Meningitis - OU College of Nursing | Main Page
53
Meningitis Ozair Naqvi, MS Epidemiologist, Communicable Disease Division Acute Disease Service Oklahoma State Department of Health
Transcript of Meningitis - OU College of Nursing | Main Page

Meningitis
Ozair Naqvi, MS
Epidemiologist, Communicable Disease Division
Acute Disease Service
Oklahoma State Department of Health

Objectives
• Describe the occurrence of meningitis
• Describe the signs and symptoms of
meningitis
• Describe when these vaccinations should be
given

Meningitis and Public Health
• Two specific conditions that require
immediate response by public health
officials:
– Meningococcal Invasive Disease
• Neisseria meningitides
– Haemophilus influenzae Invasive Disease
• Haemophilus influenza type b (Hib)

Epidemiology of Meningococcal
Invasive Disease Globally
• Large epidemics of
meningococcal
disease occur in the
African “meningitis
belt”
• In each epidemic,
tens of thousands
of cases and
thousands of
deaths may occur

Epidemiology of Neisseria
meningitidis
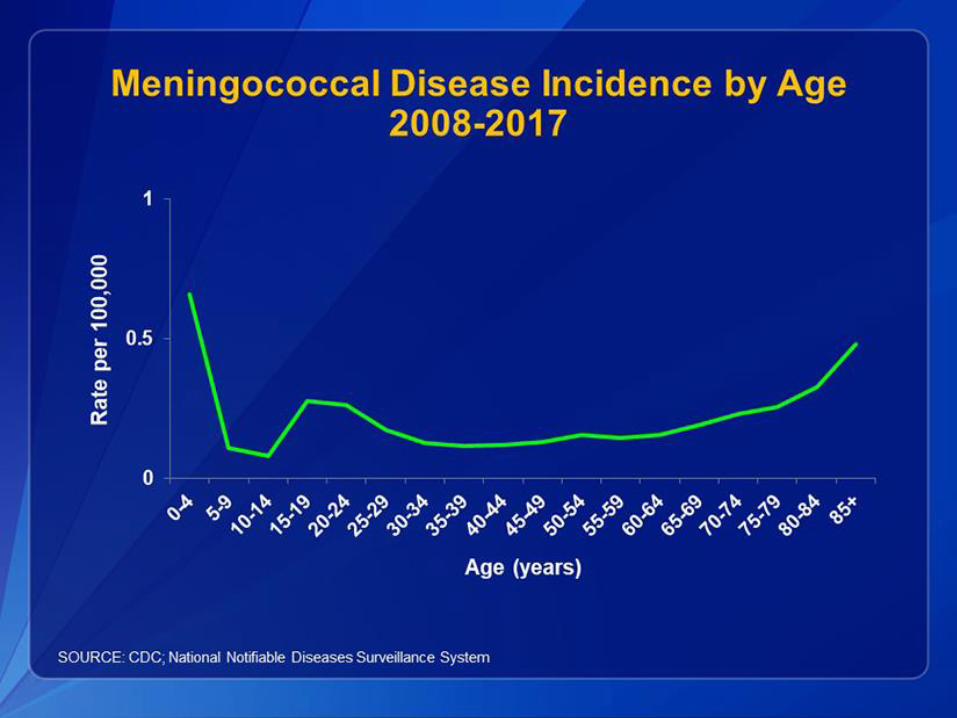
Epidemiology of Neisseria
meningitidis

Epidemiology of Neisseria
meningitidis

0
10
20
30
40
50
60
CA
SE
S
YEAR
Incidence of Meningococcal Invasive
Disease in Oklahoma from 1990-2018

Epidemiology of Haemophilus
influenzae Invasive Disease
• In developing countries, where routine vaccination with Hib
vaccine is not widely available, Hib remains a major cause
of lower respiratory tract infections in infants and children
• In the United States, Hib disease is not common. In 2015,
the incidence of invasive Hib disease was 0.08 cases per
100,000 in children younger than 5 years of age
– Occurs primarily in underimmunized children and in infants too
young to have completed the primary immunization series
– Less than 10 cases in Oklahoma since 2000

