metabolisme bilirubin
41
Bilirubin Metabolism Bilirubin Metabolism Harliansyah, Ph.D Harliansyah, Ph.D Dept of Biochemistry, Dept of Biochemistry, FKUY FKUY 201 201 3 3 , May , May
description
metabolisme bilirubin
Transcript of metabolisme bilirubin
-
Bilirubin MetabolismHarliansyah, Ph.DDept of Biochemistry, FKUY2013, May
-
What Is Bilirubin?Bilirubin is the by product of the breakdown of heme which is found in red blood cells.
Normal red blood cell destruction accounts for 80% of daily bilirubin produced in the newborn.
Infants produce twice as much bilirubin per day than as an adult.
There are two types of bilirubin - unconjugated (indirect) bilirubin and conjugated (direct) bilirubin.
-
Bilirubin complexed to albumin (Unconjugated Bilirubin) is transported to liver, where it is processed into Conjugated Bilirubin, by the liver cells.
In this form Bilirubin enters the bile fluids for transport to the small intestine (Conjugated Bilirubin is converted to Urobilinogen).
-
Unconjugated BilirubinUnconjugated (indirect) bilirubinFat-solubleNot yet metabolized by by the liver Is not easily excreted Is the biggest concern for newborn jaundice If it is not converted it can be deposited into the skin which causes the yellowing of the skin or into the brain which can lead to kernicterus.
-
Conjugated BilirubinConjugated (direct) bilirubin Water solubleIt is metabolized by the liverIt is mostly excreted in stool and some in the urine
-
Bilirubin Metabolism- 1Red blood cells are broken down in the Reticuloendothelial System Red blood cells break down to hemoglobin which is further broken down to iron, globin, and heme Bilirubin albumin complex
-
Bilirubin Metabolism- 2Unconjugated bilirubin is then carried to the liver by albumin Heme is further broken down to biliverdin then to unconjugated bilirubin by the enzyme biliverdin reductase Bilirubin albumin complex
-
Bilirubin Metabolism- 3 The liver then converts unconjugated bilirubin to conjugated bilirubin where it is excreted in the intestines The intestines then convert the conjugated bilirubin into urobilinogen and then stercobilin Bilirubin albumin complex
-
Bilirubin Metabolism- 4Urobilinogen is excreted in the urine Stercobilin is excreted in the stool Bilirubin albumin complex
-
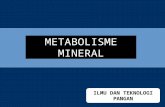
Mechanism of Bilirubin FormationEnzyme-catalysed degradation of haem. Haem degradation begins by haem oxygenase-catalysed oxidation of the a-bridge carbon of haem, which is converted to CO, leading to opening of the tetrapyrrole ring and release of the iron molecule. The resulting biliverdin molecule is subsequently reduced to bilirubin by cytosolic biliverdin reductase.
-
Murray et al., 2009
-
Ryter et al., 2002
-
What Is Physiologic Jaundice Physiologic jaundice is an exaggerated normal process seen in 60% of term infants, and 80% of premature infants It normally occurs during the first week of lifeIt is normally benign and self-limitingAssociated with a bilirubin level greater than 5-7mg/dL
-
Factors That Contribute To Physiologic JaundicePrematurityPolycythemia
-
Penyebab Peningkatan Kadar BilrubinProses Fisiologisvolume sel darah merah tinggi kompensasi tekanan partial oksigen yang rendahumur sel darah merah pendek dan peningkatan resirkulasi enterohepatal dari bilirubin Kurangnya ambilan (uptake) hati dampak penurunan konsentrasi protein pengikat bilirubin (seperti ligandin) Kurangnya konjugasi masih rendahnya aktivitas glukoronil transferase
-
Prematurity & HyperbilirubinemiaPremature infants are more susceptible to hyperbilirubinemia due to: Immature hepatic systemDelayed enteral feedingsDecrease in serum albumin levels
-
Prematurity & HyperbilirubinemiaImmature hepatic system - leads to decreased elimination of bilirubin from the system; therefore, higher levels of indirect bilirubin are in the blood which leads to hyperbilirubinemia
Bilirubin albumin complex
-
Prematurity & HyperbilirubinemiaDelayed enteral feedings - if feedings are delayed it decreases intestinal motility and removal of meconium, which leads to reabsorption of direct bilirubin, which is converted back to indirect bilirubin. Which means bilirubin increases in the blood and leads to hyperbilirubinemia
Bilirubin albumin complex
-
Prematurity & HyperbilirubinemiaDecrease in serum albumin levels - if there is a decrease in the amount of albumin receptors available, bilirubin does not bind to the albumin; therefore, is considered free bilirubin. Which means bilirubin increases in the blood and leads to hyperbilirubinemia Bilirubin albumin complex
-
Polycythemia & HyperbilirubinemiaPolycythemia is an increased level of red blood cells (RBCs) in the circulatory system
A infant has more RBCs than an adult, and the lifespan of an RBC is shorter in neonates
Increased RBCs and a shorter lifespan leads to increased destruction of RBCs, which leads to more bilirubin in the blood, which leads to hyperbilirubinemia
-
