Microcephaly and congenital nephrotic …Garty,Eisenstein, Sandbank, Kaffe, Dagan, Gadoth I1 111 III...
5
J7 Med Genet 1994;31:121-125 Microcephaly and congenital nephrotic syndrome owing to diffuse mesangial sclerosis: an autosomal recessive syndrome Department of Paediatrics and the Kipper Institute of Paediatric Immunology, Beilinson Medical Centre, Petah Tiqva 49100, Israel B Z Garty Paediatric Nephrology Unit, Beilinson Medical Centre, Petah Tiqva, and Sackler Faculty of Medicine, Tel Aviv University, Israel B Eisenstein Pathology Department, Beilinson Medical Centre, Petah Tiqva, and Sackler Faculty of Medicine, Tel Aviv University, Israel J Sandbank The Genetics Clinic, Mount Sinai Medical Center, New York, NY, USA S Kaffe Department of Paediatrics, Soroka Medical Centre, Beer Sheva, Israel R Dagan Neurology Department, Beilinson Medical Centre, Petah Tiqva, and Sackler Faculty of Medicine, Tel Aviv University, Israel. N Gadoth Correspondence to Dr Garty. Received 9 February 1993 Revised version accepted for publication 24 August 1993 Ben Zion Garty, Bella Eisenstein, Judith Sandbank, Sara Kaffe, Ron Dagan, Nathan Gadoth Abstract Three sibs born to consanguineous par- ents had congenital nephrotic syndrome, microcephaly, and psychomotor retard- ation. Pathology of the kidneys showed diffuse mesangial sclerosis with deposits of IgG and C3 in the mesangium and glomerular basement membranes. All three children died before the age of 3 years. Of 19 published cases of children with the association of congenital neph- rotic syndrome and microcephaly, only four had histological evidence of diffuse mesangial sclerosis, and two of their sibs probably had the same disease. The asso- ciation of nephrotic syndrome owing to congenital diffuse mesangial sclerosis, microcephaly, and mental retardation appears to be a distinct syndrome with an autosomal recessive mode of inheritance. Nephrotic syndrome in the first year of life (congenital nephrotic syndrome) is rare. In- fantile microcystic disease, or the Finnish type nephrotic syndrome, is the best documented form of the syndrome.4 Other known causes of congenital nephrotic syndrome are intrauter- ine infection,56 renal vein thrombosis,7 and mercury intoxication.8 Minimal change neph- rotic syndrome, congenital focal glomerular sclerosis, membranous glomerulopathy, or dif- fuse mesangial sclerosis are uncommon causes of nephrotic syndrome in the first year of life."' The association of congenital nephrotic syn- drome, microcephaly, and mental retardation has been reported in 19 children,12-2' but only six of them had diffuse mesangial sclerosis (table).'121 We report a family with three mic- rocephalic children who had severe psychomo- tor retardation and congenital nephrotic syn- drome owing to diffuse mesangial sclerosis. (_J Med Genet 1994;31:121-125) Congenital microcephaly is associated with a variety of pathological conditions, including chromosomal aberrations, metabolic diseases, intrauterine infections, postradiation injury, and chronic hypoxaemia.' In its isolated form, it is usually inherited in an autosomal recessive mode2 and is accompanied by severe mental retardation. Occasionally it is inherited in an autosomal dominant mode, and in these patients the retardation is usually milder.