Meningococcal Invasive
Disease Background
Organism: Neisseria meningitidis
Incubation Period: Varies 2 to 10 days (commonly 3 to 4 days)
Infectious Period: As long as the organism is present in the nasopharynx (may be weeks to months) Ends when the patient has been on appropriate
antibiotics for at least 24 hours
Asymptomatic carriage can be as high as 25% without cases of meningococcal invasive disease in the community; carriage may be higher with cases occurring in the community

Meningococcal Invasive Disease
Background
Mode of transmission: Direct exposure to respiratory droplets or direct contact with discharges from the nose or throat
Symptoms:
Meningitis: stiff neck, high fever, headache, nausea, vomiting, or mental confusion
Meningococcemia: fever, petechial or purpuric rash, hypotension, disseminated intravascular coagulation, and multiorgan failure
Case fatality rate of meningococcal disease: Lowered from 50% to 8-15% thanks to antibiotics, intensive care units, and improved supportive measures
Fatality rate of meningococcemia is up to 40%
Haemophilus influenzae Invasive
Disease Background
Haemophilus influenzae Invasive Disease: caused by bacteria Haemophilus influenzae. Type b (Hib) is the only type which control measures are necessary
Transmission:
direct exposure to respiratory droplets or direct contact with discharges from nose or throat
In neonates, infection is acquired intrapartum by aspiration of amniotic fluid or contact with genital tract secretions

Haemophilus influenzae Invasive
Disease Background
Incubation Period: Incubation period is unknown, but
most likely 2 to 4 days
Communicability: As long as organism is present in the
nose and throat. Communicability ends when client has
been on appropriate antibiotics for at least 24 hours

Haemophilus influenzae Invasive
Disease Background
Symptoms:
Meningitis: high fever, vomiting, lethargy,
meningeal irritation consisting of bulging
fontanelle in infants or stiff neck in older children
Clinical Illness: meningitis, septicemia,
pneumonia, cellulitis, arthritis, epiglottitis,
pericarditis, endocarditis, and osteomyelitis

Meningococcal: Confirm the diagnosis
To begin an investigation we need laboratory
confirmation:
Culture: Neisseria meningitidis from a
normally sterile site
OR
Gram negative diplococci on the gram stain
OR
Detection of N. meningitidis antigen from
CSF

Hib: Confirm the diagnosis
Culture Gold standard
Must be from sterile site (blood, CSF, aspirates from joints, pericardium, pleural fluid, etc.)
OSDH Public Health Lab confirms and serotypes all isolates received from Oklahoma labs
Antigen testing Clinicians may request antigen test on sterile site
fluid, esp when Type B (Hib) is suspected
Real-time Polymerase Chain Reaction (RT-PCR) Can be used for detection of Hib from sterile site in
which organism could not be detected by culture

Differentiating Bacterial vs. Viral
Meningitis LabsSpecimen Viral Bacterial
WBC CSF 6-100 Cells> 100 Cells
Elevated (50-1000)
Protein CSFSlightly Elevated Elevated
(45-150) (50-1000)
Glucose CSFNormal Below Normal
(> 40) (< 40)
Gram Stain CSF/Blood No Organisms
Gram + Cocci: Streptococcus pneumoniae
Gram - Rods: Haemophilus influenzae
Gram - Cocci: Neisseria meningitidis
WBC Differential CSFLymphocytes: 60-70% Mostly Neutrophils
Monocytes: 30-40% Few Lymphocytes & Monocytes
C-Reactive Protein Blood < 1 > 1
Bacterial Antigen/Latex
AgglutinationCSF No Antigen Detected Positive for Specific Bacteria
Bacterial Culture CSF/Blood No Growth Growth

Bacterial vs. Viral MeningitisViral
• It is often less severe than bacterial
meningitis, and most people get better
on their own in 7 to 10 days (no specific
treatment)
• Non-polio enteroviruses are the most
common cause of viral meningitis in the
United States, especially from late spring
to fall
• Initial symptoms of viral meningitis are
similar to those for bacterial meningitis,
not as severe
• Close contacts of someone with viral
meningitis can become infected with the
virus that made that person sick.
However, these close contacts are not
likely to develop meningitis
Bacterial
• Meningococcal meningitis is caused by
the bacteria Neisseria meningitidis, and
causes a more severe disease that
requires prompt treatment of the patient
with antibiotics
• Symptoms include stiff neck, high fever,
headache, nausea, vomiting, mental
confusion, petechial or purpuric rash,
hypotension, or multiorgan failure
• Can be caused by bacteria such as
Haemophilus, Streptococcus, or
Neisseria meningitidis, which are spread
by direct contact with saliva or
respiratory droplets from the nose and
throat of an infected person
The type of meningitis can only be confirmed through laboratory tests

