
Member Benefits Program - sacrealtor.org · Gold 80 500/30 BENEFIT HMO Lifetime Maximum Unlimited...
68
Sacramento, CA 95864 Lic #0787081 www.amesgrenz.com Phone (916) 486-2900 3435 American River Drive, Suite C Contact Robyn Caspary for Benefit information Member Benefits Program Ames‐Grenz Insurance Services, Inc.
Transcript of Member Benefits Program - sacrealtor.org · Gold 80 500/30 BENEFIT HMO Lifetime Maximum Unlimited...

Sacramento, CA 95864
Lic #0787081www.amesgrenz.com
Phone (916) 486-2900
3435 American River Drive, Suite C
Contact Robyn Caspary for Benefit information
Member Benefits Program
Ames‐Grenz Insurance Services, Inc.

BENEFIT
Lifetime Maximum
Calendar Year Deductible :
Individual / Family
Calendar Year Max Out‐of‐Pocket:
Individual / Family
Office Visit
Most Laboratory Tests
Most X‐rays & Diagnostics
MRI/CT/PET
Preventive Care Exam
Hospitalization
Outpatient Surgery
Emergency Room
Urgent Care Center
Maternity:
Inpatient
Prenatal/First Postpartum Visit
Mental Health:
Inpatient
Outpatient
Substance Abuse:
Inpatient Detox Only
Prescriptions:
Generic
Deductible (Brand Name)
Brand
Pediatric Dental & Vision (Up to age 19)
Deductible / Waiting Period
Annual Out‐of‐Pocket Maximum
Office Visit
Cleaning & Exam
Periodontics
Restorative
Endodontics
Prosthodontics
Orthodontics (Medically Necessary)
Pediatric Vision (Up to age 19)
Includes Exam and Eyewear
Adult Vision Exam
Adult Optical (Eyewear)
Provider Restrictions
Kaiser Members & Dependents
Open Enrollment
One standard pair of frames & lenses or contact lenses per calendar year
$85 ‐ $350 Copay Depending on Procedure
$25 ‐ $350 Copay Depending on Procedure
$85 ‐ $300 Copay Depending on Procedure
New Members: May join the 1st of the month following 30 days of membership.
Qualifying Events: you may join within 30 days after you have a loss of coverage,
marriage, birth or adoption. Over
Age Dependents: may remain on coverage up to age 26.
November 1st ‐ November 30th
$0 Copay
$175 allowance
Kaiser
Eligibility Guidelines ‐ GUARANTEED ISSUE
$0 Copay
$15 Copay
$0 Deductible & No Waiting Periods
$65 ‐ $350 Copay Depending on Procedure
$350 Copay
None
$20 Copay
$290 per Day (Days 1‐5) per Admission
$350 per Child / $700 Multichild
$0 Copay
$290 per Day (Days 1‐5) per Admission
$20 Copay
$290 per Day (Days 1‐5) per Admission
(Up to a 30‐Day Supply)
$5 Copay
$150 Copay (waived if admitted directly to hospital)
$40 Copay
$150 Copay
$0 Copay
$0 Copay
$20 Copay
Unlimited
None
$290 per Day (Days 1‐5) per Admission
$290 Copay per Procedure
KAISER PERMANENTE
Platinum 90 0/20HMO
$4,000 / $8,000 (Embedded)
$20 (Primary) $40 (Specialty)
December 1, 2016 ‐ November 30, 2017

Gold 80 500/30BENEFIT HMO
Lifetime Maximum Unlimited
Calendar Year Deductible :
Individual / Family $500 / $1,000 (1)
Calendar Year Max Out‐of‐Pocket:
Individual / Family $6,250 / $12,500
Office Visit $30 Copay
Most Laboratory Tests $20 Copay
Most X‐rays & Diagnostics $20 Copay
MRI/CT/PET $250 Copay
Preventive Care Exam $0 Copay
Hospitalization $600 per Day (Days 1‐5) per Admission After Deductible
Outpatient Surgery $600 Copay per Procedure After Deductible
Emergency Room
$250 Copay After Deductible
(waived if admitted directly to hospital)
Urgent Care Center $30 Copay
Maternity:
Inpatient $600 per Day (Days 1‐5) per Admission After Deductible
Prenatal/First Postpartum Visit $0 Copay
Mental Health:
Inpatient $600 per Day (Days 1‐5) per Admission After Deductible
Outpatient $30 copay
Substance Abuse:
Inpatient Detox Only $600 per Day (Days 1‐5) per Admission After Deductible
Prescriptions: (Up to a 30‐Day Supply)
Generic $15 Copay
Deductible (Brand Name) None
Brand $50 Copay
Pediatric Dental & Vision (Up to age 19)
Deductible / Waiting Period $0 Deductible & No Waiting Periods
Annual Out‐of‐Pocket Maximum $350 per Child / $700 Multichild
Office Visit $0 Copay
Cleaning & Exam $0 Copay
Periodontics $85 ‐ $350 Copay Depending on Procedure
Restorative $25 ‐ $350 Copay Depending on Procedure
Endodontics $85 ‐ $300 Copay Depending on Procedure
Prosthodontics $65 ‐ $350 Copay Depending on Procedure
Orthodontics (Medically Necessary) $350 Copay
Pediatric Vision (Up to age 19)
Includes Exam and Eyewear
Adult Vision Exam $0 Copay
Adult Optical (Eyewear) Not Covered
Provider Restrictions
Kaiser Members & Dependents
Open Enrollment
Kaiser
Eligibility Guidelines ‐ GUARANTEED ISSUE
New Members: May join the 1st of the month following 30 days of membership.
Qualifying Events: you may join within 30 days after you have a loss of coverage, marriage, birth or adoption.
Over Age Dependents: may remain on coverage up to age 26.
$50 Copay
$0 Deductible & No Waiting Periods
One standard pair of frames & lenses or
contact lenses per calendar year
One standard pair of frames & lenses or
contact lenses per calendar year
$85 ‐ $300 Copay Depending on Procedure
$35 Copay
$655 per Day (Days 1‐5) per Admission
November 1st ‐ November 30th
$65 ‐ $350 Copay Depending on Procedure
$350 Copay
Not Covered
$0 Copay
$15 Copay
$350 per Child / $700 Multichild
Unlimited
None
$655 per Day (Days 1‐5) per Admission
$655 Copay per Procedure
$250 Copay
(waived if admitted directly to hospital)
$50 Copay
$250 Copay
$0 Copay
$655 per Day (Days 1‐5) per Admission
(Up to a 30‐Day Supply)
HMO
KAISER PERMANENTE
Gold 80 0/35
$0 Copay
$6,200 / $12,400
$35 (Primary) $55 (Specialty)
$35 Copay
December 1, 2016 ‐ November 30, 2017
(1) This plan has an embedded deductible and out‐of‐pocket maximum. Each family member will begin paying copayments or coinsurance after meeting his or her individual
deductible, or whenthe family deductible is satisfied. Individual family members are no longer subject to cost sharing when they reach their individual out‐of‐pocket maximum, or
when the family out‐of pocket maximum is met.
None
$655 per Day (Days 1‐5) per Admission
$35 copay
$25 ‐ $350 Copay Depending on Procedure
$0 Copay
$0 Copay
$85 ‐ $350 Copay Depending on Procedure
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
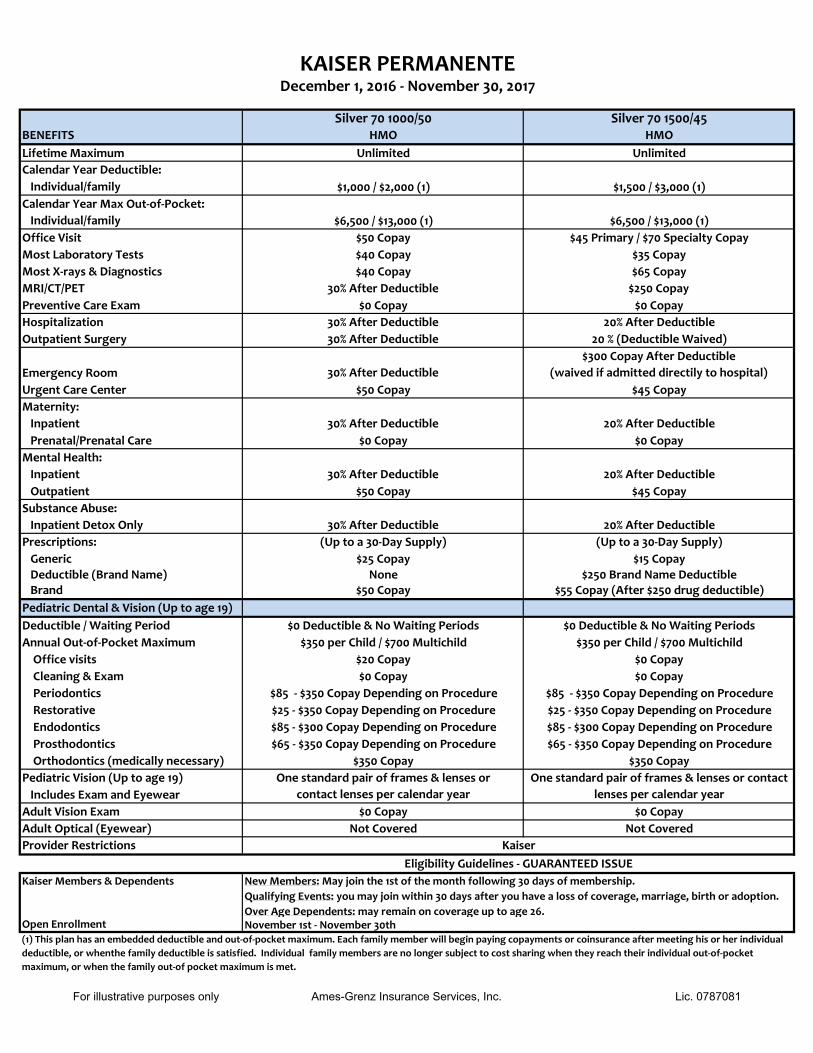
Silver 70 1000/50 Silver 70 1500/45BENEFITS HMO HMO
Lifetime Maximum Unlimited Unlimited
Calendar Year Deductible:
Individual/family $1,000 / $2,000 (1) $1,500 / $3,000 (1)
Calendar Year Max Out‐of‐Pocket:
Individual/family $6,500 / $13,000 (1) $6,500 / $13,000 (1)
Office Visit $50 Copay $45 Primary / $70 Specialty Copay
Most Laboratory Tests $40 Copay $35 Copay
Most X‐rays & Diagnostics $40 Copay $65 Copay
MRI/CT/PET 30% After Deductible $250 Copay
Preventive Care Exam $0 Copay $0 Copay
Hospitalization 30% After Deductible 20% After Deductible
Outpatient Surgery 30% After Deductible 20 % (Deductible Waived)
Emergency Room 30% After Deductible
$300 Copay After Deductible
(waived if admitted directily to hospital)
Urgent Care Center $50 Copay $45 Copay
Maternity:
Inpatient 30% After Deductible 20% After Deductible
Prenatal/Prenatal Care $0 Copay $0 Copay
Mental Health:
Inpatient 30% After Deductible 20% After Deductible
Outpatient $50 Copay $45 Copay
Substance Abuse:
Inpatient Detox Only 30% After Deductible 20% After Deductible
Prescriptions: (Up to a 30‐Day Supply) (Up to a 30‐Day Supply)
Generic $25 Copay $15 Copay
Deductible (Brand Name) None $250 Brand Name Deductible Brand $50 Copay $55 Copay (After $250 drug deductible)
Pediatric Dental & Vision (Up to age 19)
Deductible / Waiting Period $0 Deductible & No Waiting Periods $0 Deductible & No Waiting Periods
Annual Out‐of‐Pocket Maximum $350 per Child / $700 Multichild $350 per Child / $700 Multichild
Office visits $20 Copay $0 Copay
Cleaning & Exam $0 Copay $0 Copay
Periodontics $85 ‐ $350 Copay Depending on Procedure $85 ‐ $350 Copay Depending on Procedure
Restorative $25 ‐ $350 Copay Depending on Procedure $25 ‐ $350 Copay Depending on Procedure
Endodontics $85 ‐ $300 Copay Depending on Procedure $85 ‐ $300 Copay Depending on Procedure
Prosthodontics $65 ‐ $350 Copay Depending on Procedure $65 ‐ $350 Copay Depending on Procedure
Orthodontics (medically necessary) $350 Copay $350 Copay
Pediatric Vision (Up to age 19)
Includes Exam and Eyewear
Adult Vision Exam $0 Copay $0 Copay
Adult Optical (Eyewear) Not Covered Not Covered
Provider Restrictions
Kaiser Members & Dependents
Open Enrollment November 1st ‐ November 30th(1) This plan has an embedded deductible and out‐of‐pocket maximum. Each family member will begin paying copayments or coinsurance after meeting his or her individual
deductible, or whenthe family deductible is satisfied. Individual family members are no longer subject to cost sharing when they reach their individual out‐of‐pocket
maximum, or when the family out‐of pocket maximum is met.
Kaiser
Eligibility Guidelines ‐ GUARANTEED ISSUE
KAISER PERMANENTE
New Members: May join the 1st of the month following 30 days of membership.
Qualifying Events: you may join within 30 days after you have a loss of coverage, marriage, birth or adoption.
Over Age Dependents: may remain on coverage up to age 26.
One standard pair of frames & lenses or
contact lenses per calendar year
One standard pair of frames & lenses or contact
lenses per calendar year
December 1, 2016 ‐ November 30, 2017
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
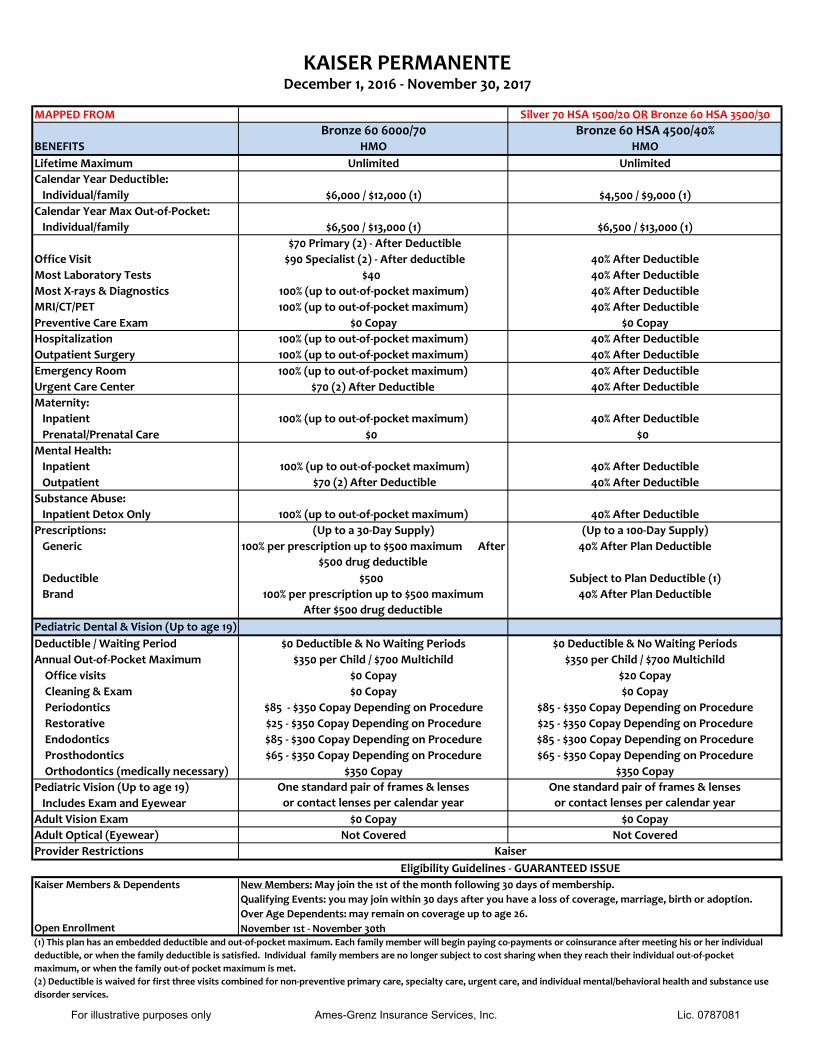
MAPPED FROM Silver 70 HSA 1500/20 OR Bronze 60 HSA 3500/30
Bronze 60 6000/70 Bronze 60 HSA 4500/40%BENEFITS HMO HMO
Lifetime Maximum Unlimited Unlimited
Calendar Year Deductible:
Individual/family $6,000 / $12,000 (1) $4,500 / $9,000 (1)
Calendar Year Max Out‐of‐Pocket:
Individual/family $6,500 / $13,000 (1) $6,500 / $13,000 (1)
Office Visit 40% After Deductible
Most Laboratory Tests 40% After Deductible
Most X‐rays & Diagnostics 40% After Deductible
MRI/CT/PET 40% After Deductible
Preventive Care Exam
$70 Primary (2) ‐ After Deductible$90 Specialist (2) ‐ After deductible
$40
100% (up to out‐of‐pocket maximum) 100% (up to out‐of‐pocket maximum)
$0 Copay $0 Copay
Hospitalization 100% (up to out‐of‐pocket maximum) 40% After Deductible
Outpatient Surgery 100% (up to out‐of‐pocket maximum) 40% After Deductible
Emergency Room 40% After Deductible
Urgent Care Center
100% (up to out‐of‐pocket maximum)
$70 (2) After Deductible 40% After Deductible
Maternity:
Inpatient 100% (up to out‐of‐pocket maximum) 40% After Deductible
Prenatal/Prenatal Care $0 $0
Mental Health:
Inpatient 40% After Deductible
Outpatient
100% (up to out‐of‐pocket maximum) $70 (2) After Deductible 40% After Deductible
Substance Abuse:
Inpatient Detox Only 100% (up to out‐of‐pocket maximum) 40% After Deductible
Prescriptions: (Up to a 30‐Day Supply) (Up to a 100‐Day Supply)
Generic 100% per prescription up to $500 maximum After
$500 drug deductible
40% After Plan Deductible
Deductible $500 Subject to Plan Deductible (1)
Brand 100% per prescription up to $500 maximum
After $500 drug deductible
40% After Plan Deductible
Pediatric Dental & Vision (Up to age 19)
Deductible / Waiting Period $0 Deductible & No Waiting Periods $0 Deductible & No Waiting Periods
Annual Out‐of‐Pocket Maximum $350 per Child / $700 Multichild $350 per Child / $700 Multichild
Office visits $0 Copay $20 Copay
Cleaning & Exam $0 Copay $0 Copay
Periodontics $85 ‐ $350 Copay Depending on Procedure $85 ‐ $350 Copay Depending on Procedure
Restorative $25 ‐ $350 Copay Depending on Procedure $25 ‐ $350 Copay Depending on Procedure
Endodontics $85 ‐ $300 Copay Depending on Procedure $85 ‐ $300 Copay Depending on Procedure
Prosthodontics $65 ‐ $350 Copay Depending on Procedure $65 ‐ $350 Copay Depending on Procedure
Orthodontics (medically necessary) $350 Copay $350 Copay
Pediatric Vision (Up to age 19)
Includes Exam and Eyewear
Adult Vision Exam $0 Copay $0 Copay
Adult Optical (Eyewear) Not Covered Not Covered
Provider Restrictions
Kaiser Members & Dependents
Open Enrollment
KAISER PERMANENTE
New Members: May join the 1st of the month following 30 days of membership.
Qualifying Events: you may join within 30 days after you have a loss of coverage, marriage, birth or adoption.
Over Age Dependents: may remain on coverage up to age 26.
November 1st ‐ November 30th(1) This plan has an embedded deductible and out‐of‐pocket maximum. Each family member will begin paying co-payments or coinsurance after meeting his or her individual
deductible, or when the family deductible is satisfied. Individual family members are no longer subject to cost sharing when they reach their individual out‐of‐pocket
maximum, or when the family out‐of pocket maximum is met.
(2) Deductible is waived for first three visits combined for non-preventive primary care, specialty care, urgent care, and individual mental/behavioral health and substance use disorder services.
Eligibility Guidelines ‐ GUARANTEED ISSUE
Kaiser
One standard pair of frames & lenses
or contact lenses per calendar year
One standard pair of frames & lenses
or contact lenses per calendar year
December 1, 2016 ‐ November 30, 2017
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $19.99 $19.99 $19.99 $19.99 $19.99 $19.99 $19.99
0–18 Medical $126.96 $123.55 $166.47 $169.86 $195.43 $194.79 $215.42
0–18 Total $146.95 $143.54 $186.46 $189.85 $215.42 $214.78 $235.41
19–20 $126.96 $123.55 $166.47 $169.86 $195.43 $194.79 $215.42
21 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
22 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
23 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
24 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
25 $200.74 $195.34 $263.21 $268.57 $309.00 $307.99 $340.60
26 $204.74 $199.23 $268.45 $273.92 $315.15 $314.12 $347.39
27 $209.53 $203.90 $274.74 $280.34 $322.54 $321.48 $355.53
28 $217.33 $211.49 $284.96 $290.77 $334.54 $333.45 $368.76
29 $223.73 $217.71 $293.35 $299.34 $344.39 $343.26 $379.62
30 $226.93 $220.83 $297.55 $303.62 $349.31 $348.17 $385.05
31 $231.73 $225.50 $303.84 $310.04 $356.70 $355.53 $393.19
32 $236.53 $230.17 $310.13 $316.46 $364.09 $362.90 $401.33
33 $239.52 $233.08 $314.06 $320.47 $368.70 $367.50 $406.42
34 $242.72 $236.20 $318.26 $324.75 $373.63 $372.41 $411.85
35 $244.32 $237.75 $320.36 $326.89 $376.09 $374.86 $414.56
36 $245.92 $239.31 $322.45 $329.03 $378.55 $377.31 $417.28
37 $247.52 $240.87 $324.55 $331.17 $381.01 $379.77 $419.99
38 $249.12 $242.42 $326.65 $333.31 $383.48 $382.22 $422.70
39 $252.32 $245.54 $330.84 $337.59 $388.40 $387.13 $428.13
40 $255.52 $248.65 $335.04 $341.87 $393.32 $392.04 $433.56
41 $260.32 $253.32 $341.33 $348.29 $400.71 $399.40 $441.70
42 $264.92 $257.79 $347.36 $354.44 $407.79 $406.46 $449.50
43 $271.31 $264.02 $355.75 $363.00 $417.64 $416.27 $460.36
44 $279.31 $271.80 $366.23 $373.70 $429.95 $428.54 $473.93
45 $288.71 $280.95 $378.55 $386.27 $444.41 $442.96 $489.87
46 $299.91 $291.84 $393.24 $401.25 $461.65 $460.14 $508.87
47 $312.50 $304.10 $409.75 $418.11 $481.04 $479.47 $530.24
48 $326.90 $318.11 $428.63 $437.37 $503.20 $501.55 $554.67
49 $341.09 $331.92 $447.24 $456.36 $525.05 $523.33 $578.76
50 $357.09 $347.49 $468.21 $477.76 $549.67 $547.87 $605.90
51 $372.88 $362.86 $488.92 $498.89 $573.98 $572.11 $632.70
52 $390.28 $379.78 $511.73 $522.16 $600.76 $598.79 $662.21
53 $407.87 $396.91 $534.80 $545.70 $627.84 $625.79 $692.07
54 $426.87 $415.39 $559.71 $571.12 $657.08 $654.93 $724.29
55 $445.86 $433.87 $584.61 $596.53 $686.32 $684.07 $756.52
56 $466.45 $453.91 $611.61 $624.08 $718.02 $715.67 $791.47
57 $487.25 $474.15 $638.88 $651.90 $750.02 $747.57 $826.75
58 $509.44 $495.74 $667.98 $681.60 $784.19 $781.62 $864.40
59 $520.44 $506.44 $682.39 $696.31 $801.11 $798.50 $883.06
60 $542.63 $528.04 $711.49 $726.00 $835.28 $832.55 $920.72
61 $561.82 $546.72 $736.66 $751.68 $864.82 $861.99 $953.29
62 $574.42 $558.98 $753.18 $768.53 $884.21 $881.32 $974.66
63 $590.21 $574.35 $773.89 $789.67 $908.52 $905.55 $1,001.46
64+ $599.82 $583.68 $786.48 $802.50 $923.31 $920.28 $1,017.75
Counties: Alpine, Amador, Butte, Calaveras, Colusa, Del Norte, Glenn, Humboldt, Lake, Lassen, Mendocino, Modoc, Nevada, Plumas, Shasta, Sierra,
Siskiyou, Sutter, Tehama, Trinity, Tuolumne, and Yuba
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 1
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $15.99 $15.99 $15.99 $15.99 $15.99 $15.99 $15.99
0–18 Medical $133.64 $130.05 $175.23 $178.80 $205.72 $205.04 $226.76
0–18 Total $149.63 $146.04 $191.22 $194.79 $221.71 $221.03 $242.75
19–20 $133.64 $130.05 $175.23 $178.80 $205.72 $205.04 $226.76
21 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
22 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
23 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
24 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
25 $211.30 $205.62 $277.06 $282.71 $325.26 $324.20 $358.53
26 $215.51 $209.72 $282.58 $288.34 $331.74 $330.65 $365.67
27 $220.56 $214.63 $289.20 $295.10 $339.51 $338.40 $374.24
28 $228.77 $222.62 $299.96 $306.08 $352.15 $351.00 $388.17
29 $235.51 $229.17 $308.79 $315.09 $362.52 $361.33 $399.60
30 $238.87 $232.45 $313.21 $319.59 $367.70 $366.50 $405.31
31 $243.92 $237.37 $319.83 $326.35 $375.47 $374.25 $413.88
32 $248.97 $242.28 $326.45 $333.11 $383.25 $382.00 $422.45
33 $252.13 $245.35 $330.59 $337.33 $388.11 $386.84 $427.81
34 $255.50 $248.63 $335.01 $341.84 $393.29 $392.01 $433.52
35 $257.18 $250.27 $337.22 $344.09 $395.88 $394.59 $436.38
36 $258.87 $251.91 $339.42 $346.35 $398.48 $397.17 $439.24
37 $260.55 $253.54 $341.63 $348.60 $401.07 $399.76 $442.09
38 $262.23 $255.18 $343.84 $350.85 $403.66 $402.34 $444.95
39 $265.60 $258.46 $348.25 $355.36 $408.84 $407.51 $450.66
40 $268.97 $261.74 $352.67 $359.86 $414.03 $412.67 $456.38
41 $274.02 $266.65 $359.29 $366.62 $421.80 $420.42 $464.95
42 $278.86 $271.36 $365.64 $373.10 $429.25 $427.85 $473.16
43 $285.59 $277.92 $374.47 $382.11 $439.62 $438.18 $484.59
44 $294.01 $286.11 $385.51 $393.37 $452.58 $451.10 $498.87
45 $303.90 $295.73 $398.48 $406.60 $467.80 $466.27 $515.66
46 $315.69 $307.20 $413.93 $422.37 $485.95 $484.36 $535.65
47 $328.95 $320.11 $431.32 $440.11 $506.36 $504.70 $558.15
48 $344.10 $334.85 $451.19 $460.39 $529.68 $527.95 $583.86
49 $359.05 $349.39 $470.78 $480.38 $552.68 $550.88 $609.22
50 $375.88 $365.78 $492.86 $502.90 $578.60 $576.71 $637.79
51 $392.51 $381.96 $514.66 $525.15 $604.19 $602.22 $666.00
52 $410.82 $399.77 $538.66 $549.65 $632.38 $630.31 $697.07
53 $429.34 $417.80 $562.95 $574.43 $660.89 $658.73 $728.49
54 $449.33 $437.25 $589.16 $601.18 $691.66 $689.40 $762.42
55 $469.33 $456.71 $615.38 $627.93 $722.44 $720.08 $796.34
56 $491.00 $477.80 $643.80 $656.93 $755.81 $753.34 $833.12
57 $512.89 $499.10 $672.50 $686.21 $789.50 $786.92 $870.26
58 $536.25 $521.83 $703.13 $717.47 $825.46 $822.76 $909.90
59 $547.83 $533.10 $718.31 $732.96 $843.28 $840.52 $929.54
60 $571.19 $555.83 $748.94 $764.21 $879.24 $876.36 $969.18
61 $591.39 $575.49 $775.43 $791.24 $910.34 $907.36 $1,003.46
62 $604.65 $588.40 $792.82 $808.98 $930.75 $927.71 $1,025.96
63 $621.28 $604.57 $814.62 $831.23 $956.34 $953.22 $1,054.17
64+ $631.38 $614.40 $827.85 $844.74 $971.88 $968.70 $1,071.30
Counties: Marin, Napa, Solano, and Sonoma
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 2
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $15.99 $15.99 $15.99 $15.99 $15.99 $15.99 $15.99
0–18 Medical $126.96 $123.55 $166.47 $169.86 $195.43 $194.79 $215.42
0–18 Total $142.95 $139.54 $182.46 $185.85 $211.42 $210.78 $231.41
19–20 $126.96 $123.55 $166.47 $169.86 $195.43 $194.79 $215.42
21 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
22 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
23 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
24 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
25 $200.74 $195.34 $263.21 $268.57 $309.00 $307.99 $340.60
26 $204.74 $199.23 $268.45 $273.92 $315.15 $314.12 $347.39
27 $209.53 $203.90 $274.74 $280.34 $322.54 $321.48 $355.53
28 $217.33 $211.49 $284.96 $290.77 $334.54 $333.45 $368.76
29 $223.73 $217.71 $293.35 $299.34 $344.39 $343.26 $379.62
30 $226.93 $220.83 $297.55 $303.62 $349.31 $348.17 $385.05
31 $231.73 $225.50 $303.84 $310.04 $356.70 $355.53 $393.19
32 $236.53 $230.17 $310.13 $316.46 $364.09 $362.90 $401.33
33 $239.52 $233.08 $314.06 $320.47 $368.70 $367.50 $406.42
34 $242.72 $236.20 $318.26 $324.75 $373.63 $372.41 $411.85
35 $244.32 $237.75 $320.36 $326.89 $376.09 $374.86 $414.56
36 $245.92 $239.31 $322.45 $329.03 $378.55 $377.31 $417.28
37 $247.52 $240.87 $324.55 $331.17 $381.01 $379.77 $419.99
38 $249.12 $242.42 $326.65 $333.31 $383.48 $382.22 $422.70
39 $252.32 $245.54 $330.84 $337.59 $388.40 $387.13 $428.13
40 $255.52 $248.65 $335.04 $341.87 $393.32 $392.04 $433.56
41 $260.32 $253.32 $341.33 $348.29 $400.71 $399.40 $441.70
42 $264.92 $257.79 $347.36 $354.44 $407.79 $406.46 $449.50
43 $271.31 $264.02 $355.75 $363.00 $417.64 $416.27 $460.36
44 $279.31 $271.80 $366.23 $373.70 $429.95 $428.54 $473.93
45 $288.71 $280.95 $378.55 $386.27 $444.41 $442.96 $489.87
46 $299.91 $291.84 $393.24 $401.25 $461.65 $460.14 $508.87
47 $312.50 $304.10 $409.75 $418.11 $481.04 $479.47 $530.24
48 $326.90 $318.11 $428.63 $437.37 $503.20 $501.55 $554.67
49 $341.09 $331.92 $447.24 $456.36 $525.05 $523.33 $578.76
50 $357.09 $347.49 $468.21 $477.76 $549.67 $547.87 $605.90
51 $372.88 $362.86 $488.92 $498.89 $573.98 $572.11 $632.70
52 $390.28 $379.78 $511.73 $522.16 $600.76 $598.79 $662.21
53 $407.87 $396.91 $534.80 $545.70 $627.84 $625.79 $692.07
54 $426.87 $415.39 $559.71 $571.12 $657.08 $654.93 $724.29
55 $445.86 $433.87 $584.61 $596.53 $686.32 $684.07 $756.52
56 $466.45 $453.91 $611.61 $624.08 $718.02 $715.67 $791.47
57 $487.25 $474.15 $638.88 $651.90 $750.02 $747.57 $826.75
58 $509.44 $495.74 $667.98 $681.60 $784.19 $781.62 $864.40
59 $520.44 $506.44 $682.39 $696.31 $801.11 $798.50 $883.06
60 $542.63 $528.04 $711.49 $726.00 $835.28 $832.55 $920.72
61 $561.82 $546.72 $736.66 $751.68 $864.82 $861.99 $953.29
62 $574.42 $558.98 $753.18 $768.53 $884.21 $881.32 $974.66
63 $590.21 $574.35 $773.89 $789.67 $908.52 $905.55 $1,001.46
64+ $599.82 $583.68 $786.48 $802.50 $923.31 $920.28 $1,017.75
Counties: El Dorado, Placer, Sacramento, and Yolo
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 3
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $140.32 $136.55 $183.99 $187.74 $216.00 $215.30 $238.10
0–18 Total $155.31 $151.54 $198.98 $202.73 $230.99 $230.29 $253.09
19–20 $140.32 $136.55 $183.99 $187.74 $216.00 $215.30 $238.10
21 $220.98 $215.04 $289.75 $295.66 $340.16 $339.05 $374.96
22 $220.98 $215.04 $289.75 $295.66 $340.16 $339.05 $374.96
23 $220.98 $215.04 $289.75 $295.66 $340.16 $339.05 $374.96
24 $220.98 $215.04 $289.75 $295.66 $340.16 $339.05 $374.96
25 $221.87 $215.90 $290.91 $296.84 $341.52 $340.41 $376.46
26 $226.29 $220.20 $296.71 $302.76 $348.33 $347.19 $383.96
27 $231.59 $225.36 $303.66 $309.85 $356.49 $355.32 $392.96
28 $240.21 $233.75 $314.96 $321.38 $369.76 $368.55 $407.58
29 $247.28 $240.63 $324.23 $330.84 $380.64 $379.40 $419.58
30 $250.82 $244.07 $328.87 $335.57 $386.08 $384.82 $425.58
31 $256.12 $249.23 $335.82 $342.67 $394.25 $392.96 $434.58
32 $261.42 $254.39 $342.78 $349.77 $402.41 $401.10 $443.58
33 $264.74 $257.62 $347.12 $354.20 $407.51 $406.18 $449.20
34 $268.27 $261.06 $351.76 $358.93 $412.96 $411.61 $455.20
35 $270.04 $262.78 $354.08 $361.30 $415.68 $414.32 $458.20
36 $271.81 $264.50 $356.40 $363.66 $418.40 $417.03 $461.20
37 $273.58 $266.22 $358.71 $366.03 $421.12 $419.74 $464.20
38 $275.35 $267.94 $361.03 $368.39 $423.84 $422.46 $467.20
39 $278.88 $271.38 $365.67 $373.12 $429.28 $427.88 $473.20
40 $282.42 $274.82 $370.30 $377.85 $434.73 $433.31 $479.20
41 $287.72 $279.98 $377.26 $384.95 $442.89 $441.44 $488.20
42 $292.80 $284.93 $383.92 $391.75 $450.71 $449.24 $496.82
43 $299.87 $291.81 $393.19 $401.21 $461.60 $460.09 $508.82
44 $308.71 $300.41 $404.78 $413.04 $475.21 $473.65 $523.82
45 $319.10 $310.52 $418.40 $426.93 $491.19 $489.59 $541.44
46 $331.47 $322.56 $434.63 $443.49 $510.24 $508.58 $562.44
47 $345.40 $336.11 $452.88 $462.12 $531.67 $529.94 $586.06
48 $361.31 $351.59 $473.75 $483.40 $556.16 $554.35 $613.06
49 $377.00 $366.86 $494.32 $504.40 $580.32 $578.42 $639.68
50 $394.68 $384.06 $517.50 $528.05 $607.53 $605.54 $669.68
51 $412.13 $401.05 $540.39 $551.41 $634.40 $632.33 $699.30
52 $431.36 $419.76 $565.60 $577.13 $664.00 $661.83 $731.92
53 $450.81 $438.69 $591.09 $603.15 $693.93 $691.66 $764.91
54 $471.80 $459.11 $618.62 $631.23 $726.25 $723.87 $800.54
55 $492.79 $479.54 $646.15 $659.32 $758.56 $756.08 $836.16
56 $515.55 $501.69 $675.99 $689.78 $793.60 $791.00 $874.78
57 $538.54 $524.06 $706.13 $720.52 $828.97 $826.27 $913.77
58 $563.07 $547.93 $738.29 $753.34 $866.73 $863.90 $955.39
59 $575.22 $559.75 $754.23 $769.60 $885.44 $882.55 $976.02
60 $599.75 $583.62 $786.39 $802.42 $923.20 $920.18 $1,017.64
61 $620.96 $604.27 $814.20 $830.81 $955.85 $952.73 $1,053.63
62 $634.88 $617.82 $832.46 $849.43 $977.29 $974.09 $1,077.26
63 $652.34 $634.80 $855.35 $872.79 $1,004.16 $1,000.88 $1,106.88
64+ $662.94 $645.12 $869.25 $886.98 $1,020.48 $1,017.15 $1,124.88
Counties: San Francisco and San Mateo
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 4 & 8
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $126.96 $123.55 $166.47 $169.86 $195.43 $194.79 $215.42
0–18 Total $141.95 $138.54 $181.46 $184.85 $210.42 $209.78 $230.41
19–20 $126.96 $123.55 $166.47 $169.86 $195.43 $194.79 $215.42
21 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
22 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
23 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
24 $199.94 $194.56 $262.16 $267.50 $307.77 $306.76 $339.25
25 $200.74 $195.34 $263.21 $268.57 $309.00 $307.99 $340.60
26 $204.74 $199.23 $268.45 $273.92 $315.15 $314.12 $347.39
27 $209.53 $203.90 $274.74 $280.34 $322.54 $321.48 $355.53
28 $217.33 $211.49 $284.96 $290.77 $334.54 $333.45 $368.76
29 $223.73 $217.71 $293.35 $299.34 $344.39 $343.26 $379.62
30 $226.93 $220.83 $297.55 $303.62 $349.31 $348.17 $385.05
31 $231.73 $225.50 $303.84 $310.04 $356.70 $355.53 $393.19
32 $236.53 $230.17 $310.13 $316.46 $364.09 $362.90 $401.33
33 $239.52 $233.08 $314.06 $320.47 $368.70 $367.50 $406.42
34 $242.72 $236.20 $318.26 $324.75 $373.63 $372.41 $411.85
35 $244.32 $237.75 $320.36 $326.89 $376.09 $374.86 $414.56
36 $245.92 $239.31 $322.45 $329.03 $378.55 $377.31 $417.28
37 $247.52 $240.87 $324.55 $331.17 $381.01 $379.77 $419.99
38 $249.12 $242.42 $326.65 $333.31 $383.48 $382.22 $422.70
39 $252.32 $245.54 $330.84 $337.59 $388.40 $387.13 $428.13
40 $255.52 $248.65 $335.04 $341.87 $393.32 $392.04 $433.56
41 $260.32 $253.32 $341.33 $348.29 $400.71 $399.40 $441.70
42 $264.92 $257.79 $347.36 $354.44 $407.79 $406.46 $449.50
43 $271.31 $264.02 $355.75 $363.00 $417.64 $416.27 $460.36
44 $279.31 $271.80 $366.23 $373.70 $429.95 $428.54 $473.93
45 $288.71 $280.95 $378.55 $386.27 $444.41 $442.96 $489.87
46 $299.91 $291.84 $393.24 $401.25 $461.65 $460.14 $508.87
47 $312.50 $304.10 $409.75 $418.11 $481.04 $479.47 $530.24
48 $326.90 $318.11 $428.63 $437.37 $503.20 $501.55 $554.67
49 $341.09 $331.92 $447.24 $456.36 $525.05 $523.33 $578.76
50 $357.09 $347.49 $468.21 $477.76 $549.67 $547.87 $605.90
51 $372.88 $362.86 $488.92 $498.89 $573.98 $572.11 $632.70
52 $390.28 $379.78 $511.73 $522.16 $600.76 $598.79 $662.21
53 $407.87 $396.91 $534.80 $545.70 $627.84 $625.79 $692.07
54 $426.87 $415.39 $559.71 $571.12 $657.08 $654.93 $724.29
55 $445.86 $433.87 $584.61 $596.53 $686.32 $684.07 $756.52
56 $466.45 $453.91 $611.61 $624.08 $718.02 $715.67 $791.47
57 $487.25 $474.15 $638.88 $651.90 $750.02 $747.57 $826.75
58 $509.44 $495.74 $667.98 $681.60 $784.19 $781.62 $864.40
59 $520.44 $506.44 $682.39 $696.31 $801.11 $798.50 $883.06
60 $542.63 $528.04 $711.49 $726.00 $835.28 $832.55 $920.72
61 $561.82 $546.72 $736.66 $751.68 $864.82 $861.99 $953.29
62 $574.42 $558.98 $753.18 $768.53 $884.21 $881.32 $974.66
63 $590.21 $574.35 $773.89 $789.67 $908.52 $905.55 $1,001.46
64+ $599.82 $583.68 $786.48 $802.50 $923.31 $920.28 $1,017.75
Counties: Contra Costa
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 5
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $133.64 $130.05 $175.23 $178.80 $205.72 $205.04 $226.76
0–18 Total $148.63 $145.04 $190.22 $193.79 $220.71 $220.03 $241.75
19–20 $133.64 $130.05 $175.23 $178.80 $205.72 $205.04 $226.76
21 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
22 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
23 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
24 $210.46 $204.80 $275.95 $281.58 $323.96 $322.90 $357.10
25 $211.30 $205.62 $277.06 $282.71 $325.26 $324.20 $358.53
26 $215.51 $209.72 $282.58 $288.34 $331.74 $330.65 $365.67
27 $220.56 $214.63 $289.20 $295.10 $339.51 $338.40 $374.24
28 $228.77 $222.62 $299.96 $306.08 $352.15 $351.00 $388.17
29 $235.51 $229.17 $308.79 $315.09 $362.52 $361.33 $399.60
30 $238.87 $232.45 $313.21 $319.59 $367.70 $366.50 $405.31
31 $243.92 $237.37 $319.83 $326.35 $375.47 $374.25 $413.88
32 $248.97 $242.28 $326.45 $333.11 $383.25 $382.00 $422.45
33 $252.13 $245.35 $330.59 $337.33 $388.11 $386.84 $427.81
34 $255.50 $248.63 $335.01 $341.84 $393.29 $392.01 $433.52
35 $257.18 $250.27 $337.22 $344.09 $395.88 $394.59 $436.38
36 $258.87 $251.91 $339.42 $346.35 $398.48 $397.17 $439.24
37 $260.55 $253.54 $341.63 $348.60 $401.07 $399.76 $442.09
38 $262.23 $255.18 $343.84 $350.85 $403.66 $402.34 $444.95
39 $265.60 $258.46 $348.25 $355.36 $408.84 $407.51 $450.66
40 $268.97 $261.74 $352.67 $359.86 $414.03 $412.67 $456.38
41 $274.02 $266.65 $359.29 $366.62 $421.80 $420.42 $464.95
42 $278.86 $271.36 $365.64 $373.10 $429.25 $427.85 $473.16
43 $285.59 $277.92 $374.47 $382.11 $439.62 $438.18 $484.59
44 $294.01 $286.11 $385.51 $393.37 $452.58 $451.10 $498.87
45 $303.90 $295.73 $398.48 $406.60 $467.80 $466.27 $515.66
46 $315.69 $307.20 $413.93 $422.37 $485.95 $484.36 $535.65
47 $328.95 $320.11 $431.32 $440.11 $506.36 $504.70 $558.15
48 $344.10 $334.85 $451.19 $460.39 $529.68 $527.95 $583.86
49 $359.05 $349.39 $470.78 $480.38 $552.68 $550.88 $609.22
50 $375.88 $365.78 $492.86 $502.90 $578.60 $576.71 $637.79
51 $392.51 $381.96 $514.66 $525.15 $604.19 $602.22 $666.00
52 $410.82 $399.77 $538.66 $549.65 $632.38 $630.31 $697.07
53 $429.34 $417.80 $562.95 $574.43 $660.89 $658.73 $728.49
54 $449.33 $437.25 $589.16 $601.18 $691.66 $689.40 $762.42
55 $469.33 $456.71 $615.38 $627.93 $722.44 $720.08 $796.34
56 $491.00 $477.80 $643.80 $656.93 $755.81 $753.34 $833.12
57 $512.89 $499.10 $672.50 $686.21 $789.50 $786.92 $870.26
58 $536.25 $521.83 $703.13 $717.47 $825.46 $822.76 $909.90
59 $547.83 $533.10 $718.31 $732.96 $843.28 $840.52 $929.54
60 $571.19 $555.83 $748.94 $764.21 $879.24 $876.36 $969.18
