

Medicare 2022 Changes
41
Brandy Bauer Ann Kayrish Medicare 2022 Changes November 4, 2021
Transcript of Medicare 2022 Changes

Brandy BauerAnn Kayrish
Medicare 2022 Changes
November 4, 2021
Agenda Costs in 2022
Landscape of Part D & MA plans
2022 Changes to Telehealth Benefits
Health & Drug Plan Considerations
Changes Related to Part B Covered
Services
Resources This resource was supported in part by grant 90MINC0002-01-01 from the U.S. Administration for Community Living, Department of Health and Human Services. Points of view or opinions do not necessarily represent official ACL policy.
Access webinar materials

2022 Costs

5
Original Medicare Costs: Part A2021 2022
Part A Deductible $1,484 ?
Hospital Copay/Days 61-90 $371 ?
Hospital Copay/Days 91-150 $742 ?
Skilled Nursing Facility Copay/Days 21-
100
$185.50 ?
Part A Monthly Premium (<30 credits) $471 ?
Part A Monthly Premium (30-39 credits) $259 ?

6
Original Medicare Costs: Part B
2021 2022
Part B Deductible $203 ?
Standard monthly premium $148.50 ?
Income Related Monthly Adjustment
Amount (IRMAA): Singles with incomes*
between $88,000 - $500,000+
Between $207.90
and $504.90
?
IRMAA: Couples with incomes* between
$176,000 and $750,000+
Between $207.90
and $504.90
?
* Per 2019 tax returns; singles included married couples filing separately
7
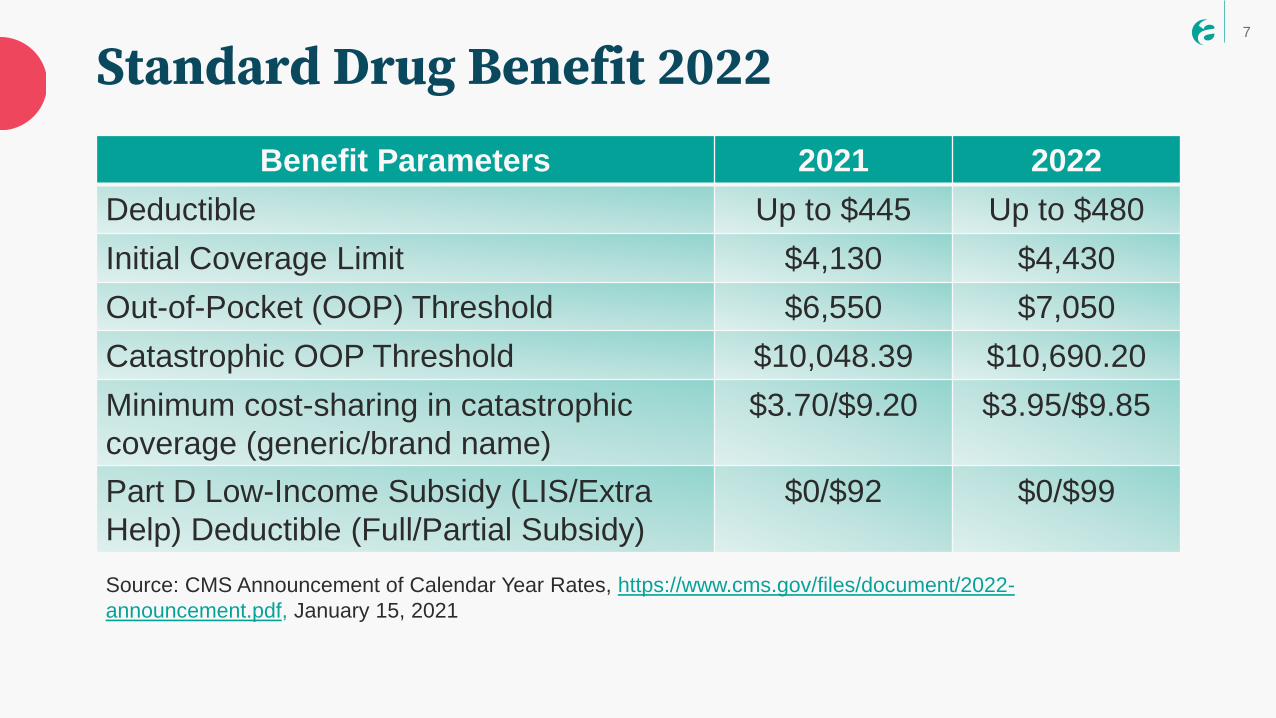
Standard Drug Benefit 2022
Benefit Parameters 2021 2022
Deductible Up to $445 Up to $480
Initial Coverage Limit $4,130 $4,430
Out-of-Pocket (OOP) Threshold $6,550 $7,050
Catastrophic OOP Threshold $10,048.39 $10,690.20
Minimum cost-sharing in catastrophic
coverage (generic/brand name)
$3.70/$9.20 $3.95/$9.85
Part D Low-Income Subsidy (LIS/Extra
Help) Deductible (Full/Partial Subsidy)
$0/$92 $0/$99
Source: CMS Announcement of Calendar Year Rates, https://www.cms.gov/files/document/2022-
