METABOLIC SYSTEM DISORDER -...
53
PATHOLOGICAL FINDING METABOLIC SYSTEM DISORDER PATHOLOGICAL FINDING MS K23.1 & 2 dr.Joko S. Lukito, SpPA, dr. Soekimin, SpPA Departemen Patologi Anatomi Fakultas Kedokteran Universitas Sumatera Utara Medan
Transcript of METABOLIC SYSTEM DISORDER -...
PATHOLOGICAL FINDING
METABOLIC SYSTEM DISORDER
PATHOLOGICAL FINDING
MS K23.1 & 2
dr.Joko S. Lukito, SpPA, dr. Soekimin, SpPA
Departemen Patologi Anatomi Fakultas Kedokteran
Universitas Sumatera Utara Medan
DIABETES MELLITUS
Chronic disorder of carbohydrate, fat and protein metabolism due to defective or deficient insulin secretory response.
• Demographics : 3% of world population,
54,000 deaths/year in US,
#7 leading cause of death.#7 leading cause of death.
Lifetime risk: type 1 – 0.5%, type 2 – 5%.
• Causes : destruction of islets due to pancreatitis, tumors, drugs (steroids, thiazides, pentamidine), hemochromatosis (“bronze diabetes” due to hemosiderin deposition in pancreas), hereditary ceruloplasmin deficiency, surgery, infections (congenital rubella, CMV, coxsackievirus , endocrinopathies (pituitary, adrenal, pregnancy), gestational diabetes or idiopathic.

DIAGNOSIS
• Blood glucose rises markedly for a sustained period.
• High fasting glucose.
• Impaired glucose tolerance.

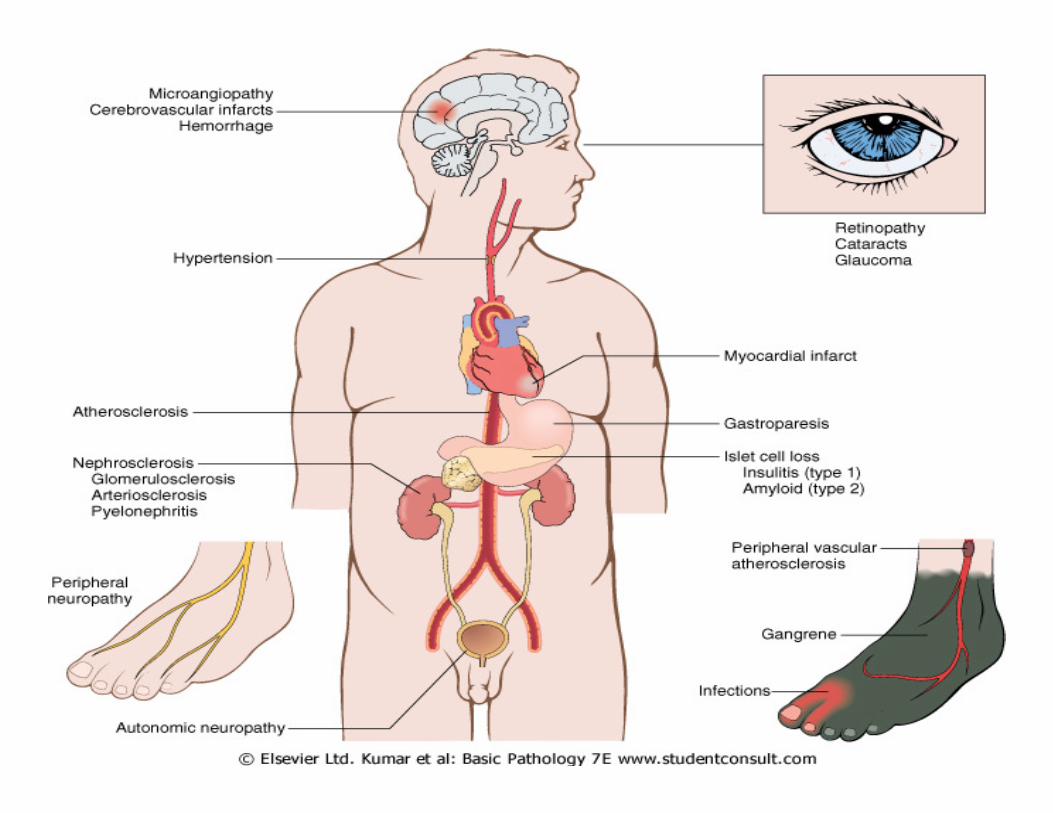
Long term complications
• Damage to blood vessels in kidneys (nodular
Kimmelstiel-Wilson glomerulopathy,
pyelonephritis, papillary necrosis)
• Eyes (exudative and proliferative retinopathy)• Eyes (exudative and proliferative retinopathy)
• Nerves (symmetric polyneuropathy);
Brain (stroke)
• Peripheral vascular disease and coronary artery
heart disease
• Morbidity / death