Meningococcal Public Health
Investigation Steps
1. Confirm Diagnosis
2. Interview case/guardian/parent as soon as possible
• Complete disease report (obtain/verify following):
• Hospital dates
• Symptoms and specific onset dates
• Treatment
• High-risk setting
• Contacts
3. Contact Investigation
• Identify all close contacts in 7 days prior to illness onset to 24 hours after initiation of appropriate antibiotic
• Recommend post-exposure prophylaxis as necessary
Meningococcal Contact Identification
and Investigation
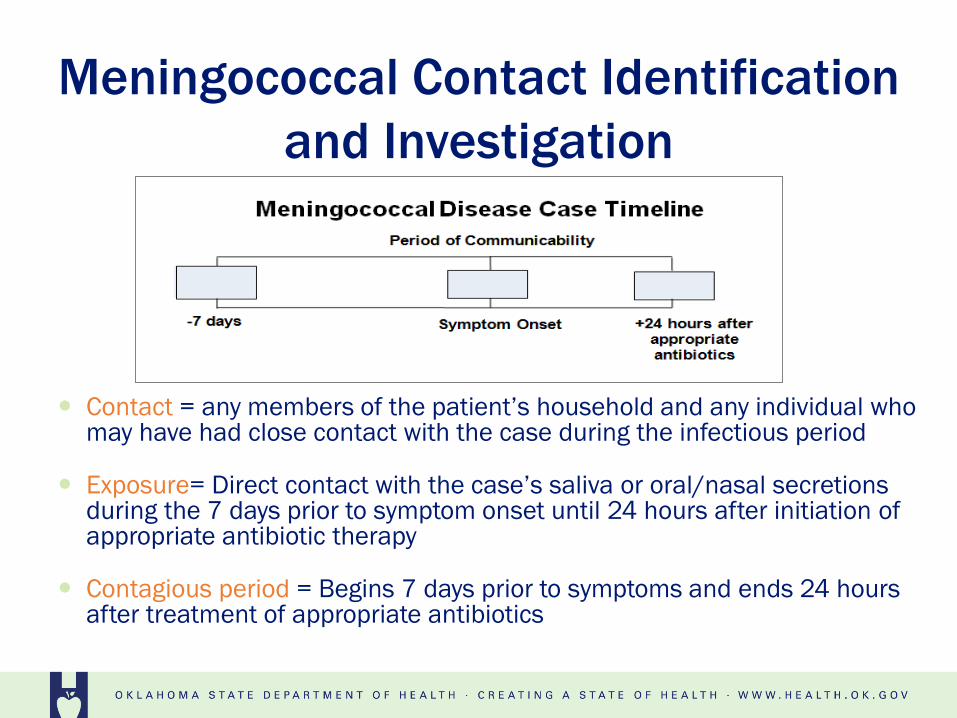
Contact = any members of the patient’s household and any individual who may have had close contact with the case during the infectious period
Exposure= Direct contact with the case’s saliva or oral/nasal secretions during the 7 days prior to symptom onset until 24 hours after initiation of appropriate antibiotic therapy
Contagious period = Begins 7 days prior to symptoms and ends 24 hours after treatment of appropriate antibiotics

Meningococcal Contact Identification
and Investigation
Exposure Examples: Sharing food or eating/drinking utensils
Sharing lip gloss, lipstick, cigarettes, or similar items
Kissing
Explosive cough or sneeze to the face
Mouth-to-mouth resuscitation
Unprotected exposure, not wearing procedure mask or surgical mask, while performing a full medical examination of the nose and throat including medical/dental examination or procedure (suction, intubation, etc.)
Child care or pre-school contacts
Passengers seated directly next to the patient during airline flights lasting more than 8 hours

Meningococcal Contact Investigation
Household contacts
Recommended to ALL household contacts
regardless of vaccination status
Household-like and close, personal contacts
Recommended to anyone with intimate contact
or direct saliva contact

Meningococcal Contact Investigation
Community residential programs or facilities
Recommended to persons who had direct
contact with oral/nasal secretions of the case or
household-like contact
School setting
Not routinely recommended for all classmates
Identify close contacts (i.e. boyfriend/girlfriend)
as well as those with direct contact to nasal/oral
secretions

Meningococcal Contact Investigation
Group or residential homes
Recommend PEP to close contacts (i.e., roommates, those with direct contact to nasal/oral secretions)
Healthcare setting
Recommend PEP to healthcare workers performing full medical examination of the nose or throat without wearing PPE
Includes hospital staff and first responders.