announcement.pdf, January 15, 2021
8
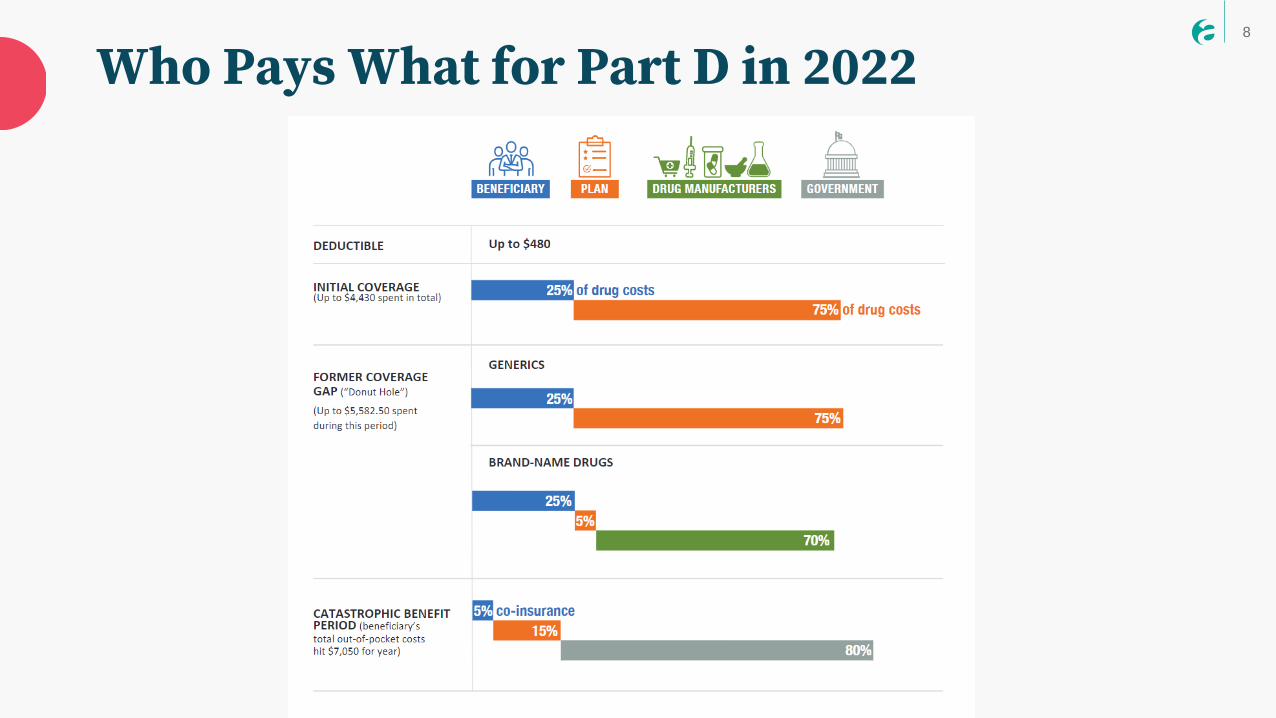
Who Pays What for Part D in 2022
9
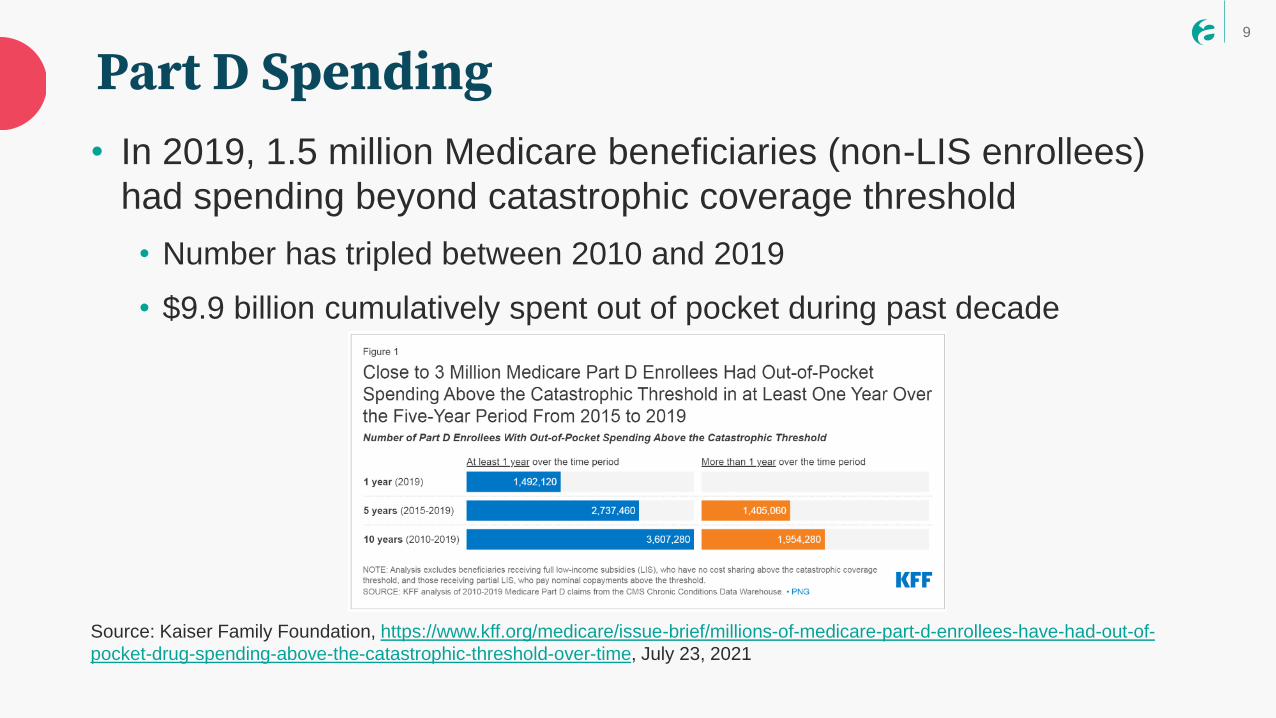
• In 2019, 1.5 million Medicare beneficiaries (non-LIS enrollees)
had spending beyond catastrophic coverage threshold
• Number has tripled between 2010 and 2019
• $9.9 billion cumulatively spent out of pocket during past decade
Source: Kaiser Family Foundation, https://www.kff.org/medicare/issue-brief/millions-of-medicare-part-d-enrollees-have-had-out-of-
pocket-drug-spending-above-the-catastrophic-threshold-over-time, July 23, 2021
Part D Spending
Landscape of Part D & MA Plans
11
• 23% decrease in the number of prescription drug plans (PDPs)
available across the country (n=766, down from 996 in 2021)
• Typical beneficiary will have choice between 23 plans
o NY has lowest number of offerings, and Arizona the highest
• 42% of enrollees are in a plan with 4 or more stars in 2022
• Average Part D monthly premium nationally is $33/month
o Varies widely, from $5.50 to $207.20
o ¾ of beneficiaries without low-income subsidy will pay higher premiums if
they remain in their current plan
Sources: Kaiser Family Foundation, https://www.kff.org/medicare/press-release/a-record-3834-medicare-advantage-plans-will-be-available-
in-2022-up-8-percent-from-2021-while-the-number-of-medicare-part-d-stand-alone-plans-is-decreasing-mainly-due-to-firm-consolidations/,
November 2, 2021; CMS, https://www.cms.gov/files/document/2022-star-ratings-fact-sheet1082021.pdf, October 8, 2021
2022 Part D Landscape
12
• ~13 million receive Extra Help in 2021
• 198 plans available for enrollment of LIS beneficiaries for no
premium (24% reduction over 2021)
• 26% of all PDPs are benchmark plans
• Across the country, benchmark plans range from 4 to 9,
depending on the state (e.g., Alaska 4 and Arizona 9)
