Merrily Evdokimoff, RN, PHD Sylena Keeping, RN, MSN, … 1030... · Oxford Dictionary 23 ......
96
Merrily Evdokimoff, RN, PHD Sylena Keeping, RN, MSN, MBA Paula McCartney, RN, BS Geri McCallig, BSN Valerie Donnelly, RN,MS Susan White, RN 1 DONNELLY & ASSOCIATES International Health Care Management Consultants Steering the Course to Quality Improvement
Transcript of Merrily Evdokimoff, RN, PHD Sylena Keeping, RN, MSN, … 1030... · Oxford Dictionary 23 ......
Merrily Evdokimoff, RN, PHD Sylena Keeping, RN, MSN, MBA
Paula McCartney, RN, BS Geri McCallig, BSN
Valerie Donnelly, RN,MS Susan White, RN
1
DONNELLY & ASSOCIATESInternational Health Care Management ConsultantsSteering the Course to Quality Improvement
At the conclusion of the program, the participant will be able to:
1. Identify challenges in recruiting/retention within the current health care climate.
2. List critical components of a successful recruitment/retention program
3. Identify “critical thinking” competencies as well as procedural competencies included in a comprehensive employee orientation program.
2

According to the AACN, “the purpose of the new grad is to provide holistic, compassionate care based on a foundation, among others, of altruism, ethics, honesty, integrity, and teamwork.”
AACN. (2016, Feb 3). The essentials of baccalaureate nursing education for professional nursing practice. Retrieved from the American Association of Colleges of Nursing.
3
4
Nursing Shortage
Competitive environment
New grads , no jobs
Inexperienced applicants
Turnover rate 19%
Most were inexperienced in the field of Home Health
Job Satisfaction
Mentoring
Leadership Interest
In-depth Orientation
