
Middle Ear Barotrauma in Scuba Divers
10
Journal of Wilderness Medicine, 5,389-398 (1994) ORIGINAL ARTICLE Middle ear barotrauma in scuba divers MICHAEL J. KORIWCHAK, MD* and JAY A. WERKHAVEN, MD Department of Otolaryngology, Vanderbilt University Medical Center, S-2100 Medical Center North, Nashville, Tennessee 37232-2559, U.S.A. Middle ear barotrauma is the most common health hazard of scuba diving. To investigate the overall incidence of middle ear barotrauma, a prospective incidence study of 51 novice divers and 46 experienced divers was conducted. Otoscopy was performed on the divers before and immediately following a single dive. The overall incidence of mild barotrauma was 40%, and the incidence of severe barotrauma was 27%. No tympanic membrane perforations were found. The most common presenting symptoms were difficulty clearing ears during descent, ear pressure, and ear pain. Barotrauma was not associated with diver age, sex, experience, otolaryngologic history, or medica- tions. Barotrauma was associated with poor underwater visibility, difficulty clearing ears during ascent, and hearing loss after surfacing. Key words: diving; barotrauma; hazard; middle ear Introduction Sport scuba diving has undergone remarkable expansion in the past 15 years. The sport has grown from approximately 213 000 scuba divers in 1975 [1] to current estimates of 2-3.5 million [2]. Each year approximately 200000 new scuba divers become certified [3]. This constitutes a large and rapidly growing group with unique health risks and health problems. Ear complaints constitute the most common problem for which divers seek medical attention. In a series of 1001 disorders in 650 scuba divers, ear complaints were the most common (65%) [3]. Furthermore, divers may avoid seeking medical attention in relatively remote dive locations and seek medical attention after returning home. Thus, physicians may expect to see increasing numbers of diving-related ear complaints, regard- less of geographic location. Mechanism of middle ear barotrauma (Figure 1) At sea level, the pressures of the external auditory canal and middle ear are equal at 760 mm Hg (1 atm); see Fig. 1. Descent to 2.6 ft below the surface raises the pressure in the external canal to 800 mm, creating a 40-mm gradient across the tympanic membrane. This produces a sensation of pressure in the ear. At this point, the diver must perform the Valsalva maneuver to actively equalize the pressure in the middle ear. If the diver does not equalize and descends to 3.9 ft, the pressure gradient across the tympanic membrane increases to 90 mm Hg. The relative low pressure in the middle ear ruptures blood vessels 'To whom correspondence should be addressed. Additional reprints of this chapter may be obtained from the Reprints Department, Chapman & Hall, One Penn Plaza, New York, NY 10119. 0953-9859 © 1994 Chapman & Hall
-
Upload
yehezkiel-kurniawan -
Category
Documents
-
view
30 -
download
0
description
careful scuba divers.
Transcript of Middle Ear Barotrauma in Scuba Divers

Journal of Wilderness Medicine, 5,389-398 (1994)
ORIGINAL ARTICLE
Middle ear barotrauma in scuba diversMICHAEL J. KORIWCHAK, MD* and JAY A. WERKHAVEN, MD
Department ofOtolaryngology, Vanderbilt University Medical Center, S-2100 Medical Center North,Nashville, Tennessee 37232-2559, U.S.A.
Middle ear barotrauma is the most common health hazard of scuba diving. To investigate the overallincidence of middle ear barotrauma, a prospective incidence study of 51 novice divers and 46experienced divers was conducted. Otoscopy was performed on the divers before and immediatelyfollowing a single dive. The overall incidence of mild barotrauma was 40%, and the incidence ofsevere barotrauma was 27%. No tympanic membrane perforations were found. The most commonpresenting symptoms were difficulty clearing ears during descent, ear pressure, and ear pain.Barotrauma was not associated with diver age, sex, experience, otolaryngologic history, or medications. Barotrauma was associated with poor underwater visibility, difficulty clearing ears duringascent, and hearing loss after surfacing.
Key words: diving; barotrauma; hazard; middle ear
Introduction
Sport scuba diving has undergone remarkable expansion in the past 15 years. The sport hasgrown from approximately 213 000 scuba divers in 1975 [1] to current estimates of 2-3.5million [2]. Each year approximately 200000 new scuba divers become certified [3]. Thisconstitutes a large and rapidly growing group with unique health risks and healthproblems. Ear complaints constitute the most common problem for which divers seekmedical attention. In a series of 1001 disorders in 650 scuba divers, ear complaints were themost common (65%) [3]. Furthermore, divers may avoid seeking medical attention inrelatively remote dive locations and seek medical attention after returning home. Thus,physicians may expect to see increasing numbers of diving-related ear complaints, regardless of geographic location.