• Asset limits for Extra Help in 2022 are $8,400/$12,600
(single/married) for full subsidy; $14,010/$27,950 for partial
subsidy (not including $1500 per person burial allowance)Source: Kaiser Family Foundation, https://www.kff.org/medicare/fact-sheet/an-overview-of-the-medicare-part-d-prescription-drug-
benefit/, October 13, 2021; CMS, CY2022 Resource Limits Memo, October 25, 2021
2022 Part D Landscape & Extra Help
13
• 3,834 MA plans nationally (8% increase over 2021)
o Average person has access to 39 MA plans
o Alaska has 2 (hybrid Medical Savings Accounts); Florida has 583
o 65 counties have no plans
o Over 1,100 Special Needs Plans, including 700 Dual-eligible Special Needs Plans (D-SNPs)
• 89% of MA plans include prescription drug coverage
• Average premium submitted by health plans for 2022 is $19/month
o 59% of MA plans will have a $0 premium (beyond Part B premium)
Sources: CMS https://www.cms.gov/newsroom/press-releases/cms-releases-2022-premiums-and-cost-sharing-information-medicare-
advantage-and-prescription-drug, September 30, 2021; KFF, https://www.kff.org/medicare/issue-brief/medicare-advantage-2022-spotlight-
first-look/, November 2, 2021
2022 Medicare Advantage Landscape
14
• 90% of plans offer vision, fitness, telehealth, hearing OR dental
benefits (scope of service varies)
• Plans with at least 4 stars more likely to offer supplemental
benefits, with meals (70%), transportation (40%) being most
frequently offered
• 90% of beneficiaries are currently in a MA-PD with four or more
stars in 2022
• No plans received a low performance icon on Plan Finder this
yearSources: CMS, https://www.cms.gov/files/document/2022-star-ratings-fact-sheet1082021.pdf, October 8, 2021; Avalere Health,
https://avalere.com/insights/more-medicare-advantage-plans-will-offer-non-medical-benefits-in-2022, October 19, 2021
2022 MA Landscape (cont.)

