Metastatic Breast Cancer and Emerging Research Kathryn J. Ruddy, MD MPH Assistant Professor of...
42
Metastatic Breast Cancer and Emerging Research Kathryn J. Ruddy, MD MPH Assistant Professor of Oncology Mayo Clinic
-
Upload
allan-warner -
Category
Documents
-
view
217 -
download
0
Transcript of Metastatic Breast Cancer and Emerging Research Kathryn J. Ruddy, MD MPH Assistant Professor of...
Metastatic Breast Cancer and Emerging Research
Kathryn J. Ruddy, MD MPHAssistant Professor of Oncology
Mayo Clinic

Overview
• What is metastatic disease?• Breast cancer subtypes
– Treatment of Her2+ disease– Treatment of ER+ disease– Treatment of ER-/Her2- disease
• Exciting new research directions

Metastatic breast cancer
• Stage IV disease– Has spread from the breast and axillary lymph
nodes to other organs
• Accounts for 5-10% of all breast cancer at the time of diagnosis
• Stage IV breast cancer is usually incurable, but can often be controlled for years utilizing sequential drug therapy
Treatment for metastatic disease
• Treated primarily with systemic therapy, but sometimes with palliative radiation also; surgery is rarely utilized
• After the disease develops resistance to one drug, a patient is switched to a new drug
• Aims of therapy are to:– Prolong time to progression– Prolong survival– Palliate
• Reduce tumor burden• Minimize treatment toxicity
• Disease subtype is critical to treatment decision-making
• There are three main subtypes of breast cancer
• Oncologists use breast cancer subtype to guide treatment decisions
• Clinical trials often focus on specific subtypes
Breast cancer subtypes

Subtypes
TALK to your doctor if you are not sure what type of breast cancer you have
Slide courtesy of Nancy Lin

Hormone receptorpositive
Triple-negative
HER2-Positive
*Note, these are just examples. Each patient is different and treatment is tailored accordingly.
Slide courtesy of Nancy Lin
Treatment
HER2+ disease: a paradigm for advances in
targeted therapy

HER2+ disease: major advances
• HER2 is an important target; anti-HER2 drugs can be effective with chemo, with endocrine therapy, or alone
• Meaningful progress has been made with novel therapies that are well tolerated
• Resistance is a major challenge but new technologies are allowing this to be overcome
1998
TrastuzumabApproved
2002
First PreoperativeTrials Reported Paving
The Way For Use inEarly Stage Disease
2005
Three LargeAdjuvant Trials
Reported
2005
LapatinibApproved
2007-2008
Initial Trialsof T-DM1,Neratinib
2010
PreoperativeTrials of
Dual Blockade
PertuzumabApproved
2012
2013
T-DM1Approved
Slide courtesy of Ian Krop

