Metabolic modulation as a novel cancer treatment · PDF fileMetabolic modulation as a novel...
7
Metabolic modulation as a novel cancer treatment Peter Dromparis, Gopinath Sutendra and Evangelos D. Michelakis, Department of Medicine, University of Alberta, Edmonton, Canada Correspondence: Evangelos D. Michelakis, University of Alberta, Edmonton, T6G 2B7 Canada. Tel: +1 780-407-1576, fax: +1 780-407-6452, e-mail: [email protected] Abstract The Warburg effect refers to the cancer’s metabolic shift from mitochondrial oxidation to anaerobic gly- colysis, even when oxygen is present. Although this metabolic anomaly was long believed to be due to irreversible mitochondrial damage, it now appears mitochondria in cancer are actively suppressed. Since mitochondria are extensively integrated into the metabolic, signaling and apoptotic biology of the cell, mitochondrial suppression in combination with glycolysis-driven metabolism allows cancer to mas- terfully inhibit intrinsic cell death mechanisms and promote rapid proliferation even in sub-optimal condi- tions. In this review, we analyze cancer’s metabolic strategy and describe how active mitochondrial suppression is compatible with both the genetic and evolutionary models of cancer. Furthermore, we discuss several strategies for mitochondrial activation and review current pre-clinical and clinical studies of agents showing promise in effectively and selectively targeting cancer. Keywords: cancer, metabolic, apoptosis, dichloroacetate, glycolysis ■ Heart Metab. (2011) 51:20–26 Introduction We currently perceive cancer as an accumulation of numerous chromosomal, genetic and bio- chemical abnormalities that result in dysfunctional cells. However, if so extensively damaged, how does cancer escape death, even flourish, in hypoxic and acidic conditions? Perhaps can- cer should be viewed as the “healthiest“ of cells, developing exquisite mechanisms to sup- press cell death (which is mostly regulated by mitochondria) and survive in otherwise uninhab- itable microenvironments, essentially achieving what medicine strives for—immortality. One way that cancer could achieve this is by developing strategies to effectively suppress mito- chondrial function. Here, we summarize cancer’s metabolic strategies to evade death and dis- cuss potentially effective and selective mitochondria-targeting therapies that induce apoptosis in cancerous but not non-cancerous tissues. Mitochondria: a central role in cellular biology Mitochondria produce energy through the oxidation of carbohydrates and lipids. In glucose oxidation (GO), pyruvate is de-carboxylated to acetyl-CoA by the gate-keeping mitochondrial enzyme pyruvate dehydrogenase (PDH). In fatty acid oxidation (FAO), fatty acids enter the mitochondria through carnitine palmitoyl-transferase-1 (CPT-1) and are also converted to acetyl-CoA (Fig. 1). The Krebs’ cycle extracts electrons derived from acetyl-CoA and feeds New Therapeutic Approaches NEW THERAPEUTIC APPROACHES - PETER DROMPARIS 20 Heart Metab. (2011) 51:20–26
Transcript of Metabolic modulation as a novel cancer treatment · PDF fileMetabolic modulation as a novel...

Metabolic modulation as a novelcancer treatment
Peter Dromparis, Gopinath Sutendra and Evangelos D. Michelakis, Department of Medicine,University of Alberta, Edmonton, Canada
Correspondence: Evangelos D. Michelakis, University of Alberta, Edmonton, T6G 2B7 Canada.Tel: +1 780-407-1576, fax: +1 780-407-6452, e-mail: [email protected]
AbstractThe Warburg effect refers to the cancer’s metabolic shift from mitochondrial oxidation to anaerobic gly-colysis, even when oxygen is present. Although this metabolic anomaly was long believed to be due toirreversible mitochondrial damage, it now appears mitochondria in cancer are actively suppressed.Since mitochondria are extensively integrated into the metabolic, signaling and apoptotic biology of thecell, mitochondrial suppression in combination with glycolysis-driven metabolism allows cancer to mas-terfully inhibit intrinsic cell death mechanisms and promote rapid proliferation even in sub-optimal condi-tions. In this review, we analyze cancer’s metabolic strategy and describe how active mitochondrialsuppression is compatible with both the genetic and evolutionary models of cancer. Furthermore, wediscuss several strategies for mitochondrial activation and review current pre-clinical and clinical studiesof agents showing promise in effectively and selectively targeting cancer.
