Microconsult iteration1 findings
17
Project Mars | Outpatient Practice Redesign MICRO-CONSULTS Iteration 1: Proof of Concept Experimental Findings & Next Steps
-
Upload
mayo-clinic-center-for-innovation -
Category
Documents
-
view
214 -
download
0
description
Â
Transcript of Microconsult iteration1 findings
Project Mars | Outpatient Practice Redesign
MICRO-CONSULTS
Iteration 1: Proof of Concept
Experimental Findings & Next Steps
© 2013 MFMER
Iteration 1: Experiment Findings | Overview
WHAT: An integrated care model where multiple providers meet with a patient simultaneously
in a clinical space using technology that allows them to virtually connect and collaborate.
Typically effective for a focused question that leads to diagnosis and adjustment to treatment.
Can be scheduled or unscheduled.
WHY: Not all patients need or have immediate
access for a traditional appointment. Micro-consults
become a more formalized “curbside”. They will
provide:
Increased access
Decreased itinerary length
Improved diagnosis and treatment options
Less duplicity of resources – people and space
Aligns with near-future reimbursement models

© 2013 MFMER
Four separate experiments were completed for Iteration 1 findings
Experiment 1: Scalability Study – Met with providers to review their days’ appointments to identify
which consults could have been a micro-consult
Goal was to understand where micro-consults would have the greatest impact in the practice
5 providers chosen to represent different types of providers; Dr. Feyereisn, Dr. Wermers, Dr. Ommen,
Dr. Lightner, Dr. Huddleston
Experiment 2: GIM – Attempt to predict micro-consults based on pre-visit information. GIM was
identified from the scalability study as a key partner
Goal was to understand the needs for complex, non-acute patients
3 initiating providers; Dr. Feyereisn, Dr. Lundstrom, Dr. Mikhail
Experiment 3: Dialysis – Identify dialysis patients who need micro-consults with a specialist
Goal was to understand the needs for complex, acute patients to intervene to avoid potential ED visits
2 initiating providers; Dr. Williams and Christy Gossett, RN, CNP
36 receiving providers recruited to be “on-call” for potential micro-consults*
*A full list of providers who agreed to participate as receiving specialist can be found in Appendix 1.
Iteration 1: Experiment Findings | Experiment and Partners
© 2013 MFMER
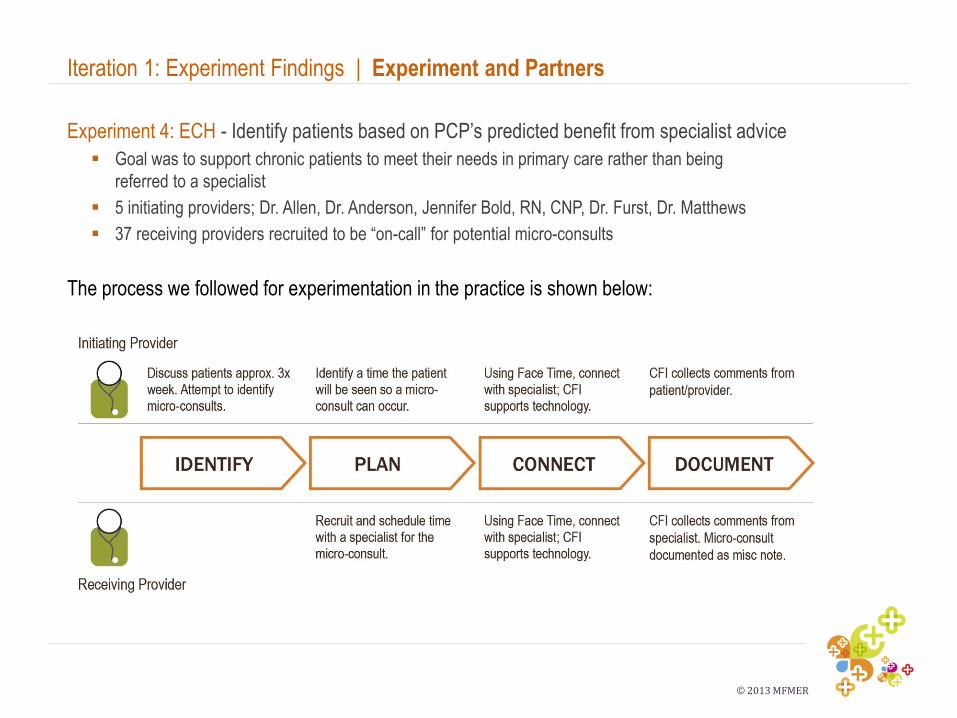
Experiment 4: ECH - Identify patients based on PCP’s predicted benefit from specialist advice
Goal was to support chronic patients to meet their needs in primary care rather than being
referred to a specialist
5 initiating providers; Dr. Allen, Dr. Anderson, Jennifer Bold, RN, CNP, Dr. Furst, Dr. Matthews
37 receiving providers recruited to be “on-call” for potential micro-consults
The process we followed for experimentation in the practice is shown below:
Iteration 1: Experiment Findings | Experiment and Partners
© 2013 MFMER
Experimentation in the practice, all had the following qualitative and quantitative metrics:
Appointment Length: The length of the micro-consult or coordinated care appointment.
