodevelopment of premature babies. it also suggested that these imbalances are too often tolerated during daily anesthetic prac-tice. although this message is providing a bal-ance and is absolutely correct, the distinctive headline “Anesthetists rather than anesthetics
E D I T O R I A L
How should pediatric anesthesia respond on the discussion about neurotoxicity in daily practice?
Jost KaUFMaNN 1, 2 *, Michael lascHat 1
1Department of Pediatric Anesthesia, Children’s Hospital of Cologne, Cologne, Germany; 2Faculty of Health, University Witten/Herdecke, Witten, germany*Corresponding author: Jost Kaufmann, Department of Pediatric Anesthesia, Children’s Hospital of Cologne, Amsterdamer Str. 59, D-50735 Cologne, Germany. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
Lavoro: 10897-MAStitolo breve: PEDIATRIC ANESTHESIA AND NEUROTOXICITY IN DAILY PRACTICEprimo autore: KaUFMaNNpagine: 259-61citazione: Minerva Anestesiol 2016;82:000-000
comment on p. 294
Minerva Anestesiologica 2016 March;82(3):259-61© 2015 EDIZIONI MINERVA MEDICAthe online version of this article is located at http://www.minervamedica.it

KaUFMaNN PEDIATRIC ANESTHESIA AND NEUROTOXICITY IN DAILY PRACTICE
260 MiNerVa aNestesiologica March 2016
4. this institutional competence also re-quires the treatment of vulnerable babies with-in well-prepared structures; this necessitates adoption of institution-wide teaching and edu-cation of their special needs;
5. pediatric anesthesia should be performed or supervised by trained pediatric anesthesi-ologists only. it is well accepted that this group can provide stability and will result in less complications than someone only occasionally treating such patients;
6. finally, pediatric anesthesiologists should respond and be recognized as competent partners for perioperative medicine of a very special patient group. as such they must be involved in the planning of the necessity and best time point for elective surgery to reach the best possible compromise between surgi-cal interests and the issue of an optimal patient safety.
Frank Weber et al. defend a “wait-and-see” kind of approach concerning the influence of the daily practice due to the debate on neuro-toxicity and supported this by valid evidence and an unexcited but consequent questioning of daily practice. this is actually the only rea-sonable way forward. We share their desire for more evidence from future clinical prospective trials. We would like to extend this request to an increased use and evaluation of comprehen-sive cardiovascular and cerebral monitors (e.g. Nirs). We need to get close to an optimal ho-meostasis until now the ‘other’ important but less recognized threat to baby brains.
References
1. rappaport Ba, suresh s, Hertz s, evers as, orser Ba. anesthetic neurotoxicity — clinical implications of ani-mal models. N Engl J Med 2015;372:796-7.
2. Weiss M, Bissonnette B, engelhardt t, soriano s. an-esthetists rather than anesthetics are the threat to baby brains. Pediatr Anesth 2013;23:881-2.
3. Weber F, van Beek s, scoones g. Potential neurotoxicity of anaesthetic drugs in young children: who cares? a sur-vey among european anaesthetists. Minerva anestesiol 2016;82:294-303.
4. anand KJ. clinical importance of pain and stress in pre-term neonates. Biol Neonate 1998;73:1-9.
5. Bouza H. the impact of pain in the immature brain. J Matern Fetal Neonatal Med 2009;22:722-32.
6. Porter FL, Grunau RE, Anand KJ. Long-term effects of pain in infants. J Dev Behav Pediatr 1999;20:253-61.
cases only affecting the preoperative plan-ning.
Just 18% reported changes in their individu-al practice of anesthesia. a remarkably portion of one third of the participant declared an an-esthesia without the use of anesthetics (high-dose opioids only and muscle relaxant drugs) to be ethically justifiable. The intention is to avoid cardiovascular instability in those vul-nerable patients. there is good evidence from neonatal intensive care that inadequate seda-tion and analgesia is harmful for developing babies both physically 4, 5 (increasing rate of cerebral hemorrhage) and psychologically 6, 7 (life-time reduced stress and pain-tolerance). this statement, however, does not answer the question, if adequate pain and stress relieve can be achieved by opioids only (for instance remifentanil) or not. At this point, no final judgment can be given and one should not create the impression of being able to achieve this. It just remains to note that some experts perform anesthesia without sedative drugs and some do not.
Modern pediatric anesthesia should be able to achieve both adequate depth of anesthesia and pain control as well as stable cardiovascu-lar conditions. as long as essential questions in neurodevelopment are not answered con-clusively, pediatric anesthesiologists should rely on what is known and can be summarized clearly:
1. local anesthesia should be used wherever applicable and possible (e.g. as a sole method); this allows the amount of sedative medication to be kept low but still achieving clinically ad-equate depth of anesthesia.
2. the focus on homeostasis should result in proper monitoring using all modern methods that are available (e.g. generous use of inva-sive blood pressure measurement and transcu-taneous capnography);
3. a compromised cardiovascular situation must be addressed immediately with appro-priate fluid therapy and catecholamines. This requires prior preparation and practical knowl-edge (e.g. a list how to prepare practicable di-lutions and weight-dependent drug-rates). this is institutional competence;

PEDIATRIC ANESTHESIA AND NEUROTOXICITY IN DAILY PRACTICE KaUFMaNN
Vol. 82 - No. 3 MiNerVa aNestesiologica 261
to increased pain sensitivity in later childhood? Pain 2005;114:444-54.
7. Peters JW, Schouw R, Anand KJ, van Dijk M, Duiv-envoorden HJ, Tibboel D. Does neonatal surgery lead
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: October 20, 2015. - Manuscript accepted: October 19, 2015. - Manuscript received: August 29, 2015.(Cite this article as: Kaufmann J, laschat M. How should pediatric anesthesia respond on the discussion about neurotoxicity in daily practice? Minerva Anestesiol 2016;82:259-61)
262 Minerva anestesiologica March 2016
oxidant capacity and immunoparalysis during their icU stay, it seems attractive to modulate these responses. However, in daily practice the actual immune-status in individual patients is rarely measured. in addition, to demonstrate beneficial effects these immune-modulating nutrients should induce a combination of mul-tiple actions such as reducing an overactive inflammatory response, restoring reduced an-tioxidant capacity and preventing occurrence of immunoparalysis. From a basic science per-spective this may be a wrong assumption and has never been proven for single nutrients and thus can be considered to good to be true.
it has been suggested that low baseline plasma glutamine levels reflect conditional deficiency and are associated with increased mortality. However, recently at least 12 stud-ies challenging aspects of this hypothesis have been summarized.5 at discharge high plasma glutamine levels are associated with increased long-term (1-year) mortality.6 there is a trend that glutamine supplementation confers more harm in patients with higher baseline gluta-mine levels.4 recently several researchers have suggested that glutamine supplemen-tation may be a maladaptive response to an adaptive process.7, 8
With respect to fish oil we lack studies that show an association of low baseline eicosa- pentaenoic acid (ePa) and docosahexaenoic
For decades trials have been performed to study effects of enriched or supplemented
(par)enteral nutrition with immune-modulat-ing macronutrients (e.g. glutamine, arginine and fish-oil) and micronutrients (e.g. selenium, vitamin c, vitamin e, and zinc) versus stan-dard feeds on outcome of ICU patients.1 this concept is also known as pharmaconutrition, suggesting specific nutritional components may exert pharmacological beneficial effects.
In this issue of Minerva Anestesiologica, annetta et al. have reported results of a re-view of the latest evidence-based information on immunonutrition, concluding that there is no convincing evidence that immunonutrients may be beneficial for critically-ill patients.2 they suggest that these substances invariably increase costs of health care and may be unsafe or even harmful in some subgroups, particu-larly in septic patients.3, 4 Therefore, currently routine administration of immune-nutrients (glutamine, arginine, omega-3 fatty acids and selenium) cannot be recommended in the crit-ically-ill.
Why do the latest large multicenter trials not show benefits and even show harm in contrast with earlier observations?
As many ICU patients encounter phases of systemic inflammatory response, reduced anti-
E D I T O R I A L
The end of an era of pharmaconutrition and immunonutrition trials for the critically-ill patient?
Barbara FESTEN, Arthur R. van ZANTEN *
Department of Intensive Care, Gelderse Vallei Hospital, Ede, The Netherlands*Corresponding author: Arthur R. van Zanten, Hospital Medical Director, Department of Intensive Care, Gelderse Vallei Hospital, Ede, The Netherlands. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva anestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: titolo breve: PHARMACONUTRITION AND IMMUNONUTRITION TRIALSprimo autore: FESTENpagine: 262-4citazione: Minerva Anestesiol 2016;82:262-4
comment on p. 320.
Minerva Anestesiologica 2016 March;82(3):262-4© 2015 EDIZIONI MINERVA MEDICAThe online version of this article is located at http://www.minervamedica.it

PHarMaconUtrition anD iMMUnonUtrition trials FESTEN
vol. 82 - no. 3 Minerva anestesiologica 263
lected: ICU patients do not consistently have low baseline glutamine levels.5 Moreover, glu-tamine deficiency is not associated with sever-ity of illness (APACHE–II scores).11
not only low, but also high baseline gluta-mine levels are associated with increased mor-tality.10 in sepsis probably only high glutamine levels are related to mortality, not low levels.11
Based on data from the REDOXS and Meta-Plus studies it was suggested that after gluta-mine supplementation specifically patients with multiple organ dysfunction syndrome, re-nal failure and medical patients with circulato-ry failure were at high-risk for higher 6-month mortality.4, 12
selenium has been studied in randomized clinical trials in critically-ill patients both as monotherapy or in antioxidant cocktails. Me-ta-analyses have suggested benefits with sele-nium therapy in the most severely ill patients. in the largest study on glutamine and antioxi-dants, the REDOXS study, no improvements in clinical outcomes with antioxidants were found and harm was shown in patients with renal dysfunction.11 in addition, the MetaPlus study investigators found increased 6-month mortality in medical patients when provided extra glutamine and selenium in enriched en-teral nutrition. recently, it was suggested that effects of selenium and glutamine may be de-pendent on the dose, the route of administra-tion, and whether administered in combination or with other nutrients and the specific patient population studied.5
Over time benefits of glutamine supple-mentation in studies have disappeared. since 2003 no positive studies on mortality have been published.13 Most beneficial results on glutamine were reported in older single-cen-ter studies. considering exclusive parenteral glutamine supplementation multicenter rcts show increased mortality, in contrast to single center studies showing reduced mortality.14, 15 typically multicenter trials are valued as more important than single-center studies.
in some studies non-isonitrogenous inter-ventions have been studied.5 Benefits of glu-tamine supplementation in these studies may be due to higher protein intake. In addition,
(DHa) levels and worse outcome. Plasma EPA-levels after fish oil supplementation in critically-ill rarely have been studied. there-fore, we cannot be sure whether levels are low in critically-ill patients, and whether supple-mentation normalizes plasma levels and in-duces beneficial or negative effects. This may provide an explanation that with respect to fish oil supplementation divergent results have been published.
supplemental glutamine does not reduce the endogenous production from the muscle in critically-ill patients and muscle production of glutamine in the critically-ill is not maxi-mized. these observations are not concordant with a conditional deficiency hypothesis.5
Free drugs induce pharmacological effects. Maybe we should study associations of im-mune-modulating nutrients taking into account aspects of protein-binding and third-spacing and no longer rely on total plasma levels. Fur-thermore, we are unaware of up-regulation or down-regulation of (post)receptor and other intracellular metabolic pathways for specific immune-modulating nutrients during critical illness.
It is questionable whether reference plasma levels and recommended daily allowances can be extrapolated to critically-ill patients. vita-min D supplementation was recently studied in icU patients. amrein and collaborators used high dose supplementation once at a dose of 540,000 IU followed by monthly maintenance doses of 90,000 IU for 5 months. It did not re-duce hospital length of stay, hospital mortality, or 6-month mortality. in the severe vitamin D deficiency subgroup (≤12 ng/mL) hospital mortality was significantly lower, but this find-ing should be considered hypothesis generat-ing and requires further study. Remarkably, many patients on high dose supplementation did not demonstrate normalized plasma levels of 25-hydroxyvitamin D.9 We lack dose-find-ing studies for almost all immune-modulating nutrients for critically-ill patients.
recent summarized data on glutamine sug-gested we have studied the wrong subgroups of critically-ill patients. Those patients with low glutamine levels were frequently not se-

FESTEN PHarMaconUtrition anD iMMUnonUtrition trials
264 Minerva anestesiologica March 2016
4. Van Zanten AR, Sztark F, Kaisers UX, Zielmann S, Fel-binger TW, Sablotzki AR, et al. High-protein enteral nutrition enriched with immune-modulating nutrients vs standard high-protein enteral nutrition and nosocomial infections in the ICU: a randomized clinical trial. JAMA 2014;312:514-24.
5. Van Zanten AR. Glutamine and antioxidants: status of their use in critical illness. curr opin clin nutr Metab Care 2015;18:179-86.
6. Smedberg M, Grass JN, Pettersson L, Norberg Å, Rooy-ackers O, Wernerman J. Plasma glutamine concentra-tion after intensive care unit discharge: an observational study. Crit Care 2014;18:677.
7. van den Berghe g. low glutamine levels during criti-cal illness--adaptive or maladaptive? N Engl J Med 2013;368:1549-50.
8. Van Zanten AR, Hofman Z, Heyland DK. Consequenc-consequenc-es of the REDOXS and METAPLUS Trials: the end of an era of glutamine and antioxidant supplementation for critically ill patients? JPEN J Parenter Enteral Nutr 2015;39:890-2.
9. Amrein K, Schnedl C, Holl A, Riedl R, Christopher KB, Pachler C, et al. Effect of high-dose vitamin D3 on hospital length of stay in critically ill patients with vi-tamin D deficiency: the VITdAL-ICU randomized clini-cal trial. JAMA 2014;312:1520-30. Erratum in: JAMA 2014;312:1932.
10. Rodas PC, Rooyackers O, Hebert C, Norberg A, Werner-man J. Glutamine and glutathione at ICU admission in relation to outcome. Clin Sci (Lond) 2012;122:591-7.
11. Heyland DK, Elke G, Cook D, Berger MM, Wischmeyer Pe, albert M, et al.; Canadian Critical Care Trials Group. Glutamine and Antioxidants in the critically ill patient: a post hoc analysis of a large-scale randomized trial. JPEN J Parenter Enteral Nutr 2015;39:401-9.
12. Manzanares W, Langlois PL, Heyland DK. Pharmaconu-trition with selenium in critically ill patients: what do we know? Nutr Clin Pract 2015;30:34-43.
13. Fadda V, Maratea D, Trippoli S, Messori A. Temporal trend of short-term mortality in severely ill patients re-ceiving parenteral glutamine supplementation. clin nutr 2013;32:492-3.
14. Wischmeyer PE, Dhaliwal R, McCall M, Ziegler TR, Heyland DK. Parenteral glutamine supplementa-tion in critical illness: a systematic review. Crit Care 2014;18:R76.
15. Pasin L, Landoni G, Zangrillo A. glutamine and antioxidants in critically ill patients. N Engl J Med 2013;369:482-4.
16. Buijs N, Brinkmann SJ, Oosterink JE, Luttikhold J, Schierbeek H, Wisselink W, et al. intravenous glutamine supplementation enhances renal de novo arginine syn-thesis in humans: a stable isotope study. Am J Clin Nutr 2014;100:1385-91.
glutamine can be metabolized to arginine.16 in sepsis patients, arginine supplementation has been associated with increased mortality, possibly by inducing nitric oxide production. Thus, interfering with the glutamine metabolic pathway may potentially lead to unpredictable arginine production.
In conclusion, as the first dictum in medicine is to do no harm, we should now abandon the concept of immunonutrition or pharmaconutri-tion for lack of benefits and serious safety con-cerns, at least until the proper basic research has clarified the potential harmful pathways.8 Moreover, we have to design studies that select patients in homogeneous subgroups of ICU pa-tients, with real deficiencies and not those with adaptive responses. control groups have to be selected carefully, and evidence from small single centers should lead to confirmative pro-spective multicenter trials. critical care nutri-tion has arrived in the era of evidence-based medicine. Supposed beneficial concepts have to be prospectively tested. the latest trials as summarized by annetta et al.,2 in our opinion should lead to revised guidelines downgrading immunonutrition and pharmaconutrition for use in critically-ill patients.
References 1. Hegazi RA, Wischmeyer PE. Clinical review: optimizing
enteral nutrition for critically ill patients--a simple data-driven formula. Crit Care 2011;15:234.
2. annetta Mg, Pittiruti M, vecchiarelli P, silvestri D, cari-cato a, antonelli M. immunonutrients in critically ill pa-tients: an analysis of the most recent literature. Minerva Anestesiol 2015;81:323-34.
3. Heyland D, Muscedere J, Wischmeyer PE, Cook D, Jones G, Albert M, et al.; Canadian Critical Care Trials Group. A randomized trial of glutamine and antioxidants in critically ill patients. N Engl J Med 2013;368:1489-97.
Funding.—Inclusion fees for patients in the MetaPlus trial from Nutricia were paid to the local ICU research foundation.Conflicts of interest.—Dr. Festen declares no conflict of interest. Dr. van Zanten has received honoraria for advisory board meetings, and lectures, and travel expenses from Abbott, Baxter, Danone, Fresenius Kabi, Nestlé, Novartis, and Nutricia.Article first published online: July 28, 2015. - Manuscript accepted: July 23, 2015. - Manuscript revised: July 22, 2015. - Manuscript received: May 27, 2015.(Cite this article as: Festen B, van Zanten AR. The end of an era of pharmaconutrition and immunonutrition trials for the critically-ill patient? Minerva Anestesiol 2016;82:262-4)

Vol. 82 - No. 3 MiNerVa aNestesiologica 265
thors report a useful classification of the risk factors identified by several studies: patient versus procedure-related and modifiable ver-sus non-modifiable factors. The most intrigu-ing message of this review is that two main pitfalls hamper the translation in the clinical practice of the knowledge derived from studies on predictive scores: first, describing and ex-plaining statistical associations does not nec-essarily mean predicting outcome; second, the physician needs reliable and validated tools to modify the clinical practice in order to reduce incidence of PPCs.
Every year more than two hundreds millions major surgical procedures are performed, with a significant burden in terms of public health costs and more than one million patients devel-oping complications,3 with PPCs being a major determinant.4 Thus, risk stratification for PPCs could be a first important step toward a reduc-tion in surgery-related mortality, which has been shown to be higher than expected in large prospective multicenter studies such as the Eu-ropean Surgical Outcomes Study (EuSOS).5
The single risk factors identified by the dif-ferent cohort studies are not univocal. The most reported ones are advanced age,2, 6, 7 low preoperative SpO2,2 recent respiratory infec-tion,2 preoperative anemia,2 type or setting of surgery,2, 6, 8 duration of surgery,2, 7 high Amer-
in this issue of Minerva Anestesiologica, Mazo et al.1 present a systematic review and
in-depth analysis concerning the development and clinical application, in form of scores, of predictive models for postoperative pulmo-nary complications (PPC). The authors pro-pose an articulate methodological reflection on the design, validation and implementation of these clinical scores. The attention is ini-tially focused on statistical modeling, discuss-ing the appropriateness of choice of potential predictors of outcome, as well as the relevance of external validation of predictive scores. In anesthesia, there is particular interest towards simple clinical predictors of PPCs that can be assessed at the pre-operative visit. In this paper, Mazo et al. underline how researchers should make efforts to translate descriptive explanatory models into useful tools for the clinical practice. The authors report that, sur-prisingly, despite the high incidence of PPCs, limited efforts were made by the scientific community to validate scores to predict their incidence: since 2000, 1519 studies in differ-ent fields of medicine included prospective ex-ternal validation of risk scores, of them only 40 concerning the postoperative period, and only one regarding PPCs incidence.2 the au-
E D I T O R I A L
Predictive scores for postoperative pulmonary complications:
time to move towards clinical practiceLorenzo BALL, Paolo PELOSI*
Department of Surgical Sciences and Integrated Diagnostics, IRCCS AOU San Martino-IST, University of Genoa, Genoa, Italy*Corresponding author: Paolo Pelosi, Department of Surgical Sciences and Integrated Diagnostics, IRCCS AOU San Martino-IST, University of Genova, Largo Rosanna Benzi 8, 16131 Genova, Italy. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva AnestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: 10788-MAStitolo breve: PREDICTIVE SCORES FOR PPCprimo autore: BALLpagine: 265-7citazione: Minerva Anestesiol 2016;82:265-7
Comment on p. 332.
Minerva Anestesiologica 2016 March;82(3):265-7© 2015 EDIZIONI MINERVA MEDICAThe online version of this article is located at http://www.minervamedica.it

BALL PREDICTIVE SCORES FOR PPC
266 MiNerVa aNestesiologica March 2016
along with a careful respiratory monitoring 14 seems to be a preventive measure that any cli-nician could and should implement.
Several preoperative interventions have been suggested to reduce the incidence of PPCs: smoking cessation, correction of ane-mia, delaying surgery in patients with recent respiratory infection, choosing shorter surgical procedures in high-risk patients. Concerning postoperative management, different measures have been tested or are under investigation, in-cluding but not limited to postoperative incen-tive spirometry or respiratory physiotherapy, bundle interventions like the I-COUGH proto-col15 and postoperative short-term CPAP. Most of these strategies have not been systemati-cally tested on large prospective randomized trials: this opens a new space for predictive scores. In fact, patient selection based on vali-dated predictive scores should be considered in the design of all future studies, in order to rapidly achieve an adequate level of evidence on preventive measures, identifying sub-sets of high-risk patients potentially benefiting from the different approaches.
The methodological robustness advocated by Mazo and coworkers1 should be an epitome for research practice, not limited to the field of prevention of postoperative pulmonary com-plications. Figure 1 illustrates applications of predictive scores for PPCs in clinical activ-ity and research. Concerning research, scores can help in the design of smaller pilot studies focusing on high-risk patients, and in wider cohorts are useful to match or stratify patient subgroups according to their risk class.
Reducing complications, hospital length of stay and ultimately patient mortality after sur-gery will be a challenge in the next decades. A battle that must be fought by researchers alongside with first-line clinicians, with the consciousness that every single measure that we adopt in the clinical routine has a small impact on percent incidence of complications but, given the high and growing number of sur-gical interventions performed every day, this translates in thousands of lives that could be potentially saved: it is time to move towards the clinical practice!
ican Society of Anesthesiologists class,6, 8 chronic obstructive pulmonary disease,6,8 con-gestive heart failure,6, 8 perioperative nasogas-tric tube placement7 and positive cough test.7 Not all of these factors are easy to modify, thus the road to clinical application of predictive scores splits in two interconnected paths: risk assessment and tailored patient management. A quick risk stratification seems a reasonable way for a better resource allocation,9 choosing at the preoperative visit which patients could benefit from a planned admission to the inten-sive care unit, the postanesthesia care unit or the direct admission to the surgical ward. Peri-operative care medicine is a growing branch of anesthesiology, investigating different in-terventions that can modify the course of the occurrence of postoperative complications. It has been widely demonstrated that mechanical ventilation itself can initiate lung injury also in healthy lungs, providing the rationale for applying protective ventilation strategies also in the operating room,10, 11 and a recent meta-analysis concluded that the routine application of low tidal volumes should be considered for all patients,12 while the role of routine high PEEP plus recruitment maneuvers alone was reshaped by a large randomized trial.13 Thus, adopting protective ventilatory strategies12
Figure 1.—Potential applications of scores for predicting postoperative pulmonary complications.

PREDICTIVE SCORES FOR PPC BALL
Vol. 82 - No. 3 MiNerVa aNestesiologica 267
tive respiratory complications. Anesthesiology 2013; 118:1276-85.
9. Mazo V, Sabate S, Canet J. A race against time: planning postoperative critical care. Anesthesiology 2013;119:498-500.
10. Eikermann M, Kurth T. Apply Protective Mechanical Ventilation in the Operating Room in an Individualized Approach to Perioperative Respiratory Care. Anesthesi-ology 2015;123:12-4.
11. Guldner A, Kiss T, Serpa Neto A, Hemmes SN, Canet J, Spieth PM, et al. Intraoperative Protective Mechani-cal Ventilation for Prevention of Postoperative Pulmo-nary Complications: A Comprehensive Review of the Role of Tidal Volume, Positive End-expiratory Pres-sure, and Lung Recruitment Maneuvers. Anesthesiology 2015;123:692-713.
12. Serpa Neto A, Hemmes SN, Barbas CS, Beiderlinden M, Biehl M, Binnekade JM, et al. Protective versus Conven-tional Ventilation for Surgery: A Systematic Review and Individual Patient Data Meta-analysis. Anesthesiology 2015;123:66-78.
13. Hemmes SN, Gama de Abreu M, Pelosi P, Schultz MJ. High versus low positive end-expiratory pressure dur-ing general anaesthesia for open abdominal surgery (PROVHILO trial): a multicentre randomised controlled trial. Lancet 2014;384:495-503.
14. Ball L, Sutherasan Y, Pelosi P. Monitoring respiration: what the clinician needs to know. Best Pract Res Clin An-aesthesiol 2013;27:209-23.
15. Cassidy MR, Rosenkranz P, McCabe K, Rosen JE, McAneny D. I COUGH: reducing postoperative pulmo-nary complications with a multidisciplinary patient care program. JAMA Surg 2013;148:740-5.
References 1. Mazo V, Sabaté S, Canet J. How to optimize and use pre-
dictive models for postoperative pulmonary complica-tions. Minerva Anestesiol 2016;82:335-45.
2. Mazo V, Sabate S, Canet J, Gallart L, de Abreu MG, Bel-da J, et al. Prospective external validation of a predictive score for postoperative pulmonary complications. Anes-thesiology 2014;121:219-31.
3. Weiser TG, Makary MA, Haynes AB, Dziekan G, Berry WR, Gawande AA, et al. Standardised metrics for global surgical surveillance. Lancet 2009;374:1113-7.
4. Serpa Neto A, Hemmes SN, Barbas CS, Beiderlinden M, Fernandez-Bustamante A, Futier E, et al. Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or tho-racic surgery: a systematic review and meta-analysis. Lancet Respir Med 2014;2:1007-15.
5. Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, spies c, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet 2012;380:1059-65.
6. Smetana GW, Lawrence VA, Cornell JE, American Col-lege of P. Preoperative pulmonary risk stratification for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006;144:581-95.
7. McAlister FA, Bertsch K, Man J, Bradley J, Jacka M. In-cidence of and risk factors for pulmonary complications after nonthoracic surgery. Am J Respir Crit Care Med 2005;171:514-7.
8. Brueckmann B, Villa-Uribe JL, Bateman BT, Grosse-Sundrup M, Hess DR, Schlett CL, et al. Development and validation of a score for prediction of postopera-
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: September 3, 2015. - Manuscript accepted: July 31, 2015. - Manuscript revised: July 23, 2015. - Manu-script received: July 2, 2015.(Cite this article as: Ball L, Pelosi P. Predictive scores for postoperative pulmonary complications: time to move towards clinical practice. Minerva Anestesiol 2016;82:265-7)

268 Minerva anestesiologica March 2016
different combinations will likely be needed to fulfil different roles. Moreover, no test will ever be perfect and all biomarkers will have to be used in conjunction with other clinical elements.
As highlighted by Douglas and Russell,4 biomarkers have three key potential roles in sepsis: diagnosis, prediction of response to therapy, and prognosis. Accurate recognition of the presence of an infection is vital, espe-cially if the infection is associated with some form of organ dysfunction (what we call “sep-sis”). In these conditions, early diagnosis, al-lowing rapid, appropriate therapy to be started, is of utmost importance to prevent complica-tions and deterioration into multiple organ failure and death.5, 6 Importantly, diagnostic techniques can involve not only identifying the presence of infection, but also ruling out infec-tion in a patient with suggestive clinical signs and symptoms, but who may not need antibi-otics. Biomarkers can also help to separate vi-ral from bacterial infections, or may indicate that coverage of fungal pathogens is necessary (or not, so avoiding unnecessary antifungal therapy). Some techniques, for example using microbial DNA, can also help more rapidly identify specific microorganisms than conven-tional microbiological techniques.7 although this approach is not perfect and cannot (yet) replace traditional culture and sensitivity test-
our understanding of the molecular mecha-nisms of sepsis has advanced immeasur-
ably since Schottmueller first made the link 100 years ago between infection and the host response stating that “Sepsis is present if a focus has developed from which pathogenic bacteria, constantly or periodically, invade the blood stream in such a way that this causes subjective and objective symptoms”.1 We now know that sepsis, the dysregulated host response to infection,2 is a highly complex reaction that involves the expression of hun-dreds of genes and the repression of a similar number.3 Yet, there is still much we do not un-derstand. In this issue of Minerva Anestesiolo-gica, Douglas and Russell, established experts in this field, provide a comprehensive article 4 covering some of the newly developed (and developing) genomics technology that will help unravel further the complexities of sepsis, and importantly what impact this new knowl-edge may have on our ability to more effec-tively and rapidly diagnose and treat sepsis by the identification and validation of biomarkers.
Given the multifaceted nature of the sepsis response, the chances of finding a single sep-sis (bio)marker are remote; this concept is too naïve. Rather, combinations of biomarkers will be of greater value and more reliable, and
E D I T O R I A L
How genomics can improve the management of septic patients
Jean-louis vincent
Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles, Brussels, BelgiumCorresponding author: Jean-Louis Vincent, Department of Intensive Care, Erasme Hospital, Route de Lennik 808, 1070 Brussels, Belgium. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva AnestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: 10854-MAStitolo breve: GENOMICS IN SEPSIS MANAGEMENTprimo autore: VINCENTpagine: 268-70citazione: Minerva Anestesiol 2016;82:000-000
Comment on p. 343.
Minerva Anestesiologica 2016 March;82(3):268-70© 2015 eDiZioni Minerva MeDicaThe online version of this article is located at http://www.minervamedica.it

GENOMICS IN SEPSIS MANAGEMENT vincent
Vol. 82 - No. 3 Minerva anestesiologica 269
most from activated protein C,9 although this observation came too late for this drug, which is no longer available.10 Nevertheless, related compounds will likely appear in the future and may benefit from this approach. Improved use of steroids is another example. Wong et al. re-vealed how steroids can modify gene expres-sion in septic patients 11 and later showed how this approach could help to identify patients in septic shock who may benefit from steroids, or be harmed by them.12
Mortality rates for patients with sepsis re-main unacceptably high, yet results of studies of new therapies in patients with sepsis have been disappointing. The field of genomics is opening up a whole new means of diagnosing, prognosticating, and directing treatment in sepsis, which will necessitate a change in our approach to the management of these patients and to trial design. The review by Douglas and russell 4 provides an excellent base to help understand current use of this technology and explore future applications.
References
1. Schottmueller H. Wesen und Behandlung der Sepsis. Inn Med 1914;31:257-80.
2. Vincent JL, Opal S, Marshall JC, Tracey KJ. Sepsis defi-nitions: time for change. Lancet 2013;381:774-5.
3. Wong HR, Cvijanovich N, Allen GL, Lin R, Anas N, Meyer K, et al. Genomic expression profiling across the pediatric systemic inflammatory response syn-drome, sepsis, and septic shock spectrum. Crit Care Med 2009;37:1558-66.
4. Douglas JJ, Russell JA. The role of genomics to identify biomarkers and signaling molecules during severe sepsis. Minerva Anestesiol 2016;82:346-61.
5. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: interna-tional guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39:165-228.
6. Weiss SL, Fitzgerald JC, Balamuth F, Alpern ER, Lavelle J, Chilutti M et al. Delayed antimicrobial therapy increas-es mortality and organ dysfunction duration in pediatric sepsis. Crit Care Med 2014;42:2409-17.
7. Vincent JL, Brealey D, Libert N, Abidi NE, O’Dwyer M, Zacharowski K, et al. Rapid Diagnosis of Infection in the Critically Ill (RADICAL), a multicenter study of molecu-lar detection in bloodstream infections, pneumonia and sterile site infections. Crit Care Med 2015;43:2283-91.
8. Bouadma L, Luyt CE, Tubach F, Cracco C, Alvarez A, Schwebel, C et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet 2010;375:463-74.
9. Man M, Close SL, Shaw AD, Bernard GR, Douglas IS,
ing, it may help orient early antibiotic choices towards the most likely causative organisms.
Many biomarker studies have demonstrat-ed that the concentration of the biomarker in question is higher in non-survivors than in sur-vivors of sepsis. But the use of sepsis mark-ers for prognosis is probably less relevant to the clinician. Prognostic biomarkers can help in triage decisions, because a patient with biomarker values suggestive of severe infec-tion should probably be admitted to the ICU rather than to the regular floor. However, it is extremely unlikely that decisions to discon-tinue therapeutic efforts would (or should) be based on the level of a biomarker. In fact, the opposite may be true; for example, one would not withdraw life support if a raised biomarker level indicated that there was a chance of per-sisting sepsis with, therefore, some remaining hope of treatment and cure.
Perhaps the most appealing use of biomark-ers is their potential therapeutic application. In this context, they have several potential functions. First, repeated measurements can help follow the response to therapy. A change in biomarker level, indicating reduced sever-ity of infection, could be used as a surrogate for an appropriate response to therapy. If there is a marked and consistent change, this could be seen as an indication to shorten the dura-tion of the antibiotic therapy.8 If, on the other hand, biomarker values do not change in the right direction, this may indicate that the anti-biotic regimen is not appropriate and should be altered, a reassessment of the need to drain a septic source should be made, and/or a further search for an infected focus should be institut-ed. A second possible therapeutic application is in the correct orientation of therapy. Genom-ics, proteomics, metabolomics can identify the predominant processes in individual patients enabling therapies to be targeted more appro-priately than is currently the case. As a simple example, a patient who expresses a lot of tumor necrosis factor (TNF) will be more likely to benefit from anti-TNF strategies than a patient with less-marked TNF expression. Likewise, genetic markers could potentially have helped to identify patients who would have benefited

vincent GENOMICS IN SEPSIS MANAGEMENT
270 Minerva anestesiologica March 2016
with repression of adaptive immunity gene programs in pediatric septic shock. Am J Respir Crit Care Med 2014;189:940-6.
12. Wong HR, Cvijanovich NZ, Anas N, Allen GL, Thomas NJ, Bigham MT, et al. Developing a clinically feasible personalized medicine approach to pediatric septic shock. Am J Respir Crit Care Med 2015;191:309-15.
Kaner RJ, et al. Beyond single-marker analyses: mining whole genome scans for insights into treatment responses in severe sepsis. Pharmacogenomics J 2013;13:218-26.
10. Vincent JL. The rise and fall of drotrecogin alfa (activat-ed). Lancet Infect Dis 2012;12:649-51.
11. Wong HR, Cvijanovich NZ, Allen GL, Thomas NJ, Fre-ishtat RJ, Anas N, et al. corticosteroids are associated
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: September 3, 2015. - Manuscript accepted: September 3, 2015. - Manuscript received: July 31, 2015.(Cite this article as: Vincent JL. How genomics can improve the management of septic patients. Minerva Anestesiol 2016;82:268-70)
Vol. 82 - No. 3 MiNerVa aNestesiologica 271
From an ethical point of view, DcD pro-grams should be supported by a large scale awareness of the fact that DcD donation never affects patient treatment in terms of appro-priateness criteria. Most potential DcD do-nors die in icU after limitation of futile treat-ment including life support (controlled DcD, cDcD);6 in this case, organ donation repre-sents an acceptable end-of-life outcome.4, 5, 7
in italy, cDcD has been previously con-sidered unadvisable 8 in view of a probable conflict of interest in end-of-life procedures, which still pose problems in spite of the ex-cellent guidelines provided by the italian so-ciety of anesthesiology and intensive care (siaarti).9
italian law demands an excessive certainty of death, requesting an absence of ecg activity for 20 minutes, against the 5 minutes required in most countries; thus DcD has been consid-ered unsuitable in italy in spite of successful DcD programs run in several countries.10
Nevertheless, since 2007 the pilot project alba 11 has proved that DcD is possible in ita-ly for kidney transplantation after unexpected cardiac arrest occurring outside or inside the hospital (uncontrolled DcD, uDcD),6 using post mortem abdominal organ perfusion by ECMO before retrieval. Unfortunately, diffi-culties in organization and shortage in resourc-es have limited this procedure and the number of utilized organs.
Deceased organ donation (oD) should be strongly pursued as an essential target
of the Health system, basically in intensive care units (icU) and emergency Departments (eD), since a great number of patients await-ing a transplant cannot benefit from this life saving treatment due to the persisting organ shortage.1 Deceased oD may occur after death declaration based on neurological criteria (do-nation after brain death, DBD) or cardiac cri-teria (donation after circulatory death, DcD).2
in 2014, italy achieved 1383 donors and only one after cardiac death, leading to 2981 transplants against more than 8800 awaiting patients.3
ethical and clinical cornerstones related to donation procedures are high quality patient treatment and full respect of the dead-donor rule.
Unfortunately oD is an uncommon activity for most icU professionals and not system-atically included into end-of-life patients. Pro-gressive changes in etiology and the increased age of patients dying in icU with acute cere-bral lesions might greatly decrease the number of brain deaths and DBD transplantable organs. consequently DcD becomes a strategic target for the future; yet, DcD should never replace donation after brain death, which represents the essential context for multiorgan recovery.4, 5
E D I T O R I A L
organ donation after circulatory death in italy? Yes we can!
alessandro NaNNi costa, Francesco Procaccio *
centro Nazionale trapianti (cNt), istituto superiore di sanità, rome, italy*corresponding author: Francesco Procaccio, via giano Della Bella, 34, rome, italy. e-mail: [email protected]
anno: 2016Mese: MarchVolume: 82No: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 11021-Mastitolo breve: orgaN DoNatioN aFter circUlatorY DeatH iN italYprimo autore: NaNNi costapagine: 271-3citazione: Minerva anestesiol 2016;82:000-000
comment on p. 359.
Minerva anestesiologica 2016 March;82(3):271-3© 2015 eDiZioNi MiNerVa MeDicathe online version of this article is located at http://www.minervamedica.it

NaNNi costa orgaN DoNatioN aFter circUlatorY DeatH iN italY
272 MiNerVa aNestesiologica March 2016
prolongation of ischemic organ damage, on the basis of international consensus.20
it is notable that DcD donations leading to kidney and liver transplants have been recently and successfully performed in italian hospitals besides the pilot alba project; different death modalities in icU and innovative sequences of organ preservation have been managed with comprehensive medical expertise and organi-zation derived from DBD donor treatment and organ preservation. in our opinion, some criti-cal facts should be taken into consideration:
— intensivists and surgeons can be flex-ible and efficient in identifying potential DCD donors and managing recovered organs: these procedures seem to easily blend into the na-tional and regional networks;
— preclinical and standardized clinical data are lacking in the italian context: only ad hoc trials and national registries might validate decisions by controlled outcome studies;
— rules and policies that make italy one of the leader countries for safety and quality in transplantation can be properly applied to DcD programs;
— national governance of DcD programs is needed to recommend regional sustainable economical criteria, share experiences among centers and optimize results.
a great number of citizens declare their will to donate their organs after death realizing a magnificent act of personal and social value. But their wishes can be fulfilled only if the health system makes both DBD and DcD do-nation feasible in all the italian hospitals that are well recognized for their excellence in crit-ical care thanks to intensivists’ commitment and clinical leadership. organ donation after circulatory death is by now within our range, “integrating the highest standard of care for the dying and the legitimate interests of those awaiting a life-saving organ”.19
References
1. WHo: the Madrid resolution on organ donation and transplantation: national responsibility in meeting the needs of patients, guided by the WHo principles. trans-plantation 2011;91suppl 11: s29-31.
in 2014 an innovative DcD protocol for lung donation has been successfully imple-mented using lung protective maneuvers and ex vivo reconditioning (Valenza F, personal communication). since organ reperfusion may ideally improve perspectives of organ viability after warm ischemia,12 DcD can be practiced in italy without a previous shortening of the no-touch period, which would be desirable in the near future.
in order to clarify criteria for DcD dissemi-nation in italy,13 a strong partnership between the italian National centre for transplantation (CNT) and Scientific Societies was mandato-ry.14 First of all, cNt has provided a position paper 15 and an operative document,16 encour-aging DcD programs in those hospitals which already experienced advanced treatment of cardiovascular failure routinely including ex-tracorporeal life-support (ecls). Death dur-ing ecls can be determined either by neu-rological or cardiac criteria;17 thus both DBD or DcD may occur, being ecMo continued 18 or restarted after death declaration to limit the ischemic organ damage and monitor function-ality before recovery.
in this issue of Minerva Anestesiologica, giannini et al.19 present the results of the joint committee on DcD appointed by siaarti and the italian society for transplantation.
this paper can be a precious tool for all professionals potentially involved in DcD or-gan donation since it deals with critical issues and essential messages, concerning the ethical reasons and clinical results of DcD as well as practical criteria for invasive maneuvers be-fore and after death declaration.
the authors consider the dissemination of uDcD feasible and underline the urgent need of an open debate on cDcD in the italian con-test. comprehensive education and training is needed to spread basic knowledge of the DcD process among professionals and increase the awareness that both DBD and DcD are possible and appropriate, as logical and ethical conclu-sion of end-of life care in icUs and emergency Departments.5, 7 Finally, it is clearly suggested that the current 20-minute period should be reconsidered and shortened, as unnecessary

orgaN DoNatioN aFter circUlatorY DeatH iN italY NaNNi costa
Vol. 82 - No. 3 MiNerVa aNestesiologica 273
death: current practices, ongoing challenges and potential improvements (review). transplantation 2014;97:258-64.
13. Fanelli V, geraci PM, Mascia l. Donation after cardiac death: is a “paradigm shift” feasible in italy? Minerva anestesiol 2013;79:534-40.
14. Vesconi s, Procaccio F. Donation after cardiocirculatory death in italy? it is within our range. Minerva anestesiol 2013;79:1443.
15. cNt Position Paper: Determinazione di morte con criteri cardiaci. Prelievo di organi a scopo di trapianto da dona-tore in asistolia. elementi informativi essenziali (parte i); [internet]. avaiable from: http://trapianti.net/wp-content/uploads/2013/10/PP_DcD_Parteprima_10_luglio_.pdf [cited 2015, oct 30].
16. cNt: Donazione di organi a cuore fermo (DcD) in ita-lia. (raccomandazioni operative); [internet]. available from: http://trapianti.net/wpcontent/uploads/2013/10/raccomandazioni_operative_DcD_08_.pdf [cited 2015, oct 30].
17. cNt: criteri clinici e raccomandazioni pratiche inerenti l’accertamento di morte di soggetti sottoposti ad assisten-za circolatoria extracorporeal. [internet]. available from: http://trapianti.net/wp-content/uploads/2015/10/lg_ ecMo_-Def.pdf [cited 2015, oct 24].
18. Migliaccio Ml, Zagli g, cianchi g, lazzeri c, Bo-nizzoli M, cecchi a, et al. extracorporeal membra-ne oxygenation in brain-death organ and tissues do-nors: a single-centre experience (letter). Br J anaesth 2013;111:673.
19. Giannini A, Abelli A, Azzoni P, Biancofiore G, Citterio F, geraci P, et al. “Why can’t i give you my organs after my heart has stopped beating?” an overview of the main clinical, organisational, ethical and legal issues concerning organ donation after circulatory death in italy. Minerva an-. Minerva an-estesiol 2016;82:362-71.
20. shemie sD, Hornby l, Baker a, teitelbaum J, torrance s, Young K, et al. international guideline development for the determination of death. intensive care Med 2014;40:788-97.
2. Domínguez-gil B, Delmonico Fl, shaheen Fa, Mate-sanz r, o’connor K, Minina M, et al. the critical path-the critical path-way for deceased donation: reportable uniformity in the approach to deceased donation. transpl int 2011;24:373-8.
3. sistema informativo trapianti, centro Nazionale tra-pianti. attività di donazione al 31 Dicembre 2014; [in-ternet]. available from: http://www.trapianti.salute.gov.it/imgs/c_17_pubblicazioni_2380_allegato.pdf [cited 2015, oct 24].
4. Manara ar, Murphy Pg, o’callaghan g. Donation after circulatory death. Br J anaesth 2012;108:108-21.
5. Domínguez-gil B, Murphy P, Procaccio F. the ten small changes that could improve organ donation in the inten-sive care Unit. int care Med 2016;42:264-7.
6. Kootstra g, Daemen JH, oomen aP: categories of non-heart-beating donors. transplantation Proc 1995;27:2893-4
7. accorD consortium. Variations in end-of-life care pathways for patients with a devastating brain injury in europe. Final Deliverable; [internet]. available from: http://www.accordja.eu/sites/default/files/down-load_documents/accorD_WP5_Variations_in_end-of-life_care_pathways__for_patients_with_a_devastat-ing_brain_injury_in_europe.pdf [cited 2015, oct 24].
8. comitato Nazionale per la Bioetica. i criteri di accer-tamento della morte; 2010 [internet]. available from: http://www.governo.it/bioetica/pareri_abstract/criteri_accertamento_morte20100624.pdf [cited 2015, oct 24].
9. end-of-life care and the intensivist: siaarti recom-mendations on the management of the dying patient. Minerva anestesiol 2006;72:927-6
10. Domínguez-gil B, Haase-Kmomwijk B, Van leiden H, Neuberger J, coene l, Morel P, et al. current situation of donation after circulatory death in european countries. transpl int 2011;24:676-86.
11. geraci P, sepe V. Non-heart-beating organ donation in italy. Minerva anestesiol 2011;77:613-23.
12. Morrissey Pe, Monaco aP. Donation after circulatory
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: November 17, 2015. - Manuscript accepted: November 13, 2015. - Manuscript received: November 3, 2015.(Cite this article as: Nanni costa a, Procaccio F. organ donation after circulatory death in italy? Yes we can! Minerva anestesiol 2016;82:271-3)
274 Minerva anestesiologica March 2016
moderate to severe postoperative acute pain 2 and as many as 20-53% of tKa patients will present with chronic pain.3, 4 the negative im-pact of pain on the rehabilitation and quality of life strongly contributes to poor outcome and dissatisfaction.5 With the expected growing number of procedures performed every year,6 pain after tKa currently represents a major health related problem.
Recent developments in the field of post-
Despite progresses made in the understand-ing of pain mechanisms and the introduc-
tion of new concepts and techniques (i.e. lo-co-regional techniques, preventive analgesia), both acute and persistent pain after total knee arthroplasty (tKa) still stand as an unresolved issue.1 tKa, a major joint surgery, is a painful procedure, 45 to 58% of patients experiencing
O R I G I N A L A R T I C L E
Dynamic view of postoperative pain evolution after total knee arthroplasty:
a prospective observational studyirina grosU 1 *, emmanuel tHienPont 2, Marc De KocK 1,
Jean louis scHoltes 1, Patricia lavanD’HoMMe 1
1Department of anesthesiology, saint luc University clinic, catholic University of louvain, Brussels, Belgium; 2Department of orthopaedic surgery, saint luc University clinic, University catholic University of louvain, Brussels, Belgium*corresponding author: irina grosu, secrétariat d’anesthésiologie, 10 avenue Hippocrate 1200 Bruxelles, Belgium. e-mail: [email protected]
anno: 2016Mese: Marchvolume: 82no: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10420-Mastitolo breve: DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKaprimo autore: grosUpagine: 274-83citazione: Minerva anestesiol 2016;82:274-83
a B s t r a c tBacKgroUnD: Having a dynamic view of postoperative pain resolution allows a better understanding of the transi-tion towards chronic pain. sleep and quality of life are important determinants of satisfaction after total knee arthroplasty (tKa), besides functional recovery and pain.MetHoDs: For 114 patients undergoing tKa we recorded the presence of pain at rest, pain evoked at movement and pain located at the incision site in the acute (postoperative day 1, 2, 3, 8), subacute (30 days, 3 months) and chronic (6 months and 1 year) period. analgesics consumption and need of medical assistance for pain were questioned. Quality of life measured by the impact on enjoyment of life, sleep and mood were monitored.resUlts: average incidence for subacute pain was 54% at rest, 66% at mobilization. For chronic pain, the incidence was 14% at rest, 22% during mobilization. Pain at rest peaked at day 30 while pain during mobilization displayed a pla-teau between day 8 and 3 months. three per cent of the patients complained at 1 year of pain at the incision site. 11% of patients still took analgesics one year after the surgery. More than 40% of patients reported moderate to severe alterations of sleep and quality of life in the acute period, decreasing to less than a half at one year.conclUsions: the trajectories of the different types of pain after tKa show their non-linear evolution, highlighting the need of a better pain control at precise moments. sleep disturbances and alterations of quality of life are still present one year after the surgery.(Cite this article as: grosu i, thienpont e, De Kock M, scholtes Jl, lavand’Homme P. Dynamic view of postoperative pain evolution after total knee arthroplasty: a prospective observational study. Minerva anestesiol 2016;82:274-83)Key words: Pain - arthroplasty, replacement, Knee - Quality of life - Pain.
comment in p. 257
Minerva anestesiologica 2016 March;82(3):274-83© 2015 eDiZioni Minerva MeDicathe online version of this article is located at http://www.minervamedica.it

DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa grosU
vol. 82 - no. 3 Minerva anestesiologica 275
the primary objectives of this study are: 1) to follow the evolution of the different compo-nents involved in pain after tKa, knee pain at rest, pain at mobilization and pain located at the incision site along with the need of anal-gesic treatment over one year after the proce-dure; and 2) to examine the quality of life by the components enjoyment of life, sleep and mood over the same period.
the secondary objectives were to observe the influence of acute and subacute pain on chronic pain and the influence of preoperative opioid intake on postoperative pain behavior.
Materials and methods
after approval by the institutional ethical committee (University catholic of louvain, Brussels, Belgium, iPorP 2008/04Fev/45) and written informed consent, patients sched-uled for primary tKa by a single surgeon (e.t.) were included in this prospective ob-servational study between august 2009 and December 2010. the follow-up period was 12 months. the exclusion criteria were patient’s refusal to participate, inability to understand French and to answer the questionnaires and contra-indications to one or more of the drugs used in the multimodal analgesic regimen.
Perioperative management
cemented posterior-stabilized tKa was performed through a minimally invasive me-dial parapatellar approach. surgery was per-formed under general anesthesia including sin-gle dose of ketamine at induction, sufentanil, propofol and atracurium. Maintenance was obtained with sevoflurane in a mixture of oxy-gen/air (50%-50%). the doses of drugs used for anesthesia were left to the discretion of the anesthetist in charge of the patient. a laryngeal masque airway was used in the absence of con-traindications.
cefazolin for infection prophylaxis and tranexamic acid were administered to all pa-tients before incision of the skin. low molecu-lar weight heparin (enoxaparin adapted to the patient’s weight) was given s.c. daily begin-
operative pain have highlighted the benefit of having a dynamic view of postoperative pain resolution to better understand the tran-sition towards persistent pain and thereby to realize risk stratification for patients prone to develop chronic pain.7, 8 studies have clearly shown that the severity of acute pain is a risk factor for developing chronic pain after gen-eral surgery as well as after tKa 9 and the development of pain trajectories is a recent concept allowing to get a better view of pain resolution.10, 11 The identification of patients that will exhibit greater pain scores in the subacute period seems possible as reported after tKa 11 but to our knowledge, no pain trajectories going from acute, to subacute and finally chronic pain have been reported yet after tKa. only a small fraction of the stud-ies reporting pain after knee arthroplasty use adequate validated scores to evaluate pain, while their majority assess pain by using pain scores included as secondary parameters of postsurgery functional knee scores (WoM-ac 12, oxford Knee score 13). even less stud-ies take in consideration the different types of pain existent after knee arthroplasty i.e. pain at rest and pain during mobilization, which have different mechanisms, characteristics and implications on patient functional recov-ery and quality of life.14
even if tKa is usually an effective proce-dure in alleviating pain and functional disabil-ity, a significant proportion of patients report a poor quality of life after tKa.15 the self-reported outcomes in terms of quality of life do not always correlate with the successful clinical and radiological results and stand as an independent predictor of poor satisfaction af-ter tKa.16 it has been already pointed out that sleep disturbances affect a big proportion of patients in the acute postoperative period.2, 17 improving the quality of life in all its affected dimensions arises though as an independent goal after tKa. Disturbances of sleep and other components of the quality of life should be assessed along with residual pain and func-tional recovery on longer periods and specific measures would logically result in better out-comes after tKa.

grosU DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa
276 Minerva anestesiologica March 2016
and then at home at day 8, day 30, 3 months, 6 months and 1 year after tKa by phone inter-view (Figure 1).
We considered 3 periods during postopera-tive pain evolution: 1. acute pain, from day 1 to day 8, 2. subacute pain, from day 8 until 3 months and 3. chronic pain beyond 3 months (at 6 and 12 months) after knee replacement.
analgesics consumption, including medica-tion’s name and dose and the need of medi-cal assistance for pain were also questioned at home.
Finally, once the patient returned home, the impact of pain on the daily quality of life as expressed by mood, sleep and enjoyment of life were evaluated with the French version of the Brief Pain inventory (BPi) question-naire.19
Statistical analysis
statistical analysis was performed with sig-mastat® 3.5 (systat software gmbH, erkrath, germany). results are expressed as mean±sD or median (interquartile range). the normal
ning 8 hours after the surgery for 21 days post-operatively for thromboprophylaxis.
Postoperative pain was managed by stan-dardized multimodal analgesia. a single shot femoral nerve block was performed with 20 ml of 0.5% ropivacaine before surgery. Pa-tients with negative Preincisional test were excluded. all patients received 200 mg cele-coxib every 12 hours and 1 g paracetamol ev-ery 6 hours. oral morphine 10 mg with rapid onset of action was available as rescue anal-gesic treatment on patient request. after dis-charge from the hospital and for a period of three weeks, the patients continued to take 200 mg celecoxib every 12 hours, 1 g paracetamol every 6 hours and tramadol if needed, maxi-mum 400 mg a day. thereafter, the necessity of analgesic treatment was reassessed during the routine checkup by the surgeon. all the patients were included in a rehabilitation pro-gram and were discharged from the hospital between day 4 and day 7, after having proved to be able to get in and out of bed, to walk un-assisted and to climb stairs.
Data collection
the recorded preoperative parameters in-cluded preoperative pain intensity, presence of pain elsewhere as well as the preoperative intake of opioids and antidepressants drugs. a verbal Descriptor scale of 5 points (score 0 to 4) where pain was reported as absent (0), mild (1), moderate (2), severe (3) or extremely severe (4) was used to assess all the different types of pain assessed in this study.
average and maximal pain, the presence of pain at rest, pain evoked at movement and pain located at the incision site were recorded sepa-rately. Besides the use of the verbal Descrip-tor scale as aforementioned, the sF-MPQ-2 score 18 in its French version was also used to qualify pain. this included the main terms used to assess the neuropathic pain: ‘‘hot-burning pain”, ‘‘cold-freezing pain”, ‘‘pain caused by light touch”, ‘‘itching”, ‘‘tingling or ‘pins and needles,’” and ‘‘numbness”. all the aforementioned pain scores were recorded at postoperative day 1, 2, 3 during hospital stay
Figure 1.— chronogram of the recorded parameters in the study.
140 patients16 patients refused the study
124 patientsWere excluded:
Patients undergoing spinal anesthesiapatients presenting immediate complications
114 patientsDay 8=86 responses (75%)Day 30=82 responses (72%)
3 months=76 responses (67%)6 months=74 responses (65%)
1 year=68 responses (60%)
➔➔

DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa grosU
vol. 82 - no. 3 Minerva anestesiologica 277
and 66% associated with mobilization and for chronic pain of 14% at rest and 22% during mobilization.
Pain at rest peaked at day 30 while pain
distribution of the data was assessed by the Kolmogorov-smirnov test. several of the data were not normally distributed and were analyzed using Kruskal-Wallis anova on ranks with Dunn’s method for pairwise mul-tiple comparisons or Mann-Whitney test for unpaired data. comparisons of the observed proportions were performed using χ2 analysis and the Fisher exact test if appropriate. cor-relations between the presence and severity of preoperative and acute postoperative pain and the presence of subacute and even further, chronic pain, were performed. correlations be-tween the preoperative opioid intake and the severity of postoperative pain at different mo-ments of the survey as well between the pres-ence of incisional pain and neuropathic pain were also assessed. correlations were tested using spearman rank order test or Pearson’s product moment test as needed. a P-value of less than 0.05 was considered to be significant.
Results
the study was proposed to 140 consecutive patients undergoing tKa; 124 patients gave their informed written consent to participate and a total of 114 patients were finally enrolled (Figure 2). thirty-nine men and 75 women, aged 66±10 years, and with a BMi of 27±5 kg/m2 completed the study.
Mean surgery duration was 88±21 min and tourniquet time was 55±20 min. average intra-operative doses of intravenous analgesics, ket-amine and sufentanil were 25±10 mg and 14±6 µg, respectively.
response rates to the questionnaires during the follow up period are reported in Figure 2.
Pain was considered when expressed with the verbal Descriptor scale as moderate, se-vere and extremely severe. the different types of pain observed in the study, pain at rest, dur-ing movement and pain located at incision site, along with their evolution over time are pre-sented in Figure 3.
With respect to the three periods of time we previously considered, the data show an aver-age incidence for subacute pain of 54% at rest
Figure 2.—Flowchart.
Postoperative day 1: vDs, sF-MPQ-2
Postoperative day 2: vDs, sF-MPQ-2
Postoperative day 3: vDs, sF-MPQ-2
Postoperative day 8: vDs, sF-MPQ-2,analgesic consumption,
need of medical assistance, BPi
Postoperative day 30: vDs, sF-MPQ-2,analgesic consumption,
need of medical assistance, BPi
3 months after the surgery: vDs, sF-MPQ,-2, analgesic consumption,
need of medical assistance, BPi
6 months after the surgery: vDs, sF-MPQ,-2, analgesic consumption,
need of medical assistance, BPi
1 year after the surgery: vDs, sF-MPQ,-2, analgesic consumption,
need of medical assistance, BPi
➔➔
➔➔
➔➔
➔

grosU DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa
278 Minerva anestesiologica March 2016
surgery. Further, at that time, an average 11% of the patients were still taking some analge-sics: acetaminophen (17%), nsaiDs (8%) and/or opioids (8%). the impact of postopera-tive pain on the daily enjoyment of life, mood and sleep is detailed in table i. regular use of analgesics (including opioids) and seek for medical assistance is shown in table ii.
Preoperative pain intensity was corre-lated with the intensity of acute pain at day 1 (r=0.279; P=0.007) and day 8 (r=0.408; P=0.027). early postoperative pain intensity (at day 1) also correlated with pain intensity at day 8 (r=0.461; P=0.014), at day 30 and at 3 months (r=0.320; P=0.009). Pain intensity reported at day 30 was correlated with pain intensity at 3 months (r=0.397; P=0.001) and at 6 months (r=0.310; P=0.013) while pain intensity at 6 months was strongly cor-related with pain intensity reported at 1 year (r=0.456; P=0.0004). the severity of acute pain (cumulative value of maximal pain inten-sity recorded at days 1, 2 and 3) was associated
during mobilization displayed a plateau be-tween day 8 and 3 months (average incidence of 55%). the incidence of pain at incision site displayed a constant decrease from day 8, with 3% of the patients complaining at 1 year. incisional pain had neuropathic features, as defined by one or more of the 6 items of the neuropathic subscale of sF-MPQ-2, with posi-tive correlation coefficients at day 8 (R=0.437; P=0.007), day 30 (r=0.253; P=0.023) and 3 months (r=0.458; P=0.001) postoperatively. More, the presence of incisional pain was cor-related with the intensity of the pain from day 8 until 6 months. (r=0.569; P=0.001).
average and maximal pain intensity at the different time points of the follow up are shown in Figure 4a, B. Moderate to severe average pain was reported by 54% of patients the first day, 44% the second day and 27% the third day, descending to 14%, 10% and 15% at 3 months, 6 months and 1 year after the surgery respectively. Worst pain was described as mod-erate to severe by 70% of patients on the first postoperative day, 68% and 41% of patients on the second and third day, diminishing to 30%, 27% and 22% of patients at 3, 6 months and 1 year after the surgery respectively.
More than 40% of patients reported moder-ate to severe alteration of their enjoyment of life as well as their quality of sleep in the acute period after the surgery after the surgery, de-creasing to less than a half one year after the
Figure 3.—evolution of the different types of pain after tKa over the time.
a
BFigure 4.— evolution of pain intensity as reported by the pa-tients during the follow-up. a) average pain; B) worst pain.

DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa grosU
vol. 82 - no. 3 Minerva anestesiologica 279
bilization and incisional pain were recorded separately. the use of pain trajectories by contrast with pain assessment at discrete time points allows picturing how pain evolves, maybe helping caregivers to identify specific problems and to design adapted strategies. if we consider distinct time points, our results are confirmatory to those reported by the literature for acute and chronic pain after tKa. eigh-
to the presence of persisting pain at rest at 3 months (r=0.260, P=0.045) and the presence of chronic pain at rest at 6 months and 1 year post-surgery (r=0.350, P=0.009).
Preoperative knee pain was estimated as moderate by 71 patients (63%), as severe by 33 patients (28%) and only 10 patients (9%) had no preoperative pain. Preoperative opioid analgesic treatment concerned 9 patients (8%) and 36 patients (32%) reported regular intake of an antidepressant drug. Figure 5 shows the evolution or pain trajectories in patients with a regular preoperative opioid intake by com-parison with the other patients. the former patients experienced higher postoperative pain scores during the follow up period. no effect of preoperative regular antidepressant intake was found (data not shown).
Discussion
We have observed the incidence and the resolution over one year of different types of pain after tKa. Pain at rest, pain during mo-
Table I.—�Impact of postoperative pain on the enjoyment of life, mood and sleep during the first year after TKA. Data are expressed as percentages of patients’ population (%).
none a little Moderate a lot
enjoyment of life Day 8 10 35 35 20Day 30 19 48 29 43 months 24 56 19 16 months 40 46 8 612 months 53 24 20 3
Mood Day 8 72 22 6 0Day 30 54 39 3 43 months 56 35 9 06 months 57 32 8 312 months 69 17 8 6
sleep Day 8 27 27 33 13Day 30 33 33 25 93 months 50 29 17 46 months 65 21 8 612 months 61 12 12 15
Table II.—�Regular use of analgesics and seek for medical assistance during the first year after TKA. Data are ex-pressed as percentages of patients’ population (%).
analgesics use Day 8 Day 30 3 months 6 months 12 months
– Paracetamol 83 60 51 20 17 – nsaiDs 25 28 14 6 8 – opioids 47 40 28 14 8
Medical assistance For Pain 0 13 14 8 16
Figure 5.—Pain resolution according to preoperative opioid intake. P value <0.05.

grosU DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa
280 Minerva anestesiologica March 2016
although we expected that incisional pain had neuropathic features, this was true only in the acute and subacute period and not later in its evolution. neuropathic pain after tKa only concerns a small percentage of patients, 6 to 10% according to literature.21, 24, 25 the increasing use of minimal invasive techniques in TKA, reducing tissue and nervous fiber de-struction is certainly one of the reasons for the decreasing incidence of neuropathic pain after tKa,26, 27 when comparing to the higher inci-dences observed a decade ago.28 However, it is worth noting that alterations in skin sensations reported after tKa may correlate with the in-ability to kneel and thereby cause functional handicap and dissatisfaction for the patient, early in the postoperative period.29
in the current study we have outlighted the disturbances of different aspects of the patient’s quality of life over time after tKa. sleep deprivation has long-term consequences on rehabilitation and is also a predictive fac-tor of developing persistent pain after tKa.30 if it is pain and/or other factors that induce sleep deprivation, a special attention should be accorded to measures directed to amelio-rate sleep quality. according to Wylde and as a confirmation by our results, up to 40% of patients present sleep disturbances during the first three postoperative days,2 but this seems to not be associated with the pain scores or inflammatory response.17 Furthermore, our results show that sleep disturbances go way beyond the acute intra-hospital period, with almost 30% of patients reporting moderate to severe sleep problems even one year after the surgery. sleep, together with the enjoyment of life and mood, are affected at long term after tKa, as underlined by our data, contribut-ing to poor outcome and dissatisfaction of the affected patients.5, 31 Furthermore, taking in consideration that residual pain is one of the factors contributing to patient dissatisfaction 5 and that sleep deprivation affects pain percep-tion, induces generalized hyperalgesia and in-creases anxiety,32 direct measures in order to ameliorate sleep should be taken before this feedback occurs. this could also explain the results showing that the best patient-relevant
teen and 32% of patients experienced pain at rest and during mobilization respectively, dur-ing the first postoperative day, similar to the results reported in a recent prospective study (20% and 33% respectively) 20 and 20%, 5% and 3% of patients experienced pain during mobilization, pain at rest and incisional pain, respectively at one year after the surgery. this corresponds to the reported percentages in the literature that situate chronic pain after tKa between 10 and 34%.3, 9, 21 the variability in the reported incidences of chronic pain can be explained by the different definitions used to define and the different scores used to quantify chronic pain after tKa.1
subacute pain after tKa emerges in the last years as an independent entity, which deserves better acknowledgement in order to improve analgesia after patient discharge.22 54% and 66% of our patients reported pain at rest and during mobilization respectively, consequence of the return to the normal life activities, while the early rehabilitation programs have ended. andersen et al. also observed similar pain in-cidences at 30 day postsurgery, 52 and 78% respectively.22 Morze et al. were the first to examine the weekly resolution of knee pain, using the pain trajectories up to three months after the surgery. they demonstrated that the overall time taken to reduce the worst pain to half can go up to 12 weeks for 32% of pa-tients.11 the use of pain trajectories allows to picture how pain evolves, maybe helping the caregivers to identify specific problems. One strong point of our study is the record of tra-jectories for the different identified types of pain up to one year after tKa. We have no-ticed the non-linear evolution with a peak of pain at rest at 30 days and a plateau of pain at mobilization through the entire subacute period. this highlights the active role of anes-thesiologists in preventing the transition from acute to persistent postsurgical pain, not only by the means of “protective” strategies of an-esthesia but also by a better postoperative pain control, with regular follow ups and adaptation of the analgesic strategies, that could address both pharmacologic and non-pharmacologic measures.23

DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa grosU
vol. 82 - no. 3 Minerva anestesiologica 281
tive chronic opioid use exhibited higher post-operative pain scores during the entire follow up period in our study, as previously shown in another study.42 the prevalence of opioids intake (9% before tKa) remained unchanged at one year after the surgery, an observation similar to a recent european study where a slight increase in opioid consumption was seen at one year after tKa.43 the same fact has been also reported by an Us study with a higher prevalence of opioid use (24% pre-operative use, slightly reduced to 17% at one year after the surgery.42, 44 opioids might not be the best preoperative analgesic alternative and if an opioid medication is mandatory in order to control pain at some point in the evo-lution of knee arthritis, this could represent the moment when surgery should not be de-layed anymore.
one of the limitations of our study is the in-consistent rate of participation to the study, as presented in the flowchart. It is possible that the presence of pain or of a diminished quality of life affected the willingness of response of the patients. a second limitation of the study is the absence of the evaluation of quality of life preoperatively, which would have allowed assessing changes between preoperative and postoperative values at different times of the study.
Conclusions
Pain after tKa presents in different forms, each with different mechanisms and character-istics and, consequently, with different impli-cations on the functional recovery and quality of life after tKa. recording the trajectories of these different types of pain after tKa shows their non-linear evolution, highlighting the specific periods of time when a better pain control is needed.
sleep disturbances and alterations of quality of life go beyond the first postoperative days and may affect an important proportion of the patients even at one year after the surgery, with consequences on rehabilitation and persistent pain.
outcomes after tKa are seen one year after the surgery, with a continuous deterioration in the following years after.33
in the current study we observed that up to 17% of patients still took some analgesic medication one year after tKa, opioids in-cluded, similar to other studies 21 (13%). the side effects related to a chronic analgesic in-take in a fragile population,34 represents a real concern.
the severity of acute postoperative pain is a well-recognized risk factor for the develop-ment of persistent pain after surgery.35 in our patients, the cumulative value of the maximal pain intensity recorded at day 1, 2 and 3 was associated with the presence of chronic pain at 6 months and 1 year after the surgery and not the single score of pain intensity. therefore we can suppose that besides the severity of acute postoperative pain, the time spent in severe pain may constitute a risk factor to develop chronic pain after surgery.9, 36, 37
Another interesting finding is that the inten-sity of acute pain correlated with the intensity of subacute pain (at 30 days and 3 months) and then that the intensity of subacute pain (pain reported at 30 days after the surgery) was a risk factor for severe chronic pain at 3 and 6 months after the surgery. although the major risk factors for chronic post-surgical pain have been described, the complexity of chronic pain mechanisms still makes it impossible to pre-dict who will and who will not develop chronic pain after the surgery.38 Moreover, the factors involved in the transition from acute to chron-ic pain seem to differ from those involved in the maintenance of persistent pain when es-tablished.39 in this context, the subacute pain period, as the transition period from acute to chronic pain, presents a major interest, and positive correlations between subacute and chronic pain suggest that a bigger attention should be accorded to this period.
a regular preoperative opioid intake is as-sociated with decreased pain thresholds and modified endogenous pain modulation, i.e. opioid-induced hyperalgesia, a state that can contribute to postoperative pain severity and persistence.40, 41 the patients with preopera-

grosU DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa
282 Minerva anestesiologica March 2016
pain and function in determining patient satisfaction af-ter total knee replacement. Data from the national Joint registry for england and Wales. J Bone Joint surg Br 2007;89:893-900.
5. scott ceH, Howie cr, MacDonald D, Biant lc. Pre-dicting dissatisfaction following total knee replacement: a prospective study of 1217 patients. J Bone Joint surg Br 2010;92:1253-8.
6. Kurtz s, ong K, lau e, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United states from 2005 to 2030. J Bone Joint surg am 2007;89:780-5.
7. chapman cr, Donaldson gW, Davis JJ, Bradshaw DH. improving individual measurement of postoperative pain: the pain trajectory. J Pain 2011;12:257-62.
8. lavand’homme P. the progression from acute to chronic pain. curr opin anaesthesiol 2011;24:545-50.
9. Puolakka Pae, rorarius MgF, roviola M, Puolakka tJs, nordhausen K, lindgren l. Persistent pain following knee arthroplasty. eur J anaesthesiol 2010;27:455-60.
10. lavand’homme PM, grosu i, France M-n, thienpont e. Pain trajectories identify patients at risk of persistent pain after knee arthroplasty: an observational study. clin or-thop relat res 2014;472:1409-15.
11. Morze cJ, Johnson nr, Williams g, Moroney M, lam-berton t, Mcauliffe M. Knee Pain During the First three Months after Unilateral total Knee arthroplasty. J ar-throplasty 2013;28:1565-70.
12. Bellamy n, campbell J, stevens J, Pilch l, stewart c, Mahmood Z. validation study of a computerized version of the Western ontario and McMaster Universities va3.0 osteoarthritis index. J rheumatol 1997;24:2413-5.
13. Dawson J, Fitzpatrick r, Murray D, carr a. Question-naire on the perceptions of patients about total knee re-placement. J Bone Joint surg Br 1998;80:63-9.
14. srikandarajah s, gilron i. systematic review of move-ment-evoked pain versus pain at rest in postsurgical clinical trials and meta-analyses: a fundamental dis-tinction requiring standardized measurement. Pain 2011;152:1734-9.
15. Wylde v, Dieppe P, Hewlett s, learmonth iD. total knee replacement: is it really an effective procedure for all? the Knee 2007;14:417-23.
16. Kim tK, chang cB, Kang Yg, Kim sJ, seong sc. causes and predictors of patient’s dissatisfaction after uncomplicated total knee arthroplasty. J arthroplasty 2009;24:263-71.
17. Krenk l, Jennum P, Kehlet H. sleep disturbances af-ter fast-track hip and knee arthroplasty. Br J anaesth 2012;109:769-75.
18. Dworkin rH, turk Dc, revicki Da, Harding g, coyne Ks, Peirce-sandner s, et al. Development and initial validation of an expanded and revised version of the short-form Mcgill Pain Questionnaire (sF-MPQ-2). Pain 2009;144:35-42.
19. tan g, Jensen MP, thornby Ji, shanti BF. validation of the Brief Pain inventory for chronic nonmalignant pain. J Pain 2004;5:133-7.
20. liu ss, Buvanendran a, rathmell JP, sawhney M, Bae JJ, Moric M, et al. Predictors for moderate to severe acute postoperative pain after total hip and knee replacement. int orthop 2012;36:2261-7.
21. aveline c, roux al, Hetet Hl, gautier JF, vautier P, cognet F, et al. Pain and recovery after total Knee ar-throplasty: a 12-Month Follow-up after a Prospective randomized study evaluating nefopam and Ketamine for early rehabilitation. clin J Pain 2014;30:749-54.
22. andersen lØ, gaarn-larsen l, Kristensen BB, Hus-ted H, otte Ks, Kehlet H. subacute pain and function after fast-track hip and knee arthroplasty. anaesthesia 2009;64:508-13.
References
1. grosu i, lavand’homme P, thienpont e. Pain after knee arthroplasty: an unresolved issue. Knee surg sports trau-matol arthrosc 2014;22:1744-58.
2. Wylde v, rooker J, Halliday l, Blom a. acute postoper-ative pain at rest after hip and knee arthroplasty: severity, sensory qualities and impact on sleep. orthop traumatol surg res 2011;97:139-44.
3. Beswick aD, Wylde v, gooberman-Hill r, Blom a, Di-eppe P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? a systematic review of prospective studies in unselected patients. BMJ open 2012;2:e000435-5.
4. Baker Pn, van der Meulen JH, lewsey J, gregg PJ, na-tional Joint registry for england and Wales. the role of
Key messages
— Pain after tKa presents in differ-ent forms that should be taken in account separately: pain at rest, pain during mo-bilization and incisional pain. the use of pain trajectories for each of these types of pain, by contrast with pain assessment at discrete time points, allows picturing how pain evolves over time.
— Disturbances of different aspects of the patient’s quality are present up to one year after tKa. sleep deprivation has long-term consequences on rehabilitation and is also a predictive factor of developing persistent pain after tKa. sleep, together with the enjoyment of life and mood, are affected at long term after tKa, contrib-uting to poor outcome and dissatisfaction of the affected patients. Furthermore, tak-ing in consideration that residual pain is one of the factors contributing to patient dissatisfaction and that sleep depriva-tion affects pain perception, direct mea-sures in order to ameliorate sleep should be taken before this feedback occurs.
— Besides the severity of acute post-operative pain, the time spent in severe pain may constitute a risk factor to develop chronic pain after surgery. subacute peri-od, as the transition period from acute to chronic pain, presents a major interest, and positive correlations between subacute and chronic pain suggest that a bigger attention should be accorded to this period.
DYnaMic vieW oF PostoPerative Pain evolUtion aFter tKa grosU
vol. 82 - no. 3 Minerva anestesiologica 283
prospective study of patient-relevant outcomes after total knee replacement. osteoarthr cartil 2009;17:601-6.
34. steyaert a, lavand’homme P. Postoperative opioids: let us take responsibility for the possible consequences. eur J anaesthesiol 2013;30:50-2.
35. althaus a, Hinrichs-rocker a, chapman r, arránz Becker o, lefering r, simanski c, et al. Development of a risk index for the prediction of chronic post-surgical pain. eur J Pain 2012;16:901-10.
36. singh Ja, gabriel s, lewallen D. the impact of gender, age, and preoperative pain severity on pain after tKa. clin orthop relat res 2008;466:2717-23.
37. liu ss, Buvanendran a, rathmell JP, sawhney M, Bae JJ, Moric M, et al. a cross-sectional survey on Preva-lence and risk Factors for Persistent Postsurgical Pain 1 Year after total Hip and Knee replacement. reg anesth Pain Med 2012;37:415-22.
38. gilron i, Kehlet H. Prevention of chronic pain after sur-gery: new insights for future research and patient care. can J anaesth 2014;61:101-11.
39. Katz J. one man’s risk factor is another man’s outcome: difference in risk factor profiles for chronic postsurgi-cal pain maintenance vs transition. Pain 2012;153:505- 6.
40. chen l, Malarick c, seefeld l, Wang s, Houghton M, Mao J. altered quantitative sensory testing outcome in subjects with opioid therapy. Pain 2009;143:65-70.
41. Yarnitsky D. conditioned pain modulation (the diffuse noxious inhibitory control-like effect): its relevance for acute and chronic pain states. curr opin anaesthesiol 2010;23:611-5.
42. Zywiel Mg, stroh Da, lee sY, Bonutti PM, Mont Ma. chronic opioid use prior to total knee arthroplasty. J Bone Joint surg am 2011;93:1988-93.
43. Fuzier r, serres i, Bourrel r, Palmaro a, Montastruc J-l, lapeyre-Mestre M. analgesic drug consumption increases after knee arthroplasty: a pharmacoepide-miological study investigating postoperative pain. Pain 2014;155:1339-45.
44. Franklin PD, Karbassi Ja, li W, Yang W, ayers Dc. re-duction in narcotic use after primary total knee arthro-plasty and association with patient pain relief and satis-faction. J arthroplasty 2010;25(6 suppl):12-6.
23. de Kock M. expanding our horizons: transition of acute postoperative pain to persistent pain and establishment of chronic postsurgical pain services. anesthesiology 2009;111:461-3.
24. Buvanendran a, Kroin Js, valle Della cJ, Kari M, Mor-ic M, tuman KJ. Perioperative oral pregabalin reduces chronic pain after total knee arthroplasty: a prospective, randomized, controlled trial. anesthesia & analgesia 2010;110:199-207.
25. Wylde v, Hewlett s, learmonth iD, Dieppe P. Persistent pain after joint replacement: prevalence, sensory quali-ties, and postoperative determinants. Pain 2011;152:566-72.
26. thienpont e. Faster recovery after minimally invasive surgery in total knee arthroplasty. Knee surg sports trau-matol arthrosc 2013;21:2412-7.
27. Khanna a, gougoulias n, longo Ug, Maffulli n. Mini-mally invasive total knee arthroplasty: a systematic re-view. orthop clin north am 2009;40:479-89-viii.
28. Harden rn, Bruehl s, stanos s, Brander v, chung oY, saltz s, et al. Prospective examination of pain-related and psychological predictors of crPs-like phenomena following total knee arthroplasty: a preliminary study. Pain 2003;106:393-400.
29. Hassaballa M, artz n, Weale a, Porteous a. alteration in skin sensation following knee arthroplasty and its im-pact on kneeling ability: a comparison of three common surgical incisions. Knee surg sports traumatol arthrosc 2012;20:1983-7.
30. cremeans-smith JK, Millington K, sledjeski e, greene K, Delahanty Dl. sleep disruptions mediate the relation-ship between early postoperative pain and later function-ing following total knee replacement surgery. J Behav Med 2006;29:215-22.
31. larsen K, Hansen tB, søballe K, Kehlet H. Patient-re-ported outcome after fast-track knee arthroplasty. Knee surg sports traumatol arthrosc 2012;20:1128-35.
32. schuh-Hofer s, Wodarski r, Pfau DB, caspani o, Magerl W, Kennedy JD, et al. one night of total sleep depriva-tion promotes a state of generalized hyperalgesia: a sur-rogate pain model to study the relationship of insomnia and pain. Pain 2013;154:1613-21.
33. nilsdotter a-K, toksvig-larsen s, roos eM. a 5 year
Funding.—the present work has been realized with the support of a national grant from the sarB (society of anesthesiology and reanimation of Belgium).Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: 2015, July 16. - Manuscript accepted: 2015, July 14. - Manuscript revised: 2015, July 8. - Manuscript received: January 11, 2015.

284 Minerva anestesiologica March 2016
because of altered drug pharmacokinetics (PKs),3, 4 a continuous (ci) rather than inter-mittent infusion (ii) of vancomycin has been proposed to optimize drug concentrations.5, 6 although this strategy is not more effective than intermittent infusion,7 it has been associ-ated with a lower risk of acute kidney injury (aKi) and a reduction in the total duration and
vancomycin remains one of the first-choice therapeutic options for treating
severe gram-positive infections with meticil-lin-resistant Staphylococcus aureus (Mrsa), ampicillin-resistant Enterococcus faecium or pneumococcal infections due to strains resis-tant to penicillin and third and fourth-genera-tion cephalosporins.1, 2 in critically ill patients,
O R I G I N A L A R T I C L E
continuous vs. intermittent vancomycin therapy for gram-positive infections not caused by methicillin-resistant Staphylococcus Aureus
Wieslawa DUsZYnsKa 1*, Fabio s. taccone 2, Magdalena HUrKacZ 3, anna Wiela-HoJensKa 3, andrzej KÜBler 1
1Department of anesthesiology and intensive care, Wroclaw Medical University, Wroclaw, Poland; 2Department of intensive care, erasme Hospital, Université libre de Bruxelles, Bruxelles, Belgium; 3Department of clinical Pharmacology, Wroclaw Medical University, Wroclaw, Poland*corresponding author: Wieslawa Duszynska, Department of anesthesiology and intensive care, Wroclaw University Hospital, Borowska street 213, 50-556 Wroclaw, Poland. e-mail: [email protected]
anno: 2016Mese: Marchvolume: 82no: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10484-Mastitolo breve: vancoMYcin in non-Mrsa inFectionsprimo autore: DUsZYnsKapagine: 284-93citazione: Minerva anestesiol 2016;82:284-93
a B s t r a c tBacKgroUnD: the aim of this study was to evaluate the effects of vancomycin pharmacokinetics (PKs) on effective-ness and safety in the treatment of gram-positive infections due to pathogens other than methicillin-resistant Staphylo-coccus aureus (Mrsa).MetHoDs: Prospective study including septic patients received either continuous (n.=21) or intermittent (n.=21) in-fusions of vancomycin; the target drug concentration was 15-20 mg/l and target area under the curve of vancomycin concentrations over the minimum inhibitory concentration of the pathogen on day 1 (aUc24/Mic) >400. clinical and microbiological responses, the development of acute kidney injury (aKi) and therapy costs were recorded.resUlts: the median aUc24/Mic was 195(133-343) vs. 189(136-328) mg/l*h in the continuous and intermittent infusion groups. target drug concentrations were achieved in 15/21 vs. 9/21 (P=0.12) patients and aUc24/Mic>400 in only 5/21 vs. 3/21 (P=0.35) patients of continuous and intermittent groups, respectively. High clinical cure (17/21 for continuous vs. 17/21 for intermittent, P=1.00) and microbiological eradication (17/21 vs. 15/21, P=0.47) were observed in both groups and not associated with drug concentrations or with aUc24/Mic. aKi was diagnosed during therapy in 5/21 patients in the continuous group and 8/21 in the intermittent group (P=0.32). the median total therapy costs were lower in the continuous than in the intermittent group (377 [304-485] vs. 552 [371-644] €, P=0.04).conclUsions: vancomycin resulted in high clinical response during non-Mrsa gram-positive infections treatment even at drug concentrations lower than those for Mrsa. a continuous infusion of vancomycin was associated with a significant reduction in therapy costs compared to intermittent infusions.(Cite this article as: Duszynska W, taccone Fs, Hurkacz M, Wiela-Hojenska a, Kübler a. gram-positive infections not caused by methicillin-resistant staphylococcus aureus. Minerva anestesiol 2016;82:284-93)Key words: vancomycin - Methicillin-resistant staphylococcus aureus - infection - infusions, intravenous.
Minerva anestesiologica 2016 March;82(3):284-93© 2015 eDiZioni Minerva MeDicathe online version of this article is located at http://www.minervamedica.it
vancoMYcin in non-Mrsa inFections DUsZYnsKa
vol. 82 - no. 3 Minerva anestesiologica 285
as several daily vancomycin measurements, are routine practice in our icU. Patients were included in two periods: 1) from May 2012 to september 2013, patients received ii; and 2) from october 2013 to april 2014, patients received CI. Inclusion criteria were: age ≥18 years and microbiologically confirmed Gram-positive infection; only non-Mrsa infections were eventually considered for the final analy-sis. exclusion criteria were: chronic renal fail-ure requiring hemodialysis (HD), aKi already treated by renal replacement therapy (crrt), pregnancy, patients with burns or cystic fibro-sis, known intolerance to glycopeptides.
Drug regimens
vancomycin (eDicin, lek Pharmaceuti-cals, ljubliana, slovenia) was used for both ii and ci. according to recent recommenda-tions, vancomycin was empirically initiated in associated therapy with other antibiotics active against gram-negative bacterial strains when a gram-positive infection was also suspected.14 in the ci group, the initial daily dose (DD) of vancomycin was 30 mg/kg calculated using the total body weight (tBW),1 while on subse-quent days DD was adjusted according to van-comycin concentrations. the loading dose was 0.5 g according to a previous study 8 and to lo-cal practice. in the ii group, a loading dose of 25 mg/kg was given at a maximal rate of 1 g/h and followed by a maintenance DD, adjusted as shown in appendix 1.15
Drug measurement, dose adjustment and phar-macokinetic evaluation
Blood drug concentration was determined by a validated enzyme multiplied immunoassay technique (eMit), using a viva-e™ analyzer (siemens, Dublin, ireland). these measure-ments were controlled daily using internal and external control systems. the limit of quanti-fication (LOQ) was 0.8 mg/L. Blood samples were taken immediately after the administra-tion of the loading dose (cmax) and 30 minutes thereafter (cpeak). in both groups, drug concen-trations were measured 24, 48, 72 and 96 hours
costs of therapy, in particular for Mrsa infec-tions.8, 9
interestingly, only a few reports are available on the effectiveness of continuous and intermit-tent infusions for the treatment of non-Mrsa infections study population.8, 10 Moreover, while some pharmacodynamics (PD) studies have shown that a ratio of the area under the curve (aUc) of vancomycin concentrations over the minimum inhibitory concentration (Mic; i.e., aUc/Mic) greater than 400 was as-sociated with the highest probability of clinical and microbiological success in Mrsa infec-tions,11, 12 there are no data on the optimal aUc/Mic in the treatment of non-Mrsa infections.
considering that the threshold for vanco-mycin sensitivity is different among different gram-positive strains,13 but target vancomycin concentrations for severe infections are consid-ered to be between 15 and 20 mg/l regardless of the underlying pathogen,2 there is an urgent need to determine the optimal dosage and drug regimen for non-Mrsa infections and which aUc/Mic or drug concentration threshold is associated with the best clinical and microbio-logical response in this setting.
the aim of this study was, therefore, to compare the effectiveness of continuous and intermittent infusions of vancomycin and to determine the optimal aUc/Mic and vanco-mycin concentrations for the treatment of sep-tic patients with non-Mrsa gram-positive infections. We also evaluated whether there were any differences in the total costs and the occurrence of aKi between the two strategies.
Materials and methods
Study population
the study was conducted in a 20-bed in-tensive care unit (icU) in the Department of anesthesiology and intensive care, Medical University Wroclaw (Poland). the study pro-tocol was approved by the University Bioeth-ics committee and performed in accordance with the 1964 Declaration of Helsinki. Writ-ten consent was waived because both continu-ous and intermittent vancomycin infusions,

DUsZYnsKa vancoMYcin in non-Mrsa inFections
286 Minerva anestesiologica March 2016
Clinical/microbiological end-points
as duration of therapy for non-Mrsa infec-tions in our icU is for a maximum of 7 days, the evaluation of both clinical and microbiologic responses to vancomycin was performed 24 hours after completing drug administration, i.e., on day 8, by two different expert physicians (at least one microbiologist). clinical cure was de-fined as hemodynamic stabilization with resolu-tion of clinical infection signs (body temperature <37.5 °c) and laboratory (reduction of white blood cells count, crP or Pct concentrations by more than 80% compared to baseline) abnor-malities, with no further need for vancomycin. Clinical failure was defined as a persistence or progression of clinical symptoms of infec-tion, initial recovery followed by deterioration, change to broader spectrum antibiotic therapy (escalation), increased radiological infiltrates/compute tomography (ct)-scan pathology and/or worsening of laboratory data and/or need sur-gery source control or cathecholamines. Micro-biological eradication was defined as a negative culture (from the blood, intra-abdominal fluids, csF etc.) on day 8 after initiation of therapy. Microbiological failure was defined as the per-sistence colonization of the new gram-positive or the same pathogen(s) in laboratory samples. all materials for microbiological tests were sampled and diagnosed qualitatively and quan-titatively according to accepted standards of mi-crobiological diagnostics.13, 17
AKI
AKI was defined according to the Acute Kidney injury network (aKin) criteria, i.e., an increase in serum creatinine (sCr) of ≥0.3 mg/dl or 1.5 to 2 times increase from base-line on at least 2 consecutive days and/or a de-creased urine output (<0.5 ml/kg/h for more than 6 hours) during vancomycin therapy until 72 hours after drug discontinuation.20
Pharmaco-economic evaluation
the daily dose of vancomycin and its costs were compared in the ii and ci groups. a 1.0
after the start of the loading dose (ctrough in the ii and cplateau in the ci group). at each sam-pling, 4 ml of blood were collected and im-mediately processed in the the Pharmacology laboratory. only total vancomycin concen-trations were measured. target vancomycin concentrations for both cplateau and ctrough were 15-20 mg/l; drug concentrations less than 15 mg/L were defined as “insufficient” and greater than 20 mg/L as “excessive”. The decision to maintain drug levels within these ranges were based on the significant risk of AKI when the threshold of 20 mg/l was exceeded.1, 7 if drug concentrations were greater than 20 mg/l, the daily dose was reduced by 25% for ci or the next dose was delayed by 6 hours for ii. if drug concentrations were less than 15 mg/dl, an ad-ditional loading dose of 0.5 g was given in the ii and the total daily dose of vancomycin was increased by 25% in both groups. For patients not achieving adequate drug concentrations at 96 hours and still receiving vancomycin, daily drug concentrations were recorded on the sub-sequent days of therapy.
PK parameters were calculated by applying a two-compartment model using the Kinetica 5.0 Thermo Fisher Scientific Software (Poch sa, gliwice, Poland). the following kinetic parameters were measured: total volume of distribution (vd), drug half-life (t1/2), drug clearance (CL), the AUC/MIC over the first 24 hours (aUc24/Mic) and the median daily AUC/MIC over the first 96 hours of therapy (aUc96/Mic).
Infection diagnosis
infections were diagnosed based on center of Disease control and Prevention’s national Healthcare safety network (cDc/nHsn) and standard criteria, and the severity of sep-sis was assessed using current recommenda-tions.14, 16-19 the Mic was determined using the e-test method (e-test, Biomérieux, Marcy l’etoile, France), after the strain was identi-fied. Inflammatory biomarkers (body tem-perature, white blood cells count, c-reactive protein [crP] and procalcitonin [Pct] levels) were measured daily during treatment.

vancoMYcin in non-Mrsa inFections DUsZYnsKa
vol. 82 - no. 3 Minerva anestesiologica 287
in all 42 patients, vancomycin was used in combination with β-lactams (17/21 for CI and 15/21 for ii) and/or colistin (5/21 for ci and 8/21 for ii). in all isolated pathogens, vanco-mycin was considered as the first-line therapy, as de-escalation to a narrow-spectrum drug was not possible. the median duration of van-comycin therapy was 7 [(7-10)] and similar in the two groups (table ii). the mean daily dose of vancomycin as well as total drug dose and median Mic were also similar between groups (table ii).
PK analysis showed a higher vd and total drug cl in the ci compared to the ii group (table ii) the median aUc24/Mic was similar in the two groups; however, the aUc96/Mic was significantly higher in the continuous than in the intermittent infusion group. only 5/21 (24%) and 3/21 (14%) patients in the ci and ii groups had an aUc24/Mic>400 (P=0.35); simi-larly, 5/21 (24%) and 2/21 (10%) patients had an aUc96/Mic>400, respectively (P=0.21). Fig-ure 1 shows the time-course of drug concentra-tions over the first 96 hours of therapy in the two groups; ci was associated with a shorter time to achieve target concentration than ii (24 [0-48] vs. 72 [24-120] hours, P=0.02). During the study period, 15/21 (67%) and 9/21 (43%; P=0.12) pa-tients reached target concentrations at least once in the ci and ii groups, whereas 4/21 and 9/21 had drug concentrations less than 15 mg/l and 2/21 (P=0.09) and 3/21 greater than 20 mg/l (P=0.32), respectively. only 3/21 patients in ci and 5/21patients in ii had concentrations less than 10 mg/l on day 1 of therapy (P=0.69).
clinical cure (17/21 [81%] with continu-ous vs. 17/21 [81%] with intermittent infu-sion; P=1.00) and microbiological eradication (17/21 [81%] vs. 15/21 [72%]; P=0.47) were similar between groups. clinical cure and mi-crobiological eradication rates were similar in patients who reached target concentrations at least once compared to those who did not (23/29 vs. 11/13, P=0.86; 22/29 vs. 10/13, P=0.80). similar results were found in patients who reached target concentrations at least once when compared to those who did not ac-cording to the different types of drug adminis-tration (ci=14/17 vs. 3/4, P=0.73; for clinical
or 0.5 g vial of vancomycin at the time of the study cost €17 and €13, respectively. the cost of each vancomycin measurement using eMit was €10. the mean daily cost of equipment (i.e., syringes, saline solutions for drug dilu-tion and infusion kits) was €6 in the continu-ous infusion group and between €6 and €18 in the intermittent infusion group, depending on the number of doses. the costs of Mic evalua-tion were not considered as this method is rou-tinely used in the icU in our hospital.
Statistical analysis
statistical analyses were performed us-ing the sPss 18.0 for Windows nt software package (sPss inc. chicago, il, Usa 2014). Descriptive statistics were computed for all study variables. a Kolmogorov-smirnov test was used, and histograms and normal quantile plots were examined to verify the normality of distribution of continuous variables. Discrete variables are expressed as counts (percent-age); continuous variables, which were nor-mally distributed, we expressed as mean±sD while those not normally distributed as me-dian (range). the data were analyzed using the Mann-Whitney U test or Fisher’s exact test, as appropriate. the discriminative ability of aUc24/Mic or aUc96/Mic to predict eradi-cation or clinical cure was evaluated using re-ceiver operating characteristic (roc) curves with the corresponding aUc. a P<0.05 was considered as statistically significant.
Results
Forty-two septic patients (21 in the intermit-tent infusion group and 21 in the continuous infusion group) with severe non-Mrsa gram-positive infection were included in the study (9 were excluded in the first and 8 in the sec-ond period because of Mrsa infections). the most common types of infection were peritoni-tis (15/42) and cla-Bsi (8/42), with the most common pathogens being coagulase-negative Staphylococcus (n.=26) and Enterococcus faecium (n.=14). Demographics and clinical data of patients are shown in table i.

DUsZYnsKa vancoMYcin in non-Mrsa inFections
288 Minerva anestesiologica March 2016
results were also observed when patients with aUc24/Mic>400 were compared to patients with aUc24/MIC≤400 in the two groups (con-tinuous infusion=4/5 vs. 13/16, P=0.86 for clinical cure and microbiological eradication; intermittent infusion = 3/3 vs. 14/18, P=0.37 for clinical cure – 3/3 vs. 12/18, P=0.23 for mi-crobiological eradication).
the aUc24/Mic was similar in patients with clinical cure (n=34) and those with clini-cal failure (n.=8) (191 [119-366] vs. 195 [139-292] mg*h/l, P=0.66) and also in patients with microbiological eradication (n.=32) and those
cure – 13/17 vs. 4/4, P=0.29; for microbio-logical eradication; ii=9/12 vs. 8/9, P=0.88 for clinical cure – 9/12 vs. 6/9, P=0.67 for microbiological eradication). among patients who did not reach target concentration at least once, rates of clinical cure and microbiological eradication were similar between groups (3/4 vs. 8/9, P=0.91 – 4/4 vs. 6/9; P=0.18).
Patients with an aUc24/Mic> 400 had simi-lar rates of clinical cure and microbiological eradication than patients with lower aUc24/Mic values (7/8 [87%] vs. 27/34 (79%), P=0.6; – 7/8 [87%] vs. 25/34 [74%], P=0.4). similar
Table I.—�Demographic and clinical data of patients according to the method of drug administration. Data are pre-sented as counts (percentage), mean (±SD) or median (range), as appropriate.
continuous infusionn.=21
intermittent infusionn.=21 P value
Female/male, n 4/17 3/18 0.5age (years) 62±14 54±15 0.03tBW (Kg) 77±11 84±10 0.29aPacHe ii score 21±6 21±7 0.73concomitant nephrotoxic agents, n. (%)
colistin 5 (24) 8 (38) 0.25aminoglycosides - 2 (10) 0.24nsaiDs 4 (19) 5 (24) 0.5contrast media 3 (14) 2 (10) 0.43Diuretics 6 (29) 5 (24) 0.49others - -
type of infection, n. (%)Peritonitis 6 (29) 9 (42) 0.33cla-Bsi 4 (19) 4 (19) 1.0ssti 3 (14) 2 (10) 0.63cns infection 4 (19) 3 (14) 0.67HaP/vaP 3 (14) 1 (5) 0.29others 1 (5) 2 (10) 0.55
Identified microorganisms, N. (%)cn staphylococcus 14 (71) 12 (62) 0.52enterococcus faecium 5 (24) 9 (38) 0.19streptococcus pneumoniae 2 (5) -
on the day of van initiationseptic shock 9 (43) 8 (38) 0.5Mechanical ventilation, n (%) 21(100) 21(100) 1.0temperature, °c 37.9±0.9 38.1±1.5 0.95White blood cell count, 103/mm3 15.3 (11.3-17.8) 14.3 (10.8-20.3) 0.67crP, ng/ml 147 (110-242) 189 (140-242) 0.31Procalcitonin, ng/ml 0.93 (0.39-17.3) 1.34 (0.46-3.02) 0.98Hematocrit, % 28±4 29±5 0.85serum proteins, g/dl 5.0±0.9 4.9±0.8 0.88albumin, g/dl 2.0±0.5 2.0±0.4 0.87serum creatinine, mg/dl 1.0±0.6 1.1±0.7 0.45creatinine clearance, ml/min 94±47 102±66 0.97
icU stay, days 36 [15-65] 38 (17-63) 0.57TBW: total body weight; APACHE: Acute Physiology and Chronic Health Evaluation; NSAIDs: non-steroidal anti-inflammatory drugs; VAN: vancomycin; icU: intensive care unit; crP: c-reactive protein; HaP: hospital-acquired pneumonia; vaP: ventilator-associated pneumonia; cns: central nervous system; ssti: skin and soft tissue infection; cla-Bsi: central line-associated bloodstream infection; cn: coagulase-negative.
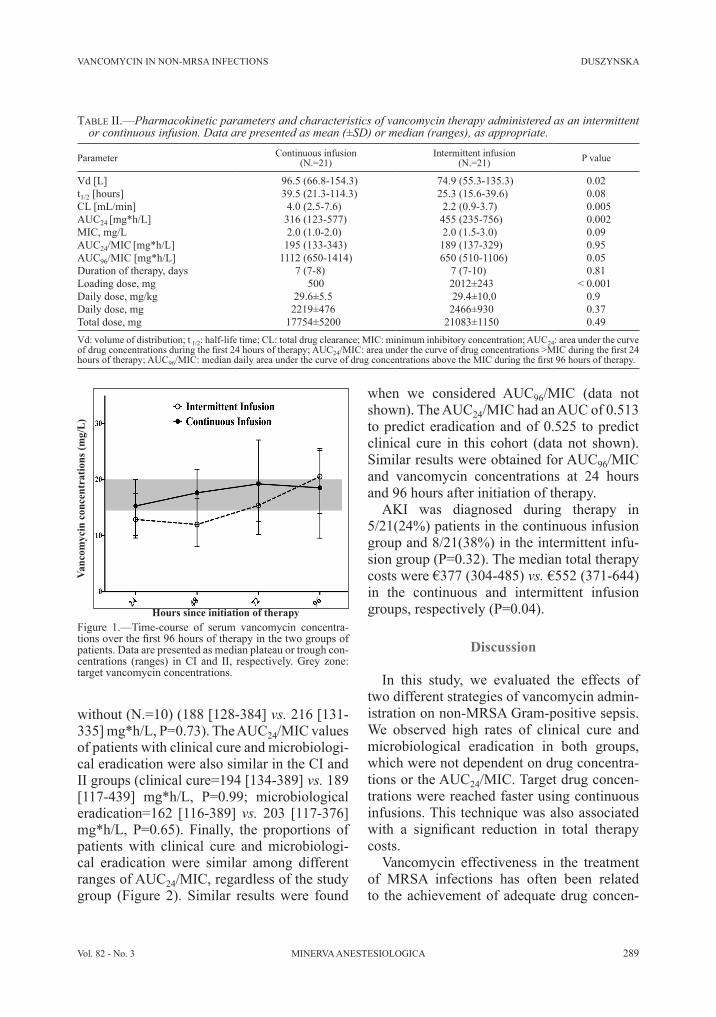
vancoMYcin in non-Mrsa inFections DUsZYnsKa
vol. 82 - no. 3 Minerva anestesiologica 289
without (n.=10) (188 [128-384] vs. 216 [131-335] mg*h/l, P=0.73). the aUc24/Mic values of patients with clinical cure and microbiologi-cal eradication were also similar in the ci and ii groups (clinical cure=194 [134-389] vs. 189 [117-439] mg*h/l, P=0.99; microbiological eradication=162 [116-389] vs. 203 [117-376] mg*h/l, P=0.65). Finally, the proportions of patients with clinical cure and microbiologi-cal eradication were similar among different ranges of aUc24/Mic, regardless of the study group (Figure 2). similar results were found
Table II.—�Pharmacokinetic parameters and characteristics of vancomycin therapy administered as an intermittent or continuous infusion. Data are presented as mean (±SD) or median (ranges), as appropriate.
Parameter continuous infusion(n.=21)
intermittent infusion(n.=21) P value
vd [l] 96.5 (66.8-154.3) 74.9 (55.3-135.3) 0.02t1/2 [hours] 39.5 (21.3-114.3) 25.3 (15.6-39.6) 0.08cl [ml/min] 4.0 (2.5-7.6) 2.2 (0.9-3.7) 0.005aUc24 [mg*h/l] 316 (123-577) 455 (235-756) 0.002Mic, mg/l 2.0 (1.0-2.0) 2.0 (1.5-3.0) 0.09aUc24/Mic [mg*h/l] 195 (133-343) 189 (137-329) 0.95aUc96/Mic [mg*h/l] 1112 (650-1414) 650 (510-1106) 0.05Duration of therapy, days 7 (7-8) 7 (7-10) 0.81loading dose, mg 500 2012±2434 < 0.001Daily dose, mg/kg 29.6±5.54 29.4±10.0 0.9Daily dose, mg 2219±4764 2466±9304 0.37total dose, mg 17754±52004 21083±11504 0.49vd: volume of distribution; t 1/2: half-life time; cl: total drug clearance; Mic: minimum inhibitory concentration; aUc24: area under the curve of drug concentrations during the first 24 hours of therapy; AUC24/MIC: area under the curve of drug concentrations >MIC during the first 24 hours of therapy; aUc96/MIC: median daily area under the curve of drug concentrations above the MIC during the first 96 hours of therapy.
Figure 1.—time-course of serum vancomycin concentra-tions over the first 96 hours of therapy in the two groups of patients. Data are presented as median plateau or trough con-centrations (ranges) in ci and ii, respectively. grey zone: target vancomycin concentrations.
when we considered aUc96/Mic (data not shown). the aUc24/Mic had an aUc of 0.513 to predict eradication and of 0.525 to predict clinical cure in this cohort (data not shown). similar results were obtained for aUc96/Mic and vancomycin concentrations at 24 hours and 96 hours after initiation of therapy.
aKi was diagnosed during therapy in 5/21(24%) patients in the continuous infusion group and 8/21(38%) in the intermittent infu-sion group (P=0.32). the median total therapy costs were €377 (304-485) vs. €552 (371-644) in the continuous and intermittent infusion groups, respectively (P=0.04).
Discussion
in this study, we evaluated the effects of two different strategies of vancomycin admin-istration on non-Mrsa gram-positive sepsis. We observed high rates of clinical cure and microbiological eradication in both groups, which were not dependent on drug concentra-tions or the aUc24/Mic. target drug concen-trations were reached faster using continuous infusions. this technique was also associated with a significant reduction in total therapy costs.
vancomycin effectiveness in the treatment of Mrsa infections has often been related to the achievement of adequate drug concen-
Vanc
omyc
in c
once
ntra
tions
(mg/
L)
Hours since initiation of therapy

