Memory consolidation and accelerated forgetting in children with idiopathic generalized epilepsy
7
Memory consolidation and accelerated forgetting in children with idiopathic generalized epilepsy Michelle Davidson a , Liam Dorris a,b, * , Mary O’Regan b , Sameer M. Zuberi b a Section of Psychological Medicine, University of Glasgow, Glasgow, UK b Fraser of Allander Neurosciences Unit, Royal Hospital for Sick Children, Glasgow, UK Received 23 March 2007; revised 4 May 2007; accepted 12 May 2007 Available online 21 August 2007 Abstract Whether children with idiopathic generalized epilepsy exhibit accelerated forgetting of verbal and nonverbal information in compar- ison to healthy controls matched for age and IQ was explored. Twenty-one children with IGE were compared with 21 healthy controls on measures of verbal and visuospatial memory at delays of 30 minutes and 1 week by use of a minimum-learning criterion controlled for initial learning. For the auditory–verbal memory test, group performance was comparable at 30 minutes, but children with IGE recalled significantly less than controls at 1 week. When the number of learning trials to criterion was controlled, the main effects of group and delay became nonsignificant. No group differences were found with respect to recognition performance. Comparisons for the visuospatial task were nonsignificant. Overall, poor initial learning efficiency led to retrieval difficulties, specifically at the longer delay, and was more common in the IGE group. These results, although preliminary, have implications for education planning in childhood IGE. Ó 2007 Elsevier Inc. All rights reserved. Keywords: Memory; Accelerated forgetting; Consolidation; Idiopathic generalized epilepsy 1. Introduction Although many people with temporal lobe epilepsy (TLE) complain of memory difficulties, their performance on standardized memory tests is often observed to be within the average range or disproportionate to their sub- jective complaints [1–3]. Although not widely researched, a number of case reports and small group studies have demonstrated that despite normal learning and retention of information at standard delays of around 30 minutes, such patients exhibit an accelerated rate of forgetting over longer retention periods of days or weeks [1,4–8]. These findings pose a challenge to traditional models of memory, which have assumed that information has reached long- term memory once it has been stored for longer than a few minutes [5]. The ‘‘accelerated forgetting’’ phenomenon indicates that memories have an extended period of vulnerability during which they undergo a process of slow consolidation before reaching long-term/permanent storage [1]. Indeed, the con- cept of memory consolidation and the formation of lasting memories has been the subject of much attention over the previous century, based mainly on observations of patients with temporally graded retrograde amnesia [9–11]. Despite this interest, the exact mechanism and time scale of mem- ory consolidation remain unclear, and the concept has proved complex. There is some consensus that medial tem- poral lobe (MTL) structures, particularly the hippocampal formation, are critical in the early stages of memory stor- age. This is clear from the long-known association between MTL damage and classic amnesia, in which patients are unable to store new information [6]. It is suggested that over time, the neural substrate of memory storage is grad- ually reorganized and lasting memories come to reside in 1525-5050/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.yebeh.2007.05.004 * Corresponding author. Address: Fraser of Allander Neurosciences Unit, Royal Hospital for Sick Children, Glasgow G3 8SJ, UK. Fax: +44 141 201 9270. E-mail address: [email protected] (L. Dorris). www.elsevier.com/locate/yebeh Available online at www.sciencedirect.com Epilepsy & Behavior 11 (2007) 394–400
-
Upload
michelle-davidson -
Category
Documents
-
view
213 -
download
0
Transcript of Memory consolidation and accelerated forgetting in children with idiopathic generalized epilepsy

Available online at www.sciencedirect.com
www.elsevier.com/locate/yebeh
Epilepsy & Behavior 11 (2007) 394–400
Memory consolidation and accelerated forgetting in childrenwith idiopathic generalized epilepsy
Michelle Davidson a, Liam Dorris a,b,*, Mary O’Regan b, Sameer M. Zuberi b
a Section of Psychological Medicine, University of Glasgow, Glasgow, UKb Fraser of Allander Neurosciences Unit, Royal Hospital for Sick Children, Glasgow, UK
Received 23 March 2007; revised 4 May 2007; accepted 12 May 2007Available online 21 August 2007
Abstract
Whether children with idiopathic generalized epilepsy exhibit accelerated forgetting of verbal and nonverbal information in compar-ison to healthy controls matched for age and IQ was explored. Twenty-one children with IGE were compared with 21 healthy controls onmeasures of verbal and visuospatial memory at delays of 30 minutes and 1 week by use of a minimum-learning criterion controlled forinitial learning. For the auditory–verbal memory test, group performance was comparable at 30 minutes, but children with IGE recalledsignificantly less than controls at 1 week. When the number of learning trials to criterion was controlled, the main effects of group anddelay became nonsignificant. No group differences were found with respect to recognition performance. Comparisons for the visuospatialtask were nonsignificant. Overall, poor initial learning efficiency led to retrieval difficulties, specifically at the longer delay, and was morecommon in the IGE group. These results, although preliminary, have implications for education planning in childhood IGE.� 2007 Elsevier Inc. All rights reserved.