61 $591.39 $575.49 $775.43 $791.24 $910.34 $907.36 $1,003.46
62 $604.65 $588.40 $792.82 $808.98 $930.75 $927.71 $1,025.96
63 $621.28 $604.57 $814.62 $831.23 $956.34 $953.22 $1,054.17
64+ $631.38 $614.40 $827.85 $844.74 $971.88 $968.70 $1,071.30
Counties: Alameda
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 6
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $137.65 $133.95 $180.49 $184.17 $211.89 $211.20 $233.56
0–18 Total $152.64 $148.94 $195.48 $199.16 $226.88 $226.19 $248.55
19–20 $137.65 $133.95 $180.49 $184.17 $211.89 $211.20 $233.56
21 $216.77 $210.95 $284.23 $290.03 $333.68 $332.59 $367.82
22 $216.77 $210.95 $284.23 $290.03 $333.68 $332.59 $367.82
23 $216.77 $210.95 $284.23 $290.03 $333.68 $332.59 $367.82
24 $216.77 $210.95 $284.23 $290.03 $333.68 $332.59 $367.82
25 $217.64 $211.79 $285.37 $291.19 $335.02 $333.92 $369.29
26 $221.98 $216.01 $291.05 $296.99 $341.69 $340.57 $376.64
27 $227.18 $221.07 $297.88 $303.95 $349.70 $348.56 $385.47
28 $235.63 $229.30 $308.96 $315.26 $362.71 $361.53 $399.82
29 $242.57 $236.05 $318.06 $324.54 $373.39 $372.17 $411.59
30 $246.04 $239.42 $322.60 $329.18 $378.73 $377.49 $417.47
31 $251.24 $244.49 $329.43 $336.14 $386.74 $385.47 $426.30
32 $256.44 $249.55 $336.25 $343.10 $394.75 $393.46 $435.13
33 $259.70 $252.71 $340.51 $347.45 $399.75 $398.45 $440.64
34 $263.16 $256.09 $345.06 $352.09 $405.09 $403.77 $446.53
35 $264.90 $257.78 $347.33 $354.42 $407.76 $406.43 $449.47
36 $266.63 $259.46 $349.61 $356.74 $410.43 $409.09 $452.41
37 $268.37 $261.15 $351.88 $359.06 $413.10 $411.75 $455.36
38 $270.10 $262.84 $354.15 $361.38 $415.77 $414.41 $458.30
39 $273.57 $266.21 $358.70 $366.02 $421.11 $419.73 $464.18
40 $277.04 $269.59 $363.25 $370.66 $426.45 $425.05 $470.07
41 $282.24 $274.65 $370.07 $377.62 $434.45 $433.03 $478.90
42 $287.23 $279.50 $376.61 $384.29 $442.13 $440.68 $487.36
43 $294.16 $286.25 $385.70 $393.57 $452.81 $451.33 $499.13
44 $302.83 $294.69 $397.07 $405.17 $466.15 $464.63 $513.84
45 $313.02 $304.61 $410.43 $418.80 $481.84 $480.26 $531.13
46 $325.16 $316.42 $426.35 $435.04 $500.52 $498.89 $551.72
47 $338.82 $329.71 $444.26 $453.31 $521.55 $519.84 $574.90
48 $354.43 $344.90 $464.72 $474.20 $545.57 $543.79 $601.38
49 $369.82 $359.87 $484.90 $494.79 $569.26 $567.40 $627.49
50 $387.16 $376.75 $507.64 $517.99 $595.96 $594.01 $656.92
51 $404.28 $393.41 $530.10 $540.90 $622.32 $620.28 $685.98
52 $423.14 $411.77 $554.82 $566.14 $651.35 $649.22 $717.98
53 $442.22 $430.33 $579.84 $591.66 $680.71 $678.49 $750.35
54 $462.81 $450.37 $606.84 $619.21 $712.41 $710.08 $785.29
55 $483.41 $470.41 $633.84 $646.76 $744.11 $741.68 $820.23
56 $505.73 $492.14 $663.12 $676.64 $778.48 $775.94 $858.12
57 $528.28 $514.07 $692.68 $706.80 $813.18 $810.53 $896.37
58 $552.34 $537.49 $724.23 $738.99 $850.22 $847.44 $937.20
59 $564.26 $549.09 $739.86 $754.94 $868.58 $865.74 $957.43
60 $588.32 $572.51 $771.41 $787.14 $905.61 $902.65 $998.25
61 $609.14 $592.76 $798.70 $814.98 $937.65 $934.58 $1,033.56
62 $622.79 $606.05 $816.60 $833.25 $958.67 $955.54 $1,056.74
63 $639.92 $622.71 $839.06 $856.16 $985.03 $981.81 $1,085.79
64+ $650.31 $632.85 $852.69 $870.09 $1,001.04 $997.77 $1,103.46
Counties: Santa Clara, Monterey, San Benito, and Santa Cruz
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 7 & 9
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $15.99 $15.99 $15.99 $15.99 $15.99 $15.99 $15.99
0–18 Medical $120.28 $117.04 $157.71 $160.92 $185.15 $184.54 $204.08
0–18 Total $136.27 $133.03 $173.70 $176.91 $201.14 $200.53 $220.07
19–20 $120.28 $117.04 $157.71 $160.92 $185.15 $184.54 $204.08
21 $189.41 $184.32 $248.36 $253.42 $291.57 $290.61 $321.39
22 $189.41 $184.32 $248.36 $253.42 $291.57 $290.61 $321.39
23 $189.41 $184.32 $248.36 $253.42 $291.57 $290.61 $321.39
24 $189.41 $184.32 $248.36 $253.42 $291.57 $290.61 $321.39
25 $190.17 $185.06 $249.35 $254.44 $292.73 $291.78 $322.68
26 $193.96 $188.75 $254.32 $259.51 $298.56 $297.59 $329.11
27 $198.51 $193.17 $260.28 $265.59 $305.56 $304.56 $336.82
28 $205.89 $200.36 $269.97 $275.47 $316.93 $315.90 $349.35
29 $211.95 $206.26 $277.91 $283.58 $326.26 $325.20 $359.64
30 $214.99 $209.21 $281.89 $287.64 $330.93 $329.85 $364.78
31 $219.53 $213.63 $287.85 $293.72 $337.93 $336.82 $372.49
32 $224.08 $218.05 $293.81 $299.80 $344.92 $343.80 $380.21
33 $226.92 $220.82 $297.53 $303.60 $349.30 $348.16 $385.03
34 $229.95 $223.77 $301.51 $307.66 $353.96 $352.81 $390.17
35 $231.46 $225.24 $303.49 $309.68 $356.30 $355.13 $392.74
36 $232.98 $226.72 $305.48 $311.71 $358.63 $357.46 $395.31
37 $234.49 $228.19 $307.47 $313.74 $360.96 $359.78 $397.88
38 $236.01 $229.66 $309.46 $315.77 $363.29 $362.11 $400.46
39 $239.04 $232.61 $313.43 $319.82 $367.96 $366.76 $405.60
40 $242.07 $235.56 $317.40 $323.87 $372.62 $371.41 $410.74
41 $246.62 $239.99 $323.36 $329.96 $379.62 $378.38 $418.45
42 $250.97 $244.23 $329.08 $335.79 $386.33 $385.06 $425.85
43 $257.04 $250.12 $337.02 $343.90 $395.66 $394.36 $436.13
44 $264.61 $257.50 $346.96 $354.03 $407.32 $405.99 $448.99
45 $273.51 $266.16 $358.63 $365.94 $421.02 $419.65 $464.09
46 $284.12 $276.48 $372.54 $380.13 $437.35 $435.92 $482.09
47 $296.05 $288.09 $388.19 $396.10 $455.72 $454.23 $502.34
48 $309.69 $301.37 $406.07 $414.35 $476.71 $475.15 $525.48
49 $323.14 $314.45 $423.70 $432.34 $497.41 $495.79 $548.30
50 $338.29 $329.20 $443.57 $452.61 $520.74 $519.04 $574.01
51 $353.26 $343.76 $463.19 $472.63 $543.77 $542.00 $599.40
52 $369.74 $359.80 $484.80 $494.68 $569.14 $567.28 $627.36
53 $386.40 $376.02 $506.65 $516.98 $594.80 $592.85 $655.64
54 $404.40 $393.53 $530.25 $541.06 $622.50 $620.46 $686.17
55 $422.39 $411.04 $553.84 $565.13 $650.20 $648.07 $716.71
56 $441.90 $430.02 $579.42 $591.24 $680.23 $678.00 $749.81
57 $461.60 $449.19 $605.25 $617.59 $710.55 $708.23 $783.23
58 $482.63 $469.65 $632.82 $645.72 $742.91 $740.49 $818.91
59 $493.05 $479.79 $646.48 $659.66 $758.95 $756.47 $836.59
60 $514.07 $500.25 $674.05 $687.79 $791.31 $788.73 $872.26
61 $532.25 $517.94 $697.89 $712.12 $819.30 $816.63 $903.11
62 $544.19 $529.56 $713.54 $728.08 $837.67 $834.94 $923.36
63 $559.15 $544.12 $733.16 $748.11 $860.71 $857.89 $948.75
64+ $568.23 $552.96 $745.08 $760.26 $874.71 $871.83 $964.17
Counties: Mariposa, Merced, San Joaquin, Stanislaus, and Tulare
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 10
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $15.99 $15.99 $15.99 $15.99 $15.99 $15.99 $15.99
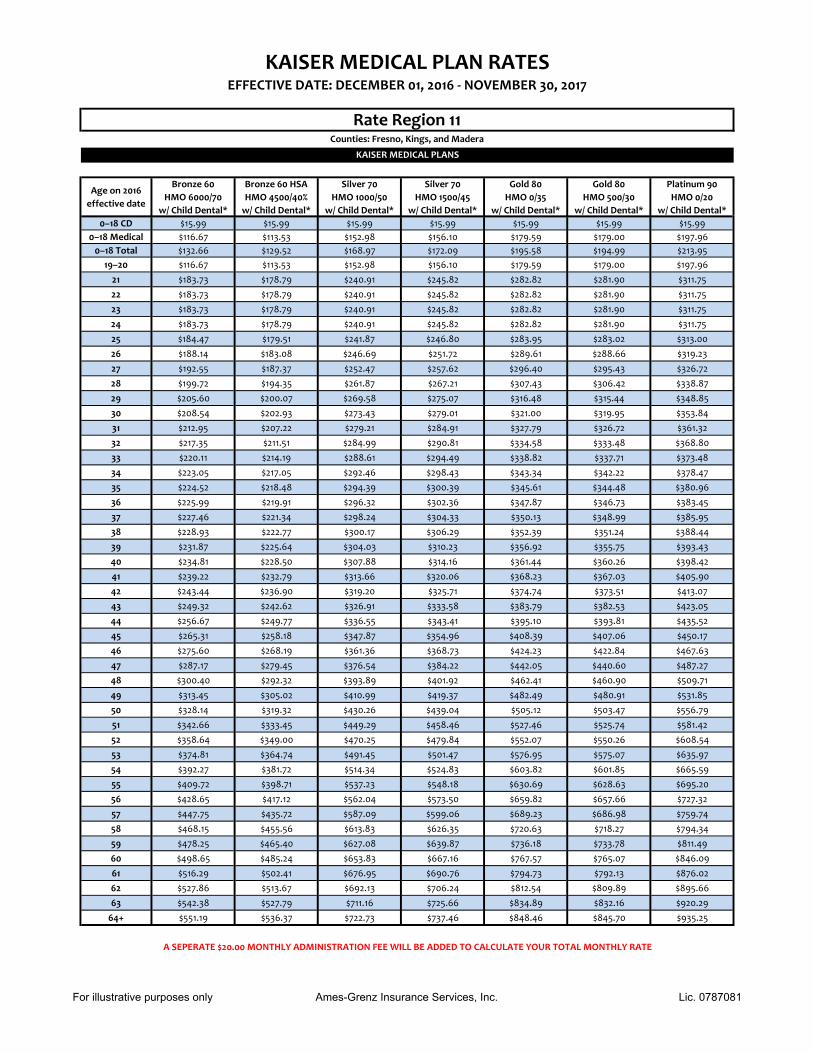
0–18 Medical $116.67 $113.53 $152.98 $156.10 $179.59 $179.00 $197.96
0–18 Total $132.66 $129.52 $168.97 $172.09 $195.58 $194.99 $213.95
19–20 $116.67 $113.53 $152.98 $156.10 $179.59 $179.00 $197.96
21 $183.73 $178.79 $240.91 $245.82 $282.82 $281.90 $311.75
22 $183.73 $178.79 $240.91 $245.82 $282.82 $281.90 $311.75
23 $183.73 $178.79 $240.91 $245.82 $282.82 $281.90 $311.75
24 $183.73 $178.79 $240.91 $245.82 $282.82 $281.90 $311.75
25 $184.47 $179.51 $241.87 $246.80 $283.95 $283.02 $313.00
26 $188.14 $183.08 $246.69 $251.72 $289.61 $288.66 $319.23
27 $192.55 $187.37 $252.47 $257.62 $296.40 $295.43 $326.72
28 $199.72 $194.35 $261.87 $267.21 $307.43 $306.42 $338.87
29 $205.60 $200.07 $269.58 $275.07 $316.48 $315.44 $348.85
30 $208.54 $202.93 $273.43 $279.01 $321.00 $319.95 $353.84
31 $212.95 $207.22 $279.21 $284.91 $327.79 $326.72 $361.32
32 $217.35 $211.51 $284.99 $290.81 $334.58 $333.48 $368.80
33 $220.11 $214.19 $288.61 $294.49 $338.82 $337.71 $373.48
34 $223.05 $217.05 $292.46 $298.43 $343.34 $342.22 $378.47
35 $224.52 $218.48 $294.39 $300.39 $345.61 $344.48 $380.96
36 $225.99 $219.91 $296.32 $302.36 $347.87 $346.73 $383.45
37 $227.46 $221.34 $298.24 $304.33 $350.13 $348.99 $385.95
38 $228.93 $222.77 $300.17 $306.29 $352.39 $351.24 $388.44
39 $231.87 $225.64 $304.03 $310.23 $356.92 $355.75 $393.43
40 $234.81 $228.50 $307.88 $314.16 $361.44 $360.26 $398.42
41 $239.22 $232.79 $313.66 $320.06 $368.23 $367.03 $405.90
42 $243.44 $236.90 $319.20 $325.71 $374.74 $373.51 $413.07
43 $249.32 $242.62 $326.91 $333.58 $383.79 $382.53 $423.05
44 $256.67 $249.77 $336.55 $343.41 $395.10 $393.81 $435.52
45 $265.31 $258.18 $347.87 $354.96 $408.39 $407.06 $450.17
46 $275.60 $268.19 $361.36 $368.73 $424.23 $422.84 $467.63
47 $287.17 $279.45 $376.54 $384.22 $442.05 $440.60 $487.27
48 $300.40 $292.32 $393.89 $401.92 $462.41 $460.90 $509.71
49 $313.45 $305.02 $410.99 $419.37 $482.49 $480.91 $531.85
50 $328.14 $319.32 $430.26 $439.04 $505.12 $503.47 $556.79
51 $342.66 $333.45 $449.29 $458.46 $527.46 $525.74 $581.42
52 $358.64 $349.00 $470.25 $479.84 $552.07 $550.26 $608.54
53 $374.81 $364.74 $491.45 $501.47 $576.95 $575.07 $635.97
54 $392.27 $381.72 $514.34 $524.83 $603.82 $601.85 $665.59
55 $409.72 $398.71 $537.23 $548.18 $630.69 $628.63 $695.20
56 $428.65 $417.12 $562.04 $573.50 $659.82 $657.66 $727.32
57 $447.75 $435.72 $587.09 $599.06 $689.23 $686.98 $759.74
58 $468.15 $455.56 $613.83 $626.35 $720.63 $718.27 $794.34
59 $478.25 $465.40 $627.08 $639.87 $736.18 $733.78 $811.49
60 $498.65 $485.24 $653.83 $667.16 $767.57 $765.07 $846.09
61 $516.29 $502.41 $676.95 $690.76 $794.73 $792.13 $876.02
62 $527.86 $513.67 $692.13 $706.24 $812.54 $809.89 $895.66
63 $542.38 $527.79 $711.16 $725.66 $834.89 $832.16 $920.29
64+ $551.19 $536.37 $722.73 $737.46 $848.46 $845.70 $935.25
Counties: Fresno, Kings, and Madera
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 11
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $15.99 $15.99 $15.99 $15.99 $15.99 $15.99 $15.99
0–18 Medical $119.36 $116.15 $156.51 $159.70 $183.73 $183.13 $202.53
0–18 Total $135.35 $132.14 $172.50 $175.69 $199.72 $199.12 $218.52
19–20 $119.36 $116.15 $156.51 $159.70 $183.73 $183.13 $202.53
21 $187.97 $182.92 $246.46 $251.49 $289.34 $288.40 $318.94
22 $187.97 $182.92 $246.46 $251.49 $289.34 $288.40 $318.94
23 $187.97 $182.92 $246.46 $251.49 $289.34 $288.40 $318.94
24 $187.97 $182.92 $246.46 $251.49 $289.34 $288.40 $318.94
25 $188.72 $183.65 $247.45 $252.50 $290.50 $289.55 $320.22
26 $192.48 $187.31 $252.38 $257.53 $296.29 $295.32 $326.60
27 $196.99 $191.70 $258.30 $263.56 $303.23 $302.24 $334.25
28 $204.32 $198.83 $267.91 $273.37 $314.52 $313.49 $346.69
29 $210.34 $204.68 $275.79 $281.42 $323.78 $322.72 $356.90
30 $213.35 $207.61 $279.74 $285.44 $328.40 $327.33 $362.00
31 $217.86 $212.00 $285.65 $291.48 $335.35 $334.25 $369.65
32 $222.37 $216.39 $291.57 $297.51 $342.29 $341.17 $377.31
33 $225.19 $219.13 $295.26 $301.29 $346.63 $345.50 $382.09
34 $228.19 $222.06 $299.21 $305.31 $351.26 $350.11 $387.19
35 $229.70 $223.52 $301.18 $307.32 $353.58 $352.42 $389.75
36 $231.20 $224.99 $303.15 $309.33 $355.89 $354.73 $392.30
37 $232.71 $226.45 $305.12 $311.34 $358.21 $357.04 $394.85
38 $234.21 $227.91 $307.10 $313.36 $360.52 $359.34 $397.40
39 $237.22 $230.84 $311.04 $317.38 $365.15 $363.96 $402.50
40 $240.23 $233.77 $314.98 $321.40 $369.78 $368.57 $407.61
41 $244.74 $238.16 $320.90 $327.44 $376.73 $375.49 $415.26
42 $249.06 $242.36 $326.57 $333.22 $383.38 $382.13 $422.60
43 $255.07 $248.22 $334.45 $341.27 $392.64 $391.36 $432.80
44 $262.59 $255.53 $344.31 $351.33 $404.21 $402.89 $445.56
45 $271.43 $264.13 $355.90 $363.15 $417.81 $416.45 $460.55
46 $281.95 $274.37 $369.70 $377.24 $434.02 $432.60 $478.41
47 $293.80 $285.90 $385.22 $393.08 $452.24 $450.77 $498.51
48 $307.33 $299.07 $402.97 $411.19 $473.08 $471.53 $521.47
49 $320.68 $312.05 $420.47 $429.04 $493.62 $492.01 $544.11
50 $335.71 $326.69 $440.19 $449.16 $516.77 $515.08 $569.63
51 $350.56 $341.14 $459.66 $469.03 $539.63 $537.86 $594.83
52 $366.92 $357.05 $481.10 $490.91 $564.80 $562.95 $622.57
53 $383.46 $373.15 $502.79 $513.04 $590.26 $588.33 $650.64
54 $401.31 $390.53 $526.20 $536.93 $617.75 $615.73 $680.94
55 $419.17 $407.90 $549.62 $560.82 $645.24 $643.13 $711.24
56 $438.53 $426.74 $575.00 $586.73 $675.04 $672.83 $744.09
57 $458.08 $445.77 $600.63 $612.88 $705.13 $702.83 $777.26
58 $478.95 $466.07 $627.99 $640.80 $737.25 $734.84 $812.66
59 $489.28 $476.13 $641.55 $654.63 $753.16 $750.70 $830.20
60 $510.15 $496.43 $668.91 $682.54 $785.28 $782.71 $865.61
61 $528.19 $513.99 $692.57 $706.69 $813.06 $810.40 $896.23
62 $540.04 $525.52 $708.09 $722.53 $831.28 $828.57 $916.32
63 $554.89 $539.97 $727.56 $742.40 $854.14 $851.35 $941.52
64+ $563.91 $548.76 $739.38 $754.47 $868.02 $865.20 $956.82
Counties: San Luis Obispo, Santa Barbara, and Ventura
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 12
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $15.99 $15.99 $15.99 $15.99 $15.99 $15.99 $15.99
0–18 Medical $113.39 $110.34 $148.68 $151.71 $174.55 $173.98 $192.40
0–18 Total $129.38 $126.33 $164.67 $167.70 $190.54 $189.97 $208.39
19–20 $113.39 $110.34 $148.68 $151.71 $174.55 $173.98 $192.40
21 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
22 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
23 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
24 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
25 $179.29 $174.47 $235.08 $239.87 $275.98 $275.07 $304.21
26 $182.86 $177.94 $239.76 $244.65 $281.47 $280.55 $310.27
27 $187.14 $182.11 $245.38 $250.38 $288.07 $287.13 $317.54
28 $194.11 $188.89 $254.51 $259.70 $298.79 $297.81 $329.35
29 $199.82 $194.45 $262.00 $267.35 $307.59 $306.58 $339.05
30 $202.68 $197.23 $265.75 $271.17 $311.98 $310.96 $343.90
31 $206.96 $201.40 $271.37 $276.90 $318.58 $317.54 $351.17
32 $211.25 $205.57 $276.99 $282.64 $325.18 $324.12 $358.44
33 $213.93 $208.18 $280.50 $286.22 $329.30 $328.23 $362.99
34 $216.79 $210.96 $284.25 $290.04 $333.70 $332.61 $367.84
35 $218.21 $212.35 $286.12 $291.96 $335.90 $334.80 $370.26
36 $219.64 $213.74 $287.99 $293.87 $338.10 $336.99 $372.68
37 $221.07 $215.13 $289.87 $295.78 $340.30 $339.18 $375.11
38 $222.50 $216.52 $291.74 $297.69 $342.50 $341.38 $377.53
39 $225.36 $219.30 $295.49 $301.51 $346.89 $345.76 $382.38
40 $228.21 $222.08 $299.23 $305.33 $351.29 $350.14 $387.23
41 $232.50 $226.25 $304.85 $311.07 $357.89 $356.72 $394.50
42 $236.61 $230.25 $310.24 $316.56 $364.21 $363.02 $401.47
43 $242.32 $235.81 $317.73 $324.21 $373.01 $371.79 $411.16
44 $249.46 $242.76 $327.10 $333.77 $384.00 $382.75 $423.28
45 $257.86 $250.92 $338.10 $344.99 $396.92 $395.62 $437.52
46 $267.86 $260.65 $351.21 $358.37 $412.31 $410.97 $454.49
47 $279.11 $271.60 $365.96 $373.43 $429.63 $428.23 $473.58
48 $291.96 $284.11 $382.82 $390.63 $449.42 $447.95 $495.40
49 $304.64 $296.45 $399.45 $407.59 $468.94 $467.41 $516.91
50 $318.93 $310.35 $418.18 $426.70 $490.93 $489.32 $541.15
51 $333.03 $324.08 $436.67 $445.58 $512.64 $510.97 $565.08
52 $348.57 $339.20 $457.04 $466.36 $536.56 $534.80 $591.45
53 $364.28 $354.49 $477.65 $487.39 $560.75 $558.91 $618.11
54 $381.25 $371.00 $499.89 $510.09 $586.86 $584.94 $646.89
55 $398.21 $387.51 $522.14 $532.78 $612.97 $610.97 $675.68
56 $416.61 $405.41 $546.25 $557.39 $641.29 $639.19 $706.89
57 $435.18 $423.48 $570.60 $582.24 $669.87 $667.68 $738.40
58 $455.00 $442.77 $596.59 $608.76 $700.38 $698.10 $772.03
59 $464.82 $452.32 $609.47 $621.90 $715.50 $713.16 $788.69
60 $484.64 $471.61 $635.46 $648.42 $746.01 $743.58 $822.33
61 $501.78 $488.29 $657.94 $671.35 $772.40 $769.88 $851.41
62 $513.03 $499.24 $672.69 $686.41 $789.72 $787.14 $870.50
63 $527.14 $512.97 $691.19 $705.28 $811.43 $808.78 $894.44
64+ $535.71 $521.31 $702.42 $716.76 $824.64 $821.94 $908.97
Counties: Imperial, Inyo, and Mono
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 13
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $113.39 $110.34 $148.68 $151.71 $174.55 $173.98 $192.40
0–18 Total $128.38 $125.33 $163.67 $166.70 $189.54 $188.97 $207.39
19–20 $113.39 $110.34 $148.68 $151.71 $174.55 $173.98 $192.40
21 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
22 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
23 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
24 $178.57 $173.77 $234.14 $238.92 $274.88 $273.98 $302.99
25 $179.29 $174.47 $235.08 $239.87 $275.98 $275.07 $304.21
26 $182.86 $177.94 $239.76 $244.65 $281.47 $280.55 $310.27
27 $187.14 $182.11 $245.38 $250.38 $288.07 $287.13 $317.54
28 $194.11 $188.89 $254.51 $259.70 $298.79 $297.81 $329.35
29 $199.82 $194.45 $262.00 $267.35 $307.59 $306.58 $339.05
30 $202.68 $197.23 $265.75 $271.17 $311.98 $310.96 $343.90
31 $206.96 $201.40 $271.37 $276.90 $318.58 $317.54 $351.17
32 $211.25 $205.57 $276.99 $282.64 $325.18 $324.12 $358.44
33 $213.93 $208.18 $280.50 $286.22 $329.30 $328.23 $362.99
34 $216.79 $210.96 $284.25 $290.04 $333.70 $332.61 $367.84
35 $218.21 $212.35 $286.12 $291.96 $335.90 $334.80 $370.26
36 $219.64 $213.74 $287.99 $293.87 $338.10 $336.99 $372.68
37 $221.07 $215.13 $289.87 $295.78 $340.30 $339.18 $375.11
38 $222.50 $216.52 $291.74 $297.69 $342.50 $341.38 $377.53
39 $225.36 $219.30 $295.49 $301.51 $346.89 $345.76 $382.38
40 $228.21 $222.08 $299.23 $305.33 $351.29 $350.14 $387.23
41 $232.50 $226.25 $304.85 $311.07 $357.89 $356.72 $394.50
42 $236.61 $230.25 $310.24 $316.56 $364.21 $363.02 $401.47
43 $242.32 $235.81 $317.73 $324.21 $373.01 $371.79 $411.16
44 $249.46 $242.76 $327.10 $333.77 $384.00 $382.75 $423.28
45 $257.86 $250.92 $338.10 $344.99 $396.92 $395.62 $437.52
46 $267.86 $260.65 $351.21 $358.37 $412.31 $410.97 $454.49
47 $279.11 $271.60 $365.96 $373.43 $429.63 $428.23 $473.58
48 $291.96 $284.11 $382.82 $390.63 $449.42 $447.95 $495.40
49 $304.64 $296.45 $399.45 $407.59 $468.94 $467.41 $516.91
50 $318.93 $310.35 $418.18 $426.70 $490.93 $489.32 $541.15
51 $333.03 $324.08 $436.67 $445.58 $512.64 $510.97 $565.08
52 $348.57 $339.20 $457.04 $466.36 $536.56 $534.80 $591.45
53 $364.28 $354.49 $477.65 $487.39 $560.75 $558.91 $618.11
54 $381.25 $371.00 $499.89 $510.09 $586.86 $584.94 $646.89
55 $398.21 $387.51 $522.14 $532.78 $612.97 $610.97 $675.68
56 $416.61 $405.41 $546.25 $557.39 $641.29 $639.19 $706.89
57 $435.18 $423.48 $570.60 $582.24 $669.87 $667.68 $738.40
58 $455.00 $442.77 $596.59 $608.76 $700.38 $698.10 $772.03
59 $464.82 $452.32 $609.47 $621.90 $715.50 $713.16 $788.69
60 $484.64 $471.61 $635.46 $648.42 $746.01 $743.58 $822.33
61 $501.78 $488.29 $657.94 $671.35 $772.40 $769.88 $851.41
62 $513.03 $499.24 $672.69 $686.41 $789.72 $787.14 $870.50
63 $527.14 $512.97 $691.19 $705.28 $811.43 $808.78 $894.44
64+ $535.71 $521.31 $702.42 $716.76 $824.64 $821.94 $908.97
Counties: Kern, Riverside, San Bernardino, and SanDiego
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 14, 17 & 19
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $110.09 $107.13 $144.35 $147.29 $169.46 $168.91 $186.80
0–18 Total $125.08 $122.12 $159.34 $162.28 $184.45 $183.90 $201.79
19–20 $110.09 $107.13 $144.35 $147.29 $169.46 $168.91 $186.80
21 $173.37 $168.71 $227.32 $231.96 $266.87 $266.00 $294.17
22 $173.37 $168.71 $227.32 $231.96 $266.87 $266.00 $294.17
23 $173.37 $168.71 $227.32 $231.96 $266.87 $266.00 $294.17
24 $173.37 $168.71 $227.32 $231.96 $266.87 $266.00 $294.17
25 $174.06 $169.38 $228.23 $232.88 $267.94 $267.06 $295.35
26 $177.53 $172.76 $232.78 $237.52 $273.28 $272.38 $301.23
27 $181.69 $176.81 $238.23 $243.09 $279.68 $278.77 $308.29
28 $188.45 $183.39 $247.10 $252.14 $290.09 $289.14 $319.76
29 $194.00 $188.79 $254.37 $259.56 $298.63 $297.65 $329.18
30 $196.77 $191.48 $258.01 $263.27 $302.90 $301.91 $333.88
31 $200.94 $195.53 $263.47 $268.84 $309.30 $308.29 $340.94
32 $205.10 $199.58 $268.92 $274.41 $315.71 $314.68 $348.00
33 $207.70 $202.11 $272.33 $277.88 $319.71 $318.67 $352.41
34 $210.47 $204.81 $275.97 $281.60 $323.98 $322.92 $357.12
35 $211.86 $206.16 $277.79 $283.45 $326.12 $325.05 $359.47
36 $213.25 $207.51 $279.61 $285.31 $328.25 $327.18 $361.83
37 $214.63 $208.86 $281.42 $287.16 $330.39 $329.31 $364.18
38 $216.02 $210.21 $283.24 $289.02 $332.52 $331.43 $366.53
39 $218.79 $212.91 $286.88 $292.73 $336.79 $335.69 $371.24
40 $221.57 $215.61 $290.52 $296.44 $341.06 $339.95 $375.95
41 $225.73 $219.66 $295.97 $302.01 $347.46 $346.33 $383.01
42 $229.72 $223.54 $301.20 $307.34 $353.60 $352.45 $389.77
43 $235.26 $228.94 $308.48 $314.77 $362.14 $360.96 $399.19
44 $242.20 $235.69 $317.57 $324.04 $372.82 $371.60 $410.95
45 $250.35 $243.62 $328.25 $334.95 $385.36 $384.10 $424.78
46 $260.05 $253.06 $340.98 $347.94 $400.31 $399.00 $441.25
47 $270.98 $263.69 $355.30 $362.55 $417.12 $415.75 $459.79
48 $283.46 $275.84 $371.67 $379.25 $436.33 $434.91 $480.97
49 $295.77 $287.82 $387.81 $395.72 $455.28 $453.79 $501.85
50 $309.64 $301.31 $406.00 $414.28 $476.63 $475.07 $525.39
51 $323.33 $314.64 $423.96 $432.60 $497.71 $496.09 $548.63
52 $338.42 $329.32 $443.73 $452.78 $520.93 $519.23 $574.22
53 $353.67 $344.17 $463.74 $473.19 $544.42 $542.64 $600.11
54 $370.14 $360.19 $485.33 $495.23 $569.77 $567.91 $628.05
55 $386.61 $376.22 $506.93 $517.26 $595.12 $593.18 $656.00
56 $404.47 $393.60 $530.34 $541.16 $622.61 $620.57 $686.30
57 $422.50 $411.14 $553.98 $565.28 $650.36 $648.24 $716.89
58 $441.75 $429.87 $579.22 $591.03 $679.99 $677.76 $749.54
59 $451.28 $439.15 $591.72 $603.78 $694.66 $692.39 $765.72
60 $470.53 $457.88 $616.95 $629.53 $724.29 $721.92 $798.38
61 $487.17 $474.07 $638.77 $651.80 $749.91 $747.45 $826.62
62 $498.09 $484.70 $653.10 $666.41 $766.72 $764.21 $845.15
63 $511.79 $498.03 $671.05 $684.74 $787.80 $785.23 $868.39
64+ $520.11 $506.13 $681.96 $695.88 $800.61 $798.00 $882.51
Counties: Los Angeles 906‐912, 915, 917, 918, and 935
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 15
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $115.59 $112.49 $151.57 $154.66 $177.94 $177.35 $196.14
0–18 Total $130.58 $127.48 $166.56 $169.65 $192.93 $192.34 $211.13
19–20 $115.59 $112.49 $151.57 $154.66 $177.94 $177.35 $196.14
21 $182.04 $177.14 $238.69 $243.55 $280.21 $279.30 $308.88
22 $182.04 $177.14 $238.69 $243.55 $280.21 $279.30 $308.88
23 $182.04 $177.14 $238.69 $243.55 $280.21 $279.30 $308.88
24 $182.04 $177.14 $238.69 $243.55 $280.21 $279.30 $308.88
25 $182.77 $177.85 $239.64 $244.53 $281.33 $280.42 $310.11
26 $186.41 $181.40 $244.42 $249.40 $286.94 $286.00 $316.29
27 $190.78 $185.65 $250.15 $255.25 $293.66 $292.70 $323.70
28 $197.88 $192.56 $259.45 $264.74 $304.59 $303.60 $335.75
29 $203.70 $198.22 $267.09 $272.54 $313.56 $312.53 $345.63
30 $206.61 $201.06 $270.91 $276.43 $318.04 $317.00 $350.58
31 $210.98 $205.31 $276.64 $282.28 $324.77 $323.71 $357.99
32 $215.35 $209.56 $282.37 $288.13 $331.49 $330.41 $365.40
33 $218.08 $212.22 $285.95 $291.78 $335.70 $334.60 $370.04
34 $220.99 $215.05 $289.77 $295.68 $340.18 $339.07 $374.98
35 $222.45 $216.47 $291.68 $297.62 $342.42 $341.30 $377.45
36 $223.91 $217.89 $293.59 $299.57 $344.66 $343.54 $379.92
37 $225.36 $219.30 $295.50 $301.52 $346.90 $345.77 $382.39
38 $226.82 $220.72 $297.41 $303.47 $349.15 $348.01 $384.86
39 $229.73 $223.56 $301.22 $307.37 $353.63 $352.47 $389.80
40 $232.65 $226.39 $305.04 $311.26 $358.11 $356.94 $394.75
41 $237.01 $230.64 $310.77 $317.11 $364.84 $363.65 $402.16
42 $241.20 $234.72 $316.26 $322.71 $371.28 $370.07 $409.26
43 $247.03 $240.38 $323.90 $330.50 $380.25 $379.01 $419.15
44 $254.31 $247.47 $333.45 $340.25 $391.46 $390.18 $431.50
45 $262.86 $255.80 $344.67 $351.69 $404.63 $403.31 $446.02
46 $273.06 $265.72 $358.03 $365.33 $420.32 $418.95 $463.32
47 $284.53 $276.88 $373.07 $380.68 $437.97 $436.54 $482.78
48 $297.63 $289.63 $390.26 $398.21 $458.15 $456.65 $505.02
49 $310.56 $302.21 $407.20 $415.50 $478.04 $476.48 $526.95
50 $325.12 $316.38 $426.30 $434.99 $500.46 $498.83 $551.66
51 $339.50 $330.37 $445.15 $454.23 $522.60 $520.89 $576.06
52 $355.34 $345.79 $465.92 $475.42 $546.98 $545.19 $602.93
53 $371.36 $361.37 $486.92 $496.85 $571.64 $569.77 $630.11
54 $388.65 $378.20 $509.60 $519.99 $598.26 $596.30 $659.45
55 $405.95 $395.03 $532.27 $543.13 $624.88 $622.83 $688.80
56 $424.70 $413.28 $556.86 $568.21 $653.74 $651.60 $720.61
57 $443.63 $431.70 $581.68 $593.54 $682.88 $680.65 $752.74
58 $463.83 $451.36 $608.18 $620.58 $713.98 $711.65 $787.02
59 $473.85 $461.11 $621.31 $633.97 $729.40 $727.01 $804.01
60 $494.05 $480.77 $647.80 $661.01 $760.50 $758.01 $838.29
61 $511.53 $497.77 $670.71 $684.39 $787.40 $784.83 $867.95
62 $523.00 $508.94 $685.75 $699.73 $805.05 $802.42 $887.41
63 $537.38 $522.93 $704.61 $718.97 $827.19 $824.49 $911.81
64+ $546.12 $531.42 $716.07 $730.65 $840.63 $837.90 $926.64
Counties: Los Angeles other
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 16
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Age on 2016
effective date
Bronze 60
HMO 6000/70
w/ Child Dental*
Bronze 60 HSA
HMO 4500/40%
w/ Child Dental*
Silver 70
HMO 1000/50
w/ Child Dental*
Silver 70
HMO 1500/45
w/ Child Dental*
Gold 80
HMO 0/35
w/ Child Dental*
Gold 80
HMO 500/30
w/ Child Dental*
Platinum 90
HMO 0/20
w/ Child Dental*
0–18 CD $14.99 $14.99 $14.99 $14.99 $14.99 $14.99 $14.99
0–18 Medical $121.68 $118.41 $159.54 $162.80 $187.30 $186.69 $206.46
0–18 Total $136.67 $133.40 $174.53 $177.79 $202.29 $201.68 $221.45
19–20 $121.68 $118.41 $159.54 $162.80 $187.30 $186.69 $206.46
21 $191.62 $186.47 $251.25 $256.37 $294.96 $294.00 $325.13
22 $191.62 $186.47 $251.25 $256.37 $294.96 $294.00 $325.13
23 $191.62 $186.47 $251.25 $256.37 $294.96 $294.00 $325.13
24 $191.62 $186.47 $251.25 $256.37 $294.96 $294.00 $325.13
25 $192.39 $187.21 $252.26 $257.40 $296.14 $295.17 $326.44
26 $196.22 $190.94 $257.28 $262.53 $302.04 $301.05 $332.94
27 $200.82 $195.42 $263.31 $268.68 $309.12 $308.11 $340.74
28 $208.29 $202.69 $273.11 $278.68 $320.62 $319.58 $353.42
29 $214.42 $208.66 $281.15 $286.88 $330.06 $328.98 $363.83
30 $217.49 $211.64 $285.17 $290.98 $334.78 $333.69 $369.03
31 $222.09 $216.12 $291.20 $297.14 $341.86 $340.74 $376.83
32 $226.69 $220.59 $297.23 $303.29 $348.94 $347.80 $384.63
33 $229.56 $223.39 $301.00 $307.14 $353.36 $352.21 $389.51
34 $232.63 $226.37 $305.02 $311.24 $358.08 $356.91 $394.71
35 $234.16 $227.86 $307.03 $313.29 $360.44 $359.27 $397.31
36 $235.69 $229.36 $309.04 $315.34 $362.80 $361.62 $399.92
37 $237.22 $230.85 $311.05 $317.39 $365.16 $363.97 $402.52
38 $238.76 $232.34 $313.06 $319.44 $367.52 $366.32 $405.12
39 $241.82 $235.32 $317.08 $323.54 $372.24 $371.03 $410.32
40 $244.89 $238.31 $321.10 $327.65 $376.96 $375.73 $415.52
41 $249.49 $242.78 $327.13 $333.80 $384.04 $382.79 $423.33
42 $253.90 $247.07 $332.91 $339.70 $390.82 $389.55 $430.80
43 $260.03 $253.04 $340.95 $347.90 $400.26 $398.95 $441.21
44 $267.69 $260.50 $351.00 $358.15 $412.06 $410.71 $454.21
45 $276.70 $269.26 $362.81 $370.20 $425.92 $424.53 $469.49
46 $287.43 $279.70 $376.88 $384.56 $442.44 $441.00 $487.70
47 $299.50 $291.45 $392.70 $400.71 $461.03 $459.52 $508.19
48 $313.30 $304.87 $410.79 $419.17 $482.26 $480.69 $531.59
49 $326.90 $318.11 $428.63 $437.37 $503.20 $501.56 $554.68
50 $342.23 $333.03 $448.73 $457.88 $526.80 $525.08 $580.69
51 $357.37 $347.76 $468.58 $478.14 $550.10 $548.31 $606.38
52 $374.04 $363.98 $490.44 $500.44 $575.77 $573.88 $634.66
53 $390.90 $380.39 $512.55 $523.00 $601.72 $599.76 $663.27
54 $409.11 $398.11 $536.42 $547.36 $629.74 $627.69 $694.16
55 $427.31 $415.82 $560.29 $571.71 $657.76 $655.62 $725.05
56 $447.05 $435.03 $586.17 $598.12 $688.15 $685.90 $758.54
57 $466.98 $454.42 $612.30 $624.78 $718.82 $716.47 $792.35
58 $488.25 $475.12 $640.19 $653.24 $751.56 $749.11 $828.44
59 $498.79 $485.37 $654.01 $667.34 $767.79 $765.28 $846.33
60 $520.06 $506.07 $681.89 $695.80 $800.53 $797.91 $882.42
61 $538.45 $523.97 $706.01 $720.41 $828.84 $826.13 $913.63
62 $550.52 $535.72 $721.84 $736.56 $847.43 $844.66 $934.11
63 $565.66 $550.45 $741.69 $756.81 $870.73 $867.88 $959.80
64+ $574.86 $559.41 $753.75 $769.11 $884.88 $882.00 $975.39
Counties: Orange
KAISER MEDICAL PLANS
EFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
KAISER MEDICAL PLAN RATES
Rate Region 18
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Mapped From Gateway 1800 HSA Gold HMO
Gateway 30 Gateway 70 Gateway 2000 HSA BENEFITS Platinum HMO Platinum HMO Gold HMOLifetime Maximum Unlimited Unlimited Unlimited
$2,000 Single Coverage
Calendar Year Deductible: None None $2,600 Single w/ Family
$4,000 Family Coverage
$2,000 Single Coverage
Calendar Year Max Out‐of‐Pocket: $4,000 / $8,000 $4,000 / $8,000 $2,600 Single w/ Family
$4,000 Family Coverage
Office Visit $30 per Visit $20 per Visit Covered in Full After Deductible
Preventive Services Covered in Full Covered in Full Covered In Full
Diagnostic X‐Ray & Lab Covered in Full Covered in Full Covered in Full After Deductible
Imaging (CT/PET Scans & MRIs) $100 per Visit $100 per Visit Covered in Full After Deductible
Hospitalization $300 per Day, Days 1‐3 30% Covered in Full After Deductible
Outpatient Surgery Facility $100 per Visit $100 per Visit Covered in Full After Deductible
Outpatient Surgery Professional Covered in Full Covered in Full Covered in Full After Deductible
Emergency Room $150 per Visit $150 per Visit Covered in Full After Deductible
Urgent Care Center $50 per Visit $50 per Visit Covered in Full After Deductible
Maternity: Inpatient $300 per Day, Days 1‐3 30% Covered in Full After Deductible
Prenatal/First Postpartum Visit Covered in Full Covered in Full Covered in Full
Mental Health: Inpatient $300 per Day, Days 1‐3 30% Covered in Full After Deductible
Outpatient $30 per Visit $20 per Visit Covered in Full After Deductible
Substance Abuse: Inpatient Detox Only $300 per Day, Days 1‐3 30% Covered in Full After Deductible
Prescriptions: (Up to a 30‐Day Supply) (Up to a 30‐Day Supply) (Up to a 30‐Day Supply)
Generic $10 Copay $10 Copay Covered in Full After Deductible
Deductible (Brand Name) None None Medical Deductible Applies
Brand $30 copay $30 copay Covered in Full After Deductible
Non Formulary $50 copay $50 copay Covered in Full After Deductible
Pediatric Dental & Vision (Up to age 19)
Annual Out‐of‐Pocket Maximum None None None
Deductible / Waiting Period $0 Deductible / No Waiting Period $0 Deductible / No Waiting Period $0 Deductible / No Waiting Period
Annual Maximum N/A N/A N/A
Office Visit $0 Copay $0 Copay $0 Copay
Diagnostic & Preventive: X‐Ray, Exam, Cleanings $0 Copay $0 Copay $0 Copay
Basic Services: $40 ‐ $365 Copay $40 ‐ $365 Copay $40 ‐ $365 Copay
Basic restorative Depending on Procedure Depending on Procedure Depending on Procedure
Major Services: Crown, Cast, Prothodontists, $40 ‐ $365 Copay $40 ‐ $365 Copay $40 ‐ $365 Copay
Endodontics, Periodontics, Oral Surgery Depending on Procedure Depending on Procedure Depending on Procedure
Orthodontics (Medically Necessary) $1,000 Maximum $1,000 Maximum $1,000 Maximum
Pediatric Vision (Up to age 19)
Includes Exam and Eyewear
Adult Vision Exam $0 Copay $0 Copay $0 Copay
Adult Optical (Eyewear) Not Covered Not Covered Not Covered
Provider Restrictions
WHA Members & Dependents
Open Enrollment November 1st ‐ November 30th.
