Mental Health and Schools Together-NH A Guide to Supporting Collaborative Practice Sponsored by the...
75
Mental Health and Schools Together-NH A Guide to Supporting Collaborative Practice Sponsored by the Mental Health and Schools Together (MAST-NH) Initiative New Hampshire Center for Effective Behavioral Interventions and Supports at SERESC (NH CEBIS) www.nhcebis.seresc.net
-
Upload
eric-burns -
Category
Documents
-
view
232 -
download
1
Transcript of Mental Health and Schools Together-NH A Guide to Supporting Collaborative Practice Sponsored by the...
Mental Health and Schools Together-NH
A Guide to Supporting Collaborative Practice
Sponsored by the Mental Health and Schools Together (MAST-NH) Initiative
New Hampshire Center for Effective Behavioral Interventions and Supports at SERESC (NH CEBIS)
www.nhcebis.seresc.net
MAST-NH (Mental Health & Schools Together) Emerged From a Clear Need for Change
Planning MAST-NH began as we surmised that effective systems to support children & families w/ intensive needs were not in place Require multi-systems collaboration Anecdotal & research data supported the premise
We learned effective systems features that were needed & addressed some roadblocks
MAST-NH developed to design & begin to implement a vision to better support schools, children & families
Targets Mental Health, an issue so often a factor in working w/ children with intensive needs
MAST Cornerstone is systems-building & collaboration amongst home, school & mental health providers Supports PBIS model: build a FULL continuum of support
Funding for the Mental Health and Schools Together
New Hampshire Initiative is provided by
The United States Department of Education
Office of Safe and Drug-Free SchoolsDana Carr, Project Director
Mental Health and Schools Together-NH:A Guide to Supporting Collaborative
Practice
Shared Challenges,
Shared Students
Shared Work, Shared Success
Hopes for Today: A Mental Health Primer
Discuss the role schools and educators play in supporting good mental health through UNIVERSAL interventions
for ALL Children
Hopes for Today: A Mental Health Primer
Discuss the role schools and educators play in supporting the mental
health of SOME children who are at risk for
chronic problem behavior through TARGETED
interventions
Hopes for Today: A Mental Health Primer
Discuss the role schools and educators play (in
collaboration with community-based
providers) in supporting children with mental
illness and their families through INTENSIVE
interventions
Other Hopes for Today:
Discuss indicators of healthy social/ emotional development & information regarding the prevalence of mental illness
Discuss the connections between mental health & behavioral/ academic outcomes in school
Discuss our work in NH to: Improve on-going communications when schools &
community-based agencies are involved with common families
Develop the vision for linking home, school & MH providers for more effective work with children & families with intensive needs
I’d Guess There are Differing Views in this Audience
“Discussing Mental Health issues is just not a good use of my time – it’s not relevant to me”
“I am a skeptic, I think any effort we make to help our most troubled students and their families will probably be ineffective”
“It seems that educators have now become de facto mental health providers” “I embrace this idea” “I see this as an unfortunate reality “I believe that is simply NOT the correct role for educators”
Well.. I’m not here to try to tell you what to think – rather, to provide information and food for thought.
I respect and understand all these feelings and beliefs

MY big wish for today…
If nothing else, that the discussion today fuels some hope in you that through partnership with families and other community systems, we can discover how to better support children and families – so that we can achieve outcomes that allow us ALL to do our jobs more effectively
The Values/Principles/Vision that Guide this Work
Shared Work and communication are critical when it comes to supporting children & families with intensive needs
Identification and implementation of effective practices (supports, services, & strategies) that are efficiently accessible
Construct systems (processes, protocols) that support collaborative work that are reviewed continually for effectiveness and efficiency
Today’s Presentation is NOT intended to
Encourage schools to take on sole ownership or feel isolated in supporting mental health of students or student’s families (in fact, to the contrary)
Suggest that school staff members should EVER diagnose mental illness, emotional disorders, OR discuss medication issues with students or families
Provide extensive, in-depth information on any aspect of mental health or illness
“The children of today are too much in love with living. They have
terrible manners, mock authority, and have no respect for their
elders. …I can only fear what kind of awful creatures they will
become.”
Socrates, 369 B.C.
Schools and Children’s Mental Health
There is considerable evidence that children’s schooling plays an important role in their adjustment.
Success in school is clearly associated with positive mental health & well-being.
