From Teaching Argument Writing by George Hillocks Jr. English III.

MICROTIA Emily Tignor, MD
Faculty Advisor: Shraddha Mukerji, MD The University of Texas Medical Branch
Department of Otolaryngology Grand Rounds Presentation
October 30, 2013

DISCUSSION TOPICS
Embryology
Etiology
Presentation
Associated Anomalies
Classification
Management
AURICLE EMBRYOLOGY
Week 5 (inner ear week 3)
1st and 2nd branchial arches
Hillocks 1-6
1-3: 1st branchial arch
4-6: 2nd branchial arch
Multiple theories of embryogenesis of final auricular structure
AURICLE EMBRYOLOGY
Traditional theory:
1 = tragus,
2,3 = helix,
4,5 = anti helix,
6 = anti tragus and lobule
Other theories: 4-6 form 85% of the auricle

AURICLE EMBRYOLOGY

AURICLE and EAC EMBRYOLOGY
Migration:
Starts anterior
Migrates dorsal and cephalic: weeks 8-12
Final position: 20 weeks
EAC:
1st branchial cleft
Epithelial plug: weeks 4-5
Begins recanalization: week 21
Open with formed TM: week 28

MICROTIA ETIOLOGY
Vascular
Stapedial artery insult
Teratogens
Retinoic acid inhibitors
Thalidomide
Mycophenolate mofetil
Genetic
Chromosomal: XO, Trisomy 13, 15, 18, 21, 22
Other mutations: Treacher Collins syndrome, neural crest cell migration failure
MICROTIA
Definition: “The abnormal development of the external ear that results in a malformed auricle” -Kelley & Scholes, 2007
Incidence: 0.83-17.4/10,000 live births
Strongly associated with hearing loss
80% have conductive hearing loss
20% have sensorineural hearing loss
Associated with psychological stigma and burden

MICROTIA: PRESENTATION
More common in males:
Male: Female ratio = 2.5:1
More common in Japanese, Hispanic, Native American
Prevalence increased at high altitudes
Multiparity
MICROTIA: PRESENTATION
Unilateral in 90% of cases
Bilateral in only 10% of cases
Right side > Left side (60% right)
Hearing loss normally in affected ear
can be bilateral or in the ear without microtia
MICROTIA: ASSOCIATED ANOMALIES
50% microtia cases associated with other anomalies
Common associated anomalies:
Congenital aural atresia (CAA)
• Present in almost all cases of severe microtia
• Cholesteatoma (Associated with CAA)
Hemifacial microsomia
Acrofacial Dysostosis
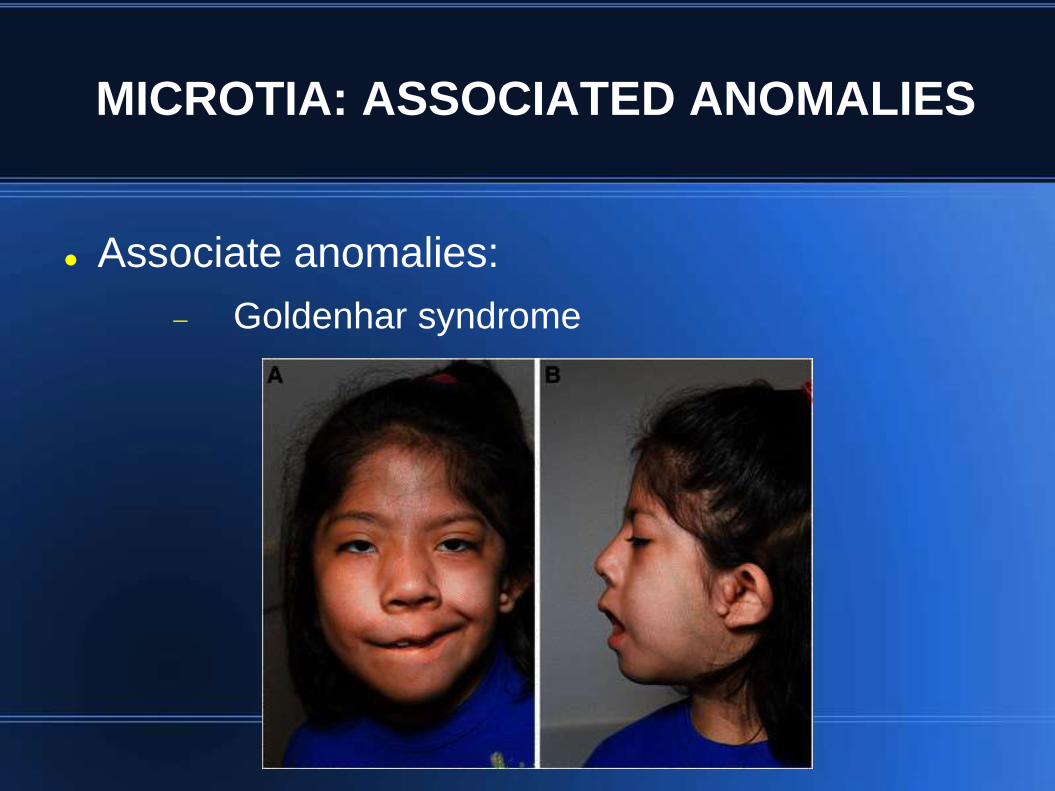
MICROTIA: ASSOCIATED ANOMALIES
Associate anomalies:
Goldenhar syndrome
MICROTIA: ASSOCIATED ANOMALIES
• Associated anomalies:
• Treacher Collins Syndrome

