
MEDICINES POLICY - Bolton NHS FT · Medicines Policy is peer-reviewed and validated by the...
130
Version 3.0 POLICY MEDICINES POLICY Page 1 of 130 Date August 2016 Next Review Date August 2019 MEDICINES POLICY Document type: Policy Version: 3.0 Author (name): Ann Eccles, Jiri Prochazka Author (designation): Deputy Chief Pharmacist, Senior Pharmacist Validated by Medicines Safety Group Committee Date validated 8 th June 2016 Ratified by: Clinical Governance and Quality Committee Date ratified: 3 rd August 2016 Name of responsible committee/individual: Medicines Safety Committee Name of Executive Lead (for policies only) Steve Hodgson Master Document Controller: Suzanne Schneider Date uploaded to intranet: 22/08/16 Key words administration, storage, controlled drugs, disposal Review date: August 2019 Equality Impact Bolton NHS Foundation Trust strives to ensure equality of opportunity for all service users, local people and the workforce. As an employer and a provider of healthcare Bolton NHS FT aims to ensure that none are placed at a disadvantage as a result of its policies and procedures. This document has therefore been equality impact assessed to ensure fairness and consistency for all those covered by it regardless of their individuality. The results are shown in the Equality Impact Assessment (EIA).
Transcript of MEDICINES POLICY - Bolton NHS FT · Medicines Policy is peer-reviewed and validated by the...
Version 3.0 POLICY MEDICINES POLICY Page 1 of 130
Date August 2016 Next Review Date August 2019
MEDICINES POLICY
Document type: Policy
Version: 3.0
Author (name): Ann Eccles,
Jiri Prochazka
Author (designation): Deputy Chief Pharmacist,
Senior Pharmacist
Validated by Medicines Safety Group Committee
Date validated 8th June 2016
Ratified by: Clinical Governance and Quality Committee
Date ratified: 3rd August 2016
Name of responsible committee/individual: Medicines Safety Committee
Name of Executive Lead (for policies only) Steve Hodgson
Master Document Controller: Suzanne Schneider
Date uploaded to intranet: 22/08/16
Key words
administration, storage, controlled drugs, disposal
Review date: August 2019
Equality Impact
Bolton NHS Foundation Trust strives to ensure equality of opportunity for all service users, local people and the
workforce. As an employer and a provider of healthcare Bolton NHS FT aims to ensure that none are placed at a
disadvantage as a result of its policies and procedures. This document has therefore been equality impact assessed
to ensure fairness and consistency for all those covered by it regardless of their individuality. The results are shown
in the Equality Impact Assessment (EIA).

Version 3.0 POLICY MEDICINES POLICY Page 2 of 130
Date August 2016 Next Review Date August 2019
Version Control Schedule
Version Type of Change
Date Revisions from previous issues
2.0 MAJOR April 15
Key changes (not exhaustive list):
Medicines Safety Group now included as key committee.
Patient’s bodyweight on outpatient prescriptions for children now required.
Insulin preparations now to be prescribed by brand names
Use of stop date clarified, medicines will be administered on the stop date.
Explicitly stated that delegation under PGD prohibited.
Second check now not required for oral tramadol in addition to Oramorph.
Erroneous entries in controlled drugs register cannot be crossed out.
Second check now specifically required for all calculations.
The same member of ward staff cannot order and collect medicines from Pharmacy.
Ketamine is now a Controlled Drug
Refers to newly produced Guidelines for the management of patients with a history of opioid misuse.
Nurse competency assessment requirement to discharge patient with medication.
New Appendix - Procedure for Obtaining Medicines Out of Hours.
Appendix 3: Role of Unregistered Staff in the Administration of Medicines - Substantial changes.
Specimen signatures of persons authorized to order controlled drugs are only to be submitted once every 12 months.
Appendix 4: SOP for Controlled Drugs - now includes
information on opening, closing & transfer of wards.
Covert administration now separate policy.
Blank records on the wardex are not acceptable, as they indicate a dose omitted without justification.
Version 3.0 POLICY MEDICINES POLICY Page 3 of 130
Date August 2016 Next Review Date August 2019
3.0
Major
June
16
Key Changes:
CD section and Standard Operating Procedure updated including guidance on disposal of unused Patient Controlled Analgesia (PCAs)
If the start date was prior to admission the abbreviation ‘GP’ (General Practitioner) should be written in the start date box on the wardex.
Tapentadol included as a CD in Appendix 5
Medicines Reconciliation section updated
Key cupboards use included
Reference to FT Document ‘Choosing medicines for patients unable to take solid oral dosage forms’
Second person check in paediatrics reviewed.
Ambient room temperature monitoring included
PGD template updated
Medical gases storage updated
Reference to Naloxone national guidance included
Procedure for obtaining meds out of hours updated
Reference to Policy on completing Medicines Administration Record (MAR) charts in Community Services
Guidance on use of multi dose vials
List of Critical Medicines updated
Self-administration flowchart updated
Use of Patients Own Drugs (PODs) flowchart updated
Pharmacy Audit calendar included as Appendix 20
Version 3.0 POLICY MEDICINES POLICY Page 4 of 130
Date August 2016 Next Review Date August 2019
Table of contents
Table of contents ................................................................................................................. 4
Introduction .......................................................................................................................... 6
Purpose of the Policy ........................................................................................................... 7
Definitions ............................................................................................................................ 8
Key Staff and Staff Groups Involved in Medicines Management ......................................... 9
Prescribing of Medicines ................................................................................................... 12
Patient Group Directions (PGDs) ...................................................................................... 23
Administration of Medicines ............................................................................................... 25
Controlled Drugs................................................................................................................ 34
Use of Methadone for Management of Opioid Withdrawal ................................................ 40
Guidelines for the Handling of Illicit Substances ................................................................ 44
Admission to bed based services and medicines reconciliation ........................................ 47
Medicines on discharge ..................................................................................................... 50
Mental capacity and Covert Administration of Medicines .................................................. 53
Self-Administration of Medicines ....................................................................................... 54
Unlicensed medicines ........................................................................................................ 56
Storage of Medicines ......................................................................................................... 59
Supply of Medicines .......................................................................................................... 64
General rules for supply of medicines to Community Services .......................................... 69
Carriage of Medicines ........................................................................................................ 71
Disposal and Return of Medicines ..................................................................................... 72
Reporting and Management of Medication Errors and Near Misses ................................. 74
Medicines Management Training....................................................................................... 76
Monitoring Compliance ...................................................................................................... 77
Appendix 1- Protocol for safe and secure handling of medicines in Community Services. 79
Appendix 2 – Patient Group Direction Template ............................................................... 85
Appendix 3 – The Role of Unregistered Staff in the Administration of Medicines .............. 91
Appendix 4 – SOP for Controlled Drugs for Royal Bolton Hospital .................................... 95
Appendix 5 - Storage and Recording Requirements for Controlled Drugs ...................... 101
Appendix 6 - Protocol for Use of Controlled Drug Denaturing Kits in Community ........... 103

Version 3.0 POLICY MEDICINES POLICY Page 5 of 130
Date August 2016 Next Review Date August 2019
Appendix 7 - Form for the removal or destruction of unauthorised drugs or other suspicious substances ...................................................................................................................... 105
Appendix 8 - Self Administration of Medicines Algorithm ................................................ 106
Appendix 9 - Self Administration of Medicines Assessment Record ............................... 106
Appendix 10 - Self Administration Consent Form ............................................................ 107
Appendix 11 - Information for Patients about Self Administration of their Medicines ....... 109
Appendix 12a – Disclaimer for the Prescribing of Unlicensed Medication – Single Consultant ....................................................................................................................... 111
Appendix 12b – Disclaimer for the Prescribing of Unlicensed Medication – Multiple Consultants ..................................................................................................................... 112
Appendix 13 – List of Unlicensed Medicines that do not require a disclaimer ................. 113
Appendix 14 - Fridge Monitoring Sheet ........................................................................... 113
Appendix 15 - Procedure for Obtaining Medicines Out of Hours ..................................... 115
Appendix 16 - Procedure for Dispensing medication for urgent discharge when Pharmacy is closed …………………………………………………………………………………………..115
Appendix 17 - Algorithm for the use of patients’ own drugs (PODs) ................................ 117
Appendix 18 - Protocol to remove discontinued and out of date medication from patients home …………………………………………………………………………………………..119
Appendix 19 – Assembly of Patient’s Medicines for Discharge. Assessment Criteria and Record of Competence .................................................................................................... 123
Appendix 20 – Medicines management annual audit ...................................................... 123
References ...................................................................................................................... 126
EQUALITY IMPACT ASSESSMENT OF MEDICINES POLICY ..................................... 129
Version 3.0 POLICY MEDICINES POLICY Page 6 of 130
Date August 2016 Next Review Date August 2019
Introduction
1. Medicines management encompasses the way medicines are:
selected
procured
delivered
prescribed
prepared
administered
reviewed
disposed
2. This will optimise the contribution that medicines make to producing informed and desired outcomes of patient care (Audit Commission 2001).
3. It is a requirement for NHSLA Risk Management Standards for acute trusts and
Care Quality Commission that the Trust has a medicines policy with clear lines of accountability for medicines management.
4. Medicines are used in all areas of the Trust and are the responsibility of all
healthcare care professionals.
5. The importance of appropriate procedures to ensure the safe, effective and economic use of medicines is paramount and is a key component of clinical governance. There is a need to contribute to maximising the effective use of medicines, minimising medicine-related morbidity for patients and using Trust resources effectively.

Version 3.0 POLICY MEDICINES POLICY Page 7 of 130
Date August 2016 Next Review Date August 2019
Purpose of the Policy
6. The purpose of the Medicines Policy is to provide an operational framework that includes all activities associated with the routine use of medicines, including prescribing, dispensing and supply, storage and security, administration and disposal. The policy has several aims:
Ensure safe systems of work, and therefore, protect patients and staff by reducing risk and the potential for error.
Dispel confusion and provide clarity.
Ensure all legislation and guidance is adhered to with respect to medicines.
Provide a framework for teaching, training, audit and future development.

Version 3.0 POLICY MEDICINES POLICY Page 8 of 130
Date August 2016 Next Review Date August 2019
Definitions
7. A Practitioner is a person who is registered with a recognized professional body.
8. A ‘Wardex’ is the term used for the inpatient prescription chart used in inpatient
bed areas.
9. Medicine Administration Record Sheet (MARS) is the term used for the patient prescription chart used in community areas.
10. An FP10 is the term used for prescriptions issued by GPs, non-medical
prescribers or hospital doctors in a clinic setting.
11. Bed based services’ is the term used to refer to services that provide in-patient care e.g. wards in Hospital or Darley Court.

Version 3.0 POLICY MEDICINES POLICY Page 9 of 130
Date August 2016 Next Review Date August 2019
Key Staff and Staff Groups Involved in Medicines Management
12. Executive Directors will ratify the Medicines Policy.
13. Medicines Policy is peer-reviewed and validated by the Medicines Safety Group.
14. They will maintain an overview of significant risks via the Risk Management
Committee and by monitoring the Risk Register.
15. The Chief Executive will designate an Accountable Officer who will be responsible for all aspects of the safe and secure management of Controlled Drugs.
16. Divisional Directors will ensure their local managers recognise which sections
of the Medicines Management Policy and appendices must be implemented within their areas, that they promote use of the policy by all staff and that they communicate any changes in policy to staff in a timely manner. They will ensure their local managers highlight medicines-related risks specific to their area and consider methods of risk reduction. They will seek advice from divisional pharmacists when necessary.
17. Heads of Division will ensure that the Trust’s Medicines Policy and its
appendices are implemented throughout the areas they control, in order that the risks associated with medicine use are minimized, Trust resources are used effectively and patients’ benefit therapeutically. They will promote the policy to consultants and they, in turn, to their teams.
18. Heads of Service will oversee the application of this policy into their services
and ensure its implementation is undertaken within their management structure, with the necessary controls to achieve the policy’s aims. They will liaise with divisional pharmacists to obtain expert medicines advice when necessary.
19. Divisional Clinical Leads will be familiar with all applicable sections of the policy
and will ensure that appropriate mechanisms are in place to implement these in their areas. They will liaise with and support matrons to ensure ward / department managers are carrying out safe medicines practice.
20. Matrons will be familiar with all applicable sections of the policy and will liaise
closely with their General Managers, Ward and Department Managers, and Divisional Pharmacists, to ensure the appropriate medicine-related procedures are followed. They will review controls following incidents and will ensure day to day adherence to the policy.
21. Ward and Department Managers will ensure the procedures contained within
the Medicines Policy and appendices are followed by all their healthcare
Version 3.0 POLICY MEDICINES POLICY Page 10 of 130
Date August 2016 Next Review Date August 2019
professional staff. They will ensure that all staff are aware of how to access the policy, and appendices.
22. They must bring the policy to the attention of all new staff who deal with
medicines as part of their daily role. They will identify any areas of significant risk and take action to control this risk. They will be familiar with relevant sections of the policy and appendices and promote and demonstrate good practice associated with medicines use.
23. All health care professional staff will ensure they are familiar with all relevant
sections of the Medicines Policy and will follow the correct procedure when undertaking any medicine-related task. They will report any concerns relating to medication risk to their line manager or pharmacist so action can be taken. Staff will report any medication incidents or near misses using the hospital incident reporting system. All health care professionals involved in the daily use of medicines must complete mandatory medicines management training as described in the Trust’s mandatory training needs analysis every two years.
24. The Chief Pharmacist has statutory responsibility as superintendent pharmacist
under the Human Medicines Regulations 2012 and the Medicines Act. S/he is responsible for Medicines Management throughout the Trust on behalf of the Chief Executive and is responsible for monitoring and disseminating results of audits, highlighting medication risks, reviewing financial medicines pressures and managing the introduction of new medicines.
25. The Drugs and Therapeutics Committee reports to the Clinical Governance and
Quality Committee. It is chaired by the Medical Director with representation from senior medical and Pharmacy staff. It considers new drug requests for adding to the Bolton NHS Foundation Trust Formulary.
26. The Clinical Standards Board and the Clinical Standard Operational Group are
health economy groups that agree local pathways of care and clinical guidelines with reference to national guidance including NICE guidance. They take local accountability, identify audit requirements, respond to monitoring, work with local clinical network groups on pathways of care and clinical guidelines. They agree prioritisation of pathway and guideline development for Bolton Health Economy and promote high quality, rational, cost-effective prescribing and clinical care across the whole of Bolton.
27. It is their role to recognise potential implications of new drugs and new
technologies on clinical care, including changes on local guidance, service and cost implications.
28. Membership from the Trust includes the Chief Pharmacist, the Medical Director
and the Deputy Director of Nursing.
Version 3.0 POLICY MEDICINES POLICY Page 11 of 130
Date August 2016 Next Review Date August 2019
29. The Trust Clinical Governance and Quality Committee is provided with assurance on the divisional audit programmes, forward plans, multidisciplinary involvement in clinical audit, and also approves the development of appropriate clinical guidelines and care pathways within the Foundation Trust in response to NICE Guidance and other relevant national guidance. It will receive quarterly reports from pharmacy and a senior pharmacist is a member of this committee. The committee reports into the Quality and Assurance Committee
30. Medicines Safety Group The Purpose of the group is to develop, implement
and maintain a medication governance strategy and work plan within Bolton Foundation Trust around the safe and effective use and management of medicines. The Medicines Safety Group reports into the Clinical Governance and Assurance Committee.
31. Antibiotic Stewardship Committee The Antimicrobial Stewardship Committee is
a multidisciplinary Committee set up to develop and implement the Trust’s antimicrobial stewardship programme for all adults and children admitted to hospital. The ASC is accountable to the Trust’s Infection Control Committee and the Medicines Safety Committee. The purpose of the committee is:
Provide staff with clear guidance on the principles of appropriate antimicrobial use. This is supported by specific prescribing guidance which is available on the intranet.
Inform all staff of their responsibilities in the safe, effective and appropriate prescribing, administration and monitoring of antimicrobials in adults and children.
Optimise clinical outcomes whilst minimising the unintended consequences of antibiotic use such as the acquisition of HCAI, adverse drug events and the emergence of antibiotic resistance.
32. The Head of Governance ensures good practice is maintained, the
organization learns from its mistakes and the quality of service provided to patients continually improves.
33. All staff have a personal and professional responsibility to act within their own
scope of practice / professional standards / training with respect to the handling, distribution, prescription, storage and administration of medicines. Staff responsible for the safe and effective use of medicines include:
Pharmacy Staff.
Medical Staff.
Nursing Staff.
Other professional groups (AHPs, ODPs)
All Other Staff (Transport, Security, Management)

Version 3.0 POLICY MEDICINES POLICY Page 12 of 130
Date August 2016 Next Review Date August 2019
Prescribing of Medicines
PRESCRIBING OF MEDICINES (IN-PATIENTS)
34. All prescriptions must be written by a medical or dental practitioner or an approved Non-Medical Prescriber.
35. Non-Medical Prescribing (NMP) is prescribing by registered nurses, midwives,
health visitors, pharmacists, optometrists, radiographers and specified allied health professionals who have successfully completed a recognized NMP qualification at university. Non-medical prescribers must only ever prescribe within their scope of competence, knowledge and experience. NMPs working in hospital settings must ensure that the patient’s drug chart/wardex is signed and clearly marked “NMP” or with their prescribing qualification i.e. V300
36. Medical students, physician assistants or nursing staff not registered as Non-
Medical Prescribers are not allowed to sign prescriptions or to prepare prescriptions for signature by medical staff.
37. The patient’s name, hospital number, date of birth, ward, allergy status,
bodyweight and the name of the consultant must be clearly visible on the prescription sheet. This may be handwritten or preferably a combination of handwritten and ID label.
38. The date on which treatment is to commence must be entered on the
prescription sheet. Dates where treatment is not intended or when the time of administration has already been missed, must be crossed out on the chart (e.g. treatment to start the next day or post op or treatment to be stopped after a number of days)
39. The name of the medicine should be written legibly in black ink using approved
generic names. Proprietary names (i.e. brand names) must not be used. Exceptions to this rule are:
multi-ingredient preparations with no approved generic names
products whose proprietary names define a specific formulation (e.g. slow-release theophylline preparations)
insulin preparations
40. Prescribers should consider the contraindications and interactions with other medicines and arrange for appropriate monitoring of medication & its effects. If the drug being prescribed requires the patients renal function to be confirmed before the drugs is commenced, U&Es should be taken as a base line before the drug is prescribed e.g.

Version 3.0 POLICY MEDICINES POLICY Page 13 of 130
Date August 2016 Next Review Date August 2019
41. LMWH and aminoglycosides. Liver function should be monitored in the same way for e.g. amiodarone, methotrexate
42. The dose must be expressed in S.I. Units. Quantities less than 1 gram must be
written as milligrams. Decimal points should be avoided, for example 500mg not 0.5g to avoid confusion. Whenever a decimal point is necessary, great care must be exercised by both the prescriber and the nurse administering the drug. The terms MICROGRAM and NANOGRAM must not be abbreviated but must be printed in full and used for quantities less than one milligram. When prescribing drugs expressed as Units, the full word must be used and not abbreviated to “U”. Only the following abbreviations are acceptable:-
Quantity Approved Abbreviation
milligram mg
gram g
kilogram kg
litre L
millilitre ml
millimole mmol
43. The dose required must not be expressed in terms of the dosage form for
single ingredient preparations e.g. “ATENOLOL 2 tablets” is not acceptable. It should be written as e.g. “ATENOLOL 100mg”.
ROUTE OF ADMINISTRATION
44. Only the following abbreviations are acceptable:
Route Approved Abbreviation
Intravenous IV
Intradermal ID
Intramuscular IM
Subcutaneous SC
By mouth PO or O
Sublingual SL / Sub-ling
Per rectum PR
Per vagina PV
By inhalation INH
By nebuliser NEB
Topically TOP
Right eye RE
Left eye LE
Nasogastric NG
Percutaneous Endoscopic Gastrostomy tube
PEG

Version 3.0 POLICY MEDICINES POLICY Page 14 of 130
Date August 2016 Next Review Date August 2019
45. All other routes must be written in full.
46. Only one route of administration may be specified for each medicine e.g. PARACETAMOL PO/IV is not acceptable.
47. When the route of administration is changed the dose must be recalculated by
the prescriber. DOSAGE FREQUENCY
48. For ‘As required’ medicines the frequency of administration must be written by the prescriber. A maximum dose in 24 hours must also be stated.
49. Pre-medication (before surgical procedures) should be given in accordance
with a locally agreed protocol.
50. For “regular medicines” prescribing times should be in accordance with regular medicine rounds wherever possible. A 6am dose should only be ordered if there is a good therapeutic reason.
PRESCRIBER’S SIGNATURE
51. All items on the inpatient prescription sheet must bear the full signature of the prescriber. The prescriber must print their name clearly on the first entry of the prescription.
52. For controlled drugs, the prescriber’s full signature is always necessary (see
Section 9).
53. The signature of a medical student or non-registered prescriber is not acceptable. Prescribers must complete the full prescription personally.
DISCONTINUING MEDICINES
54. The date when a medicine is discontinued must be entered into the “stop date” box; medicines will still be administered until the last dose on the ‘stop date’.
55. The entry must be initialed on the prescription chart by the prescriber
discontinuing the medicine.
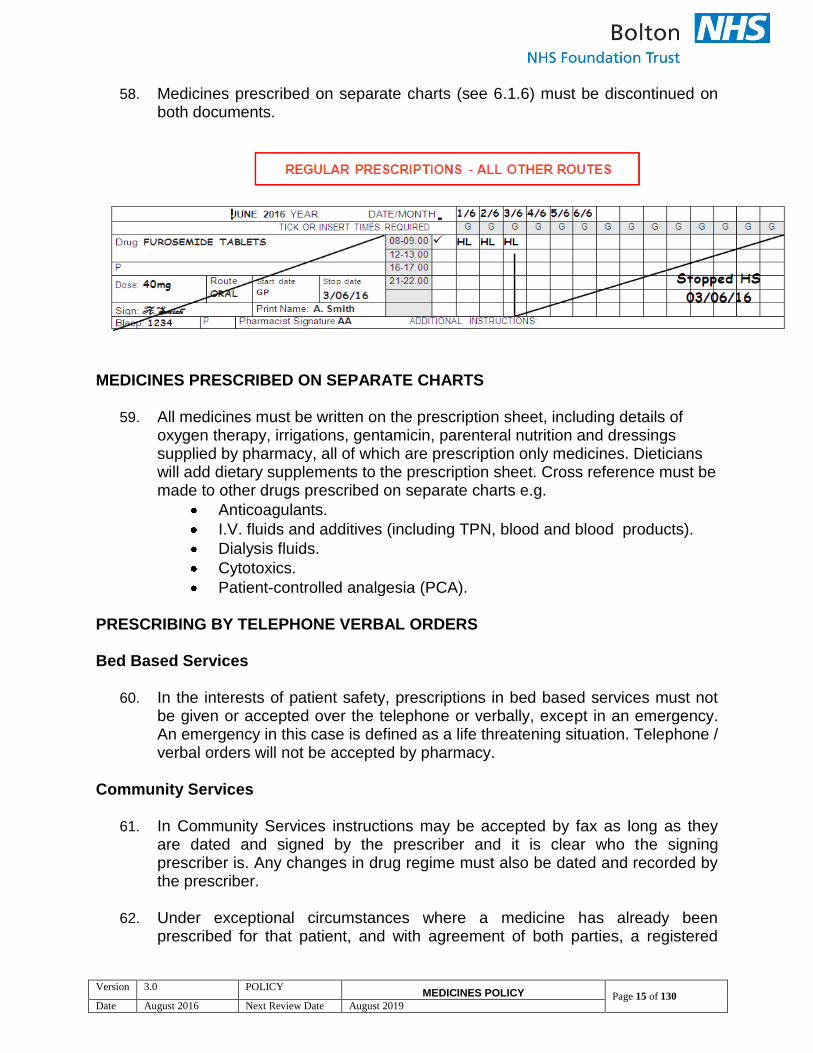
56. A diagonal line should be drawn through the prescription so that its cancellation is obvious, but the prescription should not be obliterated. A vertical line should be used to indicate the time at which the prescription is to stop.
57. Incorrect entries must have a line drawn through and the word ‘cancel’ written
against them by the prescriber and signed. See below:
Version 3.0 POLICY MEDICINES POLICY Page 15 of 130
Date August 2016 Next Review Date August 2019
58. Medicines prescribed on separate charts (see 6.1.6) must be discontinued on both documents.
MEDICINES PRESCRIBED ON SEPARATE CHARTS
59. All medicines must be written on the prescription sheet, including details of oxygen therapy, irrigations, gentamicin, parenteral nutrition and dressings supplied by pharmacy, all of which are prescription only medicines. Dieticians will add dietary supplements to the prescription sheet. Cross reference must be made to other drugs prescribed on separate charts e.g.
Anticoagulants.
I.V. fluids and additives (including TPN, blood and blood products).
Dialysis fluids.
Cytotoxics.
Patient-controlled analgesia (PCA). PRESCRIBING BY TELEPHONE VERBAL ORDERS Bed Based Services
60. In the interests of patient safety, prescriptions in bed based services must not be given or accepted over the telephone or verbally, except in an emergency. An emergency in this case is defined as a life threatening situation. Telephone / verbal orders will not be accepted by pharmacy.
Community Services
61. In Community Services instructions may be accepted by fax as long as they are dated and signed by the prescriber and it is clear who the signing prescriber is. Any changes in drug regime must also be dated and recorded by the prescriber.
62. Under exceptional circumstances where a medicine has already been
prescribed for that patient, and with agreement of both parties, a registered
Version 3.0 POLICY MEDICINES POLICY Page 16 of 130
Date August 2016 Next Review Date August 2019
nurse may accept a telephone message from a prescriber for an alteration (e.g., dose alteration) to a prescription to be administered in the patient’s home under following conditions:
63. Two persons must acknowledge the message, one of which must be a
registered nurse. The second person will be selected at the discretion of the registered nurse.
64. The nurse receiving the call must repeat the prescription to the prescriber to
ensure accuracy.
65. A record must be made of the nature of the message, date, time; name of the prescriber and both parties receiving the instruction must witness the record.
66. The alteration must be confirmed in writing by the prescriber on the next normal
working day.
67. Verbal alteration cannot be accepted for Controlled Drugs. VALIDITY OF PRESCRIPTIONS
68. Unless the course of treatment is clearly specified, the prescription will be considered valid until cancelled by the prescriber (see 6.1.5 and 6.1.11). This should be done by using the “stop date” box, all IV antibiotics should be reviewed daily, with the exception of deep seated/high risk infections (e.g. meningitis, endocarditis, bone and joint infection) which MUST have a stop or review date. See the Trust Guide Antibiotic Policy for further information on prescribing antibiotics.
69. Prescriptions must be re-written if the patient is re-admitted or transferred from
another hospital.
70. Medicines Charts are only valid in the organisation where originally written.
71. Only Bolton NHS Foundation Trust Medicines Charts can be used in any FT service.
PRESCRIBING BY STAFF FOR THEMSELVES AND THEIR FAMILIES
72. It has been agreed within the Bolton NHS Foundation Trust that:
Medical staff / Non-Medical Prescribers (NMPs) may not prescribe for themselves or their families, in line with current General Medical Council (GMC) and other relevant professional body’s recommendations.
Medical staff / Non-Medical Prescribers may only prescribe for any other staff members when they have been referred for treatment to the Trust as a

Version 3.0 POLICY MEDICINES POLICY Page 17 of 130
Date August 2016 Next Review Date August 2019
registered patient and they are formally registered as an outpatient, inpatient, AED patient, day case or Occupational Health patient.
In emergencies, staff should attend existing facilities in out-patients, the Accident & Emergency Department or Occupational Health, where a senior doctor will prescribe according to the formulary as necessary. The current prescription charge will be payable if applicable.
Green FP10 (HP) prescription forms should never be used by medical staff / Non-Medical Prescribers to prescribe for themselves or their families. Green FP10 (HP)s must not be used to order food or toilet articles and other prescriptions which are not drugs or appliances other than those specified in the drug tariff. They should not be used for unlicensed creams / ointments as substantial extra charges are imposed on the Trust. The use of these forms is routinely audited. Invoices will be raised and disciplinary proceedings considered if any unauthorized use is found.
ESCALATING CONCERNS
73. Any concerns about unusual, excessive or inappropriate prescribing of
medicines should be raised with the Ward Pharmacist and an incident form completed.
RE-WRITING OF PRESCRIPTIONS
74. Prescriptions must be rewritten by a medical practitioner or an approved non-medical prescriber (NMP).
75. When a prescriber rewrites a prescription chart, they take full clinical
responsibility for the prescription.
76. Rewriting of prescription charts should normally take place during daytime by medical prescribers.
77. If a change in dose, frequency or route of administration is required, the whole
prescription (for the drug affected) must be re-written and the original entry discontinued.
78. Prescription charts should also be re-written when they become untidy
especially after medications have been stopped and / or changed or the prescription form has been contaminated in any way (eg spillage etc).
79. When re-writing prescriptions, the prescriber must ensure that the date entered
is the date when the therapy commenced and not the date of re-writing. If the start date was prior to admission the abbreviation ‘GP’ (General Practitioner) should be written in the start date box. It should be indicated on the prescription sheet that the treatment has been reviewed. The date of re-writing the

