Welcome to Anaesthesia! Dr Basil Almahdi Consultant Anaesthetist.

Medicine for the Obstetric AnaesthetistCathy Nelson-Piercy
Consultant Obstetric Physician, Guy’s & St Thomas’ Foundation Trust and Imperial College Healthcare Trust
Professor of Obstetric Medicine, King’s Health Partners
KCL Division of Women’s Health

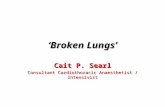
MBRRACE - Maternal death rate 2003-12(Three year rolling averages)
0
2
4
6
8
10
12
14
16
2004 2005 2006 2007 2008 2009 2010 2011
Rat
e pe
r 100
000
mat
erni
ties
Mid-year of each three-year period
Direct and Indirect maternal death rate
Direct maternal death rate
Indirect maternal death rate

Indirect maternal deaths 1985-2011(Three year periods)
0
1
2
3
4
5
6
7
8
9
10
1985-1987 1988-1990 1991-1993 1994-1996 1997-1999 2000-2002 2003-2005 2006-2008 2009-2011
Rat
e pe
r 100
000
mat
erni
ties
Triennium

Causes of maternal death

Causes of maternal death
0.00
0.50
1.00
1.50
2.00
2.50
Rat
e pe
r 100
,000
mat
erni
ties
Solid bars show indirect causes, hatched bars show direct causes
74% of women who died 2009-12 had a pre-existing medical disorder

Medical Problems in Pregnancy
Pre-existingAsthmaEpilepsyHypertensionDiabetesNeurologicalSLE / RA / CTDRenalCardiac
Pregnancy - specificPre-eclampsia
Thromboembolism
Gestational Diabetes
Obstetric cholestasis
Hyperemesis
Acute Fatty Liver Pregnancy
CoincidentalPneumonia, H1N1,Malaria, Hepatitis


• 1188 currently pregnant
• 5605 recently pregnant (within 42 days)
• 12.1% of total female admission aged 16-50 years
• Mean age 30
• Maternity admissions 290/100,000 maternities
• Maternal death rate 14/100,000 in 2011 CMACE report
ICNARC 2009-2012 Page 7


Pregnant Post partumObstetric 9% 70%PPH 36%Pre-eclampsia 2% 4%HELLP 0.7% 2.5%Non obstetric 91% 30%Pneumonia 23% 4.3%Pulmonary oedema
1.9% 1.6%
Pelvic infection 1.9%AKI 0.3% 0.8%Asthma 8% 0.6%Cardiovascular 8% 5.6%GI 10% 4.5%Neuro 9% 3.5%Endo 12% 1.6%
Page 9

Acute Medical Problems on Labour Ward
Chest pain
Breathlessness
Oliguria/ anuria/ AKI
Headache
Seizure
Sepsis
Page 10

Diagnosis of PE in pregnancySuspected PE
ABG, ECG, CXR
Start anticoagulation LMWH treatment dose UNSTABLE
STABLE Clinically urgent (out of hours)
DOPPLER USS LEGS
Anticoagulate with LMWH Thrombolysis/i.v. heparin/ thrombectomy
Portable echo
Suggestive of massive PE
CTPA
+ve -ve
CXR abnormalCXR normal
V/Q scan
+ve
-ve
+ve-veStop
anticoagulation
Still suspicious of PE
ABG, arterial blood gas; ECG, electrocardiogram; CXR, Chest X-ray; USS, ultrasound sonography; CTPA, computerised tomography pulmonary angiography Modified from: Scarsbrook et al. Clin Radiol 2006;61:1–12

Treatment of acute PE in pregnancy
High dose LMWH:
eg. Enoxaparin 1mg/kg/bd (= ACS dose)
NOT 1.5 mg/kg od (= non-pregnant dose)
RCOG Green Top Guideline no. 37b
Thrombolysis:SHOULD NOT BE WITHELD in massive PE, with haemodynamic instability
Ahearn et al. 2002;
Leonhardt G et al. J Thromb Thrombolysis. 2006;21:271-6.

Case 1

Page 14

SVT
Vagotonic manoeuvres are safe
Adenosine – safe
Verapamil is effective second line therapyUp to 10mg can be given without affecting fetal HR
Beta-blockers also safe

•39 yr old asian, 37 weeks pregnant
•c/o dizziness and epigastric pain
•o/e sweaty, BP 94/68, HR 84
Case 2

Case 2: which of the following are appropriate?
A. Troponin
B. Thrombolysis
C. Transfer to catheter lab
D. Primary angioplasty
E. Aspirin
F. Clopidogrel

Case 3
• 38 year old primip, 39 weeks pregnant
• C/o chest and back pain
• O/e BP 165/85, HR 124, O2 sats 97%
• Urinalysis NAD
• ‘Writhing around the bed’, ‘won’t lie down to be examined’
• Not in labour!