MICROTIA: CLASSIFICATION
Marx Classification
Type 1:
Mild deformity
All structural
components of
auricle present

MICROTIA: CLASSIFICATION
Type 2:
Atypical microtia
Some auricular structures
Helical changes
Auditory meatus patent
MICROTIA: CLASSIFICATION
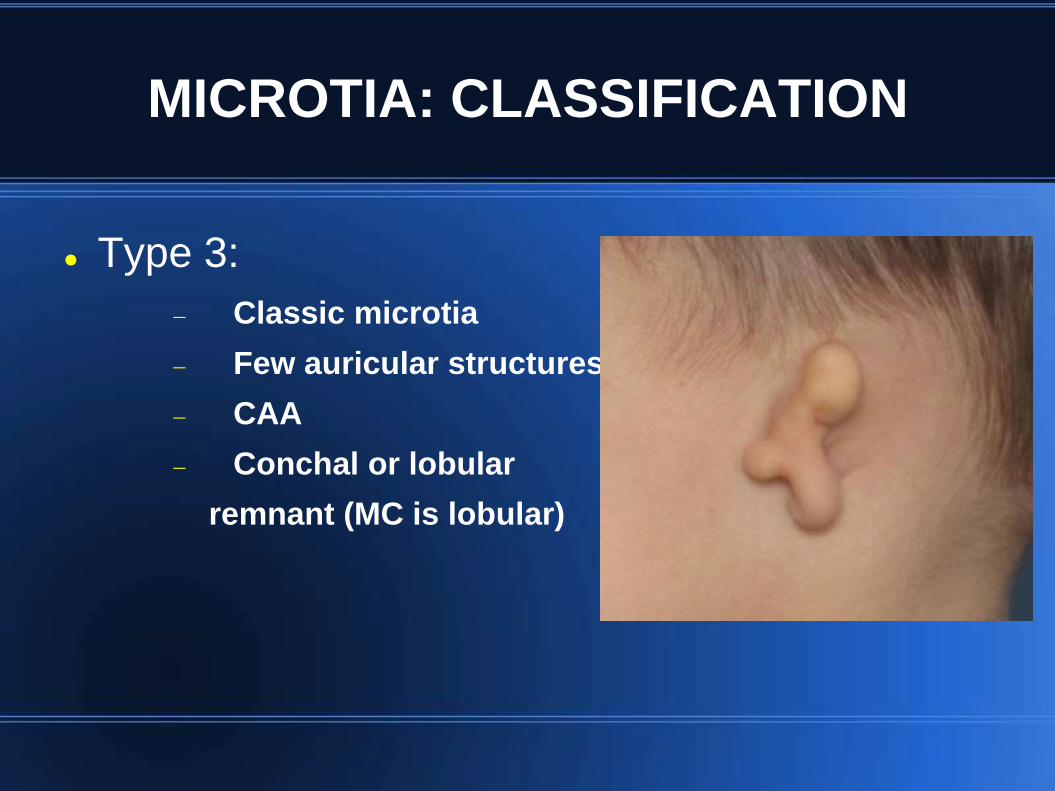
Type 3:
Classic microtia
Few auricular structures
CAA
Conchal or lobular
remnant (MC is lobular)