Trastuzumab in HER2+ metastatic breast cancer
Graphic adapted from image at http://www.gene.com/gene/research/focusareas/oncology/herpathwayexpertise.jsp
Protein Receptor
HER2 Gene
Normal Cell
HER2+ Cell
Slamon et al, NEJM 2001
Can combine with many different chemotherapies (e.g., paclitaxel, docetaxel, vinorelbine, capecitabine) and
targeted agents (e.g., lapatinib)
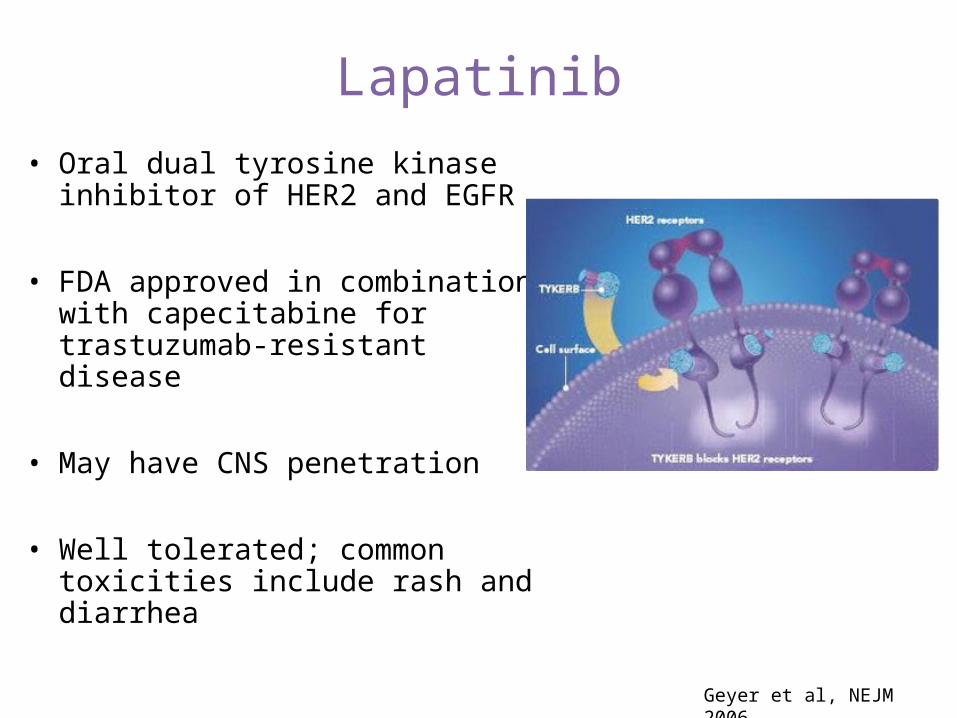
Lapatinib
• Oral dual tyrosine kinase inhibitor of HER2 and EGFR
• FDA approved in combination with capecitabine for trastuzumab-resistant disease
• May have CNS penetration
• Well tolerated; common toxicities include rash and diarrhea
Geyer et al, NEJM 2006
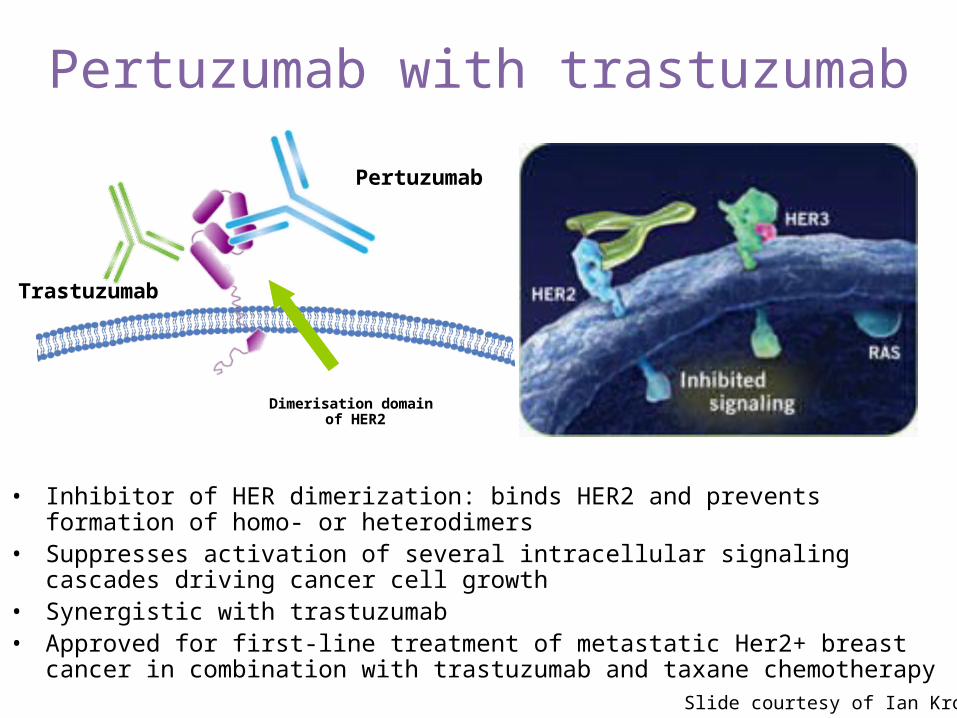
Pertuzumab with trastuzumabHER2 receptor
Trastuzumab
Pertuzumab
Dimerisation domain of HER2
• Inhibitor of HER dimerization: binds HER2 and prevents formation of homo- or heterodimers
• Suppresses activation of several intracellular signaling cascades driving cancer cell growth
• Synergistic with trastuzumab• Approved for first-line treatment of metastatic Her2+ breast cancer in combination
with trastuzumab and taxane chemotherapy Slide courtesy of Ian Krop

CLEOPATRA: phase 3 study of pertuzumab in untreated metastatic disease
1:1 HER2-positiveMBC
Docetaxel + trastuzumab + placebo
Docetaxel + trastuzumab + pertuzumab
N=808
Pertuzumab prolongs time until progression by six months (from 12.5 to 18.5 months)
Baselga et al, SABCS 2011 and NEJM, 2011