Meningococcal Contact Identification
and Investigation• PEP is recommended to all exposed contacts
regardless of vaccination historyDrug Age of
Contacts
Dosage Cautions
Rifampin ≤ 1 month 5 mg/kg, orally, every 12 hours x 2
days
Can interfere with efficacy of oral
contraceptives and some seizure and
anticoagulant medications> 1 month 10 mg/kg (max dose 600mg),
orally, every 12 hours x 2 days
Ceftriaxone ≤ 15 years 125 mg, IM (single dose) To decrease pain at injection site, dilute with
1% lidocaine> 15 years 250 mg, IM (single dose)
Ciprofloxacin ≥ 1 month 20 mg/kg; (max 500 mg), orally
single dose
Not recommended routinely for people
younger than 15 years of age
Azithromycin 10 mg/kg (max 500 mg), single
dose
Not recommended routinely

Hib Public Health Investigation Steps
1. Confirm Diagnosis
2. Interview case/guardian/parent as soon as possible
• Complete disease report (obtain/verify following):• Hospital dates
• Symptoms and specific onset dates
• Treatment
• High-risk setting
• Contacts
3. Contact Investigation
• Identify all close contacts in 7 days prior to illness onset to 48 hours after initiation of appropriate antibiotic
• Recommend post-exposure prophylaxis as necessary
4. If household contacts <4 years
• Gather Hib vaccination hx to determine susceptibles
• Determine if any of these children have immunocompromising condition

Hib Post-Exposure Prophylaxis (PEP)
Recommend appropriate antibiotic prophylaxis to: 1) Case
2) HH contacts
3) CCS contacts
Only recommend PEP to contacts considered exposed to case 7 days prior to hospital admission and until 48 hours after initiation of appropriate antibiotics If last date of exposure has been more than 14 days
or if a pregnant women, PEP is not recommended.

Hib Post-Exposure Prophylaxis (PEP) 1. Case
If treated with ampicillin or chloramphenicol needs rifampin prior to discharge
If treated with cefotaxime or ceftriaxone no rifampin needed
2. Household Contacts Rifampin recommended for all household contacts if at
least one child <4 years of age in home (other than the case) and if: i. Infants <12 months who not received primary 2- or 3-series
ii. Child 1-3 years who is inadequately vaccinated
iii. Child has immunological impairment, regardless of child’s Hib vaccine status

Recommended Dosage for Rifampin
Prophylaxis of Contacts to a Case of H.
influenzae type b
1 Not to be taken during pregnancy.
2 Side effects of Rifampin include orange discoloration of urine, discoloration of soft contact lenses (removal
recommended for duration of chemotherapy), discoloration of teeth, nausea, vomiting, and diarrhea. May interfere
with efficacy of oral contraceptives and some seizure prevention and anticoagulant medications.
Source: American Academy of Pediatrics. Haemophilus influenzae Infections. In: Pickering LK, Baker CJ, Kimberlin
DW, Long SS, eds. Red Book: 2009 Report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL:
American Academy of Pediatrics; 2009: 316-317.
Contacts Dosage
Infants < 1 month age Not established, some experts
recommend lowering dose to 10
mg/kg once daily for 4 days
Children >1 month age and adults 20 mg/kg (maximum dose 600 mg)
once daily for 4 days

Meningitis Rumors

Meningitis in Schools

Meningitis in Schools

Meningococcal Immunization
Recommendations
• MenACWY is
given as part of
7th grade
vaccinations
• MenB is given
prior to starting
college

Hib Immunization
Recommendations
• ActHIB, Hiberix, or Pentacel: 4-dose series at 2, 4,
6, 12–15 months
• PedvaxHIB: 3-dose series at 2, 4, 12–15 months