Keywords: Memory; Accelerated forgetting; Consolidation; Idiopathic generalized epilepsy
1. Introduction
Although many people with temporal lobe epilepsy(TLE) complain of memory difficulties, their performanceon standardized memory tests is often observed to bewithin the average range or disproportionate to their sub-jective complaints [1–3]. Although not widely researched,a number of case reports and small group studies havedemonstrated that despite normal learning and retentionof information at standard delays of around 30 minutes,such patients exhibit an accelerated rate of forgetting overlonger retention periods of days or weeks [1,4–8]. Thesefindings pose a challenge to traditional models of memory,which have assumed that information has reached long-
1525-5050/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.yebeh.2007.05.004
* Corresponding author. Address: Fraser of Allander NeurosciencesUnit, Royal Hospital for Sick Children, Glasgow G3 8SJ, UK. Fax: +44141 201 9270.
E-mail address: [email protected] (L. Dorris).
term memory once it has been stored for longer than afew minutes [5].
The ‘‘accelerated forgetting’’ phenomenon indicates thatmemories have an extended period of vulnerability duringwhich they undergo a process of slow consolidation beforereaching long-term/permanent storage [1]. Indeed, the con-cept of memory consolidation and the formation of lastingmemories has been the subject of much attention over theprevious century, based mainly on observations of patientswith temporally graded retrograde amnesia [9–11]. Despitethis interest, the exact mechanism and time scale of mem-ory consolidation remain unclear, and the concept hasproved complex. There is some consensus that medial tem-poral lobe (MTL) structures, particularly the hippocampalformation, are critical in the early stages of memory stor-age. This is clear from the long-known association betweenMTL damage and classic amnesia, in which patients areunable to store new information [6]. It is suggested thatover time, the neural substrate of memory storage is grad-ually reorganized and lasting memories come to reside in

M. Davidson et al. / Epilepsy & Behavior 11 (2007) 394–400 395
the neocortex, becoming independent of MTL structures[12]. Thus, the faster changing connections of the hippo-campus allow us to learn quickly, whereas the slowerchanging connections of the neocortex are necessary forthe long-term integration and retention of such learnedinformation [11]. Despite the disagreement in the literatureabout the specific mechanism of memory consolidation, itseems clear that it must involve some form of interactionbetween the MTL and the neocortex.
It has therefore been suggested that accelerated forget-ting may result either from organic damage to neocorticalstorage sites or from disruption to the transfer of informa-tion between the MTL and neocortex due to, for example,epileptiform activity [6]. Although all the case reports andgroup studies discussed here involved patients with TLE, itseems plausible that generalized epileptiform activity couldalso disrupt slow consolidation processes. Consistent withthis suggestion, Squire [13] found evidence of acceleratedforgetting in depressed patients who had been treated withelectroconvulsive therapy (ECT), a procedure that pro-duces a generalized convulsive seizure. Participants weretested 2 hours after receiving ECT and served as theirown controls, being tested again (using different stimulusmaterial) 4 months later. There was no difference in theirmemory performance at delays of 10 minutes or 2 hours,but significantly poorer performance was observed at the32-hour delay after receiving ECT. In addition, after equat-ing initial learning, patients who had received ECT exhib-ited an accelerated rate of forgetting in comparison topatients with Korsakoff’s syndrome and a patient withdiencephalic amnesia, whose difficulties were of the typeseen in classic amnesia. Squire [13] concluded that thisaccelerated forgetting occurred because of the effects ofgeneralized seizure activity on the temporal lobes.
The existing research on accelerated forgetting hasfocused almost exclusively on TLE or temporal lobe dys-function, with few studies including samples of patientswith primary generalized epileptic seizures. Furthermore,the phenomenon does not appear to have been studiedin pediatric epilepsy samples, despite the potentially nega-tive impact on educational attainment should it exist.Indeed, there is evidence that children with idiopathicgeneralized epilepsy (IGE) often show poorer educationalattainment than their healthy peers and, despite being ofaverage intelligence, can also be at long-term risk oflearning impairment even when seizures are well con-trolled [14–18].
IGE denotes a group of disorders characterized by gen-eralized seizures that occur in the absence of structuralbrain damage, with no abnormal neurological signs[19,20] and for which no etiology can be found other thana genetic predisposition [21]. The majority of affected chil-dren follow a normal developmental course, and the prog-nosis with respect to seizure control is generally favorable.IGE therefore provides a unique opportunity to study theeffects of epileptiform activity on memory consolidation,in comparison to previous literature that has generally
focused on severe TLE, often involving pre- or postsurgicalpatients.
The current study aimed to compare retention of verbaland visual information over an extended delay of 1 weekbetween children with IGE and healthy controls matchedfor age and IQ.
2. Methods
The ethics committee of the Yorkhill Division of the NHS GreaterGlasgow Primary Care Division approved the study. Permission to recruitvia local schools was granted by Glasgow City Council EducationServices.