December 1, 2016 ‐ November 30, 2017
WESTERN HEALTH ADVANTAGE
One pair of standard frames & lenses
or contact lenses per calendar year
One pair of standard frames & lenses
or contact lenses per calendar year
One pair of standard frames & lenses
or contact lenses per calendar year
Western Health Advantage HMO
Eligibility Guidelines ‐ GUARANTEED ISSUE
Members may apply at anytime except if you are a new member, then it is the 1st of the month following new membership.
Qualifying Events: you may join within 30 days after you have a loss of coverage, marriage, birth or adoption.
Over Age Dependents: may remain on coverage up to age 26.
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
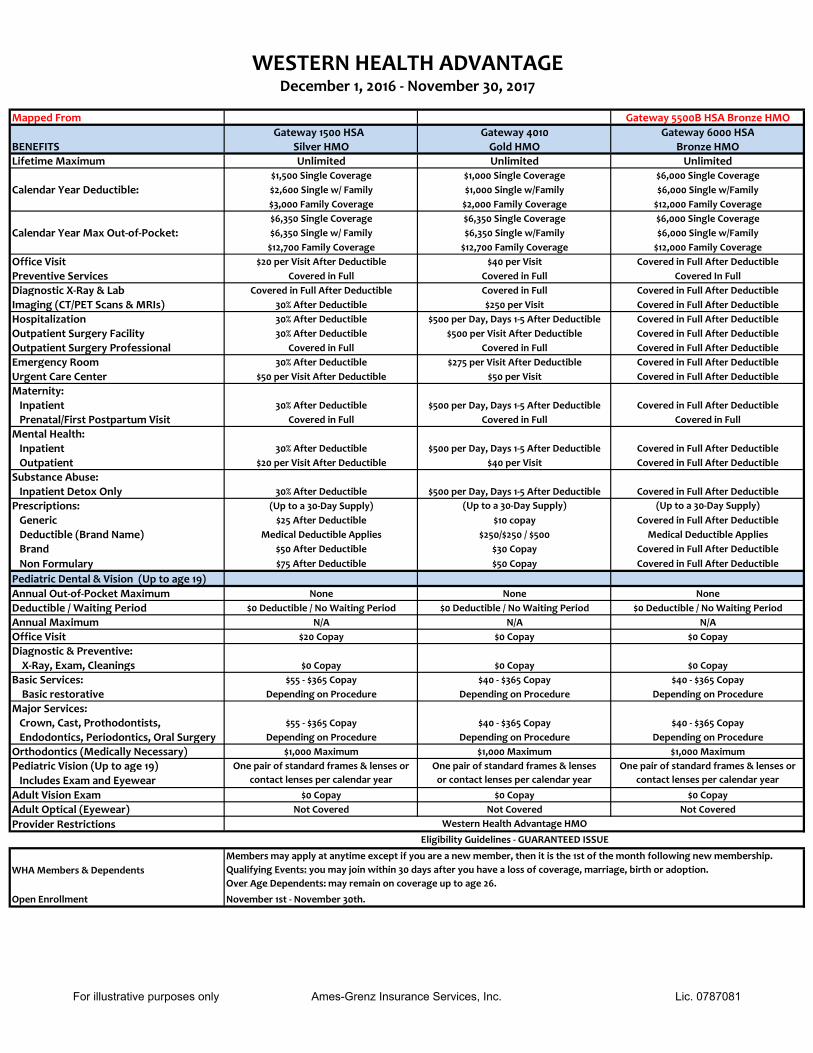
Mapped From Gateway 5500B HSA Bronze HMO
Gateway 1500 HSA Gateway 4010 Gateway 6000 HSA
BENEFITS Silver HMO Gold HMO Bronze HMO
Lifetime Maximum Unlimited Unlimited Unlimited$1,500 Single Coverage $1,000 Single Coverage $6,000 Single Coverage
Calendar Year Deductible: $2,600 Single w/ Family $1,000 Single w/Family $6,000 Single w/Family
$3,000 Family Coverage $2,000 Family Coverage $12,000 Family Coverage
$6,350 Single Coverage $6,350 Single Coverage $6,000 Single Coverage
Calendar Year Max Out‐of‐Pocket: $6,350 Single w/ Family $6,350 Single w/Family $6,000 Single w/Family
$12,700 Family Coverage $12,700 Family Coverage $12,000 Family Coverage
Office Visit $20 per Visit After Deductible $40 per Visit Covered in Full After Deductible
Preventive Services Covered in Full Covered in Full Covered In Full
Diagnostic X‐Ray & Lab Covered in Full After Deductible Covered in Full Covered in Full After Deductible
Imaging (CT/PET Scans & MRIs) 30% After Deductible $250 per Visit Covered in Full After Deductible
Hospitalization 30% After Deductible $500 per Day, Days 1‐5 After Deductible Covered in Full After Deductible
Outpatient Surgery Facility 30% After Deductible $500 per Visit After Deductible Covered in Full After Deductible
Outpatient Surgery Professional Covered in Full Covered in Full Covered in Full After Deductible
Emergency Room 30% After Deductible $275 per Visit After Deductible Covered in Full After Deductible
Urgent Care Center $50 per Visit After Deductible $50 per Visit Covered in Full After Deductible
Maternity:
Inpatient 30% After Deductible $500 per Day, Days 1‐5 After Deductible Covered in Full After Deductible
Prenatal/First Postpartum Visit Covered in Full Covered in Full Covered in Full
Mental Health:
Inpatient 30% After Deductible $500 per Day, Days 1‐5 After Deductible Covered in Full After Deductible
Outpatient $20 per Visit After Deductible $40 per Visit Covered in Full After Deductible
Substance Abuse:
Inpatient Detox Only 30% After Deductible $500 per Day, Days 1‐5 After Deductible Covered in Full After Deductible
Prescriptions: (Up to a 30‐Day Supply) (Up to a 30‐Day Supply) (Up to a 30‐Day Supply)
Generic $25 After Deductible $10 copay Covered in Full After Deductible
Deductible (Brand Name) Medical Deductible Applies $250/$250 / $500 Medical Deductible Applies
Brand $50 After Deductible $30 Copay Covered in Full After Deductible
Non Formulary $75 After Deductible $50 Copay Covered in Full After Deductible
Pediatric Dental & Vision (Up to age 19)
Annual Out‐of‐Pocket Maximum None None None
Deductible / Waiting Period $0 Deductible / No Waiting Period $0 Deductible / No Waiting Period $0 Deductible / No Waiting Period
Annual Maximum N/A N/A N/A
Office Visit $20 Copay $0 Copay $0 Copay
Diagnostic & Preventive:
X‐Ray, Exam, Cleanings $0 Copay $0 Copay $0 Copay
Basic Services: $55 ‐ $365 Copay $40 ‐ $365 Copay $40 ‐ $365 Copay
Basic restorative Depending on Procedure Depending on Procedure Depending on Procedure
Major Services:
Crown, Cast, Prothodontists, $55 ‐ $365 Copay $40 ‐ $365 Copay $40 ‐ $365 Copay
Endodontics, Periodontics, Oral Surgery Depending on Procedure Depending on Procedure Depending on Procedure
Orthodontics (Medically Necessary) $1,000 Maximum $1,000 Maximum $1,000 Maximum
Pediatric Vision (Up to age 19)
Includes Exam and Eyewear
Adult Vision Exam $0 Copay $0 Copay $0 Copay
Adult Optical (Eyewear) Not Covered Not Covered Not Covered
Provider Restrictions
WHA Members & Dependents
Open Enrollment November 1st ‐ November 30th.
Western Health Advantage HMO
Eligibility Guidelines ‐ GUARANTEED ISSUE
Members may apply at anytime except if you are a new member, then it is the 1st of the month following new membership.
Qualifying Events: you may join within 30 days after you have a loss of coverage, marriage, birth or adoption.
Over Age Dependents: may remain on coverage up to age 26.
December 1, 2016 ‐ November 30, 2017
WESTERN HEALTH ADVANTAGE
One pair of standard frames & lenses or
contact lenses per calendar year
One pair of standard frames & lenses
or contact lenses per calendar year
One pair of standard frames & lenses or
contact lenses per calendar year
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
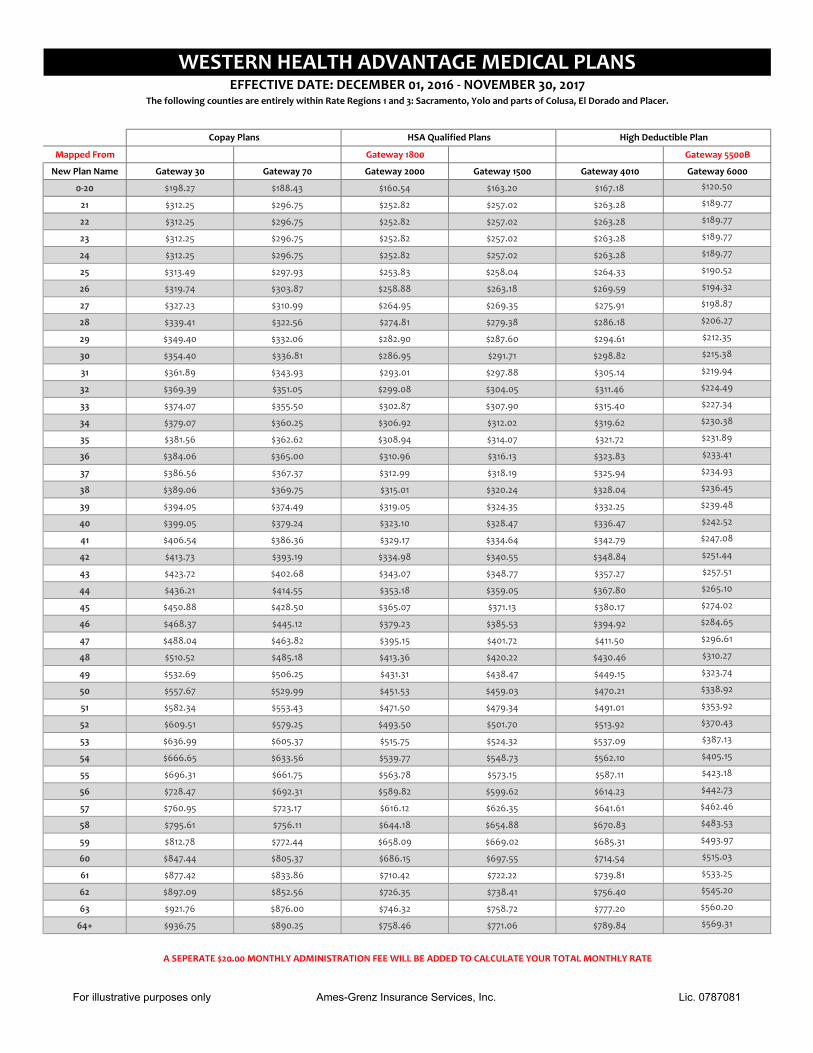
Mapped From Gateway 1800 Gateway 5500B
New Plan Name Gateway 30 Gateway 70 Gateway 2000 Gateway 1500 Gateway 4010 Gateway 6000
0‐20 $198.27 $188.43 $160.54 $163.20 $167.18 $120.50
21 $312.25 $296.75 $252.82 $257.02 $263.28 $189.77
22 $312.25 $296.75 $252.82 $257.02 $263.28 $189.77
23 $312.25 $296.75 $252.82 $257.02 $263.28 $189.77
24 $312.25 $296.75 $252.82 $257.02 $263.28 $189.77
25 $313.49 $297.93 $253.83 $258.04 $264.33 $190.52
26 $319.74 $303.87 $258.88 $263.18 $269.59 $194.32
27 $327.23 $310.99 $264.95 $269.35 $275.91 $198.87
28 $339.41 $322.56 $274.81 $279.38 $286.18 $206.27
29 $349.40 $332.06 $282.90 $287.60 $294.61 $212.35
30 $354.40 $336.81 $286.95 $291.71 $298.82 $215.38
31 $361.89 $343.93 $293.01 $297.88 $305.14 $219.94
32 $369.39 $351.05 $299.08 $304.05 $311.46 $224.49
33 $374.07 $355.50 $302.87 $307.90 $315.40 $227.34
34 $379.07 $360.25 $306.92 $312.02 $319.62 $230.38
35 $381.56 $362.62 $308.94 $314.07 $321.72 $231.89
36 $384.06 $365.00 $310.96 $316.13 $323.83 $233.41
37 $386.56 $367.37 $312.99 $318.19 $325.94 $234.93
38 $389.06 $369.75 $315.01 $320.24 $328.04 $236.45
39 $394.05 $374.49 $319.05 $324.35 $332.25 $239.48
40 $399.05 $379.24 $323.10 $328.47 $336.47 $242.52
41 $406.54 $386.36 $329.17 $334.64 $342.79 $247.08
42 $413.73 $393.19 $334.98 $340.55 $348.84 $251.44
43 $423.72 $402.68 $343.07 $348.77 $357.27 $257.51
44 $436.21 $414.55 $353.18 $359.05 $367.80 $265.10
45 $450.88 $428.50 $365.07 $371.13 $380.17 $274.02
46 $468.37 $445.12 $379.23 $385.53 $394.92 $284.65
47 $488.04 $463.82 $395.15 $401.72 $411.50 $296.61
48 $510.52 $485.18 $413.36 $420.22 $430.46 $310.27
49 $532.69 $506.25 $431.31 $438.47 $449.15 $323.74
50 $557.67 $529.99 $451.53 $459.03 $470.21 $338.92
51 $582.34 $553.43 $471.50 $479.34 $491.01 $353.92
52 $609.51 $579.25 $493.50 $501.70 $513.92 $370.43
53 $636.99 $605.37 $515.75 $524.32 $537.09 $387.13
54 $666.65 $633.56 $539.77 $548.73 $562.10 $405.15
55 $696.31 $661.75 $563.78 $573.15 $587.11 $423.18
56 $728.47 $692.31 $589.82 $599.62 $614.23 $442.73
57 $760.95 $723.17 $616.12 $626.35 $641.61 $462.46
58 $795.61 $756.11 $644.18 $654.88 $670.83 $483.53
59 $812.78 $772.44 $658.09 $669.02 $685.31 $493.97
60 $847.44 $805.37 $686.15 $697.55 $714.54 $515.03
61 $877.42 $833.86 $710.42 $722.22 $739.81 $533.25
62 $897.09 $852.56 $726.35 $738.41 $756.40 $545.20
63 $921.76 $876.00 $746.32 $758.72 $777.20 $560.20
64+ $936.75 $890.25 $758.46 $771.06 $789.84 $569.31
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
High Deductible PlanCopay Plans HSA Qualified Plans
WESTERN HEALTH ADVANTAGE MEDICAL PLANSEFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
The following counties are entirely within Rate Regions 1 and 3: Sacramento, Yolo and parts of Colusa, El Dorado and Placer.
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Mapped From Gateway 1800 Gateway 5500B
New Plan Name Gateway 30 Gateway 70 Gateway 2000 Gateway 1500 Gateway 4010 Gateway 6000
0‐20 $206.27 $196.03 $167.01 $169.78 $173.92 $125.36
21 $324.84 $308.71 $263.02 $267.38 $273.89 $197.42
22 $324.84 $308.71 $263.02 $267.38 $273.89 $197.42
23 $324.84 $308.71 $263.02 $267.38 $273.89 $197.42
24 $324.84 $308.71 $263.02 $267.38 $273.89 $197.42
25 $326.13 $309.94 $264.07 $268.44 $274.98 $198.20
26 $332.63 $316.11 $269.33 $273.79 $280.46 $202.15
27 $340.43 $323.52 $275.64 $280.21 $287.03 $206.89
28 $353.10 $335.56 $285.90 $290.64 $297.71 $214.59
29 $363.49 $345.44 $294.31 $299.19 $306.48 $220.91
30 $368.69 $350.38 $298.52 $303.47 $310.86 $224.07
31 $376.48 $357.79 $304.84 $309.89 $317.43 $228.80
32 $384.28 $365.20 $311.15 $316.31 $324.01 $233.54
33 $389.15 $369.83 $315.09 $320.32 $328.12 $236.50
34 $394.35 $374.77 $319.30 $324.59 $332.50 $239.66
35 $396.95 $377.24 $321.41 $326.73 $334.69 $241.24
36 $399.55 $379.71 $323.51 $328.87 $336.88 $242.82
37 $402.15 $382.18 $325.61 $331.01 $339.07 $244.40
38 $404.75 $384.65 $327.72 $333.15 $341.26 $245.98
39 $409.94 $389.59 $331.93 $337.43 $345.64 $249.14
40 $415.14 $394.53 $336.13 $341.71 $350.03 $252.30
41 $422.94 $401.94 $342.45 $348.12 $356.60 $257.04
42 $430.41 $409.04 $348.50 $354.27 $362.90 $261.58
43 $440.80 $418.91 $356.91 $362.83 $371.66 $267.89
44 $453.80 $431.26 $367.43 $373.52 $382.62 $275.79
45 $469.06 $445.77 $379.80 $386.09 $395.49 $285.07
46 $487.26 $463.06 $394.53 $401.07 $410.83 $296.13
47 $507.72 $482.51 $411.10 $417.91 $428.09 $308.56
48 $531.11 $504.74 $430.03 $437.16 $447.81 $322.78
49 $554.17 $526.65 $448.71 $456.15 $467.25 $336.79
50 $580.16 $551.35 $469.75 $477.54 $489.16 $352.59
51 $605.82 $575.74 $490.53 $498.66 $510.80 $368.18
52 $634.08 $602.60 $513.41 $521.92 $534.63 $385.36
53 $662.67 $629.76 $536.56 $545.45 $558.73 $402.73
54 $693.53 $659.09 $561.54 $570.85 $584.75 $421.49
55 $724.39 $688.42 $586.53 $596.25 $610.77 $440.24
56 $757.85 $720.22 $613.62 $623.79 $638.98 $460.58
57 $791.63 $752.32 $640.97 $651.60 $667.46 $481.11
58 $827.69 $786.59 $670.17 $681.28 $697.87 $503.02
59 $845.55 $803.57 $684.64 $695.99 $712.93 $513.88
60 $881.61 $837.83 $713.83 $725.66 $743.33 $535.79
61 $912.80 $867.47 $739.08 $751.33 $769.63 $554.75
62 $933.26 $886.92 $755.65 $768.18 $786.88 $567.18
63 $958.92 $911.31 $776.43 $789.30 $808.52 $582.78
64+ $974.52 $926.13 $789.06 $802.14 $821.67 $592.26
A SEPERATE $20.00 MONTHLY ADMINISTRATION FEE WILL BE ADDED TO CALCULATE YOUR TOTAL MONTHLY RATE
Copay Plans HSA Qualified Plans
WESTERN HEALTH ADVANTAGE MEDICAL PLANSEFFECTIVE DATE: DECEMBER 01, 2016 ‐ NOVEMBER 30, 2017
The following counties are entirely within Rate Regions 2: Marin, Napa, Sonoma and part of Solano.
High Deductible Plan
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
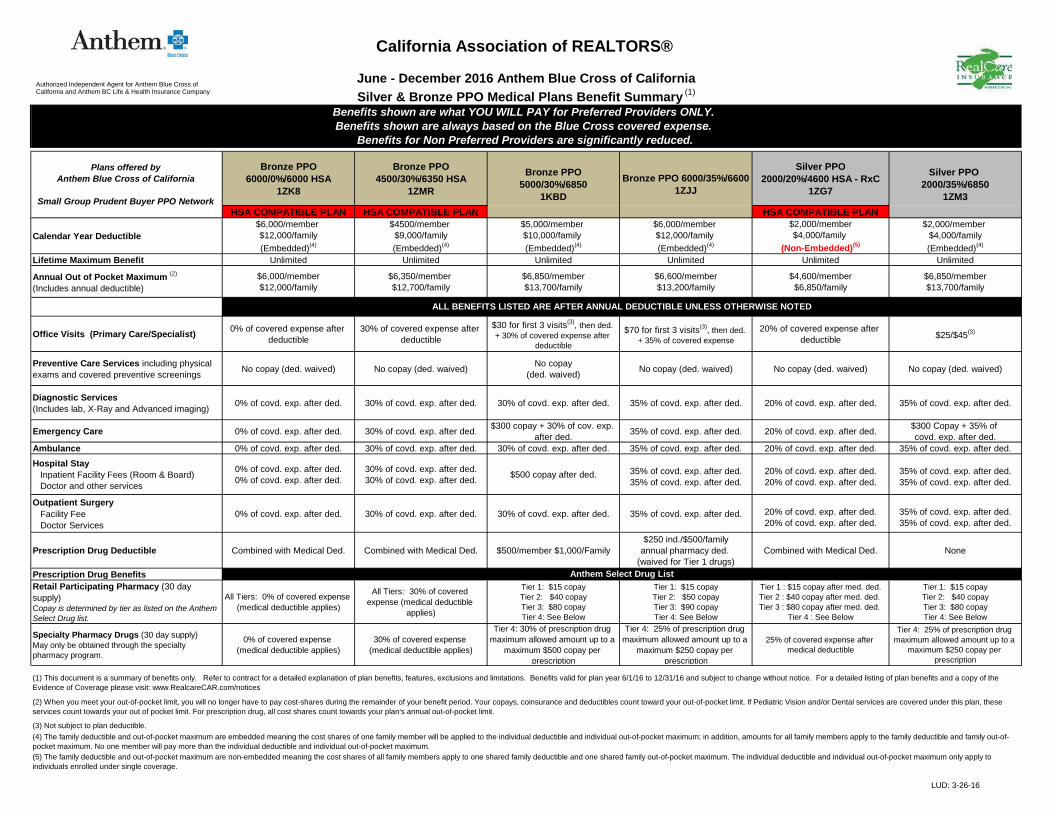
LUD: 3-26-16
Bronze PPO6000/0%/6000 HSA
1ZK8
Bronze PPO4500/30%/6350 HSA
1ZMR
Silver PPO2000/20%/4600 HSA - RxC
1ZG7
HSA COMPATIBLE PLAN HSA COMPATIBLE PLAN HSA COMPATIBLE PLAN
Calendar Year Deductible$6,000/member $12,000/family(Embedded)(4)
$4500/member $9,000/family(Embedded)(4)
$5,000/member $10,000/family (Embedded)(4)
$6,000/member $12,000/family (Embedded)(4)
$2,000/member$4,000/family
(Non-Embedded)(5)
$2,000/member $4,000/family(Embedded)(4)
Lifetime Maximum Benefit Unlimited Unlimited Unlimited Unlimited Unlimited Unlimited
Annual Out of Pocket Maximum (2)
(Includes annual deductible) $6,000/member$12,000/family
$6,350/member $12,700/family
$6,850/member$13,700/family
$6,600/member$13,200/family
$4,600/member$6,850/family
$6,850/member$13,700/family
Office Visits (Primary Care/Specialist) 0% of covered expense after deductible
30% of covered expense after deductible
$30 for first 3 visits(3), then ded. + 30% of covered expense after
deductible
$70 for first 3 visits(3), then ded. + 35% of covered expense
20% of covered expense after deductible $25/$45(3)
Preventive Care Services including physical exams and covered preventive screenings No copay (ded. waived) No copay (ded. waived) No copay
(ded. waived) No copay (ded. waived) No copay (ded. waived) No copay (ded. waived)
Diagnostic Services(Includes lab, X-Ray and Advanced imaging) 0% of covd. exp. after ded. 30% of covd. exp. after ded. 30% of covd. exp. after ded. 35% of covd. exp. after ded. 20% of covd. exp. after ded. 35% of covd. exp. after ded.
Emergency Care 0% of covd. exp. after ded. 30% of covd. exp. after ded. $300 copay + 30% of cov. exp. after ded. 35% of covd. exp. after ded. 20% of covd. exp. after ded. $300 Copay + 35% of
covd. exp. after ded.Ambulance 0% of covd. exp. after ded. 30% of covd. exp. after ded. 30% of covd. exp. after ded. 35% of covd. exp. after ded. 20% of covd. exp. after ded. 35% of covd. exp. after ded.
Hospital Stay Inpatient Facility Fees (Room & Board) Doctor and other services
0% of covd. exp. after ded.0% of covd. exp. after ded.
30% of covd. exp. after ded.30% of covd. exp. after ded. $500 copay after ded. 35% of covd. exp. after ded.
35% of covd. exp. after ded.20% of covd. exp. after ded.20% of covd. exp. after ded.
35% of covd. exp. after ded.35% of covd. exp. after ded.
Outpatient Surgery Facility Fee Doctor Services
0% of covd. exp. after ded. 30% of covd. exp. after ded. 30% of covd. exp. after ded. 35% of covd. exp. after ded. 20% of covd. exp. after ded.20% of covd. exp. after ded.
35% of covd. exp. after ded.35% of covd. exp. after ded.
Prescription Drug Deductible Combined with Medical Ded. Combined with Medical Ded. $500/member $1,000/Family $250 ind./$500/family
annual pharmacy ded. (waived for Tier 1 drugs)
Combined with Medical Ded. None
Prescription Drug BenefitsRetail Participating Pharmacy (30 day supply)Copay is determined by tier as listed on the Anthem Select Drug list.
All Tiers: 0% of covered expense (medical deductible applies)
All Tiers: 30% of covered expense (medical deductible
applies)
Tier 1: $15 copayTier 2: $40 copayTier 3: $80 copayTier 4: See Below
Tier 1: $15 copayTier 2: $50 copayTier 3: $90 copayTier 4: See Below
Tier 1 : $15 copay after med. ded.Tier 2 : $40 copay after med. ded. Tier 3 : $80 copay after med. ded.
Tier 4 : See Below
Tier 1: $15 copayTier 2: $40 copayTier 3: $80 copayTier 4: See Below
Specialty Pharmacy Drugs (30 day supply)May only be obtained through the specialty pharmacy program.
0% of covered expense (medical deductible applies)
30% of covered expense (medical deductible applies)
Tier 4: 30% of prescription drug maximum allowed amount up to a
maximum $500 copay per prescription
Tier 4: 25% of prescription drug maximum allowed amount up to a
maximum $250 copay per prescription
25% of covered expense after medical deductible
Tier 4: 25% of prescription drug maximum allowed amount up to a
maximum $250 copay per prescription
California Association of REALTORS®
June - December 2016 Anthem Blue Cross of CaliforniaSilver & Bronze PPO Medical Plans Benefit Summary (1)
Benefits shown are what YOU WILL PAY for Preferred Providers ONLY. Benefits shown are always based on the Blue Cross covered expense.
Benefits for Non Preferred Providers are significantly reduced.
(4) The family deductible and out-of-pocket maximum are embedded meaning the cost shares of one family member will be applied to the individual deductible and individual out-of-pocket maximum; in addition, amounts for all family members apply to the family deductible and family out-of-pocket maximum. No one member will pay more than the individual deductible and individual out-of-pocket maximum.(5) The family deductible and out-of-pocket maximum are non-embedded meaning the cost shares of all family members apply to one shared family deductible and one shared family out-of-pocket maximum. The individual deductible and individual out-of-pocket maximum only apply to individuals enrolled under single coverage.
ALL BENEFITS LISTED ARE AFTER ANNUAL DEDUCTIBLE UNLESS OTHERWISE NOTED
Anthem Select Drug List
Bronze PPO5000/30%/6850
1KBD
Plans offered byAnthem Blue Cross of California
Small Group Prudent Buyer PPO Network
Silver PPO 2000/35%/6850
1ZM3
Bronze PPO 6000/35%/66001ZJJ
(3) Not subject to plan deductible.
(2) When you meet your out-of-pocket limit, you will no longer have to pay cost-shares during the remainder of your benefit period. Your copays, coinsurance and deductibles count toward your out-of-pocket limit. If Pediatric Vision and/or Dental services are covered under this plan, these services count towards your out of pocket limit. For prescription drug, all cost shares count towards your plan's annual out-of-pocket limit.
(1) This document is a summary of benefits only. Refer to contract for a detailed explanation of plan benefits, features, exclusions and limitations. Benefits valid for plan year 6/1/16 to 12/31/16 and subject to change without notice. For a detailed listing of plan benefits and a copy of the Evidence of Coverage please visit: www.RealcareCAR.com/notices
Authorized Independent Agent for Anthem Blue Cross of California and Anthem BC Life & Health Insurance Company

LUD 3-26-16
Gold PPO 2000/0%/2500 HSA- RxC
1ZGF
HSA COMPATIBLE PLAN
Calendar Year Deductible$2,000/member
$4,000/family(Non-Embedded)(5)
$1,000/member $3,000/family(Embedded)(4)
$500/member $1,500/family(Embedded)(4)
$0/member$0/family
$200/member$600/family
(Embedded)(4)
Lifetime Maximum Benefit Unlimited Unlimited Unlimited Unlimited UnlimitedAnnual Out of Pocket Maximum (2)
(Includes annual deductible) $2,500/member
$5,000/family$4,000/member
$8,000/family$4,500/member
$9,000/family$5,500/member$11,000/family
$3,000/member$6,000/family
Office Visits (Primary Care/Specialist) $0 of covered expense after deductible $20/$40 Copay (3) $30/$60 Copay (3) $20/$40 Copay (3) $10/$30 Copay (3)
Preventive Care Services including physical exams and covered preventive screenings No copay (deductible waived) No copay (deductible waived) No copay (deductible waived) No copay (deductible waived) No copay (deductible waived)
Diagnostic Services(Includes lab, X-Ray and Advanced imaging) $0 of covered expense after ded. 20% of covered expense after ded. 20% of covered expense after
deductible 30% of covered expense after ded. 10% of covered expense after ded.
Emergency Care $0 of covered expense after ded. $200 Copay + 20% of covered expense after ded.
$200 Copay + 20% of covered expense after deductible
$200 Copay + 30% of covered expense after deductible
$200 Copay and then 10% of covered expenses after deductible
Ambulance $0 of covered expense after ded. 20% of covered expense after ded. 20% of covered expense after deductible 30% of covered expense after ded. 10% of covered expense after ded.
Hospital Stay Inpatient Facility Fees (Room & Board) Doctor and other services
0% of covered expense after ded.0% of covered expense after ded.
20% of covered expense after ded.20% of covered expense after ded.
20% of covered expense after ded.20% of covered expense after ded.
30% of covered expense after ded.30% of covered expense after ded.
10% of covered expense after ded.10% of covered expense after ded.
Outpatient Surgery Facility Fee Doctor Services
0% of covered expense after ded.0% of covered expense after ded.
20% of covered expense after ded.20% of covered expense after ded.
20% of covered expense after ded.20% of covered expense after ded.
30% of covered expense after ded.30% of covered expense after ded.
10% of covered expense after ded.10% of covered expense after ded.
Prescription Drug Deductible Combined with medical deductible$250 annual pharmacy deductible
$500/family(waived for Tier 1 drugs)
$250 annual pharmacy deductible $500/family
(waived for Tier 1 drugs)
$250 annual pharmacy deductible$500/family
(waived for Tier 1 drugs) None
Prescription Drug BenefitsRetail Participating Pharmacy (30 day supply)Copay is determined by tier as listed on the tiered drug formulary list. For more information consult your physician or visit www.anthem.com/ca, click on Customer Care
Tier 1 : $15 copayTier 2 : $40 copayTier 3 : $80 copay Tier 4 : See Below
Tier 1: $15 copayTier 2: $40 copay Tier 3: $80 copayTier 4: See Below
Tier 1: $15 copayTier 2: $40 copay Tier 3: $80 copay Tier 4: See Below
Tier 1 : $15 copayTier 2 : $40 copay Tier 3 : $80 copayTier 4 : See Below
Tier 1 : $10 copayTier 2 : $35 copayTier 3 : $70 copay Tier 4 : See Below
Specialty Pharmacy Drugs (30 day supply)May only be obtained through the specialty pharmacy program.
25% of covered expense after medical deductible
Tier 4: 25% of prescription drug maximum allowed amount up to a maximum $250
copay per prescription
Tier 4: 25% of prescription drug maximum allowed amount up to a
maximum $250 copay per prescription
Tier 4 : 25%of prescription drug maximum allowed amount up to a
maximum $250 copay per prescription
Tier 4 : 25% of prescription drug maximum allowed amount up to a
maximum $250 copay per prescription
Platinum PPO 200/10%/30001ZH1
Gold PPO 20/30%/55001ZF9
Gold PPO 500/20%/45001ZHT
Gold PPO 1000/20%/40001ZH9
California Association of REALTORS® June - December 2016 Anthem Blue Cross of California
Platinum and Gold PPO Medical Plans Benefit Summary (1)
Benefits shown are what YOU WILL PAY for Preferred Providers ONLY. Benefits shown are always based on the Blue Cross covered expense.
Benefits for Non Preferred Providers are significantly reduced.
Plans offered by Anthem Blue Cross of California
Small Group Prudent Buyer PPO Network
ALL BENEFITS LISTED ARE AFTER ANNUAL DEDUCTIBLE UNLESS OTHERWISE NOTED
Anthem Select Drug List
(5) The family deductible and out-of-pocket maximum are non-embedded meaning the cost shares of all
(1) This document is a summary of benefits only. Refer to contract for a detailed explanation of plan benefits, features, exclusions and limitations. Benefits valid for plan year 6/1/15 to 5/31/16 and subject to change without notice. For a detailed listing of plan benefits and a copy of the Evidence of Coverage please visit: www.RealcareCAR.com/notices
(2) When you meet your out-of-pocket limit, you will no longer have to pay cost-shares during the remainder of your benefit period. Your copays, coinsurance and deductibles count toward your out-of-pocket limit. If Pediatric Vision and/or Dental services are covered under this plan, these services count towards your out of pocket limit. For prescription drug, all cost shares count towards your plan's annual out-of-pocket limit.
(3) Not subject to plan deductible.
(4) The family deductible and out-of-pocket maximum are embedded meaning the cost shares of one family member will be applied to the individual deductible and individual out-of-pocket maximum; in addition, amounts for all family members apply to the family deductible and family out-of-pocket maximum. No one member will pay more than the individual deductible and individual out-of-pocket maximum.
Authorized Independent Agent for Anthem Blue Cross of California and Anthem BC Life & Health Insurance Company

LUD: 3-26-16
Plans offered by Anthem Blue Cross of CaliforniaCaliforniaCare Network
Gold HMO 50/30%/68501ZHR
Gold HMO 500/20%/50001ZFD
Calendar Year Deductible (3) None $500/member$1,500/family(Embedded)(4)
Lifetime Maximum Benefit Unlimited UmlimitedAnnual Out of Pocket Maximum (2)
(Includes annual deductible) $6,850/member$13,700/family
$5,000/member$10,000/family
Office Visits (Primary Care/Specialist) $50/$100 Copay $30/$60 Copay
Preventive Care Services including physical exams, preventive screenings, flu vaccine, immunizations, health education, intervention services, and HIV testing (including screenings for cancer, HPV, diabetes, cholesterol, blood pressure, hearing and vision)
No copay (deductible waived) No copay (deductible waived)
Diagnostic Services(Includes lab, X-Ray) 0% 20% of covered expense after deductible
Emergency Care $350 Copay + 30% of covered expense $200 Copay + 20% of covered expense after deductible
Ambulance 30% of covered expense 20% of covered expense after deductibleHospital Stay Inpatient Facility Fees (Room & Board) Doctor and other services
$750 copay per day up to 4 daysCovered in full
20% of covered expense after deductibleCovered in full
Outpatient Surgery Facility Fee Doctor Services
Outpatient facility fee: $500 CopayCovered in full
20% of covered expense after deductibleCovered in full
Prescription Drug Deductible$250 annual pharmacy deductible
$500/family (waived for Tier 1 drugs)
$250 annual pharmacy deductible$500/family
(waived for Tier 1 drugs)
Prescription Drug Benefits
Retail Participating Pharmacy (30 day supply)Copay is determined by tier as listed on the tiered drug formulary list. For more information consult your physician or visit www.anthem.com/ca, click on Customer Care
Tier 1: $15 copayTier 2: $50 copay Tier 3: $90 copay Tier 4: See Below
Tier 1 : $15 copayTier 2 : $40 copayTier 3 : $80 copayTier 4 : See Below
Specialty Pharmacy Drugs (30 day supply)May only be obtained through the specialty pharmacy program.
Tier 4: 25% of prescription drug maximum allowed amount up to a maximum $250 copay per prescription
Tier 4 : 25% of prescription drug maximum allowed amount up to a maximum $250 copay per prescription
(4) The family deductible and out-of-pocket maximum are embedded meaning the cost shares of one family member will be applied to the individual deductible and individual out-of-pocket maximum; in addition, amounts for all family members apply to the family deductible and family out-of-pocket maximum. No one member will pay more than the individual deductible and individual out-of-pocket maximum.
Anthem Select Drug List
ALL BENEFITS LISTED ARE AFTER ANNUAL DEDUCTIBLE UNLESS OTHERWISE NOTED
California Association of REALTORS®
June - December 2016 Anthem Blue Cross of CaliforniaHMO Medical Plans Benefit Summary (1)
Benefits shown are what YOU WILL PAY for Contracted Providers ONLY. Benefits for Non Contracted Providers are not covered.
Benefits shown are always based on the Blue Cross covered expense.
(1) This document is a summary of benefits only. Refer to contract for a detailed explanation of plan benefits, features, exclusions and limitations. Benefits valid for plan year 6/1/16 to 12/31/16 and subject to change without notice. For a detailed listing of plan benefits and a copy of the Evidence of Coverage please visit: www.RealcareCAR.com/notices
(2) When you meet your out-of-pocket limit, you will no longer have to pay cost-shares during the remainder of your benefit period. Your copays, coinsurance and deductibles count toward your out-of-pocket limit. If Pediatric Vision and/or Dental services are covered under this plan, these services count towards your out of pocket limit. For prescription drug, all cost shares count towards your plan's annual out-of-pocket limit.
(3) The annual medical deductible applies to all facility services, home dialysis, and home infusion therapy services, ambulance, DME and hospice services.