Factors That Contribute To Pathologic JaundiceHemolytic anemia Rh incompatibility ABO incompatibilityG6PD (glucose-6-phosphate deficiency) deficiency
-
Proses patologisPeningkatan ProduksiInkompatibilitas golongan Defek biokimia (enzim) eritrosit: enzim G6PD, Pyruvat Kinase, Hexokinase Abnormalitas struktur (membran) eritrosit: Sferositosis herediter, Elliptositosis herediter, Piknositosis infantil Infeksi: Bakterial, Viral, dan Protozoaldefek/kegagalan konjugasiDef. kongenital enzim glukoronil transferase (sindroma Crigler-Najjar dan sindroma Gilbert) Inhibisi enzim glukoronil transferase (karena pengaruh obat dan sindroma Lucey-Driscoll
kelainan ambilan (uptake) oleh hatiSekuestrasi sel darah merah
-
Genetics & HyperbilirubinemiaThe study was conducted in TaiwanThe reason for this is because the Asian population has twice the incidence of hyperbilirubinemia than the Caucasian population. They were looking to identify potential genetic defects that contribute to the higher incidence of hyperbilirubinemia
-
Genetics & HyperbilirubinemiaThe three enzymes are: G6PD - glucose-6-phosphate dehydrogenaseOTAP 2 - organic anion transporter 2UGT1A1 - UDP- glucuronsyltransferase 1A1
-
G6PDThe G6PD enzyme is responsible for reducing NADP+(nicotinamide adenine dinucleotide phosphate) to NADPH (reduced nicotinamide adenine dinucleotide phosphate) Pentose Phosphate Pathway
-
Gen G6PD terletak pada Xq28
-
G6PDWithout adequate levels of NADPH, red blood cells are more prone to stress and oxidation, which leads to hemolysis of red blood cells If there is a G6PD deficiency there will not be adequate levels of NADPH; therefore, leading to increased hemolysis of red blood cellsIncreased hemolysis of red blood cells leads to increased levels of bilirubin, which then leads to hyperbilirubinemia
-
Varian defisiensi enzim G6PD
KelasTingkat defisiensiAktivitas Enzim G6PD KeteranganIBerat
-
Organic Anion Transporter 2 OATP 2 The function of the OATP 2 enzyme is involved in the hepatic uptake of unconjugated bilirubin
Bilirubin albumin complex
-
Organic Anion Transporter 2 OATP 2In the study done, the identified polymorphisms in the OATP 2 enzyme, which led to increased risk for hyperbilirubinemia in the Asian population If the enzyme activity is delayed there will be increased levels of unconjugated bilirubin in the blood, therefore leading to hyperbilirubinemia
-
UDP - Glucuronsyltransferase 1A1 (UGT1A1)
The function of UGT1A1 is to convert unconjugated or indirect bilirubin to conjugated or direct bilirubin
Bilirubin albumin complex
-
UDP - Glucuronsyltransferase 1A1 UGT1A1In the study done, the authors identified polymorphisms in the UGT1A1 enzyme which, led to increased risk for hyperbilirubinemia in the Asian population If the enzyme activity is delayed there will be increased bilirubin in the blood, therefore leading to hyperbilirubinemia
-
Physiologic JaundiceversusPathologic Jaundice
PhysiologicOccurs 24 hours after birth
Prematurity
PolycythemiaPathologicOccurs less than 24 hours after birth
Hemolytic anemia
G6PD deficiency
-
KernicterusKernicterus is used to describe the yellow staining of the brain nuclei as seen on autopsy (kern means nuclear region of the brain; icterus means jaundice).Kernicterus is a rare, irreversible complication of hyperbilirubinemia
If bilirubin levels become markedly elevated, the unconjugated bilirubin may cross into the blood brain barrier and stain the brain tissues
If staining of the brain tissues occurs there is permanent injury sustained to areas of the brain which leads to neurological damage
-
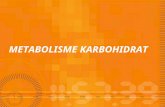
Picture Of A Brain With KernicterusYellow staining in the brain due to increased unconjugated bilirubin passing through the blood brain barrierRetrieved April 30, 2006, fromhttp://www.urmc.rochester.edu/neuroslides/slide156.htmlUsed with permission (9)
-
DiagnosticIn term infants a normal bilirubin level is between 1.0 - 10.0 mg/dLIf an infant has a hematocrit greater than 65% this places that infant at risk for hyperbilirubinemiaIf the reticulocyte count is greater than 5% in the first week of life, this identifies the infant as trying to replace destroyed red blood cellsA normal albumin level in a term infant is between 2.6 - 3.6 g/dL
-
Manifestasi Klinis Defisiensi G6PDhiperbilirubinemia pada neonatusserum bilirubin > 5 mg/dL, tidak melebihi 10 mg/dL pada bayi kurang bulan dan kurang dari 12 mg/dL pada bayi cukup bulan.Anemia dan ikterus Hiperbilirubinemia seringkali memerlukan transfusi tukarsering terjadi pada varian G6PD Mediteranean (kelas II)dapat menjadi kern icterus dengan gangguan neurologi berat bahkan dapat menyebabkan kematian
-
2. hemolisis akut paparan obat, infeksi, konsumsi kacang-kacanganSetelah 1-3 hari terpapar obat, gejala klinis yang muncul:Demam, Letargi, kadang disertai gejala GIT, Hemoglobinuria* (urine berwarna merah gelap hingga coklat), ikterus dan anemia, Takikardia, syok hipovolemi hemolisis intravascular
-
Thank You