MICROTIA: CLASSIFICATION
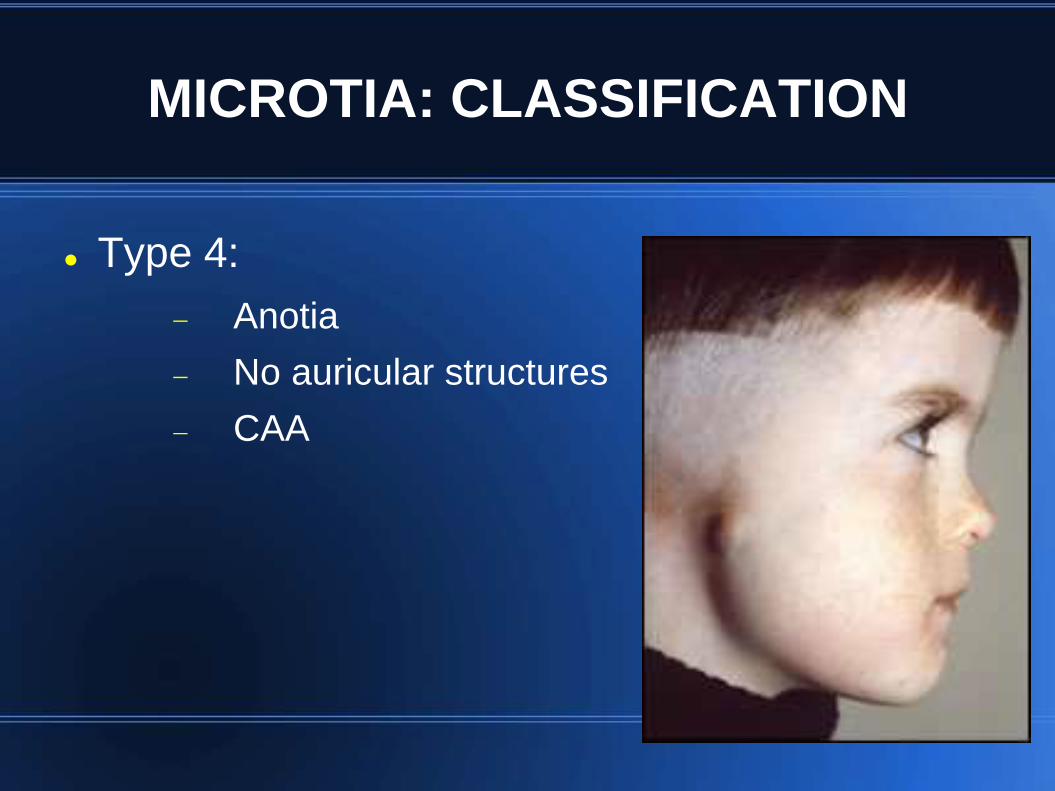
Type 4:
Anotia
No auricular structures
CAA
MICROTIA: AUDIOLOGY
Hearing status
Degree of microtia associated with degree of middle ear deformity
CHL common in microtic ear
Non microtic ear can have hearing loss
Protect normal hearing ear
Lower threshold for ventilation tubes
Bilateral hearing loss
Indication for bone anchored hearing aids

