
Microvascular approach to scalp replantation and reconstruction: A thirty-six year experience
7
MICROVASCULAR APPROACH TO SCALP REPLANTATION AND RECONSTRUCTION: A THIRTY-SIX YEAR EXPERIENCE FERNANDO HERRERA, M.D., 1,2 RUDOLF BUNTIC, M.D., 1 DARRELL BROOKS, M.D., 1 GREGORY BUNCKE, M.D., 1 and ANUJA K. ANTONY, M.D., M.P.H. 1,3 * Background: Soft tissue defects of the scalp may result from multiple etiologies and can be challenging to reconstruct. We discuss our ex- perience with scalp replantation and secondary microvascular reconstruction over 36 years, including techniques pioneered at our institu- tion with twin–twin scalp allotransplant and innervated partial superior latissimus dorsi (LD) for scalp/frontalis loss. Methods: A retrospec- tive review of all patients presenting with scalp loss requiring microvascular reconstruction at a single center was performed from January 1971 to January 2007. Medical records were reviewed for age, gender, defect size/location, etiology, type of reconstruction, recipient ves- sels used, vein grafts, and complications. Results: Thirty-three patients were identified; mean age was 33 years (range, 7–79). Mean scalp defect size was 442 cm 2 (range, 120–900 cm 2 ). Thirty-six microvascular reconstructions were performed; of these, 10 scalp replants and 26 microvascular tissue transfers. Of these 26, 17 were LD based (partial superior LD with and without reinnervation, LD combined with serratus, LD combined with parascapular, LD combined with split rib, LD only) and 2 free scalp allotransplant among others. The superfi- cial temporal artery and vein was used as recipient vessels in 70% of cases. Overall, microvascular success rate was 92%; complications occurred in 14 cases, nine major (tumor recurrence [n 5 2], partial flap loss [n 5 2], replant loss [n 5 3, size <300 cm 2 ], hematoma [n 5 2]) and five minor (donor site seroma /hematoma [n 5 3], flap congestion [n 5 1], superficial wound infection [n 5 1]). Conclusions: Every attempt should be made at scalp replantation when the patient is stable and the parts salvageable. Larger avulsion defects had higher suc- cess rates after replantation than smaller defects (<300 cm 2 ), with the superficial temporal artery and vein most commonly used for recipi- ent vessels (P 5 0.0083). Microvascular tissue transfer remains a mainstay of treatment for scalp defects, with LD-based flaps, demon- strating excellent versatility for a range of defects. V V C 2012 Wiley Periodicals, Inc. Microsurgery 00:000–000, 2012. Soft tissue defects of the scalp can arise from acute trauma, extirpation of tumors, radiation necrosis, and other iatrogenic causes. Reconstructing these defects can be challenging to the plastic surgeon depending on the underlying etiology. In the setting of trauma, shearing forces applied to the scalp may result in avulsion at the loose areolar tissue layer between the galea and the peri- osteum. The exact defect size will vary, depending on specific direction and strength of the force applied. To obtain good functional and cosmetic results, immediate revascularization using microsurgical techniques and replacement of the scalp in the correct anatomical position is the procedure of choice whenever possible. Secondary reconstruction is required when the avulsed portion of the scalp is unsalvageable or fails replantation. Alternatively, chronic wounds and extirpation of tumors of the scalp will also require secondary reconstruction. Microvascular transfers are often adopted in lieu of local flaps and tissue expansion when the defects are large and stable soft tissue coverage is not available. Prior to the advent of microsurgical techniques, replacement of the avulsed scalp as a composite graft was largely unsuccess- ful. 1 Miller et al. 2 were the first to report successful microvascular replantation of the entire scalp. Since then, advances in techniques and widespread use of microsur- gery over the last several decades have made revasculari- zation and secondary reconstruction of such defects not only possible but aesthetically pleasing. 3–5 We discuss our experience with scalp replantation and secondary microvascular reconstruction over 36 years at a single institution. PATIENTS AND METHODS A retrospective chart review was performed for all patients presenting with scalp loss that required microvas- cular techniques to reconstruct the defect by either replantation of native scalp or with the use of free tissue transplantation from January 1971 to January 2007 at a single institution (The Buncke Clinic, Division of Micro- surgical Transplantation and Replantation, San Francisco, CA). Table 1 summarizes the patient’s demographic data. The medical records were reviewed for age, gender, defect size/location, etiology, type of reconstruction, flap choice, recipient vessels used, vein grafts, complications, and follow-up. Complications were recorded and divided into two categories: major and minor. Major flap-related complications included early return to the operating room for exploration or hematoma evacuation, partial or complete flap loss, and tumor recurrence. Minor compli- cations included superficial wound infections, donor site hematoma or seroma, and mild flap congestion treated 1 The Buncke Clinic and Division of Microsurgery, California Pacific Medical Center, San Francisco, CA 2 University of California Los Angeles, Division of Plastic and Reconstructive Surgery, Los Angeles, CA 3 Division of Plastic and Reconstructive Surgery, University of Illinois at Chi- cago, Chicago, IL *Correspondence to: Anuja K Antony, M.D., M.P.H., Director of Microsur- gery, Division of Plastic and Reconstructive Surgery, University of Illinois at Chicago Medical Center, Chicago, Illinois. E-mail: [email protected] Received 20 January 2012; Accepted 6 July 2012 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/ micr.22037 V V C 2012 Wiley Periodicals, Inc.
