
Methods of Blood Collection and Anticoagulants
108
METHODS OF BLOOD COLLECTION AND ANTICOAGULANTS MODERATOR – Dr MAHANTHACHAR PRESENTED BY - Dr SHREYA PRABHU 1
-
Upload
shreya-d-prabhu -
Category
Healthcare
-
view
100 -
download
4
Transcript of Methods of Blood Collection and Anticoagulants

METHODS OF BLOOD COLLECTION AND
ANTICOAGULANTS
MODERATOR – Dr MAHANTHACHAR
PRESENTED BY - Dr SHREYA PRABHU
1
BLOOD COLLECTION
2
PRECOLLECTION VARIABLES
In preparing patient for phlebotomy,care should be taken to minimize physiologic factors related to activities that might influence laboratory determinations.
These include-
Diurnal variation
Exercise
Diet
Stress
Posture
Age
Gender
Personal Habits
3
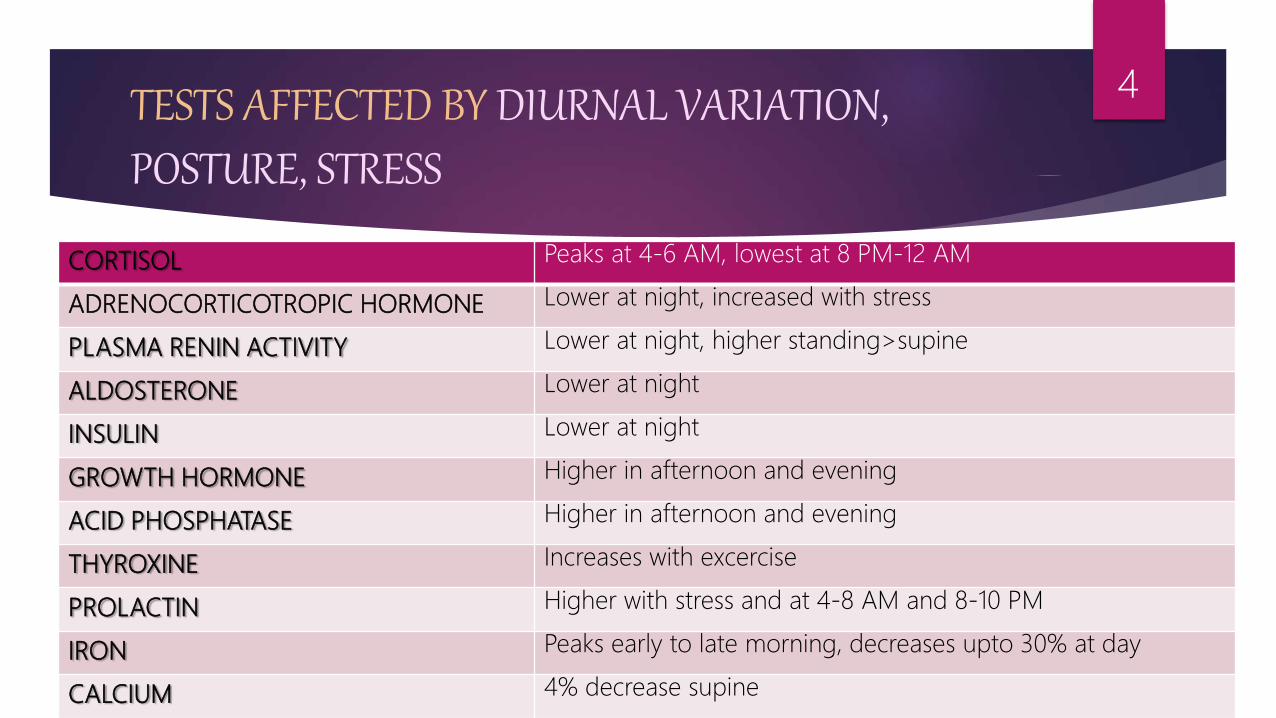
TESTS AFFECTED BY DIURNAL VARIATION, POSTURE, STRESS
CORTISOL Peaks at 4-6 AM, lowest at 8 PM-12 AM
ADRENOCORTICOTROPIC HORMONE Lower at night, increased with stress
PLASMA RENIN ACTIVITY Lower at night, higher standing>supine
ALDOSTERONE Lower at night
INSULIN Lower at night
GROWTH HORMONE Higher in afternoon and evening
ACID PHOSPHATASE Higher in afternoon and evening
THYROXINE Increases with excercise
PROLACTIN Higher with stress and at 4-8 AM and 8-10 PM
IRON Peaks early to late morning, decreases upto 30% at day
CALCIUM 4% decrease supine
4

BLOOD COLLECTION
SITE
VENIPUNCTURE/SPECIMEN COLLECTION
DEVICE
SITE PREPARATION
PERSONAL SAFTEY
TIME OF COLLECTION
THE TEST ORDER
STORAGE AND PRESERVATION
SPECIMEN REJECTION
5

TESTS PERFORMED ON COLLECTED BLOOD
HEMATOLOGICAL TESTS
BIOCHEMICAL TESTS
SEROLOGICAL TESTS
CULTURAL TESTS
6
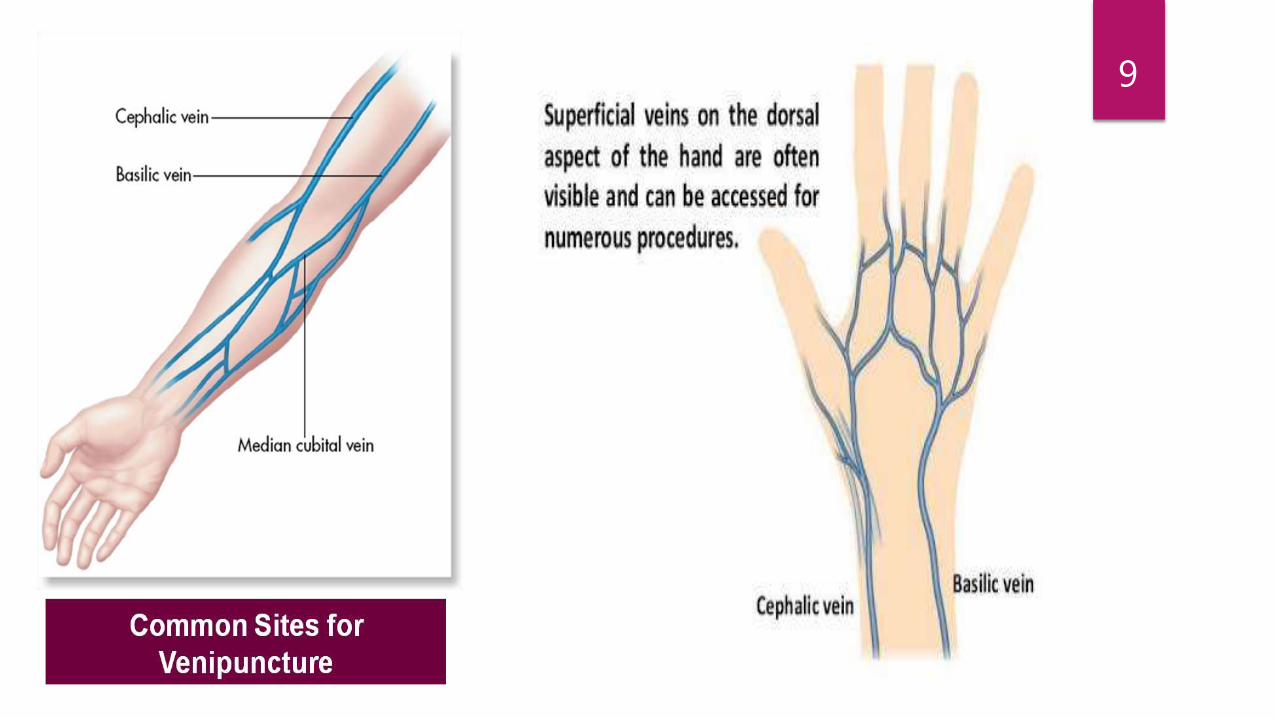
SITE
Blood can be collected from 3 different sources-
1. Capillary
2. Venous ( most common)
3. Arterial
7
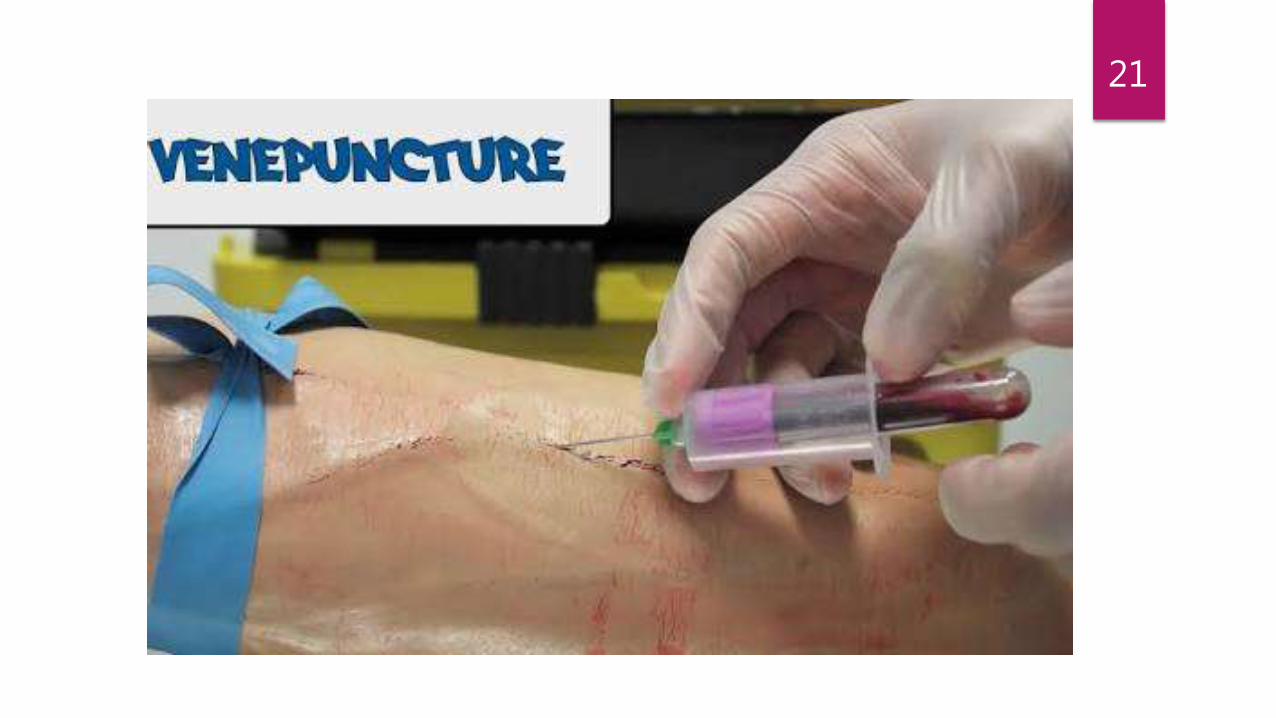
VENIPUNCTURE
Venipuncture is a routine and common procedure done to collect venous blood directly from the vein.
Best site- Ante-cubital fossa
In order to do this safely, the phlebotomist must have a basic understanding of the following;
I. Anatomy
II. The criteria for choosing a vein
III. The device used
IV. Skin preparation
V. Personal safety – infection control policy
8
9
10