Mechanism of middle ear barotrauma (Figure 1)
At sea level, the pressures of the external auditory canal and middle ear are equal at 760mm Hg (1 atm); see Fig. 1. Descent to 2.6 ft below the surface raises the pressure in theexternal canal to 800 mm, creating a 40-mm gradient across the tympanic membrane. Thisproduces a sensation of pressure in the ear. At this point, the diver must perform theValsalva maneuver to actively equalize the pressure in the middle ear. If the diver does notequalize and descends to 3.9 ft, the pressure gradient across the tympanic membraneincreases to 90 mm Hg. The relative low pressure in the middle ear ruptures blood vessels
'To whom correspondence should be addressed. Additional reprints of this chapter may be obtained from theReprints Department, Chapman & Hall, One Penn Plaza, New York, NY 10119.
0953-9859 © 1994 Chapman & Hall

390 Koriwchak and Werkhaven
Fig. 1. Mechanism of middle ear barotrauma in scuba divers. At the surface, pressures in theexternal auditory canal (A) and middle ear (B) are equal at 760 mm Hg. As the diver descends, thepressure in the external ear rises. If the diver does not equalize the middle ear pressure byperforming the Valsalva maneuver, the pressure gradient across the tympanic membrane may rise toas high as 90 mm Hg at a depth of 3.9 ft. The tympanic membrane may rupture when the gradientexceeds 100 mm Hg.
in the tympanic membrane and middle ear mucosa. These changes in the tympanicmembrane are visible with an otoscope. A middle ear effusion of either blood or serousfluid may also result.
Because the pressure in the nasopharynx equals the ambient pressure at depth, thepressure gradient across the tympanic membrane is also present across the eustachiantube. A high pressure gradient locks the eustachian tube closed, and active equalization bythe diver is impossible unless the pressure gradient is reduced by ascending. If the diverfails to equalize and continues to descend, the pressure gradient across the tympanicmembrane rises to 230 mm Hg at 10 ft and 345 mm Hg at 15 ft. The tympanic membranemay rupture at pressures beyond 100 mm Hg [4].
Although equalization during descent is an active process performed by the diver,expanding air in the middle ear during ascent vents passively through the eustachian tubeto the nasopharynx. Occasionally, the mucosa of the eustachian tube becomes edematousfrom forced equalization and/or middle ear barotrauma, and passive equalization isimpaired. This causes a sensation of pressure and pain in the ear during ascent.
Whereas the pathophysiology of middle ear barotrauma is understood, its epidemiologyand frequency are not known. Current information is mostly limited to data from doctorvisits by injured divers. As middle ear barotrauma may be asymptomatic, and as manysymptomatic divers do not see a doctor, there is a significant selection bias. The purpose ofthis study was to survey and examine all divers at the water's edge, regardless of symptoms.Our goal was to identify risk factors in both diving conditions and divers themselves to helppredict the occurrence of middle ear barotrauma.
Middle ear barotrauma in divers
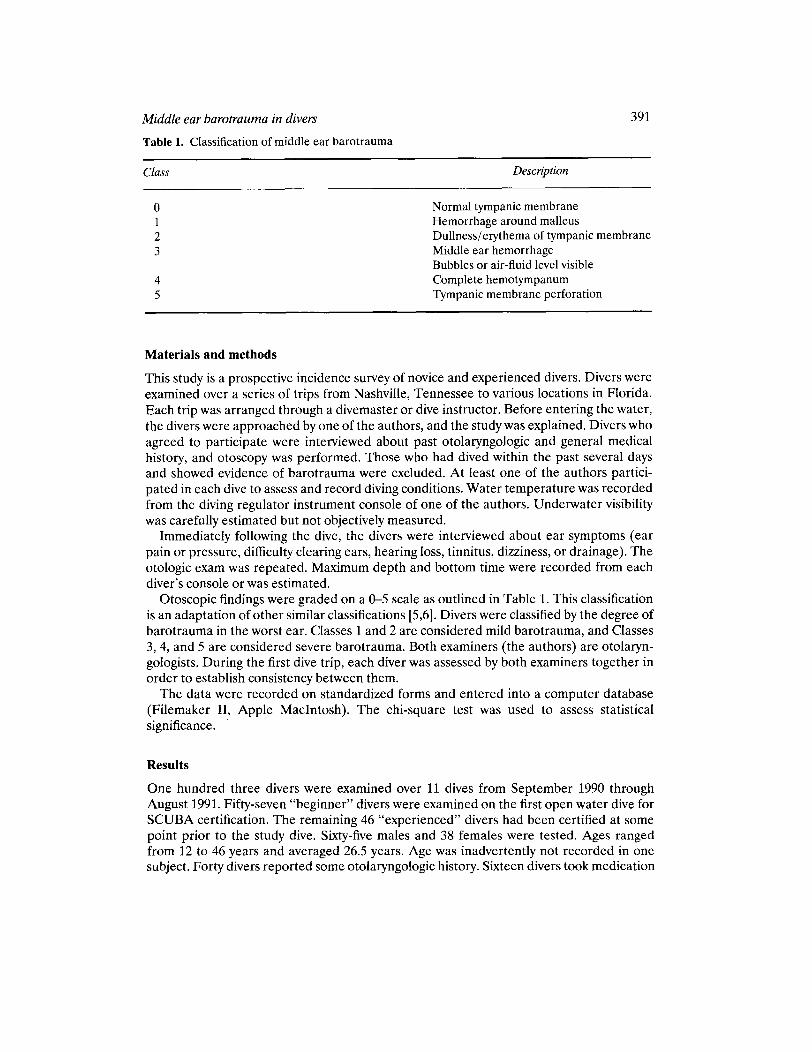
Table 1. Classification of middle ear barotrauma
Class
o123
45
391
Description
