Metal Exposure after Hip Replacement and the Risks … · Metal Exposure after Hip Replacement and...
3
Volume 03 / Issue 02 / June 2015 boa.ac.uk Page 42 JTO Peer-Reviewed Articles Metal Exposure after Hip Replacement and the Risks of Systemic Toxicity J. Mark Wilkinson Can exposure to high circulating metal concentrations cause systemic illness? A failing MOMHR prosthesis is associated with circulating cobalt and chromium concentrations that may be several times higher than those seen in patients with well-functioning prostheses 9 . Case reports of patients with failed prostheses also suggest that very high blood metal concentrations are associated with systemic effects including cardiac, neurological, and endocrine dysfunction 10-14 . A recent systematic review of the relationship between metal exposure and features of systemic toxicity was conducted by Bradberry, Wilkinson, and Ferner 15 . In this review we searched Medline and Embase between 1980 and 28th February 2014 for published cases of possible cobalt or chromium toxicity associated with hip prostheses. Although there were 23 reports describing original case data, a total of only 18 individual patient cases were described within the reports. In 10 of these cases the patient had undergone revision of a fractured ceramic-containing bearing to a cobalt-chrome containing bearing and the source of the elevated systemic cobalt concentrations was ascribed to accelerated wear of the revision metal- containing bearing due to ceramic 3rd body wear (Figure 2). The other eight patients had received a primary MOM prosthesis. Three main categories of systemic toxicity were identified, including neuro-ocular toxicity (14 patients), cardiotoxicity (11 patients), and thyrotoxicity (9 patients). The median blood cobalt concentration in these cases was 398µg/L (range 13.6 to 6521), and was substantially higher in the failed ceramic bearing group than in the primary MOM prosthesis group. Removal of the prosthesis in these cases was usually associated with a fall in systemic cobalt concentrations and an improvement in clinical symptoms. Prof. J. Mark Wilkinson Large diameter metal on metal bearings in total hip arthroplasty and hip resurfacing (MOMHR) have been inserted in large numbers both in the United Kingdom and worldwide in recent years (Figure 1). However, because of high prosthesis failure rates the use of these devices has undergone a dramatic decline since its peak at 31% of cases reported to the NJR in 2007 to 1% of cases in 2013. More recently, dual modular necked femoral prostheses have also been implicated in early prosthesis failure 1 . Potential adverse systemic effects of metal release from failing prostheses remain a concern 2 , and our knowledge to date in this area is reviewed here together with the prospects for future understanding in this area 3,4 . Background Cobalt and chromium are the principal metals released by MOM prostheses 5 . Both metals are essential trace elements in man, with physiological circulating concentrations of between 0.1 and 0.2µg/L. Blood levels of cobalt and chromium rise after MOMHR 5,6 , with late steady state median blood concentrations of between 1.5 and 2.3µg/L in patients with well- functioning prostheses 7,8 . The majority of MOMHR prostheses have been inserted in younger, more active patients, and the majority of these prostheses are functioning well. The median life-expectancy of prostheses in this age group equates to a duration of exposure to cobalt and chromium that is in excess of 20 years. Figure 1: Plain pelvic radiograph showing a patient with a metal-on- metal hip resurfacing
Transcript of Metal Exposure after Hip Replacement and the Risks … · Metal Exposure after Hip Replacement and...

Volume 03 / Issue 02 / June 2015 boa.ac.uk Page 42
JTO Peer-Reviewed Articles
Metal Exposure after Hip Replacement and the Risks of Systemic Toxicity
J. Mark Wilkinson
Can exposure to high circulating metal concentrations cause systemic illness? A failing MOMHR prosthesis is associated with circulating cobalt and chromium concentrations that may be several times higher than those seen in patients with well-functioning prostheses9. Case reports of patients with failed prostheses also suggest that very high blood metal concentrations are associated with systemic effects including cardiac, neurological, and endocrine dysfunction10-14.