MICROTIA: MANAGEMENT
Observation
Type 1 microtia
Prior to surgery: 5-8 years
Advantages: no risk, possibility for future reconstruction
Disadvantages: cosmesis, psychosocial issues
Main focus: hearing and speech
MICROTIA: MANAGEMENT
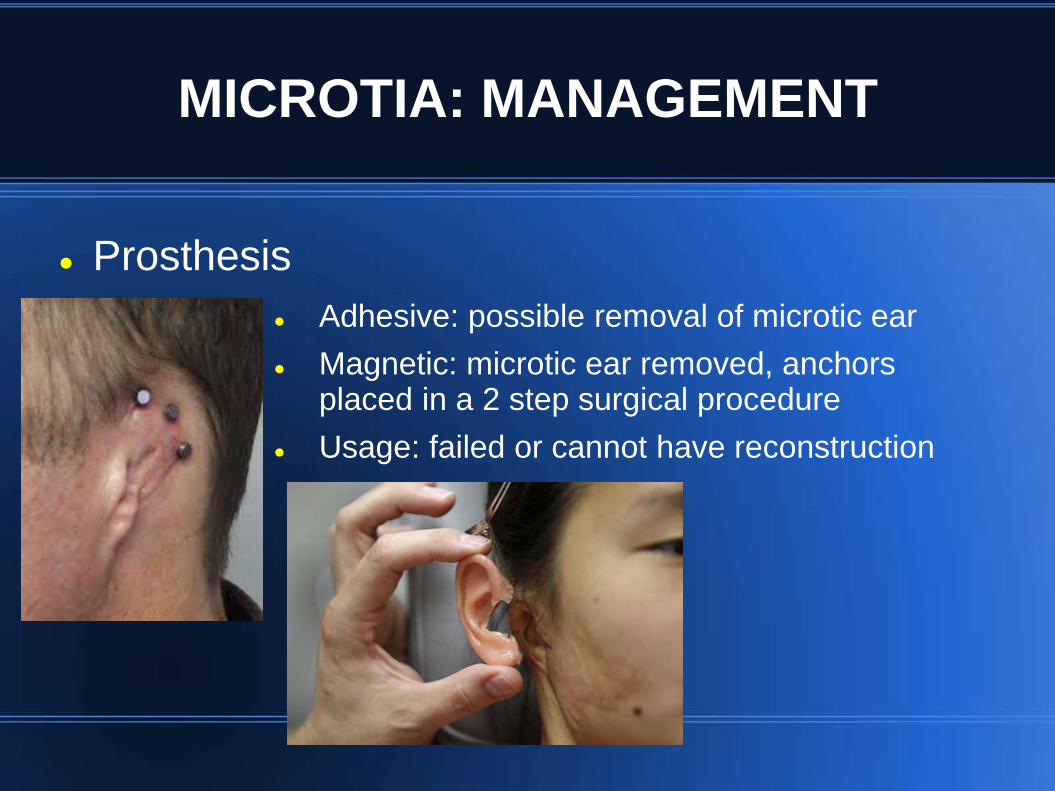
Prosthesis
Adhesive: possible removal of microtic ear
Magnetic: microtic ear removed, anchors placed in a 2 step surgical procedure
Usage: failed or cannot have reconstruction