Version 3.0 POLICY MEDICINES POLICY Page 18 of 130
Date August 2016 Next Review Date August 2019
prescription should be recorded in the rewrite box on the front of the prescription sheet.
80. Every re-written prescription chart must be checked for accuracy by a
pharmacist.
81. A pharmacist must also ensure that the medication history section and all the pharmacy endorsements and annotations are copied onto the new chart.
OTHER ENTRIES
82. The ‘Special Instructions’ box on the front of the wardex must be used in the following situations:
On insulin
Type 2 diabetic patient
Special diet
On warfarin
This must also be recorded on any subsequent prescription chart.
83. The prescriber may indicate the length of treatment e.g. for 5 days. This may be confirmed by completing the “stop date” box in advance.
BOLTON NHS FOUNDATION TRUST AND GREATER MANCHESTER MEDICINE MANAGEMENT GROUP FORMULARIES
84. New products are introduced by the Drugs & Therapeutics Committee in consultation with Trust Consultants, local GPs and the CCG.s.
85. The joint formulary across Greater Manchester has been produced under the
direction of the Greater Manchester Medicines Management Group (GMMMG). The aim of the formulary is to maximise safe, effective and economic prescribing. It ensures that patients receive seamless care across the primary-secondary care interface and reduces the need for switching programmes. Adherence to the formulary is strongly recommended by GMMMG and this formulary supersedes all local formularies. The formulary is applicable to new initiations and treatments in approximately 80% of patients. http://www.nyrdtc.nhs.uk/GMMMG/Groups/formulary/html/formulary.html
86. Newly prescribed items which are not stocked will need Consultant approval
(with reasons for the choice of non-formulary therapy) before they can be ordered. Forms for this purpose can be requested from the relevant senior pharmacist for the specialty- via the pharmacy office -5555 or via a New Drug Request Form which should be submitted to the Drugs and Therapeutics Group. An Individual Funding Request may be used for specific patient requests.
Version 3.0 POLICY MEDICINES POLICY Page 19 of 130
Date August 2016 Next Review Date August 2019
87. When using the patient’s own drugs during their stay and at discharge, they need to be transferred to the patient’s locker and administered in the usual manner. These drugs remain the property of the patient and permission must be sought from the patient to dispose of any discontinued or out of date medicines prior to discharge. They must not be administered to any other patient.
88. If the patient is transferred, the drugs must be sent with the patient. See
Section on Controlled Drugs.
89. If a patient is admitted on a non-formulary preparation which is not stocked by pharmacy and patient’s own supply is not available or not suitable for use, then the pharmacy department will order a small supply to cover. It will only be ordered if it cannot be replaced by a formulary medicine.
SUPPLY OF PRESCRIBED MEDICINES
90. Medicines are unlike any other items of commerce and for this reason the purchase, storage and distribution must be under the control of a pharmacist. The Trust Standing Financial Instructions delegates the financial responsibility, within pre-set limits, for tenders and the signing of orders for medicines to the Chief Pharmacist and authorised deputy, who have procedures to ensure that legal and ethical requirements are met. Medical, nursing, technical and other staff are not permitted to undertake contracting or tendering for, or purchasing of, medicinal products intended for administration to patients within the Trust.Staff must also not accept free samples of any medication.
OUT-PATIENT PRESCRIPTIONS
91. The requirements for out-patient prescriptions are generally as indicated in for inpatient prescription but see also prescriptions for Controlled drugs.
92. Outpatient prescribing must be in line with the Out Patient Prescribing Policy. A
maximum of 28 days’ supply will be dispensed, with ‘when required’ (prn) analgesics a small pack will be supplied unless they are being taken regularly when two packs will be given. An original pack will be dispensed for inhalers and topical preparations unless circumstances dictate that a different supply is necessary. This includes:
Hospital only medicines - these cannot be prescribed by General Practitioners.
Clinical trial medicines.
Pulsed / cyclical treatment.
Reducing doses of drugs e.g. steroids will be supplied for up to 4 weeks, then passed on to GP
Drugs for tuberculosis treatment.
Haematology treatment.
Chemotherapy treatment
Version 3.0 POLICY MEDICINES POLICY Page 20 of 130
Date August 2016 Next Review Date August 2019
Drugs to ensure sufficient supply over public / bank holidays.
Drugs classified as red by the Greater Manchester Medicines Management Group.
PRESCRIBING USING THE PRESCRIPTION CHART General Statements
93. The “P” section in all parts of the chart is for pharmacy annotation. Pharmacists may also provide additional information / instruction in the “Additional Instructions” box. Pharmacists write in green pen to distinguish their entries from the prescriber.
Patient Demographics and Individual Information
94. All sections must be completed.
95. Known allergies and intolerances as well as the record of completion of the VTE Risk Assessment must be completed and signed by the prescriber.
96. A patient sticker should be used but if none are available the patient name
must be clearly written together with their RBH Unit Number and their RMC number.
Medication on Admission
97. This section is generally completed by pharmacy staff. When pharmacy staff are not available at admission it is acceptable to complete the medication history section and the remainder will be completed by pharmacy staff.
Intravenous Antibiotics
98. Intravenous Antibiotics:
When prescribing intravenous anti-infectives (antibiotics, antifungals and antivirals), the indication for treatment must be included – Generalised use of the term “Infection” is not acceptable. All prescriptions for antibiotics must state on that prescription chart and in the case notes the clinical indication and intended treatment duration (or review date) of the antibiotic prescribed. The indication should be as specific as is known at the time (e.g. ‘sepsis? cause’) and must be updated as more information is available.
• With the exception of high risk or deep seated infections (e.g. empyema, endocarditis, liver abscess, bone and joint infection) requiring prolonged intravenous therapy, all IV antibiotics must be reviewed every 24 hours.
• High risk or deep seated infections must have either a stop or review date documented both in the medical notes and on the prescription chart. This will allow the prescribing team to assess clinical progress, microbiology
Version 3.0 POLICY MEDICINES POLICY Page 21 of 130
Date August 2016 Next Review Date August 2019
results and continued appropriateness of therapy, including choice of agent(s), route, dose and frequency (including any necessary adjustments for worsening or improving organ function).
• Refer to the Trust Antibiotic Stewardship Policy.
99. A stop date or a review by date must be added at the time of prescribing. All prescriptions for intravenous antibiotics turn Red after two days. This means that nursing staff will question the validity of the prescription if it has not been reviewed
Oral Anti- Infectives (Antibiotics, Antifungals and Antivirals)
100. The same requirement for indication, stop or review date and extended duration apply for oral anti-infectives as for intravenous anti-infectives.
As Required Medication
101. For ‘As required’ medicines the frequency of administration must be written by the prescriber. A maximum dose in 24 hours must also be stated.
Regular Injections (not antibiotics)
102. Any regular injections except antibiotics must be prescribed in this section. Regular Prescriptions (all other routes)
103. This includes topical, inhaled, rectal etc as well as oral. It is NOT for IVs.
104. As with all other prescriptions, each entry must be signed and dated. Once stopped, the date and the reason for stopping the prescription must be added. The prescription requires bleep number, signature and printed name of the prescriber.
Once Only Medications
105. This section is intended for medications that will only normally be administered once, such as prophylactic antibiotics, pre-operative medications, sedation, vaccines, etc.
Insulin
106. This section is intended to be used for patients who are prescribed insulin by injection.
Venous Thromboembolism (VTE) Risk Assessment
107. All patients should be risk assessed on admission and when there is a significant change in their condition as to whether they are at risk of a VTE

Version 3.0 POLICY MEDICINES POLICY Page 22 of 130
Date August 2016 Next Review Date August 2019
and prophylactic treatment should be initiated if indicated. The pre-printed prescription for a formulary low molecular weight heparin should be completed if indicated.

Version 3.0 POLICY MEDICINES POLICY Page 23 of 130
Date August 2016 Next Review Date August 2019
Patient Group Directions (PGDs)
108. A Patient Group Direction (PGD) is a written instruction for the supply or administration of medicine (or medicines) where the patient may not be individually identified before presenting for treatment.
109. All PGDs have to be drawn up locally and must meet legal, ethical and trust
criteria. The following should be referred to when developing or updating PGDs:
Pharmacy Department - NHS Bolton Foundation Trust. “SOP for the Introduction of a new Patient Group Direction (PGD) and Review Process for Existing PGDs”. (2012).
The template for development of a local PGD is contained as Appendix 2 of this Policy.
National Prescribing Centre (NPC) “Patient Group Directions” guide and competency framework (2009) http://www.npc.nhs.uk/non_medical/resources/patient_group_directions.pdf
110. Only the following registered healthcare professionals, acting as named
individuals, can use PGDs:
nurses
midwives
health visitors
paramedics
optometrists
podiatrists
chiropodists
radiographers
orthoptists
physiotherapists
pharmacists
dieticians
occupational therapists & prosthetists
speech & language therapists.
dental hygienists
dental therapist
Version 2.0 POLICY MEDICINES POLICY Page 24 of 130
Date June 2016 Next Review Date June 2019
111. A record or list of the individuals named as competent to use PGDs will be kept
by a senior person in each service – only these staff will be able to operate within a PGD. The PGD is a legal document and every healthcare professional must read and sign the PGDs prior to use, sending a copy of the signature sheet to their manager.
112. The healthcare professional should refer to the relevant PGD at all times when
operating within them i.e. a copy of the relevant PGD should be readily available.
113. All staff operating within PGDs are expected to participate in audit of the use of
PGDs, if necessary/appropriate. 114. A PGD can include flexible dose ranges so that staff can select the most
appropriate dose for the patient. 115. The majority of clinical care should be provided on an individual, patient
specific basis. 116. The supply and administration of medicines under PGD should be reserved for
the limited number of situations where this offers an advantage for patient care (without compromising patient safety).
117. The use of PGDs must also be consistent with appropriate professional
relationships and accountability, i.e. the nurse or allied health professional (AHP) must act within their own expertise and competence.
118. Only designated registered staff listed in 7.3 may operate under a PGD. This
must not be delegated.
Version 2.0 POLICY MEDICINES POLICY Page 25 of 130
Date June 2016 Next Review Date June 2019
Administration of Medicines
PURPOSE AND SCOPE OF THE SECTION 119. The administration of medicines is an integral and essential entry criterion for
the Professional registration (NMC, 2009). Medicines administration is not solely a mechanistic task but a task that requires thought and the application of professional judgments. Registered practitioners must have the knowledge and skills required for the safe administration of medicines and keep those skills up to date (NMC, 2008).
120. This section of the policy sets out guidance for practitioners and their
responsibilities in the safe and effective administration of medicines to a correctly identified patient.
121. This applies to all Practitioners who are required to administer medicines in the
course of their work, including temporary staff.
See policy introduction (Section Introduction) which outlines staff group roles and responsibilities in relation to medicines.
Refer to relevant statutory and professional guidance alongside this policy.
122. Please see Appendix 3 for the role of unregistered staff in administration of
medicines. POLICY STATEMENT - Administration of Medicines 123. The safe and reliable administration of medicines is at the heart of patient
safety. Patients require the correct drug, in the correct dose, at the correct time. The policy supports this through setting out the processes to support staff in the safe administration of medicines.
GUIDELINES/ PROCEDURES/METHODS
The Prescription Chart (Wardex) 124. Do not administer medicines to a patient if a prescription chart is illegible, or not
completed fully, or if there is any doubt about the appropriateness or dose of any drug.
125. In the event that a chart is incomplete, the practitioner should highlight this and
ask for this to be corrected before administering any medicines that are not correctly prescribed.
126. In most circumstances, the Wardex is used to prescribe any medications or
indicate where a Patient Group Direction applies (section 6.4.5).
Version 2.0 POLICY MEDICINES POLICY Page 26 of 130
Date June 2016 Next Review Date June 2019
127. A medical, dental practitioner or an approved non-medical prescriber (NMP) can prescribe. The NMP will indicate this status by adding the code V300 or NMP on the prescription chart (see Non-medical Prescribing Policy). A register of signatures of all current NMPs is held in the Pharmacy Department.
Calculations, Checking and Preparation Avoid interruptions and distractions 128. Avoid distractions and interruptions whilst making up or administering any
medicines. 129. Before starting the procedure gather what equipment you may need, and carry
out any preliminary checks and observations if necessary prior to administration.
130. Attention should be paid to reduce the incidence of unnecessary interruptions,
such as organising breaks to ensure that the ward has a full compliment of staff during these periods.
131. Delegate responsibility to another member of staff to answer the phone or
queries or deal with patient requests to minimize interruptions. Checking of medications in both Bed Based & Community settings 132. Recommendations on safe administration of medicines state that in the
majority of cases a first or second level registered nurse, should be able to administer medicines without involving a second person check.
133. Full accountability for the correct administration of the medicine lies with the
administering practitioner, unless checking with another registered practitioner and in this case, both are equally accountable. In no circumstances can accountability be delegated to a student or support staff.
Second Person Check in Bed Based Services
134. A second person check is required for the following:
All medicines administered to babies and children on the paediatric ward and Neonatal Unit should be double checked by either a registered nurse or doctor. Low risk medications may be administered following a single check by a registered nurse if agreed at the speciality Quality Forum. The Medicines Safety Committee must be informed of all locally agreed medicines for single checking:
Controlled drugs with the exception of Oramorph solution 10mg/5mls, oral Tramadol, Temazepam and other Schedule 4 and 5 Controlled Drugs.
Intravenous injections whether bolus or infusion.
Version 2.0 POLICY MEDICINES POLICY Page 27 of 130
Date June 2016 Next Review Date June 2019
Where a need for a calculation of fractional dose or dilution is necessary, e.g. Heparin that is not a standard dose and requires a calculation to determine the correct dose, mixing of oral antibiotic solutions
All Chemotherapy or Cytotoxic preparations (refer to Policy for the Prescribing and Preparation of Cancer Chemotherapy).
Insulin Second Person Check in Community 135. In the majority of circumstances, one-person medicines administration as
opposed to two is acceptable. Exceptions to the Second Check Rule 136. There are certain situations where a second check is impracticable, such as
during a cardiac arrest, or where the administration of the medicine is an integral part of a defined therapeutic clinical procedure or intervention, e.g. the anaesthetising of patients during surgery.
137. When carrying out calculations consider the following:
Take time to work out calculations
Recheck answers
Do not be rushed
Answers or quantities that look wrong probably are, have an initial mental estimate of the dose.(2nd member of staff to check calculation)
It is acceptable to use calculators as part of the checking process.
If using a medical device 2 staff should calculate the rate and check that this corresponds to the rate set on infusion pump.
Preparing Substances for Injection:
138. Intravenous solutions must not be prepared for injection in advance of their
immediate use, or to administer medication drawn into a syringe or container by another practitioner when not in their presence. An exception to this is an already established infusion or medication prepared under the direction of a pharmacist from a central intravenous additive service and labeled for that patient.
139. For specific information regarding the preparation and administration of
Chemotherapy please refer to:
Policy and Procedure for the Management of Cytotoxic Chemotherapy Spillage and Contamination of Personnel
Policy and Procedure for Chemotherapy Administration.
140. As per NPSA alert 2007, most injections do not contain antimicrobial preservative and are licensed for single use only. Even those that do contain preservative may not be suitable for multi-dose use. Storage of single-dose

Version 2.0 POLICY MEDICINES POLICY Page 28 of 130
Date June 2016 Next Review Date June 2019
products, to prepare more than one dose, increases the risk of bacterial contamination. Only vials licensed and labelled "multi-dose" by the manufacturer may be used for this purpose, except for use in a single am or pm clinic. Use for more than one patient adds a risk of cross-infection, so strict aseptic non-touch technique (ANTT) must be followed.
Infusion Pumps 141. Infusion pumps must be checked at each handover by the nurse coming on
shift and the nurse finishing their shift, checking the drug / IV solution and the rate of infusion.
142. If an infusion rate needs altering, e.g. insulin sliding scale, this must be a 2
person check. Medicines Administered without a Prescription
143. The agreed range of medicines that can be administered at the discretion of registered practitioner without a prescription is printed on the wardex (only applicable to bed based services using a wardex). If any of the agreed medicines are administered, this must be recorded on the prescription chart. Administration of Liquid Medicines and Crushed medication via Oral and Enteral Routes Oral/ Enteral Syringes and Tablet Crushing Pots 144. Never use Intravenous (IV) syringes for the measuring of, or administration of
oral and enteral medicines. 145. An appropriate oral/enteral syringe must be used to administer and measure
oral liquid medicines when a medicine spoon or measuring pot cannot be used. 146. Oral/enteral syringes are colour coded purple and labeled ‘ORAL/ENTERAL’ 147. Tablets/capsules should only be crushed/opened under medical or pharmacy
advice. Tablet Crushing Pots are used only under the direction of a Pharmacist or Prescriber. They are obtained via the ward pharmacist or technician. They should be marked indelibly with the patient’s name as they are for single patient use only.
148. The tablet crusher may be used for different tablets, although they should be
crushed separately. Pots can be reused indefinitely for a named patient if cleaned.
149. If the prescription is endorsed as DISSOLVE or DISPERSE in water then
please do not crush the tablets first; crushing is a last resort.
Version 2.0 POLICY MEDICINES POLICY Page 29 of 130
Date June 2016 Next Review Date June 2019
150. Modified Release (MR) tablets MUST NEVER be crushed and administered.
151. For further information please refer to:
Clinical Practice Guidance for the Management of Feeding Gastrostomies for Adults in a Primary Care Setting
NPSA/2007/19.
Bolton NHS FT Document, ‘Choosing medicines for patients unable to take solid oral dosage forms’.
Procedure for the administration and recording of medicines 152. Check the following before administration:
Identify the patient: Check the name, date of birth and hospital number on the Wardex/MARS with the patient and check the details correspond with the wristband (bed based services only). Where possible ask the patient to state their name and date of birth. Refer to Positive Identification Policy.
Always check the Wardex/MARs that the patient has no known allergies or contraindications to the prescribed medicine - even if none are recorded check allergy status with patient.
Note any instructions from pharmacy indicating potential interactions between prescribed medicines.
Inform the prescribing practitioner immediately where allergies are found or contra-indications to any prescribed medicine are identified/observed.
Ensure the prescribed medicine has not already been given.
Review all parts of the Wardex /MARS, so no drugs are missed or duplicated. Community teams should also check the record of visit sheet.
Medicines dispensed for a named patient should only be administered to that patient.
Check expiry date for all medications and the date when solutions opened – discard if dates not found.
153. Administration:
Select the medicine required and follow the 5R for each;
Right Patient
Right medicine
Right date and time
Right dose
Right route
Discuss the medications being administered with the patient and or carer and check there is an understanding of the purpose of the drug and any common side effects.
The person administering the drugs can assign another person to support the patient to take their medicine, but this remains under their direct supervision.

Version 2.0 POLICY MEDICINES POLICY Page 30 of 130
Date June 2016 Next Review Date June 2019
Initial, date and time as indicated on the Wardex/MARs, that the medicine has been given and taken by the patient.
Record any adverse effects or variables using your clinical and professional judgement to determine any necessary follow up actions.
154. The overall responsibility for the administration of the drugs lies with the
registered practitioner. Under no circumstances should medicines be left unsupervised on a patient’s locker or at the bedside. Student nurses must be directly supervised at all times if they are assisting with medicines administration.
Refusal of medication 155. Where the patient refuses a medicine:
Ensure they are aware of the risks of omitting these.
Document this clearly in the patient record and where appropriate inform the medical staff.
If the patient is not capable of consenting to take their medication refer to the Covert Administration of Medicines Policy.
Safe administration 156. Safe administration of insulin:
Always measure and administer single insulin (bolus) doses using an insulin syringe or commercial insulin pen device (never using intravenous syringes).
An insulin syringe must always be used to measure and prepare insulin for any intravenous infusion.
The term ‘units’ should be used at all times and abbreviations, such as ‘U’ or ‘IU’, are never used.
Even if patient is on a IV variable rate insulin infusion (‘sliding scale’) their long acting insulins eg Lantus, Levemir or Tresiba must be continued
For further information please refer to NPSA/2010/RRR013
OMISSIONS AND DELAYED MEDICINES
157. Most medicines can be given plus or minus one to two hours from the time prescribed on the Wardex/MARS with the exception of Critical Medicines (see section 6.7 below) 158. Reasons for any omissions or delays of medicines must be recorded using the appropriate codes on the Wardex/MARs and also in the collaborative/patient records. 159. Blank records on the wardex are not acceptable, as they indicate a dose omitted without justification.

Version 2.0 POLICY MEDICINES POLICY Page 31 of 130
Date June 2016 Next Review Date June 2019
160. If there is no identifiable clinical reason/justification for omitting the dose, this MUST be reported as a clinical incident. Any omissions based on a clinical need are exempt from reporting as a clinical incident. CRITICAL MEDICINES 161. The following set out the critical medicines where it is crucial that these are
administered within one hour of the stated time. Critical Medicines:
Resuscitation medicines including colloid or crystalloid intravenous fluids
Systemic anti-infectives
Anticoagulants or thrombolytics.
Anticonvulsants.
Parkinson’s disease medicines
Insulin or oral hypoglycaemics
Strong opioids 162. If one dose is missed this MUST be reported as a Clinical Incident.
All staff should be aware that omission or delay of critical medicines are patient safety incidents and should be reported (NPSA, 2010 / RRR 009).
NALOXONE 163. NHS/PSA/Re/2015/009 relating to naloxone use can be life-saving in
respiratory depression and respiratory arrest, in patients where it is not indicated, or in larger than recommended doses, can cause a rapid reversal of the physiological effects for pain control, leading to intense pain and distress. Two dosing regimens exist for naloxone, these are: higher initial dose regimens and lower initial dose regimens. Please refer to local treatment guidelines or BNF for further information.
RECORD KEEPING 164. The administering practitioner must make an indelible record of administration
in the patient’s records by completing the Wardex/MARS and in the Controlled Drug Register/ Home Controlled Drug Register Card.
165. Any errors in the recording of administration must be clearly cancelled with a
single line in indelible ink through the initials. The reasons for this must be explained and captured in the collaborative record/nursing record.
NIL BY MOUTH AND OR DIFFICULTY SWALLOWING 166. If a patient has swallowing difficulties or is nil by mouth the practitioner must
contact the prescriber or seek advice directly from Pharmacy Department. See also: Bolton NHS FT Document, ‘Choosing medicines for patients unable to take solid oral dosage forms’.
Version 2.0 POLICY MEDICINES POLICY Page 32 of 130
Date June 2016 Next Review Date June 2019
VERBAL MESSAGES 167. A verbal instruction by a Doctor to administer an un-prescribed medicine is only
acceptable where failure to administer would result in serious harm to the patient. In this case, the Practitioner must fully justify and be accountable for his or her actions.
168. In the community setting a registered nurse may accept a telephone message
from a prescriber for an alteration (e.g., dose alteration) to a prescription to be administered in the patient’s home:
169. When taking a verbal message the Practitioner must provide the Doctor with
full details of the symptoms, relevant medical history, current medication record and any known allergies or contra-indications to drugs.
170. In the community setting, the registered nurse and where possible a second
practitioner will be involved in receiving of a verbal message. In bed based services two registered nurses must acknowledge the message. All verbal messages must be documented in the Wardex/MARs and collaborative records.
171. The following should be confirmed with the Doctor:
Patient's identity
Name and form of medicine
Route of administration
Dose prescribed
Date and time for administration
Name of Practitioner
Name of Doctor. 172. A record of the message must be made in the patient's Health Record and in
the once only section of the prescription sheet and both parties receiving the instruction must witness the record. The Doctor must confirm and sign the prescription before going off duty. The alteration must be confirmed in writing by the prescriber within 24 hours in community setting. Verbal alteration cannot be accepted for Controlled Drugs.
TRANSCRIBING (FOR COMMUNITY SERVICES ONLY) 173. This is the transferring of ‘direction to supply or administer’ from one source to
another and should only be undertaken in exceptional circumstances. MEDICATION ADMINISTRATION RECORD (MAR) CHARTS IN COMMUNITY SERVICES
Version 2.0 POLICY MEDICINES POLICY Page 33 of 130
Date June 2016 Next Review Date June 2019
174. Refer to Policy for the Preparation of Medication Administration (MAR) charts in Community Services. The addition of Controlled Drugs to the MAR chart should be completed by a prescriber.
MEDICINES FOR PERSONAL USE: 175. Medicines, which are provided by the Trust for the use of patients, must never
be taken or given for personal use by hospital/community staff. 176. Staff who become ill on duty should be referred to either Occupational Health,
Accident and Emergency or their General Practitioner (GP). 177. The Hospital Pharmacy Department has a small stock of over the counter
medicines available to purchase within Pharmacy working hours.
Version 2.0 POLICY MEDICINES POLICY Page 34 of 130
Date June 2016 Next Review Date June 2019
Controlled Drugs
DEFINITIONS 178. Controlled Drugs are those drugs covered by the Misuse of Drugs Act 1971
and associated Regulations. Medicines classed as controlled drugs can be found in the current Misuse of Drugs Regulations at www.homeoffice.gov.uk or in the current issue of the BNF NICE guidelines NG46 covers the safe use and management of controlled drugs https://www.nice.org.uk/guidance/ng46
179. Under the Health Act 2006, the Trust has appointed an Accountable Officer for
the safe and effective use of Controlled Drugs. This Accountable Officer is the Chief Pharmacist, who will audit the use of controlled drugs at regular periods and report the results to the Trust Board and the Local Information Network.
180. Medical, Pharmacy, Nursing and other staff still retain their own professional
and legal responsibilities around the use of Controlled Drugs. 181. The ward / department managers are responsible for the safe and secure
storage and the use of Controlled Drugs within their own areas. 182. All areas that handle Controlled Drugs should have Standard Operating
Procedures (SOPs). These SOPs should cover all aspects of risk management and audit trails for ordering, storing, prescribing, dispensing, recording, supplying, administration, and destruction of CDs appropriate to the setting and the team. Each team should have clear written SOPs in place that are known, understood and followed by practitioners and staff. Standard Operating Procedure for Royal Bolton Hospital and Bolton Community Unit (wards and also other areas) constitutes part of this Policy. The same member of ward staff cannot order and collect medicines from Pharmacy. Arrangements for the management of CDs when wards are opened, closed and transferred of wards are included in Appendix 4.
PRESCRIBING OF CONTROLLED DRUGS 183. All medical staff (not students and unregistered locums) may prescribe
Controlled Drugs, but may not prescribe diamorphine or cocaine for the treatment of addiction unless licensed by the Home Office to do so. Prescribing of diamorphine for pain control (including for substance misuse patients if clinically appropriate) is allowed under Home Office guidelines.
184. Under the Supplementary Prescribing regulations, Controlled Drugs may be prescribed if included in an approved Clinical Management Plan.
185. On 23rd April 2012, the Misuse of Drugs Regulations 2001 was amended to
enable independent nurse and pharmacist prescribers to prescribe controlled drugs listed in Schedule 2 to 5, except diamorphine, cocaine and dipipanone
Version 2.0 POLICY MEDICINES POLICY Page 35 of 130
Date June 2016 Next Review Date June 2019
for the treatment of addiction, within their scope of practice, competence and experience.
186. The amendment also regulates the mixing of medicines that include controlled
drugs, enables morphine and diamorphine to be supplied by independent nurses and pharmacists where administration of such drugs is required for the immediate, necessary treatment of sick or injured persons. The Trust leads on NMP, the Head of Professional Practice and the Chief Pharmacist are available for further advice and guidance.
187. The National Patient Safety Agency document “Reducing Dosing Errors with
Opioid Medicines” published in July 2008 states that any practitioner who is involved in the prescribing, dispensing or administering of Controlled Drugs should:
Confirm any recent opioid dose, formulation, frequency of administration and any other analgesics prescribed for the patient.
Ensure any intended dose increase is safe (not normally more than 50% higher than previous dose).
Ensure they are familiar with the medicines e.g. starting dose, frequency, dosing increments, overdose and side effects.
188. Controlled drugs prescriptions for out-patients or discharges frequently present
problems due to non-compliance with the regulations. All prescribers should ensure that all legal requirements are fulfilled (see the list below):
Full name and address of the patient
Full name of the controlled drug
Form of the drug, e.g. tablets
Strength of the preparation, if several exist
Dose
Total quantity of the preparation, or the total number of specified dose units, in both words and figures
Hospital Number or patient’s NHS Number (not a legal requirement but good practice).
189. And in addition:
The prescription must be signed and dated by the prescriber. Prescriptions generated via Ascribe will include the date which must be countersigned by the prescriber.
Controlled Drug Prescriptions are only valid for 28 days. The quantity of Schedule 2, 3, and 4 CDs to be prescribed at any one time must not exceed 30 days.
190. Controlled Drugs preparations must be prescribed by the appropriate
formulation e.g.
Oxycodone Modified Release (MR) tablets 5mg
Oxycodone liquid 5mg/5ml
Oxycodone capsules 5mg
Version 2.0 POLICY MEDICINES POLICY Page 36 of 130
Date June 2016 Next Review Date June 2019
191. The standard release products must be supplied unless a modified release
(MR) preparation is specifically prescribed. Any concerns must be checked with a prescriber/pharmacist and the medicine not administered until clarification is received.
192. Prescribers must not prescribe or administer CDs for themselves, family or
friends 193. Responding to requests for abusable drugs: Analgesics 194. Patients in hospital may require treatment for painful conditions. Their usual
daily dose of methadone may not control additional pain, so they may require pain relief as in any other patient. Non-steroidal anti-inflammatory drugs may be used as appropriate. Opioids may be necessary, but should be dictated by clinical need for analgesia.
Benzodiazepines 195. Where possible, these should be avoided. If night sedation is required, do not
initiate temazepam. Patients who are prescribed benzodiazepines by their GP or CDT should continue to receive them.
Cyclizine, Pregabalin & Gabapentin 196. Avoid due to potential of abuse.
Others 197. The BNF lists drugs with abuse potential (see under Misuse of Drugs Act). If in
doubt, check with a pharmacist. Ketamine is a drug with the potential to be abused.
198. Midwives’ exemptions: Registered midwives may administer parenterally, a
number of specified CDs in the course of their professional practice. These are:
Diamorphine
Morphine
Pentazocine lactate
Pethidine hydrochloride STORAGE OF CONTROLLED DRUGS 199. All Controlled Drugs must be received into the area by a designated person
appropriate to the area (as per Standard Operating Procedure). 200. All Controlled Drugs must be stored in a locked safe, cabinet or room, which is
so constructed and maintained as to prevent unauthorized access to the drugs. A purpose built CD cabinet is recommended. Keys must only be available to
Version 2.0 POLICY MEDICINES POLICY Page 37 of 130
Date June 2016 Next Review Date June 2019
authorised members of staff and at any time the key-holder should be readily identifiable to allow access to the CD cupboard.
201. If CD keys are missing, immediate actions must be taken to locate them, if the
keys cannot be found this must be escalated to the senior manager on duty who will contact the Accountable Officer or another senior pharmacist. Arrangements must be made to ensure patients receive prescribed CDs at the designated time. An incident form must be completed and the police informed.
202. For list of medicines to be stored in the CD cupboard, see Appendix 5 (Storage
Requirements for Controlled Drugs). 203. TTO CDs must be kept in CD cupboard separated from ward stock; no other
medicines should be stored in the CD cupboard unless specified by a Trust policy or agreed with Pharmacy (e.g. storage of concentrated IV potassium solutions, Propess® or mifepristone).
204. High strength Midazolam (5mg/ml or 2mg/ml) must only be kept as stock in a
clinical area performing conscious sedation such as general anaesthesia, intensive care, palliative care or where it has been formally risk assessed. NPSA/2008/RRR011.
RECORD KEEPING
205. Record of supplies received and administered must be made in a Controlled
Drugs Register which should be a bound book, not loose leaf. 206. Daily stock count of stocks of Controlled Drugs, including patients own
Controlled Drugs, is recorded in Controlled Drugs Daily Count Book. 207. A record of controlled drugs received from patients, their administration and
returns back to patients or relatives acting on their behalf is maintained in Patient’s Own Controlled Drugs Book.
208. All orders of stocks of Controlled Drugs should be made using Controlled
Drugs Order Book, unless ordering performed by pharmacists (community services).
209. Each CD item ordered needs to be on a separate page. The responsible healthcare professional ordering the CD must have supplied a copy of their signature to Pharmacy on an annual basis.
210. Controlled Drug Stationery are issued and recorded by Pharmacy including:
Controlled Drug Register,
Controlled Drugs Daily Count Book,
Patient’s Own Controlled Drug Book
Controlled Drugs Order Book
Version 2.0 POLICY MEDICINES POLICY Page 38 of 130
Date June 2016 Next Review Date June 2019
211. All Controlled Drug Stationery as listed above must be stored on the ward or clinical area in a locked drawer or cupboard (not the CD cupboard).
212. Loss or theft of CD stationery must be reported to the Chief Pharmacist and
Accountable officer. 213. All entries in the CD Register must be countersigned by a second registered
nurse. If a registered nurse is not available then another registered practitioner e.g. doctor, pharmacist or pharmacy technician must countersign the register.
214. If a mistake is made it should be bracketed in such a way that the original entry
is still clearly legible. This should be signed, dated and witnessed by a second registered nurse, midwife or other registered professional or by an appropriately trained healthcare assistant. The witness should also sign the correction
215. On reaching the end of the page in the CD register the balance should be
transferred to another page, it is good practice for this to be witnessed. 216. Completed ward requisition books and CD Registers must be retained for a
minimum of two years from the date of the last entry. 217. In a patient’s own home, CDs that are administered by a registered nurse must
be recorded on the Home Controlled Drug Register Card (CH226) and if possible verified by a second member of staff, who will also provide advice on safe storage.
RECEIPT AND CHECKING STOCK OF CONTROLLED DRUGS 218. Check CDs against the requisition, tamper evident seal broken, enter CDs into
controlled drug book and check balances tally. 219. Records of receipt of CDs onto wards/departments should be recorded in
letters not numbers i.e. 10 (TEN) 220. Two registered nurses, midwives or registered health professionals should
perform a daily check of stock of CDs. It is not necessary to open packs with tamper-evident seals for stock checking purposes.
221. When carrying out the daily check of CD liquids, in line with DH guidelines, a
visual check to confirm the quantity will suffice. The balance must be confirmed to be correct on completion of a bottle. Any discrepancies of +/-5% must be reported to the Ward Pharmacist and an incident form completed. This will enable the discrepancies to be rectified at the earliest opportunity and avoid compounding discrepancies. The administration of Controlled Drugs is covered in Appendix 4