Adverse event, n (%)
Placebo+ trastuzumab + docetaxel
(n = 397)
Pertuzumab+ trastuzumab + docetaxel
(n = 407)
Diarrhea 184 (46.3) 272 (66.8)
Alopecia 240 (60.5) 248 (60.9)
Neutropenia 197 (49.6) 215 (52.8)
Nausea 165 (41.6) 172 (42.3)
Fatigue 146 (36.8) 153 (37.6)
Rash 96 (24.2) 137 (33.7)
Decreased appetite 105 (26.4) 119 (29.2)
Mucosal inflammation 79 (19.9) 113 (27.8)
Asthenia 120 (30.2) 106 (26.0)
Peripheral edema 119 (30.0) 94 (23.1)
Constipation 99 (24.9) 61 (15.0)
Febrile neutropenia* 30 (7.6) 56 (13.8)
Dry skin 17 (4.3) 43 (10.6)
Toxicities
Baselga et al, SABCS 2011 and NEJM, 2011
*Febrile neutropenia rate 12% vs 26% in Asia, 10% or less in all other regions--No difference in cardiac toxicity rate (2% v 1%)*Febrile neutropenia rate 12% vs 26% in Asia, 10% or less in all other regions--No difference in cardiac toxicity rate (2% v 1%)
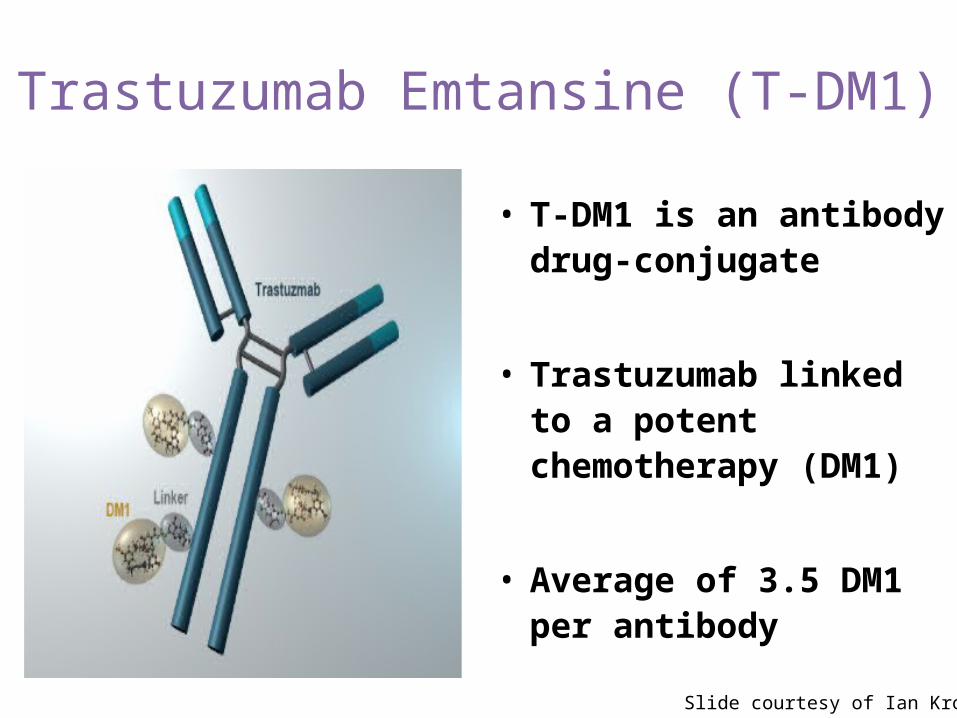