2.1. Design
A repeated-measures case–control design was used, with cases beingmatched for age and IQ on a pairwise basis. Four participants with IGEcould not be matched for age within 12 months; the age differences forthese pairs ranged from 16 to 24 months. All participants were matchedfor IQ within 1 SD on the Wechsler Abbreviated Scale of Intelligence [22].
2.2. Power calculation
Power was calculated using 8-week recall data from a study by Blakeet al. [1], involving an adult TLE sample. This study was chosen as thedesign most closely approximating that of the current study, and the sam-ple included participants with less severe TLE than in previous studies.Although the delay period used by Blake et al. was significantly longerthan 1 week, this study was felt to be the most methodologically robust,as it was the only one to systematically assess longer term recall in ade-quately sized groups. We also chose a 1-week recall period as we wererecruiting children from the age of 6 and felt that a shorter delay wouldbe more developmentally appropriate. Assuming normal distribution,equal variances between the groups, and a significance level of 0.05, wecalculated that 18 participants were required for each group to achieve apower of 0.8.
2.3. Participants
All children between the ages of 6 and 16 who had attended either theepilepsy clinic or the EEG department at the Royal Hospital for Sick Chil-dren and whom were identified as having an established diagnosis of IGEwere invited to participate. Twenty-seven children with IGE consented totake part in the study, although four were subsequently excluded (twobecause of failure to reach the 90% learning criterion for the Stories sub-test, one because of comorbid attention deficit hyperactivity disorder, andone because the diagnosis of IGE was revised to generalized epilepsy withfebrile seizures plus). Two children were not tested because of late returnof consent forms. Twenty-one children with IGE aged between 8 and 16were therefore included in final analyses (7 male, 14 female). Diagnoseswere confirmed by a consultant neurologist prior to neuropsychologicalassessment, through review of medical files and existing EEG recordsand according to ILAE criteria [20]. No patient had a history of develop-mental delay, Full Scale IQ less than 70, or history of head injury or anyneurological condition other than IGE. Clinical data for the IGE groupare summarized in Table 1.
Thirty-six control group participants were recruited via four local pri-mary and secondary schools using the same exclusion criteria applied tothe IGE group. Five children were subsequently excluded (one had expres-sive language disorder, one had been diagnosed with cerebral palsy, twowere below the lower age limit for the study, and one child was excludedbecause English was not the first language), and one child was lost to fol-low-up due to absence from school. Control subjects were also excluded ifthey had a positive family history of epilepsy. After participants werematched as closely as possible for age and IQ, an additional nine control

Table 1Clinical characteristics of IGE group (n = 21)
Syndromal diagnosisChildhood absence epilepsy 9 (40.9)a
Juvenile absence epilepsy 1 (4.8)Juvenile myoclonic epilepsy 4 (19.0)Generalized tonic–clonic seizure only 4 (19.0)Unclassified IGE 3 (14.3)
Epilepsy statusActive 16 (76.2)Remitted 5 (22.7)
Current seizure frequencyNone in last 2 years (remitted) 5 (22.7)Daily 3 (14.3)1 or 2 per week 4 (19)1 or 2 per month 2 (9.5)Fewer than 1 per month 7 (33.3)
Current number of antiepileptic drugs0 4 (19.0)1 15 (71.4)2 2 (9.5)
Antiepileptic drug prescribedSodium valproate 10 (47.6)Lamotrigine 4 (19.0)Sodium valproate/lamotrigine polytherapy 1 (4.8)Levetiracetam/clobazam polytherapy 1 (4.8)None 5 (22.7)
a Results are expressed as n (%).
Table 3Memory and educational progress ratings for the IGE group (n = 21)
Child rating of memory problemsNo problems 16 (76.2)a
A little problematic 1 (4.8)Quite problematic 1 (4.8)Very problematic 3 (14.3)
Parent rating of child’s memory problemsNo problems 14 (66.7)Mildly problematic 2 (9.5)Quite problematic 4 (19.0)Very problematic 1 (4.8)
Delayed school entry 0
396 M. Davidson et al. / Epilepsy & Behavior 11 (2007) 394–400
group participants remained and were not included in analyses. Matchingtook place before the results of memory testing were scored to avoid bias.All children and a parent/guardian gave their informed consent toparticipate.
Demographic and assessment data for the two groups are summarizedin Table 2. There was a greater proportion of females in the control group,although the groups were statistically comparable with respect to age, FullScale IQ, Verbal IQ, and Performance IQ (see Table 2).
2.4. Assessment procedures: Standard
The Wechsler Abbreviated Scale of Intelligence (WASI) [22] wasadministered to all participants to provide a brief measure of intellectualability. This test consists of two verbal and two nonverbal subtests andyields overall (Full Scale), Verbal (VIQ), and Performance (PIQ) IQscores. Information was also collected from IGE group participants andtheir parents/guardians with respect to epilepsy/seizure variables, func-tional memory difficulties, and school progress.