Authorized Independent Agent for Anthem Blue Cross of California and Anthem BC Life & Health Insurance

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $184.45 $180.08 $189.18 $184.29 $210.41 $224.3021 $290.47 $283.59 $297.92 $290.22 $331.35 $353.2322 $290.47 $283.59 $297.92 $290.22 $331.35 $353.2323 $290.47 $283.59 $297.92 $290.22 $331.35 $353.2324 $290.47 $283.59 $297.92 $290.22 $331.35 $353.2325 $291.63 $284.72 $299.11 $291.38 $332.68 $354.6426 $297.44 $290.40 $305.07 $297.19 $339.30 $361.7127 $304.41 $297.20 $312.22 $304.15 $347.25 $370.1928 $315.74 $308.26 $323.84 $315.47 $360.18 $383.9629 $325.04 $317.34 $333.37 $324.76 $370.78 $395.2630 $329.68 $321.87 $338.14 $329.40 $376.08 $400.9231 $336.65 $328.68 $345.29 $336.36 $384.03 $409.3932 $343.63 $335.49 $352.44 $343.33 $391.99 $417.8733 $347.98 $339.74 $356.91 $347.68 $396.96 $423.1734 $352.63 $344.28 $361.67 $352.33 $402.26 $428.8235 $354.95 $346.55 $364.06 $354.65 $404.91 $431.6536 $357.28 $348.82 $366.44 $356.97 $407.56 $434.4737 $359.60 $351.08 $368.82 $359.29 $410.21 $437.3038 $361.93 $353.35 $371.21 $361.61 $412.86 $440.1239 $366.57 $357.89 $375.98 $366.26 $418.16 $445.7840 $371.22 $362.43 $380.74 $370.90 $423.47 $451.4341 $378.19 $369.23 $387.89 $377.87 $431.42 $459.9142 $384.87 $375.76 $394.74 $384.54 $439.04 $468.0343 $394.17 $384.83 $404.28 $393.83 $449.64 $479.3344 $405.79 $396.18 $416.19 $405.44 $462.90 $493.4645 $419.44 $409.50 $430.20 $419.08 $478.47 $510.0646 $435.71 $425.39 $446.88 $435.33 $497.03 $529.8547 $454.00 $443.25 $465.65 $453.61 $517.90 $552.1048 $474.92 $463.67 $487.10 $474.51 $541.76 $577.5349 $495.54 $483.80 $508.25 $495.12 $565.28 $602.6150 $518.78 $506.49 $532.09 $518.33 $591.79 $630.8751 $541.73 $528.90 $555.62 $541.26 $617.97 $658.7752 $567.00 $553.57 $581.54 $566.51 $646.80 $689.5053 $592.56 $578.52 $607.76 $592.05 $675.95 $720.5954 $620.15 $605.46 $636.06 $619.62 $707.43 $754.1555 $647.75 $632.41 $664.36 $647.19 $738.91 $787.7056 $677.67 $661.62 $695.05 $677.08 $773.04 $824.0957 $707.88 $691.11 $726.03 $707.27 $807.50 $860.8258 $740.12 $722.59 $759.10 $739.48 $844.28 $900.0359 $756.09 $738.18 $775.49 $755.44 $862.50 $919.4660 $788.34 $769.66 $808.55 $787.66 $899.28 $958.6761 $816.22 $796.89 $837.16 $815.52 $931.09 $992.5862 $834.52 $814.75 $855.92 $833.80 $951.97 $1,014.8363 $857.47 $837.16 $879.46 $856.73 $978.15 $1,042.73
64+ $871.41 $850.77 $893.76 $870.66 $994.05 $1,059.69Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
SILVER PPO PLANS
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 1
Region 1 includes the counties of: Alpine, Amador, Butte, Calaveras, Colusa, Del Norte, Glenn, Humboldt, Lake, Lassen, Mendocino, Modoc, Nevada, Plumas, Shasta, Sierra, Siskiyou, Sutter, Tehama, Trinity, Tuolumne, and Yuba
Rates Effective 6/1/16 through 12/31/16
BRONZE PPO PLANS
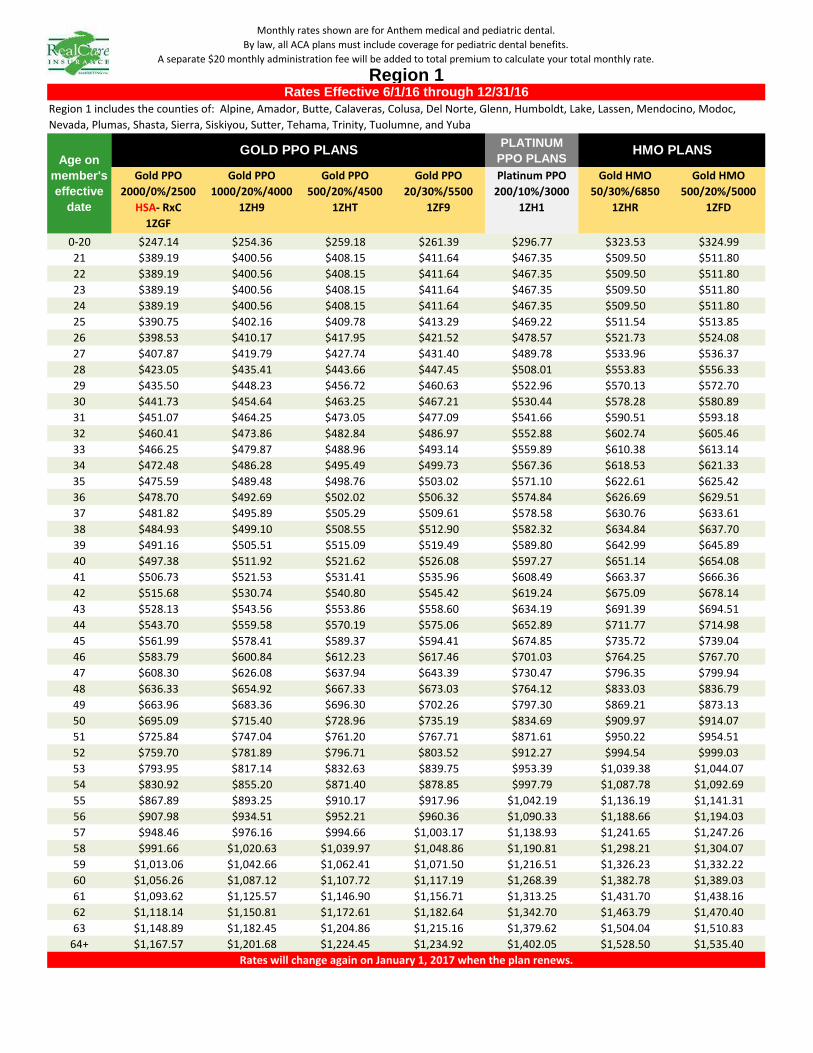
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $247.14 $254.36 $259.18 $261.39 $296.77 $323.53 $324.9921 $389.19 $400.56 $408.15 $411.64 $467.35 $509.50 $511.8022 $389.19 $400.56 $408.15 $411.64 $467.35 $509.50 $511.8023 $389.19 $400.56 $408.15 $411.64 $467.35 $509.50 $511.8024 $389.19 $400.56 $408.15 $411.64 $467.35 $509.50 $511.8025 $390.75 $402.16 $409.78 $413.29 $469.22 $511.54 $513.8526 $398.53 $410.17 $417.95 $421.52 $478.57 $521.73 $524.0827 $407.87 $419.79 $427.74 $431.40 $489.78 $533.96 $536.3728 $423.05 $435.41 $443.66 $447.45 $508.01 $553.83 $556.3329 $435.50 $448.23 $456.72 $460.63 $522.96 $570.13 $572.7030 $441.73 $454.64 $463.25 $467.21 $530.44 $578.28 $580.8931 $451.07 $464.25 $473.05 $477.09 $541.66 $590.51 $593.1832 $460.41 $473.86 $482.84 $486.97 $552.88 $602.74 $605.4633 $466.25 $479.87 $488.96 $493.14 $559.89 $610.38 $613.1434 $472.48 $486.28 $495.49 $499.73 $567.36 $618.53 $621.3335 $475.59 $489.48 $498.76 $503.02 $571.10 $622.61 $625.4236 $478.70 $492.69 $502.02 $506.32 $574.84 $626.69 $629.5137 $481.82 $495.89 $505.29 $509.61 $578.58 $630.76 $633.6138 $484.93 $499.10 $508.55 $512.90 $582.32 $634.84 $637.7039 $491.16 $505.51 $515.09 $519.49 $589.80 $642.99 $645.8940 $497.38 $511.92 $521.62 $526.08 $597.27 $651.14 $654.0841 $506.73 $521.53 $531.41 $535.96 $608.49 $663.37 $666.3642 $515.68 $530.74 $540.80 $545.42 $619.24 $675.09 $678.1443 $528.13 $543.56 $553.86 $558.60 $634.19 $691.39 $694.5144 $543.70 $559.58 $570.19 $575.06 $652.89 $711.77 $714.9845 $561.99 $578.41 $589.37 $594.41 $674.85 $735.72 $739.0446 $583.79 $600.84 $612.23 $617.46 $701.03 $764.25 $767.7047 $608.30 $626.08 $637.94 $643.39 $730.47 $796.35 $799.9448 $636.33 $654.92 $667.33 $673.03 $764.12 $833.03 $836.7949 $663.96 $683.36 $696.30 $702.26 $797.30 $869.21 $873.1350 $695.09 $715.40 $728.96 $735.19 $834.69 $909.97 $914.0751 $725.84 $747.04 $761.20 $767.71 $871.61 $950.22 $954.5152 $759.70 $781.89 $796.71 $803.52 $912.27 $994.54 $999.0353 $793.95 $817.14 $832.63 $839.75 $953.39 $1,039.38 $1,044.0754 $830.92 $855.20 $871.40 $878.85 $997.79 $1,087.78 $1,092.6955 $867.89 $893.25 $910.17 $917.96 $1,042.19 $1,136.19 $1,141.3156 $907.98 $934.51 $952.21 $960.36 $1,090.33 $1,188.66 $1,194.0357 $948.46 $976.16 $994.66 $1,003.17 $1,138.93 $1,241.65 $1,247.2658 $991.66 $1,020.63 $1,039.97 $1,048.86 $1,190.81 $1,298.21 $1,304.0759 $1,013.06 $1,042.66 $1,062.41 $1,071.50 $1,216.51 $1,326.23 $1,332.2260 $1,056.26 $1,087.12 $1,107.72 $1,117.19 $1,268.39 $1,382.78 $1,389.0361 $1,093.62 $1,125.57 $1,146.90 $1,156.71 $1,313.25 $1,431.70 $1,438.1662 $1,118.14 $1,150.81 $1,172.61 $1,182.64 $1,342.70 $1,463.79 $1,470.4063 $1,148.89 $1,182.45 $1,204.86 $1,215.16 $1,379.62 $1,504.04 $1,510.83
64+ $1,167.57 $1,201.68 $1,224.45 $1,234.92 $1,402.05 $1,528.50 $1,535.40Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
HMO PLANS
Monthly rates shown are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 1Rates Effective 6/1/16 through 12/31/16
Region 1 includes the counties of: Alpine, Amador, Butte, Calaveras, Colusa, Del Norte, Glenn, Humboldt, Lake, Lassen, Mendocino, Modoc, Nevada, Plumas, Shasta, Sierra, Siskiyou, Sutter, Tehama, Trinity, Tuolumne, and Yuba
GOLD PPO PLANS
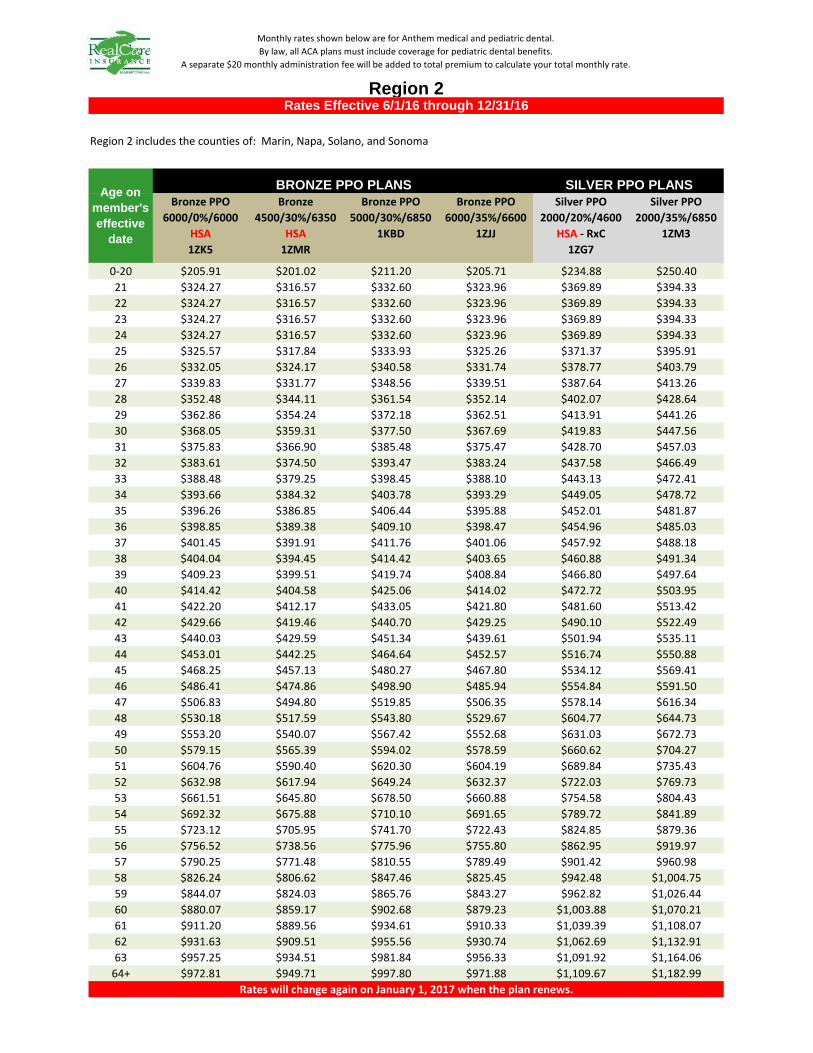
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $205.91 $201.02 $211.20 $205.71 $234.88 $250.4021 $324.27 $316.57 $332.60 $323.96 $369.89 $394.3322 $324.27 $316.57 $332.60 $323.96 $369.89 $394.3323 $324.27 $316.57 $332.60 $323.96 $369.89 $394.3324 $324.27 $316.57 $332.60 $323.96 $369.89 $394.3325 $325.57 $317.84 $333.93 $325.26 $371.37 $395.9126 $332.05 $324.17 $340.58 $331.74 $378.77 $403.7927 $339.83 $331.77 $348.56 $339.51 $387.64 $413.2628 $352.48 $344.11 $361.54 $352.14 $402.07 $428.6429 $362.86 $354.24 $372.18 $362.51 $413.91 $441.2630 $368.05 $359.31 $377.50 $367.69 $419.83 $447.5631 $375.83 $366.90 $385.48 $375.47 $428.70 $457.0332 $383.61 $374.50 $393.47 $383.24 $437.58 $466.4933 $388.48 $379.25 $398.45 $388.10 $443.13 $472.4134 $393.66 $384.32 $403.78 $393.29 $449.05 $478.7235 $396.26 $386.85 $406.44 $395.88 $452.01 $481.8736 $398.85 $389.38 $409.10 $398.47 $454.96 $485.0337 $401.45 $391.91 $411.76 $401.06 $457.92 $488.1838 $404.04 $394.45 $414.42 $403.65 $460.88 $491.3439 $409.23 $399.51 $419.74 $408.84 $466.80 $497.6440 $414.42 $404.58 $425.06 $414.02 $472.72 $503.9541 $422.20 $412.17 $433.05 $421.80 $481.60 $513.4242 $429.66 $419.46 $440.70 $429.25 $490.10 $522.4943 $440.03 $429.59 $451.34 $439.61 $501.94 $535.1144 $453.01 $442.25 $464.64 $452.57 $516.74 $550.8845 $468.25 $457.13 $480.27 $467.80 $534.12 $569.4146 $486.41 $474.86 $498.90 $485.94 $554.84 $591.5047 $506.83 $494.80 $519.85 $506.35 $578.14 $616.3448 $530.18 $517.59 $543.80 $529.67 $604.77 $644.7349 $553.20 $540.07 $567.42 $552.68 $631.03 $672.7350 $579.15 $565.39 $594.02 $578.59 $660.62 $704.2751 $604.76 $590.40 $620.30 $604.19 $689.84 $735.4352 $632.98 $617.94 $649.24 $632.37 $722.03 $769.7353 $661.51 $645.80 $678.50 $660.88 $754.58 $804.4354 $692.32 $675.88 $710.10 $691.65 $789.72 $841.8955 $723.12 $705.95 $741.70 $722.43 $824.85 $879.3656 $756.52 $738.56 $775.96 $755.80 $862.95 $919.9757 $790.25 $771.48 $810.55 $789.49 $901.42 $960.9858 $826.24 $806.62 $847.46 $825.45 $942.48 $1,004.7559 $844.07 $824.03 $865.76 $843.27 $962.82 $1,026.4460 $880.07 $859.17 $902.68 $879.23 $1,003.88 $1,070.2161 $911.20 $889.56 $934.61 $910.33 $1,039.39 $1,108.0762 $931.63 $909.51 $955.56 $930.74 $1,062.69 $1,132.9163 $957.25 $934.51 $981.84 $956.33 $1,091.92 $1,164.06
64+ $972.81 $949.71 $997.80 $971.88 $1,109.67 $1,182.99Rates will change again on January 1, 2017 when the plan renews.
SILVER PPO PLANS
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 2Rates Effective 6/1/16 through 12/31/16
Region 2 includes the counties of: Marin, Napa, Solano, and Sonoma
Age on member's effective
date
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $275.86 $283.93 $289.34 $291.80 $331.30 $356.59 $358.2021 $434.43 $447.14 $455.66 $459.53 $521.73 $561.56 $564.1022 $434.43 $447.14 $455.66 $459.53 $521.73 $561.56 $564.1023 $434.43 $447.14 $455.66 $459.53 $521.73 $561.56 $564.1024 $434.43 $447.14 $455.66 $459.53 $521.73 $561.56 $564.1025 $436.17 $448.93 $457.48 $461.37 $523.82 $563.81 $566.3626 $444.86 $457.87 $466.60 $470.56 $534.25 $575.04 $577.6427 $455.28 $468.60 $477.53 $481.59 $546.77 $588.51 $591.1828 $472.23 $486.04 $495.30 $499.51 $567.12 $610.42 $613.1829 $486.13 $500.35 $509.88 $514.21 $583.82 $628.39 $631.2330 $493.08 $507.50 $517.17 $521.57 $592.16 $637.37 $640.2531 $503.50 $518.24 $528.11 $532.60 $604.69 $650.85 $653.7932 $513.93 $528.97 $539.05 $543.62 $617.21 $664.33 $667.3333 $520.45 $535.67 $545.88 $550.52 $625.03 $672.75 $675.7934 $527.40 $542.83 $553.17 $557.87 $633.38 $681.73 $684.8235 $530.87 $546.41 $556.82 $561.55 $637.55 $686.23 $689.3336 $534.35 $549.98 $560.46 $565.22 $641.73 $690.72 $693.8437 $537.82 $553.56 $564.11 $568.90 $645.90 $695.21 $698.3638 $541.30 $557.14 $567.75 $572.57 $650.08 $699.70 $702.8739 $548.25 $564.29 $575.04 $579.93 $658.42 $708.69 $711.8940 $555.20 $571.44 $582.33 $587.28 $666.77 $717.67 $720.9241 $565.63 $582.18 $593.27 $598.31 $679.29 $731.15 $734.4642 $575.62 $592.46 $603.75 $608.88 $691.29 $744.07 $747.4343 $589.52 $606.77 $618.33 $623.58 $707.99 $762.04 $765.4844 $606.90 $624.65 $636.56 $641.96 $728.86 $784.50 $788.0545 $627.32 $645.67 $657.97 $663.56 $753.38 $810.89 $814.5646 $651.65 $670.71 $683.49 $689.30 $782.60 $842.34 $846.1547 $679.01 $698.88 $712.20 $718.25 $815.46 $877.72 $881.6948 $710.29 $731.07 $745.00 $751.33 $853.03 $918.15 $922.3049 $741.14 $762.82 $777.36 $783.96 $890.07 $958.02 $962.3550 $775.89 $798.59 $813.81 $820.72 $931.81 $1,002.95 $1,007.4851 $810.21 $833.92 $849.81 $857.02 $973.03 $1,047.31 $1,052.0552 $848.01 $872.82 $889.45 $897.00 $1,018.42 $1,096.17 $1,101.1253 $886.24 $912.17 $929.55 $937.44 $1,064.33 $1,145.58 $1,150.7654 $927.51 $954.64 $972.83 $981.10 $1,113.89 $1,198.93 $1,204.3555 $968.78 $997.12 $1,016.12 $1,024.75 $1,163.46 $1,252.28 $1,257.9456 $1,013.53 $1,043.18 $1,063.05 $1,072.08 $1,217.20 $1,310.12 $1,316.0557 $1,058.71 $1,089.68 $1,110.44 $1,119.87 $1,271.46 $1,368.52 $1,374.7158 $1,106.93 $1,139.31 $1,161.02 $1,170.88 $1,329.37 $1,430.85 $1,437.3359 $1,130.82 $1,163.91 $1,186.08 $1,196.16 $1,358.06 $1,461.74 $1,468.3560 $1,179.04 $1,213.54 $1,236.66 $1,247.16 $1,415.98 $1,524.07 $1,530.9761 $1,220.75 $1,256.46 $1,280.40 $1,291.28 $1,466.06 $1,577.98 $1,585.1262 $1,248.12 $1,284.63 $1,309.11 $1,320.23 $1,498.93 $1,613.36 $1,620.6663 $1,282.44 $1,319.96 $1,345.11 $1,356.53 $1,540.15 $1,657.73 $1,665.22
64+ $1,303.29 $1,341.42 $1,366.98 $1,378.59 $1,565.19 $1,684.68 $1,692.30Rates will change again on January 1, 2017 when the plan renews.
HMO PLANS
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 2Rates Effective 6/1/16 through 12/31/16
Region 2 includes the counties of: Marin, Napa, Solano, and Sonoma
GOLD PPO PLANSAge on
member's effective
date
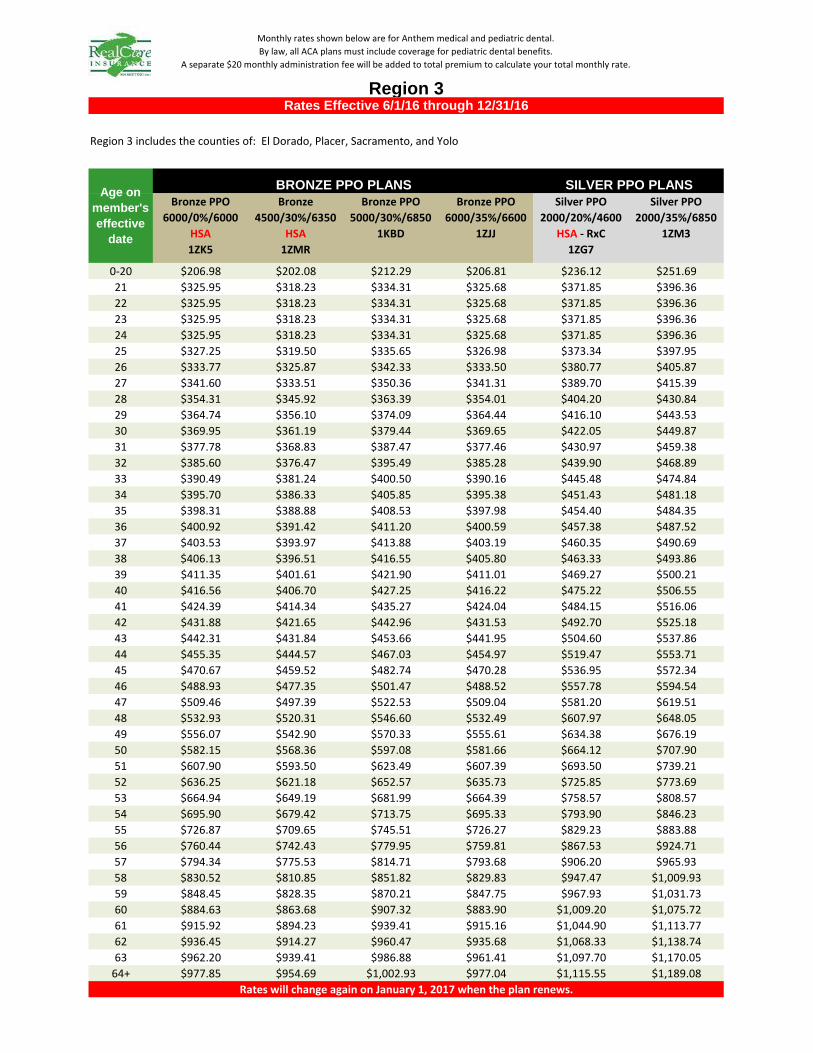
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $206.98 $202.08 $212.29 $206.81 $236.12 $251.6921 $325.95 $318.23 $334.31 $325.68 $371.85 $396.3622 $325.95 $318.23 $334.31 $325.68 $371.85 $396.3623 $325.95 $318.23 $334.31 $325.68 $371.85 $396.3624 $325.95 $318.23 $334.31 $325.68 $371.85 $396.3625 $327.25 $319.50 $335.65 $326.98 $373.34 $397.9526 $333.77 $325.87 $342.33 $333.50 $380.77 $405.8727 $341.60 $333.51 $350.36 $341.31 $389.70 $415.3928 $354.31 $345.92 $363.39 $354.01 $404.20 $430.8429 $364.74 $356.10 $374.09 $364.44 $416.10 $443.5330 $369.95 $361.19 $379.44 $369.65 $422.05 $449.8731 $377.78 $368.83 $387.47 $377.46 $430.97 $459.3832 $385.60 $376.47 $395.49 $385.28 $439.90 $468.8933 $390.49 $381.24 $400.50 $390.16 $445.48 $474.8434 $395.70 $386.33 $405.85 $395.38 $451.43 $481.1835 $398.31 $388.88 $408.53 $397.98 $454.40 $484.3536 $400.92 $391.42 $411.20 $400.59 $457.38 $487.5237 $403.53 $393.97 $413.88 $403.19 $460.35 $490.6938 $406.13 $396.51 $416.55 $405.80 $463.33 $493.8639 $411.35 $401.61 $421.90 $411.01 $469.27 $500.2140 $416.56 $406.70 $427.25 $416.22 $475.22 $506.5541 $424.39 $414.34 $435.27 $424.04 $484.15 $516.0642 $431.88 $421.65 $442.96 $431.53 $492.70 $525.1843 $442.31 $431.84 $453.66 $441.95 $504.60 $537.8644 $455.35 $444.57 $467.03 $454.97 $519.47 $553.7145 $470.67 $459.52 $482.74 $470.28 $536.95 $572.3446 $488.93 $477.35 $501.47 $488.52 $557.78 $594.5447 $509.46 $497.39 $522.53 $509.04 $581.20 $619.5148 $532.93 $520.31 $546.60 $532.49 $607.97 $648.0549 $556.07 $542.90 $570.33 $555.61 $634.38 $676.1950 $582.15 $568.36 $597.08 $581.66 $664.12 $707.9051 $607.90 $593.50 $623.49 $607.39 $693.50 $739.2152 $636.25 $621.18 $652.57 $635.73 $725.85 $773.6953 $664.94 $649.19 $681.99 $664.39 $758.57 $808.5754 $695.90 $679.42 $713.75 $695.33 $793.90 $846.2355 $726.87 $709.65 $745.51 $726.27 $829.23 $883.8856 $760.44 $742.43 $779.95 $759.81 $867.53 $924.7157 $794.34 $775.53 $814.71 $793.68 $906.20 $965.9358 $830.52 $810.85 $851.82 $829.83 $947.47 $1,009.9359 $848.45 $828.35 $870.21 $847.75 $967.93 $1,031.7360 $884.63 $863.68 $907.32 $883.90 $1,009.20 $1,075.7261 $915.92 $894.23 $939.41 $915.16 $1,044.90 $1,113.7762 $936.45 $914.27 $960.47 $935.68 $1,068.33 $1,138.7463 $962.20 $939.41 $986.88 $961.41 $1,097.70 $1,170.05
64+ $977.85 $954.69 $1,002.93 $977.04 $1,115.55 $1,189.08Rates will change again on January 1, 2017 when the plan renews.
SILVER PPO PLANS
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 3Rates Effective 6/1/16 through 12/31/16
Region 3 includes the counties of: El Dorado, Placer, Sacramento, and Yolo
Age on member's effective
date
BRONZE PPO PLANS
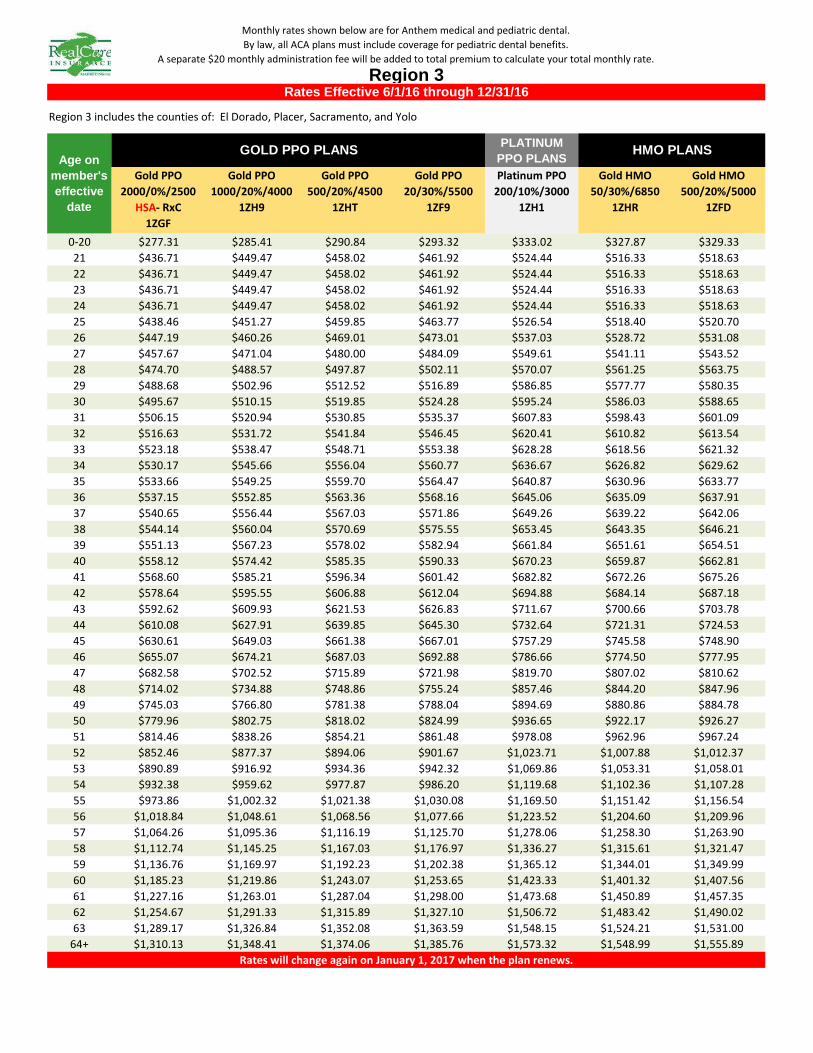
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $277.31 $285.41 $290.84 $293.32 $333.02 $327.87 $329.3321 $436.71 $449.47 $458.02 $461.92 $524.44 $516.33 $518.6322 $436.71 $449.47 $458.02 $461.92 $524.44 $516.33 $518.6323 $436.71 $449.47 $458.02 $461.92 $524.44 $516.33 $518.6324 $436.71 $449.47 $458.02 $461.92 $524.44 $516.33 $518.6325 $438.46 $451.27 $459.85 $463.77 $526.54 $518.40 $520.7026 $447.19 $460.26 $469.01 $473.01 $537.03 $528.72 $531.0827 $457.67 $471.04 $480.00 $484.09 $549.61 $541.11 $543.5228 $474.70 $488.57 $497.87 $502.11 $570.07 $561.25 $563.7529 $488.68 $502.96 $512.52 $516.89 $586.85 $577.77 $580.3530 $495.67 $510.15 $519.85 $524.28 $595.24 $586.03 $588.6531 $506.15 $520.94 $530.85 $535.37 $607.83 $598.43 $601.0932 $516.63 $531.72 $541.84 $546.45 $620.41 $610.82 $613.5433 $523.18 $538.47 $548.71 $553.38 $628.28 $618.56 $621.3234 $530.17 $545.66 $556.04 $560.77 $636.67 $626.82 $629.6235 $533.66 $549.25 $559.70 $564.47 $640.87 $630.96 $633.7736 $537.15 $552.85 $563.36 $568.16 $645.06 $635.09 $637.9137 $540.65 $556.44 $567.03 $571.86 $649.26 $639.22 $642.0638 $544.14 $560.04 $570.69 $575.55 $653.45 $643.35 $646.2139 $551.13 $567.23 $578.02 $582.94 $661.84 $651.61 $654.5140 $558.12 $574.42 $585.35 $590.33 $670.23 $659.87 $662.8141 $568.60 $585.21 $596.34 $601.42 $682.82 $672.26 $675.2642 $578.64 $595.55 $606.88 $612.04 $694.88 $684.14 $687.1843 $592.62 $609.93 $621.53 $626.83 $711.67 $700.66 $703.7844 $610.08 $627.91 $639.85 $645.30 $732.64 $721.31 $724.5345 $630.61 $649.03 $661.38 $667.01 $757.29 $745.58 $748.9046 $655.07 $674.21 $687.03 $692.88 $786.66 $774.50 $777.9547 $682.58 $702.52 $715.89 $721.98 $819.70 $807.02 $810.6248 $714.02 $734.88 $748.86 $755.24 $857.46 $844.20 $847.9649 $745.03 $766.80 $781.38 $788.04 $894.69 $880.86 $884.7850 $779.96 $802.75 $818.02 $824.99 $936.65 $922.17 $926.2751 $814.46 $838.26 $854.21 $861.48 $978.08 $962.96 $967.2452 $852.46 $877.37 $894.06 $901.67 $1,023.71 $1,007.88 $1,012.3753 $890.89 $916.92 $934.36 $942.32 $1,069.86 $1,053.31 $1,058.0154 $932.38 $959.62 $977.87 $986.20 $1,119.68 $1,102.36 $1,107.2855 $973.86 $1,002.32 $1,021.38 $1,030.08 $1,169.50 $1,151.42 $1,156.5456 $1,018.84 $1,048.61 $1,068.56 $1,077.66 $1,223.52 $1,204.60 $1,209.9657 $1,064.26 $1,095.36 $1,116.19 $1,125.70 $1,278.06 $1,258.30 $1,263.9058 $1,112.74 $1,145.25 $1,167.03 $1,176.97 $1,336.27 $1,315.61 $1,321.4759 $1,136.76 $1,169.97 $1,192.23 $1,202.38 $1,365.12 $1,344.01 $1,349.9960 $1,185.23 $1,219.86 $1,243.07 $1,253.65 $1,423.33 $1,401.32 $1,407.5661 $1,227.16 $1,263.01 $1,287.04 $1,298.00 $1,473.68 $1,450.89 $1,457.3562 $1,254.67 $1,291.33 $1,315.89 $1,327.10 $1,506.72 $1,483.42 $1,490.0263 $1,289.17 $1,326.84 $1,352.08 $1,363.59 $1,548.15 $1,524.21 $1,531.00
64+ $1,310.13 $1,348.41 $1,374.06 $1,385.76 $1,573.32 $1,548.99 $1,555.89
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 3
Region 3 includes the counties of: El Dorado, Placer, Sacramento, and Yolo
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $213.45 $208.36 $218.91 $213.25 $243.46 $259.5321 $336.14 $328.13 $344.74 $335.82 $383.40 $408.7122 $336.14 $328.13 $344.74 $335.82 $383.40 $408.7123 $336.14 $328.13 $344.74 $335.82 $383.40 $408.7124 $336.14 $328.13 $344.74 $335.82 $383.40 $408.7125 $337.48 $329.44 $346.12 $337.16 $384.93 $410.3426 $344.21 $336.01 $353.01 $343.88 $392.60 $418.5227 $352.27 $343.88 $361.29 $351.94 $401.80 $428.3328 $365.38 $356.68 $374.73 $365.04 $416.76 $444.2729 $376.14 $367.18 $385.76 $375.78 $429.02 $457.3530 $381.52 $372.43 $391.28 $381.16 $435.16 $463.8931 $389.59 $380.30 $399.55 $389.22 $444.36 $473.6932 $397.65 $388.18 $407.83 $397.28 $453.56 $483.5033 $402.70 $393.10 $413.00 $402.31 $459.31 $489.6334 $408.07 $398.35 $418.51 $407.69 $465.45 $496.1735 $410.76 $400.97 $421.27 $410.37 $468.51 $499.4436 $413.45 $403.60 $424.03 $413.06 $471.58 $502.7137 $416.14 $406.22 $426.79 $415.75 $474.65 $505.9838 $418.83 $408.85 $429.55 $418.43 $477.72 $509.2539 $424.21 $414.10 $435.06 $423.80 $483.85 $515.7940 $429.59 $419.35 $440.58 $429.18 $489.99 $522.3341 $437.65 $427.23 $448.85 $437.24 $499.19 $532.1442 $445.39 $434.77 $456.78 $444.96 $508.01 $541.5443 $456.14 $445.27 $467.81 $455.71 $520.27 $554.6244 $469.59 $458.40 $481.60 $469.14 $535.61 $570.9745 $485.39 $473.82 $497.80 $484.92 $553.63 $590.1846 $504.21 $492.20 $517.11 $503.73 $575.10 $613.0747 $525.39 $512.87 $538.83 $524.89 $599.25 $638.8148 $549.59 $536.49 $563.65 $549.07 $626.86 $668.2449 $573.45 $559.79 $588.13 $572.91 $654.08 $697.2650 $600.35 $586.04 $615.71 $599.77 $684.75 $729.9651 $626.90 $611.96 $642.94 $626.30 $715.04 $762.2452 $656.15 $640.51 $672.93 $655.52 $748.40 $797.8053 $685.73 $669.39 $703.27 $685.07 $782.14 $833.7754 $717.66 $700.56 $736.02 $716.98 $818.56 $872.6055 $749.59 $731.73 $768.77 $748.88 $854.98 $911.4256 $784.21 $765.53 $804.28 $783.47 $894.47 $953.5257 $819.17 $799.65 $840.13 $818.39 $934.35 $996.0358 $856.48 $836.08 $878.40 $855.67 $976.90 $1,041.3959 $874.97 $854.12 $897.36 $874.14 $997.99 $1,063.8760 $912.28 $890.54 $935.62 $911.42 $1,040.55 $1,109.2461 $944.55 $922.05 $968.72 $943.65 $1,077.35 $1,148.4862 $965.73 $942.72 $990.44 $964.81 $1,101.51 $1,174.2263 $992.29 $968.64 $1,017.67 $991.34 $1,131.80 $1,206.51
64+ $1,008.42 $984.39 $1,034.22 $1,007.46 $1,150.20 $1,226.13
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 4
Region 4 includes the county of: San Francisco
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $285.94 $294.28 $299.89 $302.44 $343.36 $320.37 $321.8221 $450.30 $463.43 $472.26 $476.29 $540.72 $504.52 $506.8122 $450.30 $463.43 $472.26 $476.29 $540.72 $504.52 $506.8123 $450.30 $463.43 $472.26 $476.29 $540.72 $504.52 $506.8124 $450.30 $463.43 $472.26 $476.29 $540.72 $504.52 $506.8125 $452.10 $465.28 $474.15 $478.20 $542.88 $506.54 $508.8426 $461.11 $474.55 $483.59 $487.72 $553.70 $516.63 $518.9727 $471.91 $485.67 $494.93 $499.15 $566.67 $528.74 $531.1428 $489.48 $503.75 $513.35 $517.73 $587.76 $548.41 $550.9029 $503.89 $518.58 $528.46 $532.97 $605.07 $564.56 $567.1230 $511.09 $525.99 $536.02 $540.59 $613.72 $572.63 $575.2331 $521.90 $537.12 $547.35 $552.02 $626.69 $584.74 $587.3932 $532.70 $548.24 $558.68 $563.45 $639.67 $596.85 $599.5633 $539.46 $555.19 $565.77 $570.60 $647.78 $604.41 $607.1634 $546.66 $562.60 $573.32 $578.22 $656.43 $612.49 $615.2735 $550.27 $566.31 $577.10 $582.03 $660.76 $616.52 $619.3236 $553.87 $570.02 $580.88 $585.84 $665.09 $620.56 $623.3837 $557.47 $573.73 $584.66 $589.65 $669.41 $624.60 $627.4338 $561.07 $577.43 $588.44 $593.46 $673.74 $628.63 $631.4939 $568.28 $584.85 $595.99 $601.08 $682.39 $636.70 $639.5940 $575.48 $592.26 $603.55 $608.70 $691.04 $644.78 $647.7041 $586.29 $603.39 $614.88 $620.13 $704.02 $656.89 $659.8742 $596.65 $614.04 $625.74 $631.08 $716.45 $668.49 $671.5243 $611.06 $628.87 $640.86 $646.33 $733.76 $684.63 $687.7444 $629.07 $647.41 $659.75 $665.38 $755.39 $704.81 $708.0145 $650.23 $669.19 $681.94 $687.76 $780.80 $728.53 $731.8346 $675.45 $695.15 $708.39 $714.44 $811.08 $756.78 $760.2247 $703.82 $724.34 $738.14 $744.44 $845.15 $788.56 $792.1448 $736.24 $757.71 $772.15 $778.73 $884.08 $824.89 $828.6349 $768.21 $790.61 $805.68 $812.55 $922.47 $860.71 $864.6250 $804.24 $827.69 $843.46 $850.65 $965.73 $901.07 $905.1651 $839.81 $864.30 $880.76 $888.28 $1,008.44 $940.93 $945.2052 $878.99 $904.62 $921.85 $929.72 $1,055.49 $984.82 $989.2953 $918.61 $945.40 $963.41 $971.63 $1,103.07 $1,029.22 $1,033.8954 $961.39 $989.42 $1,008.28 $1,016.88 $1,154.44 $1,077.15 $1,082.0455 $1,004.17 $1,033.45 $1,053.14 $1,062.13 $1,205.81 $1,125.08 $1,130.1956 $1,050.55 $1,081.18 $1,101.78 $1,111.18 $1,261.50 $1,177.05 $1,182.3957 $1,097.38 $1,129.38 $1,150.90 $1,160.72 $1,317.73 $1,229.52 $1,235.1058 $1,147.36 $1,180.82 $1,203.32 $1,213.59 $1,377.75 $1,285.52 $1,291.3559 $1,172.13 $1,206.31 $1,229.29 $1,239.78 $1,407.49 $1,313.27 $1,319.2360 $1,222.11 $1,257.75 $1,281.71 $1,292.65 $1,467.51 $1,369.27 $1,375.4861 $1,265.34 $1,302.24 $1,327.05 $1,338.37 $1,519.42 $1,417.70 $1,424.1462 $1,293.71 $1,331.43 $1,356.80 $1,368.38 $1,553.49 $1,449.49 $1,456.0763 $1,329.29 $1,368.05 $1,394.11 $1,406.01 $1,596.21 $1,489.34 $1,496.10
64+ $1,350.90 $1,390.29 $1,416.78 $1,428.87 $1,622.16 $1,513.56 $1,520.43
HMO PLANS
Rates will change again on January 1, 2017 when the plan renews.