Insulin-Dependent Diabetes Mellitus
(IDDM)• Juvenile onset, Type 1 10% of all cases• Beta cell mass causing severe, absolute lack of
insulin.• Onset : age < 20 years, normal weight, decreased
blood insulin, anti-islet cell antibodies (+), DKA common.common.
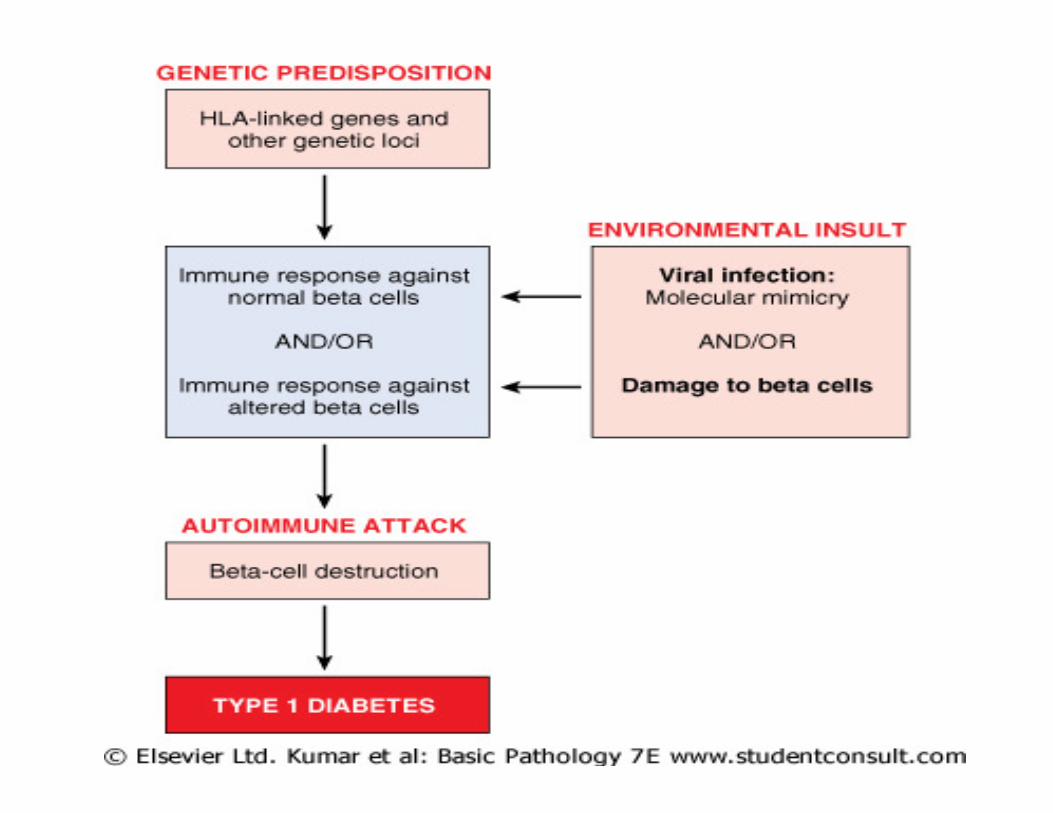
• Islet cell destruction :due to genetic predisposition, autoimmunity, environmental insult; initially with mononuclear cell infiltrates
• Autoimmunity :usually chronic (years); clinical disease when 90% of islet cells are destroyed.Associated with CD8+ T cell infiltrate, Coxsakie vir.
• Clinical : PPP (polyuria, polydipsia, polyphagia) and DKA
• Low/absent plasma insulin, high plasma glucagon, unstable glucose tolerance (very sensitive to changes in insulin, diet, exercise, infection, stress),
Insulin-Dependent Diabetes Mellitus (IDDM)
changes in insulin, diet, exercise, infection, stress),
• Presence of free fatty acids (due to breakdown of adipose stores), which produces ketone bodies (acetoacetic acid and beta-hydroxybutyric acid)
• Micro: early insulinitis with marked islet atrophy and fibrosis and severe beta cell depletion

Non-Insulin Dependent
Diabetes Mellitus
• Adult onset, NIDDM; type 2 80-90% of cases of diabetes
• Usually > 30 years old, obese (80% of cases).
• Relative insulin deficiency is due to insulin resistance or derangement in beta cell secretion of resistance or derangement in beta cell secretion of insulin
• Mild/moderate insulin deficiency; beta cells may be “exhausted” due to chronic hyperglycemia and persistent beta cell stimulation.
• Insulin resistance in peripheral tissues also seen in obesity and pregnancy.

