Medullary Sponge Kidney Associated with Congenital Hem ihypertrophy
8
EDITORIAL COMMITrEE Tomas Berl, Editor William Henrich Mark Paller Fred Silva Denver, CO Toledo, OH Minneapolis, MN Oklahoma City, OK NEPHROLOGY TRAINING PROGRAM: DUKE UNIVERSITY MEDICAL CENTER The nephrology training program at the Duke University School of Medicine provides comprehensive training in clinical nephrology. dialysis, renal transplantation, and hypertension. Fellowship options include a 3-year clinical investigator pathway, a 3-year basic science investigator pathway, and a 2-year clinical training track. Each fellow completes a clinical program that includes rotation on three services: the transplant service, the acute nephrology service, and the consult service at the Durham Veterans’ Affairs Medical Center. During the transplant rotation, the fellow is involved in the evaluation of donor and recipient candidates for kidney and simultaneous kidney-pancreas transplant. Post-transplant care is primarily the responsibility of the nephrology division. The acute service provides interventional support to Duke University Medical Center’s intensive care units. an inpatient renal ward, and a general renal consultation service. Outpatient activities include the longitudinal management of fellows’ own renal transplant, dialysis, chronic renal failure, and nephrology referral patients. Clinical facilities include the 1 100-bed Duke University Medical Center and the 450-bed Durham Veterans’ Affairs Medical Center. The division directs five outpatient dialysis facilities, providing care for over 375 dialysis patients. Active peritoneal and home hemodialysis programs are included. The renal transplant program at Duke University Medical Center averages 70 kidney and simultaneous kidney-pancreas transplants each year. The Duke Hypertension Center provides the opportunity for clinical experience in refractory hypertension. A National Institutes of Health (NIH)- supported General Clinical Research Center is often used by the division. The basic science investigator pathway includes 2 years of research under the direction of a faculty sponsor. The division currently has a NIH-training grant as welt as a Transplantation Program Project Grant with three faculty members involved. NIH-funded basic science investigation is also ongoing in areas including metabolic bone disease, genetic predisposition for hypertension. signal transduction, and receptor regulation. Advanced training in biostatistics. study design. and epidemiology (including the opportunity to pursue a Masters of Health Science degree) is available to fellows choosing the clinical investigator pathway. NIH- and industry-funded trials in hemodialysis vascular access, cardiovascular disease in renal failure patients, adequacy of dialysis and dialysis membranes, use of atrial natriuretic peptide in acute renal failure, and treatment of metabolic bone disease in hemodialysis patients are ongoing. The straight clinical pathway includes 18 months of intensive clinical training that encompasses all areas of nephrotogy. including the management of outpatient hemodialysis and significant outpatient transplant and hyper- tension experience. with a brief exposure to clinical research. In addition, structured exposures to renal pathology and histocompatibility are available. Medullary Sponge Kidney Associated with Congenital Hem ihypertrophy Olafur Skuli Indridason, Laura Thomas, and Michael Berkoben2 L. Thomas, Department of Radiology, Duke University O.S. Indridason, M. Berkoben, Division of Nephrology, Medical Center, Durham, NC Duke University Medical Center, Durham, NC (J. Am. Soc. Nephrol. 1996; 7:1123-1130) ABSTRACT Medullary sponge kidney is a developmental disor- 1 Received September 21. 1995. Accepted February 10. 1996. . . . 2 Correspondence to Dr. M. Berkoben, Box 3014, Duke University Medical Center, der characterized by ectatuc and cystic malformation Durham, NC 27710. of the collecting ducts and tubules. Clinical manifes- 104&6673/0708-1 123$03.OOIO tations include urinary tract infections, renal stones, Journal of the American SocIety of Nephrology . . Copyright © 1996 by the American Society of Nephrology and hematuria. It can be associated with other de- Journal of the American Society of Nephrology 1123
Transcript of Medullary Sponge Kidney Associated with Congenital Hem ihypertrophy

EDITORIAL COMMITrEE
Tomas Berl, Editor William Henrich Mark Paller Fred Silva
Denver, CO Toledo, OH Minneapolis, MN Oklahoma City, OK
NEPHROLOGY TRAINING PROGRAM:DUKE UNIVERSITY MEDICAL CENTER
The nephrology training program at the Duke University School of Medicine provides comprehensive training inclinical nephrology. dialysis, renal transplantation, and hypertension. Fellowship options include a 3-year clinicalinvestigator pathway, a 3-year basic science investigator pathway, and a 2-year clinical training track.
Each fellow completes a clinical program that includes rotation on three services: the transplant service, the acutenephrology service, and the consult service at the Durham Veterans’ Affairs Medical Center. During the transplantrotation, the fellow is involved in the evaluation of donor and recipient candidates for kidney and simultaneouskidney-pancreas transplant. Post-transplant care is primarily the responsibility of the nephrology division. The acute
service provides interventional support to Duke University Medical Center’s intensive care units. an inpatient renal ward,and a general renal consultation service. Outpatient activities include the longitudinal management of fellows’ ownrenal transplant, dialysis, chronic renal failure, and nephrology referral patients.