Trastuzumab Emtansine (T-DM1)
• T-DM1 is an antibody drug-conjugate
• Trastuzumab linked to a potent chemotherapy (DM1)
• Average of 3.5 DM1 per antibody
Slide courtesy of Ian Krop
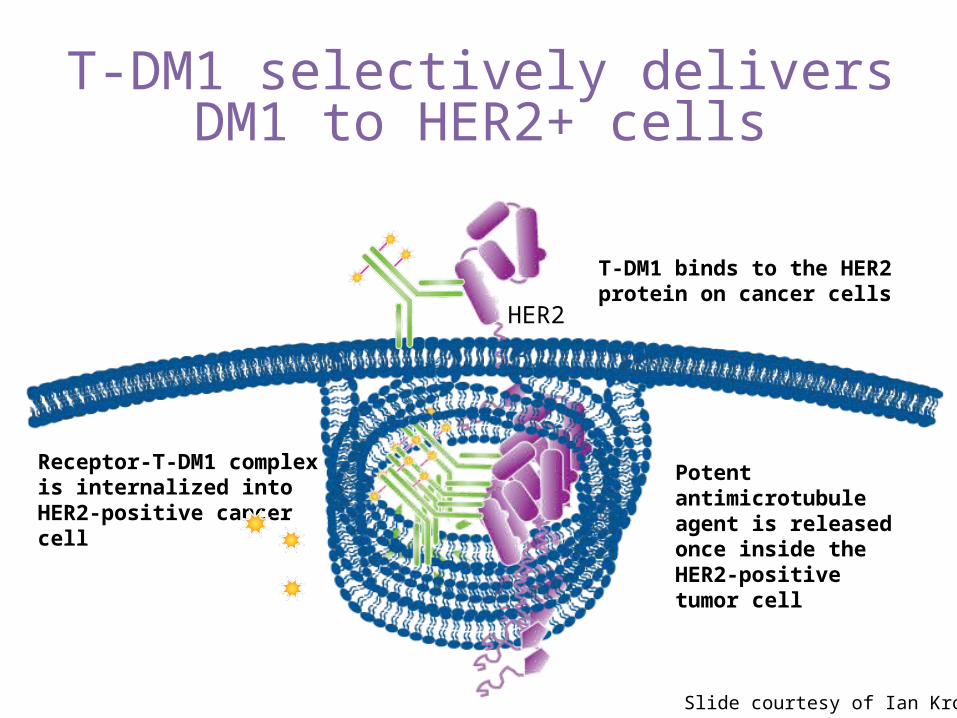
T-DM1 selectively delivers DM1 to HER2+ cells
Receptor-T-DM1 complex is internalized into HER2-positive cancer cell
Potent antimicrotubule agent is released once inside the HER2-positivetumor cell
T-DM1 binds to the HER2 protein on cancer cells
HER2
Slide courtesy of Ian Krop
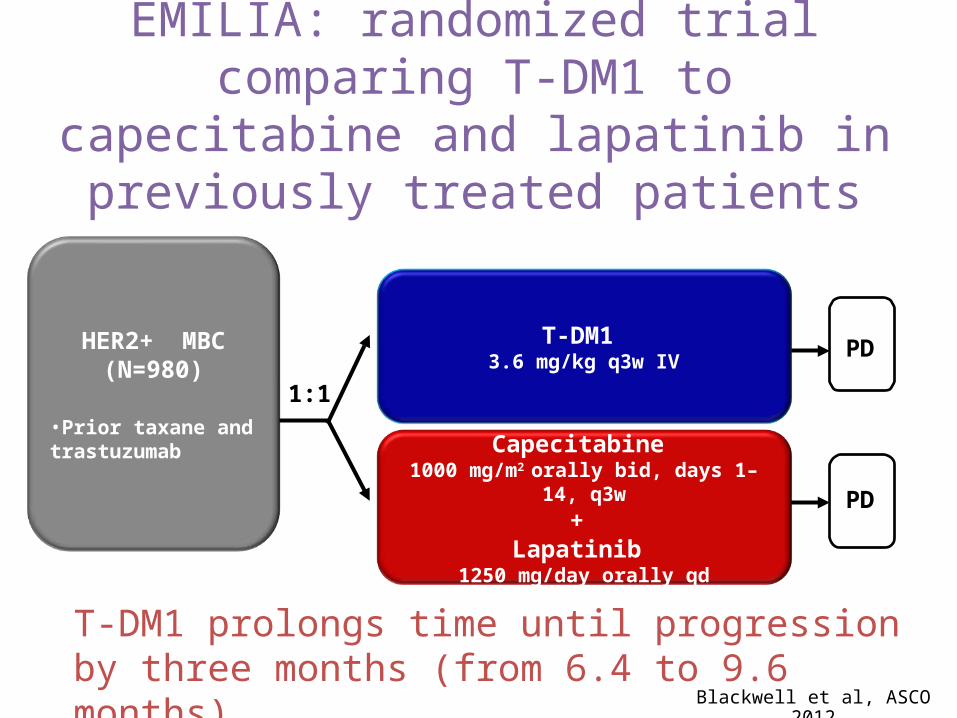
EMILIA: randomized trial comparing T-DM1 to capecitabine and lapatinib
in previously treated patients
1:1
HER2+ MBC (N=980)
•Prior taxane and trastuzumab
PDT-DM1 3.6 mg/kg q3w IV
Capecitabine 1000 mg/m2 orally bid, days 1–14, q3w
+ Lapatinib
1250 mg/day orally qd
PD
Blackwell et al, ASCO 2012
T-DM1 prolongs time until progression by three months (from 6.4 to 9.6 months)