PHLEBOTOMY TRAY
ITEMS TO BE INCLUDED-
a) Syringes and needles
b) Tourniquet
c) Specimen containers ( or evacuated tube system) – plain and with various anticoagulants
d) Request form
e) 70% isopropanol swabs and cellulose pads
f) Adhesive dressings
g) Self sealing plastic bags
h) Rack to hold specimen upright during process of filling
i) A puncture resistant disposal container should also be available
11

12

13

NEEDLES should not be too fine/ too large/ too long
Vary from large (16 G) to small (23 G)
For adults- 19 or 21 G suitable
For children- 23 G
Ideally should have short shaft (15mm)
Butterfly needles- when blood has to be collected from a very small vein
Come in 21, 23, 25 G
14

15
SYRINGE
TOURNIQUET
BUTTERFLY NEEDLE

SKIN PREPARATION
Skin cleansing with an alcohol swab.
Asepsis should be maintained.
The two main sources of microbial contamination are:
a) The hands of the phlebotomist
b) The skin of the patient
Good hand washing and drying techniques. If hand washing facilities are unavailable, an alcohol based hand wash solution is an acceptable substitute
16

VENOUS PUNCTURE TECHNIQUE
PROCEDURE:
Verify computer printed labels match requisitions
Check patient identification band against labels and requisition forms
Ask patient for his/her demographics
Position patient properly
Assemble equipment and supplies
Apply tourniquet on the upper arm and ask to make a fist
Select suitable vein for puncture
17
Put on gloves
Cleanse the site
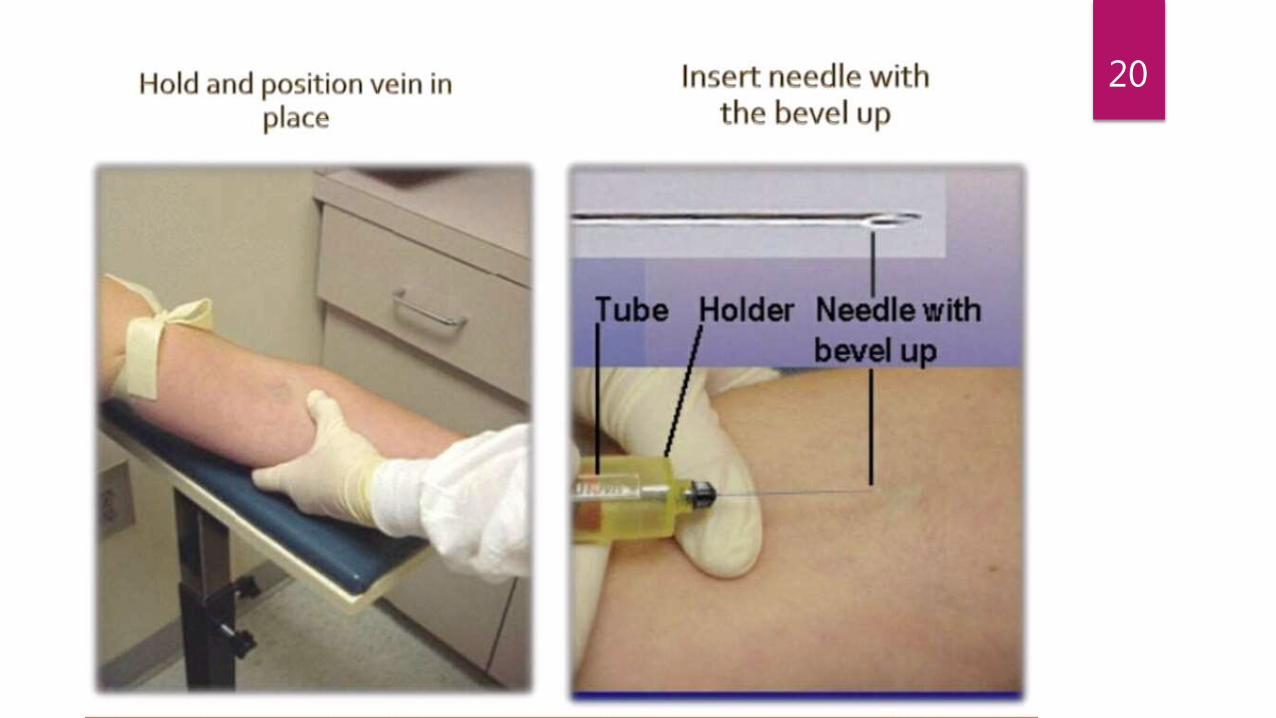
Anchor vein firm
Enter skin with needle at 30 degree angle/ < to arm with bevel up of the needle
Follow geography of vein and insert needle smooth
Using a syringe , pull back on the barrel with a slow, even tension as blood flows into the syringe
Release tourniquet when blood begins to flow.
Never withdraw needle without releasing tourniquet
18
Withdraw needle and then apply pressure to the site.
Mix and invert tubes with anticoagulants
Check patient’s condition
Dispose material in designated containers using universal precautions
Label the tubes with –
a. Patient’s name
b. Identification number
c. Date and time of collection
d. Identification of person collecting specimen
Deliver sample to appropriate lab section
19
20
21
PRECAUTION
Area must be cleansed / sterilized properly
Tourniquet should not be applied for long time
Blind attempts should not be made
Once needle withdrawn pressure should be applied and maintained for 1-2 mintues, if not can cause ECCHYMOSES
22
POST-PHLEBOTOMY PROCEDURE
Check again patient’s details and make sure it corresponds to details on request form
Each submitted specimen must be labeled with the patient’s Demographics (written exactly as it appears on the Test Request Form) and the tests to be conducted.
Patient dempographics include – Patient name, sex, age, DOB, DOA, DOE, hospital number, room number, lab number, physician and physician’s pharmacy code number
Use one Test Requisition form only
23
Label each specimen with the patient’s name, and time of specimen collection
Write the Total number of specimens submitted on the Test Requisition form
Specimens should be sent in individual plastic bags/ set upright in a holder or rack, separated from request form to prevent contamination in event of leaking
Without separating needle from syringe place both together with swab and any dressings in a puncture resistant container
24