Clinical facilities include the 1 100-bed Duke University Medical Center and the 450-bed Durham Veterans’ AffairsMedical Center. The division directs five outpatient dialysis facilities, providing care for over 375 dialysis patients. Activeperitoneal and home hemodialysis programs are included. The renal transplant program at Duke University Medical
Center averages 70 kidney and simultaneous kidney-pancreas transplants each year. The Duke Hypertension Centerprovides the opportunity for clinical experience in refractory hypertension. A National Institutes of Health (NIH)-
supported General Clinical Research Center is often used by the division.
The basic science investigator pathway includes 2 years of research under the direction of a faculty sponsor. Thedivision currently has a NIH-training grant as welt as a Transplantation Program Project Grant with three faculty membersinvolved. NIH-funded basic science investigation is also ongoing in areas including metabolic bone disease, geneticpredisposition for hypertension. signal transduction, and receptor regulation.
Advanced training in biostatistics. study design. and epidemiology (including the opportunity to pursue a Masters ofHealth Science degree) is available to fellows choosing the clinical investigator pathway. NIH- and industry-funded trialsin hemodialysis vascular access, cardiovascular disease in renal failure patients, adequacy of dialysis and dialysis
membranes, use of atrial natriuretic peptide in acute renal failure, and treatment of metabolic bone disease in
hemodialysis patients are ongoing.
The straight clinical pathway includes 18 months of intensive clinical training that encompasses all areas ofnephrotogy. including the management of outpatient hemodialysis and significant outpatient transplant and hyper-tension experience. with a brief exposure to clinical research. In addition, structured exposures to renal pathology andhistocompatibility are available.
Medullary Sponge Kidney Associated with CongenitalHem ihypertrophyOlafur Skuli Indridason, Laura Thomas, and Michael Berkoben2
L. Thomas, Department of Radiology, Duke University
O.S. Indridason, M. Berkoben, Division ofNephrology, Medical Center, Durham, NC
Duke University Medical Center, Durham, NC (J. Am. Soc. Nephrol. 1996; 7:1123-1130)
ABSTRACTMedullary sponge kidney is a developmental disor-
1 Received September 21. 1995. Accepted February 10. 1996. . . .
2 Correspondence to Dr. M. Berkoben, Box 3014, Duke University Medical Center, der characterized by ectatuc and cystic malformationDurham, NC 27710. of the collecting ducts and tubules. Clinical manifes-104&6673/0708-1 123$03.OOIO tations include urinary tract infections, renal stones,Journal of the American SocIety of Nephrology . .
Copyright © 1996 by the American Society of Nephrology and hematuria. It can be associated with other de-
Journal of the American Society of Nephrology 1123

Medullary Sponge Kidney and Congenital Hemihypertrophy
1124 Volume 7 . Number 8 . 1996
velopmental disorders. A case of medullary spongekidney associated with congenital hemihypertrophy,complicated by nephrocalcinosis and nephrolithia-sis, is reported here.
Key Words: Hypercalciuria. kidney calculi. renal tubular aci-
dosis, nephrocalcinosis
M edullary sponge kidney is characterized by ec-
tatic and cystic malformations of the collecting
ducts and tubules of one or more papillae of one or
both kidneys. The cysts measure 1 to 7.5 mm in
diameter, are most prominent in the Inner paplllae,
are lined with cuboidal or columnar epithellum, and
communicate with the dilated ducts and tubules (1-
3). In and of themselves, these anatomic abnormali-
ties produce no symptoms. The morbidity of this
disorder is the result of nephrobithiasis and urinary
tract infectIon, both of which are thought to be sec-
ondary to the anatomic abnormalities. Not surpris-
ingly, then, medullary sponge kidney is often diag-
nosed incidentally by intravenous urography In the
work-up of hematuria, kidney stones, or urinary tract
infections ( 1 ). Although usually diagnosed In adult
life, the disorder is thought to be congenital. It has
been described in association with other congenitaldisorders ( 1 ,4). We report a case of medullary sponge
kidney associated with congenital hemihypertrophy.
The case also demonstrates many of the salient dm1-
cab features of medublary sponge kidney.
CASE REPORT
The patient is a 35-yr-old man who experiencedacute renal colic from a kidney stone in October 1992.Initial evaluation was remarkable for hypercalciurla
(450 mg/24 h), borderline hyperuricosuria (789
mg/24 h), and a high urinary sodium excretion rate
(383 mmol/24 h). He had normal citrate excretion (2.6
mmol/24 h) but mildly elevated oxalate excretion
(44.0 mg/24 h) rates. His serum creatinine concentra-
tion was 1 . 1 mg/dL, BUN 24 mg/dL, sodium 143
mmol/L, potassium 4.2 mmol/L, chloride 103
mmol/L, and CO2 29 mmoh/L. His serum calcium
concentration was 10. 1 mg/dL, phosphorus 3.4 mgI
dL, uric acid 6.2 mg/dL, and albumin 4.6 g/dL. The
serum intact parathyroid hormone bevel was 38
pg/mL (normal range, 13 to 64 pg/mL), the serum
1 ,25-dlhydroxyvltammn D level was 29 pg/mL (normal
range, 15 to 50 pg/mL), and the serum 25-hydroxyvi-
tamin D level was 27 ng/mL (normal range, 15 to 80
ng/mL). The hemogram was normal. Urinalysis
showed pH 6.0, specific gravity 1.014, and 19 white
blood cells per high-powered field (hpf). An abdominal
radiograph demonstrated extensive bilateral nephro-
calcinosis (Figure 1 ). Computed tomography of theabdomen demonstrated extensive bilateral nephrocal-
cinosis and milk of calcium (chalky white liquid) in
ectatic renal tubules (Figure 2). A high fluid intake
and dietary sodium and oxalate restriction were pre-
scribed. In March 1993, a 24-h urine sample was
Figure 1. Abdominal radiograph done on initial presentationshowed extensive nephrocalcinosis.