Keywords: cancer, metabolic, apoptosis, dichloroacetate, glycolysis
■ Heart Metab. (2011) 51:20–26
Introduction
We currently perceive cancer as an accumulation of numerous chromosomal, genetic and bio-chemical abnormalities that result in dysfunctional cells. However, if so extensively damaged,how does cancer escape death, even flourish, in hypoxic and acidic conditions? Perhaps can-cer should be viewed as the “healthiest“ of cells, developing exquisite mechanisms to sup-press cell death (which is mostly regulated by mitochondria) and survive in otherwise uninhab-itable microenvironments, essentially achieving what medicine strives for—immortality. Oneway that cancer could achieve this is by developing strategies to effectively suppress mito-chondrial function. Here, we summarize cancer’s metabolic strategies to evade death and dis-cuss potentially effective and selective mitochondria-targeting therapies that induce apoptosisin cancerous but not non-cancerous tissues.
Mitochondria: a central role in cellular biology
Mitochondria produce energy through the oxidation of carbohydrates and lipids. In glucoseoxidation (GO), pyruvate is de-carboxylated to acetyl-CoA by the gate-keeping mitochondrialenzyme pyruvate dehydrogenase (PDH). In fatty acid oxidation (FAO), fatty acids enter themitochondria through carnitine palmitoyl-transferase-1 (CPT-1) and are also converted toacetyl-CoA (Fig. 1). The Krebs’ cycle extracts electrons derived from acetyl-CoA and feedsNe
wTh
erape
uticA
pproa
ches
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
20 Heart Metab. (2011) 51:20–26

them into the electron transport chain (ETC). Aselectrons transfer, H+ are extruded across the innermitochondrial membrane, creating an electrochemicalgradient, the mitochondrial membrane potential (ΔΨm).ΔΨm drives H+ re-entry through adenosine-5’-tri-phosphate (ATP) synthase, where they combine withoxygen to produce ATP, completing oxidative phos-phorylation. Thus, the flux of fuel into the mitochon-dria and respiration are closely linked with ΔΨm,which can be imaged with voltage-sensitive dyes andthus be a marker of mitochondrial activity. In addition,because ΔΨm is critical in setting the threshold forapoptosis as described below, fuel supply is alsointimately linked to cell death.
Mitochondria are major regulators of apoptosis.Upon opening of the mitochondrial transition pore
(MTP), pro-apoptotic mediators are released into thecytoplasm and ignite the apoptotic process. MTP is amega-channel that spans the mitochondrial mem-brane and is both redox- and voltage-sensitive, thusregulated in part by ΔΨm (Fig. 1) [1]. While ΔΨmdepolarization promotes MTP opening, hyperpolariza-tion increases its opening threshold, establishingan apoptosis-resistant state. Thus, ΔΨm could alsobe a surrogate for apoptosis resistance. Furthermore,since ΔΨm depends on metabolism, fuel supplyand apoptosis are intrinsically linked. As discussedbelow, most solid cancers are characterized by hyper-polarized mitochondria compared to non-canceroustissues, pointing to mitochondria’s critical role in thewell-known apoptosis resistance in cancer.
Mitochondria are extensively integrated into cellsignaling. In addition to H+ extrusion, the ETC alsogenerates superoxide (mitochondria-derived reactiveoxygen species –mROS). Unstable mROS, like super-oxide, can be dismutated into more stable mROS andleave the mitochondria to regulate redox-sensitive tar-gets like the voltage-gated potassium channels (Kv) inthe plasma membrane. As mitochondria are importantO2 sensors, this axis (ETC-mROS-Kv channels) is thebasis of hypoxic pulmonary vasoconstriction. mROSalso regulate other redox-sensitive targets like the tran-scription factors p53 [2] and hypoxia inducible factor-1α(HIF1α) [3], important in both vascular diseases andcancer (Fig. 1).
Mitochondria may also signal by releasingmetabolicsubstrates. Alpha-ketoglutarate (αKG) is a Krebs’cycle intermediate that, once in the cytosol, acts asa co-factor for prolyl-hydroxylases which degradeHIF1α [3]. In other words, this critical transcription fac-tor that drives angiogenesis in both cancer and vascu-lar diseases, is regulated by at least two mitochondria“signals”, mROS and αKG, both of which are linked tofuel processing and mitochondrial respiration.
Mitochondria can also sequester calcium. Being themost negatively charged organelles, they function asCa++ sinks, in a ΔΨm-dependent manner. Amongthe myriad of Ca++-dependent signaling processesare transcription factors that are integral in both vascu-lar disease and cancer, like the nuclear factor of acti-vated T-cells (NFAT) [3].