PERSONAL SAFETY
Protection for all personnel is paramount when handling blood products and body fluids.
Universal Precautions to be followed:
1) Every patient should be regarded as a potential biohazard
2) GLOVES MUST BE WORN.
3) Avoid needle stick injury –Hepatitis B and HIV viruses transmitted in blood and body fluids
4) Dispose of sharps and or soiled equipment appropriately and safely; keep gloves on whilst disposing of equipment, then dispose of gloves safely.
25
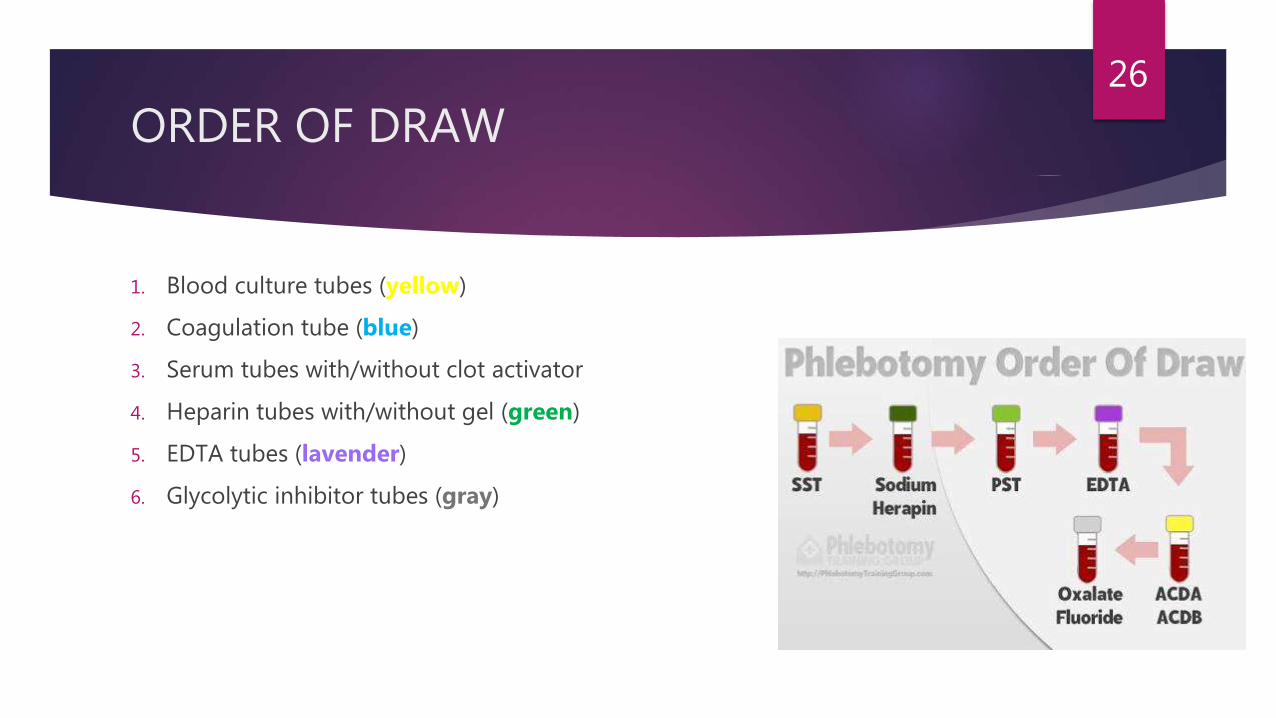
ORDER OF DRAW
1. Blood culture tubes (yellow)
2. Coagulation tube (blue)
3. Serum tubes with/without clot activator
4. Heparin tubes with/without gel (green)
5. EDTA tubes (lavender)
6. Glycolytic inhibitor tubes (gray)
26
SPECIMEN REJECTION
Clotted specimen
Severely hemolyzed specimen
Improperly labeled or unlabeled specimen
Specimen too old
Failure to meet volume criteria
Improperly collected (diluted) capillary specimen
Leaking tube
Delay in transport
Collection of specimen in wrong tube
27

COMPLICATIONS
Immediate local complications :
Haemoconcentration
Collapse of the vein
Failure of blood to enter the syringe .
Needle not in position
28
Immediate general complications:
Syncope
Late local complications :
Thrombosis of the vein
Thrombophlebitis
Hematoma.
29
COLLECTION OF BLOOD FOR HEMATOLOGICAL EXAMINATIONS:
Hb, RBC, WBC, DLC, Platelet count, Red Cell Indices, Peripheral Smear
COLLECTION OF BLOOD FOR BIOCHEMICAL EXAMINATIONS:
Fasting conditions are advisable
Venous blood to be preferred.
30
COLLECTION OF BLOOD FOR SEROLOGICAL EXAMINATIONS:
5 ml of blood is collected in a plain bulb & is allowed to clot at 37 deg for 1– 2 hours.
Alternately if immediate investigations are needed, the blood is defibrinated, centrifuged & serum is separated.
E.g. ; Diagnosis of Syphilis, Enteric fever ( Widal Test ) , HIV , HBsAg determination.
COLLECTION OF BLOOD FOR CULTURAL EXAMINATION:
5 - 10 cc of blood is collected in a 25 – 50 cc of Harley’s broth or Robertson’s cooked meat medium & incubated.
E.g. : Bacterial endocarditis, Enteric Fever , Septicemias
31
COMMON ERRORS IN SPECIMEN COLLECTION
Misidentification of patient
Mislabelling of specimen
Short draws/wrong anticoagulant/blood ratio
Mixing problems/clots
Wrong tubes/wrong anticoagulant
Hemolysis/lipemia
Hemoconcentration from prolonged tourniquet time
Exposure to light/extreme temperature
Improperly timed specimen/delayed delivery to laboratory
Processing errors
32
CAUSES FOR MISLEADING RESULTS RELATED TO SPECIMEN COLLECTION
PRE-COLLECTION
Urination within 30 min
Food or water intake within 20 minutes
Stress
Drugs/ dietary supplement administration within 8 hours
33
DURING COLLECTION
Different time
Posture, lying, standing, sitting
Haemoconcentration from prolonged tourniquet pressure
Excessive negative pressure when drawing blood
Incorrect tube
Capillary versus venous blood
34
HANDLING OF SPECIMEN
Insufficient or excess anticoagulant
Inadequate mixing of blood with anticoagulant
Error in patient and/or specimen identification
Inadequate specimen storage conditions
Delay in transit to laboratory
35

CAPILLARY BLOOD
36
CAPILLARY BLOOD
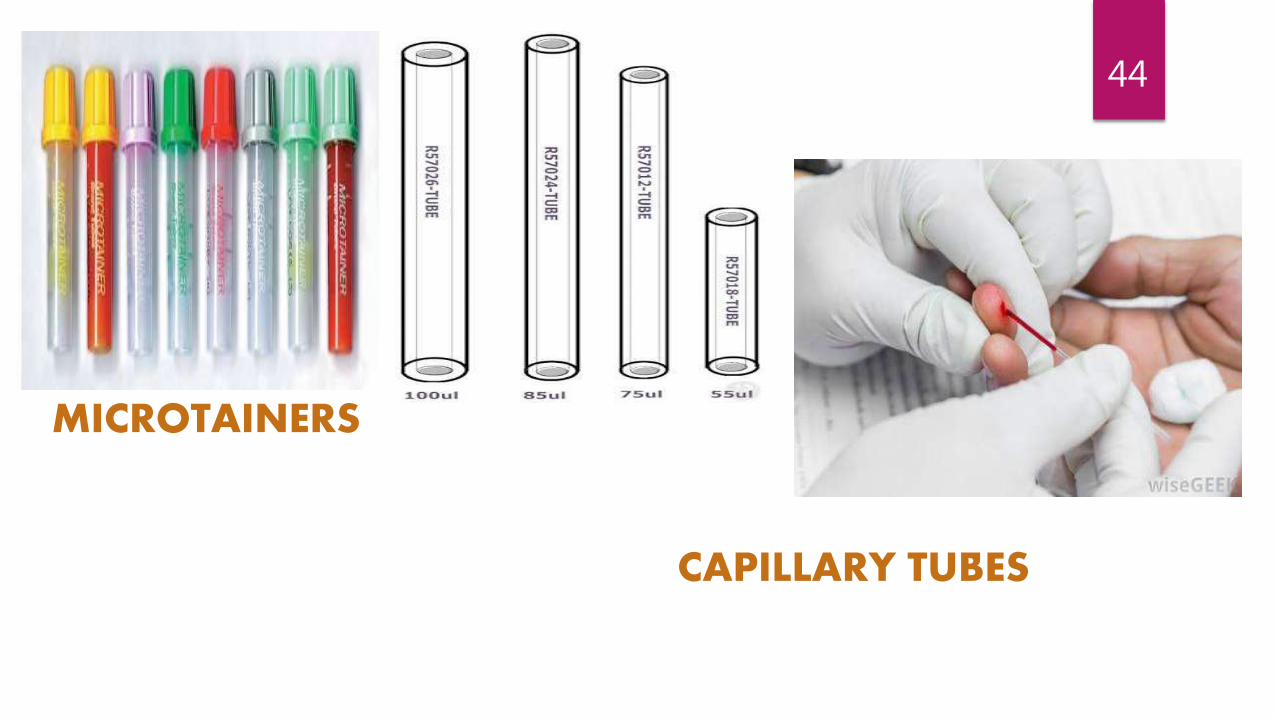
For routine assays requiring small amount of blood (into capillary tubes coated with
Heparin or anticoagulated microcollection device)
Obtained by SKIN PRICK/PUNCTURE METHOD
Prick site should be free of congestion/ oedema/ cyanosed/ cold
37

38

INDICATIONS
IN ADULTS-
Extreme obesity
Severe burns
Thrombotic tendencies
In Geriatric patients because skin is thinner and less elastic- hematoma more likely to occur from a venipunctutre
39