Rates Effective 6/1/16 through 12/31/16
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 4
Region 4 includes the county of: San Francisco
Age on member's effective
date
GOLD PPO PLANS
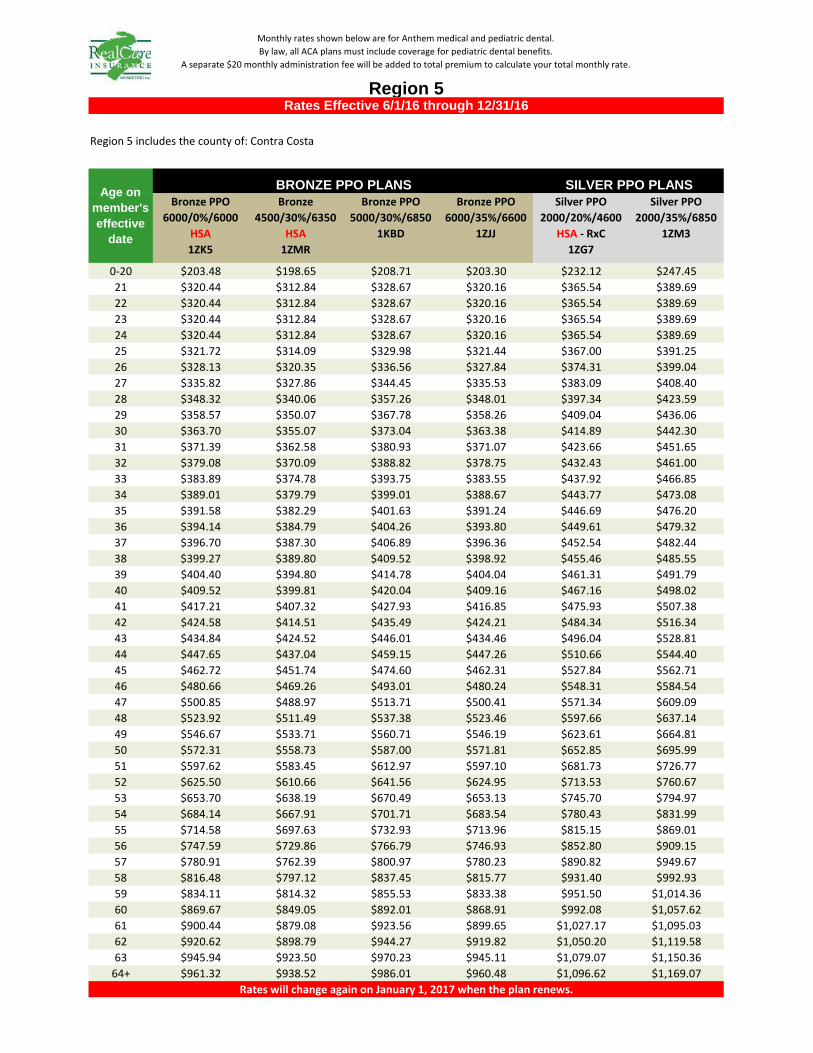
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $203.48 $198.65 $208.71 $203.30 $232.12 $247.4521 $320.44 $312.84 $328.67 $320.16 $365.54 $389.6922 $320.44 $312.84 $328.67 $320.16 $365.54 $389.6923 $320.44 $312.84 $328.67 $320.16 $365.54 $389.6924 $320.44 $312.84 $328.67 $320.16 $365.54 $389.6925 $321.72 $314.09 $329.98 $321.44 $367.00 $391.2526 $328.13 $320.35 $336.56 $327.84 $374.31 $399.0427 $335.82 $327.86 $344.45 $335.53 $383.09 $408.4028 $348.32 $340.06 $357.26 $348.01 $397.34 $423.5929 $358.57 $350.07 $367.78 $358.26 $409.04 $436.0630 $363.70 $355.07 $373.04 $363.38 $414.89 $442.3031 $371.39 $362.58 $380.93 $371.07 $423.66 $451.6532 $379.08 $370.09 $388.82 $378.75 $432.43 $461.0033 $383.89 $374.78 $393.75 $383.55 $437.92 $466.8534 $389.01 $379.79 $399.01 $388.67 $443.77 $473.0835 $391.58 $382.29 $401.63 $391.24 $446.69 $476.2036 $394.14 $384.79 $404.26 $393.80 $449.61 $479.3237 $396.70 $387.30 $406.89 $396.36 $452.54 $482.4438 $399.27 $389.80 $409.52 $398.92 $455.46 $485.5539 $404.40 $394.80 $414.78 $404.04 $461.31 $491.7940 $409.52 $399.81 $420.04 $409.16 $467.16 $498.0241 $417.21 $407.32 $427.93 $416.85 $475.93 $507.3842 $424.58 $414.51 $435.49 $424.21 $484.34 $516.3443 $434.84 $424.52 $446.01 $434.46 $496.04 $528.8144 $447.65 $437.04 $459.15 $447.26 $510.66 $544.4045 $462.72 $451.74 $474.60 $462.31 $527.84 $562.7146 $480.66 $469.26 $493.01 $480.24 $548.31 $584.5447 $500.85 $488.97 $513.71 $500.41 $571.34 $609.0948 $523.92 $511.49 $537.38 $523.46 $597.66 $637.1449 $546.67 $533.71 $560.71 $546.19 $623.61 $664.8150 $572.31 $558.73 $587.00 $571.81 $652.85 $695.9951 $597.62 $583.45 $612.97 $597.10 $681.73 $726.7752 $625.50 $610.66 $641.56 $624.95 $713.53 $760.6753 $653.70 $638.19 $670.49 $653.13 $745.70 $794.9754 $684.14 $667.91 $701.71 $683.54 $780.43 $831.9955 $714.58 $697.63 $732.93 $713.96 $815.15 $869.0156 $747.59 $729.86 $766.79 $746.93 $852.80 $909.1557 $780.91 $762.39 $800.97 $780.23 $890.82 $949.6758 $816.48 $797.12 $837.45 $815.77 $931.40 $992.9359 $834.11 $814.32 $855.53 $833.38 $951.50 $1,014.3660 $869.67 $849.05 $892.01 $868.91 $992.08 $1,057.6261 $900.44 $879.08 $923.56 $899.65 $1,027.17 $1,095.0362 $920.62 $898.79 $944.27 $919.82 $1,050.20 $1,119.5863 $945.94 $923.50 $970.23 $945.11 $1,079.07 $1,150.36
64+ $961.32 $938.52 $986.01 $960.48 $1,096.62 $1,169.07
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 5
Region 5 includes the county of: Contra Costa
BRONZE PPO PLANS
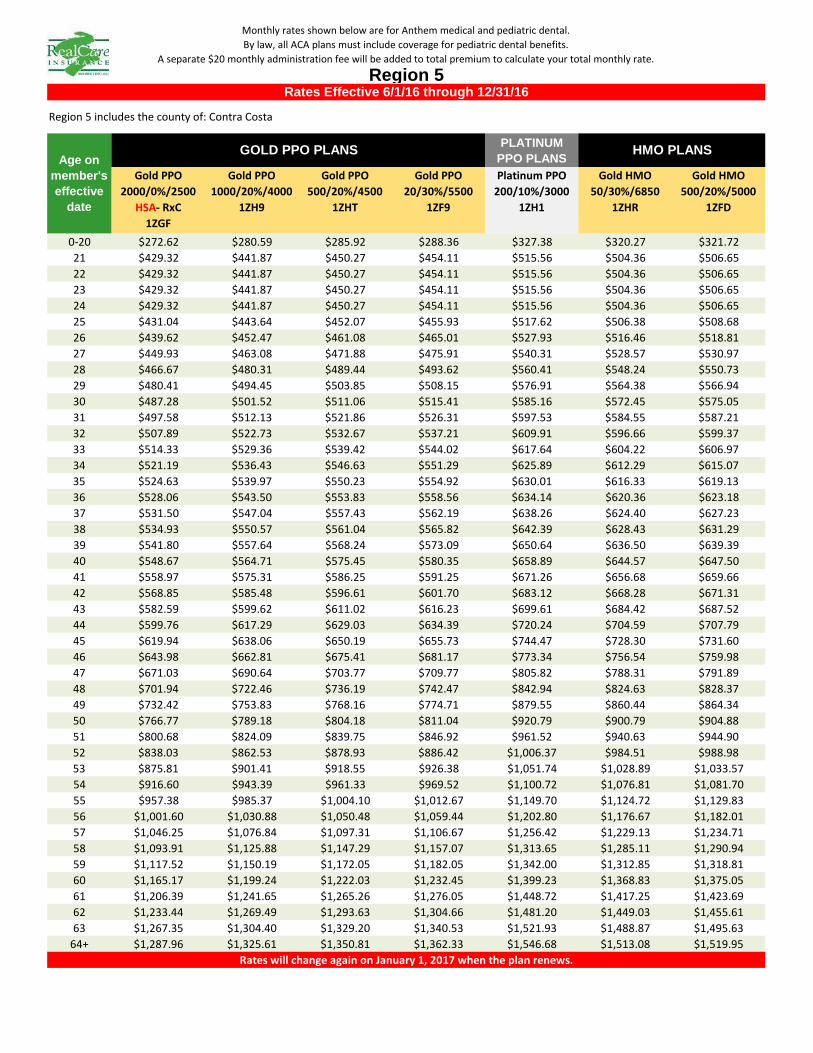
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $272.62 $280.59 $285.92 $288.36 $327.38 $320.27 $321.7221 $429.32 $441.87 $450.27 $454.11 $515.56 $504.36 $506.6522 $429.32 $441.87 $450.27 $454.11 $515.56 $504.36 $506.6523 $429.32 $441.87 $450.27 $454.11 $515.56 $504.36 $506.6524 $429.32 $441.87 $450.27 $454.11 $515.56 $504.36 $506.6525 $431.04 $443.64 $452.07 $455.93 $517.62 $506.38 $508.6826 $439.62 $452.47 $461.08 $465.01 $527.93 $516.46 $518.8127 $449.93 $463.08 $471.88 $475.91 $540.31 $528.57 $530.9728 $466.67 $480.31 $489.44 $493.62 $560.41 $548.24 $550.7329 $480.41 $494.45 $503.85 $508.15 $576.91 $564.38 $566.9430 $487.28 $501.52 $511.06 $515.41 $585.16 $572.45 $575.0531 $497.58 $512.13 $521.86 $526.31 $597.53 $584.55 $587.2132 $507.89 $522.73 $532.67 $537.21 $609.91 $596.66 $599.3733 $514.33 $529.36 $539.42 $544.02 $617.64 $604.22 $606.9734 $521.19 $536.43 $546.63 $551.29 $625.89 $612.29 $615.0735 $524.63 $539.97 $550.23 $554.92 $630.01 $616.33 $619.1336 $528.06 $543.50 $553.83 $558.56 $634.14 $620.36 $623.1837 $531.50 $547.04 $557.43 $562.19 $638.26 $624.40 $627.2338 $534.93 $550.57 $561.04 $565.82 $642.39 $628.43 $631.2939 $541.80 $557.64 $568.24 $573.09 $650.64 $636.50 $639.3940 $548.67 $564.71 $575.45 $580.35 $658.89 $644.57 $647.5041 $558.97 $575.31 $586.25 $591.25 $671.26 $656.68 $659.6642 $568.85 $585.48 $596.61 $601.70 $683.12 $668.28 $671.3143 $582.59 $599.62 $611.02 $616.23 $699.61 $684.42 $687.5244 $599.76 $617.29 $629.03 $634.39 $720.24 $704.59 $707.7945 $619.94 $638.06 $650.19 $655.73 $744.47 $728.30 $731.6046 $643.98 $662.81 $675.41 $681.17 $773.34 $756.54 $759.9847 $671.03 $690.64 $703.77 $709.77 $805.82 $788.31 $791.8948 $701.94 $722.46 $736.19 $742.47 $842.94 $824.63 $828.3749 $732.42 $753.83 $768.16 $774.71 $879.55 $860.44 $864.3450 $766.77 $789.18 $804.18 $811.04 $920.79 $900.79 $904.8851 $800.68 $824.09 $839.75 $846.92 $961.52 $940.63 $944.9052 $838.03 $862.53 $878.93 $886.42 $1,006.37 $984.51 $988.9853 $875.81 $901.41 $918.55 $926.38 $1,051.74 $1,028.89 $1,033.5754 $916.60 $943.39 $961.33 $969.52 $1,100.72 $1,076.81 $1,081.7055 $957.38 $985.37 $1,004.10 $1,012.67 $1,149.70 $1,124.72 $1,129.8356 $1,001.60 $1,030.88 $1,050.48 $1,059.44 $1,202.80 $1,176.67 $1,182.0157 $1,046.25 $1,076.84 $1,097.31 $1,106.67 $1,256.42 $1,229.13 $1,234.7158 $1,093.91 $1,125.88 $1,147.29 $1,157.07 $1,313.65 $1,285.11 $1,290.9459 $1,117.52 $1,150.19 $1,172.05 $1,182.05 $1,342.00 $1,312.85 $1,318.8160 $1,165.17 $1,199.24 $1,222.03 $1,232.45 $1,399.23 $1,368.83 $1,375.0561 $1,206.39 $1,241.65 $1,265.26 $1,276.05 $1,448.72 $1,417.25 $1,423.6962 $1,233.44 $1,269.49 $1,293.63 $1,304.66 $1,481.20 $1,449.03 $1,455.6163 $1,267.35 $1,304.40 $1,329.20 $1,340.53 $1,521.93 $1,488.87 $1,495.63
64+ $1,287.96 $1,325.61 $1,350.81 $1,362.33 $1,546.68 $1,513.08 $1,519.95
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 5
Region 5 includes the county of: Contra Costa
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $214.34 $209.25 $219.82 $214.13 $244.49 $260.6321 $337.54 $329.53 $346.17 $337.22 $385.02 $410.4422 $337.54 $329.53 $346.17 $337.22 $385.02 $410.4423 $337.54 $329.53 $346.17 $337.22 $385.02 $410.4424 $337.54 $329.53 $346.17 $337.22 $385.02 $410.4425 $338.89 $330.85 $347.55 $338.57 $386.56 $412.0826 $345.64 $337.44 $354.48 $345.31 $394.26 $420.2927 $353.74 $345.35 $362.79 $353.41 $403.50 $430.1428 $366.91 $358.20 $376.29 $366.56 $418.52 $446.1529 $377.71 $368.74 $387.36 $377.35 $430.84 $459.2830 $383.11 $374.02 $392.90 $382.74 $437.00 $465.8531 $391.21 $381.93 $401.21 $390.84 $446.24 $475.7032 $399.31 $389.83 $409.52 $398.93 $455.48 $485.5533 $404.37 $394.78 $414.71 $403.99 $461.25 $491.7134 $409.77 $400.05 $420.25 $409.39 $467.41 $498.2735 $412.47 $402.69 $423.02 $412.08 $470.49 $501.5636 $415.17 $405.32 $425.79 $414.78 $473.57 $504.8437 $417.87 $407.96 $428.56 $417.48 $476.65 $508.1238 $420.57 $410.59 $431.33 $420.18 $479.73 $511.4139 $425.98 $415.87 $436.87 $425.57 $485.90 $517.9840 $431.38 $421.14 $442.41 $430.97 $492.06 $524.5441 $439.48 $429.05 $450.71 $439.06 $501.30 $534.3942 $447.24 $436.63 $458.68 $446.82 $510.15 $543.8343 $458.04 $447.17 $469.75 $457.61 $522.47 $556.9744 $471.54 $460.35 $483.60 $471.10 $537.87 $573.3845 $487.41 $475.84 $499.87 $486.95 $555.97 $592.6846 $506.31 $494.30 $519.26 $505.83 $577.53 $615.6647 $527.58 $515.06 $541.06 $527.07 $601.79 $641.5248 $551.88 $538.78 $565.99 $551.35 $629.51 $671.0749 $575.84 $562.18 $590.57 $575.30 $656.84 $700.2150 $602.85 $588.54 $618.26 $602.27 $687.65 $733.0551 $629.51 $614.57 $645.61 $628.92 $718.06 $765.4752 $658.88 $643.24 $675.72 $658.25 $751.56 $801.1853 $688.58 $672.24 $706.19 $687.93 $785.44 $837.3054 $720.65 $703.55 $739.07 $719.96 $822.02 $876.2955 $752.71 $734.85 $771.96 $752.00 $858.59 $915.2856 $787.48 $768.79 $807.61 $786.73 $898.25 $957.5657 $822.58 $803.06 $843.62 $821.81 $938.29 $1,000.2458 $860.05 $839.64 $882.04 $859.24 $981.03 $1,045.8059 $878.62 $857.77 $901.08 $877.78 $1,002.21 $1,068.3860 $916.08 $894.34 $939.51 $915.22 $1,044.94 $1,113.9361 $948.49 $925.98 $972.74 $947.59 $1,081.91 $1,153.3462 $969.75 $946.74 $994.55 $968.83 $1,106.16 $1,179.1963 $996.42 $972.77 $1,021.89 $995.47 $1,136.58 $1,211.62
64+ $1,012.62 $988.59 $1,038.51 $1,011.66 $1,155.06 $1,231.32
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 6
Region 6 includes the couny of: Alameda
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $287.17 $295.54 $301.16 $303.75 $344.85 $320.31 $321.7321 $452.23 $465.41 $474.27 $478.34 $543.07 $504.42 $506.6622 $452.23 $465.41 $474.27 $478.34 $543.07 $504.42 $506.6623 $452.23 $465.41 $474.27 $478.34 $543.07 $504.42 $506.6624 $452.23 $465.41 $474.27 $478.34 $543.07 $504.42 $506.6625 $454.04 $467.27 $476.17 $480.25 $545.24 $506.44 $508.6926 $463.08 $476.58 $485.65 $489.82 $556.10 $516.53 $518.8227 $473.94 $487.75 $497.03 $501.30 $569.14 $528.63 $530.9828 $491.57 $505.90 $515.53 $519.96 $590.32 $548.30 $550.7429 $506.05 $520.79 $530.71 $535.26 $607.70 $564.45 $566.9530 $513.28 $528.24 $538.30 $542.92 $616.38 $572.52 $575.0631 $524.13 $539.41 $549.68 $554.40 $629.42 $584.62 $587.2232 $534.99 $550.58 $561.06 $565.88 $642.45 $596.73 $599.3833 $541.77 $557.56 $568.18 $573.05 $650.60 $604.30 $606.9834 $549.01 $565.01 $575.76 $580.70 $659.29 $612.37 $615.0935 $552.63 $568.73 $579.56 $584.53 $663.63 $616.40 $619.1436 $556.24 $572.45 $583.35 $588.36 $667.98 $620.44 $623.1937 $559.86 $576.18 $587.15 $592.18 $672.32 $624.47 $627.2538 $563.48 $579.90 $590.94 $596.01 $676.67 $628.51 $631.3039 $570.71 $587.35 $598.53 $603.67 $685.35 $636.58 $639.4040 $577.95 $594.79 $606.12 $611.32 $694.04 $644.65 $647.5141 $588.80 $605.96 $617.50 $622.80 $707.08 $656.75 $659.6742 $599.20 $616.67 $628.41 $633.80 $719.57 $668.36 $671.3243 $613.68 $631.56 $643.58 $649.11 $736.95 $684.50 $687.5444 $631.77 $650.18 $662.56 $668.24 $758.67 $704.67 $707.8045 $653.02 $672.05 $684.85 $690.72 $784.19 $728.38 $731.6246 $678.35 $698.12 $711.41 $717.51 $814.61 $756.63 $759.9947 $706.84 $727.44 $741.28 $747.65 $848.82 $788.41 $791.9148 $739.40 $760.95 $775.43 $782.09 $887.92 $824.73 $828.3949 $771.50 $793.99 $809.10 $816.05 $926.48 $860.54 $864.3650 $807.68 $831.22 $847.05 $854.32 $969.92 $900.89 $904.8951 $843.41 $867.99 $884.51 $892.10 $1,012.83 $940.74 $944.9252 $882.75 $908.48 $925.78 $933.72 $1,060.07 $984.63 $989.0053 $922.55 $949.44 $967.51 $975.81 $1,107.86 $1,029.02 $1,033.5954 $965.51 $993.65 $1,012.57 $1,021.26 $1,159.45 $1,076.94 $1,081.7255 $1,008.47 $1,037.86 $1,057.62 $1,066.70 $1,211.05 $1,124.86 $1,129.8556 $1,055.05 $1,085.80 $1,106.47 $1,115.97 $1,266.98 $1,176.81 $1,182.0457 $1,102.08 $1,134.20 $1,155.80 $1,165.71 $1,323.46 $1,229.27 $1,234.7358 $1,152.28 $1,185.86 $1,208.44 $1,218.81 $1,383.74 $1,285.26 $1,290.9759 $1,177.15 $1,211.46 $1,234.52 $1,245.12 $1,413.61 $1,313.01 $1,318.8460 $1,227.35 $1,263.12 $1,287.17 $1,298.21 $1,473.89 $1,369.00 $1,375.0861 $1,270.77 $1,307.80 $1,332.70 $1,344.14 $1,526.03 $1,417.42 $1,423.7162 $1,299.26 $1,337.12 $1,362.58 $1,374.27 $1,560.24 $1,449.20 $1,455.6363 $1,334.98 $1,373.89 $1,400.05 $1,412.06 $1,603.14 $1,489.05 $1,495.66
64+ $1,356.69 $1,396.23 $1,422.81 $1,435.02 $1,629.21 $1,513.26 $1,519.98Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
GOLD PPO PLANS
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 6
Region 6 includes the couny of: Alameda
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
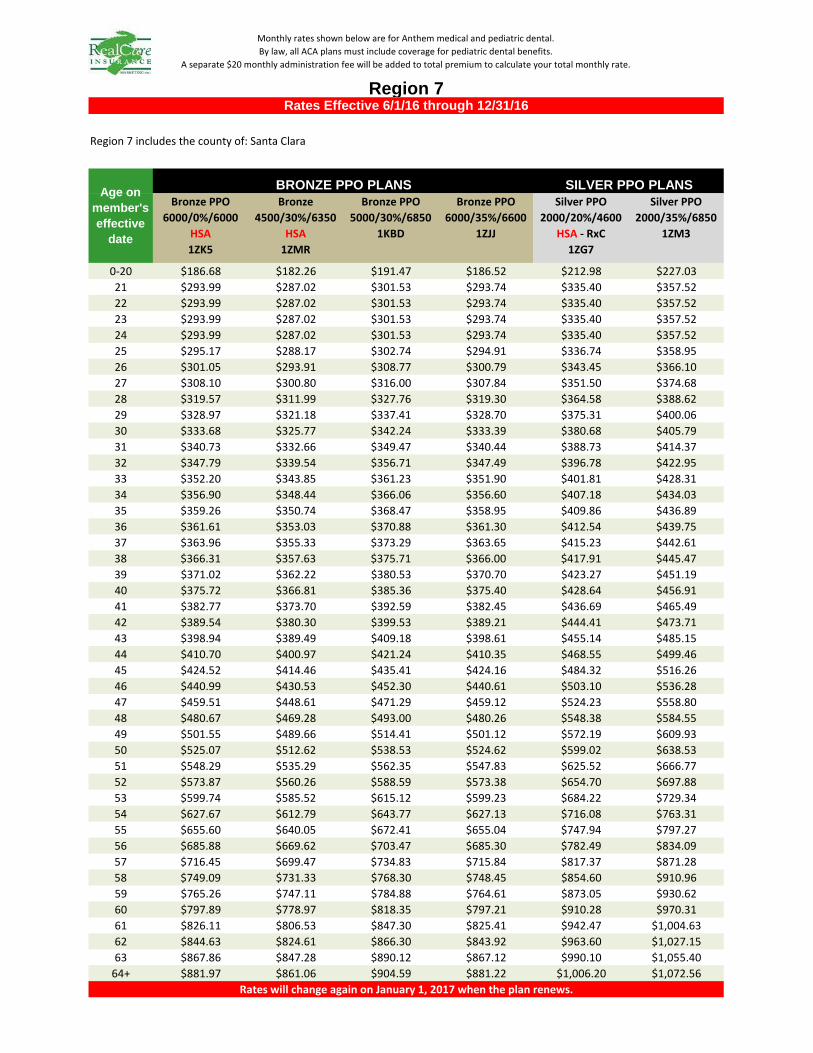
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $186.68 $182.26 $191.47 $186.52 $212.98 $227.0321 $293.99 $287.02 $301.53 $293.74 $335.40 $357.5222 $293.99 $287.02 $301.53 $293.74 $335.40 $357.5223 $293.99 $287.02 $301.53 $293.74 $335.40 $357.5224 $293.99 $287.02 $301.53 $293.74 $335.40 $357.5225 $295.17 $288.17 $302.74 $294.91 $336.74 $358.9526 $301.05 $293.91 $308.77 $300.79 $343.45 $366.1027 $308.10 $300.80 $316.00 $307.84 $351.50 $374.6828 $319.57 $311.99 $327.76 $319.30 $364.58 $388.6229 $328.97 $321.18 $337.41 $328.70 $375.31 $400.0630 $333.68 $325.77 $342.24 $333.39 $380.68 $405.7931 $340.73 $332.66 $349.47 $340.44 $388.73 $414.3732 $347.79 $339.54 $356.71 $347.49 $396.78 $422.9533 $352.20 $343.85 $361.23 $351.90 $401.81 $428.3134 $356.90 $348.44 $366.06 $356.60 $407.18 $434.0335 $359.26 $350.74 $368.47 $358.95 $409.86 $436.8936 $361.61 $353.03 $370.88 $361.30 $412.54 $439.7537 $363.96 $355.33 $373.29 $363.65 $415.23 $442.6138 $366.31 $357.63 $375.71 $366.00 $417.91 $445.4739 $371.02 $362.22 $380.53 $370.70 $423.27 $451.1940 $375.72 $366.81 $385.36 $375.40 $428.64 $456.9141 $382.77 $373.70 $392.59 $382.45 $436.69 $465.4942 $389.54 $380.30 $399.53 $389.21 $444.41 $473.7143 $398.94 $389.49 $409.18 $398.61 $455.14 $485.1544 $410.70 $400.97 $421.24 $410.35 $468.55 $499.4645 $424.52 $414.46 $435.41 $424.16 $484.32 $516.2646 $440.99 $430.53 $452.30 $440.61 $503.10 $536.2847 $459.51 $448.61 $471.29 $459.12 $524.23 $558.8048 $480.67 $469.28 $493.00 $480.26 $548.38 $584.5549 $501.55 $489.66 $514.41 $501.12 $572.19 $609.9350 $525.07 $512.62 $538.53 $524.62 $599.02 $638.5351 $548.29 $535.29 $562.35 $547.83 $625.52 $666.7752 $573.87 $560.26 $588.59 $573.38 $654.70 $697.8853 $599.74 $585.52 $615.12 $599.23 $684.22 $729.3454 $627.67 $612.79 $643.77 $627.13 $716.08 $763.3155 $655.60 $640.05 $672.41 $655.04 $747.94 $797.2756 $685.88 $669.62 $703.47 $685.30 $782.49 $834.0957 $716.45 $699.47 $734.83 $715.84 $817.37 $871.2858 $749.09 $731.33 $768.30 $748.45 $854.60 $910.9659 $765.26 $747.11 $784.88 $764.61 $873.05 $930.6260 $797.89 $778.97 $818.35 $797.21 $910.28 $970.3161 $826.11 $806.53 $847.30 $825.41 $942.47 $1,004.6362 $844.63 $824.61 $866.30 $843.92 $963.60 $1,027.1563 $867.86 $847.28 $890.12 $867.12 $990.10 $1,055.40
64+ $881.97 $861.06 $904.59 $881.22 $1,006.20 $1,072.56
SILVER PPO PLANS
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 7Rates Effective 6/1/16 through 12/31/16
Region 7 includes the county of: Santa Clara
BRONZE PPO PLANS
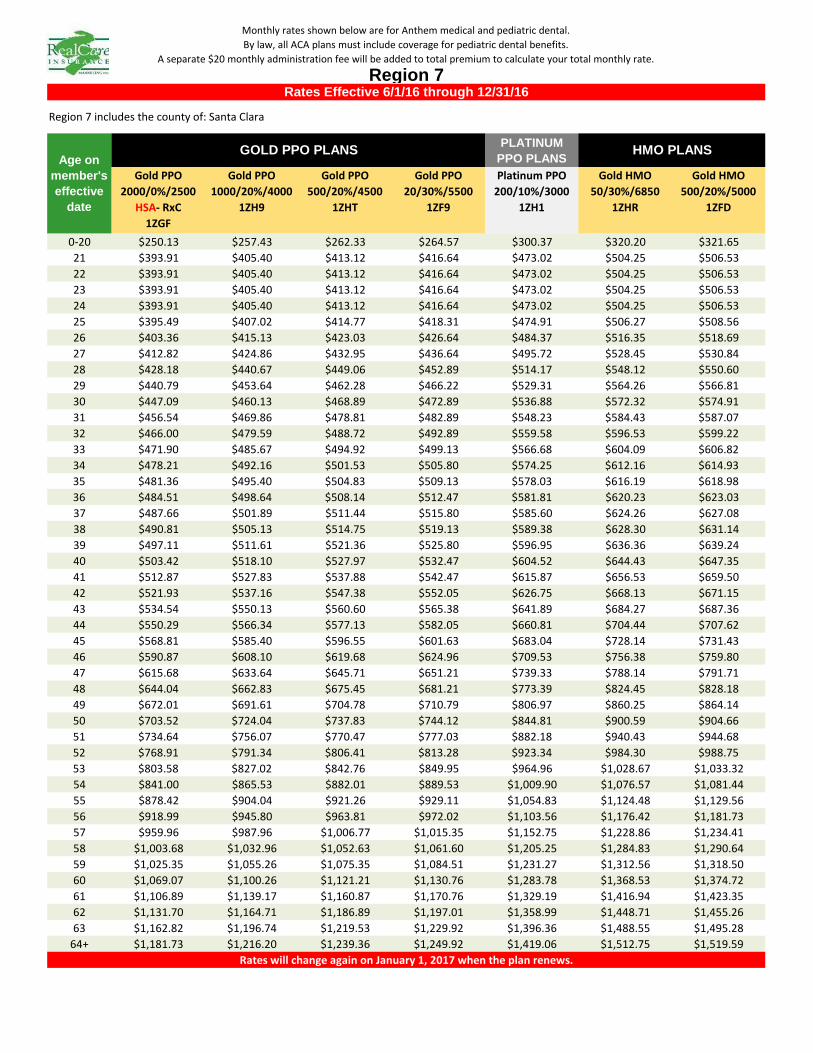
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $250.13 $257.43 $262.33 $264.57 $300.37 $320.20 $321.6521 $393.91 $405.40 $413.12 $416.64 $473.02 $504.25 $506.5322 $393.91 $405.40 $413.12 $416.64 $473.02 $504.25 $506.5323 $393.91 $405.40 $413.12 $416.64 $473.02 $504.25 $506.5324 $393.91 $405.40 $413.12 $416.64 $473.02 $504.25 $506.5325 $395.49 $407.02 $414.77 $418.31 $474.91 $506.27 $508.5626 $403.36 $415.13 $423.03 $426.64 $484.37 $516.35 $518.6927 $412.82 $424.86 $432.95 $436.64 $495.72 $528.45 $530.8428 $428.18 $440.67 $449.06 $452.89 $514.17 $548.12 $550.6029 $440.79 $453.64 $462.28 $466.22 $529.31 $564.26 $566.8130 $447.09 $460.13 $468.89 $472.89 $536.88 $572.32 $574.9131 $456.54 $469.86 $478.81 $482.89 $548.23 $584.43 $587.0732 $466.00 $479.59 $488.72 $492.89 $559.58 $596.53 $599.2233 $471.90 $485.67 $494.92 $499.13 $566.68 $604.09 $606.8234 $478.21 $492.16 $501.53 $505.80 $574.25 $612.16 $614.9335 $481.36 $495.40 $504.83 $509.13 $578.03 $616.19 $618.9836 $484.51 $498.64 $508.14 $512.47 $581.81 $620.23 $623.0337 $487.66 $501.89 $511.44 $515.80 $585.60 $624.26 $627.0838 $490.81 $505.13 $514.75 $519.13 $589.38 $628.30 $631.1439 $497.11 $511.61 $521.36 $525.80 $596.95 $636.36 $639.2440 $503.42 $518.10 $527.97 $532.47 $604.52 $644.43 $647.3541 $512.87 $527.83 $537.88 $542.47 $615.87 $656.53 $659.5042 $521.93 $537.16 $547.38 $552.05 $626.75 $668.13 $671.1543 $534.54 $550.13 $560.60 $565.38 $641.89 $684.27 $687.3644 $550.29 $566.34 $577.13 $582.05 $660.81 $704.44 $707.6245 $568.81 $585.40 $596.55 $601.63 $683.04 $728.14 $731.4346 $590.87 $608.10 $619.68 $624.96 $709.53 $756.38 $759.8047 $615.68 $633.64 $645.71 $651.21 $739.33 $788.14 $791.7148 $644.04 $662.83 $675.45 $681.21 $773.39 $824.45 $828.1849 $672.01 $691.61 $704.78 $710.79 $806.97 $860.25 $864.1450 $703.52 $724.04 $737.83 $744.12 $844.81 $900.59 $904.6651 $734.64 $756.07 $770.47 $777.03 $882.18 $940.43 $944.6852 $768.91 $791.34 $806.41 $813.28 $923.34 $984.30 $988.7553 $803.58 $827.02 $842.76 $849.95 $964.96 $1,028.67 $1,033.3254 $841.00 $865.53 $882.01 $889.53 $1,009.90 $1,076.57 $1,081.4455 $878.42 $904.04 $921.26 $929.11 $1,054.83 $1,124.48 $1,129.5656 $918.99 $945.80 $963.81 $972.02 $1,103.56 $1,176.42 $1,181.7357 $959.96 $987.96 $1,006.77 $1,015.35 $1,152.75 $1,228.86 $1,234.4158 $1,003.68 $1,032.96 $1,052.63 $1,061.60 $1,205.25 $1,284.83 $1,290.6459 $1,025.35 $1,055.26 $1,075.35 $1,084.51 $1,231.27 $1,312.56 $1,318.5060 $1,069.07 $1,100.26 $1,121.21 $1,130.76 $1,283.78 $1,368.53 $1,374.7261 $1,106.89 $1,139.17 $1,160.87 $1,170.76 $1,329.19 $1,416.94 $1,423.3562 $1,131.70 $1,164.71 $1,186.89 $1,197.01 $1,358.99 $1,448.71 $1,455.2663 $1,162.82 $1,196.74 $1,219.53 $1,229.92 $1,396.36 $1,488.55 $1,495.28
64+ $1,181.73 $1,216.20 $1,239.36 $1,249.92 $1,419.06 $1,512.75 $1,519.59
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 7
Region 7 includes the county of: Santa Clara
Age on member's effective
date
GOLD PPO PLANS
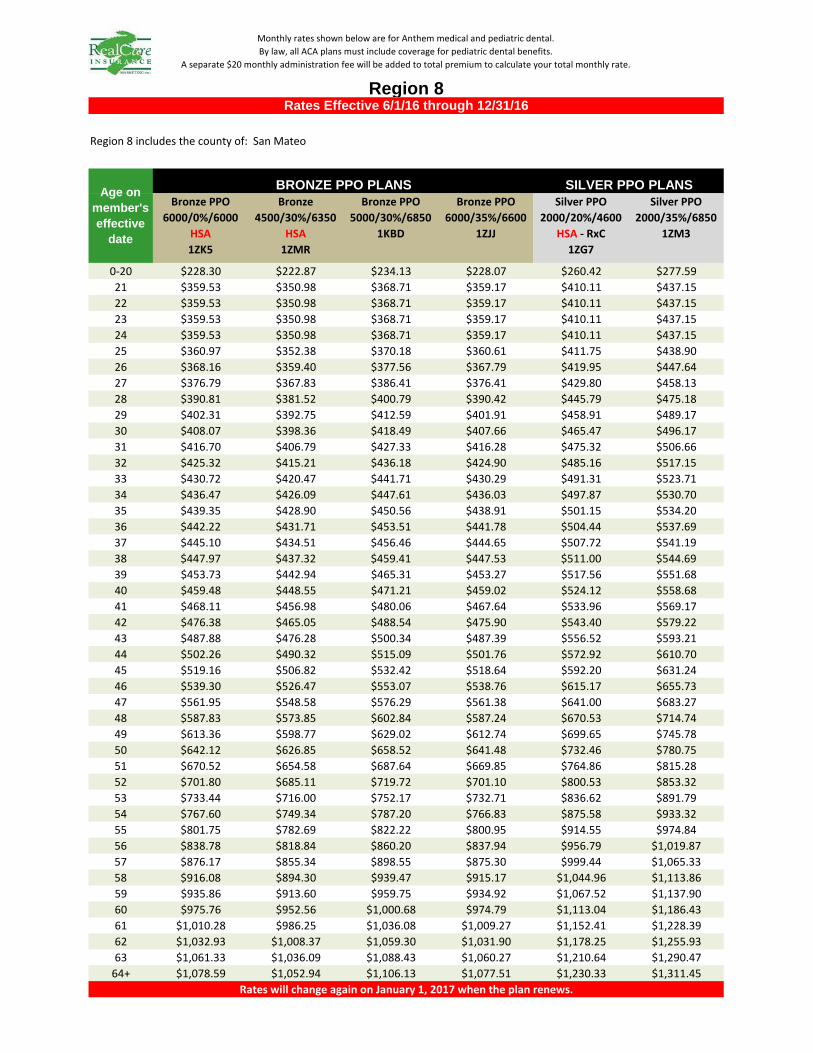
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $228.30 $222.87 $234.13 $228.07 $260.42 $277.5921 $359.53 $350.98 $368.71 $359.17 $410.11 $437.1522 $359.53 $350.98 $368.71 $359.17 $410.11 $437.1523 $359.53 $350.98 $368.71 $359.17 $410.11 $437.1524 $359.53 $350.98 $368.71 $359.17 $410.11 $437.1525 $360.97 $352.38 $370.18 $360.61 $411.75 $438.9026 $368.16 $359.40 $377.56 $367.79 $419.95 $447.6427 $376.79 $367.83 $386.41 $376.41 $429.80 $458.1328 $390.81 $381.52 $400.79 $390.42 $445.79 $475.1829 $402.31 $392.75 $412.59 $401.91 $458.91 $489.1730 $408.07 $398.36 $418.49 $407.66 $465.47 $496.1731 $416.70 $406.79 $427.33 $416.28 $475.32 $506.6632 $425.32 $415.21 $436.18 $424.90 $485.16 $517.1533 $430.72 $420.47 $441.71 $430.29 $491.31 $523.7134 $436.47 $426.09 $447.61 $436.03 $497.87 $530.7035 $439.35 $428.90 $450.56 $438.91 $501.15 $534.2036 $442.22 $431.71 $453.51 $441.78 $504.44 $537.6937 $445.10 $434.51 $456.46 $444.65 $507.72 $541.1938 $447.97 $437.32 $459.41 $447.53 $511.00 $544.6939 $453.73 $442.94 $465.31 $453.27 $517.56 $551.6840 $459.48 $448.55 $471.21 $459.02 $524.12 $558.6841 $468.11 $456.98 $480.06 $467.64 $533.96 $569.1742 $476.38 $465.05 $488.54 $475.90 $543.40 $579.2243 $487.88 $476.28 $500.34 $487.39 $556.52 $593.2144 $502.26 $490.32 $515.09 $501.76 $572.92 $610.7045 $519.16 $506.82 $532.42 $518.64 $592.20 $631.2446 $539.30 $526.47 $553.07 $538.76 $615.17 $655.7347 $561.95 $548.58 $576.29 $561.38 $641.00 $683.2748 $587.83 $573.85 $602.84 $587.24 $670.53 $714.7449 $613.36 $598.77 $629.02 $612.74 $699.65 $745.7850 $642.12 $626.85 $658.52 $641.48 $732.46 $780.7551 $670.52 $654.58 $687.64 $669.85 $764.86 $815.2852 $701.80 $685.11 $719.72 $701.10 $800.53 $853.3253 $733.44 $716.00 $752.17 $732.71 $836.62 $891.7954 $767.60 $749.34 $787.20 $766.83 $875.58 $933.3255 $801.75 $782.69 $822.22 $800.95 $914.55 $974.8456 $838.78 $818.84 $860.20 $837.94 $956.79 $1,019.8757 $876.17 $855.34 $898.55 $875.30 $999.44 $1,065.3358 $916.08 $894.30 $939.47 $915.17 $1,044.96 $1,113.8659 $935.86 $913.60 $959.75 $934.92 $1,067.52 $1,137.9060 $975.76 $952.56 $1,000.68 $974.79 $1,113.04 $1,186.4361 $1,010.28 $986.25 $1,036.08 $1,009.27 $1,152.41 $1,228.3962 $1,032.93 $1,008.37 $1,059.30 $1,031.90 $1,178.25 $1,255.9363 $1,061.33 $1,036.09 $1,088.43 $1,060.27 $1,210.64 $1,290.47
64+ $1,078.59 $1,052.94 $1,106.13 $1,077.51 $1,230.33 $1,311.45
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 8
Region 8 includes the county of: San Mateo