2.5. Assessment procedures: Experimental assessment of memory
retention
The Stories and Dot Locations subtests of the Children’s MemoryScale (CMS) [23] were used to assess verbal and visuospatial memory. Par-ticipants were required to learn two short stories to 90% accuracy and a
Table 2Mean age and IQ for the IGE and control groups and results ofindependent sample t tests
IGE group Control group t(40) P
Age (range) 11.5 (8–16) 11.9 (7–16) 0.50 0.62Full Scale IQ (SD) 99.4 (14.4) 98.5 (11.6) 0.22 0.75Verbal IQ (SD) 98.9 (13.4) 96.1 (11.6) 0.74 0.47Performance IQ (SD) 99.8 (15.4) 101.6 (12.7) �0.43 0.67
pictorial array of dots to 83% accuracy over at least two consecutive trials.In the case of the Dot Locations subtest, this 83% learning criterionallowed for one error in each of the two age versions, which had differenttotal scores. In accordance with standardized administration procedures,three versions of the Stories subtest and two versions of the Dot Locationssubtest were used depending on the age of the child. Children who wereunable to reach the learning criteria within a maximum of 10 consecutivetrials were excluded from the study and did not participate any further.Delayed recall and recognition were assessed 30 minutes after the lastlearning trial and, then again, 7 days later. Children were instructed notto rehearse the material during the 1-week delay or to write it down.
Recall scores for both the Stories and Dot Locations subtests wereconverted into percentages to allow comparison between versions for dif-ferent age groups, which differed with respect to maximum total score. Itwas not possible to convert raw scores into Z scores because of the smallnumber of participants who received the versions for children agedbetween 6 and 8. As Stories recognition scores were comparable acrossversions; analyses were conducted using raw scores. The distributions ofall variables were examined using the Kolmogorov–Smirnov test to deter-mine normality.
2.6. Statistical analysis
All statistical analyses were conducted using SPSS for Windows. Nor-mally distributed data were analyzed using split-plot analysis of variance(ANOVA), with a within-participants factor of delay (30 minutes vs 1week) and a between-participants factor of group (IGE vs control).Planned comparisons were conducted using independent t tests orMann–Whitney U tests as appropriate. Two-tailed tests were used whencomparing IQ and age between the groups, and one-tailed tests were usedfor all main analyses. a significance levels were set at 60.05 for the mainanalyses and 60.008 for planned comparisons to account for multipletesting.
3. Results
Table 3 summarizes the functional memory ratings andeducational progress variables for the IGE group. Parentsreported a higher frequency of memory problems than chil-dren, with one-third (n = 7) indicating that their child’s
Repeated school year 0
Ever received learning support in school 5 (22.7)
Parent’s rating of school progressNo problems 12 (57.1)Mildly concerned 4 (19.0)Fairly concerned 4 (19.0)Very concerned 1 (4.8)
a Results are expressed as n (%).
84
86
88
90
92
94
96
98
100
Mea
n %
reca
ll
Groupepilepsycontrol
M. Davidson et al. / Epilepsy & Behavior 11 (2007) 394–400 397
memory caused some degree of difficulty on a day-to-daybasis. Only four children (19.0%) felt their memory wasproblematic. However, those children who felt they haddifficulties with memory were more likely to rate these asvery problematic (n = 3) than were their parents (n = 1).All children in the IGE group were attending mainstreamschools, although five (23.8%) had at some time receivedlearning support. A large proportion of parents (n = 9,42.9%) reported some degree of concern about their child’sprogress in school. No participant had been delayed inschool entry or repeated a school year.
last learning trial 30 minutes 1 weekDelay
74
76
78
80
82
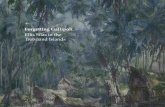
Fig. 1. Stories recall scores for the IGE and control groups across delays.
3.1. Analysis 1: Long-term memory
Descriptive statistics for performance on the Stories sub-test are summarized in Table 4. Independent t tests indi-cated that the IGE group required significantly morelearning trials than controls to reach criterion(t(40) = 2.46, P = 0.009, d = 0.75).
A split-plot ANOVA conducted on the Stories recalldata revealed significant main effects of group(F(1, 40) = 4.83, P = 0.017) and delay (F(1,40) = 36.93,P < 0.001) and a significant group · delay interaction(F(1, 40) = 5.59, P = 0.012). These data are illustratedgraphically in Fig. 1. With partial g2 used as a measureof effect size, 48% of the overall variance was attributableto the effect of delay, 11% to the effect of group, and12% to the group · delay interaction.
Planned independent t tests revealed no significantgroup differences at 30 minutes (t(40) = �0.96, P = 0.175;d = �0.29), but confirmed that the IGE group recalled sig-nificantly less than controls at 1 week (t(40) = �2.56,P = 0.007, d = �0.78). There was no effect of gender oneither the initial learning, 1-week recall, or recognitionvariable.
Mann–Whitney U tests conducted on the Stories recog-nition data revealed no significant group differences ateither 30 minutes (U = 173.5, P = 0.108) or 1 week(U = 183.0, P = 0.167). Small effect sizes were obtainedfor Stories recognition at both the 30-minute (r = 0.26)and 1-week (r = 0.21) delays, indicating that only a smallproportion of the variance in performance was accountedfor by the effect of group.