Neisseria meningitidis Outbreak in an
Elementary School — Oklahoma, 2010

Timeline
10March
March 10
• Preliminary CSF culture N. meningitidis from
7 year-old boy: Case A
• Household members and close contacts identified
• Chemoprophylaxis recommended for contacts

Timeline
Index
Case
Reported
10March 11
March 11
• 6:20–8:20 AM: Cases B, C, D reported (1 death)
• All attended same school
• Rural northeast Oklahoma
• School district population 1,850 students
• 9:45 AM: Investigation team departs OSDH

School District A
Lower Elementary
School
High School
Upper Elementary
School
Middle School

Investigation
• Active surveillance to identify additional cases – Contacted hospital IPs daily to identify new cases
– Contacted laboratories daily for any preliminary results
– Contacted local pediatricians to identify in possible new cases
• N. meningitidis serogrouping at state public health laboratory – Requested all isolates be sent to OSDH PHL
• Pulsed-field gel electrophoresis (PFGE), polymerase chain reaction (PCR), and multilocus sequence typing (MLST) at CDC

Case Definitions
• Epidemiologically linked to School District A
• Disease onset no earlier than March 1, 2010
• Samples taken from normally sterile body site
• Confirmed: Neisseria meningitidis isolated by culture
• Probable: N. meningitidis-specific nucleic acid detected by polymerase chain reaction (PCR)
• Suspect: fever and rash in hospitalized person
Timeline
Index
Case
Reported
10March
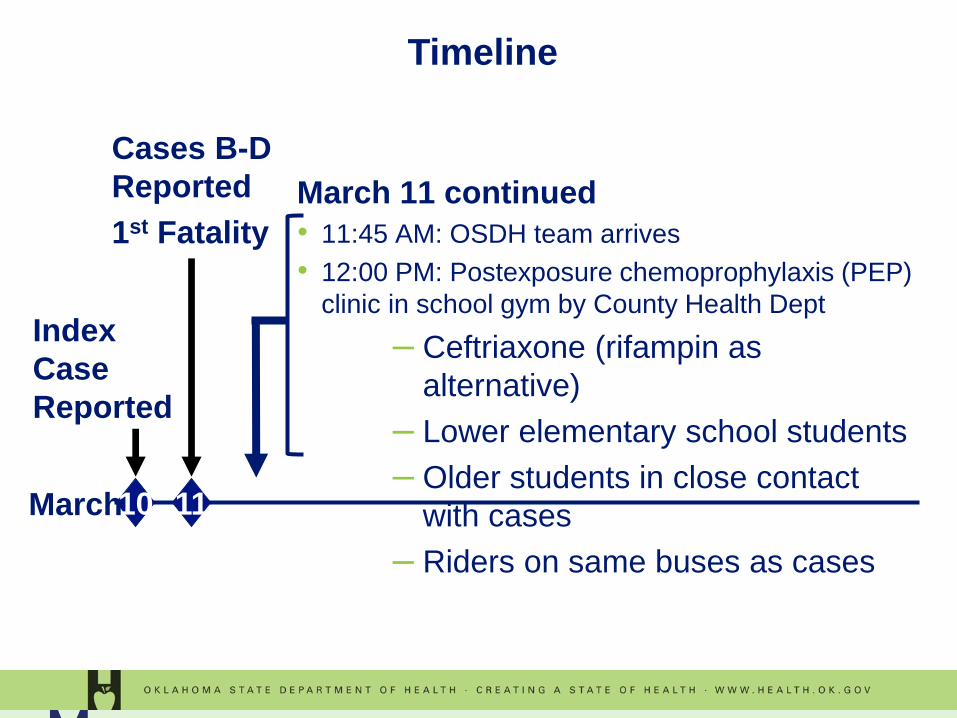
March 11 continued
• 11:45 AM: OSDH team arrives
• 12:00 PM: Postexposure chemoprophylaxis (PEP)
clinic in school gym by County Health Dept
– Ceftriaxone (rifampin as
alternative)
– Lower elementary school students
– Older students in close contact
with cases
– Riders on same buses as cases
Cases B-D
Reported
1st Fatality
11