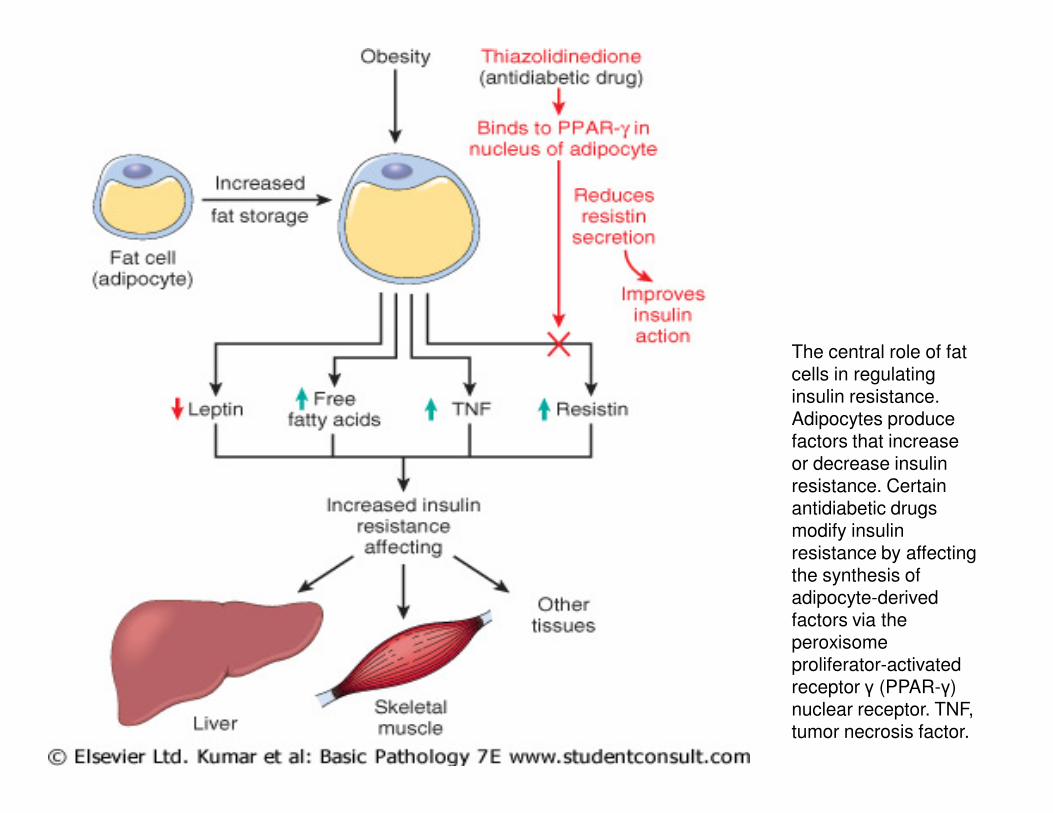
The central role of fat cells in regulating insulin resistance. Adipocytes produce factors that increase or decrease insulin resistance. Certain antidiabetic drugs modify insulin resistance by affecting the synthesis of adipocyte-derived factors via the peroxisome proliferator-activated receptor γ (PPAR-γ) nuclear receptor. TNF, tumor necrosis factor.

Histology :
1. Alveoli
2. Islets of Langerhans :a cells
b cellsd cells
3. Interlobular
septa4. Interlobular
ducts
Normal pankreas with islet of Langerhans.
Endocrine
function :
1. Insulin (beta cells)2. Glucagon
(alpha cells)
3. Somatostatin
(delta cells)

Microscopic findings:
• Type 1 :
inconsistent reduction in number and size of
islets, uneven insulinitis (T lymphocytes).
• Type 2 :• Type 2 :
• subtle reduction in islet cell mass, amyloid
replacement of islets due to amylin fibrils
(also seen in aging nondiabetics);
• associated with marked fatty replacement.
• Infants of diabetic mothers – islet cell
hypertrophy/hyperplasia.

The pancreas is a compound, acinar, serous , exocrine gland with islets of endocrine cells. This low-magnification view shows the organization of acinar parenchyma into irregular lobules, separated by prominent clear spaces. The amount of space is an artefact. Since the size of interlobular spaces (which contain loose connective tissue) is easily altered by manipulation (stretching or compression). Connective tissue of an interlobular septum is visible at right, including a prominent blood vessel.

This is an insulitis of an islet of
Langerhans (type I DM). The
presence of the lymphocytic
infiltrates in this edematous islet
suggests an autoimmune
mechanism for this process. The
destruction of the islets leads to
an absolute lack of insulin that
characterizes type I DM.

An islet of Langerhans demonstrates amorphous pink deposition of
amyloid in a patient with type II diabetes mellitus.


Complications of diabetes
1. Microangiopathy
2. Nephropathy
3. Retinopathy3. Retinopathy
4. Neuropathy
5. Dermopathy

Microangiopathy
Microangiopathy: diffuse basement membrane thickening with protein leakage in capillaries.
Red Skin and Rubeosis Facei
Facial involvement rubeosis facei d/t dilatation of superficial venous plexus.dilatation of superficial venous plexus.
In the eye grounds and skin.
Periungual telangiectasia.
Assumed to play a role in diabetic neuropathy
diabetic foot.
Increased tendency for diabetic platelets to aggregate � plasma viscosity and sluggish microcirculation.