Therefore, suppression of mitochondrial functionhas the potential to influence a myriad of cellularprocesses critical in cancer biology. Suppressed
Glucose
DNAsynthesis
Fatty acids
Fatty acids
Citrate
mROS
∆Ψm
Acetyl-CoA
Randle Cycle
Acetyl-CoA
Membranesynthesis
PPP
GLY
Pyruvate
1
3
5
1 2
3
5
6
4
64
2
Glycoslysis Inhibitors Mitochondria Activators3-bromopyruvate, lonidamine, 2-deoxyglucose
PKM2 inhibitors
LDH inhibitors
PDK inhibitors (DCA)
FAS Inhibitors
FAO Inhibitors
PDH
PDK
DiffusibleMetabolitesETC
MTP
HIF1α
αKG
CTP-1
Krebs’Cycle
Lactate + HNAD +
+
+H
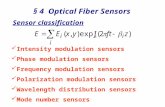
Fig. 1 Metabolic targets in cancer therapy. A metabolic shiftaway from mitochondrial oxidation to alternative pathways supportsrapid proliferation and apoptosis resistance. Mitochondrial suppres-sion is achieved in part by inhibition of PDH, which resultsin decreased mitochondrial signaling molecules (mROS and αKG)and mitochondrial membrane potential hyperpolarization, closingthe MTP. The decrease in signaling molecules can activate numer-ous transcription factors including HIF1α, which sustains this phe-notype. The glycolytic pathway (GLY) provides sufficient ATP andsupports DNA synthesis (via PPP) and other biosynthetic pathways.Numerous mutations in the Krebs’ cycle (see text) can result in anaccumulation of citrate which is critical for the de novo synthesisof fatty acids required for proliferating cells. Increasing mitochondrialfunction by promoting flux into the mitochondria has shown promiseas an anticancer strategy (see text). This can be done directly withPDK inhibitors like DCA (4), or indirectly with LDH inhibitors (shunt-ing pyruvate into the mitochondria) (3), PKM2 inhibitors (increasingpyruvate synthesis) (2), FAS inhibitors (5), and FAO inhibitors (6)(stimulate GO via the Randle cycle). Strategies that inhibit glycolysis(1) result in rapid depletion of cellular ATP and exhibit a lack of selec-tivity to cancer cells.
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
Heart Metab. (2011) 51:20–26 21

mitochondria would increase MTP opening thresh-olds, suppress mROS, inhibit Kv-channels, and acti-vate HIF1α and NFAT, all promoting a proliferative andanti-apoptotic state.
Mitochondria as integrators of early genetic
and environmental signals in cancer
A number of common molecular abnormalitiesdescribed in cancer have direct metabolic and mito-chondrial effects that result in suppressed oxidativephosphorylation and mitochondrial function. Forexample, p53 loss-of-function, cancer’s most com-mon genetic anomaly, strongly promotes a glycolyticphenotype by upregulating glycolytic enzymes includ-ing phosphoglycerate mutase and the rate-limitingenzyme hexokinase (HK) [4]. p53 also regulates Tp53-induced glycolysis and apoptosis regulator (TIGAR),an enzyme with fructose-2,6-bisphosphatase activity[2]. When suppressed, fructose-2,6-bisphosphateaccumulates and potently simulates the rate-limitingglycolytic enzyme phosphofructokinase-1. Moreoverp53 regulates the expression of the ETC proteincytochrome-c oxidase and suppresses the expressionof glucose transporters (GLUTs) [2]. Thus, as a result ofp53 loss-of-function, ATP supply is maintained byelevated cytoplasmic glycolysis and glucose uptake,compatible with the increased 18-fluorodeoxyglucosepositron emission tomography (PET) signal in mosttumors compared to non-cancerous tissues.
Similarly, activation of Akt (or PTEN loss-of-function)not only enhances the activity of rate limiting glycolyticenzymes but also translocates GLUTs to the cell mem-brane. c-myc upregulates nearly all glycolytic enzymesincluding Hk [4, 5]. Intriguingly, in addition to regulatingcarbohydrate metabolism, several cytoplasmic glyco-lytic enzymes directly suppress apoptosis [5] or evenmodulate mitochondrial function. For example, acti-vated Hk translocates to the outer mitochondrial mem-brane and binds the voltage-dependent anion channel(VDAC) [6]. This prevents anion efflux contributing tothe ΔΨm hyperpolarization that characterizes mostcancers [7] and prevents MTP opening [6].
Mitochondrial enzyme mutations also impair mito-chondrial function and promote a glycolytic pheno-type. The Krebs’ cycle enzymes succinate dehydro-genase (SDH) [8], fumarate hydratase (FH) [9] andisocitrate dehydrogenase (IDH) [10, 11] are all associ-
ated with cancers like renal cell carcinoma, paragan-gliomas, or glioblastomas.