Version 2.0 POLICY MEDICINES POLICY Page 39 of 130
Date June 2016 Next Review Date June 2019
DESTRUCTION OF CONTROLLED DRUGS 222. Any Controlled Drugs on clinical areas that are out of date or patients’ own
drugs that are no longer required must be promptly returned to Pharmacy by either the ward Pharmacist or the Ward Technician using the appropriate documentation. The ward or department should keep a record of drugs returned to pharmacy in the form of a returns advice note with duplicate pages so that both the pharmacy and the ward have a record of the transaction, (returns book pending).
223. Any out of date stock of Controlled Drugs (i.e. any controlled drugs not
dispensed for individual patients) must be destroyed by a person specifically authorized by the Trust Accountable Officer or the Controlled Drug Liaison Officer for Greater Manchester.
224. Any out of date Controlled Drugs that have been dispensed for a particular
patient can also be destroyed by a pharmacist in the presence of an appropriate witness.
225. Small amounts of CDs (less than 10ml) can be destroyed on the wards by
emptying the remaining volume into sharps bin and the emptied vial/ampoule discarded in the sharps bin.
226. Patient Controlled Analgesia (PCA) syringes that have been completed can be
disposed of in the yellow bin. PCAs that still contain liquid CDs (more than 10ml) must be denatured on the ward using denaturing kits following the instructions on the individual kits. The kit should then be placed in the blue medicines waste bin.
227. Patient’s own Controlled Drugs may be destroyed in patient’s own homes if
deemed appropriate. Such destruction may only be performed by a registered healthcare professional using a controlled drug denaturing kit in the presence of a suitable witness. The denaturing kit should subsequently be returned to the licensed waste carrier. (See Appendix 6)
DISCREPANCIES 228. If there is a discrepancy of stocks of Controlled Drugs, the person discovering
such discrepancy must notify their manager. An incident form must be completed and the Trust Accountable Officer must be notified.
MONITORING 229. See Section 5 (Monitoring Compliance).
.
Version 2.0 POLICY MEDICINES POLICY Page 40 of 130
Date June 2016 Next Review Date June 2019
Use of Methadone for Management of Opioid Withdrawal
INTRODUCTION 230. Opioid withdrawal symptoms are unpleasant but not life threatening. In
contrast, methadone overdose, or its administration to the opioid naive, can be fatal. Opioid withdrawal is not a medical emergency, so methadone does not need to be prescribed in the Accident and Emergency Department.
231. In pregnancy, opioid or benzodiazepine withdrawal can precipitate serious
foetal problems. Rapid stabilisation of symptoms is essential.
232. For comprehensive guidance, see the Guidelines for the management of patients with a history of opioid misuse on Trust intranet.
WHO CAN PRESCRIBE METHADONE
233. Doctors and non-medical prescribers (NMPs) do not need a special licence to prescribe methadone in the management of drug addiction.
234. Oral methadone should be prescribed as Methadone Mixture 1mg per ml.
235. Parenteral methadone should not routinely be prescribed. If the parenteral route is unavoidable, methadone should be given intramuscularly, not intravenously as the injection is only licensed for intramuscular use. When converting the dose from oral to intramuscular, start with the ratio of 2:1 (half the oral dose given intramuscularly) and then adjust the dose after 12 hours as needed. Patients must not self-inject whilst in hospital.
CAUTION: WHEN NOT TO GIVE METHADONE
236. The doctor must write on the prescription chart “Do not give if drowsy”.
237. The nurse must monitor the patient every time.
238. Do not give methadone to a patient who is drowsy, sedated, ataxic, with slurred speech or asleep. Never wake a patient up to give methadone. If any of these applies, the nurse must ask for a medical review. Do not give methadone if the patient has been absent from the ward and you suspect illegal drug use.
TAKING THE DRUG HISTORY
239. In addition to taking a full drug history, the doctor, the nurse or the pharmacy team must find out whether the patient is:
Version 2.0 POLICY MEDICINES POLICY Page 41 of 130
Date June 2016 Next Review Date June 2019
Established on a methadone programme by confirmation with the Community Drugs Team or a GP. Or
Using “street” drugs or on an unconfirmed dose of methadone.
MANAGING PATIENTS ESTABLISHED ON A METHADONE PROGRAMME
240. In pregnancy, opioid or benzodiazepine withdrawal can precipitate serious foetal problems. Rapid stabilisation of symptoms is essential.
241. The doctor should confirm the dose with the clinic or GP, who should liaise with the community pharmacy where the patient is registered, to cancel outstanding prescriptions
242. Establish the total daily dose from clinic and prescribe as advised by them. Do not increase the established dose without relevant Community Drug Team advice. If the patient is in for a while, consider getting community team’s advice on possible reduction
243. Methadone should be prescribed in milligrams, not by volume alone. Use Methadone Mixture 1milligram per ml. Do not prescribe on a “when required” basis and write on prescription “Do not give if drowsy”
244. Do not give methadone if patient is drowsy, sedated, ataxic, has slurred speech or is asleep.
245. Never wake a patient to give them methadone.
246. The nurse must monitor the patient, observing the Cautions in Section 10.3 above, on “When not to give methadone”.
247. If the patient brings in their own prescribed medication, they must give permission for its use or destruction. Ward staff must record receipt in the Controlled Drugs Register or green log book, store it in the CD cupboard, and arrange for a pharmacist to transfer back to pharmacy for destruction.
MANAGING PATIENTS ON “STREET” HEROIN OR UNCONFIRMED PRESCRIBED METHADONE DOSE
248. In pregnancy, opioid or benzodiazepine withdrawal can precipitate serious foetal problems. Rapid stabilisation of symptoms is essential.

Version 2.0 POLICY MEDICINES POLICY Page 42 of 130
Date June 2016 Next Review Date June 2019
249. Do not start methadone unless there is objective evidence of withdrawal symptoms Use Clinical Opiate Withdrawal Scale (COWS) to objectively assess withdrawal symptoms. This can be found in the Guidelines for the Management of patients with a history of opioid misuse on Trust intranet.
250. Then prescribe as per the Guidelines for the Management of patients with a history of opioid misuse and write on prescription “Do not give if drowsy”
251. Patients must be advised that in-patient methadone is prescribed to cover their hospital medical/surgical treatment. It is not the start of a programme.
252. Use the admission as an opportunity to see if the patient requires referral to the appropriate Community Drug Team, who work to defined catchment areas and refer if agreed - document in notes and on front of wardex in drug history section
253. Do not give methadone if patient is drowsy, sedated, ataxic, has slurred speech or is asleep.
254. Never wake a patient to give them methadone.
255. The nurse must monitor the patient every time, observing the Cautions in Section 3 above, on when not to give methadone.
MANAGING PATIENTS ON METHADONE WHO ARE ALSO USING STREET OPIATES
256. In pregnancy, opioid or benzodiazepine withdrawal can precipitate serious foetal problems. Rapid stabilisation of symptoms is essential.
257. There are those patients who are established on methadone or have been established on it since admission (Categories 10.5 & 10.6 above), who continue to use street opiates. In these situations, seek advice from the relevant Community Drug Team.
OBJECTIVE WITHDRAWAL SYMPTOMS 258. See the Guidelines for Management of Patients with History of Opioid Misuse. DISCHARGE PRESCRIBING OF METHADONE
259. The patient should go back to their usual prescriber. For patients in an established programme, the clinic must be notified of discharge at least one day beforehand and the details of who will supply the methadone prescription
Version 2.0 POLICY MEDICINES POLICY Page 43 of 130
Date June 2016 Next Review Date June 2019
needs to be agreed and documented. Methadone is only allowed on discharge if there are exceptional circumstances, with a maximum supply of two days.
SOURCES OF ADVICE 260. The Community Drugs Team and pharmacy are available for advice.

Version 2.0 POLICY MEDICINES POLICY Page 44 of 130
Date June 2016 Next Review Date June 2019
Guidelines for the Handling of Illicit Substances
Introduction 261. Many patients who misuse drugs are admitted, treated or visit the Trust, either
as a direct result of drug misuse or for other reasons. In some cases, the fact that a patient misuses drugs is already known to the medical and nursing staff. In others, it is not.
262. There is a risk of illicit substances being used on Trust premises so all staff are
expected to be vigilant and act accordingly should any illicit substance be located or they are suspicious of substances being brought into the Trust by visitors or patients.
263. When a member of staff takes possession of the substance, he or she is
placed in a vulnerable position unless it can be demonstrated that the substance was taken for the purpose of delivering it into the safe custody of a person lawfully entitled to possess it or destroy it. It is therefore important that all actions relating to the taking into safe custody or destruction of suspected substances are fully and correctly documented and witnessed and the procedures below followed. The senior nurse in charge and the senior doctor on duty must be consulted. If the senior doctor is not a consultant, he/she should discuss it with the duty consultant. Unless large quantities of drugs are involved, the main aim is to ensure that the drugs are handled and destroyed in a safe and legal manner.
264. Where large quantities of unauthorised drugs or other substances are found on
a patient’s person, i.e. greater than that considered to be for personal use the police should always be informed and fully assisted in their enquiries. An officer will attend the ward / department and initiate enquiries. The legal position is that the public interest overrides that of confidentiality.
265. The discovery of quantities of unauthorised drugs consistent with the patient’s
own personal use rarely leads to a successful prosecution. Furthermore, a heavy handed response can compromise patient care and cause considerable disruption of ward routines and the waste of much time and effort. The police are aware of this and do not wish to compromise patient care. Consequently, following discussions with Greater Manchester Police, it is recommended that the decision to contact the police or dispose lawfully of the substance should be taken jointly by the ward manager in conjunction with the consultant with clinical responsibility for the patient.
266. Under no circumstances can a Schedule 1 (Class A, B or C) drug (includes
cannabis and lysergide which are not used medicinally) be handed back to a patient at discharge, as the person doing so could be guilty of an offence of unlawful supply of a Controlled Drug.
Version 2.0 POLICY MEDICINES POLICY Page 45 of 130
Date June 2016 Next Review Date June 2019
Procedure to be followed when a patient is found to be in possession of unauthorised drugs or other suspicious substances: 267. The member of staff finding the substance should immediately inform the nurse
in managerial charge of the ward or department.
268. The ward or department nurse manager should place the substance in a suitable secure container with a label identifying the source (patient’s initials and hospital number) and a brief description of the contents (“brownish powder” or “brown resinous material”, not what the contents are believed to be). The label should be over the seal and signed by the nurse in charge and a witness.
269. The container should then be placed in a locked controlled drugs cupboard.
270. The ward or department nurse manager should inform the consultant in charge of the patient that the patient is in possession of an illicit substance.
271. The ward manager should complete Part A of the “Form for removal and
destruction of unauthorised drugs or other suspicious substances” (Appendix 7 of this Policy). An entry should also be made in the back of the controlled drug register including the date of removal, description of the substance and patient’s name.
272. Where the ward manager and the patient’s consultant agree that the quantity of
the substance found is consistent with the patient’s own personal use, then the ward pharmacist should be contacted to remove the substance for destruction. In this case, Parts B and C should be completed as indicated, by the ward manager, the consultant and the pharmacist. One copy of the form should be filed in the patient’s medical record and one copy retained by the pharmacy department. If the patient objects to this course of action, contact the Police Incident Management Unit.
273. Where either the ward manager or the consultant in charge, or both, consider
that the quantity of the substance found is greater than is consistent with the patient’s own personal use, Part B must be completed. The ward manager / consultant should then contact the Police Incident Management Unit.
274. If the police officer attends, the ward staff should co-operate fully with the
officer. In some cases, the officer may not need to know the identity of the source patient. However, if he or she does, this should be provided by the doctor. In the investigation of an alleged criminal offence, confidentiality is unlikely to be a sufficient defence in law against disclosure.
275. Each case will be treated on its own merits and it is therefore not possible to
indicate the precise action the police will take. However, the patient will never be questioned or removed from the ward or department if it is considered by the consultant in charge to be inappropriate on clinical grounds.
Version 2.0 POLICY MEDICINES POLICY Page 46 of 130
Date June 2016 Next Review Date June 2019
276. Following his enquiries, the police officer will remove the suspicious substance
from the ward. Part D should be signed by the police officer and the nurse witnessing the transfer. One copy should be given to the police officer, and one copy filed in the patient’s medical record.

Version 2.0 POLICY MEDICINES POLICY Page 47 of 130
Date June 2016 Next Review Date June 2019
Admission to bed based services and medicines reconciliation
INTRODUCTION 277. Effective medicines reconciliation is an essential component of clinical
governance, ensuring patient safety through the safe and appropriate use of medicines in each individual patient. More than half of all hospital medicines errors occur at interfaces of care and most commonly at admission. Effective medicines reconciliation could therefore reduce these errors and the harm they cause. The NICE/NPSA Guidance stated that all healthcare organisations that admit adult inpatients (16years or over) should aim for medicines reconciliation.
DEFINITION 278. The process of identifying the most accurate list of a patient’s medicines –
including the name, dosage, frequency and route of administration – and comparing them to the current list prescribed for use, recognising any discrepancies, and documenting any changes, thus resulting in a complete list of medications accurately communicated. This information should be maintained and documented on the prescription chart during a patient’s stay along with details of any changes made and the reason(s) for stopping/changing a medicine, throughout their stay. This should be reliably communicated between the teams when care is transferred to another ward or hospital and at discharge to the GP or other relevant primary care providers. The whole process is called medicines reconciliation. Medicines reconciliation is MORE than a medication/drug history, and separate to a medicines review/clinical check.
279. This process should only be undertaken by a member of the pharmacy team,
nursing or medical staff. 280. There are three main parts to completing comprehensive medicines
reconciliation: Collecting the information, Checking the information and Communicating the information. To NOTE: Pharmacy technicians often collate the medication history in order for a pharmacist to complete a medicines reconciliation. [For further details of pharmacy roles and responsibilities please refer to DOP 90.4.]
281. It is the responsibility of medical staff to ensure that any changes in a patient’s
medication during their in-patient stay is documented clearly in the patient’s notes and on the patient’s prescription chart. This information must also be documented on the discharge summary
. 282. It is the responsibility of non-medical staff to ensure that any discrepancies
identified from the medicines reconciliation process are highlighted, documented and escalated for appropriate action to the medical team looking after the patient to ensure swift resolution
Version 2.0 POLICY MEDICINES POLICY Page 48 of 130
Date June 2016 Next Review Date June 2019
ADMISSION 283. When patients are admitted to bed based services, it is important to ensure that
the medicines prescribed on admission correspond to those that the patient was taking before admission.
284. This involves taking a careful medication history from the patient, using the
most recently available information sources, resolving any discrepancies and documenting which medicines are to be continued, stopped, withheld or changed. Medicines to be continued should be prescribed on the prescription chart, along with any new medicines started on admission.
285. All completed medicines reconciliation should be signed and dated by the
person responsible for compiling the information. 286. Process in bed based services:-
Patients should have their medicines reconciled within 24 hours of admission
as per NICE/NPSA guidelines.
287. A minimum of 2 information sources should be used to obtain a list of
medicines taken by the patient prior to admission. These sources include:-
Patients themselves
Patient’s own medicines brought in with them
Patient’s carer or relatives
Past discharge summaries from recent hospital admissions or drug charts filed in the medical notes
Summary of Care Records – to be printed and placed in the nursing notes. (see Separate policy)
GP referral letter
Telephone enquiries to patient’s GP, nursing home, community hospital or community pharmacy, fax from GP
Medicine information card or repeat prescription form
Copy of medication chart(s) / Medicines Administration Record Sheet from the nursing home or community hospital where the patient resides
288. Over the counter medication, herbal remedies/alternative medicines,
recreational drugs should be documented. 289. Known/suspected allergies and intolerance to drugs should be recorded with
details of reactions.
290. Medicines which have been discontinued/withheld on admission should be
documented with details in the patient’s notes.
Version 2.0 POLICY MEDICINES POLICY Page 49 of 130
Date June 2016 Next Review Date June 2019
291. Compliance/ special requirement issues i.e. does the patient require a blister pack, a Haleraid® to use their inhalers, non-click lock bottles where poor manual dexterity etc.
TAKING MEDICATION HISTORIES IN COMMUNITY SERVICES 292. As part of their duties, some staff may on occasion take a patient’s medication
history; any practitioner should consider why they need to take this history if purely for recording purposes.
293. If it is felt that a medication history is needed, then the information should come
from a recognized source, such as:
The latest recent repeat medication slip provided by the GP practice –which should be confirmed with the prescriber, patient or carer as appropriate
the patients’ medication containers, (ensuring that the medication is current by contacting the appropriate community pharmacy),
A recent hospital discharge summary. The dates of the last admission should be checked wherever possible.
294. Wherever possible confirmation should be sought from the patient/carer that
the information matches the medication that they are actually taking and any discrepancies are recorded along with the source of the information.
295. If a practitioner is concerned about the effects of a medicine on a patient, they
should refer to the prescriber or to a pharmacist and if necessary contact the patients’ doctor themselves.
296. Some practitioners may be competent to give general information on the
effects of medicines e.g. general side effects of non-steroidal anti-inflammatory drugs (NSAIDs). It is inappropriate for staff who are not prescribers to change any parameter of a Prescription Only Medicine without first discussing it with the GP, doctor, or other independent prescriber, unless working within the remit of a Patient Group Direction or Supplementary Prescribing framework.
297. Prescribed treatments that are not licensed medicines, e.g. nutritional
supplements, should not be amended unless the practitioner is working within their own professional competence and accountable for their actions. Professionals should contact the dietician for guidance if there are concerns regarding nutritional products prescribed. Any advice given, in relation to the medication, must be recorded in the patients’ notes and any concerns referred back to the prescriber.
Version 2.0 POLICY MEDICINES POLICY Page 50 of 130
Date June 2016 Next Review Date June 2019
Medicines on discharge
INTRODUCTION 298. This section should be read in conjunction with the Adult Hospital Discharge
and Transfer of Care Policy. 399. All clinical correspondence for outpatients should be forwarded to the patients
GP within 5 working days of attendance 300. Discharge summaries for in patient and day cases should be issued to GPs
within 24/48 hours of discharge. ROYAL BOLTON HOSPITAL 301. Medical, nursing and pharmacy staff involved in the discharge process are
expected to refer to and follow this policy and the procedures outlined via the training provided by the training department on the use of the Ascribe system and standard work. Registered nurses must also complete the Assembly of Patient’s Discharge Assessment Criteria and Record of Competence before they assemble patients’ medicines for discharge– see Appendix 19.
302. Discharge medication (TTOs) should be prescribed as soon as a patient is
identified as medically fit for discharge and plans are agreed for a safe discharge. It is in the interests of patients and staff alike that every effort be made to ensure discharge prescriptions are written at least 24 hours in advance of the planned discharge date. Good discharge planning will facilitate the processing of discharge prescriptions during normal Pharmacy opening hours.
303. Medical staff (and Non-medical prescribers involved in writing Electronic
Discharge Summaries) should review patient’s medication before discharge and complete all relevant sections of Electronic Discharge Summary (see also Admission to bed based services and medicines reconciliation section).
304. If injectable medicines or Controlled Drugs are to be administered by District
Nurses at patient’s home, written request for such administration has to be completed by the prescriber stating the medicine to be administered, dose, route and timing of administration. The prescriber has to sign such request and also print their name.
305. Patient’s discharge medication needs to be clinically checked by a pharmacist
and will be dispensed by Pharmacy Department except medicines of which the patient has got a sufficient own supply. Every patient should have a minimum of 7 days supply of each medicine for discharge, unless less is required to finish a course of treatment or for any other clinical reason.
Version 2.0 POLICY MEDICINES POLICY Page 51 of 130
Date June 2016 Next Review Date June 2019
306. For discharges when Pharmacy is closed, please refer to “Procedure to be followed for dispensing medication for urgent discharge when Pharmacy is closed” see Appendix 16.
307. When the prescription has been dispensed the discharge medication must be
stored in the patient’s bedside locker, unless items need to be stored in the fridge, Controlled Drugs cupboard or for larger bulk items in a designated area.
308. Immediately prior to discharge the TTO list must be printed off and the nurse
must check all the medicines against the TTO list adhering to the principles set out on the Assembly of Discharge Medicines competency.
309. Medicines not listed on the TTO list should not be supplied to the patient on
discharge, they must be removed, labels crossed through and returned to Pharmacy. Medicines brought to hospital by the patient however constitute patient’s property and can only be removed with patient’s consent. If such consent is declined, medicines need to be clearly marked as stopped by crossing through the label and writing “STOPPED” on it. This should also be documented in patient’s notes.
310. The nurse discharging patient must check that the patient understands how to
take their medications at home, including changes and discontinued medicines and record it on the discharge checklist (at the end of the Patient Assessment & Care Document (R276).
311. The patient must be given a printed copy of their Electronic Discharge
Summary. 312. On discharge the nurse must leave the empty locker open ready for cleaning
prior to the next patient allocated to the bed. 313. Before discharging patients with medications, registered nurses must have
completed IT Ascribe training and must have been assessed and signed off as competent to complete the Assembly of Discharge Medicines. This competency can be found on the Pharmacy homepage of the Trust intranet.
COMMUNITY SERVICES (DARLEY COURT) 314. The Pharmacy team should be informed of any planned discharges to enable
them to work with the Prescribers to obtain a supply of medication necessary for discharge.
315. The Pharmacy team, when available, will assemble the discharge medication,
ensuring the patient has a minimum of seven day’s supply, reconciling the medication against the current medication chart.
316. A Discharge Medication Letter will be generated; detailing all current
medication and any items discontinued or amended during the patients stay

Version 2.0 POLICY MEDICINES POLICY Page 52 of 130
Date June 2016 Next Review Date June 2019
and where appropriate a Medication Administration Record Sheet (MARS) for carers use.
317. The Pharmacy team ensures the discharge medication letter is faxed to the
patients GP within 24/48 hours of the patients discharge. 318. When Pharmacy staff, are unavailable, it is the nurse’s responsibility to ensure
medication is assembled against the current medication chart and discharged with the patient.
319. If the medication is unavailable an FP10 prescription should be requested from
the Medical Prescriber and obtained from the community Pharmacy using the out of hour’s taxi service if necessary.
320. It is the responsibility of the nursing staff to inform the Pharmacy team of any
discharges they have not been involved in to enable them to forward a Discharge Medication Letter to the patient’s GP.
CONTROLLED DRUGS 321. If the patient is being discharged on Controlled Drugs that will be administered
by District Nurses, the medicines administration chart should be completed and signed by the prescriber prior to discharge.
Version 2.0 POLICY MEDICINES POLICY Page 53 of 130
Date June 2016 Next Review Date June 2019
Mental capacity and Covert Administration of Medicines
322. If a patient is not capable of consenting to take their medication, it is still possible to administer the medication if it is considered to be in their best interests.
323. The use of administration of covert medication is likely to be appropriate only in
patients with severe dementia, acute deliriums or a profound learning disability. 324. Covert administration is the term used for administration of medicines that are
administered in a disguised format, for example in food or in a drink, without the knowledge or consent of the person receiving them.
325. The practice of offering medication in food or drink is only allowable in
particular circumstances and could be open to abuse. The Covert Administration Policy provides guidance as to when this practice is lawful, and to ensure that if it happens it has been properly considered, thorough consultations have been made and that the practice is transparent and open to public scrutiny and audit.
326. The decision to administer medicines covertly must not be routine practice and
must be a contingency/emergency measure. 327. For further guidance please read in conjunction with the Trust Policy on Mental
Capacity Act 2005, Consent to Examination or Treatment Policy and the Covert Administration of Medicines Policy).

Version 2.0 POLICY MEDICINES POLICY Page 54 of 130
Date June 2016 Next Review Date June 2019
Self-Administration of Medicines
PATIENT SELF-ADMINISTRATION 328. Self-administration of medicines should be considered where a patient may
benefit from such a process. Examples of this would be those patients using medicines such as inhalers or GTN sprays, or patients who have long standing conditions such as Parkinson’s disease if the timing of their medicines is crucial.
329. Registered nurses, midwives and the pharmacy team are responsible for the
initial and continued assessment of patients who are self-administering and have continuing responsibility for recognising and acting upon changes in a patient’s condition with regards to safety of the patient and others.
330. In the case of medicines that require specific storage arrangements, a patient
may self-administer under the supervision of a registered nurse. 331. Paediatric patients are excluded from self-administration. 332. Controlled Drugs are excluded from self-administration with the exception of
Patient Controlled Analgesia (PCA). PATIENT ASSESSMENT AND CONSENT 333. Where patients consent to self-administration of their medicines, the following
points should be considered:
The nurse, the pharmacist and the doctor retain professional and legal responsibility for the patient’s medication whilst they are in hospital. Patients take the responsibility for their actions relating to self-administration of their medicines.
Patients can withdraw consent at any time.
The medicines should be fully labelled, with directions for use to every patient who is involved in self administration.
Information given and supervision should be tailored to meet individual patient need.
334. Patients should be assessed for suitability for the following:
Level 0a: Full self-administration following documented assessment.
Level 0b: Full self-administration of selected medicines only, following documented assessment.
Level 1: Patient needs supervision with their medicines. Patient is given access to medicines under supervision of the nurse. As a minimum the nurse and patient must together check the medicine dose to be taken. The nurse will if appropriate educate the patient on how the medicines are to be administered and why they are prescribed.
Version 2.0 POLICY MEDICINES POLICY Page 55 of 130
Date June 2016 Next Review Date June 2019
Level 2: Full Nurse administration of all types of medication
Level 3: Not applicable, Community Services/ Domiciliary settings only.
335. Self-Administration of Medicines Algorithm can be found in Appendix 8, Self-
Administration of Medicines Assessment Record in Appendix 9, Self-Administration Consent Form in Appendix 10 and Self- Administration Patient Information Leaflet in Appendix 11 of this Policy.
336. Please note: Individual medicines may require a different level of support. OTHER REQUIREMENTS 337. Medicines will be kept in the medicines locker with the exceptions of specified
medicines such as GTN spray or asthma reliever inhalers which may be kept with the patient and self-administered as required, however these medicines must not be left unattended.
338. At each medicine round the nurse must check with the patient if the medicine
has been taken and must document the date, time taken and confirm self-administration with the relevant code on the Wardex. The code to be used is “S”. Any change in the patient’s condition that affect the level of self-medicating ability needs to be picked up and acted on immediately and the self-medicating status reassessed.
339. Pharmacists are available for advice if necessary.

Version 2.0 POLICY MEDICINES POLICY Page 56 of 130
Date June 2016 Next Review Date June 2019
Unlicensed medicines
DEFINITIONS 340. Unlicensed prescribing is defined as:
Prescribing of a medicine, which does not have a valid UK product license and therefore cannot be marketed in the UK.(unlicensed medicine)
Prescribing of a drug with a valid UK product license at a dose, via a route or for an indication that is not listed in the product license (unlicensed use). This is also known as prescribing off-label.
341. Unlicensed medicine is defined as a:
Product that has a license in another country.-These can be imported into the UK for a named patient, but are then considered unlicensed as they do not have a UK license.
Product that no longer has a product license. - Either because the licence has been suspended, revoked or not renewed. These are sometimes still manufactured, but only in an unlicensed capacity for a named patient.
Special -These are bespoke products, prepared for the needs of a specific patient for when a licensed preparation is unsuitable. For example: a liquid, preservative-free, or additive-free preparation. The active ingredient is often, but not always, taken from the licensed drug.
Product being used in clinical trials - unless the product has a UK product license and is being used in accordance with its license in a clinical trial.
342. Clinical trial drugs are treated differently by the Trust, and do not fall under this
section of Medicines Policy. They are subject to strict clinical trials regulations. For advice on clinical trials drugs please contact the Research and Development Department on ext. 3848 or the Clinical Trials Pharmacist or Technician and via the Pharmacy office, ext. 5555.
UNLICENSED MEDICINES AND PGDs 343. An unlicensed medicine should only be administered to a patient against a
prescription and not against a patient group direction. 344. Medication which is being used off-label may be administered under a patient
group direction if such use is exceptional, justified by best practice and the status of the product is clearly described
PRESCRIBER’S RESPONSIBILITY 345. Unlicensed drugs or off-label uses should only be prescribed where a licensed
alternative is not available or not suitable for the necessary clinical management of the patient.