-
Upload
fernando-herrera -
Category
Documents
-
view
213 -
download
0
Transcript of Microvascular approach to scalp replantation and reconstruction: A thirty-six year experience

MICROVASCULAR APPROACH TO SCALP REPLANTATION ANDRECONSTRUCTION: A THIRTY-SIX YEAR EXPERIENCE
FERNANDO HERRERA, M.D.,1,2 RUDOLF BUNTIC, M.D.,1 DARRELL BROOKS, M.D.,1
GREGORY BUNCKE, M.D.,1 and ANUJA K. ANTONY, M.D., M.P.H.1,3*
Background: Soft tissue defects of the scalp may result from multiple etiologies and can be challenging to reconstruct. We discuss our ex-perience with scalp replantation and secondary microvascular reconstruction over 36 years, including techniques pioneered at our institu-tion with twin–twin scalp allotransplant and innervated partial superior latissimus dorsi (LD) for scalp/frontalis loss. Methods: A retrospec-tive review of all patients presenting with scalp loss requiring microvascular reconstruction at a single center was performed from January1971 to January 2007. Medical records were reviewed for age, gender, defect size/location, etiology, type of reconstruction, recipient ves-sels used, vein grafts, and complications. Results: Thirty-three patients were identified; mean age was 33 years (range, 7–79). Mean scalpdefect size was 442 cm2 (range, 120–900 cm2). Thirty-six microvascular reconstructions were performed; of these, 10 scalp replants and26 microvascular tissue transfers. Of these 26, 17 were LD based (partial superior LD with and without reinnervation, LD combined withserratus, LD combined with parascapular, LD combined with split rib, LD only) and 2 free scalp allotransplant among others. The superfi-cial temporal artery and vein was used as recipient vessels in 70% of cases. Overall, microvascular success rate was 92%; complicationsoccurred in 14 cases, nine major (tumor recurrence [n 5 2], partial flap loss [n 5 2], replant loss [n 5 3, size <300 cm2], hematoma [n 52]) and five minor (donor site seroma /hematoma [n 5 3], flap congestion [n 5 1], superficial wound infection [n 5 1]). Conclusions: Everyattempt should be made at scalp replantation when the patient is stable and the parts salvageable. Larger avulsion defects had higher suc-cess rates after replantation than smaller defects (<300 cm2), with the superficial temporal artery and vein most commonly used for recipi-ent vessels (P 5 0.0083). Microvascular tissue transfer remains a mainstay of treatment for scalp defects, with LD-based flaps, demon-strating excellent versatility for a range of defects. VVC 2012 Wiley Periodicals, Inc. Microsurgery 00:000–000, 2012.
Soft tissue defects of the scalp can arise from acute
trauma, extirpation of tumors, radiation necrosis, and
other iatrogenic causes. Reconstructing these defects can
be challenging to the plastic surgeon depending on the
underlying etiology. In the setting of trauma, shearing
forces applied to the scalp may result in avulsion at the
loose areolar tissue layer between the galea and the peri-
osteum. The exact defect size will vary, depending on
specific direction and strength of the force applied. To
obtain good functional and cosmetic results, immediate
revascularization using microsurgical techniques and
replacement of the scalp in the correct anatomical
position is the procedure of choice whenever possible.
Secondary reconstruction is required when the avulsed
portion of the scalp is unsalvageable or fails replantation.
Alternatively, chronic wounds and extirpation of tumors
of the scalp will also require secondary reconstruction.