DUsZYnsKa vancoMYcin in non-Mrsa inFections
290 Minerva anestesiologica March 2016
to ii, although this parameter was not predic-tive of clinical and microbiological outcomes. These findings may have been related to dif-ferences in cardiac output, fluid administration and renal or non-renal elimination, which we did not specifically assess in both groups. Sec-ond, we used a lower than recommended load-ing doses in our study 1, 6 and, as we showed that therapeutic efficacy could be obtained with lower concentrations than for Mrsa in-fections, this strategy could potentially be used in this setting. of course, this should be tested in future studies and, as we did not consider patients on rrt, even different drug regimens may be considered in this patient population.
aKi may develop in as many as 47% of pa-tients with septic shock and in 19% of these patients it may be caused or enhanced by the concomitant administration of nephrotoxic agents.32 in two retrospective studies, ci of vancomycin was associated with an incidence of aKi ranging from 24 to 30%, especially when drug concentrations exceeded an aUc24/Mic>400 or 30 mg/l.33-35 in two meta-anal-yses, the use of vancomycin monitoring sig-nificantly decreased the development of AKI (or=0.25; P<0.0001);7, 36 also, ci was asso-ciated with a significantly lower risk of AKI when compared to ii (rr 0.6; P=0.02).7 When considering drug concentrations, a higher risk of aKi was found with ctrough greater than15 mg/l during ii or greater than 28 mg/l during
trations, which have been identified as being between 20 and 30 mg/l at steady-state for a ci 6, 21 and a trough concentration of 15-20 mg/l for ii 15, 22-24 or an aUc24/Mic greater than 400 mg*h/l.11 However, several studies have questioned the need to reach such high drug levels in the treatment of Mrsa infec-tions.25, 26 in our study, we found no associa-tion between drug concentrations and clinical or microbiological responses. Moreover, drug concentrations and aUc/Mic had a very poor predictive value for these two outcomes. We, therefore, showed that, in non-Mrsa infec-tions, a high rate of therapeutic success was obtained for vancomycin levels less than those recommended to treat Mrsa infections. as such, further research is needed to evaluate whether also lower dose regimens could be used to treat non-Mrsa infections.27, 28
It is difficult to provide recommendations from our data on the optimal vancomycin regi-men to use in this setting. First, a large vari-ability in drug PKs has been observed in criti-cally ill patients.29 increased vd and renal drug CL can significantly contribute to lower than expected drug concentrations when recom-mended regimens are used.30 By contrast, he-modynamic instability and organ dysfunction would result in drug accumulation.31 in our study, the presence of larger vd and higher cl in the ci group may have resulted in a further reduction of initial aUc/Mic when compared
Figure 2.—the proportion of patients with clinical cure (a) and microbiological eradication (B) in the two groups of patients.ii: intermittent infusion; ci: continuous infusion.
a B

vancoMYcin in non-Mrsa inFections DUsZYnsKa
vol. 82 - no. 3 Minerva anestesiologica 291
the findings related to the differences between continuous and intermittent infusion. Fifth, we studied heterogeneous infections, including peritonitis or central nervous system (cns) infections, in which drug penetration may be limited. optimal vancomycin concentrations in non-Mrsa infections should be evaluated in bacteremia due to these pathogens, as this would limit most of the differences related to the source of infection. sixth, we did not con-duct post-hoc analyses to identify any potential difference between different pathogens (i.e. coagulase-negative Staphylococci vs. Entero-coccus faecium) because of the limited number of isolates. Finally, we used a nomogram for vancomycin adaption during ii, which has not been specifically validated for use in critically ill patients.
Key messages
— vancomycin therapy resulted in high clinical and microbiological responses dur-ing non-Mrsa gram-positive infections.
— Both continuous and intermittent infusion were effective, although continu-ous administration was associated with a significant reduction in therapy costs when compared to intermittent infusion.
— clinical response was achieved at drug concentrations lower than those for MRSA infections, although an “optimal” drug level could not be identified.
References
1. rybak MJ, lomaestro BM, rotscahfer Jc, Moellering r, craig r, Billeter M, et al. vancomycin therapeutic guide-lines: a summary of consensus recommendations from the infectious Diseases society of america, the american society of Health-system Pharmacists, and the society of infectious Diseases Pharmacists. am J Health syst Pharm 2009;49:325-7.
2. liu c, Bayer a, cosgrove sl, Daum rs, Fridkin sK, gorwitz rJ, et al. clinical Practice guidelines by the in-fectious Diseases society of america for the treatment of methicillin-resistant staphylococcus aureus infections in adults and children: executive summary. clin infect Dis 2011;52:285-92.
3. llopis-salvia P, Jimenes-torres nv. Population pharma-cokinetic parameters of vancomycin in critically ill pa-tients. J clin Pharm ther 2006;31:447-54.
ci.34, 35, 37 the occurrence of aKi in our study was similar to that reported in previous studies conducted in septic patients treated with van-comycin.
in this study, continuous infusion with a tDM strategy enabled savings of more than €100 per patient. similar results were reported in an earlier study in which the 10-day treat-ment-cost per patient was reduced by 23% when compared to intermittent infusions.8 in a national survey, continuous infusion of an-tibiotics, including vancomycin, was com-monly adopted because it was considered as less toxic and associated with cost-savings.38 Moreover, the economic advantages suggested in the present study do not include possible savings in nursing time spent on preparation and administration of a single infusion (instead of two to three doses), and reduced costs of monitoring related to the overall better stabil-ity of serum drug concentrations when using continuous infusions.
this study has several limitations. First, it was a single-center study, which could limit the applicability of the results to other icUs. also, the different temporal frames of patients’ enrollment may have been resulted in different management of such patients and potentially influenced the clinical and microbiological re-sponses. second, the sample size was limited and patients were not randomized; a sample-size estimation was not performed because of the lack of data on vancomycin therapy for non-Mrsa infections. Moreover, the differ-ences in PK parameters between groups may have accounted for some of the changes in drug concentrations rather than the mode of administration per se. third, only total antibi-otic concentrations were measured, while free vancomycin concentrations may significantly vary because of unpredicatable protein bind-ing.39 Fourth, we observed a very high rate of clinical cure when compared to results of study describing the response to vancomycin for Mrsa pneumonia.40 Moreover, as 20% of patients had cla-Bsi, removal of the culprit line could be sometimes sufficient to treat the infection. also, the non-blinded study assess-ment of clinical outcomes may have biased

DUsZYnsKa vancoMYcin in non-Mrsa inFections
292 Minerva anestesiologica March 2016
continuous infusion: pharmacokinetic, pharmacody-namic and toxicological aspects. int J antimicrob agents 2013;41:439-46.
22. Kullar r, Davis sl, taylor tn, Kaye Ks, rybak MJ. ef-fects of targeting higher vancomycin through levels on clinical outcomes and costs in matched patients cohort. Pharmacotherapy 2012;32:195-201.
23. akers Ks, cota JM, chung KK, renz eM, Mende K, Murray cK. serum vancomycin levels resulting from continuous or intermittent infusion in critically ill burn patients with or without continuous renal replacement therapy. J Burn care resp 2012;33:e254-262.
24. Jeffres Mn, isakow W, Doherty Ja, McKinnon Ps, ritchie DJ, Micek st, et al. Predictors of mortality for methicillin-resistant Staphylococcus aureus health-care-associated pneumonia: specific evaluation of vancomycin pharmacokinetic indices. chest 2006;130:947-55.
25. lodise tP, lomaestro BM, graves J, Drusano gl. larg-larg-er vancomycin doses (at least four grams per day) are associated with increased incidence of nephrotoxicity. antimicrob agents chemother 2008;52:1330-6.
26. chung J. oh JM, cho eM, Jang HJ, Hong sB, lim cM, et al. optimal dose of vancomycin for treating methicilin-resistant staphylococcus aureus pneumo-nia in critically ill patients. anaesth intensive care 2011;39:1030-7.
27. Baptista JP, sousa e, Martins PJ, Pimentel JM. aug-mented renal clearance in septic patients and implica-tions for vancomycin. int J antimicrob agents 2012; 39:420-3.
28. Hidayat LK, Hsu DI, Quist R, Shriner KA, Wong-Ber-inger a. High-dose vancomycin therapy for methicilin resistant Staphylococcus aureus infections: efficacy and toxicity arch intern Med 2006;166:2138-44.
29. Blot s, Koulenti D, akova M, Basetti M, De Waele JJ, Dimopoulos g, et al. Does contemporary vancomycin dosing achieve therapeutic targets in a heterogenius clini-cal cohort of critically ill patients? Data from the multi-national Dali study. crit care 2014;18:r99.
30. Del Dot Me, lipman J, tett se. vancomycin pharma-vancomycin pharma-cokinetics in critically ill patients receiving continuous venovenous hemodiafiltration. Br J Clin Pharmacol 2004;58:259-68.
31. Pea F, Porecca l, Baraldo M, Furlanut M. High van-comycin dose regimens required by intensive care unit patients cotreated with drugs to improve haemodynam-ics following cardiac surgical procedures. J antimicrob chemother 2000;45:329-35.
32. Uchino s, Kellum Ja, Bellomo r, Doig gs, Morimatsu H, Morgera s, et al. Beginning and ending supportive therapy for the Kidney (Best Kidney) investigators. acute renal failure in critically ill patients: a multina-tional multicenter study. JaMa 2005;294:813-8.
33. spapen HD, van Doorn JK, Diltoer M, verbrugge W, Jacobs r, Dobbeleir n, et al. retrospective evaluation of possible renal toxicity associated with continuous infu-sion of vancomycin in critically ill patients. ann inten-sive care 2011;1:26.
34. cianferoni s, Devigili a, ocampos-Martinez e, Penac-cini l, scolletta s, abdelhadii a, et al. Development of acute kidney injury during continuous infusion of vanco-mycin in septic patients. infection 2013;41:811-20.
35. Patel n, Pai MP, rodvold Ka, lomaestro B, Drusano gl, lodise tP. vancomycin: We can’t get there from here. clin infect Dis 2011;52:969-74.
36. Ye ZK, Tang HL, Zhai SD. Benefits of therapeutic drug monitoring of vancomycin: a systematic review and me-ta-analysis. Plos one 2013;8:e77169.
37. Bosso Ja, nappi J, rudisill c, Wellein M, Bookstaver PB, swindler J. relationship between vancomycin trough concentrations and nephrotoxicity: a prospec-
4. Del Mar Fernadez de gatta garcia M, revilla n, calvo Mv, Dominguez- gil a, sanchez navarro a. Pharma-cokinetic /pharmacodynamic analysis of vancomycin in icU patients. intensive care Med 2007;33:279-85.
5. Jeurissen a, sluyts i, rutsaert r. a higher dose of van-comycin in continuous infusion is needed in critically ill patients. int J antimicrob agents 2011;37:75-7.
6. roberts Ja, taccone Fs, Udy aa, vincent Jl, Jacobs F, lipman J. vancomycin dosing in critically ill patients: robust methods for improved continuous –infusion regi-ments. antimicrob agents chemother 2011;55:2704-9.
7. cataldo Ma, tacconelli e, grilli e, Pea F, Petrosillo n. continuous versus intermittent infusion of vancomycin for the treatment of gram-positive infections: system-atic review and meta-analysis. J antimicrob chemother 2012;67:17-24.
8. Wysocki M, Delatour F, Faurisson F, rauss a, Pean Y. Misset B, et al. continuous versus intermittent infu-continuous versus intermittent infu-sion of vancomycin in severe staphylococcal infections: prospective multicenter randomized study. antimicrob agents chemother 2001;45:2460-7.
9. vuagnat a, stern r, lotthe a, schuhmacher H, Duong M, Hoffmeyer P, et al. High dose vancomycin for os-teomyelitis: continuous vs. intermittent infusion. J clin Pharm ther 2004;29:351-7.
10. James JK, Palmer sM, levine DP, rybak MJ. compari-son of conventional dosing versus continuous-infusion vancomycin therapy for patients with suspected or doc-umented gram-positive infections. antinicrob agents chemother 1996;40:696-700.
11. Moise-Broder Pa, Forrest a, Birmingham Mc, schen-tag JJ. Pharmacodynamics of vancomycin and other antimicrobials in patients with staphylococcus aureus lower respiratory tract infections. clin Pharmacokinet 2004;43:925-42.
12. Holmes ne, turnidge JD, Muckhof WJ, robinson Jo, Korman tM, o’sullivan Mv, et al. vancomycin aUc/Mic ratio and 30 day mortality in patients with staphy-lococcus aureus bacteriemia. antimicrob agents chem-other 2013;57:1654-63.
13. european committee on antimicrobial susceptibility testing (eUcast 2013). clinical breakpoints [internet]. available from: http://www.eucast.org/clinical break-points/ [cited 2016, Feb 18].
14. Dellinger rP, levy MM, rhodes a, annane D, gerlach H, opal sM, et al. surviving sepsis campaign: interna-tional guidelines for management of severe sepsis and septic shock. crit care Med 2012;41:580-6.
15. Michalets el, Pounders cl, Hollis sJ, sutherland s. outcomes associated with aUc/Mic nomogram dosing of vancomycin. annals Pharmacother 2011;45:687-9.
16. Horan tc, andrus M, Dudeck Ma. cDc/nHsn surveil-cDc/nHsn surveil-lance definition of health care –associated infection and criteria for specific types of infections in the acute care setting. am J infect control 2008;36:309-32.
17. CDC/NHSN Surveillance definition for specific types of infections January 2014 [internet]. available from www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf [cited 2016, Feb 18].
18. lopez n, Kobayashi l, coimbra r. a comprehensive review of abdominal infections. World J emerg surg 2011;6:7.
19. White B, seaton ra. complicated skin and soft tissue infections: literature review of evidence for and experi-ence with daptomycin. infect Drug resist 2011;4:115-7.
20. Mehta rl, Kellum Ja, shah sv, Molitoris Ba, ronco c, Warnock Dg, et al. acute Kidney injury network: report of an initiative to improve outcomes in acute kidney in-jury. crit care 2007;11:r31.
21. ampe e, Delaere B, Hecq JD, tulkens PM. implemen-tation of protocol for administration of vancomycin by

vancoMYcin in non-Mrsa inFections DUsZYnsKa
vol. 82 - no. 3 Minerva anestesiologica 293
tients treated for gram-positive infections. int J antimi-crob agents 2009;34:555-60.
40. Wunderink rg, niederman Ms, Kollef MH, shorr aF, Kunkel MJ, Baruch a, et al. linezolid in methicillin-resistant staphylococcus aureus nosocomial pneumo-nia: a randomized, controlled study. clin infect Dis 2012;54:621-9.
tive multicenter trial. antimicrob agents chemother 2011;55:5475-9.
38. george JM, colton BJ, rodvold Ka. national survey on continuous and extended infusions of antibiotics. am J Health syst Pharm 2012;69:1895-904.
39. Berthoin K, ampe e, tulkens PM. correlation between free and total vancomycin serum concentrations in pa-
Appendix 1
Nomogram dosing of vancomycin in intermittent infusion group [15].crcl, (ml/min) >10-30 >30-50 >50-70 >70-90 >90-100 >100
tBW, kgs50 1.0 g q 48 0.75 g q 24 0.5 g.bid 1.0 g bid 0.75 g tid 0.75 g tid55 1.0 g q 48 0.75 g q 24 0.5 g bid 1.0 g bid 0.75 g tid 0.75 g tid60 1.25 g q 48 0.5 g bid 0.75 g bid 1.0 g bid 0.75 g tid 0.75 g tid65 1.25 g q 48 0.5 g bid 0.75 g bid 1.0 g bid 0.75 g tid 1.0 g tid70 1.25 g q 48 0.5 g bid 0.75 g bid 1.0 g bid 0.75 g tid 1.0 g tid75 1.25 g q 48 0.5 g bid 0.75 g bid 0.75 g tid 1.0 g tid 1.0 g tid80 1.5 g q 48 0.5 g bid 1.0 g bid 0.75 g tid 1.0 g tid 1.0 g tid85 1.5 g q 48 0.5 g bid 1.0 g bid 0.75 g tid 1.0 g tid 1.25 g tid90 1.75 g q 48 0.75 g bid 1.0 g bid 0.75 g tid 1.0 g tid 1.25 g tid95 1.75 g q 48 0.75 g bid 1.0 g bid 0.75 g tid 1.0 g tid 1.25 g tid100 2.0 g q 48 0.75 g bid 1.25 g bid 1.0 g tid 1.25 g tid 1.25 g tid
crcl: creatinine clearance; tBW: total body weight; q 24/48 – every 24 or 48 hr; bid: twice daily; tid: three times per day.
Authors’ contribution.—WD conceived the study protocol; WD participated in the design and coordination of the study; WD and MH supervised data collection; WD, Fst participated in data interpretation; WD and MH were responsible for drug dosing and adjust-ment; WD carried out the literature search; WD and Fst drafted the present manuscript; aK and aW-H revised the manuscript. all authors read and approved the final version of the manuscript.Acknowledgments.—We thank all the nurses and doctors and the staff from the Microbiology laboratory and Monika Wieczorek for helping with this study, Dr. Krystyna glowacka from the Department of clinical Pharmacology Wroclaw Medical University for assaying plasma samples by eMit.Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: July 16, 2015. - Manuscript accepted: July 14, 2015. - Manuscript revised: July 8, 2015. - Manuscript received: February 8, 2015.

294 Minerva anestesiologica March 2016
Human database studies on the impact of sin-gle- or multiple exposures to general anesthe-sia at a young age, using various non-validated surrogate parameters for neurodevelopment, present conflicting results.6 in the meantime several national and international (pediat-ric) anesthesia societies as well as the United states Food and Drug administration 1 have designated this topic as a high priority.
the possibility of neurotoxicity of anesthet-ic drugs in young children is currently one
of the most widely debated issues in pediatric anesthesia.1-4 the number of animal studies published is extensive, with the vast majority of the papers reporting on neurotoxic effects of virtually all currently used anesthetic drugs.5
O R I G I N A L A R T I C L E
Potential neurotoxicity of anesthetic drugs in young children: who cares?
a survey among european anesthetistsFrank WeBer*, stefan van BeeK, gail scoones
Department of anesthesia, erasmus University Medical center - sophia children’s Hospital, rotterdam, the netherlands*corresponding author: Frank Weber, Department of anesthesia, erasmus University Medical center - sophia children’s Hospital, Wytemaweg 80, 3015CN Rotterdam, The Netherlands. E-mail: [email protected]
anno: 2016Mese: Marchvolume: 82no: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10739-Mastitolo breve: Potential neUrotoXicitY oF anestHetic DrUgs in cHilDrenprimo autore: WeBerpagine: 294-300citazione: Minerva anestesiol 2016;82:294-300
a B s t r a c tBacKgroUnD: Potential neurotoxicity of anesthetic drugs is currently one of the most intensely discussed issues in pediatric anesthesia. Prospective human data are sorely lacking and there is an on-going debate among experts in the field whether one should (or can) extrapolate animal data to humans. Data regarding the thoughts of practicing anesthetists regarding this topic have not been published.MetHoDs: a web-based survey to assess the thoughts of practicing (european) anesthetists regarding neurotoxicity and how it may have influenced their daily practice of pediatric anesthesia.RESULTS: The majority (68.7%) of respondents regard neurotoxicity as an important topic, which they need to further explore. Two thirds have already changed their clinical practice and 44.3% were concerned about potential neurotoxic-ity. Anesthetists from children’s hospitals were less likely to routinely inform parents about neurotoxicity (P=0.005) and more often applied an opioid-only anesthesia technique in selected premature neonates than general hospital based anesthetists (P<0.0001). Prospective human longitudinal studies focusing on neurodevelopment were given the highest priority for future research, whereas animal studies scored lowest.CONCLUSIONS: Practicing anesthetists care about potential neurotoxicity of anesthetic drugs in young children. Col-leagues working in children’s hospital have slightly different attitudes to deal with the topic, compared to those working in general hospitals. The vast majority of our colleagues are waiting for prospective human research data that may help to unravel the current controversy surrounding potential anesthetic drug neurotoxicity and help to improve the safety of pediatric anesthesia.(Cite this article as: Weber F, van Beek S, Scoones G. Potential neurotoxicity of anesthetic drugs in young children: who cares? A survey among European anesthetists. Minerva Anestesiol 2016;82:294-300)Key words: Anesthesia - Toxicity - Infant, newborn - Infant - Child.
Comment in p. 259
Minerva anestesiologica 2016 March;82(3):294-300© 2015 eDiZioni Minerva MeDicaThe online version of this article is located at http://www.minervamedica.it

Potential neUrotoXicitY oF anestHetic DrUgs in cHilDren WeBer
Vol. 82 - No. 3 Minerva anestesiologica 295
Statistical analysis
Pearson’s χ2 test was applied to relate the answers to the questions concerning neurotox-icity to the personal data, which were acquired in part one of the survey. Analyses were per-formed stratified for working experience in an-esthesia, not necessarily in pediatric anesthesia, (<10 years vs. ≥10 years) and workplace (chil-dren’s hospital vs. general hospital). In order to be able to perform valid analyses some ques-tions regarding neurotoxicity had to be either condensed (i.e. from 10 items to 3) or even di-chotomized. The questions regarding the coun-tries where respondents were currently work-ing, could not be condensed or dichotomized and were therefore excluded from any further analyses other than descriptive statistics.
Results
We received a total of 377 responses, of which a single response had to be excluded from analysis due to significant incongruity of the answers given to the questions concerning personal data and workplace, resulting in a to-tal of 376 valid responses. Not all respondents answered all questions of the questionnaire.
respondents came form 32 european coun-tries (N.=373) and 3 non-European countries (N.=3). 306 of the respondents were special-ist anesthetists, 37 were anesthesia residents, 1 was a nurse anesthetist, 1 was a physician assistant and 31 did not provide information regarding their professional title. Due to the composition of the respondents we decided to regard this research as a survey among euro-pean anesthetists. A number of 242 (64%) of the respondents worked in general hospitals, the remaining 134 (36%) in children’s hospi-tals. Anesthetists working in children’s hos-pitals were significantly older (P<0.001) and had significantly more working experience in anesthesia (P<0.003), not specifically address-ing experience in pediatric anesthesia, than those working in general hospitals. A hundred and sixty-six (50.8%) out of 327 respondents considered themselves as being well informed about the possibility of anesthetic drug induced
What we have been missing until now is a picture of what practicing anesthetists think about this topic.
We therefore conducted a survey among (european) anesthetists to assess their personal opinion with regard to possible neurotoxicity and how it affects their current practice of pe-diatric anesthesia.
Materials and methods
the Pediatric anesthesia research group at erasmus Mc - sophia children’s Hospital designed a web-based 7 survey to investigate the thoughts of practicing anesthetists regard-ing potential neurotoxicity of anesthetic drugs in young children.
The survey consisted of two major parts. The first part starts with questions concern-ing demographics, workplace and annual per-sonal case-loads relating to patient age groups and surgical specialties. The second part of the survey was related to the thoughts of the re-spondents regarding potential neurotoxicity of anesthetic drugs in young children. In order to minimize the risk of bias the answer choices to any of our multiple choice questions were ran-domized for each respondent. The entire survey is accessible as supplementary digital content.
The survey was approved by the scientific committee of the european society of anes-thesiology (esa) and any informed consent from human subjects was obtained as required. In the first instance an invitation to participate in the survey was submitted to all members of the esa by the monthly esa enewsletter on April 30, 2014. Due to a very low initial response rate (N.=32), on June 11 2014 the scientific committee of the ESA, together with the principle investigator of an international prospective complication registration trial (aPricot - anesthesia Practice in children observational trial,8 endorsed by the esa clinical trial network, decided to invite the lo-cal coordinators of all 323 aPricot centers by e-mail to participate in the survey. The local coordinators were asked to spread the survey within their departments. The survey was ac-cessible online until August 31 2014.

WeBer Potential neUrotoXicitY oF anestHetic DrUgs in cHilDren
296 Minerva anestesiologica March 2016
experience compared to those with <10 years of working experience (P=0.001).
Ninety-three (28.4%) out of 327 respondents regarded the possibility of anesthetic drug in-duced neurotoxicity in young children as one of the most important topics in their professional field, 224 (68.5%) were interested but felt a need to further explore the topic and 10 (3.1%) found the topic as being completely irrelevant. Anes-thetists with ≥10 years of working experience assigned a higher importance to topic than those with <10 years of working experience (P=0.001).
With respect to the degree of concern about neurotoxicity the 10 point Likert-scale (0= not at all, to 10= very much) was condensed to three items (not concerned - neutral - con-cerned). Sixty (18.3%) of 327 respondents were not concerned, 122 (37.3%) held a neu-tral position, and 145 (44.3%) were concerned.
Two thirds (N.= 251) of the respondents re-ported that the possibility of neurotoxicity af-fected their daily practice in children younger than 3 years of age. A number of 158 (42%) dis-cusses (age related) indications for surgery with the surgeons, and 107 (28.5%) address this issue with the parents during the pre-anesthetic con-sultation. Sixty six respondents (17.5%) reported individual practice changes – these included ef-forts to minimize exposure times to anesthesia, the avoidance of specific anesthetic drugs, a more liberal use of opioids and/or regional an-esthesia, focus on blood-pressure- and end-tidal co2-control, eeg-monitoring and efforts to cluster surgical procedures in individual patients.
Working experience significantly influenced the position held with respect to the questions on how much anesthetists were convinced that both the animal studies and the retrospective pe-diatric cohort studies published so far provide sufficient evidence to change current pediatric anesthetic practice (see Figure 1). Anesthetists with working experience ≥10 years were more likely to disagree on this question than those who had <10 years working experience (respec-tively 40% vs. 33%, P<0.0001 for animal stud-ies and 26% vs.20%, P<0.0001 for human stud-ies). Two-hundred and five (65.1%) out of 315 respondents found it unethical to anesthetize un-stable, ventilated premature neonates scheduled
neurotoxicity in young children. A hundred and fifty-three (46.8%) were aware of the topic but did not consider themselves sufficiently in-formed and 9 (2.6%) respondents have never heard about anesthetic drug neurotoxicity be-fore. Anesthetists working at children’s hos-pitals felt better informed than those working in general hospitals (P<0.0001). The same ap-plied to colleagues with ≥10 years of working
Figure 1.—Enough evidence to change clinical practice? level of agreement (agree - neutral - disagree) to change current practice of pediatric anesthesia based on the evi-dence of animal data (left) and retrospective human database studies (right); influence of working experience.
a
B
Working experience (years)

Potential neUrotoXicitY oF anestHetic DrUgs in cHilDren WeBer
Vol. 82 - No. 3 Minerva anestesiologica 297
ects, prospective longitudinal human studies on anesthetic drug neurotoxicity with a focus on neurodevelopment were given the highest priority for future research projects, whereas animal trials scored lowest (see Figure 4).
Because of the number of respondents (N.=376) and the complex structure of the questions concerning personal annual case-loads it was not possible to perform any valid and meaningful analyses of these items.
Discussion
this survey among european anesthetists is, to our best knowledge, the first to assess the thoughts of practicing anesthetists concerning the potential threat of anesthetic drug induced neurotoxicity in young children.
The majority (68.7%) of surveyed European anesthetists regarded anesthetic drug induced neurotoxicity as an interesting topic, which they should further investigate, 28.4% found it one of the most important topics in anesthesia today, and 2.9% found the whole discussion completely irrelevant. This reflects accurately the authors’ personal experience gathered from informal inter-collegial conversation at both general- and pediatric anesthesia meetings.
for patent ductus ligation or laparotomy, with only high-dose opioids and a muscle relaxant, whereas 110 (34.9%) found this approach ethi-cal. The working place was the only dependent factor whether or not to judge this approach as being ethical (P=0.001). This anesthesia tech-nique is more frequently used in children’s hos-pitals (P<0.0001); for details see Figure 2.
anesthetists working in children’s hospi-tals were less likely to routinely inform par-ents about potential neurotoxicity, compared to colleagues working in general hospitals (P=0.0005, see Figure 3).
one-hundred and two respondents recom-mended more animal studies, 282 recommen-dations for further pediatric studies were given and 8 respondents found it needless to conduct any further studies.
When asked to prioritize future research proj-
Figure 3.—Do you routinely inform parents?Percentage of respondents who recommend to routinely in-form either all parents, parents of infants <1 year or no par-ents about the possibility of anesthetic drug neurotoxicity; influence of working place.
Figure 2.—High-dose opioids and no hypnotics in prema-ture neonates.attitude towards anesthetising selected premature neonates using a high-dose opioid technique without hypnotic drugs; influence of working place. A) Percentage of respondents regarding the technique either ethical or unethical; B) per-centage of respondents who either apply the technique or not
a
B

WeBer Potential neUrotoXicitY oF anestHetic DrUgs in cHilDren
298 Minerva anestesiologica March 2016
be regarded as a scientific flaw, but in our par-ticular field of interest this appears to be the best we can do and the papers are being pub-lished in the top journals of our specialty.
We found that anesthetists working at chil-dren’s hospital have a somewhat different way of dealing with neurotoxicity than those working in general hospitals. They are less likely to actively inform parents about potential neurotoxicity. Furthermore, a special anesthesia technique us-ing high dose opioids and muscle relaxants and no hypnotic agents in a highly selected patient population among extreme premature neonates is applied much more accepted and more frequent-ly used by colleagues working in a children’s hospital (see Figure 2). The main reason to apply this technique is normally not to avoid potential anesthetic drug neurotoxicity but to achieve an unmatched cardiovascular stability in these ex-tremely vulnerable patients. In a 2008 editorial McGowan et al. eloquently reminded all anes-thetists who are involved in pediatric cases not to forget the known threats and dangers to baby brains, such as hypotension and hypoxia.9 in our institution there is a trend towards the early ap-plication of low-dose continuous norepineph-rine in hypotensive anesthetized infants, even in premature babies, in order to re-establish and maintain sufficient cerebral perfusion pressure. Monitoring of regional cerebral oxygenation us-ing near infrared spectroscopy helps us to titrate the amount of norepinephrine and/or extra fluid.
this approach focuses on safe conduct of anesthesia and avoidance of well-known risks, such as arterial hypotension. It is in accor-dance with the key-statements of the recently founded saFetots initiative,4 where the fo-cus is more on safe conduct of anesthesia than on drug safety or possible toxicity.
the vast majority of the colleagues work-ing in general hospitals found this high-dose opioid technique to be unethical (see Figure 2). australian pediatric anesthetist andrew David-son recently asked the provoking question “is it time to question the mantra that all babies need a hypnotic agent such as sevoflurane”10 in the same editorial he furthermore mentioned that “in our institution we often anesthetize babies in the neonatal unit with just large doses of opioid
With our present practice strongly influ-enced by the principles of evidence based medicine, it is very difficult to modify our anesthetic techniques based on the extrapola-tion of results from animal or laboratory work, retrospective human database studies and heu-ristic decision making. The majority of the ret-rospective human studies published so far as-sessed possible long-term neurodevelopmental effects of exposure to anesthetic drugs using surrogate outcome parameters, which were chosen on grounds of availability rather than scientific reasoning. In other fields of medical research such an approach would most likely
Figure 4.—Future trials.Ranking of future trials in the field of anesthetic drug neuro-toxicity in young children.Percentage of respondents per rank.

Potential neUrotoXicitY oF anestHetic DrUgs in cHilDren WeBer
Vol. 82 - No. 3 Minerva anestesiologica 299
complied with our request. As a consequence it is impossible to provide or even estimate a re-sponse rate.
initially we wanted our survey to be submit-ted to all members of the esa and the ameri-can society of anesthesiologists (asa), to be able to compare the thoughts of our ameri-can colleagues to those of our european col-leagues. Unfortunately we were not able to convince the asa research committee regard-ing the importance of the topic. The ESA re-search committee approved our survey, but due to the media-code of the esa it was not possible to e-mail an invitation to participate to the society’s individual members.
in our survey anesthetists working in chil-dren’s hospitals were older and had more working experience than those working in gen-eral hospitals. This may have influenced the answers to (at least some) of our questions. In order to minimize this confounding effect we stratified our analyses for working experience.
We are aware of the fact that there is in-adequate scientific information and a lack of sufficient evidence regarding anesthetic drug neurotoxicity in young children. Interestingly, compared to the younger group, the more expe-rienced and older colleagues were more likely to question the existence of anesthetic drug induced neurotoxicity, supposedly because of this lack of hard evidence. This finding is in accordance with recent work by Besedes et al., who showed that older subjects are more likely to apply heuristic approaches in decision mak-ing than younger subjects.15 We regard this as an important finding for the planning and im-plementation of future initiatives and trials in the field of anesthesia safety in young children.
Conclusions
Practicing anesthetists care about potential neurotoxicity of anesthetic drugs in young children.
Many anesthetists have already changed their daily practice of pediatric anesthesia (avoidance of specific drugs, discuss indica-tions with surgeons, etc.).
and no volatile or intravenous general anesthetic agents. Others do the same”. At Sophia Chil-dren’s Hospital this technique is applied with increasing frequency in the same patient popu-lation as previously described by Davidson. We are aware of the fact, that asking a question about anesthetizing a child without an anesthetic agent has an extremely high potential to spark vigor-ous emotions. There is, however, a significant risk with emotions when we have to deal with serious matters. Iconic psychologist and Nobel Prize winner Daniel Kahneman recently got to the point: “emotions… explain most of the occa-sions on which people depart from rationality”.11
High-dose opioid techniques currently ap-pear to be gaining increasing popularity in neonatal anesthesia.12 recent data on remi-fentanil indicated anti apoptotic effects on the immature mouse brain.13 this, in addition to its other unique pharmacological properties,14 may make remifentanil become the opioid of choice in this specific population group.
the majority of the anesthetists surveyed found it necessary to further investigate the topic. Prospective clinical trials on possible effects of anesthetic drugs on neurodevelopmental out-come have been given the highest priority (see Figure 4), whereas further animal research was given the lowest priority. Interestingly, research projects focusing on anesthetic drug action in neonates scored second, whereas retrospective human database studies scored third, or second last. As it stands, practicing anesthetists are, in the first place interested in future studies with a chance to provide new information that can eas-ily be implemented into clinical practice, without the uncertainties of extrapolation of results ob-tained from other species.
the results of this survey do not claim to be representative, mainly due to the rather low number of respondents (N.=376). Fortunately the majority of respondents came from institu-tions that participated in the esa clinical trial network endorsed aPricot project, indicat-ing a certain degree of affinity towards pediatric anesthesia. The local coordinators of the APRI-cot centers were asked to spread our survey within their departments. Unfortunately we have no information as to whether they actually

WeBer Potential neUrotoXicitY oF anestHetic DrUgs in cHilDren
300 Minerva anestesiologica March 2016
References 1. Servick K. Biomedical Research. Researchers strug-
gle to gauge risks of childhood anesthesia. Science 2014;346:1161-2.
2. Rappaport BA, Suresh S, Hertz S, Evers AS, Orser BA. anesthetic neurotoxicity--clinical implications of animal models. N Engl J Med 2015;372:796-7.
3. Hansen TG. Anesthesia-related neurotoxicity and the developing animal brain is not a significant problem in children. Paediatr Anaesth 2015;25:65-72.
4. Weiss M, Vutskits L, Hansen TG, Engelhardt T. Safe An-esthesia For Every Tot - The SAFETOTS initiative. Curr Opin Anesthesiol 2015;28:302-7.
5. Jevtovic-Todorovic V, Absalom AR, Blomgren K, Bram-brink A, Crosby G, Culley DJ, et al. Anesthetic neuro-toxicity and neuroplasticity: an expert group report and statement based on the BJA Salzburg Seminar. Br J Anaesth 2013;111:143-51.
6. Olsen EA, Brambrink AM. Anesthetic neurotoxic-ity in the newborn and infant. Curr Opin Anesthesiol 2013;26:535-42.
7. Survey Monkey; [Internet]. Available from: www.sur-veymonkey.com [cited 2016, Feb 18].
8. European Society of Anaesthesiology. Clinical Trial Net-work; [Internet]. Available from: http://www.esahq.org/apricot [cited 2016, Feb 18].
9. McGowan FX, Jr., Davis PJ. Anesthetic-related neuro-toxicity in the developing infant: of mice, rats, monkeys and, possibly, humans. Anesth Analg 2008;106: 599-602.
10. Davidson AJ. Neurotoxicity and the need for anesthesia in the newborn: does the emperor have no clothes? anes-thesiology 2012;116:507-9.
11. Kahneman D. Thinking, Fast and Slow: Penguin Books, 2012.
12. Thompson ME. Preventing neurotoxicity: don’t for-get high-dose narcotic anesthetic. Paediatr Anaesth 2014;24:1110-1.
13. Tourrel F, de Lendeu PK, Abily-Donval L, Chollat C, Marret s, Dufrasne F, et al. The antiapoptotic effect of remifentanil on the immature mouse brain: an ex vivo study. Anesth Analg 2014;118:1041-51.
14. Penido MG, Garra R, Sammartino M, Pereira E, Silva Y. Remifentanil in neonatal intensive care and anesthesia practice. Acta Paediatr 2010;99:1454-63.
15. Besedes T, Deck C, Sarangi S, Shor M. Age Effects and Heuristics in Decision Making. Rev Econ Stat 2012;94:580-95.
compared to anesthetists working in gener-al hospitals, colleagues working in children’s hospitals felt better informed about potential neurotoxicity, were less likely to routinely in-form parents about this potential threat, and more frequently applied an analgesia based anesthesia to premature neonates.
The results of this survey confirm the inter-est of practicing anesthetists in future studies that may help to improve the safety of anesthe-sia in young children.
Key messages
— there is no consensus regarding the relevance of potential neurotoxicity of an-esthetic drugs in young children among practicing European anesthetists.
— as a result of the discussions regard-ing potential anesthetic drug neurotoxicity a considerable number of anesthetists have adjusted their daily practice of anesthesia in young children.
— anesthetists working in children’s hospitals are more reluctant to actively in-form parents about neurotoxicity than col-leagues working in general hospitals.
— Practicing anesthetists are signifi-cantly more interested in future prospec-tive longitudinal human studies with a fo-cus on neurodevelopmental outcome after anesthesia than in additional animal trials.
Acknowledgements.—The authors are grateful to Ms. Sandrine Damster and Mr. Benoit Plichon from the research department of the European Society of Anesthesiology (ESA) and to Prof. Andreas Hoeft, former ESA Research Committee Chairperson and Chairman of the Department of anesthesiology and intensive care Medicine, University of Bonn, germany, for their outstanding support of this project.We acknowledge the statistical support provided by our colleague Dr. Sanne Hoeks, clinical epidemiologist at the Department of Anesthesia, ErasmusMC, Rotterdam, The Netherlands.Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: September 3, 2015. - Manuscript accepted: August 12, 2015. - Manuscript revised: July 18, 2015. - Manuscript received: June 8, 2015.For supplementary materials, please see the online version of this article.

Vol. 82 - No. 3 MiNerVa aNestesiologica 301
cause identification may take at least 48 hours. In sepsis, appropriate and early empiric thera-py significantly decreases the mortality rate.1
In this study, we evaluated the diagnostic performance of commercial multiplex real-time PCR (LightCycler® SeptiFast, Roche, Mannheim, Germany), which produces results more rapidly than conventional blood culture
sepsis is a multisystem disease that typical-ly leads to hemodynamic changes, shock,
organ dysfunction, organ failure, and high mortality. Causative microorganisms cannot be isolated in many cases of suspected sepsis because of the low sensitivity of blood culture. Even if the causative pathogen can be isolated, initial therapy is often given empirically be-
O R I G I N A L A R T I C L E
Comparison of blood culture and multiplex real-time PCR
for the diagnosis of nosocomial sepsisFatih DINÇ 1, Halis aKaliN 2, Cüneyt ÖZAKIN 1, Melda SINIRTAŞ 1, Nesrin KEBABÇI 2,
Remzi IŞÇIMEN 3, Nermin KELEBEK GIRGIN 3, Ferda KAHVECI 3
1Department of Microbiology and Clinical Microbiology, Faculty of Medicine, Uludağ University, Bursa, Turkey; 2Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Uludağ University, Bursa, Turkey; 3Department of Anesthesiology and Reanimation, Faculty of Medicine, Uludağ University, Bursa, TurkeyCorresponding author: Halis Akalin, Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Uludağ University, 16059 Bursa, Turkey. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva AnestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: 10506-MAStitolo breve: BLOOD CULTURE AND REAL-TIME PCR IN SEPSISprimo autore: DINÇpagine: 301-9citazione: Minerva Anestesiol 2016;82:301-9
A B S T R A C TBACKGROUND: In many cases of suspected sepsis, causative microorganisms cannot be isolated. Multiplex real-time PCR generates results more rapidly than conventional blood culture systems.METHODS: In this study, we evaluated the diagnostic performance of multiplex real-time PCR (LightCycler® septiFast, Roche, Mannheim, Germany), and compared with blood cultures and cultures from focus of infection in nosocomial sepsis.RESULTS: Seventy-eight nosocomial sepsis episodes in 67 adult patients were included in this study. The rates of mi-croorganism detection by blood culture and PCR were 34.2% and 47.9%, respectively. Sixty-five microorganisms were detected by both methods from 78 sepsis episodes. Nineteen of these microorganisms were detected by both blood culture and PCR analysis from the same sepsis episode. There was statistically moderate concordance between the two methods (κ=0.445, P<0.001). There was no significant agreement between the blood culture and PCR analysis in terms of micro-organism detected (κ=0.160, P=0.07). Comparison of the results of PCR and cultures from focus of infection revealed no significant agreement (κ=0.110, P=0.176). However, comparison of the results of PCR and blood cultures plus cultures from focus of infection (positive blood culture and/or positive culture from focus of infection) showed poor agreement (κ=0.17, P=0.026). When the blood culture was used as the gold standard, the sensitivity, specificity, positive and nega-tive predictive value of PCR in patients with bacteremia was 80%, 69%, 57% and 87%, respectively.CONCLUSIONS: SeptiFast may be useful when added to blood culture in the diagnosis and management of sepsis.(Cite this article as: Dinç F, Akalin H, Özakin C, Sinirtaş M, Kebabçi N, Işçimen R, et al. Comparison of blood culture and multiplex real-time PCR for the diagnosis of nosocomial sepsis. Minerva Anestesiol 2016;82:301-9)Key words: Sepsis - Real-time polymerase chain reaction - Cell culture techniques.
Minerva Anestesiologica 2016 March;82(3):301-9© 2015 EDIZIONI MINERVA MEDICAThe online version of this article is located at http://www.minervamedica.it

DINÇ BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS
302 MiNerVa aNestesiologica March 2016
els were incubated in the Phoenix™ 100 BD system (Becton, Dickinson and Company) and evaluated.
Central-venous-catheter cultures were ex-amined by Maki’s semi-quantitative method.4
The SeptiFast Test
The SeptiFast Test is able to detect 25 differ-ent pathogens directly from blood by real-time multiplex PCR. A 3 mL whole blood sample for PCR analysis was obtained from the same peripheral vein immediately after the blood was drawn for the first blood culture. The sam-ples were placed in sterile EDTA tubes and transferred to the Central Microbiology Labo-ratory within 2 hours. In the Central Micro-biology Laboratory, the samples were main-tained at 4 °C. DNA extraction was initiated within three days. To avoid contamination, all molecular procedures were performed accord-ing to the manufacturer’s instructions (Roche Diagnostics GmbH, Mannheim, Germany).
DNA extraction was performed by using SeptiFast MGRADE Lys kit and Prep kit. Blood samples were placed in a MagNA Lyser instrument for 70 seconds at 700 rpm for me-chanical lysis with ceramic beads. Extracted DNA samples were maintained at -20 °C until to amplification. An in-vitro nucleic acid am-plification test for the detection and identifi-cation of DNA from bacterial and fungal mi-croorganisms was performed by the SeptiFast multiplex real-time PCR in a LightCycler® 2.0 instrument (Roche Diagnostics GmbH, Mannheim, Germany). Analysis of melting curves was done by using SeptiFast Identifica-tion Software (SIS, Roche Diagnostics GmbH, Mannheim, Germany).
Patients’ characteristics
During blood sample collection, the same individual recorded the patient’s body tem-perature, blood pressure, and pulse, in addition to the presence of a urinary catheter, ventilator support, and central vascular catheter. General information (age, gender, height, weight), clin-ical data, immunostatus, previous operations,
systems, and compared with blood cultures and other cultures from focus of infection.
Materials and methods
This study was performed with the approval of the Medical Research Ethics Board of the Faculty of Medicine at Uludağ University (ap-proval dated 8th March 2011, no.: 2011-6/9).
The study enrolled prospectively non-neutropenic patients older than 18 who were suspected or diagnosed with bacterial or fun-gal nosocomial sepsis, severe sepsis, or septic shock and were hospitalized in Reanimation and ICU or Internal Diseases wards at Uludağ University Hospital between 14th May 2012 and 7th November 2012 and who gave their in-formed consent.
Definition of sepsis and nosocomial infection
Sepsis, severe sepsis, and septic shock were defined according to consensus criteria estab-lished by the American College of Chest Phy-sicians and the Society of Critical Care Medi-cine (ACCP/SCCM) in 1991.2
Nosocomial infections were diagnosed based on the Centers for Disease Control and Prevention (CDC) criteria.3
Blood cultures
When a single patient experienced two sep-sis episodes, these episodes were accepted as different if there was at least a one-week inter-val between the two sepsis episodes.
BACTEC™ Plus Aerobic/F (Becton, Dickin-son and Company, Franklin Lakes, NJ, USA) was used for blood culture. Sufficient blood to fill two to three bottles (8-10 mL per bottle) was drawn from different suitable veins.
The blood cultures that gave positive signals were plated on 5% sheep-blood agar (BBL™ Prepared Plated Media, Becton, Dickinson and Company) and then incubated for 18-24 hours at 35 °C. The growing colonies that formed were transferred to an automatic identification panel (Phoenix™ PMIC/ID-70 and Phoenix™ NMIC/ID-99) to 0.5 McFarland turbidity. Pan-

BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS DINÇ
Vol. 82 - No. 3 MiNerVa aNestesiologica 303
tients who had received antibiotic therapy within 48 hours before sample collection were categorized as “those who previously used an-tibiotic therapy.”
Statistical analysis
Continuous variables was reported with me-dian (minimum-maximum) values while cat-egorical variables was reported as frequency and related percentage values. The agreement between blood culture and PCR methods was examined using Cohen’s κ coefficient. κ values normally lies between 0 and 1, with 0 indicat-ing agreement purely by chance and 1 indicat-ing perfect agreement. Although κ coefficients should be interpreted within the clinical context, values below <0.20 poor agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60 moderate agree-ment, 0.61-0.80 good agreement and 0.81-1.00 very good agreement. Comparisons of categori-cal variables between groups were performed using χ2 test. The level of statistically significant difference was set at P<0.05. Statistical analy-ses were performed with SPSS software v.13.0 (IBM Corporation, Chicago, IL, USA).
Results
The study included 78 samples obtained from nosocomial sepsis episodes in 67 pa-tients. In total, 24 (36%) female adults and 43 (64%) male adults were enrolled. The mean age of the subjects was 55.7 (21-95) years.
In the patients with sepsis, the most com-mon underlying diseases were hypertension (23.8%), diabetes mellitus (14.9%), chronic lung disease (13.4%), cerebrovascular disease (13.4%), and solid organ malignancy (11.9%). Twenty patients (29.8%) had no underlying disease.
Fifty-five (82%) patients were hospitalized in the intensive care unit, and 12 (18%) were hospitalized in wards other than intensive care units. During the 78 sepsis episodes, 63 (80.7%) of the patients who experienced sep-sis were on mechanical ventilation, 71 (91%) had a urinary catheter, and 64 (82%) had a cen-tral venous catheter.
antibiotics used, the Glasgow coma score, and the APACHE II score were obtained from each patient’s file. Detailed information about the blood culture sample that was obtained concomitantly with the PCR sample (time to blood culture positivity, growth, etc.) and cul-ture results for potential infection foci were obtained from the records of the microbiology laboratory.
Evaluation of culture and PCR results
An infectious disease specialist on the study team retrospectively evaluated the focus of in-fection, the severity of the sepsis, whether the microorganisms detected using blood culture and PCR analysis were causative pathogens. PCR results were not reported to the microbi-ology laboratory and clinicians until after the study was completed.
Causative pathogen: Blood culture results without contaminants were considered to represent causative pathogens. Retrospective evaluation of the focus of infection, agreement with blood culture, and the results obtained from the culture of other clinical samples was used to determine whether the microorganism detected using PCR analysis was the causative pathogen.
Blood culture contamination: The growth was considered contamination if microorgan-isms present in the epidermal flora (coagulase-negative staphylococci [CoNS] including S. epidermidis, diphtheroids — Corynebacteri-um spp., Streptococcus spp. — viridans group streptococci, Aerococcus spp., Micrococcus spp., Bacillus spp. except Bacillus anthracis) were isolated in only one of two concomitantly obtained blood cultures or if only one of two blood cultures obtained within 48 hours was positive.3
PCR contamination: CoNS and Streptococ-cus spp. detected using PCR were considered contamination based on the following criteria:
1. negative result in concomitantly obtained blood culture, and/or
2. lack of growth of the same microorgan-ism in other cultures.
Previous use of antibiotic therapy: the pa-

DINÇ BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS
304 MiNerVa aNestesiologica March 2016
culture and PCR were evaluated together, the rate of pathogen detection was 51.2%.
When the blood culture was accepted refer-ence method, the sensitivity, specificity, posi-tive and negative predictive value of PCR was 80%, 69%, 57% and 87%, respectively (Ta-ble II).
Comparison of the results of blood culture and PCR from samples obtained during sep-sis episodes revealed a statistically moderate agreement between the two methods (Table II).
When the 27 microorganism species that grew in the blood culture were analyzed, the
The most common infection foci of sepsis were the lung in the intensive care unit and the urinary system and central venous catheters outside the intensive care unit (Table I). In all patients who experienced sepsis, the 28-day mortality rate was 41.7%.
During sepsis, the microorganism detec-tion rate using blood culture was 34.2%. Four positive blood cultures were considered as contamination. The microorganism detection rate using PCR was 47.9%. One positive result obtained by PCR was considered as contami-nation. In the patients with sepsis, when blood
Table I.—�Microbiologically documented focus of infection during the sepsis events.Intensive care unit
(N.=65)Out of intensive care unit
(N.=14)total
(N.=79)*
Pneumonia 20* – 20Pyelonephritis 2 6 8Central venous catheter-associated bacteremia 23* 4 27Intra-abdominal infection 4 2 6Skin and soft tissue infection or surgical site infection 5 2 7Mediastinitis 1 – 1No focus of infection 10 – 10*One patient had diagnosed pneumonia and central venous catheter-associated bacteremia during the one sepsis event.
Table II.—�Compliance of blood culture and PCR results obtained during the sepsis events.Positive blood culture (%) Negative blood culture (%) Total (%)
PCR positive 20 (80%) 15 (31.2%) 35 (47.9%)PCR negative 5 (20%) 33 (68.8%) 38 (52.1%)total 25 (34.2%) 48 (65.8%) 73 (100%)κ=0.445 (P<0.001)General compliance rate: (20+33)/73 (72.6%)Compliance of the PCR with positive blood culture: 20/25 (80%)Compliance of the PCR with negative blood culture: 33/48 (68.8%)
Table III.—�Compliance of the microorganisms that grew in the blood culture with the cultures obtained from other sites.Other cultures Non-compliant Compliant total
A. baumannii 2 2 eta 4C. matruchotii 1 (1 cont.) – 1E. coli - 1 wound 1E. faecalis 2 – 2K. oxytoca 1 – 1K. pneumoniae 1 5 (3 ETA, 1 bile, 1 CVC) 6S. aureus 1 1 urine 2S. capitis spp ureolyticus 2 (1 cont.) – 2S. epidermidis 5 (2 cont.) – 5S. haemolyticus 1 2 cVc 3S. hominis 2 – 2S. maltophilia 1 1 cVc 2Total (causative pathogen) 15 (55.6%) 12 (44.4%) 27Total (cont. + causative pathogen) 19 (61.3%) 12 (38.7%) 31cont.: contamination; ETA: endotracheal aspirate culture; CVC: central venous catheter culture.

BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS DINÇ
Vol. 82 - No. 3 MiNerVa aNestesiologica 305
fection (positive blood culture and/or positive culture from focus of infection) showed poor agreement (κ=0.17, P=0.026).
There was better agreement between the results obtained from blood culture and PCR for Klebsiella pneumoniae/oxytoca, S. aureus, and Stenotrophomonas maltophilia. PCR per-formed better than blood culture, especially in the detection of fungal species, such as Aspergillus fumigatus, Candida albicans, C. parapsilosis, and Pseudomonas aeruginosa (Table VI).
There were two blood culture sets in which more than one microorganism was detected during sepsis. PCR had a higher capacity to de-tect multiple microorganisms. PCR concomi-tantly detected two microorganism species in seven samples and three microorganism spe-cies in five samples. All microorganism spe-cies that were detected more than once using both blood culture and PCR were considered pathogens.
agreement with culture results other than blood culture was 44.4% (Table III).
The agreement between PCR-based detec-tion of causative pathogens and the results ob-tained from the cultures other than blood cul-ture was 55.8% (Table IV).
From blood culture and PCR, 60 pathogenic microorganism species were isolated dur-ing 78 sepsis episodes. Of these species, 19 were isolated during the same episode by both methods. Blood culture identified the growth of eight microorganism species that were not detected by PCR. PCR detected 33 microor-ganism species that were not identified using blood culture. The agreement between the two methods was not statistically significant (Ta-ble V).
Comparison of the results of PCR and cul-tures from focus of infection revealed no sig-nificant agreement (κ=0.110, P=0.176). How-ever, comparison of the results of PCR and blood cultures plus cultures from focus of in-
Table IV.—�Compliance of the microorganisms detected using PCR with the cultures obtained from other body sites.Other cultures Non-compliant Compliant total
A. baumannii 1 6 (5 ETA, 1 ETA + CVC) 7Aspergillus fumigatus – 1 high serum galactomannan 1Candida albicans – 1 cVc 1Candida parapsilosis 1 1 cVc 2E. cloacae/aerogenes 5 – 5Enterococcus faecalis 1 4 (2 wound-pus, 2 CVC) 5Enterococcus faecium – 1 eta 1Escherichia coli – 2 wound-pus 2K. peumoniae/oxytoca 1 7 (1 wound-pus, 2 CVC, 1 bile, 2 ETA, 1 ETA + drainage fluid) 8coNs 12 (1 cont.) 2 cVc 14P. aeruginosa 1 2 (1 bile, 1 CVC) 3S. aureus 1 1 urine 2S. maltophilia 1 1 cVc 2Total (causative pathogen) 23 (44.2%) 29 (55.8%) 52Total (cont. + causative pathogen) 24 (45.3%) 29 (54.7%) 53cont.: contamination; ETA: endotracheal aspirate culture; CVC: central venous catheter culture.
Table V.—�Compliance of blood culture and PCR in terms of isolated microorganisms.Blood culture positive (%) Blood culture negative (%) total
PCR positive 19 (70.4%) 33 (50%) 52PCR negative 8 (29.6%) 33 (50%) 41total 27 66 93κ=0.160 (P=0.072)General compliance of PCR with blood culture: (19+33)/93 (55.91%)Compliance of PCR with positive blood culture: 19/27 (70.4%)Compliance of PCR with negative blood culture: 33/66 (50%)

DINÇ BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS
306 MiNerVa aNestesiologica March 2016
showed that blood culture positivity rarely ex-ceeded 50%.6, 7-19
We observed 80% sensitivity and 69% spec-ificity of PCR in terms of blood culture results. Fernandez-Romero et al. reported 71% sensi-tivity and 88% specificity,20 while Lehmann et al. reported 69% sensitivity and 81% specific-ity.14 Ozkaya-Parlakay et al. found 75% sensi-tivity and 100% specificity.21 In a recent meta-analysis, Chang et al. reported 75% sensitivity and 92% specificity.22 The quality of the stud-ies and heterogeneity of patients could be re-sponsible for these results.
In our study, the detection rate for causative microorganisms during sepsis was 34.2% by blood culture and 47.9% by PCR. In other stud-ies performed using SeptiFast, blood culture positivity ranged from 8-41%, and PCR posi-tivity ranged from 11 to 41%.8, 9, 11, 13, 14, 17-19, 23 PCR is better at detecting causative pathogens. In addition, we think that the wide variation in rates of detection may result from the char-acteristics of the patient population, the ret-rospective or prospective design of the study, differences in the rates of antibiotic use before sampling, and differences in blood culture sys-tems used.
In our study, although we observed no mi-croorganism growth using blood culture dur-ing 15 sepsis episodes, PCR allowed us to detect causative pathogens. Although the level
During 45 sepsis episodes in which an an-tibiotic was used before sample collection, blood culture positivity was 13 (28.8%), and PCR positivity was 21 (46.6%). Blood culture and PCR positivity were not significantly dif-ferent between the patients who received anti-biotic therapy before sepsis and those who did not (P=0.725).
In the patients who initiated antibiotic ther-apy before sepsis, fourteen pathogens were detected by blood culture and 33 by PCR (P=0.450).
In the 29 blood culture samples in which bacterial growth was detected during the sep-sis episodes, the average time to the appear-ance of the positive signal was 37.8 hours (1 day and 13 hours). The average time required for bacterial identification was 87.2 hours (3 days and 15 hours). Although the extraction of microorganism DNA and the time to identifi-cation using PCR varied by the number of con-comitantly analyzed samples and decreased with experience of the operator, the average duration was 6 h 15 min.
Discussion
In the diagnosis of sepsis, blood culture is the most important diagnostic microbiologi-cal test.5, 6 In recent years, studies of several groups of patients diagnosed with sepsis
Table VI.—�Microorganisms detected using blood culture and PCR during sepsis events.Microorganism Only blood culture Blood culture and PCR Only PCR total
A.baumannii 2 pathogen 2 pathogen 5 pathogen 9 pathogenA. fumigatus 1 pathogen 1 pathogenC. albicans 1 pathogen 1 pathogenC. parapsilosis 2 pathogen 2 pathogenC. matruchotii 1 cont. 1 cont.E. cloacae/aerogenes 5 pathogen 5 pathogenE. faecalis 2 pathogen 5 pathogen 7 pathogenE. faecium 1 pathogen 1 pathogenE. coli 1 pathogen 1 pathogen 2 pathogenK. peumoniae/oxytoca 7 pathogen 1 pathogen 8 pathogencoNs 4 pathogen + 3 cont. 5 pathogen 8 pathogen + 1 cont. 17 pathogen + 4 cont.P. aeruginosa 3 pathogen 3 pathogenS. aureus 2 pathogen 2 pathogenS. maltophilia 2 pathogen 2 pathogentotal 12
(8 pathogen + 4 cont.)19
(19 pathogen + 0 cont.)34
(33 pathogen + 1 cont.)65
(60 pathogen + 5 cont.)cont.: contamination.

BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS DINÇ
Vol. 82 - No. 3 MiNerVa aNestesiologica 307
though 8-10 mL of blood were obtained for each blood culture vial, only 1-5 mL was used for SeptiFast, as the manufacturer has reported that this amount is sufficient.
The thick cell wall of fungi and gram-posi-tive bacteria makes DNA extraction difficult, and this is believed to lower the sensitivity of PCR.8 However, in our study, despite the growth of two isolates of the gram-negative A. baumannii, these bacteria were not detected by PCR, leading us to question this view.
During PCR, there may be competition be-tween low levels of bacterial DNA and high levels of human genomic DNA, resulting in decreased sensitivity.26 In another study per-formed using SeptiFast, PCR was inhibited in three subjects with leukocyte counts >30,000/mm3.16 However, in our study, the leukocyte counts of five patients who showed growth of causative microorganisms in blood culture and negative results in PCR were between the 8920-22,500 mm3.
The inability to detect microorganisms by PCR may be explained by technical difficul-ties and mutations in the target region. Further studies are warranted.
In existing blood culture systems, the use of antibiotics before sample collection decreases their sensitivity. By contrast, antibiotic use has no effect on the sensitivity of PCR-based tests.27 Thus, in many studies performed using SeptiFast, the sensitivity of PCR was increased compared to blood culture in patients treated with antibiotics.6, 13, 14, 17-19, 23, 25 Similarly, in our study, the percentage of positive results obtained from blood culture during the sepsis episodes in which antibiotics were used before sample collection (28.8%) was lower than that
of detection varied in our study, PCR shows promise, with more microorganisms detected with PCR than with blood cultures during sep-sis episodes. The same was observed in many other studies (Table VII).6, 11, 13, 14, 18
In our study, despite the lack of fungal growth in blood culture, PCR revealed two cases of C. parapsilosis, one case of C. albicans, and one case of A. fumigatus, which were thought to be the causative microorganisms. Similarly, in other studies conducted using SeptiFast, more fungi were detected by PCR than by blood cul-ture.9, 11, 13, 18, 19, 23, 24
The SeptiFast system was designed to pre-vent the detection of CoNS and Streptococcus spp. DNA molecules at low concentrations, which may reflect contamination at various steps of the work flow.25 Like other studies conducted with SeptiFast, our study revealed lower rates of contamination using PCR com-pared to blood culture.9, 13, 14, 25
In five (6.4%) sepsis episodes in our study, despite the growth of microorganisms that were thought to be causative pathogens based on positive blood culture results, the PCR results were negative. More specifical-ly, eight causative pathogen species (two A. baumannii, two E. faecalis, four CoNS) grew in the blood culture but were not detected us-ing PCR. Although these causative microor-ganisms grew in blood culture, many other studies showed that they are not detected us-ing PCR.8, 9, 11, 12, 14, 17, 23 Therefore, negative PCR results should be interpreted with cau-tion.
Negative PCR results may be explained by the fact that the blood volume obtained was lower than that used for blood culture. Al-
Table VII.—�Blood culture and PCR positivity rates in some studies conducted using SeptiFast.Blood culture negative
PCR positive(%)
Blood culture positivePCR negative
(%)
Blood culture positivePCR positive
(%)
Blood culture negativePCR negative
(%)
Bloos et al. (2010) 8 22 3 13 62Avolio et al. (2010) 12 7 9 21 63Dierkes et al. (2009) 9 14 9 14 63Mancini et al. (2008) 11 14 1 19 66Vince et al. (2008) 23 23 10 10 57Westh et al. (2009) 14 14 3 11 72Tschiedel et al. (2012) 17 13 6 11 70

DINÇ BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS
308 MiNerVa aNestesiologica March 2016
References
1. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, opal sM, et al. Surviving Sepsis Campaign: Interna-tional guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39:165-228.
2. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sep-sis. Chest 1992;101:1644-55.
3. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveil-lance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008;36:309-32.
4. Maki DG, Weise CE, Sarafin HW. A semiquantative cul-A semiquantative cul-ture method for identifying intravenous catheter-related infection. N Engl J Med 1977;296:1305-9.
5. Mylotte JM, Tayara A. Blood cultures: clinical aspects and controversies. Eur J Clin Microbiol Infect Dis 2000;19:157-63.
6. Pasqualini L, Mencacci A, Leli C, Montegna P, Cardaccia a, cenci e, et al. Diagnostic performance of a multiple real-time PCR assay in patients with suspected sepsis hospitalized in an internal medicine ward. J Clin Micro-biol 2012;50:1285-8.
7. Previsdomini M, Gini M, Cerutti B, Dolina M, Per-ren A. Predictors of positive blood cultures in critically ill patients: a retrospective evaluation. Croat Med J 2012;53:30-9.
8. Bloos F, Hinder F, Becker K, Sachse S, Mekontso Dessap A, Straube E, et al. A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis. Intensive Care Med 2010;36:241-7.
9. Dierkes C, Ehrenstein B, Siebig S, Linde HJ, Reischl U, Salzberger B. Clinical impact of a commercially avail-able multiplex PCR system for rapid detection of patho-gens in patients with presumed sepsis. BMC Infectious Diseases 2009;9:126.
10. Josefson P, Strålin K, Ohlin A, Ennefors T, Dragsten B, Andersson L, et al. Evaluation of a commercial multi-plex PCR test (SeptiFast) in the etiological diagnosis of community-onset bloodstream infections. Eur J Clin Microbiol Infect Dis 2011;30:1127-34.
11. Mancini N, Clerici D, Diotti R, Perotti M, Ghidoli N, De Marco D, et al. Molecular diagnosis of sepsis in neutro-penic patients with haematological malignancies. J Med Microbiol 2008;57:601-4.
12. Avolio M, Diamante P, Zamparo S, Modolo ML, Gros-so S, Zigante P, et al. Molecular identifi cation of blood-Molecular identification of blood-stream pathogens in patients presenting to the emergency department with suspected sepsis. Shock 2010;34:27- 30.
13. Lucignano B, Ranno S, Liesenfeld O, Pizzorno B, Putig-nani L, Bernaschi P, et al. Multiplex PCR allows rapid and accurate diagnosis of bloodstream infections in new-borns and children with suspected sepsis. J Clin Micro-biol 2011;49:2252-8.
14. Westh H, Lisby G, Breysse F, Böddinghaus B, Choma-rat M, Gant V, et al. Multiplex real-time PCR and blood culture for identification of bloodstream pathogens in patients with suspected sepsis. Clin Microbiol Infect 2009;15:544-51.
15. Lodes U, Bohmeier B, Lippert H, König B, Meyer F. PCR-based rapid sepsis diagnosis effectively guides clinical treatment in patients with new onset of sirs. Lan-genbecks Arch Surg 2012;397:447-55.
16. Wallet F, Nseir S, Baumann L, Herwegh S, Sendid B, Boulo M, et al. Preliminary clinical study using a mul-tiplex real-time PCR test for the detection of bacterial
observed by PCR (46.6%). Likewise, in our study, PCR detected more microorganism spe-cies than blood culture after antibiotic use.
In our study, the results of blood culture and PCR showed moderate (67.9%) agree-ment. In other studies performed using Septi-Fast, the agreement ranged between 67% and 85%.8, 9, 11, 12, 14, 17, 23 By contrast, in our study, there was no significant agreement between the two methods in terms of species detection. As many more microorganism species were detected using PCR than using blood culture, this result was not surprising.
A previous study showed that in at least 10% of septic patients, the antibiotic therapy did not cover the causative pathogen, despite the use of broad-spectrum antibiotics.2 al-though approaches other than culture are not sufficiently rapid to allow the postponement of empiric antibiotic therapy, they can substan-tially shorten the time required to re-arrange or de-escalate the antibiotic therapy and may thus decrease the development of resistant pathogens, the length of the hospital stay, and additional costs.28
Therefore, many studies performed using SeptiFast have evaluated the effect of PCR on therapy during sepsis. They concluded that the use of PCR, which yields rapid results, could reduce the rates of inappropriate therapy in cases of sepsis.9, 16, 17, 19, 29-31
In conclusion, we consider that SeptiFast may be useful when added to blood culture in the diagnosis and management of sepsis. On the other hand, we should know the risk of false negative results with PCR.
Key messages
— The microorganism detection rate was found to be higher by PCR when com-pared to blood cultures.
— The rate of pathogen detection im-proved by combination of blood cultures and PCR.
— The rate of pathogen detection was found to be higher by PCR, in patients who received previous antibiotic treatment.

BLOOD CULTURE AND REAL-TIME PCR IN SEPSIS DINÇ
Vol. 82 - No. 3 MiNerVa aNestesiologica 309
O, Park LP, et al. Multiplex PCR to diagnose bloodstream infections in patients admitted from the emergency de-partment with sepsis. J Clin Microbiol 2010; 48:26-33.
25. Lehmann LE, Hunfeld KP, Emrich T, Haberhausen G, Wissing H, Hoeft A, et al. A Multiplex real-time PCR as-say for rapid detection and differentiation of 25 bacterial and fungal pathogens from whole blood samples. Med Microbiol Immunol 2008;197:313-24.
26. Jordan JA, Durso MB. Real time polymerase chain re-action for detecting bacterial DNA directly from blood of neonates being evaluated for sepsis. J Mol Diagn 2005;7:575-81.
27. Regueiro BJ, Varela-Ledo E, Martinez-Lamas L, Rodriguez-Calviño J, Aguilera A, Santos A, et al. auto-mated extraction improves multiplex molecular detection of infection in septic patients. PLoS One 2010;5:e13387.
28. van Loon HJ, Vriens MR, Fluit AC, Troelstra A, van der Werken C, Verhoef J, et al. Antibiotic rotation and de-Antibiotic rotation and de-velopment of gram-negative antibiotic resistance. Am J Respir Crit Care Med 2005;171:480-7.
29. Bravo D, Blanquer J, Tormo M, Aguilar G, Borrás R, solano c, et al. Diagnostic accuracy and potential clinical value of the LightCycler SeptiFast assay in the manage-ment of bloodstream infections occurring in neutropenic and critically ill patients. Int J Infect Dis 2011;15:e326-31.
30. Maubon D, Hamidfar-Roy R, Courby S, Vesin A, Mau-rin M, Pavese P, et al. Therapeutic impact and diagnostic performance of multiplex PCR in patients with malignan-cies and suspected sepsis. J Infect 2010;61:335-42.
31. Grif K, Fille M, Würzner R, Weiss G, Lorenz I, Gruber G, et al. Rapid detection of bloodstream pathogens by real-time PCR in patients with sepsis. Wien Klin Wochenschr 2012;124:266-70.
and fungal DNA directly in blood. Clin Microbiol Infect 2010;16:774-9.
17. Tschiedel E, Steinmann J, Buer J, Onnebrink JG, Felder-hoff-Müser U, Rath PM, et al. Results and relevance of molecular detection of pathogens by SeptiFast — a retro-spective analysis in 75 critically ill children. Klin Padiatr 2012;224:12-6.
18. Yanagihara K, Kitagawa Y, Tomonaga M, Tsukasaki K, Kohno S, Seki M, et al. Evaluation of pathogen detec-tion from clinical samples by real-time polymerase chain reaction using a sepsis pathogen DNA detection kit. Criti-cal Care 2010;14:R159.
19. Mauroa MV, Cavalcantia P, Peruginia D, Noto A, Sperlì D, Giraldi C. Diagnostic utility of lightcycler SeptiFast and procalcitonin assays in the diagnosis of bloodstream infection in immunocompromised patients. Diagn Micro-biol Infect Dis 2012;73:308-11.
20. Fernandez-Romero N, Quiles I, Jimenez C, Oliva MOL, Rivas B, Mingorance J, et al. Use of multiplex PCR in diagnosis of bloodstream infections in kidney patients. Diagn Microbiol Infect Dis 2014;80:93-6.
21. Ozkaya-Parlakay A, Cengiz AB, Ceyhan M, Hascelik G, Kara A, Celik M, et al. Evaluation of multiplex real time polymerase chain reaction and procalcitonin in the diag-nosis of sepsis. Clin Lab 2014;60:1075-81.
22. Chang SS, Hsieh WH, Liu TS, Lee SH, Wang CH, Chou Hc, et al. Multiplex PCR system for rapid detection of pathogens in patients with presumed sepsis — A systemic review and meta-analysis. PLOS One 2013;8:e62323.
23. Vince A, Lepej SZ, Barsić B, Dusek D, Mitrović Z, Serventi-Seiwerth R, et al. LightCycler SeptiFast assay as a tool for the rapid diagnosis of sepsis in patients during antimicrobial therapy. J Med Microbiol 2008;57:1306-7.
24. Tsalik EL, Jones D, Nicholson B, Waring L, Liesenfeld
Funding.—This work was supported by Uludağ University Scientific Research Projects Found.Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: May 29, 2015. - Manuscript accepted: May 27, 2015. - Manuscript revised: May 13, 2015. - Manuscript received: February 20, 2015.
310 Minerva anestesiologica March 2016
cedure is designed to achieve a loco-regional control of the tumor by removing all visible cancer and coupling it with regional high dos-es chemotherapy. Besides cancers arising from the peritoneal surface, HiPec showed its abil-
cytoreductive surgery (crs) and hyper-thermic intraperitoneal chemotherapy
procedure (HiPec) is an established treatment for an increasing number of malignancies in-volving peritoneal carcinomatosis. this pro-
O R I G I N A L A R T I C L E
time course of cytokines, hemodynamic and metabolic parameters during hyperthermic
intraperitoneal chemotherapyFederico coccolini 1 *, Davide corBella 2, Paolo FinaZZi 2, Pietro BraMBillasca 2,
alberto Benigni 2, viviana PrUssiani 2, Marco ceresoli 1, roberto ManFreDi 1, elia Poiasina 1, Paolo Bertoli 1, Fausto catena 3, andrea BiancHetti 4,
Mario BonteMPelli 4, luca F. lorini 2, valter sonZogni 2, luca ansaloni 1
1Department of general surgery, “Papa giovanni XXiii” Hospital, Bergamo, italy; 2Department of anesthesiology, “Papa giovanni XXiii” Hospital, Bergamo, italy; 3Department of emergency surgery, Maggiore Hospital, Parma, italy; 4Department of laboratory Medicine, “Papa giovanni XXiii” Hospital, Bergamo, italy*corresponding author: Federico coccolini, Department of general surgery, “Papa giovanni XXiii” Hospital, Piazza oMs 1, 24127 Bergamo, italy. e-mail: [email protected]
anno: 2016Mese: Marchvolume: 82no: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10333-Mastitolo breve: sYsteMic resPonse to HiPecprimo autore: coccolinipagine: 310-19citazione: Minerva anestesiol 2016;82:310-19
a B s t r a c tBacKgroUnD: systemic response to cytoreductive surgery (crs) and hyperthermic intraperitoneal chemotherapy (HIPEC) causes the activation of endocrine, metabolic, hemodynamic and inflammatory processes. The aim of this work is to describe and analyze the time course of the inflammatory markers concentration during CRS+HIPEC in plasma and peritoneal fluids and the association with hemodynamic and metabolic parameters.MetHoDs: Pre-, intra- and postoperative data were collected. tumor necrosis factor (tnF), interleukine 6 (il-6), pro-calcitonin (PCT), cancer antigen 125 (CA-125) in blood and in peritoneal fluids were evaluated.resUlts: thirty-eight patients were included, 29 (76.3%) of them were female. Mean/median Pci was 9.2/5, primary malignancy was 5 colorectal cancer (13.2%), 5 gastric cancer (13.2%), 23 ovarian cancer (60.5%) and 5 other malignan-cies (13.2%). combined clinical risk 0-1 was reached in all patients. cardiac index, heart rate and central venous pressure increased during the procedure, while stroke volume variation showed a decrease. Mean arterial pressure and superior vena cava oxygenation were stable throughout the whole procedure. tnF and ca-125 were steady during the whole procedure; il-6 had a relevant increase from baseline to start of perfusion (P<0.01); Pct had a steady increase at every time point. Peritoneal sampling showed a statistically significant increase (P<0.01) between start and end of the perfusion phase for all markers but tnF. serum and peritoneal marker concentration were similar for tnF, Pct and ca-125. il-6 showed a sharp difference.CONCLUSIONS: The most significant variations were in IL-6 and PCT levels. The cytokines level parallels the hemo-dynamic derangements. treatment during HiPec should mimic the established treatment during sepsis and septic shock.(Cite this article as: coccolini F, corbella D, Finazzi P, Brambillasca P, Benigni a, Prussiani v, et al. time course of cy-tokines, hemodynamic and metabolic parameters during hyperthermic intraperitoneal chemotherapy. Minerva anestesiol 2016;82:310-19)Key words: Inflammation - Cytokines - Adjuvant chemotherapy - Cytoreduction surgical procedures.
Minerva anestesiologica 2016 March;82(3):310-19© 2016 eDiZioni Minerva MeDicathe online version of this article is located at http://www.minervamedica.it

sYsteMic resPonse to HiPec coccolini
vol. 82 - no. 3 Minerva anestesiologica 311
and some cytokines (il-10) as well as it re-duces the concentration of pro-inflammatory mediators (il-1 and il-8).6, 7, 12 some observa-tional reports seem to confirm that anesthetic technique may affect the prognosis.6, 7, 12
cancer, surgery, hyperthermia and high-dose chemotherapy are potent stressful factor.8 systemic response to these insults causes the activation of endocrine, metabolic, hemody-namic and inflammatory processes, as outlined by increased inflammatory markers.13 all these elements are part of the Systemic Inflamma-tory response syndrome (sirs), whose most studied cases are sepsis and septic shock. sep-sis treatment is supported by a bulk of studies that allow a high level of evidence for some recommendations. the mechanisms of septic shock and HiPec storm are likely related and might respond to similar palliative maneuvers.
the aim of this study was to describe the time course of serum and peritoneal inflamma-tory markers concentration during HiPec. We will also provide a description of the changes of hemodynamic and metabolic parameters during the procedure.
Materials and methods
this is a prospective, single center, non-interventional study of cytokines kinetics. Written informed consent was collect from all patients. the study was approved by our in-stitutional ethical Board (approval dated 30th May 2012, protocol no. 727/2012).
all patients admitted for crs and HiPec with a diagnosis of peritoneal carcinosis with-out distant metastasis were consecutively enrolled. exclusion criteria were: recurrent carcinomatosis, distant metastasis, disease progression after chemotherapy, infiltration and retraction of mesentery, liver and/or kid-ney impairment. the following data were col-lected: demographics, peritoneal cancer index, histological type, asa score, cc score,14 in-traoperative hemodynamic (heart rate [Hr], mean arterial pressure [MaP], superior vena cava oxygenation [scvo2], stroke volume variation [svv], cardiac index [ci], sys-temic vascular resistance index [svri],
ity to increase survival rate in ovarian, colon and advanced gastric cancer.1, 2 Morbidity and mortality rate after the procedure are compara-ble with the ones from other major oncological procedures.3 Quality of life of the patients sur-viving 6 months is similar to baseline and it is even better in the case of patients with signifi-cant ascites.4 the procedure is performed on a routine base in several centers with an increas-ing number of patients yearly. Whereas post-operative morbidity and mortality, peritoneal kinetics of pharms, quality of life and long-term survivorship have been extensively stud-ied, anesthesiology support has several open questions. intra and perioperative support to the patients has been reviewed recently.5 the majority of papers deals with the hemody-namic parameters description and reports the results of the local treatment protocol.6-9 little effort has been poured into the elucidations of the relationship between the physiologic derangements observed and their causality. the procedure can be seen as made up by two different moments: the cytoreduction and the hyperthermic phase.5 the main feature of the CRS is extensive tissue injury and debulk, pa-tient cooling and fluid loss from the laparot-omy. During the hyperthermic phase, there is a hyperdynamic shock in the presence of an acute abdominal compartment syndrome due to the filling of the abdominal cavity. These two conflicting features seriously challenge the ability of the anesthesiologist to keep ad-equate organ function.
Tumors and inflammation share some char-acteristics as highlighted by the presence of in-flammatory cells and inflammatory mediators in cancer masses and by their role in angio-genesis and tissue remodeling.10 interleukins 1 and 6 (il-1 and -6), tumor necrosis factor alpha (TNF-α) and pro-calcitonin (PCT) play an important role in the inflammatory process, tumor progression and metastatic develop-ment.10 Controlling the inflammation may re-duce tumor dissemination and recurrence.6, 11
anesthesia may modulate stress response and the inflammatory process. Animal studies highlighted as epidural anesthesia improves the anticancer action of natural Killer cells

coccolini sYsteMic resPonse to HiPec
312 Minerva anestesiologica March 2016
nance was with sevoflurane or desflurane with a Mac between 0.7 and 1.0. if an epidural catheter was in place, a bolus was performed at the start of the procedure before skin inci-sion of ropivacaine 0.375% to avoid deep hy-potension followed by a continuous infusion of ropivacaine 0.2% plus sufentanil 0.75 μg/ml. remifentanil infusion was not standard-ized but tailored according to hemodynamic parameters and procedure phases. Under gen-eral anesthesia a radial artery catheter was inserted by a blind, percutaneous technique. advanced hemodynamic monitoring was al-ternatively performed with: Picco (Pulse index contour continuous cardiac output, Pulsion Medical systems, Feldkirchen, ger-many), vigileo (edwards lifesciences, irvine, ca, Usa) or swan ganz catheter. endpoint for hemodynamic were a MaP>65 mmHg and an svo2>75%. Fluids load and inotropic sup-port was not standardized and it was up to the anesthetist in charge. During the hyperthermic phase norepinephrine was suggested as the vasoactive drug of choice. Human albumin 20% was the first choice colloid to be used to counteract the protein lost from the peritoneal surface during the hyperthermic phase and to balance the ascites. at the end of the procedure all the patients were transferred to icU deeply sedated and under mechanical ventilation for postoperative monitoring and weaning.
HiPec was performed using a heat exchang-er, 2 roller pumps and a heater/cooler unit (exi-per, Medica s.p.a., Medolla, Modena, italy or Performer lrt, ranD, Medolla, Modena, italy). Hyperthermic intraperitoneal chemotherapy was performed as an open procedure with the coliseum technique 15, 16 using cisplatin (100 mg/m2) and/or paclitaxel (175 mg/m2) and/or doxo-rubicin (35 mg/m2), depending on the previous systemic chemotherapy undergone by each in-dividual patient. intraperitoneal chemotherapy was performed for 90 minutes, with a peritoneal and outflow thermal plateau of 41.5 °C.
Statistical analysis
the sample size was set to 38 patients due to funding restriction. the achieved power was
central venous pressure [cvP], epinephrine, norepinephrine, dopamine (mcg/kg/minute), calculated equivalent dose of norepinephrine, metabolic (glycemia and serum lactate con-centration) and pharmacologic data were col-lected. TNF-α, IL-6, PCT and CA-125 in se-rum and in peritoneal fluids were evaluated.
surgical procedure was divided into time frames: baseline (t0, samples were collected af-ter invasive monitoring was instituted and be-fore skin incision), induction of hyperthermia (t1, 5 minutes after warm chemotherapeutic cir-culation start), end of HiPec phase (t2) and end of surgery (t3). Hemodynamic parameters, va-soactive drugs administration and blood sam-ples were collected at every time frame. at ev-ery time frame, blood specimens (5 ml) were drawn from a peripheral vein, and collected di-rectly into heparinized tubes. aliquots of per-fusate were collected at t2 and t3. all blood and perfusate tubes were centrifuged (2500 rpm, 10 minutes, 4 °C) and the liquid fraction was transferred into cryovial. all the samples were stored at -20°C until analysis. The concentra-tions of TNF-α, IL-6, PCT and CA-125 were determined by a solid-phase sandwich en-zyme-linked immunosorbent assay (elisa) in duplicates. commercially-available elisa kits (Biosource/invitrogen Hu) were used us-ing the procedures provided by the manufac-turer. Prior assays were performed to assess the level of cytokines in peritoneal fluid. When necessary, samples were diluted using the ap-propriate diluent buffer and reanalyzed. We performed an internal quality control by using the same lot of each kit and the same serum/peritoneal fluid sample for all the experiments.
Conduction of anesthesia and hyperthermic perfusion protocol
Before induction of anesthesia an epidural catheter was inserted at thoracic level (t8-9) with the patient awake and in the sitting posi-tion. the catheter was under skin tunneled for 5 cm. induction was achieved with propofol 1.5 mg/kg, fentanyl 2 μg/kg and cis-atracuri-um 0.15 mg/kg followed by a continuous per-fusion at 1.5 μg/kg/min. Anesthesia mainte-

sYsteMic resPonse to HiPec coccolini
vol. 82 - no. 3 Minerva anestesiologica 313
variables Friedman test was used as general test and Wilcoxon matched-pairs signed rank sum test for two adjacent time frame. Statisti-cally significance was set at P<0.05 for general tests. For comparison between two adjacent time points a Bonferroni correction for multi-ple comparison was applied and the statistical threshold was set at P<0.017.
statistical analysis was done with the inter-cooled stata 12.0 statistical package (stata-corp, college station, tX, Usa).
Results
thirty-eight patients were enrolled. Pre-, intra- and postoperative data are reported in table i, along with the type and amount of in-fusion, and intra- and postoperative analgesia regimen. advanced hemodynamic monitor-
calculated a priori considering a clinically rele-vant increase in il-6 factor from baseline to the start of the hyperthermic phase (student’s t-test for mean, two-tailed paired data). Baseline of il-6 for a asa 1-2 patient undergoing surgery is 2.3±1.5 17 while il-6 for patients undergoing HiPec is 3.0.18 the power was 0.79 setting an alpha at 0.05 and the effect size of 0.467. gPow-er 3.1 for Mac was used for power analysis.19
continuous variables are presented as mean±standard deviation and median (range, minimum-maximum). normal distribution was checked by shapiro-Francia test. in case of normally distributed variables a repeated measures a one-group anova was used as a general test for differences across consecu-tive measurements while comparison between two adjacent time frame was done by a paired student’s t-test; for non-normally distributed
Table I.—�Preoperative, intraoperative and analgesia data.
Preoperative datagender (female/male) 29/9 (80.6%)BMi 24.3±4.4; 24.5 [16.4-32.0]age 56.3±10.2; 48.5 [33.1-71.7]asa score 1 (1, 2.6%)
2 (19, 50%)3 (18, 47.4%)
Pathologycolo-rectal cancer 5 (13.2%)gastric cancer 5 (13.2%)ovarian cancer 23 (60.5%)other 5 (13.2%)
intraoperative dataPci 9.2±8.5; 5 [0-28]cc score 0-1 38 (100%)anesthesia induction (min) 55.5±16.9; 54 [10-100]cytoreduction (min) 283.1±74.4; 273.5 [150-450]HiPec (min) 89.2±13.4; 90 [50-125]reconstruction (min) 105.9±52.5; 105 [40-280]Diuresis (ml) 3214.7±1810.8; 2900 [740-8600]Blood loss (ml) 636.4±460.8; 600 [0-2000]Fresh frozen plasma (ml) 189.7±371.3; 0 [0-1200]Human albumin 20% (ml) 322.1±156.8; 300 [0-600]red blood cells (ml) 487.6±420.4; 600 [0-1500]crystalloids (ml) 7390.9±2641.3; 7,000 [4500-13,700]colloids - hydroxyethilstarch 6% (ml) 772.7±1118.7; 500 [0-6000]
intraoperative analgesiaepidural 28 (82.4%)intravenous 6 (17.6%)
Postoperative analgesiaepidural 29 (85.3%)intravenuos 5 (14.7%)
Pci: Peritoneal cancer index; HiPec: hyperthermic intraperitoneal chemotherapy.Data are expressed as mean±sD; median [range] or absolute number and percentage.
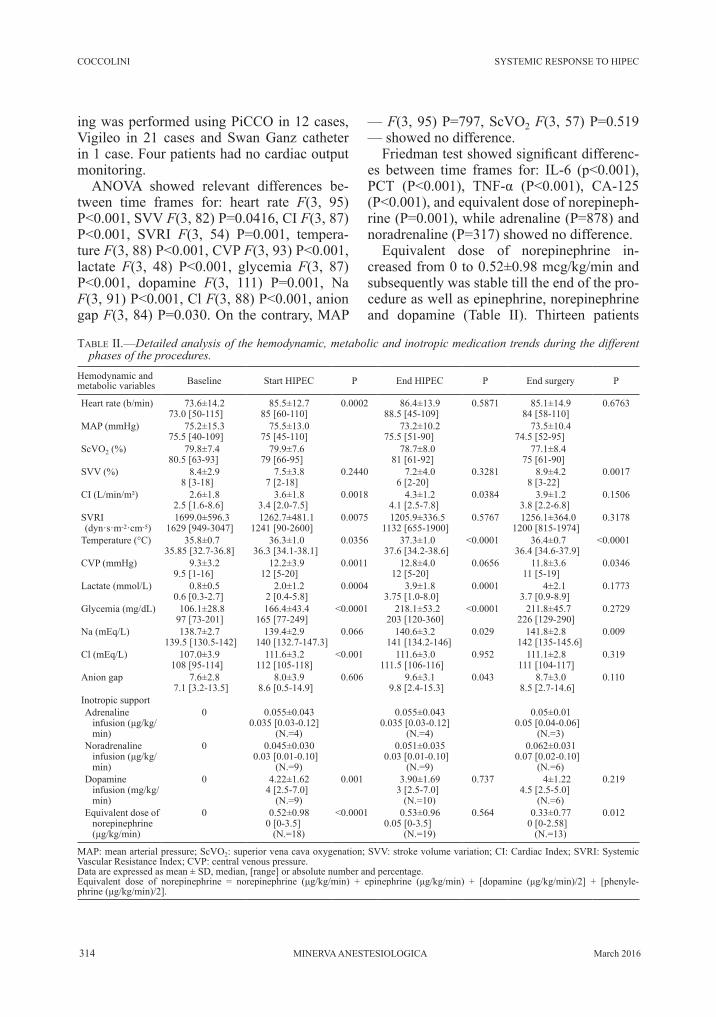
coccolini sYsteMic resPonse to HiPec
314 Minerva anestesiologica March 2016
— F(3, 95) P=797, scvo2 F(3, 57) P=0.519 — showed no difference.
Friedman test showed significant differenc-es between time frames for: il-6 (p<0.001), PCT (P<0.001), TNF-α (P<0.001), CA-125 (P<0.001), and equivalent dose of norepineph-rine (P=0.001), while adrenaline (P=878) and noradrenaline (P=317) showed no difference.
equivalent dose of norepinephrine in-creased from 0 to 0.52±0.98 mcg/kg/min and subsequently was stable till the end of the pro-cedure as well as epinephrine, norepinephrine and dopamine (table ii). thirteen patients
ing was performed using Picco in 12 cases, vigileo in 21 cases and swan ganz catheter in 1 case. Four patients had no cardiac output monitoring.
anova showed relevant differences be-tween time frames for: heart rate F(3, 95) P<0.001, svv F(3, 82) P=0.0416, ci F(3, 87) P<0.001, svri F(3, 54) P=0.001, tempera-ture F(3, 88) P<0.001, cvP F(3, 93) P<0.001, lactate F(3, 48) P<0.001, glycemia F(3, 87) P<0.001, dopamine F(3, 111) P=0.001, na F(3, 91) P<0.001, cl F(3, 88) P<0.001, anion gap F(3, 84) P=0.030. on the contrary, MaP
Table II.—�Detailed analysis of the hemodynamic, metabolic and inotropic medication trends during the different phases of the procedures.
Hemodynamic and metabolic variables Baseline start HiPec P end HiPec P end surgery P
Heart rate (b/min) 73.6±14.273.0 [50-115]
85.5±12.785 [60-110]
0.0002 86.4±13.988.5 [45-109]
0.5871 85.1±14.984 [58-110]
0.6763
MaP (mmHg) 75.2±15.375.5 [40-109]
75.5±13.075 [45-110]
73.2±10.275.5 [51-90]
73.5±10.474.5 [52-95]
scvo2 (%) 79.8±7.480.5 [63-93]
79.9±7.679 [66-95]
78.7±8.081 [61-92]
77.1±8.475 [61-90]
svv (%) 8.4±2.98 [3-18]
7.5±3.87 [2-18]
0.2440 7.2±4.06 [2-20]
0.3281 8.9±4.28 [3-22]
0.0017
ci (l/min/m²) 2.6±1.82.5 [1.6-8.6]
3.6±1.83.4 [2.0-7.5]
0.0018 4.3±1.24.1 [2.5-7.8]
0.0384 3.9±1.23.8 [2.2-6.8]
0.1506
svri (dyn·s·m-2·cm-5)
1699.0±596.31629 [949-3047]
1262.7±481.11241 [90-2600]
0.0075 1205.9±336.51132 [655-1900]
0.5767 1256.1±364.01200 [815-1974]
0.3178
Temperature (°C) 35.8±0.735.85 [32.7-36.8]
36.3±1.036.3 [34.1-38.1]
0.0356 37.3±1.037.6 [34.2-38.6]
<0.0001 36.4±0.736.4 [34.6-37.9]
<0.0001
cvP (mmHg) 9.3±3.29.5 [1-16]
12.2±3.912 [5-20]
0.0011 12.8±4.012 [5-20]
0.0656 11.8±3.611 [5-19]
0.0346
lactate (mmol/l) 0.8±0.50.6 [0.3-2.7]
2.0±1.22 [0.4-5.8]
0.0004 3.9±1.83.75 [1.0-8.0]
0.0001 4±2.13.7 [0.9-8.9]
0.1773
glycemia (mg/dl) 106.1±28.897 [73-201]
166.4±43.4165 [77-249]
<0.0001 218.1±53.2203 [120-360]
<0.0001 211.8±45.7226 [129-290]
0.2729
na (meq/l) 138.7±2.7139.5 [130.5-142]
139.4±2.9140 [132.7-147.3]
0.066 140.6±3.2141 [134.2-146]
0.029 141.8±2.8142 [135-145.6]
0.009
cl (meq/l) 107.0±3.9108 [95-114]
111.6±3.2112 [105-118]
<0.001 111.6±3.0111.5 [106-116]
0.952 111.1±2.8111 [104-117]
0.319
anion gap 7.6±2.87.1 [3.2-13.5]
8.0±3.98.6 [0.5-14.9]
0.606 9.6±3.19.8 [2.4-15.3]
0.043 8.7±3.08.5 [2.7-14.6]
0.110
inotropic supportadrenaline
infusion (μg/kg/min)
0 0.055±0.0430.035 [0.03-0.12]
(n.=4)
0.055±0.0430.035 [0.03-0.12]
(n.=4)
0.05±0.010.05 [0.04-0.06]
(n.=3)noradrenaline
infusion (μg/kg/min)
0 0.045±0.0300.03 [0.01-0.10]
(n.=9)
0.051±0.0350.03 [0.01-0.10]
(n.=9)
0.062±0.0310.07 [0.02-0.10]
(n.=6)Dopamine
infusion (mg/kg/min)
0 4.22±1.624 [2.5-7.0]
(n.=9)
0.001 3.90±1.693 [2.5-7.0]
(n.=10)
0.737 4±1.224.5 [2.5-5.0]
(n.=6)
0.219
equivalent dose of norepinephrine (μg/kg/min)
0 0.52±0.980 [0-3.5]
(n.=18)
<0.0001 0.53±0.960.05 [0-3.5]
(n.=19)
0.564 0.33±0.770 [0-2.58]
(n.=13)
0.012
MaP: mean arterial pressure; scvo2: superior vena cava oxygenation; svv: stroke volume variation; ci: cardiac index; svri: systemic vascular resistance index; cvP: central venous pressure.Data are expressed as mean ± sD, median, [range] or absolute number and percentage.Equivalent dose of norepinephrine = norepinephrine (μg/kg/min) + epinephrine (μg/kg/min) + [dopamine (μg/kg/min)/2] + [phenyle-phrine (μg/kg/min)/2].

sYsteMic resPonse to HiPec coccolini
vol. 82 - no. 3 Minerva anestesiologica 315
was similar for tnF, Pct and ca-125 whereas il-6 showed a sharp difference between them (peritoneal vs. serum concentration, table iii; start of the perfusion P<0.01, end of the perfu-sion P<0.01).
Discussion
the crs and HiPec is a complex proce-dure with significant metabolic alterations and fluid shift, and burdened by a significant post-operative morbidity and mortality even in an asa 1-2.
Our data confirm the classical descrip-tion of the procedure 6, 7, 9 as a hyperdynamic shock in the presence of an acute abdominal compartment syndrome. Different continuous co monitoring systems were used during the study, mainly Picco and vigileo with a third-generation Flotrac. this can be a bias of the study as little accordance between thermodi-lution and pulse-contour analysis systems is reported 20 during hemodynamic instability whereas good accordance is reported during stable condition. However, the target was the changes in hemodynamic parameters and not their absolute value during the procedure.
Hr shows an increasing trend during HiPec and decrease at the end, although not signifi-
were transferred in icU while still on aminic support (table ii, end of surgery equal to icU admission). the days under mechanical venti-lation were 2 (1-20), but 28 patients were ex-tubated in 48 hours. icU length of stay was 3 (1-21) days, but 25 patients were discharged in 72 hours.
lactate and glycaemia showed a clini-cally relevant increase in every phase of the procedure until the end of the hyperthermic phase (table ii). anion gap was stable dur-ing the different phases of the procedure, whereas cl showed a slight increase from baseline to the start of hyperthermia and na from the start until the end of the hyperther-mic perfusion.
cytokines and tumor markers serum con-centration showed these results: tnF and ca-125 were steady during the whole procedure; il-6 had an increasing trend during the pro-cedure that was statistically significant when compared baseline with start of perfusion (P<0.01); PCT had a statistically significant increase at every time point. on the contrary peritoneal sampling showed a statistically sig-nificant increase (P<0.01) between start and end of the perfusion phase for all markers but tnF (table iii).
serum and peritoneal marker concentration
Table III.—�Detailed analysis of cytokine trends during the different phases of the procedure.Baseline start of perfusion P end of perfusion P end of surgery P
cytokines – plasmatnF 9.3±1.0
9.0 [7.7-12.4]13.2±19.3
9.8 [8.5-125.4]<0.001 10.2±1.6
9.9 [8.5-17.7]0.392 10.1±1.1
9.9 [8.5-13.2]0.751
il-6 58.3±235.54.9 [2.9-1425.6]
439.6±417.8289.2 [3.6-1742.5]
<0.001 555.7±1068.6222.8 [37.9-5224.0]
0.038 603.8±1180.1145.6 [25.0-5224.0]
0.085
Pro-calcitonin 0.1±0.20.04 [0.04-1.14]
0.3±0.50.11 [0.04-1.98]
<0.001 1.0±1.60.42 [0.04-6.45]
<0.001 1.9±2.90.97 [0.04-13.36]
<0.001
ca125 107.3±413.410.5 [2-2334]
65.3±252.67 [2-1446]
<0.001 56.8±209.07.5 [2-1157]
0.099 56.9±203.07 [2-1053]
0.382
cytokines – peritoneumtnF 11.0±1.8
10.8 [8.33-16.64]10.5±1.4
10.1 [8.62-13.89]0.060
il-6 2333.8±2817.61302.6 [53.2-12,266.0]
6214.4±4792.56048.2 [280.3-21,958.0]
<0.001
Pro-calcitonin 0.3±0.90.07 [0.04-5.00]
0.7±1.40.15 [0.04-05.91]
<0.001
ca125 14.1±17.69 [1-101]
26.3±38.815 [1-223]
<0.001
tnF: tumor necrosis factor; il-6: interleukin 6; ca-125: cancer antigen 125.Data are expressed as mean±sD, median [range] or absolute number and percentage.

coccolini sYsteMic resPonse to HiPec
316 Minerva anestesiologica March 2016
is characterized by hyperthermia second-ary to the warm abdominal perfusion. Keep-ing central body normothermia is of utmost importance as coagulation, hemodynamic, glycemic and renal balance is related to this goal and the higher the temperature the more sever is the derangement.6, 7 typically, this is achieved by active warming the patient dur-ing crs phase (i.e. hot liquids and forced air warmers) and active cooling during HiPec. Though statistically significant, temperature variations in the present cohort of patients where minor and 95% of the patients experi-enced a peak temperature lower than 38.5 °C with an average value of peak temperature of 37.3 °C. Present data could suggest that the minor hemodynamic impact could be relat-ed to better temperature control. the steady increase in glycaemia level parallels the de-rangements in inflammatory markers. This is easily explained by the well-known effect of an increased peripheral insulin resistance in the inflammatory states.
anion gap was stable during the whole pro-cedure. na and cl concentration showed an increase that even if relevant was still in the physiologic range and not at risk to cause hy-perchloremic metabolic acidosis.
Inflammatory mediators in plasma and in peritoneal fluids are different between patients with and without cancer, and between the dif-ferent types of cancers.18 this could suggest peritoneotropic characteristics different from one cancer to another. vlaeminck-guillem et al.18 recently suggested the possible role as prognostic factor for the long-term outcome of the patient of these cytoplasmic and intra-peritoneal mediators. anyway our sample was too little to catch differences between different types of cancers.
tnF is a cytokine involved in systemic in-flammation, apoptotic cell death, proliferation and cellular differentiation. the overproduc-tion of tnF is implicated in carcinogenesis.6, 7 it also acts as a promoter of the production of acute phase proteins. Moreover, it leads to hy-potension due to vasodilatation and decreased myocardial contractility.6, 7 its plasma level is increased in the course of septic shock.6, 7
cant (table ii). MaP variations were minimal (table ii) probably due to the strict adherence to the anesthesia protocol that involves the use of vasopressors (mainly norepinephrine) dur-ing the hyperthermic phase. inotropic support was present in no patient at the start of the pro-cedure, in 18 patients (47.3%) during the first minutes of HiPec phase and in 19 at the end (50%) to counteract systemic vasodilatation induced by hyperthermia. this was mirrored by the svri drop at the HiPec start. However SVRI showed a not significant increase at the end of surgery during the cooling down phase (table ii).
no variations in scvo2 were detected (table ii). it was already high at the start of surgery, as expected under general anesthesia, and no variations were seen during the HiPec phase. We saw rarely an scvo2 lower than 65%, a safe threshold for hemodynamic op-timization.21, 22 this probably was due to the aggressive fluid resuscitation, early hemody-namic support by inotropes and hyperdynamic state during hyperthermia. However, the lack of decrease in scvo2 may be an inadequate sign of tissue perfusion as we had a steady in-crease in lactate level (table ii).
cvP trend analysis is a puzzling topic in this procedure as it can be affected by variables such as vascular tone, volume filling, intratho-racic and intraperitoneal pressure. it increases at the start of the HiPec phase and shows a not significant reduction toward the end of the procedure (Table II). This fluctuation is prob-ably due to the introduction, and removal, of large volumes chemotherapy in the abdominal cavity. However high, cvP, increased lactate level and a stable ci during the hyperthermic phase may suggest some degree of cardiac im-pairment.
CI showed a significant increase during the HiPec phase to decrease afterwards (ta-ble ii). this peak-and-valley swinging trend is related to the on-set of the hyperthermic state as extensively described in literature.6, 7
Metabolic alteration has several causes and effects. temperature control is challeng-ing. Whereas crs is related to hypothermia due to wide visceral exposure, HiPec phase
sYsteMic resPonse to HiPec coccolini
vol. 82 - no. 3 Minerva anestesiologica 317
increase lesser (table iii). Moreover Pct plasmatic level continues to increase till the 3rd postoperative day (data not shown). How-ever, the value of PCT increased significantly during all the phases. This confirms the PCT release during clinical situations other than in-fectious.
the ca-125 is an important biomarker commonly used for the diagnostic and prog-nostic evaluation of some types of cancer. the evaluation of serum ca-125 is mainly used in the follow-up of ovarian cancer, but it can still be high in the case of primary or metastatic cancer of the endometrium, fallo-pian tubes, lung, breast and gastrointestinal tract.6, 7 recently, a relationship among ca-125, congestive heart failure and the severity of clinical and hemodynamic parameters has been found.25 the increase of these values may be induced by cytokines, such as il-6.25 Present data show that the values of ca-125 appear to decrease in serum during surgery even if not statistically significant, while sig-nificantly increasing in the peritoneal perfus-ate during HiPec as a production of the me-sothelial cells consequent to the hyperthermic and surgical stress. Moreover, this data could be related to the increase of values of il-6 in the perfusate itself, or to tumor and meso-thelial cell death and cytolysis, although it is impossible to differentiate those two effects. However, it seems to confirm once again the effectiveness of peritoneal-plasma barrier in maintaining the most of intra-abdominal pro-cess confined to the abdominal cavity.26 last-ly ca-125 plasmatic level showed to be in-creased in 3rd and 7th postoperative days (data not shown).
the data presented suggest the similarity between HiPec phase and the septic state. these two states share the same feature of hemodynamic collapse with poor peripheral tissue perfusion that needs inotropic support and fluid replacement, massive third space creation, temperature unbalance, hypergly-cemia and cytokine rise. anesthesiologists have to face the difficulties of maintaining hemodynamic and metabolic parameters as close to physiological value as possible. the
Present data show how the values of tnF in serum and perfusate do not vary significantly (table iii). its level continues to rise in plasma until the 3rd postoperative day in the few pa-tients who had this level checked in the post-operative period (data not shown). these data do not allow to hypothesize an action of tnF on hemodynamic.
the il-6 acts as both a pro-and an anti-in-flammatory factor, with an important role in the immune response, cell proliferation and apoptosis. High levels of il-6 are involved in the various stages of tumor development.6, 7 IL-6 acts as an anti-inflammatory cytokine by inhibiting tnF and il-1.6, 7 the plasma levels of il-6 rise dramatically at the HiPec start and remain high for a long time until the 3rd postoperative day and tending to normal-ize the 7th (data not shown). In peritoneal flu-ids, il-6 concentration is thousands of times serum concentration. the trend shows a con-tinuous increase through the whole procedure (table iii). il-6 plasmatic values rise during HiPec and do not fall subsequently. at peri-toneal level, values increase significantly. Sta-tistically significant is the comparison of the increase in serum and peritoneal levels. this difference seems to indicate the effectiveness of loco-regional treatment if interpreting il-6 as a result of the massive tumor cell death. vlaeminck-guillem et al.18 reported similar results, with an increase of il-6 both in se-rum and peritoneum with an exponential dif-ference between the patients with and without cancer.6, 7 Moreover, this difference suggests a paracrine role of the il-6 with a local produc-tion exceeding the passage from the serum into the peritoneum.
the Pct is a marker of bacterial infec-tions, but its increase is also seen in some sirs conditions not necessarily borne by in-fectious events, such as the cardiogenic shock and trauma surgery.23, 24 tnF and il-6 can stimulate its extra thyroid synthesis.23, 24 it has chemotactic properties for lymphocytes and modulates the production of nitric oxide (no) by endothelial cells.23, 24 its values consider-ably increase in serum throughout the surgery, while, in absolute values in the peritoneum

coccolini sYsteMic resPonse to HiPec
318 Minerva anestesiologica March 2016
Key messages
— During HiPec some degrees of circulatory failure are present despite a healthy patients, an invasive hemodynamic monitoring, and an aggressive fluid and inotropic support therapy.
— the hyperthermic phase of the pro-cedure is characterized by a sharp and pre-dictable increase of inflammation markers. this period can be used to test the ability of different anesthetic technique or drugs to reduce or blunt the inflammatory response during surgery.
References
1. coccolini F, cotte e, glehen o, lotti M, Poiasina e, cat-ena F, et al. intraperitoneal chemotherapy in advanced gastric cancer. Meta-analysis of randomized trials. eur J surg oncol 2014;40:12-26.
2. coccolini F, gheza F, lotti M, virzì s, iusco D, gh-ermandi c, et al. Peritoneal carcinomatosis. WJg 2013;19:6979-94.
3. chua tc, Yan tD, saxena a, Morris Dl. should the treatment of peritoneal carcinomatosis by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy still be regarded as a highly morbid procedure? a sys-tematic review of morbidity and mortality. ann surg 2009;249:900-7.
4. McQuellon rP, loggie BW, Fleming ra, russell gB, lehman aB, rambo tD. Quality of life after intraperi-toneal hyperthermic chemotherapy (iPHc) for peritoneal carcinomatosis. eur J surg oncol 2001;27:65-73.
5. corbella D, Piraccini e, Finazzi P, Brambillasca P, Prus-siani v, corso Mr. anesthetic management of cytoreduc-tive surgery and hyperthermic intraperitoneal chemother-apy procedures. World J obstet gynecol 2013;2:129-36.
6. shime n, lee M, Hatanaka t. cardiovascular changes during continuous hyperthermic peritoneal perfusion. anesth analg 1994;78:938-42.
7. raue W, tsilimparis n, Bloch a, Menenakos c, Hart-mann J. volume therapy and cardiocircular function dur-ing hyperthermic intraperitoneal chemotherapy. eur surg res 2009;43:365-72.
8. Desborough JP. the stress response to trauma and sur-gery. Br J anaesth. 2000;85:109-17.
9. schmidt c, creutzenberg M, Piso P, Hobbhahn J, Bucher M. Peri-operative anaesthetic management of cytoreduc-tive surgery with hyperthermic intraperitoneal chemo-therapy. anaesthesia 2008;63:389-95.
10. Grivennikov SI, Greten FR, Karin M. Immunity, inflam-mation, and cancer. cell 2010;140:883-99.
11. Coussens LM, Werb Z. Inflammation and cancer. Nature 2002;420:860-7.
12. lin l, liu c, tan H, ouyang H, Zhang Y, Zeng W. an-aesthetic technique may affect prognosis for ovarian serous adenocarcinoma: a retrospective analysis. Br J anaesth 2011;106:814-22.
13. Desborough JP. the stress response to trauma and sur-gery. Br J anaesth 2000;85:109-17.
three cornerstones of the management of a patient undergoing crs and HiPec are con-tinuous hemodynamic evaluation and prompt support, accurate temperature control and aggressive correction of every physiologic derangement, as in the case of sepsis. the similarity in the pathophysiology and sup-portive treatment between sirs ad HiPec suggest the possibility to apply some of the established sepsis treatment to this proce-dure. For example, forced diuresis to prevent acute kidney failure can be ineffective as systemic concentration of chemotherapeutic agent is far below the toxic threshold and a diuretic forced diuresis is no longer recom-mended for cisplatin toxicity.27 Moreover it has no effect on renal perfusion that is linked to the circulating volume and ci. Beside this high diuretic doses, especially in the presence of a lower than normal perfused kidney, pro-duce a persistent diuresis for hours after the procedure enhancing a vicious circle of poor peripheral tissue perfusion.
the HiPec procedure can be considered as a peculiar model of sirs. it has some ad-vantageous characteristics: a predictable and sharp rise in cytokine levels followed by a re-duction until normalization at the end of the hyperthermic perfusion phase, a setting with a full monitored patient, predictable metabolic and hemodynamic derangements. this situa-tion can be a good “experimental setting” in which it is possible to test if different anesthet-ic approach (i.e. analgesia regimen, metabolic correction, different preoperative feeding) can have a positive effect in reducing the inflam-matory response to the surgery and hyperther-mia.
Conclusions
cytokines level parallels the hemodynamic and metabolic derangements seen mainly in the hyperthermic phase of the procedure. il-6 and Pct showed the most clinically relevant variations. HiPec can be a good setting to tai-lor anesthesia intervention to the reduction of inflammatory response and test its effective-ness.

sYsteMic resPonse to HiPec coccolini
vol. 82 - no. 3 Minerva anestesiologica 319
Bennett eD. changes in central venous saturation after major surgery, and association with outcome. Crit Care 2005;9:r694-9.
22. grocott MPW, Dushianthan a, Hamilton Ma, Mythen Mg, Harrison D, rowan K. Perioperative increase in global blood flow to explicit defined goals and out-comes following surgery. cochrane Database syst rev 2012;11:cD004082.
23. Wanner ga, Keel M, steckholzer U, Beier W, stocker r, ertel W. relationship between procalcitonin plasma levels and severity of injury, sepsis, organ failure, and mortality in injured patients. Crit Care Med 2000;28:950-7.
24. Maisel as, choudhary r. Biomarkers in acute heart fail-ure--state of the art. nat rev cardiol 2012;9:478-90.
25. vizzardi e, nodari s, D’aloia a, chiari e, Faggiano P, Metra M. ca 125 tumoral marker plasma levels relate to systolic and diastolic ventricular function and to the clini-cal status of patients with chronic heart failure. echocar-diography 2008;25:955-60.
26. Sugarbaker PH. Peritoneum as the first-line of defense in carcinomatosis. J surg oncol 2007;95:93-6.
27. launay-vacher v, rey J-B, isnard-Bagnis c, Deray g, Daouphars M. Prevention of cisplatin nephrotoxic-ity: state of the art and recommendations from the eu-ropean society of clinical Pharmacy special interest group on cancer care. cancer chemother Pharmacol 2008;61:903-9.
14. Jaquet P, sugarbaker PH. clinical research methodolo-gies in diagnosis and staging of patients with peritoneal carcinomatosis. cancer treat res 1996;82:359-74.
15. sugarbaker PH. Management of peritoneal-surface ma-lignancy: the surgeon’s role. langenbecks arch surg 1999;384:576Y587.
16. sarnaik aa, sussman JJ, ahmad sa, Mcintyre Bc, lowy aM. technology for the delivery of hyperthermic intraoperative intraperitoneal chemotherapy: a survey of techniques. recent results cancer res 2007;169:75Y82.
17. Braz Mg, Braz lg, Braz Jr, Pierine Dt, correa cr, Fer-reira al, et al. comparison of oxidative stress in asa physical status i patients scheduled for minimally inva-sive surgery under balanced or intravenous anesthesia. Minerva anestesiol 2013;79:1030-8.
18. vlaeminck-guillem v, Bienvenu J, isaac s, grangier B, Golfier F, Passot G, et al. intraperitoneal cytokine level in patients with peritoneal surface malignancies. a study of the renaPe (French network for rare Peritoneal Ma-lignancies). ann surg oncol 2013;20:2655-62.
19. Faul F, erdfelder e, lang ag, Buchner a. g*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav res Methods 2007;39:175-91.
20. schlöglhofer t, gilly H, schima H. semi-invasive meas-urement of cardiac output based on pulse contour: a re-view and analysis. can J anaesth 2014;61:452-79.
21. Pearse r, Dawson D, Fawcett J, rhodes a, grounds rM,
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: July 8, 2015. - Manuscript accepted: July 6, 2015. - Manuscript revised: July 1, 2015. - Manuscript received: December 1, 2014.