Captured through the technology.
Impact and Acceptance of the Technology: Captured qualitatively through debrief interviews
with both providers and the patient regarding their impressions of the technology from a
performance and overall acceptance perspective.
Value: Captured qualitatively through debrief interviews with both providers and the patient
regarding the value of the interaction.
Patient and Provider Satisfaction: Captured qualitatively, and in most instances through
numerical rating, with both providers and the patient, regarding the satisfaction and overall
thoughts about the interaction.
Additional metrics that were experiment specific included:
Frequency of micro-appointment: For the scalability study, the percentage of micro-consults
relative to number of overall appointments.
Referral Status: For the ECH study, if the patient is referred to the outpatient practice
immediately following the micro-consult.
Iteration 1: Experiment Findings | Metrics
© 2013 MFMER
Chart review to identify potential micro-consults. In total we evaluated 154 appointments
comprised of new and established patients. 48 micro-consults were identified* across departments
comprising 31% of overall appointments.
Dr. Ommen: 25 appointments; 6 (23%) could have been micro-consults
Dr. Wermers: 19 appointments; 6 (35%) could have been micro-consults
Dr. Feyereisn: 22 appointments; 11 (50%) could have been micro-consults
Dr. Lightner: 62 appointments; 14 (23%) could have been micro-consults
Dr. Huddleston: 26 appointments; 6 (23%) could have been micro-consults
Implications: There is a significant opportunity for a micro-consult care interaction across Mayo
Clinic, specifically the opportunity to initiate micro-consults in GIM as well as specialties. In
surgical practices the potential is in receiving micro-consults but should be balanced with other
interactions such as eConsults and Remote Recheck.
This study allowed us to focus on GIM as one of our key partners.
*A full list of specialties that would have been on the initiating or receiving end of potential micro-consults is included in Appendix 2.
Iteration 1: Experiment Findings | Results of Scalability Study
© 2013 MFMER
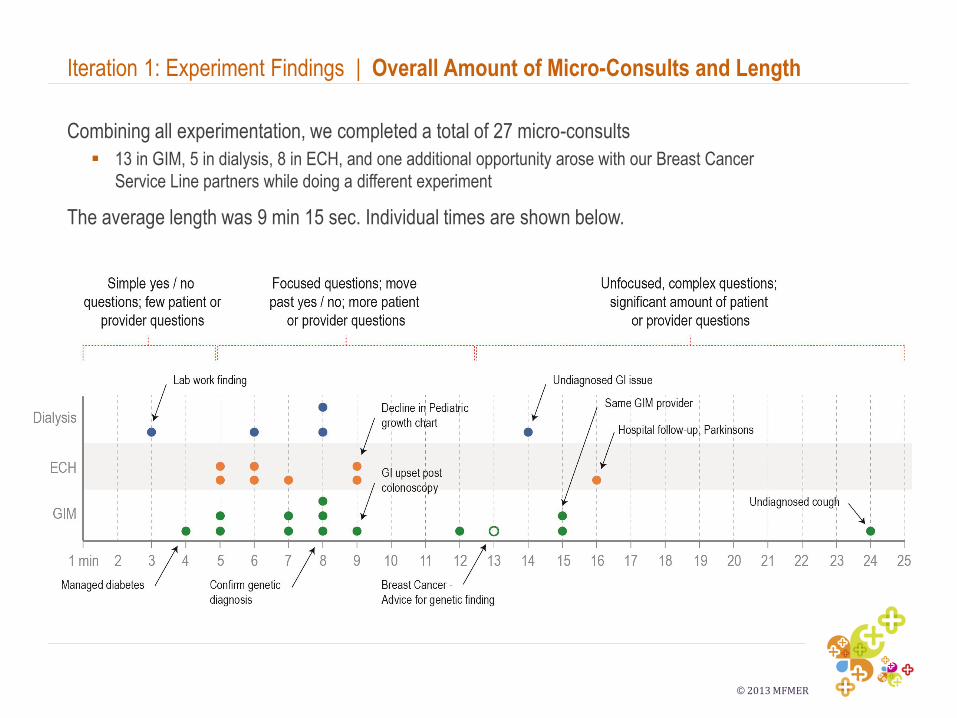
Combining all experimentation, we completed a total of 27 micro-consults
13 in GIM, 5 in dialysis, 8 in ECH, and one additional opportunity arose with our Breast Cancer
Service Line partners while doing a different experiment
The average length was 9 min 15 sec. Individual times are shown below.