Microvascular transfers are often adopted in lieu of local
flaps and tissue expansion when the defects are large and
stable soft tissue coverage is not available. Prior to the
advent of microsurgical techniques, replacement of the
avulsed scalp as a composite graft was largely unsuccess-
ful.1 Miller et al.2 were the first to report successful
microvascular replantation of the entire scalp. Since then,
advances in techniques and widespread use of microsur-
gery over the last several decades have made revasculari-
zation and secondary reconstruction of such defects not
only possible but aesthetically pleasing.3–5 We discuss
our experience with scalp replantation and secondary
microvascular reconstruction over 36 years at a single
institution.
PATIENTS AND METHODS
A retrospective chart review was performed for all
patients presenting with scalp loss that required microvas-
cular techniques to reconstruct the defect by either
replantation of native scalp or with the use of free tissue
transplantation from January 1971 to January 2007 at a
single institution (The Buncke Clinic, Division of Micro-
surgical Transplantation and Replantation, San Francisco,
CA). Table 1 summarizes the patient’s demographic data.
The medical records were reviewed for age, gender,
defect size/location, etiology, type of reconstruction, flap
choice, recipient vessels used, vein grafts, complications,
and follow-up. Complications were recorded and divided
into two categories: major and minor. Major flap-related
complications included early return to the operating room
for exploration or hematoma evacuation, partial or
complete flap loss, and tumor recurrence. Minor compli-
cations included superficial wound infections, donor site
hematoma or seroma, and mild flap congestion treated
1The Buncke Clinic and Division of Microsurgery, California Pacific MedicalCenter, San Francisco, CA2University of California Los Angeles, Division of Plastic and ReconstructiveSurgery, Los Angeles, CA3Division of Plastic and Reconstructive Surgery, University of Illinois at Chi-cago, Chicago, IL
*Correspondence to: Anuja K Antony, M.D., M.P.H., Director of Microsur-gery, Division of Plastic and Reconstructive Surgery, University of Illinois atChicago Medical Center, Chicago, Illinois. E-mail: [email protected]
Received 20 January 2012; Accepted 6 July 2012
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/micr.22037
VVC 2012 Wiley Periodicals, Inc.

conservatively. Fisher’s exact test was performed to ana-
lyze flap failure based on flap size.
RESULTS
Between January 1971 and January 2007, 33 patients
were identified with scalp defects requiring microvascular
reconstruction to replant or cover these acquired defects.
A total of 36 microvascular tissue transfers or replanta-
tions were performed in 33 patients (Fig. 1). Overall, mi-
crovascular success rate in our series was 92%. There
were 17 male and 16 female patients. The average age
was 33 years, ranging from 7 to 79 years and the average
defect size was 442 cm2 (range, 120–900 cm2). The
mean follow-up in our study was 32 months, ranging
from 8 months to 6 years. The soft tissue defects resulted
from a variety of etiologies. Eighteen of these patients
sustained traumatic avulsion of a portion or total scalp;
eight of which were not amenable to replantation. The
majority of the patients in the traumatic group were
female (12) versus male (6). The avulsion injuries were
secondary to motor vehicle accidents in 14 patients, one
go-kart accident, one linen press accident, one drive shaft
accident, and one mountain lion attack. Tumor extirpation
resulted in eight scalp defects; three defects from unsta-
ble scars/chronic wounds; two resulting from radiation
necrosis while treating a scalp malignancy; one wound
was the result of electrical burn; and one wound was
from a birth-related injury.
Ten scalp replants were performed; three failed and
required further reconstruction. One failed replant resulted
from a large scalp hematoma, resulting in extrinsic com-
pression of the pedicle. The other two failures resulted
from venous thrombosis in the early postoperative period.