MICROTIA: MANAGEMENT
Prosthesis
Advantages: cosmesis
Disadvantages:
Adhesive:
future reconstruction difficult
dislodgment
remove at night
cost
Magnetic:
no future reconstruction
remove at night/daily maintenance
cost
surgery
MICROTIA: MANAGEMENT
Reconstruction
Types:
Autogenous rib: four step procedure
Medpor: porous polyethylene, more difficult procedure
Advantages: cosmesis, low maintenance
Autogenous rib: lower risk for extrusion/infection
Medpor: no donor site morbidity
Disadvantages: surgery, flap failure, scar
Autogenous rib: donor site morbidity, pneumothorax
Medpor: higher risk for extrusion/infection
MICROTIA: MANAGEMENT
Reconstruction
Autogenous rib reconstruction stages
1: Cartilage implantation
2: Lobule transfer
3: Creation of post auricular sulcus
4: Tragus reconstruction
Complications:
Hematoma
Pneumothorax
MICROTIA: MANAGEMENT
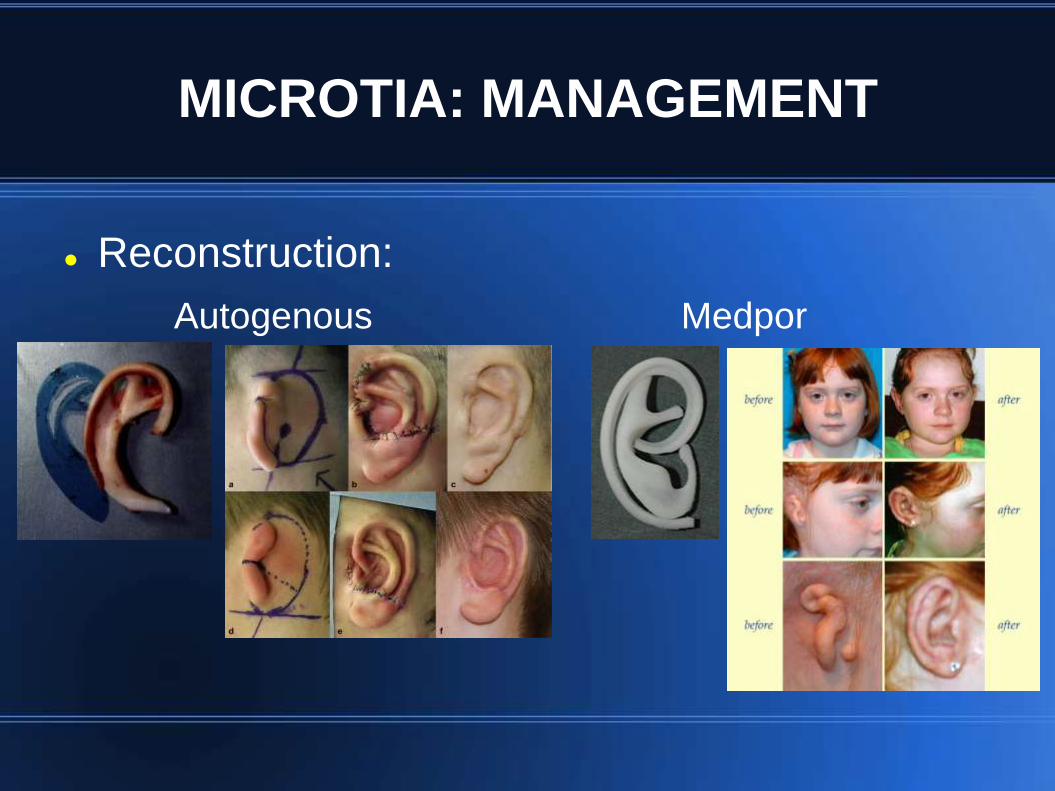
Reconstruction:
Autogenous Medpor