Iteration 1: Experiment Findings | Overall Amount of Micro-Consults and Length
© 2013 MFMER
Each micro-consult was evaluated to understand what slot type it would have filled if it had
been a referred consult (e.g. new, established, return)
Matching the appointment time to the slot times in each department and subtracting the
lengths of the micro-consults, we saved a total of 1035 appointment minutes or 17.25 total
appointment hours for 27 micro-consults. Specifically:
146 minutes for 3 Cardiovascular micro-consults; 193 minutes for 6 Endocrinology micro-consults;
136 minutes for 4 Gastrointestinal micro-consults
For each micro-consult we also looked at the approximate availability of the referred to
department or specialty. Overall we saved patients a total of 118 days on their itinerary we
an average of 4 days across all patients. Specifically:
• Longest next available appointment were in the following departments / specialties: Pulmonology,
Cardiology, Endocrinology, and Nephrology
Iteration 1: Experiment Findings | Time Savings
© 2013 MFMER
Value: All of the micro-consults were considered a success (to some degree) except one
which involved an undiagnosed cough. Some of the longer, more unfocused questions, while
not optimal to the receiving provider, did provide initiating providers information they did not
know and helped them move forward with treatment of their patients.
Impact: All but two eliminated the need for an additional referral
Iteration 1: Experiment Findings | Impact and Value
Initiating Provider’s Comments
Dialysis: We were able to schedule an EGD for the
patient, something I could not order without a GI
consult. This allowed patient care to move forward
quickly and satisfy the patient who was significantly
impacted by the condition. – Christy Gossett R.N.,
C.N.P
ECH: The micro-consult saved a full consult to
Endocrinology, avoided unnecessary testing, and
reassured me that my evaluation so-far was
complete. – Jennifer Bold R.N., C.N.P
ECH: The micro-consult helped anxious parents
looking for answers. The specialist re-enforced my
advice and treatment plan. – Dr. Allen
GIM: The micro-consult summed up a two-week
investigation into the patients condition, which was a
rare genetic mutation, that provided her the answers
she needed before returning home to Mississippi.
Speaking with the Geneticist also provided the parent
insights that her brother could also have the same
genetic mutation. – Dr. Feyereisn
GIM - The micro-consult expedited the process a
great deal and after confirming the diagnosis with
Endocrinology the patient changed his travel plans
and opted for surgery the next day at Mayo Clinic.
– Dr. Mikhail
© 2013 MFMER
Iteration 1: Experiment Findings | Impact and Value
Receiving Provider’s Comments
GI: This is excellent. Far superior to a face-to-face
with the patient, because the Dialysis NP was present
and she could help interpret relevant medical
information. There is great potential for this process.
We could potentially do 6 of these in an hour, saving
everyone time and money. - Dr. Loftus
Pediatric Endocrinology: This micro-consult added
value for the PCP and because we did this “face-to-
face” where I was able to see the child, and ask
questions to the mother, I changed my opinion that
immediate bone tests were necessary. Due to this
type of interaction I felt comfortable supporting a wait-
and-see approach. – Dr. Ltief
CV: The micro-consult is what we do everyday, just
with technology. It is essentially how we practice now.