Descriptive statistics for performance on the Dot Loca-tions subtest are summarized in Table 5. Analyses for this
Table 4Descriptive statistics for performance of the IGE and control groups on the S
IGE group
Mean (SD)
Number of learning trials to criterion 9.05 (3.9)Last learning trial (% recall) 93.8 (3.2)30-Minute recall (% recall) 87.7 (7.3)1-Week recall (% recall) 75.8 (13.8)30-Minute recognition score (out of 30) 28.3 (1.3)1-Week recognition score (out of 30) 27.5 (2.4)
test were conducted using data from 19 children with IGEand 19 matched controls.
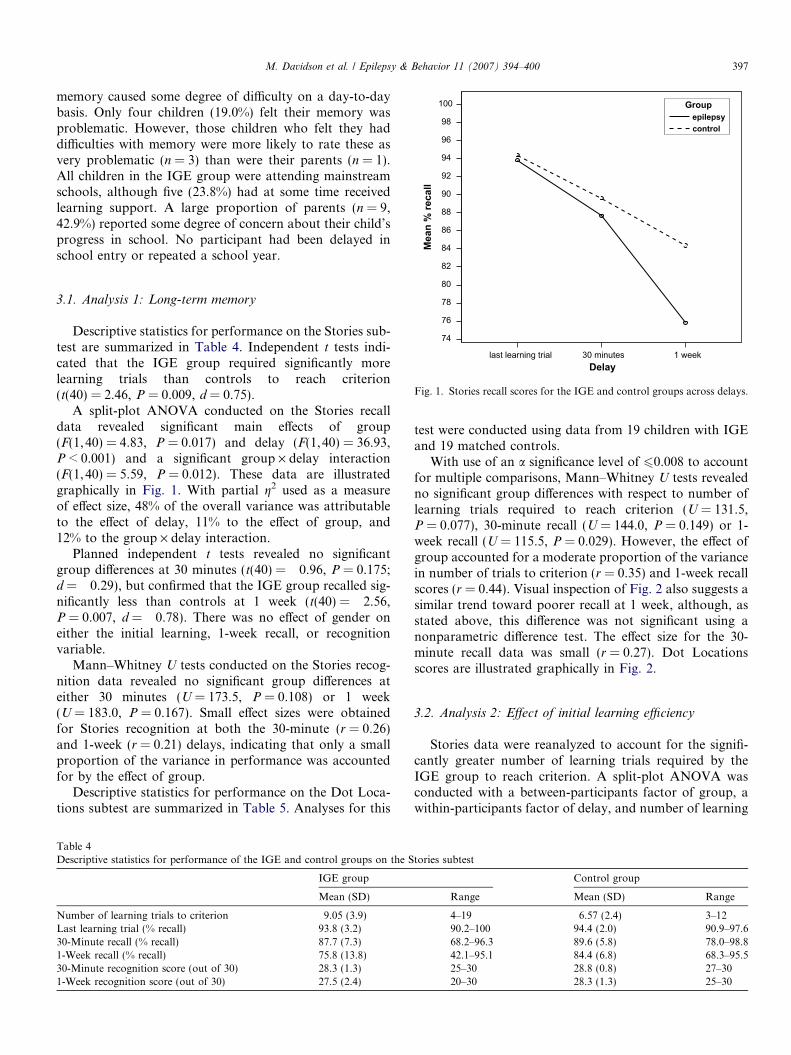
With use of an a significance level of 60.008 to accountfor multiple comparisons, Mann–Whitney U tests revealedno significant group differences with respect to number oflearning trials required to reach criterion (U = 131.5,P = 0.077), 30-minute recall (U = 144.0, P = 0.149) or 1-week recall (U = 115.5, P = 0.029). However, the effect ofgroup accounted for a moderate proportion of the variancein number of trials to criterion (r = 0.35) and 1-week recallscores (r = 0.44). Visual inspection of Fig. 2 also suggests asimilar trend toward poorer recall at 1 week, although, asstated above, this difference was not significant using anonparametric difference test. The effect size for the 30-minute recall data was small (r = 0.27). Dot Locationsscores are illustrated graphically in Fig. 2.
3.2. Analysis 2: Effect of initial learning efficiency
Stories data were reanalyzed to account for the signifi-cantly greater number of learning trials required by theIGE group to reach criterion. A split-plot ANOVA wasconducted with a between-participants factor of group, awithin-participants factor of delay, and number of learning
tories subtest
Control group
Range Mean (SD) Range
4–19 6.57 (2.4) 3–1290.2–100 94.4 (2.0) 90.9–97.668.2–96.3 89.6 (5.8) 78.0–98.842.1–95.1 84.4 (6.8) 68.3–95.525–30 28.8 (0.8) 27–3020–30 28.3 (1.3) 25–30

Table 5Descriptive statistics for performance of the IGE and control groups on the Dot Locations subtesta
IGE group Control group
Mean (SD) Range Mean (SD) Range
Number of learning trials to criterion 2.3 (1.1) 1–5 1.8 (1.0) 1–4% Recall Last learning trial 97.7 (5.7) 87.5–100 9.5 (6.1) 83.3–10030 minutes 85.3 (16.8) 37.5–100 89.7 (17.0) 50.0–1001 week 68.9 (23.3) 25–100 83.3 (18.2) 50–100
a Based on comparison of 19 children with IGE and 19 controls.