MH Risk IndicatorsOsher, Dwyer, and Jackson (2004)
Alienation Segregation Academic Frustration Chaotic Transitions Negative Relationships with
Adults and Peers Teased, Bullied School-driven Mobility
‘School hopping’ School failure Suspension, Expulsion, Drop
Out
Positive MH Indicators Osher, Dwyer, and Jackson (2004)
Making Interpersonal Connections
Positive Relationships with Adults and Peers
Academic Success Successful Transitions Caring Interactions Interactions with Pro-
social Peers Stability Over Time
Early Recognition: Prevention Means Knowing What to Look for
One clue to healthy development is when we see evidence of children meeting typical human needs: Need for belonging
Need for recognition and attention
Resiliency
Need for control and power
Self-Regulation
Need for Accomplishment, Mastery and Competence
The ABCs of Children’s Mental Health (Whelley, 2005)
Relationship Between Academics and Behavior
The relationship between academic underachievement (particularly reading) and externalizing behaviors suggests that students may act out to avoid academic tasks
The relationship between academic underachievement (particularly reading) and internalizing behaviors suggests that students may withdraw to escape academic tasks
Classroom teachers can play a key role in supporting mental health and identifying students who MAY be in need of assistance
Schools and Children’s Mental HealthYou Are Already Providing It!
Schools ARE commonly regarded as the de facto providers of mental health services for children and youth (Burns, et al., 1995; Farmer,et al., 2003).
21% of US children ages 9 to 17 have a diagnosable mental or addictive disorder that causes at least minimal impairment and behavioral challenges
Who Comes To School?
US Surgeon General’s Latest Report on Children’s Mental Health
10% of US children and adolescents suffer from a serious mental disorder that causes significant functional impairment at home, at school and with peers
Who Comes To School?
US Surgeon General’s Latest Report on Children’s Mental Health
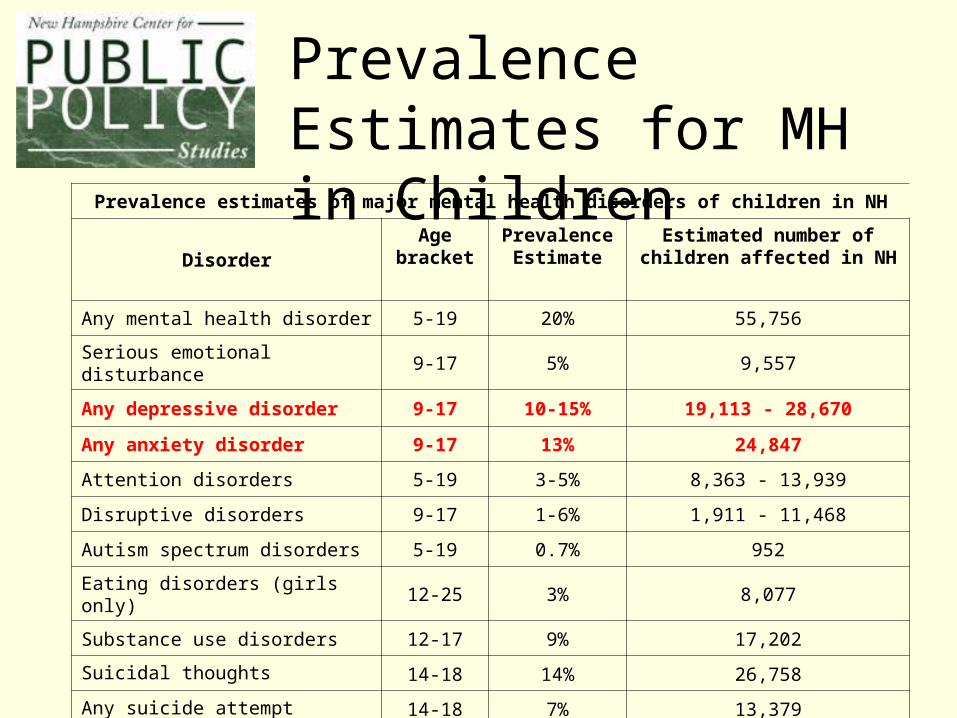
Prevalence estimates of major mental health disorders of children in NH
DisorderAge
bracketPrevalence Estimate
Estimated number of children affected in NH
Any mental health disorder 5-19 20% 55,756
Serious emotional disturbance 9-17 5% 9,557
Any depressive disorder 9-17 10-15% 19,113 - 28,670
Any anxiety disorder 9-17 13% 24,847
Attention disorders 5-19 3-5% 8,363 - 13,939
Disruptive disorders 9-17 1-6% 1,911 - 11,468
Autism spectrum disorders 5-19 0.7% 952
Eating disorders (girls only) 12-25 3% 8,077
Substance use disorders 12-17 9% 17,202
Suicidal thoughts 14-18 14% 26,758
Any suicide attempt 14-18 7% 13,379
Prevalence Estimates for MH in Children
The Fictitious Story of Lizzy Watson
The Cast Lizzy Watson: A Female Student (now in 9th grade)
Mrs. Watson: Lizzy’s Mother
Mr. Jones: Lizzy’s 9th Grade Math Teacher
Mr. Strickland: High School Principal
Mrs. Gerhardt: Lizzy’s 1st Grade Teacher
Mr. Smith: Lizzy’s 3rd Grade Teacher