320 Minerva anestesiologica March 2016
acids, arginine, selenium) have been admin-istered alone or in association, coupled with the normal constituents of the basic nutrition (macro and micronutrients) but in very high quantities so to magnify their expected phar-macological effect.
some of these immunonutrients proved to be effective in several studies, but inconsistently. Most of the clinical studies demonstrating some benefit from immunonutrition were conducted in the setting of elective surgery for gastrointes-tinal cancer.4-6 in the critically ill, the evidence has been controversial: while older single-cen-ter studies demonstrated some benefit, most re-
in the last two decades, much attention has been focused on the correct way to feed crit-
ically ill patients. The most recent scientific evidence is still confirming a very old con-cept, i.e. that an adequate delivery of energy and protein improves patient’s outcome.1-3 Furthermore, efforts have been made to inves-tigate pharmacologically active nutrients that may modulate the metabolic and inflammatory response to surgery and stress and enhance immune function. these so-called “immuno-nutrients” (mainly: glutamine, omega-3 fatty
R E V I E W
immunonutrients in critically ill patients: an analysis of the most recent literatureMaria g. annetta 1*, Mauro PittirUti 2, Pietro veccHiarelli 3, Davide silvestri 1, anselmo caricato 1, Massimo antonelli 1
1Department of anesthesia and intensive care, catholic University, rome, italy; 2Department of surgery, catholic University, rome, italy; 3intensive care Unit, Belcolle Hospital, viterbo, italy*corresponding author: Maria g. annetta, Department of anesthesia and intensive care, catholic University, largo Francesco vito 1, 00168 rome, italy. e-mail: [email protected]
anno: 2016Mese: Marchvolume: 82no: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10513-Mastitolo breve: iMMUnonUtrients in criticallY ill Patientsprimo autore: annettapagine: 320-31citazione: Minerva anestesiol 2016;82:320-31
a B s t r a c tModulation of inflammatory and immune response to critical illness has been the goal of much research in the last decade and a variety of drugs and nutrients (so called “immunonutrients”) have been tested in experimental models with promis-ing results. Though, in the clinical setting of intensive care, their efficacy have been inconsistently proven, most likely because the effects of each drug may vary in relation to the timing, the dose, the route of administration, the interaction with other nutrients, the severity of illness and many other factors. though the early studies of the beginning of this century (2000-2009) have shown some clinical benefits, recent multicenter trials (2011-2015) have failed to prove a con-sistent benefit of immunonutrition in terms of mortality or other clinical endpoints. Reviewing the latest evidence-based documents on this subject (multicenter trials, systematic reviews, meta-analyses and international guidelines), there is no convincing evidence that immunonutrients may be beneficial in the critically ill. Considering that these substances invariably increase the costs of health care and may be unsafe or even harmful in some subgroups, particularly in septic patients, we conclude that routine administration of immune-nutrients (glutamine, arginine, omega-3 fatty acids, sele-nium, etc.) cannot be currently recommended in the critically ill.(Cite this article as: annetta Mg, Pittiruti M, vecchiarelli P, silvestri D, caricato a, antonelli a. immunonutrients in criti-cally ill patients: an analysis of the most recent literature. Minerva anestesiol 2016;82:320-31)Key words: critical illness - arginine - glutamine - selenium - Fatty acids, omega-3 - antioxidants.
Minerva anestesiologica 2016 March;82(3):320-31© 2015 eDiZioni Minerva MeDicathe online version of this article is located at http://www.minervamedica.it
comment in p. 262

iMMUnonUtrients in criticallY ill Patients annetta
vol. 82 - no. 3 Minerva anestesiologica 321
have been canceled or downgraded in the most recent guidelines, such as the 2013 surviving sepsis campaign (ssc) guidelines 11 and the 2013 canadian clinical Practice (ccP) guide-lines 12, 13 (table ii).
Obviously, there is an actual difficulty in de-signing and carrying out good quality clinical trials in critically ill patients, due to the hetero-geneity of the population (sepsis, septic shock, trauma, emergency surgery, burns, etc.), the dif-
cent multicenter trials 7-9 have shown no benefit or even some negative effect (table i).
there is no consensus about the overall ef-ficacy of immunonutrients in the critically ill, not even in the international guidelines. con-sidering the positive results of the first clinical studies, the guidelines developed before 2010 — such as the 2009 guidelines of the ameri-can society of Parenteral and enteral nutrition (asPen) 10 — contain recommendations that
Table I.—�Results of the most recent multicenter studies on immunonutrients in ICU patients.signet study 20 reDoX study 8 MetaPlUs study 9
Year of publication 2011 2013 2014type of study rct Double blind rct rctPatients 502 icU pts 1223 icU pts
(mechanically ventilated, multiple organ dysfunction)
301 icU pts(mechanically ventilated)
route Parenteral Parenteral + enteral enteralimmunonutrients glutamine, selenium glutamine, antioxidants glutamine, omega-3 Fa,
antioxidantseffects of immunonutrients on mortality no effect increased mortality
(glutamine)increased 6-month mortality in medical icU pts (P=0.04)
effects on infection no effect increased urinary tract infections (antioxidants)
(P=0.02)
no effect
effects on los no effect no effect no effect
Table II.—�Recommendations on immunonutrition according to the international guidelines.guidelines statement strength
2006 esPen guidelines 19 glutamine should be added to standard enteral formula in burned patients and in trauma patients
grade a
id. There are not sufficient data to support glutamine supplementation in surgical or heterogeneous critically ill patients
2009 asPen guidelines 10 immune-modulating enteral formulations (supplemented with agents such as arginine, glutamine, nucleic acid, ω-3 fatty acids, and antioxidants) should be used for the appropriate patient population (major elective surgery, trauma, burns, head and neck cancer, and critically ill patients on mechanical ventilation), with caution in patients with severe sepsis
grade a(surgical icU pts)
grade B(medical icU pts)
2009 esPen guidelines 18 Fish oil enriched lipid emulsions probably decrease length of stay in critically ill patients
grade B
2009 ccP guidelines 12 We recommend the use of an enteral formula with fish oils, borage oils and antioxidants in patients with acute lung injury (ali) and acute respiratory Distress syndrome (arDs)
2013 ccP guidelines 13 When Pn is prescribed to critically ill patients, parenteral supplementation with glutamine should be considered. However, we strongly recommend that glutamine NOT be used in critically ill patients with shock and multi-organ failure. There are insufficient data to generate recommendations for iv glutamine in critically ill patients receiving en
id. The use of an enteral formula with fish oils, borage oils and antioxidants in patients with ali and arDs should be considered
id. Based on 4 level 1 studies and 22 level 2 studies, we do not recommend diets supplemented with arginine and other select nutrients be used for critically ill patients
2013 ssc guidelines 11 We suggest using nutrition with no specific immunomodulating supplementa-tion in patients with severe sepsis
grade 2c

annetta iMMUnonUtrients in criticallY ill Patients
322 Minerva anestesiologica March 2016
nutrition. When glutamine was given by the enteral route, the results were much less con-clusive.10, 18
on the basis of this early series of studies, the 2006 guidelines of the european soci-ety of Parenteral and enteral nutrition (es-Pen) 19 and the 2009 asPen guidelines 10 recommended glutamine supplementation in icU patients, particularly in trauma, burns and elective surgery (table ii).
More recently, the results of several large clinical trials have changed the scene and questioned the effectiveness and safety of glu-tamine.
in 2011, a large european 10-center trial (the scottish intensive care glutamine or sele-nium evaluative trial — signet) evaluated the incidence of infection and mortality in icU patients receiving parenteral nutrition supple-mented with glutamine, selenium or both.20 no difference was reported in terms of infections, mortality, length of stay, days of antibiotic us-age, either giving glutamine alone or in combi-nation with selenium (table i).
in 2013, a large multicenter, placebo-con-trolled, double blind trial (reDoX trial) compared the effects of glutamine and antioxi-dants (selenium).8 glutamine was not associ-ated with any clinical benefit; on the contrary, in the study group there was a non-significant increase of 28-day mortality, plus a significant increase of in-hospital mortality and 6-month mortality (table i). a post hoc analysis by the same authors 21 confirmed these results, con-cluding that both glutamine and antioxidants may be harmful in patients with multiple organ failure.
the more recent MetaPlus study was a randomized multicenter trial conducted in 14 icUs in europe and published in 2014.9 there was no statistically significant difference in terms of infection, duration of mechanical ven-tilation, icU or hospital length of stay, but glu-tamine supplementation was associated with a higher mortality.
Most of the previous studies showing some benefits of glutamine supplementation were single-center studies involving small popula-tions of patients. also, much of the positive
ferences in age and nutritional status, the variety of commercial preparations, the different routes and modalities of delivery, the unpredictable gastro-intestinal tolerance and so on.
though, to use or not to use immunonutri-tion may have a relevant impact on the cost of health care, as many of these formulas are much more expensive than standard nutrition; the limited economic resources and the overall rising cost of healthcare impose an evidence-based approach in our daily medical practice, so to avoid waste of funds. at the same time, the safety of the patient — a goal far more im-portant than cost-containment — may be sig-nificantly affected, for better or for worse, by the adoption of such products.
in this review, our intent was to examine the literature on immunonutrition in the critically ill, with special focus on the most recent meta-analyses, so to define its margins of safety and effectiveness.
Glutamine
glutamine is the primary metabolic fuel for many rapidly proliferating cells such as enterocytes and immune cells. it has antioxi-dant effects, maintains the gut barrier function, yields energy to lymphocytes and neutrophils and stimulates the nucleotide synthesis.14
the rationale of the studies on glutamine supplementation is based on the observation that glutamine is generally depleted in critically ill patients. Plasma glutamine concentration at ad-mission to intensive care unit (icU) is an inde-pendent predictor of unfavorable outcome. very low or very high levels of plasma glutamine at 24 hours after icU admission are associated with an increased 6-month mortality.15 it has been re-cently speculated that the low plasma glutamine level in the acute phase of critical illness may be part of the adaptive response to stress.16
the older studies on glutamine supplemen-tation were mostly single-center studies with small numbers of patients on parenteral nutri-tion.17 results from these studies were encour-aging in terms of outcome benefits, so that the meta-analyses including these studies recom-mended the use of glutamine during parenteral

iMMUnonUtrients in criticallY ill Patients annetta
vol. 82 - no. 3 Minerva anestesiologica 323
ever, analyzing the role of multi-center versus single-center trial bias on outcome, only the single-center trials demonstrated a significant effect of parenteral glutamine on overall mor-tality and on infection.
that same year, a cochrane meta-analysis 25 reviewed the effects of glutamine supplemen-tation on infection rate and mortality in criti-cally ill adults and in adults after major sur-gery. this review found “moderate” evidence that glutamine supplementation reduced the infection rate and the number of days on me-chanical ventilation, plus “low quality” evi-dence that glutamine supplementation reduced length of hospital stay in critically ill or surgi-cal patients. there was no effect on mortality and length of icU stay.
in another recent meta-analysis,26 hospital mortality and six-month mortality were not different between study and control group. there was no difference between patients re-ceiving enteral or parenteral glutamine. in the subgroup given high dose glutamine (above 0.5 g/kg/day), mortality rate was significantly higher then in the control group (P=0.03). in the glutamine group, the infection rate was significantly lower than in the control group (P=0.02), particularly in surgical icU patients (P=0.04). Parenteral glutamine was also as-sociated with a significant reduction of noso-
evidence was based on studies in surgical pa-tients on parenteral nutrition supplemented with glutamine.
the meta-analyses conducted in the last two years (2013-2014) yielded results that are quite different if compared to older meta-analyses; still, conclusions have been somehow incon-sistent (table iii).
in 2013 Bollhalder conducted a meta-analy-sis on the effects of parenteral glutamine sup-plementation.22 Although a significant reduc-tion in infectious complications and in hospital length of stay was observed, there was no ef-fect on overall mortality.
Using a meta-regression analysis, Fadda et al. analyzed the same studies included by Bollhalder’s meta-analysis with the same endpoints (short-term mortality defined as in-hospital mortality) but considering a temporal trend.23 their analysis showed that the trials carried out before the year 2003 reported a better short-term survival, while this benefit tended to be small or even absent in the trials conducted after the 2003.
in a systematic review published in 2014, Wischmeyer 24 found a non-significant reduc-tion of overall mortality, infectious compli-cations and length of stay in icU, but a sig-nificant reduction of hospital mortality and hospital length of stay (los) (table iii). How-
Table III.—�Effects of glutamine supplementation on major clinical endpoints in ICU pts: results from the most recent meta-analyses.
Meta-analysis Mortality infections icU days Hospital days
Bollhalder 2013 22
40 rct 3107 pts (21 on surgical pts 11 on icU pts)
no(P=0.145)
reduced(P=0.009)
reduced(P=0.001)
Wischmeyer 2014 24
26 rct 2482 icU pts
no(P=0.10)
no(P=0.09)
no(P=0.09)
reduced (?)(P=0.02)
(only in single-centre trials)cochrane 2014 25
53 studies 4671 pts (both surgical and icU pts)
no(P=0.10)
reduced(P=0.00001)
no reduced (?)(low quality evidence)
chen 2014 26
18 trials 3383 icU pts
no(P=0.87)
reduced(P=0.02)
no(P=0.24)
Maratea 2014 27
23 trials 3344 icU pts
no

annetta iMMUnonUtrients in criticallY ill Patients
324 Minerva anestesiologica March 2016
lished in 2011,7, 30, 31 there was a revision of the literature about the role of omega-3 in critical-ly ill, and the most recent guidelines — such as the 2013 ccP guidelines — downgraded their recommendations (table ii).
in a systematic review, Manzanares et al.32 evaluated the effects of omega-3-based lipid emulsion vs. soybean oil (rich in omega-6 Fa) on clinical outcome. no effect was detected on mortality, duration in ventilation, or icU length of stay. the same authors published an-other meta-analysis on omega-3 during enteral or parenteral nutrition.33 again, no statistically significant difference were found on mortality, duration of mechanical ventilation, infection, or length of stay in icU.
that same year, in 2013, a new meta-analy-sis investigated the role of omega-3 Fa in par-enteral nutrition.34 no difference was found in mortality or infection. A significant reduction in hospital stay was found, but such result was strongly influenced by one single small study. the conclusion was that although omega-3 Fa may reduce hospital stay, no recommendation could be issued, considering the poor quality of the evidence.
the effects of omega-3 Fa were investigated by chen et al.35 No significant effect on overall mortality was found. Parenteral omega-3 Fa had no effect on mortality (P=0.15), while en-teral supplementation — after exclusion of the oMega trial,7 that was identified as source of heterogeneity – significantly reduced mortality (P=0.007). the main limitation of this analysis was the limited sample size of the trials. the heterogeneity of the population and the differ-ent route of supplementation were other major biases.
in another recent meta-analysis, Zhu et al. investigated the effect of enteral omega-3 Fa.36 the author’s conclusion was that in pa-tients with arDs, enteral supplementation of omega-3 Fa was ineffective in terms of 28-day mortality, ventilation-free days, and icU-free days.
very recently, santacruz Herrera et al. (37) published another meta-analysis on arDs. a reduction of mortality was found only in stud-ies in which omega-3 Fa had been compared
comial infections (P=0.03). the length of hospital stay was not affected by glutamine supplementation.
a trial-sequential analysis tried to synthesize the results of the randomized studies focused on glutamine supplementation in critically ill patients.27 this trial re-examined the trials of the Bollhalder meta-analysis plus the reDoX trial. the endpoint was mortality. the author’s conclusion was that glutamine in critical ill-ness is ineffective and may even be toxic.
In conclusion, the potential benefits of glu-tamine supplementation, most specifically on the incidence of infection, appear to be associ-ated with the supplementation of this aminoac-id by the parenteral route in surgical patients. there is little or no evidence that glutamine may be of any benefit in ICU patients, while there is some recent evidence that it may be harmful, particularly if given enterally and/or at a high dosage.
table iii summarizes the results of the meta-analyses discussed above.
Omega-3 fatty acids
omega-3 fatty acids (Fa) are poly-unsatu-rated fatty acids with a double bound between the third and the fourth carbon. as mammals cannot synthesize the carbon-carbon double bonds, these compounds are essential to the diet. omega-6 Fa promote the synthesis of prostaglandin E2 and leukotriene B4, which are highly pro-inflammatory, while omega-3 FA promote the synthesis of less inflamma-tory eicosanoids such as prostaglandin e3 and leukotriene B5 and decrease the release of pro-inflammatory cytokines IL-1 and TNF-alpha.28, 29
a popular hypothesis is that these com-pounds may improve the clinical outcomes of critically ill patients, reducing the inflammato-ry response. Many clinical trials based on this hypothesis have been made in the last 20 years. as the results of these studies were promising, in 2006-2009 most guidelines – asPen, es-Pen, ccP — recommended enteral formula containing omega-3 Fa (table ii).
after a few important clinical trials pub-

iMMUnonUtrients in criticallY ill Patients annetta
vol. 82 - no. 3 Minerva anestesiologica 325
tation may reverse the immune-compromised status.42 Plasma levels of arginine during sep-sis have been measured, with contrasting re-sults, depending at which stage of the disease they were measured.43 Arginine deficiency is most likely to be a feature of the earlier stages of sepsis, while plasma levels of arginine in-crease progressively as the septic state wors-ens. thus, the more severe is the sepsis, the less likely is that arginine supplementation may benefit: on the contrary, it may even do harm.
in 2001, Heyland et al. published a meta-analysis on arginine supplementation in icU patients showing evidence of adverse effects.44 Provision of supplemental arginine in severe sepsis could promote the synthesis of large quantities of no that may cause hypotension, cardiac insufficiency, increased tissue and en-dothelial permeability and organ failure.45 to counteract vasodilation and hypotension in patients with septic shock, administration of a nonselective nitric oxide synthase inhibitor (546c88) was tested by lopez et al.,46 but their trial was stopped early after review by the in-dependent data safety monitoring board, since the day-28 mortality was 59% in the treated group vs. 49% in the placebo group (P<0.001).
arginine supplementation in critically ill patients increases no production amplifying
to a high-fat control solution (P=0.001), while trials using a low-fat control group showed a non-significant increase in mortality. The benefits observed in the trials where the high-fat formulas were used is probably due to the presence of a high quantity of omega-6 Fa in the control group. the content of fat in this control group (55% of energy) was far beyond what is currently recommended in clinical practice.10, 18, 19
in conclusion, there is no convincing evi-dence that omega-3 Fa supplementation may have any role in parenteral or enteral nutrition of the critically ill, not even in arDs patients.
table iv shows the main results of the meta-analyses quoted in the text.
Arginine
arginine is a semi essential aminoacid syn-thesized and its metabolism occurs via mul-tiple pathways that produce nitric oxide (no), polyamines, proline, glutamate, creatine, and agmatine.38 the route of glutamine adminis-tration may influence its metabolism.39-41 ex-perimental data indicate that arginine improves immune function, while its deficiency impairs immune response and thus may increase the risk of nosocomial infections.
it was postulated that arginine supplemen-
Table IV.—�Effects of omega-3 FA supplementation on major clinical endpoints in ICU pts: results from the most recent meta-analyses.
Meta-analysis Mortality infections ventilation days icU days Hospital days
Manzanares 2013 32
12 rct 806 pts
n.(P=0.20)
n.(p=0.35)
n.(P=0.09)
n.(P=0.13)
Manzanares 2014 33
6 rct 390 pts
no(P=0.08)
no(P=0.35)
no(P=0.17)
no(P=0.84)
Palmer 2013 34
8 studies 391 pts
no(P=0.32)
no(P=0.41)
no(p=0.80)
reduced (?)(low quality evidence)
chen 2014 35
12 trials 1208 pts
no(P=0.18)
Zhu 2014 36
7 studies 955 pts
no(P=0.44)
no(P=0.36)
no(P=0.33)
santacruz 2015 37
7 studies 802 arDs pts
no(p=0.37)
no small reduction

annetta iMMUnonUtrients in criticallY ill Patients
326 Minerva anestesiologica March 2016
zation recommends a daily intake of 70 µg/day signaling a risk of toxicity at 900 µg/day.54 there is much controversy regarding the op-timal dosage, the route of administration, the duration of the treatment and the potentially toxic levels.55 the 2009 asPen guidelines 10 included antioxidants in the list of immuno-nutrients to be used in both surgical icU and medical icU patients, “with caution in patients with severe sepsis”.
in 2012, a meta-analysis analyzed all ran-domized clinical trials (rct) about the effects of micronutrients as pharmaceutical agents (both vitamins and trace elements) on clinical outcome in critically ill patients.56 antioxi-dants were associated with a significant reduc-tion of mortality and duration of mechanical ventilation, a non-significant reduction in in-fections and no overall effect on icU or hos-pital los. the reduction of mortality was sig-nificantly greater in the subgroup of patients with higher risk of death (10% mortality in control group) (P=0.003) whereas there was no significant effect observed for trials of pa-tients with lower mortality risk. Trials using a dose of more than 500 µg/day showed a trend towards a lower mortality (P=0.07). Parenter-al administration of selenium was associated with a trend towards a reduction in mortal-ity and infections, but enteral administration could not be analyzed, because only 1 rct re-ported the effects of enteral selenium on clini-cal outcome.56 in conclusion, the results of this meta-analysis showed a significant reduction in mortality with high dose of parenteral se-lenium in particular in patients with high risk of death. though, this meta-analysis did not include the most recent and largest rcts on pharmaconutrition: the reDoX trial and the MetaPlus trial (table i).8, 9
in the reDoX trial the patients received an
the systemic inflammatory response syndrome and increasing mortality.47
the 2006-2009 guidelines from esPen and asPen, as already quoted above, recom-mended the use of an enteral formula contain-ing arginine in some populations of patients, with the exception of severe sepsis (table ii).
an updated analysis of literature from the canadian group in 2013 12, 13 recommended to avoid arginine supplementation in all icU pa-tients, thus confirming an earlier meta-analysis by Marik and Zaloga.48 Both meta-analyses found no effects on mortality, infection, hospi-tal length of stay, or icU stay (table v). given the possible harm in septic patients 47 and the increased cost, the committee recommended against the use of arginine in critically ill pa-tients.
Antioxidants
the antioxidant endogenous defense system in humans consists of a variety of molecules (mostly, trace elements such as copper, man-ganese, zinc, iron and selenium) that protect tissues from injury induced by reactive oxygen species and reactive nitrogen species. in icU patients, plasma level of these microelements may be often reduced, because of interstitial leakage from capillary endothelium, insuffi-cient oral intake, and/or loss during continu-ous renal replacement therapy.49, 50 selenium serum levels have been correlated to immuno-globulin levels, neutrophil and macrophages function, defense against oxidative damage and regulation of thyroid hormones.51-53
the studies evaluating the role of selenium have been characterized by a huge heteroge-neity of methods. some clinical studies have tested selenium “megadoses”, typically around 1000 µg/day, while the World Health Organi-
Table V.—�Effects of arginine supplementation on major clinical endpoints in ICU pts: results from the most recent meta-analyses.
Meta-analysis Mortality infections icU days Hospital days
Marik 2008 48
24 studies (3013 pts)no no no no
ccP group 2013 12, 13
24 studies (2666 pts)no
(P=0.40)no
(P=0.88)no
(P=0.37)no
(P=0.42)

iMMUnonUtrients in criticallY ill Patients annetta
vol. 82 - no. 3 Minerva anestesiologica 327
supplemented with immunonutrients showed a higher 6-month mortality (P=0.04).
in a meta-analysis published in 2013, alhaz-zani analyzed the effect of selenium in septic patients.61 the analysis showed that intrave-nous selenium supplementation at doses ≥100 µg/day in comparison to placebo was associ-ated with lower mortality. though, there was no difference in icU length of stay or in noso-comial pneumonia. The significant heteroge-neity among trials reporting adverse events precluded an adequate pooling of results.
that same year, a similar meta-analysis on selenium in sepsis 62 concluded that parenteral selenium supplementation for at least 7 days (P=0.01), with a pre-loading bolus (P=0.01) and at high-dosage (P=0.04) might be associ-ated with a lower mortality risk.
More recently, a further meta-analysis by landucci et al. showed that selenium supple-mentation was associated with a reduction in 28-day mortality of borderline statistical sig-nificance (P=0.04) but the estimate was very imprecise.63 the results of this meta-analysis showed a reduction of 28-day mortality, with no effect on 6-month mortality regardless of the dose, the bolus and the length of supple-mentation.
in conclusion, while some meta-analyses have found a favorable effect of selenium on mortality (Table VI), data are difficult to in-terpret. therefore, this precludes to provide evidence-based recommendations for supple-mentation of antioxidants in the critically ill.
antioxidant cocktail via enteral route including vitamin c, vitamin e, beta-carotene, zinc and selenium (300 µg) and high dose of sodium selenite (total selenite dose of 800 µg). There was no effect on clinical outcome. though, the incidence of urinary tract infections was significantly higher among the supplemented patients (P=0.02); the same was noted for deep surgical wound infection (P=0.07). in their post hoc analysis, Heyland et al. found that both glutamine and antioxidant appeared particularly harmful in patients with renal dys-function.21
these unexpected results were explained in various ways. the phase of the critical illness might have been too advanced, already evolved toward two or more organ failures, when the supplementation was initiated. also, the dos-age of selenium was too high if compared to the recommended doses.54, 57-59 Finally, when given as a cocktail with other nutrients and vi-tamins, the bioavailability of enteral selenium may be unpredictable. in fact, it has been prov-en that the enteral administration of selenium with ascorbic acid can reduce the availability of selenium to almost zero levels.60
the MetaPlus study 9 was a double-blind, multicenter study (table i). glutamine, ome-ga-3 Fa and various antioxidants (vitamin c, zinc, vitamin e and selenium) were given to the study group. No significant difference in the incidence of infection or in any other clini-cal outcomes was found between the control group and the study group. Medical patients
Table VI.—�Effects of antioxidants supplementation on major clinical endpoints in ICU pts: results from the most recent meta-analyses.
Meta-analysis Mortality infections ventilation days icU days Hospital days
Manzanares 2012 56
21 studies 2531 pts
reduced(P=0.002)
no(P=0.08)
reduced(P=0.02)
no(P=0.38)
no(P=0.73)
alhazani 2013 61
9 studies 792 pts
reduced(P=0.03)
no(P=0.74)
no(P=0.12)
Huang 2013 62
9 studies 965 pts
reduced(P=0.04)
landucci 2014 63
9 studies 921 pts
reduced (?)(low quality evidence)
no(P=0.67)
no(P=0.09)

annetta iMMUnonUtrients in criticallY ill Patients
328 Minerva anestesiologica March 2016
in contrast, critical illness is associated with a more intense ad more complex systemic in-flammatory response, secondary to an excess of nitric oxide, reactive oxygen species and proinflammatory mediators. In this pathophys-iologic condition, nutrients that further stimu-late the inflammatory process, as arginine, may be deleterious. Furthermore, in the same critically ill patient a hyper-inflammation state may coexist with a depression of cellular im-mune response, making the effects of immune-nutrients even more unpredictable.
another problem is that in most studies multiple nutrients were combined into single nutritional products. so, interaction between nutrients may influence their mechanisms of action, lifespan and effects on target organs. it is possible that some nutrients, tested indi-vidually, may have some positive or negative effects in some groups of patients, but - when combined together or administered to hetero-geneous group of patients - may have an oppo-site effect. one more area of uncertainty is the optimal dose of each nutrient, which is mostly undetermined. Dose-finding studies in nutri-tion literature are very rare. the reDoX trial results demonstrated that too high doses of glutamine and selenium might be dangerous. However, the route of administration may in-fluence the availability of nutrients plasma lev-els. enteral absorption may be altered in criti-cally ill patients, so that the intake of nutrients is unpredictable. the relevance of an initial loading bolus before the continuous infusion and the timing of supplementation are another unknown area: pharmacokinetic studies of im-munonutrients are few and inconclusive.
Conclusions
Modulation of inflammatory and immune response to critical illness has been the goal of much research in sepsis, arDs, trauma and burn. a variety of drugs and nutrients have been tested in experimental models with prom-ising results. though, in the clinical setting of ICU patients, no consistent efficacy has been demonstrated yet, most likely because the ef-fects of the various immunonutrients may vary
the ssc guidelines suggest to avoid selenium in severe sepsis 11 and the ccP guidelines state that the use of trace elements “should be con-sidered” in critically ill patients.12, 13
Discussion
Modulation of the immune response in the setting of critical illness has been the goal of much research in the last two decades. Many experimental and clinical trials have investi-gated different nutrients with theoretical im-muno-enhancing properties, hoping that they might improve the patient’s clinical outcome. the results of these trials are controversial, and so are the conclusions of the meta-anal-yses, with the noteworthy feature that the old-est and smallest studies show more evidence of favorable effect than the latest and largest ones. after 20 years of clinical studies and countless millions of research funds, no defini-tive positive treatment effect of immunonutri-ents has been proven in critically ill patients. Many have argued that there are significant methodological limitations in the existing lit-erature that may limit the interpretation of the studies. Generally speaking, the oldest trials are too small (<100 patients) and have a poor randomization quality. the patient’s popula-tion differs enormously in terms of age, stage of illness, etc., between studies and even in-side the same study. the degree of systemic inflammation and the balance of inflamma-tion/anti-inflammation activity, as well as the regional and systemic generation of reactive oxygen species, are unknown variables which may vary significantly between patients and in the same patient, explaining the spectrum of different effects of immunonutrients — from beneficial to harmful — in postsurgical pa-tients vs. critically ill patients and in different clinical subgroups. surgical trauma may be as-sociated with a limited activation of systemic inflammation but with a relevant suppression of cellular defense function, which increases the risk of infection. In this setting, arginine and other immune-enhancing substances may restore the competence of the cellular defense system and reduce infectious complications.

iMMUnonUtrients in criticallY ill Patients annetta
vol. 82 - no. 3 Minerva anestesiologica 329
quiring intensive care: a meta-analysis of randomized tri-als. injury 2011;42:50-6.
3. Ekpe K, Novara A, Mainardi JL, Fagon JY, Faisy C. Methicillin-resistant staphylococcus aureus bloodstream infections are associated with a higher energy deficit than other icU-acquired bacteremia. intensive care Med 2014;40:1878-87.
4. Drover JW, Dhaliwal R, Weitzel L, Wischmeyer PE, Ochoa JB, Heyland D: Perioperative use of arginine-sup-plemented diets: a Systematic review of the evidence. J am coll surg 2011;212:385-99.
5. Braga M, gianotti l:Perioperative immunonutrition: cost-benefit analysis. JPEN 2005;29(Suppl):S57-S61.
6. Braga M, Wischmeyer PE, Drover JW, Heyland DK:Clinical evidence for pharmaconutrition in major elective surgery. JPEN 2013;37(Suppl):S66-S72.
7. rice t, Wheeler aP, thompson Bt, deBoisblanc BP, Steingrub J, Pock P:Enteral omega-3 fatty acid, linolenic acid and antioxidant supplementation in acute lung in-jury. JAMA 2011;306:1574-81.
8. Heyland D, Muscedere J, Wischmeyer PE, Cook D, Jones G, Albert M, et al. a randomized trial of glutamine and antioxidants in critically ill patients. N Engl J Med 2013;368:1489-97.
9. Van Zanten AH, Sztark F, Kaisers UX, Zielmann S, Fel-binger TW, Sablotzki AR, et al. High-protein enteral nutrition enriched with immune-modulating nutrients vs standard high-protein enteral nutrition and nosocomial infections in the ICU: a randomized clinical trial. JAMA 2014;312:514-24.
10. McClave SA, Martindale RG, Vanek VW, McCarthy M, roberts P, taylor B, et al. guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient:society of critical care Medicine (sccM) and american society for Parenteral and en-teral Nutrition (ASPEN). JPEN J Parenter Enteral Nutr 2009;33:277-316.
11. Dellinger rP, levy MM, rhodes a, annane D, gerlach H, opal sM, et al. surviving sepsis campaign:international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39:165-228.
12. critical care nutrition. canadian clinical practice guide-lines 2013 [internet]. available from: http://www.critical-carenutrition.com [cited 2016, Feb 18].
13. Dhaliwal R, Cahill N, Lemieux M, Heyland DK. The canadian critical care nutrition guidelines in 2013: an update on current recommendations and implementation strategies. nutr clin Pract 2014;29:29-43.
14. Wischmeyer Pe. glutamine: mode of action in critical illness. crit care Med 2007;35(suppl):s541-4.
15. Rodas PC, Rooyackers O, Hebert C, Norberg A, Werneman J. Glutamine and glutathione at ICU admission in relation to clinical outcome. clin sci 2012;122:591-7.
16. van den Berghe g. low glutamine levels during critical illness: adaptive or maladaptive? NEJM 2013;368:1549-50.
17. Griffiths RD, Jones C, Palmer TE. Six-month outcome of critically ill patients given glutamine-supplemented parenteral nutrition. nutrition 1997;13:295-302.
18. singer P, Berger MM, van den Berghe g, Biolo g, calder P, Forbes a, et al. esPen:esPen guidelines on parenter-al nutrition: intensive care. clin nutr 2009;28:387-400.
19. Kreymann KG, Berger MM, Deutz NE, Hiesmayr M, Jolliet P, Kazandjiev G, et al. DgeM (german soci-ety for nutritonal Medicine), esPen (european soci-ety for Parenteral and enteral nutrition). esPen guide-lines on enteral nutrition: intensive care. clin nutrition 2006;25:210-23.
20. Andrews PJD, Avenell A, Noble DW, Campbell MK, croal Bl, simpson Wg, et al. randomized trial of glutamine, selenium, or both, to supplement parenteral
in relation to the timing, the dose, the route of administration, the interaction with other nu-trients, the severity of illness and many other factors.
While the current literature shows no con-vincing evidence that immunonutrients may be beneficial in the critically ill, these substances invariably increase the costs of health care and may be unsafe or even harmful in some sub-groups, particularly in septic patients. thus, in terms of safety and cost-effectiveness, the ad-ministration of immune-nutrients (glutamine, arginine, omega-3 Fas, selenium, etc.) cannot be currently recommended in the critically ill.
Key messages
— immunonutrients (mainly: gluta-mine, omega-3 fatty acids, arginine, sele-nium) are pharmacologically active nutri-ents that may theoretically modulate the metabolic and inflammatory response to surgery and stress and/or enhance immune function.
— The clinical benefit of these sub-stances in the critically ill has been sug-gested by single-center trials and low qual-ity studies carried out at the beginning of this century (2000-2009), but has not been confirmed by the latest evidence-based documents (multicenter trials, systematic reviews, meta-analyses and international guidelines) on this subject.
— considering that immunonutrients increase the costs of health care and may be unsafe or even harmful in some subgroups, particularly in septic patients, their routine administration cannot be currently recom-mended in the critically ill.
References
1. Alberda C, Gramlich L, Jones N, Jeejeeboy K, Day AG, Dhaliwal r, et al. the relationship between nutritional intake and clinical outcomes in critically ill patients: re-sults of an international multicenter observational study. intensive care Med 2009;35:1728-37.
2. Doig gs, Heighes Pt, simpson F, sweetman ea. early enteral nutrition reduces mortality in trauma patients re-

annetta iMMUnonUtrients in criticallY ill Patients
330 Minerva anestesiologica March 2016
38. Wu G, Bazer FW, Davis TA, Kim SW, Li P, Rhodas JM, et al. arginine metabolism and nutrition in growth, health and disease. amino acids 2009;37:153-68.
39. Wu G, Bazer FW, Cudd TA, Jobgen WS, Kim SW, Las-sala a, et al. Pharmacokinetics and safety of arginine supplementation in animals. J Nutr 2007;137:S1673-80.
40. ligthart-Melis gc, van de Poll Mcg, Boelens Pg, De-jong cHc, Deutz neP, van leeuwen PaM. glutamine is an important precursor for the novo synthesis of arginine in humans. Am J Clin Nutr 2008;87:1282-9.
41. ligthart-Melis gc, van de Poll Mc, Dejong cH, Boelens Pg, Deutz ne, van leeuwen Pa, et al. the route of ad-ministration (enteral or parenteral) affects the conversion of isotopically labeled l-(2-15n)glutamine into citrulline and arginine in humans. JPEN J Parenter Enteral Nutr 2007;31:343-50.
42. Mizock BA. Immunonutrition and critial illness: an up-date. nutrition 2010;26:701-7.
43. Chiarla C, Giovannini I, Siegel JH. Plasma arginine cor-Plasma arginine cor-relations in trauma and sepsis. amino acids 2006;30:81-6.
44. Heyland DK, Novak F. immunonutrition in the critically ill patient: more harm than good? JPEN J Parenter En-teral nutr 2001;25(suppl):s51-6.
45. Hibbs JB. Infection and nitric oxide. J Infect Dis 2002;185(suppl 1):s9-17.
46. Lopez A, Lorente JA, Steingrub J, Bakker J, McLuckie a, Willatts s, et al. Multiple-center, randomized, placebo controlled, double-blind study of the nitric oxide syn-thase inhibitor 546c88:effect on survival in patients with septic shock. Crit Care Med 2004;32:21-30.
47. Heyland DK, Samis A. Does immunonutrition in patients with sepsis do more harm than good? intensive care Med 2003;29:667-71.
48. Marik PE, Zaloga GP. Immunonutrition in critically ill patients:a systematic review and analysis of literature. intensive care Med 2008;11:1980-90.
49. Motoyama T, Okamoto K, Kukita I, Hamaguchi M, Ki-noshita Y, ogawa H. Possible role of increased oxidant stress in multiple organ failure after systemic inflamma-tory response syndrome. crit care Med 2003;31:1048-52.
50. Berger MM, chiolero r. antioxidant supplementation in sepsis and systemic inflammatory response syndrome. crit care Med 2001;35:s584-90.
51. Arther JR, McKenzie RC, Backett GJ. Selenium in the immune system. J Nutr 2003;133:14575-95.
52. lowes Da, galley HF. Mitochondrial protection by the thioredoxin-2 and glutathione systems in an in vitro en-dothelial model of sepsis. Biochem J 2011;436:123-32.
53. Berger MM, Reymond MJ, Shenkin A, Rey F, Wardle C, cayeux c, et al. Influence of selenium supplements on the post-traumatic alterations of the thyroid axis:a place-bo controlled trial. intensive care Med 2001;27:91-100.
54. World Health organization (WHo):selenium, enviro-mental Health criteria 58. geneva, switzerland: WHo; 1987.
55. Pierre JF, Heneghan AF, Lawson CM, Wischmeyer PE, Kozar RA, Kudsk KA. Pharmaconutrition review: physiological mechanisms. JPEN J Parenter Enteral Nutr 2013;37:s51-65.
56. Manzanares W, Dhaliwal R, Jiang X, Murch L, Hey-land D. antioxidant micronutrients in the critically ill:a systematic review and meta-analysis. critical care 2012;16:r66.
57. Sriram K, Lonchyna VA. Micronutrient supplementation in adult nutrition therapy: practical considerations. JPEN J Parenter Enteral Nutr 2009;33:548-62.
58. Shenkin A. Selenium in intravenous nutrition. Gastroen-terology 2009;137:s61-9.
59. angstwurm MWa, gaertner r. Practicalities of selenium
nutrition for critically ill patients. BMJ 2011;342:1542-50.
21. Heyland DK, Elke G, Cook D, Berger MM, Wische-myer Pe, albert M, et al. on behalf of the canadian critical care trails group. glutamine and antioxidants in the critically ill patient:a post-hoc analysis of a large-scale randomized trial. JPEN J Parenter Enteral Nutr 2015;39:401-9.
22. Bollhalder L, Pfeil AM, Tomonaga Y, Schwenkglenks M. a systematic literature review and meta-analysis of randomized clinical trials of parenteral glutamine supple-mentation. clin nutr 2013;32:213-23.
23. Fadda v, Maratea D, trippoli s, Messori a. temporal trend of short-term mortality in severely ill patients re-ceiving parenteral glutamine supplementation. clin nutr 2013;32:492-3.
24. Wischmeyer Pe, Dhaliwal r, Mccall M, Ziegler tr, Heyland D. Parenteral glutamine supplementation in crit-ical illness:a systematic review. crit care 2014;18:r76.
25. Tao KM, Li XQ, Yang LQ, Yu WF, Lu ZJ, Sun YM, et al. glutamine supplementation for critically adults (review). cochrane 2014;9.
26. Chen QH, Yang Y, He HL, Xie JF, Cai SX, Liu AR, et al. the effect of glutamine therapy on outcomes in critically ill patients:a meta-analysis of randomized controlled tri-als. crit care 2014;18:r8.
27. Maratea D, Fadda v, trippoli s, Messori a. glutamine in critically ill patients: trial-sequential analysis. clin nutr 2014;33:735-6.
28. calder Pc. omega-3 polyunsaturated fatty acids and in-flammatory processes: nutrition or pharmacology? Br J clin Pharmacol 2013;75:645-62.
29. Calder PC.Rationale and use of n-3 fatty acids in artificial nutrition. Proc soc 2010;69:565-73.
30. grau carmona t, Moran garcia v, garcia de lorenzo a, Heras de la Calle G, Quesada Bellver B, Lopez-Martines J, et al. effect of an enteral diet enriched with eicosap-entaenoic acid, gamma-linolenic acid and anti-oxidant on the outcome of mechanically ventilated, critically ill, septic patients. clin nutr 2011;30:578-84.
31. Stapleton Rd, Martin TR, Weiss NS, Crowley JJ, Gundel SJ, Nathens AB, et al. a phase ii randomized placebo- controlled trial of omega-3 fatty acids for the treatment of acute lung injury. crit care Med 2011;39:1655-62.
32. Manzanares W, Dhaliwal R, Jurewitsch B, Stapleton RD, Jeejeebhoy KN, Heyland DK. Alternative lipid emulsions in the critically ill:a systematic review of the evidence. intensive care Med 2013;39:1683-94.
33. Manzanares W, Dhaliwal R, Jurewitsch B, Stapleton RD, Jeejeebhoy KN, Heyland DK. Parenteral fish oil in the critically ill:a systematic review and meta-analysis. JPEN J Parenter Enteral Nutr 2014;38:20-8.
34. Palmer AJ, Clement KM, Ajibola O, Avenell A. The role of omega-3 fatty acid supplemented parenteral nutrition in critical illness in adults:a systematic review and meta-analysis. crit care Med 2013;41:307-16.
35. Chen W, Jiang H, Zhou ZY, Tao YX, Cai B, Liu J, et al. is omega-3 fatty acids enriched nutrition support safe for critically ill patients? a systematic review and meta-anal-ysis. nutrients 2014;6:2148-64.
36. Zhu D, Zhang Y, li s, gan l, Feng H, nie W. enteral omega-3 fatty acid supplementation in adult patients with acute respiratory distress syndrome: a systematic review of randomized controller trials with meta-analysis and tri-al sequential analysis. intensive care Med 2014;40:504-12.
37. Santacruz CA, Orbegozo D, Vincent JL, Preiser JC. Modulation of dietary lipid composition during acute respiratory distress syndrome (arDs): a systematic re-view and meta-analysis. JPEN J Parenter Enteral Nutr 2015;39:837-46.

iMMUnonUtrients in criticallY ill Patients annetta
vol. 82 - no. 3 Minerva anestesiologica 331
view and meta-analysis of randomized controlled trials. crit care Med 2013;41:1555-64.
62. Huang ts, shyu Yc, chen HY, lin lM, lo cl, Yuan ss, et al. effect of parenteral selenium supplementation in critically ill patients:a systematic review and meta-analysis. Plos one 2013;8:e54431.
63. landucci F, Mancinelli P, De gaudio r, virgili g. seleni-seleni-um supplementation in critically ill patients:a systematic review and meta-analysis. J Critical Care 2014;29:150-6.
supplementation in critically ill patients. curr opin clin nutr Metab care 2006;9:233-8.
60. Robinson MF, Huemmer PK. Effect of a megadose of ascorbic acid, a meal and orange juice on the absorp-tion of selenium as sodium selenite. N Engl J Med 1985;98:627-9.
61. Alhazzani W, Jacobi J, Sindi A, Hartog C, Reinhart K, Kokkoris S, et al. the effect of selenium therapy on mor-tality in patients with sepsis syndrome:a systematic re-
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: May 13, 2015. - Manuscript accepted: May 8, 2015. - Manuscript revised: April 24, 2015. - Manuscript received: February 22, 2015.

332 Minerva anestesiologica March 2016
relative weights, and the wide range of predic-tors reflects the heterogeneity of the popula-tions studied and the different surgical settings and outcomes considered by the developers of scoring system s. In any case, deciding what clinical steps to take with confidence on the basis of a risk score remains a daunting prob-lem for health care planners and individual cli-nicians alike.
Proposing new predictive models
Understanding how risk is analyzed and models proposed and validated is clearly es-sential for developers of new clinical tools. However, it is also helpful for end users, the clinicians who manage patient comfort and safety and the planners who manage resources.
longer hospital stays and higher postop-erative morbidity and mortality are seri-
ous concerns for patients and hospital sys-tems alike, and the greatest contributors to the overall risk of these developments after surgery are cardiovascular and postoperative pulmonary complications (PPCs). The litera-ture on the most frequent and deleterious PPCs or on composites — combinations of several respiratory complications — that have been linked to mortality, hospital stay and costs was recently summarized.1 The annual reported economic burden attributable to respiratory complications alone in the United States ex-ceeds $3 billion (USD).2 However, the differ-ent mortality rates and effects on postoperative length of stay seem to suggest that PPCs have
R E V I E W
How to optimize and use predictive models for postoperative pulmonary complications
valentín MaZo 1, sergi saBatÉ 2, Jaume CANET 1 *
1Department of Anesthesiology, Hospital Universitari Germans Trias i Pujol, Badalona, Barcelona, Spain; 2 Department of Anesthesiology, Fundació Puigvert. Barcelona, Spain*Corresponding author: Jaume Canet, Department of Anesthesiology, Hospital Universitari Germans Trias i Pujol, Carretera del Canyet s/n. Badalona 08916 Barcelona, Spain. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva anestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: 10255-MAStitolo breve: OPTIMIZING PPCsprimo autore: MAZOpagine: 332-42citazione: Minerva Anestesiol 2016;82:332-42
a B s t r a c tPulmonary complications are a source of greater postoperative morbidity and mortality and longer hospital stays. Al-though many factors have been implicated as predictors, few models have been developed with the rigorous methodology required for clinically useful tools. In this article we attempt to describe what to look for when developing or assessing a newly proposed predictive tool and to discuss what must be taken into consideration on incorporating a model into clinical practice. Above all, we stress that we still lack evidence for the clinical and cost effectiveness of many measures proposed for reducing risk or for managing complications perioperatively. For a good predictive model to truly prove its utility in clinical decision-making, such evidence is required.(Cite this article as: Mazo V, Sabaté S, Canet J. How to optimize and use predictive models for postoperative pulmonary complications. Minerva Anestesiol 2016;82:332-42)Minerva Anestesiol 2016;82:332-42))Key words: Postoperative complications - Risk factors - Prevention and control - Lungs.
Minerva Anestesiologica 2016 March;82(3):332-42© 2016 EDIZIONI MINERVA MEDICAThe online version of this article is located at http://www.minervamedica.it
Comment in p. 265

OPTIMIZING PPCs MaZo
Vol. 82 - No. 3 Minerva anestesiologica 333
In deciding size, the score developer must bear in mind that the number of factors to test should not exceed a reasonable ratio (1/10) respect to the number of events observed. Fi-nally, a priori, it would be ideal to study co-horts prospectively because information that is more consistent with assumptions about candidate factors can be collected systemati-cally. However, in any case, existing databas-es of proven quality can be a good support for retrospective studies exploring potential new factors.
Identifying risk factors: the search for candidates and the statistical selection of relevant predictors
choosing candidate predictors involves looking at the universe of hypothetical risk factors before proposing a limited number to test. To that end, the modelers set selection criteria, which will be affected by their experi-ence and their beliefs about risk. A geneticist’s approach will differ from a public health plan-ner’s, and the perspectives of both will differ from that of a hospital clinician with specific responsibilities. The professional bias of anes-thesiologists regarding PPCs leads us to take an interest in variables assessed during the pre-operative visit. The preoperative assessment is a rich source of information about patient characteristics, lifestyle habits, and comorbid-ity that might confer risk, as well as relevant characteristics of the planned surgery. It there-fore seems logical to us that data collected at this time can be labeled candidate predictors of PPC risk, and for planning purposes, ear-lier prediction is of greater potential interest. Clearly, predictions could be even more accu-rate if also based on data collected in the op-erating room or related to specific events that occur there. However, the type of prediction based on events close to an unwanted outcome is very different from one made earlier in the planning process, at the time of preoperative assessment, allocation of resources or adop-tion of preoperative preventive measures.6 Fi-nally, prospective developers of a new clinical tool would be unwise to fail to consider fac-
Developing a new predictive model is meth-odologically complex. Care in designing risk analysis will keep a newly proposed risk score from becoming just one more among so many that seem to provide little or no new knowl-edge, to be of questionable practical utility. Before a research group undertakes a large prospective study involving thousands of pa-tients and many data collectors, it is important to know exactly why the models currently available seem deficient. If we conclude we can improve on those models, the complex tasks will be worthwhile. Otherwise, we may make a more clinically useful contribution by helping to validate preexisting tools and hone them for use in our own setting or other similar ones.
We acknowledge the relevance of the de-bate on whether a predictive or explanatory model 3 is wanted, but we will not enter into that discussion here as it involves consider-ations that are more theoretical than practical from the clinician’s point of view. Briefly, we note that causes cannot be inferred from obser-vational epidemiological studies of risk; only experimental studies can shed light on causes. However, it may be that some of the predic-tors selected by a model are counted as causes already demonstrated in the literature. In such cases, a model might well be explanatory in part, as the clinician intuits a cause-effect rela-tionship between the predictor selected by the model and the outcome.
Population to be studied and sample size
A model based on a relatively heteroge-neous sample of patients that reflects a consid-erable portion of the range of an anesthesiolo-gist’s routine practice has greater face validity to the clinician: in other words, it seems more worthwhile. Otherwise, conclusions based on a risk score for restricted populations would be applicable only to a limited number of pa-tients with the same peculiar characteristics of those in the development sample. In addition to the make-up of a sample, its size 4, 5 will be a particularly important aspect to consider when evaluating the applicability of a score.