65
70
75
80
85
90
95
100
last learning trial 30-minDelay
IGE
Mea
n %
Rec
all
1-week
Control
Fig. 2. Dot Locations recall scores for the IGE and control groups acrossdelays.
398 M. Davidson et al. / Epilepsy & Behavior 11 (2007) 394–400
trials to criterion as covariate. This analysis revealed nosignificant main effects of group (F(1,39) = 0.60,P = 0.23) or delay (F(1, 39) = 1.94, P = 0.086) but a signif-icant group · delay interaction (F(1,39) = 3.42, P = 0.036).A significant main effect of number of learning trials to cri-terion was observed (F(1, 39) = 25.46, P < 0.001). Withpartial g2 used as a measure of effect size, only 1.5% ofthe variance was attributable to the effect of group, 4.7%to the effect of delay, 8.1% to the group · delay interaction,and 39.5% to the effect of number of learning trials tocriterion.
It was not possible to conduct similar analyses for theDot Locations data, which were not normally distributed.However, correlational analyses using Spearman’s q indi-cated no significant relationship between the numbers oflearning trials to criterion and 30-minute or 1-week recallfor either the IGE or control group.
3.3. Discussion
The present study aimed to investigate memory in chil-dren with IGE over delays longer than those typicallyassessed by standardized memory tests, comparing perfor-mance with healthy matched controls. It was hypothesizedthat the groups would not be distinguished on measures ofinitial learning or recall/recognition at a 30-minute delay,
but that children with IGE would exhibit an acceleratedrate of forgetting, with poorer recall/recognition scoresthan controls at the 1-week delay.
The results indicated that, contrary to expectations, chil-dren with IGE exhibited poorer initial learning efficiencythan controls on the Stories subtest, requiring a greaternumber of trials to reach 90% accuracy. Initial analysesfor Stories recall indicated that, as hypothesized, thegroups performed comparably at the 30-minute delay,but children with IGE recalled significantly less than con-trols after 1 week. However, the lack of group differenceswith respect to Stories recognition indicates that the poorerperformance of the IGE group was due to difficulties withthe retrieval of successfully stored auditory–verbal infor-mation at longer delays rather than poor retention (and,hence, failed consolidation). Furthermore, when the effectof initial learning efficiency was controlled for, the maineffects of group and delay were no longer significant. Ittherefore seems that the group differences initially observedwere due to the poorer learning efficiency of the IGEgroup, which had a negative impact on access to storedinformation only at the longer delay of 1 week. Poorer ini-tial learning did not appear to affect retrieval at the 30-min-ute delay.
The results for visuospatial memory were less clear.Analyses revealed no group differences with respect to ini-tial learning or recall at either delay on the Dot Locationssubtest, suggesting equivalent rates of learning and forget-ting. However, moderate effect sizes were obtained for thenumber of learning trials required to reach criterion andrecall at the 1-week delay. In addition, it is possible thatthe ‘‘forced choice’’ response method for this task resultedin reduced ability to discriminate differences in recall abil-ity. Children are required to place all counters on theresponse grid to represent the array of dots shown in thelearning trials, and are instructed to guess if unsure.Because the number of counters is equal to half the avail-able number of squares on the grid, the total possible var-iance in scores is limited, and it seems likely that somecorrect responses will occur through chance. As the DotLocations subtest does not incorporate a recognition com-ponent, it was not possible to comment on whether lowermean scores in the IGE group were due to poorer retrievalrather than retention.
The findings of the present study suggest that poor ini-tial learning efficiency leads to retrieval difficulties with

M. Davidson et al. / Epilepsy & Behavior 11 (2007) 394–400 399
increasing time and that such inefficiency is more commonin children with IGE than controls. These findings are notconsistent with prevailing interpretations of consolidationtheory, which suggest that a failure of consolidation leadsto a failure of long-term (neocortical) storage [24]. How-ever, various recent findings have posed a challenge to thisview of consolidation. Numerous animal studies have dem-onstrated that the administration of various amnesticagents within a time-limited period after learning resultsin retrograde amnesia for that learning [25]. However,reports of spontaneous recovery of this ‘‘lost’’ memoryand observations that exposure to cues associated withthe initial learning can elicit the previously conditionedresponse indicate that the ‘‘consolidation-blocking’’ agentsdid not prevent memory storage, but merely prevented itsexpression [25]. It has therefore been suggested that abroader definition of consolidation as the process of stabil-ization of the memory trace and its maturation into a formsuitable for later retrieval may be appropriate [24]. Theresults of the present study could be interpreted as consis-tent with this broader definition.
