Medically Managed Weight Loss: A Discussion of ...tenant_id/ckeditor_assets/attachments/... ·...
41
Medically Managed Weight Loss: A Discussion of Metabolically-directed Nutritional Approaches Wesley Eichorn, DO and Susan Jevert-Eichorn, DO Assistant Professors Western Michigan University Homer Stryker M.D. School of Medicine Department of Family and Community Medicine August 1, 2019
Transcript of Medically Managed Weight Loss: A Discussion of ...tenant_id/ckeditor_assets/attachments/... ·...

Medically Managed Weight Loss: A Discussion of
Metabolically-directed Nutritional Approaches Wesley Eichorn, DO and Susan Jevert-Eichorn, DO
Assistant Professors
Western Michigan University Homer Stryker M.D. School of Medicine
Department of Family and Community Medicine
August 1, 2019

Disclosure Statement
• Neither of us have a financial relationship with or interest in a commercial interest
• Both presenters restrict carbohydrate intake as part of their dietary patterns and Dr. Eichorn
incorporates fasting as part of his lifestyle

References1. Mozaffarian D, Rosenberg I, Uauy R. History of modern nutrition science - implications for current research, dietary guidelines, and food policy. BMJ.
2018;361(k2392). doi:10.1136/bmj.k2392
2. POLLACK H. Dietary fats and their relationship to atherosclerosis. Circulation. 1957;16(2):161-162. doi:10.1161/01.CIR.16.2.161
3. Medicine: The Fat of the Land - TIME. TIME Magazine. 1961.
4. Ahrens EHJ, HIRSCH J, OETTE K, FARQUHAR JW, STEIN Y. Carbohydrate-induced and fat-induced lipemia. Trans Assoc Am Physicians. 1961.
5. Yudkin J. DIET AND CORONARY THROMBOSIS. HYPOTHESIS AND FACT. Lancet. 1957. doi:10.1016/S0140-6736(57)90614-1
6. 2005 Dietary Guidelines Advisory Committee Report Appendix G-5: History of the Dietary Guidelines for Americans.
https://health.gov/dietaryguidelines/dga2005/report/PDF/G5_History.pdf. Accessed June 4, 2019.
7. 2015-2020 Dietary Guidelines - health.gov. https://health.gov/dietaryguidelines/2015/guidelines/. Accessed June 23, 2019.
8. Cynthia OL, Margaret CD. Products - Health E Stats - Overweight, Obesity, and Extreme Obesity Among Adults 2009-
2010. https://www.cdc.gov/nchs/data/hestat/obesity_adult_11_12/obesity_adult_11_12.htm. Accessed June 23, 2019.
9. Anthony SF. Harrison’s Internal Medicine 20th Edition.; 2018.
10.Goldman-Cecil Medicine 25th Edition.
11.Bays HE, McCarthy W, Christensen S, Seger J, Wells S, Long J, Shah NN, Primack C. Obesity Algorithm Slides, presented by the Obesity
Medicine Association. www.obesityalgorithm.org. 2019. https://obesitymedicine.org/obesity-algorithm-powerpoint/(Accessed = 6-23-19)
12.Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease [published erratum appears in JAMA
1999 Apr 21;281(15):1380] [see comments]. JAMA. 1998;280(23):2001-2007. https://www.ornish.com/wp-content/uploads/Intensive-lifestyle-
changes-for-reversal-of-coronary-heart-disease1.pdf. Accessed June 19, 2019.
13.Tobias DK, et al. Effect of low-fat diet interventions versus other diet interventions on long-term weight change in adults: a systematic review
and meta-analysis. Lancet Diabetes & Endocrinology 2015; 3:968-979.