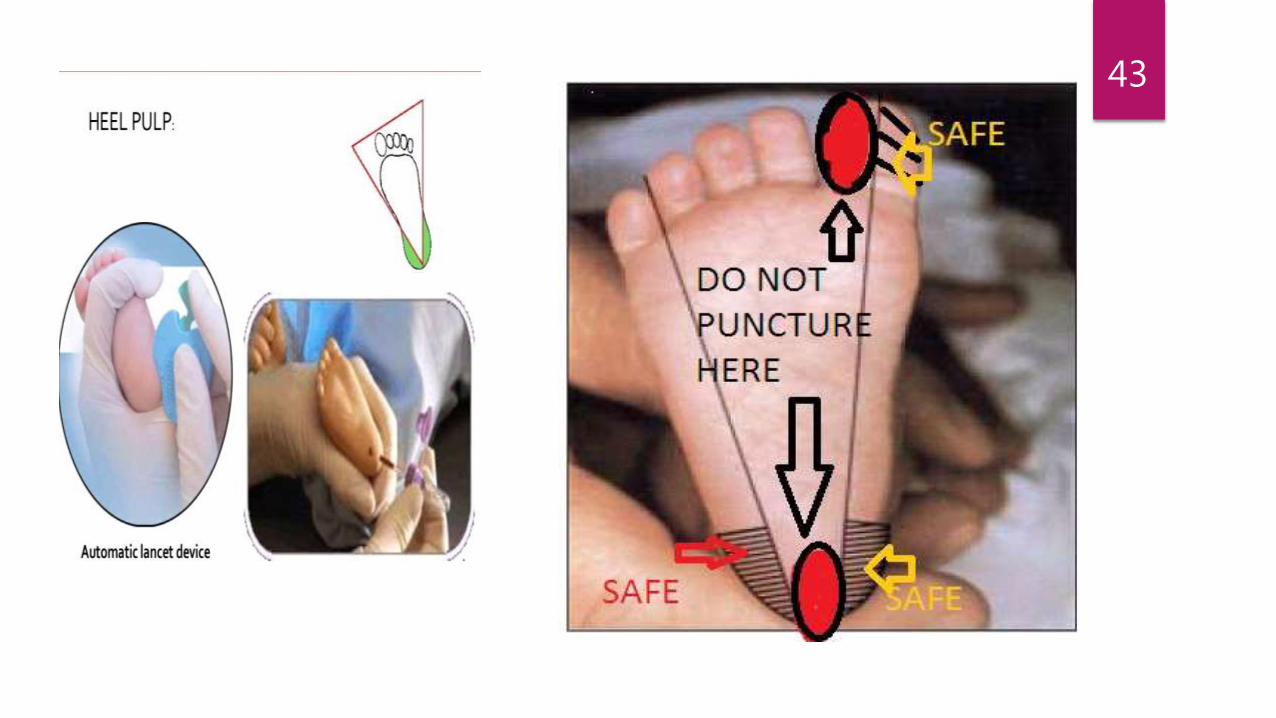
SKIN PUNCTURE TECHNIQUE
Select an appropriate puncture site
For infants <12 months- Lateral/ Medial plantar heel surface
For infants >12 months, children, adults- Palmar surface of last digit of second/third/fourth finger
Warm the puncture site- arterial enriched blood
Cleanse the site
Make puncture with sterile lancet perpendicular to skin surface
Discard first drop of blood by wiping it away
40
Collect the specimen in suitable container by capillary action
Apply pressure and dispose of the puncture device
Label the specimen container with date and time of collection and patient
demographics
Indicate in report that test results are from skin puncture
41

42
LANCET
SKIN PUNCTURE
43
44
MICROTAINERS
CAPILLARY TUBES
ARTERIAL BLOOD
45

ARTERIAL BLOOD
Technically more difficult to perform
Increased pressure in arteries make it difficult to stop bleeding
Order of preference- Radial> Brachial> Femoral arteries
Specially required for estimation of ABG, pH, CO2 , O2
Anticoagulant amount should be 0.05ml liquid Heparin for each millilitre of blood
46

47

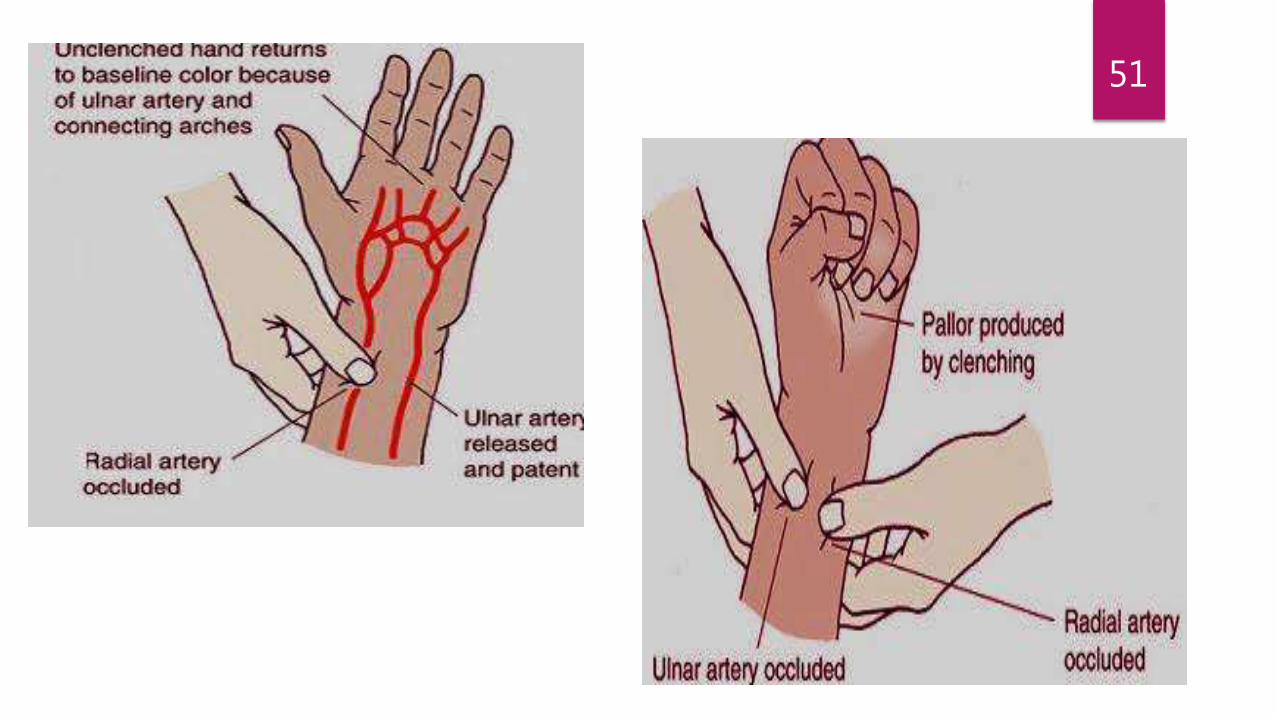
Before blood collected from Radial artery in the wrist, one should perform MODIFIED ALLEN TEST to determine whether Ulnar artery can provide collateral circulation to the hand after the Radial artery punctured
48
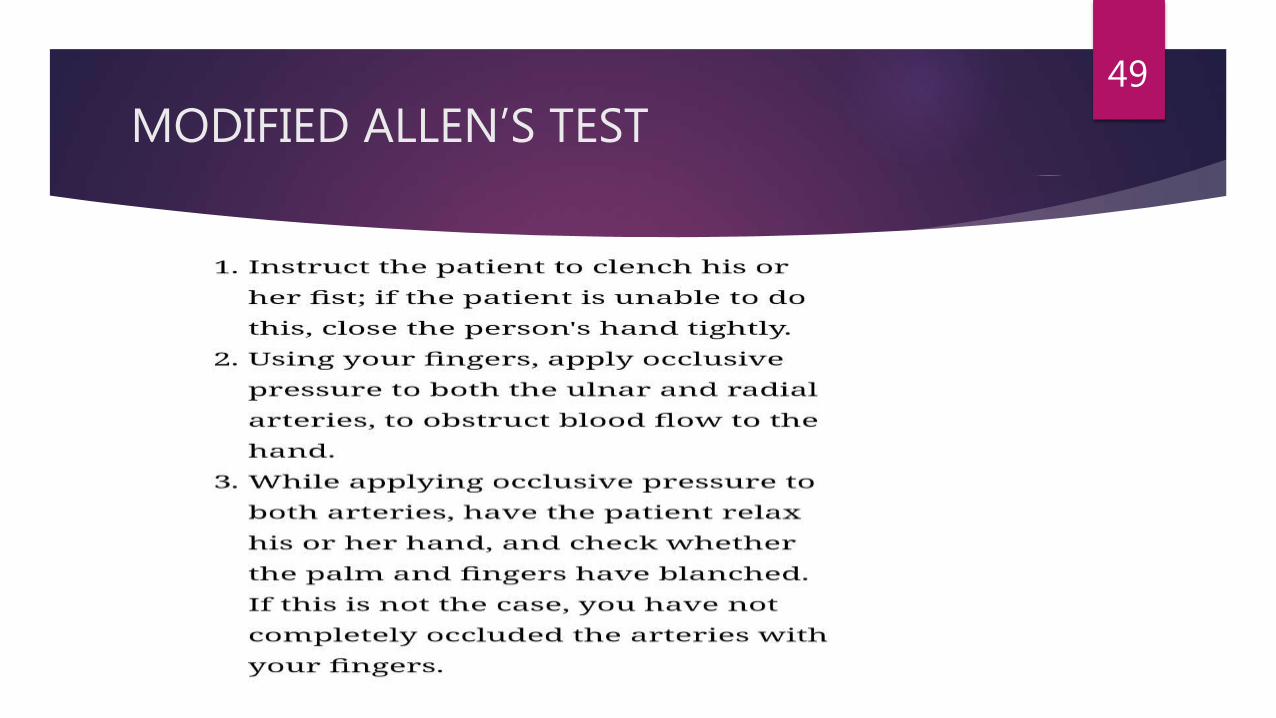
MODIFIED ALLEN’S TEST49
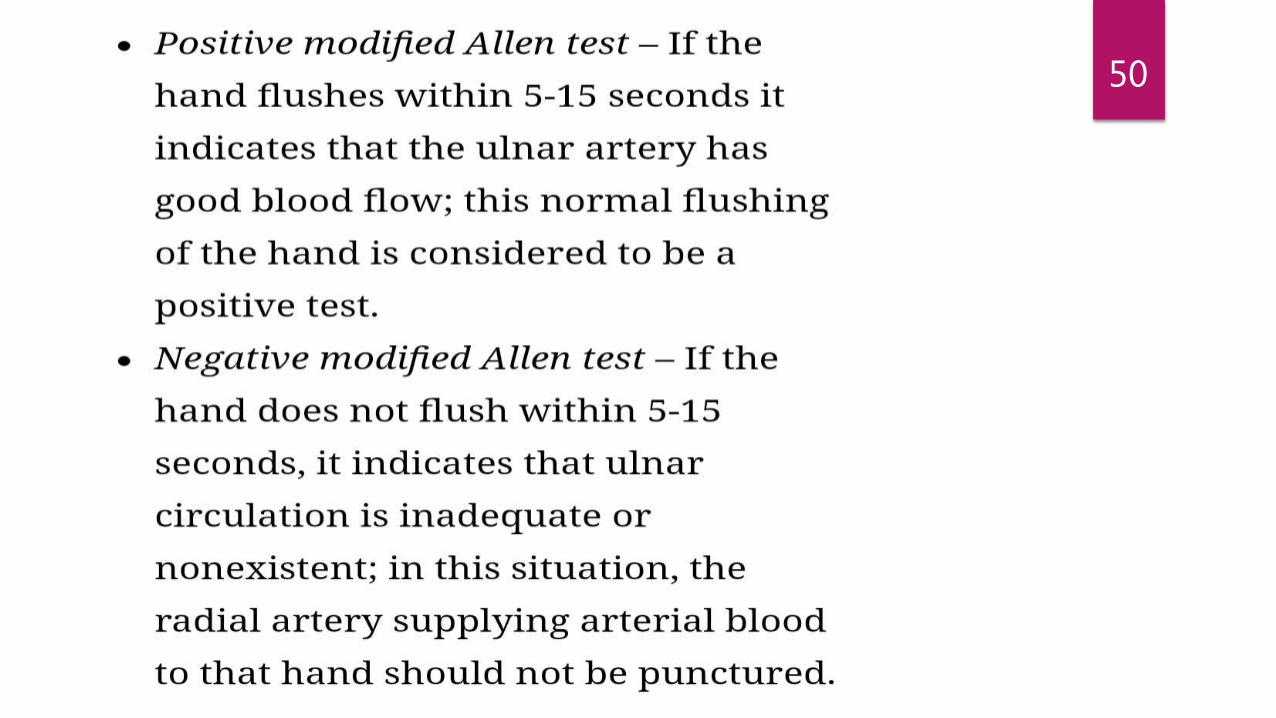
50
51