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $305.85 $314.79 $320.76 $323.51 $367.28 $361.88 $363.5121 $481.65 $495.73 $505.14 $509.46 $578.39 $569.89 $572.4622 $481.65 $495.73 $505.14 $509.46 $578.39 $569.89 $572.4623 $481.65 $495.73 $505.14 $509.46 $578.39 $569.89 $572.4624 $481.65 $495.73 $505.14 $509.46 $578.39 $569.89 $572.4625 $483.58 $497.71 $507.16 $511.50 $580.70 $572.17 $574.7526 $493.21 $507.63 $517.26 $521.69 $592.27 $583.57 $586.2027 $504.77 $519.53 $529.39 $533.91 $606.15 $597.24 $599.9428 $523.55 $538.86 $549.09 $553.78 $628.71 $619.47 $622.2629 $538.97 $554.72 $565.25 $570.09 $647.22 $637.71 $640.5830 $546.67 $562.65 $573.33 $578.24 $656.47 $646.83 $649.7431 $558.23 $574.55 $585.46 $590.46 $670.35 $660.50 $663.4832 $569.79 $586.45 $597.58 $602.69 $684.24 $674.18 $677.2233 $577.02 $593.88 $605.16 $610.33 $692.91 $682.73 $685.8134 $584.72 $601.82 $613.24 $618.48 $702.17 $691.85 $694.9735 $588.58 $605.78 $617.28 $622.56 $706.79 $696.41 $699.5536 $592.43 $609.75 $621.32 $626.64 $711.42 $700.96 $704.1337 $596.28 $613.71 $625.36 $630.71 $716.05 $705.52 $708.7138 $600.14 $617.68 $629.40 $634.79 $720.67 $710.08 $713.2939 $607.84 $625.61 $637.49 $642.94 $729.93 $719.20 $722.4440 $615.55 $633.54 $645.57 $651.09 $739.18 $728.32 $731.6041 $627.11 $645.44 $657.69 $663.32 $753.06 $742.00 $745.3442 $638.19 $656.84 $669.31 $675.03 $766.37 $755.10 $758.5143 $653.60 $672.71 $685.47 $691.34 $784.88 $773.34 $776.8344 $672.87 $692.53 $705.68 $711.72 $808.01 $796.14 $799.7345 $695.50 $715.83 $729.42 $735.66 $835.20 $822.92 $826.6346 $722.48 $743.60 $757.71 $764.19 $867.59 $854.84 $858.6947 $752.82 $774.83 $789.53 $796.29 $904.02 $890.74 $894.7548 $787.50 $810.52 $825.90 $832.97 $945.67 $931.77 $935.9749 $821.69 $845.72 $861.77 $869.14 $986.73 $972.23 $976.6250 $860.23 $885.37 $902.18 $909.90 $1,033.00 $1,017.82 $1,022.4151 $898.28 $924.54 $942.09 $950.14 $1,078.70 $1,062.84 $1,067.6452 $940.18 $967.66 $986.03 $994.47 $1,129.02 $1,112.43 $1,117.4453 $982.57 $1,011.29 $1,030.49 $1,039.30 $1,179.92 $1,162.58 $1,167.8254 $1,028.32 $1,058.38 $1,078.47 $1,087.70 $1,234.86 $1,216.72 $1,222.2055 $1,074.08 $1,105.48 $1,126.46 $1,136.10 $1,289.81 $1,270.85 $1,276.5956 $1,123.69 $1,156.54 $1,178.49 $1,188.57 $1,349.38 $1,329.55 $1,335.5557 $1,173.78 $1,208.09 $1,231.03 $1,241.55 $1,409.54 $1,388.82 $1,395.0958 $1,227.24 $1,263.12 $1,287.10 $1,298.10 $1,473.74 $1,452.08 $1,458.6359 $1,253.73 $1,290.39 $1,314.88 $1,326.12 $1,505.55 $1,483.42 $1,490.1160 $1,307.20 $1,345.41 $1,370.95 $1,382.67 $1,569.75 $1,546.68 $1,553.6661 $1,353.44 $1,393.00 $1,419.44 $1,431.58 $1,625.28 $1,601.39 $1,608.6162 $1,383.78 $1,424.23 $1,451.27 $1,463.68 $1,661.71 $1,637.29 $1,644.6863 $1,421.83 $1,463.39 $1,491.17 $1,503.93 $1,707.41 $1,682.32 $1,689.90
64+ $1,444.95 $1,487.19 $1,515.42 $1,528.38 $1,735.17 $1,709.67 $1,717.38
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 8
Region 8 includes the county of: San Mateo
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $211.56 $206.54 $217.00 $211.37 $241.34 $257.2621 $333.16 $325.26 $341.73 $332.87 $380.07 $405.1422 $333.16 $325.26 $341.73 $332.87 $380.07 $405.1423 $333.16 $325.26 $341.73 $332.87 $380.07 $405.1424 $333.16 $325.26 $341.73 $332.87 $380.07 $405.1425 $334.49 $326.56 $343.10 $334.20 $381.59 $406.7626 $341.16 $333.07 $349.93 $340.86 $389.19 $414.8627 $349.15 $340.87 $358.13 $348.85 $398.31 $424.5928 $362.14 $353.56 $371.46 $361.83 $413.14 $440.3929 $372.81 $363.97 $382.40 $372.48 $425.30 $453.3530 $378.14 $369.17 $387.86 $377.81 $431.38 $459.8331 $386.13 $376.98 $396.07 $385.80 $440.50 $469.5632 $394.13 $384.78 $404.27 $393.79 $449.62 $479.2833 $399.13 $389.66 $409.39 $398.78 $455.32 $485.3634 $404.46 $394.87 $414.86 $404.10 $461.40 $491.8435 $407.12 $397.47 $417.59 $406.77 $464.45 $495.0836 $409.79 $400.07 $420.33 $409.43 $467.49 $498.3237 $412.45 $402.67 $423.06 $412.09 $470.53 $501.5638 $415.12 $405.27 $425.80 $414.76 $473.57 $504.8039 $420.45 $410.48 $431.26 $420.08 $479.65 $511.2940 $425.78 $415.68 $436.73 $425.41 $485.73 $517.7741 $433.77 $423.49 $444.93 $433.40 $494.85 $527.4942 $441.44 $430.97 $452.79 $441.05 $503.59 $536.8143 $452.10 $441.38 $463.73 $451.70 $515.75 $549.7744 $465.42 $454.39 $477.40 $465.02 $530.96 $565.9845 $481.08 $469.68 $493.46 $480.66 $548.82 $585.0246 $499.74 $487.89 $512.60 $499.31 $570.11 $607.7147 $520.73 $508.38 $534.12 $520.28 $594.05 $633.2348 $544.72 $531.80 $558.73 $544.24 $621.41 $662.4049 $568.37 $554.89 $582.99 $567.88 $648.40 $691.1750 $595.02 $580.91 $610.33 $594.51 $678.81 $723.5851 $621.34 $606.61 $637.33 $620.80 $708.83 $755.5952 $650.33 $634.91 $667.06 $649.76 $741.90 $790.8353 $679.65 $663.53 $697.13 $679.05 $775.34 $826.4954 $711.30 $694.43 $729.59 $710.68 $811.45 $864.9755 $742.95 $725.33 $762.06 $742.30 $847.56 $903.4656 $777.26 $758.83 $797.26 $776.59 $886.70 $945.1957 $811.91 $792.66 $832.80 $811.20 $926.23 $987.3358 $848.89 $828.76 $870.73 $848.15 $968.42 $1,032.3059 $867.22 $846.65 $889.52 $866.46 $989.32 $1,054.5860 $904.20 $882.76 $927.46 $903.41 $1,031.51 $1,099.5561 $936.18 $913.98 $960.26 $935.36 $1,068.00 $1,138.4462 $957.17 $934.47 $981.79 $956.34 $1,091.94 $1,163.9763 $983.49 $960.17 $1,008.79 $982.63 $1,121.97 $1,195.97
64+ $999.48 $975.78 $1,025.19 $998.61 $1,140.21 $1,215.42
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 9
Region 9 includes the counties of: Santa Cruz, Monterey, and San Benito
BRONZE PPO PLANS
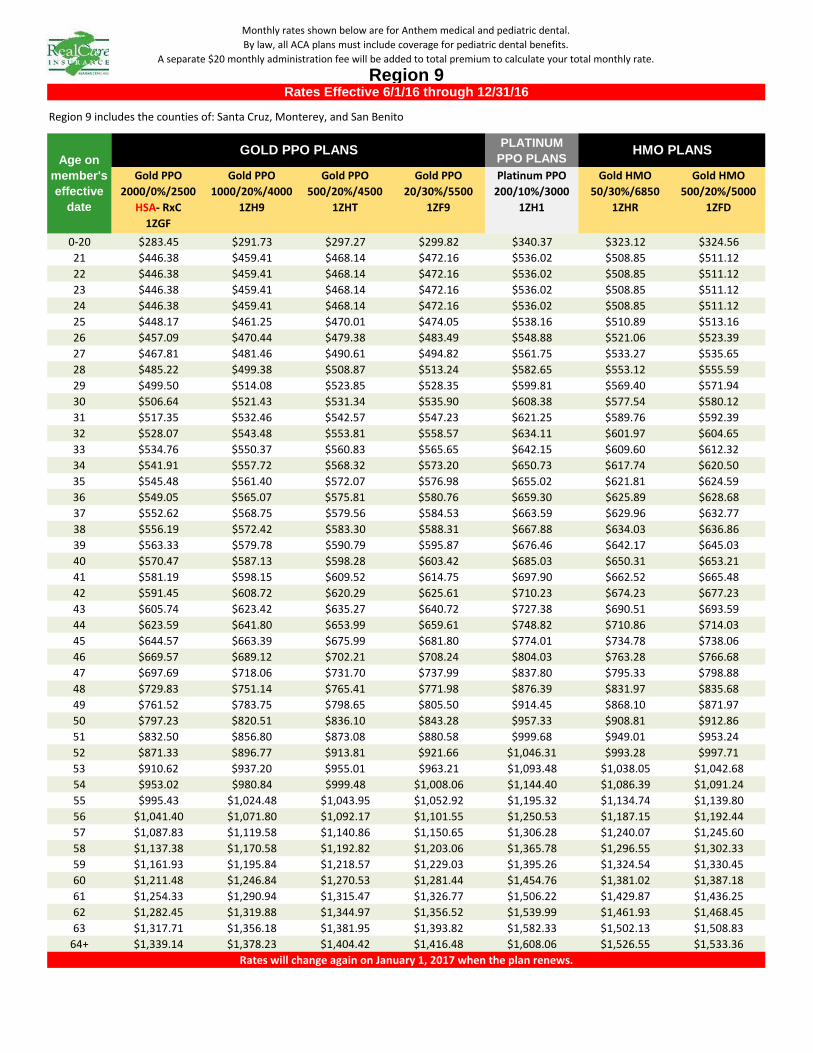
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $283.45 $291.73 $297.27 $299.82 $340.37 $323.12 $324.5621 $446.38 $459.41 $468.14 $472.16 $536.02 $508.85 $511.1222 $446.38 $459.41 $468.14 $472.16 $536.02 $508.85 $511.1223 $446.38 $459.41 $468.14 $472.16 $536.02 $508.85 $511.1224 $446.38 $459.41 $468.14 $472.16 $536.02 $508.85 $511.1225 $448.17 $461.25 $470.01 $474.05 $538.16 $510.89 $513.1626 $457.09 $470.44 $479.38 $483.49 $548.88 $521.06 $523.3927 $467.81 $481.46 $490.61 $494.82 $561.75 $533.27 $535.6528 $485.22 $499.38 $508.87 $513.24 $582.65 $553.12 $555.5929 $499.50 $514.08 $523.85 $528.35 $599.81 $569.40 $571.9430 $506.64 $521.43 $531.34 $535.90 $608.38 $577.54 $580.1231 $517.35 $532.46 $542.57 $547.23 $621.25 $589.76 $592.3932 $528.07 $543.48 $553.81 $558.57 $634.11 $601.97 $604.6533 $534.76 $550.37 $560.83 $565.65 $642.15 $609.60 $612.3234 $541.91 $557.72 $568.32 $573.20 $650.73 $617.74 $620.5035 $545.48 $561.40 $572.07 $576.98 $655.02 $621.81 $624.5936 $549.05 $565.07 $575.81 $580.76 $659.30 $625.89 $628.6837 $552.62 $568.75 $579.56 $584.53 $663.59 $629.96 $632.7738 $556.19 $572.42 $583.30 $588.31 $667.88 $634.03 $636.8639 $563.33 $579.78 $590.79 $595.87 $676.46 $642.17 $645.0340 $570.47 $587.13 $598.28 $603.42 $685.03 $650.31 $653.2141 $581.19 $598.15 $609.52 $614.75 $697.90 $662.52 $665.4842 $591.45 $608.72 $620.29 $625.61 $710.23 $674.23 $677.2343 $605.74 $623.42 $635.27 $640.72 $727.38 $690.51 $693.5944 $623.59 $641.80 $653.99 $659.61 $748.82 $710.86 $714.0345 $644.57 $663.39 $675.99 $681.80 $774.01 $734.78 $738.0646 $669.57 $689.12 $702.21 $708.24 $804.03 $763.28 $766.6847 $697.69 $718.06 $731.70 $737.99 $837.80 $795.33 $798.8848 $729.83 $751.14 $765.41 $771.98 $876.39 $831.97 $835.6849 $761.52 $783.75 $798.65 $805.50 $914.45 $868.10 $871.9750 $797.23 $820.51 $836.10 $843.28 $957.33 $908.81 $912.8651 $832.50 $856.80 $873.08 $880.58 $999.68 $949.01 $953.2452 $871.33 $896.77 $913.81 $921.66 $1,046.31 $993.28 $997.7153 $910.62 $937.20 $955.01 $963.21 $1,093.48 $1,038.05 $1,042.6854 $953.02 $980.84 $999.48 $1,008.06 $1,144.40 $1,086.39 $1,091.2455 $995.43 $1,024.48 $1,043.95 $1,052.92 $1,195.32 $1,134.74 $1,139.8056 $1,041.40 $1,071.80 $1,092.17 $1,101.55 $1,250.53 $1,187.15 $1,192.4457 $1,087.83 $1,119.58 $1,140.86 $1,150.65 $1,306.28 $1,240.07 $1,245.6058 $1,137.38 $1,170.58 $1,192.82 $1,203.06 $1,365.78 $1,296.55 $1,302.3359 $1,161.93 $1,195.84 $1,218.57 $1,229.03 $1,395.26 $1,324.54 $1,330.4560 $1,211.48 $1,246.84 $1,270.53 $1,281.44 $1,454.76 $1,381.02 $1,387.1861 $1,254.33 $1,290.94 $1,315.47 $1,326.77 $1,506.22 $1,429.87 $1,436.2562 $1,282.45 $1,319.88 $1,344.97 $1,356.52 $1,539.99 $1,461.93 $1,468.4563 $1,317.71 $1,356.18 $1,381.95 $1,393.82 $1,582.33 $1,502.13 $1,508.83
64+ $1,339.14 $1,378.23 $1,404.42 $1,416.48 $1,608.06 $1,526.55 $1,533.36Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 9
Region 9 includes the counties of: Santa Cruz, Monterey, and San Benito
Age on member's effective
date
GOLD PPO PLANS HMO PLANS
Rates Effective 6/1/16 through 12/31/16
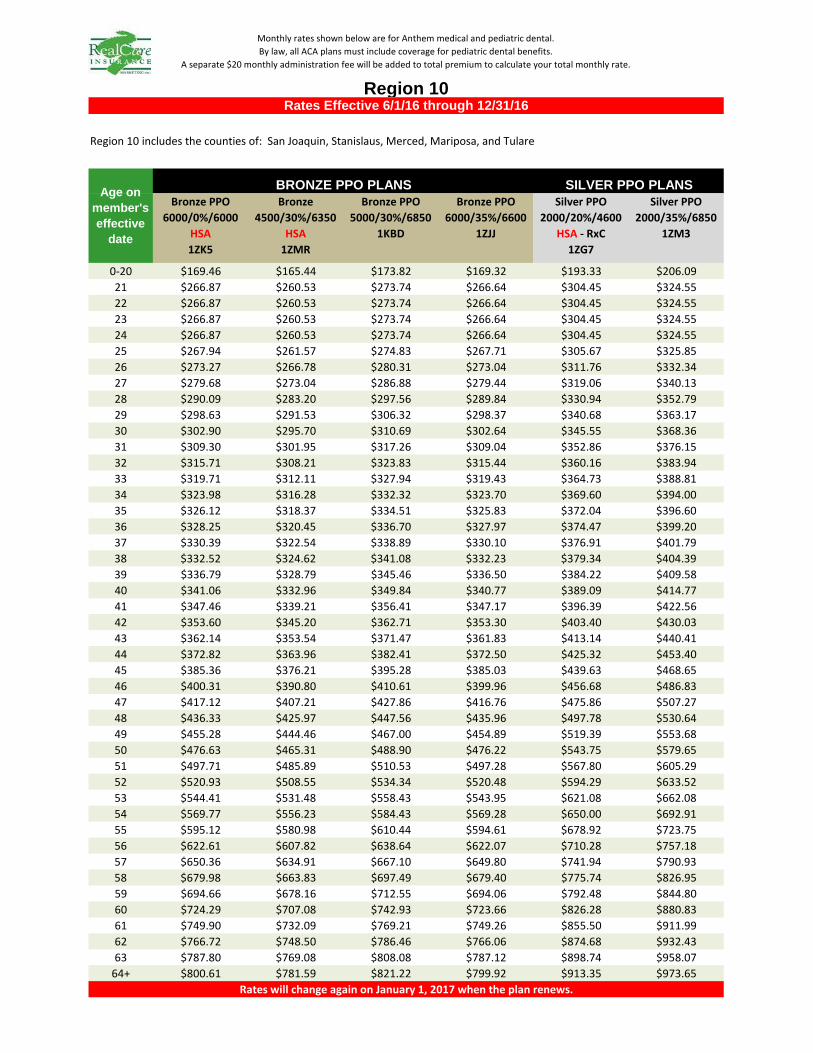
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $169.46 $165.44 $173.82 $169.32 $193.33 $206.0921 $266.87 $260.53 $273.74 $266.64 $304.45 $324.5522 $266.87 $260.53 $273.74 $266.64 $304.45 $324.5523 $266.87 $260.53 $273.74 $266.64 $304.45 $324.5524 $266.87 $260.53 $273.74 $266.64 $304.45 $324.5525 $267.94 $261.57 $274.83 $267.71 $305.67 $325.8526 $273.27 $266.78 $280.31 $273.04 $311.76 $332.3427 $279.68 $273.04 $286.88 $279.44 $319.06 $340.1328 $290.09 $283.20 $297.56 $289.84 $330.94 $352.7929 $298.63 $291.53 $306.32 $298.37 $340.68 $363.1730 $302.90 $295.70 $310.69 $302.64 $345.55 $368.3631 $309.30 $301.95 $317.26 $309.04 $352.86 $376.1532 $315.71 $308.21 $323.83 $315.44 $360.16 $383.9433 $319.71 $312.11 $327.94 $319.43 $364.73 $388.8134 $323.98 $316.28 $332.32 $323.70 $369.60 $394.0035 $326.12 $318.37 $334.51 $325.83 $372.04 $396.6036 $328.25 $320.45 $336.70 $327.97 $374.47 $399.2037 $330.39 $322.54 $338.89 $330.10 $376.91 $401.7938 $332.52 $324.62 $341.08 $332.23 $379.34 $404.3939 $336.79 $328.79 $345.46 $336.50 $384.22 $409.5840 $341.06 $332.96 $349.84 $340.77 $389.09 $414.7741 $347.46 $339.21 $356.41 $347.17 $396.39 $422.5642 $353.60 $345.20 $362.71 $353.30 $403.40 $430.0343 $362.14 $353.54 $371.47 $361.83 $413.14 $440.4144 $372.82 $363.96 $382.41 $372.50 $425.32 $453.4045 $385.36 $376.21 $395.28 $385.03 $439.63 $468.6546 $400.31 $390.80 $410.61 $399.96 $456.68 $486.8347 $417.12 $407.21 $427.86 $416.76 $475.86 $507.2748 $436.33 $425.97 $447.56 $435.96 $497.78 $530.6449 $455.28 $444.46 $467.00 $454.89 $519.39 $553.6850 $476.63 $465.31 $488.90 $476.22 $543.75 $579.6551 $497.71 $485.89 $510.53 $497.28 $567.80 $605.2952 $520.93 $508.55 $534.34 $520.48 $594.29 $633.5253 $544.41 $531.48 $558.43 $543.95 $621.08 $662.0854 $569.77 $556.23 $584.43 $569.28 $650.00 $692.9155 $595.12 $580.98 $610.44 $594.61 $678.92 $723.7556 $622.61 $607.82 $638.64 $622.07 $710.28 $757.1857 $650.36 $634.91 $667.10 $649.80 $741.94 $790.9358 $679.98 $663.83 $697.49 $679.40 $775.74 $826.9559 $694.66 $678.16 $712.55 $694.06 $792.48 $844.8060 $724.29 $707.08 $742.93 $723.66 $826.28 $880.8361 $749.90 $732.09 $769.21 $749.26 $855.50 $911.9962 $766.72 $748.50 $786.46 $766.06 $874.68 $932.4363 $787.80 $769.08 $808.08 $787.12 $898.74 $958.07
64+ $800.61 $781.59 $821.22 $799.92 $913.35 $973.65
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 10
Region 10 includes the counties of: San Joaquin, Stanislaus, Merced, Mariposa, and Tulare
BRONZE PPO PLANS
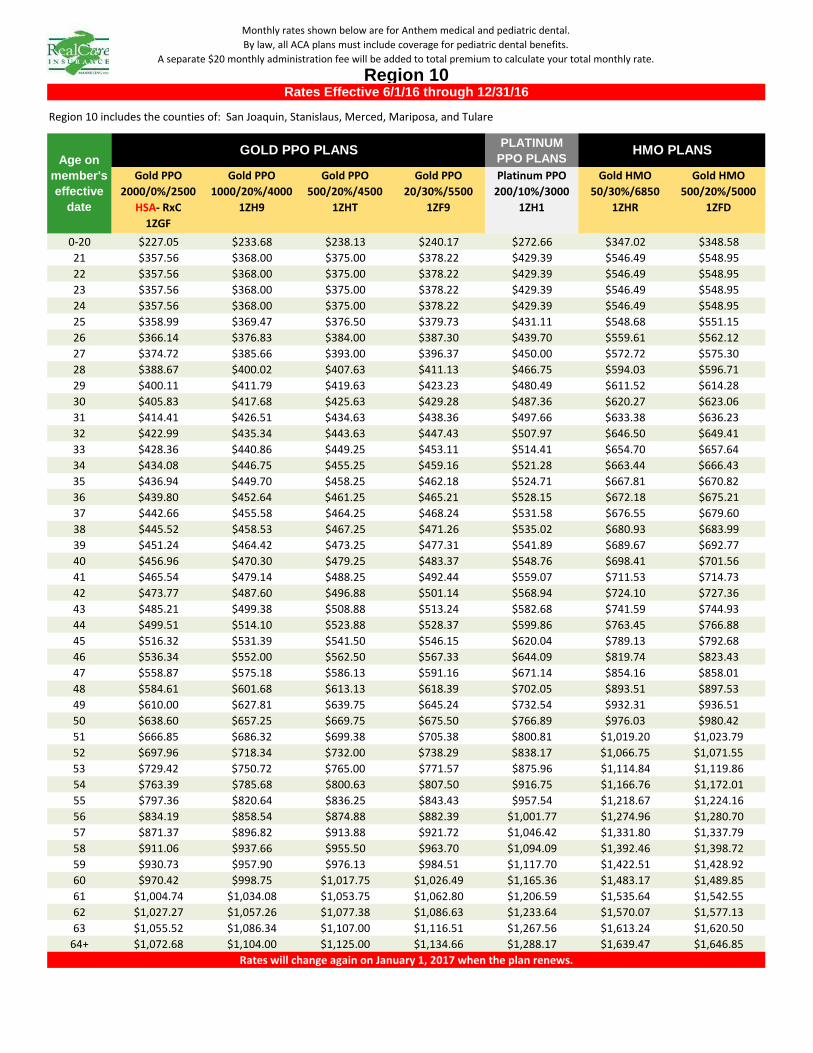
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $227.05 $233.68 $238.13 $240.17 $272.66 $347.02 $348.5821 $357.56 $368.00 $375.00 $378.22 $429.39 $546.49 $548.9522 $357.56 $368.00 $375.00 $378.22 $429.39 $546.49 $548.9523 $357.56 $368.00 $375.00 $378.22 $429.39 $546.49 $548.9524 $357.56 $368.00 $375.00 $378.22 $429.39 $546.49 $548.9525 $358.99 $369.47 $376.50 $379.73 $431.11 $548.68 $551.1526 $366.14 $376.83 $384.00 $387.30 $439.70 $559.61 $562.1227 $374.72 $385.66 $393.00 $396.37 $450.00 $572.72 $575.3028 $388.67 $400.02 $407.63 $411.13 $466.75 $594.03 $596.7129 $400.11 $411.79 $419.63 $423.23 $480.49 $611.52 $614.2830 $405.83 $417.68 $425.63 $429.28 $487.36 $620.27 $623.0631 $414.41 $426.51 $434.63 $438.36 $497.66 $633.38 $636.2332 $422.99 $435.34 $443.63 $447.43 $507.97 $646.50 $649.4133 $428.36 $440.86 $449.25 $453.11 $514.41 $654.70 $657.6434 $434.08 $446.75 $455.25 $459.16 $521.28 $663.44 $666.4335 $436.94 $449.70 $458.25 $462.18 $524.71 $667.81 $670.8236 $439.80 $452.64 $461.25 $465.21 $528.15 $672.18 $675.2137 $442.66 $455.58 $464.25 $468.24 $531.58 $676.55 $679.6038 $445.52 $458.53 $467.25 $471.26 $535.02 $680.93 $683.9939 $451.24 $464.42 $473.25 $477.31 $541.89 $689.67 $692.7740 $456.96 $470.30 $479.25 $483.37 $548.76 $698.41 $701.5641 $465.54 $479.14 $488.25 $492.44 $559.07 $711.53 $714.7342 $473.77 $487.60 $496.88 $501.14 $568.94 $724.10 $727.3643 $485.21 $499.38 $508.88 $513.24 $582.68 $741.59 $744.9344 $499.51 $514.10 $523.88 $528.37 $599.86 $763.45 $766.8845 $516.32 $531.39 $541.50 $546.15 $620.04 $789.13 $792.6846 $536.34 $552.00 $562.50 $567.33 $644.09 $819.74 $823.4347 $558.87 $575.18 $586.13 $591.16 $671.14 $854.16 $858.0148 $584.61 $601.68 $613.13 $618.39 $702.05 $893.51 $897.5349 $610.00 $627.81 $639.75 $645.24 $732.54 $932.31 $936.5150 $638.60 $657.25 $669.75 $675.50 $766.89 $976.03 $980.4251 $666.85 $686.32 $699.38 $705.38 $800.81 $1,019.20 $1,023.7952 $697.96 $718.34 $732.00 $738.29 $838.17 $1,066.75 $1,071.5553 $729.42 $750.72 $765.00 $771.57 $875.96 $1,114.84 $1,119.8654 $763.39 $785.68 $800.63 $807.50 $916.75 $1,166.76 $1,172.0155 $797.36 $820.64 $836.25 $843.43 $957.54 $1,218.67 $1,224.1656 $834.19 $858.54 $874.88 $882.39 $1,001.77 $1,274.96 $1,280.7057 $871.37 $896.82 $913.88 $921.72 $1,046.42 $1,331.80 $1,337.7958 $911.06 $937.66 $955.50 $963.70 $1,094.09 $1,392.46 $1,398.7259 $930.73 $957.90 $976.13 $984.51 $1,117.70 $1,422.51 $1,428.9260 $970.42 $998.75 $1,017.75 $1,026.49 $1,165.36 $1,483.17 $1,489.8561 $1,004.74 $1,034.08 $1,053.75 $1,062.80 $1,206.59 $1,535.64 $1,542.5562 $1,027.27 $1,057.26 $1,077.38 $1,086.63 $1,233.64 $1,570.07 $1,577.1363 $1,055.52 $1,086.34 $1,107.00 $1,116.51 $1,267.56 $1,613.24 $1,620.50
64+ $1,072.68 $1,104.00 $1,125.00 $1,134.66 $1,288.17 $1,639.47 $1,646.85
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 10
Region 10 includes the counties of: San Joaquin, Stanislaus, Merced, Mariposa, and Tulare
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $151.76 $148.14 $155.65 $151.62 $173.11 $184.5421 $238.99 $233.29 $245.12 $238.77 $272.62 $290.6122 $238.99 $233.29 $245.12 $238.77 $272.62 $290.6123 $238.99 $233.29 $245.12 $238.77 $272.62 $290.6124 $238.99 $233.29 $245.12 $238.77 $272.62 $290.6125 $239.95 $234.22 $246.10 $239.73 $273.71 $291.7726 $244.73 $238.89 $251.00 $244.50 $279.16 $297.5827 $250.46 $244.49 $256.89 $250.23 $285.71 $304.5628 $259.78 $253.59 $266.45 $259.54 $296.34 $315.8929 $267.43 $261.05 $274.29 $267.18 $305.06 $325.1930 $271.25 $264.78 $278.21 $271.00 $309.42 $329.8431 $276.99 $270.38 $284.09 $276.73 $315.97 $336.8232 $282.73 $275.98 $289.98 $282.46 $322.51 $343.7933 $286.31 $279.48 $293.65 $286.05 $326.60 $348.1534 $290.13 $283.21 $297.58 $289.87 $330.96 $352.8035 $292.05 $285.08 $299.54 $291.78 $333.14 $355.1336 $293.96 $286.95 $301.50 $293.69 $335.32 $357.4537 $295.87 $288.81 $303.46 $295.60 $337.50 $359.7838 $297.78 $290.68 $305.42 $297.51 $339.68 $362.1039 $301.61 $294.41 $309.34 $301.33 $344.05 $366.7540 $305.43 $298.14 $313.26 $305.15 $348.41 $371.4041 $311.16 $303.74 $319.15 $310.88 $354.95 $378.3742 $316.66 $309.11 $324.78 $316.37 $361.22 $385.0643 $324.31 $316.57 $332.63 $324.01 $369.95 $394.3644 $333.87 $325.91 $342.43 $333.56 $380.85 $405.9845 $345.10 $336.87 $353.95 $344.78 $393.66 $419.6446 $358.49 $349.94 $367.68 $358.16 $408.93 $435.9247 $373.54 $364.63 $383.12 $373.20 $426.11 $454.2248 $390.75 $381.43 $400.77 $390.39 $445.73 $475.1549 $407.72 $397.99 $418.17 $407.34 $465.09 $495.7850 $426.84 $416.66 $437.78 $426.44 $486.90 $519.0351 $445.72 $435.09 $457.15 $445.31 $508.44 $541.9952 $466.51 $455.38 $478.47 $466.08 $532.15 $567.2753 $487.54 $475.91 $500.04 $487.09 $556.14 $592.8454 $510.24 $498.07 $523.33 $509.77 $582.04 $620.4555 $532.95 $520.24 $546.62 $532.46 $607.94 $648.0656 $557.56 $544.27 $571.86 $557.05 $636.02 $677.9957 $582.42 $568.53 $597.36 $581.88 $664.37 $708.2258 $608.95 $594.42 $624.57 $608.39 $694.64 $740.4759 $622.09 $607.25 $638.05 $621.52 $709.63 $756.4660 $648.62 $633.15 $665.26 $648.02 $739.89 $788.7261 $671.56 $655.54 $688.79 $670.94 $766.06 $816.6162 $686.62 $670.24 $704.23 $685.99 $783.24 $834.9263 $705.50 $688.67 $723.59 $704.85 $804.77 $857.88
64+ $716.97 $699.87 $735.36 $716.31 $817.86 $871.83
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 11
Region 11 includes the counties of: Madera, Fresno, and Kings.
BRONZE PPO PLANS
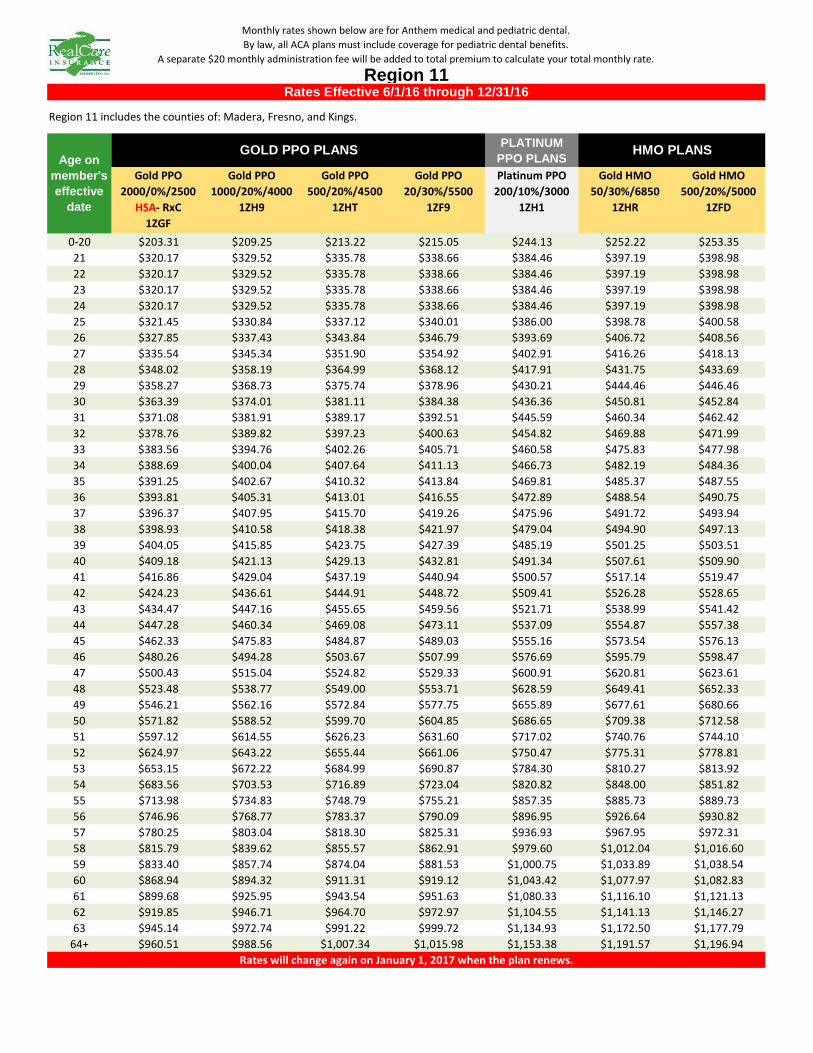
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $203.31 $209.25 $213.22 $215.05 $244.13 $252.22 $253.3521 $320.17 $329.52 $335.78 $338.66 $384.46 $397.19 $398.9822 $320.17 $329.52 $335.78 $338.66 $384.46 $397.19 $398.9823 $320.17 $329.52 $335.78 $338.66 $384.46 $397.19 $398.9824 $320.17 $329.52 $335.78 $338.66 $384.46 $397.19 $398.9825 $321.45 $330.84 $337.12 $340.01 $386.00 $398.78 $400.5826 $327.85 $337.43 $343.84 $346.79 $393.69 $406.72 $408.5627 $335.54 $345.34 $351.90 $354.92 $402.91 $416.26 $418.1328 $348.02 $358.19 $364.99 $368.12 $417.91 $431.75 $433.6929 $358.27 $368.73 $375.74 $378.96 $430.21 $444.46 $446.4630 $363.39 $374.01 $381.11 $384.38 $436.36 $450.81 $452.8431 $371.08 $381.91 $389.17 $392.51 $445.59 $460.34 $462.4232 $378.76 $389.82 $397.23 $400.63 $454.82 $469.88 $471.9933 $383.56 $394.76 $402.26 $405.71 $460.58 $475.83 $477.9834 $388.69 $400.04 $407.64 $411.13 $466.73 $482.19 $484.3635 $391.25 $402.67 $410.32 $413.84 $469.81 $485.37 $487.5536 $393.81 $405.31 $413.01 $416.55 $472.89 $488.54 $490.7537 $396.37 $407.95 $415.70 $419.26 $475.96 $491.72 $493.9438 $398.93 $410.58 $418.38 $421.97 $479.04 $494.90 $497.1339 $404.05 $415.85 $423.75 $427.39 $485.19 $501.25 $503.5140 $409.18 $421.13 $429.13 $432.81 $491.34 $507.61 $509.9041 $416.86 $429.04 $437.19 $440.94 $500.57 $517.14 $519.4742 $424.23 $436.61 $444.91 $448.72 $509.41 $526.28 $528.6543 $434.47 $447.16 $455.65 $459.56 $521.71 $538.99 $541.4244 $447.28 $460.34 $469.08 $473.11 $537.09 $554.87 $557.3845 $462.33 $475.83 $484.87 $489.03 $555.16 $573.54 $576.1346 $480.26 $494.28 $503.67 $507.99 $576.69 $595.79 $598.4747 $500.43 $515.04 $524.82 $529.33 $600.91 $620.81 $623.6148 $523.48 $538.77 $549.00 $553.71 $628.59 $649.41 $652.3349 $546.21 $562.16 $572.84 $577.75 $655.89 $677.61 $680.6650 $571.82 $588.52 $599.70 $604.85 $686.65 $709.38 $712.5851 $597.12 $614.55 $626.23 $631.60 $717.02 $740.76 $744.1052 $624.97 $643.22 $655.44 $661.06 $750.47 $775.31 $778.8153 $653.15 $672.22 $684.99 $690.87 $784.30 $810.27 $813.9254 $683.56 $703.53 $716.89 $723.04 $820.82 $848.00 $851.8255 $713.98 $734.83 $748.79 $755.21 $857.35 $885.73 $889.7356 $746.96 $768.77 $783.37 $790.09 $896.95 $926.64 $930.8257 $780.25 $803.04 $818.30 $825.31 $936.93 $967.95 $972.3158 $815.79 $839.62 $855.57 $862.91 $979.60 $1,012.04 $1,016.6059 $833.40 $857.74 $874.04 $881.53 $1,000.75 $1,033.89 $1,038.5460 $868.94 $894.32 $911.31 $919.12 $1,043.42 $1,077.97 $1,082.8361 $899.68 $925.95 $943.54 $951.63 $1,080.33 $1,116.10 $1,121.1362 $919.85 $946.71 $964.70 $972.97 $1,104.55 $1,141.13 $1,146.2763 $945.14 $972.74 $991.22 $999.72 $1,134.93 $1,172.50 $1,177.79
64+ $960.51 $988.56 $1,007.34 $1,015.98 $1,153.38 $1,191.57 $1,196.94
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 11
Region 11 includes the counties of: Madera, Fresno, and Kings.