SUMMARY
Microtia is auricular failure to develop
Embryology: branchial arches 1-2
Etiology: mainly sporadic, possible genetic causes
Associated anomalies: 50% of cases
commonly associated with CAA
SUMMARY
Type 1: minimal deformity
Type 2: helix deformity
Type 3: no recognizable auricular structures
Type 4: no auricle
Management: observation, prosthesis, reconstruction
Monitor hearing and speech
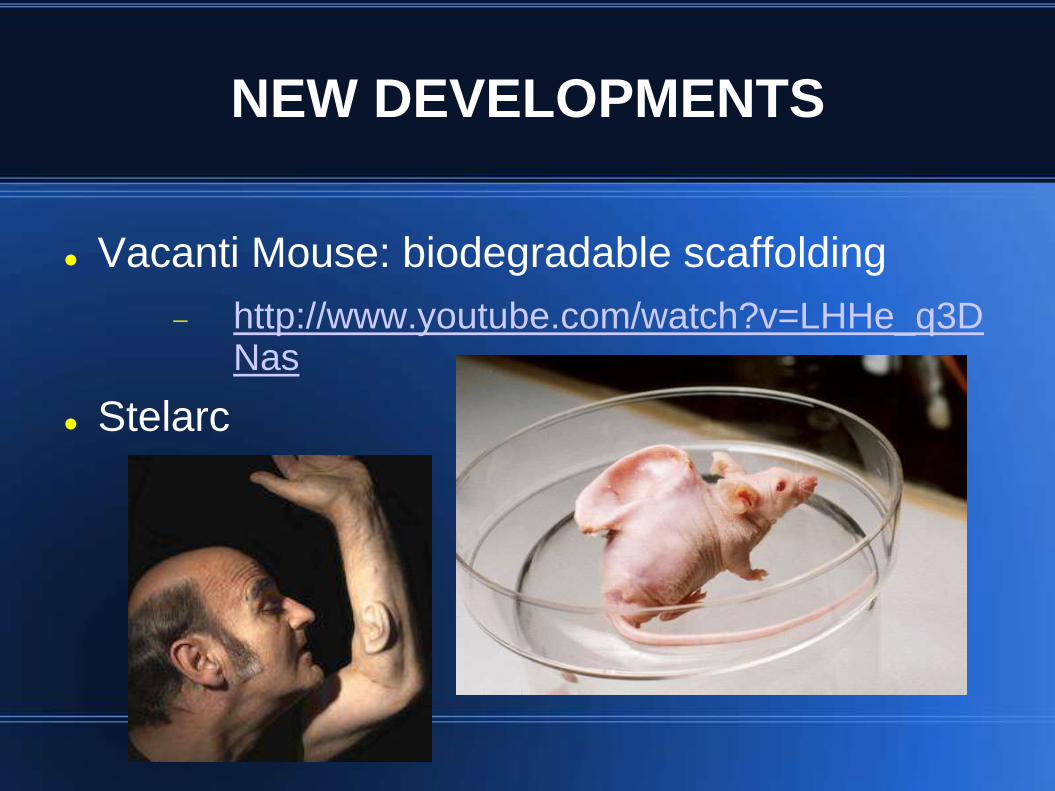
NEW DEVELOPMENTS
Vacanti Mouse: biodegradable scaffolding
http://www.youtube.com/watch?v=LHHe_q3DNas
Stelarc
RESOURCES
Genc, S., Kahraman, E., Ozel, H., Arslan, I., Demir, A., & Selcuk, A. (2012). Microtia and congenital aural atresia. Journal of Craniofacial Surgery, 23 (6): 1733-1735.
Hitchinson, J., Caldarelli, D., & Gould, H. (1981). Classification and multidisciplinary management of microtia. Otolaryngology Clinics of North America, 14(4): 885-893.
Kelley, P., & Scholes, M. (2007). Microtia and congenital aural atresia. Otolaryngology Clinics of North America, 40: 61-80.
Luquetti, D., Heike, C., & Cox, T. (2012). Microtia: epidemiology and genetics. American Journal of Medical Genetics, 158(1): 124-139.
Murakami, C., Quatela, V., Sie, K., & Shvidler, J. (2010). Chapter 192: Microtia reconstruction. Cummings Otolaryngology 5th Edition: 2741-2751
Parisier, S., Fayad, J., Kimmelman, C., Sclafani, A., & Alexiades, G. (2008). Chapter 62: Pediatric otorhinolaryngology: microtia, canal atresia, and middle ear anomalies. Ballenger's Otolaryngology: 759-767.
Wieczorek, D. (2013). Human facial dysostoses. Clinical Genetics 83(6): 499-510.
Saim, A., Cao, Y., Weng. Y., Chang, C., Vacanti, M., & Eavey, R. (2000). Engineering autogenous cartilage in the shape of a helix using an injectable hydrogel scaffold. Laryngoscope, 110(10pt1): 1694-1697.
Giardini-Rosa, R., Joazeiro, P., Thomas, K., Collavino, K, Weber, J. & Waldman, S. (2013). Development of scaffold-free elastic cartilaginous constructs with structural similarities to auricular cartilage. Tissue Engineering, In process of publishing.