Gangrene foot
Diabetic dermopathyDiabetic dermopathy
Diabetic Bullae,Fingers
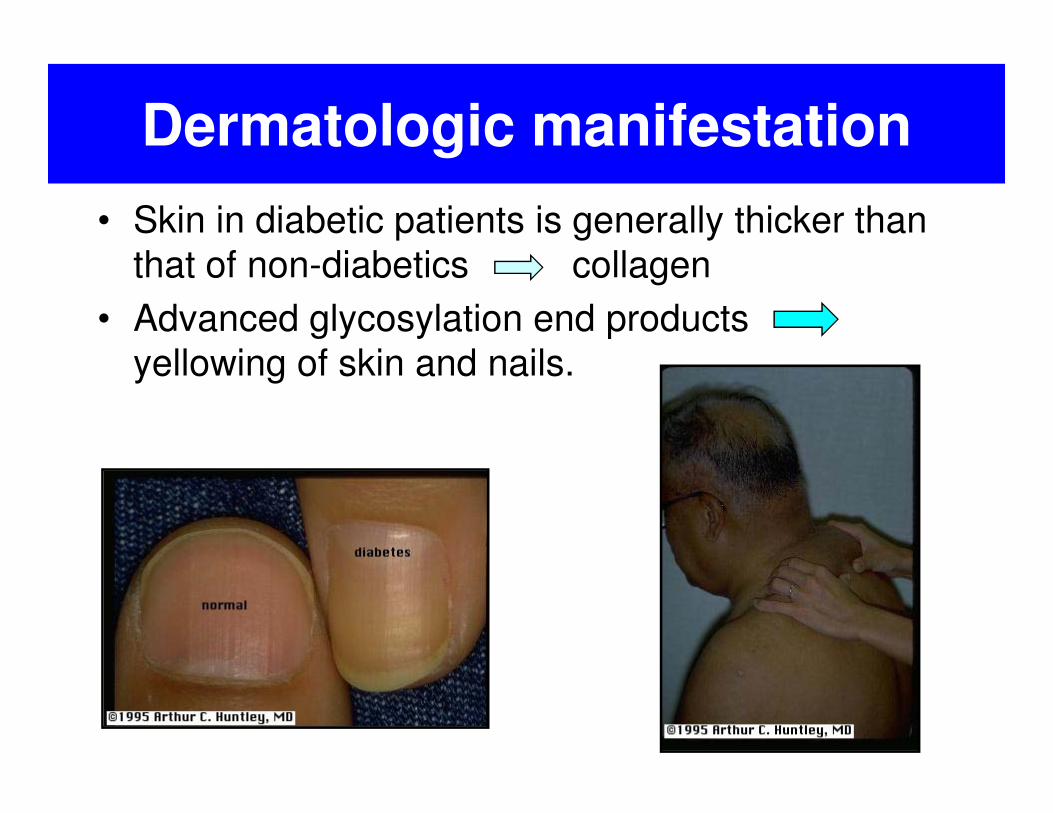
• Skin in diabetic patients is generally thicker than
that of non-diabetics collagen
• Advanced glycosylation end products
yellowing of skin and nails.
Dermatologic manifestation

CUTANEOUS INFECTIONS IN
DIABETES MELLITUS
• Etio : Candida, Pseudomonas, Dermatophytosis
• Foot ulcer.
• Foliculitis � carbuncle
Candidiasis, Fingernails

Gangrenous necrosis and ulceration involving the lower extremity is shown here. Diabetics have accelerated atherosclerosis that can be extensive to involve peripheral vasculature and predispose to this complication.
A diabetic foot with a previous
healed transmetatarsal amputation
demonstrates an ulcer in the
region of the ankle.
Vascular complications
• Atherosclerosis in aorta and large/medium sized vessels
• Myocardial infarction : common cause of death, M=F
• Gangrene of lower extremities; relative risk is • Gangrene of lower extremities; relative risk is 100:1
• Micro :
hyaline arteriolosclerosis, associated with hypertension, more common/severe in diabetes but not specific; amorphous hyaline thickening in arteriolar wall

Hyaline arteriolosclerosis. Note a markedly thickened, tortuous afferent
arteriole in the kidney. The amorphous nature of the thickened vascular
wall is evident. (Periodic acid-Schiff.) (Courtesy of Dr. M. A. Venkatachalam,
Department of Pathology, University of Texas Health Science Center at San Antonio, San
Antonio, TX.)

Nephropathy
• #2 cause of death in patients with diabetes after MI.
• Glomeruli - capillary basement membrane thickening.
• Nodular glomerulosclerosis :
ball-like deposits of laminated matrix within ball-like deposits of laminated matrix within mesangial core of lobule;
push capillary loops to periphery, may have perinodular halos; called Kimmelstiel-Wilson lesion and
may contain trapped mesangial cells;
low sensitivity (10-35%) but highly specific for diabetes mellitus.