Ms. Perry: Lizzy’s 7th grade Teacher
Mrs. Nelson: Middle School Guidance Counselor
Process for the Periodic ‘Think’ Sessions
Presenter will periodically pose questions to think about after pieces of the story
Doesn’t need to be silent – can be quiet discussion with person next to you Can’t expect silence for a full minute, but please use quiet
voices Our limited time together means that we’ll need to get
right back to the presentation as soon as the minute ends Quick silence when presenter raises his hand
Practice
We begin near the end of her school experience– the beginning of 9th grade
Team Conference Mr. Jones, 9th
grade teacher
The Fictitious Story of Lizzy Watson
Discussion Questions:1 minute Think
Can you recall situations where children left you feeling hopeless and discouraged?
Can you remember talking with a child and you just didn’t know what to say next – didn’t know what to do next?
We Don’t Want to Lose Anyone!
And Yet We Do!Mental Illness and Dropout
Students with mental illness have the highest dropout rate of any disability group
Nationally, 50% of children with serious emotional & behavioral disorders and 30% of students with other disabilities drop out of high school
Over half of the adolescents in the United States who fail to complete their secondary education have a diagnosable psychiatric disorder
Sources: Stoep et al., 2003; U.S. Dept. of Education, 2001
Many Students Not Getting Needed Mental Health Supports
We know that 50% of all mood, anxiety, impulse-control and substance-use disorders start by age 14…
… But, in any given year, it is estimated that only 20% of children with any type of mental disorder receive mental health services (Goodman et al., 1997).
… And studies indicated that of those children who did receive services, fewer than 50% received the appropriate service relative to their need (Kazdin, 1996).
Center for Evidence Based Practice: Young Children with Challenging Behavior
www.challengingbehavior.org
The proportion of preschool children meeting the criteria for the clinical diagnosis of ODD (Oppositional Defiant Disorder) ranges from 7% to 25% of children in the United States, depending on the population surveyed.
( Webster-Stratton, 1997) Center for Evidence Based Practice: Young
Children with Challenging Behavior www.challengingbehavior.org
Of the young children who show early signs of problem behavior, it has been estimated that fewer than 10% receive services for these difficulties. Kazdin & Kendall, 1998 Center for Evidence Based Practice: Young
Children with Challenging Behavior www.challengingbehavior.org
The Fictitious Story of Lizzy Watson
Lizzy in First Grade Lizzy screened for
vision, hearing and academics – but not for behavior
Adequate academic skills
Sweet, shy, soft spoken
Mrs. Gerhardt, First Grade Teacher
Early Struggles have Lasting Effect
Children who fall behind in 1st grade have a one in eight chance of ever catching up to grade level without extraordinary efforts
(Journal of Educational Psychology, 1994)