Despite this, the memory impairments observed in chil-dren with IGE appear to be qualitatively different fromthose reported in the majority of previously publishedreports of accelerated forgetting, in which recognition aswell as recall performance were generally severelyimpaired. In addition, hypothesizing disrupted consolida-tion in the IGE group would be difficult due to the (pre-sumed) absence of organic brain damage and the lowincidence of seizures in the delay period. Instead, it seemsthat impaired long-term recall was due to problems at thestage of initial encoding.
One important issue that requires further study concernsthe impact of antiepileptic drugs (AEDs) on memoryencoding and consolidation processes. Around 80% (17/21) of the children in this study were taking medication(15 received monotherapy and 2 duotherapy). Of thosereceiving monotherapy, 10 were taking sodium valproateand 4 lamotrigine. Although sodium valproate and lamo-trigine have generally been considered to be drugs with asafe cognitive profile, they do, in common with all AEDs,have absolute cognitive side effects mostly resulting in amild, general psychomotor slowing [26,27]. However,although both seizures and AED therapy have been impli-cated in causing cognitive problems [28–30], the underlyingbrain disease giving rise to epilepsy can also have a negativeeffect on cognition. Addressing the question of whetherthose children with treated IGE are more prone to initialacquisition deficits of the form observed in the presentstudy than those children with untreated IGE requires farlarger sample sizes and would be an important basis onwhich to look at cognition and AEDs in childhood IGEusing a multicenter collaboration.
Qualitative observations of memory performance indi-cated that recall of the stories was poorly organized duringlearning for many of the children with IGE (and some con-trols), leading to a greater number of trials to reach crite-
rion. Recall frequently did not occur in the sequence inwhich the story was presented, and the stories appearedto be encoded as a collection of information ‘‘chunks’’rather than a coherent whole, tied together by a theme. Itseems possible that poorer quality memory traces may besufficient for recall at the 30-minute delay but, through pro-cesses of normal forgetting with increasing time, may resultin the threshold for retrieval failure being reached soonerthan for better quality traces. Such processes are poorlyunderstood, although retroactive interference from infor-mation encoded during the delay has been suggested asone likely mechanism [31].
It is of note that although the two groups were of equalintellectual ability, children with IGE manifested deficits inthe storage of information. One-third of parents reportedthat their child’s memory difficulties caused some degreeof functional impairment, and almost half were concernedabout their child’s progress in school. These findings are inkeeping with a growing body of evidence suggesting thatdespite overall average intellectual ability, children withIGE may manifest subtle impairments in many areas ofcognition leading to functional impairment [14–18].Although the finding of poorer encoding of informationin children with IGE is not uncommon, the differentialimpact of poor initial learning on recall at short and longdelays is worthy of note. While current standardized clini-cal memory tests can detect encoding difficulties, they donot reflect the degree of recall impairment that may resultfrom such difficulties because of reliance on delays of only30 minutes. Accelerated ‘‘forgetting’’ seems a potentiallyrelevant consideration in all cases of generalized epilepsyin childhood.
Although many children with epilepsy do well academi-cally and occupationally, they are, as a group, at far higherrisk for learning problems [16]. As a group, they do lesswell than their peers, even during periods when they arenot having active seizures [32,33]. Therefore, the currentfinding of poor initial encoding abilities has implicationsfor how we consider vulnerability in these children. Thefinding of a specific deficit in initial encoding, where in factchildren with IGE required 50% more learning trials toreach the 90% criterion than controls, has significant impli-cations for the classroom. It is also important to considerthat this difference was found using the quiet and distrac-tion-free environment of a hospital consulting room witha high level of adult attention and support. Presumably,these learning deficits would be amplified within a busyclassroom.
The present study was in many ways exploratory, andthe findings need to be replicated in larger samples. Thiswould also allow comparison between individual IGE syn-dromes. Future research should focus on improving meth-ods for assessing nonverbal memory and on developingstandardized clinical tests that allow comparison of recallperformance at longer delays with rigorous normativedata. In addition, it would be of interest to test recall andrecognition performance at delays beyond 1 week to deter-

400 M. Davidson et al. / Epilepsy & Behavior 11 (2007) 394–400
mine the precise nature of the ‘‘forgetting’’ curve in thisclinical population.
Acknowledgments
We thank all of the children who participated in thestudy and the staff at Our Lady of Assumption RomanCatholic Primary School, Thornwood Primary School,and Cleveden Secondary School.
References
[1] Blake RV, Wroe SJ, Breen EK, McCarthy RA. Accelerated forget-ting in patients with epilepsy: evidence for impairment in memoryconsolidation. Brain 2000;123:472–83.
[2] Corcoran R, Thompson P. Memory failure in epilepsy: retrospectivereports and prospective recordings. Seizure 1992;1:37–42.
[3] Gleissner U, Helmstaedter C, Quiske A, Elger CE. The performance–complaint relationship in patients with epilepsy: a matter of dailydemands? Epilepsy Res 1998;32:401–9.
[4] O’Connor M, Sieggreen MA, Ahern G, Schomer D, Mesulam M.Accelerated forgetting in association with temporal lobe epilepsy andparaneoplastic encephalitis. Brain Cogn 1997;35:71–84.