Lartey, Cummings & Profetto-McGrath, J. (2014). Interventions that promote retention of experienced registered nurses in health care settings: a systematic review. Journal Of Nursing Management22(8), 1027-1041. 6
Complexity
Complex knowledge base as generalist
Expansive competencies required
Uncontrolled environment
Autonomy
Critical Thinking (problem solving)
7
Home Care Values (Smith-Toner & Markley, 2007)
Home care nurse values (autonomy, team, professionalism, fair wages)
Teamwork
Leadership
Care co-ordination
Communication
Resource Allocation
8
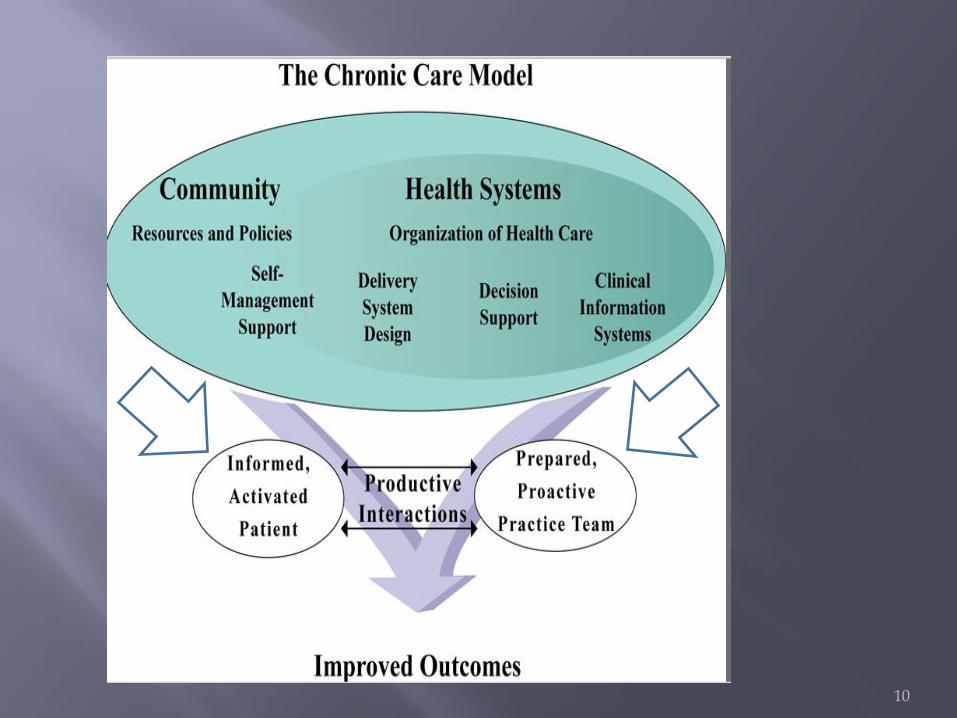
Chronic Care Model
Critical Thinking
Coleman’s Transitional Care Model
Evidence Based Practice Guidelines
Benner’s Novice to Expert
(Summary of Generational ….)
9
10
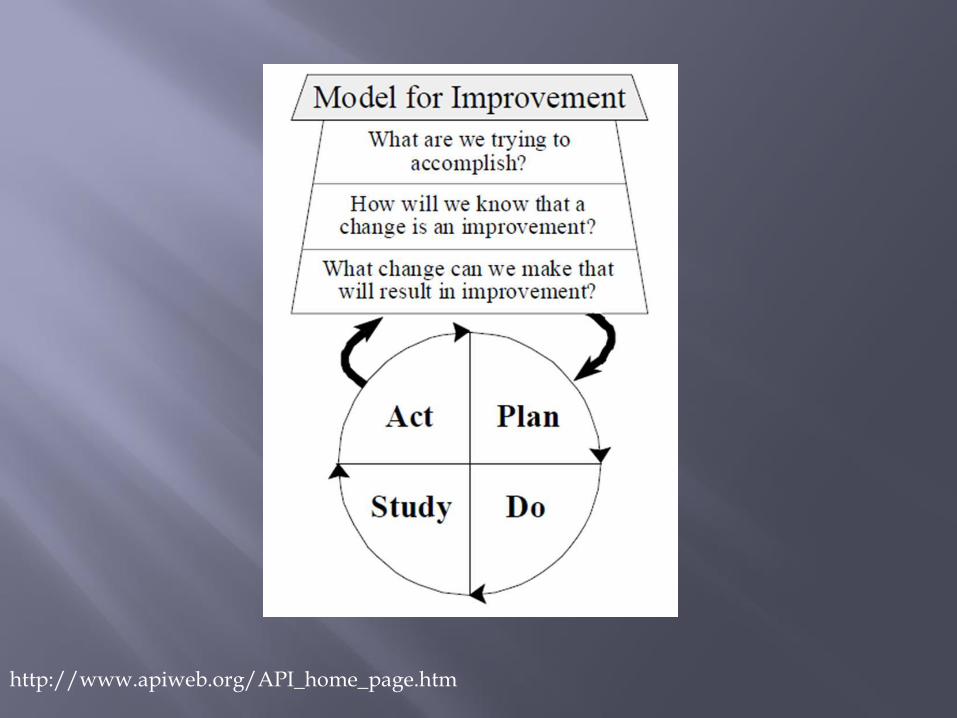
http://www.apiweb.org/API_home_page.htm

1. What surprises me?
2. What puzzles me?
3. Do you see any patterns or themes emerge?
4. Anything you should know immediately?
5. What things can wait?
6. Does anything else come to mind?
12

1. Medication Self-Management
2. Patient Centered Health Record
3. Early, consistent communication with PCP/Specialists
4. Red Flags

Coaching
Motivational Interviewing (MI)
Teach Back
SBAR for Patients/Families
Use of Health Literacy Principles
Use of Personal Health Record
Identification of Patient Self-Management goals by patient/family
Use of Adult Learning Principles
14
Sustaining critical thinking Relationship of clinical and didactic OASIS as an integral part of the assessment
process Value of supportive, non-blaming environment:
Just Culture Use of environment to support learning
(managers teach, simultaneous didactic and clinical
Based on principles of adult learning
15