A recent systematic review of the relationship between metal exposure and features of systemic toxicity was conducted by Bradberry, Wilkinson, and Ferner15. In this review we searched Medline and Embase between 1980 and 28th
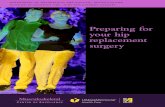
February 2014 for published cases of possible cobalt or chromium toxicity associated with hip prostheses. Although there were 23 reports describing original case data, a total of only 18 individual patient cases were described within the reports. In 10 of these cases the patient had undergone revision of a fractured ceramic-containing bearing to a cobalt-chrome containing bearing and the source of the elevated systemic cobalt concentrations was ascribed to accelerated wear of the revision metal-containing bearing due to ceramic 3rd body wear (Figure 2). The other eight patients had received a primary MOM prosthesis. Three main categories of systemic toxicity were identified, including neuro-ocular toxicity (14 patients), cardiotoxicity (11 patients), and thyrotoxicity (9 patients). The median blood cobalt concentration in these cases was 398µg/L (range 13.6 to 6521), and was substantially higher in the failed ceramic bearing group than in the primary MOM prosthesis group. Removal of the prosthesis in these cases was usually associated with a fall in systemic cobalt concentrations and an improvement in clinical symptoms.
Prof. J. Mark Wilkinson
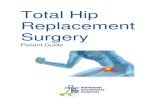
Large diameter metal on metal bearings in total hip arthroplasty and hip resurfacing (MOMHR) have been inserted in large numbers both in the United Kingdom and worldwide in recent years (Figure 1). However, because of high prosthesis failure rates the use of these devices has undergone a dramatic decline since its peak at 31% of cases reported to the NJR in 2007 to 1% of cases in 2013. More recently, dual modular necked femoral prostheses have also been implicated in early prosthesis failure1. Potential adverse systemic effects of metal release from failing prostheses remain a concern2, and our knowledge to date in this area is reviewed here together with the prospects for future understanding in this area3,4.
BackgroundCobalt and chromium are the principal metals released by MOM prostheses5. Both metals are essential trace elements in man, with physiological circulating concentrations of between 0.1 and 0.2µg/L. Blood levels of cobalt and chromium rise after MOMHR5,6, with late steady state median blood concentrations of between 1.5 and 2.3µg/L in patients with well-functioning prostheses7,8. The majority of MOMHR prostheses have been inserted in younger, more active patients, and the majority of these prostheses are functioning well. The median life-expectancy of prostheses in this age group equates to a duration of exposure to cobalt and chromium that is in excess of 20 years.
Figure 1: Plain pelvic radiograph showing a patient with a metal-on-metal hip resurfacing

Volume 03 / Issue 02 / June 2015 boa.ac.uk Page 43
functioning MOM prostheses remains unclear. Chronic industrial and accidental over-exposure to cobalt or chromium associates with solid organ damage including the heart, liver, kidneys, pituitary and thyroid glands, and thus there is a theoretical case for association after MOMHR. The United States Government Centers for Disease Control and Prevention regulations and advisories for cobalt recommends a threshold limit value of atmospheric cobalt of 0.02µg/m3 for exposed cobalt workers www.cdc.gov/niosh/topics/cobalt. Biological monitoring for this level of exposure equates to a biological exposure index at the end of shift at the end of the work week of 1µg/L in blood and 15µg/L in urine. Linna et al16, found cobalt workers exposed to a blood cobalt level of 2.5µg/L over nine years had echocardiographic evidence of altered left ventricular function versus unexposed controls. These studies suggest that blood metal concentrations below the MHRA investigation threshold of 7µg/L have potential for association with adverse systemic effects.
We undertook a detailed cross-sectional health screen at a mean of eight years after surgery in 35 clinically asymptomatic patients who had previously received a MOM hip resurfacing (MOMHR) versus 35 individually age and sex matched asymptomatic patients who had received a conventional hip replacement (THA)17. All subjects underwent a detailed battery of investigations, including clinical history and examination, and assessments of cardiac, neurological, neuropsychological, endocrine, renal, hepatobiliary, and bone density and turnover. Cardiac ejection fraction was 7% lower (P=0.04) and left ventricular end-diastolic diameter was 6% larger (P=0.007) in the MOMHR versus the THA group. Total body bone mineral density was 5% higher (P=0.02) and bone turnover was 14% lower (P=0.006) in the MOMHR versus conventional THA group. Diuretic prescription was
associated with a 40% increase in the fractional excretion of chromium (mean difference 0.5%, P=0.03). In follow up studies in these patient groups we found that the MOM exposure patients had lower grey matter density in the occipital cortex and basal ganglia of the brain measured by MRI than the patients who received a conventional THA, but no other structural differences in the brain18. However, we found no evidence of clinical deficits in visual or auditory function in asymptomatic MOM patients versus the THA controls19.