`3 Case reports The family was of Jewish North African ori- gin. The pedigree is shown in fig 1. There were consanguineous marriages in generations III and IV-V. The father of the proband was the mother's uncle. Except for the proband and two of his sibs, there were no other family members with kidney disease or psychomotor retardation. The other five sibs, as well as the parents, were healthy and did not have micro- cephaly. The mother of the proband did not smoke and had not taken medication or alcohol Clinical and pathological findings in the patients with congenital nephrotic syndrome owing to diffuse mesangial sclerosis and microcephaly Case Sex Micro- Onset of Kidney Mental Neurological Dysmorphic Age at Notes Ref cephaly nephr syn histology retardation symptoms features death 1 F + 1 d Mesangial sclerosis + Seizures No 3 mth 16 2 M + 6 d Diffuse mesangial ? Decreased vision & Wide set eyes; sclerosis hearing small nose 2 mth 19 3 F + 6 d Mesangial sclerosis Hypertonic arms; Floppy ears; contractures 2 mth 20 seizures of hands & feet 4 M + 12 d - NM NM Floppy ears; I mth Sib of 20 hypertelorism case 3 5 M + 14 mth Mesangial sclerosis Severe Seizures; hypertonic limbs; Micrognathia; 18 mth 21 poor head control; no large ears visual fixation 6 F + 9 mth - Severe Hypertonic limbs; seizures; Large ears; 3 y Sib of 21 poor vision & hearing small midface case 5 7 M + 1 mth Diffuse messangial Severe Hypertonic limbs; poor Large, low set, floppy 2 y Consan- Present sclerosis. IgG and head control; strabismus; ears; sparse, thin hair; guinity report C3 deposit in the poor vision & hearing micrognathia; bilateral mesangium undescended testes 8 F + 1 mth Identical to case 7 Severe Identical Large, low set, floppy 15 mth Sib of Present ears; sparse hair cases 7 & 9 report 9 M + 1 y - Severe Hypertonic limbs ? 3 y Present report NM = not mentioned. 121 on September 21, 2020 by guest. Protected by copyright. http://jmg.bmj.com/ J Med Genet: first published as 10.1136/jmg.31.2.121 on 1 February 1994. Downloaded from
Transcript of Microcephaly and congenital nephrotic …Garty,Eisenstein, Sandbank, Kaffe, Dagan, Gadoth I1 111 III...

J7 Med Genet 1994;31:121-125
Microcephaly and congenital nephroticsyndrome owing to diffuse mesangial sclerosis:an autosomal recessive syndrome
Department ofPaediatrics and theKipper Institute ofPaediatricImmunology,Beilinson MedicalCentre, Petah Tiqva49100, IsraelB Z GartyPaediatric NephrologyUnit, BeilinsonMedical Centre, PetahTiqva, and SacklerFaculty of Medicine,Tel Aviv University,IsraelB EisensteinPathologyDepartment,Beilinson MedicalCentre, Petah Tiqva,and Sackler Faculty ofMedicine, Tel AvivUniversity, IsraelJ SandbankThe Genetics Clinic,Mount Sinai MedicalCenter, New York,NY, USAS KaffeDepartment ofPaediatrics, SorokaMedical Centre, BeerSheva, IsraelR DaganNeurologyDepartment,Beilinson MedicalCentre, Petah Tiqva,and Sackler Faculty ofMedicine, Tel AvivUniversity, Israel.N Gadoth
Correspondence toDr Garty.Received 9 February 1993Revised version accepted forpublication 24 August 1993
Ben Zion Garty, Bella Eisenstein, Judith Sandbank, Sara Kaffe, Ron Dagan,Nathan Gadoth
AbstractThree sibs born to consanguineous par-ents had congenital nephrotic syndrome,microcephaly, and psychomotor retard-ation. Pathology of the kidneys showeddiffuse mesangial sclerosis with depositsof IgG and C3 in the mesangium andglomerular basement membranes. Allthree children died before the age of 3years. Of 19 published cases of childrenwith the association of congenital neph-rotic syndrome and microcephaly, onlyfour had histological evidence of diffusemesangial sclerosis, and two of their sibsprobably had the same disease. The asso-
ciation of nephrotic syndrome owing tocongenital diffuse mesangial sclerosis,microcephaly, and mental retardationappears to be a distinct syndrome with anautosomal recessive mode of inheritance.