All three cases resulted in a secondary surgery for explo-
ration and attempts at salvage. Partial avulsion replants of
Table 1. Patient Demographics and Summary
Patient Sex Age Etiology Reconstruction Recipient vessels Vein graft Complications
1 M 26 Avulsion Replanted scalp STAx2, PA Yes None
2 F 17 Avulsion Replanted scalp STA,SOA/STV Yes SSI
3 F 10 Avulsion Replanted scalp STA/FV No None
4 F 27 Avulsion Replanted scalp X No None
5 F X Avulsion Replanted scalp STA/STV Yes None
6 F 33 Avulsion Replanted scalp STA/STV Yes None
7* F 21 Avulsion Replanted scalp STA/STV x Failed replant
8* M X Avulsion Replanted scalp Occipital A/V Yes Failed replant
9* F X Avulsion Replanted scalp STA/STV Yes Failed replant
10 F 22 Avulsion LD/Serratus ant FA/FV No None
11 F 17 Avulsion Latissimus STA/STV No None
12 M 39 Avulsion LD/parascapular X No None
13 M 17 Avulsion Radial FFF X Yes None
14 M 43 Avulsion Partial superior latissimus STA/STV, TdN Yes None
15 M 70 Avulsion Partial superior latissimus STA/FV No Donor site hematoma
16 F 24 Avulsion Latissimus FA/FV No None
17 F 22 Avulsion LD/serratus ant FA/FV No None
18a** F 23 Avulsion Replanted partial scalp LSTA/STV Yes None
b 24 Partial free scalp R STA/STV Yes Hematoma
c 29 Partial free scalp L STA/STV Yes Flap congestion
19 M 29 Neurofibroma Omentum STA/STV No None
20 M 15 Electrical Groin flap STA/STV No Hematoma
21 M 59 Basal cell Groin flap STA/STV No Tumor recurrence
22a** M 7 Congenital Groin flap Occipital A/V Yes Partial flap loss
b Latissimus Sup thyroid a. Yes None
23 M 60 Meningioma Latissimus Occipital A/V Yes Donor site seroma
24 F 17 Medulloblastoma Latissumus STA/STV No None
25 M 32 Fibrosarcoma LD/split rib graft STA/STV No None
26 M 35 Chronic wound Latissimus STA/STV No Partial flap loss
27 F 45 Dermatofibrosarcoma Serratus ant FA/FV No None
28 M 57 Chronic wound Latissimus STA/STV No Donor site seroma
29 M 10 Neurofibrosarcoma Latissimus STA/STV No None
30 M 33 XRT necrosis Serratus ant STA/STV No None
31 F 58 Meningioma Latissimus STA/STV No None
32 F 45 XRT necrosis Latissimus STA/STV No None
33 M 79 Chronic wound Latissimus STA/STV Yes Marjolin ulcer
*Patients 7,8,9 had flap dimensions <300 cm2.**Patient 18 had three microvascular procedures, one partial replantation, and two partial scalp allotransplantation flaps from her twin sister and is designatedas 18 a, b, and c. Patient 22 had two flaps and is designated as 22a and b.
2 Herrera et al.
Microsurgery DOI 10.1002/micr

<300 cm2 were designated as small and those >301 cm2
were designated as large. Smaller replant size <300 cm
was significantly associated with failure (P 5 0.0083).
Secondary microvascular scalp reconstruction was per-
formed in the remaining 23 patients; all secondary flaps
completely survived except for two cases which sustained
partial flap loss. A total of 26 microvascular free tissue
transfers were performed in the secondary reconstruction
group. Flap choices included 17 latissimus dorsi (LD)-
based flaps (two partial superior LD flaps with and without
reinnervation, two LD combined with serratus flap, one LD
combined with parascapular flap, one LD combined with
split rib, and 11 LD only flaps with STSG), three groin
flaps, two serratus anterior flaps, two partial scalp allotrans-
plants from an identical twin, one omental flap, and one
radial forearm fasciocutaneous free flap.
A variety of recipient vessels were used including the
superficial temporal (ST) artery (n 5 26), facial artery
(n 5 4), occipital artery (n 5 3), superior thyroid artery
(n 5 1), supra-orbital artery (n 5 1), and postauricular
artery (n 5 1). The majority of recipient veins used were
the ST veins (>70%), followed by facial vein, and occi-
pital vein in three patients. Vein grafts were required in
15 cases (seven in primary replant and eight in secondary
reconstructive). Overall complications occurred in 14
cases (39%); these were divided into nine major and five
minor complications (Fig. 2). There was no significant
difference in complications between the cases with the
use of vein graft compared to those without (P 5 0.286)
(Table 2). During the third twin–twin transplant operation
(of three surgeries performed in one set of twins), superfi-
cial subcutaneous veins were used for outflow. Postopera-
tively, the flap became very congested requiring leech
therapy. The twins were HLA identical and crossmatched
against each other with no reaction and for that reason
antirejection medications were not used. A representative
case is shown in Figures 3–6.