Normal tympanic membraneHemorrhage around malleusDullness/erythema of tympanic membraneMiddle ear hemorrhageBubbles or air-fluid level visibleComplete hemotympanumTympanic membrane perforation
Materials and methods
This study is a prospective incidence survey of novice and experienced divers. Divers wereexamined over a series of trips from Nashville, Tennessee to various locations in Florida.Each trip was arranged through a divemaster or dive instructor. Before entering the water,the divers were approached by one of the authors, and the study was explained. Divers whoagreed to participate were interviewed about past otolaryngologic and general medicalhistory, and otoscopy was performed. Those who had dived within the past several daysand showed evidence of barotrauma were excluded. At least one of the authors participated in each dive to assess and record diving conditions. Water temperature was recordedfrom the diving regulator instrument console of one of the authors. Underwater visibilitywas carefully estimated but not objectively measured.
Immediately following the dive, the divers were interviewed about ear symptoms (earpain or pressure, difficulty clearing ears, hearing loss, tinnitus, dizziness, or drainage). Theotologic exam was repeated. Maximum depth and bottom time were recorded from eachdiver's console or was estimated.
Otoscopic findings were graded on a 0-5 scale as outlined in Table 1. This classificationis an adaptation of other similar classifications [5,6]. Divers were classified by the degree ofbarotrauma in the worst ear. Classes 1 and 2 are considered mild barotrauma, and Classes3,4, and 5 are considered severe barotrauma. Both examiners (the authors) are otolaryngologists. During the first dive trip, each diver was assessed by both examiners together inorder to establish consistency between them.
The data were recorded on standardized forms and entered into a computer database(Filemaker II, Apple MacIntosh). The chi-square test was used to assess statisticalsignificance. .
Results
One hundred three divers were examined over 11 dives from September 1990 throughAugust 1991. Fifty-seven "beginner" divers were examined on the first open water dive forSCUBA certification. The remaining 46 "experienced" divers had been certified at somepoint prior to the study dive. Sixty-five males and 38 females were tested. Ages rangedfrom 12 to 46 years and averaged 26.5 years. Age was inadvertently not recorded in onesubject. Forty divers reported some otolaryngologic history. Sixteen divers took medication

392
Table 2. Middle ear barotrauma in scuba divers (postdive exam)
Koriwchak and Werkhaven
Class No. ofdivers %
a 33 321 25 242 18 173 17 174 10 105 a a
Total 103 100
either to protect against motion sickness or to improve the ability to equalize the ears. Ofthe 38 female divers, 16 took oral contraceptives. No significant tympanic membraneabnormalities were noted on the predive otoscopic exams.
Table 2 outlines the postdive otoscopic findings for the entire group of 103 divers.Approximately 32% had a normal tympanic membrane after diving (class 0). Forty-onepercent had mild barotrauma (Classes 1 or 2) and the remaining 27% had severebarotrauma (Classes 3 or 4). No tympanic membrane perforations (Class 5) were observed.