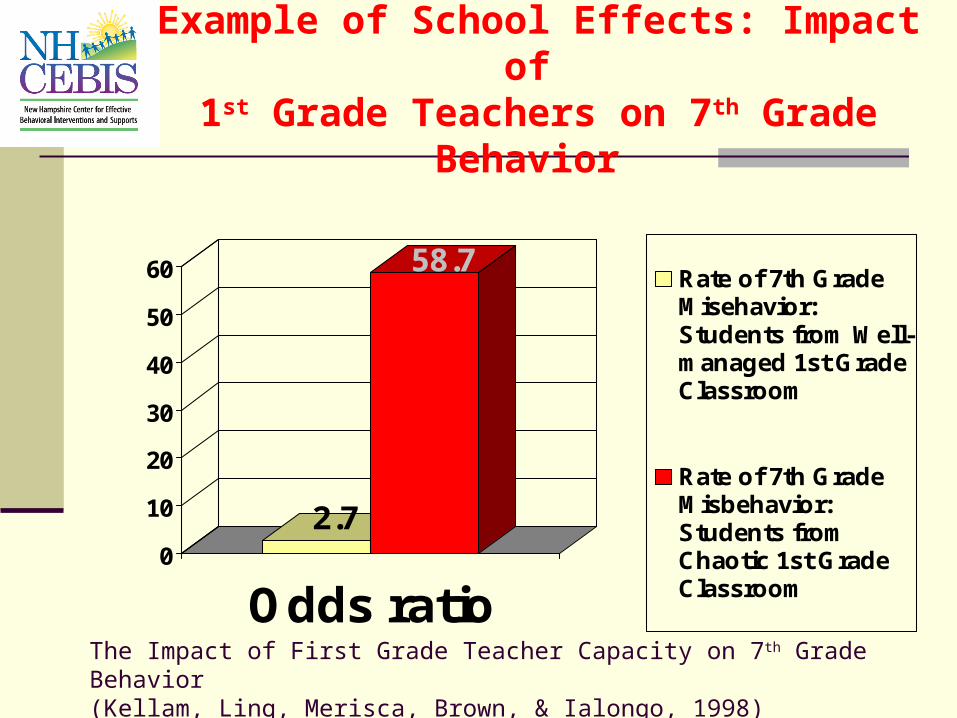
Example of School Effects: Impact of 1st Grade Teachers on 7th Grade Behavior
2.7
58.7
0
10
20
30
40
50
60
Odds ratio
Rate of 7th GradeMisehavior:Students from Well-managed 1st GradeClassroom
Rate of 7th GradeMisbehavior:Students fromChaotic 1st GradeClassroom
The Impact of First Grade Teacher Capacity on 7th Grade Behavior(Kellam, Ling, Merisca, Brown, & Ialongo, 1998)
The Fictitious Story of Lizzy Watson
Lizzy in Fifth Grade Mr. Smith, 5th grade teacher On grade level, but work of
poor quality, and hardly ever finished
No friends Low participation in class Not eligible for school
services
Lizzy
If Lizzy had a broken leg, you’d know what was wrong; If she wasn’t reading in 5th grade, You’d know who to speak to; If she was throwing chairs through the window, You’d know there was something really wrong; but, it seems that mental health issues aren’t always clear cut or as visible as other types of issues
Lizzy isn’t really a behavior problem and she isn’t presenting major academic problems. Perhaps it’s just her temperament? Perhaps she is like her dad – a little different.
Discussion Questions1 Minute Think
Have you run across a student where your gut tells you something’s wrong, but you’re not sure what to do about it – you’re not sure if you are over-reacting? Not sure if it really is a problem?
Do you know where to turn get information if you had concerns? Do you know who to go to if you wanted to talk through your concerns or just vent your thoughts?
Do some students like Lizzy fall between the cracks in terms of qualifying for extra supports and services?
A recent analysis of three national databases indicated that nearly 80% of low income youths in need of mental health services did not receive services within the preceding 12 months, with rates approaching 90% for uninsured families (Kataoka, Zhang, & Wells, 2002).
Many Students Not Getting Needed Mental Health Supports
Barriers to Involvement in Child Mental Health Interventions
McKay (2007) Poverty, single parent status and
stress Concrete obstacles: time,
transportation, child care, competing priorities
Stigma associated with mental illness and seeking care
Previous negative experiences with mental health or institutions
Scarce mental health resources Concerns about confidentiality Isolation
Even those families who receive mental health services experience attrition rates of greater than 50%, with low-income, minority children at especially high risk (Kazdin, 1996; Kazdin, Holland, & Crowley, 1997; Yeh, et al., 2003).
Keeping Mental Health Services Alive
The Fictitious Story of Lizzy Watson
Lizzy in 7th grade Mrs. Perry, 7th grade LA
teacher Failing some classes; barely
passing others Socially isolated except for
Sheila Superficial cutting behavior
beginning Discipline referrals for
disrespect Won’t go to counseling
Discussion Questions
Have you ever been frustrated with not having clear expectations about follow-up and on-going communications amongst home, school and mental health providers?