Nephrotic syndrome in the first year of life(congenital nephrotic syndrome) is rare. In-fantile microcystic disease, or the Finnish typenephrotic syndrome, is the best documentedform of the syndrome.4 Other known causes ofcongenital nephrotic syndrome are intrauter-ine infection,56 renal vein thrombosis,7 andmercury intoxication.8 Minimal change neph-rotic syndrome, congenital focal glomerularsclerosis, membranous glomerulopathy, or dif-fuse mesangial sclerosis are uncommon causes
of nephrotic syndrome in the first year of life."'The association of congenital nephrotic syn-
drome, microcephaly, and mental retardationhas been reported in 19 children,12-2' but onlysix of them had diffuse mesangial sclerosis(table).'121 We report a family with three mic-rocephalic children who had severe psychomo-tor retardation and congenital nephrotic syn-drome owing to diffuse mesangial sclerosis.
(_J Med Genet 1994;31:121-125)
Congenital microcephaly is associated with a
variety of pathological conditions, includingchromosomal aberrations, metabolic diseases,intrauterine infections, postradiation injury,and chronic hypoxaemia.' In its isolated form,it is usually inherited in an autosomal recessivemode2 and is accompanied by severe mentalretardation. Occasionally it is inherited in an
autosomal dominant mode, and in thesepatients the retardation is usually milder.`3
Case reportsThe family was of Jewish North African ori-gin. The pedigree is shown in fig 1. There were
consanguineous marriages in generations IIIand IV-V. The father of the proband was themother's uncle. Except for the proband andtwo of his sibs, there were no other familymembers with kidney disease or psychomotorretardation. The other five sibs, as well as theparents, were healthy and did not have micro-cephaly. The mother of the proband did notsmoke and had not taken medication or alcohol
Clinical and pathological findings in the patients with congenital nephrotic syndrome owing to diffuse mesangial sclerosis and microcephaly
Case Sex Micro- Onset of Kidney Mental Neurological Dysmorphic Age at Notes Refcephaly nephr syn histology retardation symptoms features death
1 F + 1 d Mesangial sclerosis + Seizures No 3 mth 162 M + 6 d Diffuse mesangial ? Decreased vision & Wide set eyes;
sclerosis hearing small nose 2 mth 193 F + 6 d Mesangial sclerosis Hypertonic arms; Floppy ears; contractures 2 mth 20
seizures of hands & feet4 M + 12 d - NM NM Floppy ears; I mth Sib of 20
hypertelorism case 35 M + 14 mth Mesangial sclerosis Severe Seizures; hypertonic limbs; Micrognathia; 18 mth 21
poor head control; no large earsvisual fixation
6 F + 9 mth - Severe Hypertonic limbs; seizures; Large ears; 3 y Sib of 21poor vision & hearing small midface case 5
7 M + 1 mth Diffuse messangial Severe Hypertonic limbs; poor Large, low set, floppy 2 y Consan- Presentsclerosis. IgG and head control; strabismus; ears; sparse, thin hair; guinity reportC3 deposit in the poor vision & hearing micrognathia; bilateralmesangium undescended testes
8 F + 1 mth Identical to case 7 Severe Identical Large, low set, floppy 15 mth Sib of Presentears; sparse hair cases 7 & 9 report
9 M + 1 y - Severe Hypertonic limbs ? 3 y Presentreport
NM = not mentioned.
121
on Septem
ber 21, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Garty, Eisenstein, Sandbank, Kaffe, Dagan, Gadoth
I1
111
III
IV
Iv
V
Vl
Figure 1 Family pedigree.
during the pregnancies. Data regarding pla-cental weight of the different pregnancies andalphafetoprotein measurements are not avail-able.
CASE 1 (VI.8)The boy was the term product of a normalpregnancy and delivery. Birth was 4400 g andmarked microcephaly was noted.During the first months of life, generalised
oedema, recurrent vomiting, and psychomotorretardation were seen. On admission, at the ageof 11 months, the patient had puffy eyes andmild pitting oedema of the ankles and sacrum.