[5] Kapur N, Millar J, Colbourn C, Abbott P, Kennedy P, Docherty T.Very long-term amnesia in association with temporal lobe epilepsy:evidence for multiple-stage consolidation processes. Brain Cogn1997;35:58–70.
[6] Mayes AR, Isaac CL, Holdstock JS, Cariga P, Gummer A, RobertsN. Long-term amnesia: a review and detailed illustrative case study.Cortex 2003;39:567–603.
[7] Martin RC, Loring DW, Meador KJ, Lee GP, Thrash N, Arena JG.Impaired long-term retention despite normal verbal learning inpatients with temporal lobe dysfunction. Neuropsychology1991;5:3–12.
[8] Jokeit H, Daamen M, Zang H, Janszky J, Ebner A. Seizuresaccelerate forgetting in patients with left-sided temporal lobeepilepsy. Neurology 2001;57:125–6.
[9] Lechner HA, Squire LR, Byrne JH. 100 Years of consolidation—remembering Muller and Pilzecker. Learn Memory 1999;6:77–87.
[10] McGaugh JL. Memory—a century of consolidation. Science2000;287:248–51.
[11] Meeter M, Murre JMJ. Consolidation of long-term memory:evidence and alternatives. Psychol Bull 2004;130:843–57.
[12] Alvarez P, Squire LR. Memory Consolidation and the medialtemporal lobe: a simple network model. Proc Natl Acad Sci USA1994;9:7041–5.
[13] Squire LR. Two forms of human amnesia: an analysis of forgetting. JNeurosci 1981;1:635–40.
[14] Sturniolo MG, Galletti F. Idiopathic epilepsy and school achieve-ment. Arch Dis Child 1994;70:424–8.
[15] Wirrell EC, Camfield CS, Camfield PR, Dooley JM, Gordon KE,Smith B. Long-term psychosocial outcome in typical absenceepilepsy: sometimes a wolf in sheep’s clothing. Arch Paediatr AdolescMed 1997;15:152–8.
[16] Bailet LL, Turk WR. The impact of childhood epilepsy on neuro-cognitive and behavioural performance a prospective longitudinalstudy. Epilepsia 2000;41:426–31.
[17] Echenne B, Cheminal R, Roubertie A, Rivier F. Are idiopathicgeneralized epilepsies of childhood really benign? Epileptic Disord2001;3(Spec. No. 2):SI67–72.
[18] Henkin Y, Sadeh M, Kivity S, Shabtai E, Kishon-Rabin L, GadothN. Cognitive function in idiopathic generalised epilepsy of childhood.Dev Med Child Neurol 2005;47:126–32.
[19] Commission on Classification and Terminology of the InternationalLeague Against Epilepsy. Proposal for revised classification ofepilepsies and epileptic syndromes. Epilepsia 1989;30:389–399.
[20] International League Against Epilepsy Task Force on Classificationand Terminology. Available at: http://www.epilepsy.org/; 2004.
[21] Koutroumanidis M. Idiopathic generalised epilepsies. NationalSociety for Epilepsy; 2003. Available at: www.e-epilepsy.org.uk.
[22] Wechsler D. Manual for the Wechsler Abbreviated Scale of Intelli-gence (WASI). San Antonio, TX: Harcourt Assessment; 1999.
[23] Cohen MJ. The Children’s Memory Scale. San Antonio, TX: Psy-chological Corp; 1997.
[24] Dudai Y. The neurobiology of consolidation, or, how stable is theengram? Annu Rev Psychol 2004;55:51–86.
[25] Riccio DC, Millin PM, Gisquet-Verrier P. Retrograde amnesia:forgetting back. Curr Directions Psychol Sci 2003;12:41–4.
[26] Aldenkamp AP, Alpherts WCJ, Blennow G, et al. Withdrawal ofantiepileptic medication—effects on cognitive function in children:the multicentre Holmfrid Study. Neurology 1993;43:41–50.
[27] Aldenkamp AP, De Krom M, Reijs R. Newer antiepileptic drugs andcognitive issues. Epilepsia 2003;44(Suppl. 4):21–9.
[28] Holmes GL, Khazipov R, Ben-Ari Y. Seizure-induced damage in thedeveloping human: relevance of experimental models. Prog Brain Res2002;135:321–34.
[29] Holmes GL. Effects of early seizures on later behaviour andepileptogenicity. Ment Retard Dev Disabil Rev 2004;10:101–5.
[30] Dickson JM, Wilkinson ID, Howell SJL, Griffiths PD, Grunewald RA.Idiopathic generalised epilepsy: a pilot study of memory and neuronaldysfunction in the temporal lobes, assessed by magnetic resonancespectroscopy. J Neurol Neurosurg Psychiatry 2006;77:834–40.
[31] Wixted JT. The psychology and neuroscience of forgetting. AnnuRev Psychol 2004;55:235–69.
[32] Stores G. School-children with epilepsy at risk for learning andbehaviour problems. Dev Med Child Neurol 1978;20:502–8.
[33] Seidenberg M, Beck N, Geisser M, et al. Academic achievement ofchildren with epilepsy. Epilepsia 1986;27:753–9.