ECG Rhythm Interpretation Rubina Barolia Salima Moez ECG Interpretation.

www.ecgwaves.com | Learn ECG Interpretation Online
ECGWAVES.COM
POCKETGUIDETO
ECGINTERPRETATION
DrArazRawshani,MD,PhD
UniversityofGothenburg
2017
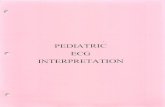
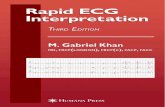
P
P
R
QS
TU
P-wave duration
PR interval
QRS duration
J point
J 60 point
ST segment
TP intervalST-T segment

www.ecgwaves.com | Learn ECG Interpretation Online
MethodologicalECGInterpretationTheECGmustalwaysbeinterpretedsystematically.Failuretoperformasystematicinterpretationof
theECGmaybedetrimental.Theinterpretationalgorithmpresentedbelowiseasytofollowandit
canbecarriedoutbyanyone.ThereaderwillgraduallynoticethatECGinterpretationismarkedly
facilitatedbyusinganalgorithm,asitminimizestheriskofmissingimportantabnormalitiesandalso
speedsuptheinterpretation.
1.Rhythm
ASSESSMENTS EVALUATION
Assessventricular(RRintervals)
andatrial(PPintervals)rateand
rhythm.
♥Isventricularrhythmregular?
Whatistheventricularrate
(beats/min)?
♥Isatrialrhythmregular?What
istheatrialrate(beats/min)?
♥P-wavesshouldprecedeevery
QRScomplexandtheP-wave
shouldbepositiveinleadII.
♥Sinusrhythm(whichisthenormalrhythm)hasthe
followingcharacteristics:(1)heartrate50–100beatsper
minute;(2)P-waveprecedeseveryQRScomplex;(3)theP-
waveispositiveinleadIIand(4)thePRintervalisconstant.
♥Causesofbradycardia:sinusbradycardia,sinoatrialblock,
sinoatrialarrest/inhibition,second-degreeAVblock,third-
degreeAVblock.Notethatescaperhythmsmayariseduring
bradycardia.Alsonotethatbradycardiaduetodysfunctionin
thesinoatrialnodeisreferredtoassinusnodedysfunction
(SND).IfapersonwithECGsignsofSNDissymptomatic,the
conditionisclassifiedassicksinussyndrome(SSS).
♥Causesoftachycardia(tachyarrhythmia)withnarrowQRS
complexes(QRSduration<0,12s):sinustachycardia,
inappropriatesinustachycardia,sinoatrialre-entry
tachycardia,atrialfibrillation,atrialflutter,atrialtachycardia,
multifocalatrialtachycardia,AVNRT,AVRT(pre-excitation,
WPW).Notethatnarrowcomplextachyarrhythmiararely
causescirculatorycompromiseorcollapse.
♥Causesoftachycardia(tachyarrhythmia)withwideQRS
complexes(QRSduration≥0,12s):ventriculartachycardiais
themostcommoncauseanditispotentiallylife-threatening.
Notethat10%ofwidecomplextachycardiasactuallyoriginate
fromtheatriabuttheQRScomplexesbecomewidedueto
abnormalventriculardepolarization(e.gsinustachycardia
withsimultaneousleftbundlebranchblock).
2.P-waveandPRinterval
ASSESSMENTS EVALUATION
♥P-wavealwayspositiveinlead
II(actuallyalwayspositiveinleads
II,IIIandaVF).
♥P-wavedurationshouldbe
<0,12s(allleads).
♥P-wavemustbepositiveinleadII,otherwisetherhythm
cannotbesinusrhythm.
♥P-wavemaybebiphasic(diphasic)inV1(thenegative
deflectionshouldbe<1mm).Itmayhaveaprominent
secondhumpintheinferiorlimbleads(particularlyleadII).