Blood pressure was 100/60 mmHg, pulse rate110/minute, and respiratory rate 24/minute.Weight was 8000 g (3rd centile for his age),length 74 cm (60th centile for his age), andhead circumference 40 cm (- 5 SD below themean for his age). The nose was small and theears were large and low set, with unusuallysoft auricles. Strabismus, high arched palate,micrognathia, and sparse, thin hair were alsopresent. Examination of the heart and lungsshowed no abnormalities. There was no viscero-megaly and the kidneys were not palpable. Thescrotum was underdeveloped with bilateralundescended testes. The penis was normal.There was bilateral overlapping of the first toeby the second.
Neurological evaluation disclosed poor headcontrol, inability to sit up or turn, and absenceof interest in his surroundings. The anteriorfontanelle was small and barely palpable. Thecranial nerves were unremarkable. Motor ex-
amination showed muscle wasting without fas-ciculation and absence of purposeful move-
ments. Strength was decreased mainly in the
proximal muscles, with a tendency to hyperto-nicity and scissoring of both legs. The fistswere constantly clenched. Pain sensation wasgrossly intact and deep tendon reflexes werehyperactive with flexor plantar responses. Thepatient neither responded to noise nor fol-lowed objects with his eyes for more than a fewseconds. Constant head rolling was presentand he seldom smiled. Fundoscopic examina-tion was normal.
Laboratory data showed haemoglobin11-3 g/dl, white blood count 7 x 109 cells/l(45% neutrophils, 40% lymphocytes, 15%monocytes), platelets 460 x 109/l, blood ureanitrogen 3 9 mmol/l, and creatinine 35-4 imol/1. Total serum protein measured 30 g/l, withalbumin 19 g/l; C3 component of the comple-ment was 1.3 g/l, C4 0-3 g/l, CH50 70%. Cho-lesterol was 0-65 mmol/l, triglycerides0 75 mmol/l, and total lipids 4-6 mmol/l. IgGwas 2-3 g/l (normal for age: 7-2 ± 2 7 g/l), IgA0-6 g/l (normal: 0 7 ± 0 3 g/l), IgM 1-3 g/l (nor-mal: 0 63 + 0 3 g/l). Urine analysis showed 5 to10 erythrocytes in high power field and granu-lar casts. Daily urinary protein excretion was3-8 to 4-8 g (mainly albumin). Creatinine clear-ance was 100 to 105 ml/min/1 73 m2.The following laboratory tests were normal:
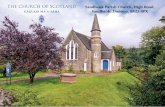
serum sodium, potassium, chloride, calcium,phosphorus, magnesium, bilirubin, aspartateaminotransferase (SGOT), lactate dehydroge-nase (LDH), creatinine kinase (CK), uric acid,pH, lactate, pyruvate, T4, serology for rubella,toxoplasma, cytomegalovirus and syphilis,cerebrospinal fluid, electrocardiography, elec-troencephalography, and electromyography.The karyotype was of a normal male. Intra-venous pyelography showed mild enlargementof both kidneys. Skull radiography disclosed asmall cranium; the rest of the skeletal radio-graphic survey was normal. Bone age was 9months. Cerebral CT scan showed a smallposterior fossa with enlargement of the fourthventricle and ambient cisterna compatible withcerebellar hypoplasia. There was also a milddegree of enlargement of the lateral and thirdventricles (fig 2).
Percutaneous kidney biopsy showed hyper-cellularity of mesangial cells, an increase inPAS positive material in the mesangial matrix,and mild thickening of the capillary wall. Oc-casional segments showed obliteration of theirnormal structure. A few immature glomeruliwere noted, as well as microcystic transforma-tion of a few tubuli (fig 3). Electron micro-scopy of the glomeruli showed effacement ofthe epithelial foot processes and dilatation ofthe mesangium owing to hypercellularity andabundance of matrix. Electron dense depositswere present in the subendothelial region ofthe peripheral and axial glomerular basementmembrane and in the mesangium. The laminadensa was irregular and sometimes thinner andsometimes thicker than usual (fig 4). Immu-nofluorescence staining showed massive de-posits of IgG and C3 in the mesangium andglomerular basement membrane. These find-ings suggested the diagnosis of infantile diffusemesangial sclerosis. The patient was dis-charged and was lost to detailed follow up. He
122
on Septem
ber 21, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Microcephaly and congenital nephrotic syndrome owing to diffuse mesangial sclerosis: an autosomal recessive syndrome
Figure 2 Cerebral CT scan showing enlargement of thefourth ventricle and cerebellar hypoplasia.
developed renal failure and died at the age of 2years.