• Diffuse glomerulosclerosis: diffuse increase in mesangial matrix, mesangial cell proliferation, basement membrane thickening; seen in most patients with diabetes mellitus after 10 years; when marked, causes nephrotic syndrome; not
NephropathyCont’d
when marked, causes nephrotic syndrome; not specific
• Also renal atherosclerosis and arteriolosclerosis; changes to efferent arteriole are specific for diabetes
• Pyelonephritis and necrotizing papillitis also common.
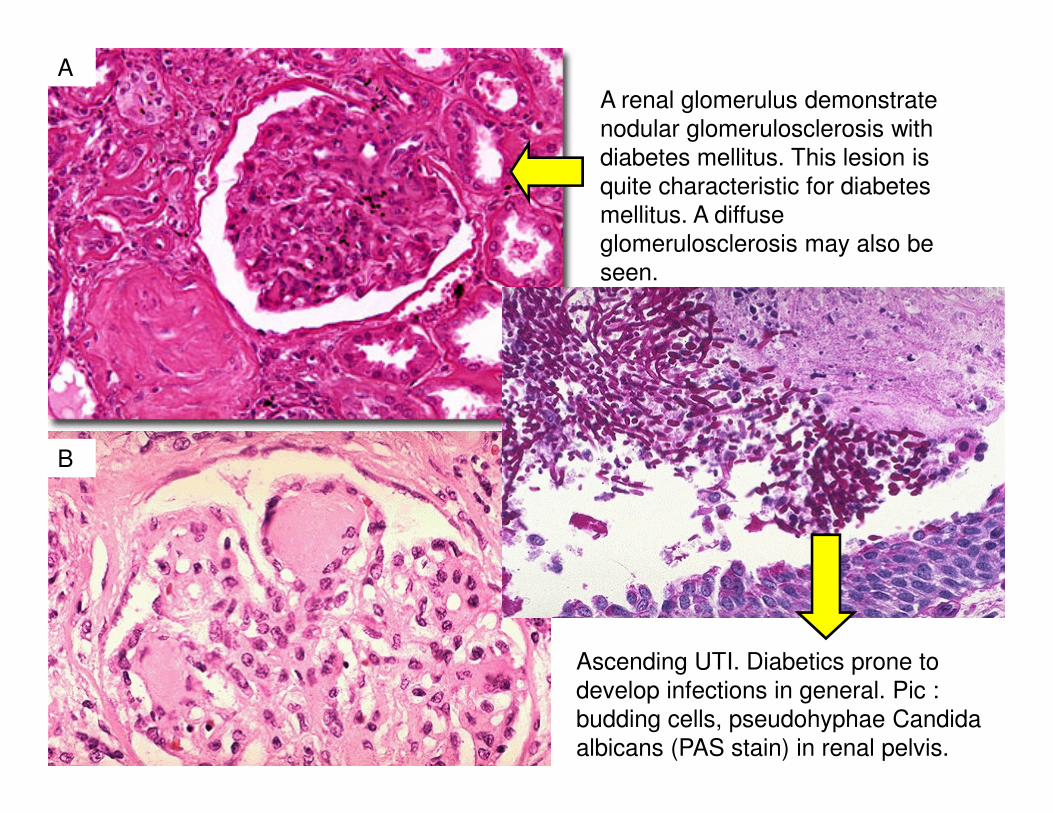
A renal glomerulus demonstrate
nodular glomerulosclerosis with
diabetes mellitus. This lesion is
quite characteristic for diabetes
mellitus. A diffuse
glomerulosclerosis may also be
seen.
A
Ascending UTI. Diabetics prone to
develop infections in general. Pic :
budding cells, pseudohyphae Candida
albicans (PAS stain) in renal pelvis.
B

A renal glomerulus with
nodular glomerulosclerosis,
along with hyaline
arteriolosclerosis in the small
arteriole to the lower right of
the glomerulus, is shown here
with PAS stain.

Ocular Manifestations
• # 4 cause of blindness in US
• Associated with retinopathy, cataracts, glaucoma, infection.
Diabetic retinopathy on funduscopic
examination.
Cataracts of the crystalline lens with
opacification.
normal retinae

DIABETIC NEUROPATHY
Autonomic Neuropathy
the first nervous tissue affected in diabetics �nonmyelinated nerve fibers, such as those of the autonomic nervous system
Diabetics often develop sensory neuropathy on the Diabetics often develop sensory neuropathy on the feet, especially with long-standing disease. The clinical presentation usually involves tingling and numbness starting in the toes. The level of neuropathy may vary from mild numbness of the distal toes to profound anesthesia and neuropathic ulcers. Thermal sensitivity

Lipid
Metabolic Metabolic
Disorder

Hyperlipidemia
• Disorders caused by the accumulation of lipids are called lipidoses.
• Other enzyme abnormalities result in the body being unable to properly convert fats into energy are called fatty acid oxidation disorders.
Hyperlipidemia : strong
risk factor for ischemic
heart disease.
Obese (abdominal
obesity more dangerous
than subcutaneous
obesity).