DISCUSSION
Scalp defects may result from a number of causes
including traumatic, oncologic resection, iatrogenic, radia-
tion induced, and congenital. Replacement of absent tis-
sue can be challenging to the reconstructive surgeon
especially in the face of previous operations, radiation, or
a severely scarred wound bed.6,7 The treatment is based
on the underlying cause, size of the defect, status of the
avulsed parts, and available recipient vessels. Tradition-
ally, scalp reconstruction options range from primary
repair with galeal scoring for small defects (<300 cm2),
local advancement, or rotational flaps for moderate size
defects (2–25 cm2), skin grafting if pericranium is pres-
ent, staged tissue expansion, rotational Orticochea-type
flaps for large defects, and finally microvascular tissue
transfer for very large defects that cannot be managed
Figure 1. Reconstructive flap choices. Scalp replant n 5 10, latissi-
mus only þSTSG (LD only) n 5 11, groin flap (GF) n 5 3, radial
forearm fasciocutaneous free flap (RFFC) n 5 1, omentum n 5 1,
partial superior latissimus (PS-LD) n 5 2, partial free scalp allotrans-
plantation (Scalp Allo) n 5 2, serratus anterior (SA) n 5 2, Latissi-
musþserratus (LD-SA) n 5 2, Latissimus-parascapular (LD-Para) n
5 1, Latissimus-split rib (LD-rib) n 5 1. [Color figure can be viewed
in the online issue, which is available at wileyonlinelibrary.com.]
Figure 2. Microvascular anastomoses. Superficial temporal artery
(STA), facial artery (FA), postauricular artery (PA), occipital artery
(OA), supraorbital artery (SOA), and superior thyroid artery (sup
thyroid). [Color figure can be viewed in the online issue, which is
available at wileyonlinelibrary.com.]
Table 2. Major and Minor Complications
Complication N %
Major 9 25
Tumor recurrence 2 5.6
Partial flap loss 2 5.6
Failed replanted scalp 3 8.3
Flap hematoma 2 5.6
Minor 5 13.8
Superficial wound infection 1 2.7
Donor site hematoma 1 2.7
Donor site seroma 2 5.6
Flap congestion 1 2.7
Total 14 38.8
Microvascular Approach 3
Microsurgery DOI 10.1002/micr
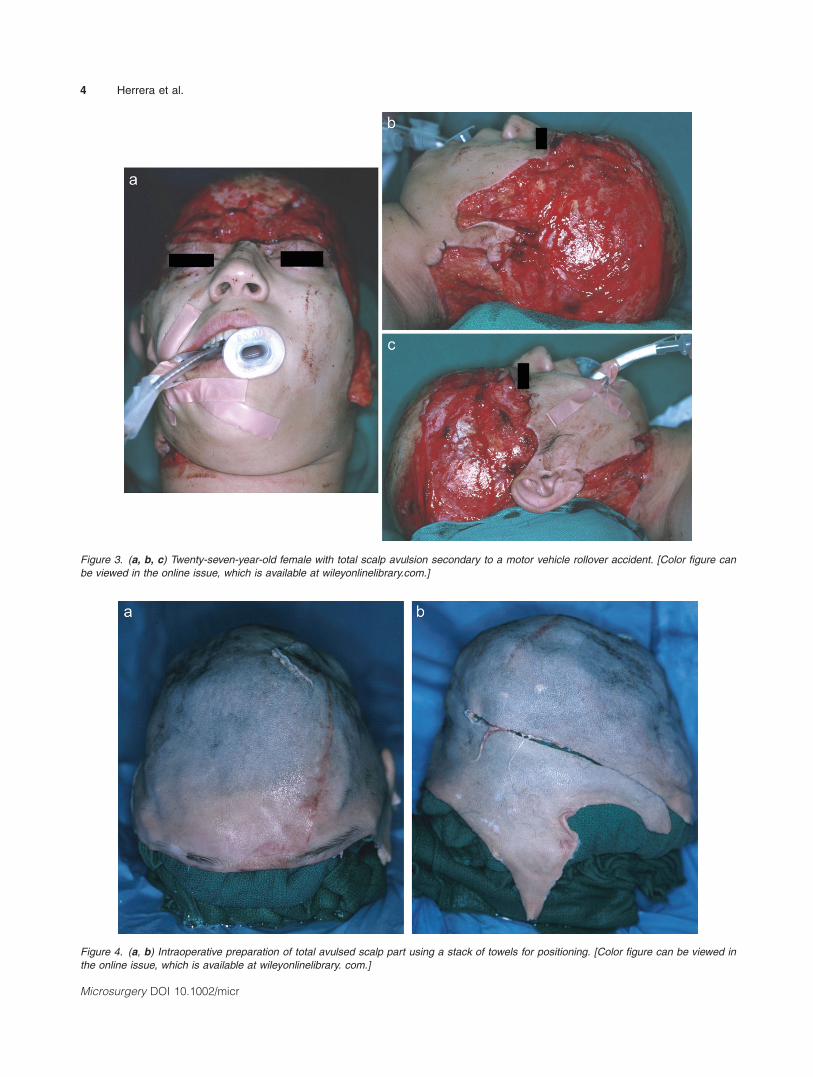
Figure 3. (a, b, c) Twenty-seven-year-old female with total scalp avulsion secondary to a motor vehicle rollover accident. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Figure 4. (a, b) Intraoperative preparation of total avulsed scalp part using a stack of towels for positioning. [Color figure can be viewed in
the online issue, which is available at wileyonlinelibrary. com.]