Version 2.0 POLICY MEDICINES POLICY Page 57 of 130
Date June 2016 Next Review Date June 2019
346. The Trust requires that unlicensed prescribing should be undertaken by or
under the direction of a consultant or a registrar with experience in that clinical area.
347. Prescribers are free to prescribe unlicensed drugs or off-label, however, in
doing so, they hold responsibility and therefore liability and may be called upon to justify their actions in the event of an adverse reaction. The manufacturer will only be held responsible or strictly liable if the misadventure occurred as a result of a defect in the product. The Trust will accept liability for the use of medicines for indications not included in the product license provided such use would be considered standard practice by their peer group, and the above requirements have been undertaken.
348. For unlicensed medicines, the consultant is required to sign a disclaimer
(Appendix 12), stating the intended use and whether other prescribers in their team can prescribe the named medicine on their behalf. Disclaimers are valid for 2 years and only apply to the specific conditions laid out by the prescriber.
349. Where a prescriber has been invited to prescribe a drug that has been initiated
by a consultant, a shared care arrangement should be secured. This would involve the prescriber:
Familiarising themselves with the drug, including the side effect profile.
Satisfying themselves that the rationale for the use of the drug in that patient is clinically appropriate.
Taking responsibility for adequate monitoring or being satisfied that this is being done effectively by a third party.
Having access to consultant support if a problem arises.
350. The prescriber should, where possible, inform the patient of the unlicensed status, and obtain patient consent. A written record should be kept of these discussions.
PHARMACISTS’ RESPONSIBILITY 351. To obtain unlicensed medicines only on the written authority of a consultant. 352. To ensure a disclaimer has been completed for an unlicensed medicine before
dispensing the prescription. 353. To explain to healthcare staff the practical implications of using unlicensed
medicines or medicines for unlicensed uses. 354. To raise awareness to prescribers who have prescribed an unlicensed use of a
medicine. 355. To assess the quality of an unlicensed product prior to releasing the product for
use, in accordance with pharmacy procedures regarding procurement. Note

Version 2.0 POLICY MEDICINES POLICY Page 58 of 130
Date June 2016 Next Review Date June 2019
that the final responsibility of a faulty product lies with the supplier, even in the case of unlicensed medicines.
356. To follow pharmacy procedures regarding procurement and dispensing of
unlicensed medicines.
NURSE’S RESPONSIBILITY 357. It is nurse’s responsibility to question the doctor or pharmacist if an instruction
to administer a medicine is thought to be outside the terms of a product licence.
358. A nurse may refuse to administer medicines being used outside the terms of
their product license if that is judged to be in the best interests of the patient. Refusal to administer should not occur solely because a medicine is unlicensed.
UNLICENSED MEDICINES NOT REQUIRING A DISCLAIMER
359. A list of such unlicensed medicines is in Appendix 13 of this Policy. 360. Drugs on this list do not require a clinical disclaimer to be completed by the
prescriber. That is, a specific consultant does not need to take overarching responsibility. The trust will take responsibility as laid out above, if all other responsibilities are fulfilled as above.
Version 2.0 POLICY MEDICINES POLICY Page 59 of 130
Date June 2016 Next Review Date June 2019
Storage of Medicines
STORAGE OF MEDICINES IN BED BASED SERVICES Responsibilities of ward / department managers: 361. The Ward / Department Manager is responsible for ensuring that all medicines
are stored securely in locked metal cupboards to which only authorised staff have access, and that keys are passed only to authorised staff as appropriate. Particular attention should be paid to medicines stored in non-designated locations, for example resuscitation trolleys and treatment rooms. Those wards using bedside lockers must pay particular attention to the security of these lockers.
362. Estates Department will change the key pad door codes annually as part of
contracted work, if the Ward/Department Manager requires the code changing in the interim a cost will be incurred.
363. The keys to the cupboard(s), fridge(s), trolley(s), etc. are to be held by the
Team Leaders on each ward / department. While a nurse is in charge of a ward or department, he or she is responsible for all the medicines on it. In the event of any discrepancies or apparent loss, the ward or senior pharmacist must be informed as soon as the pharmacy is next open. If there appears to have been a loss, the Incident Reporting Procedure should be followed.
364. If keys being kept by one individual would impact adversely on patient care due
to access to emergency medicines, then a digital key safe attached to the treatment room wall would be suitable. An application must be made in writing to the Chief Pharmacist before a key safe is installed with the clinical reason for the application. The keys must be confirmed as being back in the safe at shift handover.
365. All medicines should be kept in their original pack, including any information
leaflet. This does not apply to an insulin pen in use out of the fridge or to bulk IV fluids.
366. Bulk IV fluids removed from original box must be stored in clearly labelled
containers fit for purpose. 367. These locations should only be used for the storage of medicines and for no
other purpose. 368. All the storage areas should be locked, but the Emergency Drugs (CPR) Box
should be accessible without difficulty at all times. Storage cupboards include: Main cupboards
Version 2.0 POLICY MEDICINES POLICY Page 60 of 130
Date June 2016 Next Review Date June 2019
369. Internal and external medicines that do not require specific storage arrangements should be segregated, either in separate cupboards or at least on different shelves.
370. Epidural infusion fluids should be stored in a separate area to IV fluids Storage of refrigerated medicines 371. For drugs that require refrigeration, the refrigerator used should conform to
MHRA guidance. 372. Refrigerators to store medicines must maintain an air temperature of between
2-8°c and the fridge must be lockable. 373. Temperature monitoring must take place on a daily basis (preferably at the
same time each day) by ward/department staff and the actual, minimum and maximum temperature should be recorded on the ‘Daily Temperature Monitoring Form’ (see Appendix 14) with the thermometer being reset daily.
374. Temperature monitoring should be via an electronic maximum/minimum
thermometer, with an accuracy of +/- 1°c (minimum specification), which should be readable from outside of the refrigerator.
375. Temperature monitoring probes should be sited in a central location within the
refrigerator. They should not be placed on the inside of the door. 376. Temperature monitoring forms should be kept for one year before destruction. 377. Refrigerators must be maintained and defrosted in line with manufacturers’
guidelines. The refrigerator should be cleaned on a weekly basis by ward/department staff (as part of the general cleaning rota).
378. If a temperature deviation is identified ensure the refrigerator door is closed,
reset the thermometer and recheck after 10 minutes. If a second deviation is recorded, place the affected stock in a bag marked “DO NOT USE”. Ideally quarantine affected stock in another refrigerator, ensuring affected and unaffected stock are kept separate. Alternatively retain in the malfunctioning refrigerator and ensure the door is kept closed. Check the monitoring form for when the refrigerator was last working and try and determine how long the drugs have been stored outside the required temperatures.
379. Complete an incident via the Trusts incident reporting system and contact
pharmacy for advice. Do not use quarantined stock until Pharmacy has advised that the stock is safe to use.
Ambient temperature monitoring within clinical rooms

Version 2.0 POLICY MEDICINES POLICY Page 61 of 130
Date June 2016 Next Review Date June 2019
380. Unless stated otherwise in product literature and/or drug label, the majority of medicinal products that do not require refrigeration can be stored under conditions of controlled room temperature without compromise to their stability and recommended shelf life. These products are usually labeled ‘do not store above 25°C.
381. To ensure the integrity of medicinal products ambient temperature monitoring
must take place on a daily basis (preferably at the same time each day) and the actual, maximum and minimum temperature should be recorded on the ‘Daily Temperature Monitoring Form’ (see Appendix14) with the thermometer being reset daily.
382. If the ambient temperature exceeds 25°C first actions/considerations would be:
Is there an obvious cause that can be remedied? For example, has the thermometer or probe been positioned incorrectly or is it damaged?
Check the temperature control setting within the storage area. Can the room temperature be reduced?
Liaise with Estates to alter the air conditioning (if applicable) or review the air balance within the room (for rooms where there are ceiling vents).
If there is no obvious cause, take steps to protect the medicines e.g.
If too warm move stock to cooler areas e.g. on lower shelves, out of sunlight and away from heat-generating equipment.
If too cold, move stock that should be stored above 15°C to higher shelves and away from windows and outside walls
If temperature recordings are greater than 25°C an incident form must be completed via the Trusts incident reporting system and pharmacy must be contacted for advice regarding the affected medication and whether this needs to be segregated or quarantined
Temperature monitoring forms must be kept for one year before destruction.
Disinfectant cupboard
383. For preparations which are not used for patients e.g. Haztabs
Reagents cupboard
384. Contains urine testing and blood testing strips or any other reagent
preparations
Sterile fluids for infusion and irrigation
385. Fluids are normally stored in a designated area on wards / departments which must be locked. Stock should be rotated to ensure use within expiry dates. Epidural infusion fluids should be stored in a separate area to IV fluids, those containing controlled drugs can be stored in the standard Controlled Drug Cupboard.
Version 2.0 POLICY MEDICINES POLICY Page 62 of 130
Date June 2016 Next Review Date June 2019
Medical gases
386. Medical gas cylinders must be stored in a well-ventilated area away from flammable substances. They must be secured with a chain in a suitable trolley or designated area.
Patient’s own drugs / bedside lockers and patient transfer
387. When a new patient is admitted, a check that the locker is empty must be
performed. When a bed is empty, the locker must be empty and kept unlocked with the door open to ensure no medicines remain unchecked.
388. All patient’s own drugs or drugs dispensed for discharge for that patient must
be supplied only against the discharge prescription as per protocol to that patient. All the patients drugs in the locker- either own or dispensed whilst in- must be transferred with the patient to any new bed based service.
389. Part of the discharge or transfer procedure must include checking that the
patient’s drugs have been removed from the locker and are with the patient. When a new patient is admitted, a check that the locker is empty must be performed. When a bed is empty, the locker must be empty and kept unlocked with the door open to ensure no medicines remain unchecked.
390. For all patients transferred during an in-patient stay, the receiving nurse must
amend the prescription chart with the new ward and consultant and confirm with the transferring nurse that all drugs have been transferred with the patient
RECEIPT AND STORAGE OF MEDICINES IN COMMUNITY SERVICES Receipt of medicines 391. When medications are delivered to community premises the driver will hand
over the transit container to a clinic administrator or clerk and will obtain a signature if required for the receipt of delivery. Medicines delivered from supplier to the clinics will be checked by designated FT staff against the copy order form/requisition and delivery note to ensure accuracy for:
Correct drug
Correct formulation
Correct strength
Correct quantity
Shelf-life of products
Storage requirements
Good condition of the product
Requirements for safe handling
392. After checking, the delivery note will be retained for a period of 2 years. The name(s) and quantities of medicines received are then entered in the stock sheets, which should also be stored securely.
Version 2.0 POLICY MEDICINES POLICY Page 63 of 130
Date June 2016 Next Review Date June 2019
393. Items for refrigeration must be checked and placed in the correct refrigerator
immediately. 394. Any queries related to the supply of medicines should be directed to the
supplier. Storage of medicines 395. In clinic sites and medical rooms within special schools, the responsibility for
the safe keeping of medicines lies with the designated person(s) who controls access by keys to the medicines. When not in use, sets of keys should be stored in a locked key cupboard or other secure place. A second set of keys should be kept in an appropriate, secure location.
396. All medicinal products should be stored in a locked cupboard or a locked
refrigerator reserved for the storage of medicinal products. Premises should be alarmed when not in use.
397. Medicines should be segregated as follows:
Medicines for internal use.
Medicines for external use (including disinfectants).
Refrigerator medicines.
Diagnostic reagents cupboard.
Area for flammable liquids.
Area for sterile topical fluids.
Medical gasses stored in appropriate storage facility.
398. Where premises are shared by a number of clinics, each clinic is responsible for its own stock of medicines, which must be stored separately (ideally in a separate cupboard but at least in a separate area of a communal locked cupboard).
399. Resuscitation medicines may be held at strategic and accessible sites during a
clinic session. They should be secured when the clinic is not running sessions. Once a pack has been opened, it should be returned to the supplier and a replacement provided. These medications should be checked and maintained as detailed in the FT resuscitation policy.
400. In the patient’s home, staff must encourage patients to store all medicines
(including gases such as oxygen) in a safe place away from children and according to the manufacturer’s instructions. Patients should also be encouraged not to hoard drugs but instead return any unwanted medicines to the local pharmacy for safe destruction and to inform the GP if they are not taking their medicines.
401. Medicines must never be transferred from the container in which they are
dispensed into another container.

Version 2.0 POLICY MEDICINES POLICY Page 64 of 130
Date June 2016 Next Review Date June 2019
402. Oxygen and nitrous oxide cylinders should be stored in a secure area free of
grease within clinics. Safety chains or a stand should be used to ensure that non-portable cylinders are physically stable. Store away from flames and heat sources. A designated person must ensure that they are in working order, are correctly stored, have not exceeded any stated expiry dates and should check the cylinders once a month. A log of checks must be kept up to date.
403. In Foundation Trust Community Services premises, refrigerated items such as
vaccines must be stored in a locked drugs refrigerator and a daily log kept of temperatures using a maximum and minimum thermometer (Appendix 14).The refrigerator must be designed for vaccine storage. Domestic fridges are NOT appropriate. The person monitoring the temperature should sign the log entries. In the event of a breakdown in the refrigerator, the RBH FT Pharmacy should be contacted to ascertain whether any of the affected medicines could be saved.
404. A log should be kept of the time at which items are removed from the
refrigerator to ensure that items returned to the refrigerator have not been out for more than three hours (good practice).
405. Vaccines should be stored in a cool box with an ice pack pre-frozen, (which is
not touching the vaccines), for 5 hours when not refrigerated and ideally individual vaccines should not be returned to the fridge on more than one occasion. Any that are returned should be marked as such with the date and used first on the next occasion that the vaccine is required.
Version 2.0 POLICY MEDICINES POLICY Page 65 of 130
Date June 2016 Next Review Date June 2019
Supply of Medicines
BACKGROUND 406. The NHS Plan for Pharmacy England and Wales advocates the more cost-
effective use of medicines, the re-use of patients’ own drugs (PODs) is one way of reducing unnecessary duplication of supply and waste. Patients are encouraged to bring their medicines into hospital / community services so that they may be administered to them during their stay. Named patient drugs are medicines supplied and labelled by a Hospital / Community Pharmacy.
SUPPLY OF MEDICINES TO NAMED PATIENTS QUANTITY SUPPLIED 407. All supplies for named patients will be for one month for hospital wards and as
appropriate for individual patients in community services, using the manufacturer’s original pack wherever possible.
408. Exceptions to this general rule include:
Antibiotics: the appropriate course length will be supplied.
Inhalers, creams and ointments, suppositories, pessaries, eye drops and ointments: the smallest appropriate manufacturer’s original pack will be supplied.
Unusually bulky items that could not practically be accommodated on the ward: a quantity will be supplied after consideration of available storage space.
Short expiry medications: an appropriate quantity will be supplied after consideration of the expiry date.
Controlled Drugs, short term hypnotics, some laxatives, analgesics and when required (PRN) medicines
Drugs with frequently varying dosage, for example oral corticosteroids (e.g. Prednisolone, dexamethasone), and potassium supplements.
Oral anticoagulants (e.g. warfarin, phenindione, nicoumalone), will be supplied as a named patients, but labelled ‘as directed’ to allow for flexibility in dosage.
Injections, infusions, Nebules and dressings
409. Exceptions to the rule will be dispensed for named patients use at the discretion of the pharmacist/pharmacy technician where there is a reasonable likelihood that the patient will be discharged on the medication. Otherwise, stock should be used during the patients’ stay. Items will be dispensed on discharge if necessary.
CRITERIA FOR SUPPLY 410. Medicines will be supplied to patients:
Whose PODs are found to be unsuitable for re-use.

Version 2.0 POLICY MEDICINES POLICY Page 66 of 130
Date June 2016 Next Review Date June 2019
Who fail to bring in, or refuse re-use of, their PODs Where patients state they have their medicines at home.
Who have less than seven days supply of their medicines
Who have had a new medication started during their stay
PRE-PACKS 411. A small range of commonly used medicines may be available pre- labelled (pre
packs). Examples include analgesics, antibiotics, and laxatives. Pharmacy staff may issue these to patients (once checked by another approved pharmacy staff member). The patients’ name, the date dispensed, and the dose details must be entered in the relevant spaces on the pre-pack. A hospital address sticker should also be added.
SUPPLY OF MEDICINES OUTSIDE NORMAL PHARMACY WORKING HOURS (OUT OF HOURS) Royal Bolton Hospital 412. See Appendix 15 for the procedure for obtaining medicines outside normal
Pharmacy working hours. 413. Appendix 16 details the Procedure to be followed for dispensing medication for
urgent discharges when Pharmacy is closed. Community Services 414. The out of hours (OOH) service should be accessed. OOH GP’s will provide an
FP10 prescription which can be obtained from a Community Pharmacy. Darley Court 415. The Pharmacy out of Hours/Emergency Delivery Service procedure should be
used for supply of Urgent medication only. TRANSFER OF MEDICINES 416. PODs and named patient medicines must be transferred with the patient via
the transfer bag for medicines. Royal Bolton Hospital 417. The nurse transferring the patient must ensure the locker is empty and all
appropriate medicines are with the patient before the transfer can be completed. If the bed is empty, the locker must be open.
Community Services
Version 2.0 POLICY MEDICINES POLICY Page 67 of 130
Date June 2016 Next Review Date June 2019
418. It is the responsibility of the nurse/ health care professional to ensure all appropriate medicines are transferred with the patient. If the medication is unavailable a FP10 prescription should be supplied for all current items
DISCONTINUED MEDICINES Royal Bolton Hospital 419. These should be removed from the patient’s locker by the nursing staff or
Pharmacy staff as soon as they are crossed off the prescription. The change must be brought to the attention of the ward pharmacy team.
Community Services 420. Discontinued items should NOT be transferred with the patient. The patient’s
verbal permission should be obtained before removing the discontinued items which should be disposed of in the green PHS waste bin.
RE-LABELLING OF MEDICINES Royal Bolton Hospital 421. PODs and named patient medicines should only be re-labelled by Pharmacy
staff. 422. Medicines must be in packaging with a clearly visible expiry date. Other
medicines may be re-labelled at the discretion of a pharmacist. Following a dose adjustment to an existing medication, a POD or named patient medicine can continue to be used for the patient, but following the new prescribed dose instructions. The nursing staff must alert the pharmacy staff to the change on the next working day.
423. Pharmacy staff will then re-label the medicine with the new dose instructions at
the earliest convenience. Re-labelling may be delayed if it is likely that the dose will be changed again before discharge. It is essential that this be done before the medicine is issued on a discharge prescription.
Community Services 424. Medicines should not be relabelled. For any changes in doses a new supply
should be requested via the medical prescriber and obtained via a community pharmacy
RESUPPLY OF MEDICINE
Royal Bolton Hospital
425. Pharmacy will resupply medicines to patients when their own supply, or those issued by Pharmacy, has diminished to less than 7 days’ worth. New supplies
Version 2.0 POLICY MEDICINES POLICY Page 68 of 130
Date June 2016 Next Review Date June 2019
should be locked in the patient’s locker for use when the original supply runs out completely. Do not start the new pack until the previous pack is finished.
Community Services 426. Further supplies of medicines for individual patients may be re-ordered by Trust
staff through patient’s GP depending on individual patient needs. 427. Note: ordering medication may need to be included in the patients care plan to
enable carers to complete this task on behalf of the patient. 428. In Darley Court the Pharmacy team will ensure patients medication is re-
ordered throughout the patients stay. Any newly commenced items or dose changes should be brought to the attention of the Pharmacy Team.
PATIENT’S OWN DRUGS (PODS) 429. PODs can only be administered to the patient they belong to. These drugs
remain the property of the patient and permission must be sought from the patient to dispose of any discontinued or out of date medicines prior to discharge. They must not be administered to any other patient.
430. PODs must be assessed for suitability to re-use. See Appendix 16 for the
procedure. 431. During normal pharmacy working hours, this process will be carried out by
pharmacy staff. 432. Outside pharmacy hours, the ward nurse or admitting doctor may assess and
authorize the use of PODs until pharmacy authorization can be given on the next working day.
433. All suitable PODs must be stored in the individual patient’s locker, which must
be kept locked. 434. Any PODs found to be unsuitable for re-use should be ordered from the
Pharmacy Department when they are next open. Should the pharmacy be closed and the medications are required urgently, they may be obtained from the emergency cupboard, or other wards, in the usual way for short-term use. The pharmacy will re-label or supply a patient labelled pack (described previously), on the next working day.

Version 2.0 POLICY MEDICINES POLICY Page 69 of 130
Date June 2016 Next Review Date June 2019
General rules for supply of medicines to Community Services
435. The usual route of medicine procurement is by a patient specific prescription written by a Doctor, Dentist, or other Non-Medical Prescriber.
436. Medicines should be prescribed only when they are necessary, and in all cases
the benefits of administering the medicine should be considered to the risk involved. (BNF 63, 2012 www.bnf.org.uk).
437. Medicines shall be obtained only from bona fide suppliers. These will be:
Pharmacy Department at the Royal Bolton Hospital
Farillon (usual national supplier of vaccines)
Directly from the manufacturer
National Pharmaceutical Wholesalers
Community Pharmacies 438. A list of stock medicines specific to the various services will be held in clinics
and health centres. 439. The list and the quantity of stock to be held in each clinic shall be decided by
consultation between the Pharmacy Team, staff working in the clinics and appropriate senior medical, nursing or other professional staff.
440. The lists will be subject to regular review as required by those staff. Urgently
required items, not on the list, will only be provided after submitting a separate request, authorized by the appropriate line manager.
441. Stock control will be undertaken by a designated person(s) on regular basis but at least monthly to maintain agreed stock levels. This will include reconciliation of existing stock with the records in stock sheets.
442. The designated person must be from the appropriate staff group listed in the
paragraph 17.9. The responsible lead/manager must be notified of any discrepancies between stock records and levels.
443. The following personnel may request the supply of medicines identified on the
list for their service subject to their name being included on a list of authorised signatories:
Registered Nurses
Dental Nurse
Dental Practitioner
Community Paediatrician
Registered Podiatrist
Registered Physiotherapist
Registered Pharmacist
Registered Orthoptist
Registered Pharmacy Technician
Other designated FT staff
Version 2.0 POLICY MEDICINES POLICY Page 70 of 130
Date June 2016 Next Review Date June 2019
444. Specimen signatures of the above must be provided to the supplier (if
necessary) to confirm authorization for supply and should be updated on an annual basis or when a designated manager wishes to amend the register.
445. Medicines to be ordered from a supplier will be ordered on an official order
form or on-line. A copy of an order form will be retained to check against the goods received. N.B. Telephone orders will not be accepted.
446. Order forms/prescription pads must be kept in a secure area at all times i.e. in
a locked cupboard/drawer within a locked room. 447. When available, sugar-free medicines should be requested for patients/clients,
especially children.
Version 2.0 POLICY MEDICINES POLICY Page 71 of 130
Date June 2016 Next Review Date June 2019
Carriage of Medicines
COMMUNITY SERVICES 448. Bolton NHS FT Community Services staff may carry Prescription Only
Medicines that have been prescribed for named patients. The drugs must be transported out of sight in a locked car from the dispensing pharmacy direct to the patient. Alternatively, the dispensing pharmacy may be prepared to deliver directly to the patient. If staff feel exposed to potential security risks in the course of their duties they should contact their line manager and/or the police.
449. Registered nurses should carry adrenaline 1 in 1000, ideally in the form of a
pre-assembled syringe and needle in approved anaphylaxis packs. Suitably trained professionals should have access to adrenaline 1 in 1000 in clinics where local anesthetics are administered. Staff will then be able to respond to anaphylactic reactions in patients and administer the drug according to the Patient Group Direction. Staff should ensure that they are up to date with training requirements for the treatment of anaphylaxis.
ROYAL BOLTON HOSPITAL 450. Bolton NHS FT Hospital Services staff, wearing a valid trust ID badge, may
transfer medicines from the Pharmacy Department to clinical areas. 451. If the drugs are not transported by Pharmacy staff then they must be
transported in a sealed container from the pharmacy direct to the end user. 452. When transferring a patient, their drugs should be transported in a green
transfer bag. 453. A Standard Operating Procedure exists in Pharmacy Department for the
transfer of medicines between patient areas.
Version 2.0 POLICY MEDICINES POLICY Page 72 of 130
Date June 2016 Next Review Date June 2019
Disposal and Return of Medicines
COMMUNITY SERVICES 454. Please refer to Bolton NHS FT Healthcare Waste Management Policy and the
DH document Safe Management of Healthcare Waste. 455. The following principles should be adopted when disposing of medicines:
Witnessed accountability
Secure transit
Adequate documentation
Legally authorised persons to carry out and, where necessary, witness destruction
456. No medication, however small in quantity, should be disposed of in domestic or
commercial refuse or via the sewerage system.
457. Part-used multi-dose vials of vaccine will be destroyed in the clinic at the end of each session in the special waste sharps bin. Expired/unwanted vaccines may also be disposed of in the same way. A record is to be made in the stock book. Service managers must ensure appropriate procedures are in place at all premises from the service for which they are responsible is provided.
458. All sharps and syringes must be safely disposed of in Sharps Bins in
accordance with the organization’s Clinical Waste policy. For disposal of cytotoxic drugs and waste, see the organization’s Healthcare Waste Policy.
459. Prescribed medicines are the property of the patient and remain so when no
longer needed. The patient (or their representative) should, be encouraged to return the medication to a community pharmacy.
460. In exceptional circumstances, where every other option to remove unused
medication has been explored, a professionally qualified member of staff may return medication to a community pharmacy. A record of the medicines and quantities removed must be made and signed by the nurse or healthcare professional and the patient (or their representative). Medicines must be returned to a community pharmacy for safe disposal. See Appendix 17 “Protocol to remove discontinued and out of date medication from patients home” for further guidance.
461. Oxygen or nitrous oxide cylinders – any empty or unwanted oxygen or nitrous
oxide cylinders will be replaced or collected by the supplier. Equipment for the delivery of oxygen belongs to the supplying contractor (usually Air Products, telephone 0800 373580)
ROYAL BOLTON HOSPITAL

Version 2.0 POLICY MEDICINES POLICY Page 73 of 130
Date June 2016 Next Review Date June 2019
462. Please refer to Bolton NHS FT Healthcare Waste Management Policy and the DH document Safe Management of Healthcare Waste.

Version 2.0 POLICY MEDICINES POLICY Page 74 of 130
Date June 2016 Next Review Date June 2019
Reporting and Management of Medication Errors and Near Misses
INTRODUCTION AND BACKGROUND
Be Safe, be Honest – Report
463. See Trust Clinical Incident Policy and Management of Medication Error Policy. 464. All Drug Incidents / Near Misses are classed as Clinical Incidents and must be
reported using the usual incident reporting procedure. 465. The ward pharmacist / on-call pharmacist, senior pharmacy manager or
medicines safety nurse are available for advice and guidance and will be able to assist with any remedial action, advice regarding patient treatment, policy development and root cause investigations.
466. If a practitioner realises that an error has been made e.g. a drug has been omitted, given incorrectly or the procedure has failed, the following steps should be taken:
Check the patient’s well-being, explain to them what has happened and reassure them
Obtain advice if necessary e.g. from line manager, prescriber, Medicines Management Team, Medicines Information or medicines safety nurse in Pharmacy Department at Royal Bolton Hospital or the Out of hours service.
Arrange any necessary immediate treatment or follow-up for the patient.
Document the error in the nursing records (community staff) or patient records (hospital staff).
If a serious error occurs resulting in harm to the patient, the manager or director on call must be notified immediately.
Any errors involving Controlled Drugs must be reported to the Accountable officer for the Foundation Trust (The chief pharmacist).
Midwives should also inform their Supervisor of Midwives.
Report the incident using the incident reporting procedure and inform the line manager and prescriber at the first opportunity
467. In addition to this policy, health care professionals should, at all times, follow their own professional code of conduct. For registered nurses, the Nursing and Midwifery Council has guidelines for the administration of medicines which is available at www.nmc-uk.org.
468. Local policies and guidelines should be followed and advice sought if necessary
ADVERSE DRUG REACTION (ADR) REPORTING AND MANAGEMENT What is an Adverse Drug Reaction?

Version 2.0 POLICY MEDICINES POLICY Page 75 of 130
Date June 2016 Next Review Date June 2019
469. An unwanted or harmful reaction experienced following the administration of a
drug or combination of drugs under normal conditions of use and suspected to be related to the drug
470. Ref. MHRA Suspected adverse drug reaction (ADR) reporting and the Yellow
Card Scheme, Guidance notes 471. Suspected adverse drug reactions should be reported through the Yellow Card
Scheme. Yellow cards help identify trends in adverse drug reactions and so improve medicines safety in the long-term. Reporting is a professional responsibility and can be done by any healthcare professional. Patients can also report adverse reactions independently to the Yellow Card Scheme.
472. Yellow cards can be found online at www.yellowcard.gov.uk and at the back of
the BNF. You only need a suspicion to report, you do not have to be certain. Please include as much information as possible but do not be put off reporting just because some details are not known.
473. Please report all suspected adverse drug reactions for new medicines
(identified by the black triangle ▼ symbol in the BNF and all serious suspected ADRs for established vaccines and medicines, including unlicensed medicines, herbal remedies, and medicines used off-label. If you are unsure whether or not to report, please report anyway.”
Areas of special interest: 474. Please report all suspected adverse reactions involving:
children
elderly
delayed drug effects
congenital anomalies
herbal remedies
Pharmacy involvement
475. The ward pharmacist or Medicines Information team must be informed of any suspected adverse drug reaction and can provide essential advice in the management of any ADR. The on-call pharmacist is available for advice outside normal pharmacy hours.