Figure 2. Computed tomography scan of abdomen demon-strated ectatic tubules and extensive nephrocalcinosis.
taken, which contained 367 mg calcium and 205
rnmol sodium. In December 1993, a 24-h urine sam-
ple was taken, containing 323 rng calcium and 304
mmol sodium. Urinalysis was remarkable for hema-
tuna and pyuria, but a urine culture yielded no
growth. An abdominal radiograph demonstrated pro-
gression of nephrocalcinosis. The patient was referred
to us for further evaluation and management.
At the time ofhis first visIt to us in January 1994, he
was asymptomatic, was following the prescribed diet,
and was maintaining a urine volume greater than 2 L
per day. His past medical history was remarkable forsurgical repair of an umbilical hernia in 1 976 and
surgery for a discrepancy in leg length in the early
1970s. He had no history ofgout, inflammatory bowel
disease, chronic diarrhea, hyperparathyroidism, neckirradiation, or granubomatous disease. His only med-
ication was a multivitamin that included vitamins A
(10,000 IU), C (3000 mg), and D (100 IU). He was a
vegetarian. He did not drink milk or eat cheese. He
took no antacids, calcium supplements, or protein
supplements. The family history was significant in
that his mother passed a kidney stone shortly after

Indridason et al
Journal of the American Society of Nephrology 1125
giving birth to him. In addition, the patient reported
that one of his mother’s arms was much smaller than
the other. The physical examination was unremark-
able except that the right leg was larger than the left
(Figure 3). The circumference of the right thigh was
58.8 cm and that of the left 55.2 cm. The circumfer-
ence of the right calf was 40.8 cm and that of the left
36.0 cm. Pertinent laboratory data included a serum
potassium level of3.8 mEq/L, a serum CO2 bevel of 33mEq/L, and a serum creatinine concentration of 1.2
mg/dL. Urinalysis showed a specific gravity of 1 .0 10,
pH of5.0, 19 white blood cells per hpf, and 3 red blood
cells per hpf. A urine culture again yielded no growth.
A 24-h urine sample contained 208 mg calcium, 105
mmol sodium, 42 mg oxalate, and 4.4 mmol citrate. It
was recommended that the patient discontinue taking
the multivitamin. Because of persistent hypercalci-
uria, a thiazide diuretic was prescribed. He refused to
take it. In November 1994, his serum creatine level
was 1 .0 mg/dL and serum CO2 bevel was 29 mEq/L. A
24-h urine sample contained 384 mg calcium, 155
mmob sodium, and 838 mg uric acid. An abdominal
radiograph demonstrated no progression of nephro-
calcinosis. He has continued to pass minute kidney
stones on occasion, but has experienced no renal
colic, hematuria, or urinary tract infections.
ETIOLOGY
The association of medullary sponge kidney with
congenital abnormalities and the unchanging nature
of the cystic lesions over time suggest that it is a
developmental disorder ( 1 ,4). It Is usually sporadic
but has been reported in two or more successive
generations of several families (1).
PREVALENCE
In a geographical area of the United Kingdom with a
population of 254,000, Mayall found 1 2 cases of med-
ullary sponge kidney in 2600 intravenous urograms,
suggesting a prevalence of 5 per 100,000 in the gen-
eral population (5). This is likely to be an underesti-
matlon, as asymptomatic patients do not undergo
urography. Other studies have shown a prevalence of
0.5 to 1 % in unselected patients undergoing urogra-
phy ( 1 ,6). In patients with stones, the prevalence has
been reported to be 2.6 to 2 1 % ( 1 ,6-8). When corn-pared with men with calcium stones, women with
calcium stones are more likely to have medullary
sponge kidney ( 1 ,7). The prevalence of medullary
sponge kidney may be as high as 25% in women with
calcium stones (1).
PATHOPHYSIOLOGY
The cysts frequently contain calcific deposits. These
deposits are radio-opaque, frequently appear in clus-
ters on plain film of the abdomen, and are composed of
an admixture of calcium apatite and calcium oxalate
or of calcium apatite alone ( 1 ). Erosion of these con-
cretions through the papillary wall into the renal
pelvis may head to symptomatic stone disease.
Several factors contribute to the formation of intra-
papillary calcium concretlons (Table 1 ). First, urinary
stasis within the cysts likely plays a role ( 1 ). Second,
cellular debris and hyahine material In the cysts may
provide a matrix for stone formation ( 1 ). Third, Im-
paired urinary acidification may decrease the solubil-
ity of calcium apatite (9-12). Finally, any or all of the
risk factors for idiopathic calcium stone disease (hy-
percalciuria, hyperoxaburia, hyperuricosuria, hypoci-
Figure 3. Views showing enlarged right leg of patient.