4 Herrera et al.
Microsurgery DOI 10.1002/micr

with alternative techniques.8,9 Microvascular techniques
offer solutions for managing the challenging scalp region
where often local or regional options are limited or
unavailable. Immediate microvascular replantation of par-
tial or complete scalp avulsions injuries should be
attempted in all cases if the patient is stable and the part
is salvageable. Replacing ‘‘like-with-like’’ tissue will
result in the most favorable outcome. Secondary micro-
vascular reconstruction should be reserved for situations
where the avulsed scalp is not salvageable, failed scalp
replantation, and acquired defects.
In our series, the etiology of scalp defects was di-
vided into either acute traumatic or secondary acquired
scalp wounds owing to various causes. In the traumatic
group, over half of the patients underwent scalp replanta-
tion. The remaining eight patients were not candidates for
replantation either secondary to nonsalvageable parts or
delayed presentation. Vein grafts were necessary in two-
thirds of the scalp replantations to avoid microvascular
anastomosis within the zone of injury. We performed both
single arterial and multiple arterial anastomoses in our
replantation group. The ST vessels were used as the pri-
mary recipient vessels in all but one case. The single case
in which the ST vessels were not used was owing to the
posterior location of the defect and the occipital vessels
were used in this patient. The consistent anatomy of the ST
artery makes this a reliable recipient vessel for use in mi-
crovascular surgery.10–12 In the three failed replants, the
partial scalp defect was <300 cm2 and a single arterial and
venous anastomosis were performed. The recipient vessels
used in the failed replants included occipital vessels (n 5
1) and ST vessels (n 5 2), and vein grafting was used in
two cases. Limitations in vessel availability incurring
inflow/outflow obstruction and restricted dimensions (of
the avulsed portion) for adequate debridement of trauma-
tized tissue likely played a role in ultimate failure of the
less sizeable partial scalp replantations.
Very few large series of scalp replantation exist in
the literature since the first successful attempt performed
in 1976.2 Cheng et al. described their series of 20
patients all with avulsion injuries of the scalp. They
reported complete replant survival in 16, partial survival
Figure 5. (a–c) Intraoperative images of 27-year-old female with total scalp avulsion after successful scalp replantation. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Microvascular Approach 5
Microsurgery DOI 10.1002/micr

in three, and one failure.13 They advocated for the use of
at least two arteries and vein grafts to debride all possi-
bly injured vessels. Yin et al. reported a series of eight
patients of which three injuries were actually a result of
sharp amputation.14 There was only one case that resulted
in failure. This resulted from venous congestion as no
vein was performed owing to extensive injury to the flap.
They reported that the use of single or multiple arterial
anastomoses had little effect on successful outcomes;
rather, the venous outflow was the critical issue.
The LD flap (in various forms) was the most com-
monly used microvascular tissue transfer in our series
(65%). The LD muscle free flap, popularized by Maxwell
and Godina, can be used to cover large scalp defects.15,16
This flap can also be expanded as a combined flap for
very large defects or when one needs to reconstruct com-
posite tissue, such as skin, muscle, and bone.17–19 In our
series, the LD flap was combined with serratus, parascap-
ular, and split rib to address composite and more exten-
sive defects. For smaller defects, the latissimus can be
split longitudinally on a transverse intramuscular branch
of the thoracodorsal vessels to address ‘‘rectus muscle-
sized’’ defects. Our institution first described the latissi-
mus muscle flap as a partial superior latissimus flap,
thereby preserving form and muscle function.20 This
modification was used in two cases of smaller size
defects (150 cm2), one of which was used for innervated
reconstruction (using the thoracodorsal nerve) of lost
frontalis function with successful restoration. Preservation
of the cutaneous paddle over the anterior two-thirds of
the muscle is possible21; however, we generally prefer
split thickness skin grafts as coverage to allow the muscle
flap to atrophy over time and give a better overall aes-
thetic appearance in nonhair-bearing males. The large
size, predictable blood supply, long pedicle, versatility,
and ease of harvesting this flap make this our first choice
for scalp coverage when necessary.