SummaryExposure to very high circulating concentrations of cobalt associates with cardiac, neurological, and thyroid disease. We found in the majority of these cases the associating problem is accelerated wear of a cobalt-containing revision bearing used to replace a fractured ceramic bearing. The case for an adverse effect of chronic exposure to low circulating metal concentrations remains less clear. Our findings of differences in bone and cardiac function between patients groups suggest that chronic exposure to low elevated metal concentrations in patients with well-functioning MOMHR prostheses may have systemic effects. Long-term epidemiological studies that link registry data with other clinical datasets may provide sufficient power to definitively establish whether such associations are clinically relevant.
Clinical toxicological assessment of systemic features in patients with metal-containing hip prosthesesProposed assessment criteria for cobalt-related disease:1. History: A MOM or a fractured ceramic-containing prosthesis
has been replaced by a metal component; local symptoms of pain are present; the patient’s symptoms are consistent with known cardiac, neurological, or thyroid effects of cobalt, and for which any other explanation is less likely.2. Clinical and investigation findings: There are objective signs consistent with known cardiac, neurological, or thyroid effects of cobalt, for which any other explanation is less likely. Local abnormalities (damaged prosthesis, metallosis) on radiology or at surgery are present.3. Timing: Clinical features develop months to years after factors increasing blood cobalt concentrations.4. Cobalt concentration: Measured cobalt concentrations are substantially higher than those in patients with well-functioning prostheses.5. Response to removal of the prosthesis: Blood cobalt concentration falls after removal of the prosthesis, and the fall is usually accompanied by clinical improvement.
Mark Wilkinson is an arthroplasty surgeon with a special interest in the interactions between patients and their prostheses. His work includes studying the effects of metal exposure on bone, the heart, and other solid organs, and the risk factors for prosthesis failure.
Correspondence
Email: [email protected]
References
References can be found online at www.boa.ac.uk/publications/JTO or by scanning the QR Code.
Figure 2: Radiograph showing a fractured ceramic head after THA. The head and liner were subsequently exchanged to a cobalt-chrome on polyethylene bearing that later resulted in accelerated wear of the
prosthetic head, metallosis, and grossly elevated whole blood cobalt
concentrations.
How might we link systemic illness with metal exposure?Based on these findings we proposed toxicological criteria for assessing the likelihood that clinical features are related to cobalt toxicity15: clinical effects consistent with the known neurological, cardiac, or thyroid effects of cobalt, and for which any other explanation is less likely; increased blood cobalt concentrations (substantially higher than those in patients with well-functioning prostheses) several months after hip replacement; a fall in the blood cobalt concentration after treatment, accompanied by signs of improvement in features. When judged by these criteria, the systemic features in 10 of the reported cases were felt likely to be related to cobalt exposure from a metal-containing hip prosthesis.