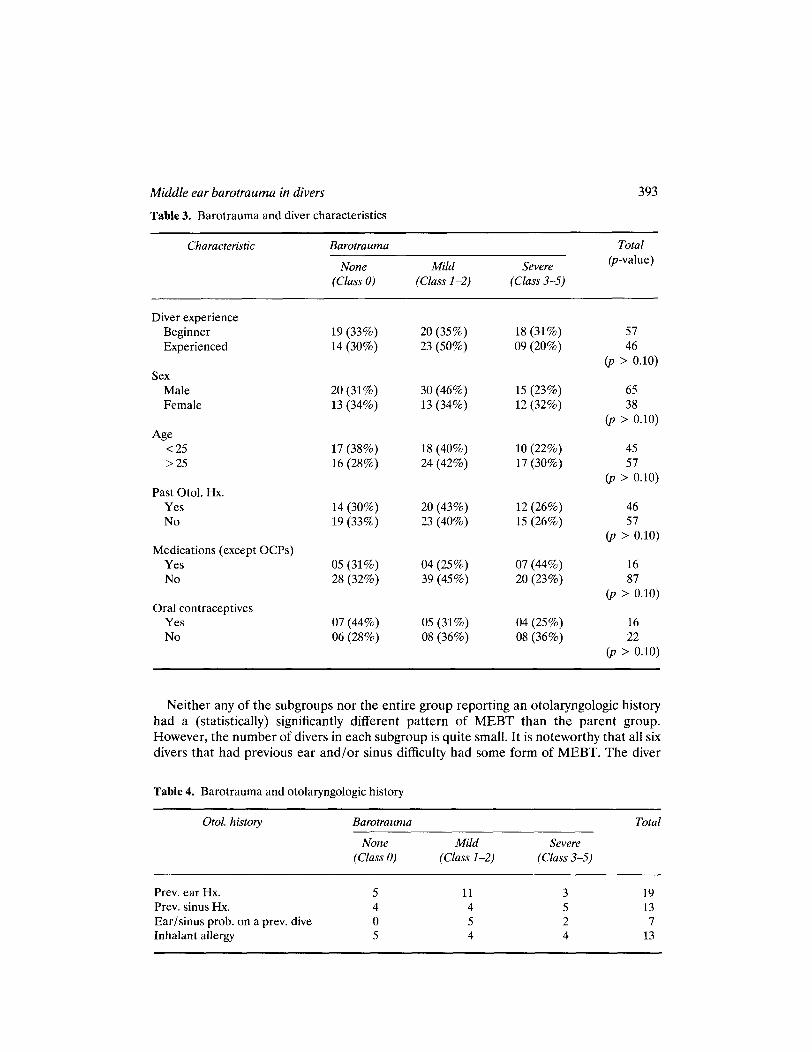
Middle ear barotrauma and diver experience (Table 3)
When beginner divers are compared to experienced divers, a trend is observed in whichexperienced divers tend to sustain mild middle ear barotrauma (MEBT), whereas beginner divers have roughly equal proportions of mild and severe MEBT. However, thedifference is not statistically significant (p > .10). Moreover, the proportions of bothbeginner and experienced divers sustaining MEBT of any kind were similar (66% vs. 70%).
MEBT and sex/age (Table 3)
The proportion of each sex sustaining MEBT of any kind are very similar (69% vs. 66%).Although males tend to receive mild MEBT and females have a roughly equal likelihood ofsustaining either mild or severe MEBT, the difference is not statistically significant(p > .10).
When examined with respect to age, MEBT appears somewhat more frequently in thoseover 25 years of age (72% vs. 66%). However, the difference is not statistically significant(p > 0.10).
MEBT and otolaryngologic history (Tables 3 and 4)
Forty divers reported some otolaryngologic history. Ear problems were most commonlyreported. These included a history of PE tubes in childhood (four cases), otitis media (fourcases), and otitis externa (four cases). The remainder consisted of minor problems such asoccasional earaches or cerumen. Divers with sinus problems included four with "occasional sinusitis" and four with "sinus headaches." This group included the only diver thathad a previous major otolaryngologic procedure (nasal polypectomy). Six divers reporteddifficulty with clearing the ears or sinuses on previous dives. Thirteen divers had a historyof inhalant allergies.