Th3RESA: randomized trial comparing T-DM1 to physician’s choice
Study treatment continues until
disease progression or unmanageable
toxicity
HER2 positive
Metastatic breast cancer
Prior trastuzumab, lapatinib and
chemotherapy
T-DM1 q3w
Treatment of physician’s choice
N = 7952:1 randomization
2
1
Wildiers et al, ECC-ESMO 2013
T-DM1 prolongs time until progression by three months (from 3.3 to 6.2 months)
T-DM1 is well-tolerated
• Common side effects:– Decreased platelet count– Elevated liver tests
• Does not cause typical chemotherapy side effects
• No hair loss• Significant nausea or diarrhea are not common• Does not cause immune suppression or significant
neuropathy
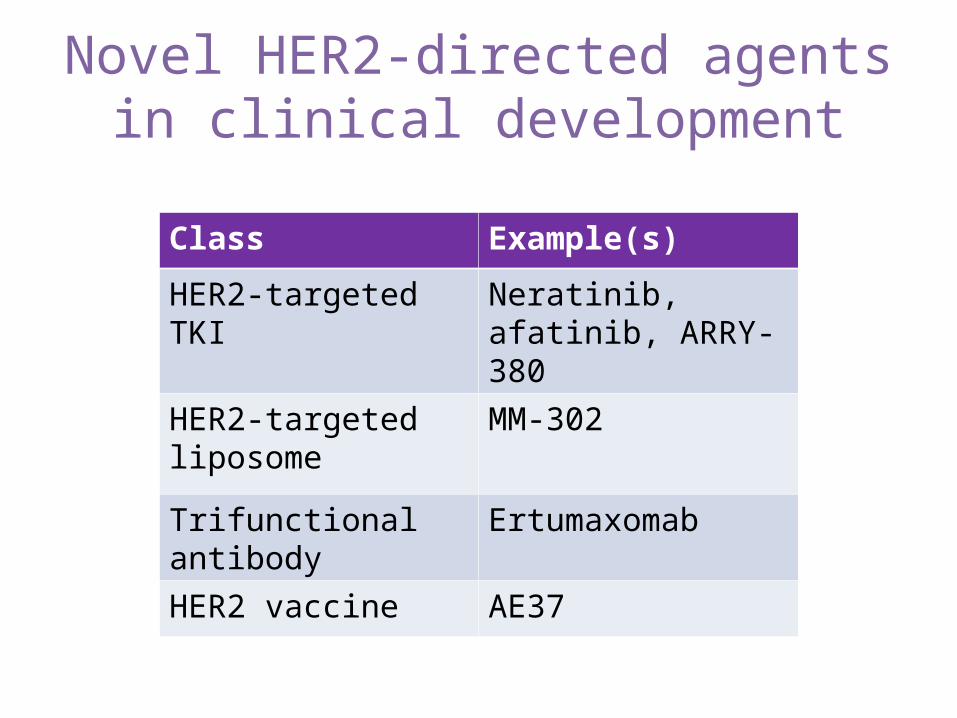
Novel HER2-directed agents in clinical development
Class Example(s)
HER2-targeted TKI Neratinib, afatinib, ARRY-380
HER2-targeted liposome
MM-302
Trifunctional antibody Ertumaxomab
HER2 vaccine AE37