Changes to Telehealth
16
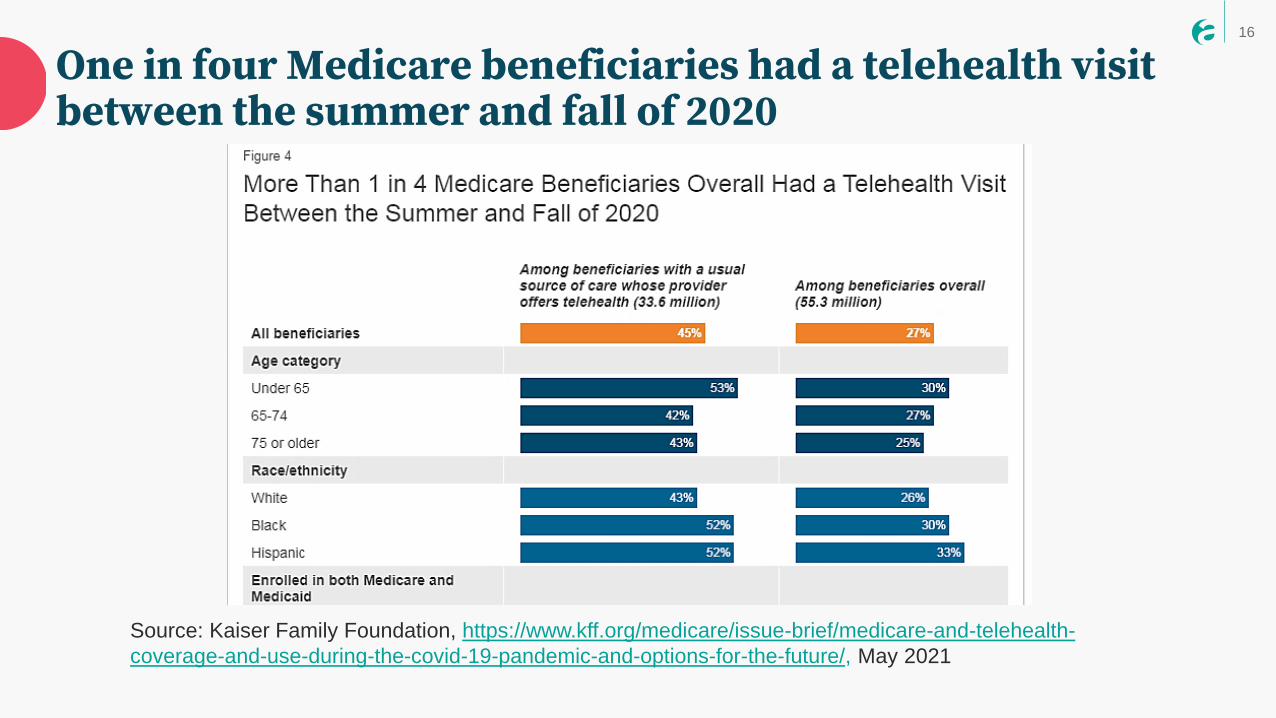
One in four Medicare beneficiaries had a telehealth visit between the summer and fall of 2020
Source: Kaiser Family Foundation, https://www.kff.org/medicare/issue-brief/medicare-and-telehealth-
coverage-and-use-during-the-covid-19-pandemic-and-options-for-the-future/, May 2021