Middle ear barotrauma in divers 393
Table 3. Barotrauma and diver characteristics
Characteristic Barotrauma Total
None Mild Severe(p-value)
(Class 0) (Class 1-2) (Class 3-5)
Diver experienceBeginner 19 (33%) 20 (35%) 18(31%) 57Experienced 14 (30%) 23 (50%) 09 (20%) 46
(p > 0.10)Sex
Male 20 (31%) 30 (46%) 15 (23%) 65Female 13 (34%) 13 (34%) 12 (32%) 38
(p > 0.10)Age
<25 17 (38%) 18 (40%) 10 (22%) 45>25 16 (28%) 24 (42%) 17 (30%) 57
(p > 0.10)Past Otol. Hx.
Yes 14 (30%) 20 (43%) 12 (26%) 46No 19 (33%) 23 (40%) 15 (26%) 57
(p > 0.10)Medications (except OCPs)
Yes 05 (31%) 04 (25%) 07 (44%) 16No 28 (32%) 39 (45%) 20 (23%) 87
(p > 0.10)Oral contraceptives
Yes 07 (44%) 05 (31%) 04 (25%) 16No 06 (28%) 08 (36%) 08 (36%) 22
(p > 0.10)
Neither any of the subgroups nor the entire group reporting an otolaryngologic historyhad a (statistically) significantly different pattern of MEBT than the parent group.However, the number of divers in each subgroup is quite small. It is noteworthy that all sixdivers that had previous ear and/or sinus difficulty had some form of MEBT. The diver
Table 4. Barotrauma and otolaryngologic history
Otol. history
Prevo ear Hx.Prevo sinus Hx.Ear/sinus prob. on a prevo diveInhalant allergy
Barotrauma
None Mild Severe(Class 0) (Class 1-2) (Class 3-5)
5 11 34 4 50 5 25 4 4
