
Microtia Recon Slides 0410
31
Microtia Microtia Reconstruction Reconstruction Jing Shen, M.D. Jing Shen, M.D. Francis B. Quinn, M.D. Francis B. Quinn, M.D. UTMB – Dept of Otolaryngology UTMB – Dept of Otolaryngology October 2004 October 2004
-
Upload
josue-salinas-santos -
Category
Documents
-
view
65 -
download
5
Transcript of Microtia Recon Slides 0410

Microtia ReconstructionMicrotia Reconstruction
Jing Shen, M.D.Jing Shen, M.D.Francis B. Quinn, M.D.Francis B. Quinn, M.D.
UTMB – Dept of OtolaryngologyUTMB – Dept of OtolaryngologyOctober 2004October 2004

EpidemiologyEpidemiology
Occurs 1 in 7,000 to 8,000 infantsOccurs 1 in 7,000 to 8,000 infants Occurs more often in right earsOccurs more often in right ears Occurs more often in malesOccurs more often in males Higher incidence in Hispanics and Asians Higher incidence in Hispanics and Asians
than in blacks and whitesthan in blacks and whites Fewer than 15% with positive family Fewer than 15% with positive family
historyhistory Associated with other congenital Associated with other congenital
malformationsmalformations

Embryology of AuricleEmbryology of Auricle
From From The Ear comprehensive otology: The Ear comprehensive otology:
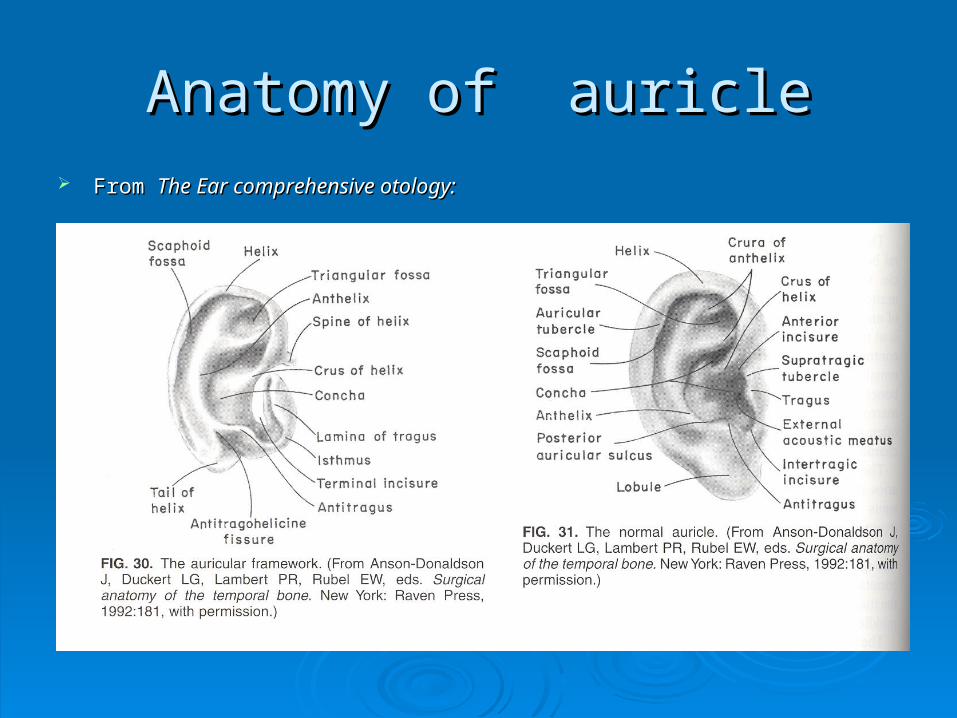
Anatomy of auricleAnatomy of auricle From From The Ear comprehensive otology:The Ear comprehensive otology:
External ear anatomyExternal ear anatomy
Muscles: 3 extrinsic and 6 intrinsic Muscles: 3 extrinsic and 6 intrinsic Sensory: Sensory:
Posterior portion: greater auricular nerve and lesser Posterior portion: greater auricular nerve and lesser occipital nerveoccipital nerve
Anterior portion: auriculotemporal nerve, anterior Anterior portion: auriculotemporal nerve, anterior branch of greater auricular nerve and Arnold’s branch branch of greater auricular nerve and Arnold’s branch of vagus nerveof vagus nerve
Vascular:Vascular: Posterior auricular arteryPosterior auricular artery Superficial temporal arterySuperficial temporal artery

Anatomical RelationAnatomical Relation

Classification of MicrotiaClassification of Microtia
Many classification systemsMany classification systems Grade I, II, III: Grade I, II, III:
Grade I: all anatomic subunits present but Grade I: all anatomic subunits present but misshapenmisshapen
Grade II: anatomic subunits either deficient or Grade II: anatomic subunits either deficient or absentabsent
Grade III: classic “peanut ear” and anotiaGrade III: classic “peanut ear” and anotia


History of microtia reconstructionHistory of microtia reconstruction
Dr. Tanzer 1959: 1Dr. Tanzer 1959: 1stst article on auricular article on auricular reconstruction with autogenous rib reconstruction with autogenous rib cartilage, 6 stages procedurecartilage, 6 stages procedure
Dr. Brent 1974: 4 stages procedure, Dr. Brent 1974: 4 stages procedure, foremost authority on auricular foremost authority on auricular reconstructionreconstruction
Dr. Nagata 1985: 2 stages procedureDr. Nagata 1985: 2 stages procedure