17
• Remain covered until December 31, 2023
• Examples: Emergency department visits, home visits for established patients, discharge day management services
Retain coverage for temporary service on the Medicare telehealth services list
• Covered until the end of the PHE to allow CMS to collect data
• Examples: Home visits for new patients, assessment of tinnitus, ophthalmological service exams for new patients
https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes
Category 3 telehealth services added during the PHE & considered temporary
Other temporary services added during the PHE
18
Authorized permanent coverage of extended virtual check-ins• Communication-based technology
service
• Established patients only
• Initiated by the patient
• In-lieu of in-person visit
• May last up to 20 minutes
• Approved for audio-only or
audio/video communications
19
Beneficiary concerns
• Confusion on which services will be permanently available via telehealth
• Standard cost sharing applies for telehealth services and cost sharing maybe more with longer check-in
• Extended virtual check-in may delay next in-person appointment
• Beneficiaries always have the option to be seen in-person and should contact 1-800-Medicare to report access issues
20
Maintaining access to mental health services
Background
• Prevalence of audio-only visits for mental health counseling during the PHE
• Shortage of mental health care professionals
• Inadequate broadband access
• Less critical need for visualization
• Termination could harm access to care
21
Removed barriers for mental and behavioral health telehealth services
• Removed longstanding geographic restrictions
o No longer limited to rural or identified health professional shortage
areas
• Established the patient’s home as an allowable originating site
• Authorized federally qualified health clinics (FQHCs) and rural health clinics (RHCs) to act as distant site providers
• Established permanent coverage for audio-only services