Thus, mitochondria appear to integrate a largenumber of diverse genetic signals that all result in acommon phenotype (i.e., hyperpolarized mitochondriawith suppressed function, upregulated glycolysis andsecondary signaling consequences) promoting prolif-eration and suppressing apoptosis. The evolving met-abolic theory of cancer that suggests that the mito-chondrial and metabolic remodeling promotes a pro-proliferative and apoptosis-resistant state is compati-ble with the genetic theory of cancer that has domi-nated the field for forty years but has failed to delivereffective and selective cancer therapies (except fewand isolated examples, such as imatinib mesylate).
Actively suppressed mitochondria are also compat-ible with the evolutionary model of cancer, which sug-gests that early carcinogenesis is hypoxia-driven [12].Here, decreased oxygen suppresses respiration andlimits proton influx through ATP synthase. This wouldresult in mitochondrial hyperpolarization and subse-quent mitochondria-dependent metabolic signalingand apoptosis suppression. HIF1α facilitates a shiftfrom mitochondrial oxidation to glycolysis, whichensures ATP production even in sustained hypoxia[12]. In addition to upregulating GLUTs, HIF1α upregu-lates pyruvate dehydrogenase kinase (PDK), theenzyme that tonically inhibits PDH, limiting pyruvateflux into the mitochondria (Fig. 1). When angiogenesisoccurs and tumor oxygen delivery is restored, theupregulated PDK maintains mitochondrial suppres-sion, and at this point, loss of secondary mitochondrialsignals (mROS, αKG) sustains HIF1α even in theabsence of hypoxia, maintaining a glycolytic state.
Mitochondrial suppression in cancer may have pro-proliferative effects in addition to the apoptosis inhibi-tion and HIF1α driven angiogenesis. Metabolitesthat are now not oxidized in the mitochondria areshifted toward biosynthetic pathways important forrapidly proliferating cells [13]. For instance, glucose-6-phosphate (the product of Hk) can be shunted intothe pentose phosphate pathway (PPP) wherebyribulose-5-phosphate is produced for nucleotide syn-thesis (Fig. 1). This pathway also produces NADPH,which protects against oxidative stress and is used inde novo lipid and amino acid synthesis [13]. Thus thebeneficial effects of an overall mitochondrial suppres-sion in cancer may extend to multiple levels.
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
22 Heart Metab. (2011) 51:20–26

Mitochondrial activators in cancer
Not surprisingly, therapies targeting single genetic ormolecular abnormalities are ineffective in most can-cers, which are commonly heterogeneous in nature.For example, there is significant diversity in glioblas-toma multiform (GBM), where a given tumor includesmultiple abnormalities and therefore is unlikely torespond to single target strategies [14]. A common fea-ture among all GBM (and most solid tumor) cells is met-abolic remodeling. In the 1920s, Warburg suggestedthat this feature of most cancers is caused by abnormalmitochondria. However, his theory was dismissed andmost considered mitochondria inhibition as a second-ary effect, possibly a result of oxidative damage.
DCA and preclinical studies
Recently, we showed that cancer cells treated withdichloroacetate (DCA), a PDK inhibitor (and thus aPDH activator), acutely increased GO [15]. BecauseGO occurs exclusively in the mitochondria, thesedata suggested that cancer mitochondria are perhapsfunctionally and reversibly suppressed, not perma-nently damaged, providing strong rationale for thedevelopment of similar drugs as novel cancer thera-pies. We first published the preclinical effects of DCAin cancer in 2007. We found that non-small cell lung,breast and GBM cancer cells had hyperpolarized ΔΨmcompared to non-cancerous cells and that DCA rap-idly depolarized mitochondria to normal levels, sug-gesting restoration of mitochondrial function [15]. Inkeeping with this, DCA decreased the glycolysis toGO ratio by enhancing GO and lowering lactate pro-duction. DCA induced mitochondria-dependent apo-ptosis and reduced proliferation both in vitro and invivo [15]. DCA-treated cancer cells had increasedmROS, activated Kv-channels and inhibited NFAT.Importantly, DCA did not affect mitochondria andtheir downstream targets in non-cancerous cells.DCA also decreased tumor size in a xenotransplantmodel (Fig. 2). Since then, many independent studieshave confirmed our findings (reviewed in [16]) in colon[17], prostate [18], endometrial [19] or metastaticbreast cancer [20]. In vivo, DCA was effective inattenuating aggressive metastatic breast cancer[20] (Fig. 2). In another study, DCA was chemicallylinked to cisplatin, a commonly used cancer drugthat induces DNA cross-linking [21]. This newmolecule, mitaplatin, was cancer selective, inducing
mitochondrial-dependent apoptosis and reversing theapoptosis resistance that limits cisplatin’s effectiveness.