– Dr. Brozovich
Patient Comments
ECH: The most positive thing is that we are all
immediately on the same page. Dr. Allen knows
what the specialist said and can ask questions I
wouldn't have thought of. I don't have to try to
remember for my next appointment, everyone
already knows the story. – Patient
GIM: I liked the practicality of it - I didn't have to
wait a few days to get this appointment. – Patient
GIM: I liked being able to speak with the specialist
sooner and with Dr. Lundstrom in the room, he
knew what to ask and could mediate. - Patient
Dialysis: This was very helpful, we knew Randy
needed to be seen by a specialist and didn't know
when that could happen, the sooner the better. It's
good to use the time that he is in dialysis, he is a
captive patient and driving here on Tuesday or
Thursday would be hard because it is a long drive
and on dialysis days he is so wiped out
afterwards. –Patients wife
© 2013 MFMER
For the most part, initiating providers, receiving providers, and patients all reported high levels of
satisfaction with the experience. We asked the following question*:
On a scale of 1 to 7 with 1 being the lowest and 7 being the highest, please rank your level of satisfaction.
Overall only two people gave the interaction a ranking lower than 5. One was a specialist who was asked to
answer an unfocused question and the second was a dermatologist who participated on a micro-consult that
had technology issues. She also mentioned she would like to see the patient’s rash in better detail.
– The average ranking for initiating providers was 6.1
– The average ranking for receiving providers was 5.7
– The average ranking for patients was 6.2
Specific feedback from receiving providers, essentially those who do not gain any immediate value from
this interaction, was:
Many provides mentioned that if this interaction would become part of their practice they would need to have
time protected to do these and / or get credit for them. Several mentioned that there have been many add-on’s
to the typical day including eConsults and appointment triage which have been maxing out physician time.
While many took the time to review the patients clinical note prior to the micro-consult, a few mentioned feeling
unprepared; however, this concern did not negatively influence any of the interactions. One provider specifically
did not prepare as he wanted to try it as “real-time” as possible.
*Survey questions were developed after experimentation began. 18 of the 26 micro-consults had survey questions captured by all participants.
Iteration 1: Experiment Findings | Overall Satisfaction
© 2013 MFMER
Two challenges emerged related to if, and how, these interactions can occur.
Real-time availability versus scheduled: In experimentation we attempted to identify micro-consults to allow us
time to “schedule” them with the receiving specialists. With all, we reviewed next day appointments and with
GIM also used pre-visit information.
– While we were able to predict some, we often heard from our providers their need arose real-time during
an appointment based on new information or situation.
– With dialysis patients there was more scheduling flexibility as dialysis is multiple times a week and typically
have a 2-4 hour window for the micro-consult as they are receiving dialysis; however, while some could be
scheduled, others needed same day attention.
Timing: Arranging a time for a specialist to connect with a scheduled appointment in GIM and ECH proved
challenging due to real-time variables, such as earlier appointments running late. This impacted when the
connection between two providers and the patient occurred.
– Delays in GIM were approximately 10-15 minutes while in ECH they were much greater. Some micro-
consults in ECH occurred 45 minutes to an hour later than originally scheduled.
Implications: The next round of prototyping should support real-time scheduling and rely on technology
or other solutions that indicate availability of specialists. Additionally, we should better connect pre-visit
information to experimental areas to understand benefits outside of GIM of pre-visit.
Iteration 1: Experiment Findings | Scheduling Challenges
© 2013 MFMER
We had significantly more micro-consult requests than we could schedule, even with 26
providers available to cover the experiment. Specifically we had 26 requests we could
not full in ECH and 5 requests we could not fill in GIM.
Scheduling: Our current scheduling system does not support this type of interaction.
Providers are not given time to do these and, as they are hard to accurately schedule, it is
hard to fit them in between patients.
– Knowing this challenge, we contacted multiple providers in departments with the highest
referrals and focused on recruiting providers who were staffing clinics and / or had
flexibility with administrative time. Even with this planning it wasn’t enough, as providers
get add-on patients and take vacation.