Does chronic exposure to low metal concentrations cause systemic illness?The case for adverse systemic effects due to long term chronic low level elevation of metal concentrations associated with well-
Journal of Trauma and Orthopaedics: Volume 03, Issue 02, pages 42-43 Title: Metal Exposure after Hip Replacement and the Risks of Systemic Toxicity
Author: J. Mark Wilkinson
© 2015 British Orthopaedic Association

References 1. Cooper HJ, Urban RM, Wixson RL, Meneghini RM, Jacobs JJ. Adverse local tissue reaction arising from corrosion at the femoral neck-body junction in a dual-taper stem with a cobalt-chromium modular neck. J Bone Joint Surg Am 2013;95-10:865-72. 2. Wilkinson JM. Metal-on-metal hip prostheses: where are we now? BMJ 2012;345:e7792. 3. Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet 2012;379-9822:1199-204. 4. Keegan GM, Learmonth ID, Case CP. A systematic comparison of the actual, potential, and theoretical health effects of cobalt and chromium exposures from industry and surgical implants. Crit Rev Toxicol 2008;38-8:645-74. 5. Heisel C, Streich N, Krachler M, Jakubowitz E, Kretzer JP. Characterization of the running-in period in total hip resurfacing arthroplasty: an in vivo and in vitro metal ion analysis. J Bone Joint Surg Am 2008;90 Suppl 3:125-33. 6. Daniel J, Ziaee H, Pradhan C, Pynsent PB, McMinn DJ. Blood and urine metal ion levels in young and active patients after Birmingham hip resurfacing arthroplasty: four-year results of a prospective longitudinal study. J Bone Joint Surgr 2007;89-B-2:169-73. 7. Hartmann A, Lutzner J, Kirschner S, Witzleb WC, Gunther KP. Do Survival Rate and Serum Ion Concentrations 10 Years After Metal-on-Metal Hip Resurfacing Provide Evidence for Continued Use? Clin Orthop 2012;470-11:3118-26. 8. Holland JP, Langton DJ, Hashmi M. Ten-year clinical, radiological and metal ion analysis of the Birmingham Hip Resurfacing: from a single, non-designer surgeon. J Bone Joint Surg 2012;94-B-4:471-6. 9. Hart AJ, Sabah SA, Bandi AS, Maggiore P, Tarassoli P, Sampson B, J AS. Sensitivity and specificity of blood cobalt and chromium metal ions for predicting failure of metal-on-metal hip replacement. J Bone Joint Surg Br 2011;93-10:1308-13. 10. Steens W, von FG, Katzer A. Severe cobalt poisoning with loss of sight after ceramic-metal pairing in a hip--a case report. Acta Orthop 2006;77-5:830-2. 11. Rizzetti MC, Liberini P, Zarattini G, Catalani S, Pazzaglia U, Apostoli P, Padovani A. Loss of sight and sound. Could it be the hip? Lancet 2009;373-9668:1052. 12. Oldenburg M, Wegner R, Baur X. Severe cobalt intoxication due to prosthesis wear in repeated total hip arthroplasty. J Arthroplasty 2009;24-5:825 e15-20. 13. Ikeda T, Takahashi K, Kabata T, Sakagoshi D, Tomita K, Yamada M. Polyneuropathy caused by cobalt-chromium metallosis after total hip replacement. Muscle Nerve 2010;42-1:140-3. 14. Tower SS. Arthroprosthetic cobaltism associated with metal on metal hip implants. BMJ 2012;344:e430. 15. Bradberry SM, Wilkinson JM, Ferner RE. Systemic toxicity related to metal hip prostheses. Clin Toxicol (Phila) 2014:1-11. 16. Linna A, Oksa P, Groundstroem K, Halkosaari M, Palmroos P, Huikko S, Uitti J. Exposure to cobalt in the production of cobalt and cobalt compounds and its effect on the heart. Occup Environ Med 2004;61-11:877-85. 17. Prentice JR, Clark MJ, Hoggard N, Morton AC, Tooth C, Paley MN, Stockley I, Hadjivassiliou M, Wilkinson JM. Metal-on-Metal Hip Prostheses and Systemic Health: A Cross-Sectional Association Study 8 Years after Implantation. PLoS One 2013;8-6:e66186. 18. Clark MJ, Prentice JR, Hoggard N, Paley MN, Hadjivassiliou M, Wilkinson JM. Brain structure and function in patients after metal-on-metal hip resurfacing. AJNR Am J Neuroradiol 2014;35-9:1753-8. 19. Prentice JR, Blackwell CS, Raoof N, Bacon P, Ray J, Hickman SJ, Wilkinson JM. Auditory and Visual Health after Ten Years of Exposure to Metal-on-Metal Hip Prostheses: A Cross-Sectional Study Follow Up. PLoS One 2014;9-3:e90838.