52
ARTERIAL PUNCTURE PROCEDURE
Prepare ABG syringe according to established procedures
Needle (18-20 gauge) should pierce skin at 45-60 degrees for brachial, 90 degree for femoral(23-25 gauge). Pulsations of blood into syringe confirm that it will fill by arterial pressure alone
After blood collected, place dry gauge over puncture site while quickly withdrawing the needle and the collection device
Compress the puncture site quickly, expel air from the syringe, activate needle safety feature, discard into sharps container
Mix specimen thoroughly by gently rotating/ inverting
Place in ice water
53

CENTRAL VENOUS ACCESS
INDICATIONS:
Ready access to patient’s circulation
Eliminates multiple phlebotomies
Useful in crtical care and surgical situations to draw blood/administer blood products/drugs and provide parenteral nutrition
Indwelling catheters are surgically inserted into CEPHALIC VEIN/ INTERNAL JUGULAR VEIN/ SUBCLAVIAN VEIN/ FEMORAL VEIN
54

ORDER OF DRAW FROM CATHETER LINES
Draw 3-5ml in a syringe and discard
Blood for blood culture
Blood for anticoagulated tubes
Blood for clot tubes
55
PRECAUTIONS TO PREVENT HAEMOLYSIS
Apparatus should be clean and dry
The bore of needles should not be too fine/small
Blood should be withdrawn slowly without strong suction
Needle should be removed from syringe before the blood is expressed into the bottles
Mix blood with anticoagulants by gentle swirling
Blood should not be kept too long sitting at room temperature and if refrigerated should not be frozen
56

STORAGE OF BLOOD BEFORE TESTS DONE
Ideally tests should be done immediately after blood is collected-
Within 2 hours- PT, other coagulation tests, Platelet count, blood smearing
Within 3 hours- ESR
Within 24 hours- RBC count, PCV, Hb, WBC count, Reticulocyte countcount
57
SPECIMEN TRANSPORT
Accounts for approximately 1/3rd TAT
Excessive agitation avoided
Protected from direct exposure to sunlight
Kept at 4ºC immediately after collection and transported on ice for analysis of unstable constitutents
Specimen requiring refrigeration must be maintained between 2-10*C
58