We have also used a number of alternative free tissue
transfers to cover moderate to large sized defects. Partial
scalp tissue allotransplantation, omentum, radial forearm
fasciocutaneous, groin, and serratus flaps were included
in this series. Several authors have reported the use of al-
ternative flaps to cover moderate to large sized defects,
such as the anterolateral thigh flap, deep inferior epigas-
tric perforator flaps, and medial arm flaps with good
results.4,22–25
The omentum was used in one patient for a subtotal
defect after tumor extirpation. This microvascular flap is
ideal for large defects in highly irradiated wound beds.26
The major disadvantage is the donor site morbidity owing
to a midline laparotomy required to harvest the tissue.
Our institution first reported a pre-expanded twin–twin
scalp allotransplant tissue transfer in 1990 for reconstruc-
tion of a traumatic scalp defect that was partially treated
with replantation.27 Although composite tissue allotrans-
plantation (CTA) for the scalp in a nontwin donor has
Figure 6. (a, b) Twenty-seven-year-old female 1-year postoperative result after total scalp replantation. [Color figure can be viewed in the
online issue, which is available at wileyonlinelibrary.com.]
6 Herrera et al.
Microsurgery DOI 10.1002/micr

yet to be described, increasing understanding of immuno-
suppressive therapy and the development of CTA pro-
grams may pave the way for expanding microvascular
methods for treating scalp defects. Still, further refine-
ments may develop with the incorporation of improved
imaging and virtual planning technologies in secondary
reconstruction patients.28,29
CONCLUSIONS
The overall microvascular success rate in our series
was 92% which is consistent with the literature’s success
rates.30 Reconstruction of scalp defects can be challeng-
ing and many options exist based on the size of the
defect and etiology. In acute traumatic injuries, every
attempt should be made at replantation when the patient
is stable and the parts are salvageable. Larger scalp avul-
sion defects appear to have a greater success rates when
compared to smaller partial scalp avulsions (<300 cm2)
injuries. Free microvascular tissue transfers for secondary
scalp reconstruction remain a mainstay of treatment. LD-
based free muscle flaps are useful for this location with
high versatility for a range of defects and minimal mor-
bidity in skilled hands.
REFERENCES
1. Gottlieb LJ, Krieger LM. From the reconstructive ladder to thereconstructive elevator. Plast Reconstr Surg 1994;93:1503–1504.
2. Miller GD, Anstee EJ, Snell JA. Successful replantation of anavulsed scalp by microvascular anastomoses. Plast Reconstr Surg1976;58:133–136.
3. Newman MI, Hanasono MM, Disa JJ, Cordeiro PG, Mehrara BJ.Scalp reconstruction: a 15-year experience. Ann Plast Surg2004;52:501–506.
4. Lutz BS. Aesthetic and functional advantages of the anterolateralthigh flap in reconstruction of tumor-related scalp defects. Microsur-gery 2002;22:258–264.
5. Pennington DG, Stern HS, Lee KK. Free-flap reconstruction of largedefects of the scalp and calvarium. Plast Reconstr Surg1989;83:655–661.
6. Serafin D, Deland M. Reconstruction with vascularized compositetissue in patients with excessive injury following surgery and irradia-tion. Ann Plast Surg 1982;8:35.
7. Robson MC, Zachary LS, Schmidt DR, Faibisoff B, Hekmatpanah J.Reconstruction of large cranial defects in the presence of heavy radi-ation damage and infection utilizing tissue transferred by microvas-cular anastomoses. Plast Reconstr Surg 1989;83:438–442.
8. Leedy JE, Janis JE, Rohrich RJ. Reconstruction of acquired scalpdefects: An algorithmic approach. Plast Reconstr Surg 2005;116:54–72.
9. Lee B, Bickel K, Levin S. Microsurgical reconstruction of extensivescalp defects. J Reconstr Microsurg 1999;15:255–262; discussion263–264.
10. Lipa JE, Butler CE. Enhancing the outcome of free latissimus dorsimuscle flap reconstruction of scalp defects. Head Neck 2004;26:46–53.
11. Hansen SL, Foster RD, Dosanjh AS, Mathes SJ, Hoffman WY, LeonP. Superficial temporal artery and vein as recipient vessels for facialand scalp microsurgical reconstruction. Plast Reconstr Surg.2007;120:1879–1884.