www.ecgwaves.com | Learn ECG Interpretation Online
♥P-waveamplitudeshouldbe
≤2,5mm(allleads).PRinterval
mustbe0,12–0,22s(allleads).
♥Pmitrale:increasedP-waveduration,enhancedsecond
humpinleadIIandenhancednegativedeflectioninV1.
♥Ppulmonale:increasedP-waveamplitudesinleadIIand
V1.
♥IfP-wavenotclearlyvisible:lookforretrograde(inverted)
P-waves,whichcanbelocatedanywherebetweentheJpoint
andtheterminalpartoftheT-wave.
♥PRinterval>0,22s:first-degreeAVblock.
♥PRinterval<0,12s:Pre-excitation(WPWsyndrome).
♥Second-degreeAV-blockMobitztypeI(Wenckebach
block):repeatedcyclesofgraduallyincreasingPRinterval
untilanatrialimpulse(P-wave)isblockedinthe
atrioventricularnodeandtheQRScomplexdoesnotappear.
♥Second-degreeAV-blockMobitztypeII:intermittently
blockedatrialimpulses(noQRSseenafterP)butwith
constantPRinterval.
♥Third-degreeAV-block:Allatrialimpulses(P-waves)are
blockedbytheatrioventricularnode.Anescaperhythm
arises(cardiacarrestensuesotherwise),whichmayhave
narroworwideQRScomplexes,dependingonitsorigin.
ThereisnorelationbetweenP-wavesandtheescape
rhythm'sQRScomplexes,andatrialrhythmistypicallyfaster
thantheescaperhythm(bothrhythmsaretypicallyregular).
3.QRScomplex
ASSESSMENTS EVALUATION
♥QRSdurationmustbe<0,12s
(normally0,07-0,10s).
♥Theremustbeatleastone
limbleadwithR-waveamplitude
>5mmandatleastonechest
(precordial)leadwithR-wave
amplitude>10mm;otherwise
thereislowvoltage.
♥Highvoltageexistsifthe
amplitudesaretoohigh,i.eifthe
followingconditionissatisfied:S-
waveV1orV2+R-waveV5>35
mm.
♥LookforpathologicalQ-waves.
PathologicalQ-wavesare≥0,03s
and/oramplitude≥25%ofR-wave
amplitudeinsamelead,inatleast
2anatomicallycontiguousleads.
♥IstheR-waveprogressionin
thechestleads(V1–V6)normal?
♥WideQRScomplex(QRSduration≥0.12s):Leftbundle
branchblock.Rightbundlebranchblock.Nonspecific
intraventricularconductiondisturbance.Hyperkalemia.Class
Iantiarrhythmicdrugs.Tricyclicantidepressants.Ventricular
rhythmsandventricularextrasystoles(premature
complexes).Artificialpacemakerwhichstimulatesinthe
ventricle.Aberrantconduction(abberancy).Pre-excitation
(Wolff-Parkinson-Whitesyndrome).
♥ShortQRSduration:noclinicalrelevance.
♥Highvoltage:Hypertrophy(anylead).Leftbundlebranch
block(leadsV5,V6,I,aVL).Rightbundlebranchblock(V1–
V3).Normalvariantinyounger,well-trainedandslender
individuals.
♥Lowvoltage:Normalvariant.Misplacedleads.
Cardiomyopathy.Chronicobstructivepulmonarydisease.
Perimyocarditis.Hypothyreosis(typicallyaccompaniedby
bradycardia).Pneumothorax.Extensivemyocardialinfarction.
Obesity.Pericardialeffusion.Pleuraleffusion.Amyloidosis.
♥PathologicalQ-waves:Myocardialinfarction.Left-sided
pneumothorax.Dextrocadia.Perimyocarditis.
Cardiomyopathy.Amyloidosis.Bundlebranchblocks.Anterior