ANTICOAGULANTS
59
DEFINITION
A substance that prevents coagulation or clotting of blood but doesn’t dissolve an already formed clot.
Uses
• Storage of blood for blood transfusion or hematological testing
• Therapeutic
60
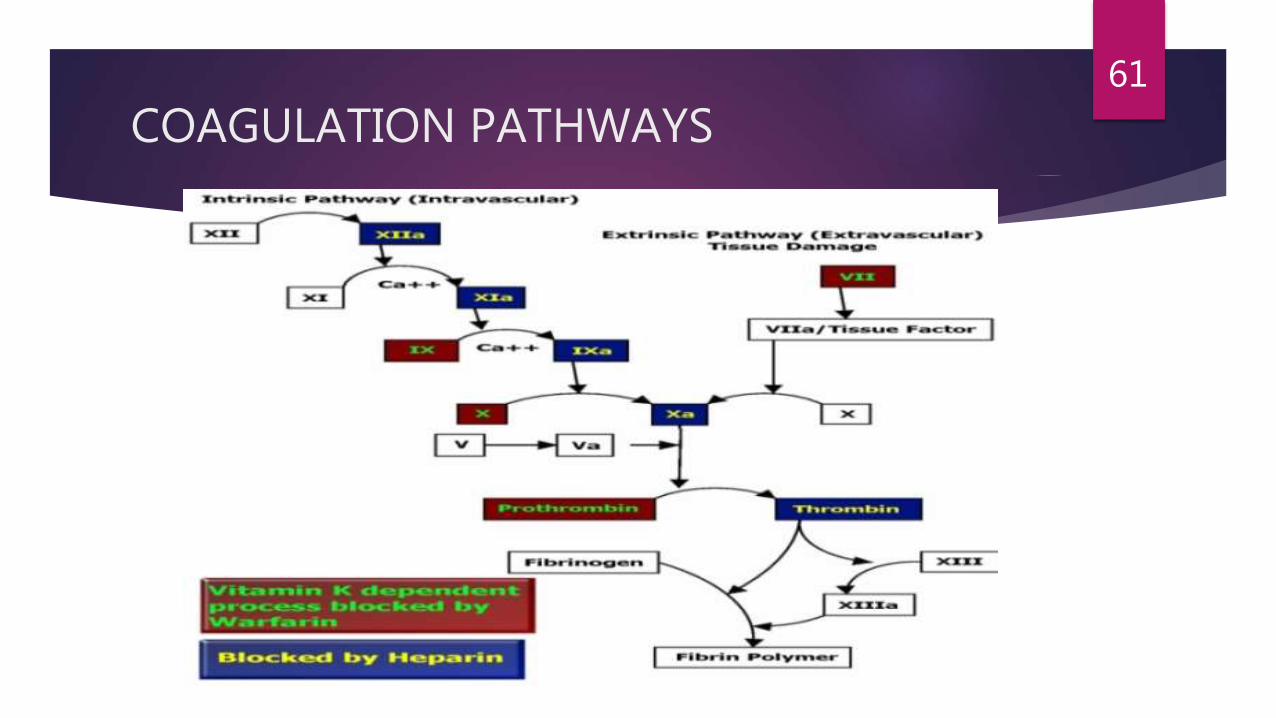
COAGULATION PATHWAYS61
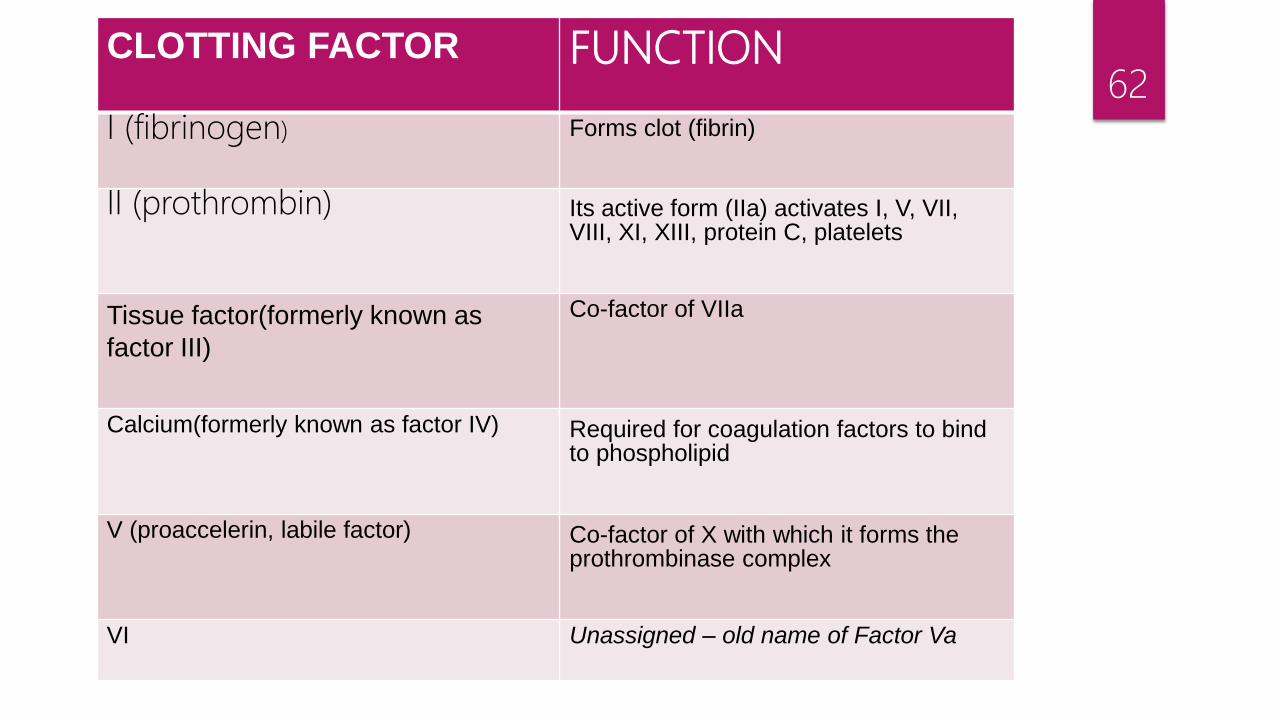
62CLOTTING FACTOR FUNCTION
I (fibrinogen) Forms clot (fibrin)
II (prothrombin) Its active form (IIa) activates I, V, VII, VIII, XI, XIII, protein C, platelets
Tissue factor(formerly known as
factor III)
Co-factor of VIIa
Calcium(formerly known as factor IV) Required for coagulation factors to bind to phospholipid
V (proaccelerin, labile factor) Co-factor of X with which it forms the prothrombinase complex
VI Unassigned – old name of Factor Va
63
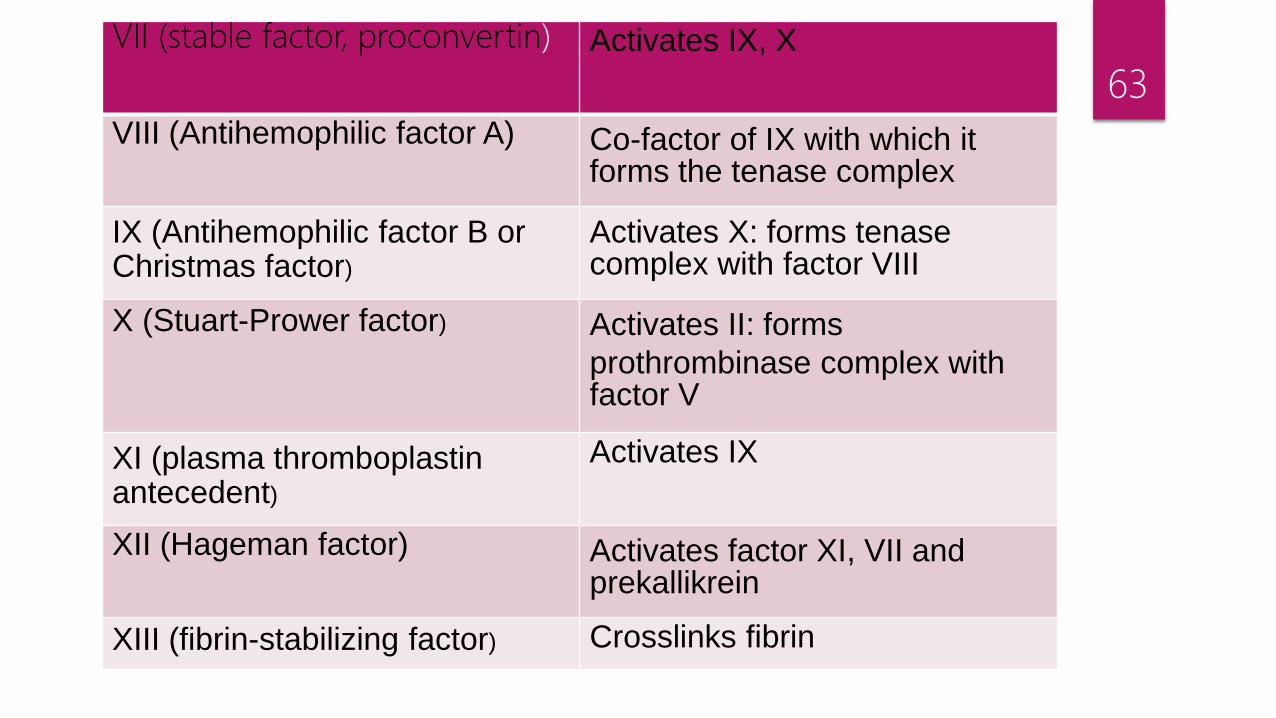
VII (stable factor, proconvertin) Activates IX, X
VIII (Antihemophilic factor A) Co-factor of IX with which it forms the tenase complex
IX (Antihemophilic factor B or Christmas factor)
Activates X: forms tenase complex with factor VIII
X (Stuart-Prower factor) Activates II: forms
prothrombinase complex with factor V
XI (plasma thromboplastin antecedent)
Activates IX
XII (Hageman factor) Activates factor XI, VII and prekallikrein
XIII (fibrin-stabilizing factor) Crosslinks fibrin

STORAGE LESIONS
A set of biochemical and biomechanical changes occur during storage leading to decreased viability of the cells and its physiological functions
RBC’s:
Decreased ATP and 2,3 DPG levels, pH- acidic
Poor functioning of Na-K pump- accumulation of K in stored blood
Oxidative damage with lipid peroxidation
Loss in membrane lipids affects deformability and osmotic fragility
Morphological changes- Disc changes to echinocytes and to spherocytes
64
Increased cellular rigidity d/t decrease in deformability
Decrease in critical hemolytic volume(CHV) in parallel with membrane lipid content
CHV is largest volume to which RBC swells before haemolysis
Decrease in osmotic fragility
65
PLATELETS:
Loss of discoid shape, microscopic platelet aggregate formation, fragmentation, appearance of disintegrated balloon forms
Blood stored for >24 hour at 2-6ºC has few viable platelets and granulocytes
Heat labile coagulation factors V & VIII decrease on storage upto 50% in first 72hrs
To ensure that blood retains its in vivo environment Anticoagulants are added
66

Drop in pH and dextrose level causes anaerobic glycolysis in RBC to generate ATP.
Decreased ph causes Decreased 2,3-DPG and cells ability to release oxygen to the tissues.
Metabolic functions slow down in cold temperature, ATP levels decreases.
ELECTROLYTE: loss of potassium from RBC to plasma
passage of sodium from plasma to cells
plasma ammonia levels also increase
67
COMMONLY USED ANTICOAGULANTS
EDTA (ETHYLENE DIAMINE TETRA ACETIC ACID)
DOUBLE OXALATE
SODIUM CITRATE
SODIUM FLUORIDE
HEPARIN
ACD (ACID CITRATE DEXTROSE)
CPD (CITRATE PHOSPHATE DEXTROSE)
CPDA (CITRATE PHOSPHATE DEXTROSE ADENINE)
68
EDTA
Used for routine hematological work
MOA: chelating effect on calcium molecule in blood.
Three types of EDTA salts used in salt or liquid form-
Sodium- di/tri
Potassium- di/tri
Lithium- di
DIPOTASSIUM SALT more soluble than DISODIUM SALT, hence preferred
Solubility- K2> Na2> Li2
69

DILITHIUM SALT is equally effective, sample of blood can be used for chemical investigations
TRIPOTASSIUM SALTS are available in liquid form with disadvantage of:
Dilution
Shrinkage of RBC
Decrease in 2-3% PCV in 4 hours
Gradual increase in MCV
TRISODIUM EDTA not recommended because of high pH
70

Coding of vial- LAVENDER CAP
Recommended concentration-
K2-EDTA -1.5-2.0mg/ml
71

CHANGES OCCURRING DUE TO PROLONGED STORAGE in EDTA
72

USES
TLC
DLC
ESR (by wintrobe method)
CBC
RETICULOCYTE COUNT
PLATELET COUNT
73
DISADVANTAGES
Excess EDTA irrespective of salt, affects both RED CELLS and LEUCOCYTES- causing shrinkage and degenerative changes
On RBC-
Crenation, Spherocytic change
Significant decrease in PCV
Increase in MCHC
On WBC-
Leuco-agglutination
74
On PLATELETS-
Cause them to swell and disintegrate- causing artificially high count
Responsible for activity of naturally occurring antiplatelet auto-antibody causing satelitism
Blood films from EDTA fails to demonstrate BASOPHILIC STIPPLING of RBC in poisoning
EDTA also appears to suppress platelet degranulation
Monocyte activation measured by release of tissue factor & TNF is lowered with EDTA than with citrate & heparin
75

DOUBLE OXALATE
Acts by chelating calcium in blood
POTASSIUM OXALATE: Used at a concentration of 2mg/ml
Causes RBC shrinkage- 8% shrink in PCV
AMMONIUM OXALATE: Used at a concentration of 2mg/ml
Causes swelling of RBC
Thus not used individually for PCV, ESR or Blood smears
76

BALANCED OXALATE/ DOUBLE OXALATE/ WINTROBE’S MIXTURE:
To balance swelling and shrinking effect of both salts, they are combined in a mixture with ratio of 3 parts of NH4 oxalate to 2 parts of K oxalate which is used at concentration of 2mg/ml of blood
Prepared in a solution of 20 mg/ml- 2mg/0.1ml of solution- pipetted into containers-incubated to evaporate the fluid- redissolves in blood
Avoid high temperature as it inactivates anticoagulants
77