12. van Driel AA, Mureau MA, Goldstein DP, Gilbert RW, Irish JC,Gullane PJ, Neligan PC, Hofer SO. Aesthetic and oncologic outcomeafter microsurgical reconstruction of complex scalp and foreheaddefects after malignant tumor resection: an algorithm for treatment.Plast Reconstr Surg 2010;126:460–470.
13. Cheng K, Zhou S, Jiang K, Wang S, Dong J, Huang W, Chang T.Microsurgical replantation of the avulsed scalp: report of 20 cases.Plast Reconstr Surg 1996;97:1099–1106.
14. Yin JW, Matsuo JM, Hsieh CH, Yeh MC, Liao WC, Jeng SF.Replantation of total avulsed scalp with microsurgery: Experience ofeight cases and literature review. J Trauma 2008;64:796–802.
15. Maxwell GP, Stueber K, Hoopes JE. A free latissimus dorsi myocu-taneous flap: Case report. Plast Reconstr Surg 1978;62:462–466.
16. Godina M. The tailored latissimus dorsi free flap. Plast ReconstrSurg 1987;80:304–306.
17. Takayanagi S, Ohtsuka M, Tsukie T. Use of the latissimus dorsi andthe serratus anterior muscles as a combined flap. Ann Plast Surg1988;20:333–339.
18. Whitney TM, Buncke HJ, Alpert BS, Buncke GM, LineaweaverWC. The serratus anterior free-muscle flap: Experience with 100consecutive cases. Plast Reconstr Surg 1990;86:481–489.
19. Lee JW, Hsueh YY, Lee JS. Composite skull and dura defect recon-struction using combined latissimus dorsi musculocutaneous and ser-ratus anterior muscle-rib free flap coupled with vascularized galeatransfer: A case report. Microsurgery 2010;30:632–635.
20. Buntic RF, Horton KM, Brooks D, Lee CK. The free partial superiorlatissimus muscle flap: Preservation of donor-site form and function.Plast Reconstr Surg 2008;121:1659–1663.
21. Moelleken BR, Mathes SA, Chang N. Latissimus dorsi muscle-mus-culocutaneous flap in chest-wall reconstruction. Surg Clin North Am1989;69:977–990.
22. Lutz BS, Wei FC, Chen HC, Lin CH, Wei CY. Reconstruction ofscalp defects with free flaps in 30 cases. Br J Plast Surg1998;51:186–190.
23. Ioannides C, Fossion E, McGrouther AD. Reconstruction for largedefects of the scalp and cranium. J Craniomaxillofac Surg1999;27:145–152.
24. Haddock MC, Creagh T, Sivarajan V. Double-free, flow-through flapreconstruction for complex scalp defects: A case report. Microsur-gery 2011;31:327–330.
25. Chang KP, Lai CH, Chang CH, Lin CL, Lai CS, Lin SD. Free flapoptions for reconstruction of complicated scalp and calvarial defects:Report of a series of cases and literature review. Microsurgery2010;30:13–18.
26. Losken A, Carlson GW, Culbertson JH, Scott Hultman C, KumarAV, Jones GE, Bostwick J 3rd, Jurkiewicz MJ. Omental free flapreconstruction in complex head and neck deformities. Head Neck2002;24:326–331.
27. Furnas H, Lineaweaver WC, Alpert BS, Buncke HJ. Scalp recon-struction by microvascular free tissue transfer. Ann Plast Surg1990;24:431–444.
28. Antony AK, Chen WF, Kolokythas A, Weimer KA, Cohen MN. Useof virtual surgery and stereolithography-guided osteotomy for man-dibular reconstruction with the free fibula. Plast Recon Surg2011;128:1080–1084.
29. Karanas YL, Antony A, Rubin G, Chang J. Preoperative CT angiog-raphy for free fibula transfer. Microsurgery 2004;24:125–127.
30. Khouri RK, Cooley BC, Kunselman ,AR, Landis JR, Yeramian P,Ingram D, Natarajan N, Benes CO, Wallemark C. A prospectivestudy of microvascular free-flap surgery and outcome. Plast ReconstrSurg 1998;102:711.
Microvascular Approach 7
Microsurgery DOI 10.1002/micr








![Intentional Replantation: An Updated Protocols in ... · conventional treatment, and accidental avulsion (unintentional replantation) [8]. On the other hand, contraindications of](https://static.fdocuments.us/doc/165x107/5ed55ef56933f508e973f125/intentional-replantation-an-updated-protocols-in-conventional-treatment-and.jpg)