• Hyperlipidemia is often secondary to uncontrollable diabetes, biliary cirrhosis, and lipoid nephrosis.
• Excess proliferation of fat cells � lipoma.
• In genetic lipid storage diseases, lipid accumulates because of a disturbance in lipid metabolism. Genetic diseases due to gene defects result in abnormal lipid metabolism. defects result in abnormal lipid metabolism.
• Large accumulation of lipid appears in many cells, but particularly the reticuloendothelial cells of the lymph nodes, liver, spleen, and bone marrow.
• Abnormal lipid storage occurs in Niemann-Pick, Gaucher's, and Tay-Sachs diseases.
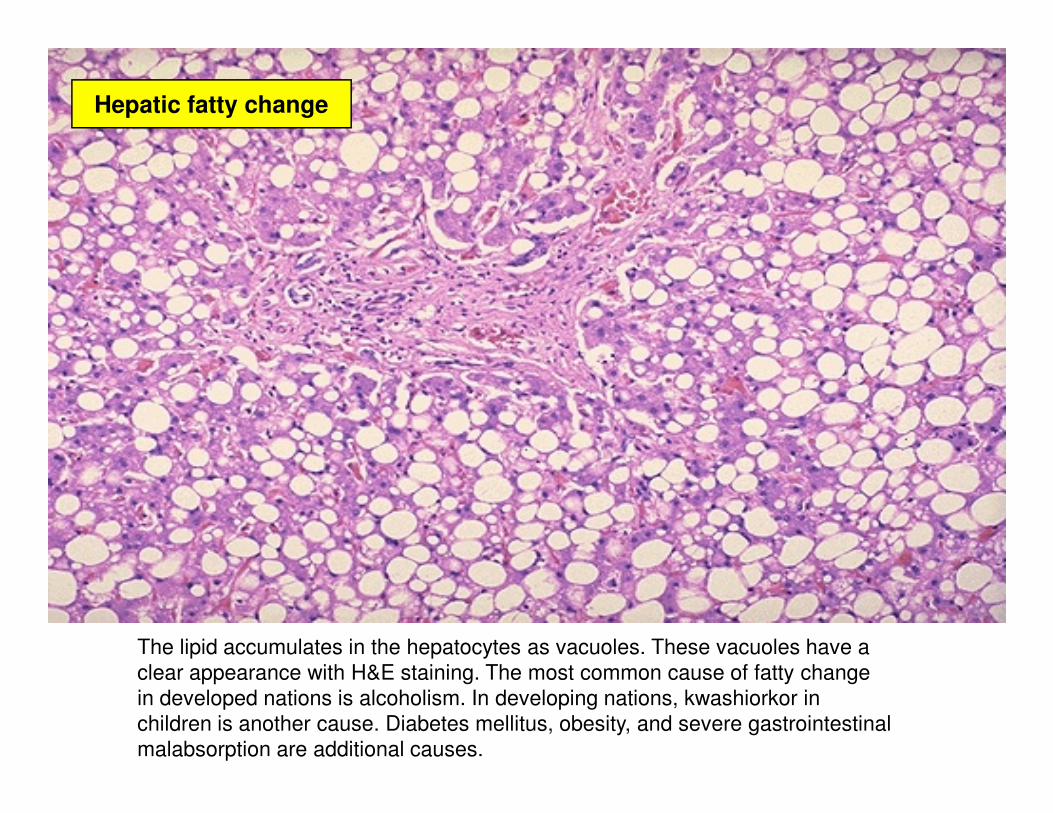
Hepatic fatty change
The lipid accumulates in the hepatocytes as vacuoles. These vacuoles have a
clear appearance with H&E staining. The most common cause of fatty change
in developed nations is alcoholism. In developing nations, kwashiorkor in
children is another cause. Diabetes mellitus, obesity, and severe gastrointestinal
malabsorption are additional causes.

GAUCHER'S DISEASE
• Glucocerebrosides, which are a product of fat metabolism, accumulate in tissues.
• The most common lipidosis.
• Leads to an enlarged liver and spleen and a brownish pigmentation of the skin. Accumulations of glucocerebrosides in the eyes cause yellow spots called pigmentation of the skin. Accumulations of glucocerebrosides in the eyes cause yellow spots called pingueculae to appear.
• Accumulations in the bone marrow can cause pain and destroy bone.
• Adults form, infantile form and juvenile form.
• Th/ : enzyme replacement therapy (intravenous), every 2 weeks.