www.ecgwaves.com | Learn ECG Interpretation Online
♥Istheelectricalaxisnormal?
Electricalaxisisassessedinlimb
leadsandshouldbebetween–30°
to90°.
fascicularblock.Pre-excitation.Ventricularhypertrophy.
Acutecorpulmonale.Myxoma.
♥FragmentedQRScomplexesindicatesmyocardialscarring
(mostlyduetoinfarction).
♥AbnormalR-waveprogression:Myocardialinfarction.
Rightventricularhypertrophy(reversedR-waveprogression).
Leftventricularhypertrophy(amplifiedR-waveprogression).
Cardiomyopathy.Chroniccorpulmonale.Leftbundlebranch
block.Pre-excitation.
♥DominantR-waveinV1/V2:Misplacedchestelectrodes.
Normalvariant.Situsinversus.Posterolateral
infarction/ischemia(ifpatientexperienceschestdiscomfort).
Rightventricularhypertrophy.Hypertrophiccardiomyopathy.
Rightbundlebranchblock.Pre-excitation.
♥Rightaxisdeviation:Normalinnewborns.Rightventricular
hypertrophy.Acutecorpulmonale(pulmonaryembolism).
Chroniccorpulmonale(COPD,pulmonaryhypertension,
pulmonaryvalvestenosis).Lateralventricularinfarction.Pre-
excitation.Switchedarmelectrodes(negativePandQRS-Tin
leadI).Situsinversus.Leftposteriorfascicularblockis
diagnosedwhentheaxisisbetween90°and180°withrS
complexinIandaVLaswellasqRcomplexinIIIandaVF
(withQRSduration<0.12seconds),providedthatother
causesofrightaxisdeviationhavebeenexcluded.
♥Leftaxisdeviation:Leftbundlebranchblock.Left
ventricularhypertrophy.Inferiorinfarction.Pre-excitation.
Leftanteriorfascicularblockisdiagnosediftheaxisis
between-45°and90°withqR-complexinaVLandQRS
durationis0,12s,providedthatothercausesofleftaxis
deviationhavebeenexcluded.
♥Extremeaxisdeviation:Rarelyseen.Probablymisplaced
electrodes.IftherhythmiswideQRScomplextachycardia,
thenthecauseisprobablyventriculartachycardia.
4.STsegment
ASSESSMENTS EVALUATION
♥TheST-segmentshouldbeflat
andisoelectric(inlevelwiththe
baseline).Itmaybeslightly
upslopingatthetransitionwith
theT-wave.
• ♥STsegmentdeviation
(elevationanddepression)
ismeasuredintheJpoint.
♥BenignSTsegmentelevationisverycommoninthe
population,particularlyintheprecordialleads(V2–V6).Upto
90%(insomeage-ranges)ofhealthymenandwomendisplay
concaveST-segmentelevationsinV2–V6(thisiscalled
male/femalepattern).ST-segmentelevationswhicharenot
benignnorduetoischemiaarerathercommon(listed
below).
• ♥ST-segmentdepressionisuncommonamonghealthy
individuals.ST-segmentdepressionisparticularlysuspicious
inthechestleads.Guidelinesrecommendthat<0.5mmST-
segmentdepressionbeacceptedinallleads.