ER+ disease: improving on already very effective
treatments
Endocrine therapy for metastatic disease
• Premenopausal– Tamoxifen– Ovarian
suppression/ablation– Ovarian suppression +
aromatase inhibition– Megace
• Postmenopausal– Tamoxifen– Aromatase Inhibitor +/-
everolimus– Fulvestrant– Megace
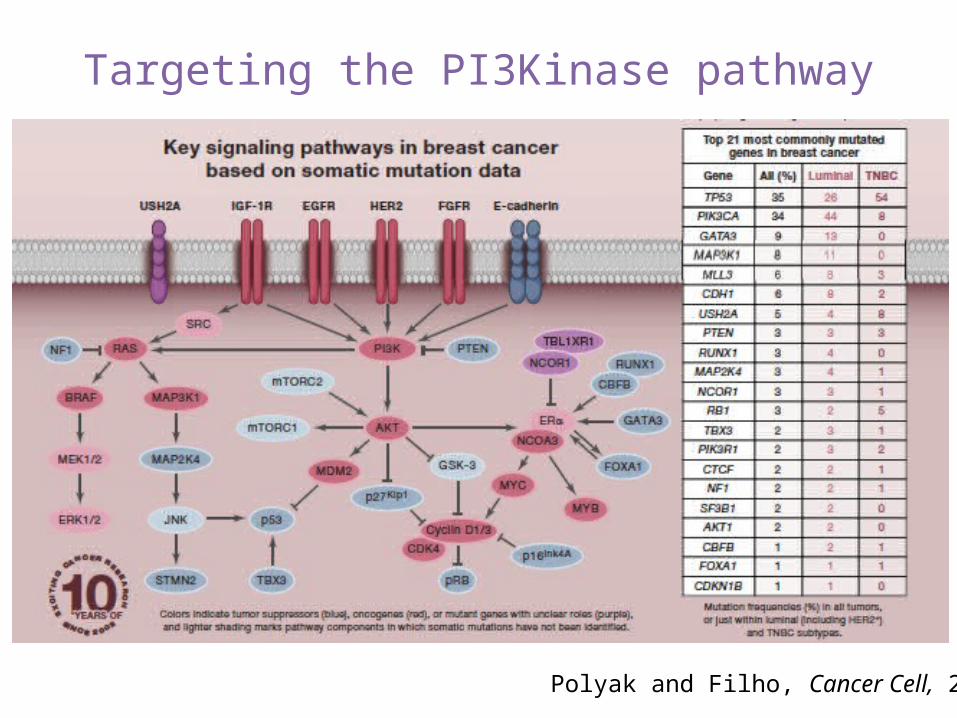
Polyak and Filho, Cancer Cell, 2012
Targeting the PI3Kinase pathway
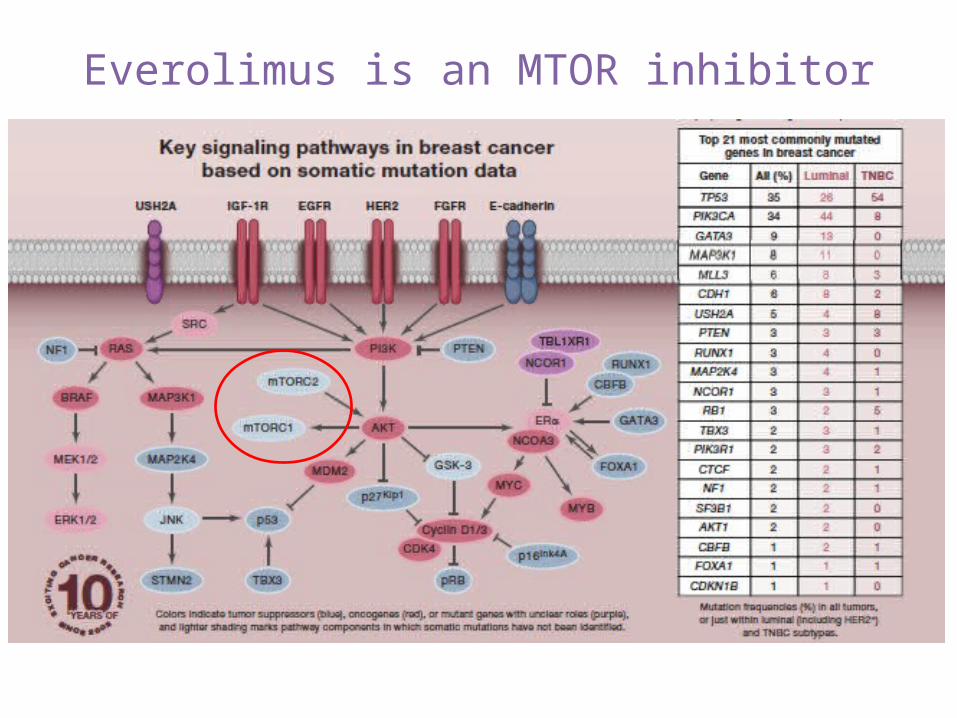
Everolimus is an MTOR inhibitor