Medullary Sponge Kidney and Congenital Hemihypertrophy
1 126 Volume 7 . Number 8 . 1996
TABLE 1 . Factors that may promote formation ofintrapapillary concretions
Urinary StasisInfectionIntraluminal DebrisImpaired Urinary AcidificationRisk Factors for Calcium Stone Disease (Hypercalciuria,
Hyperoxaiuria, Hypocitraturla, Hyperuricosuria)
traturia) may be present In patients with medulbary
sponge kidney ( 1 ,6,8). The impaired urinary acidifica-
tion and the hypercalciurla of medullary sponge kid-
ney merit further comment.
Impaired Urinary Acidification
The terminal collecting duct is a principal site of theanatomic lesions of medulbary sponge kidney (1,2).
The terminal collecting duct also plays a major role In
urinary acidification. Indeed, investigators have re-
ported impaired distal acidification in a substantialproportion of patients with medullary sponge kidney.
Higashihara and coworkers (9) studied 1 1 stone form-
ers with medullary sponge kidney. Baseline arterialblood pH was normal in all, but the baseline plasma
bicarbonate concentration was low In seven patients.
The urine pH of four patients did not fall below 5.3after ammonium chloride loading and thus met the
criteria for partial distal renal tubular acidosis. All
four had low plasma bicarbonate concentrations. The
urine pH of another five patients did not fall below5. 10. When compared with healthy subjects and to
patients with bilateral stones, the 1 1 patients with
medullary sponge kidney had lower baseline plasma
bicarbonate concentrations (mean, 22. 1 mEq/L) and
had higher urine pH values in response to ammoniumchloride loading. Similarly, Osther and colleagues (10)
studied 13 stone formers with medublary sponge kid-
ney and found two with complete and six with partial
distal renal tubular acidosis. More recently, Osther et
at. ( 13) reported his findings In ten women with med-
ullary sponge kidney. Four had partial renal tubular
acidosis. When compared with the six women withnormal urinary acidification, the four with partial
renal tubular acidosis had lower fasting plasma bicar-
bonate concentrations (20.5 mEq/L versus 23.8
mEq/L) and lower 24-h urinary citrate excretion rates
(0.93 mmol versus 3.58 mmoh; normal, >1.8 mmol).Other investigators have found that the 24-h urInarycitrate excretion rate is bower in recurrent stone form-
ers with medullary sponge kidney than In idiopathicstone formers (11).
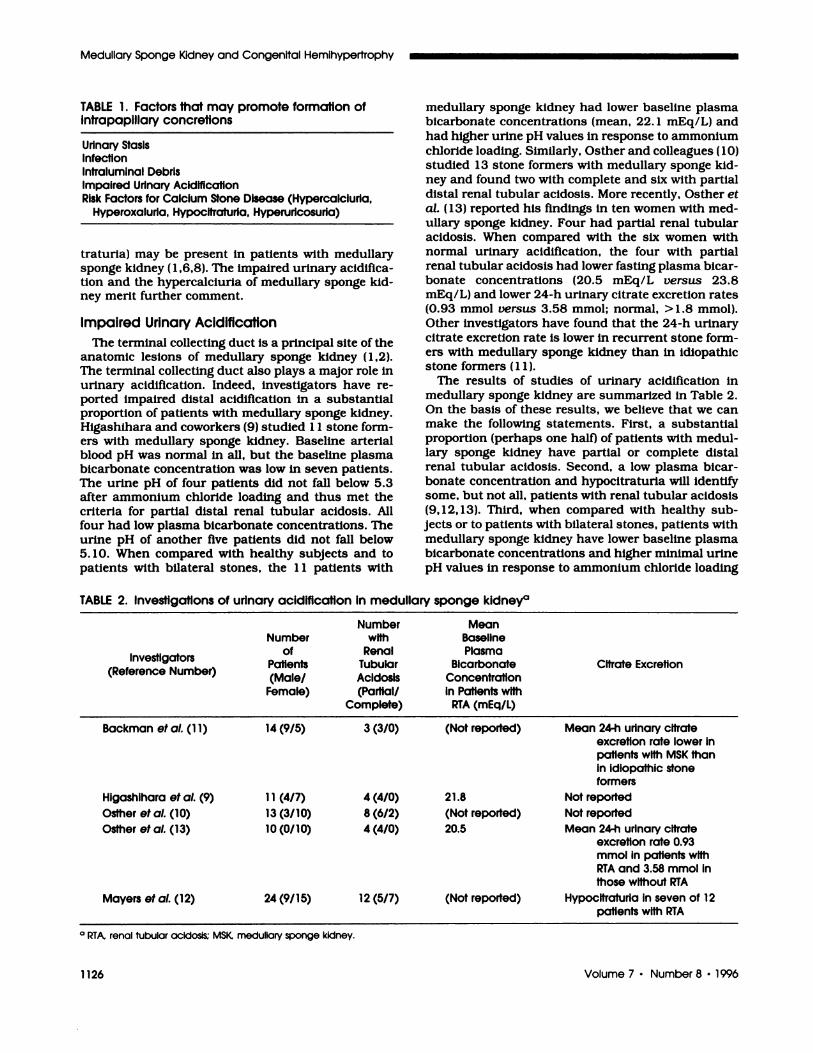
The results of studies of urinary acidification inmeduhlary sponge kidney are summarized In Table 2.