Version 2.0 POLICY MEDICINES POLICY Page 76 of 130
Date June 2016 Next Review Date June 2019
Medicines Management Training
476. The management of medicines (prescribing, storing, administering etc.) within the clinical areas plays an ever increasing part in the roles of many registered practitioners. It is therefore important that staff involved in medicines management are trained appropriately to reduce the significant number of adverse patient events relating to medicines management.
477. Registered Healthcare Professionals involved in the management of
medication should access the Medicines Management e-learning module via the Trust Intranet. Mandatory Medicines Management Training must be completed every 2 years.
478. Please find Guidance on the Role of Unregistered Staff in Appendix 3 of this
Policy. 479. Please note:
All staff who are involved in a medication error should be managed according to the Management of Medication Errors Policy.
Version 2.0 POLICY MEDICINES POLICY Page 77 of 130
Date June 2016 Next Review Date June 2019
Monitoring Compliance
480. Adherence to this policy will be monitored as a key part of the pharmacy service delivery. Specific audits are detailed in the Pharmacy Department Audit Calendar (see appendix 20).
481. Pharmacy staff visit trust wards daily (Monday – Friday) and monitor
prescribing for clinical efficacy, safety, appropriateness and compliance with Bolton NHS Foundation Trust Formulary (including Trust Antibiotic Guidelines).
Additional monitoring is as stated below: 482. Prescribing in the Royal Bolton Hospital is monitored by the pharmacy
department. All outpatient prescriptions (with the exception of a very small number of FP10s (HP) prescriptions written in emergency situations outside pharmacy hours) are monitored and checked in the dispensary. This monitoring by a pharmacist is a legal and professional requirement. The dispensary is a Registered Pharmacy and as such is subject to inspection and audit by the General Pharmaceutical Council Inspectorate and Enforcement Division. Any concerns about unusual, excessive or inappropriate prescribing must be escalated.
483. Quality of medicines: This is a professional requirement for pharmacists.
External support is provided by Quality Control North West (QCNW) and the Regional Tendering Process for Pharmaceuticals. Any defects are reported through the pharmacy to QCNW who hold a database of defects and cascade any MHRA Safety Alerts. Action on these defects and alerts is stored in pharmacy.
484. Storage of medicines: Ward managers are responsible for ensuring medicines
are stored appropriately on each ward. Pharmacy Technicians carry out a three monthly audit on the storage of medicines in hospital clinical areas. Any discrepancies are reported through senior nursing staff.
485. Administration of medicines: The ward managers carry out an omitted dose
audit, this is carried out monthly and the results are reported back to the Medicines Safety Group.
486. Controlled Drugs (including the use of Methadone and Illicit Substances:
Pharmacy staffs carry out a three monthly audit on the use and storage of controlled drugs. This is reported through the Trust Accountable Officer for Controlled Drugs and further reported to the Controlled Drugs Local Information Network. This Network produces an annual report. Pharmacy and a Divisional Manager audit any returned controlled drugs / illicit substances (or substances believed to be illicit) twice a year.

Version 2.0 POLICY MEDICINES POLICY Page 78 of 130
Date June 2016 Next Review Date June 2019
487. Bolton System of Care Accreditation (BSCA): The BSCA process has been developed to draw together available information about patient care, adapted in part from the CQC Quality and Safety outcomes, to analyse the care that patients receive within an area such as hospital ward or community services. The process aims to respond in a systematic way should areas of concern be identified. Action will then be taken to effectively diagnose and resolve issues.
488. There are a number of standards within BCSA, including:
• Controlled Drug Management
• Wardex standards
• Daily fridge checks
489. This process is systematically adopted in Bolton NHS Foundation Trust,
reviewing every ward/department in order to assure the Trust Board of the quality of patient care, this includes monitoring the environment, care provided and leadership.
490. Community Services: In Community Services, all areas that handle medicines
carry out an annual audit to ensure that medicines are stored safely and securely. A sample audit is included in Appendix 1 and each team should use this as a template to complete the audit. It should be completed and returned to the line manager with an action plan, if appropriate.
Version 2.0 POLICY MEDICINES POLICY Page 79 of 130
Date June 2016 Next Review Date June 2019
Appendix 1- Protocol for safe and secure handling of medicines in Community Services
Annual review Year …………….
Area or Department of Employment …………………………………………
These standards apply to all Bolton NHS Foundation Trust employed staff
working in community services It should be available for inspection as necessary.
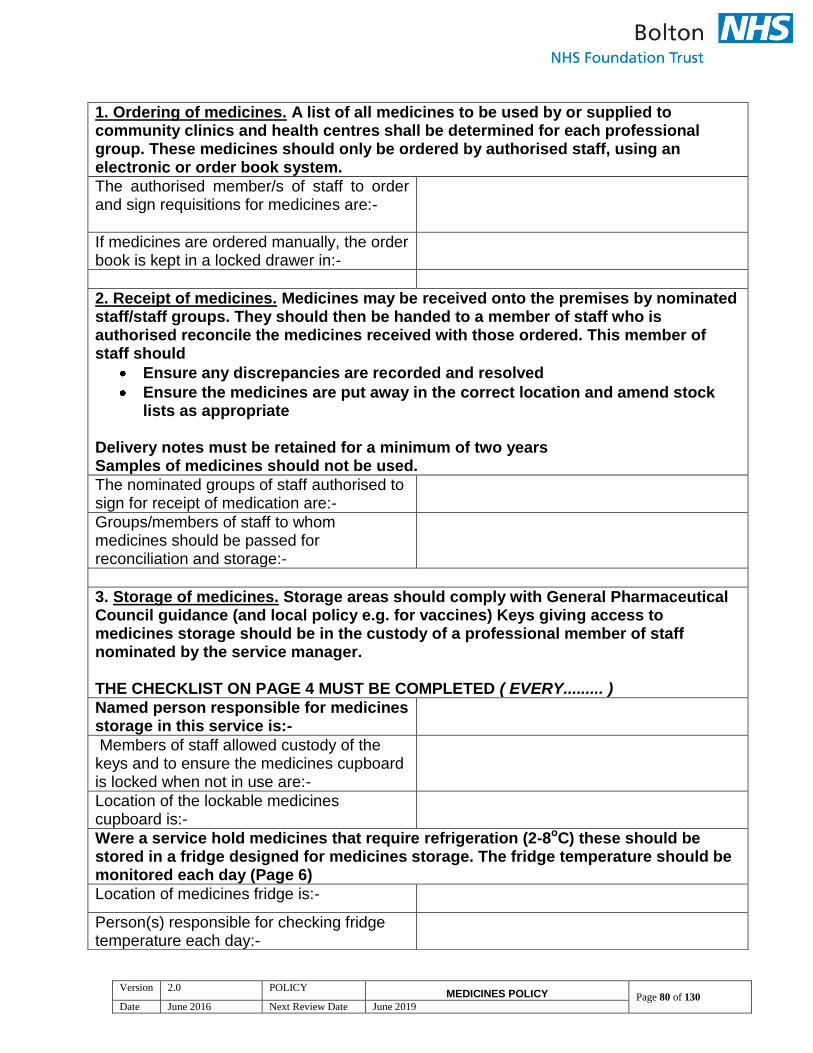
Version 2.0 POLICY MEDICINES POLICY Page 80 of 130
Date June 2016 Next Review Date June 2019
1. Ordering of medicines. A list of all medicines to be used by or supplied to community clinics and health centres shall be determined for each professional group. These medicines should only be ordered by authorised staff, using an electronic or order book system.
The authorised member/s of staff to order and sign requisitions for medicines are:-
If medicines are ordered manually, the order book is kept in a locked drawer in:-
2. Receipt of medicines. Medicines may be received onto the premises by nominated staff/staff groups. They should then be handed to a member of staff who is authorised reconcile the medicines received with those ordered. This member of staff should
Ensure any discrepancies are recorded and resolved
Ensure the medicines are put away in the correct location and amend stock lists as appropriate
Delivery notes must be retained for a minimum of two years Samples of medicines should not be used.
The nominated groups of staff authorised to sign for receipt of medication are:-
Groups/members of staff to whom medicines should be passed for reconciliation and storage:-
3. Storage of medicines. Storage areas should comply with General Pharmaceutical Council guidance (and local policy e.g. for vaccines) Keys giving access to medicines storage should be in the custody of a professional member of staff nominated by the service manager. THE CHECKLIST ON PAGE 4 MUST BE COMPLETED ( EVERY......... )
Named person responsible for medicines storage in this service is:-
Members of staff allowed custody of the keys and to ensure the medicines cupboard is locked when not in use are:-
Location of the lockable medicines cupboard is:-
Were a service hold medicines that require refrigeration (2-8oC) these should be stored in a fridge designed for medicines storage. The fridge temperature should be monitored each day (Page 6)
Location of medicines fridge is:-
Person(s) responsible for checking fridge temperature each day:-
Version 2.0 POLICY MEDICINES POLICY Page 81 of 130
Date June 2016 Next Review Date June 2019
4. Administration of medicines. Individual staff must ensure that:
They are trained and competent to administer medication and comply with all professional standards, local policy and national guidance
A record of administration is made in the appropriate Medication Record Chart. If medicines cannot be administered for any reason the MAR is annotated accordingly.
A named person is responsible for ensuring that
Version 2.0 POLICY MEDICINES POLICY Page 82 of 130
Date June 2016 Next Review Date June 2019
A regular audit takes place of a sample of the Medication Record Chart to ensure they are completed correctly.
An action plan is completed and forwarded to the line manager where appropriate.
Person responsible for regular MAR sheet audit is:-
5. Disposal of medicines. Out of date medication should be appropriately packaged and returned to a licensed waste carrier for destruction. The Pharmacy Department at RBH should be contacted for advice relating to excess stock. Details of stock returned should be recorded and stock lists amended as necessary
6. Controlled Drugs. All areas that handle Controlled Drugs (CD’s) should have Standard Operating Procedure (SOP). The SOP should cover all aspects of controlled drug risk management and audit trails for the ordering, storing, prescribing, dispensing, recording, supply, administration, and destruction of CDs appropriate to the setting and the team. THE CHECKLIST ON PAGE 5 MUST BE COMPLETED (EVERY.......)
Staff member responsible for ensuring an SOP is available and controlled drugs are handled as detailed in the SOP
The nominated staff holding keys to the CD cupboard are:-
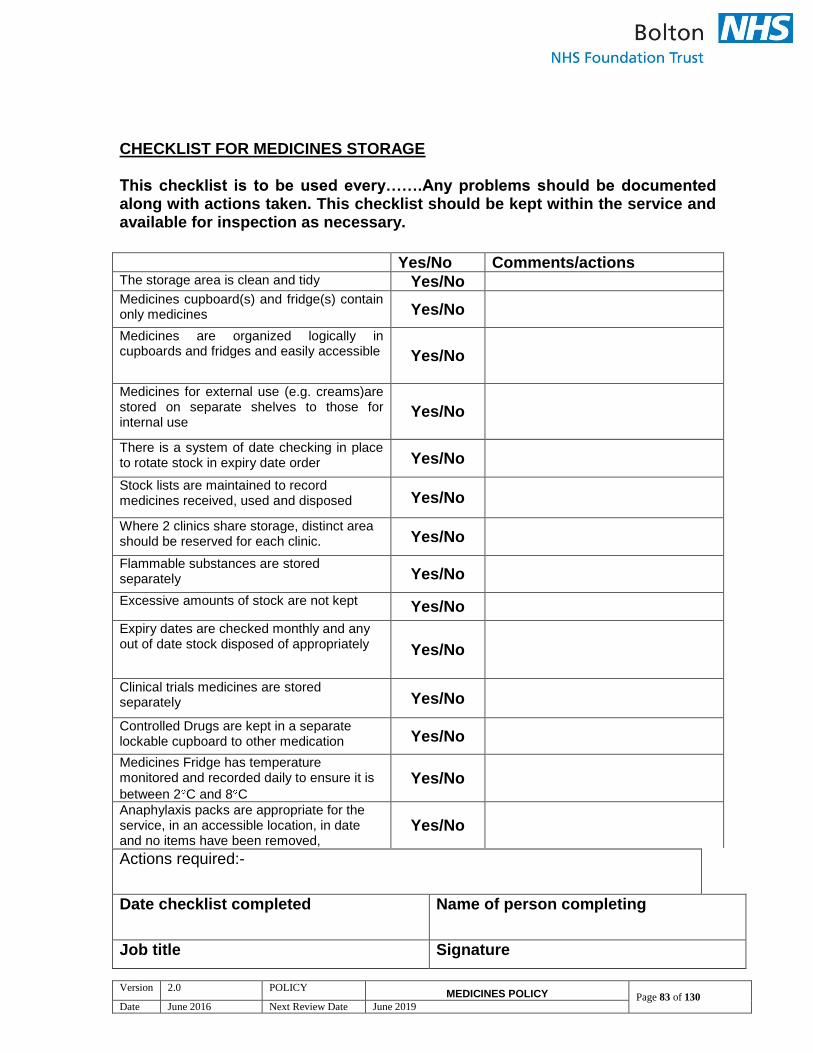
Version 2.0 POLICY MEDICINES POLICY Page 83 of 130
Date June 2016 Next Review Date June 2019
CHECKLIST FOR MEDICINES STORAGE This checklist is to be used every…….Any problems should be documented along with actions taken. This checklist should be kept within the service and available for inspection as necessary.
Actions required:-
Date checklist completed Name of person completing
Job title Signature
Yes/No Comments/actions The storage area is clean and tidy Yes/No Medicines cupboard(s) and fridge(s) contain only medicines Yes/No
Medicines are organized logically in cupboards and fridges and easily accessible Yes/No
Medicines for external use (e.g. creams)are stored on separate shelves to those for internal use
Yes/No
There is a system of date checking in place to rotate stock in expiry date order Yes/No
Stock lists are maintained to record medicines received, used and disposed Yes/No
Where 2 clinics share storage, distinct area should be reserved for each clinic. Yes/No
Flammable substances are stored separately Yes/No
Excessive amounts of stock are not kept Yes/No
Expiry dates are checked monthly and any out of date stock disposed of appropriately Yes/No
Clinical trials medicines are stored separately Yes/No
Controlled Drugs are kept in a separate lockable cupboard to other medication Yes/No
Medicines Fridge has temperature monitored and recorded daily to ensure it is
between 2 C and 8 C Yes/No
Anaphylaxis packs are appropriate for the service, in an accessible location, in date and no items have been removed,
Yes/No

Version 2.0 POLICY MEDICINES POLICY Page 84 of 130
Date June 2016 Next Review Date June 2019
CHECKLIST FOR CONTROLLED DRUGS This checklist is to be used every…….Any problems should be documented along with actions taken. This checklist should be kept within the service and available for inspection as necessary.
Yes/No
Comments/ actions required
The current Standard Operating Procedure (SOP) is available.
Yes/No
The CD cupboard is kept in a lockable area not normally accessible to patients
Yes/No
The room containing the CD cupboard is kept tidy
Yes/No
The CD’s are stored in a locked secure container that is not portable
Yes/No
If a safe is used to store CD’s there is a separate receptacle within the safe to keep the CD’s
Yes/No
The CD register contains entries of all stock received or removed
Yes/No
All the entries have been initialled (by 2 members of staff if possible).
Yes/No
Does controlled drug stock balance agree with that in register? If no this must be investigated
Yes/No
Actions required:-
Date checklist completed Name of person completing
Job title Signature

Version 2.0 POLICY MEDICINES POLICY Page 85 of 130
Date June 2016 Next Review Date June 2019
Protocol checked by ……………………………………….. (Signature)
Name in block capitals …………………………………………… Job Title …………………………………………… Date …………………………………………… This protocol must be reviewed no later than……………………..
Version 2.0 POLICY MEDICINES POLICY Page 86 of 130
Date June 2016 Next Review Date June 2019
Appendix 2 - PGD Template
Administration or supply (as appropriate)
of (name of the drug) in the (name of the ward/department)
Document type: Patient Group Direction
Version:
Author (name):
Author (designation):
Validated by
Date validated
Ratified by: Drugs & Therapeutics Committee
Date ratified:
Name of responsible committee/individual:
Name of Executive Lead (for policies only) N/A
Master Document Controller:
Date uploaded to intranet: N/A
Key words
Review date:
Version control
Version Type of Change Date Revisions from previous issues
Equality Impact
Bolton NHS Foundation Trust strives to ensure equality of opportunity for all service users, local people and the workforce. As an employer and a provider of healthcare Bolton NHS FT aims to ensure that none are placed at a disadvantage as a result of its policies and procedures. This document has therefore been equality impact assessed to ensure fairness and consistency for all those covered by it regardless of their individuality. The results are shown in the Equality Impact Assessment (EIA)
Version 2.0 POLICY MEDICINES POLICY Page 87 of 130
Date June 2016 Next Review Date June 2019
Contents
Content Page 3-4
Monitoring Page 4
Authorisation Page 5-6
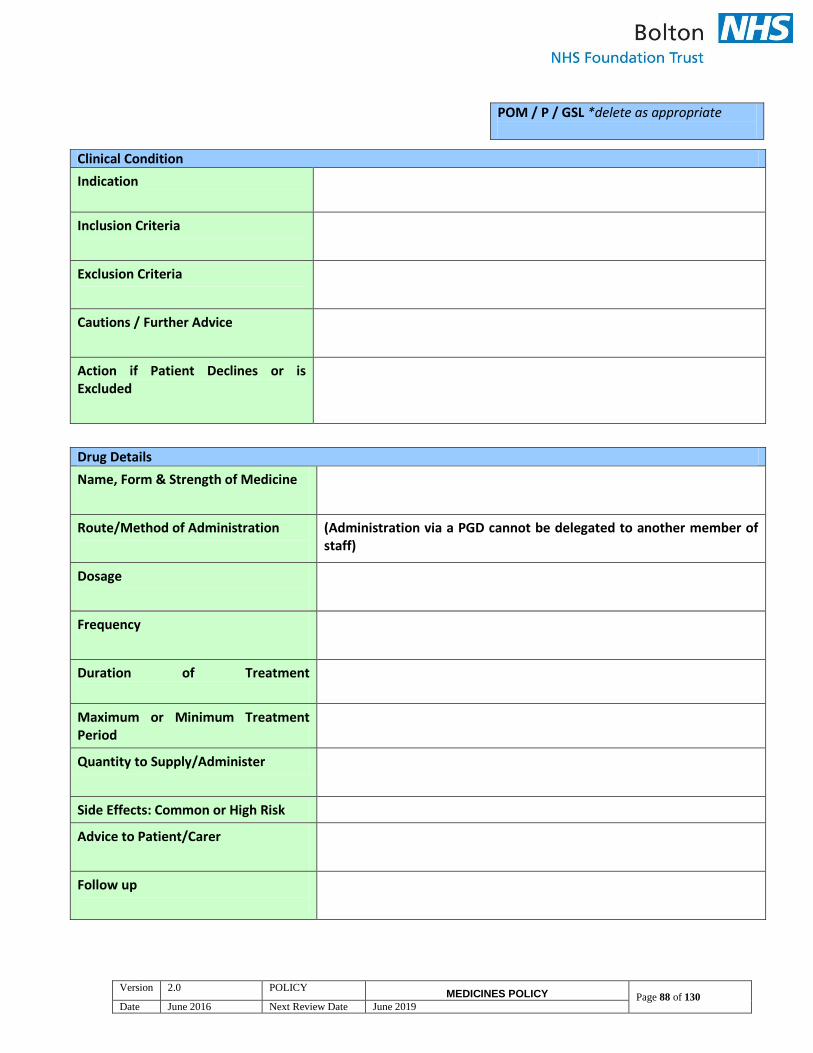
Version 2.0 POLICY MEDICINES POLICY Page 88 of 130
Date June 2016 Next Review Date June 2019
POM / P / GSL *delete as appropriate
Clinical Condition
Indication
Inclusion Criteria
Exclusion Criteria
Cautions / Further Advice
Action if Patient Declines or is Excluded
Drug Details
Name, Form & Strength of Medicine
Route/Method of Administration
(Administration via a PGD cannot be delegated to another member of staff)
Dosage
Frequency
Duration of Treatment
Maximum or Minimum Treatment Period
Quantity to Supply/Administer
Side Effects: Common or High Risk
Advice to Patient/Carer
Follow up
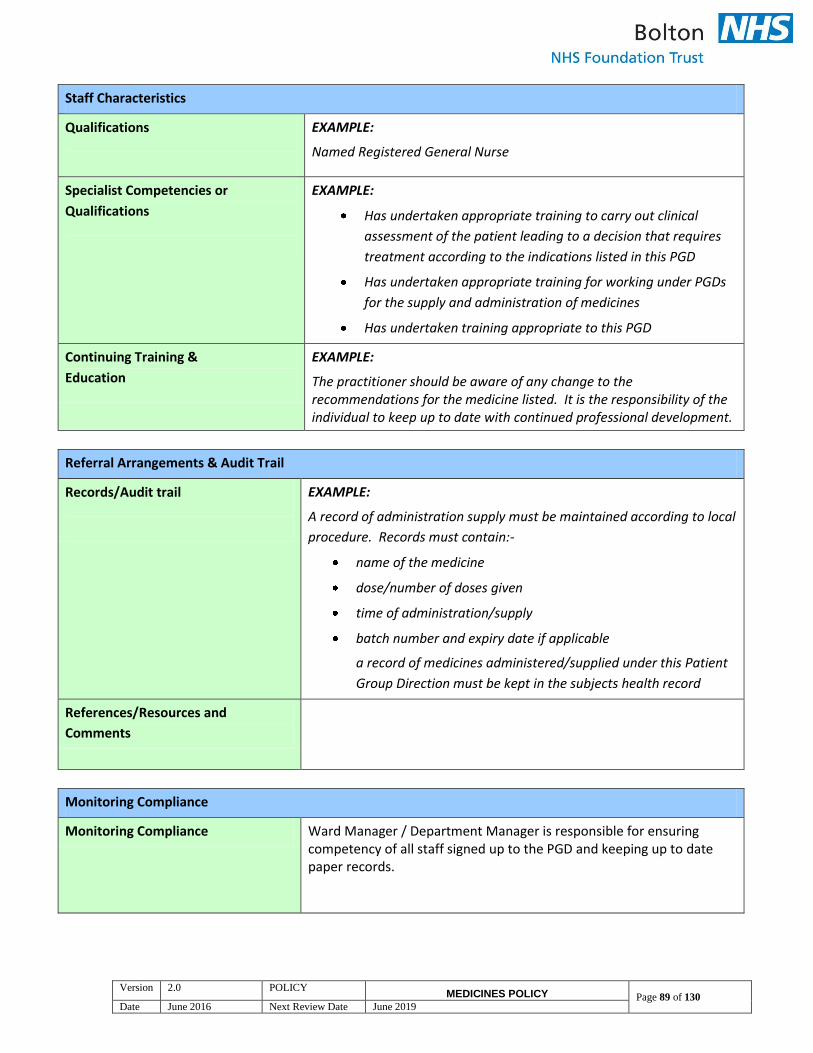
Version 2.0 POLICY MEDICINES POLICY Page 89 of 130
Date June 2016 Next Review Date June 2019
Staff Characteristics
Qualifications
EXAMPLE:
Named Registered General Nurse
Specialist Competencies or
Qualifications
EXAMPLE:
Has undertaken appropriate training to carry out clinical
assessment of the patient leading to a decision that requires
treatment according to the indications listed in this PGD
Has undertaken appropriate training for working under PGDs
for the supply and administration of medicines
Has undertaken training appropriate to this PGD
Continuing Training &
Education
EXAMPLE:
The practitioner should be aware of any change to the recommendations for the medicine listed. It is the responsibility of the individual to keep up to date with continued professional development.
Referral Arrangements & Audit Trail
Records/Audit trail
EXAMPLE:
A record of administration supply must be maintained according to local
procedure. Records must contain:-
name of the medicine
dose/number of doses given
time of administration/supply
batch number and expiry date if applicable
a record of medicines administered/supplied under this Patient
Group Direction must be kept in the subjects health record
References/Resources and
Comments
Monitoring Compliance
Monitoring Compliance Ward Manager / Department Manager is responsible for ensuring competency of all staff signed up to the PGD and keeping up to date paper records.

Version 2.0 POLICY MEDICINES POLICY Page 90 of 130
Date June 2016 Next Review Date June 2019
This patient group direction must be agreed to and signed by all health care professionals involved in its use. The
NHS Trust should hold the original signed copy. The PGD must be easily accessible in the clinical setting.
Organisation
Bolton NHS Foundation Trust
*FOR PHARMACY OFFICE USE ONLY*
Authorisation Part 1
Clinical Lead / Head of Division
Name:
Signature: Date:
Medical Director Name: Mr Stephen Hodgson
Signature: Date:
Director of Nursing Name: Trish Armstrong - Child
Signature: Date:
Chief Pharmacist Name: Steven Simpson
Signature: Date:
Authorisation Part 2
Ratified by the Drugs & Therapeutics
Committee
Name:
Signature: Date:

Version 2.0 POLICY MEDICINES POLICY Page 91 of 130
Date June 2016 Next Review Date June 2019
Authorisation
PGDs DO NOT REMOVE INHERENT PROFESSIONAL OBLIGATIONS OR ACCOUNTABILITY. It is the responsibility of each professional to practice only within the bounds of their own competence and in accordance with their own Code of Professional Conduct. Note to Authorising Managers: authorised staff should be provided with an individual copy of the clinical content of the PGD and a photocopy of the document showing their authorisation. I have read and understood the Patient Group Direction and agree to supply/administer this medicine only in accordance with this PGD.
Name of Professional Signature Authorising Manager Date
Version 2.0 POLICY MEDICINES POLICY Page 92 of 130
Date June 2016 Next Review Date June 2019
Appendix 3 – The Role of Unregistered Staff in the Administration of Medicines
1. THE ROLE OF UNREGISTERED STAFF IN THE ADMINISTRATION OF MEDICINES
If it has been agreed that it is in the best interests of a particular group of patients that an unregistered member of staff administers specified medication eg the instillation of eye drops to enlarge the pupil prior to examination of the eye, this must first have the approval of the Trust Medicines Safety Committee. Registered practitioners are responsible for the delegation of any aspects of the administration of medicinal products to unregistered staff and are accountable to ensure that the unregistered member of staff is competent to carry out the task and that robust governance processes are in place which have been approved by the Trust Medicines Safety Group.
In bed based services on completion of an initial assessment of need by a registered nurse, unregistered staff (i.e. Assistant Practitioners, Healthcare Assistants and Healthcare Support Workers) can assist a registered nurse with medicine administration where the patient may need time to take the medicine, or when they are caring for a particular patient at the time of the administration of the prescribed medicine. The registered nurse retains the responsibility for checking both the medicine and the identification of the patient.
2. GUIDANCE FOR STUDENT NURSES IN THE ADMINISTRATION OF MEDICINES
Student nurses can participate in the administration of medicines following theoretical preparation from Higher Educational Institute (HEI). They must be under the direct supervision of a registered practitioner who must ensure that the student has received instruction in the administration of medicines; knowledge of the Medicines Policy, Positive Patient Identification Policy and Medical Devices Policy, and is competent to undertake the task. Once a 2ndor3rd year student has been observed and completed the practice checklist for second checking, at the discretion of their mentor, they can then carry out second checks, in all areas except high risk areas which are: Neonatal Unit, Intensive Care Unit, High Dependency Unit and Coronary Care Unit. The registered practitioner should ask for verification of the observed practice checklist. At all times the registered practitioner is accountable. Student nurses can:
Act as the ‘second checker’ in the administration of controlled drugs inclusive of patient controlled analgesia after completing the Trust competencies (as long as these do not require a second check of the calculation)