DCA and early clinical experience
DCA has been used clinically for decades to symptom-atically treat congenital mitochondrial diseases includ-ing PDH deficiencies and their resulting lactic acidosis.This, along with promising pre-clinical findings pro-vided the rationale for early phase clinical trials in can-cer. The first such study was recently published exam-ining DCA’s effects in GBM, a highly vascular anddeadly brain cancer [22]. Examination of 49 freshlyexcised tumors showed mitochondrial hyperpolariza-tion compared to non-cancerous brain tissue, whichwas reversed with acute DCA, supporting reversiblemitochondrial inactivation in this tumor. The tumorsshowed high PDK2 expression, the most DCA-sensitive PDK isoform [23] (Fig. 3a). DCA was orallyadministered to five (previously treated) patients at adose of 6.25mg/kg bid giving plasma concentrationsof 0.266-0.626mM after at least three months,well within the range for PDK2 inhibition (Ki=0.2mM[23]). Importantly, none of the patients developedhematologic, hepatic, renal or cardiac toxicity. Periph-eral neuropathy was the only apparent toxicity, which
CT scan
Con
trol
∆Ψm PET Lung Metastasis
DC
A-t
reat
ed
Human non-smallcell lung cancer cells
Human non-small cell lungcancer xenotransplant model
Human breast cancerxenotransplant model
Fig. 2 Metabolic modulation of human cancers with dichloroace-tate depolarizes mitochondria and reduces tumor growth andmetastases in vivo. Human non-small cell lung cancer cells stainedwith the ΔΨm-sensitive dye (TMRM- red) and nuclear stain (Dapi-blue). Acute administration of DCA depolarizes ΔΨm, as measuredby a reduction in TMRM stain (left panel). Oral administration of DCAreduces tumor size (CT) and glucose uptake (18FDG-PET) in humannon-small cell lung cancer xenotransplant rat model (middle panel)(Modified with permission from [34]). Oral administration of DCAreduces lung metastases in a xenotransplant model with humanmammary carcinoma (right panel) (Modified with permissionfrom [20]).
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
Heart Metab. (2011) 51:20–26 23

was reversed at lower doses. This study’s majorstrength was comparing tumor tissue obtained beforeand after DCA therapy. Post-DCA, tumor tissuesexhibited higher PDH activity, confirming PDK2 inhibi-tion in vivo. Further examination revealed p53 activa-tion, HIF1α inactivation and decreased vascularity.Moreover, the tumors were less proliferative, moreapoptotic (Fig. 3a) and some, but not all, showed evi-dence of regression or stability (Fig. 3b) [22]. Evenmore exciting was the apparent effects on putativeGBM stem cells (GBM-SC; CD133+/Nestin+), whichare the most apoptosis-resistant cells and the causeof recurrence after remission. In line with this, the
GBM-SC had the highest ΔΨm within the tumor invivo. DCA induced apoptosis in these cells in vitro(Fig. 3c) and in vivo, suggesting that this traditionallyresilient population is also metabolically vulnerable [22].
Lactate dehydrogenase
LDH-A, a downstream target of HIF1α[3], convertspyruvate into lactate, restoring NAD+ to sustain glycoly-sis and preventing pyruvate oxidation. Inhibition ofLDH-A may restore mitochondrial function by promot-ingmitochondrial pyruvate metabolism, in a sensemim-icking DCA (Fig. 1). LDH-A inhibition decreases lactate,depolarizes mitochondria, increases respiration and
PDKII is higly expressed in human GBMDCA reduces proliferation
a
b cDCA stabilises a patient with advanced GBM
DCA induces apoptosis in putativepatient+dericed GBM stem cells
Pos
t-D
CA
Pre
-DC
A
Pos
t-D
CA
Pre
-DC
A
Pos
t-D
CA
Pre
-DC
A
DCA induces apoptosis in human GBM
TUNEL
CD133 NESTINPET-MRI MERGE
BASELINE
Surgery(x2)+DCA
+ 15 MONTHS
PET-MRI MERGE TUNEL MERGE
+DAPIPDKII PCNA MERGE+DAPI
100 µm 100 µm
20 µm
Fig. 3 Metabolic modulation with DCA attenuates proliferation and induces apoptosis in human GBM tissue and putative human GBM-SC, resulting in clinical stabilization in some patients. (a) Representative images of human GBM tissue taken before and after chronic oralDCA administration. DCA reduces proliferation (PCNA-red) and cell density (nuclei-blue). GBM tumors maintain high levels of PDKII that areexpressed throughout the tumor, even after DCA, suggesting maintained efficacy during chronic use (left panel). DCA induces apoptosis(TUNEL-green) in GBM tissue (right panel). (b) T1 axial MRI superimposed with 18FDG-PET scan in a GBM patient. Note the elevatedof 18FDG uptake in the tumor compared to non-cancerous brain tissue, indicating a high reliance on glucose. After two debulking surgerieswith concurrent DCA therapy for 15 months, there was a significant reduction in tumor size and FDG-PET signal intensity (arrows). (c) DCAinduces apoptosis (TUNEL-green) in human CD133+ (purple)/Nestin+(red) GBM-SC clusters, suggesting that this classically apoptosis-resistant population of cells is susceptible to metabolism-based therapies (modified with permission from [22]).