www.ecgwaves.com | Learn ECG Interpretation Online
• ♥CausesofST-segmentelevation:Ischemia.STsegment
elevationmyocardialinfarction(STEMI/STE-AKS).Prinzmetal's
angina(coronaryvasospasm).Male/femalepattern.Early
repolarization.Perimyocarditis.Leftbundlebranchblock.
Nonspecificintraventricularconductiondisturbance.Left
ventricularhypertrophy.Brugadasyndrome.Takotsubo
cardiomyopathy.Hyperkalemia.Postcardioversion.
Pulmonaryembolism.Pre-excitation.Aorticdissection
engagingthecoronaryarteries.Leftventricularaneurysm.
• ♥CausesofST-segmentdepression:Ischemia.Non-ST
segmentelevationmyocadialinfarction(NSTEMI/NSTE-AKS).
PhysiologicalST-segmentdepression.Hyperventilation.
Hypokalemia.Highsympathethictone.Digoxin.Leftbundle
branchblock.Rightbundlebranchblock.Pre-excitation.Left
ventricularhypertrophy.Rightventricularhypertrophy.Heart
failure.Tachycardia.
• ♥Causesofwaves/deflectionsintheJpoint(Jwave
syndromes):Brugadasyndrome.Earlyrepolarization.
5.T-wave
ASSESSMENTS EVALUATION
• ♥ShouldbeconcordantwiththeQRScomplex.Shouldbepositive
inmostleads.
• ♥T-waveprogressionshouldbe
normalinchestleads.
• ♥Inlimbleadstheamplitudeis
highestinleadII,andinthechest
leadstheamplitudeishighestin
V2–V3.
♥Normalvariants:Anisolated(single)T-waveinversionis
acceptedinleadV1andleadIII.InsomeinstancestheT-wave
inversionsfromchildhoodmaypersistinV1–V3(V4),whichis
calledpersistentjuvenileT-wavepattern.Rarely,allT-waves
remaininverted,whichiscalledglobalidiopathicT-wave
inversion(V1–V6).
• ♥T-waveinversionwithoutsimultaneousST-segment
deviation:Thisisnotasignofongoingischemia,butmaybe
post-ischemic.Onetypeofpost-ischemicT-waveinversionis
especiallyacute,namelyWellen'ssyndrome(characterizedby
deepT-waveinversionsinV1–V6inpatientwithrecent
episodesofchestpain).Cerebrovascularinsult(bleeding).
Pulmonaryembolism.Perimyocarditis(afternormalizationof
theST-segmentelevation,T-wavesbecomeinvertedin
perimyocarditis).Cardiomyopathy.
• ♥T-waveinversionwithsimultaneousST-segment
deviation:acute(ongoing)myocardialischaemia.
• ♥HighT-waves:Normalvariant.Earlyrepolarization.
Hyperkalemia.Leftventricularhypertrophy.Leftbundle
branchblock.Occasionallyperimyocarditis.High(hyperacute)
T-wavesmaybeseenintheveryearlyphaseofSTEMI.

www.ecgwaves.com | Learn ECG Interpretation Online
6.QTcintervalandU-wave
ASSESSMENTS EVALUATION
♥QTcdurationmen≤0,45s.
♥QTcdurationwomen≤0,46s.
♥ProlongedQTcdurationmay
causemalignantarrhythmias
(torsadedepointes,whichisa
typeofventriculartachycardia).
♥ShortenedQTcduration(≤0.32
s)israre,butmayalsocause
malignantventricular
arrhythmias.
♥TheU-waveisseen
occasionally,especiallyinwell-
trainedindividuals,andduring
lowheartrate.ItislargestinV3–
V4.AmplitudeisonefourthofT-
waveamplitude.
♥AcquiredQTprolongation:antiarrhythmicdrugs
(procainamide,disopyramide,amiodarone,sotalol),
psychiatricmedications(tricyclicantidepressants,SSRI,
lithiumetc);antibiotics(macrolides,kinolones,atovaquone,
klorokine,amantadin,foscarnet,atazanavir);hypokalemia,
hypocalcemia,hypomagnesemia;cerebrovascularinsult
(bleeding);myocardialischemia;cardiomyopathy;
bradycardia;hypothyroidism;hypothermia.Acompletelistof
drugscausingQTprolongationcanbefoundhere.
• ♥CongenitalQTprolongation:geneticdiseaseofwhich
thereareapproximately15variants.
• ♥ShortQTcsyndrome(≤0,32s):causedbyhyperkalcemia
anddigoxintreatment.Maycausemalignantventricular
arrhythmia.
• ♥NegativeU-wave:highspecificityforheartdisease
(includingischemia).
•
7.ComparewithearlierECGtracings
ItisfundamentaltocomparethecurrentECGwithpreviousrecordings.Allchangesareofinterest
andmayindicatepathology.
8.ClinicalcontextECGchangesshouldbeputintoaclinicalcontext.Forexample,ST-segmentelevationsarecommon
inthepopulationandshouldnotraisesuspicionofmyocardialischemiaifthepatientdonothave
symptomssuggestiveofischemia.
Theguidecontinuesonthenextpage.