On the basis of these results, we believe that we canmake the following statements. First, a substantial
proportion (perhaps one half) of patients with medul-bary sponge kidney have partial or complete distal
renal tubular acidosis. Second, a low plasma bicar-
bonate concentration and hypocitraturia will identifysome, but not all, patients with renal tubular acidosis
(9, 12, 13). Third, when compared with healthy sub-
jects or to patients with bilateral stones, patients with
medullary sponge kidney have lower baseline plasma
bicarbonate concentrations and higher minimal urinepH values in response to ammonium chloride loading
TABLE 2. Investigations of urinary acidification in medullary sponge kidneya
Number MeanNumber with Baseline
.investigators(Reference Number)
of.
Patients(Male/
Female)
RenalTubularAcidosis(Partial/
Complete)
Plasma.
BicarbonateConcentrationin Patients with
PTA (mEq/L)
.
Citrate Excretion
Backman et al. (1 1) 14 (9/5) 3 (3/0) (Not reported) Mean 24-h urinary citrateexcretion rate lower inpatients with MSK thanin idiopathic stoneformers
Higashihara et al. (9) 11 (4/7) 4 (4/0) 21.8 Not reportedOsther et a!. (10) 13 (3/10) 8 (6/2) (Not reported) Not reported
Osther et a!. (1 3) 10 (0/ 10) 4 (4/0) 20.5 Mean 24-h urinary citrateexcretion rate 0.93mmol in patients withPTA and 3.58 mmol Inthose without PTA
Mayers et a!. (12) 24 (9/ 15) 12 (5/7) (Not reported) Hypocitraturia in seven of 12patients with PTA
a PTA, renal tubular acidosis; MSK medullary sponge kidney.

Indridason et al
Journal of the American Society of Nephrology 1127
(9). It seems likely, therefore, that many patients with
medublary sponge kidney have subclinical impairment
of urinary acidification. Proton secretion may be im-
paired in cystic terminal collecting ducts. If only a
fraction of the terminal collecting ducts are cystic, the
patient may still be able to maintain normal systemic
pH and excrete maximally acid urine (pH < 5.3) in
response to ammonium chloride loading. Increased
urine pH wIthin cystic ducts, however, may promote
intraductal precipitation of calcium apatite and bead
to clinical stone disease. Although impaired urinary
acidification may characterize many patients with
medulbary sponge kidney, it does not follow that alkali
therapy will be beneficial (see the Treatment section).
Hypercalciuria
In large series of cases of medullary sponge kidney,
the prevalence ofhypercalciuria Is approximately 40%
(7, 14). Parks and coworkers found that hypercalciuria
was no more prevalent in stone formers with medul-
lary sponge kidney than in stone formers without
medullary sponge kidney (7). In addition, the same
causes of hypercalciuria are present in patients with
medullary sponge kidney as in patients without the
disorder (6,8, 15, 16). Table 3 lists the possible causes
of hypercalciuria in patients with medullary sponge
kidney. Some investigators have reported a prepon-
derance of absorptive hypercalciuria (8), whereas oth-
ers have reported a preponderance of renal hypercal-
ciuria ( 1 7). Although physiologic regulation of calcium
excretion occurs primarily In the cortical distal
nephron under the influence of parathyroid hormone
and calcitriol, calcium reabsorption does occur along
the inner medullary collecting duct of the rat. Some
researchers have speculated that impaired calcium
reabsorption in the cystic ducts may cause the hyper-
calciuria of medulbary sponge kidney. In contrast,
Higashihara and coworkers ( 1 7) have reported that
metabolic acidosis causes renal hypercalciuria. These
Investigators studied 1 6 patients with medulbary
sponge kidney. Seven patients exhibited renal hyper-
calciuria. These patients had higher urine pH values
in response to acid loading and lower plasma bicar-
TABLE 3. Hypercalciuria of medullary sponge kidney
bonate concentrations (22.5 mEq/L) than healthy
control subjects. Six of the seven patients had low
plasma bicarbonate concentrations. Administration of
2 to 4 g of sodium bicarbonate daily reduced calcium
excretion from 5.05 to 2.91 mg/kg per day and re-duced the frequency of stone passage. Osther et at.(13) studied ten women with bilateral medullarysponge kidney. Four women had incomplete distal
renal tubular acidosis. When compared with the six
patients without renal tubular acidosis. and with ten
healthy women, these four patients had lower plasma
bicarbonate concentrations, increased urinary excre-
tion rates of calcium, and decreased urinary excretionrates of citrate. The practical implications of these
findings will be discussed in the Treatment section.
The robe of hyperparathyroidism in the hypercalci-uria of medulbary sponge kidney is debatable. Hyper-
parathyroidism has been demonstrated in a few pa-
tients ( 1 ,6). In large series, however, the prevalence of
hyperparathyroidism In patients with medullary
sponge kidney is not different from that of patients
with idiopathic calcium stone disease (6,7).