USES:
Hb
PCV
WBC
PT
ESR (Wintrobe Method)
78
DISADVANTAGES:
Calcium in the blood combines with oxalate to form insoluble calcium
oxalate which precipitates
They are phagocytosed by neutrophils- distort WBC morphology- not
good for smears
Never used in blood to be transfused- as it is toxic and calcium oxalate
precipitate may harm
79
TRISODIUM CITRATE
Acts by chelating calcium in blood
Used as 3.2% and 3.8% solution
It is used in a concentration of :-
1 part sodium citrate to 4 parts whole blood for ESR (by westergren)
1 part sodium citrate to 9 parts whole blood for coagulation profile.
80

CITRATE VIAL
Citrate is usually in BLUE VACUTAINER
TUBE. It is in liquid form in the tube and is used for coagulation tests. It gets rid of the calcium, but not as strongly as EDTA
81

USES PT
APTT
ESR(by westergren method)
DISADVANTAGES Alters concentration of blood as it is always used in solution form , hence not used
for routine hematology.
82

SODIUM FLOURIDE
Sodium fluoride has a double action on the blood:
It prevents clotting by chelating calcium.
It prevents all phosphatase action, inhibit glucose oxidase activity
in enzymatic glucose reaction.
Prevents glycolysis for 3 days
It is used for determination of blood sugar.
In bacterial specticemia, fluoride inhibition of glycolysis is
neither adequate nor effective in preserving glucose
concentration
83
Common disadvantages with calcium chelators
They inhibit various plasma enzyme activities like:
Amylase activity inhibited by oxalate and citrate
LDH and Acid Phosphatase inhibited by oxalate
Fluoride , Heparin or EDTA interfere with accurate determination of electrolytes
84
HEPARIN
Lithium or Sodium salt of Heparin at a concentration of 10-20 IU/ml of blood is commonly used for chemistry, gas analysis and emergency tests
Lithium is recommended
Doesnot alter the size of RBC- minimum chance of lysis after blood has been drawn– best anticoagulant for osmotic fragility tests and suitable for phenotyping
85
ACTION
Heparin is a naturally-occurring anticoagulant produced by basophils and mast cells
Heparin accelerates the action of Antithrombin III, neutralising Thrombin and prevents formation of Fibrin
Heparin acts as an anticoagulant, preventing the formation of clots and extension of existing clots within the blood.
Heparin does not break down clots that have already formed
86

AMOUNT FOR
BLOOD STORAGE:5 – 10 IU /mL of blood
SAMPLE COLLECTION: 0.5- 2.0 IU/mL
87

USES
Ammonia
Carboxyhemoglobin
Blood gases
Electrolytes ( doesnot affect the levels of
ions)
ESR
Methaemoglobin
Osmotic Fragility
HLA Typing
88

Disadvantages Costly
In Leishman stained peripheral blood film blue color is imparted to the background due to presence of plasma protiens
Not suitable for blood counts as it often induces platelet and leucocyte clumping
Should not be used in study of PCR with restriction enzymes because it inhibits enzyme activity
89

90
CRENATED RBC
PLATELET CLUMP
LEUCOAGGLUTINATIONCHANGES IN BLOOD SMEAR DUE TO EXCESS ANTICOAGULANT
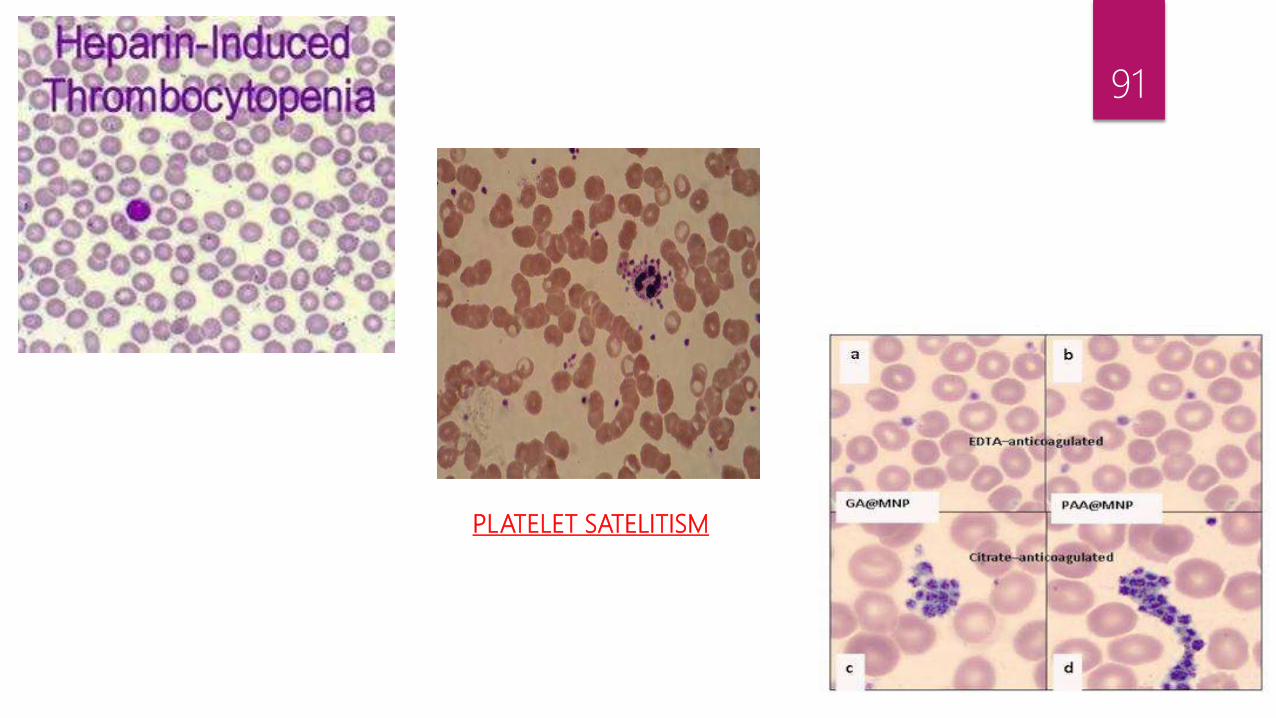
91
PLATELET SATELITISM

COLOUR CODING OF VIALS
92

93
SODIUM CITRATEFOR COAGULATION STUDIES
K-OXALTE/SODIUM FLOURIDEGLUCOSE DETERMINATION
NO ADDITIVECOLLECTION OF SERUM
ACDPRESERVE RBC FOR BLOOD BANKING &HLA Typing
HEPARININHIBIT THROMBIN ACTIVATION
EDTAFOR ROUTINE HAEMATOLOGY

TUBE COLOUR AND ANTICOAGULANT/ ADDITIVE 94
STOPPER COLOR ANTICOAGULANT SPECIMEN ACTION
RED (glass) None Serum/Chemistry, serology N/A
RED (plastic) Clot activator Serum/Chemistry, serology Silica clot activator
LAVENDER (glass) K3EDTA in liquid form Whole blood/ Hematology Chelates Calcium
LAVENDER K2EDTA/ spray dried Whole blood/ Hematology Chelates Calcium
PINK K2EDTA/ spray dried Whole blood/ blood bank and molecular diagnostics
Chelates Calcium
WHITE EDTA and gel Plasma/ molecular genitics Chelates Calcium
LIGHT BLUE Sodium Citrate Plasma/ Coagulation Chelates Calcium
LIGHT BLUE Thrombin and Soya bean trypsin inhibitor
Plasma/ Coagulation Fibrin degradation products

95STOPPER COLOR ANTICOAGULANT SPECIMEN ACTION
BLACK Sodium Citrate Plasma Chelates Calcium
LIGHT GREEN/ BLACK
Lithium Heparin and gel Plasma/ chemistry Inhibhits Thrombin formation
GREEN Sodium Heparin, LithiumHeparin
Plasma/ chemistry Inhibhits Thrombin formation
ROYAL BLUE Sodium Heparin, K2EDTA Plasma/ chemistry, Toxicology
Heparin-InhibhitsThrombin formationEDTA-ChelatesCalcium
GRAY Sodium Fluoride/Potassium Oxalate
Plasma/ Glucose testing
Inhibits glycolysis