Version 2.0 POLICY MEDICINES POLICY Page 93 of 130
Date June 2016 Next Review Date June 2019
Act as the ‘second checker’ in giving take-home medicines to patients at discharge after appropriate training session
Act as the `second checker` in Normal Saline Flush when performing Cannulation, Sodium Chloride 0.9%, Dextrose Saline 5%, Dextrose/Saline 0.45%/0.9%, Hartman’s solution.
There are a number of restrictions and the Student Nurse cannot carry out any of the following tasks;
Hold the drug keys or complete drug rounds
Sign for any medication alone, in the case of IV infusions these should be countersigned by a registered nurse
Act as ‘second checker’ for intravenous antibiotics, or insulin
Act as a ‘second checker where a dose calculation needs to be performed
Administer a saline flush or commence fluids via a central venous line
3. HEALTH CARE SUPPORT WORKERS SUPPORTING CHILDREN WITH SPECIAL/COMPLEX NEEDS WHO ARE CARED FOR AT HOME
Registered nurses may delegate the administration of certain medicines to Health Care Support Workers (HCSWs) who are based in specific community settings i.e. children who attend special schools and children with complex needs who are cared for in their own homes, provided that necessary governance processes are in place.. “A registered nurse is responsible for the delegation of any aspects of the administration of medicinal products and they are accountable to ensure that the care assistant is competent to carry out the task. In the care of children with complex needs, where an individual care plan has been written and signed off by a registered nurse and the unregistered practitioner has been assessed by a registered nurse as competent to undertake the specific administration of medicinal products to a specific named patient, this may be undertaken, for example, children with complex health needs in community settings, palliative care” (NMC Standards for Medicines Management, 2010) Medications may only be administered by HCSWs via the following routes:
Oral
Inhalation
Rectal
Nasogastric
Percutaneous Endoscopic Gastrostomy (PEG)
Nebulised
Topical
Buccal
Health Care Support Workers must not administer medicines via the Intravenous , Intramuscular or Subcutaneous route. A written instruction for the medication, which may be in the form of a prescription or a Patient Specific Direction, must be given by a doctor, dentist or non medical prescriber and a consent form must have been signed by the patient’s parent or legal guardian. Once the medication has been administered, the HCSW must record this on the record of administration sheet.
Version 2.0 POLICY MEDICINES POLICY Page 94 of 130
Date June 2016 Next Review Date June 2019
HCSWs must undertake specific training in the administration of the prescribed medicines and their competence must be confirmed by a registered nurse. A copy of the completed competency assessment form must be kept in the individual’s personal file and training must be recorded on their electronic staff record (ESR). Competency should be reviewed annually as part of the appraisal process.
Proposal for Unregistered Staff to Administer Prescribed Medication
In certain circumstances it may be beneficial to patients and meet the needs of the service if unregistered members of staff are permitted to administer specific medications within a robust clinical governance framework. In order for this practice to be considered, approval must be sought from the Trust Medicines Safety Group. The proposal must be supported by the Divisional Nurse Director. Name of ward/department/service: Division: Name of manager submitting application: Signature: Designation: Date: Please give details about the medication/s you wish the unregistered staff to administer, including indication, dose, strength, route and frequency: Please explain how it will benefit patients and improve the service if unregistered staff could administer the medication detailed above: Please give details about the unregistered staff that are required to administer specified medication: Name Job Title Pay Band
1.
Version 2.0 POLICY MEDICINES POLICY Page 95 of 130
Date June 2016 Next Review Date June 2019
Please confirm that the following have been developed and agreed by the multi-disciplinary team: (Please tick)
A prescription, or Patient Specific Direction, for every patient, written by a doctor or non
medical prescriber □
A Standard Operating Procedure, listing the names of the unregistered staff □ Arrangements for the safe storage and selection of the specified medication □
A training programme, tailored specifically for unregistered staff □
An assessment of theoretical competency □
An assessment of practical competency □
A system for annual review of competence □
A training/annual review record for each member of staff □
A named, registered professional in the department who has agreed to be responsible
for maintaining training and competency records for the unregistered staff □
(NB Unregistered staff can NOT operate under a Patient Group Direction.)
Signatures I confirm that the information provided is correct and that the governance processes and documentation listed above have been developed. Signature of ward/department/service manager: Print name:
Signature of Divisional Nurse Director: Print name
Please e-mail the completed pro-forma to Medicines Safety Nurse, Bolton Foundation Trust.
Version 2.0 POLICY MEDICINES POLICY Page 96 of 130
Date June 2016 Next Review Date June 2019
Appendix 4 - Standard Operating Procedure for Controlled Drugs for Royal Bolton Hospital
PRESCRIBING OF CONTROLLED DRUGS
See Section 6 of the Medicines Policy
RECORD-KEEPING
1. The following books are to be kept on every ward or any other area receiving Controlled Drugs:
a) Controlled Drugs Record Book (CD register) – main register, all stock of Controlled Drugs received and administered to be recorded in there, keeps running balances of all stocks of controlled drugs
b) Controlled Drugs Order Book – to be used for all orders of controlled drugs c) Controlled Drugs Daily Drug Count Book – a record of daily stock check. d) Patient’s Own Controlled Drugs Book – a record of controlled drugs
received from patients, their administration and returns back to patients or relatives acting on their behalf
e) Authorisation List – a list of staff authorized to order Controlled Drugs. Controlled Drugs will not be supplied if person ordering is not an authorized signatory.
2. New books and registers can be obtained from Pharmacy Department. 3. Completed Controlled Drugs Record Books and Controlled Drugs Order
Books to be stored on wards for at least the legal minimum of two years, after the date of the last entry, and then destroyed securely.
4. It is recommended that all controlled drug records be kept securely for as long as possible regardless of the legal minimum. Five years would be considered appropriate.
ORDERING CONTROLLED DRUGS FOR INPATIENTS
1. Controlled Drugs Order Book must be used for all orders. 2. Fill in full information regarding name of drug, form, strength, ampoule size
(for injections where more than one exists) and quantity required. 3. A separate page must be used for each item. Ensure the carbon is placed
between the white and pink sheets of the requisition and it is the correct way round.
4. Only registered nurses authorised to do this by their Ward or Department Manager can order Controlled Drugs.
5. The name of the nurse requesting the Controlled Drugs should be printed underneath the signature.
Version 2.0 POLICY MEDICINES POLICY Page 97 of 130
Date June 2016 Next Review Date June 2019
6. A list of authorised signatories is held in the Pharmacy department for each ward. Ward/Department managers are required to complete an authorization form for any new signatory to be added to the existing list.
7. Pharmacy also has to be provided with a complete list of authorised signatories every 12 months.
8. Staff should assess each day whether stocks need to be ordered, using the ward CD register as a guide. This should be done by the night staff the day
before so the orders are ready for collection in the morning. Ideally this should not be the same staff that have done the daily stock check.
9. Pharmacy will phone each of the acute wards in the morning between 8-8.30am to check which wards have CD orders that need collecting.
10. Pharmacy will collect the controlled drug order books from the acute wards they have phoned before 10am, and drugs will be delivered back to the wards after 2pm.
11. For all other wards, requisition books should be sent to Pharmacy before the cut off time of 10am on weekdays.
12. Orders should only be sent after 10am in the following circumstances:
CDs required for patients who are newly admitted on non-stock controlled drugs
CDs required for end of life patients 13. Orders for Controlled Drugs for the weekend must be placed before 10am on
Friday. Therefore on a Thursday evening staff should assess usage needed to last until Monday morning.
14. Only in exceptional situations will Controlled Drugs be supplied from Pharmacy on Saturday or Sunday. See exceptions listed in point 12 above. Any orders that are outside these exceptions (i.e for routine stocks) will result in an Incident form being completed.
OBTAINING CONTROLLED DRUGS IN AN EMERGENCY OUT-OF-HOURS
1. Single doses of Controlled Drugs can be administered from another ward’s stock.
2. For legal reasons only single doses can be administered this way. 3. Administration procedure is to be followed as per section 9. 4. A registered nurse from the supplying ward is to act as the second nurse for
the purpose of administration. 5. The CD register of the ward supplying the Controlled Drug should be signed
by the nurses of both the supplying and receiving ward. 6. The supplying nurse from the supplying ward must observe the Controlled
Drug being entered into the CD register of the receiving ward. 7. In cases of difficulty, the on-call pharmacist can provide advice.
DELIVERY OF CONTROLLED DRUGS FROM PHARMACY
1. Controlled Drugs may be collected from the Pharmacy by any member of
staff with a current Trust ID badge – the messenger.
Version 2.0 POLICY MEDICINES POLICY Page 98 of 130
Date June 2016 Next Review Date June 2019
2. The messenger will sign for receipt of the sealed bag and must then gain the signature of a registered nurse on the ward once delivered.
3. The messenger must ensure security of the Controlled Drugs in transit. 4. The registered nurse signing “received by” is responsible for the immediate
entry into the CD register and the immediate transfer to the Controlled Drugs Cupboard.
5. The top copy of the requisition should not leave the Pharmacy. 6. For patient specific prescriptions (Outpatient / TTOs) the pharmacist must
ascertain whether the person collecting a Schedule 2 or 3 Controlled Drugs is the patient, the patient’s representative or a member of staff. Signatures must be recorded.
RECEIPT OF CONTROLLED DRUGS ON WARD
1. Controlled Drugs must be received on the ward by a registered nurse,
preferably person in charge, and signed for in the presence of the messenger.
2. The drugs should be locked in the Controlled Drugs Cupboard immediately. 3. The appropriate entry should be made in the ward Controlled Drugs Record
Book (CD Register) by the person who received the controlled drugs and witnessed by a second nurse.
STORAGE OF CONTROLLED DRUGS
1. For drugs to be stored in the Controlled Drugs Cupboard, see Appendix 5.
Access and keys should be restricted to persons authorised under the Misuse of Drugs Act, i.e. the ward manager or the person in charge of the ward or area.
2. All general wards should only keep standard strength opiates as routine stock, if they need higher strength vials the ward pharmacist should be informed and these should be kept on a shelf separate from the standard strengths. (NPSA recommendation)
STOCK CHECKS OF CONTROLLED DRUGS
1. The ward or department manager / designated deputy is responsible for a
DAILY check of stocks of Controlled Drugs which must be recorded in the Controlled Drugs Daily Drug Count Book.
2. Individual areas (e.g. Theatres, Endoscopy Unit) may decide to undertake more frequent checks as deemed appropriate by the person in charge.
3. Discrepancies should be reported immediately via Safeguard system and also verbally to the matron or designated deputy and the Ward Pharmacist, who will inform the Accountable Officer.
4. A pharmacist/pre-registration pharmacist, along with the ward manager, will check the balance of Controlled Drugs at three-monthly intervals.
5. Staff undertaking the daily stock check should be rotated periodically and should not be involved in ordering or receiving of Controlled Drugs where possible.

Version 2.0 POLICY MEDICINES POLICY Page 99 of 130
Date June 2016 Next Review Date June 2019
6. Stock check should involve checking of the balance in the Controlled Drugs Register against the contents of the Controlled Drugs Cupboard to ensure all balances are checked.
7. Stock balances of liquid medicines should be checked by visual inspection, however the balance must be confirmed correct on completion of a bottle
ADMINISTRATION OF CONTROLLED DRUGS
1. Unless given by a doctor, administration of Controlled Drugs must be carried
out by two members of staff or members of the relevant department, one of whom is a registered nurse.
2. Both the administering nurse and a witness should:
a) check the prescription b) observe preparation of the dose c) take the dose to the patient d) observe administration of the dose e) reconcile the stocks remaining f) sign the register immediately
3. Administration should also be recorded on the prescription chart (All other
relevant policies, including those for parenteral and paediatric administration still apply).
4. Exceptions to these rules are:
Administration of “when required” doses of up to 30mg of morphine from 10mg in 5ml oral liquid for which a second check is not required
Administration of oral Tramadol.
Administration of IV morphine injections, where 2 registered nurses have to check the dose, however titration of the dose can be undertaken by 1 nurse only
5. Doses of CDs that need discarding must be witnessed and signed in the Controlled Drug Register by 2 nurses i.e. morphine 10mg/1ml administer 0.5mls and discard 0.5mls
6 Please see separate guidelines for administration of :
- IV morphine injections - Patient-controlled analgesia (PCA) - Epidural analgesia
PATIENTS’ OWN CONTROLLED DRUGS
1. These remain the patients’ own property, and should preferably be given
back to the patient or relatives acting on the patient’s behalf at discharge. 2. They should be locked in the Controlled Drugs cupboard, and an entry made
in the Patient’s Own Controlled Drugs Book.
Version 2.0 POLICY MEDICINES POLICY Page 100 of 130
Date June 2016 Next Review Date June 2019
3. This entry should include the patient’s name and the quantity and type of drugs, (tablets, ampoules, etc.) and be witnessed by another nurse.
4. The administration of patient’s own Controlled Drugs to the patient they belong to is recorded in the Patient’s Own Controlled Drugs Book.
5. Same procedure for administration and record keeping as in Section 9 applies.
6. Patient’s own Controlled Drugs should be returned to the patient or relatives acting on patient’s behalf at discharge if still required.
7. If the dose has changed or the medicine has been stopped, and the patient insists on the medicine to be returned to them, a single line must be drawn through the label and the pack annotated with “stopped – do not use”. The ward pharmacist is available for advice. Document in patients collaborative notes if they have insisted that their medicines be returned against advice.
8. When the drugs are released to the patient or a relative acting on patient’s behalf, the entry signing out the drugs should be countersigned by the patient or the relative.
9. General rules about discharge medication also apply. TEMPORARY WARD CLOSURE If there are short term or long term ward closures the following procedure to ensure the security of controlled drugs must be followed:
1. Arrangements should be made for the removal and temporary storage of CDs by pharmacy if necessary
2. Arrangements should be made for return of CDs to pharmacy for re-use, if appropriate
3. Information on returned CDs recorded in the Ward Controlled Drugs Register and Pharmacy Controlled Drug Register
4. Arrangements for secure storage of current CD stationery during closure TRANSFER OF WARDS When a ward moves to another location, a decision must be made as to whether its CDs and CD registers may be transferred or, where swapping of wards occurs, left on the ward. This will depend on the periods for which ward premises will be unoccupied and the security of the drugs during this time.
1. Controlled Drugs should be removed from the Controlled Drug cupboard by the Ward Manager and a Registered Nurse and placed in a controlled drug red bag.
2. The Controlled Drug Register should also be removed. 3. The removed controlled drugs should then be transferred to the designated
ward and placed in the Controlled Drug Cupboard. 4. A stock check should be undertaken. 5. Stock check should involve checking of the balance in the Controlled Drugs
Register against the contents of the Controlled Drugs Cupboard to ensure all balances are checked.

Version 2.0 POLICY MEDICINES POLICY Page 101 of 130
Date June 2016 Next Review Date June 2019
6. The pharmacist or pharmacy technician should ensure that the ward signatory lists are updated to reflect the new ward location/name.
OPENING OF A NEW WARD
1. When a new ward opens pharmacy should be informed 2. A Controlled Drug Order Book and Register should be ordered via Pharmacy 3. Any required stock Controlled Drugs should be ordered via Pharmacy as
above 4. This should be received, stored and entered in the Controlled Drug register
as above ILLICIT SUBSTANCES
1. See Section 9. 2. Illicit (or suspect) substances must never be returned to the patient or
relatives.(This would contravene the Misuse of Drugs Regulations and could constitute Supply of a Controlled Substance for which a custodial sentence is possible).
3. Security must be informed and a decision on police involvement made by the senior nurse and medical practitioner.
RETURN AND DESTRUCTION OF CONTROLLED DRUGS
Unwanted Controlled Drugs must be returned to Pharmacy via the ward pharmacist. Theatres, OPD or any other area not covered by the ward pharmacy service must ring Pharmacy for advice. Records of CDs returned The ward or department should keep a record of drugs returned to pharmacy in the form of a returns advice note with duplicate pages so that both the pharmacy and the ward have a record of the transaction. The Ward Pharmacist or the Ward Technician using the appropriate documentation can return CDs to Pharmacy.
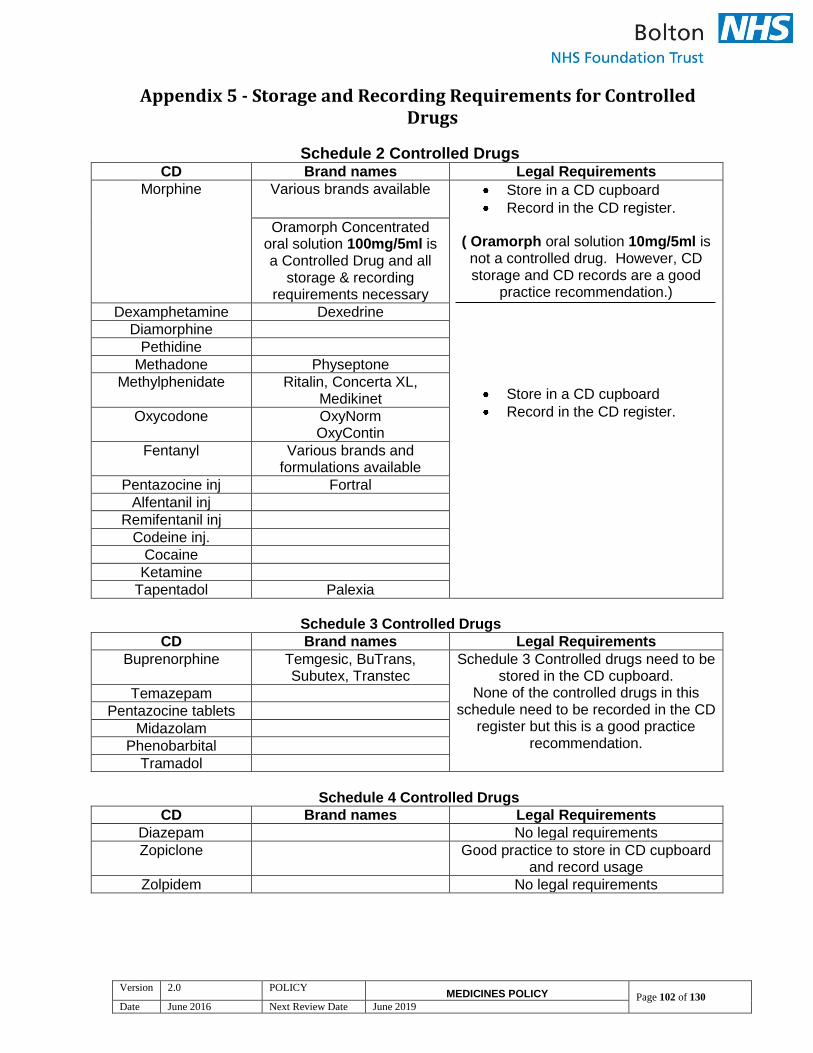
Version 2.0 POLICY MEDICINES POLICY Page 102 of 130
Date June 2016 Next Review Date June 2019
Appendix 5 - Storage and Recording Requirements for Controlled Drugs
Schedule 2 Controlled Drugs CD Brand names Legal Requirements
Morphine Various brands available
Store in a CD cupboard
Record in the CD register.
( Oramorph oral solution 10mg/5ml is not a controlled drug. However, CD storage and CD records are a good
practice recommendation.)
Store in a CD cupboard
Record in the CD register.
Oramorph Concentrated oral solution 100mg/5ml is a Controlled Drug and all
storage & recording requirements necessary
Dexamphetamine Dexedrine
Diamorphine
Pethidine
Methadone Physeptone
Methylphenidate Ritalin, Concerta XL, Medikinet
Oxycodone
OxyNorm OxyContin
Fentanyl Various brands and formulations available
Pentazocine inj Fortral
Alfentanil inj
Remifentanil inj
Codeine inj.
Cocaine
Ketamine
Tapentadol Palexia
Schedule 3 Controlled Drugs
CD Brand names Legal Requirements
Buprenorphine Temgesic, BuTrans, Subutex, Transtec
Schedule 3 Controlled drugs need to be stored in the CD cupboard.
None of the controlled drugs in this schedule need to be recorded in the CD
register but this is a good practice recommendation.
Temazepam
Pentazocine tablets
Midazolam
Phenobarbital
Tramadol
Schedule 4 Controlled Drugs
CD Brand names Legal Requirements
Diazepam No legal requirements
Zopiclone Good practice to store in CD cupboard and record usage
Zolpidem No legal requirements

Version 2.0 POLICY MEDICINES POLICY Page 103 of 130
Date June 2016 Next Review Date June 2019
Appendix 6 - Protocol for the Use of Controlled Drug Denaturing Kits in Community Services
Prescribed drugs, including CDs, are the property of the patient and remain so even after death. However, it is illegal for a person to possess CDs that have not been prescribed for them. In the first instance, the patient/patient’s relatives should be advised that CDs no longer required should be returned by them to a community pharmacy for safe destruction. Community nurses should not normally transport CDs to the community pharmacy. This should only be undertaken in circumstances where there is no other reasonable means available. If return by relatives is not possible or appropriate, the following action should be taken:
Nurse with another member of the nursing team, acting as a witness, destroys the CD using a de-naturing kit.
This should be within the agreed local Standard Operating Procedure and should include appropriate documentation in the patient nursing record.
If it is not possible for the nurse to destroy the CD in the patient’s home, the following action should be taken:
Nurse takes CDs to local community pharmacy, who would be asked to counter-sign patient nursing record.
Injectable controlled drugs that have been dispensed for a particular patient and which have been monitored and recorded by Community Services nursing staff will be destroyed in the patient’s home when they are no longer required. The drugs will be denatured using supplied kits and by the following procedure.
1. If appropriate, drugs will need to be diluted, if not in liquid form.
2. The liquid drug will be deposited in the denaturing kit, which contains an absorbent material. The instructions on the individual kit should be followed.
3. Any glass ampoule/ other material will be disposed of in the usual manner. I.e. sharps receptacle.
4. For patients of the District Nursing Service the used denaturing kit will be exchanged for an unused kit. These Kits are stored at Blackrod and Waters Meeting Health Centres. Used denaturing kits MUST be hand delivered and

Version 2.0 POLICY MEDICINES POLICY Page 104 of 130
Date June 2016 Next Review Date June 2019
exchanged on the next working day. If this is not possible then the used kit will be kept in a locked cupboard until exchange is possible. Other services are required to make suitable systems for collection and distribution of denaturing kits.
5. Monthly collections will be made from Waters Meeting and Blackrod health centres for used denaturing kits. The used kits will be kept in a container supplied by the waste collection company in a locked storage room.
6. When a CD is destroyed, details of the destruction must be recorded in the CD register.
This should include:
the name of the drug form
strength quantity
date it was destroyed the signature of the person who witnessed the destruction the signature of the professional destroying the CD
Community Nurses are not responsible for the disposal or destruction of CD’s in Care Homes. Please note:
The instructions with the kit indicate that the ampoules should be crushed prior to disposing of them. However, it may be appropriate to dispose of them into a sharps receptacle (as indicated above) as this is a safer and more practicable action.
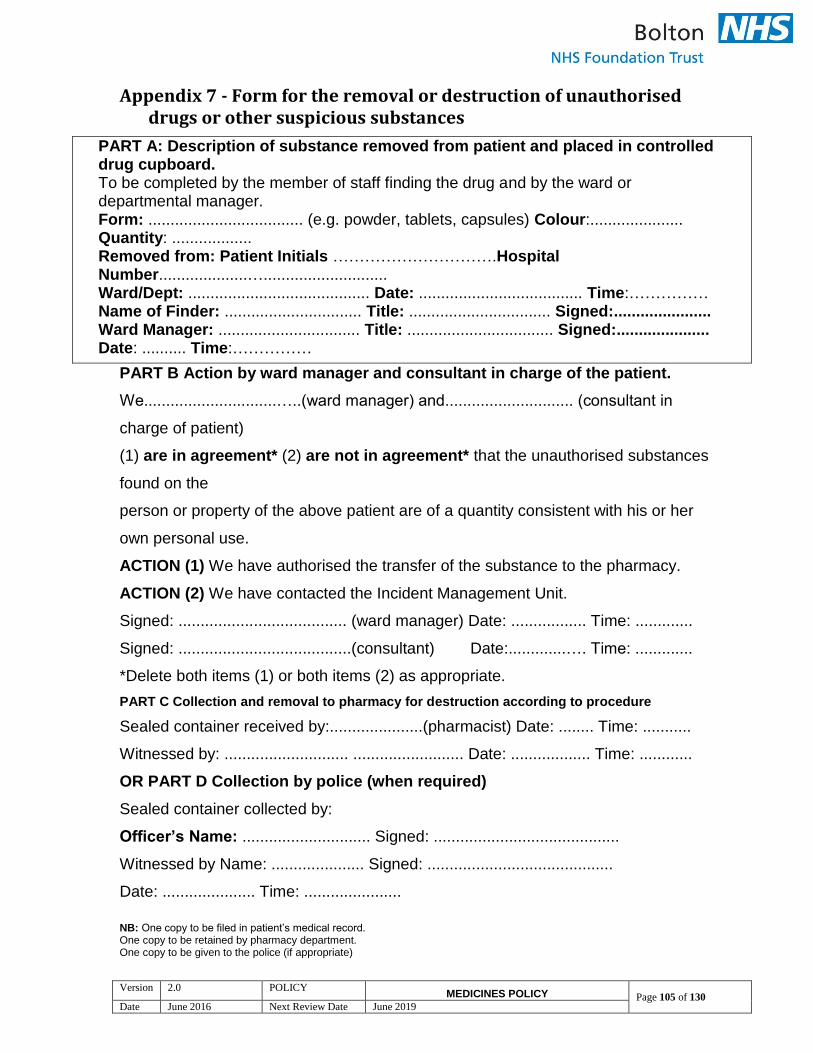
Version 2.0 POLICY MEDICINES POLICY Page 105 of 130
Date June 2016 Next Review Date June 2019
Appendix 7 - Form for the removal or destruction of unauthorised drugs or other suspicious substances
PART A: Description of substance removed from patient and placed in controlled drug cupboard. To be completed by the member of staff finding the drug and by the ward or departmental manager. Form: ................................... (e.g. powder, tablets, capsules) Colour:..................... Quantity: .................. Removed from: Patient Initials ………………………….Hospital Number....................…............................ Ward/Dept: ......................................... Date: ..................................... Time:…………… Name of Finder: ............................... Title: ................................ Signed:...................... Ward Manager: ................................ Title: ................................. Signed:..................... Date: .......... Time:……………
PART B Action by ward manager and consultant in charge of the patient.
We..............................…..(ward manager) and............................. (consultant in
charge of patient)
(1) are in agreement* (2) are not in agreement* that the unauthorised substances
found on the
person or property of the above patient are of a quantity consistent with his or her
own personal use.
ACTION (1) We have authorised the transfer of the substance to the pharmacy.
ACTION (2) We have contacted the Incident Management Unit.
Signed: ...................................... (ward manager) Date: ................. Time: .............
Signed: .......................................(consultant) Date:.............…. Time: .............
*Delete both items (1) or both items (2) as appropriate.
PART C Collection and removal to pharmacy for destruction according to procedure
Sealed container received by:.....................(pharmacist) Date: ........ Time: ...........
Witnessed by: ............................ ......................... Date: .................. Time: ............
OR PART D Collection by police (when required)
Sealed container collected by:
Officer’s Name: ............................. Signed: ..........................................
Witnessed by Name: ..................... Signed: ..........................................
Date: ..................... Time: ......................
NB: One copy to be filed in patient’s medical record. One copy to be retained by pharmacy department. One copy to be given to the police (if appropriate)
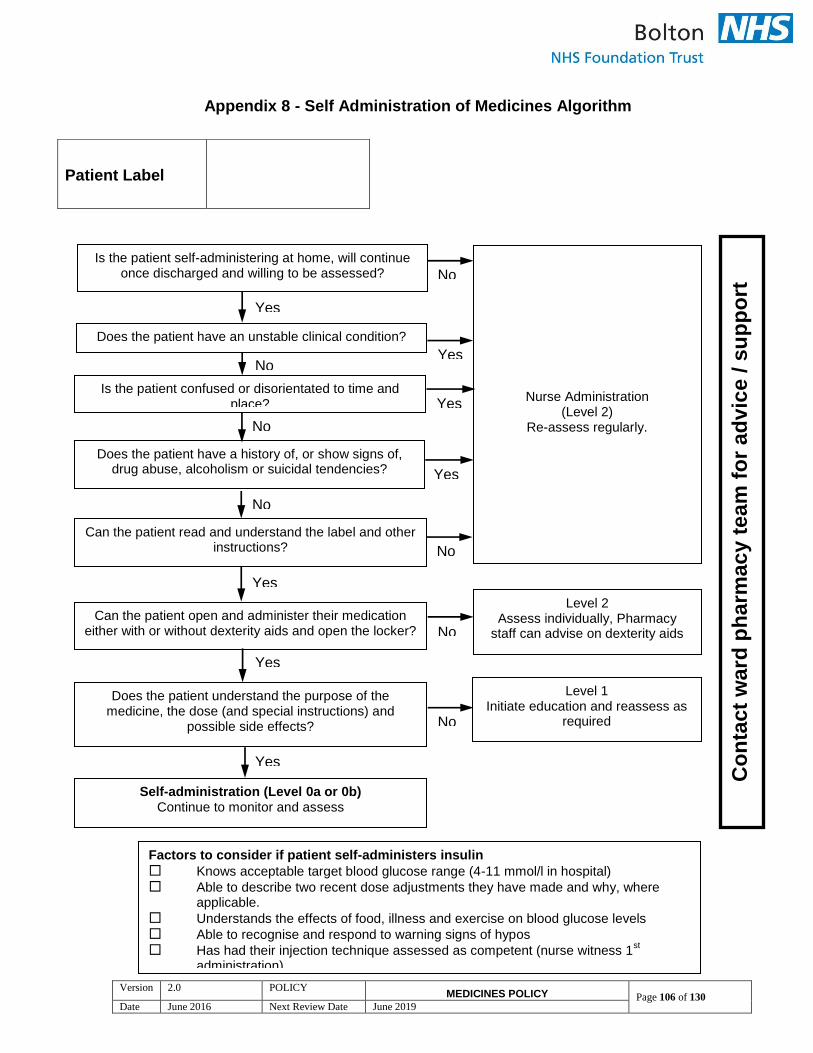
Version 2.0 POLICY MEDICINES POLICY Page 106 of 130
Date June 2016 Next Review Date June 2019
Appendix 8 - Self Administration of Medicines Algorithm
Patient Label
Nurse Administration (Level 2)
Re-assess regularly.
Does the patient have an unstable clinical condition?
Is the patient confused or disorientated to time and place?
Is the patient self-administering at home, will continue once discharged and willing to be assessed?
Does the patient have a history of, or show signs of, drug abuse, alcoholism or suicidal tendencies?
Can the patient read and understand the label and other instructions?
Level 2 Assess individually, Pharmacy
staff can advise on dexterity aids
Can the patient open and administer their medication either with or without dexterity aids and open the locker?
Does the patient understand the purpose of the medicine, the dose (and special instructions) and
possible side effects?
Self-administration (Level 0a or 0b) Continue to monitor and assess
Level 1 Initiate education and reassess as
required
Co
nta
ct
ward
ph
arm
ac
y t
ea
m f
or
ad
vic
e / s
up
po
rt
Factors to consider if patient self-administers insulin
Knows acceptable target blood glucose range (4-11 mmol/l in hospital)
Able to describe two recent dose adjustments they have made and why, where applicable.
Understands the effects of food, illness and exercise on blood glucose levels
Able to recognise and respond to warning signs of hypos
Has had their injection technique assessed as competent (nurse witness 1st
administration)
Yes
No
Yes No
No
Yes
Yes
No
Yes
No
Yes
No
Yes
No
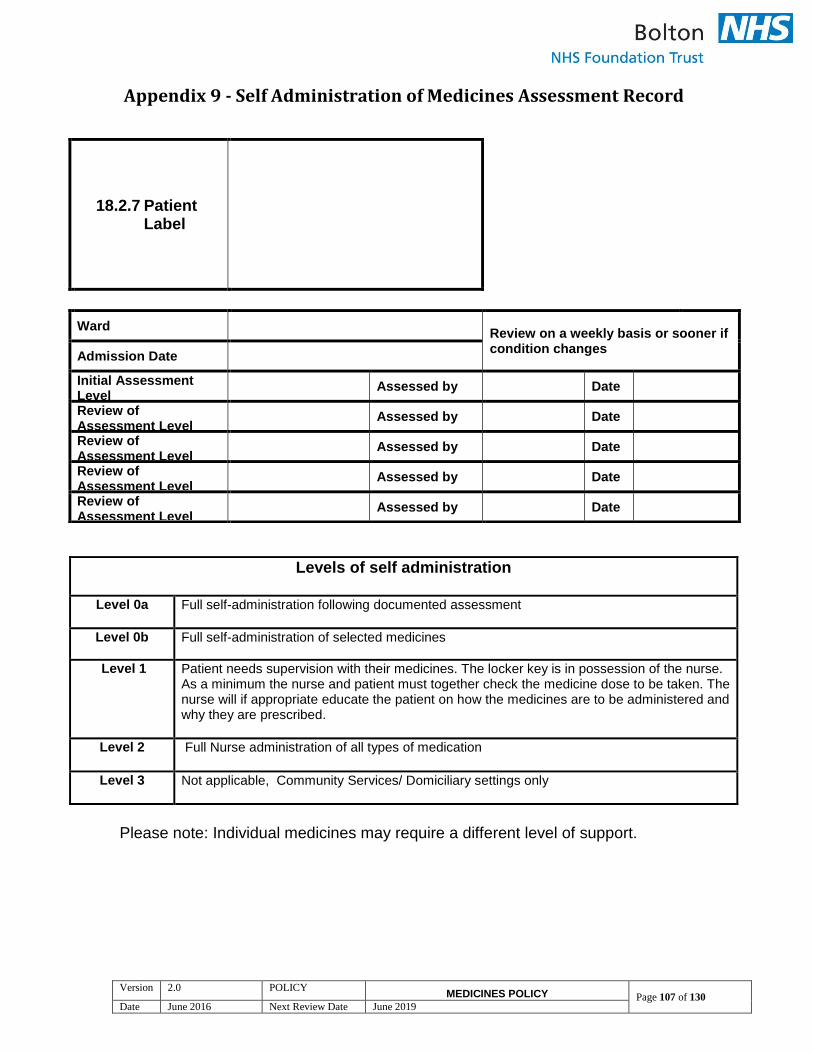
Version 2.0 POLICY MEDICINES POLICY Page 107 of 130
Date June 2016 Next Review Date June 2019
Appendix 9 - Self Administration of Medicines Assessment Record
Please note: Individual medicines may require a different level of support.
18.2.7 Patient Label
Ward Review on a weekly basis or sooner if
condition changes Admission Date
Initial Assessment Level
Assessed by Date
Review of Assessment Level
Assessed by Date
Review of Assessment Level
Assessed by Date
Review of Assessment Level
Assessed by Date
Review of Assessment Level
Assessed by Date
Levels of self administration
Level 0a
Full self-administration following documented assessment
Level 0b Full self-administration of selected medicines
Level 1 Patient needs supervision with their medicines. The locker key is in possession of the nurse. As a minimum the nurse and patient must together check the medicine dose to be taken. The nurse will if appropriate educate the patient on how the medicines are to be administered and why they are prescribed.
Level 2 Full Nurse administration of all types of medication
Level 3
Not applicable, Community Services/ Domiciliary settings only