Does it seem that school is left holding the bag when you see family or outside agencies not doing their parts?
Do you ever feel like giving up because others don’t follow through?
To be alienated is to lack a sense of belonging, to feel cut off from family, friends, school or work – the four worlds of childhood
Urie Brofenbrenner, 1986
Students with Serious Emotional Disturbance (SED) miss more days of school than do students in all other disability categories
(U.S. Department of Education, 1994)
More than half of students with SED drop out of grades 9-12, the highest rate for all disability categories.
(U.S. Department of Education, 2002)
Of those students with SED who drop out of school, 73% are arrested within five years of leaving school
(Jay & Padilla, 1987)
Center for Evidence Based Practice:
Young Children with Challenging
Behavior www.challengingbe
havior.org
Lizzy in 9th grade School meeting Not attending
classes Likely to fail
classes Waiting to drop out ‘Cutting’ more
frequent Mrs. Watson
blames school
The Fictitious Story of Lizzy Watson
Discussion Questions
We all know where this meeting could go -- we’ve all felt blamed. It would be easy for this to end in a ‘blame game’ where no one wins
What’s a typical reaction to being blamed? How do you respond?
What could be said or done that might end the blaming before it stops the problem-solving?
What could Mr. Strickland say after Mrs. Watson spoke that would have both supported his staff AND at the same time have helped the team to problem solve?

There are evidence-based practices that are effective in changing the developmental trajectory…the problem is not what to do, but rests in ensuring access to intervention and support
Center for Evidence Based Practice: Young Children with Challenging Behavior
www.challengingbehavior.org
We CAN Impact Future Performance
Creating a Caring CommunityOsher (2006)
Students perform better on tests when they believe that their teachers care about them This correlation is stronger for students who are
judged to be at risk for dropping out of high school Supportive relationships promote student
engagement, positive attitudes, a sense of belonging to school, motivation, & academic achievement
Connections with adults in the school protect against a range of anti-social outcomes which impact academic performance (e.g., substance abuse)
“Every child needs one person who is crazy about him”
Uri Bronfenbrenner, Psychologist and Co-Founder of Head Start
Lizzy’s Story Could Be Different
What would it be like for children like Lizzy and those who live and work with her if we had a full continuum of school-based and community-based supports in place?
What will it take to get there?
Creating a System of Care and Education in New Hampshire
Gaps in the Continuum of Supports were identified based on 5 years of PBIS-NH implementation
Mental health And Schools Together-New Hampshire (MAST-NH) is helping to fill in the gaps
Starts with a Commitment to Early Recognition (all along the continuum)
and Shared Work
Systematic Screening (a MAST-NH Feature)
Active promotion of Home-School connection (PBIS)
High level of direct communication and collaboration when multiple systems are involved: home-school-mental health center (MAST-NH)
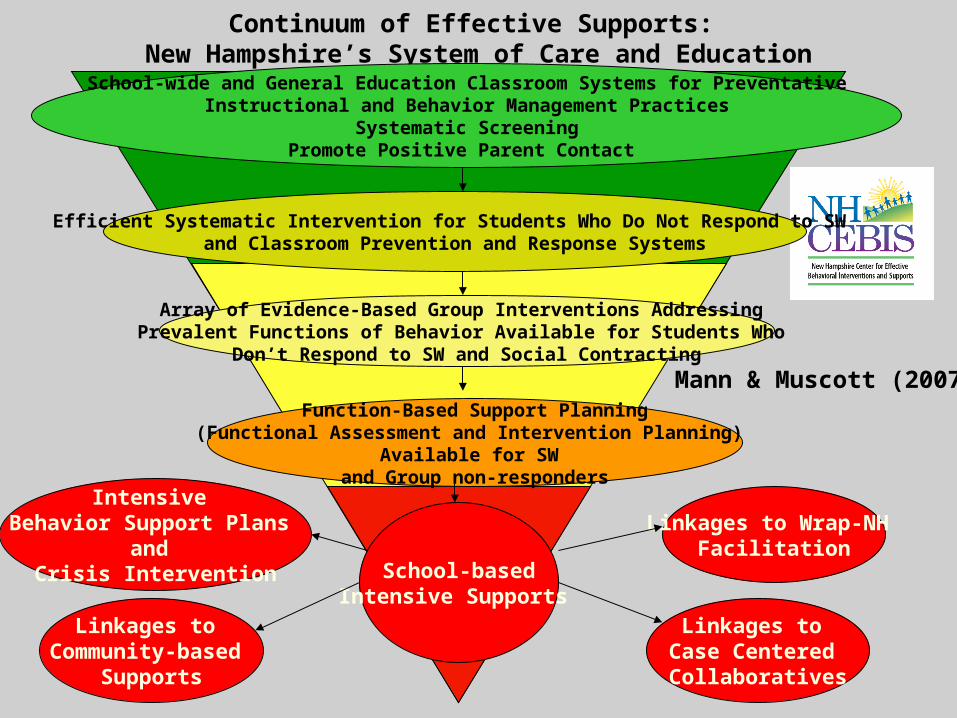
Continuum of Effective Supports: New Hampshire’s System of Care and Education