New drug approval: everolimus
Approved by the FDA in 2012 for patients with metastatic, hormone-receptor positive, HER2-negative breast cancer
*Median time from study entry until worsening of cancer
Slide courtesy of Nancy Lin
What’s next for everolimus?
• Multiple studies underway– In HER2+ cancers– In triple negative cancers– Studying this drug in combination with other
therapies

Testing the addition of an HSP90 inhibitor to hormonal therapy
Slide courtesy of Nancy Lin

Testing the addition of an HSP90 inhibitor to hormonal therapy
Ganetespib induces regression in tumors progressing on fulvestrant
Days of treatment
Tum
or v
olum
e (m
m3 )
Slide courtesy of Nancy Lin
Other agents of interest in ER+ disease
• Endoxifen • CDK 4/6 inhibitors• PI3Kinase inhibitors• Anti-IGF-1R Ab• SRC/Abl tyrosine kinase inhibitors• Combination therapy with targeted agents
that may overcome endocrine resistance

Triple negative breast cancer:
still searching for a target
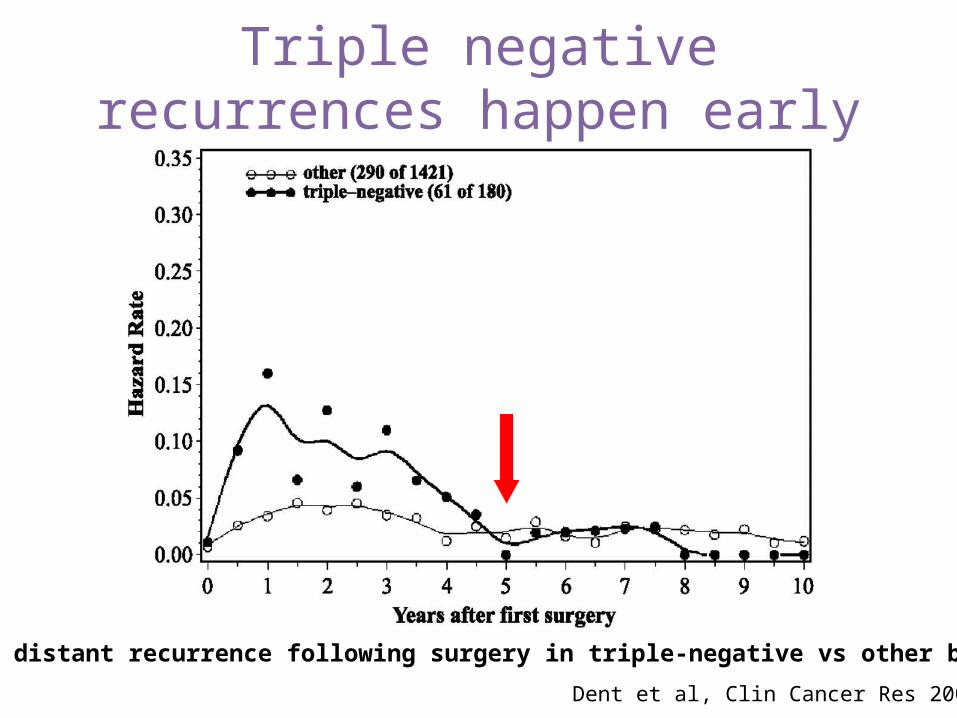
Triple negative recurrences happen early
Dent et al, Clin Cancer Res 2007
Rates of distant recurrence following surgery in triple-negative vs other breast ca
There are many chemotherapies that are active against metastatic disease
• Mitotic inhibitors– vinorelbine– paclitaxel– docetaxel
• Antifolates– methotrexate
• Topoisomerase inhibitors– doxorubicin