Safe environment
Learning organization
Mistakes may occur-how handled-non blaming environment
Whole agency must buy in to program and support of new staff
16

“Organizations where people continually expand their capacity to create the results they truly desire, where new and expansive patterns of thinking are nurtured, where collective aspiration is set free, and where people are continually learning to see the whole together.”
Peter Senge

Systems thinking
Personal mastery
Mental models
Building shared vision
Team learning
Quality
Outcomes
Service
Waste
Front Line is where the answer is
Team approach
Respect for all individuals on team
Power of the individual
Cut waste!
Sharing.
Open, respectful, and informed conversation is central.

“Understanding caring as a practice, rather than as pure sentiment or attitudes apart from the practice,
reveals the knowledge and skill that excellent caring requires.”
(Benner, 1984)
The central and most important part of an object, movement, or group, forming the basis for its activity and growth
Oxford Dictionary
23

EBP is traditionally defined in terms of a "three legged stool" integrating three basic principles: (1) the best available research evidence bearing on whether and why a treatment works, (2) clinical expertise (clinical judgment and experience) to rapidly identify each patient's unique health state and diagnosis, their individual risks and benefits of potential interventions, and (3) client preferences and values.
(Wikipedia, 2016)
24

25
Nursing leaders need to be aware of the differences in nurse’s age groups when planning transition programs. It is important to recognize and be aware of the benefits of each age group and that this diversity leads to a broader perspective of nursing care.

Birth Year Current Age Range
% of Current Workforce
Matures 1922-1943 69-90 5%
Baby Boomers 1943-1960 52-69 45%
Generation X 1960-1980 32-52 40%
Millennials 1980-2000 12-32 10%
27
McNeill, 2012
Tech Knowledge
Social Skills
Work Mentality
Creativity
Energy
Knowledge Mastery
Recognizing the importance of cultural competence in our caregivers
Engagement in culture specific education and competency testing prior to patient contact
Cultural competency and linguistic training
Utilization of in house, community, and phone interpreters 24/7 to facilitate clear communication
“The principle of respect for persons extends to all individuals with whom the nurse interacts. The nurse maintains compassionate and caring relationships with colleagues and others with a commitment to fair treatment of individuals, to integrity preserving compromise, and to resolving conflict.”
(ANA, 2001.)

5 levels of nursing experience
Novice
Advanced Beginner
Competent
Proficient
Expert
(Benner, 2011)
“Understanding the five stages of competence can help nurses support one another and appreciate
that expertise in any practice depends on experiential, situated learning over time.”
(Saver, C, 2013)
Novice
“The phrase technical understanding refers to an assumption that all action can be determined through explicitly stated theories and directives.” (Benner, 1984)
No Experience
Has general rules that are applied universally
Behavior is rule governed and inflexible
(Benner, 2011)
Advanced Beginner
Has gained prior experience in actual situations
Rules begin to be applied based on experiences
Demonstrates ability to be proficient
(Benner, 2011)
Competent
More aware of long term goals
Gains perspective from planning own actions based on correlations of principles and outcomes
Displays higher level of organization and efficiency
(Benner, 2011)

Proficient
Holistic understanding: sees the whole picture
Knows from experience what to expect and tailors plans accordingly
Perceives deviations from the normal pattern
Sees what is most important in a situation
Decision-making is easier
Lester, (2005) (Benner, 2011)

Expert
No longer relies on rules to determine actions
Has an intuitive grasp
Performance is fluid, flexible and highly proficient

Recruitment
Managers
Preceptors
Orientation: Didactic/Clinical
38
Four Legs of A Successful Program

39

Welcome!
Assimilate into culture of the agency
Develop critical thinking & clinical judgment
Expand clinical skills
Refine time management and setting priorities
Teach COPs and agency Policies/Procedures
Develop excellent documentation
40