MaZo OPTIMIZING PPCs
334 Minerva anestesiologica March 2016
restrict predictors is the very strong hope for a parsimonious model, associated with the precept that in the absence of certainty, make fewer assumptions — a principle known meta-phorically as Occam’s razor. We like to attenu-ate the application of the principle, however, and stress that in the words of Wears et al.,7 “Modelers could be usefully guided by an aphorism attributed to Albert Einstein: Things should be kept as simple as possible, but no simpler.” We argue that if the goal is a model that is clinically useful, the laudable principles of logic and scientific elegance might some-times need to be revisited. The desire for sim-plicity is based on the falsifiability criterion, under which simpler theories are preferable to more complex ones because they can be more easily tested. However, deliberately limiting the complexity of the model is not in the clini-cian’s interest when the problem is evidently complex. We therefore concur with Wears et al. — and indeed with their forerunners, Ein-stein and many less famous scientists — that models should be no simpler than they must be in order to be useful. If we step back from this philosophical approach and focus specifi-cally on the question of choosing the best pos-sible subset of predictor variables, we would have to agree with Harrell 8 and Steyerberg,9 who think that smaller models are also sought because they are easier to interpret and use in practice, especially if some of the possible ad-ditional variables will be difficult or costly to measure in future patients. These authors ar-gue that from a mathematical perspective the gold standard model would be a nonrestrictive one and that the price of parsimony lies in first knowing how to choose the right candidate predictors in the first place, from among many possible ones. In any case, we should not be dogmatic. In fact, we note that some of the techniques described in our article — such as bootstrapping to avoid overfitting or discard-ing variables to reduce the number of highly collinear ones — are in themselves tools that help reduce the final number of predictors to score in the clinic. In short, the goal is to achieve a balance between simplicity, usabil-ity, and reliability.
tors that other researchers have reported to be important or decisive.
In any case, on subjecting the development dataset to bivariable analysis, finding a strong association between a factor and the outcome would strengthen the factor’s candidacy for inclusion in the prediction model. Finding no significant association, on the other hand, would rule such a factor out of the new model. Bivariable analysis is necessary because all factors the anesthesiologists collected at pre-operative visits cannot be entered into logistic regression, even if each one might increase the predictive capacity of the model very slight-ly. If too many are added the reasonable ratio of 1 factor to 10 observed events mentioned above will be lost, leading to overfitting of the model. The result of overfitting will be a model that is scarcely replicable in different datasets. Moreover, in case of high colinearity between factors (poorly tolerated on logistic regression even if the factors are strongly associated with the outcome), clinical judgment provides the best criteria for choosing or discarding factors as candidates For example, we note that the American Society of Anesthesiologists (ASA) classification and preoperative oxyhemoglo-bin saturation by pulse oximetry (SpO2) might be found to be colinear; or there may well be colinearity between smoking, chronic obstruc-tive pulmonary disease and SpO2. In these cases, the relative merits of using one or the other must be assessed. There is no doubt that smoking is a risk factor for PPCs but from the perspective of the preoperative visit, spo2 is potentially easier to quantify objectively. Re-specting colinearity between ASA class and spo2, the clinician might well prefer SpO2 as a quickly assessed objective predictor for PPC but ASA class as a predictor of length of hospi-tal stay or mortality. A preliminary exploratory search for subsets of variables that provide better predictive performance without violat-ing initially proposed criteria is highly recom-mendable, we think. In any case it is not wrong to do so and should not be confused with the practice known as “going fishing” for associa-tions.
another approach that leads developers to

OPTIMIZING PPCs MaZo
Vol. 82 - No. 3 Minerva anestesiologica 335
PPC risk factors most often cited in the literature
Many factors have been implicated in the development of PPCs. The most comprehen-sive revision of the topic, published in 2006, emphasized factors supported by level A evi-dence.16 The authors grouped the factors as patient-dependent (advanced age, functional dependence, asa class >2, congestive heart failure, and chronic obstructive pulmonary disease), surgical (aortic aneurysm; neurosur-gery and thoracic, abdominal, upper abdomi-nal, head and neck, vascular, and emergency surgeries; prolonged surgery; and general an-esthesia), or analytical (albumin level <35 g/l). Worth noting is that the 2006 review did not find published evidence supporting some plau-sible predictors (such as asthma, sleep apnea, obesity or spirometry).16 Smetana et al. there-fore concluded that while consensus exists on the value of spirometry before lung resection and in determining candidacy for coronary artery bypass, its value before extrathoracic surgery remains unproven. These and other authors had already suggested grouping fac-tors as modifiable or unmodifiable, as shown in Table I.1, 16–34
In order to update our current understand-ing of the PPC risk situation, we searched PubMed (time frame, 2000 to August 2014) for titles or abstracts with the terms “postop-erative pulmonary complications”, finding 445 items. Only a few of those studies developed PPC prediction models in settings that reached beyond very specific disease or surgical con-texts. Two of these specific studies, with pneu-monia 22 and respiratory failure 35 as outcomes, respectively, were performed in American vet-erans’ hospitals and showed significant gender bias (>95% male). Six others used retrospec-tive datasets of patients to develop a score predicting single PPC outcomes: unplanned reintubation,18, 28, 34 postoperative pulmonary failure, 30 and adult respiratory distress syn-drome.25, 36 Finally, only two were prospec-tive studies in patients undergoing a wide range of surgeries; one of them 27 found age, positive cough test, perioperative nasogastric
Validating a model
A principle to remember is that statisti-cal optimism presides over any model in the first phase, when it is supported only by the development sample.8 an internal validation process must be planned to ensure that the model predicts events in patients outside this sample. A model can be validated in several ways: by splitting the dataset into two random samples for cross validation; or better, by re-peatedly cross validating in several different randomly sampled portions of the dataset; or even better, by bootstrapping, a technique of computer-intensive resampling procedures that replicate the resampling process between 50 and 500 times.10 All of these methods are intended to measure the performance of the newly proposed regression model in the dif-ferent randomized subsamples of the develop-mental sample.8, 9
The key measures to consider in predictive accuracy will now be outlined. First, discrimi-nation, or the ability of a model to distinguish subjects with high risk from subjects at low risk, an attribute that is commonly quantified with the c-statistic. In the case of binary out-comes, this statistic is the equivalent of the area under the receiver operating characteristic curve. The second is calibration, or the statisti-cal measure of the extent to which the predicted probabilities agree with the observed events.
If after a rigorous development and internal validation of a model its accuracy is verified, it would be time to propose it to the academ-ic and clinical community as a useful tool to consider. However, its utility can only be fully recognized after a process of further external validation in increasingly realistic clinical situ-ations.11–15 This step serves to assess the mod-el’s generalizability or ability to provide ac-curate predictions in either patients who were not recruited at the time of development but who are from a highly comparable population (reproducibility), or patients drawn from a dif-ferent but also reasonably comparable popula-tion or in datasets compiled using methods that differ from those used in development sample (transportability).

MaZo OPTIMIZING PPCs
336 Minerva anestesiologica March 2016
cerned the postoperative period; yet only one referred to PPC risk. Expanding the search back to the 1960s did not change the results. Given the well-demonstrated importance of PPCs and the large number of proposed mod-els, it is surprising that the only replication, or external validation study of a PPC risk score that has emerged to date is the one carried out by the authors of this review, among others.37 In an editorial accompanying that study, which was carried out in a European multicenter co-hort, the editors underlined that the model’s utility — its specificity and sensitivity, for example — was only one aspect of interest.38 The actual methodological process of exter-nal validation itself represented an important advance in predicting PPCs, they argued, not-ing that when a journal publishes predictive score models it is in the hope that their true utility to influence clinical practice will be established with time. Such further valida-tion, as explained above, involves replication and clinical application studies to demon-
tube insertion, and duration of anesthesia to be independent predictors of PPCs after elec-tive nonthoracic surgery in 1055 consecutive patients attending the preadmission clinic of a university hospital. The other, the ARISCAT study,26 found age, preoperative SpO2 in air, acute respiratory infection during the previous month, preoperative anemia, upper abdominal or intrathoracic surgery, surgical duration and emergency surgery to be independent predic-tors (see predictors scored in Table II) in 2464 patients undergoing surgical procedures un-der general, neuraxial, or regional anesthesia. Seven of these identified articles were pub-lished later than the 2006 systematic review. We think an updated systematic review includ-ing the latest studies published in the last eight years is already warranted.
We also searched for external validations of the aforementioned risk scores, finding only one.26 Interestingly, however, when we searched for external validation studies of any risk score, 1519 items were found and 40 con-
Table I.—�Risk factors for postoperative pulmonary complications.Patient-related Procedure-related
Modifiable Low body weight 16-18
Obesity 18-20
Smoking 16, 19, 21-24
alcohol intake 16, 18, 22, 25
Respiratory infection in the last month 26
sepsis 18
Low serum albumin 16
Anemia 26
low spo 2, 26
Positive cough test 26, 27
Prolonged surgery 16, 21, 26, 31
general anesthesia 16, 22
Transfusion 16, 22, 31, 33
Prolonged hospitalization 18
Nonmodifiable Congestive heart failure 16, 28, 29
asa class >2 16, 19, 28
advanced age 16, 17, 19, 21, 22, 26, 29
COPD 16, 19, 22, 25, 28, 29
Functional dependence 16, 30
Impaired sensorium 16, 22
GERD 25
Diabetes mellitus 18, 21, 25, 31
Obstructive sleep apnea 20
Hypertension 18
liver disease 18
cancer 18
genetic variations 32
alterations in chest radiograph 16
High blood urea 16, 22
High risk procedures 16-18, 25, 26, 28, 30
Aortic aneurismthoracicAbdominalUpper abdominalNeurosurgeryVascularHead and neckProcedures with a high risk for ALI 25
Procedures with a high risk for UEPI 18
Emergency surgery 1, 16, 22, 28-30, 34
ALI/ARDS: acute lung injury/acute respiratory distress syndrome; ASA: American Society of Anesthesiologists; COPD: chronic obstructive pulmonary disease; GERD: gastroesophageal reflux disease; PPC: postoperative pulmonary complications; SpO2: oxygen saturation as mea-sured by pulse oximetry; UEPI: unanticipated early postoperative intubation.

OPTIMIZING PPCs MaZo
Vol. 82 - No. 3 Minerva anestesiologica 337
ing the degree of difference in prediction that can be present and confirming the advisability of recalibration by clinicians working in well-defined contexts with known population char-acteristics.39, 40
A valid risk scoring system, the availability of preventive measures, and
optimal cutoffs for risk stratification: three requisites for a virtuous circle
Even though mathematicians dislike impos-ing cut points on a predictive scale because they transform a numerical scale into a cate-gorical one, clinicians need such benchmarks if the scale is to be used as a tool for decision-making. To say that one patient is at high risk when there is more than a 20% probability of developing a complication, while another is at low risk when the probability is 19% is mere convention. That approach does not take into account how effective the application of the cutoffs will be on changing outcomes or containing costs. A statistical criterion for setting optimal cutoffs is the Youden Index (J=sensitivity+specificity-1), which was sug-gested by W.J. Youden in 1950 41 as a way of summarizing the performance of a diagnostic test. The index has a value of 0 when a diag-nostic test gives the same proportion of posi-tive results for groups with and without the disease: in other words, the test is useless. A value of 1 indicates that there are no false positives or false negatives: that is, the test is perfect. However, in the absence of perfection, the planning of a medical intervention is fa-cilitated by knowing how many false negatives would avoid treatment (or how many false positives would be treated) if the cut point
strate transportability. Because the validation study cited in the editorial was conducted in 63 centers enrolling 5099 patients across 21 European countries, it was possible to estimate the geographical transportability of the model under assessment. An interesting finding was that although the model discriminated well in the total population, its calibration was poorer in some European regions (Table III), reveal-
Table II.—�The Seven ARISCAT Risk Predictors, β re-gression coefficients and Points Assigned.*
score
Patient-dependent predictorsAge (yr)
≤0 051-80 3>80 16
Preoperative SpO2≥96% 091-95% 8≤90% 24
Respiratory infection in the last monthno 0Yes 17
Preoperative anemia (Hb≤10 g/dL)no 0Yes 11
Surgery-dependent predictorsSurgical incision
Peripheral 0Upper abdominal 15intrathoracic 24
Duration of surgery (h)≤2 0>2-3 16>3 23
Emergency procedureno 0Yes 8
* Three levels of risk were indicated by the following cut-offs: <26 points, low risk; 26 to 44 points, moderate risk; and ≥45 points, high risk. ARISCAT: assess respiratory risk in surgical patients in Catalo-nia; SpO2: arterial oxyhemoglobin saturation by pulse oximetry; Hb: hemoglobin concentration.
Table III.—�Discrimination (c-statistic), predicted PPC rates and observed rates (95% confidence intervals) of ARIS-CAT score in PERISCOPE sample.
overall spain We ee
Discriminationc-statistic 0.80 (0.78-0.82 0.80 (0.77-0.84) 0.87 (0.83-0.90) 0.76 (0.72-0.80)
CalibrationPredicted 5.04% (4.74-5.34%) 5.45% (4.98-5.91%) 5.45% (4.84-6.06%) 4.11% (3.62-4.60%)Observed 7.92% (7.18-8.66%) 5.70% (4.68-6.72%) 8.19% (6.87-9.51%) 10.51% (8.99-12.03%)
ARISCAT: assess respiratory risk in surgical patients in Catalonia; PERISCOPE: prospective evaluation of a risk score for postoperative pulmonary complications in Europe; PPC: postoperative pulmonary complication; WE: Western Europe; EE: Eastern Europe.

MaZo OPTIMIZING PPCs
338 Minerva anestesiologica March 2016
pathophysiology of breathing and mechanical ventilation. Despite having a broad theoretical basis, however, the level of scientific evidence for these physical interventions is weak to date. In the last few years, interest in studying how intraoperative ventilatory management influ-ences the development of PPCs has grown, given that the role of such management has been confirmed in the critical care setting. Cur-rently, a protective ventilation strategy refers to the use of a low tidal volume (4-8 mL/kg of predicted body weight), with positive end-ex-piratory pressure (PEEP) and with or without recruitment maneuvers. Recent publications have addressed this strategy. In a meta-analy-sis of mostly observational studies, Hemmes et al. 51 reported that intraoperative lung protec-tive ventilation reduced the risk of pulmonary complications. Another meta-analysis 52 of four interesting clinical trials 53–56 concluded that protective ventilation could reduce the incidence of atelectasis and pulmonary infec-tions but not the incidence of acute lung injury. It seems accepted that a low tidal volume pro-tects against alveolar damage and that its pos-sible effects on the collapse of dependent areas should be countered with low levels of PEEP and recruitment maneuvers. However, recently the PROVHILO clinical trial 57 (on PROtec-tive Ventilation during general anesthesia for open abdominal surgery) advocated the use of low tidal volumes with very low levels of PEEP (>12 cmH2o vs. <2 cmH2O) but without recruitment maneuvers. These examples illus-trate a trend toward consensus but also show that there is still a way to go before we fully understand perioperative ventilator support.
Clinical guidelines on strategies to reduce PPCs after non-cardiothoracic surgery 58 ar-gued that lung expansion therapy (incentive spirometry, deep breathing exercises and con-tinuous positive airway pressure) were the only strategies of proven benefit. Although no phys-iotherapy treatment has been identified as su-perior to others and some reviewers have not-ed that the evidence supporting preoperative physiotherapy protocols to prevent PPCs in critically ill patients is poor,59, 60 the safety and low cost of many of these measures has simply
were to shift toward one side of the receiver operating characteristic curve or the other. As vickers et al. 42 have shown, decision curve analysis needs to be applied to determine the net benefit of implementing an intervention as a result of different predictions of risk level. Clinicians tend increasingly to avoid excessive dichotomization, however, and wish to be able to detect gray zones of moderate or intermedi-ate risk 43, 44 that favor the adoption of more moderate and less costly measures in line with the gradual progression of any disease or ther-apeutic process.
Strategies to reduce PPC risk
Any measure which would allow a clinician to mitigate or eliminate any of the modifiable risk factors listed (Table I) or discussed above could contribute decisively to lowering risk for PPCs.45 Since, for example, surgical pro-cedures lasting more than three hours are as-sociated with higher PPC risk 16, 26, 27, 31, 46–49 a shorter procedure should ideally be attempted in patients at high risk. To guide our attempt to modify some factors, however, information is still needed. For example, a recent study found that 30-day postoperative respiratory events were found to be more frequent in cur-rent smokers than in former smokers or never smokers, and smoking cessation at least a year prior to elective surgery appeared to improve a number of outcomes, such as mortality and respiratory, arterial and venous events.24 How-ever, the duration of abstinence from smoking necessary for a reduction in PPCs has not been firmly established. Smetana et al. 50 have ad-vised that a duration of at least eight weeks of cessation seems to be optimal and should be targeted whenever possible. Other examples of potential strategies for risk modification might be delaying elective surgery in the presence of an upper respiratory infection in the last month 26, 51 or correcting anemia before surgery with pharmacologic or nutritional strategies.26
Besides these efforts to modify specifically identified risks, other measures to protect or improve perioperative respiratory function overall have been based on knowledge of the

OPTIMIZING PPCs MaZo
Vol. 82 - No. 3 Minerva anestesiologica 339
timodal approach may be advisable clinically even though it might obscure the identification of the best individual measures. We might say that an ideal compromise has been reached when we have been able to apply a few effec-tive and inexpensive measures with few iatro-genic effects to every patient, while reserving more sophisticated, expensive and aggressive measures for high-risk patients. Establish-ing intermediate care areas for patients with moderate to high risk would be very useful for facilitating an appropriate postoperative phys-iotherapy program and basic monitoring for PPCs so they can be detected early and treated.
Conclusions
Prediction, prevention, and early diagnosis should be essential objectives that help to mini-mize the impact a PPC may have on both patient recovery and health costs. Predictive modeling requires both complex clinical knowledge and rigorous methodology (Figure 1). The final de-
led to the assumption that it is highly reason-able to continue to use the measures named in the 2006 guidelines after high-risk surgery. Evidence in support of physiotherapeutic mea-sures is beginning to emerge, however. A non-randomized before–after trial conducted by the Pulmonary Care Working Group found that a standardized postoperative program known by the acronym I COUGH,23 (Incentive spirom-etry, Coughing and deep breathing, Oral care, Understanding of patient and family, Getting out of bed frequently and Head-of-bed eleva-tion) reported reduced incidences of postop-erative pneumonia (from 2.6% to 1.6%) and unplanned intubation (from 2.0 to 1.2%) with the implementation of the low-cost measures.
Measures that mitigate or eliminate specific risk factors and general preventive measures (physiotherapy or protective ventilation) not strictly related to particular risk factors are clearly complementary, and applying one does not exclude applying the others. As in many other areas of postoperative patient care, a mul-
Figure 1.—Developing and optimizing a new predictive model.

MaZo OPTIMIZING PPCs
340 Minerva anestesiologica March 2016
RN, Watson CB. Clinical and economic burden of post-operative pulmonary complications: Patient safety sum-mit on definition, risk-reducing interventions, and pre-ventive strategies. Crit Care Med 2011;39:2163-72.
3. Shmueli G. To Explain or to Predict? Statistical Science 2010;25:289-310.
4. Perduzzi P, Concato J, Kemper E, Holdford TR, Feistein AA. Simulation of the number of events per variable in logistic regression analysis. J Clin Epidemiol 1996;49:1373-9.
5. Vergouwe Y, Steyerberg EW, Eijkemans MJ, Habbema JD. Substantial effective sample sizes were required for external validation studies of predictive logistic regres-sion models. J Clin Epidemiol 2005;58:475-83.
6. Mazo V, Sabaté S, Canet J. A race against time: planning postoperative critical care. Anesthesiology 2013;119:498-500.
7. Wears RL, Lewis RJ. Statistical Models and Occam’s Ra-zor. Academic Emergency Medicine 1999;6:93-4.
8. Harrell FE Jr: Regression Modeling Strategies: With applications to linear Models, logistic regression and Survival Analysis. New York: Springer-Verlag New York; 2001.
9. Steyerberg EW, Harrell FE Jr., Borsboom GJ, Eijkemans MJ, Vergouwe Y, Habbema JD. Internal validation of pre-dictive models: efficiency of some procedures for logistic regression analysis. J Clin Epidemiol 2001;54:774-81.
10. Steyerberg EW: Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating. New York: Springer Publishing Company; 2009.
11. Moons KG, Kengne AP, Grobbee DE, Royston P, Vergou-we Y, Altman DG, Woodward M. Risk prediction models: II. External validation, model updating, and impact as-sessment. Heart 2012;98:691-8.
12. Justice AC, Covinsky KE, Berlin JA. Assessing the gen-eralizability of prognostic information. Ann Intern Med 1999;130:515-24.
13. Altman DG, Royston P. What do we mean by validating a prognostic model? Stat Med 2000;19:453-73.
14. Moons KG, Altman DG, Vergouwe Y, Royston P. Prog-nosis and prognostic research: Application and im-pact of prognostic models in clinical practice. BMJ 2009;338:b606.
15. Altman DG, Vergouwe Y, Royston P, Moons KG. Prog-Prog-nosis and prognostic research: Validating a prognostic model. BMJ 2009;338:b605.
16. Smetana GW, Lawrence VA, Cornell JE; American co-llege of Physicians. Preoperative pulmonary risk stratifi-cation for noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006;144:581-95.
17. Semenov YR, Starmer HM, Gourin CG. The effect of pneumonia on short-term outcomes and cost of care after head and neck cancer surgery. Laryngoscope 2012;122:1994-2004.
18. Ramachandran SK, Nafiu OO, Ghaferi A, Tremper KK, Shanks A, Kheterpal S. Independent predictors and out-comes of unanticipated early postoperative tracheal intu-bation after nonemergent, noncardiac surgery. Anesthesi-ology 2011;115:44-53.
19. Agostini P, Cieslik H, Rathinam S, Birshay E, Kalkat MS, Rajesh PB et al. Postoperative pulmonary complications following thoracic surgery: are there any modifiable risk factors? Thorax 2010;65:815-8.
20. Kandasamy T, Wright ED, Fuller J, Rotemberg BW. The incidence of early postoperative complications following uvulopalatopharyngoplasty: identification of predictive risk factors. J Otolaryngol Head Neck Surg 2013;42:15.
21. Gupta PK, Gupta H, Kaushik M, Fang X, Miller WJ, Mor-row le et al. Predictors of pulmonary complications after bariatric surgery. Surg Obes Relat Dis 2012;8:574-81.
cision about the usefulness of a predictive PPC Score will ultimately rest on finding reliable evidence that stratifying respiratory risk has helped identify clearly effective measures of prevention and early treatment. There is much further research to do. The research that is needed, once risk a score is established, is that provides a continuous process of feedback that will hone risk stratification and support rigor-ous clinical trials in better-targeted populations. In other words, information from research feed-back loops from well-designed studies will af-fect optimal cutoffs for predictive scales and provide practical guidance on steps to take.
at present we see what perhaps appears to be a vicious circle: doubtful risk stratification based on arbitrary or nonvalidated traditional assumptions suggest interventions that are of theoretical but unproven benefit, undermining our sense that we understand risk clearly. We think this vicious circle can become a virtuous one if active scientific and clinical feedback loops are operating. In addition, we note that even if effective risk-reduction or treatment strategies cannot be identified in this process, a clear awareness of level of risk is a patient’s right, as it might inform the decision to decline or consent to surgery.
Key messages
— PPCs have great impact on recovery and health care costs.
— Predictive modeling requires a rigor-ous methodology: wise selection candidate predictors is essential and models must undergo a careful process of internal and external validation.
— The evaluation of the usefulness of models cannot be dissociated from thera-peutic measures available.
References
1. Sabaté S, Mazo V, Canet J. Predicting postoperative pul-monary complications: implications for outcomes and costs. Curr Opin Anaesthesiol 2014;27:201-9.
2. Shander A, Fleisher LA, Barie PS, Bigatello LM, Sladen

OPTIMIZING PPCs MaZo
Vol. 82 - No. 3 Minerva anestesiologica 341
ence: Changes in ANESTHESIOLOGY. Anesthesiology 2014;121:209-11.
39. Toll DB, Janssen KJ, Vergouwe Y, Moons KG. Valida-valida-tion, updating and impact of clinical prediction rules: A review. J Clin Epidemiol 2008;61:1085-94.
40. Janssen KJ, Moons KG, Kalkman CJ, Grobbee DE, Vergouwe Y. Updating methods improved the perform-ance of a clinical prediction model in new patients. J Clin Epidemiol 2008;61:76-86.
41. Youden WJ. Index for rating diagnostic tests. Cancer 1950;3:32-5
42. Vickers AJ, Elkin EB. Decision curve analysis: a novel model method for evaluating prediction models. Med De-cis Making 2006;26:565-74.
43. Cannesson M, Le Manach Y, Hofer CK, Goarin JP, Lehot JJ, vallet B, et al. Assessing the diagnostic accuracy of pulse pressure variations for the prediction of fluid responsiveness: a “grey zone” approach. Anesthesiology 2011;115:231-41.
44. Duwat A, Zogheib E, Guinot PG, Levy F, Trojette F, Diof M, et al. The gray zone of the Qualitative assessment of respiratory changes in inferior vena cava diameter in ICU patients. Crit Care 2014;18:R14.
45. Canet J, Mazo V. Postoperative pulmonary complica-tions. Minerva Anestesiol 2010;76:138-43.
46. Diez-Sebastian J, Herruzo R, Garcia-Caballero J. Preven-tion of early-onset pneumonia in surgical patients by che-moprophylaxis. Am J Surg 2012;204:441-6.
47. Fuller RL, McCullough EC, Bao MZ, Averill RF. Estimat-McCullough EC, Bao MZ, Averill RF. Estimat-. Estimat-ing the costs of potentially preventable hospital acquired complications. Health Care Financ Rev 2009;30:17-32
48. Reeve JC, Nicol K, Stiller K, McPherson KM, Birch P, Gordon IR, et al. Does physiotherapy reduce the in-Does physiotherapy reduce the in-cidence of postoperative pulmonary complications fol-lowing pulmonary resection via open thoracotomy? A preliminary randomised single-blind clinical trial. Eur J Cardiothorac Surg 2010;37:1158-66.
49. Scholes RL, Browning L, Sztendur EM, Denehy L. Dura-Browning L, Sztendur EM, Denehy L. Dura-. Dura-tion of anaesthesia, type of surgery, respiratory comorbid-ity, predicted VO2max and smoking predict postoperative pulmonary complications after upper abdominal surgery: an observational study. Aust J Physiother 2009;55:191-8.
50. Smetana GW. Strategies to reduce postoperative pulmo-nary complications. UpToDate 2013. In: King TE, Aron-son MD, editors. Waltham, MA: UpToDate.
51. Hemmes SN, Serpa Neto A, Schultz MJ. Intraoperative ventilatory strategies to prevent postoperative pulmonary complications: a meta-analysis. Curr Opin Anaesthesiol 2013;26:126-33.
52. Tao T, Bo L, Chen F, Xie Q, Zou Y, Hu B, et al. effect of protective ventilation on postoperative pulmonary com-plications in patients undergoing general anaesthesia: a meta-analysis of randomised controlled trials. BMJ Open 2014;4:e005208.
53. Treschan TA, Kaisers W, Schaefer MS, Bastin B, Sch-Kaisers W, Schaefer MS, Bastin B, Sch-malz U, Wania V, et al. Ventilation with low tidal volumes during upper abdominal surgery does not improve post-operative lung function. Br J Anaesth 2012;109:263-71.
54. Weingarten TN, Whalen FX, Warner DO, Gajic O, Schears GJ, Snyder MR, et al. Comparison of two ven-Comparison of two ven-tilatory strategies in elderly patients undergoing major abdominal surgery. Br J Anaesth 2010;104:16-22.
55. Severgnini P, Selmo G, Lanza C, Chiesa A, Frigerio A, Bacuzzi A, et al. Protective mechanical ventilation dur-ing general anesthesia for open abdominal surgery im-proves postoperative pulmonary function. Anesthesiol-ogy 2013;118:1307-21.
56. Futier E, Constantin JM, Paugam-Burtz C, Pascal J, Eu-Constantin JM, Paugam-Burtz C, Pascal J, Eu-rin M, Neuschwander A, et al. a trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med 2013;369:428-37.
57. PROVE Network Investigators for the Clinical Trial
22. Arozullah AM, Khuri SF, Henderson WG, Daley J;Participants in the National Veterans Affairs Surgical Quality Improvement Program: Development and valida-tion of a multifactorial risk index for predicting postop-erative pneumonia after major noncardiac surgery. Ann Intern Med 2001;135:847-57.
23. Cassidy MR, Rosenkranz P, McCabe K, Roben JE, McAneny D. I COUGH: reducing postoperative pulmo-nary complications with a multidisciplinary patient care program. JAMA Surg 2013;148:740-5.
24. Musallam KM, Rosendaal FR, Zaatari, Soweid A, Hobal-lah JJ, Sfeir PM, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergo-ing major surgery. JAMA Surg 2013;148:755-62.
25. Kor DJ, Warner DO, Alsara A, Fernandez-Perez ER, Ma-linchoc M, Kashyap R, et al. Derivation and diagnostic accuracy of the surgical lung injury prediction model. Anesthesiology 2011;115:117-28.
26. Canet J, Gallart L, Gomar C, Paluzie G, Vallés J, Castillo J, et al. Prediction of postoperative pulmonary complica-tions in a population-based surgical cohort. Anesthesiol-ogy 2010;113:1338-50.
27. McAlister FA, Bertsch K, Man J, Bradley J, Jacka M. In-cidence of and risk factors for pulmonary complications after nonthoracic surgery. Am J Respir Crit Care Med 2005;171:514-7.
28. Brueckmann B, Villa-Uribe JL, Bateman BT, Grosse-Sundrup M, Hess DR, Schlett CL, et al. Development and validation of a score for prediction of postoperative res-piratory complications. Anesthesiology 2013;118:1275-85.
29. Li C, Yang WH, Zhou J, Wu Y, Li YS, Whey SH, et al. Risk factors for predicting postoperative complications after open infrarenal abdominal aortic aneurysm repair: results from a single vascular centre in China. J Clin An-esth 2013;25:371-8.
30. Gupta H, Gupta PK, Fang X, Miller WJ, Cemay S, Forse ra, et al. Development and validation of a risk calcu-lator predicting postoperative respiratory failure. Chest 2011;140:1207-15.
31. Nobili C, Marzano E, Oussoultzoglou E, Rosso E, Addeo P, Bachellier P et al. Multivariate analysis of risk factors for pulmonary complications after hepatic resection. Ann Surg 2012;255:540-50.
32. Kim JY, Hildebrandt MA, Pu X, Ye Y, Correa AM, Va-porciyan AA, et al. Variations in the vascular endothelial growth factor pathway predict pulmonary complications. Ann Thorac Surg 2012;94:1079-85.
33. Marda M, Pandia MP, Rath GP, Bithal PK, Dash HH. Post-operative pulmonary complications in patients un-dergoing transoral odontoidectomy and posterior fixation for craniovertebral junction anomalies. J Anaesthesiol Clin Pharmacol 2013;29:200-4.
34. Hua M, Brady JE, Li G. A scoring system to predict un-planned intubation in patients having undergone major surgical procedures. Anesth Analg 2012;115:88-94.
35. Arozullah AM, Daley J, Henderson WG, Khuri SF. Mul-tifactorial risk index for predicting postoperative respira-tory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Im-provement Program. Ann Surg 2000;232:242-53
36. Blum JM, Stentz MJ, Dechert R, Jewell E, Engoren M, Rosenberg AL, Park PK. Preoperative and intraoperative predictors of postoperative acute respiratory distress syn-drome in a general surgical population. Anesthesiology 2013;118:19-29
37. Mazo V, Sabaté S, Canet J, Gallart Ll, de Abreu MG, Belda J, et al. Prospective external validation of a pre-dictive score for postoperative pulmonary complications. Anesthesiology 2014;121:219-31.
38. Eisenach JC, Houle TT. Replication to Advance Sci-

MaZo OPTIMIZING PPCs
342 Minerva anestesiologica March 2016
59. Imberger G, McIlroy D, Pace NL, Wetterslev J, Brok J, Møller AM. Positive end-expiratory pressure (PEEP) dur-. Positive end-expiratory pressure (PEEP) dur-Positive end-expiratory pressure (PEEP) dur-ing anaesthesia for the prevention of mortality and post-operative pulmonary complications (review). Cochrane Database Syst Rev 2010;CD007922.
60. Ireland CJ, Chapman TM, Matheu SF, Herbison GP, Zacharias M. Continuous positive airway pressure (CPAP) during the postoperative period for preven-tion of postoperative morbidity and mortality following major abdominal surgery. Cochrane Database Syst Rev 2014;CD008930.
Network of the European Society of Anaesthesiology, Hemmes SN, Gama de Abreu M, Pelosi P, Schultz MJ. High versus low positive end-expiratory pressure dur-ing general anaesthesia for open abdominal surgery (PROVHILO trial): a multicentre randomised controlled trial. Lancet 2014;384:495-503
58. Lawrence VA, Cornell JE, Smetana GW; American College of Physicians. Strategies to reduce postopera-. Strategies to reduce postopera-Strategies to reduce postopera-tive pulmonary complications after noncardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006;144:596-608.
Acknowledgments.—The authors wish to thank Mary Ellen Kerans, M.A. (freelance editor, Barcelona, Spain) who revised the English usage in some versions of the manuscript.Funding.—Supported by grant Fundació La Marató de TV3 (Televisió de Catalunya), Barcelona, Spain; grant #041610-2003 and through the European Society of Anaesthesiology’s Clinical Trials Network.Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: May 20, 2015. - Manuscript accepted: May 18, 2015. - Manuscript revised: April 27, 2015. - Manus-cript received: October 27, 2014.

Vol. 82 - No. 3 MiNerVa aNestesiologica 343
ognition, personalized resuscitation, pathogen identification and treatment.4, 5
The early diagnosis of sepsis stills remains problematic. Numerous studies have shown that delays in intervention are linked with high-er mortality.6 The recent 2012 version of the Survival Sepsis Guidelines lists the diagnostic criteria for sepsis, which states: infection, docu-mented or suspected and some of the following: general, inflammatory, hemodynamic, organ dysfunction and tissue perfusion variables. This if nothing else stresses the point that if one sus-pects sepsis and has virtually some of the asso-ciated clinical or laboratory features that appro-priate intervention should commence rapidly.
one diagnostic strategy relies on clinical and routine laboratory measurements to establish diagnosis and define pre-test probability, while
sepsis is the host’s deleterious, non-resolv-ing inflammatory response to infection that
leads to organ dysfunction.1 the frequency of sepsis is increasing because of aging popula-tion, increased frequency of resistant organ-isms, and more complex surgery and immuno-suppressive drugs. Despite the paucity of positive trials in sepsis, the mortality of sepsis has decreased over the past decade because of earlier recognition in the Emergency De-partment and because of early initiation of antibiotics, fluids, vasopressor and inotropic agents.2, 3 Recent randomized controlled trials have challenged the legitimacy of early hemo-dynamic driven goals, which now stresses the fundamental importance of early sepsis rec-
R E V I E W
The role of genomics to identify biomarkers and signaling molecules during severe sepsis
James J. DOUGLAS *, James A. RUSSELL
Centre for Heart Lung Innovation, St. Paul’s Hospital and University of British Columbia, Division of Critical Care Medicine, Vancouver, Canada*Corresponding author: James J. Douglas, Centre for Heart Lung Innovation, St. Paul’s Hospital, 1081 Burrard Street, Vancouver, V6Z 1Y6 BC, Canada. E-mail: [email protected]
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: Minerva AnestesiologicaCod Rivista: Minerva Anestesiol
Lavoro: 10295-MAStitolo breve: BIOMARKERS OF SEVERE SEPSISprimo autore: DOUGLASpagine: 343-58citazione: Minerva Anestesiol 2016;82:343-58
A B S T R A C TEarly strategies to diagnose, manage and predict outcome of sepsis are essential to further improve morbidity and mortal-ity of sepsis. Whereas biomarkers have become mainstay in other fields of medicine, their clinical utility in sepsis remains generally much less proven and so biomarkers are much less used clinically. The Human Genome Project embellished genomics, transcriptomics, proteomics and metabolomics and continues to expand our knowledge of the genetic, gene expression, protein translational and metabolic discoveries that could lead to clinical biomarker tests related to sepsis thereby allowing insight into the disease as never seen before. We explore the genomic approach to biomarker identifica-tion and validation by reviewing pertinent studies related to the diagnosis (diagnostic biomarkers), prediction of response to therapies (predictive biomarkers) and (prognostic biomarkers) outcomes of sepsis.(Cite this article as: Douglas JJ, Russell JA. The role of genomics to identify biomarkers and signaling molecules during severe sepsis. Minerva Anestesiol 2016;82:343-58)Key words: Sepsis - Biomarkers - Diagnosis - Genetic testing - Genomics - Proteomics.
Minerva Anestesiologica 2016 March;82 (3):343-58© 2015 EDIZIONI MINERVA MEDICAThe online version of this article is located at http://www.minervamedica.it
Comment in p. 268.

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
344 MiNerVa aNestesiologica March 2016
sion studies looking at the innate immune response to bacterial infection is associated with the expression of more than 3000 genes, making gene expression studies a potentially useful tool for understanding the pathogenesis. Many plasma protein biomarkers are intrigu-ing and could one day become routine clinical practice. In other words, we are agnostic as to whether a biomarker is genomic, mRNA ex-pression or protein expression. The definition of a successful useful biomarker will depend more on its operational statistical analytic characteristics achieve adequate rigor and pre-cision to become used clinically.
Biomarkers and the sepsis guidelines
Despite the potential uses of biomarkers within sepsis, the surviving sepsis campaign has been slow to incorporate any biomarkers.11 in fact, the guidelines has only a grade 2 rec-ommendation for the use of 1,3 beta-D-glucan assay (grade 2B), anti-mannan antibody assays (grade 2C) for the diagnosis of invasive candi-diasis and grade 2C recommendation for use of low procalcitonin levels or similar biomark-ers to assist with discontinuation of empiric antibiotics. the guidelines appropriately state that despite the continuing emergence of data, procalcitonin and other similar biomarkers are limited in their ability to discriminate between sepsis and severe inflammatory states without infection.12 However this data is still in its in-fancy; additional new larger well-designed studies on more rapid discontinuation of an-tibiotics and potential risk stratification, other outcome measures including ICU and hospital length of stay along with hospital costs may solidify the role of procalcitonin in sepsis management.13-15 the guidelines state that the ability of procalcitonin-based antibiotic dis-continuation has never been shown to reduce the prevalence of antimicrobial resistance or Clostridium difficile, however these are diffi-cult studies to perform. Relevant studies may include 6 or 12 month follow-up including specific evaluation for high risk organisms (i.e. Methicillin resistant Staphylococcus aureus, vancomycin resistant enterococcus or carbap-
novel biomarkers could be used to aid diagno-sis, to monitor disease progression and response to therapy and to inform prognosis. Herein lies the rapidly expanding field of analytical tools measuring biological parameters, also known as biomarkers. The Biomarkers Defin-itions Working Group defined a biomarker as a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmaco-logical responses to a therapeutic intervention.7 Highly sensitive and specific biomarkers are now mainstay as substitutes — in randomized controlled trials and indeed in clinical practice — for clinical outcomes especially in the fields of oncology and HiV. in sepsis, the potential uses of biomarkers include diagnosis, in differ-entiating viral from bacterial infection, in dif-ferentiating an inflammatory from an infectious process, prognostication, and in predicting re-sponse to treatment (efficacy and safety) and in predicting relapse. Despite investigation and publication of more than 170 distinct biological molecules that fulfill some of these criteria, no one clinically useful biomarker in sepsis has been firmly established in practice.8
The molecular mechanisms of sepsis can now be investigated using advanced tools including genomics, transcriptomics, pro-teomics, metabolomics and protein immunoas-says. Thus, potential sepsis biomarkers evalu-ate genetics (DNA), gene expression (mRNA) or protein expression or levels in blood or tis-sue. The genetic influence on the pathogenesis of acute inflammatory conditions including sepsis are often overlooked, but well docu-mented. In adoptee studies risk of death from infection was fivefold more heritable than death from cancer.9 this suggests that genetic variation of the human host to development of infection and to injurious host responses are critical determining factors to outcome of sep-sis. The Center for Disease Control (CDC) has embraced the usefulness of genomic data and through its department of The Office of Public Health Genomics (OPHG) works to identify, evaluate and implement genomic strategies against the leading chronic, infectious, envi-ronmental and occupation diseases.10 Expres-

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 345
with particular diseases and to date has identi-fied more than 14,000 SNPs. This GWAS ap-proach has been successful in the identification of genetic variants associated with many com-mon diseases including type 2 diabetes, cystic fibrosis and neurofibromatosis.
Transciptomics, also referred to as expres-sion profiling, is the study of the complete set of rNa transcripts that are produced by the genome under certain circumstances. Chal-lenges involved in the study of sepsis, include which tissue to sample, time sensitive features of a rapid process (leading to lead time bias in clinical studies) and establishing a gold stan-dard for the diagnosis of sepsis.17 Expression profiling commonly employs microarray tech-nology, or commonly called biochip, which is a collection of microscopic DNA attached to a surface that rely on hybridization of the surface DNA to a patient sample that can then detected and quantified. Different microar-ray platforms include printed, in situ synthe-sized, high-density bead arrays, electronic and liquid-bead suspension. The FDA initiated microarray quality control (MAQC) project is a standards and quality measure assessment currently in its third and final stage with gen-eration of benchmark datasets with reference samples and evaluation of various bioinfor-matic strategies.
Proteomics is the study of proteins and formed as an extension of the Human Genome Project. The study of the proteome is more complex than studies of genes or mRNA ex-pression due to changes in proteins such as post-translational modifications, alternative splicing, formation of complexes, protein deg-radation and the fact that much of transcribed
enemase producing organisms) to define better the risk of readmission could add credibility to the role of procalcitonin-guided antibiotics.
Genomic biomarkers and genomic methods of evaluation
The completion of the human genome proj-ect in 2001 succeeded by sequencing more than 30,000 genes in a single human being. Since that time the costs of sequencing have plummeted and several new sequencing technologies and multiple platforms are well-established. Ge-nomics is the discipline in genetics that applies recombinant DNA, DNA sequencing methods, and bioinformatics to sequence, assemble, and analyze the function and structure of genomes (the complete set of DNA within a single cell of an organism). Functional genomics is the active process of correlating these findings to clinical medicine. Functional genomics can focus on a single gene and how this gene’s se-quence alters gene expression in response to a septic challenge, can focus on a small number of so-called candidate genes, can use so-called Genome Wide Association Studies (GWAS) that canvass specific variants (single nucleo-tide polymorphisms [SNPs]) across the whole genome or could even measure the whole ge-nome. Techniques used in functional genomics include SNP analysis, genetic interaction map-ping, mutagenesis, RNA interference (RNAi) and genome annotation. The National Human Genome Research Institute (NHGRI) serves a reservoir for exploration of the human genome and its relationship with various diseases and treatments.16 Most techniques to date rely on GWAS to associate specific genetic variations
Figure 1.—Genomic approach to sepsis management.