96STOPPER COLOR ANTICOAGULANT SPECIMEN ACTION
YELLOW Sterile containingSodium Polyanetholesulfonat
Serum/ microbiologyculture
Aids in bacterial recovery by inhibhitingcomplement, phagocytes and certain antibodies
YELLOW Acid citrate dextrose Plasma/ blood bank, HLA phenotypingpaternity testing
WBC preservation
TAN (glass) Sodium heparin Plasma/ lead testing Inhibits Thrombin formation
TAN (plastic) K2EDTA Plasma/ lead testing Chelates Calcium
YELLOW/GRAY and ORANGE
Thrombin Serum/ chemistry Clot activator
RED/GRAY andGOLD
Clot activator separation gel
Serum/ chemistry Silica Clot activator
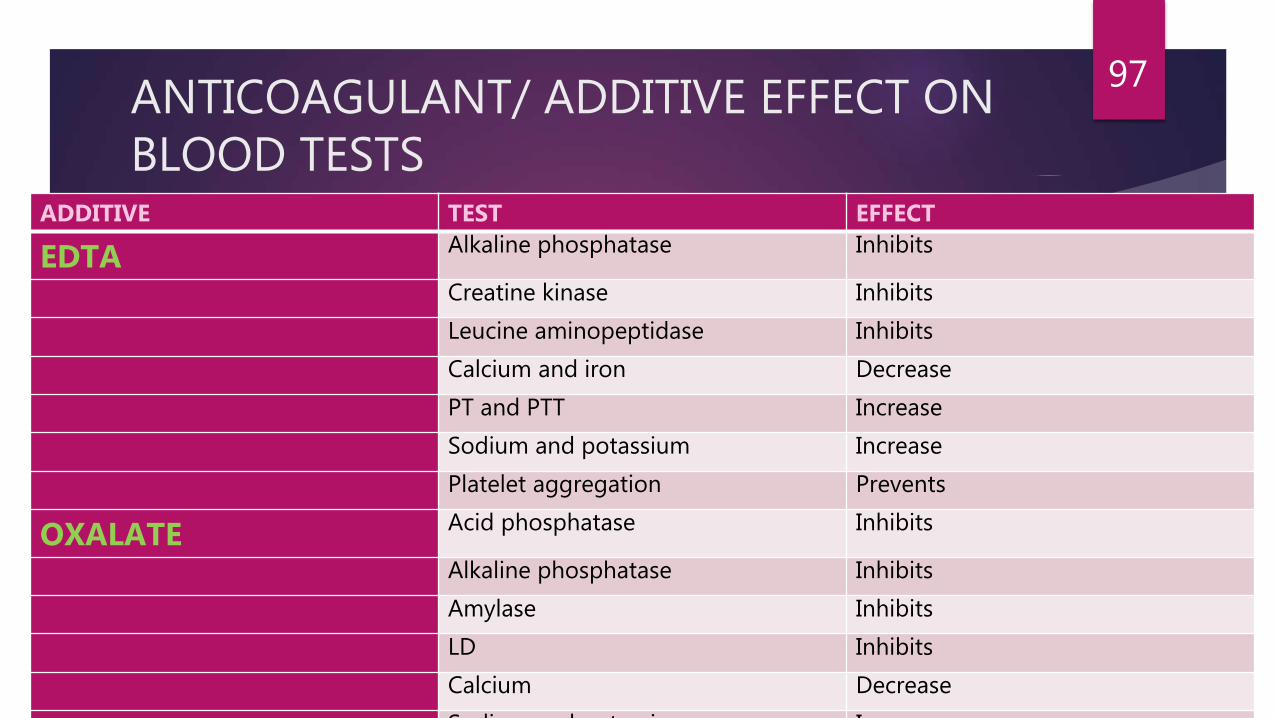
ANTICOAGULANT/ ADDITIVE EFFECT ON BLOOD TESTS
ADDITIVE TEST EFFECT
EDTA Alkaline phosphatase Inhibits
Creatine kinase Inhibits
Leucine aminopeptidase Inhibits
Calcium and iron Decrease
PT and PTT Increase
Sodium and potassium Increase
Platelet aggregation Prevents
OXALATE Acid phosphatase Inhibits
Alkaline phosphatase Inhibits
Amylase Inhibits
LD Inhibits
Calcium Decrease
Sodium and potassium Increase
97

98ADDITIVE TEST EFFECT
CITRATE ALT and AST Inhibits
Alkaline phosphatase Inhibits
Acid phosphatase Stimulates
Amylase Decreases
Calcium Decreases
Sodium and potassium Increase
Labile coagulation factors Preserve
HEPARIN T3 Increases
Thyroxine Increases
PT and PTT Increase
Wright’s stain Causes blue background
Lithium (LiHep tubes only) Increases
Sodium (NaHep tubes only) increases

99
ADDITIVE TEST EFFECT
FLUORIDES Acid phosphatase Decreases
Alkaline phosphatase Decreases
Amylase Decreases
Creatine kinase Decreases
ALT and AST Decreases
Cell morphology Distorts

ANTICOAGULANTS FOR BLOOD STORAGE
ACD (Acid Citrate Dextrose)
CPD(Citrate Phosphate Dextrose)
CPDA-1(Citrate Phosphate Dextrose Adenine)
HEPARIN
100
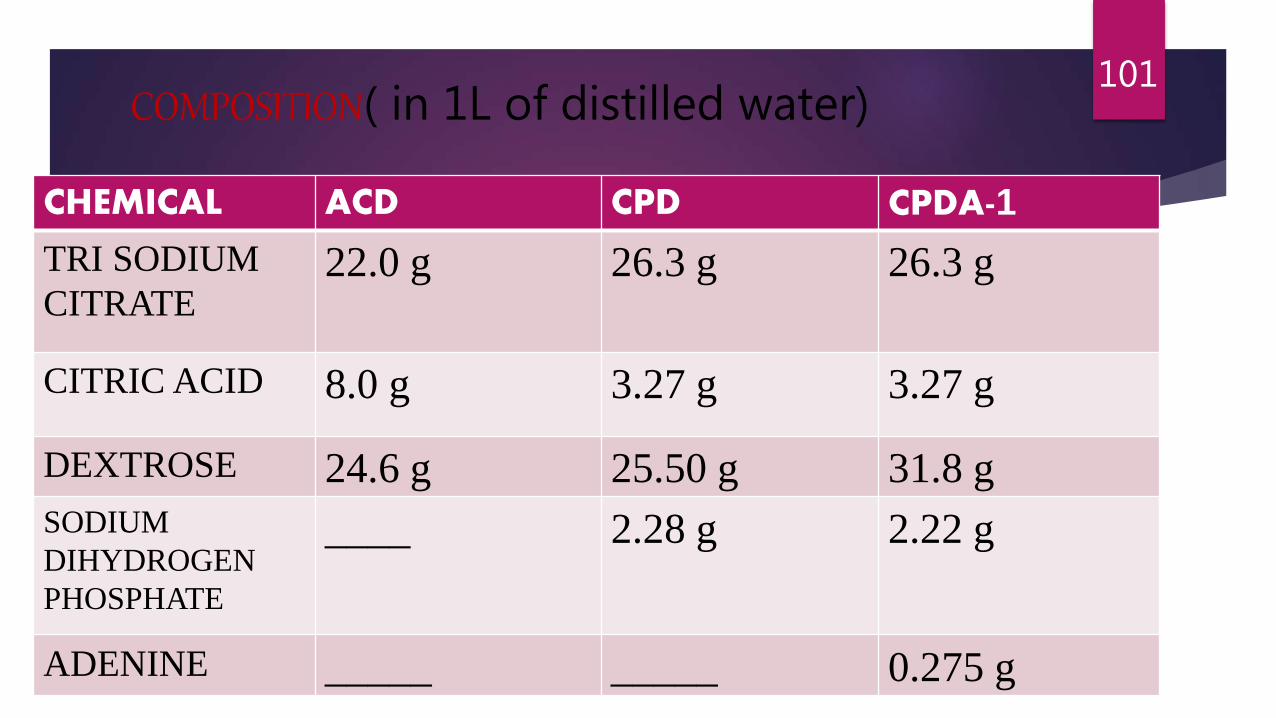
COMPOSITION( in 1L of distilled water)
CHEMICAL ACD CPD CPDA-1
TRI SODIUM
CITRATE22.0 g 26.3 g 26.3 g
CITRIC ACID 8.0 g 3.27 g 3.27 g
DEXTROSE 24.6 g 25.50 g 31.8 g
SODIUM
DIHYDROGEN
PHOSPHATE
____ 2.28 g 2.22 g
ADENINE _____ _____ 0.275 g
101

15ml of ACD and 14ml of CPD & CPDA-1 is required for preservation of 100ml of blood
Initial pH of ACD 5.0 and of CPD & CPDA-1 is 5.6
Also storage time at 2-6ºC for ACD & CPD is 21 days and for CPDA-1 is 35days
102

FUNCTION OF VARIOUS COMPONENTS
o CITRATE
Causes chelation of calcium
SODIUM DIPHOSPHATE
Prevents fall in pH
o DEXTROSE
Addition of glucose prolongs survival of stored RBC as it is required for metabolism. Glucose passes from plasma to RBC and is utilized for energy production.
2 PATHWAYS for energy production :
• 90% by Embedem Mayeroff pathway in which there is breakdown of glucose into lactate through anaerobic glycolysis.
103

Prevents carmalization of glucose in citrate dextrose solution during autoclaving.
o ADENINE
It is added in modified CPD as it improves viability of RBC because of enhanced
enhanced ATP production.
104

• 10% by Pentose phosphate pathway through aerobic glycolysis.
The various intermediaries formed are necessary for maintaining
their ability to deliver oxygen to tissues through generation of
2,3-DPG.
Viability correlates with the level of ATP.
o CITRIC ACID
Fairly weak tribasic hydroxyacid
Along with tri sodium citrate which is alkaline gives an optimal pH.
105
ADDITIVE SYSTEM
To extend RBC storage to 42 days and to harvest maximum amount of plasma, additive systems are now available in which storage environment of RBC is altered by adding certain nutrients after removal of plasma
Its made by adding the following components to the CPD :-
• Sodium chloride-adjusts osmotic pressure
• Adenine – maintains high level of ATP in RBC
• Dextrose
• Mannitol- prevents disintegration of RBC
106

REFERENCES
1) Henry Laboratory Methods 22nd Edition
2) Clinical Laboratory Hematology 3rd Edition- McKenzie/ Williams
3) Dacie and Lewis Practical Hematology
4) Handbook of Medical Laboratory Technology- Robert H Carman
107
108


