41
Choosing the Right Preceptors Educator, Clinical Managers, Quality collaborate
Qualifications
Seasoned RNs who meet standards:
Excellent Clinical skills
Good Clinical Documentation, including OASIS
Knowledgeable re: COPs
Knowledge of and demonstrated compliance re: agency policies and procedures
MOTIVATED to participate in the program
42

Set the expectation that all staff are to act as mentors / support system for new staff
eeeeeeeeeeee
Individual meeting with each potential preceptor to discuss willingness and motivation to participate
Consideration given on preceptors’ assignment / productivity to allow time to teach
43

No more than 2 weeks before Orienteesarrive
One Class: Didactic & Discussion
Overview of the orientation program Expectations of the preceptor and orientee
roles
Principles of adult education
How to give constructive feedback
Novice to Expert
44
45
New Grads
Rigorous process including application, resume, letter of interest, 3 references, transcripts, panel interviews
Nurses New to Home Care
Applications on line, resume, interview
46
Agency Orientation with HR
Clinical Orientation with Education
Joint Visits with Preceptors
Begin prior to didactic and continue throughout classes
Give context to classes
Allow immediate application of new material
47

48
Workshops to develop clinical skills
Wound Care with WOCN
Compression wraps
Venipuncture
CVAD
Pharmacology Education
Interspersed with didactic classes and practiced with preceptor oversight in the field
49

50
Joint visits with Education Staff and Clinical Managers
Assess progress
“Fine tune” skills
“Sign off” on clinical skills
51
Weekly feedback from Preceptors and Orientees
Designed to identify any needs we could address
Learning needs
Interpersonal needs
Emotional needs
52
53
What was the best thing that happened this week? What made it a great experience?
What progress is your orientee making toward skills / documentation?
Did you experience any difficulties this week, either clinical or nonclinical?
What support did you receive to make it a positive learning experience?
What goals is your orientee working on for next week?
Is there anything else you would like us to know or that we can do to help you?
54

What was the best thing that happened this week? What made it a great experience?
What types of patients did you care for this week? What skills did you see or do?
Did you experience any difficulties this week, either clinical or nonclinical?
What support did you receive to make it a positive learning experience?
Who was your preceptor this week? What are your goals for next week? Is there anything else you would like us to know
or that we can do to help you?
55

Monthly support meetings
With Educator – No Managers or Preceptors
Time for New Grads to talk freely about challenges, successes, frustrations
Learn from one another
Motivate and support one another
56
57
Resolve went into effect October 15th, 2015
COR Health 1st Agency in the State of Maine under the new law to receive
approval for a new grad RN preceptor program

Private Duty Nursing
Pediatric Care of Medically Complex Children
58

Provide new grads tools and resources needed to provide quality home care
Seek to “raise the bar”
Evidence based program
Expert clinical guidance
Offers a pediatric core curriculum
New Grads and Return to Work RNs
1:1 mentor for 6 months-1 year
Individualized Learning Plan
60
Experienced RNs who are new to home care receive components of the program
Pediatric Training Component
Skills competency
Specialized 1:1 Orientation to client specific needs
Experienced RNs assigned to a new client
Skills competency
Specialized 1:1 orientation to client specific needs
61

62
Promotes full consideration of the physical, psychological, financial, emotional, cultural, and social well being of our clients.
Inclusion of family members and other home and community supports
Recognizes that “health” is more than freedom from disease & clients are more than a diagnosis.