• Gangliosides � products of fat metabolism, accumulate in tissues.
• At a very early age, children with this disease become progressively retarded and appear to have floppy muscle tone.
TAY-SACHS DISEASE
have floppy muscle tone.
• Spasticity followed by paralysis, dementia, and blindness.
• These children usually die by age 3 or 4.
• Tay-Sachs disease can be identified in the fetus by chorionic villus sampling or amniocentesis.
• The disease cannot be treated or cured.
NIEMANN-PICK DISEASE
• Deficiency of a specific enzyme results in the accumulation of sphingomyelin or cholesterol.
• Several forms : depending on the severity of the enzyme deficiency and thus accumulation of sphingomyelin or cholesterol.
• Type A : Children fail to grow properly and have multiple neurologic problems � die by age 3.
• Type A : Children fail to grow properly and have multiple neurologic problems � die by age 3.
• Type B : develop fatty growths in the skin, areas of dark pigmentation, and an enlarged liver, spleen, and lymph nodes; may be mentally retarded.
• Type C : develop symptoms in childhood, with seizures and neurologic deterioration.
• None of the types of Niemann-Pick disease can be cured, and children tend to die of infection or progressive dysfunction of the central nervous system.
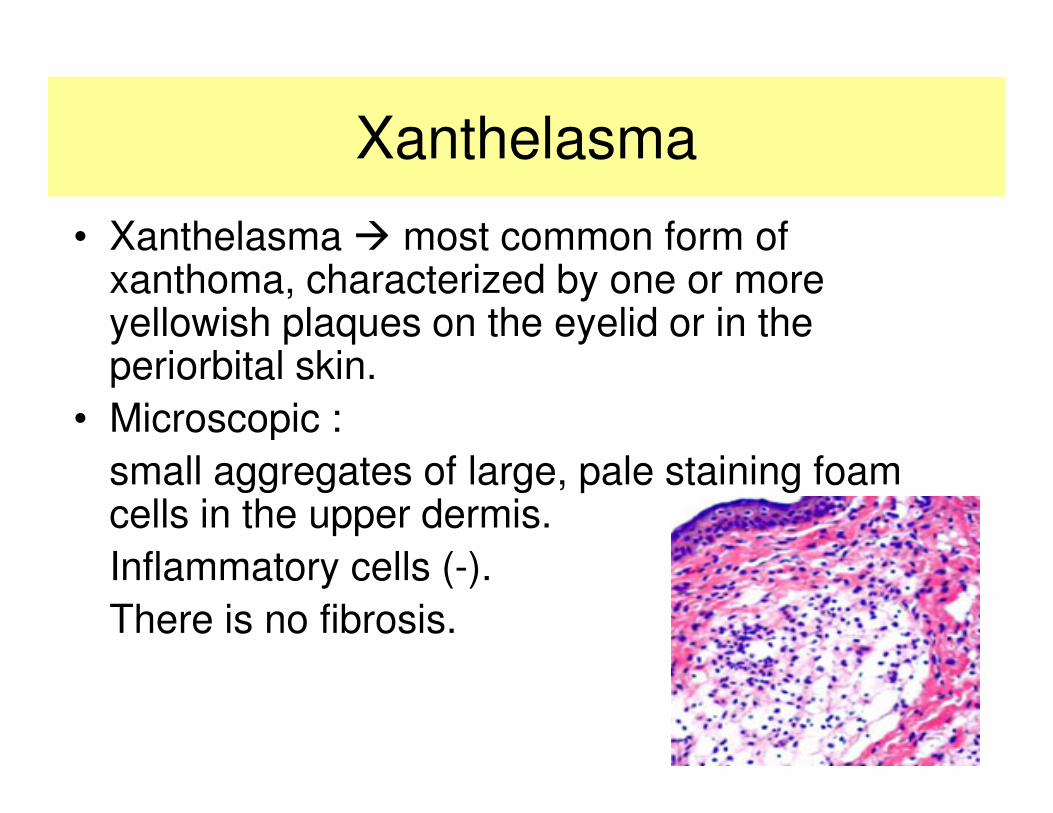
Xanthelasma
• Xanthelasma � most common form of xanthoma, characterized by one or more yellowish plaques on the eyelid or in the periorbital skin.
• Microscopic :• Microscopic :
small aggregates of large, pale staining foam cells in the upper dermis.
Inflammatory cells (-).
There is no fibrosis.

Xanthelasma
palpebrapalpebra

Xanthelasma of the chest
Eruptive xanthoma (elbow)

PROTEIN
CALORIE CALORIE
MALNUTRITION

Malnutrition
• Malnutrition may be due to inadequate food absorption or inadequate food intake (inadequate supply, increased requirements).
• The diagnosis of malnutrition depends on an accurate dietary history, evaluation of height, weight, head circumference and past rates of accurate dietary history, evaluation of height, weight, head circumference and past rates of growth, measurement of midarm circumference and skinfold thickness and other tests.
• Chronic malnutrition : deficits of more than a single nutrient. There is usually associated immunologic insufficiency (white blood cell count < 1500/mm3 and anergy to skin test antigens).