CASE 2 (VI.3)The sister of case 1, born at term after anuneventful pregnancy and delivery, was ex-amined at the age of 12 months. Head circum-ference was 39 5 cm (-5 SD below the meanfor her age). There was poor head control andsevere psychomotor retardation. Deep tendonreflexes were hyperactive and the limbs were
spastic. She could not turn and showed nointerest in her surroundings or in social com-munication. Pitting oedema of the ankles andsacrum was present. She had strabismus,sparse hair, and large, low set, floppy ears, likeher brother.
Laboratory tests showed hypoproteinaemia,hypoalbuminaemia, and hyperlipidaemia(total lipids were 1040 mg/dl). Urine analysisshowed massive proteinuria, microscopichaematuria, and granular casts. Kidney biopsyshowed similar changes to those seen in case 1.She was treated with 2 mg/kg/day of predni-sone but without apparent effect. During thesecond year of life, rapid deterioration in kid-ney function occurred, and serum creatininelevel reached 530 gmol/l. She died at the age of15 months of E coli septicaemia. Necropsycould not be performed.
CASE 3 (VI.1)This patient, the brother of patients 1 and 2,also had a "little head", hypertonia of thelimbs, severe psychomotor retardation,oedema, and proteinuria. His kidney functiondeteriorated gradually and he died before theage of 3 years. The clinical evaluation of thispatient was performed at another hospital andkidney histology was not available.
DiscussionThe characteristic features of congenital neph-rotic syndrome associated with microcephalyare severe mental retardation, rapid deteriora-tion of kidney function, unresponsiveness tomedication, and usually fatal outcome beforethe age of 3 years. Nineteen cases of thisassociation, first described by Galloway andMowat,'2 have been reported.12-2' Additionalfindings include neurological abnormalities,
Btw
toI !. i
40%. 0 t o
t *A% 01%I 0
% 0
4% N 4.$
t 4 0
4
123
on Septem
ber 21, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Garty, Eisenstein, Sandbank, Kaffe, Dagan, Gadoth
..~~~~
s.
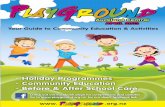
Figure 4 Electron microscopy ofglomerular tuft showing subendothelial andparamesangial subendothelial deposits (arrow heads), increase in mesangial matrix(thick arrow), thinning of lamina densa (short thin arrows), and partial effacement offoot processes (long thin arrows).
such as abnormal muscle tone and seizures,and minor dysmorphic features, such as an
unusually shaped head, low set, floppy ears,
micrognathia, and, occasionally, hiatus her-nia.'2-14 Histology of the kidneys was reportedin 12 of the 19 affected patients. However,some were evaluated by light microscopy onlyand in most cases immunofluorescence stain-ing was not mentioned. Some patients under-went renal biopsy and in others tissue was
obtained at necropsy. Thus, the available in-formation on kidney histology is incomplete. Ifwe divide the patients according to the classifi-cations of Habib and Bois" and Kaplan et al,9four had diffuse mesangial sclerosis,'-21 threemicrocystic dysplasia,'2 14 three focal glomeru-losclerosis,'41620 one had mesangial prolifera-tion,21 and one a combination of microcysticdysplasia and focal glomerulosclerosis." De-spite the variability in kidney histology, most
patients had a similar clinical course of declin-ing renal function and early death. Only two
patients reached the age of 5 years.'620 How-ever, it is clear that, based on renal histologyfindings, these are different entities. A similardeteriorating clinical course was also noted inthe patients with the "isolated" form of con-
genital nephrotic syndrome,22 without micro-cephaly.Our patients' kidney histology showed dif-
fuse mesangial sclerosis. Congenital nephroticsyndrome resulting from diffuse mesangialsclerosis has been reported in association withocular abnormalities (nystagmus, cataract, or
microphthalmia),2324 male pseudohermaphro-ditism and Wilms's tumor (Drash syn-
drome),21 or microcephaly.Of special interest in our patients is the
finding of IgG and C3 deposits in the mesan-
gium and of IgG deposits along the basement
membrane. No immune complex depositswere mentioned in the other cases of congen-ital nephrotic syndrome and microcephaly,except for a patient with focal glomeruloscler-osis reported by Roos et al,'6 who showeddeposits of IgM in the basal membrane of thecapillary loops, and the patient with mesangialproliferation, reported by Cooperstone et al,2'who had segmental distribution of fine granu-lar deposits of IgM.