Implications: We need to think creatively and solve this problem for the next round of
experimentation, especially in light of the fact we could not fill 72% of ECH requests and
38% of GIM requests. Ideas include:
Provide protected time for specific providers to participate in the experiment
Scale the next experiment to whole departments and include situational awareness of who
has availability so there is greater possibility of success
Iteration 1: Experiment Findings | Provider Availability
© 2013 MFMER
For Iteration 1 we chose to use Face Time on an iPad and support each micro-consult by bringing
both providers iPads that we knew connected. Even with these precautions, we had the following
technology challenges:
Wi-Fi Connection: In many instances the broadband connection was slow and the video skipped. In two
instances the first calls dropped before connecting and in two instances we could not connect between
locations, specifically locations outside of Gonda / Mayo.
Sound Quality: While most micro-consult participants thought the sound quality was adequate, one provider
hooked his iPad to speakers for better sound. We also observed the dialysis environment made the audio
hard to hear, though participants did not comment on this as being negative, rather it was expected.
Picture Quality: In the cases of our Dermatology consults, it was recommended we take a 'dermascopic'
photo for better visibility. We also heard from Orthopedics that being able to connect to a larger monitor may
help in instances where they may want to see the patients walk.
Limitations of Technology: Using technology as an alternative to face-to-face appointments limits the ability
to execute a physical exam. While none of the providers specifically minded this, understanding this was a
micro-consult instead of a full consult, several did comment that this means they need to trust the other
provider to do a proper exam that may have nuances for each specialty.
Implications: The next iteration prototype should be attempt to be as user friendly as possible and the
technology should be seamless. Many commented if the connection did not work in real-time they
would not try and troubleshoot.
Iteration 1: Experiment Findings | Technology
© 2013 MFMER
Iteration 2: For the next iteration we want to create a lo-fi prototype that will allow micro-
consults to happen between two providers without our involvement in scheduling and
technology support. The specific goals of Iteration 2 include understanding:
Workflow implications: Understanding how providers, on their own, can identify, initiate and
execute a micro-consult.
Scheduling implications: Working to identify and plan micro-consults as well as allow micro-
consults to happen real-time.
Technology implications: Understanding how the prototype changes micro-consult
interactions and learnings for how the micro-consult functionality can best connect to Smart