Introduce to home health care
Integrate into culture/organizational structure
485 development
Critical thinking
Ensure compliance
Provide pediatric foundation
Develop competencies
Improve communications
64

Agency Orientation
Home Health Orientation
Interdisciplinary
Pediatric Specific Training
Client Specific Competencies
CEU Requirements
Mandated Learning Sessions
Didactic Component
1:1 Preceptor in the Field (6-12 months)
65
Resource Intensive Investment
Oversight/Implementation
Preceptor Selection and Training
Application/Selection of Program Participants
Matriculation/Support
Regular Review Sessions & Goal Setting
Evidence Based Procedures
Standardized Skill Demonstrations
66

67

68

69
Visits with Preceptor
Visits with Clinical Specialists
Rotation through Departments
70
Clinical: AM
2-3 hours
3 x/week
Outsourced
C
Didactic Lecture: PM
Closing Discussion Conducted by Education Co-ordinator
• Home Care Uniqueness• COP’s• Communication• Assessment• Care Planning/Critical Thinking• Case Management/Collaboration• Performance Improvement /OBQI,
OBQM• Putting the Pieces Together
71
Agency organization
Nurses’ role in agency operations
Professional Boundaries
Advocacy
Autonomy
72
Patient Care:
Loss of control over environment – guest in patient’s home
Negotiated autonomy
Patient self determination
Emphasis on patient/caregiver Self-Care
Special Challenges :
Pets
Hoarding
73
Skilled need and medical necessity
Doctor’s orders
Scope of Home Health services
Intermittent Care
Medicare Benefit versus other payers
DPH
Certifying organizations and their roles
74

Motivational Interviewing
Written and verbal communication
Telephone communication - SBAR
Teach Back
Adult Learning Principles
75
OASIS/485
Admission visit
Assessments at all OASIS time points
Assessments on each re-visit
Documentation
76
Historical importance of OASIS
Integration of OASIS data and physical assessments
Basis of care planning/development of 485
Emphasis on data collection, process and end-result outcomes
Importance to agency financial outcomes
Areas of focus: Systems reviews
Functional limitations
Ability of patient to achieve self management
77
Care Planning - Characteristics of a Critical Thinker
Reflection – use of assessment data, weighing facts
Problem solving based on reasons- not prejudice, preference or fears
Intellectual skills – theory, knowledge
An inquiring attitude
Fairness without bias
Independent or autonomous thinking
Ability to draw a conclusion, make a decision
78

Establishing Goals What outcomes do I/patient/family hope to
achieve Identifying Problems
What issues need to be addressed in order to achieve outcomes
What knowledge is required What resources are required or can help Whose perspectives must be considered
Formulating Interventions Professional standards and practice Based on clinical reasoning
79

Thinking Critically
Collaboration with physician/other community providers
Case conferencing
Patient Self-Management Tools
Preventing hospitalizations
Discharge planning
80
Collect Data
Outcomes /OASIS data
Home Health Compare
Satisfaction Surveys
Potentially Avoidable Events
Infections, incidents, complaints, and falls
Clinical record review
Identify Problems
Plan for Improvement
81

Managing Your Day
Visit scheduling-patient needs
Geography
Documentation requirements
Needs of agency-productivity, extra visits
Organization of Car and Office
Supplies
Clinical Bag
Personal Safety
82

Insurance regulations
HHA delegation, supervision, and care planning
Identifying abuse and/or neglect
Pain management/ responsibilities of clinicians
Eligibility for Hospice
Medication management and reconciliation
83

84

Retention Rates /New Grad Satisfaction
Improved Engagement of Preceptors
Client/Family Satisfaction
85

Routine feedback is integral to preceptee growth
Allowing for new grads to interact “normalizes” the experience
Adequate administrative support crucial
Learning sessions need to be relevant to practice
Tailoring learning plan according to individual needs improves engagement
86

New Graduate Program
New graduates
Classroom education ~80 hours
Skills labs
Field Preceptor Model
1 year duration internship
Lower salary
Milestone achievements attached to salary increments
Budget $90,000.00

Nurses new to home care retention rate: 75%
New Grad retention rate: 75%
ROI
Professional stimulation for preceptors
Energy, enthusiasm influences morale
Highly functioning new staff nurses
Preceptor / orientee match is critical.
If you ask for feedback, you better be open to hearing it!
Still searching for the perfect schedule for classes.
Daily closing discussion
Would like to include other disciplines in the future.
Content collaboration between clinical and didactic is crucial
Class discussions, experiences and humor, help content “come alive”
89