Total
1913
713
Middle ear barotrauma in divers 395
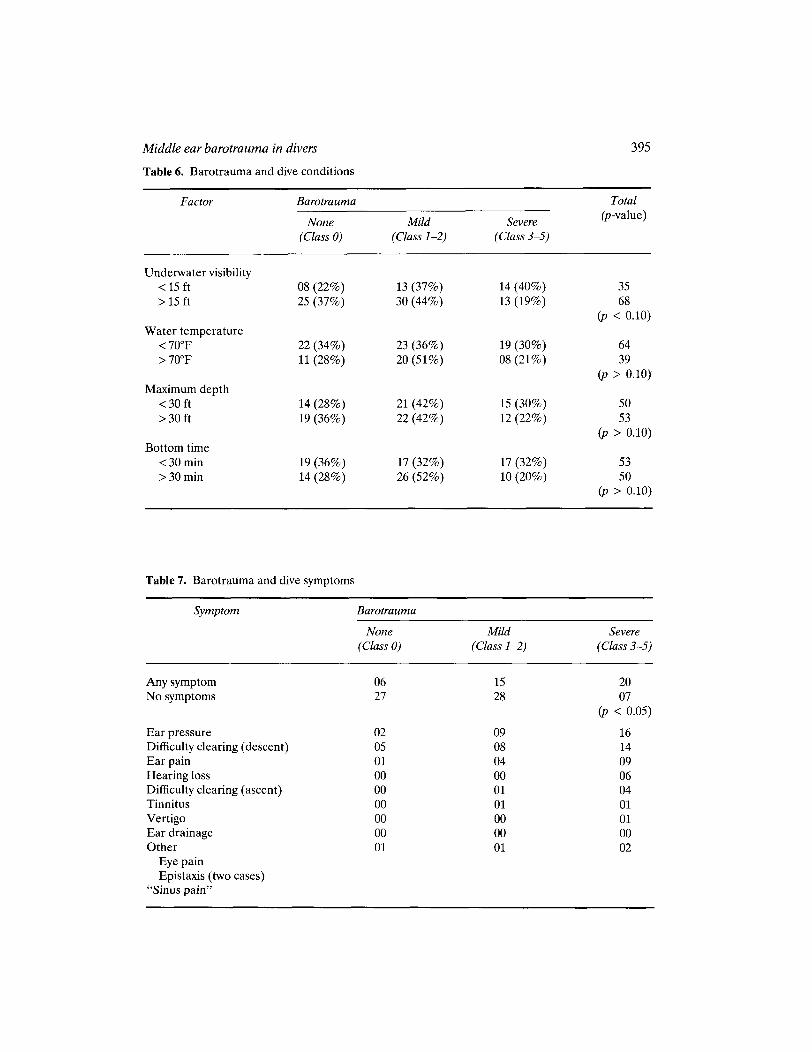
Table 6. Barotrauma and dive conditions
Factor Barotrauma Total
None Mild Severe(p-value)
(Class 0) (Class 1-2) (Class 3-5)
Underwater visibility< 15 ft 08 (22%) 13 (37%) 14 (40%) 35> 15 ft 25 (37%) 30 (44%) 13 (19%) 68
(p < 0.10)Water temperature
<70°F 22 (34%) 23 (36%) 19 (30%) 64> 70°F 11 (28%) 20 (51%) 08 (21 %) 39
(p > 0.10)Maximum depth
<30 ft 14 (28%) 21 (42%) 15 (30%) 50>30 ft 19 (36%) 22 (42%) 12 (22%) 53
(p > 0.10)Bottom time
<30 min 19 (36%) 17 (32%) 17 (32%) 53>30min 14 (28%) 26 (52%) 10 (20%) 50
(p > 0.10)
Table 7. Barotrauma and dive symptoms
Symptom Barotrauma
None Mild Severe(Class 0) (Class 1-2) (Class 3-5)
Any symptom 06 15 20No symptoms 27 28 07
(p < 0.05)
Ear pressure 02 09 16Difficulty clearing (descent) 05 08 14Ear pain 01 04 09Hearing loss 00 00 06Difficulty clearing (ascent) 00 01 04Tinnitus 00 01 01Vertigo 00 00 01Ear drainage 00 00 00Other 01 01 02
Eye painEpistaxis (two cases)
"Sinus pain"

396 Konwchak and Werkhaven
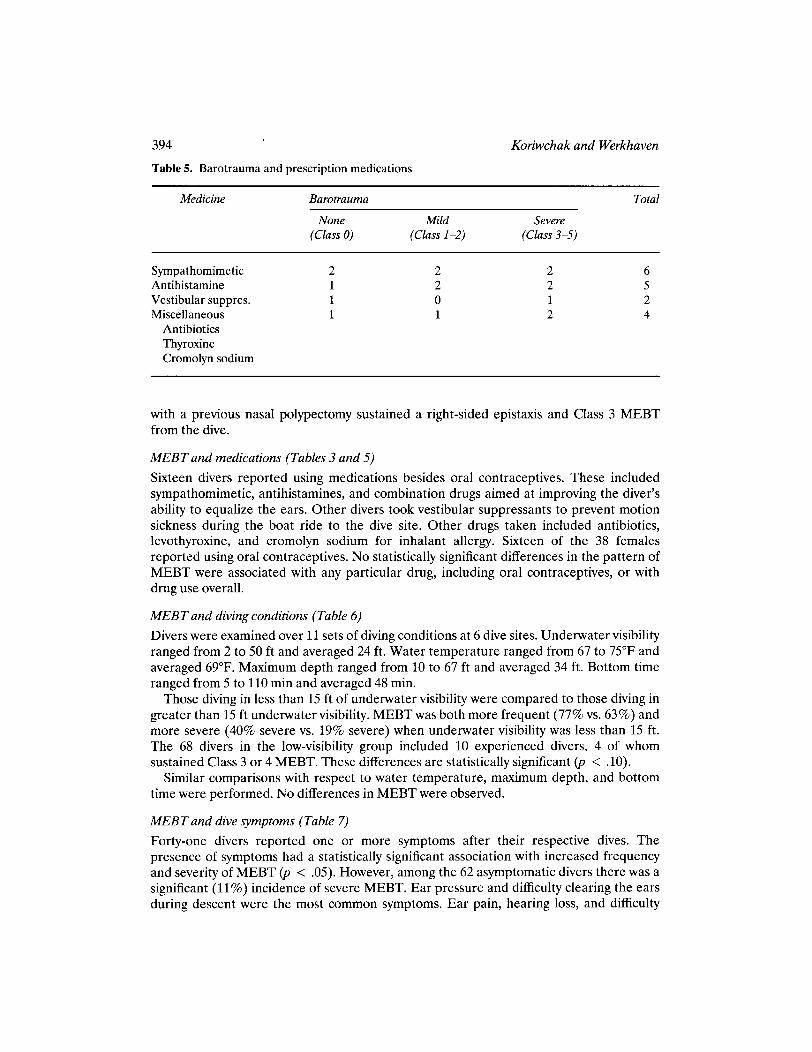
clearing the ears during ascent were less common but were much more strongly predictiveof severe MEBT. Tinnitus, vertigo, and ear drainage were rare. Nonotologic symptomswere all related to sinus barotrauma.