Other tubular abnormalities that have been de-scribed include a vasopressin-resistant concentratingdefect ( 1 ,9) and a decreased ability to excrete an acute
potassium load ( 1 8); neither defect has proved to be
clinically significant.
CLINICAL MANIFESTATIONS
Patients are asymptomatic until kidney stones, he-
maturia, or infections develop, typically in adult life.
Stones occur in 50 to 65% of these patients (19-2 1).
When compared with calcium stone formers withoutmedulbary sponge kidney, calcium stone formers with
the disorder have higher rates of stone formation (7).Although intrapapillary concretions are composed of
an admixture of calcium apatite and calcium oxalate
or of calcium apatite alone, pure apatite stones are
rarely passed. Stone analysis demonstrates either
pure calcium oxahate or an admixture of calcium
oxalate and calcium apatite ( 1 ). It thus seems likely
that calcium oxalate deposition occurs in the collect-
ing system before final stone passage. Microscopic or
Etiology(Reference Number)
Laboratory Findings Mechanism
Absorptive Hypercalciuria (8) Urinary calcium excretion less than 0.1 1mg/mg creatinine after fasting andgreater than 0.26 mg/mgcreatinine after calcium loading(15,16)
Supranormal intestinal absorptionof calcium
Penal Hypercalciuria (1 7) Urinary calcium excretion greater than0.1 1 mg/mg creatinine after fasting(15,16)
Impaired calcium reabsorption bycystic ducts and/or metabolicacidosis (17)
Hyperparathyroidism Hypercalcemia; elevated serumparathyroid hormone level
Hypercalcemia

Medullary Sponge Kidney and Congenital Hemihyperirophy
1 128 Volume 7 . Number 8 ‘ 1996
frank hematurla can occur in the presence or absence
of stones ( 1 ,22). Urinary tract infections occur more
frequently in calcium stone formers with medullary
sponge kidney than in calcium stone formers without
the disorder and occur more frequently in women
than in men (7). Perltubular Inflammation has been
demonstrated in the absence of infection and may
result in sterile pyuria (2,3,9). Nephrocalcmnosis Is also
a frequent manifestation of medulbary sponge kidney.
Parks and colleagues (7) reported that nephrocalcino-
sis is present in 15% of calcium stone formers with
medullary sponge kidney and In 3% of calcium stone
formers without medullary sponge kidney.
Medullary sponge kidney is associated with several
developmental and hereditary disorders (Table 4).
Anomalies of the urinary tract, bile duct ectasia (Caro-
li’s disease), congenital pyboric stenosis, Beckwith-
Wiedemann syndrome, Ehbers-Danbos syndrome,
Marfan’s syndrome, polycystic kidney disease, and
congenital hemihypertrophy have been reported in
association with medubbary sponge kidney ( 1 ,4). An
association with primary hyperparathyroidism Is a
matter of debate.
Congenital hemlhypertrophy is characterized by
asymmetry of the body as a result of hypertrophy of all
somatic elements (muscles, bones, nerves, vessels) of
one or more body parts. Visceromegaly may be presentas well. Congenital hemihypertrophy can involve part
or all of one side of the body (complex ipsilateral
hemihypertrophy), body parts on both sides (complex
contrabaterab hemlhypertrophy), a single limb (simple
hemihypertrophy), or one side of the face (hemifaclal
hypertrophy) (23). CongenItal hemlhypertrophy has
been estimated to occur In 1 In 40,000 lIve births (24).It is frequently associated with other developmental
abnormalities such as congenital heart disease, poly-
and syndactyly. mental retardation, Proteus syn-
drome, Silver-Russell syndrome, and Beckwith-
Wiedemann syndrome. Congenital hemihypertrophy
is also associated with childhood tumors, particularly
adrenal adenomas and Wilms’ tumors (24). Nephro-
genic rests and other developmental abnormalities of
the kidney and urinary tract have been reported In
association with congenital hemihypertrophy (23,25).
Up to 10% of patients with congenital hemlhypertro-
phy have medullary sponge kidney (26,27), and up to
25% of patients with medulbary sponge kidney have
congenital hemihypertrophy (14).
TABLE 4. Developmental and inherited disordersassociated with medullary sponge kidney
Congenital HemihypertrophyBeckwith-Wiedemann SyndromeCongenital Pyloric StenosisCaroli’s DiseaseUrinary Tract MalformationsEhlers-Danlos SyndromeMarfan’s SyndromePolycystic Kidney Disease
DIAGNOSIS
Definitive diagnosis is made by intravenous urogra-
phy (IVU). (Although our patient did not undergo IVU,
It was thought that the constellation of clinical find-
ings strongly supported the diagnosis of medulbary
sponge kidney. It was not thought that IVU would
affect his management.) Renal concretions, often ar-
ranged in small clusters in the papillae. may be seenon the initial plain film. With administration of con-
trast medium, ectatic tubules are imaged as striations
radiating from the calyces (�brush”). Cysts are imaged
as round opacifications in the papillae (“bouquets of
flowers” or “bunches of grapes”). Brushes and bou-
quets appear before opacification of the calyces and
may persist after the contrast medium is cleared from
the renal pelves ( 1 ). Firm radiographic criteria for the
diagnosis of medullary sponge kidney have not been
established. In a recent study, a minimum of three
linear or round collections within one renal papilla
was required for the diagnosis of medullary sponge
kidney (6). In previous studies, more stringent criteria
(Involvement of three or more papllbae or of both
kidneys) were used ( 1 ,7,8). Another diagnostic diffi-
culty arises when only diffuse opacification of the
papillae (papillary blushing) is present. Papillary
blushing is detected by urography in 4% of stone
formers and in 3% of non-stone formers (6). Whether
this finding should be considered normal or indicative
of a mild form of medubbary sponge kidney is unclear.