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
346 MiNerVa aNestesiologica March 2016
molecular identification of pathogens, which detect pathogen molecules directly from blood samples. Barriers to universal approval of PCR detection of pathogens include limited sensitivity of the test (i.e. statistical sensitivi-ty), discordance between molecular results and blood cultures and often unclear significance of microbial DNA in blood specimens (i.e. specificity) and a poor ability to detect Strep-tococcus pneumonia bacteremia (i.e. sensitiv-ity).20 Purification of the nucleic acids from clinical samples remains a hurdle to overcome because blood can contain PCR inhibitors, re-agents, specimens may possess bacterial and/or fungal DNA, cell walls often require lysis and interference can occur from the high levels of human DNA.
A number of different molecular strategies exist for the molecular detection of patho-gens: pathogen specific assays targeting spe-cies- or genus-specific genes; assays target-ing conserved sequences in the bacterial or fungal genome (panbacterial 16S, 5S or 23S rrNa genes or panfungal 18s, 5.8s and 28s rDNAs) and multiplex assays allowing paral-lel detection of different pathogens.21 Several techniques are now well-established that have improved and adequate sensitivity for detec-tion of fastidious intracellular organisms in-cluding Brucella, rickettsiosis, Q fever and Bartonella.22
Microarray techniques have been applied to the diagnosis of sepsis. While it would be very useful clinically and convenient to have the ability to determine antibiotic resistance genes in the probe panel, the technique is still limited to the detection of pathogens such as Staphylo-coccus aureus, Pseudomonas aeruginosa, and Escherichia coli in positive blood cultures.23 in a study of neonatal sepsis, of 172 clini-cal cases, 9.88% tested positive by PCR and 4.65% by blood culture.24 Of the 17 positive by PCR, four were positive for S. epidermidis, four for coagulase negative staphylococcus and two positive each for Bacillus and Propi-onibacterium respectively, raising the concern about skin contamination.
The most used and clinically investigated molecular pathogen detection test is the Septi-
mRNA is not translated to protein.18 tradition-al methods of evaluating proteins including monoclonal antibodies and enzyme linked im-munoassays (ELISA) have given way to more complex proteomics methods such as mass spectrometry, surface-enhanced laser desorp-tion/ionization time of flight (SELDI-TOF) and protein micro arrays.
Pathogen detection
The gold standard for diagnosing bacteremia associated sepsis still remains the traditional enriched microbiology laboratory where broth blood culture is followed by identification and susceptibility testing of bacteria. although crucial for fine tuning antibiotic therapy, limi-tations include delay in waiting for growth, contamination and operator error related to inadequate volume. Molecular biology has allowed rapid molecular detection of bacteria and other organism components in blood as a complement to and perhaps one day substitute for conventional blood culture.
Molecular techniques for molecular organ-ism detection including hybridization (FISH, arrays), amplification (PCR, multiplex PCR), post-amplification detection (PCR + hybrid-ization/MALDI-TOFF MS) and non-nucleic acid based strategies (proteomics, spectrom-etry) are rapidly gaining ground.19 PCR and multiplex PCR strategies with various post-amplification techniques have sped up the diagnosis of bacteremia and primers can be used to detect the most common resistant genotypes, however it still remains that the majority of molecular tests require a positive blood culture before wide-spread clinical ap-plication. To our knowledge, there has been no large, multicenter, multinational randomized controlled trial comparing conventional blood culture to a strategy of blood culture plus mo-lecular organism detection in sepsis.
While PCR based techniques have been standard of care in culture identification of re-spiratory viruses, PCR-based techniques have been creeping into blood pathogen identifica-tion for the last 10 years. A number of com-mercially available tests are available for the

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 347
the SepsiTest (Molyzm, Germany), Magicplex (Seegene, Korea), VYOO (SIRSLab, Germa-ny) and Ibis PLEX-ID platform aimed at Cat-egory A bioterrorism organisms. These tests are in their infancy with limited or no observa-tional studies to date.29
There is another potential benefit of molecu-lar pathogen detection. One could estimate the infectious burden/organism load by determin-ing the Crossing point (Cp) value for all posi-tive results.30 The Cp value represents the PCR cycle at which the DNA becomes significantly amplified and is related to organism load.
The main benefits of pathogen detection by PCR, multiplex PCR and mass spectro-metrometry is the possibility of rapid result reporting as soon as 6 hours assuming opti-mal laboratory conditions and overall health economic savings despite the very high cost of the assay.31 Shortcomings of nucleic acid testing based assays include that the detection of microbial DNA does not necessarily indi-cate the presence of a viable microorganism(s) causing clinical condition. A second limita-tion is the inability to perform antimicrobial susceptibility testing but this could change because of refinements to include limited ge-netic testing for resistance genes such mecA in S. aureus.
Diagnosis of sepsis
Host gene expression changes could be used to diagnose sepsis. Early studies explored the human leukocyte response to endotoxin chal-lenge.32-35 in the study of talar et al.19 regard-ing gene expression changes after endotoxin exposure, the greatest change in mononuclear cell gene expression occurred at 6 hours post endotoxin with increased expression (induc-tion) of 439 and decreased expression (repres-sion) of 428 genes. By 24 hours, mononuclear cell gene expression had returned to baseline. the upregulated genes included genes associ-ated with pathogen recognition molecules and signaling cascades linked to receptors associ-ated with cell mobility and activation. In addi-tion increased gene expression occurred with cytokines, chemokines, and their respective
Fast test (Roche Diagnostics) that is approved for use in Europe but not North America. The SeptFast is a multiplex real-time PCR based assay system that detects 25 clinically signifi-cant pathogens. The SeptiFast has modest sen-sitivity for detection of bacteremia with values of 0.43-0.69 and respectable specificity of 0.81 – >0.97. However the SeptiFast test demon-strates variable pathogen detection compared to traditional blood culture testing.20, 25, 26 in-terestingly, the SeptiFast test concordance with blood culture results is only moderate. A number of studies have shown a high frequen-cy of PCR positive blood results with a nega-tive blood culture and to a lesser extent, the op-posite. False negative blood culture results can occur because of fastidious organisms, inade-quate culture conditions, autolysis, inadequate specimen and antibiotic pretreatment. Interest-ingly, in a prospective study in severe sepsis patients, PCR positivity even with a negative blood culture was associated with higher se-quential organ failure assessment (SOFA) scores and a trend towards higher mortality.27 This result could indicate that molecular detec-tion of pathogens that are not detected on rou-tine blood culture may be more useful clinical because of greater sensitivity for detection of poor prognosis.
The only molecular direct pathogen detec-tion test approved by the Food and Drug Ad-ministration (FDA) is the Cepheid Xpert. The GeneXpert is a closed, fully automated system combining sample preparation and real-time PCR for amplification and detection. Rapid detection of N. gonorrhoeae/Chlamydia, My-cobacterium tuberculosis (MTB) complex and MTB specimens with rifampin-resistance (rpoB gene) tests are already approved on the Xpert system. In June 2013 the FDA approved the Xpert MRSA blood detection test. The MRSA test requires positive blood cultures with gram stain showing gram-positive cocci in clusters and then moves to the Xpert system to identify Staphylococcus aureus or Methicil-lin-resistant Staphylococcus aureus (MRSA) in about 1 hour with a 75% and 100% sensi-tivity, respectively.28 other pathogen detection tests in variable stages of development include

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
348 MiNerVa aNestesiologica March 2016
and four controls using microarray contain-ing probes for 340 genes relevant to inflam-mation. Gene expression in sepsis was highly homogenous with 69% of genes differentially expressed between septic and controls.38 Like-wise Tang et al. measured gene expression of peripheral whole blood samples and compared septic and non-septic critically ill patients.39 a set of 50 signature genes yielded prediction accuracy of 91 and 88% amongst the training and validation sets, respectively. Interestingly, compared with the non-septic controls, sep-tic patients had reduced expression of genes involved in immune modulation and inflam-matory response consistent with the evolving observation of septic immune-paralysis or en-dotoxin tolerance. Tang et al. also compared the whole blood leukocyte gene expression profile of patients who had gram-positive and gram-negative sepsis and found no major dif-ferences suggesting that gram positive and gram negative infections share a common host response.40
another strategy used by researchers study-ing expression profiles has been the attempt at septic shock subclass stratification. Wong et al. analyzed whole blood RNA from 98 children and identified 6934 differentially regulated genes.37 these genes generated 10 coordi-nately regulated gene clusters corresponding
receptors, acute-phase transcription factors, proteases, arachidonate metabolites, and oxi-dases. repressed genes included defense re-sponse genes including those associated with co-stimulatory molecules, T and cytotoxic lymphocytes, natural killer (NK) cells, and protein synthesis.
A recent study discovered and defined a novel gene expression profile in blood that defined early sepsis.36 The genes identified were previously shown to be responsible for the well-described phenomenon of endotoxin tolerance in which a second exposure to en-dotoxin elicits a less profound inflammatory and immune response than the first endotoxin exposure. Several other groups have evaluated whole blood or specific leukocyte gene expres-sion as a diagnostic for sepsis.35, 37 these are promising studies that require further valida-tion and larger sample sizes to determine the clinical utility of measurement of leukocyte or monocyte gene expression for diagnosis of sepsis.
Transcriptomics provides another novel ap-proach to sepsis diagnosis (Table I). Whole blood profiling of patients in severe sep-sis using mRNA microarray technology can shed light on the activity of the host inflam-matory response to sepsis. Prucha et al. ana-lyzed whole blood from eight septic patients
Table I.—�Transcriptomic expression profiles showing up- and downregulated genes in studies of human sepsis.Pathway Upregulated Downregulated
Inflammatory tlr1 and 2 37
CD14 37
FPRL1 37
Properdin P factorc1q receptorc3a receptor 1s100a8, s100a12 37
PF4 37
Matrix metallopeptidase-8 (MMP-8)86
TNF 37
TNF receptor 1b 38
Prokineticin 2 38
LPS-induced TNF factor 38
raf-1 38
BMP5 37
Immune regulatory Fc-γ receptor I and IILILRA3, LILRB2, LILRB3 and LILRB4Protein kinase CMAPK14 37or p38, PAK2PI3KSrc, JAK, Ras, Rho15-Hydroxy-PG DH 38
lair 1 38
NFKBIA 38
il-11, -18 37
il-8 38
il-8ra 37
Chemokine ligand 4 38
chitinase-3 38

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 349
that incorporates effects of the host genotype, regulation of gene expression by influences such as organism load, type and location and changes rapidly over time as the sepsis pro-cess evolves so is more dynamic than under-lying host genomic approaches. However, the proteomic approach to sepsis diagnosis has important limitations because it is highly dependent on patient sample, timing of sam-pling, abundance of the protein(s) of interest and patient age.44 Proteomic approaches in-clude SELDI-TOF which involves the ioniza-tion of protein samples bound to a matrix and subsequent spectrometry and Mass Restricted analysis which organizes the ions based on mass to charge ratio. Buhimschi et al. have been instrumental in evaluating amniotic fluid in early onset neonatal sepsis using a SELDI-TOF proteomic profile. Using SELDI and Mass Restricted analysis of 104 amniotic fluid samples aimed at 4 four distinctive proteins, neutrophil defensins-1 and -2, and calgranu-lins A and C, they devised a mass restricted (MR) score (0-4) based on number of pro-teins present. in blind testing, Mr score >2 provided 100% sensitivity and specificity for detection of intra-amniotic inflammation and was associated with imminent preterm de-livery.45 They then went on to compare MR scores with development of neonatal sepsis, and found a MR score of 3-4 was associated with increased incidence of histologic funisitis and early onset sepsis.46
Proteomics has also been used successfully in studies to define severity of sepsis. For ex-ample, Paiva et al. performed a pilot study in sepsis, severe sepsis and septic shock patients and found 14 differentially expressed proteins according to sepsis classification.47 Amongst those, apo a-i and saa distinguished sepsis and severe sepsis and α-1 antitrypsin and Ig proteins were specific for septic shock.
Other studies in adult sepsis using mass spectrometry sought to identify novel bio-markers by assessing response to exogenous lipopolysaccharide (LPS) administration.48 in one study 40 429 distinct plasma proteins were quantified and 25 other proteins were observed to change significantly. Studies seeking to
to multiple signaling and metabolic pathways and from there they were able to stratify the patients into three putative subclasses that cor-responded to phenotypic outcomes. Studies like this re-confirm the heterogeneous nature of human sepsis and that perhaps previous pivotal trials (e.g. anti-TNF, IL-18a, anti-LPS, intravenous immunoglobulin) failed because they required a more homogeneous selection of patients for inclusion, selected for example by a biomarker.
While in vitro studies looking at endotoxin (lipoploysacchardie) often demonstrate an imbalance of the pro- or anti-inflammatory response, sepsis still remains a heterogenous syndrome and the transcription profile studies ratify the considerable complexity of the re-sponse to sepsis. tang et al. performed a sys-tematic review looking at 12 cohorts and 784 individuals with genome-wide expression data in early and late sepsis and found the changes in inflammatory genes were highly variable.41 Established inflammatory markers including TNF-α, IL-1 and IL-10 did not show any con-sistent pattern even after stratified by timing in sepsis, patient group or setting. Further stud-ies evaluating expression profile between sur-vivors and non-survivors have identified IL-8 with a 95% negative predictive value for mor-tality in pediatric septic shock patient.42
Septic shock associated acute kidney injury (SSAKI) is another condition that is often dif-ficult to predict and SSAKI is associated with an increased mortality compared to patients with sepsis without SSAKI. Basu et al. identi-fied 21 unique up regulated genes using mi-croarray technology in pediatric patients with SSAKI versus patients without SSAKI.43 this gene expression array predicted SSAKI with a 98% sensitivity and 80% specificity. Using two specific genes, metalloproteinase-8 and elastase-2, the investigators demonstrated a sensitivity of 100% and negative predictive value of 95%.
Proteomics technology provides yet an-other novel molecular strategy for the diag-nosis of sepsis but there are pros and cons to proteomics in sepsis. The pros include that assessment of proteomics yields information

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
350 MiNerVa aNestesiologica March 2016
associated with poor outcomes in adult and neonatal sepsis.53, 54 Some TNF-α polymor-phisms interestingly may be associated with the altered TNF-α production. The TNF-α pro-moter region SNP polymorphism at position 308 can confer either high (A) or low (G) gene transcription.55 the -308 a allele is associated with increased susceptibility to and mortality from septic shock in adults and children. TNF levels or the TNF-α -308 polymorphism could be used as a predictive biomarker to better de-fine responders to specific anti-TNF-α strate-gies (e.g. anti- TNF-α antibodies) or soluble TNF-α receptors.56-58
Similar approaches have been used for many candidate gene studies in sepsis. How-ever, in general most candidate gene studies have suffered from relatively small sample sizes, from lack of validation and often from lack of evidence of genomic mechanisms and biologic plausibility. esposito et al. looked at 47 SNPs of 18 candidate genes in 98 pre-term neonates with clinical sepsis and found geno-types associated with IL-1β and MMP-16 were associated with the risk of developing sepsis and genotypes associated with BPI and DEFβ1 were associated with reduced risk.59 Moreover genotypes in CD14 and IL-8 were associated with severe sepsis and LTA and BPI with in-creased risk of gram negative sepsis.
Several examples of gene association studies in sepsis are shown in Table II. We have evalu-ated and found associations of SNPs of inflam-matory, coagulation and innate immunity genes with altered outcomes of sepsis.60-66 Several of these discoveries if validated could ultimately guide use of vasopressors such as norepineph-rine, vasopressin and angiotensin II.63, 67-69
on contrast to candidate gene association studies of specific genes of known or possible interest in a condition, the era of the gWas has allowed a non-biased approach to evalu-ation of SNPs across the human genome. gWas studies yield insights into the breadth of genomic risks for sepsis and show that there are many novel pathways involved including pathways that were never suspected in sep-sis. to date there has been only one published gWas in sepsis.70
differentiate SIRS from sepsis using immu-nodepletion followed by mass spectrometry identified significant multi-fold changes in 10 proteins.49 Another group evaluated immuno-depleted plasma from healthy volunteers and compared that with severe sepsis or septic shock patients who had Acinetobacter bauman-nii.50 There were 19 differentially expressed proteins that are involved in inflammation, coagulation, apoptosis and oxidative stress. cao et al. used a semiquantitative plasma pro-teomic workflow coupled to high-resolution mass spectrometry to identify 772 proteins, of which 58 of them exhibited a statistically sig-nificant difference in expression level amongst patients with sepsis as a function of age.51
Urinary proteomics is another emerging non-invasive approach for sepsis diagnosis. Su et al. analyzed the urine in 15 sepsis and 15 SIRS patients and identified 130 proteins.52 of those, 34 were differentially expressed (>1.5-fold) and were involved in inflammation, im-munity and structural or cytoskeletal process-es.
Prediction of response to therapies
There are many predictive biomarkers for drugs used in other fields such as cancer and cardiovascular disease that define which pa-tients will respond to a drug (efficacy predic-tive biomarker) or who will have an adverse event (safety predictive biomarker). We review some sepsis prognostic genomic biomarkers (i.e. to estimate prognosis) as a prelude to then discussing potential predictive biomarkers. Unfortunately, suffice it to say that there are no approved or clinically used predictive genomic biomarkers for use of drugs in sepsis.
One simple example illustrates the objec-tive. If sepsis represents the imbalance be-tween pro- and anti-inflammatory biomarkers such as plasma cytokines in the response to an invading organism, then SNPs of cytokines such as tumor necrosis factor alpha (TNF-α) could be strong candidate predictive biomark-ers in sepsis for drugs that alter TNF-α. As background, it is relevant to emphasize that elevated serum concentrations of TNF-α are

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 351
better identify responders to this drug which was pulled from the market in 2012 because of the negative results of the PROWESS SHOCK trial.73
Studies of biomarkers relevant to activated protein c used another clinical application of
Activated protein C was the only approved drug for sepsis because of the originally posi-tive results of the PROWESS trial.71 Several groups formed a collaboration to identify and validate genomic biomarkers for response to activated protein C.72 such an approach could
Table II.—�Genetic association studies in human sepsis.103
Pathway genes Comment
Pattern recognition receptors CD14 GG of rs2569190 with increased risk of severe sepsis 58
tlr2 rs3804099 associated with neonatal sepsis and gram positive infections 104
tlr4 Asp299Gly/Thr399Ile – more severe sepsis and Gram-negative
infections 103
tlr5 rs5744105 associated with neonatal sepsis 104
intracellular signaling proteins IRAK1Pro-inflammatory IL-1α rs1800587 associated with sepsis susceptibility
IL-1β CT and TT of rs1143643 with increased risk of sepsis 58
rs143634 TT genotype associated with decreased risk of sepsis 105
il-6 G-174C – Possible association of GG genotype with improved survival 106
Lymphotoxin-alpha (LTA) rs1800629-AG associated with susceptibility to sepsis 107
CD86 rs17281995G/C associated with pneumonia induced sepsis 108
TNF-α TNF-308 – TNF-2 allele associated with increased susceptibility and mortality 109
TNF-β TNF NcoI – TNF-β2 allele associated with susceptibility to sepsis and poor outcome 110
FcγR FcRIIa-R131, FcRIIIa-F158, FcRIIIb-NA2 – deficient phenotype associated with increased susceptibility and mortality 111
Anti-inflammatory il-10 rs1800896 associated with neonatal sepsis and gram negative infections 104
IL-1 receptor antagonist (IL-RA) VNTR polymorphism with increased sepsis susceptibility 105
Chemokines il-8 AT of rs4073 with increased risk of severe sepsis 58
CXCL10endothelial PAI-1 4G/5G – Strong association of PAI-1 4G allele with
poor outcome from sepsis 112
ace I/D – DD genotype is associated with higher mortality 113
others Bactericidal-permeability increasing protein (BPI)
rs4358188-AG associated with reduced susceptibility to sepsis 58
Taq GG and 216 AG or GG associated with gram negative sepsis and death 114
Mannose binding lectin (MBL) Exon1 (AB/BB) associated with the risk of sepsis in neonates 115
Matrix metalloproteinase-16 (MMP-16) GG of rs2664349GG with increased risk of sepsis 58
serpine1Heat shock protein 12ARing finger protein 175Phospholipase A2, Group IIA (PLA-2G2A)
rs1891320 associated with sepsis in neonates and gram positive infections 104

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
352 MiNerVa aNestesiologica March 2016
sepsis. recently, Hung et al. performed a tran-scriptomic retrospective analysis of steroid use in pediatric septic shock.77 Although there was no difference in illness severity, organ failure or mortality, there were 319 genes differen-tially regulated between the groups, predomi-nately related to down regulation involving adaptive immunity. Shanley et al. conducted longitudinal expression profiles of signaling pathways and gene networks in children with septic shock.78 Multiple gene networks involv-ing T cell and MHC antigen presentation were downregulated on days one and three along with genes related to zinc homeostasis.
While the utility of this genomic informa-tion, remains a work in progress, there can be no denying the insight it has provided use and possible a direction for the future. in an era, that is evolving more and more to include the use of immunomodulatory therapies, under-standing the heterogeneity of sepsis and where and when to intervene may serve vital.
Biomarkers could be used to guide use of and weaning of devices used for support of patients with sepsis. For example, plasma lev-els of Brain Natriuretic Peptide (BNP) are in-creased because of volume overload and also increases in response to weaning from mechan-ical ventilation. Accordingly, a recent well-designed randomized controlled trial showed that a BNP-guided protocol for weaning from mechanical ventilation was superior to a con-ventional clinical weaning protocol.79, 80
Prognostic biomarkers
There is a very large literature of prognos-tic biomarkers (protein, mRNA expression and genomic) in sepsis (Table III). Prognostic bio-markers could be used to estimate prognosis and then triage patients and advise families and other care-givers. Prognostic biomarkers can also be used as a bridge to discovery of novel therapeutics and novel predictive bio-markers.
We have recently shown that genotype of proprotein convertase subtilisin/kexin type 9 (PCSK9), an enzyme involved in cholesterol homeostasis, is associated with outcome of
genomic data: the combination of genomic biomarkers analysis with clinical variables to discover novel predictive biomarker(s). Man et al. conducted a GWAS of the PROWESS ran-domized controlled trial of activated protein C in severe sepsis to discover first, biomarkers associated with response to therapy with ac-tivated protein C and second, prognosis of se-vere sepsis.70 While prognosis was dominated by clinical variables including creatinine clear-ance, APACHE II, age and protein C levels, a combination of genetic markers each con-sidered clinically meaningful (ARR>12.5%) were analyzed to assess the response to treat-ment with activated protein C. Survival anal-ysis was completed for the top combination markers that were associated with a favorable treatment response of 41.7% ARR (original ARR of 6.1%). However, none of the genomic markers achieved statistical significance for predicting response to activated protein C. As an aside but relevant, plasma levels of protein C were also not a significant predictive bio-marker of response to activated protein C in PROWESS SHOCK.73
Studies in neonatal sepsis have found a strong correlation between birth weights, gestational age, duration of rupture of mem-branes and clinical chorioamnionitis along with polymorphisms in various inflammatory and anti-inflammatory cytokine genes for in-creased risk of development of sepsis. Such an approach could be coupled with studies of response to drugs used in neonatal sepsis to discover and validate predictive biomark-ers for neonatal sepsis. Whether future sepsis prediction models will incorporate various ge-netic polymorphisms remains to be seen. Fur-thermore, whether prenatal screening should include various inflammatory genes, includ-ing TNF and TNF receptor (TNFR), which are associated with clinical disease remains to be evaluated.74
the use of corticosteroids in sepsis re-mains very controversial because of conflict-ing results of the positive French trial 75 and the negative CORTICUS trial.76 as a result, some investigators seek to identify predictive biomarker(s) for response to corticosteroids in

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 353
regulated in survivors participated in innate immunity including cytokines, chemokine receptors and toll-receptor pathway effectors. Another study in pediatric septic shock found that amongst the 63 gene probes differentiating survivors from non-survivors, two isoforms of metallothionein (MT) a protein involved in zinc sequestration had increased expression in the non-survivors.86 Metalloproteinase-8 has emerged as a potential biomarker with strong correlation with organ failure and decreased survival along with a strong negative predic-tive value in adult and pediatric cohorts and pharmacologic blockade of metalloprotein-ase-8 is now being investigated.87
Protein expression and proteomic approach-es are also growing in sepsis. Kalenka et al. us-ing proteome analysis and gel electrophoresis studied the sera from survivors and non-survi-vors of sepsis and septic shock.88 Six proteins were differentially expressed including Chain A (Bb segment of factor B), complement factor B, alpha-a-B-glycoprotein, haptoglobin, clus-terin in two spots. Triantafilou et al. performed affinity chromatography and mass spectrom-etry analysis of LPS- and LTA (lipotechoic
sepsis, with cytokine response to sepsis, and that in sepsis animal models (cecal ligation and perforation) PCSK9 knock-out mice and mice post-treated with an antibody to PCSK9 have better outcomes.81 This is an example of how a genomic biomarker of outcome of sepsis was bridged first to discovery of a new therapeutic (anti-PCSK9) and second, a novel predictive genomic biomarker (i.e. genotype of PCSK9).82 In genomics, one well studied example is, the associations between TNF-α and -β and the outcome of sepsis.83 The TNF-α promoter 308 A is associated with suscepti-bility to and mortality from sepsis in adults and children. Furthermore, the AA or AG genotypes are associated with 5-fold greater mortality than the GG genotype in ventilated VLBW infants who develop bacteremia or fungemia.84
Examples of mRNA expression to estimate prognosis are growing in the literature. Com-paring mRNA expression patterns of survivors and non-survivors of septic shock, Pachot et al. found 28 genes that discriminated between the two with 100% sensitivity and 86% speci-ficity.85 Interestingly, many of the genes up-
Table III.—�Proteomic profiling of up- and dowregulated proteins in studies of human sepsis.Pathway Upregulated Downregulated
Inflammatory Serum amyloid A and A2 47
C-reactive protein 47
C-reactive protein precursor 48
Hypothetical Protein FLJ21294 47
LPS-binding protein 47
Vascular endothelial cadherin 47
Vitamin K-dependent protein C 47
soluble adenylyl cyclase 47
Utrophin 47
Kininogen 49
Glial fibrillary acidic protein 47
Peroxisomal carnitive octanoyltransferase 47
Β globin 47
coagulation vWF 47
Plasminogen precursor 48
Fibrinogen 49
Antithrombin-III precursor (ATIII) (PRO0309) 48
Antithrombin II 49
Lipid metabolism Apolipoprotein A-II precursor (Apo-AII) 48 Apolipoprotein A-I precursor (Apo-AI) 48
Complement c4 48
c3 49
Plasma protease C1 inhibitor precursor (C1 Inh) 48
other Serum amyloid P-component precursor (SAP) (9.5S Alpha-1-glycoprotein) 48
Transthyretin precursor (prealbumin) (TBPA) (TTR) (ATTR) 48
transthyretin 49
Serum amyloid A-4 protein precursor (constitutively expressed serum amyloid A) (C-SAA) 48
apoptosis α2-HS glycoprotein 49
Oxidative stress gst M1 49

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
354 MiNerVa aNestesiologica March 2016
tion rules into clinical practice.102 these stan-dards include: 1) outcome – clearly defined and clinically important; 2) predictive variable; 3) patient age and sex; 4) study site described; 5) mathematical techniques described. Both the outcome and predictive variable should be validated with a blind assessment prior to knowledge of outcome and evaluated in pro-spective studies (cohort, case/control, or ran-domized controlled trials as appropriate). If we were to adapt Wasson’s principles to cur-rently available genomic biomarkers, we still have inadequate data to adopt them into the surviving sepsis guidelines and clinical prac-tice.
Conclusions
There are few if any well-validated bio-markers in sepsis, whether genomic, expres-sion of mRNA or proteomic. Major problems include inadequate sample sizes of studies, lack of validation cohorts, inadequate under-standing of biologic plausibility in many cases and virtually no prospective randomized controlled trials that include predictive bio-markers of drug response. We suggest strongly as have others,103 that the abject failure of drug development in sepsis could be improved by appropriate use of predictive biomarkers to define a homogeneous population who are more likely to respond to a drug. Furthermore, as pathogens become more resistant, there is greater need for antibiotic stewardship which means that methods for rapid accurate diagno-sis followed by narrow spectrum antimicrobial treatment is better not only for the individual, but for society. While currently logistics, cost and practical considerations limit our ability to sample thousands of genes and then apply complex bioinformatics to define algorithms to drive clinical decision making, the sci-ence will evolve to allow sepsis to become a molecular medicine like cancer therapeutics. Almost more importantly than the data, the Human Genome Project has provided us the science to evaluate genomics so that genom-ics becomes simpler, more refined and cheaper over time.
acid; gram positive bacteria) binding serum proteins 89 in a study of 25 critically-ill pa-tients with a mortality rate of 40%. They found significantly higher levels of apolipoprotein, albumin, LDL, transferring and holotransfer-rin in survivors than non-survivors. Urinary proteomics has also been used to prognosticate in sepsis. su et al. found five proteins upregu-lated including selenium binding protein-1, heparin sulfate proteoglycan-2, alpha-1-B gly-coprotein, haptoglobin and lipocalin; and two proteins downregulated; lysosome-associated membrane proteins-1 and dipeptidyl pepti-dase-4.90
Although considered the newest field of gene product profiling, metabolomics has been around for centuries (e.g. glucose detec-tion in urine to diagnose diabetes mellitus). The invention of gas chromatography-mass spectrometry (GS-MS) and more recently nuclear magnetic resonance (NMR) spectros-copy has revolutionized the field of metabolo-mics and its utility is now emerging clinically. Using NMR based metabolic phenotyping, studies have shown a remarkable ability to identify patients that will develop sepsis and acute lung injury (ALI) and to discriminate SIRS from sepsis.91-97 Studies exploring sep-sis have found that the metabolomic and tran-scriptomic changes that characterize severe infections and death include impaired mito-chondrial, peroxisomal and liver functions.98 A number of studies have examined the global metabolomic profile in plasma and compared survivors to non-survivors after ICU admis-sion, with community acquired pneumonia or sepsis.99-101 Several small molecules differ significantly between survivors and non-sur-vivors that involve pathways related to oxi-dative stress, bile acid metabolism and stress response, and metabolism of lipids, amino ac-ids, carbohydrates, nucleotides and peptides. Although metabolomics has shown remark-able early results, further clinical studies are needed to validate the discoveries related to diagnosis and prognostication of outcome of sepsis.
Wasson et al. in 1995 described methodo-logical standards for adopting clinical predic-

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 355
H, opal sM, et al.; Surviving Sepsis Campaign Guide-lines Committee. Surviving Sepsis Campaign: interna-tional guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39:165-228.
12. Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a sys-tematic review and meta-analysis. Lancet Infect Dis 2013;13:426-35.
13. Lindstrom ST, Wong EK. Procalcitonin, a valuable bi-omarker assisting clinical decision-making in the man-agement of community-acquired pneumonia. Intern Med J 2014;44:390-7.
14. Bishop BM, Bon JJ, Trienski TL, Pasquale TR, Martin BR, File TM, Jr. Effect of introducing procalcitonin on antimicrobial therapy duration in patients with sepsis and/or pneumonia in the intensive care unit. Ann Phar-macother 2014;48:577-83.
15. Heyland DK, Johnson AP, Reynolds SC, Muscedere J. Procalcitonin for reduced antibiotic exposure in the criti-cal care setting: a systematic review and an economic evaluation. Crit Care Med 2011;39:1792-9.
16. Division of Genomic Medicine, National Human Genome Research Institute. A Catalog of Published Genome-Wide Association Studies [Internet]. Available from: www.ge-nome.gov/gwastudies/ [cited 2016, Jan 14].
17. Maslove DM, Wong HR. Gene expression profiling in sepsis: timing, tissue, and translational considerations. Trends Mol Med 2014;20:204-13.
18. Gygi SP, Rochon Y, Franza BR, Aebersold R. Correlation between protein and mRNA abundance in yeast. Mol Cell Biol 1999;19:1720-30.
19. Liesenfeld O, Lehman L, Hunfeld KP, Kost G. Molecu-lar diagnosis of sepsis: New aspects and recent develop-ments. Eur J Microbiol Immunol (Bp) 2014;4:1-25.
20. Josefson P, Stralin K, Ohlin A, Ennefors T, Dragsten B, andersson l, et al. Evaluation of a commercial multi-plex PCR test (SeptiFast) in the etiological diagnosis of community-onset bloodstream infections. Eur J Clin Microbiol Infect Dis 2011;30:1127-34.
21. Mancini N, Carletti S, Ghidoli N, Cichero P, Burioni R, Clementi M. The era of molecular and other non-culture-based methods in diagnosis of sepsis. Clin Microbiol Rev 2010;23:235-51.
22. Zerva L, Bourantas K, Mitka S, Kansouzidou A, Legakis NJ. Serum is the preferred clinical specimen for diag-nosis of human brucellosis by PCR. J Clin Microbiol 2001;39:1661-4.
23. Cleven BE, Palka-Santini M, Gielen J, Meembor S, Kro-nke M, Krut O. Identification and characterization of bac-terial pathogens causing bloodstream infections by DNA microarray. J Clin Microbiol 2006;44:2389-97.
24. Shang S, Chen G, Wu Y, Du L, Zhao Z. Rapid diag-nosis of bacterial sepsis with PCR amplification and microarray hybridization in 16S rRNA gene. Pediatr Res 2005;58:143-8.
25. Lehmann LE, Hunfeld KP, Steinbrucker M, Brade V, Book M, Seifert H, et al. Improved detection of blood stream pathogens by real-time PCR in severe sepsis. In-tensive Care Med 2010;36:49-56.
26. Herne V, Nelovkov A, Kutt M, Ivanova M. Diagnos-tic performance and therapeutic impact of LightCycler SeptiFast assay in patients with suspected sepsis. Eur J Microbiol Immunol (Bp) 2013;3:68-76.
27. Bloos F, Hinder F, Becker K, Sachse S, Mekontso Dessap a, straube e, et al. A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis. Intensive Care Med 2010;36:241-7.
28. Kelley PG, Grabsch EA, Farrell J, Xie S, Montgomery J, Mayall B, et al. Evaluation of the Xpert MRSA/SA Blood culture assay for the detection of staphylococcus aureus
Key messages — Genomics is the discipline in genet-
ics that applies recombinant DNA, DNA sequencing methods, and bioinformatics to sequence, assemble, and analyze the func-tion and structure of genomes (the com-plete set of DNA within a single cell of an organism).
— The molecular mechanisms of sepsis can now be investigated using advanced tools including genomics, transcriptomics, proteomics, metabolomics and protein im-munoassays.
— in sepsis, the potential uses of bio-markers include diagnosis, in differen-tiating viral from bacterial infection, in differentiating an inflammatory from an infectious process, prognostication, and in predicting response to treatment (efficacy and safety) and in predicting relapse.
References
1. Vincent JL, Opal SM, Marshall JC, Tracey KJ. Sepsis definitions: time for change. Lancet 2013;381:774-5.
2. Stevenson EK, Rubenstein AR, Radin GT, Wiener RS, Walkey AJ. Two decades of mortality trends among pa-tients with severe sepsis: a comparative meta-analysis. Crit Care Med 2014;42:625-31.
3. Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zea-land, 2000-2012. JAMA 2014;311:1308-16.
4. Peake SL, Delaney A, Bailey M, Bellomo R, Cameron PA, Cooper DJ, et al. goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014;371:1496-506.
5. Pro CI, Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld la, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med 2014;370:1683-93.
6. Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Mas-sone R, Furia FF, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med 2010;38:1045-53.
7. Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther 2001;69:89-95.
8. Pierrakos C, Vincent JL. Sepsis biomarkers: a review. Crit Care 2010;14:R15.
9. Sorensen TI, Nielsen GG, Andersen PK, Teasdale TW. Genetic and environmental influences on premature death in adult adoptees. N Engl J Med 1988;318:727-32.
10. Public Health Genomic Implementation. Center for Dis-ease Control and Prevention [Internet]. Available from: www.cdc.gov/genomics/ [cited 2016, Jan 14].
11. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach
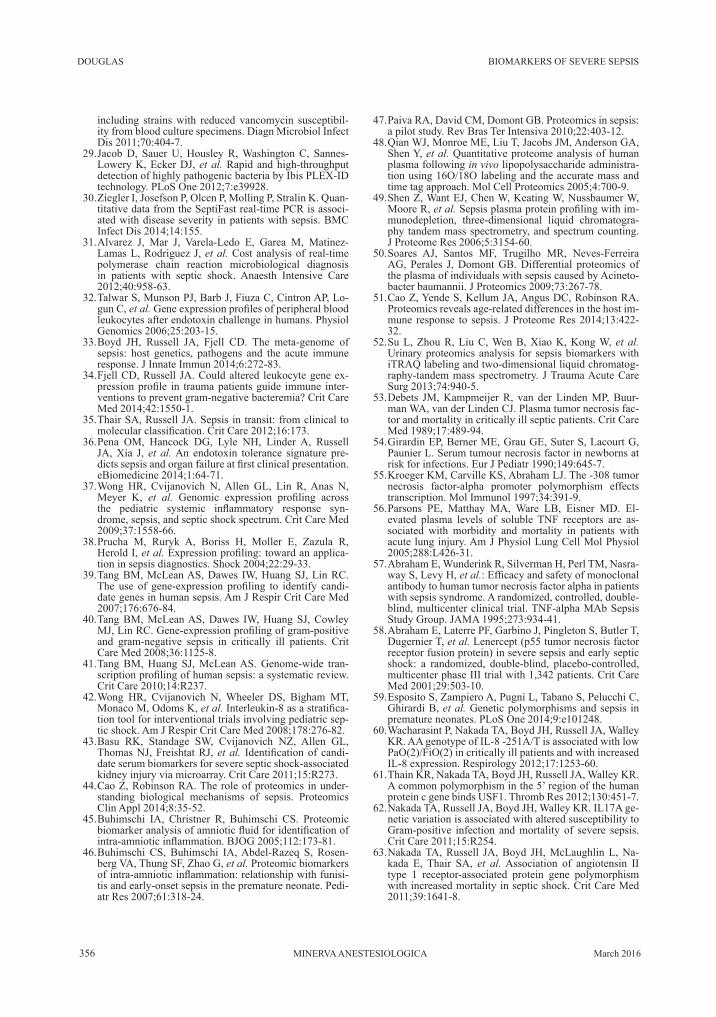
DOUGLAS BIOMARKERS OF SEVERE SEPSIS
356 MiNerVa aNestesiologica March 2016
47. Paiva RA, David CM, Domont GB. Proteomics in sepsis: a pilot study. Rev Bras Ter Intensiva 2010;22:403-12.
48. Qian WJ, Monroe ME, Liu T, Jacobs JM, Anderson GA, shen Y, et al. Quantitative proteome analysis of human plasma following in vivo lipopolysaccharide administra-tion using 16O/18O labeling and the accurate mass and time tag approach. Mol Cell Proteomics 2005;4:700-9.
49. Shen Z, Want EJ, Chen W, Keating W, Nussbaumer W, Moore r, et al. Sepsis plasma protein profiling with im-munodepletion, three-dimensional liquid chromatogra-phy tandem mass spectrometry, and spectrum counting. J Proteome Res 2006;5:3154-60.
50. Soares AJ, Santos MF, Trugilho MR, Neves-Ferreira AG, Perales J, Domont GB. Differential proteomics of the plasma of individuals with sepsis caused by Acineto-bacter baumannii. J Proteomics 2009;73:267-78.
51. Cao Z, Yende S, Kellum JA, Angus DC, Robinson RA. Proteomics reveals age-related differences in the host im-mune response to sepsis. J Proteome Res 2014;13:422-32.
52. Su L, Zhou R, Liu C, Wen B, Xiao K, Kong W, et al. Urinary proteomics analysis for sepsis biomarkers with iTRAQ labeling and two-dimensional liquid chromatog-raphy-tandem mass spectrometry. J Trauma Acute Care Surg 2013;74:940-5.
53. Debets JM, Kampmeijer R, van der Linden MP, Buur-man WA, van der Linden CJ. Plasma tumor necrosis fac-tor and mortality in critically ill septic patients. Crit Care Med 1989;17:489-94.
54. Girardin EP, Berner ME, Grau GE, Suter S, Lacourt G, Paunier L. Serum tumour necrosis factor in newborns at risk for infections. Eur J Pediatr 1990;149:645-7.
55. Kroeger KM, Carville KS, Abraham LJ. The -308 tumor necrosis factor-alpha promoter polymorphism effects transcription. Mol Immunol 1997;34:391-9.
56. Parsons PE, Matthay MA, Ware LB, Eisner MD. El-evated plasma levels of soluble TNF receptors are as-sociated with morbidity and mortality in patients with acute lung injury. Am J Physiol Lung Cell Mol Physiol 2005;288:L426-31.
57. Abraham E, Wunderink R, Silverman H, Perl TM, Nasra-way S, Levy H, et al.: Efficacy and safety of monoclonal antibody to human tumor necrosis factor alpha in patients with sepsis syndrome. A randomized, controlled, double-blind, multicenter clinical trial. TNF-alpha MAb Sepsis Study Group. JAMA 1995;273:934-41.
58. Abraham E, Laterre PF, Garbino J, Pingleton S, Butler T, Dugernier T, et al. Lenercept (p55 tumor necrosis factor receptor fusion protein) in severe sepsis and early septic shock: a randomized, double-blind, placebo-controlled, multicenter phase III trial with 1,342 patients. Crit Care Med 2001;29:503-10.
59. Esposito S, Zampiero A, Pugni L, Tabano S, Pelucchi C, Ghirardi B, et al. Genetic polymorphisms and sepsis in premature neonates. PLoS One 2014;9:e101248.
60. Wacharasint P, Nakada TA, Boyd JH, Russell JA, Walley KR. AA genotype of IL-8 -251A/T is associated with low PaO(2)/FiO(2) in critically ill patients and with increased IL-8 expression. Respirology 2012;17:1253-60.
61. Thain KR, Nakada TA, Boyd JH, Russell JA, Walley KR. A common polymorphism in the 5’ region of the human protein c gene binds USF1. Thromb Res 2012;130:451-7.
62. Nakada TA, Russell JA, Boyd JH, Walley KR. IL17A ge-netic variation is associated with altered susceptibility to Gram-positive infection and mortality of severe sepsis. Crit Care 2011;15:R254.
63. Nakada TA, Russell JA, Boyd JH, McLaughlin L, Na-kada E, Thair SA, et al. association of angiotensin ii type 1 receptor-associated protein gene polymorphism with increased mortality in septic shock. Crit Care Med 2011;39:1641-8.
including strains with reduced vancomycin susceptibil-ity from blood culture specimens. Diagn Microbiol Infect Dis 2011;70:404-7.
29. Jacob D, Sauer U, Housley R, Washington C, Sannes-Lowery K, Ecker DJ, et al. rapid and high-throughput detection of highly pathogenic bacteria by Ibis PLEX-ID technology. PLoS One 2012;7:e39928.
30. Ziegler I, Josefson P, Olcen P, Molling P, Stralin K. Quan-titative data from the SeptiFast real-time PCR is associ-ated with disease severity in patients with sepsis. BMC Infect Dis 2014;14:155.
31. Alvarez J, Mar J, Varela-Ledo E, Garea M, Matinez-Lamas L, Rodriguez J, et al. Cost analysis of real-time polymerase chain reaction microbiological diagnosis in patients with septic shock. Anaesth Intensive Care 2012;40:958-63.
32. Talwar S, Munson PJ, Barb J, Fiuza C, Cintron AP, Lo-gun c, et al. Gene expression profiles of peripheral blood leukocytes after endotoxin challenge in humans. Physiol Genomics 2006;25:203-15.
33. Boyd JH, Russell JA, Fjell CD. The meta-genome of sepsis: host genetics, pathogens and the acute immune response. J Innate Immun 2014;6:272-83.
34. Fjell CD, Russell JA. Could altered leukocyte gene ex-pression profile in trauma patients guide immune inter-ventions to prevent gram-negative bacteremia? Crit Care Med 2014;42:1550-1.
35. Thair SA, Russell JA. Sepsis in transit: from clinical to molecular classification. Crit Care 2012;16:173.
36. Pena OM, Hancock DG, Lyle NH, Linder A, Russell JA, Xia J, et al. An endotoxin tolerance signature pre-dicts sepsis and organ failure at first clinical presentation. eBiomedicine 2014;1:64-71.
37. Wong HR, Cvijanovich N, Allen GL, Lin R, Anas N, Meyer K, et al. Genomic expression profiling across the pediatric systemic inflammatory response syn-drome, sepsis, and septic shock spectrum. Crit Care Med 2009;37:1558-66.
38. Prucha M, Ruryk A, Boriss H, Moller E, Zazula R, Herold i, et al. Expression profiling: toward an applica-tion in sepsis diagnostics. Shock 2004;22:29-33.
39. Tang BM, McLean AS, Dawes IW, Huang SJ, Lin RC. The use of gene-expression profiling to identify candi-date genes in human sepsis. Am J Respir Crit Care Med 2007;176:676-84.
40. Tang BM, McLean AS, Dawes IW, Huang SJ, Cowley MJ, Lin RC. Gene-expression profiling of gram-positive and gram-negative sepsis in critically ill patients. Crit Care Med 2008;36:1125-8.
41. Tang BM, Huang SJ, McLean AS. Genome-wide tran-scription profiling of human sepsis: a systematic review. Crit Care 2010;14:R237.
42. Wong HR, Cvijanovich N, Wheeler DS, Bigham MT, Monaco M, Odoms K, et al. Interleukin-8 as a stratifica-tion tool for interventional trials involving pediatric sep-tic shock. Am J Respir Crit Care Med 2008;178:276-82.
43. Basu RK, Standage SW, Cvijanovich NZ, Allen GL, Thomas NJ, Freishtat RJ, et al. Identification of candi-date serum biomarkers for severe septic shock-associated kidney injury via microarray. Crit Care 2011;15:R273.
44. Cao Z, Robinson RA. The role of proteomics in under-standing biological mechanisms of sepsis. Proteomics Clin Appl 2014;8:35-52.
45. Buhimschi IA, Christner R, Buhimschi CS. Proteomic biomarker analysis of amniotic fluid for identification of intra-amniotic inflammation. BJOG 2005;112:173-81.
46. Buhimschi CS, Buhimschi IA, Abdel-Razeq S, Rosen-berg VA, Thung SF, Zhao G, et al. Proteomic biomarkers of intra-amniotic inflammation: relationship with funisi-tis and early-onset sepsis in the premature neonate. Pedi-atr Res 2007;61:318-24.

BIOMARKERS OF SEVERE SEPSIS DOUGLAS
Vol. 82 - No. 3 MiNerVa aNestesiologica 357
innate immune response and septic shock outcome. Sci Transl Med 2014;6:258ra143.
82. Dos Santos C, Marshall JC. Bridging lipid metabolism and innate host defense. Sci Transl Med 2014;6:258fs41.
83. Schueller AC, Heep A, Kattner E, Kroll M, Wisbauer M, sander J, et al. Prevalence of two tumor necrosis factor gene polymorphisms in premature infants with early on-set sepsis. Biol Neonate 2006;90:229-32.
84. Hedberg CL, Adcock K, Martin J, Loggins J, Kruger TE, Baier RJ. Tumor necrosis factor alpha -- 308 polymor-phism associated with increased sepsis mortality in ven-tilated very low birth weight infants. Pediatr Infect Dis J 2004;23:424-8.
85. Pachot A, Lepape A, Vey S, Bienvenu J, Mougin B, Mon-neret G. Systemic transcriptional analysis in survivor and non-survivor septic shock patients: a preliminary study. Immunol Lett 2006;106:63-71.
86. Wong HR, Shanley TP, Sakthivel B, Cvijanovich N, lin r, allen gl, et al. Genome-level expression pro-files in pediatric septic shock indicate a role for altered zinc homeostasis in poor outcome. Physiol Genomics 2007;30:146-55.
87. Solan PD, Dunsmore KE, Denenberg AG, Odoms K, Zin-garelli B, Wong HR. A novel role for matrix metallopro-teinase-8 in sepsis. Crit Care Med 2012;40:379-87.
88. Kalenka A, Feldmann RE Jr., Otero K, Maurer MH, Waschke KF, Fiedler F. Changes in the serum proteome of patients with sepsis and septic shock. Anesth Analg 2006;103:1522-6.
89. Triantafilou M, Mouratis MA, Lepper PM, Haston RM, Baldwin F, Lowes S, et al. Serum proteins modulate lipopolysaccharide and lipoteichoic acid-induced acti-vation and contribute to the clinical outcome of sepsis. Virulence 2012;3:136-45.
90. Su L, Cao L, Zhou R, Jiang Z, Xiao K, Kong W, et al. Identification of novel biomarkers for sepsis prognosis via urinary proteomic analysis using iTRAQ labeling and 2D-LC-MS/MS. PLoS One 2013;8:e54237.
91. Blaise BJ, Gouel-Cheron A, Floccard B, Monneret G, Allaouchiche B. Metabolic phenotyping of traumatized patients reveals a susceptibility to sepsis. Anal Chem 2013;85:10850-5.
92. Kamisoglu K, Sleight KE, Calvano SE, Coyle SM, Corbett SA, Androulakis IP. Temporal metabolic pro-filing of plasma during endotoxemia in humans. Shock 2013;40:519-26.
93. Mickiewicz B, Vogel HJ, Wong HR, Winston BW. Me-tabolomics as a novel approach for early diagnosis of pediatric septic shock and its mortality. Am J Respir Crit Care Med 2013;187:967-76.
94. Schmerler D, Neugebauer S, Ludewig K, Bremer-Streck S, Brunkhorst FM, Kiehntopf M. Targeted metabolomics for discrimination of systemic inflammatory disorders in critically ill patients. J Lipid Res 2012;53:1369-75.
95. Izquierdo-Garcia JL, Nin N, Ruiz-Cabello J, Rojas Y, de Paula M, Lopez-Cuenca S, et al. A metabolomic ap-proach for diagnosis of experimental sepsis. Intensive Care Med 2011 Oct 6. [Epub ahead of print]
96. Stringer KA, Serkova NJ, Karnovsky A, Guire K, Paine r 3rd, standiford tJ. Metabolic consequences of sepsis-induced acute lung injury revealed by plasma (1)H-nu-clear magnetic resonance quantitative metabolomics and computational analysis. Am J Physiol Lung Cell Mol Physiol 2011;300:L4-L11.
97. Hinkelbein J, Feldmann RE Jr, Peterka A, Schubert C, Schelshorn D, Maurer MH, et al. alterations in cerebral metabolomics and proteomic expression during sepsis. Curr Neurovasc Res 2007;4:280-8.
98. Langley RJ, Tipper JL, Bruse S, Baron RM, Tsalik EL, Huntley J, et al. Integrative “omic” analysis of experi-mental bacteremia identifies a metabolic signature that
64. Sutherland AM, Walley KR, Nakada TA, Sham AH, Wur-fel MM, Russell JA. A nonsynonymous polymorphism of IRAK4 associated with increased prevalence of gram-positive infection and decreased response to toll-like re-ceptor ligands. J Innate Immun 2011;3:447-58.
65. Thair SA, Walley KR, Nakada TA, McConechy MK, Boyd JH, Wellman H, et al. A single nucleotide polymor-phism in NF-kappaB inducing kinase is associated with mortality in septic shock. J Immunol 2011;186:2321-8.
66. Wurfel MM, Gordon AC, Holden TD, Radella F, Strout J, Kajikawa O, et al. Toll-like receptor 1 polymorphisms affect innate immune responses and outcomes in sepsis. Am J Respir Crit Care Med 2008;178:710-20.
67. Nakada TA, Russell JA, Boyd JH, Aguirre-Hernandez R, Thain KR, Thair SA, et al. beta2-adrenergic receptor gene polymorphism is associated with mortality in septic shock. Am J Respir Crit Care Med 2010;181:143-9.
68. Nakada TA, Russell JA, Wellman H, Boyd JH, Nakada E, Thain KR, et al. Leucyl/cystinyl aminopeptidase gene variants in septic shock. Chest 2011;139:1042-9.
69. Anantasit N, Boyd JH, Walley KR, Russell JA. Seri-ous adverse events associated with vasopressin and norepinephrine infusion in septic shock. Crit Care Med 2014;42:1812-20.
70. Man M, Close SL, Shaw AD, Bernard GR, Douglas IS, Kaner RJ, et al. Beyond single-marker analyses: mining whole genome scans for insights into treatment responses in severe sepsis. Pharmacogenomics J 2013;13:218-26.
71. Bernard GR, Vincent JL, Laterre PF, LaRosa SP, Dhain-aut JF, Lopez-Rodriguez A, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001;344:699-709.
72. Annane D, Mira JP, Ware LB, Gordon AC, Sevransky J, Stuber F, et al. Design, conduct, and analysis of a mul-ticenter, pharmacogenomic, biomarker study in matched patients with severe sepsis treated with or without drot-recogin Alfa (activated). Ann Intensive Care 2012;2:15.
73. Ranieri VM, Thompson BT, Barie PS, Dhainaut JF, Douglas IS, Finfer S, et al. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med 2012;366:2055-64.
74. Lobito AA, Gabriel TL, Medema JP, Kimberley FC. Disease causing mutations in the TNF and TNFR super-families: Focus on molecular mechanisms driving dis-ease. Trends Mol Med 2011;17:494-505.
75. Annane D, Sebille V, Charpentier C, Bollaert PE, Fran-cois B, Korach JM, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002; 288:862-71.
76. Sprung CL, Annane D, Keh D, Moreno R, Singer M, Freivogel K, et al. Hydrocortisone therapy for patients with septic shock. N Engl J Med 2008;358:111-24.
77. Wong HR, Cvijanovich NZ, Allen GL, Thomas NJ, Fre-ishtat rJ, anas N, et al. corticosteroids are associated with repression of adaptive immunity gene programs in pediatric septic shock. Am J Respir Crit Care Med 2014;189:940-6.
78. Shanley TP, Cvijanovich N, Lin R, Allen GL, Thomas NJ, Doctor A, et al. Genome-level longitudinal expres-sion of signaling pathways and gene networks in pediat-ric septic shock. Mol Med 2007;13:495-508.
79. Russell JA. Biomarker (BNP)-guided weaning from mechanical ventilation: time for a paradigm shift? Am J Respir Crit Care Med 2012;186:1202-4.
80. Mekontso Dessap A, Roche-Campo F, Kouatchet A, Tomicic V, Beduneau G, Sonneville R, et al. Natriuretic peptide-driven fluid management during ventilator wean-ing: a randomized controlled trial. Am J Respir Crit Care Med 2012;186:1256-63.
81. Walley KR, Thain KR, Russell JA, Reilly MP, Meyer NJ, Ferguson JF, et al. PCSK9 is a critical regulator of the

DOUGLAS BIOMARKERS OF SEVERE SEPSIS
358 MiNerVa aNestesiologica March 2016
101. Langley RJ, Tsalik EL, van Velkinburgh JC, Glickman SW, Rice BJ, Wang C, et al. An integrated clinico-metab-olomic model improves prediction of death in sepsis. Sci Transl Med 2013;5:195ra95.
102. Wasson JH, Sox HC, Neff RK, Goldman L. Clinical pre-diction rules. Applications and methodological standards. N Engl J Med 1985;313:793-9.
103. Opal SM, Dellinger RP, Vincent JL, Masur H, Angus DC. The next generation of sepsis clinical trial designs: what is next after the demise of recombinant human activated protein C? Crit Care Med 2014;42:1714-21.
distinguishes human sepsis from systemic inflamma-tory response syndromes. Am J Respir Crit Care Med 2014;190:445-55.
99. Seymour CW, Yende S, Scott MJ, Pribis J, Mohney RP, Bell LN, et al. Metabolomics in pneumonia and sepsis: an analysis of the GenIMS cohort study. Intensive Care Med 2013;39:1423-34.
100. Rogers AJ, McGeachie M, Baron RM, Gazourian L, Haspel JA, Nakahira K, et al. Metabolomic derange-ments are associated with mortality in critically ill adult patients. PLoS One 2014;9:e87538.
Conflicts of interest.—J. A. Russell is a consultant for Cubist Pharmaceuticals, Cyon Therapeutics, Ferring Pharmaceutical, Gri-. A. Russell is a consultant for Cubist Pharmaceuticals, Cyon Therapeutics, Ferring Pharmaceutical, Gri-fols, Leading Bioscience, La Jolla Pharmaceuticals, and MedImmune. He has also received grants from AstraZeneca and Ferring Pharmaceutical, and is a shareholder in Cyon Therapeutics and Leading Bioscience. J. A. Russell has also filed provisional patent applications for PCSK9 in sepsis and vasopressin in septic shock. J. J. Douglas has no conflicts of interest to disclose concerning the content of this manuscript.Article first published online: June 19, 2015. - Manuscript accepted: June 18, 2015. - Manuscript revised: June 16, 2015. - Manuscript received: November 17, 2014.