Dividing the divers into symptomatic and asymptomatic groups allows observationsregarding the sensitivity, specificity, and predictive value of symptoms with respect tosevere MEBT. Of the 41 divers reporting symptoms, 20 had severe MEBT, giving thepresence of symptoms a 49% positive predictive value for severe MEBT. Of the 62asymptomatic divers, 55 had either no MEBT or mild MEBT. Thus, the absence ofsymptoms has a predictive value of 89% for the absence of severe MEBT. Similarcalculations yield a sensitivity of 74% and a specificity of 72%.
Discussion
The increasing popularity of sport scuba diving creates a growing group with unique healthproblems. These problems include various forms of barotrauma, decompression sickness,vertigo, loss of consciousness, polluted water, poisoned air supply, otitis, drowning, andtemporomandibular joint syndrome [1-7]. Barotrauma may affect the external, middle, orinner ear, sinuses, lungs, teeth, GI tract, or facial nerve [8].
Physicians are increasingly called upon to advise prospective divers and injured divers oftheir future risk of barotrauma. Risk may be modified by previous barotrauma or bymedical problems such as otitis, sinusitis, allergies, or medications, or previous otolaryngologic procedures. This study attempts to provide some of the data necessary to counseldivers with respect to middle ear barotrauma, the most common hazard of scuba diving.
Of the 103 divers examined, approximately one-third had normal tympanic membranes,40% had mild MEBT (Classes 1 and 2), and 28% had severe MEBT (Classes 3 and 4).Although barotraumatic tympanic membrane perforations (Class 5) are frequently discussed in the literature [1,2,4,7], none were seen in this series. The total incidence ofMEBT in this series was, thus, 68%. This is a considerably higher rate than those of priorreviews. In a study assessing the effect of pseudoephedrine use on MEBT in first-timedivers, Brown et al. [9] noted a rate of of 46% in the control group. Among naval divers intraining, Bayliss found a MEBT rate of only 20% [10]. Neither of these studies examinedpreviously trained divers or attempted to assess the effect of diving conditions on MEBT.A recently published prospective study [11] of 11 divers showed that after 3 days ofrepetitive diving, otoscopy was abnormal in 82% of subjects. However, this study examinedrepetitive diving and examined a much smaller group of divers, all of whom wereexperienced. Middle ear barotrauma was not examined with respect to diver characteristics or diving conditions.
In an effort to identify characteristics among divers associated with an increased risk ofMEBT, divers were analyzed with respect to dive experience, age, sex, past otolaryngologichistory, and medication use including oral contraceptives. No relationship between MEBTand any of these characteristics has ever been suggested, and none was found. It is of someinterest, however, that experienced divers who sustain MEBT may be more likely to have amild case than beginner divers who experience MEBT. This is a reasonable trend to expectif one assumes that experienced divers have more developed ear clearing skills.
No obvious differences in MEBT risk were observed in divers that were takingmedication. There were too few divers encountered who were taking any single medicationto make further observations. Because of the common use of oral contraceptives among

Middle ear barotrauma in divers 397
women, this medication was considered separately. No differences in MEBT occurrencewere found in women taking oral contraceptives.
Prior reviews note that preexisting otolaryngologic conditions such as deviated septumor nasal polyps may raise the risk of barotrauma [2]. Our population included divers with avariety of otolaryngologic disorders including childhood PE tubes, otitis medial externa,inhalant allergy, sinusitis, and nasal polypectomy. The number in any single group was toosmall to draw conclusions regarding the risk of barotrauma. No single group carried asignificantly higher risk. A similar study conducted among pilots also found no relationshipbetween otolaryngologic disorders and barotrauma [5]. Risk factors in this area mayrequire more detailed study.
In order to identify diving conditions that may carry an increased risk of MEBT, itsfrequency and severity were examined with respect to four characteristics commonly usedto describe diving conditions. These were underwater visibility, water temperature,maximum depth, and bottom time. Interpretation of the findings must be tempered by thefact that only 11 dives, and, therefore, 11 sets of diving conditions, were observed. Becausethese did not cover many of the possible combinations of these four characteristics,analysis of each parameter independently is limited.