90
Questions?
AACN. (2016, Feb 3). The essentials of baccalaureate nursing education for professional nursing practice. Retrieved from American Association of Colleges of Nursing: http://www.aacn.nche.edu/education-resources/baccessentials08.pdf
Benner, P. (2016, March 12). Nursing Theories a Companion to Nursing Theories and Models. Retrieved from Current Nursing: http://current nursing.com/nursing theory/Patricia_Benner_From_Novice_to_Expert.html
Benner, P. (1984). From Novice to Expert: Excellence and Power in Clinical Nursing Practice, Commemorative Ed. Menlo Park: Addison-Wesley Pub Co.
91
Gordon, C. J., Aggar, C., Williams, A. M., Walker, L., Willcock, S. M., & Bloomfield, J. (2014). A transition program to primary health care for new graduate nurses: a strategy towards building a sustainable primary health care nurse workforce?. BMC Nursing, 13(1), 1-13. doi:10.1186/s12912-014-0034-x
Lartey, S., Cummings, G., & Profetto-McGrath, J. (2014). Interventions that promote retention of experienced registered nurses in health care settings: a systematic review. Journal Of Nursing Management, 22(8), 1027-1041. doi:10.1111/jonm.12105
McNeill, B.E. (2012.) Young whipper-snappers and old warhorses: understanding generational differences and finding common ground. Tar Heel Nurse. Pp 10-13.
92
Patterson, E., Hart, C., Bishop, S. & Purdy, N. (2013).Deciding if Home Care Is Right for Me: The Experience of the New Graduate Nurse, Home Health Care
Management & Practice, 25(4),147-154.
Rush, K.L., Adamack, M., Gordon, J., Janke, R., Ghement, I.R. (2015.) Orientation and transition programmecomponent predictors of new graduate workplace integration. Journal of Nursing Management. Pp143-155.
Saver, C. (2016, March 12). Novice to Expert. Retrieved from Nurse.Com: http://ce.nurse.com/ce556/novice-to-expert-through-the-stages-to success-in-nursing/coursepage/
93

Senge, P. (2006). The Fifth Discipline: The Art & Practice of The Learning Organization Paperback. New York: Doubleday
Smith-Stoner, M., Markley, J. (2007). Home Healthcare nurse recruitment and retention: Tips for retaining nurses: One State’s experience. Home Healthcare Nurse,25(3), 198-205.
DOI 10.1097/01.NHH.0000263438.15685.dd
Twigg, D., & McCullough, K. (2014). Nurse retention: A review of strategies to create and enhance positive practice environments in clinical settings. International Journal Of Nursing Studies, 51(1), 85-92. doi:10.1016/j.ijnurstu.2013.05.015
www.sinclair.edu/academics/.../crithink.pdf
94
Wikipedia. (2016, April 21). Evidence Based Practice. Retrieved from Wikipedia: https://en.wikipedia.org/wiki/Evidence-based_practice
Welk, D. (2013). Newly-licensed nurses: excellent, ethical and engaging work. Penn Nurse, 12-18.
95

Hallmark Health VNA and HospiceSylena Keeping: [email protected]
Paula McCartney: [email protected]
Donnelly & AssociatesMerrily Evdokimoff: [email protected]
Geri McCallig: [email protected]
COR HealthSusan White: [email protected]
96




![シマノ用 [1030 & 1030] サイズhedgehog-studio.sub.jp/ebay/tomo20150928_001.pdfシマノ用 [1030 & 730] サイズ Bearing size : 1030 (内径 3mm x 外径10mm x 厚さ4mm) &](https://static.fdocuments.us/doc/165x107/6045cd9b033164529741104c/ffc-1030-1030-hedgehog-ffc-1030-730.jpg)