Linkages to Wrap-NH Facilitation
School-basedIntensive Supports
Coordinator
Linkages to Community-based
Supports
School-wide and General Education Classroom Systems for PreventativeInstructional and Behavior Management Practices
Systematic ScreeningPromote Positive Parent Contact
Array of Evidence-Based Group Interventions Addressing Prevalent Functions of Behavior Available for Students Who
Don’t Respond to SW and Social Contracting
Function-Based Support Planning(Functional Assessment and Intervention Planning)
Available for SW and Group non-responders
School-basedIntensive Supports
Linkages to Case Centered Collaboratives
Mann & Muscott (2007)
Efficient Systematic Intervention for Students Who Do Not Respond to SW and Classroom Prevention and Response Systems
Intensive Behavior Support Plans
and Crisis Intervention
Supporting the Personal, Social, Physical and Academic Development of Every Child
What does your school already do to support children’s development through early intervention and prevention? Screenings? A.M. Bus Greeters? Greeting students by name? Systems for effective communication Systems for efficient referral to higher level supports Providing information and resources to families & staff Providing a continuum of effective supports?
Teaching & recognizing desired social behavior Targeted group interventions including supports that encourage
belonging, social/ emotional development & academic skill development
Knowing what ‘Function of behavior’ means and how understanding function can lead to effective support
Other ways in which student mental health is supported?
Mental Health and Schools Together-NH (MAST-NH) Major Features
1. Mental Health Primer for School Staff
2. Life Space Crisis Intervention Techniques (LSCI)
3. Assessment of School-based Systems of Emergency Preparedness
4. School-based Referral Protocols to Targeted & Intensive Teams
5. Community-based Referral Protocols to Community Mental Health Centers
6. Wraparound Facilitator Training and Development of Mentored and Peer Support System
7. Development or Expansion of Community or Regional Collaboratives
8. Community Resource Mapping to Identify Needs & Action Plan
What is MAST-NH Doing?
Enhanced the work of the Seacoast Collaborative Bringing systems throughout the community together:
DCYF (Child Welfare) DJJS (Justice) Mental Health Medical Health Schools Youth development and recreation Substance abuse Family representation
Monthly meetings, action planning Breaking down systems barriers Determining how to support families AND system partners Community Resource Mapping
What is MAST-NHDoing?
Building capacity building for Wraparound: Newly trained Wrap-NH facilitators in Somersworth area:
Kate Salvati, Strafford Learning Center Kathy Francoeur, Somersworth Schools Jon Drake, APEX II Diane Cyr, Seacoast mental health Kyle Sczepanik- family, family rep to collaborative Miranda Snow, CHOICES Gary Reynolds, SAU 44 Liz Card, HUB Parent Greg Burdwood, HUB Family Resource Center Kimberly Cartier, Rockingham Community Action Program Heidi Wyman, Strafford Learning Center, Transition Network
Building Mentor capacity to develop a system for facilitator support Kate Salvati @ SLC building system for on-going facilitator training and
support Kevin Murphy @ SLC planning for future capacity-building and funding
What is MAST-NH Doing?