In patients with "isolated" congenital neph-rotic syndrome owing to diffuse mesangialsclerosis (without microcephaly), occasionaldeposits of immune complexes were noted.For example, of three sibs with diffuse mesan-gial sclerosis one had mesangial deposits ofIgG, IgM, C3, and fibrinogen, while the othertwo, although they had a similar kidney dis-ease, had no demonstrable deposits of immunecomplexes.'0 This may have related to thestage of disease or to its differing pathogenesis.No specific metabolic abnormalities were
found in our patients or in those previouslyreported. The neurological abnormalities andthe mental retardation are probably secondaryto the severe microcephaly and the abnormalbrain structure. The mental retardation incases of severe microcephaly is negatively cor-related with brain volume, especially inpatients with autosomal recessive microce-phaly.2 Although brain histology was not avail-able in our cases, brain CT scan suggestedgeneral atrophy, which was more pronouncedin the subependymal zone, and cerebellarhypoplasia. In two previously reportedpatients with congenital nephrotic syndromeowing to diffuse mesangial sclerosis and micro-cephaly, the brain histology showed micro-gyria in the frontal, parietal, and occipitallobes20 and pachygyria with neuronal ecto-pia. 20 The association of congenital kidneydisease and neural migration defect was alsoreported in two other male sibs with glomeru-lar kidney disease causing proteinuria and hy-drocephalus.26 This may suggest a commoninsult during the first weeks of gestation affect-ing both the kidneys and the brain.Four of the 19 previously reported children
with congenital nephrotic syndrome and mic-rocephaly had histological findings of diffusemesangial sclerosis. 1821 Two sibs of thesepatients202' probably had the same kidney dis-ease as well. Thus, two of the previouslyreported patients were sporadic cases, and theother four were pairs of brothers and sistersborn to non-consanguineous parents.202' Thefact that our three patients were sibs (two boysand a girl of a family of eight sibs) and thattheir parents were consanguineous, supportthe assumption of autosomal recessive inherit-ance of this syndrome.
We are indebted to Professor Mina Ben Bassat of the PathologyDepartment for her help and suggestions.
1 Ramirez ML, Rivas F, Cantu JM. Silent microcephaly: adistinct autosomal dominant trait. Clin Genet1983;23:281-6.
2 Hecht F, Kelly JV. Little heads: inheritance and earlydetection. J Pediatr 1979;95:731-2.
3 Merlob P, Steier D, Reisner SH. Autosomal dominant
124
on Septem
ber 21, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.2.121 on 1 F
ebruary 1994. Dow
nloaded from

Microcephaly and congenital nephrotic syndrome owing to diffuse mesangial sclerosis: an autosomal recessive syndrome
isolated ("uncomplicated") microcephaly. J Med Genet1988;25:750-3.
4 Huttunen NP. Congenital nephrotic syndrome of Finnishtype: study of 75 patients. Arch Dis Child 1976;51:344-8.
5 Shahin B, Papadopoulou ZL, Jenis EH. Congenital nephro-tic syndrome associated with congenital toxoplasmosis. JPediatr 1974;85:366-70.