Platinums
• Sledge (JCO 1988) reported 47% response rate in first line metastatic disease
• Abandoned for many years because of concerns about toxicity—largely replaced by taxanes
• Recent interest in patients with triple negative breast cancer
– DNA crosslinking mechanism of action
• New data from a series of neoadjuvant studies supports activity in TNBC
Sledge et al, JCO 2008; Silver et al JCO 2010; Gronwold et al, ASCO 2009; Sikov SABCS 2013
New chemotherapy: eribulin
Approved by the FDA in 2011
Halichondria okadai•Metastatic breast cancer•At least 2 prior chemotherapies
PARP inhibitors
• PARP1 is a protein that is important for repairing single-strand DNA breaks
• PARP inhibitors prevent DNA repair, leading to cell death
• Fast-dividing tumors and tumors containing BRCA mutations, which also impair DNA repair, may be most sensitive to PARP inhibitors
• Ongoing trials are investigating the efficacy of PARP inhibitors in breast cancer, particularly triple negative breast cancer and BRCA-associated breast cancer
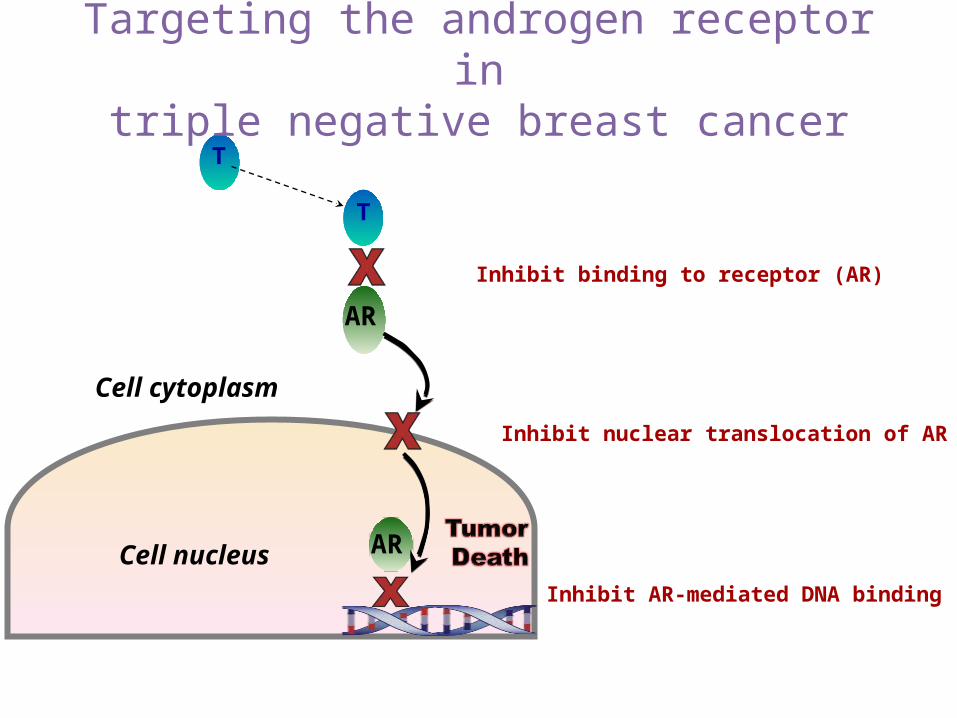
Inhibit binding to receptor (AR)
T
AR
T
Cell nucleus AR
Cell cytoplasm
Inhibit nuclear translocation of AR
Inhibit AR-mediated DNA binding
Targeting the androgen receptor intriple negative breast cancer
Other agents of interest in triple negative disease
• PI3Kinase inhibitors• SRC/Abl tyrosine kinase inhibitors• HSP90 inhibitors• More to come…

What does all this complexity mean?
•There is likely not going to be a single “cure for cancer”
•Different cancers may have different strengths & weaknesses
•Figuring this out won’t be easy!
“half empty”
Slide courtesy of Erica Mayer
What does all this complexity mean?
•There is likely not going to be a single “cure for cancer”
•Different cancers may have different strengths & weaknesses
•Figuring this out won’t be easy!
“half full”
•The opportunity to individualize therapy—one size doesn’t fit all
•We may be able take advantage of specific weaknesses of cancers and knock out specific strengths
•But should be possible!
Slide courtesy of Erica Mayer

1. How many subtypes of breast cancer are there, and by understanding this, can we find new targets and new treatments? Can we better “tailor” treatments?
2. What causes resistance to hormonal therapy? To chemotherapy? Can it be prevented or overcome?
3. What lifestyle factors (e.g., exercise?) might be important for patients with metastatic disease?
4. How can we minimize toxicities of treatment?
Outstanding research questions

Summary
• Not all breast cancers are alike
• We have many clues to guide therapy
• But we need clinical trials and continued basic and translational research to make new breakthroughs that make a difference for patients
Thank you!