Age on member's effective
date
GOLD PPO PLANS
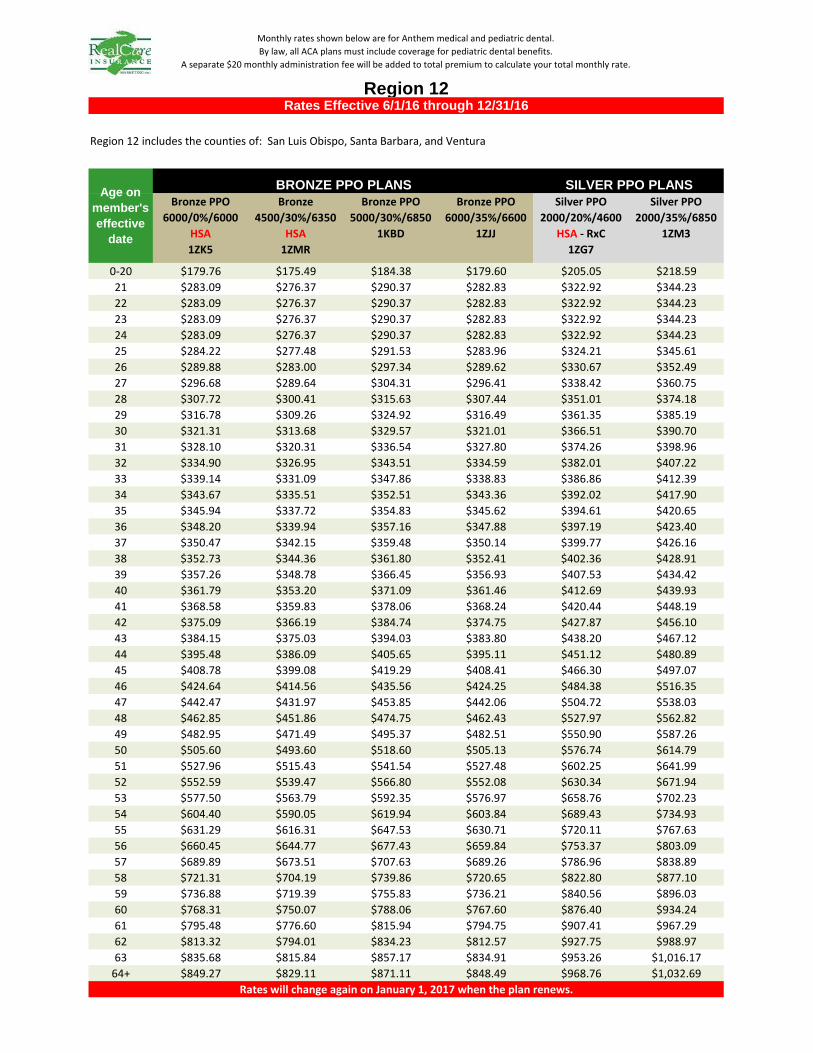
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $179.76 $175.49 $184.38 $179.60 $205.05 $218.5921 $283.09 $276.37 $290.37 $282.83 $322.92 $344.2322 $283.09 $276.37 $290.37 $282.83 $322.92 $344.2323 $283.09 $276.37 $290.37 $282.83 $322.92 $344.2324 $283.09 $276.37 $290.37 $282.83 $322.92 $344.2325 $284.22 $277.48 $291.53 $283.96 $324.21 $345.6126 $289.88 $283.00 $297.34 $289.62 $330.67 $352.4927 $296.68 $289.64 $304.31 $296.41 $338.42 $360.7528 $307.72 $300.41 $315.63 $307.44 $351.01 $374.1829 $316.78 $309.26 $324.92 $316.49 $361.35 $385.1930 $321.31 $313.68 $329.57 $321.01 $366.51 $390.7031 $328.10 $320.31 $336.54 $327.80 $374.26 $398.9632 $334.90 $326.95 $343.51 $334.59 $382.01 $407.2233 $339.14 $331.09 $347.86 $338.83 $386.86 $412.3934 $343.67 $335.51 $352.51 $343.36 $392.02 $417.9035 $345.94 $337.72 $354.83 $345.62 $394.61 $420.6536 $348.20 $339.94 $357.16 $347.88 $397.19 $423.4037 $350.47 $342.15 $359.48 $350.14 $399.77 $426.1638 $352.73 $344.36 $361.80 $352.41 $402.36 $428.9139 $357.26 $348.78 $366.45 $356.93 $407.53 $434.4240 $361.79 $353.20 $371.09 $361.46 $412.69 $439.9341 $368.58 $359.83 $378.06 $368.24 $420.44 $448.1942 $375.09 $366.19 $384.74 $374.75 $427.87 $456.1043 $384.15 $375.03 $394.03 $383.80 $438.20 $467.1244 $395.48 $386.09 $405.65 $395.11 $451.12 $480.8945 $408.78 $399.08 $419.29 $408.41 $466.30 $497.0746 $424.64 $414.56 $435.56 $424.25 $484.38 $516.3547 $442.47 $431.97 $453.85 $442.06 $504.72 $538.0348 $462.85 $451.86 $474.75 $462.43 $527.97 $562.8249 $482.95 $471.49 $495.37 $482.51 $550.90 $587.2650 $505.60 $493.60 $518.60 $505.13 $576.74 $614.7951 $527.96 $515.43 $541.54 $527.48 $602.25 $641.9952 $552.59 $539.47 $566.80 $552.08 $630.34 $671.9453 $577.50 $563.79 $592.35 $576.97 $658.76 $702.2354 $604.40 $590.05 $619.94 $603.84 $689.43 $734.9355 $631.29 $616.31 $647.53 $630.71 $720.11 $767.6356 $660.45 $644.77 $677.43 $659.84 $753.37 $803.0957 $689.89 $673.51 $707.63 $689.26 $786.96 $838.8958 $721.31 $704.19 $739.86 $720.65 $822.80 $877.1059 $736.88 $719.39 $755.83 $736.21 $840.56 $896.0360 $768.31 $750.07 $788.06 $767.60 $876.40 $934.2461 $795.48 $776.60 $815.94 $794.75 $907.41 $967.2962 $813.32 $794.01 $834.23 $812.57 $927.75 $988.9763 $835.68 $815.84 $857.17 $834.91 $953.26 $1,016.17
64+ $849.27 $829.11 $871.11 $848.49 $968.76 $1,032.69
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 12
Region 12 includes the counties of: San Luis Obispo, Santa Barbara, and Ventura
BRONZE PPO PLANS
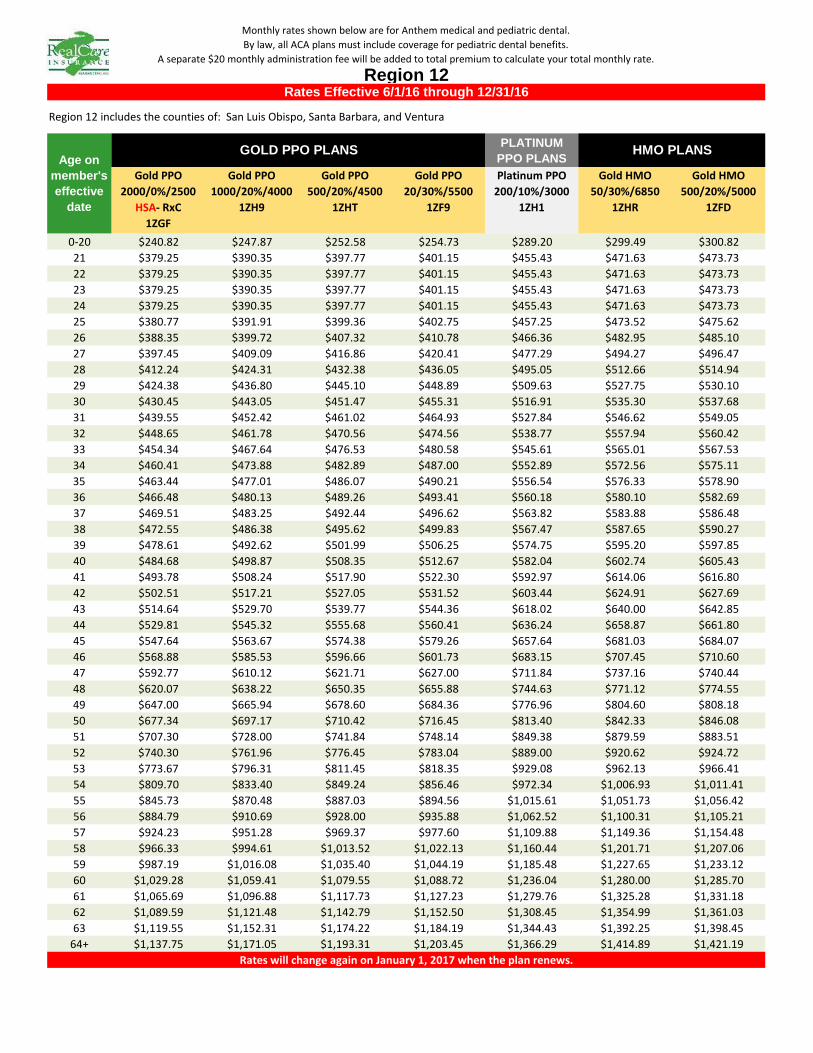
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $240.82 $247.87 $252.58 $254.73 $289.20 $299.49 $300.8221 $379.25 $390.35 $397.77 $401.15 $455.43 $471.63 $473.7322 $379.25 $390.35 $397.77 $401.15 $455.43 $471.63 $473.7323 $379.25 $390.35 $397.77 $401.15 $455.43 $471.63 $473.7324 $379.25 $390.35 $397.77 $401.15 $455.43 $471.63 $473.7325 $380.77 $391.91 $399.36 $402.75 $457.25 $473.52 $475.6226 $388.35 $399.72 $407.32 $410.78 $466.36 $482.95 $485.1027 $397.45 $409.09 $416.86 $420.41 $477.29 $494.27 $496.4728 $412.24 $424.31 $432.38 $436.05 $495.05 $512.66 $514.9429 $424.38 $436.80 $445.10 $448.89 $509.63 $527.75 $530.1030 $430.45 $443.05 $451.47 $455.31 $516.91 $535.30 $537.6831 $439.55 $452.42 $461.02 $464.93 $527.84 $546.62 $549.0532 $448.65 $461.78 $470.56 $474.56 $538.77 $557.94 $560.4233 $454.34 $467.64 $476.53 $480.58 $545.61 $565.01 $567.5334 $460.41 $473.88 $482.89 $487.00 $552.89 $572.56 $575.1135 $463.44 $477.01 $486.07 $490.21 $556.54 $576.33 $578.9036 $466.48 $480.13 $489.26 $493.41 $560.18 $580.10 $582.6937 $469.51 $483.25 $492.44 $496.62 $563.82 $583.88 $586.4838 $472.55 $486.38 $495.62 $499.83 $567.47 $587.65 $590.2739 $478.61 $492.62 $501.99 $506.25 $574.75 $595.20 $597.8540 $484.68 $498.87 $508.35 $512.67 $582.04 $602.74 $605.4341 $493.78 $508.24 $517.90 $522.30 $592.97 $614.06 $616.8042 $502.51 $517.21 $527.05 $531.52 $603.44 $624.91 $627.6943 $514.64 $529.70 $539.77 $544.36 $618.02 $640.00 $642.8544 $529.81 $545.32 $555.68 $560.41 $636.24 $658.87 $661.8045 $547.64 $563.67 $574.38 $579.26 $657.64 $681.03 $684.0746 $568.88 $585.53 $596.66 $601.73 $683.15 $707.45 $710.6047 $592.77 $610.12 $621.71 $627.00 $711.84 $737.16 $740.4448 $620.07 $638.22 $650.35 $655.88 $744.63 $771.12 $774.5549 $647.00 $665.94 $678.60 $684.36 $776.96 $804.60 $808.1850 $677.34 $697.17 $710.42 $716.45 $813.40 $842.33 $846.0851 $707.30 $728.00 $741.84 $748.14 $849.38 $879.59 $883.5152 $740.30 $761.96 $776.45 $783.04 $889.00 $920.62 $924.7253 $773.67 $796.31 $811.45 $818.35 $929.08 $962.13 $966.4154 $809.70 $833.40 $849.24 $856.46 $972.34 $1,006.93 $1,011.4155 $845.73 $870.48 $887.03 $894.56 $1,015.61 $1,051.73 $1,056.4256 $884.79 $910.69 $928.00 $935.88 $1,062.52 $1,100.31 $1,105.2157 $924.23 $951.28 $969.37 $977.60 $1,109.88 $1,149.36 $1,154.4858 $966.33 $994.61 $1,013.52 $1,022.13 $1,160.44 $1,201.71 $1,207.0659 $987.19 $1,016.08 $1,035.40 $1,044.19 $1,185.48 $1,227.65 $1,233.1260 $1,029.28 $1,059.41 $1,079.55 $1,088.72 $1,236.04 $1,280.00 $1,285.7061 $1,065.69 $1,096.88 $1,117.73 $1,127.23 $1,279.76 $1,325.28 $1,331.1862 $1,089.59 $1,121.48 $1,142.79 $1,152.50 $1,308.45 $1,354.99 $1,361.0363 $1,119.55 $1,152.31 $1,174.22 $1,184.19 $1,344.43 $1,392.25 $1,398.45
64+ $1,137.75 $1,171.05 $1,193.31 $1,203.45 $1,366.29 $1,414.89 $1,421.19
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 12
Region 12 includes the counties of: San Luis Obispo, Santa Barbara, and Ventura
Age on member's effective
date
GOLD PPO PLANS
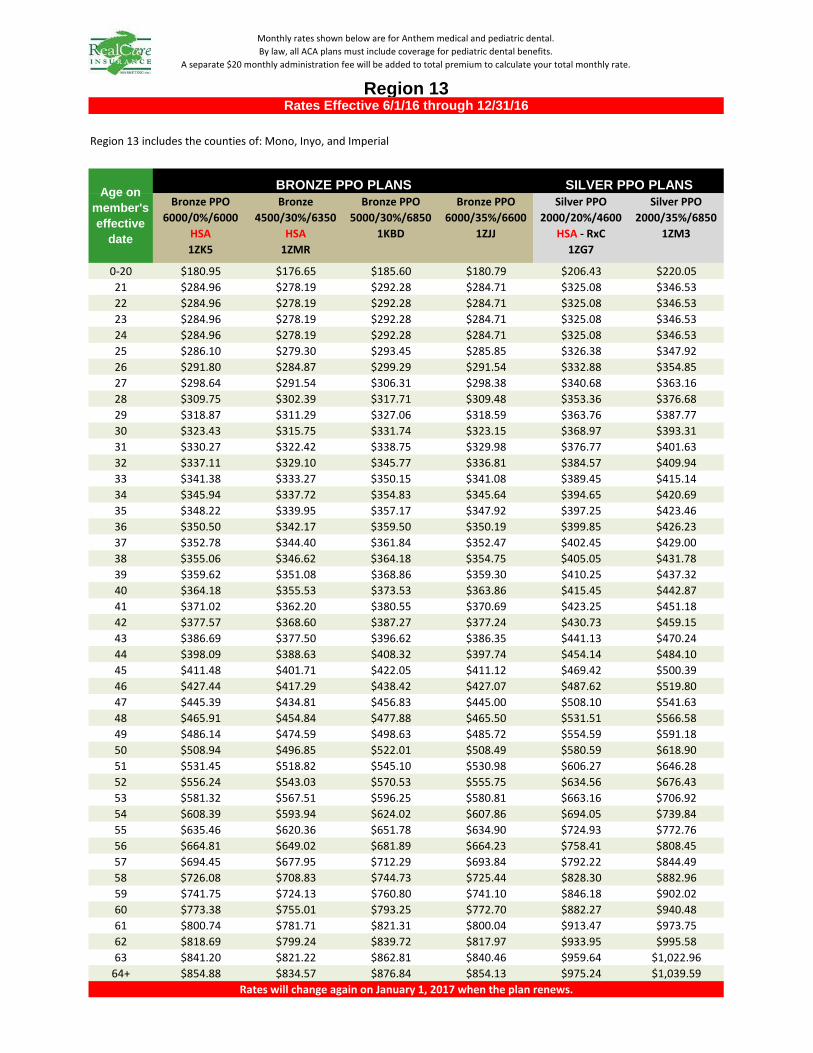
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $180.95 $176.65 $185.60 $180.79 $206.43 $220.0521 $284.96 $278.19 $292.28 $284.71 $325.08 $346.5322 $284.96 $278.19 $292.28 $284.71 $325.08 $346.5323 $284.96 $278.19 $292.28 $284.71 $325.08 $346.5324 $284.96 $278.19 $292.28 $284.71 $325.08 $346.5325 $286.10 $279.30 $293.45 $285.85 $326.38 $347.9226 $291.80 $284.87 $299.29 $291.54 $332.88 $354.8527 $298.64 $291.54 $306.31 $298.38 $340.68 $363.1628 $309.75 $302.39 $317.71 $309.48 $353.36 $376.6829 $318.87 $311.29 $327.06 $318.59 $363.76 $387.7730 $323.43 $315.75 $331.74 $323.15 $368.97 $393.3131 $330.27 $322.42 $338.75 $329.98 $376.77 $401.6332 $337.11 $329.10 $345.77 $336.81 $384.57 $409.9433 $341.38 $333.27 $350.15 $341.08 $389.45 $415.1434 $345.94 $337.72 $354.83 $345.64 $394.65 $420.6935 $348.22 $339.95 $357.17 $347.92 $397.25 $423.4636 $350.50 $342.17 $359.50 $350.19 $399.85 $426.2337 $352.78 $344.40 $361.84 $352.47 $402.45 $429.0038 $355.06 $346.62 $364.18 $354.75 $405.05 $431.7839 $359.62 $351.08 $368.86 $359.30 $410.25 $437.3240 $364.18 $355.53 $373.53 $363.86 $415.45 $442.8741 $371.02 $362.20 $380.55 $370.69 $423.25 $451.1842 $377.57 $368.60 $387.27 $377.24 $430.73 $459.1543 $386.69 $377.50 $396.62 $386.35 $441.13 $470.2444 $398.09 $388.63 $408.32 $397.74 $454.14 $484.1045 $411.48 $401.71 $422.05 $411.12 $469.42 $500.3946 $427.44 $417.29 $438.42 $427.07 $487.62 $519.8047 $445.39 $434.81 $456.83 $445.00 $508.10 $541.6348 $465.91 $454.84 $477.88 $465.50 $531.51 $566.5849 $486.14 $474.59 $498.63 $485.72 $554.59 $591.1850 $508.94 $496.85 $522.01 $508.49 $580.59 $618.9051 $531.45 $518.82 $545.10 $530.98 $606.27 $646.2852 $556.24 $543.03 $570.53 $555.75 $634.56 $676.4353 $581.32 $567.51 $596.25 $580.81 $663.16 $706.9254 $608.39 $593.94 $624.02 $607.86 $694.05 $739.8455 $635.46 $620.36 $651.78 $634.90 $724.93 $772.7656 $664.81 $649.02 $681.89 $664.23 $758.41 $808.4557 $694.45 $677.95 $712.29 $693.84 $792.22 $844.4958 $726.08 $708.83 $744.73 $725.44 $828.30 $882.9659 $741.75 $724.13 $760.80 $741.10 $846.18 $902.0260 $773.38 $755.01 $793.25 $772.70 $882.27 $940.4861 $800.74 $781.71 $821.31 $800.04 $913.47 $973.7562 $818.69 $799.24 $839.72 $817.97 $933.95 $995.5863 $841.20 $821.22 $862.81 $840.46 $959.64 $1,022.96
64+ $854.88 $834.57 $876.84 $854.13 $975.24 $1,039.59
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 13
Region 13 includes the counties of: Mono, Inyo, and Imperial
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $242.43 $249.52 $254.26 $256.42 $291.12 $269.81 $271.0221 $381.78 $392.94 $400.41 $403.81 $458.46 $424.90 $426.8022 $381.78 $392.94 $400.41 $403.81 $458.46 $424.90 $426.8023 $381.78 $392.94 $400.41 $403.81 $458.46 $424.90 $426.8024 $381.78 $392.94 $400.41 $403.81 $458.46 $424.90 $426.8025 $383.31 $394.51 $402.01 $405.43 $460.29 $426.60 $428.5126 $390.94 $402.37 $410.02 $413.50 $469.46 $435.10 $437.0427 $400.11 $411.80 $419.63 $423.19 $480.47 $445.30 $447.2928 $414.99 $427.13 $435.25 $438.94 $498.35 $461.87 $463.9329 $427.21 $439.70 $448.06 $451.86 $513.02 $475.46 $477.5930 $433.32 $445.99 $454.47 $458.32 $520.35 $482.26 $484.4231 $442.48 $455.42 $464.08 $468.02 $531.36 $492.46 $494.6632 $451.65 $464.85 $473.69 $477.71 $542.36 $502.66 $504.9033 $457.37 $470.74 $479.69 $483.76 $549.24 $509.03 $511.3134 $463.48 $477.03 $486.10 $490.23 $556.57 $515.83 $518.1435 $466.54 $480.17 $489.30 $493.46 $560.24 $519.23 $521.5536 $469.59 $483.32 $492.50 $496.69 $563.91 $522.63 $524.9637 $472.64 $486.46 $495.71 $499.92 $567.57 $526.03 $528.3838 $475.70 $489.60 $498.91 $503.15 $571.24 $529.43 $531.7939 $481.81 $495.89 $505.32 $509.61 $578.58 $536.22 $538.6240 $487.91 $502.18 $511.72 $516.07 $585.91 $543.02 $545.4541 $497.08 $511.61 $521.33 $525.76 $596.91 $553.22 $555.6942 $505.86 $520.65 $530.54 $535.05 $607.46 $562.99 $565.5143 $518.08 $533.22 $543.36 $547.97 $622.13 $576.59 $579.1744 $533.35 $548.94 $559.37 $564.12 $640.47 $593.59 $596.2445 $551.29 $567.41 $578.19 $583.10 $662.02 $613.56 $616.3046 $572.67 $589.41 $600.62 $605.72 $687.69 $637.35 $640.2047 $596.72 $614.17 $625.84 $631.16 $716.57 $664.12 $667.0948 $624.21 $642.46 $654.67 $660.23 $749.58 $694.71 $697.8249 $651.32 $670.36 $683.10 $688.90 $782.13 $724.88 $728.1250 $681.86 $701.79 $715.13 $721.20 $818.81 $758.87 $762.2651 $712.02 $732.83 $746.76 $753.11 $855.03 $792.44 $795.9852 $745.23 $767.02 $781.60 $788.24 $894.91 $829.40 $833.1153 $778.83 $801.60 $816.84 $823.77 $935.26 $866.80 $870.6754 $815.10 $838.93 $854.88 $862.13 $978.81 $907.16 $911.2255 $851.37 $876.26 $892.91 $900.50 $1,022.37 $947.53 $951.7656 $890.69 $916.73 $934.16 $942.09 $1,069.59 $991.29 $995.7257 $930.40 $957.59 $975.80 $984.08 $1,117.27 $1,035.48 $1,040.1158 $972.78 $1,001.21 $1,020.24 $1,028.91 $1,168.16 $1,082.65 $1,087.4959 $993.77 $1,022.82 $1,042.27 $1,051.12 $1,193.37 $1,106.01 $1,110.9660 $1,036.15 $1,066.44 $1,086.71 $1,095.94 $1,244.26 $1,153.18 $1,158.3461 $1,072.80 $1,104.16 $1,125.15 $1,134.71 $1,288.27 $1,193.97 $1,199.3162 $1,096.85 $1,128.92 $1,150.38 $1,160.15 $1,317.16 $1,220.74 $1,226.2063 $1,127.01 $1,159.96 $1,182.01 $1,192.05 $1,353.37 $1,254.30 $1,259.91
64+ $1,145.34 $1,178.82 $1,201.23 $1,211.43 $1,375.38 $1,274.70 $1,280.40
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 13
Region 13 includes the counties of: Mono, Inyo, and Imperial
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $150.51 $146.94 $154.38 $150.37 $171.69 $183.0321 $237.03 $231.40 $243.12 $236.81 $270.38 $288.2422 $237.03 $231.40 $243.12 $236.81 $270.38 $288.2423 $237.03 $231.40 $243.12 $236.81 $270.38 $288.2424 $237.03 $231.40 $243.12 $236.81 $270.38 $288.2425 $237.98 $232.33 $244.09 $237.76 $271.46 $289.3926 $242.72 $236.95 $248.95 $242.49 $276.87 $295.1627 $248.41 $242.51 $254.79 $248.18 $283.36 $302.0828 $257.65 $251.53 $264.27 $257.41 $293.90 $313.3229 $265.24 $258.94 $272.05 $264.99 $302.56 $322.5430 $269.03 $262.64 $275.94 $268.78 $306.88 $327.1531 $274.72 $268.19 $281.78 $274.46 $313.37 $334.0732 $280.41 $273.75 $287.61 $280.15 $319.86 $340.9933 $283.96 $277.22 $291.26 $283.70 $323.92 $345.3134 $287.75 $280.92 $295.15 $287.49 $328.24 $349.9235 $289.65 $282.77 $297.09 $289.38 $330.40 $352.2336 $291.55 $284.62 $299.04 $291.28 $332.57 $354.5437 $293.44 $286.47 $300.98 $293.17 $334.73 $356.8438 $295.34 $288.32 $302.93 $295.07 $336.89 $359.1539 $299.13 $292.03 $306.82 $298.85 $341.22 $363.7640 $302.92 $295.73 $310.71 $302.64 $345.55 $368.3741 $308.61 $301.28 $316.54 $308.33 $352.03 $375.2942 $314.06 $306.61 $322.13 $313.77 $358.25 $381.9243 $321.65 $314.01 $329.91 $321.35 $366.91 $391.1444 $331.13 $323.27 $339.64 $330.82 $377.72 $402.6745 $342.27 $334.14 $351.07 $341.95 $390.43 $416.2246 $355.55 $347.10 $364.68 $355.22 $405.57 $432.3647 $370.48 $361.68 $380.00 $370.13 $422.60 $450.5248 $387.54 $378.34 $397.50 $387.18 $442.07 $471.2749 $404.37 $394.77 $414.76 $404.00 $461.27 $491.7450 $423.34 $413.28 $434.21 $422.94 $482.90 $514.8051 $442.06 $431.56 $453.42 $441.65 $504.26 $537.5752 $462.68 $451.69 $474.57 $462.25 $527.78 $562.6453 $483.54 $472.06 $495.96 $483.09 $551.58 $588.0154 $506.06 $494.04 $519.06 $505.59 $577.26 $615.3955 $528.58 $516.02 $542.16 $528.09 $602.95 $642.7856 $552.99 $539.86 $567.20 $552.48 $630.80 $672.4657 $577.64 $563.92 $592.48 $577.11 $658.92 $702.4458 $603.95 $589.61 $619.47 $603.39 $688.93 $734.4459 $616.99 $602.33 $632.84 $616.42 $703.80 $750.2960 $643.30 $628.02 $659.83 $642.70 $733.81 $782.2861 $666.05 $650.23 $683.17 $665.44 $759.77 $809.9562 $680.99 $664.81 $698.48 $680.36 $776.80 $828.1163 $699.71 $683.09 $717.69 $699.06 $798.16 $850.88
64+ $711.09 $694.20 $729.36 $710.43 $811.14 $864.72
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 14
Region 14 includes the county of: Kern
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $201.66 $207.55 $211.49 $213.29 $242.16 $299.35 $300.7021 $317.57 $326.85 $333.06 $335.89 $381.35 $471.42 $473.5422 $317.57 $326.85 $333.06 $335.89 $381.35 $471.42 $473.5423 $317.57 $326.85 $333.06 $335.89 $381.35 $471.42 $473.5424 $317.57 $326.85 $333.06 $335.89 $381.35 $471.42 $473.5425 $318.84 $328.16 $334.39 $337.23 $382.88 $473.31 $475.4326 $325.19 $334.69 $341.05 $343.95 $390.50 $482.73 $484.9027 $332.81 $342.54 $349.05 $352.01 $399.65 $494.05 $496.2728 $345.20 $355.29 $362.04 $365.11 $414.53 $512.43 $514.7429 $355.36 $365.75 $372.69 $375.86 $426.73 $527.52 $529.8930 $360.44 $370.97 $378.02 $381.24 $432.83 $535.06 $537.4731 $368.06 $378.82 $386.02 $389.30 $441.98 $546.38 $548.8332 $375.69 $386.66 $394.01 $397.36 $451.14 $557.69 $560.2033 $380.45 $391.57 $399.01 $402.40 $456.86 $564.76 $567.3034 $385.53 $396.80 $404.33 $407.77 $462.96 $572.30 $574.8835 $388.07 $399.41 $407.00 $410.46 $466.01 $576.08 $578.6736 $390.61 $402.03 $409.66 $413.14 $469.06 $579.85 $582.4537 $393.15 $404.64 $412.33 $415.83 $472.11 $583.62 $586.2438 $395.69 $407.26 $414.99 $418.52 $475.16 $587.39 $590.0339 $400.77 $412.48 $420.32 $423.89 $481.26 $594.93 $597.6140 $405.85 $417.71 $425.65 $429.27 $487.37 $602.47 $605.1841 $413.48 $425.56 $433.64 $437.33 $496.52 $613.79 $616.5542 $420.78 $433.08 $441.30 $445.05 $505.29 $624.63 $627.4443 $430.94 $443.54 $451.96 $455.80 $517.49 $639.72 $642.5944 $443.65 $456.61 $465.28 $469.24 $532.75 $658.57 $661.5445 $458.57 $471.97 $480.94 $485.03 $550.67 $680.73 $683.7946 $476.36 $490.28 $499.59 $503.84 $572.03 $707.13 $710.3147 $496.36 $510.87 $520.57 $525.00 $596.05 $736.83 $740.1448 $519.23 $534.40 $544.55 $549.18 $623.51 $770.77 $774.2449 $541.77 $557.61 $568.20 $573.03 $650.58 $804.24 $807.8650 $567.18 $583.75 $594.85 $599.90 $681.09 $841.96 $845.7451 $592.27 $609.58 $621.16 $626.43 $711.22 $879.20 $883.1552 $619.90 $638.01 $650.13 $655.66 $744.40 $920.21 $924.3553 $647.84 $666.77 $679.44 $685.22 $777.95 $961.70 $966.0254 $678.01 $697.82 $711.08 $717.13 $814.18 $1,006.48 $1,011.0155 $708.18 $728.88 $742.72 $749.03 $850.41 $1,051.27 $1,055.9956 $740.89 $762.54 $777.03 $783.63 $889.69 $1,099.82 $1,104.7757 $773.92 $796.53 $811.67 $818.56 $929.35 $1,148.85 $1,154.0258 $809.17 $832.81 $848.64 $855.85 $971.68 $1,201.18 $1,206.5859 $826.63 $850.79 $866.96 $874.32 $992.65 $1,227.11 $1,232.6260 $861.88 $887.07 $903.92 $911.61 $1,034.98 $1,279.43 $1,285.1961 $892.37 $918.45 $935.90 $943.85 $1,071.59 $1,324.69 $1,330.6562 $912.38 $939.04 $956.88 $965.01 $1,095.62 $1,354.39 $1,360.4863 $937.47 $964.86 $983.19 $991.55 $1,125.75 $1,391.63 $1,397.89
64+ $952.71 $980.55 $999.18 $1,007.67 $1,144.05 $1,414.26 $1,420.62
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 14
Region 14 includes the county of: Kern
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $148.54 $145.02 $152.34 $148.41 $169.44 $180.6321 $233.92 $228.38 $239.91 $233.71 $266.83 $284.4622 $233.92 $228.38 $239.91 $233.71 $266.83 $284.4623 $233.92 $228.38 $239.91 $233.71 $266.83 $284.4624 $233.92 $228.38 $239.91 $233.71 $266.83 $284.4625 $234.86 $229.29 $240.87 $234.64 $267.90 $285.6026 $239.53 $233.86 $245.67 $239.32 $273.23 $291.2927 $245.15 $239.34 $251.43 $244.93 $279.64 $298.1128 $254.27 $248.25 $260.78 $254.04 $290.04 $309.2129 $261.76 $255.56 $268.46 $261.52 $298.58 $318.3130 $265.50 $259.21 $272.30 $265.26 $302.85 $322.8631 $271.11 $264.69 $278.06 $270.87 $309.26 $329.6932 $276.73 $270.17 $283.81 $276.48 $315.66 $336.5233 $280.24 $273.60 $287.41 $279.98 $319.66 $340.7834 $283.98 $277.25 $291.25 $283.72 $323.93 $345.3335 $285.85 $279.08 $293.17 $285.59 $326.07 $347.6136 $287.72 $280.91 $295.09 $287.46 $328.20 $349.8937 $289.59 $282.73 $297.01 $289.33 $330.34 $352.1638 $291.46 $284.56 $298.93 $291.20 $332.47 $354.4439 $295.21 $288.22 $302.77 $294.94 $336.74 $358.9940 $298.95 $291.87 $306.60 $298.68 $341.01 $363.5441 $304.56 $297.35 $312.36 $304.29 $347.41 $370.3742 $309.94 $302.60 $317.88 $309.67 $353.55 $376.9143 $317.43 $309.91 $325.56 $317.14 $362.09 $386.0144 $326.79 $319.05 $335.15 $326.49 $372.76 $397.3945 $337.78 $329.78 $346.43 $337.48 $385.30 $410.7646 $350.88 $342.57 $359.87 $350.57 $400.25 $426.6947 $365.62 $356.96 $374.98 $365.29 $417.06 $444.6148 $382.46 $373.40 $392.25 $382.12 $436.27 $465.0949 $399.07 $389.62 $409.29 $398.71 $455.21 $485.2950 $417.78 $407.89 $428.48 $417.41 $476.56 $508.0551 $436.26 $425.93 $447.43 $435.87 $497.64 $530.5252 $456.61 $445.80 $468.30 $456.20 $520.85 $555.2753 $477.20 $465.90 $489.42 $476.77 $544.33 $580.3054 $499.42 $487.59 $512.21 $498.97 $569.68 $607.3255 $521.64 $509.29 $535.00 $521.17 $595.03 $634.3556 $545.74 $532.81 $559.71 $545.25 $622.51 $663.6557 $570.06 $556.56 $584.66 $569.55 $650.26 $693.2358 $596.03 $581.91 $611.29 $595.49 $679.88 $724.8059 $608.89 $594.47 $624.49 $608.35 $694.56 $740.4560 $634.86 $619.82 $651.12 $634.29 $724.18 $772.0261 $657.32 $641.75 $674.15 $656.73 $749.79 $799.3362 $672.05 $656.14 $689.26 $671.45 $766.60 $817.2563 $690.53 $674.18 $708.21 $689.91 $787.68 $839.73
64+ $701.76 $685.14 $719.73 $701.13 $800.49 $853.38
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 15
Region 15 includes: The zip codes in Los Angeles County starting with 906 to 912, inclusive, 915, 917, 918, and 935.
BRONZE PPO PLANS
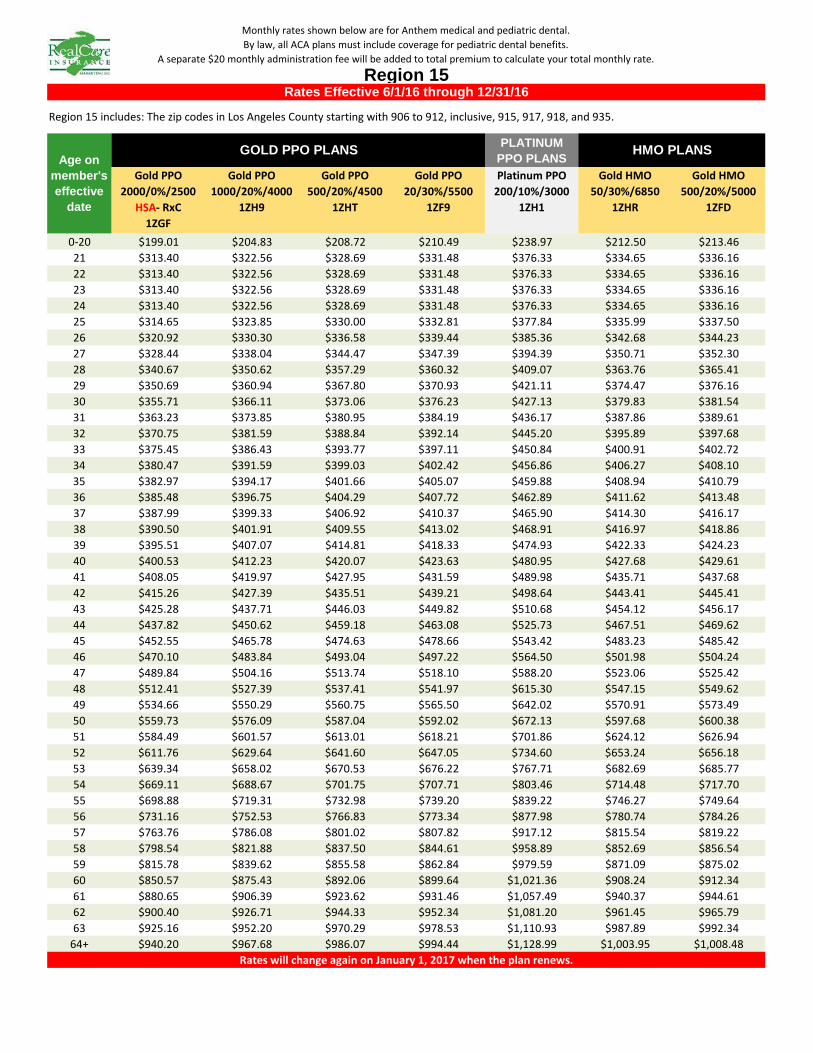
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $199.01 $204.83 $208.72 $210.49 $238.97 $212.50 $213.4621 $313.40 $322.56 $328.69 $331.48 $376.33 $334.65 $336.1622 $313.40 $322.56 $328.69 $331.48 $376.33 $334.65 $336.1623 $313.40 $322.56 $328.69 $331.48 $376.33 $334.65 $336.1624 $313.40 $322.56 $328.69 $331.48 $376.33 $334.65 $336.1625 $314.65 $323.85 $330.00 $332.81 $377.84 $335.99 $337.5026 $320.92 $330.30 $336.58 $339.44 $385.36 $342.68 $344.2327 $328.44 $338.04 $344.47 $347.39 $394.39 $350.71 $352.3028 $340.67 $350.62 $357.29 $360.32 $409.07 $363.76 $365.4129 $350.69 $360.94 $367.80 $370.93 $421.11 $374.47 $376.1630 $355.71 $366.11 $373.06 $376.23 $427.13 $379.83 $381.5431 $363.23 $373.85 $380.95 $384.19 $436.17 $387.86 $389.6132 $370.75 $381.59 $388.84 $392.14 $445.20 $395.89 $397.6833 $375.45 $386.43 $393.77 $397.11 $450.84 $400.91 $402.7234 $380.47 $391.59 $399.03 $402.42 $456.86 $406.27 $408.1035 $382.97 $394.17 $401.66 $405.07 $459.88 $408.94 $410.7936 $385.48 $396.75 $404.29 $407.72 $462.89 $411.62 $413.4837 $387.99 $399.33 $406.92 $410.37 $465.90 $414.30 $416.1738 $390.50 $401.91 $409.55 $413.02 $468.91 $416.97 $418.8639 $395.51 $407.07 $414.81 $418.33 $474.93 $422.33 $424.2340 $400.53 $412.23 $420.07 $423.63 $480.95 $427.68 $429.6141 $408.05 $419.97 $427.95 $431.59 $489.98 $435.71 $437.6842 $415.26 $427.39 $435.51 $439.21 $498.64 $443.41 $445.4143 $425.28 $437.71 $446.03 $449.82 $510.68 $454.12 $456.1744 $437.82 $450.62 $459.18 $463.08 $525.73 $467.51 $469.6245 $452.55 $465.78 $474.63 $478.66 $543.42 $483.23 $485.4246 $470.10 $483.84 $493.04 $497.22 $564.50 $501.98 $504.2447 $489.84 $504.16 $513.74 $518.10 $588.20 $523.06 $525.4248 $512.41 $527.39 $537.41 $541.97 $615.30 $547.15 $549.6249 $534.66 $550.29 $560.75 $565.50 $642.02 $570.91 $573.4950 $559.73 $576.09 $587.04 $592.02 $672.13 $597.68 $600.3851 $584.49 $601.57 $613.01 $618.21 $701.86 $624.12 $626.9452 $611.76 $629.64 $641.60 $647.05 $734.60 $653.24 $656.1853 $639.34 $658.02 $670.53 $676.22 $767.71 $682.69 $685.7754 $669.11 $688.67 $701.75 $707.71 $803.46 $714.48 $717.7055 $698.88 $719.31 $732.98 $739.20 $839.22 $746.27 $749.6456 $731.16 $752.53 $766.83 $773.34 $877.98 $780.74 $784.2657 $763.76 $786.08 $801.02 $807.82 $917.12 $815.54 $819.2258 $798.54 $821.88 $837.50 $844.61 $958.89 $852.69 $856.5459 $815.78 $839.62 $855.58 $862.84 $979.59 $871.09 $875.0260 $850.57 $875.43 $892.06 $899.64 $1,021.36 $908.24 $912.3461 $880.65 $906.39 $923.62 $931.46 $1,057.49 $940.37 $944.6162 $900.40 $926.71 $944.33 $952.34 $1,081.20 $961.45 $965.7963 $925.16 $952.20 $970.29 $978.53 $1,110.93 $987.89 $992.34
64+ $940.20 $967.68 $986.07 $994.44 $1,128.99 $1,003.95 $1,008.48
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 15
Region 15 includes: The zip codes in Los Angeles County starting with 906 to 912, inclusive, 915, 917, 918, and 935.
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $181.63 $177.31 $186.28 $181.46 $207.17 $220.8521 $286.03 $279.23 $293.35 $285.77 $326.25 $347.8022 $286.03 $279.23 $293.35 $285.77 $326.25 $347.8023 $286.03 $279.23 $293.35 $285.77 $326.25 $347.8024 $286.03 $279.23 $293.35 $285.77 $326.25 $347.8025 $287.17 $280.35 $294.52 $286.91 $327.56 $349.1926 $292.89 $285.93 $300.39 $292.63 $334.08 $356.1527 $299.76 $292.63 $307.43 $299.49 $341.91 $364.4928 $310.91 $303.52 $318.87 $310.63 $354.63 $378.0629 $320.07 $312.46 $328.26 $319.78 $365.07 $389.1930 $324.64 $316.93 $332.95 $324.35 $370.29 $394.7531 $331.51 $323.63 $339.99 $331.21 $378.12 $403.1032 $338.37 $330.33 $347.03 $338.07 $385.95 $411.4533 $342.66 $334.52 $351.43 $342.35 $390.85 $416.6634 $347.24 $338.99 $356.13 $346.92 $396.07 $422.2335 $349.53 $341.22 $358.47 $349.21 $398.68 $425.0136 $351.82 $343.45 $360.82 $351.50 $401.29 $427.7937 $354.11 $345.69 $363.17 $353.78 $403.90 $430.5838 $356.39 $347.92 $365.51 $356.07 $406.51 $433.3639 $360.97 $352.39 $370.21 $360.64 $411.73 $438.9240 $365.55 $356.86 $374.90 $365.21 $416.95 $444.4941 $372.41 $363.56 $381.94 $372.07 $424.78 $452.8442 $378.99 $369.98 $388.69 $378.65 $432.28 $460.8443 $388.14 $378.92 $398.08 $387.79 $442.72 $471.9644 $399.58 $390.08 $409.81 $399.22 $455.77 $485.8845 $413.03 $403.21 $423.60 $412.65 $471.11 $502.2246 $429.05 $418.85 $440.03 $428.66 $489.38 $521.7047 $447.06 $436.44 $458.51 $446.66 $509.93 $543.6148 $467.66 $456.54 $479.63 $467.23 $533.42 $568.6549 $487.97 $476.37 $500.46 $487.52 $556.58 $593.3550 $510.85 $498.70 $523.92 $510.39 $582.68 $621.1751 $533.45 $520.76 $547.10 $532.96 $608.46 $648.6552 $558.33 $545.06 $572.62 $557.82 $636.84 $678.9153 $583.50 $569.63 $598.43 $582.97 $665.55 $709.5154 $610.67 $596.16 $626.30 $610.12 $696.54 $742.5555 $637.85 $622.68 $654.17 $637.27 $727.54 $775.5956 $667.31 $651.44 $684.39 $666.70 $761.14 $811.4257 $697.06 $680.48 $714.89 $696.42 $795.07 $847.5958 $728.80 $711.48 $747.46 $728.14 $831.29 $886.1959 $744.54 $726.84 $763.59 $743.86 $849.23 $905.3260 $776.29 $757.83 $796.15 $775.58 $885.44 $943.9361 $803.74 $784.64 $824.31 $803.01 $916.76 $977.3262 $821.76 $802.23 $842.79 $821.02 $937.32 $999.2363 $844.36 $824.29 $865.97 $843.59 $963.09 $1,026.71
64+ $858.09 $837.69 $880.05 $857.31 $978.75 $1,043.40
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 16
Region 16 includes: The zip codes in Los Angeles County other than those identified in Region 15.