6 McDonald R, Wiggelinkhuizen J, Kaschula ROC. Thenephrotic syndrome in very young infants. Am J DisChild 1971,122:507-12.
7 Lewy PR, Wellington J. Nephrotic syndrome in associationwith renal vein thrombosis in infancy. J Pediatr1974;85:359-65.
8 Wilson VK, Thomson MC, Holzel A. Mercury nephrosis inyoung children. BMJ 1952;1:358-60.
9 Kaplan BS, Bureau MA, Drummond KN. The nephroticsyndrome in the first year of life: is a pathologic classifica-tion possible? J Pediatr 1974;85:615-21.
10 Kristal H, Lichtig C. Infantile nephrotic syndrome. Clino-pathological study of 11 cases. IsrJ7 Med Sci 1983;19:626-30.
11 Habib R, Bois E. Heterogeneite des syndromes nephro-tiques a debut precoce du nourrison (syndrome nephro-tique infantile). Helv Paediatr Acta 1973;28:91-107.
12 Galloway WM, Mowat AP. Congenital microcephaly withhiatus hernia and nephrotic syndrome in two sibs. J MedGenet 1968,5:319-21.
13 Robain 0, Lyon G. Les micrencephalies familiales parmalformation cerebrale. Acta Neuropathol (Berl)1972;20:96-109.
14 Shapiro LR, Duncan PA, Farnsworth PB, Lefkowitz M.Congenital microcephaly, hiatus hernia and nephroticsyndrome: an autosomal recessive syndrome. Birth De-fects 1976;XII:275-8.
15 Metzke H, Bromme W. Kongenitale Mikrozephalie mitMuskelhypotonie und nephrotischem Syndrom. PediatrGrenzgeh 1982;21:39-41.
16 Roos RAC, Maaswinkel-Mooy PD, Loo EM, KanhaiHHH. Congenital microcephaly, infantile spasms, psy-chomotor retardation and nephrotic syndrome in twosiblings. Eur J Pediatr 1987;146:532-6.
17 Kozlowski PB, Sner JH, Nicastri AD, Rudelli RD. Brainmorphology in the Galloway syndrome. Clin Neuropathol1989;8:85-91.
18 Robain 0, Deonna T. Pachygyria and congenital nephrosisdisorder of migration and neuronal orientation. ActaNeuropathol (Berl) 1983;60:137-41.
19 Koskimies 0, Sariola H, Holmberg C, Rapola J. Clinicalquiz. Pediatr Nephrol 1991;5:433-5.
20 Gaudelus J, Leverger G, Rault G, et al. Association d'unsyndrome nephrotique a debut precoce et d'une microce-phalie. Arch Fr Pediatr 1984;41:409-15.
21 Cooperstone BG, Friedman A, Kaplan BS. Galloway-Mowat syndrome of abnormal gyral pattern and glomeru-lopathy. Am J Med Genet 1993;47:250-4.
22 Mahan JD, Mauer SM, Sibley RK, Vernier RL. Congenitalnephrotic syndrome: evolution of medical managementand results of renal transplantation. J Pediatr 1984;105:549-57.
23 Martul EV, Cuesta MG, Churg J. Histopathologic variabil-ity of the congenital nephrotic syndrome. Clin Nephrol1987;28: 161-8.
24 Glastre C, Cochat P, Bouvier R, et al. Familial infantilenephrotic syndrome with ocular abnormalities. PediatrNephrol 1990;4:340-2.
25 Habib R, Loirat C, Gubler MC, et al. The nephropathyassociated with male pseudohermaphroditism and Wilms'tumor (Drash syndrome): a distinctive glomerular lesion.Report of 10 cases. Clin Nephrol 1985;24:269-78.
26 Palm L, Hagerstrand I, Kristoffersson U, Blennow G,Brum A, Jorgensen C. Nephrosis and disturbances ofneuralonal migration in male siblings - a new hereditarydisorder? Arch Dis Child 1986;61:545-8.
125
on Septem
ber 21, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.2.121 on 1 F
ebruary 1994. Dow
nloaded from