References14.Sackner-Bernstein J, Kanter D, Kaul S. Dietary Intervention for Overweight and Obese Adults: Comparison of Low-Carbohydrate and Low-Fat Diets.
A Meta-Analysis. Siegel A, ed. PLoS One. 2015;10(10):e0139817. doi:10.1371/journal.pone.0139817
15.Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional
Ketosis for the Management of Type 2 Diabetes: A 2-year Non-randomized Clinical Trial. bioRxiv. 2018. doi:10.1101/476275
16.Tsai AG, Wadden TA. Systematic review: an evaluation of major commercial weight loss programs in the United States. Ann Intern Med. 2005.
17.Mulholland Y, Nicokavoura E, Broom J, Rolland C. Very-low-energy diets and morbidity: a systematic review of longer-term evidence. Br J Nutr. 2012.
doi:10.1017/s0007114512001924
18.Mattson MP, Longo VD, Harvie M. Impact of intermittent fasting on health and disease processes. Ageing Res Rev. 2017;39:46-
58. doi:10.1016/j.arr.2016.10.005
19.Dorflinger LM, Ruser CB, Masheb RM. A brief screening measure for binge eating in primary care. Eat Behav. 2017;26:163-
166. doi:10.1016/j.eatbeh.2017.03.009
20.Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019. Diabetes Care. 2019;42(Supplement 1):S13 LP-
S28. doi:10.2337/dc19-S002
21.Reaven G. Insulin Resistance and Coronary Heart Disease in Nondiabetic Individuals. Arterioscler Thromb Vasc Biol. 2012;32(8):1754-
1759. doi:10.1161/ATVBAHA.111.241885/-/DC1
22.Hallberg S, McKenzie A, Williams P, et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-
Label, Non-Randomized, Controlled Study. Diabetes Ther. 2018;9:583-612. doi:10.6084/m9.figshare
23.Wallace TM, Levy JC, Matthews DR. Use and Abuse of HOMA Modeling. Diabetes Care. 2004;27(6):1487-1495.
24.Young T, Peppard PE, Gottlieb DJ. Epidemiology of Obstructive Sleep Apnea. Am J Respir Crit Care Med. 2002;165(9):1217-
1239. doi:10.1164/rccm.2109080

References25.Bezerra Bueno N, Vieira De Melo IS, Lima De Oliveira S, Da T, Ataide R. Systematic Review with Meta-analysis Very-low-carbohydrate ketogenic diet v.
low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Br J Nutr. 2018;110:1178-1187.
doi:10.1017/S0007114513000548
26.Santos FL, Esteves SS, da Costa Pereira A, Yancy WS, Nunes JPL. Systematic review and meta-analysis of clinical trials of the effects of low
carbohydrate diets on cardiovascular risk factors. Obes Rev. 2012;13(11):1048-1066. doi:10.1111/j.1467-789X.2012.01021.x
27.Auerbach BJ, Dibey S, Vallila-Buchman P, Kratz M, Krieger J. Review of 100% Fruit Juice and Chronic Health Conditions: Implications for Sugar-
Sweetened Beverage Policy. Adv Nutr. 2018. doi:10.1093/advances/nmx006
28.Faith MS, Dennison BA, Edmunds LS, Stratton HH. Fruit Juice Intake Predicts Increased Adiposity Gain in Children From Low-Income Families: Weight
Status-by-Environment Interaction. Pediatrics. 2006;118(5):2066-2075. doi:10.1542/peds.2006-1117
29.Bolton RP, Burroughs LF, Heaton KW. The role of dietary fiber in satiety, insulin: studies with fruit and fruit. Am J Clin Nutr. 1981;84(2):211-217.
doi:10.1093/ajcn/34.2.211
30.Unwin D, Haslam D, Livesey G. Journal of insulin resistance. J Insul Resist. 2016;1(1):9.
31.Monteiro CA, Moubarac JC, Levy RB, Canella DS, Da Costa Louzada ML, Cannon G. Household availability of ultra-processed foods and obesity in
nineteen European countries. Public Health Nutr. 2018;21(1):18-26. doi:10.1017/S1368980017001379
32.Harcombe Z, Baker JS, Cooper SM, et al. Evidence from randomised controlled trials did not support the introduction of dietary fat guidelines in
1977 and 1983: a systematic review and meta-analysis. Open Hear. 2015;2:e000196. doi:10.1136/openhrt-2014
33.Harcombe Z, Baker JS, DiNicolantonio JJ, Grace F, Davies B. Evidence from randomised controlled trials does not support current dietary fat
guidelines: a systematic review and meta-analysis. Open Hear. 2016;3(2):e000409. doi:10.1136/openhrt-2016-000409
34.Hooper L, Martin N, Abdelhamid A, Davey Smith G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev. 2015;(6).
doi:10.1002/14651858.CD011737

References35.Fung J. The Obesity Code : Unlocking the Secrets of Weight Loss. Vancouver: Greystone Books; 2016.
36.DUNCAN GG. Intermittent Fasts in the Correction and Control of Intractable Obesity. Trans Am Clin Climatol Assoc. 1962;74:121-129.
37.Erlandson M, Ivey LC, Seikel K. Update on Office-Based Strategies for the Management of Obesity. Am Fam Physician. 2016;94(5).
38.Malhotra A, Noakes T, Phinney S. It is time to bust the myth of physical inactivity and obesity: you cannot outrun a bad diet. Br J Sports Med.
2015;49(15):967-968. doi:10.1136/bjsports-2015-094911
39.Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK. Appropriate physical activity intervention strategies for weight loss and
prevention of weight regain for adults. Med Sci Sports Exerc. 2009;41(2):459-471. doi:10.1249/MSS.0b013e3181949333