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
24 Heart Metab. (2011) 51:20–26

decreases proliferation in cancer cells [24, 25]. Animalsinjected with LDH-A-knockdown cancer cells had smal-ler tumors and improved survival [24], and inhibition ofLDH-A reduced tumor volumes in lymphoma and pan-creatic xenotransplant models without kidney, liver orblood toxicity [25]. These promising preclinical resultsand the relative selectivity for cancer suggest LDH-Ainhibitors may be a viable therapeutic intervention.
Pyruvate kinase M2 (PKM2)
Conversion of phosphoenol-pyruvate to pyruvateoccurs as the final rate-limiting glycolytic step. Thisreaction is catalyzed by pyruvate kinase, which existsin high (PKM1) and low activity (PKM2) isoforms. Therecent identification of PKM2 has generated excite-ment since this isoform is selective to rapidly proliferat-ing cells [13]. Although it appears paradoxical, this low-activity isoform may actually promote proliferation byreducing ATP production (preventing allosteric inhibi-tion of prior glycolytic reactions) and shunting metabo-lites into biosynthetic pathways [13, 26]. PKM2 wouldalso reduce mitochondrial pyruvate influx (Fig. 1). Thus,targeting PKM2 not only reduces biosynthetic pro-cesses, but may also promote GO, similar to DCA.Indeed, inhibition of PKM2 increases oxygen consump-tion in some cancers and limits tumor growth in xeno-transplant models [27]. The PKM2 data are compatiblewith the PDH/DCA work and the idea of an overallsuppression of mitochondrial function in cancer.
Fatty acid metabolism inhibitors
Cancer’s highly proliferative nature creates a largedemand for fatty acids for membrane synthesis. Ratherthan extracellular sources, cancer obtains fatty acids viade novo synthesis from the Krebs’ cycle intermediatecitrate [28]. Citrate is upstream of many Krebs’ cycleenzyme mutations commonly associated with canceras described above. Mutations in these enzymeswould lead to accumulation of upstream metabolites(i.e., citrate) for biosynthetic purposes (Fig. 1). Inhibitionof several fatty acid biosynthetic steps has shown effi-cacy in preclinical cancer models [29, 30]. Intriguingly,fatty acid oxidation (FAO) inhibition also inhibits cancergrowth [31], as it indirectly promotes GO through theRandle cycle (i.e. FAO-generated acetyl-CoA inhibitsPDH) [32]. In other words, this strategy is similar toDCA in terms of “refueling” mitochondria with pyruvateand reversing the mitochondrial suppression and thesecondary upregulation of glycolysis.
Glycolysis inhibitors
Cancer’s glycolytic environment provides sufficientenergy and building blocks for proliferation while simul-taneously suppressing apoptosis. Although direct gly-colysis inhibition seems logical, this strategy rapidly(and predictably) depletes ATP causing ATP-independent (necrotic) cell death, which is likely todamage non-cancerous tissues as well. Inhibiting gly-colysis may not be selective since non-cancerous tis-sues (i.e., skeletal muscle, brain, etc.) also rely on gly-colysis. In fact, several recent clinical trials of glycolysisinhibitors have not been successfully completed.Clinical trials for 2-deoxyglucose (Hk inhibitor) forprostate cancer (NCT00633087) and intracranialneoplasms (NCT00247403) have been suspended.Phase II/III trials for the Hk-inhibitor lonidamine inbenign prostate hyperplasia have also been termi-nated (NCT00435448, NCT00237536). Another Hkinhibitor, 3-bromopyruvate, which pre-clinical worksuggests induces necrosis in cancer, has also demon-strated significant toxicities in animal models at dosesonly slightly higher than therapeutic doses[33]. In otherwords, the non-selectivity of these drugs may limit theirtranslational potential. In summary, the metabolicmodulators that improve coupling between glycolysisand GO, “refueling” mitochondria and “normalizing”remodeled metabolism should not be confused withglycolysis inhibitors, which rather than normalizemetabolism, cause energy starvation (Fig. 1).