Soon to be Senior Trainers in Life Space Crisis Intervention Joel Eastman Sue Cohen, SLC Glynn Talley, Powers School
‘Senior’ Trainers will be authorized to certify new trainees through a 5-day course in LSCI
These 5 have already committed to a five-day LSCI training through MAST-NH: Laurie Conley Grace Fuller Corinne White Donna Drolet Judy Tyndall Christine Williams
These folks have committed to a One-Day training (January 11): Dana Mitchell Holly Prud’homme Ted Ready Richard Walsh
What is MAST-NH Doing?
Developed training process for Intensive Systems Systematic Screening for Behavior Disorders Crisis Response/ Emergency Response Intensive Functional Assessment Person-Centered Planning (January 18th) Already attended some of our trainings in Intensive Systems:
Laurie Conley Laurie Lambert Dana Mitchell Kelly Warren
What is MAST-NHDoing?
Worked w/ Janet Salisbury of Community Partners of Strafford County, your community mental health center to: Develop a flowchart to clarify their referral process Design a ‘facilitated referral to Mental Health Services’
Design worksheet/ process for an ideal school to MH referral Join with an SAU-56 Team to establish protocols for on-
going communications amongst school, family, MH providers and medical providers
Janet Salisbury, Children’s Director @ Community Partners Rebecca Paschal of Community Partners, housed at the middle
school Representative SAU 56 Team: All Schools Represented
See Joel Eastman
What is MAST-NH Doing?
SAU 56 team with reps from each school -- to address issues related to supporting children and families with intensive needs Need a K-12 effort Developing internal referral processes and promoting a full continuum
of effective supports Addressing on-going communications with MH and medical providers Meeting at end January Community Partners will be at the table K-12 representation
MAST-NH Leadership Team Statewide A Statewide Collaborative All regions and systems represented
Supporting a common vision
Vision for Somersworth Schools
Internal protocols for referrals to Intensive Supports Systems that support staff (to decrease stress of not
knowing what to do next) Have data that supports good decision-making and
evidences progress Have a full continuum of support at each school Have a continuum of accessible community-based supports Develop specific protocols for a facilitated referral to
Community Partners or other community-based supports Develop specific protocols for on-going communications
amongst Schools, Home, MH and Medical Systems
School-Home-Mental Health Collaboration Works
School-based programs focused on consultation with teachers and parents can be effective approaches to enhancing children’s mental health (Lowie, Lever, Ambrose,Tager, & Hill, 2003; McKay, et al., 2003; Weiss, et al., 2003).
Consultation with teachers can maximize opportunities to effect children’s academic learning and classroom behavior (Fantuzzo & Atkins, 1992; Ringeisen et al., 2003).
The ‘shared work’ dilemma
Some hear ‘Shared Work’ & feel relieved that Mental Health support is not all on the shoulders of educators
Others hear ‘Shared Work’ & feel a burden & are anxious that it sounds like educators are being asked to spend precious time working outside their scope of expertise
We believe (as with Special Education) that if MH support is simply a ‘hand-off’ (“Please Fix Him”), or if clear predictors are ignored, the likelihood of effective intervention decreases
Solving the Critical Issue of Making Shared Work a Reality
How can the SAU and schools best support the work of the Community Partners?
How can Community Partners best support the work of schools?
School Administrative Unit 56
to ‘Community Partners of Strafford County’
Promoting a School Facilitated or Supported Referral
What is the process when staff from the Somersworth Schools help families facilitate a
referral to Community Partners?
Components of a Facilitated Referral from School to Community Partners (First Draft)
Parents to sign a school release to CMHC to facilitate referralSchool to call Admissions department with the following information:
Reason for referralAcademic functioningBehavioral functioning
Social functioningRecent change or deterioration in any of the areas of functioning
Special Education or 504 planContact person at school
Parents to contact Admissions Department at CMHC and provide the following information:Demographic information
Reason for referralFamily structure
Academic, behavioral and social functioningMedical information, including any medications – current and past
Insurance information
What will tell you that things are getting better?What is the school hoping for with this referral?What is the family hoping for with this referral?