Version 2.0 POLICY MEDICINES POLICY Page 108 of 130
Date June 2016 Next Review Date June 2019
Appendix 10 - Self Administration Consent Form Name of patient ……………………………………………………………………. Address ……….……………………………………………………………………….. ………………………………………………………………………………… Date of birth……………………………………………………………………………. I agree to be responsible for my medicines, as detailed below, whilst in hospital. Medicines for self-administration include: …………………………………………………………………………………………… …………………………………………………………………………………………… ………………………………………………………………………………………….. A nurse or pharmacist has explained what my medicines are for and any other important information. I will:
Ensure my medicines are either on my person or locked up securely in the locker provided. I will not leave them unattended on my locker or bedside table
Tell the nurse looking after me when I have taken my medicines
Ask the nurses or pharmacy staff if I am unsure about anything
Only takes medicines that are prescribed for me
Tell the nurse or pharmacy staff if I am running out of a medicine. I understand that I can change my mind at any time and ask the nurses to resume administering my medicines to me. Signature of patient…………………………………………………… To be completed by the assessor: Signature of assessor…………………………….……… Name of assessor…………………………………………… Date of assessment …………………………………
Version 2.0 POLICY MEDICINES POLICY Page 109 of 130
Date June 2016 Next Review Date June 2019
Appendix 11 - Information for Patients about Self Administration of
their Medicines
What is Self-Administration of Medicines? This is a scheme that allows you to take your own medicines whilst in hospital, giving you greater independence and control in taking your medicines. Why use this system? When you look after your own medicines you become more familiar and confident with your medicines, and understand more about your own health. Who can I talk to about Self Administration? Before taking part and looking after your own medicines, you can discuss this with your nurse or the pharmacy staff who visit the ward every day. They can answer any questions you may have about your medicines and self-administration. Do I have to Self-Administer? No – this is your choice, and you do not have to take part if you do not wish to. What will happen if I want to look after my medicines? If you wish to take part, a nurse or pharmacist will assess your suitability. They will ask for your agreement by getting you to sign a consent form. A nurse or pharmacist will explain self-administration and go through your medicines with you, explaining the dose, any side effects and any other important information. You will use your own medicines from home once they have been assessed as still suitable. We will supply any other medicines you need. To make this work, you will need to:
Ensure my medicines are either on your person or locked up securely in the locker provided. Do not leave them unattended on the locker or bedside table
Inform the nurse looking after you when you have taken your medicines Ask the nurses or pharmacy staff if you are unsure about anything. Only take medicines prescribed for you Tell the nurse or pharmacy staff if you are running out of a medicine.
Keeping your medicines safe If anyone tries to take your medicines or open your locker please tell a member of staff immediately. The only people who should look in your locker are you, the nurses or the pharmacy staff. We understand that you may wish to keep such things as your inhalers or GTN spray on your person, rather than in a locked cupboard, if you do so, please do not leave them unattended on your locker or bedside table. Let the nurse know what items you are keeping on you. What will happen when I go home?

Version 2.0 POLICY MEDICINES POLICY Page 110 of 130
Date June 2016 Next Review Date June 2019
A prescription will be written with the medicines you need to take home. This prescription will be checked against the medicines in your locker. These medicines will be given back to you if they are still okay to use. If more medicines are needed or your medicines need to be changed, the pharmacy staff will look after this. Please remember to return your locker key to the nurses before you leave the ward, if you’ve been given one.
If you need this leaflet in other languages or larger print then please ask a member of staff.
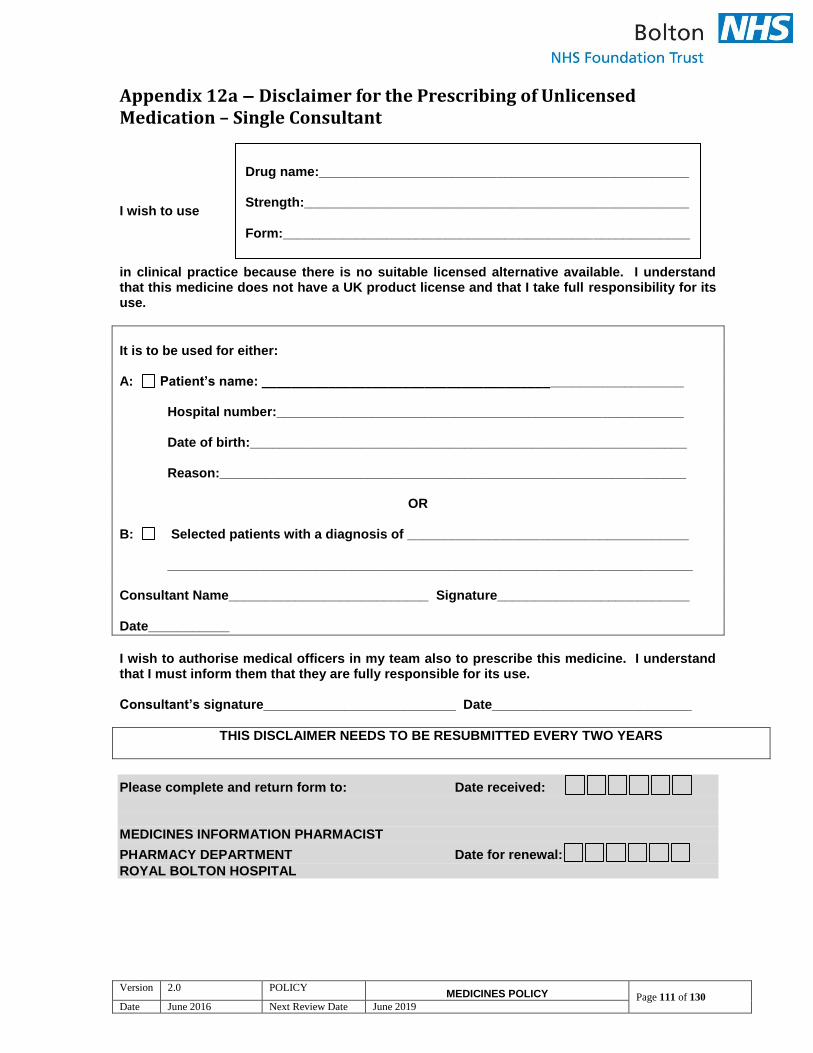
Version 2.0 POLICY MEDICINES POLICY Page 111 of 130
Date June 2016 Next Review Date June 2019
Appendix 12a – Disclaimer for the Prescribing of Unlicensed Medication – Single Consultant
I wish to use in clinical practice because there is no suitable licensed alternative available. I understand that this medicine does not have a UK product license and that I take full responsibility for its use.
It is to be used for either: A: Patient’s name: _________________________________________________________ Hospital number:_______________________________________________________ Date of birth:___________________________________________________________ Reason:_______________________________________________________________
OR B: Selected patients with a diagnosis of ______________________________________ _______________________________________________________________________ Consultant Name___________________________ Signature__________________________ Date___________
I wish to authorise medical officers in my team also to prescribe this medicine. I understand that I must inform them that they are fully responsible for its use. Consultant’s signature__________________________ Date___________________________
THIS DISCLAIMER NEEDS TO BE RESUBMITTED EVERY TWO YEARS
Please complete and return form to: Date received:
MEDICINES INFORMATION PHARMACIST
PHARMACY DEPARTMENT Date for renewal:
ROYAL BOLTON HOSPITAL
Drug name:__________________________________________________ Strength:____________________________________________________
Form:_______________________________________________________

Version 2.0 POLICY MEDICINES POLICY Page 112 of 130
Date June 2016 Next Review Date June 2019
Appendix 12b – Disclaimer for the Prescribing of Unlicensed Medication – Multiple Consultants
I wish to use in clinical practice because there is no suitable licensed alternative available. I understand that this medicine does not have a UK product license and that I take full responsibility for its use.
It is to be used for either: A: Patient’s name: __________________________________________________ Hospital number: ___________________________________________________ Date of birth: ___________________________________________________ Reason: ___________________________________________________
OR B: Selected patients with a diagnosis of ______________________________________ _______________________________________________________________________ Consultant Name___________________ Signature__________________ Date___________ Consultant Name___________________ Signature__________________ Date___________ Consultant Name___________________ Signature__________________ Date___________ Consultant Name___________________ Signature__________________ Date___________
I wish to authorise medical officers in my team also to prescribe this medicine. I understand that I must inform them that they are fully responsible for its use. Consultant’s signature_________________________________ Date____________________ Consultant’s signature_________________________________ Date____________________ Consultant’s signature_________________________________ Date____________________ Consultant’s signature_________________________________ Date____________________
THIS DISCLAIMER NEEDS TO BE RESUBMITTED EVERY TWO YEARS
Please complete and return form to: Date received:
MEDICINES INFORMATION PHARMACIST PHARMACY DEPARTMENT
ROYAL BOLTON HOSPITAL Date for renewal:
Drug name: ____________________________________ Strength:_______________________________________________
Form:_______________________________________________

Version 2.0 POLICY MEDICINES POLICY Page 113 of 130
Date June 2016 Next Review Date June 2019
Appendix 13 – List of Unlicensed Medicines that do not require a disclaimer
Internal liquids
Chlorothiazide 250mg/5ml
Caffeine citrate 50mg/5ml
Joulies Phosphate solution 1mmol/ml
Sodium chloride 25mmol/5ml
Spironolactone 50mg/5ml
Sodium bicarbonate 8.4% solution
Tablets and capsules
Magnesium Glycerophosphate 4mmol tablets
Midodrine 5mg tablets
Injections and infusions
Bupivacaine 0.1% and fentanyl 5% epidural 250ml
Morphine 50mg in 50ml syringes
Potassium chloride 10mmol in glucose 10% 500ml
Potassium chloride 10mmol in glucose 5% /sodium chloride 0.45% 500ml
Potassium chloride 10mmol in glucose 5% /sodium chloride 0.9% 500ml
Potassium chloride 10mmol in glucose 10% /sodium chloride 0.18% 500ml
Potassium chloride 20mmol in glucose 10% 500ml
Potassium chloride 20mmol in glucose 5% /sodium chloride 0.45% 500ml
Potassium chloride 20mmol in glucose 10% /sodium chloride 0.45% 500ml
Potassium chloride 20mmol in glucose 10% /sodium chloride 0.9% 500ml
Potassium chloride 40mmol in glucose 5% 500ml
Potassium chloride 40mmol in sodium chloride 0.9% 100ml
Potassium chloride 40mmol in sodium chloride 0.9% 500ml
Sodium bicarbonate 4.2% 1ml and 5ml ampoule
Externals
Adrenaline 1 in 1000, 30ml solution
Cocaine plain solution 10%
Cocaine 5% with adrenaline 1 in 2000 solution
Cocaine 10% with adrenaline 1 in 2000 solution
Iodine 2.8% solution 100ml
Liquid paraffin sterile - check theatre/DCU
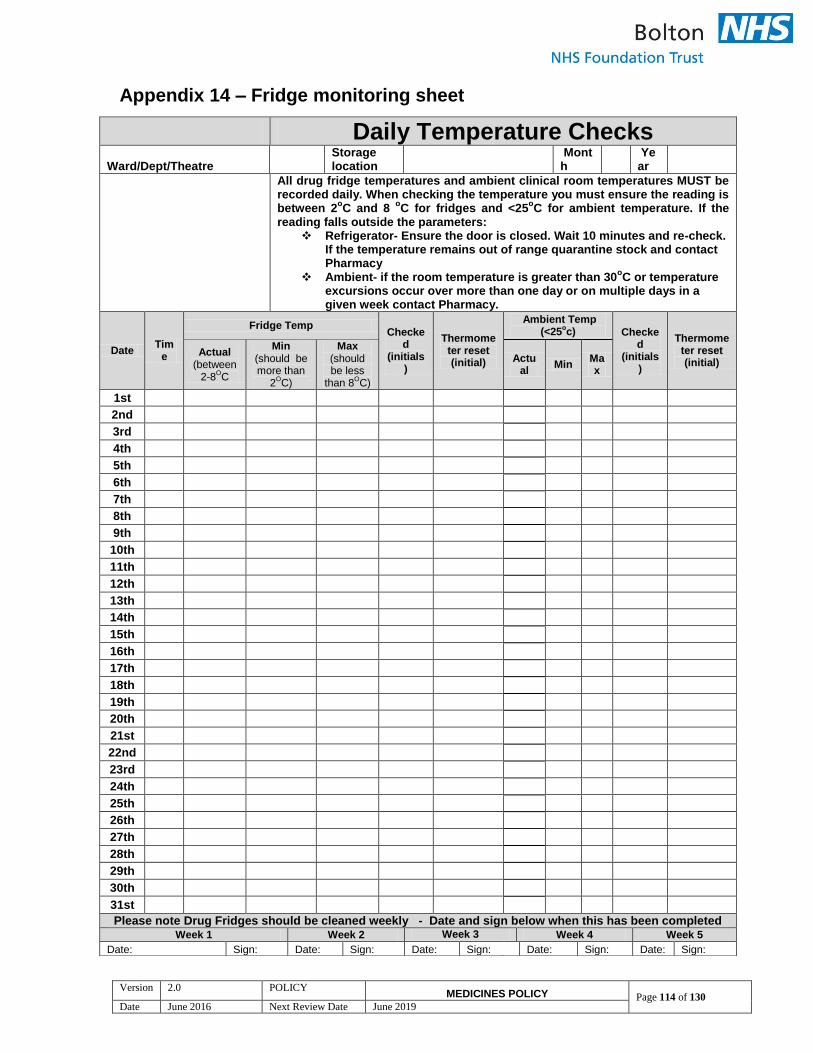
Version 2.0 POLICY MEDICINES POLICY Page 114 of 130
Date June 2016 Next Review Date June 2019
Appendix 14 – Fridge monitoring sheet
Daily Temperature Checks
Ward/Dept/Theatre Storage location
Month
Year
All drug fridge temperatures and ambient clinical room temperatures MUST be recorded daily. When checking the temperature you must ensure the reading is between 2
oC and 8
oC for fridges and <25
oC for ambient temperature. If the
reading falls outside the parameters: Refrigerator- Ensure the door is closed. Wait 10 minutes and re-check.
If the temperature remains out of range quarantine stock and contact Pharmacy
Ambient- if the room temperature is greater than 30oC or temperature
excursions occur over more than one day or on multiple days in a given week contact Pharmacy.
Date Tim
e
Fridge Temp Checke
d (initials
)
Thermometer reset (initial)
Ambient Temp (<25
oc) Checke
d (initials
)
Thermometer reset (initial)
Actual (between
2-8OC
Min (should be more than
2OC)
Max (should be less
than 8OC)
Actual
Min Max
1st
2nd
3rd
4th
5th
6th
7th
8th
9th
10th
11th
12th
13th
14th
15th
16th
17th
18th
19th
20th
21st
22nd
23rd
24th
25th
26th
27th
28th
29th
30th
31st
Please note Drug Fridges should be cleaned weekly - Date and sign below when this has been completed Week 1 Week 2 Week 3 Week 4 Week 5
Date: Sign: Date: Sign: Date: Sign: Date: Sign: Date: Sign:
Version 2.0 POLICY MEDICINES POLICY Page 115 of 130
Date June 2016 Next Review Date June 2019
Appendix 15 - Procedure for Obtaining Medicines Out of Hours Most medicines can be given plus or minus one to two hours from the time prescribed, with the exception of critical medicines i.e.
Resuscitation medicines including colloid or crystalloid intravenous fluids
Systemic anti-infectives
Anticoagulants or thrombolytics.
Anticonvulsants.
Parkinson’s disease medicines
Insulin or oral hypoglycaemics
Strong opioids
If ONE dose of any of the above is missed this MUST be reported as a clinical incident. The Procedure If a patient’s prescribed medication is not available and the pharmacy department is closed, the following action should be taken by the nursing staff: 1. Patient’s Own Medicine Check if the patient’s own medication is available. If it is not available, patient’s family or carers should be contacted with a request to bring the medication in. If it is available and is fit for use, administer the medication. 2. Emergency Drug Cupboard A list of drugs available in the Emergency Drug Cupboard is available on the Pharmacy homepage of the Trust Intranet and on the iBleep system.
If the drug is on the Emergency Drug Cupboard stock list, contact a member of the security staff (bleep 5553) to accompany a nurse to the emergency drug cupboard to collect it.
The nurse MUST carry an ID card, wardex and patient identification sticker with her/him. Any item removed from the Emergency Drug Cupboard must be recorded on the record sheet provided within the Cupboard. It’s the responsibility of the accompanying Security staff to ensure that this is done. The Emergency Drug Cupboard can only be accessed out of Pharmacy normal working hours.
3. Site Manager
Version 2.0 POLICY MEDICINES POLICY Page 116 of 130
Date June 2016 Next Review Date June 2019
If the drug is not on the emergency drug cupboard stock list, bleep the on-call Pharmacist via the switchboard, who will check the medicine stock location list to find out if the drug is available in another clinical area.
If it is available, the on-call pharmacist will authorise the named nurse to obtain the drug from the relevant ward. A Drugs Transferred between Wards slip MUST be completed and signed by both the nurse borrowing and the nurse handing over the drug. The on-call Pharmacist’s name must also be included. The nurse must take ID and the patient’s Wardex to collect the drug. 4. On-call Pharmacist The on-call Pharmacist will be called via switchboard if:
The drug is not stocked in the emergency cupboard, the Pharmacist will check if the drug is available on another ward.
There is no stock of the drug available anywhere in the hospital.

Version 2.0 POLICY MEDICINES POLICY Page 117 of 130
Date June 2016 Next Review Date June 2019
Appendix 16 Bolton NHS Foundation Trust - Pharmacy Department
IMPORTANT POINTS TO NOTE: - A doctor must in all circumstances label & check the medications. A nurse is not legally allowed to undertake this procedure. - Bottles, boxes & blank labels are available on some wards (D1, D2, F3, C1, C3, D3, D4 and M1) and in the Emergency Drug Cupboard. - Any medication which has been discontinued in hospital must not be returned to the patient.
PROCEDURE TO BE FOLLOWED FOR DISPENSING MEDICATION FOR URGENT DISCHARGE WHEN PHARMACY IS CLOSED
DISCHARGE PRESCRIPTION WRITTEN
(includes short-term leaves)
DOES PATIENT HAVE A SUPPLY OF MEDICATION?
(at home or in hospital)
YES NO
USE PATIENTS SUPPLY
(only if dose/directions are consistent with the
prescription)
SELECT MEDICATION FROM WARD* OR
EMERGENCY DRUG
CUPBOARD
DOCTOR TO DOCUMENT IN PATIENTS NOTES THAT
PATIENT HAS BEEN DISCHARGED WITH
MEDICATION OR HAS SUFFICIENT OWN SUPPLY
USE ORIGINAL MANUFACTURERS PACK (OR DISPENSE SUPPLIES
INTO BOTTLES/BOXES)
COMPLETE THE LABEL CLEARLY Do NOT use abbreviations, eg ‘1 od’ should be ‘take one daily’
(The label MUST include – drug name, form, strength, quantity supplied, full directions, patients name, date and any cautionary /
advisory labels as specified in Appendix 3 and individual drug entry in the BNF– this is a legal requirement) Doctor to sign the label
* If a pre-labelled pack is available
on the ward – then this must
be used first
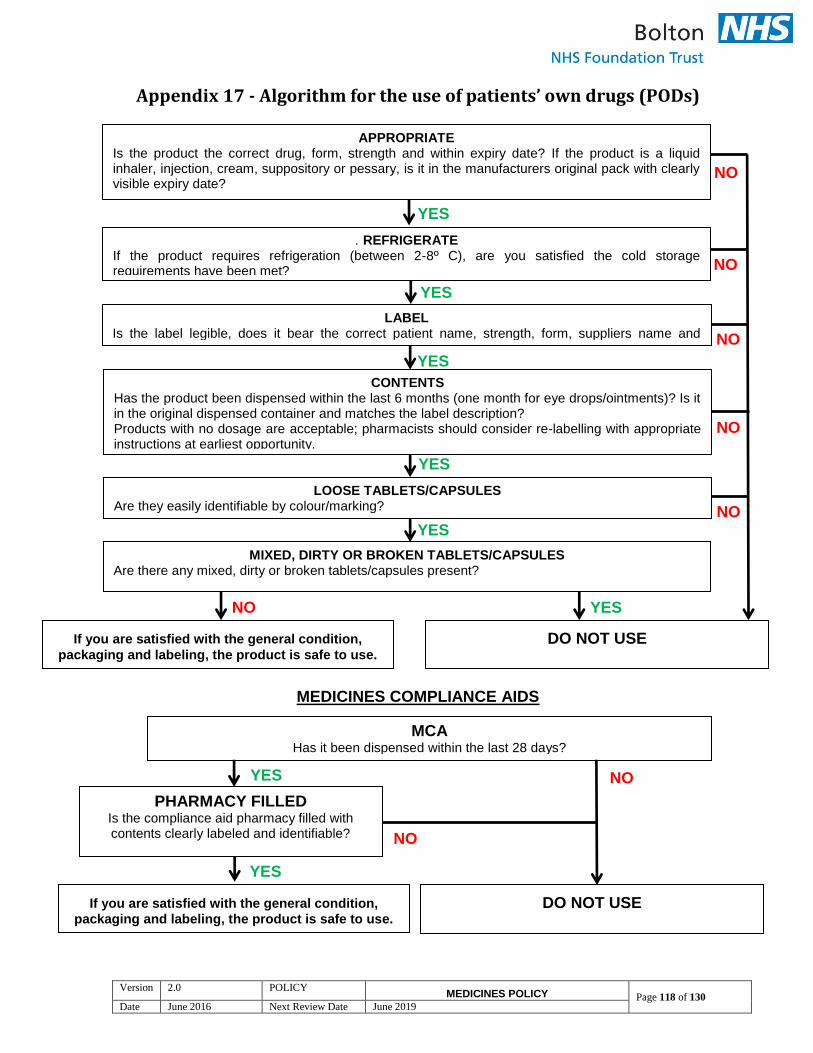
Version 2.0 POLICY MEDICINES POLICY Page 118 of 130
Date June 2016 Next Review Date June 2019
Appendix 17 - Algorithm for the use of patients’ own drugs (PODs)
MEDICINES COMPLIANCE AIDS
APPROPRIATE Is the product the correct drug, form, strength and within expiry date? If the product is a liquid inhaler, injection, cream, suppository or pessary, is it in the manufacturers original pack with clearly visible expiry date?
NO
YES
. REFRIGERATE If the product requires refrigeration (between 2-8º C), are you satisfied the cold storage requirements have been met?
YES
LABEL Is the label legible, does it bear the correct patient name, strength, form, suppliers name and address?
CONTENTS Has the product been dispensed within the last 6 months (one month for eye drops/ointments)? Is it in the original dispensed container and matches the label description? Products with no dosage are acceptable; pharmacists should consider re-labelling with appropriate instructions at earliest opportunity. Products with no dosage are acceptable; pharmacists should consider re-labelling with appropriate
LOOSE TABLETS/CAPSULES Are they easily identifiable by colour/marking?
MIXED, DIRTY OR BROKEN TABLETS/CAPSULES Are there any mixed, dirty or broken tablets/capsules present?
If you are satisfied with the general condition,
packaging and labeling, the product is safe to use. DO NOT USE
MCA Has it been dispensed within the last 28 days?
PHARMACY FILLED Is the compliance aid pharmacy filled with contents clearly labeled and identifiable?
YES
YES
NO
NO
NO
NO
NO YES
NO YES
YES
If you are satisfied with the general condition,
packaging and labeling, the product is safe to use. DO NOT USE
NO
YES

Version 2.0 POLICY MEDICINES POLICY Page 119 of 130
Date June 2016 Next Review Date June 2019
Appendix 18 - Protocol to remove discontinued and out of date medication from patients home
Medication should never be disposed of in domestic or commercial refuse, and disposal in the sewerage system is illegal. Staff must ensure the safe and secure transfer of medication from the patient’s home to the community pharmacy. Aim To reduce the volume of stored medication in a patient’s home and the risk of medication being taken inappropriately. Medicines are often returned to a community pharmacy for destruction. Any medication returned, is destroyed as the quality of the medicine can no longer be guaranteed. Healthcare professionals should be aware that professional guidance strongly recommends that medicines returned from patient stocks should not be re-issued or used to treat other patients When should medication be removed? Medication in the first instance should be returned to the pharmacy by a patient’s relative or friend where ever possible and should only be removed if leaving them poses a risk to the patient or other members of the family/carers/friends. If the patient has their regular medication delivered by their local community pharmacy, unwanted medication can be given to the driver to take back for destruction. In all cases the patient’s consent must be obtained. Medication disposal Medication should ideally be returned to the original dispensing pharmacy, however all pharmacies must accept medicines for disposal as documented in the essential services of the Pharmacy Contract. If the patient has significant quantities of medication for disposal then a referral to a pharmacist for a medication review should be considered. The pharmacist will liaise with the GP with regard to any changes deemed necessary. Medicines should never be transferred from the original pack into another container, and must not be re-labelled or the label altered. If a label has been defaced it should be referred to the originating pharmacy. Controlled drugs