22
Permanent coverage for audio-only mental and behavioral health services
1. Limited to diagnosis, evaluation, or
treatment of mental health disorders
2. Patient must be located at his/her
home (as the originating site)
3. Available to established patients only
(in-person visit within the last 6
months)
4. Beneficiaries utilizing audio–only
services must meet face-to face with
provider on a regular basis

23
5. Distant site practitioner must have interactive audio-video capabilities
6. Patient drives the decision to use or opt out of the audio-video modality
7. Claim indicates audio-only on the claim
8. RHCs and FQHCs can offer audio-only mental health services after the PHE
Permanent coverage for audio-only mental and behavioral health services (cont.)
24
Beneficiary concerns• Beneficiaries can expect to pay all regular copayment and
coinsurance amounts for services delivered via telehealth under both traditional Medicare and Medicare Advantage
• Beneficiaries utilizing audio-only services for mental and behavioral health services mut be prepared to meet with their mental health professional face to face on a regular basis

Health & Drug Plan Considerations
26
Two-tier specialty formulary option for MA-PD and Part D drug plans • Preferred specialty tier must offer lower cost-sharing
• Plans determine which drugs are placed on the preferred
specialty tier
• Plans must allow for exceptions between the two specialty tiers
• CY 2022 specialty drug tier threshold increased from $670 to
$830
Beneficiary concerns: The addition of a new another tier may cause additional confusion for beneficiaries in determining out of pocket drug cost
27
Senior savings model
• Part D and MA-PD plans can participate in model
• $35 max copay for a 30-day supply of some insulin products in deductible, initial coverage, & coverage gap phases of the Part D benefit
• Reduced copay does not apply in the catastrophic phase
• Model benefits are available to beneficiaries without LIS
• Participating plan filter has been removed from MPF
https://innovation.cms.gov/innovation-models/part-d-savings-model

28
Special circumstances special enrollment period (SEP)
• Not a new SEP for Medicare Advantage plan or prescription drug plan choice/enrollment
• Additional information on SEP added to medicare.gov website
29
Updates to Medicare Plan Finder Ability to save pharmacy and drug lists for logged in users
More prominent filter to include SNPs in search results
Removal of Insulin/senior savings program filters for MA and PDP
In-network pharmacy identifiers
Improved readability for mobile-phone users
Improved print function on plan comparison and detail pages
Increased prominence of key costs on plan detail page
New pharmacy drug cost comparison table on plan detail page
Anonymous users can email drug comparison results
30
• SSA recently clarified that COVID-19 related unemployment assistance and economic impact payments do not count as income for SSI benefits
• Extra Help benefits follow SSI rules
https://secure.ssa.gov/apps10/reference.nsf/links/09302021025535PM
https://www.ssa.gov/coronavirus/categories/monthly-benefits-and-other-financial-help/
COVID-19 stimulus payments do not count as income for Part D Extra Help

Changes Related to Part B Covered Services(PFS)
32
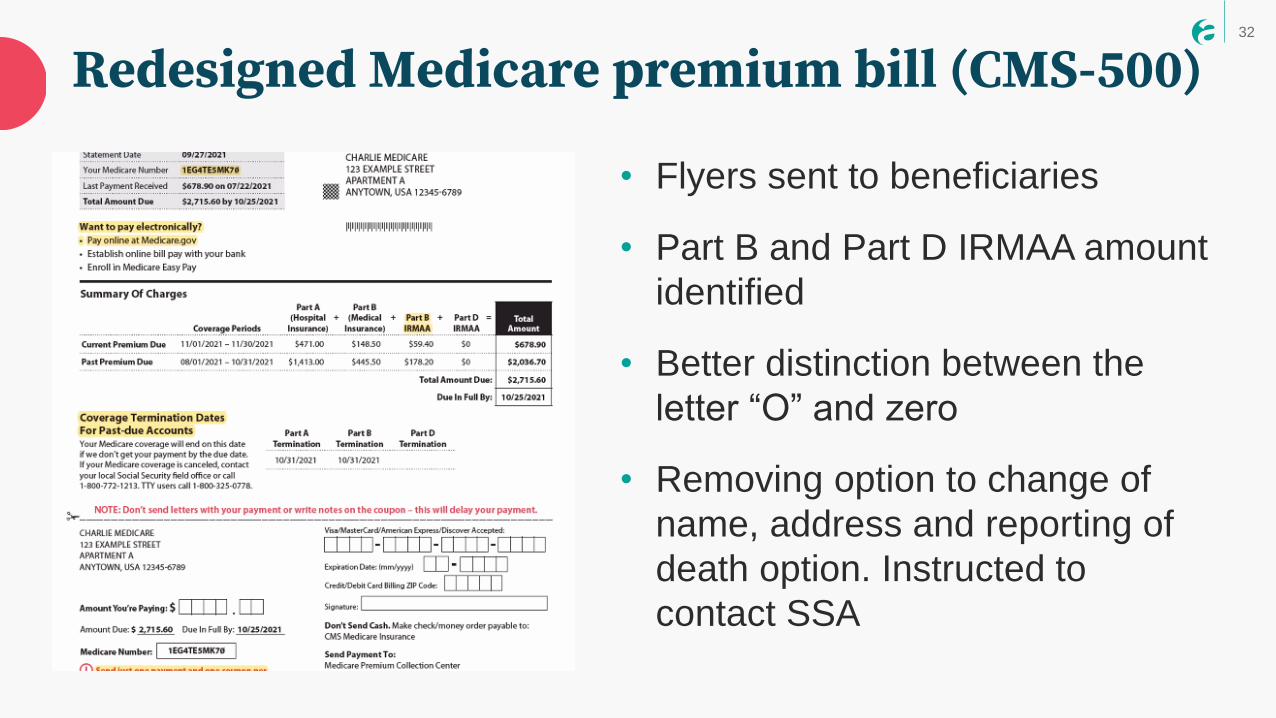
• Flyers sent to beneficiaries
• Part B and Part D IRMAA amount
identified
• Better distinction between the
letter “O” and zero
• Removing option to change of
name, address and reporting of
death option. Instructed to
contact SSA
Subhead
Redesigned Medicare premium bill (CMS-500)