Page 20


• Not all chest pain and breathlessness = PE
• Beware the hypertensive (systolic) woman with chest pain
• CXR
• Echo


Acute severe asthma
Nebulized beta2 agonists + ipratropium
Oxygen – sats 94-98%
Oral / intravenous corticosteroids
Mg SO4
Intravenous theophylline
Intravenous beta 2 agonists
Consider delivery if ventilation required
Acute asthma is very unusual in labour

6/10/06

Case 4
33 year old womanReadmitted day 5 post emLSCS (for pre-eclampsia) c/o SOB and wheezyHad been discharged home day 3 post LSCS – well
O/EBreathless, sweaty SaO2 70% on RA; 100% on 15LBP 170/90 P75 SRUrine: 1+ proteinCVS: Raised JVP, HS normalChest – bilateral wheezing, scattered crepsAbdo – soft, non tenderPeripheral oedema to thighs
AIR
pH 7.49
PaCO2 4.1
PaO2 6.2
BEx 0.6

Echo normal; Diagnosis = postpartum pre-eclampsia

Postpartum pre-eclampsia
Pregnancy related hypertension and proteinuriaoccurring after 20/40
Symptoms: visual disturbance, headache, RUQ pain, peripheral / facial oedema
Incidence of pre-eclampsia: 2-5% of all pregnanciesIncidence of pulmonary oedema in PET: 2.3-2.9%
Sibai 1987 AJOG

36 year old woman, BMI 34Readmitted day 9 post elCS (for pl praevia) c/o SOB and pleuritic painHad been discharged home day 3 post LSCS – well7 day course LMWH – poor compliance; diclofenac 50 mg tds
O/EBreathless, sweaty SaO2 82% on RA; 100% on 15LBP 130/85 P78 SRCVS: Raised JVP, HS normalChest – scattered basal crepsAbdo – soft, non tenderPeripheral oedema to thighs
Case 5
ABG on Air
pH 7.39
PaCO2 4.8
PaO2 8.8
BE -3.5

Echo normal; Diagnosis = fluid overload secondary to diclofenac

Pulmonary oedema
Pre-eclampsiaReduced colloid osmotic pressureIatrogenic Fluid shiftsBeware syntocinon Beware NSAIDs
CardiacPeripartum cardiomyopathyMitral stenosisCardiac ischaemia
Drugs e.g. tocolytics, NSAIDs

Management of pulmonary oedema
OxygenStop IV fluidsDiureticsDiamorphineInvestigate cause = ECHOPPCM = Deliver / ACEIThromboprophylaxis

Peripartum cardiomyopathyDefinition: idiopathic cardiomyopathy presenting with heart
failure secondary to LV systolic dysfunction toward the end of pregnancy or in the months following delivery, where no other cause of heart failure is found. It is a diagnosis of exclusion. The left ventricle may not be dilated but the ejection fraction is nearly always reduced below 45%.
Incidence: 1 in 3000-15000 Risk factors: multiple pregnancy, age, hypertension, ethnicityMortality rate (US studies) 3-9%Failure to fully recover after one episode predicts recurrence in future pregnancy


Pulmonary arterial hypertensionSystemic ventricular dysfunction LVEF < 30%, NYHA III/IVPrevious PPCM with any residual LV impairmentSevere mitral stenosisSevere symptomatic aortic stenosisDilated Aortic root
> 45 mm Marfan> 50 mm bicuspid AoV
Severe coarctation
Advise against pregnancy

Delivery - Complex Care Plan

Physiology and cardiovascular stress of labour
Sympathetic response increases heart rateAutotransfusion increases stroke volumeIncrease cardiac output, oxygen consumption, A-V O2 diff Hyperventilation causes respiratory alkalosis
Ventricular failure,
impaired filling, outflow obstruction
Reduced colloid osmotic
pressure
Pulmonary oedema
Increased CO
Abnormal aorta or coronary
dissection arrhythmia

Vaginal delivery is generally preferable
Advantages
Less blood lossGreater haemodynamic stabilityAvoidance of surgical stressLess post-op infectionLower risk thromboembolismFewer pulmonary complications
butIt is less predictable for the teamIOL often for practical reasonsHigher risk of em LSCS
Cardiac indications for LSCS
Abnormal aortic root > 4.5 cmAortic aneurysm or dissectionSeverely impaired LV

Shortening the second stage of labour
Limiting the active second stage (pushing) in cases where the surges in BP may be particularly harmful eg aortopathy
No pushing – forceps/ventouse
Time limited – 30 mins on no evidence
Symptom limited eg ischaemic heart disease, LV failure, severe LVOTO

Uterotonic Drugs in cardiac patients
• All uterotonics have haemodynamic consequences
• However cardiac patients do not tolerate obstetric haemorrhage well.
The contraindications to uterotonics are relative.

Oxytocin
• First-line for prophylaxis and treatment of uterine atony– Rapid onset of action but short duration
• Side effects: free water retention
Tachycardia/ECG change Hypotension
• Avoid bolus – Give 5U in 50 mls saline over 20 mins– Then 40-60U in 500mls over 4-6 hrs
Br J Anaesth 2007

Prostaglandins
• PG E1 (misoprostol) selective vasodilator• Maybe used for uterine atony – less
successful than ergot +oxytocin1
• BUT best for cardiac patients….
• PG F2α (haemabate/carboprost) – causes vasoconstriction and bronchospasm
• Should be avoided especially in PHT1 Lokugamage etal. Acta Obstet Gynaecol Obstet 2007; 99: S202-5

Ergot
Reports of:
• Severe hypertension → seizure and stroke1
• Coronary vasospasm → MI2 and death3
• Elevated PA pressures and pulmonary oedema
• Normal healthy women developing severe HTN
1 Abouleish E. Anesth Analg 1976; 55: 813-52 Hayashi Y et al. Intern Med 2003;42: 983-6
3 Lin YH et al. Acta Obstet Gynecol Scand 2005; 84: 1022

Order of Use in a cardiac patient
1) Oxytocin– Diluted in at least 20 mls– Titrate to effect carefully
2) Misoprostol– 800 µg per rectum
….Go beyond if life-threatening haemorrhage……3) PG F2α
– Do not use in asthma, shunt, elevated PA pressures, single ventricle
4) Ergotamine– Do not use in pre-eclampsia, coronary artery
disease, aortopathies, aneurysms

KCL Division of Women’s Health
Thank you for your attention