A pathologic diagnosis of medublary sponge kidney
has been established in kidneys that demonstrated
only papillary blushing on urography ( 1 ). Papillary
blushing should be considered diagnostic of medul-
lary sponge kidney if it appears before opaclfication of
the calyces, persists after contrast medium has beencleared from the pelves, and is associated with papil-
lary concretions or nephrocalcmnosis.
Computed tomography (CT), ultrasonography, and
retrograde pyelography have little utility in the diag-
nosis of medullary sponge kidney. CT without injec-
tion of contrast medium appears to be more sensitive
than IVU for detecting papillary concretions (28).
These concretlons, however, are not specific for med-
ullary sponge kidney. IVU remains far superior to CT
(even with injection of contrast medium) in the diag-nosis of medullary sponge kidney because of its far-
greater ability to image tubular ectasia ( 1 ,28). Plain
radiographs of the abdomen with or without tomogra-
phy can be obtained to assist in following the progres-
sion of nephrocabcinosls.
TREATMENT
There is no specific treatment for medullary sponge
kidney ( 1 ). Urinary tract infections are treated with
antibiotics. Patients who develop calcium stones may
have primary hyperparathyroidism or may have any
or all of the risk factors for idiopathic calcium stone
disease. Evaluation of patients with calcium stones,
then, should include measurements of the 24-h un-
Indridason et al
Journal of the American Society of Nephrology 1129
nary excretion rates of calcium, oxalate, uric acid, and
citrate. If the serum calcium level is elevated, then the
serum parathyroid hormone level should be mea-
sured. Therapy should be directed at the underlying
abnormality. Thiazide diuretics may be prescribed for
hypercalciunla and albopuninol for hyperunicosunia.
The use of alkali therapy in patients with calciumstone disease warrants further discussion.
Although many patients with medublary sponge kid-
ney have impaired urinary acidification, it does not
follow that alkali therapy will be beneficial. Alkali
therapy should certainly be prescribed for those with
systemic acidemia (complete renal tubular acidosis).
In those with partial renal tubular acidosis or more
subtle impairment of urinary acidification, however,
alkali therapy may raise urine pH and may promote
mntraductab precipitation of calcium apatite. On the
other hand, the study by Higashihara et at. demon-
strates that, in patients with renal hypercalciunia and
low plasma bicarbonate concentrations, alkali ther-
apy decreases urinary calcium excretion and may
decrease the frequency of stone passage ( 1 7). It is also
rational to prescribe alkali therapy for those with
hypocitratunia (12,14,17).
Stones within the collecting system may be treated
with extracorporeal shock-wave lithotnipsy (ESWL).
The role of ESWL in the treatment of parenchymal
stones needs to be elucidated. A study of eight pa-
tients failed to demonstrate fragmentation or evacua-
tion of parenchymal concretions after ESWL (20).
Another study did demonstrate a reduction in the
stone burden of the renal medulla in 1 7 of 22 kidneys
treated with ESWL (29). Seven patients in this study
reported a long-term decrease in frequency of stone
passage.
SUMMARY
Although our patient did not undergo intravenous
urography, we believe that the constellation of clinical
findings strongly supported the diagnosis of medul-
lary sponge kidney. There was no other explanation
for the nephrocalcinosis. He did not have renal tubu-
bar acidosis, hypervitaminosis D, hyperparathyroid-
ism, sarcoldosis, or hypercalcemia, and his history
did not suggest the milk-alkali syndrome. Our patient
demonstrates the association of medullany sponge
kidney and simple hemihypertrophy. in view of his
mother’s history, one or both may be hereditary.
Hypercalciunia and nephrocalcinosis are frequent
manifestations of medublary sponge kidney. A thiazide
diuretic was prescribed to decrease the urinary cab-
cium excretion rate and prevent progression of
nephrocalcinosis, but he has refused to take it. Be-
cause he does not have renal tubular acidosis or
hypocitraturia, alkali therapy is not indicated. A plain
radiograph of the abdomen will be obtained every 6
months to detect progression of nephrocalcmnosis.
REFERENCES
1 . Yendt ER: Medullary sponge kidney. In: Schrier RW,Gottschabk CW, Eds. Diseases of the Kidney. 5th ed.Boston: Little, Brown and Company: 1993:525-533.
2. Jaeger P, Portmann L, Ginabskl J, Campiche M, Burck-hardt P: Dietary factors and medullary sponge kidney ascauses of the so-called idiopathic renal leak of calcium.Am J Nephrol 1987:7:257-263.
3. Higashihara E, Nutahara K, Tago K, Ueno A, Niijima T:Unilateral and segmental medullary sponge kidney: Re-nab function and calcium excretion. J Urol 1984:132:743-745.