33
Reduced payment rates for physical therapy & occupational therapy assistant services
• Payment rate is 85% of 80% of applicable Part B fee schedule
amount
• Applies to all outpatient services - physician offices, rehab
facilities, SNF, hospital outpatient departments
Beneficiary concerns:
Beneficiaries should talk with the prescribing physician with any
concerns about therapy services received and to Medicare or
MA plan for questions on co-insurance or copayment amounts
34
Physician assistant services
• Physician assistants may directly bill
Medicare for services furnished under
Medicare Part B
Beneficiary concerns:
Beneficiaries will want to ensure that the PA is a participating
Medicare provider and will bill Medicare for servicers rendered.
35
Change to coinsurance associated with colorectal cancer screenings
• Gradual elimination of the coinsurance payment when a growth or
polyp is found and removed as part of a colonoscopy screening
• Coinsurance to reduced over an eight-year period:
o 20% for 2022
o 15% for 2023-2026
o 10% for 2027-2029
o 0% for 2030
36
Reminder on CMS policy on diagnostic testing
• Medicare will pay for one COVID-19 diagnostic test, one
influenza test and one respiratory syncytial virus (RSV) test
without a physician/practitioner order
• All subsequent tests must be pursuant to an order to be
reimbursable by Medicare
• The interim policy rule was published in the Federal Register
September 2, 2020
(https://www.federalregister.gov/documents/2020/09/02/2020-
19150/medicare-and-medicaid-programs-clinical-laboratory-
improvement-amendments-clia-and-patient)

Resources(PFS)
38
• Open Enrollment Toolkit: https://ncoa.org/article/medicare-
open-enrollment-toolkit
• 2022 Medicare Changes fact sheet: https://bit.ly/3a2jT42
• Part D Cost Sharing Chart:
https://www.ncoa.org/article/medicare-part-d-cost-sharing-
chart
• Who Pays What in Part D in 2022 (former donut hole
illustration): https://www.ncoa.org/article/donut-hole-part-d
Resources from NCOA
39
• CMS landscape of plans by state:
https://www.cms.gov/files/document/92921-state-state-fact-sheets-2022-
medicare-advantage-and-part-d-landscape-final.pdf
• Medicare Advantage and Part D Final Rule 2022:
https://www.cms.gov/newsroom/fact-sheets/contract-year-2022-
medicare-advantage-and-part-d-final-rule-cms-4190-f2-fact-sheet
• Medicare Physician Fee Schedule:
https://www.federalregister.gov/documents/2021/07/23/2021-
14973/medicare-program-cy-2022-payment-policies-under-the-
physician-fee-schedule-and-other-changes-to-part
• Consolidated Appropriations Act of 2021:
https://www.congress.gov/bill/116th-congress/house-bill/133/text
Resources from CMS/SSA

Like what you heard?
Learn MoreDownload handouts and
join the online discussion
Rate UsTell us what you think
in the post-event survey


