Version 2.0 POLICY MEDICINES POLICY Page 120 of 130
Date June 2016 Next Review Date June 2019
Controlled drugs should be returned, ideally to the original dispensing pharmacy. The patients permission must be obtained using the ‘Removal of Discontinued and Out of Date Medication Form’ shown below. On taking controlled drugs to the community pharmacy the pharmacist may or may not document details of the return (it is not a legal requirement but it is good practice to do so) to enable safe destruction and maintaining records of drugs returned to the pharmacy. If the patient is having controlled drugs administered by Community Services nursing staff that are no longer required then the staff can destroy them using a Controlled Drug Destruction Kit following the guidelines in Appendix 1. Oxygen Oxygen is no longer supplied by the community pharmacists, if it needs to be removed then Air Products Healthcare should be contacted (telephone 0800 3890202). Sharps disposal Sharps (e.g. needles, lancets) will not be accepted by a community pharmacy for disposal. All sharps and syringes must be safely disposed of in Sharps receptacles in accordance with the FT Clinical Waste policy. Carriage of medicines Community Services staff may carry medicines for disposal that has been prescribed for named patients. The drugs may be transported out of sight in a locked car from the patient directly to the pharmacy. Removal of Discontinued and Out of Date Medication Complete the duplicate medication removal form (an example is shown below). An explanation to the patient as to why the medication is being removed should be given. Document the reasons for medication removal using the return codes listed on the form. If you have any concerns with regard to medication contact the community pharmacist, or the pharmacy team at Darley Court (tel. 337071) for advice.
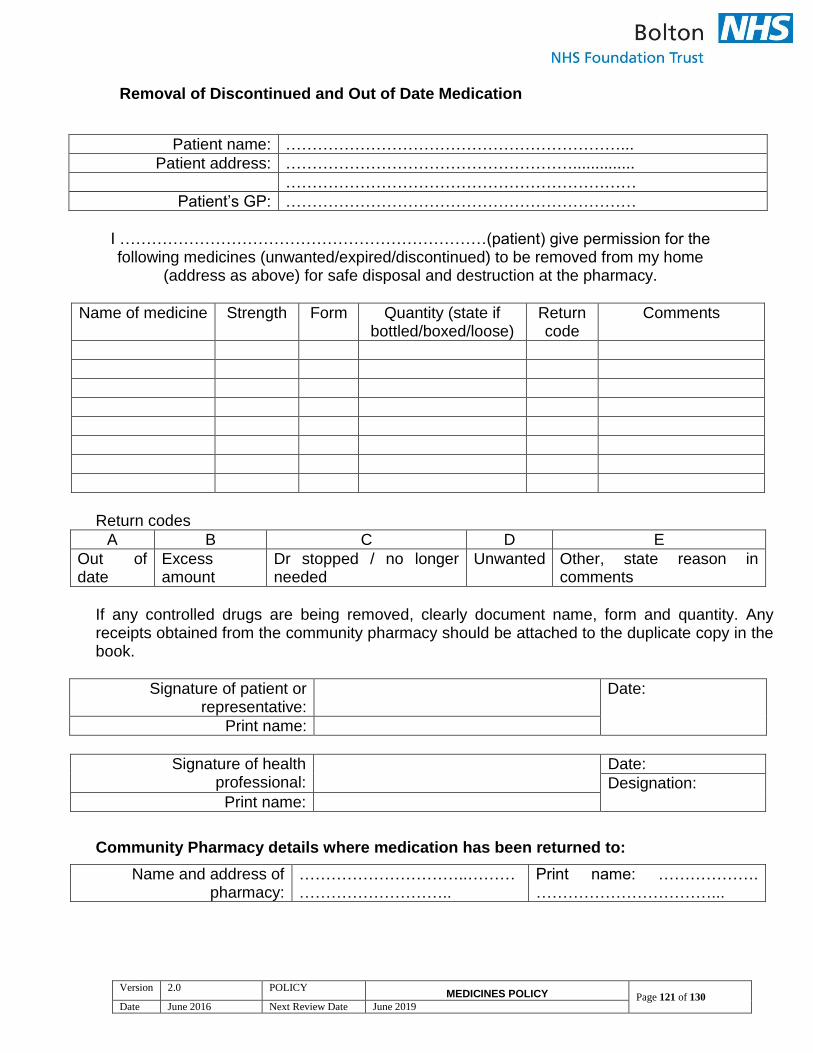
Version 2.0 POLICY MEDICINES POLICY Page 121 of 130
Date June 2016 Next Review Date June 2019
Removal of Discontinued and Out of Date Medication
Patient name: ………………………………………………………...
Patient address: ………………………………………………..............
…………………………………………………………
Patient’s GP: …………………………………………………………
I ……………………………………………………………(patient) give permission for the following medicines (unwanted/expired/discontinued) to be removed from my home
(address as above) for safe disposal and destruction at the pharmacy.
Name of medicine Strength Form Quantity (state if bottled/boxed/loose)
Return code
Comments
Return codes
A B C D E
Out of date
Excess amount
Dr stopped / no longer needed
Unwanted Other, state reason in comments
If any controlled drugs are being removed, clearly document name, form and quantity. Any receipts obtained from the community pharmacy should be attached to the duplicate copy in the book.
Signature of patient or representative:
Date:
Print name:
Signature of health professional:
Date:
Designation:
Print name:
Community Pharmacy details where medication has been returned to:
Name and address of pharmacy:
…………………………..………………………………..
Print name: ………………. ……………………………...
Version 2.0 POLICY MEDICINES POLICY Page 122 of 130
Date June 2016 Next Review Date June 2019
Pharmacy stamp / signature (patient copy and receipt
book to be stamped/signed)
Designation: ……………… ……………………………... Date: ……………………….
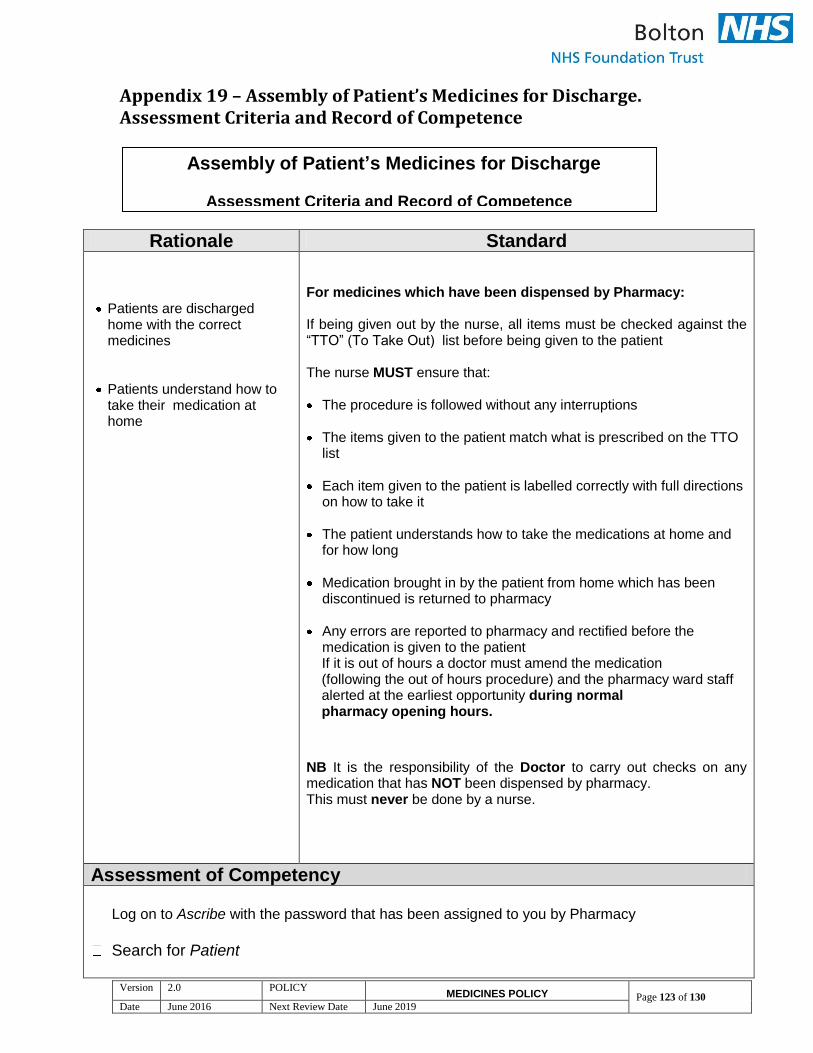
Version 2.0 POLICY MEDICINES POLICY Page 123 of 130
Date June 2016 Next Review Date June 2019
Appendix 19 – Assembly of Patient’s Medicines for Discharge. Assessment Criteria and Record of Competence
Rationale Standard
Patients are discharged home with the correct medicines
Patients understand how to take their medication at home
For medicines which have been dispensed by Pharmacy: If being given out by the nurse, all items must be checked against the “TTO” (To Take Out) list before being given to the patient The nurse MUST ensure that: The procedure is followed without any interruptions
The items given to the patient match what is prescribed on the TTO
list Each item given to the patient is labelled correctly with full directions
on how to take it The patient understands how to take the medications at home and
for how long
Medication brought in by the patient from home which has been discontinued is returned to pharmacy
Any errors are reported to pharmacy and rectified before the
medication is given to the patient If it is out of hours a doctor must amend the medication (following the out of hours procedure) and the pharmacy ward staff alerted at the earliest opportunity during normal pharmacy opening hours.
NB It is the responsibility of the Doctor to carry out checks on any medication that has NOT been dispensed by pharmacy. This must never be done by a nurse.
Assessment of Competency
Log on to Ascribe with the password that has been assigned to you by Pharmacy
Search for Patient
Assembly of Patient’s Medicines for Discharge
Assessment Criteria and Record of Competence
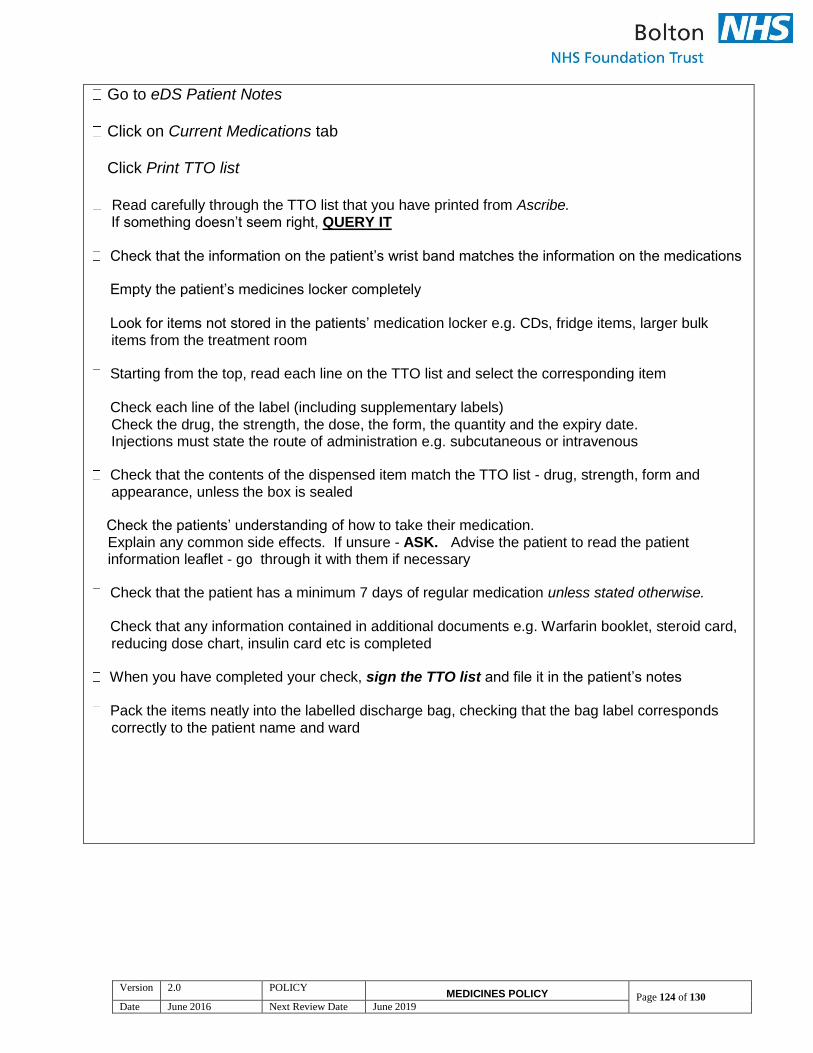
Version 2.0 POLICY MEDICINES POLICY Page 124 of 130
Date June 2016 Next Review Date June 2019
Go to eDS Patient Notes
Click on Current Medications tab
Click Print TTO list
Read carefully through the TTO list that you have printed from Ascribe. If something doesn’t seem right, QUERY IT
Check that the information on the patient’s wrist band matches the information on the medications
Empty the patient’s medicines locker completely
Look for items not stored in the patients’ medication locker e.g. CDs, fridge items, larger bulk
items from the treatment room
Starting from the top, read each line on the TTO list and select the corresponding item
Check each line of the label (including supplementary labels)
Check the drug, the strength, the dose, the form, the quantity and the expiry date. Injections must state the route of administration e.g. subcutaneous or intravenous
Check that the contents of the dispensed item match the TTO list - drug, strength, form and appearance, unless the box is sealed
Check the patients’ understanding of how to take their medication. Explain any common side effects. If unsure - ASK. Advise the patient to read the patient information leaflet - go through it with them if necessary
Check that the patient has a minimum 7 days of regular medication unless stated otherwise.
Check that any information contained in additional documents e.g. Warfarin booklet, steroid card,
reducing dose chart, insulin card etc is completed
When you have completed your check, sign the TTO list and file it in the patient’s notes
Pack the items neatly into the labelled discharge bag, checking that the bag label corresponds
correctly to the patient name and ward

Version 2.0 POLICY MEDICINES POLICY Page 125 of 130
Date June 2016 Next Review Date June 2019
Any medications which have been brought in from home and that have been discontinued by the
doctor should be returned to the hospital Pharmacy. However, if the patient insists on taking the discontinued medicines home, THE NURSE MUST STRIKE THROUGH THE LABEL AND WRITE “STOPPED” BEFORE GIVING THEM TO THE PATIENT. This must also be documented in the patient’s notes.
Ensure the patient receives their copy of the discharge summary at the point of discharge
Make sure that the medicines locker is empty and left open ready for cleaning prior to the next
patient
Declaration of Competency
Name of Nurse: Ward: Date Ascribe IT training completed Standards met: Yes No Comments/actions required:
Signature of assessor:
Designation: Date:
Please retain a copy of this form on the ward for auditing purposes.
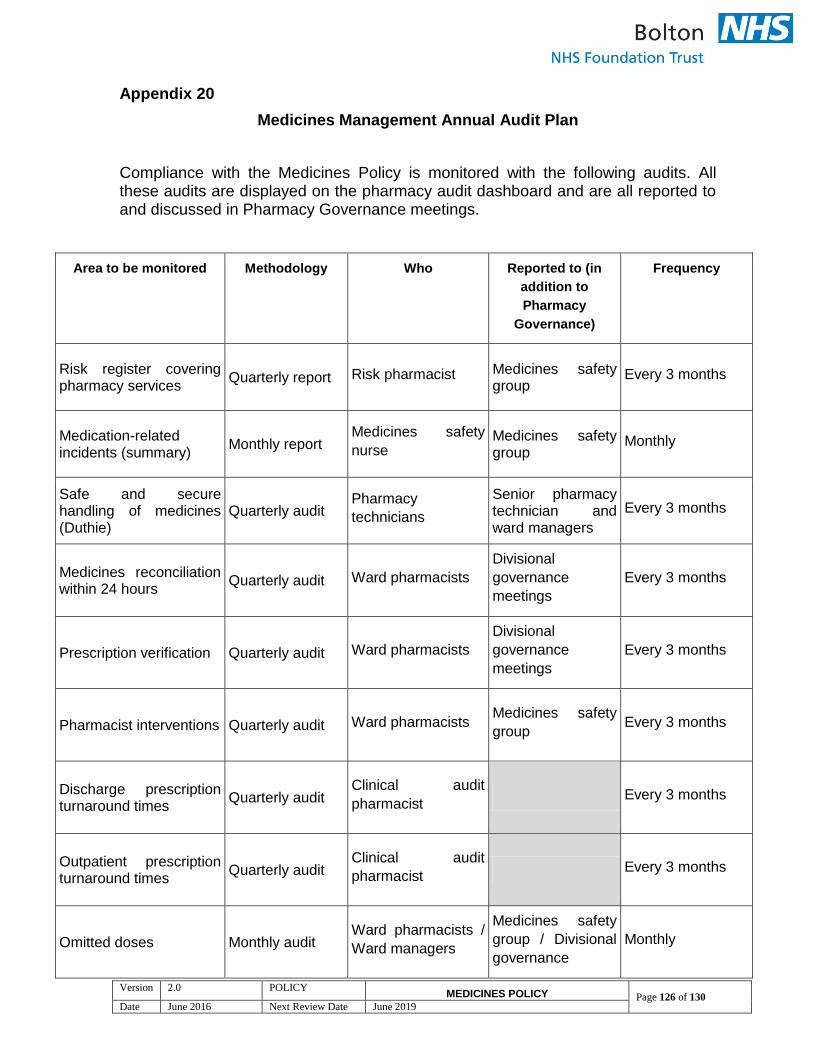
Version 2.0 POLICY MEDICINES POLICY Page 126 of 130
Date June 2016 Next Review Date June 2019
Appendix 20
Medicines Management Annual Audit Plan
Compliance with the Medicines Policy is monitored with the following audits. All these audits are displayed on the pharmacy audit dashboard and are all reported to and discussed in Pharmacy Governance meetings.
Area to be monitored Methodology Who Reported to (in
addition to
Pharmacy
Governance)
Frequency
Risk register covering pharmacy services
Quarterly report Risk pharmacist Medicines safety group
Every 3 months
Medication-related incidents (summary)
Monthly report Medicines safety
nurse Medicines safety group
Monthly
Safe and secure handling of medicines (Duthie)
Quarterly audit Pharmacy
technicians
Senior pharmacy technician and ward managers
Every 3 months
Medicines reconciliation within 24 hours
Quarterly audit Ward pharmacists
Divisional
governance
meetings
Every 3 months
Prescription verification Quarterly audit Ward pharmacists
Divisional
governance
meetings
Every 3 months
Pharmacist interventions Quarterly audit Ward pharmacists Medicines safety
group Every 3 months
Discharge prescription turnaround times
Quarterly audit Clinical audit
pharmacist Every 3 months
Outpatient prescription turnaround times
Quarterly audit Clinical audit
pharmacist Every 3 months
Omitted doses Monthly audit Ward pharmacists /
Ward managers
Medicines safety
group / Divisional
governance
Monthly
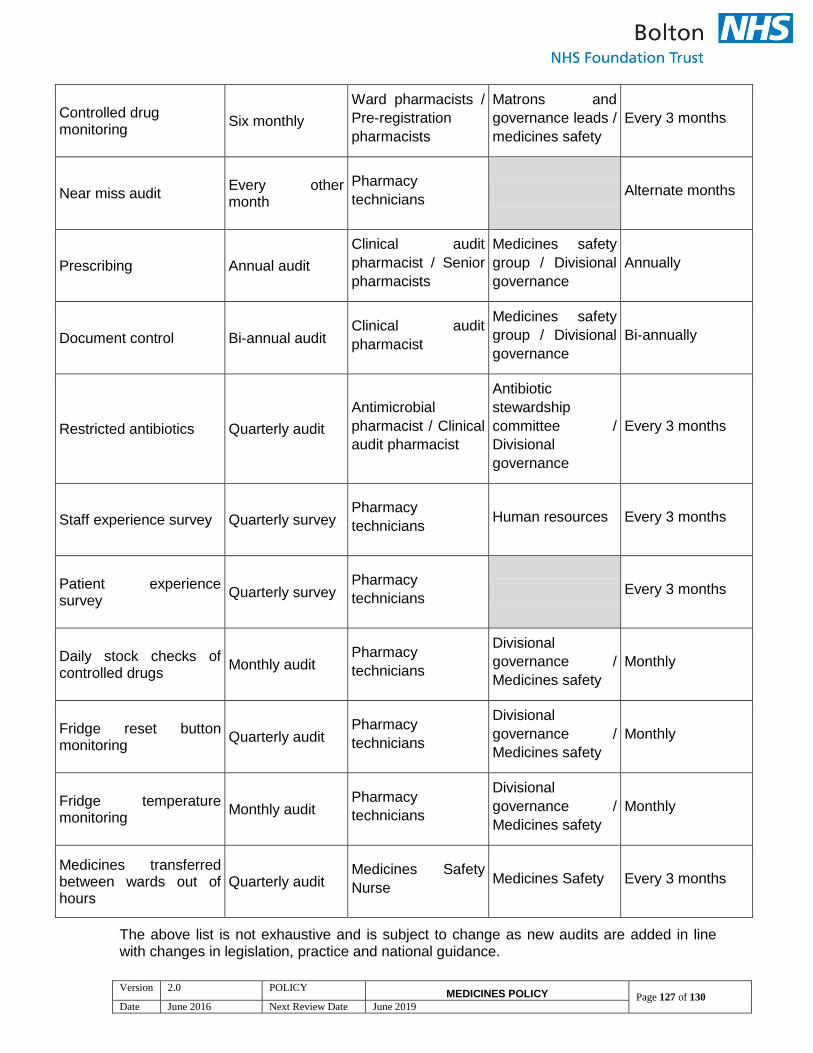
Version 2.0 POLICY MEDICINES POLICY Page 127 of 130
Date June 2016 Next Review Date June 2019
Controlled drug monitoring
Six monthly
Ward pharmacists /
Pre-registration
pharmacists
Matrons and
governance leads /
medicines safety
Every 3 months
Near miss audit Every other month
Pharmacy
technicians Alternate months
Prescribing Annual audit
Clinical audit
pharmacist / Senior
pharmacists
Medicines safety
group / Divisional
governance
Annually
Document control Bi-annual audit Clinical audit
pharmacist
Medicines safety
group / Divisional
governance
Bi-annually
Restricted antibiotics Quarterly audit
Antimicrobial
pharmacist / Clinical
audit pharmacist
Antibiotic
stewardship
committee /
Divisional
governance
Every 3 months
Staff experience survey Quarterly survey Pharmacy
technicians Human resources Every 3 months
Patient experience survey
Quarterly survey Pharmacy
technicians Every 3 months
Daily stock checks of controlled drugs
Monthly audit Pharmacy
technicians
Divisional
governance /
Medicines safety
Monthly
Fridge reset button monitoring
Quarterly audit Pharmacy
technicians
Divisional
governance /
Medicines safety
Monthly
Fridge temperature monitoring
Monthly audit Pharmacy
technicians
Divisional
governance /
Medicines safety
Monthly
Medicines transferred between wards out of hours
Quarterly audit Medicines Safety
Nurse Medicines Safety Every 3 months
The above list is not exhaustive and is subject to change as new audits are added in line with changes in legislation, practice and national guidance.
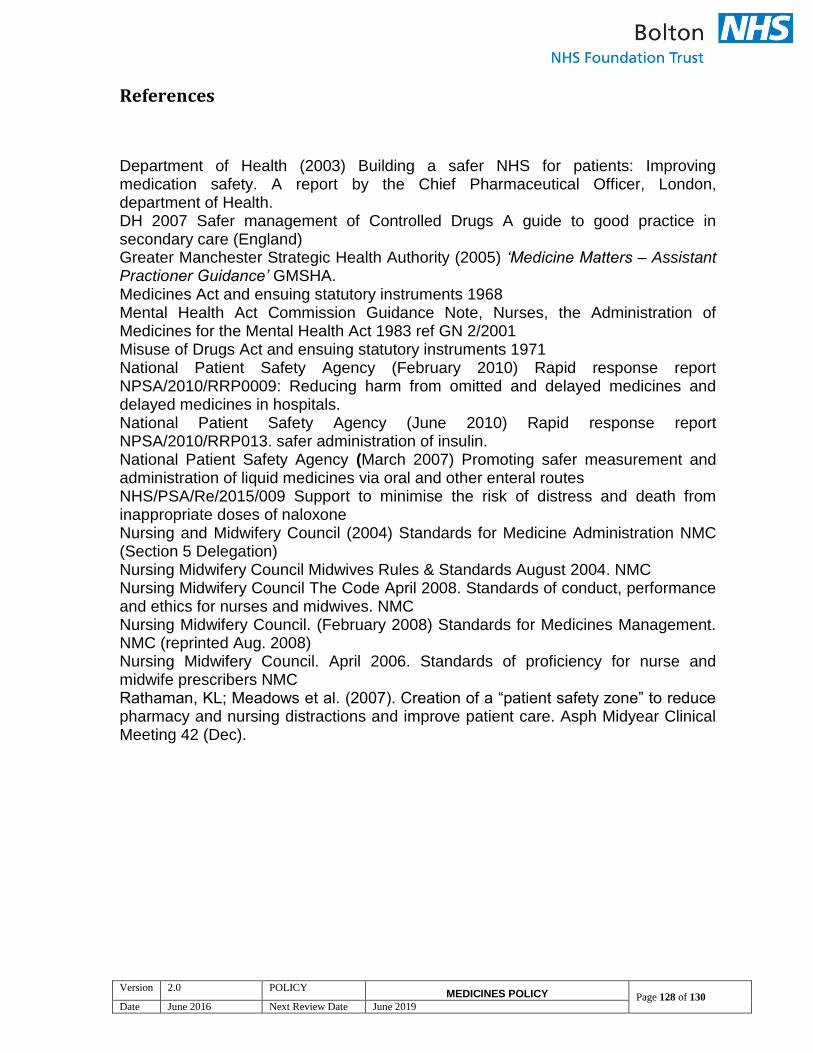
Version 2.0 POLICY MEDICINES POLICY Page 128 of 130
Date June 2016 Next Review Date June 2019
References
Department of Health (2003) Building a safer NHS for patients: Improving medication safety. A report by the Chief Pharmaceutical Officer, London, department of Health. DH 2007 Safer management of Controlled Drugs A guide to good practice in secondary care (England) Greater Manchester Strategic Health Authority (2005) ‘Medicine Matters – Assistant Practioner Guidance’ GMSHA. Medicines Act and ensuing statutory instruments 1968 Mental Health Act Commission Guidance Note, Nurses, the Administration of Medicines for the Mental Health Act 1983 ref GN 2/2001 Misuse of Drugs Act and ensuing statutory instruments 1971 National Patient Safety Agency (February 2010) Rapid response report NPSA/2010/RRP0009: Reducing harm from omitted and delayed medicines and delayed medicines in hospitals. National Patient Safety Agency (June 2010) Rapid response report NPSA/2010/RRP013. safer administration of insulin. National Patient Safety Agency (March 2007) Promoting safer measurement and administration of liquid medicines via oral and other enteral routes NHS/PSA/Re/2015/009 Support to minimise the risk of distress and death from inappropriate doses of naloxone Nursing and Midwifery Council (2004) Standards for Medicine Administration NMC (Section 5 Delegation) Nursing Midwifery Council Midwives Rules & Standards August 2004. NMC Nursing Midwifery Council The Code April 2008. Standards of conduct, performance and ethics for nurses and midwives. NMC Nursing Midwifery Council. (February 2008) Standards for Medicines Management. NMC (reprinted Aug. 2008) Nursing Midwifery Council. April 2006. Standards of proficiency for nurse and midwife prescribers NMC Rathaman, KL; Meadows et al. (2007). Creation of a “patient safety zone” to reduce pharmacy and nursing distractions and improve patient care. Asph Midyear Clinical Meeting 42 (Dec).
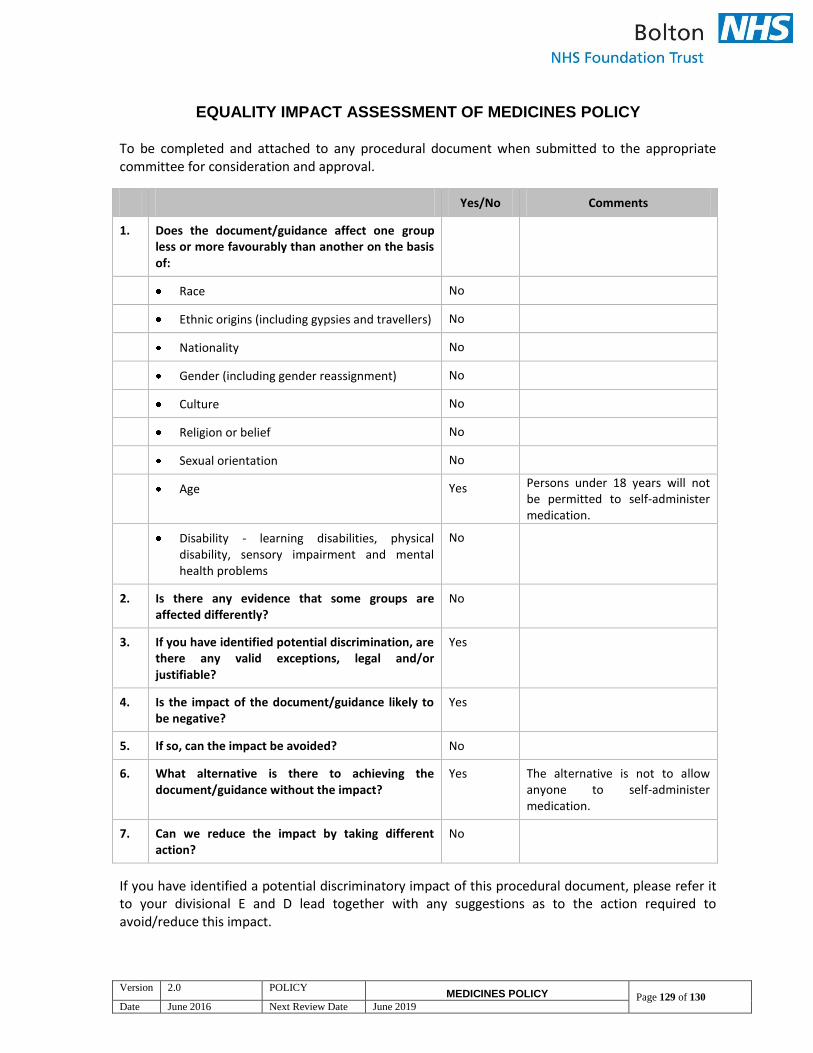
Version 2.0 POLICY MEDICINES POLICY Page 129 of 130
Date June 2016 Next Review Date June 2019
EQUALITY IMPACT ASSESSMENT OF MEDICINES POLICY
To be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval.
Yes/No Comments
1. Does the document/guidance affect one group less or more favourably than another on the basis of:
Race No
Ethnic origins (including gypsies and travellers) No
Nationality No
Gender (including gender reassignment) No
Culture No
Religion or belief No
Sexual orientation No
Age Yes Persons under 18 years will not be permitted to self-administer medication.
Disability - learning disabilities, physical disability, sensory impairment and mental health problems
No
2. Is there any evidence that some groups are affected differently?
No
3. If you have identified potential discrimination, are there any valid exceptions, legal and/or justifiable?
Yes
4. Is the impact of the document/guidance likely to be negative?
Yes
5. If so, can the impact be avoided? No
6. What alternative is there to achieving the document/guidance without the impact?
Yes The alternative is not to allow anyone to self-administer medication.
7. Can we reduce the impact by taking different action?
No
If you have identified a potential discriminatory impact of this procedural document, please refer it to your divisional E and D lead together with any suggestions as to the action required to avoid/reduce this impact.

Version 2.0 POLICY MEDICINES POLICY Page 130 of 130
Date June 2016 Next Review Date June 2019
Document Development Checklist
Type of document Formulary/prescribing guidelines
Lead author: Ann Eccles, Deputy Chief Pharmacist
Is this new or does it replace an existing document? Replaces Version 2 of the existing document
What is the rationale/ Primary purpose for the
document
To provide clear guidance on medicines management across the
Foundation Trust
What evidence/standard is the document based on? The document is based on National guidance including The
Medicines Act, Misuse of Drugs Act and NPSA
Is this document being used anywhere else, locally or
nationally?
Yes
Who will use the document? All staff involved in medicines management
Is a pilot run of the document required? (optional) No
Has an evaluation taken place? What are the results?
(optional)
No
What is the implementation and dissemination plan?
(How will this be shared?)
Via the Medicines Safety Group
How will the document be reviewed? (When, how
and who will be responsible?)
The document will be under review in the Medicines Safety Group
and will be updated by the Deputy Chief Pharmacist at least every
three years.
Are there any service implications? (How will any change to services be met? Resource implications?)
No
Keywords (Include keywords for the document
controller to include to assist searching for the policy
on the Intranet)
Medicines, administration, storage, disposal, controlled drugs
Staff/stakeholders consulted Members of the Medicines Safety Group
Any document that gives an instruction to prescribe or administer a medicine should have that instruction reviewed by the senior divisional pharmacist before it goes for ratification.
Signature of pharmacist:
EIA Completed
Signed and dated
By validator (Ann Eccles, Deputy Chief Pharmacist)
By ratifying officer (Steven Simpson, Chief Pharmacist)
.................................................................................
..................................................................................


