Conclusions
Revisiting Warburg’s original hypothesis that abnormalmetabolism causes cancer has provided newfoundoptimism. Once thought to be a secondary result ofupstream abnormalities, it now appears that cancer’smetabolic remodeling is integral for survival andexposes many therapeutic targets. Various strategiesthat restore mitochondrial metabolism have shownselectivity and efficacy in pre-clinical studies andneed to efficiently be moved into clinical trials. ●
References
1. Zamzami N, Kroemer G (2001) The mitochondrion in apopto-sis: how Pandora’s box opens. Nat Rev Mol Cell Biol 2:67–71
2. Vousden KH, Ryan KM (2009) p53 and metabolism. Nat RevCancer 9:691–700
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
Heart Metab. (2011) 51:20–26 25

3. Dromparis P, Sutendra G, Michelakis ED (2010) The role ofmitochondria in pulmonary vascular remodeling. J Mol Med88:1003–1010
4. Kim JW, Dang CV (2006) Cancer’s molecular sweet tooth andthe Warburg effect. Cancer Res 66:8927–8930
5. Kim JW, Dang CV (2005) Multifaceted roles of glycolyticenzymes. Trends Biochem Sci 30:142–150
6. Pastorino JG, Hoek JB, Shulga N (2005) Activation of glyco-gen synthase kinase 3beta disrupts the binding of hexokinaseII to mitochondria by phosphorylating voltage-dependentanion channel and potentiates chemotherapy-induced cyto-toxicity. Cancer Res 65:10545–10554
7. Chen LB (1988) Mitochondrial membrane potential in livingcells. Annu Rev Cell Biol 4:155–181
8. Douwes Dekker PB, Hogendoorn PC, Kuipers-Dijkshoorn N,Prins FA, van Duinen SG, Taschner PE, van der Mey AG, Cor-nelisse CJ (2003) SDHD mutations in head and neck paragan-gliomas result in destabilization of complex II in the mitochon-drial respiratory chain with loss of enzymatic activity andabnormal mitochondrial morphology. J Pathol 201:480–486
9. Tomlinson IP, Alam NA, Rowan AJ, Barclay E, Jaeger EE, Kel-sell D, Leigh I, Gorman P, Lamlum H, Rahman S, RoylanceRR, Olpin S, Bevan S, Barker K, Hearle N, Houlston RS,Kiuru M, Lehtonen R, Karhu A, Vilkki S, Laiho P, Eklund C,Vierimaa O, Aittomaki K, Hietala M, Sistonen P, Paetau A, Sal-ovaara R, Herva R, Launonen V, Aaltonen LA (2002) Germlinemutations in FH predispose to dominantly inherited uterinefibroids, skin leiomyomata and papillary renal cell cancer. NatGenet 30:406–410
10. Dang L, White DW, Gross S, Bennett BD, Bittinger MA, Drig-gers EM, Fantin VR, Jang HG, Jin S, Keenan MC, Marks KM,Prins RM, Ward PS, Yen KE, Liau LM, Rabinowitz JD, CantleyLC, Thompson CB, Vander Heiden MG, Su SM (2009)Cancer-associated IDH1 mutations produce 2-hydroxy-glutarate. Nature 462:739–744
11. Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, YuanW, Kos I, Batinic-Haberle I, Jones S, Riggins GJ, Friedman H,Friedman A, Reardon D, Herndon J, Kinzler KW, VelculescuVE, Vogelstein B, Bigner DD (2009) IDH1 and IDH2 mutationsin gliomas. N Engl J Med 360:765–773
12. Gatenby RA, Gillies RJ (2004) Why do cancers have highaerobic glycolysis? Nat Rev Cancer 4:891–899
13. Vander Heiden MG, Cantley LC, Thompson CB (2009) Under-standing the Warburg effect: the metabolic requirements ofcell proliferation. Science 324:1029–1033
14. Wen PY, Kesari S (2008) Malignant gliomas in adults. N Engl JMed 359:492–507
15. Bonnet S, Archer SL, Allalunis-Turner J, Haromy A, BeaulieuC, Thompson R, Lee CT, Lopaschuk GD, Puttagunta L, HarryG, Hashimoto K, Porter CJ, Andrade MA, Thebaud B, Miche-lakis ED (2007) A mitochondria-K+ channel axis is suppressedin cancer and its normalization promotes apoptosis and inhi-bits cancer growth. Cancer Cell 11:37–51
16. Papandreou I, Goliasova T, Denko NC (2010) Anticancerdrugs that target metabolism: Is dichloroacetate the new par-adigm? Int J Cancer 128:1001–1008