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $243.31 $250.42 $255.19 $257.37 $292.18 $220.76 $221.7721 $383.17 $394.37 $401.87 $405.31 $460.13 $347.65 $349.2422 $383.17 $394.37 $401.87 $405.31 $460.13 $347.65 $349.2423 $383.17 $394.37 $401.87 $405.31 $460.13 $347.65 $349.2424 $383.17 $394.37 $401.87 $405.31 $460.13 $347.65 $349.2425 $384.70 $395.95 $403.48 $406.93 $461.97 $349.04 $350.6426 $392.37 $403.83 $411.51 $415.04 $471.17 $355.99 $357.6227 $401.56 $413.30 $421.16 $424.76 $482.22 $364.34 $366.0028 $416.51 $428.68 $436.83 $440.57 $500.16 $377.90 $379.6229 $428.77 $441.30 $449.69 $453.54 $514.89 $389.02 $390.8030 $434.90 $447.61 $456.12 $460.03 $522.25 $394.58 $396.3931 $444.09 $457.07 $465.77 $469.75 $533.29 $402.93 $404.7732 $453.29 $466.54 $475.41 $479.48 $544.33 $411.27 $413.1533 $459.04 $472.46 $481.44 $485.56 $551.24 $416.48 $418.3934 $465.17 $478.77 $487.87 $492.05 $558.60 $422.05 $423.9835 $468.23 $481.92 $491.09 $495.29 $562.28 $424.83 $426.7736 $471.30 $485.08 $494.30 $498.53 $565.96 $427.61 $429.5737 $474.36 $488.23 $497.52 $501.77 $569.64 $430.39 $432.3638 $477.43 $491.39 $500.73 $505.02 $573.32 $433.17 $435.1539 $483.56 $497.69 $507.16 $511.50 $580.68 $438.73 $440.7440 $489.69 $504.00 $513.59 $517.99 $588.05 $444.30 $446.3341 $498.89 $513.47 $523.23 $527.71 $599.09 $452.64 $454.7142 $507.70 $522.54 $532.48 $537.04 $609.67 $460.64 $462.7443 $519.96 $535.16 $545.34 $550.01 $624.40 $471.76 $473.9244 $535.29 $550.93 $561.41 $566.22 $642.80 $485.67 $487.8945 $553.30 $569.47 $580.30 $585.27 $664.43 $502.01 $504.3046 $574.76 $591.56 $602.81 $607.97 $690.20 $521.48 $523.8647 $598.89 $616.40 $628.12 $633.50 $719.18 $543.38 $545.8648 $626.48 $644.79 $657.06 $662.68 $752.31 $568.41 $571.0149 $653.69 $672.80 $685.59 $691.46 $784.98 $593.09 $595.8050 $684.34 $704.34 $717.74 $723.88 $821.79 $620.90 $623.7451 $714.61 $735.50 $749.49 $755.90 $858.14 $648.37 $651.3352 $747.95 $769.81 $784.45 $791.17 $898.17 $678.61 $681.7253 $781.67 $804.51 $819.81 $826.83 $938.67 $709.21 $712.4554 $818.07 $841.98 $857.99 $865.34 $982.38 $742.23 $745.6355 $854.47 $879.45 $896.17 $903.84 $1,026.09 $775.26 $778.8156 $893.94 $920.07 $937.56 $945.59 $1,073.48 $811.07 $814.7857 $933.79 $961.08 $979.36 $987.74 $1,121.34 $847.22 $851.1058 $976.32 $1,004.85 $1,023.96 $1,032.73 $1,172.41 $885.81 $889.8659 $997.39 $1,026.55 $1,046.07 $1,055.02 $1,197.72 $904.93 $909.0760 $1,039.92 $1,070.32 $1,090.68 $1,100.01 $1,248.79 $943.52 $947.8461 $1,076.71 $1,108.18 $1,129.25 $1,138.92 $1,292.97 $976.90 $981.3662 $1,100.85 $1,133.03 $1,154.57 $1,164.46 $1,321.95 $998.80 $1,003.3763 $1,131.12 $1,164.18 $1,186.32 $1,196.48 $1,358.30 $1,026.26 $1,030.96
64+ $1,149.51 $1,183.11 $1,205.61 $1,215.93 $1,380.39 $1,042.95 $1,047.72
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 16
Region 16 includes: The zip codes in Los Angeles County other than those identified in Region 15.
Age on member's effective
date
GOLD PPO PLANS

Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $168.94 $164.93 $173.26 $168.79 $192.70 $205.4221 $266.05 $259.73 $272.85 $265.81 $303.46 $323.4922 $266.05 $259.73 $272.85 $265.81 $303.46 $323.4923 $266.05 $259.73 $272.85 $265.81 $303.46 $323.4924 $266.05 $259.73 $272.85 $265.81 $303.46 $323.4925 $267.11 $260.77 $273.94 $266.87 $304.67 $324.7826 $272.44 $265.96 $279.40 $272.19 $310.74 $331.2527 $278.82 $272.20 $285.95 $278.57 $318.03 $339.0228 $289.20 $282.33 $296.59 $288.94 $329.86 $351.6329 $297.71 $290.64 $305.32 $297.44 $339.57 $361.9930 $301.97 $294.79 $309.68 $301.69 $344.43 $367.1631 $308.35 $301.03 $316.23 $308.07 $351.71 $374.9232 $314.74 $307.26 $322.78 $314.45 $358.99 $382.6933 $318.73 $311.16 $326.87 $318.44 $363.55 $387.5434 $322.98 $315.31 $331.24 $322.69 $368.40 $392.7235 $325.11 $317.39 $333.42 $324.82 $370.83 $395.3036 $327.24 $319.47 $335.61 $326.95 $373.26 $397.8937 $329.37 $321.55 $337.79 $329.07 $375.68 $400.4838 $331.50 $323.62 $339.97 $331.20 $378.11 $403.0739 $335.76 $327.78 $344.34 $335.45 $382.97 $408.2440 $340.01 $331.93 $348.70 $339.71 $387.82 $413.4241 $346.40 $338.17 $355.25 $346.08 $395.10 $421.1842 $352.52 $344.14 $361.53 $352.20 $402.08 $428.6243 $361.03 $352.45 $370.26 $360.70 $411.80 $438.9844 $371.67 $362.84 $381.17 $371.34 $423.93 $451.9245 $384.18 $375.05 $394.00 $383.83 $438.20 $467.1246 $399.08 $389.60 $409.28 $398.72 $455.19 $485.2447 $415.84 $405.96 $426.46 $415.46 $474.31 $505.6148 $434.99 $424.66 $446.11 $434.60 $496.16 $528.9149 $453.88 $443.10 $465.48 $453.47 $517.70 $551.8750 $475.17 $463.88 $487.31 $474.74 $541.98 $577.7551 $496.18 $484.40 $508.87 $495.74 $565.95 $603.3152 $519.33 $506.99 $532.60 $518.86 $592.35 $631.4553 $542.74 $529.85 $556.61 $542.25 $619.06 $659.9254 $568.02 $554.52 $582.53 $567.50 $647.89 $690.6555 $593.29 $579.20 $608.46 $592.76 $676.72 $721.3856 $620.69 $605.95 $636.56 $620.13 $707.97 $754.7057 $648.36 $632.96 $664.94 $647.78 $739.53 $788.3558 $677.90 $661.79 $695.22 $677.28 $773.22 $824.2559 $692.53 $676.08 $710.23 $691.90 $789.91 $842.0460 $722.06 $704.91 $740.51 $721.41 $823.59 $877.9561 $747.60 $729.84 $766.71 $746.93 $852.72 $909.0162 $764.36 $746.20 $783.90 $763.67 $871.84 $929.3963 $785.38 $766.72 $805.45 $784.67 $895.81 $954.94
64+ $798.15 $779.19 $818.55 $797.43 $910.38 $970.47
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 17
Region 17 includes the counties of: San Bernardino and Riverside
BRONZE PPO PLANS
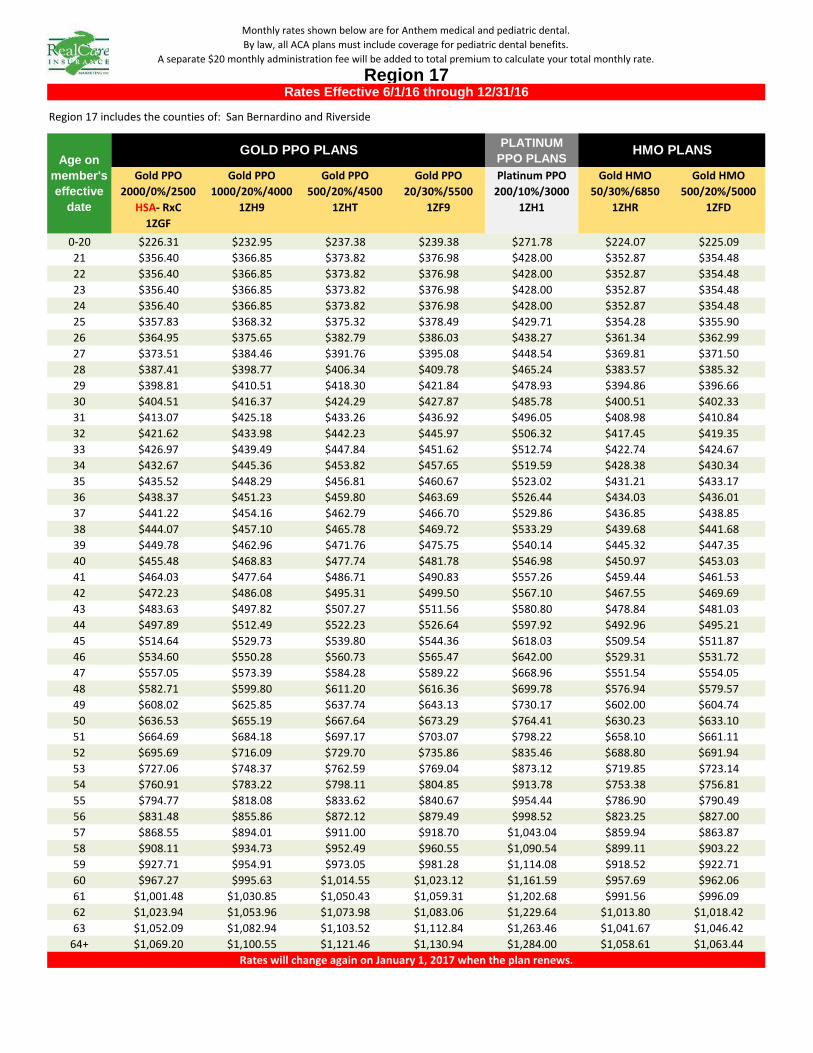
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $226.31 $232.95 $237.38 $239.38 $271.78 $224.07 $225.0921 $356.40 $366.85 $373.82 $376.98 $428.00 $352.87 $354.4822 $356.40 $366.85 $373.82 $376.98 $428.00 $352.87 $354.4823 $356.40 $366.85 $373.82 $376.98 $428.00 $352.87 $354.4824 $356.40 $366.85 $373.82 $376.98 $428.00 $352.87 $354.4825 $357.83 $368.32 $375.32 $378.49 $429.71 $354.28 $355.9026 $364.95 $375.65 $382.79 $386.03 $438.27 $361.34 $362.9927 $373.51 $384.46 $391.76 $395.08 $448.54 $369.81 $371.5028 $387.41 $398.77 $406.34 $409.78 $465.24 $383.57 $385.3229 $398.81 $410.51 $418.30 $421.84 $478.93 $394.86 $396.6630 $404.51 $416.37 $424.29 $427.87 $485.78 $400.51 $402.3331 $413.07 $425.18 $433.26 $436.92 $496.05 $408.98 $410.8432 $421.62 $433.98 $442.23 $445.97 $506.32 $417.45 $419.3533 $426.97 $439.49 $447.84 $451.62 $512.74 $422.74 $424.6734 $432.67 $445.36 $453.82 $457.65 $519.59 $428.38 $430.3435 $435.52 $448.29 $456.81 $460.67 $523.02 $431.21 $433.1736 $438.37 $451.23 $459.80 $463.69 $526.44 $434.03 $436.0137 $441.22 $454.16 $462.79 $466.70 $529.86 $436.85 $438.8538 $444.07 $457.10 $465.78 $469.72 $533.29 $439.68 $441.6839 $449.78 $462.96 $471.76 $475.75 $540.14 $445.32 $447.3540 $455.48 $468.83 $477.74 $481.78 $546.98 $450.97 $453.0341 $464.03 $477.64 $486.71 $490.83 $557.26 $459.44 $461.5342 $472.23 $486.08 $495.31 $499.50 $567.10 $467.55 $469.6943 $483.63 $497.82 $507.27 $511.56 $580.80 $478.84 $481.0344 $497.89 $512.49 $522.23 $526.64 $597.92 $492.96 $495.2145 $514.64 $529.73 $539.80 $544.36 $618.03 $509.54 $511.8746 $534.60 $550.28 $560.73 $565.47 $642.00 $529.31 $531.7247 $557.05 $573.39 $584.28 $589.22 $668.96 $551.54 $554.0548 $582.71 $599.80 $611.20 $616.36 $699.78 $576.94 $579.5749 $608.02 $625.85 $637.74 $643.13 $730.17 $602.00 $604.7450 $636.53 $655.19 $667.64 $673.29 $764.41 $630.23 $633.1051 $664.69 $684.18 $697.17 $703.07 $798.22 $658.10 $661.1152 $695.69 $716.09 $729.70 $735.86 $835.46 $688.80 $691.9453 $727.06 $748.37 $762.59 $769.04 $873.12 $719.85 $723.1454 $760.91 $783.22 $798.11 $804.85 $913.78 $753.38 $756.8155 $794.77 $818.08 $833.62 $840.67 $954.44 $786.90 $790.4956 $831.48 $855.86 $872.12 $879.49 $998.52 $823.25 $827.0057 $868.55 $894.01 $911.00 $918.70 $1,043.04 $859.94 $863.8758 $908.11 $934.73 $952.49 $960.55 $1,090.54 $899.11 $903.2259 $927.71 $954.91 $973.05 $981.28 $1,114.08 $918.52 $922.7160 $967.27 $995.63 $1,014.55 $1,023.12 $1,161.59 $957.69 $962.0661 $1,001.48 $1,030.85 $1,050.43 $1,059.31 $1,202.68 $991.56 $996.0962 $1,023.94 $1,053.96 $1,073.98 $1,083.06 $1,229.64 $1,013.80 $1,018.4263 $1,052.09 $1,082.94 $1,103.52 $1,112.84 $1,263.46 $1,041.67 $1,046.42
64+ $1,069.20 $1,100.55 $1,121.46 $1,130.94 $1,284.00 $1,058.61 $1,063.44
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 17
Region 17 includes the counties of: San Bernardino and Riverside
Age on member's effective
date
GOLD PPO PLANS
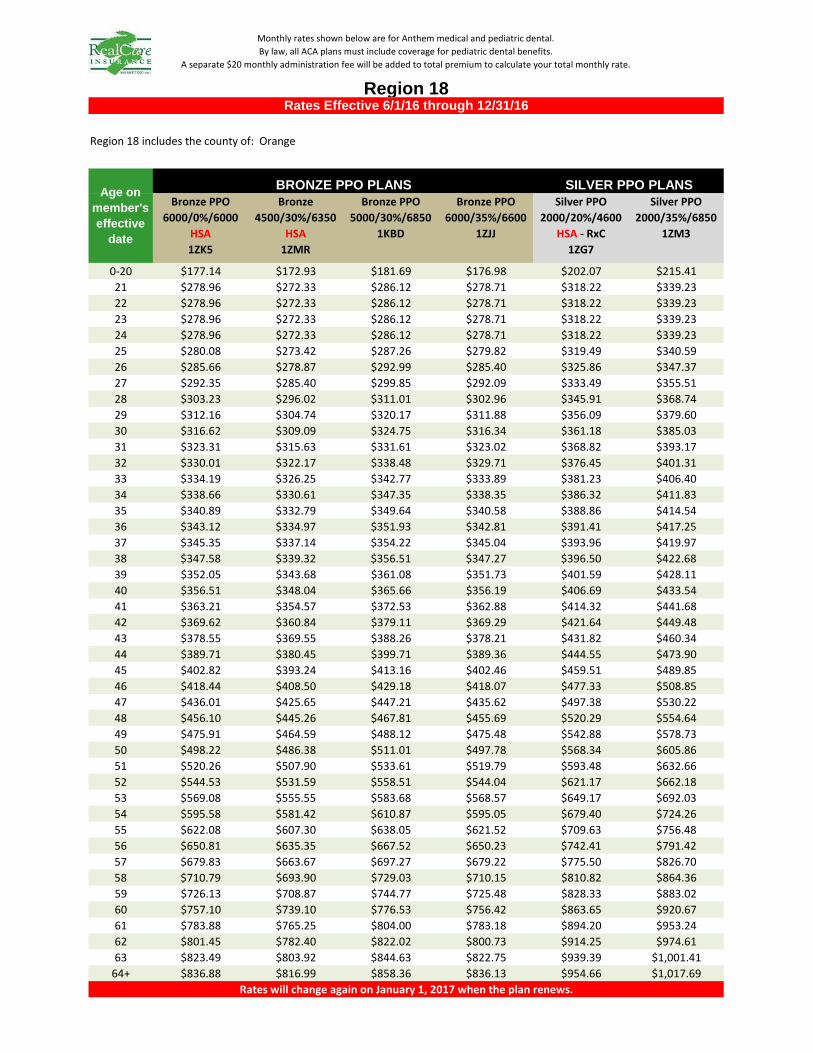
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $177.14 $172.93 $181.69 $176.98 $202.07 $215.4121 $278.96 $272.33 $286.12 $278.71 $318.22 $339.2322 $278.96 $272.33 $286.12 $278.71 $318.22 $339.2323 $278.96 $272.33 $286.12 $278.71 $318.22 $339.2324 $278.96 $272.33 $286.12 $278.71 $318.22 $339.2325 $280.08 $273.42 $287.26 $279.82 $319.49 $340.5926 $285.66 $278.87 $292.99 $285.40 $325.86 $347.3727 $292.35 $285.40 $299.85 $292.09 $333.49 $355.5128 $303.23 $296.02 $311.01 $302.96 $345.91 $368.7429 $312.16 $304.74 $320.17 $311.88 $356.09 $379.6030 $316.62 $309.09 $324.75 $316.34 $361.18 $385.0331 $323.31 $315.63 $331.61 $323.02 $368.82 $393.1732 $330.01 $322.17 $338.48 $329.71 $376.45 $401.3133 $334.19 $326.25 $342.77 $333.89 $381.23 $406.4034 $338.66 $330.61 $347.35 $338.35 $386.32 $411.8335 $340.89 $332.79 $349.64 $340.58 $388.86 $414.5436 $343.12 $334.97 $351.93 $342.81 $391.41 $417.2537 $345.35 $337.14 $354.22 $345.04 $393.96 $419.9738 $347.58 $339.32 $356.51 $347.27 $396.50 $422.6839 $352.05 $343.68 $361.08 $351.73 $401.59 $428.1140 $356.51 $348.04 $365.66 $356.19 $406.69 $433.5441 $363.21 $354.57 $372.53 $362.88 $414.32 $441.6842 $369.62 $360.84 $379.11 $369.29 $421.64 $449.4843 $378.55 $369.55 $388.26 $378.21 $431.82 $460.3444 $389.71 $380.45 $399.71 $389.36 $444.55 $473.9045 $402.82 $393.24 $413.16 $402.46 $459.51 $489.8546 $418.44 $408.50 $429.18 $418.07 $477.33 $508.8547 $436.01 $425.65 $447.21 $435.62 $497.38 $530.2248 $456.10 $445.26 $467.81 $455.69 $520.29 $554.6449 $475.91 $464.59 $488.12 $475.48 $542.88 $578.7350 $498.22 $486.38 $511.01 $497.78 $568.34 $605.8651 $520.26 $507.90 $533.61 $519.79 $593.48 $632.6652 $544.53 $531.59 $558.51 $544.04 $621.17 $662.1853 $569.08 $555.55 $583.68 $568.57 $649.17 $692.0354 $595.58 $581.42 $610.87 $595.05 $679.40 $724.2655 $622.08 $607.30 $638.05 $621.52 $709.63 $756.4856 $650.81 $635.35 $667.52 $650.23 $742.41 $791.4257 $679.83 $663.67 $697.27 $679.22 $775.50 $826.7058 $710.79 $693.90 $729.03 $710.15 $810.82 $864.3659 $726.13 $708.87 $744.77 $725.48 $828.33 $883.0260 $757.10 $739.10 $776.53 $756.42 $863.65 $920.6761 $783.88 $765.25 $804.00 $783.18 $894.20 $953.2462 $801.45 $782.40 $822.02 $800.73 $914.25 $974.6163 $823.49 $803.92 $844.63 $822.75 $939.39 $1,001.41
64+ $836.88 $816.99 $858.36 $836.13 $954.66 $1,017.69
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 18
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Region 18 includes the county of: Orange
BRONZE PPO PLANS
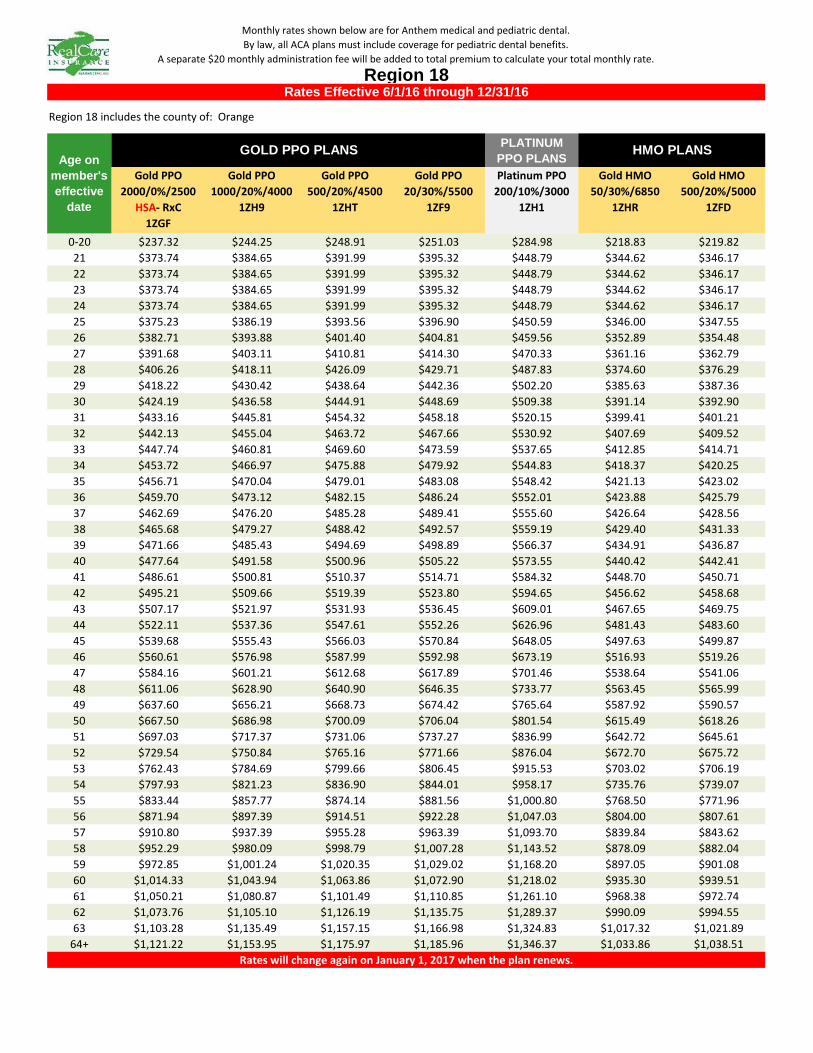
PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $237.32 $244.25 $248.91 $251.03 $284.98 $218.83 $219.8221 $373.74 $384.65 $391.99 $395.32 $448.79 $344.62 $346.1722 $373.74 $384.65 $391.99 $395.32 $448.79 $344.62 $346.1723 $373.74 $384.65 $391.99 $395.32 $448.79 $344.62 $346.1724 $373.74 $384.65 $391.99 $395.32 $448.79 $344.62 $346.1725 $375.23 $386.19 $393.56 $396.90 $450.59 $346.00 $347.5526 $382.71 $393.88 $401.40 $404.81 $459.56 $352.89 $354.4827 $391.68 $403.11 $410.81 $414.30 $470.33 $361.16 $362.7928 $406.26 $418.11 $426.09 $429.71 $487.83 $374.60 $376.2929 $418.22 $430.42 $438.64 $442.36 $502.20 $385.63 $387.3630 $424.19 $436.58 $444.91 $448.69 $509.38 $391.14 $392.9031 $433.16 $445.81 $454.32 $458.18 $520.15 $399.41 $401.2132 $442.13 $455.04 $463.72 $467.66 $530.92 $407.69 $409.5233 $447.74 $460.81 $469.60 $473.59 $537.65 $412.85 $414.7134 $453.72 $466.97 $475.88 $479.92 $544.83 $418.37 $420.2535 $456.71 $470.04 $479.01 $483.08 $548.42 $421.13 $423.0236 $459.70 $473.12 $482.15 $486.24 $552.01 $423.88 $425.7937 $462.69 $476.20 $485.28 $489.41 $555.60 $426.64 $428.5638 $465.68 $479.27 $488.42 $492.57 $559.19 $429.40 $431.3339 $471.66 $485.43 $494.69 $498.89 $566.37 $434.91 $436.8740 $477.64 $491.58 $500.96 $505.22 $573.55 $440.42 $442.4141 $486.61 $500.81 $510.37 $514.71 $584.32 $448.70 $450.7142 $495.21 $509.66 $519.39 $523.80 $594.65 $456.62 $458.6843 $507.17 $521.97 $531.93 $536.45 $609.01 $467.65 $469.7544 $522.11 $537.36 $547.61 $552.26 $626.96 $481.43 $483.6045 $539.68 $555.43 $566.03 $570.84 $648.05 $497.63 $499.8746 $560.61 $576.98 $587.99 $592.98 $673.19 $516.93 $519.2647 $584.16 $601.21 $612.68 $617.89 $701.46 $538.64 $541.0648 $611.06 $628.90 $640.90 $646.35 $733.77 $563.45 $565.9949 $637.60 $656.21 $668.73 $674.42 $765.64 $587.92 $590.5750 $667.50 $686.98 $700.09 $706.04 $801.54 $615.49 $618.2651 $697.03 $717.37 $731.06 $737.27 $836.99 $642.72 $645.6152 $729.54 $750.84 $765.16 $771.66 $876.04 $672.70 $675.7253 $762.43 $784.69 $799.66 $806.45 $915.53 $703.02 $706.1954 $797.93 $821.23 $836.90 $844.01 $958.17 $735.76 $739.0755 $833.44 $857.77 $874.14 $881.56 $1,000.80 $768.50 $771.9656 $871.94 $897.39 $914.51 $922.28 $1,047.03 $804.00 $807.6157 $910.80 $937.39 $955.28 $963.39 $1,093.70 $839.84 $843.6258 $952.29 $980.09 $998.79 $1,007.28 $1,143.52 $878.09 $882.0459 $972.85 $1,001.24 $1,020.35 $1,029.02 $1,168.20 $897.05 $901.0860 $1,014.33 $1,043.94 $1,063.86 $1,072.90 $1,218.02 $935.30 $939.5161 $1,050.21 $1,080.87 $1,101.49 $1,110.85 $1,261.10 $968.38 $972.7462 $1,073.76 $1,105.10 $1,126.19 $1,135.75 $1,289.37 $990.09 $994.5563 $1,103.28 $1,135.49 $1,157.15 $1,166.98 $1,324.83 $1,017.32 $1,021.89
64+ $1,121.22 $1,153.95 $1,175.97 $1,185.96 $1,346.37 $1,033.86 $1,038.51
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 18
Region 18 includes the county of: Orange
Age on member's effective
date
GOLD PPO PLANS
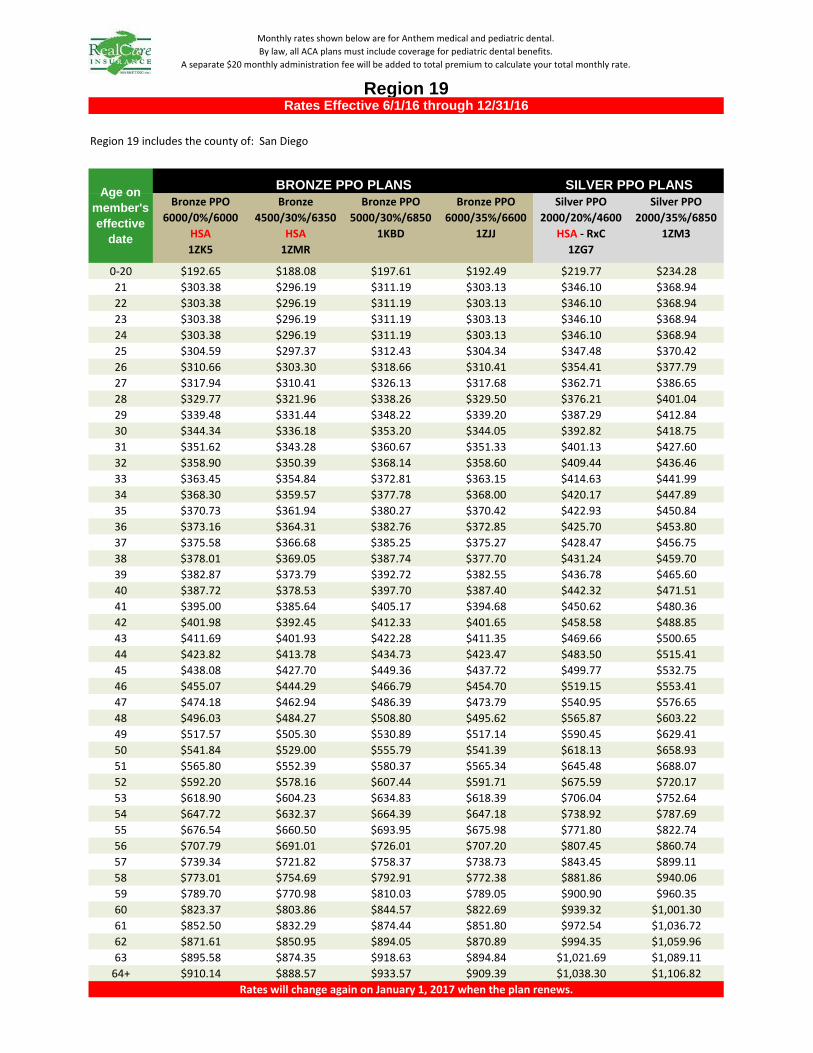
Bronze PPO 6000/0%/6000
HSA1ZK5
Bronze 4500/30%/6350
HSA1ZMR
Bronze PPO 5000/30%/6850
1KBD
Bronze PPO 6000/35%/6600
1ZJJ
Silver PPO 2000/20%/4600
HSA - RxC1ZG7
Silver PPO 2000/35%/6850
1ZM3
0-20 $192.65 $188.08 $197.61 $192.49 $219.77 $234.2821 $303.38 $296.19 $311.19 $303.13 $346.10 $368.9422 $303.38 $296.19 $311.19 $303.13 $346.10 $368.9423 $303.38 $296.19 $311.19 $303.13 $346.10 $368.9424 $303.38 $296.19 $311.19 $303.13 $346.10 $368.9425 $304.59 $297.37 $312.43 $304.34 $347.48 $370.4226 $310.66 $303.30 $318.66 $310.41 $354.41 $377.7927 $317.94 $310.41 $326.13 $317.68 $362.71 $386.6528 $329.77 $321.96 $338.26 $329.50 $376.21 $401.0429 $339.48 $331.44 $348.22 $339.20 $387.29 $412.8430 $344.34 $336.18 $353.20 $344.05 $392.82 $418.7531 $351.62 $343.28 $360.67 $351.33 $401.13 $427.6032 $358.90 $350.39 $368.14 $358.60 $409.44 $436.4633 $363.45 $354.84 $372.81 $363.15 $414.63 $441.9934 $368.30 $359.57 $377.78 $368.00 $420.17 $447.8935 $370.73 $361.94 $380.27 $370.42 $422.93 $450.8436 $373.16 $364.31 $382.76 $372.85 $425.70 $453.8037 $375.58 $366.68 $385.25 $375.27 $428.47 $456.7538 $378.01 $369.05 $387.74 $377.70 $431.24 $459.7039 $382.87 $373.79 $392.72 $382.55 $436.78 $465.6040 $387.72 $378.53 $397.70 $387.40 $442.32 $471.5141 $395.00 $385.64 $405.17 $394.68 $450.62 $480.3642 $401.98 $392.45 $412.33 $401.65 $458.58 $488.8543 $411.69 $401.93 $422.28 $411.35 $469.66 $500.6544 $423.82 $413.78 $434.73 $423.47 $483.50 $515.4145 $438.08 $427.70 $449.36 $437.72 $499.77 $532.7546 $455.07 $444.29 $466.79 $454.70 $519.15 $553.4147 $474.18 $462.94 $486.39 $473.79 $540.95 $576.6548 $496.03 $484.27 $508.80 $495.62 $565.87 $603.2249 $517.57 $505.30 $530.89 $517.14 $590.45 $629.4150 $541.84 $529.00 $555.79 $541.39 $618.13 $658.9351 $565.80 $552.39 $580.37 $565.34 $645.48 $688.0752 $592.20 $578.16 $607.44 $591.71 $675.59 $720.1753 $618.90 $604.23 $634.83 $618.39 $706.04 $752.6454 $647.72 $632.37 $664.39 $647.18 $738.92 $787.6955 $676.54 $660.50 $693.95 $675.98 $771.80 $822.7456 $707.79 $691.01 $726.01 $707.20 $807.45 $860.7457 $739.34 $721.82 $758.37 $738.73 $843.45 $899.1158 $773.01 $754.69 $792.91 $772.38 $881.86 $940.0659 $789.70 $770.98 $810.03 $789.05 $900.90 $960.3560 $823.37 $803.86 $844.57 $822.69 $939.32 $1,001.3061 $852.50 $832.29 $874.44 $851.80 $972.54 $1,036.7262 $871.61 $850.95 $894.05 $870.89 $994.35 $1,059.9663 $895.58 $874.35 $918.63 $894.84 $1,021.69 $1,089.11
64+ $910.14 $888.57 $933.57 $909.39 $1,038.30 $1,106.82
SILVER PPO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Age on member's effective
date
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 19
Region 19 includes the county of: San Diego
BRONZE PPO PLANS

PLATINUM PPO PLANS
Gold PPO 2000/0%/2500
HSA- RxC1ZGF
Gold PPO 1000/20%/4000
1ZH9
Gold PPO 500/20%/4500
1ZHT
Gold PPO 20/30%/5500
1ZF9
Platinum PPO 200/10%/3000
1ZH1
Gold HMO 50/30%/6850
1ZHR
Gold HMO 500/20%/5000
1ZFD
0-20 $258.11 $265.66 $270.71 $273.01 $309.96 $286.71 $287.9921 $406.48 $418.37 $426.32 $429.94 $488.12 $451.51 $453.5322 $406.48 $418.37 $426.32 $429.94 $488.12 $451.51 $453.5323 $406.48 $418.37 $426.32 $429.94 $488.12 $451.51 $453.5324 $406.48 $418.37 $426.32 $429.94 $488.12 $451.51 $453.5325 $408.11 $420.04 $428.03 $431.66 $490.07 $453.32 $455.3426 $416.24 $428.41 $436.55 $440.26 $499.83 $462.35 $464.4127 $425.99 $438.45 $446.78 $450.58 $511.55 $473.18 $475.3028 $441.84 $454.77 $463.41 $467.34 $530.59 $490.79 $492.9929 $454.85 $468.16 $477.05 $481.10 $546.21 $505.24 $507.5030 $461.35 $474.85 $483.87 $487.98 $554.02 $512.46 $514.7631 $471.11 $484.89 $494.10 $498.30 $565.73 $523.30 $525.6432 $480.87 $494.93 $504.34 $508.62 $577.45 $534.14 $536.5333 $486.96 $501.21 $510.73 $515.07 $584.77 $540.91 $543.3334 $493.47 $507.90 $517.55 $521.95 $592.58 $548.13 $550.5935 $496.72 $511.25 $520.96 $525.39 $596.48 $551.75 $554.2136 $499.97 $514.60 $524.37 $528.83 $600.39 $555.36 $557.8437 $503.22 $517.94 $527.78 $532.27 $604.29 $558.97 $561.4738 $506.47 $521.29 $531.19 $535.71 $608.20 $562.58 $565.1039 $512.98 $527.98 $538.02 $542.58 $616.01 $569.81 $572.3540 $519.48 $534.68 $544.84 $549.46 $623.82 $577.03 $579.6141 $529.24 $544.72 $555.07 $559.78 $635.53 $587.87 $590.5042 $538.59 $554.34 $564.87 $569.67 $646.76 $598.25 $600.9343 $551.59 $567.73 $578.52 $583.43 $662.38 $612.70 $615.4444 $567.85 $584.46 $595.57 $600.63 $681.90 $630.76 $633.5845 $586.96 $604.13 $615.61 $620.83 $704.85 $651.98 $654.9046 $609.72 $627.56 $639.48 $644.91 $732.18 $677.27 $680.3047 $635.33 $653.91 $666.34 $672.00 $762.93 $705.71 $708.8748 $664.59 $684.03 $697.03 $702.95 $798.08 $738.22 $741.5249 $693.45 $713.74 $727.30 $733.48 $832.73 $770.28 $773.7250 $725.97 $747.21 $761.41 $767.87 $871.78 $806.40 $810.0051 $758.09 $780.26 $795.09 $801.84 $910.34 $842.07 $845.8352 $793.45 $816.66 $832.18 $839.24 $952.81 $881.35 $885.2953 $829.22 $853.47 $869.69 $877.08 $995.76 $921.08 $925.2054 $867.83 $893.22 $910.19 $917.92 $1,042.14 $963.97 $968.2955 $906.45 $932.97 $950.69 $958.77 $1,088.51 $1,006.87 $1,011.3756 $948.32 $976.06 $994.60 $1,003.05 $1,138.78 $1,053.37 $1,058.0957 $990.59 $1,019.57 $1,038.94 $1,047.76 $1,189.55 $1,100.33 $1,105.2558 $1,035.71 $1,066.01 $1,086.26 $1,095.49 $1,243.73 $1,150.45 $1,155.5959 $1,058.07 $1,089.02 $1,109.71 $1,119.13 $1,270.58 $1,175.28 $1,180.5460 $1,103.19 $1,135.46 $1,157.03 $1,166.86 $1,324.76 $1,225.40 $1,230.8861 $1,142.21 $1,175.62 $1,197.96 $1,208.13 $1,371.62 $1,268.74 $1,274.4262 $1,167.82 $1,201.98 $1,224.82 $1,235.22 $1,402.37 $1,297.19 $1,302.9963 $1,199.93 $1,235.03 $1,258.50 $1,269.18 $1,440.93 $1,332.86 $1,338.82
64+ $1,219.44 $1,255.11 $1,278.96 $1,289.82 $1,464.36 $1,354.53 $1,360.59
HMO PLANS
Rates Effective 6/1/16 through 12/31/16
Rates will change again on January 1, 2017 when the plan renews.
Monthly rates shown below are for Anthem medical and pediatric dental. By law, all ACA plans must include coverage for pediatric dental benefits.
A separate $20 monthly administration fee will be added to total premium to calculate your total monthly rate.
Region 19
Region 19 includes the county of: San Diego
Age on member's effective
date
GOLD PPO PLANS

Insurance Carrier DeltaCare USA Delta DentalPlan Name Plan 11B Fee For ServicePlan Type HMO DPOProvider Network DeltaCare USA Network ONLY PPO or Premier NetworkCalendar Year Maximum Unlimited $1,000Deductible: None Single $50/Family $ 150Waived for Preventive Not Applicable Yes
Diagnostic "Delta Pays" (A) Office Visit $20 copay $26.00 Periodic Oral Evaluation No Charge $17.00 Comprehensive Oral Evaluation No Charge $22.00 Bitewing X‐rays No Charge $12.00 ‐ $26.00 Other X‐rays No Charge $5.00 ‐ $50.00
Preventive "Delta Pays" (A) Cleanings Adult No Charge $40.00
Additional Cleanings: $45.00 Not Applicable Child through Age 13 No Charge $32.00
Additional Cleanings: $35.00 Not Applicable
"Delta Pays" (A) Restorative No Charge ‐ $240 copay $53.00 ‐ $148.00 Oral Surgery No Charge ‐ $110 copay $26.00 ‐ $175.00 Endodontics (Root Canals) No Charge ‐ $250 copay $50.00 ‐ $402.00 Periodontics (Deep Cleaning) $80 copay ‐ $280 copay $39.00 ‐ $448.00
"Delta Pays" (A) Waiting Period None None Crowns $55 copay ‐ $240 copay $343.00 ‐ $391.00 Prosthodontics, Removable $20 copay ‐ $210 copay $255.00 ‐ $676.00 Prosthodontics, Fixed $40 copay ‐ $240 copay $191.00 ‐ $605.00
Orthodontia
Pretreatment/Post Treatment $200 copay / $70 copay Limited Treatment Child to 19 $950 copay Limited Treatment 19 to Adult $1,150 copay Comprehensive Treatment Child to 19 $1,700 copay Comprehensive Treatment 19 to Adult $1,900 copay
Subscriber Only $38.80 $55.84Subscriber+1 $58.47 $98.45Subscriber+2 or more $82.42 $129.24
NOT COVERED
Monthly Premium Rate
(A) For each procedure, you are responsible for the portion of the dentist's fee that is more than the amount listed in the "Delta Dental Pays" column.
Delta Dental Plan Options through the AssociationsEffective Date: December 01, 2016 ‐ November 30, 2017
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081

Vision BenefitsDeductible:
Exams
Material
Exam
Comprehensive Exam
Follow‐Up Exam
Lenses (per pair)
Frames
Contact Lenses
Cosmetic/Convenience
Medically Necessary
Subscriber Subscriber
&
Family
Monthly Rates $7.95 $20.10
Annual Rates $95.40 $241.20
Other Services:
Long Term Care Plans Life Insurance Options Prescription Drug PlansLong Term Disability Plans Medicare Supplements
No Charge
Up to $20
One comprehensive exam in any 24 consecutive months, with a follow‐up
exam at a 12 month interval.
No Charge
1 pair of standard lenses in any 24 consecutive months, or at a 12 month
interval if the prescription changes.
Up to $40
Application Requirements
Up to $105
Subscriber & (1) Child
OR
Up to $100
Subscriber & Spouse
Member/Employer group applications may be submitted at any time. Applications for new hires should
be enrolled within 30 days following the date of eligibility. Dependents must be enrolled during initial
enrollment period. If a member enrolls at any other time than December, the annual rate will be pro‐
rated.
Vision Plan through Associations Effective Date December 01, 2016 ‐ November 30, 2017
In‐Network
$15 deductible $15 deductible
Premium Rates
1 pair of standard lenses in any 24 consecutive months, or at a 12 month
interval if the prescription changes.
MEDICAL EYE SERVICES (MES)Out‐of‐Network
$179.40
Monthly rates available for groups with medical coverage upon request.
$10 deductible$10 deductible
Up to $40
1 standard frame in any 24 consecutive months.
Up to retail cost of $100
$14.95
No Charge Up to $250
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081
NEED HELP FINDING A PROVIDER?
WESTERN HEALTH ADVANTAGE
https://www.westernhealth.com/search-for-providers/?sp=home
ANTHEM BLUE CROSS
DELTA DENTAL
PREMIER ACCESS
MEDICAL EYE SERVICES
https://www.mesvision.com/homepage.htm
https://www.deltadentalins.com/find-a-
https://mydental.guardianlife.com/secure/PAWEBSITE.PROVIDER.UI/WBSPrvNewSearch.as
https://www.anthem.com/health-insurance/provider-directory/searchcriteria?qs=*dmobYvnDkpRF9B5i7bq78aM6zsOJDillMrp75xf57aA=&brand=abcbs
For illustrative purposes only Ames-Grenz Insurance Services, Inc. Lic. 0787081


