Objectives
At the conclusion of this presentation, participants will be able to:
1. Examine the risks and benefits of low fat, low carbohydrate, and low-calorie diets in treating obesity
2. Describe the effects of low fat, low carbohydrate, and low-calorie diets on cardiometabolic risk factors
3. Identify strategies for incorporating medically managed weight loss into the family practice setting





“Americans eat too much fat. With
meat, milk, butter and ice cream, the
calorie-heavy U.S. diet is 40% fat, and
most of that is saturated fat—the
insidious kind…that increases blood
cholesterol, damages arteries, and
leads to coronary disease.”
“The only sure way to control blood
cholesterol effectively….is to reduce fat
calories in the average U.S. diet by
more than one-third (from 40% to 15%
of total calories), and take an even
sterner cut (from
17% to 4% of total calories) in saturated
fats.”

Transactions of the Association of
American Physicians 1961
“We propose that carbohydrate-induced
lipemia is a common phenomenon,
especially in the areas of the world
distinguished by caloric abundance and
obesity, whereas fat induced lipemia is
probably a rare familial disorder
encountered in all age groups.”
“It may surprise some readers to learn
that the lipemic plasma was obtained
during the high-carbohydrate period,
and the clear plasma during the high-fat
regimen.”


1977 Dietary Goals for Americans• Increase carbohydrate intake to 55 to 60 percent of calories
• Decrease dietary fat intake to no more than 30 percent of calories, with a reduction in intake of
saturated fat, and recommended approximately equivalent distributions among saturated,
polyunsaturated, and monounsaturated fats to meet the 30 percent target
• Decrease cholesterol intake to 300 mg per day
• Decrease sugar intake to 15 percent of calories
• Decrease salt intake to 3 g per day


“The Dietary Guidelines is a critical tool for professionals to help
Americans make healthy choices in their daily lives to help prevent
chronic disease and enjoy a healthy diet.”


What we have been doing is not
working ….What do we know
and what don’t we know?

Hormones
play a role
Insulin
“Insulin, an anabolic hormone, promotes the storage of
carbohydrate and fat and protein synthesis” (Harrison’s)
Cecil’s

Carbohydrates• 4 kcal/gram
• Can serve as energy source
• Can serve as cellular structural elements
• May contain sugars, starch, and/or fiber
• Break down to monosaccharides
• USDA DRI is 130 grams/day
• No known carbohydrate deficiency
• Not an essential macronutrient

Fat• 9 kcal/gram
• Used as energy source and for many metabolic processes
• Essential fatty acids exist
• Fatty acid deficiency can lead to a disease state
• USDA DRI for fat is at least 30 grams/day

Protein
• 4 kcal/gram
• Contains structural building blocks
• Essential amino acids exist
• Can be used as energy source
• Deficiency can cause Kwashiorkor
• USDA DRI is 0.8 to 2 grams/kg/day

What eating pattern is best?Needs to be
o Safe
o Effective
o One the patient can adhere to

• Definitions:o Low-carbohydrate diet: 50 to 120-
150 grams of carbohydrates per
day
o Very low-carbohydrate: <50 grams
of carbohydrates per day
• Metabolic effects
o Best evidence for weight loss
o Generally improves cholesterol profile
o May reduce blood pressure
o May increase energy expenditure
o Decreased hunger
o Carbohydrate cravings
o May precipitate gout flare
o Kidney disease progression (if severe kidney disease present)
o Malaise - “keto flu”
o Takes several weeks to adapt
Restricted Carbohydrate Diets

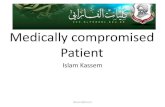
Virta Study – 2 year data
90
95
100
105
110
115
120
Baseline 1 year 2 years
Changes in Weight (kg)
Low Carb Usual care
Low Carb Intervention• Reductions in HbA1c, fasting glucose, fasting insulin,
weight, systolic blood pressure, diastolic blood pressure,
triglycerides, and liver alanine transaminase
• HDL increased
• Diabetes
• Decreased diabetes medication use
• Diabetes reversal
Usual Care• Decreased uric acid
• None of the effects listed above for the low carb group

Induction phase:
• Limit carbs to 20 grams per day
• Non-starchy “foundation” vegetables
Ongoing Weight Loss Phase
• Allows wider variety of vegetables, seeds,
nuts
• Some low-glycemic fruit/berries
Pre-maintenance phase:
• Allow carbohydrates to increase as long
as weight doesn’t
Maintenance phase
• 60-90 grams carbs per day limit
• Some more legumes, whole grains, and
fruits okay
Atkins DietAnimal products such as meat, poultry, fish, eggs, and dairy (no low-fat) are mainstays in the diet text