Vol. 82 - No. 3 MiNerVa aNestesiologica 359
E X P E R T S ’ O P I N I O N
“Why can’t i give you my organs after my heart has stopped beating?”
an overview of the main clinical, organisational, ethical and legal issues concerning organ donation after circulatory death in italy
alberto giaNNiNi 1*, Massimo aBelli 2, giampaolo aZZoNi 3, gianni BiaNcoFiore 4, Franco citterio 5, Paolo geraci 6, Nicola latroNico 7, 8, Mario PicoZZi 9,
Francesco Procaccio 10, luigi riccioNi 11, Paolo rigotti 12, Franco ValeNZa 13, sergio VescoNi 14, Nereo ZaMPeretti 15
on behalf of the Working group on DcD of the italian society of anesthesiology, analgesia and intensive care (siaarti), and the italian society for organ transplantation
1terapia intensiva Pediatrica, Fondazione irccs ca’ granda, ospedale Maggiore Policlinico, Milan, italy; 2Unità trapianto di rene, Dipartimento di chirurgia, Fondazione irccs Policlinico san Matteo, Pavia, italy; 3Dipartimento di giurisprudenza, Università di Pavia, Pavia, italy; 4s. D. anestesia e rianimazione trapianto Fegato, azienda ospedaliera Universitaria Pisana, Pisa, italy; 5trapiantologia renale, Dipartimento di scienze chirurgiche, Policlinico “a. gemelli” Università cattolica del sacro cuore, rome, italy; 6centro coordinamento Donazioni e trapianti, Fondazione irccs Policlinico san Matteo, Pavia, italy; 7Dipartimento di specialità Medico-chirurgiche, scienze radiologiche e sanità Pubblica, Università degli studi di Brescia, 8Dipartimento di anestesia e rianimazione emergenza Urgenza, azienda ospedaliera spedali civili di Brescia, Brescia, italy; 9Dipartimento di Biotecnologie e scienze della Vita, sezione di Medicina legale Università degli studi dell’insubria, Varese, italy; 10centro Nazionale trapianti, istituto superiore di sanità, rome, italy; 11centro per shock e trauma, ospedale san camillo-Forlanini, rome, italy; 12Unità trapianti di rene e Pancreas, azienda ospedaliera di Padova, Università di Padova, Padua, italy; 13Dipartimento di Fisiopatologia e dei trapianti, Università degli studi di Milano, Fondazione irccs ca’ granda, ospedale Maggiore Policlinico, Milan, italy; 14coordinamento Prelievo organi e tessuti, regione lombardia, Direzione generale salute, Milan, italy; 15servizio Qualità, sicurezza ed accreditamento, azienda Ulss n. 6 Vicenza, Vicenza, italy*corresponding author: alberto giannini, Pediatric intensive care Unit, Fondazione irccs ca’ granda – ospedale Maggiore Poli-clinico, Via della commenda 9, 20122 Milan, italy. e-mail: [email protected]
anno: 2016Mese: MarchVolume: 82No: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10470-Mastitolo breve: Donation after circulatory death in italyprimo autore: giaNNiNipagine: 359-68citazione: Minerva anestesiol 2016;82:000-000
a B s t r a c tDonation after circulatory death (DcD) is a valuable option for the procurement of functioning organs for transplantation. clinical results are promising and public acceptance is quite good in most western countries. Yet, although DcD is wide-spread in europe, several problems still persist in italy as well as in some other countries. this paper aims to describe the main clinical, organisational, ethical and legal issues at stake, bearing in mind the particular situation created by italian legislation. currently, as regards DcD, italy is somewhat different from other countries. therefore, every effort should be made for the safe and effective implementation of DcD programs: uncontrolled DcD programs should be promoted and encouraged, within the framework of shared and authoritative rules. at the same time, we need to tackle the question of controlled DcD, promoting debate among all involved subjects regarding the fundamental issues of end-of-life care
Minerva anestesiologica 2016 March;82(3):359-68© 2015 eDiZioNi MiNerVa MeDicathe online version of this article is located at http://www.minervamedica.it

giaNNiNi DoNatioN aFter circUlatorY Death iN italY
360 MiNerVa aNestesiologica March 2016
the clinical pathway that can lead to organ donation was recently coded by the World Health Organization (WHO) in a well-defined algorithm of critical pathways.4 this included both donors whose death has been declared us-ing neurological criteria (donor/donation after brain death, DBD) and those who have been declared dead using cardio-circulatory criteria (donor/donation after circulatory death, DcD). DBD and DcD are replacing the expressions, less common today, heart-beating-donor/dona-tion (hBD) and Non heart-beating-donor/do-nation (NhBD) respectively.
although the history of transplantation started with procurement of organs from non heart-beating subjects, there has recently been renewed, increasing interest in DcD.5, 6 in the period 2000-2008, 5004 organs from DcD were transplanted in europe (4261 kidneys, 505 livers, 157 lungs, 81 pancreases) 7 with en-couraging results, approximately 75% of DcD recovered organs being finally utilized. Trans-plants of kidneys procured from DcD show outcomes comparable to those of DBD. the feasibility of both lung 8 and liver 9 transplants with organs procured from DcD has also been shown, even if data for these organs are pre-liminary. the heart itself may be recovered and utilized from DcD donors, particularly if timely reperfusion is performed in the donor after declaration of death.10, 11
DCD donors were classified into categories after a consensus meeting held in Maastricht in 1995 12. these categories were recently modified during the 6th International Con-ference on organ Donation after circulatory Death organized in Paris in February 2013 (table i). these different categories allow for differentiation of DcD as controlled (cDcD) or uncontrolled (uDcD): “uncontrolled” re-fers mainly to unwitnessed and/or unexpected
Donation after circulatory death (DcD) is a valuable option for the procurement of
functioning organs for transplantation. clini-cal results are promising and public accep-tance is quite fair in most western countries. Yet, in spite of large diffusion in europe, sev-eral problems still persist in italy as well as in some other countries.
the italian society of anesthesiology, an-algesia and intensive care (siaarti) and the italian society for organ transplantation (sito) are particularly involved in this issue and in 2014 a joint multidisciplinary ad hoc Working group (Wg) was activated in cooperation with the ital-ian National transplant centre (cNt), in order to address the various aspects of this subject.
this manuscript presents the report of the WG and consists of two parts: firstly, a de-scription of the current situation of DcD both in italy and in the international context, taking into account the clinical, ethical and organiza-tional aspects; secondly, an outline of the road map for achieving the implementation of DcD programs in italy.
transplantation is often the only treatment for end stage organ failures, such as liver and heart failure, and the most realistic option for organ failures in otherwise fit and healthy indi-viduals, such as those with renal failure.1 how-ever, organs from multi-organ donors available for transplantation are far less than the number of potential recipients, so that many people die while on a waitlist: at December 31, 2014, 8758 patients were on the waitlist, with a mortality ranging from 1.7 (kidney) to 9.2% (lung) per annum.2 For this reason, organ donation from deceased persons has recently been affirmed as “having a fundamental role in maximizing the therapeutic potential of transplantation”.3
within protocols that best integrate the highest standard of care for the dying and the legitimate interests of those awaiting a life-saving organ.(Cite this article as: Giannonio A, Abelli M, Azzoni G, Biancofiore G, Citterio F, Geraci P, et al. “Why can’t i give you my organs after my heart has stopped beating?” an overview of the main clinical, organisational, ethical and legal issues concern-ing organ donation after circulatory death in italy. Minerva anestesiol 2016;82:359-68)Key words: tissue and organ procurement - transplantation - ethics.
comment in p. 271

DoNatioN aFter circUlatorY Death iN italY giaNNiNi
Vol. 82 - No. 3 MiNerVa aNestesiologica 361
and Denmark DcD is not allowed.7 Data for DcD kidney and liver transplantation in 2013 are reported in table ii.14
Ethical issues
the practice of DcD is increasing and pro-tocols are currently applied with good quanti-tative and qualitative results. Yet some ethical issues about DcD are still under discussion.
The first one is the forgoing of life supports. Withdrawing of life-supports is a common fea-ture of end-of-life care both in many european countries and in the Usa,15, 16 although spe-cific standards and laws to guide this practice are frequently absent. in order to reconcile this practice within DcD protocols, the fundamen-tal prerequisite is that the clinical decision to withdraw disproportionate treatments must be clearly independent of the possibility of organ donation. in some countries (for instance in
sudden death from cardiac arrest, both with-in an in-hospital or out-of-hospital setting; “controlled” refers to expected cardiac arrest, mainly following withdrawal of life-sustaining treatment in the intensive care unit (icU).
even if there is general agreement on the concept of DcD, only 16 out of the 27 eu-ropean Union countries (61.5%) defined the determination of circulatory death (death de-clared upon cardio-circulatory criteria) by leg-islation; only in half, death must be mandato-rily confirmed by the use of electrocardiogram (ecg),13 which allows determination of loss of electrical function.
in 2011, DcD was performed in 10 europe-an countries (austria, Belgium, France, italy, the Netherlands, switzerland, latvia, czech republic, spain and the UK). Notably, the Netherlands and Belgium do not have specific rules regulating determination of circulatory death. in germany, Finland, turkey, sweden
Table I.—�Modified European Maastricht categories of donation after circulatory death (DCD) classification.12
category sub-category Description type
Category IUncontrolled Unwitnessed ca
i a – in-hospital sudden-unexpected-irreversible ca; no attempt of resuscitation by a medical team. Wit to be considered according to national recommendations in place. in- or out-of-hospital setting.
Uncontrolledi B – out-of-hospital
Category IIUncontrolled Witnessed ca
ii a – in-hospital sudden-unexpected-irreversible ca; unsuccessful resuscitation by a medical team. in- or out-of-hospital setting
Uncontrolledii B – out-of-hospital
Category IIIcontrolled awaiting circulatory death
— Planned, expected ca; withdrawal of life-sustaining treatment; euthanasia excluded
controlled
Category IValternative death determination during/after procedure
iV a - uncontrolled and controlled ca while brain dead
sudden* or planned** ca during or after brain death diagnosis process, but before retrieval
Uncontrolled* orcontrolled**
iV B - death diagnosis during ecMo-ecls
Death determination by circulatory (DcD) or neurological (DBD) criteria
Partially controlled
ca: cardiac arrest; Wit: warm ischemia time; ecMo: extra-corporeal membrane oxygenation; ecls: extra-corporeal life support
Table II.—�Deceased Cardiac Donation (DCD) organ transplantation in 28 Countries of the European Union (EU) during the year 2013 (“utilized donors”).
austria Belgium czech republic France ireland latvia Netherlands spain UK
italy +18 eU
countries
Kidney 4 78 2 78 11 20 249 200 832 0liver 1 50 0 2 0 0 48 41 146 0(From council of europe, Newsletter transplant, september 1st 2014)

giaNNiNi DoNatioN aFter circUlatorY Death iN italY
362 MiNerVa aNestesiologica March 2016
have exceptionally been reported.23 another problem is the time interval between the loss of cardiac function and the declaration of death (“no-touch period”) which goes from 5 (most european countries) to 20 minutes (italy).24 according to the recommendations of the so-ciety of critical care Medicine (sccM) eth-ics committee, the Us current practice (which relates above all to cDcD) is that “no less than two minutes is acceptable, no more than five minutes is necessary”.25 Yet, the shorter the in-terval between asystole and incision, the great-er the possibility that the irreversible loss of intracranial functions, and hence brain death, has not yet occurred; consequently, death risks being certified using cardio-respiratory criteria when the neurological ones are not yet met for certain. so, it seems that different diagnoses of death exist that clinicians can use at their convenience.26 We wish to emphasize that this is not a problem in italy: the 20 minutes of re-corded absence of cardiac electrical activity guarantees that the whole brain is completely destroyed after such a period of no cerebral blood flow and the dead donor rule is fully re-spected.
controlled protocols also present other problematic aspects. the most important one relates to the fact that, in order to fit within the DcD protocols, the dead donor rule has to be interpreted. in most countries, cessation of circulatory function is intended as loss of effective mechanical myocardial function, while in italy the electrical cardiac function (detected by the electrocardiogram, ecg) is considered. supporters of the mechanical cardiac function claim that life depends on ef-life depends on ef-fective circulation of oxygenated blood, not on ecg activity. Furthermore, the mechani-, the mechani-cal cardiac function ceases much earlier than the electrical function, thus avoiding minutes of dangerous warm ischemia. again, the term “irreversible” should be intended in the weak-est possible way, as spontaneously irrevers-ible, meaning that no effort should be made to restore effective circulation — even if this is usually possible. indeed, this is coherent with the clinical decision of withdrawing life sup-port procedures. also this choice, opposed to
israel), withdrawing vital supports is clearly forbidden, because it would be considered the direct cause of death.17
in italy, treatment limitation in icU is rela-tively common (roughly in one third of icU deaths), but unfortunately the decision is shared with family only in less than half of cases and is still mainly under the physician’s responsibility, while the nurses are seldom in-volved.18
this urges our community to address this is-sue with specific educational initiatives aimed at implementing the SIAARTI recommenda-tions on the management of the dying pa-tient,19 to clarify the clinical and legal aspects of the end-of-life phase. this must necessarily precede any discussion on cDcD.
tissue donation (corneas, skin, tendons, etc) is relatively frequent after deaths occurred in icU, but we have no information to date that donation of solid organs has ever taken place in this setting. this is most probably due to cultural and organizational issues, as there are no legal constraints that could limit this ap-proach. such a situation is disturbing from a bioethical point of view, because organ dona-tion could be the best way to respect the wish-es of persons who want to donate their organs after death, and consequently to promote their dignity by favouring the accomplishment of their life project.
as regards the uDcD protocols, the prob-lem seems to be less important, because life-supports (cardiopulmonary resuscitation and drug administration) are withdrawn after they have proved ineffective, i.e. unable to produce a viable recovery of spontaneous circulation.
A second ethical issue is the definition of the patient’s vital status and the strict respect of the “dead donor rule”, which states that patients must be declared dead before organs are removed and that interventions aimed at organ retrieval do not accelerate or cause the death.20-22
as concerns the uncontrolled protocols, a problem lies in the duration of resuscitative efforts: no standard time has ever been estab-lished, and good outcomes after up to three hours of cardiopulmonary resuscitation (cPr)

DoNatioN aFter circUlatorY Death iN italY giaNNiNi
Vol. 82 - No. 3 MiNerVa aNestesiologica 363
noeuvres with a “low invasiveness”, mainly necessary for diagnostic work-up (as, for in-stance, blood sampling, laboratory tests, bron-choscopy, etc.) are fully acceptable. other ma-noeuvres with higher invasiveness that could be useful for organ preservation (in particular heparin administration and vessel cannulation) and so close to the end of life, are ethically ac-ceptable if they honour the donor’s wishes and allow an act (organ donation) considered by him/herself (or by the next of kin) as the best way to accomplish his/her life project.
DCD in Italy
uDCD
In Italy, the first and to date only program of uDcD has been developed and run in Pavia since 2007.32 the so-called “alba program” is based on ecMo, which starts immediately af-ter death has been declared using the circulato-ry criteria established by the italian law. selec-tive abdominal normothermic venous-arterial circulation then follows.
all the steps of the protocol have been as-sessed for consistency with italian law and ap-proved by the italian National committee for Bioethics (NcB).33 Cooperation among first-aid and emergency services represents a major challenge, as does availability of resources for the on-call dedicated DcD task force.
to date, 32 kidneys have been retrieved through uDcD, 14 of which have been trans-planted, with only 7% of “primary non func-tion” and good long-term results in compari-son with DBD grafts, in spite of an increased rate of delayed graft function (86%) [abelli M, geraci P. Personal communication], as de-scribed in other series.34
a cost-effectiveness analysis of the alba program shows that changing the current prac-tice and increasing the availability of kidneys from DcD would result in a cost-effective policy to expand the pool of kidney donors.35
Undoubtedly, the 20 minutes of “no-touch period” represents an important problem in terms of warm ischemia and graft damage. the italian NcB has recently suggested main-
the strong interpretation of irreversibility (cir-culation cannot be restarted even by external intervention) leads to a significant shortening of the no-touch period. the purported distinc-tion between the loss of effective circulation and the vitality of the cardiac muscle explains the fact that — in some countries — viable hearts can be retrieved from cDcD donors and can be successfully transplanted.11, 27, 28 this aspect does not concern italy, as the legislator, imposing a 20-minute observation of complete cessation of cardiac electrical function, over-comes this issue by implying a complete and irreversible brain function cessation and the likely loss of myocardial viability.
a third ethical issue — at least in uDcD — is the donor informed consent to procedures aimed at reducing the time of warm ischemia and improving organ preservation. these pro-cedures include large vessel cannulation, infu-sion of organoplegic solutions and heparin up to use of extracorporeal membrane oxygen-ation (ecMo).24 countries such as France and spain have passed legislation allowing pre-sumed consent: organ-preservation measures may be initiated unless the patient has specifi-cally opted out.28, 29 in italy an explicit in vita consent or, in the absence of such declaration, a “non-opposition” by relatives is required for organ and tissue donation.
this raises the question to what extent inva-sive manoeuvres are allowed whilst the final decision is pending. in fact, on one hand, there is the need to avoid further damage and to pre-serve the dignity of the person; on the other hand, there is the need for organ preservation in order to best respect the recipient.
in the literature, this aspect is still debated. the moral and legal permissibility of post mor-tem organ preservation with chest compres-sions, mechanical ventilation, and ecMo re-mains controversial in many countries and has been the subject of many peer-reviewed publi-cations. Moreover, the ethical acceptability of pre mortem interventions to facilitate cDcD is also controversial, and some official state-ments have offered divergent opinions.23, 30, 31 the Wg shares the concept of “minimal do-nor risk” and shares the opinion that those ma-

giaNNiNi DoNatioN aFter circUlatorY Death iN italY
364 MiNerVa aNestesiologica March 2016
the expressed donation wishes of the person, if known and accessible, but also allowing initia-tion of organ preservation manoeuvres.
cDCD
in italy organ procurement after cDcD is legally and ethically conceivable within the current legal framework. however, although formal impediments do not exist, we are faced with many obstacles which hinder the imple-mentation of these programs, mainly of cul-tural nature.
as previously discussed, the issue of cDcD must be seen only in the context of a compre-hensive approach to the end-of-life care in icU and, at present, this aspect of critical care in italy is still largely undervalued.
once more these considerations urge the scientific community to address this particular issue, with two main objectives: 1) towards the professionals (both icU teams and transplant teams), to improve their knowledge concern-ing issues like end-of-life care, organ donation and cDcD, and to provide sound frameworks for medical decision in these fields; 2) towards public opinion, to give correct information and to preserve public trust regarding organ pro-curement.
in particular, in italy every possible effort must be made to promote the cultural growth
taining the 20 minutes of “no touch period”.33 Notwithstanding this, we strongly believe that it would be appropriate to reconsider this time interval also in italy, because it has no substan-tial scientific basis. However, at present we are bound to respect this rule, using all the possi-ble tools to preserve and assess organ function.
the clinical experience in Pavia has clear-ly shown that the prolonged duration of “no touch period” needed to declare circulatory death according to italian legislation should not discourage the spread of uDcD programs even in our country. it is worth noting that re-cently, after the approval of a new program of uDCD lung donation, the first lung transplan-tation from a DcD donor was successfully per-formed in italy (Policlinico of Milan) [Valenza F, personal communication]. the donor died due to acute myocardial infarction and aortic rupture. after unsuccessful resuscitation, the subject was declared dead by cardiac criteria. according to the protocol, the lungs were kept inflated during the 20 minutes of no touch peri-od and, once consent to donation from the next of kin was obtained, the lungs were retrieved, submitted to ex vivo lung perfusion recondi-tioning and functional evaluation, and finally successfully transplanted.
table iii summarizes a useful practical framework for interventions aimed at possible uDcD organ donation, preserving safety and
Table III.—�The 6-step protocols for organ donation in uncontrolled donation after circulatory death (Maastricht categories II).
steps Notes
1 Clinical decision on treatment futility or inefficacy in the asystolic patient: intensive supports should be stopped, non-conventional ecls is not indicated
The treating medical staff which identifies a potential organ donor must be different and independent from the on-call dedicated DcD Multidisciplinary taskforce (DcD-Mt)
2 Death diagnosis by internationally accepted criteria (immediately after stop of life-support therapies)
invasive manoeuvres with proportional risk of complications (laboratory tests, i.V. heparin, vessel cannulation) are allowed with the aim of preserving the possibility of organ donation – in the meanwhile, consent/opposition should be verified
3 Declaration of death Flat ecg must be recorded (for 20 minutes in italy)4 information to the family (treating doctors) and
donation proposal (DCD-MT)after declaration of death, organ retrieval organization and inva-
sive manoeuvres (including ecMo) can be adopted with the aim of preserving organ functionality while the family may express non-opposition to donation (DcD-Mt)
5 complete evaluation of organ suitability as soon as the family agrees with donation
6 organ retrieval Ex situ perfusion if indicatedDcD: donation after circulatory death; ecls: extra-corporeal life support; ecMo: extra-corporeal membran oxygenation.

DoNatioN aFter circUlatorY Death iN italY giaNNiNi
Vol. 82 - No. 3 MiNerVa aNestesiologica 365
context, which is unique to each patient. As long as the patient is alive, he or she cannot be viewed as a potential reservoir of organs or other materials that could be put to use, fail-ing which the patient would be robbed of his or her death and considered, not as a finality, but as a means put prematurely to use by others. Giving priority to the desire to save lives via organ retrieval by instrumentalizing a dying patient at the expense of providing care and ensuring dignity throughout the dying process (…) is ethically unacceptable.”24
We strongly recommend that: 1) the Wlst decision is made independently of the possi-bility of organ donation; 2) the organ retrieval procedure must neither cause nor hasten death; 3) “the dead donor rule” is strictly respected; and 4) reference to an updated national guid-ance for the Wlst is used.
Moreover, we suggest that a first useful step could be to restrict DcD to severely brain-injured patients, once confirmatory investiga-tions predicting a catastrophic prognosis have been performed, following protocols which take into account specific issues, such as seda-tion (for reasons of comfort), extubation, and palliative care.
We also suggest that organ donation after Wlst should be authorized only in pilot cen-tres with a locally agreed Wlst policy, and a local team familiar with DBD and DcD proto-cols. The nature of the confirmatory investiga-tion required should be formalized by the ital-ian cNt, in order to help preserve population trust regarding organ procurement and provide a framework for medical decision-making.
New opportunities
the recent introduction of machine per-fusion devices to assess and recondition “on the bench” (or ex situ) organs after retrieval from marginal donors has great potential to improve the process of DcD, even under ital-ian law, which implies a significant increase of the warm ischemia time.
Machine perfusion is included in the alba program to evaluate the function of the pro-cured organs, being a fundamental step in the
of caregivers on end-of life issues, proportion-ality of treatment and on withdrawing of life support treatments that have become dispro-portionate.
in italy, almost all multiorgan donors are pa-tients with catastrophic brain damage who die in the icU and are declared brain dead. it is at present difficult to assess potential donation: we know that of the many patients who die with acute cerebral lesion in the icU (27,490 in 5 years in italy),36 far more die with diag-nosis of cardio-circulatory arrest rather than brain death (60.1% vs. 39.9%). We have no information about their clinical course, but we can conjecture that a not negligible number could be considered for organ donation af-ter cardiac arrest. Moreover, according to the giViti study, at least 17.1% of icU patients (irrespective of diagnosis) die after withdrawal of life support treatments (Wlst) and a recent French study, in a quite similar context, shows that a significant number of patients who died under Wlst conditions would have been eli-gible for organ donation (more than 50% of brain-injured patients who died).37
the implementation of cDcD programs in italy might therefore generate a number of po-tential donors. hopefully, this should not re-sult in a simultaneous decrease in DBD, as ob-served at an early stage of the DcD programs in some countries (as in the Netherlands, Bel-gium and the UK in the decade 2000-2009).36
DBD and DcD programs must be pursued by implementing a complementary model. Moreover, the average availability of organs from a single donor is 2.1 in the case of DcD compared to 3.6 in DBD.31
We want to point out that treatment with-drawal must not be performed with the goal of allowing donation from Maastricht type iii donors. in particular, according to the recent position statement of the ethics committee of the French intensive care society, we be-lieve that “treatment withdrawal aims to allow death to occur, that is, to avoid prolongation of the dying process by interventions that are useless, costly, and possibly degrading. The treatment-withdrawal decision can only be fully legitimate when placed in the clinical

giaNNiNi DoNatioN aFter circUlatorY Death iN italY
366 MiNerVa aNestesiologica March 2016
the high level of expertise of italian inten-sive care physicians, combined with the high profile organization of the transplant network; the protective italian law with respect to mor-al issues raised by DcD programs; the avail-ability of new extracorporeal techniques: all constitute a promising platform for the safe and effective implementation of DcD pro-grams in italy. the next steps should therefore include:
1. actions directed at promoting the spread of uDcD programs in selected centres under Nct coordination;
2. initiatives aimed at promoting the debate among all involved subjects and making rec-ommendations in the matter of cDcD in the context of end-of-life care of icU patients.
the latter is a very complex issue, with many controversial aspects: however, we do not have to start from zero. We may take into account the statements released in 2003 and 2006 by siaarti and its study group for Bioethics about end of life care in the critical care setting,18, 44 which represent an important basis for this debate. We believe that the is-sue of cDcD should also be addressed in this context.
DcD is one of the new strategies available to overcome the problem of organ shortage and we are bound to address this issue.
Key messages
— to date DcD has not been imple-mented in most european countries, in spite of its proven efficacy and the increas-ing number of persons on waiting lists for transplantation.
— the quality and appropriateness of critical care management are the ethical prerequisites for organ donation after death determination both by neurological and cardiocirculatory criteria.
— an open and clear debate on DcD following limitation of treatment in icU is necessary among both healthcare profes-sionals and the public, where the clinical decision of withdrawing disproportionate
decision whether or not to transplant organs. on-the-road italian programs for lung DcD recovery will take advantage of ex situ lung perfusion techniques which allow the so-called “reconditioning” of these organs, recovery of their function as well as their exhaustive as-sessment before grafting.39, 40 Particularly in uDcD programs, ex-situ evaluation of pro-cured organs is a mandatory step to guarantee patients’ safety.
in selected emergency cases, ecMo is used as part of extracorporeal life-support in non-conventional resuscitation protocols.41 in those patients who do not recover, death may be declared under extracorporeal circulation (see category iV B in table i) by neurologi-cal criteria including the apnea test 42 or by circulatory criteria. these subjects represent a considerable pool of donors that need to be considered, as these donors may be either DcD-like-donors or heart-beating DBD do-nors when neurological criteria are used.
Conclusions
at present italy is markedly different from other countries with respect to organ donation after circulatory death. Despite the “20-min-ute flat ECG” rule, and provided that steps are taken to respect national and regional regula-tions, uDcD programs should be encouraged in selected experienced centres, and possibly within clinical trials. the alba experience has demonstrated the feasibility and the efficacy of this program and helped in addressing many ethical and clinical issues. at present the main obstacle to its implementation seems to be re-lated mainly to organizational and economic aspects.
as far as cDcD is concerned, the time has come also in our country to promote a debate among all involved subjects. starting from the existing documents released by several sci-entific Societies about the end of life 19, 43, the debate should assess the concrete possibility of implementing a specific program in this field. the recent statement of the ethics committee of the French intensive care society 24 could represent a useful road map to follow.

DoNatioN aFter circUlatorY Death iN italY giaNNiNi
Vol. 82 - No. 3 MiNerVa aNestesiologica 367
D, Joris J, et al. What is the potential increase in the heart graft pool by cardiac donation after circulatory death? transpl int 2013;26:61-6
11. Dhital KK, iyer a, connellan M, chew hc, gao l, Doy-le a, et al. adult heart transplantation with distant pro-curement and ex-vivo preservation of donor hearts after circulatory death: a case series. lancet 2015;385:2585-91.
12. Kootstra g, Daemen Jh, oomen aP. categories of non-heart-beating donors. transplantation Proc 1995;27:2893-4.
13. cooreNor eU Project White paper [internet]. avail-able from: http://trapianti.net/coorenor-coordinating-a-european-initiative-among-national-organizations-for-organ-transplantation/ [cited 2014, aug 20].
14. council of europe, Newsletter Transplant, september 1st 2014.
15. asch Da, hansen-Flaschen J, lanken PN. Decision to limit or continue life-sustaining treatment by critical care physicians in the United States: conflicts between phy-sicians’ practices and patients’wishes. am J respir crit care Med 1995;151:288-92.
16. sprung c, cohen sl, sjokvist P, Baras M, Bulow hh, hovilehto s, et al. end-of-life practices in euro-pean intensive care Units. the ethicus study. JaMa 2003;290:790-7.
17. steinberg a, sprung cl. the dying patient: new israeli legislation. intensive care Med 2006;32:1234-7.
18. Bertolini g, Boffelli s, Malacarne P, Peta M, Marchesi M, Barbisan c, et al. end-of-life decision-making and quality of icU performance: an observational study in 84 italian units. intensive care Med 2010;36:1495-504.
19. end-of-life care and the intensivist: siaarti recom-mendations on the management of the dying patient. Minerva anestesiol 2006;72:927-63.
20. robertson Ja. the dead donor rule. hastings cent rep 1999;29:6-14.
21. truog rD, Miller Fg. the Dead Donor rule and organ transplantation. N engl J Med 2008;359:674-5.
22. Zamperetti N, Bellomo r, latronico N. heart donation and transplantation after circulatory death: ethical issues after Europe’s first case. intensive care Med 2016;42:93-5.
23. Kelly rB, Porter Pa, Meier ah, Myers Jl, thomas NJ. Duration of cardiopulmonary resuscitation before extra-corporeal rescue: how long is not long enough? asaio J 2005;51:665-7
24. gratifeaux JP, Bollaert Pe, haddad l, Kentish-Barnes N, Nitenberg g, robert r, et al. contribution of the ethics committee of the French intensive care society to de-scribing a scenario for implementing organ donation af-ter Maastricht type iii cardiocirculatory death in France. ann intensive care 2012,2:23.
25. ethics committee, american college of critical care Medicine, society of critical care Medicine. recom-mendations for non heart beating organ donation [posi-tion paper]. crit care Med 2001;29:1826-31.
26. rodriguez-arias D, tortosa Jc, Burant cJ, aubert P, aulisio MP, Youngner sJ. one or two types of death? at-titudes of health professionals towards brain death and donation after circulatory death in three countries. Med health care and Philos 2013;16:457-67.
27. Bernat Jl, D’alessandro aM, Port FK, Bleck tP, heard so, Medina J, et al. report of a National conference on Donation after cardiac Death. am J transplant 2006;6:281-91.
28. Zamperetti N, Bellomo r, ronco c. cardiac death or cir-culatory arrest? Facts and values in organ retrieval after diagnosis of death by cardio-circulatory criteria. inten-sive care Med 2009;35:1673-7.
29. Kaufman BJ, Wall sP, gilbert aJ, Dubler NN, goldfrank
treatment is completely independent of the possibility of organ donation.
— a 6-step protocol in uncontrolled DcD is suggested to regulate the inclusion of some invasive manoeuvres before and after declaration of death with the aim of preserving the possibility of donation and the quality of transplantable organs.
— in italy it has been proved that the 20 minutes of silent ecg, provided by law to over-guarantee brain death and the ‘dead donor rule’, does not impede organ dona-tion. although we believe that the current 20-minute period should be reconsidered and shortened, the issue of mandatory pro-longed warm ischemia can be mitigated by the high level of expertise of the intensiv-ists combined with the high profile orga-nization of the transplant network and the innovative organ protection and recondi-tioning by ex vivo perfusion techniques.
References
1. simpson PJ. What are the issues in organ donation in 2012? Br J anaesth 2012;108(s1):i3-i6.
2. sistema informativo trapianti, centro Nazionale tra-pianti. attività di donazione al 31 Dicembre 2014. [in-[in-ternet]. available from http://www.trapianti.salute.gov.it/imgs/c_17_pubblicazioni_2380_allegato.pdf [cited 2015, Jul 28].
3. the Madrid resolution on organ Donation and trans-plantation National responsibility in Meeting the Needs of Patients, guided by the Who Principles. transplanta-tion 2011;91(suppl 11):s29-31
4. Domínguez-gil B, Delmonico Fl, shaheen Fa, Mate-sanz r, o’connor K, Minina M, et al. the critical path-way for deceased donation: reportable uniformity in the approach to deceased donation. transpl int 2011;24:373-8.
5. Wall sP, Plunkett c, caplan a. a potential solution to the shortage of solid organs for transplantation. JaMa. 2015;313:2321-2.
6. ortega-Deballon i, hornby l, shemie sD. Protocols for uncontrolled donation after circulatory death: a sys-tematic review of international guidelines, practices and transplant outcomes. crit care 2015;19:268
7. Domínguez-gil B, haase-Kmomwijk B, Van leiden h, Neuberger J, coene l, Morel P, et al. current situation of donation after circulatory death in european countries. transpl int 2011;24:676-86.
8. Van raemdonck D, Neyrinck a, cypel M, Keshavjee s. ex-vivo lung perfusion. transpl int 2015;28:643-56.
9. Watson cJe, Dark Jh. organ transplantation: his-torical perspective and current practice. Br J anaesth 2012;108(suppl 1):i29-i42.
10. Noterdaeme t, Detry o, hans MF, Nellessen e, ledoux

giaNNiNi DoNatioN aFter circUlatorY Death iN italY
368 MiNerVa aNestesiologica March 2016
study group. eligibility for organ donation following end-of-life decisions: a study performed in 43 French in-tensive care units. intensive care Med 2014;40:1323-31.
38. Bendorf a, Kelly PJ, Kerridge ih, Mccaughan gW, My-erson B, stewart c, et al. an international comparison of the effect of policy shifts to organ donation follow-ing cardiocirculatory death (DcD) on donation rates after brain death (DBD) and transplantation rates. Plos one 2013;8:e62010.
39. cypel M, Yeung Jc, liu M, anraku M, chen F, Karolak W, et al. Normothermic ex vivo lung perfusion in clinical lung transplantation. N engl J Med 2011;364:1431-40.
40. Valenza F, rosso l, coppola s, Froio s, Palleschi a, tosi D, et al. ex vivo lung perfusion to improve donor lung function and increase the number of organs available for transplantation. transpl int 2014;27:553-61.
41. rodriguez-arias D, Deballon io. Protocols for un-Protocols for un-controlled donation after circulatory death. lancet 2012;379:1275-6.
42. Migliaccio Ml, Zagli g, cianchi g, lazzeri c, Bonizzoli M, cecchi a, et al. extracorporeal membrane oxygena-extracorporeal membrane oxygena-tion in brain-death organ and tissues donors: a single-centre experience. Br J anaesth 2013;111:673-4.
43. gristina gr, orsi l, carlucci a, causarano i, For-mica M, romanò M, per il gruppo di lavoro insuf-ficienze Croniche d’Organo. Part I. End-stage chronic organ failures: a position paper on shared care plan-ning. the integrated care Pathway. recenti Prog Med 2014;105:9-24.
44. gruppo di studio ad hoc della commissione di Bioetica della siaarti. siaarti recommendations for the ad-mission and discharge from intensive care and for the limitation of treatments in intensive care. Minerva anes-tesiol 2003;69:101-18.
lr. New York city Uncontrolled Donation after cardiac Death study group. success of organ donation after out-of-hospital cardiac death and the barriers to its accept-ance. crit care 2009;13:189.
30. gries cJ, White DB, truog rD, Dubois J, cosio cc, Dhanani s, et al. An official American Thoracic Society/international society for heart and lung transplantation/society of critical care Medicine/association of organ and Procurement organizations/United Network of or-gan sharing statement: ethical and policy considera-tions in organ donation after circulatory determination of death. am J respir crit care Med 2013;188:103-9.
31. Manara ar, Murphy Pg, o’callaghan g. Donation after circulatory death. Br J anaesth 2012;108:108-21.
32. geraci P, sepe V. Non-heart-beating organ donation in italy. Minerva anestesiol 2011;77:613-23.
33. comitato Nazionale per la Bioetica. i criteri di accerta-i criteri di accerta-mento della morte (24 giugno 2010) [internet]. available from: http://www.governo.it/bioetica/pareri_abstract/cri-teri_accertamento_morte20100624.pdf [cited 2014, Dec 26].
34. summers DM, Watson cJ, Pettigrew gJ, Johnson rJ, collett D, Neuberger JM, et al. Kidney donation after circulatory death (DcD): state of the art. Kidney int 2015;88:241-9.
35. cavallo Mc, sepe V, conte F, abelli M, ticozzelli e, Bottazzi a, et al. cost-effectiveness of kidney trans-cost-effectiveness of kidney trans-plantation from DcD in italy. transplant Proceedings 2014;46:3289-96.
36. Procaccio F, ricci a, ghirardini a, Masiero l, caprio M, troni a, et al. Deaths with acute cerebral lesions in icU: Does the number of potential organ donors depend on predictable factors? Minerva anestesiol 2015;81:636-44.
37. lesieur o, leloup M, gonzalez F, Mamzer MF; ePilat
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: September 16, 2015. - Manuscript accepted: September 10, 2015. - Manuscript revised: September 8, 2015. - Manuscript received: February 1, 2015.
Vol. 82 - No. 3 MiNerVa aNestesiologica 369
© 2015 eDiZioNi MiNerVa MeDicathe online version of this article is located at http://www.minervamedica.itMinerva anestesiologica 2016 March;82(3):369-70
regional blocks for breast surgery: is it enough?
Dear editor,
We read with interest the letter written by Bouzinac et al.1 about the association of bilateral Pecs (pectoral nerves) i block and serratus plane block (sPB) previ-
ously described by Blanco 2 for analgesia for a double radical mastectomy.
Pecs i and sPB have successfully demonstrated good quality analgesia for breast surgery and are a good alternative to thoracic paravertebral and epidur-al block.2, 3 However it is not pointed by the authors if a reconstruction with expanders or prostheses was used at the same surgical procedure. the combina-tion of Pecs i and sPB would be, in this case, a suit-able option. Nevertheless, axillary lymphadenectomy analgesia would be insufficient with a Pecs i block. two alternatives that could be considered are a single interfascial block between the serratus anterior and intercostal muscles, reaching the anterior and lat-eral cutaneous branches of the intercostal nerves, described by Dieguez,4 or the plane block between the latissimus dorsi and serratus muscle, described by Blanco,2 that would adequately reach good analgesia levels in the axillary area.
in our opinion, a simple thoracic interfascial block between the serratus anterior and intercostal muscles in the mid-axillary line, can successfully block the anterior and lateral cutaneous branches of the intercostal nerves. this block can reach the adequate metameric levels for a radical mastectomy with a single injection and avoid the combination of sPB and Pecs i when expanders or prostheses are not needed during the same surgical procedure.4, 5 as a consequence, this can also avoid a higher risk for pneumothorax, infection and intravascular in-jection caused by more punctures. in our practice, we routinely use the anterior and lateral cutaneous branches of the intercostal nerves block and Pecs i for bilateral mastectomy when expanders or prosthe-ses are implanted. We have also assessed its efficacy using the analgesia Nociception index (aNi), which correlates very well with good levels of analgesia and no intra and postoperative needs of extra opi-
L E T T E R S T O T H E E D I T O R
anno: 2016Mese: MarchVolume: 82No: 3rivista: Minerva anestesiologicacod rivista: Minerva anestesiol
lavoro: 10770-Mastitolo breve: primo autore: letters to tHe eDitorpagine: 369-70citazione: Minerva anestesiol 2016;82:000-000
Figure 1.—interfascial block of the anterior and lateral cuta-neous branches of the intercostal nerves in the mid-axillary line. serratus: serratus anterior; r: rib; l.a.: local anesthet-ic; int.: intercostal muscle; P: pleura; line: needle.
Figure 2.—in-plane approach in the mid-axillary line.

letters to tHe eDitor
370 MiNerVa aNestesiologica March 2016
© 2015 eDiZioNi MiNerVa MeDicathe online version of this article is located at http://www.minervamedica.it
regional block for breast surgery: is it enough? authors’ reply
Dear editor,
We read with interest the letter by Huercio et al.1
published in this issue of Minerva Anestesiologica and we thank them for their interest in our case re-port.2 No reconstruction was realized for our patient. However, we use to add Pecs i block to serratus plane block (sPB) each time that surgery reached major pectoralis muscle or its aponevrosis. Ultra-sound-guided, in plane approach, should prevent the risk of pleural or vasculaire puncture for both tech-niques. injection of local anesthesic (la) under the serratus anterior muscle seems to be an interesting technique when an extension of the sensitif block to the anterior branches of the intercostal nerves is re-quired. Further investigations are required to define the optimal volume of la to have an extension to the intercostobrachial nerve. it would be interest-ing to compare this new block with others recentely described in breast surgery such as sPB or Pecs ii block.
arnaud BoUZiNacDepartment of anesthesiology, clinique
Médipôle garonne, toulouse, Francecorresponding author: arnaud Bouzinac, clinique Médipôle garonne, 45 rue de gironis, 31100 toulouse, France. e-mail : [email protected]
References
1. Huercio i, abad gurumeta a, gilsanz F. regional blocks for breast surgery: is it enough? Minerva anestesiol 2016; 82:369-70
2. Bouzinac a, Brenier g, Dao M, Delbos a. Bilateral asso-ciation of pecs i block and serratus plane block for post-operative analgesia after double modified radical mastec-tomy. Minerva anestesiol 2015;81:589-90.
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: September 7, 2015. - Manuscript accepted: september 7, 2015. - Manuscript received: august 21, 2015.(Cite this article as: Bouzinac a. regional block for breast surgery: is it enough? authors’ reply. Minerva anestesiol 2016;82:370
oids.6 this combination can be easily performed un-der ultrasound guidance in the mid-axillary line lo-cating, in plane, at the 4th and 5th intercostal levels. a single dose of 10 ml of 0.25% of l-bupivacaine is injected in the interfascial plane between the ser-ratus anterior and intercostal muscles, and 10 ml of 0.25% of l-bupivacaine for Pecs i block. this tech-nique has been enough to maintain aNi levels above 50 during surgery time. Visual analgesia scale has been used for pain assessment after surgery and in the PacU, and it correlates well with good control of postoperative pain.
in our opinion, this block can also provide high-quality analgesia for modified radical mastectomy with less number of punctures and avoid the subse-quent associated risks. However, further studies are needed to evaluate this technique and possible indi-cations.
ivan HUercio *, alfredo aBaD-gUrUMeta,
Fernando gilsaNZDepartment of anesthesia and critical care,
la Paz University Hospital, Madrid, spain
*corresponding author: iván Huercio, Department of anes-thesia and critical care, la Paz University Hospital, calle de Bravo Murillo 32 5e, 28015 Madrid, spain. e-mail: [email protected]
References
1. Bouzinac a, Brenier g, Dao M, Delbos a. Bilateral asso-ciation of Pecs i block and serratus plane block for post-operative analgesia after double modified radical mastec-tomy. Minerva anestesiol 2015;8:589-90.
2. Blanco r, Parras t, McDonnell Jg, Prats-galino a. ser-ratus plane block: a novel ultrasound-guided thoracic wall nerve block. anaesthesia 2013;68:1107-13.
3. Blanco r. the ‘pecs block’: a novel technique for providing analgesia after breast surgery. anaesthesia 2011;66:847-8.
4. Diéguez garcía P, Fajardo Pérez M, lópez Álvarez s, alfaro de la torre P, Pensado castiñeiras aP. Ultrasound-assisted approach to blocking the intercostal nerves in the mid-axillary line for non-reconstructive breast and axilla surgery. rev esp anestesiol reanim 2013;60:365-70.
5. Diéguez P, Fajardo M, lópez s, alfaro P. BrilMa meth-ylene blue in cadavers. anatomical dissection. rev esp anestesiol reanim 2015;30:00107-3.
6. Boselli e, Bouvet l, Bégou g, Dabouz r, Davidson J, Deloste JY, et al. Prediction of immediate postoperative pain using the analgesia/ nociception index: a prospective observational study. Br J anaesth 2014;112:715-21.
Conflicts of interest.—the authors certify that there is no con-flict of interest with any financial organization regarding the ma-terial discussed in the manuscript.Article first published online: September 2, 2015. - Manuscript accepted: august 3, 2015. - Manuscript revised: July 30, 2015. - Manuscript received: June 23, 2015.(Cite this article as: Huercio i, abad-gurumeta a, gil-sanz F. regional blocks for breast surgery: is it enough? Minerva anestesiol 2016;82:369-70
Minerva anestesiologica 2016 March;82(3):370

letters to tHe eDitor
Vol. 82 - No. 3 MiNerVa aNestesiologica 371
beacon. He located the victim at 1.5 m under the snow, shoveled immediately, without a precise probe detec-tion and found the victim upside down. the victim ap-peared without vital signs, airway patency preserved. cardiac massage and pulmonary resuscitation (cPr) was not performed by occasional rescuers. at the arriv-al of the helicopter rescue team, he was in circulatory arrest. after cervical spine immobilization, the patient received cPr, while 45 minutes elapsed from the acci-dent. With 26° c of epitympanic temperature and asys-tole confirmed by DAE monitor, the extra corporeal life support (ecls) protocol was activated. the patient underwent endotracheal intubation, 1 mg of adrenalin intravenous was administered. after 12 minutes of flight, the patient was transported directly in the hospi-tal cath-lab, epitympanic temperature of 28° c, serum potassium 5.6 mmol/l. the patient was connected to extracorporeal membrane oxygenation (ecMo, Ma-quet cardiohelp, cinisello Balsamo, Milan, italy), right femoral vein and artery were cannulated with cannu-las 17F and 21F, respectively, plus cannulation of right antegrade femoral artery approach with a 7F catheter to allow distal territory perfusion (Fio2 0,6). once the central temperature of 30° c was reached, the heart re-
© 2015 eDiZioNi MiNerVa MeDicathe online version of this article is located at http://www.minervamedica.it
extracorporeal membrane oxygenation in avalanche victim with deep hypothermia and circulatory arrest
Dear editor,
trying to save the life of someone buried by an ava-lanche is a moral obligation. This case report testifies the first extracorporeal rewarming tried in Abruzzo, italy, on a deep hypothermic avalanche victim.
During a sunny day, following several days of snow-falls, two snowboarders decided to descend off-slope. the slope angle of 33°-35° showed previous descent tracks. The first snowboarder, 32 years old, on descend-ing triggered an avalanche and got overwhelmed. the second snowboarder started searching with avalanche
Figure 1.— icar-Medcom checklist optimized by sNaMeD (National Medical school) and cNsas (National corps for Mountain and speleological rescue). in the part below the Brain ct scan is shown.
Minerva anestesiologica 2016 March;82(3):371-2

letters to tHe eDitor
372 MiNerVa aNestesiologica March 2016
sion for mountain emergency medicine (icar MeD-coM): intended for physicians and other advanced life support personnel. resuscitation 2013;84:539-46.
3. Brown D, Brugger H, Boyd J, Paal P. accidental Hypo-thermia. N engl J Med 2012;367:1930-8.
4. Boué Y, Payen JF, Brun J, thomas s, levrat a, Blancher M, et al. survival after avalanche-induced cardiac arrest. resuscitation 2014;85:1192-6.
5. Kottmann a, Blancher M, spichiger t, elsensohn F, létang D, Boyd J, et al. the avalanche Victim resus-citation checklist, a new concept for the management of avalanche victims. resuscitation 2015;91:e7-8.
Conflicts of interest.—The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.Article first published online: 2015, November 5. - Manuscript accepted: November 4, 2015. - Manuscript revised: october 27, 2015. - Manuscript received: 2015, July 22.(Cite this article as: Facchetti g, carbuglia N, Bucci V, taraschi F, Paparoni s, gyra a, et al. extracorporeal membrane oxygena-extracorporeal membrane oxygena-tion in avalanche victim with deep hypothermia and circulatory arrest. Minerva anestesiol 2016;82:371-2)
© 2015 eDiZioNi MiNerVa MeDicathe online version of this article is located at http://www.minervamedica.it
incidence and laryngoscopic gradeof adult patients with Mallampati class zero airway
Dear editor,
The Mallampati classification of four grades as mod-ified by Samsoon and Young is an accepted method for predicting a difficult airway.1 ezri et al. proposed addi-tion of new airway Mallampati class zero, in which the epiglottis is seen on mouth opening and tongue protru-sion, and suggested that this class was the easiest for performing tracheal intubation among the five classes.2 However, the difficulty of tracheal intubation in those patients remains unclear. then, we investigated the inci-dence of Mallampati class zero airway in adult patients and the relationship with a difficult airway. The Malla-mpati classification was assessed by the same anesthe-siologist prior to surgery. laryngoscopy was performed using a Macintosh blade with a muscular relaxant and under general anesthesia. The difficulty of endotracheal intubation was assessed by the attending anesthesiolo-gist using the cormack and lehane grading scale.
We analyzed 1200 surgical patients (584 males). a Mallampati class zero airway was noted in 8 (0.7%, 95% confidence interval: 0.3-1.3%) of the patients (4 males), all of whom had an easy airway (cormack grade
sumed a spontaneous rhythm. central temperature was gradually heated to 37° C, with a constant flow of 3.5 l/min. radiological examinations demonstrated: a c2 cervical amyelic lesion, a widespread cerebral edema, an hypovolemic reduction of the aorto-caval district, endobronchial liquid, pulmonary contusions and en-doalveolar hematic material, peritoneal and retroperi-toneal fluid. The patient presented diffuse bleeding, serious vasoplegic state with hypotension refractory to inotropic and vasopressor infusion, anuria, severe pulmonary edema and an intracranial pressure (icP) of about 30 mmHg. after left femoral vein cannula-tion, hemofiltration was performed. Under continuous ecMo treatment the patient was substantially stable, but presented neurological deterioration with icP raised to 39 mmHg. subsequently the icP was enhanced to 45 mmHg, accompanied by hemodynamic and metabolic aggravation. the patient died after three days due to multiple organic failure syndrome (MoFs).
ecMo is the rewarming method with the highest survival rate for deep hypothermic treatment,1 but de-spite careful application of actual guidelines,2, 3 chances of survival for buried by avalanche, extracted in cardiac arrest, remain low.4 this case was treated according to the icar-Medcom guidelines 2 and after application of the related flow-chart (Figure 1),5 but despite of an independent heartbeat retrieval, the patient survival was not allowed. cortical suffering highlighted by ct scan showed anoxic damage (Figure 1), established before hypothermia, which has affected the prognosis. the avalanche victim, despite the preserved airway patency, did not receive immediate cPr. the asphyxia caused the circulatory arrest; the absence of immediate cPr worsened the anoxic damage.
gianluca FaccHetti 1 *, Nadia carBUglia 2, Valter BUcci 1,
Francesco tarascHi 3, saro PaParoNi 4, aglaia gYra 5, Franco MariNaNgeli 5
1National Medical school of the National Mountain rescue corps, Milan, italy; 2abruzzo Helicopter rescue Unit, Pescara, italy, 3Unit of anesthesia
and Post operative intensive care cardiac surgery, teramo, italy, 4Unit of cardiology ii, teramo,
italy, 5Department of anesthesia and resuscitation, Universty of l’aquila, l’aquila, italy
*corresponding author: gianluca Facchetti, National Medical school of the National Mountain rescue corps, Milan, italy. e-mail: [email protected]
References
1. ruttmann e, Weissenbacher a, Ulmer H, Müller l, Höfer D, Kilo J, et al. Prolonged extracorporeal membrane ox-ygenation-assisted support provides improved survival in hypothermic patients with cardiocirculatory arrest. J thorac cardiovascsurg 2007;134:594-600.
2. Brugger H, Durrer B, elsensohn F, Paal P, strapazzon g, Winterberger e, et al. resuscitation of avalanche victims: evidence-based guidelines of the international commis-
Minerva anestesiologica 2016 March;82(3):372-3

letters to tHe eDitor
Vol. 82 - No. 3 MiNerVa aNestesiologica 373
a low grade for Mallampati classification suggests an easier airway in the conventional four-grade classifica-tion system, Mallampati class zero, the lowest in the five grade classification, does not ensure an easy airway, because some of those patients have a large epiglottis.
Hirotsugu MiYosHi *, shinji KUsUNoKi, ryuji NaKaMUra, Masashi KaWaMoto
Department of anesthesiology and critical care, Hiroshima University Hospital, Hiroshima Japan
*corresponding author: Hirotsugu Miyoshi, Department of an-esthesiology and critical care, Hiroshima University Hospital, 1-2-3 Kasumi, Minami-ku, Hiroshima 734-8551, Japan. e-mail: [email protected]
References
1. Samsoon GL, Young JR. Difficult tracheal intubation: a retrospective study. anaesthesia 1987;42:487-90.
2. ezri t, cohen Y, geva D, szmuk P. Pharyngoscopic views. anesth analg 1998;87:748.
3. ezri t, Warters rD, szmuk P, saad-eddin H, geva D, Katz J, et al. the incidence of class “zero” airway and the impact of Mallampati score, age, sex, and body mass index on prediction of laryngoscopy grade. anesth analg 2001;93:1073-5.
4. Hegde HV, Prasad Kc, Bhat Mt, Hegde Js, santhosh Mysore cb, et al. Airway difficulty in Mallampati ‘class zero’ patients: a prospective double-blind observational study. eur J anaesthesiol 2012;29:338-42.
5. Mahajan r, grover VK. intubating conditions associated with the Mallampati “class zero” airway. can J anaesth 2005;52:891-2.
the content of this study was presented at the american society of anesthesiologists annual Meeting 2013, which was held in san Francisco, on october 12-16.Conflicts of interest.—the authors certify that there is no con-flict of interest with any financial organization regarding the ma-terial discussed in the manuscript.Article first published online: October 22, 2015. - Manuscript accepted: october 20, 2015. - Manuscript revised: october 16, 2015. - Manuscript received: september 17, 2015.(Cite this article as: Miyoshi H, Kusunoki s, Nakamura r, Kawamoto M. incidence and laryngoscopic grade of adult pa-tients with Mallampati class zero airway. Minerva anestesiol 2016;82:372-3)
1 in each). these results corresponded to other previous reports. ezri et al. reported that the incidence of Malla-mpati class zero airway was 1.2% (9/764 patients, 95% confidential interval: 0.6-2.2%) and all had a grade 1 laryngoscopy.3 Hegde et al. reported that the incidence of Mallampati class zero airway was 1.7% (33/1937 patients, 95% confidential interval: 1.1-2.2%) and all had an easy endotracheal intubation (cormack grade 1 or 2).4 However, observation of the glottis in 2 of our study patients was a bit more difficult as compared to the others, because of a tubular or omega-shaped large epiglottis (Figure 1). Hegde et al. reported that 37% of their Mallampati class zero airway patients had a large epiglottis and 56% had an overhanging epiglottis.4 also, Mahajan and Grover reported a case of difficult airway in a Mallampati class zero airway patient caused by a large epiglottis.5 a Mallampati class zero per se is not associated with difficult airway unless other airway characteristics contribute to the difficulty. Although
Figure 1.—omega-shaped epiglottis. image obtained with airtraq laryngoscope® (Prodol, Meditec, Viscaza, spain).
errata corrige.—in volume 65, issue no. 3 - March, pages 95-100, in the article entitled “Quality control in anesthesia. a new frontier”, the correct authors’ names are: Varrassi g., Marinangeli F., Facchetti g. instead of Varrassi g., Mariangeli F., Facchetti g.

374 MINERVA ANESTESIOLOGICA March 2016
T O P 5 0 M I N E R V A A N E S T E S I O L O G I C A R E V I E W E R S
Anno: 2016Mese: MarchVolume: 82No: 3Rivista: MINERVA ANESTESIOLOGICACod Rivista: Minerva Anestesiol
Lavoro: titolo breve: primo autore: ACKNOWLEDGEMENTSpagine: 374
Most active reviewers between August 2015-January 2016
Surname Name Numberof revisions
Savoia Gennaro 9Biasucci Daniele Guerino 8Agrò Eugenio Felice 8Bertini Pietro 7Dalfino Lidia 6Camporesi Enrico Mario 6Brazzi Luca 6Zanella Alberto 6Weiner Menachem 5Montini Luca 5Peris Adriano 5Cattano Davide 5Chelazzi Cosimo 5Donadello Katia 5Alston Theodore 4Cata Juan P. 4Sorbello Massimiliano 4El Tahan Mohamed 4Tritapepe Luigi 4Della Rocca Giorgio 4Cunha Francisco 4Guarracino Fabio 4De Pascale Gennaro 4Caruselli Marco 4Cinnella Gilda 4Deflandre Eric P. 4Aceto Paola 4Benes Jan 4Bruder Nicolas 3Max Martin 3Ting Chien-Kun 3Mauri Tommaso 3Mallat Jihad 3Sakai Tetsuro 3Calzavacca Paolo 3Vannucci Andrea 3Cavallone Laura Francesca 3Gómez-Ríos Manuel Ángel 3Camporota Luigi 3Langer Thomas 3Kopp Rüdger 3Faraoni David 3Algarra Nelson Nicolás 3Szakmany Tamas 3Ezzeldin Ibrahim Saleh 3Somaini Marta 3De Cosmo Germano Amilcare 3Turnbull David 3Boer Christa 3Abdel Raheem Mohamed Samy 3