Surgical planningSurgical planning
Timing:Timing: 47.2% operated at age 6-7, 21.1% operated 47.2% operated at age 6-7, 21.1% operated
at age 8-10 per Dr. Brentat age 8-10 per Dr. Brent Nagata operated at age 10 and chest Nagata operated at age 10 and chest
circumference at least 60 cm (confirmed with circumference at least 60 cm (confirmed with x-ray)x-ray)
Otologic surgery is in general planned Otologic surgery is in general planned after the auricular reconstruction surgeryafter the auricular reconstruction surgery Increased interest in atresia correctionIncreased interest in atresia correction

Brent techniqueBrent technique
Four stages:Four stages: Stage I: fabrication of the auricular framework Stage I: fabrication of the auricular framework
with contralateral costal cartilagewith contralateral costal cartilage Stage II: lobule transpositionStage II: lobule transposition Stage III: framework elevationStage III: framework elevation Stage IV: tragus reconstructionStage IV: tragus reconstruction

Brent techniqueBrent technique

Brent technique: stage IBrent technique: stage I

Stage IIStage II

Stage IIIStage III

Stage IVStage IV

Alternative methods for tragus Alternative methods for tragus reconstructionreconstruction

Long term result from Brent Long term result from Brent techniquetechnique

CriticismCriticism
Number of stages requiredNumber of stages required Lack of definition of the conchal bowl, the Lack of definition of the conchal bowl, the
intertragic notch, and the contour of the intertragic notch, and the contour of the antitragusantitragus
Effacement of the postauricular sulcus due Effacement of the postauricular sulcus due to contraction of the skin graftsto contraction of the skin grafts

Nagata techniqueNagata technique
2 stages:2 stages: Stage I: fabrication of auricular framework Stage I: fabrication of auricular framework
from ipsilateral costal cartilage, tragus from ipsilateral costal cartilage, tragus reconstruction, and lobule transpositionreconstruction, and lobule transposition
Stage II: framework elevationStage II: framework elevation

Nagata technique: stage INagata technique: stage I

Stage I: frameworkStage I: framework

Stage I: implantation and lobule Stage I: implantation and lobule transpositiontransposition

Stage II: elevation of frameworkStage II: elevation of framework

CriticismCriticism
High rate of flap necrosis (14%)High rate of flap necrosis (14%) Significant anterior chest wall deformitySignificant anterior chest wall deformity Unnaturally thick earUnnaturally thick ear High extrusion rate may be due to use of High extrusion rate may be due to use of
wire sutures (8%)wire sutures (8%) Universally used temporoparietal fascia Universally used temporoparietal fascia
flapflap

ComplicationsComplications
Ear reconstruction site:Ear reconstruction site: Exposure of the frameworkExposure of the framework Resorption of the frameworkResorption of the framework
Cartilage donor site:Cartilage donor site: Immediate problem: pneumothorax, Immediate problem: pneumothorax,
atelectasisatelectasis Delayed problem: anterior chest wall Delayed problem: anterior chest wall
deformity, scarringdeformity, scarring
Alloplastic reconstructionAlloplastic reconstruction
Silicone:Silicone: Good initial resultGood initial result Poor long term result secondary to implant Poor long term result secondary to implant
exposureexposure Minor trauma can cause implant failureMinor trauma can cause implant failure
Medpor: Medpor: Good short term (2 years) result in Good short term (2 years) result in
combination of temporoparietal fascia flapcombination of temporoparietal fascia flap
Prosthetic reconstructionProsthetic reconstruction Osseo-integrated anchoring device: approved Osseo-integrated anchoring device: approved
extraoral use by FDA in 1995extraoral use by FDA in 1995 Indication:Indication:
Failed autogenous reconstructionFailed autogenous reconstruction Sever soft- tissue/skeletal hypoplasiaSever soft- tissue/skeletal hypoplasia Low or unfavorable hairlineLow or unfavorable hairline Acquired total or subtotal auricular defect, usually in Acquired total or subtotal auricular defect, usually in
adultsadults Prosthesis changes every 2 to 5 yearsProsthesis changes every 2 to 5 years Meticulous hygiene at skin/implant interfaceMeticulous hygiene at skin/implant interface Preclude future autogenous reconstructionPreclude future autogenous reconstruction

Tissue engineeringTissue engineering
Cao Cao et al.et al. transplanted bovine transplanted bovine chondrocytes onto a scaffold and chondrocytes onto a scaffold and implanted in miceimplanted in mice
Need a scaffolding strong enough to Need a scaffolding strong enough to maintain its shape and not causing maintain its shape and not causing extrusionextrusion
Human auricular chondrocytes multiply Human auricular chondrocytes multiply well well in vitro in vitro and have the ability to form and have the ability to form new cartilagenew cartilage

Tissue engineeringTissue engineering

ResourceResource
More long term result photos are available More long term result photos are available at:at: www.earsurgery.com (Dr. Brent home page) (Dr. Brent home page) www.microtia.jp (Dr. Nagata home page) (Dr. Nagata home page)

















![HEAR MAPS a New Classification for Congenital Microtia ... · (Hearing, Ear [microtia], Atresia grade, Remnant earlobe, Mandible development, Asymmetry of soft tissue, Paralysis](https://static.fdocuments.us/doc/165x107/60e4c2c1d26f8d5c325501dd/hear-maps-a-new-classiication-for-congenital-microtia-hearing-ear-microtia.jpg)