17. Madhok BM, Yeluri S, Perry SL, Hughes TA, Jayne DG (2010)Dichloroacetate induces apoptosis and cell-cycle arrest incolorectal cancer cells. Br J Cancer 102:1746–1752
18. Cao W, Yacoub S, Shiverick KT, Namiki K, Sakai Y, PorvasnikS, Urbanek C, Rosser CJ (2008) Dichloroacetate (DCA) sensi-tizes both wild-type and over expressing Bcl-2 prostate can-cer cells in vitro to radiation. Prostate 68:1223–1231
19. Wong JY, Huggins GS, Debidda M, Munshi NC, De Vivo I(2008) Dichloroacetate induces apoptosis in endometrial can-cer cells. Gynecol Oncol 109:394–402
20. Sun RC, Fadia M, Dahlstrom JE, Parish CR, Board PG, Black-burn AC (2010) Reversal of the glycolytic phenotype bydichloroacetate inhibits metastatic breast cancer cell growthin vitro and in vivo. Breast Cancer Res Treat 120:253–260
21. Dhar S, Lippard SJ (2009) Mitaplatin, a potent fusion of cis-platin and the orphan drug dichloroacetate. Proc Natl AcadSci U S A 106:22199–22204
22. Michelakis ED, Sutendra G, Dromparis P, Webster L, HaromyA, Niven E, Maguire C, Gammer TL, Mackey JR, Fulton D,Abdulkarim B, McMurtry MS, Petruk KC (2010) Metabolicmodulation of glioblastoma with dichloroacetate. Sci TranslMed 2:31ra34
23. Bowker-Kinley MM, Davis WI, Wu P, Harris RA, Popov KM(1998) Evidence for existence of tissue-specific regulation ofthe mammalian pyruvate dehydrogenase complex. BiochemJ 329 (Pt 1):191–196
24. Fantin VR, St-Pierre J, Leder P (2006) Attenuation of LDH-Aexpression uncovers a link between glycolysis, mitochondrialphysiology, and tumor maintenance. Cancer Cell 9:425–434
25. Le A, Cooper CR, Gouw AM, Dinavahi R, Maitra A, Deck LM,Royer RE, Vander Jagt DL, Semenza GL, Dang CV (2010)Inhibition of lactate dehydrogenase A induces oxidative stressand inhibits tumor progression. Proc Natl Acad Sci U S A107:2037–2042
26. Vander Heiden MG, Locasale JW, Swanson KD, Sharfi H, Hef-fron GJ, Amador-Noguez D, Christofk HR, Wagner G, Rabino-witz JD, Asara JM, Cantley LC (2010) Evidence for an alterna-tive glycolytic pathway in rapidly proliferating cells. Science329:1492–1499
27. Christofk HR, Vander Heiden MG, Harris MH, Ramanathan A,Gerszten RE, Wei R, Fleming MD, Schreiber SL, Cantley LC(2008) The M2 splice isoform of pyruvate kinase is importantfor cancer metabolism and tumour growth. Nature 452:230–233
28. Deberardinis RJ, Sayed N, Ditsworth D, Thompson CB (2008)Brick by brick: metabolism and tumor cell growth. Curr OpinGenet Dev 18:54–61
29. Hatzivassiliou G, Zhao F, Bauer DE, Andreadis C, Shaw AN,Dhanak D, Hingorani SR, Tuveson DA, Thompson CB (2005)ATP citrate lyase inhibition can suppress tumor cell growth.Cancer Cell 8:311–321
30. Pizer ES, Thupari J, Han WF, Pinn ML, Chrest FJ, FrehywotGL, Townsend CA, Kuhajda FP (2000) Malonyl-coenzyme-Ais a potential mediator of cytotoxicity induced by fatty-acidsynthase inhibition in human breast cancer cells and xeno-grafts. Cancer Res 60:213–218
31. Samudio I, Harmancey R, Fiegl M, Kantarjian H, Konopleva M,Korchin B, Kaluarachchi K, Bornmann W, Duvvuri S, Taegt-meyer H, Andreeff M (2010) Pharmacologic inhibition of fattyacid oxidation sensitizes human leukemia cells to apoptosisinduction. J Clin Invest 120:142–156
32. Randle PJ (1998) Regulatory interactions between lipids andcarbohydrates: the glucose fatty acid cycle after 35 years. Dia-betes Metab Rev 14:263–283
33. Chang JM, Chung JW, Jae HJ, Eh H, Son KR, Lee KC, ParkJH (2007) Local toxicity of hepatic arterial infusion of hexo-kinase II inhibitor, 3-bromopyruvate: In vivo investigation innormal rabbit model. Acad Radiol 14:85–92
34. Michelakis ED, Webster L, Mackey JR (2008) Dichloroacetate(DCA) as a potential metabolic-targeting therapy for cancer.Br J Cancer 99:989–994
NEW THERAPEUTIC APPROACHES - PETER DROMPARIS
26 Heart Metab. (2011) 51:20–26