Malnutrition
• Insufficient protein intake; impaired absorption (chronic diarrhea), abnormal losses (nephrosis, burns) or impaired synthesis or impaired synthesis (chronic liver disease).
• Underdeveloped countries, affecting children from infancy to about 5 years of age.

Marasmus
(Infantile Atrophy, Athrepsia)• In most cases, marasmus is due to inadequate
caloric intake, but may also be due to metabolic abnormalities or congenital malformations.
• Clinical :
– failure to gain weight followed by weight loss – failure to gain weight followed by weight loss and finally emaciation.
– Fat is loss last from the cheeks.
– The abdomen may be flat or distended.
– There is muscle atrophy and hypotonia.
– The basal metabolic rate is reduced.
– The infant may be constipated or have the "starvation type" of diarrhea with mucus.

Percentage of population affected by malnutrition by country,
according to United Nations statistics.

Symptoms :– lethargy,– apathy, – irritability to inadequate growth, – loss of muscular mass, – secondary immunodeficiency and
Kwashiorkor
– edema. – renal function is decreased, – the liver and the heart may enlarge. – dermatitis is common; – the hair is sparse, thin and dyspigmentated. – Infections, – vomiting and diarrhea are common.– vitamin and mineral deficiencies; – delayed bone growth. – Mental changes may occur, followed by stupor, coma and death.
Laboratory data:
• low albumin concentration
• low plasma glucose
• ketonuria
• low plasma amino acids
• decresed K+, Mg++
Kwashiorkor
• decresed K+, Mg++
• low cholesterol
The treatment is based on management of the associated conditions (infections, dehydration, anemia, diarrhea) and institution of adequate diet.
Mental and physical retardation may be permanent.
Protein Calorie Malnutrition Immune
Function in Humans
Humoral Immunity Response1. Serum immunoglobulin levels Raised or Normal
2. Secretory IgA Decreased
3. Circulating B cells Decreased or N
4. Plaque forming cells Decreased
Cellular Immunity Response 1. PHA Decreased Decreased
2. Immunity to intracellular organisms Decreased
3. Circulating T Cells Decreased
4. Lymphokine production Decreased

GOUT / TOPHI
• Gout � arthritis / inflammation in some joints because of uric acid accumulation.
• Predilections : joints of extremities– large toe, knee, ankle, foot � >>>
– arms (hand, wrist, and elbow) � less. – arms (hand, wrist, and elbow) � less.
– fingers (uncommon).
• Symptoms :– Sudden, intense joint pain, which often first occurs in
the early morning hours.
– Swollen joint
– Warm
– Red or purple skin around the joint.

Uric Acid
• Uric acid : red meats , internal organs (liver, kidneys, tongue, heart), some shellfish, anchovies (teri), peanut.
• Normal levels for men = < 7mg/dl and • Normal levels for men = < 7mg/dl and slightly less for most women.


GOUT
• Abnormal deposits of sodium urate crystals in the joint cartilage and later release into the joint fluid.
• Uric acid crystals can also form in the kidney �kidney stones.kidney stones.
• Sodium urate is formed from uric acid, a natural chemical in the body. Uric acid comes from the natural breakdown of proteins.
• Uric acid in normal amounts remains dissolved in the blood, easily passes through the kidneys, and leaves the body as waste. Uric acid in high amounts, however, makes a person more likely to develop gout.


![MS- K2.2 GLIKOGENESIS GLIKOGENOLISIS.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000095-metabolism-system/mbs127... · - Called type V glycogen storage diseaseCalled type V glycogen](https://static.fdocuments.us/doc/165x107/5c79b16809d3f200208cb824/ms-k22-glikogenesis-read-onlyocwusuacidcoursedownload1110000095-metabolism-systemmbs127.jpg)
![G.Steven-Johnson Syndrome.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../mk_aia_slide_steven_-_johson_syndrome.pdfSteven-Johnson Syndrome • Drug induced problem • Found by Stevens](https://static.fdocuments.us/doc/165x107/5cb80efd88c993f37c8b4b5d/gsteven-johnson-read-only-ocwusuacidocwusuacidmkaiaslidesteven-johsonsyndromepdfsteven-johnson.jpg)





![CARBOHYDRATE METABOLISM 1. NEW.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000095-metabolism-system/mb… · Digestion and absorption Carbohydrate 1. Breakdown to monosaccharides](https://static.fdocuments.us/doc/165x107/608acd78d09ad558844fffc9/carbohydrate-metabolism-1-newppt-read-onlyocwusuacidcoursedownload1110000095-metabolism-systemmb.jpg)

![kuliah Hypothyroidism.ppt [Read-Only]ocw.usu.ac.id/course/download/1110000095-metabolism-system/mbs127... · FBC Anemia ECG Slow rate. Small complexes. Treatment Thyroxine. Usual](https://static.fdocuments.us/doc/165x107/5c8761f009d3f2635f8d2443/kuliah-read-onlyocwusuacidcoursedownload1110000095-metabolism-systemmbs127.jpg)