Timeline
12:30–
8:00
PM
Index
Case
Reported
10March
6:20
–
9:45
AM
Cases B-D
Reported
1st Fatality
1112:00
PM
OSDH
Team
Arrives
PEP
Clinic
#1
March 11 continued
• Active surveillance begins in 6 counties
• 12:30 PM: School closes for Spring Break
• 1:30–4:00 PM: Cases E and F reported
Case D death
• 8:00 PM: PEP clinic closes for 1st day

PEP Clinic Summary
• ~975 people as contacts warranted
prophylaxis
• 1,063 (109%) received prophylaxis

Timeline
12:30–
8:00 PM
Cases E &
F Reported
2nd Fatality
Index
Case
Reported
10March
6:20–
9:45
AM
Cases B-D
Reported
1st Fatality
11 12
12:00
PM
OSDH
Team
Arrives
PEP
Clinic
#1
March 12
• 8:22 AM: Case G, high school student
• 9:00 AM: 2nd PEP clinic opens
• 10:55 AM: Serogroup C multilocus
sequence type (MLST) ST-11/CC-11
• 12:15 and 2:00 PM: Additional
chemoprophylaxis arrives
• Decision made to hold
vaccination clinics

Index case
Case Links
Classroom A
5yo case
Classroom B Choir A and B
Asymptomatic
5yo sibling
Asymptomatic
17yo sibling
Index Case
2 additional cases
(2 deaths)
18yo case

Timeline
12:30–
8:00 PM
Cases E
& F
Reported
2nd
Fatality
Index
Case
Reported
10March
6:20–
9:45
AM
Cases B-D
Reported
1st Fatality
11
Case G
Report
ed PEP
Clinic
#2
12
12:00
PM
OSDH
Team
Arrives
PEP
Clinic
#1
March
16
• 3rd
PEP
clinic
191613 21
Scheduled
Spring
Break

Timeline
12:30–
8:00 PM
Cases E & F
Reported
2nd Fatality
Index
Case
Reported
10March
6:20–
9:45
AM
Cases B-D
Reported
1st Fatality
11
Case G
Reported
PEP
Clinic #2
12 19
PEP
Clinic #3
1613 21
12:00
PM
OSDH
Team
Arrives
PEP
Clinic
#1
March 19
• Vaccinati
on clinic
#1
Scheduled
Spring Break

Timeline
12:30–
8:00
PM
Cases E &
F Reported
2nd Fatality
Index
Case
Reported
10March
6:20–
9:45
AM
Cases B-D
Reported
1st Fatality
11
Case G
Reported
PEP
Clinic #2
12
Vaccination
Clinic #1
19
PEP
Clinic #3
1613 21
12:00
PM
OSDH
Team
Arrives
PEP
Clinic
#1
Additional
Vaccination
Clinics
22-26
Scheduled
Spring Break

Vaccination Clinic Summary
Persons vaccinated
Total 1,459
Children 1,250
Dose funding
VFC 1,092 (77%)
State 367 (23%)

Clinical and Laboratory
CharacteristicsDetection of
N. meningitidis
CaseAge
(Years)Classification Onset Death Blood CSF
A 8 Confirmed 3/08 No Culture, PCR Culture, PCR
B 7 Probable 3/10 Yes PCR PCR*
C 6 Confirmed 3/10 No Culture, PCR Not Done
D 8 Confirmed 3/10 Yes Culture, PCR Culture, PCR
E 5 Suspect 3/10 No No No
F 8 Suspect 3/11 No No Not Done
G 18 Confirmed 3/10 No Culture No
*Cerebral Tissue

Timeline
12:30–
8:00
PM
Cases E &
F Reported
2nd Fatality
Index
Case
Reported
10March
6:20–
9:45
AM
Cases B-D
Reported
1st Fatality
11
Case G
Reporte
d PEP
Clinic #2
12
Active
Surveillance
Ends
31
Vaccination
Clinic #1
19
PEP
Clinic #3
1613 21
12:00
PM
OSDH
Team
Arrives
PEP
Clinic
#1
Additional
Vaccination
Clinics
22-
26
Scheduled
Spring Break

Conclusions
• Chemoprophylaxis and vaccination well
accepted
• Rapid, two-pronged intervention interrupted
outbreak
• Use of VFC funds for outbreak-control-related
vaccine purchase another avenue to obtain and
provide vaccine in outbreak setting

Questions?
Call Acute Disease Service
24/7/365
405-271-4060
http://ads.health.ok.gov