The most significant observation regarding MEBT and diving conditions is the relationship between MEBT and underwater visibility. MEBT was both more frequent and moresevere when underwater visibility was less than 15 ft. Both experienced and novice diverswere similarly affected. A possible explanation relates the diver's need for an underwatervisual reference to determine relative position and movement underwater. Orientationand balance are coordinated by three systems: visual, proprioceptive, and vestibular [12].Orientation is maintained only if at least two systems are functioning. However, underwater conditions compromise all three of these systems. As the diver is floating freeunderwater, proprioception provides no information about orientation and movement.Because movement and acceleration are damped by the surrounding water, the vestibularsystem's ability to detect movement may be reduced. This leaves the diver to rely heavily onvisual cues to determine orientation and movement underwater. When underwatervisibility is poor, a visual reference is often unavailable. The diver may, therefore,unknowingly undergo significant changes in depth and make no effort to clear the ears.Middle ear barotrauma may result. If this is true, diving techniques such as the use of adescent line (which can provide visual and proprioceptive cues) and expert depth(buoyancy) control may reduce the risk of MEBT.
Middle ear barotrauma may occur at depths as little as 4 ft and presents with pain,hearing loss [2], dizziness, and nausea [1]. Asymptomatic barotrauma has never beenstudied. Among asymptomatic divers, we found a significant incidence of mild barotrauma(45%) and a low but measurable incidence of severe barotrauma (11 %). The three mostfrequent symptoms (difficulty clearing ears during descent, ear pressure during dive, earpain during dive) place the diver at approximately 50% risk of severe MEBT. The lessfrequent symptoms carry a higher risk of severe MEBT. Difficulty with the passive processof clearing ears during ascent is a different and more ominous symptom than difficulty withthe active process of ear clearing during descent. The former carries an 80% risk of severeMEBT, whereas in the latter the risk is only 52%. All six divers with hearing loss hadsevere MEBT.

398
Conclusions
Koriwchak and Werkhaven
1. There is a significant incidence of both mild and severe MEBT in sport scuba divers.However, TM perforations are rare.
2. There is no statistically significant relationship between MEBT and diver age, sex,experience, otolaryngologic history, or medication use.
3. MEBT may be more common and more severe when underwater visibility is less than 15ft.
4. The most common symptoms of MEBT are ear pressure and/or pain during the dive,and difficulty with ear clearing during descent. Difficulty with ear clearing during ascentand hearing loss after the dive are less common symptoms but are much strongerpredictors of MEBT.
5. The incidence of asymptomatic MEBT is low but significant.
Acknowledgments:
The authors are grateful to the following dive shops for their assistance in the project: BIueWater Scuba, Nashville, TN; Scuba South, Nashville, TN; Captain Corky's Dive Shop, KeyLargo, FL; Sea Dwellers Dive Shop, Key Largo, FL; Looe Key Reef and Resort Center,Ramrod Key, FL.
References
1. Replogle, W.H., Sanders, S.D., Keeton, J.E., and Phillips, D.M. Scuba diving injuries. Ann.Family Practice 1988; 37(6), 135-42.
2. Becker, G.D. Barotrauma resulting from scuba diving: An otolaryngological perspective. Physician Sports Med 1985; 13(3).
3. Becker, G.D. and Parell, G.J. Medical examination of the sport scuba diver. Otolaryngol HeadNeck Surg 1983; 91, 246-50.
4. Pullen, F.W. Otolaryngological aspects of diving. Insights Otolaryngol1990; 5(4).5. Ashton, D.H. and Watson, L.A. The use of tympanometry in predicting otic barotrauma. Aviat
Space Environ Med 1990; 61, 56-61.6. Kizer, Kenneth W. Medical aspects of scuba diving. In: Noble J., ed. Textbook of General
Medicine and Primary Care. Boston: Little, Brown and Co. 1987: 365-76.7. Becker, G.D. and Parell, G.J. Medical aspects of scuba diving. Instructional Course, American
Academy ofOtolaryngology-Head and Neck Surgery, September, 1986.8. Becker, G.D. Recurrent alternobaric facial paralysis resulting from scuba diving. Laryngoscope
1983; 93, 596--7.9. Brown, M., Jones, J., and Krohmer, J. Pseudoephedrine for the prevention of barotitis media: A
controlled clinical trial in underwater divers. Ann Emerg Med 1992; 21, 849-52.10. Bayliss, c.J.A. Aural barotrauma in naval divers. Arch Otolaryngol1968; 88, 49-55.11. Green, S.M., Rothrock, S.G., Hummel, C.B., and Green, E.A. Incidence and severity of middle
ear barotrauma in recreational scuba diving. J Wilderness Med 1993; 4, 270-80.12. Baldwin, R.L. Differential diagnosis of a dizzy patient. Medical Rounds 1990; 3(3),103-113.


