Space in the next iteration.
Iteration 1: Experiment Findings | Next Steps

© 2013 MFMER
Initiating Providers
GIM Providers
Dr. Feyereisn
Dr. Lundstrom
Dr. Mikhail
ECH Providers
Dr. Anderson
Dr. Furst
Dr. Matthews
Dr. Puffer
Dr. Summer
Jennifer Bold, R.N., C.N.P.
Heather Carrico, R.N., C.N.P.
Dialysis Providers
Dr. Williams
Christy Gossett, R.N., C.N.P.
Iteration 1: Experiment Findings | Appendix 1
Receiving Specialist Providers (Recruited and Participated)
Dr. Maddox, Allergy
Dr. Ghosh, Breast Clinic
Dr. Brozovich, Cardiology
Dr. Ommen, Cardiology
Dr. Wright, Cardiology
Dr. Brewer, Dermatology
Dr. D. Davis, Dermatology
Dr. M. Davis, Dermatology
Dr. McEvoy, Dermatology
Dr. Castro, Endocrinology
Dr. Kennel, Endocrinology
Dr. Lteif, Pediatric Endocrinology
Dr. Montori, Endocrinology
Dr. Wermers, Endocrinology
Dr. Kimori, Genetics
Dr. Loftus, GI
Dr. Schaffner, GI
Dr. Tung, Pediatric GI
Dr. Langstraat, Gynecologic Surgery
Dr. Hansel, GI and Hematology
Dr. Lacy, Hematology
Dr. Dillon, Nephrology
Dr. Williams, Nephrology
Dr. Bartleson, Neurology
Dr. Cutrer, Neurology
Dr. Kantarci, Neurology
Dr. Swanson, Neurology
Nancy Honeychuck., R.N., C.N.P.;
Neurology
Dr. Huddleston, Orthopedic Surgery
Dr. Turner, Orthopedic Surgery
Roger Thomas P.A.-C, Orthopedics
Dr. Moore, Otorhinolaryngology,
Dr. Shelerud, PM&R
Dr. Edell, Pulmonology
Dr. Lim, Pulmonology
Dr. Viggiano, Pulmonology
© 2013 MFMER
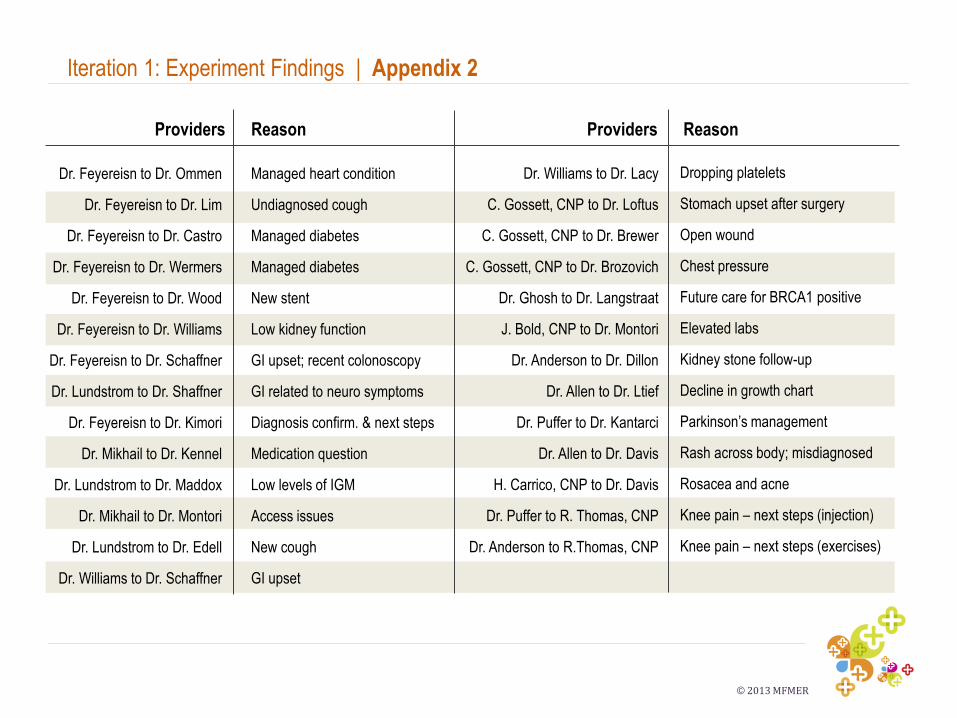
Iteration 1: Experiment Findings | Appendix 2
Dr. Feyereisn to Dr. Ommen
Dr. Feyereisn to Dr. Lim
Dr. Feyereisn to Dr. Castro
Dr. Feyereisn to Dr. Wermers
Dr. Feyereisn to Dr. Wood
Dr. Feyereisn to Dr. Williams
Dr. Feyereisn to Dr. Schaffner
Dr. Lundstrom to Dr. Shaffner
Dr. Feyereisn to Dr. Kimori
Dr. Mikhail to Dr. Kennel
Dr. Lundstrom to Dr. Maddox
Dr. Mikhail to Dr. Montori
Dr. Lundstrom to Dr. Edell
Dr. Williams to Dr. Schaffner
Dr. Williams to Dr. Lacy
C. Gossett, CNP to Dr. Loftus
C. Gossett, CNP to Dr. Brewer
C. Gossett, CNP to Dr. Brozovich
Dr. Ghosh to Dr. Langstraat
J. Bold, CNP to Dr. Montori
Dr. Anderson to Dr. Dillon
Dr. Allen to Dr. Ltief
Dr. Puffer to Dr. Kantarci
Dr. Allen to Dr. Davis
H. Carrico, CNP to Dr. Davis
Dr. Puffer to R. Thomas, CNP
Dr. Anderson to R.Thomas, CNP
Providers Reason Providers Reason
Managed heart condition
Undiagnosed cough
Managed diabetes
Managed diabetes
New stent
Low kidney function
GI upset; recent colonoscopy
GI related to neuro symptoms
Diagnosis confirm. & next steps
Medication question
Low levels of IGM
Access issues
New cough
GI upset
Dropping platelets
Stomach upset after surgery
Open wound
Chest pressure
Future care for BRCA1 positive
Elevated labs
Kidney stone follow-up
Decline in growth chart
Parkinson’s management
Rash across body; misdiagnosed
Rosacea and acne
Knee pain – next steps (injection)
Knee pain – next steps (exercises)