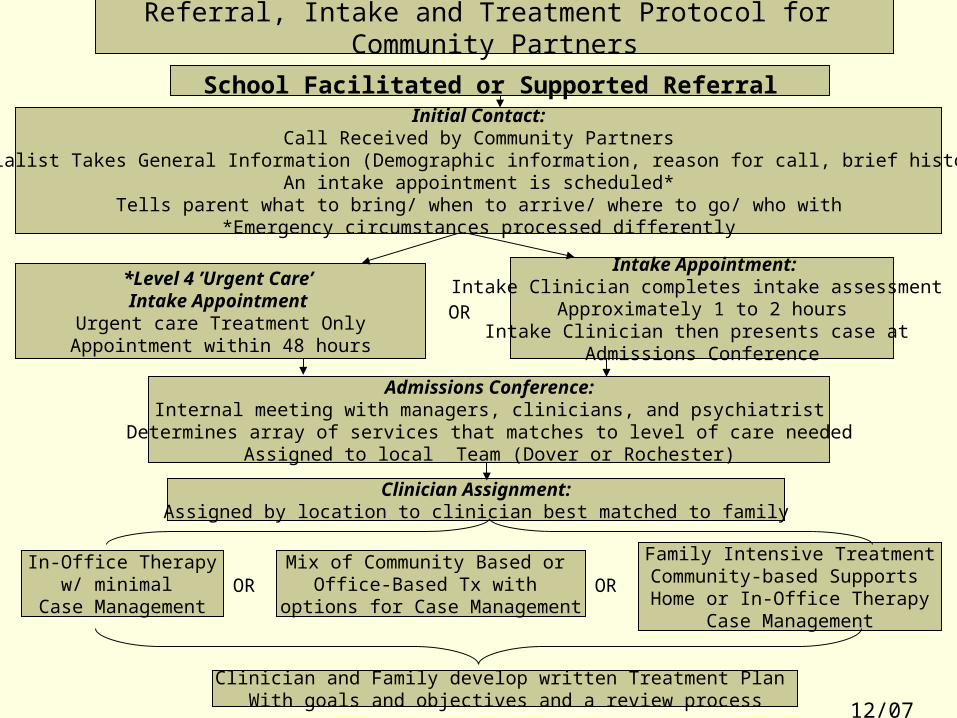
Referral, Intake and Treatment Protocol for Community Partners
School Facilitated or Supported Referral
*Level 4 ’Urgent Care’ Intake Appointment
Urgent care Treatment OnlyAppointment within 48 hours
In-Office Therapy w/ minimal
Case Management
Mix of Community Based or Office-Based Tx with
options for Case Management
Intake Appointment:Intake Clinician completes intake assessment
Approximately 1 to 2 hoursIntake Clinician then presents case at
Admissions Conference
Admissions Conference:Internal meeting with managers, clinicians, and psychiatrist
Determines array of services that matches to level of care neededAssigned to local Team (Dover or Rochester)
Family Intensive TreatmentCommunity-based Supports Home or In-Office Therapy
Case Management
Clinician Assignment:Assigned by location to clinician best matched to family
Clinician and Family develop written Treatment Plan With goals and objectives and a review process
Initial Contact:Call Received by Community Partners
Admissions Specialist Takes General Information (Demographic information, reason for call, brief history of problems)An intake appointment is scheduled*
Tells parent what to bring/ when to arrive/ where to go/ who with*Emergency circumstances processed differently
OR OR
OR
12/07
What Does Community Partners Provide? Child and Adolescent Services provides
assessment, treatment and case management services to children and adolescents.
The division emphasizes the provision of care to youngsters "at risk" and with moderate to severe emotional and behavioral disturbances.
1. Individual Therapy: Pre-school, Latency, Adolescent
2. Group Therapy: Pre-school, Latency, Adolescent, Parents/ Caregivers
3. Family Therapy
4. Emergency Services/ Crisis Stabilization
5. Prescribe Medication
6. Monitor Medication7. Admission/Discharge
Planning8. Medical/Psychiatric
Screening9. Case Management10. Community-Based
Functional Supports11. Dialectical Behavioral
Therapy Program for Adolescents
Expected Outcomes
What Can a Family Expect from Treatment?
Expected outcomes of treatment are incorporated into the individual treatment planning process
Outcomes may include: The improvement of presenting problems Improvement in emotional and behavioral
functioning Stabilization of functioning Maintenance of functioning Prevention strategies Problem-solving strategies
MAST-NH Regions and Schools
6 Regional Collaboratives Candia, Lakes Region, Littleton, Londonderry,
Monadnock, Strafford County
27 PBIS Schools
6 Community Mental Health Centers
NH CEBIS and MAST-NH (Watch for new website!)
\
http://www.nhcebis.seresc.net