Avoid entirely
• Processed and refined foods (other than low-carb)
• Foods with a high glycemic index
Allowed in more liberal phase but still need to stick to carb count
• Cereals, breads, grains
• Dairy (other than butter or cheese which are allowed in all phases)
• Starchy vegetables
• Most fruit
Atkins Diet

Restricted fat diets - “10 to 30% total calories from fat”
Metabolic effects
o Works for weight loss for some people
o Can reduce fasting blood glucose and insulin
o Decreases LDL AND HDL
o May reduce BP
o Hunger control is difficult

Ornish
Encouraged
• Foods are best eaten in their natural form
• Vegetables, fruits, whole grains, and legumes
• One serving of a soy product each day
• Limited amounts of green tea
• Fish oil 3-4 grams each day
• Small meals eaten frequently throughout the
day
Restrictions
• Limit dietary fat: < 10% of total daily calories
• Limit dietary cholesterol: ≤ 10 mg per day
• Limit sugar, sodium, and alcohol
• Avoid animal products (red meat, poultry, and
fish) and caffeine (except green tea)
• Avoid foods with trans fatty acids, including
vegetable shortening, stick margarines, and
commercially prepared foods, such as frostings;
cake, cookie, and biscuit mixes; crackers and
microwave popcorn; and deep-fried foods
• Avoid refined carbohydrates and oils

Very Low-Calorie Diets• Often delivered via meal replacement products
• Generally delivered in a supervised setting
• Rapid results
• Not generally sustainable
• Long term evidence lacking

Very Low-Calorie DietsMetabolic Effects
• Reduces fasting glucose, insulin,
and triglycerides
• May reduce HDL and LDL
• Reduces blood pressure
Risks
• Fatigue, nausea, constipation, diarrhea, hair loss,
brittle nails, cold intolerance, dysmenorrhea
• Small increase in gallstones, kidney stones, gout
flares
• May have insufficient mineral intake leading to
dysrhythmias, muscle cramps, palpitations

Fasting• Intermittent
• Daily
• Weekly
• Alternate daily
• Prolonged – not recommended except in monitored situations
• Longest recorded is 382 days (13)
• Fasting not recommended for children, pregnant or nursing women or those that are malnourished

Informal Survey … but
interesting

Practical Approach to Evaluating Patients with Obesity
Initial Visit
• Motives
• Prior attempts at weight loss
• Stressors
• Food diaries
• Physical Activity
• Screen for:
• Depression
• Binge Eating disorders
VA Binge Eating Screener
“On average, how often have you eaten
extremely large amounts of food at one time
and felt that your eating was out of control at
that time?”
• Never
• <1 time/week
• 1 time/week
• 2-4 times/week
• 5 + times/week

Testing to Consider in the Evaluation of Patients with Obesity
Comorbidity What to order
Diabetes Fasting glucose level, hemoglobin A1C or 2-hour
oral glucose tolerance test
Insulin resistance Fasting glucose and fasting insulin levels to
calculate HOMA-IR
Hypothyroidism Thyroid stimulating hormone (TSH)
Renal abnormalities Serum creatinine and glomerular filtration rate
(GFR)
Nonalcoholic fatty liver disease Aspartate aminotransferase (AST) and alanine
aminotransferase (ALT), also consider liver
ultrasound

Testing to Consider in the Evaluation of Patients with Obesity
Comorbidity What to order
Hypertriglyceridemia and low high-density
lipoprotein (HDL)
Lipid panel
Gout Uric acid if considering a low carbohydrate diet as
this may temporarily increase the risk of gout
flair
Hypovitaminosis D Vitamin D level
Cardiovascular disease Electrocardiogram particularly if considering
medication therapy
Obstructive sleep apnea Sleep study

Nutrition Counseling Key Points
1. Choose an approach that works for the patient
2. Eliminate sugar and refined carbohydrates
3. Greatly restrict highly processed foods
4. Don't be afraid of saturated fats
5. Eat only 3 meals a day, but aim for less than that
6. Participate in healthy exercise

Common Pitfalls Inhibiting Weight Loss
• Continuing to consume substantial amounts of high calorie drinks
• Excessive intake of sugar-rich candy such as in cough drops
• Using non-nutritive sweeteners
• Prescribing a diet that the patient cannot sustain long term
• Not considering food availability for the patient

Common Pitfalls - Ketogenic Diet
• Eating too many fats
• Not eating enough salt when fasting or starting a ketogenic diet

Questions?