www.ecgwaves.com | Learn ECG Interpretation Online
Thecardiacconductionsystem
Waves,intervalsanddurationsontheECG

www.ecgwaves.com | Learn ECG Interpretation Online
Thewallsoftheleftventricleandtheleadsthatview
thesewalls
TheECGleads

www.ecgwaves.com | Learn ECG Interpretation Online
P-wavechanges

www.ecgwaves.com | Learn ECG Interpretation Online
STsegmentdepressions

www.ecgwaves.com | Learn ECG Interpretation Online
STsegmentelevations

www.ecgwaves.com | Learn ECG Interpretation Online
T-wavechanges

www.ecgwaves.com | Learn ECG Interpretation Online
Electricalaxisoftheheart
Asevidentfromthefigureabove,thenormalheartaxisisbetween–30°and90°.Iftheaxisismore
positivethan90°itisreferredtoasrightaxisdeviation.Iftheaxisismorenegativethan–30°itis
referredtoasleftaxisdeviation.Theaxisiscalculated(tothenearestdegree)bytheECGmachine.
TheaxiscanalsobeapproximatedmanuallybyjudgingthenetdirectionoftheQRScomplexinleads
IandII.Thefollowingrulesapply:
• Normalaxis:NetpositiveQRScomplexinleadsIandII.
• Rightaxisdeviation:NetnegativeQRScomplexinleadIbutpositiveinleadII.
• Leftaxisdeviation:NetpositiveQRScomplexinleadIbutnegativeinleadII.
• Extremeaxisdeviation(–90°to180°):NetnegativeQRScomplexinleadsIandII.

www.ecgwaves.com | Learn ECG Interpretation Online
Pro-arrhythmicECGchangesduringsinusrhythm

www.ecgwaves.com | Learn ECG Interpretation Online
AssessmentofRPintervalfortachyarrhythmias

www.ecgwaves.com | Learn ECG Interpretation Online
Diagnosisandmanagementoftachyarrhythmiaswith
narrowQRScomplex

www.ecgwaves.com | Learn ECG Interpretation Online
Diagnosisandmanagementoftachyarrhythmiaswith
wideQRScomplex

www.ecgwaves.com | Learn ECG Interpretation Online
Intraventricularconductiondefects

www.ecgwaves.com | Learn ECG Interpretation Online
Hypertrophyanddilatation

www.ecgwaves.com | Learn ECG Interpretation Online
Classificationofacutecoronarysyndromes(ACS)

www.ecgwaves.com | Learn ECG Interpretation Online
Criteriaforacutemyocardialinfarction(AMI)
STE-ACS(STEMI)–STelevationacutemyocardialinfarction
CriteriaforSTEMINewSTsegmentelevationsinatleasttwoanatomicallycontiguousleads:
• Menage≥40years:≥2mminV2-V3and≥1mminallotherleads.
• Menage<40years:≥2,5mminV2-V3and≥1mminallotherleads.
• Women(anyage):≥1,5mminV2-V3and≥1mminallotherleads.
• Men&womenV4RandV3R:≥0,5mm,exceptfrommen<30yearsinwhomthecriteriais≥1mm.
• Men&womenV7-V9:≥0,5mm.
NSTE-ACS(NSTE-ACS)–NonSTelevationacutemyocardial
infarction:NSTEMIandunstableangina
• NewhorizontalordownslopingSTsegmentdepressions≥0,5mminatleasttwoanatomically
contiguousleads.
• Twaveinversion≥1mminatleasttwoanatomicallycontiguousleads.Theseleadsmusthave
evidentR-waves,orR-waveslargerthanS-waves.