4. Fick GM, Gabow PA: Hereditary and acquired cysticdisease of the kidney. Kidney Int 1994:46:951-964.
5. Mayalb GF: The incidence of medullary sponge kidney.Radiology 1970:21:171-174.
6. Ginaiski J, Portmann L, Jaeger P: Does medullarysponge kidney cause nephrohithiasis? Am J Roentgenol1990:155:299-302.
7. Parks JH, Coe FL, Strauss AL: Calcium nephrohithiasisand medullary sponge kidney in women. N Engl J Med1982:306: 1088-109 1.
8. O’Neill M, Breslau NA, Pak CYC: Metabolic evaluation ofnephrohithiasis in patients with medullary sponge kid-ney. JAMA 1981:245:1233-1236.
9. Higashihara E, Nutahara K, Tago K, Ueno A, Niijima T:Medullary sponge kidney and renal acidification defect.Kidney Int 1984:25:453-459.
10. Osther PJ, Hansen AB, Roehl HF: Renal acidificationdefects In medullary sponge kidney. Br J Urol 1988:61:392-394.
1 1 . Backman U, Danielson BG, Felbstrom B, Johansson G,Ljunghall 5, Wikstrom B: Clinical and laboratory find-ings in patients with medullary sponge kidney. In: SmithLH, Robertson WG, Fmnlayson B, Eds. Urohithiasis: Chin-ical and Basic Research. New York: Plenum Press: 1981:113-120.
12. Meyers AM, Whalley N, Martins M, Sonnekus M, Mar-golius LP: Recurrent renal calculi in patients with med-ullary sponge kidney. In: Ryall R, Bais R, Marshall VR,Rofe AM, Smith LH, Walker VR, Eds. Urohithiasis 2. NewYork: Plenum Press: 1994:375-378.
13. Osther PJ, Mathiasen H, Hansen AR, Nissen HM: Un-nary acidification and urinary excretion of calcium andcitrate in women with bilateral medullary sponge kidney.Urol Int 1994:52:126-130.
14. Harrison AR, Rose GA: Medullary sponge kidney. UnolRes 1979;7:197-207.
15. Broadus AE, Dominguez M, Bartter FC: Pathophysiobog-ical studies in idiopathic hypercalciuria: use of an oralcalcium tolerance test to characterize distinctive, hyper-calciunic subgroups. J Clmn Endocninol Metab 1978:47:751-760.
16. Pak CYC, Kaplan R, Bone H, Townsend J, Water 0: Asimple test for the diagnosis ofabsorptlve, resorptive andrenal hypercalciunla. N Engl J Med 1975:292:497-500.
1 7. Higashlhara E, Nutahara K, Nlijima T: Renal hypercal-ciuria and metabolic acidosis associated with medullarysponge kidney: Effect of alkali therapy. Urol Res 1988:16:9�-100.
18. Green J, Szylman P. Sznajder I, Winaver J, Better OS:Renal tubular handling of potassium in patients withmedullary sponge kidney. Arch Intern Med 1984:144:2201-2204.
19. Thompson IM, Rodriguez FR, Spence CR: Medullarysponge kidney and congenital hemihypertrophy. SouthMed J 1987:80:1455-1456.
20. Vandeursen H, Baert L: Prophylactic role of extracorpo-real shock wave hithotnipsy in the management ofnephrocalcmnosis. Br J Urol 1993:71:392-39ff.
2 1 . Nakada SY, Erturk E, Monaghan J, Cockett ATK: Role ofextracorporeal shock-wave hithotripsy In treatment ofurohithiasis in patients with medullary sponge kidney.Urology 1993:41:331-333.

Medullary Sponge Kidney and Congenital Hemihypertrophy
1 130 Volume 7 . Number 8 . 1996
22. Patriquin HB, O’Regan 5: Medullary sponge kidney inchildhood. Am J Roentgenol 1985:145:315-319.
23. Stoll C, Alembik Y, Steib JP, de Saint-Martin A: Twelvecases with hemihypertrophy: Etiology and follow up.Genet Couns 1993:4:119-126.
24. Bueno I, Ventura P, Samper MP, Perez Gonzalez JM,Bueno M: Congenital hemihypertrophy. Genet Couns1993:4:231-234.
25. Beckwith JB, Kiviat NB, Bonadio JF: Nephrogenic rests,nephrobhasomatosis, and the pathogenesis of Wilms’tumor. Pediatr Pathol 1990:10:1-36.
26. Tomooka Y, Onitsuka H, Goya T, et at.: Congenital
hemihypertrophy with adrenal adenoma and medullarysponge kidney. Br J Radiol 1988:61:851-853.
27. Sprayregen 5, Strasberg Z, Naidich TP: Medullarysponge kidney and congenital total hemihypertrophy. NYState J Med 1973:73:2768-2772.
28. Ginaiski J, Schnyder P, Portmann L, Jaeger P: Medul-lary sponge kidney on axial computed tomography:Comparison with excretory urography. Eur J Radiol199 1: 12: 104-107.
29. Holmes SAy, Eardley I, Cony DA, Nockler I, WithfieldHN: The use of extracorporeal shock wave lithotripsy formedullary sponge kidneys. Br J Urol 1992:70:352-354.