Medical problem in pregnancy
15
Medical problem in pregnancy
Transcript of Medical problem in pregnancy

Medical problem in pregnancy
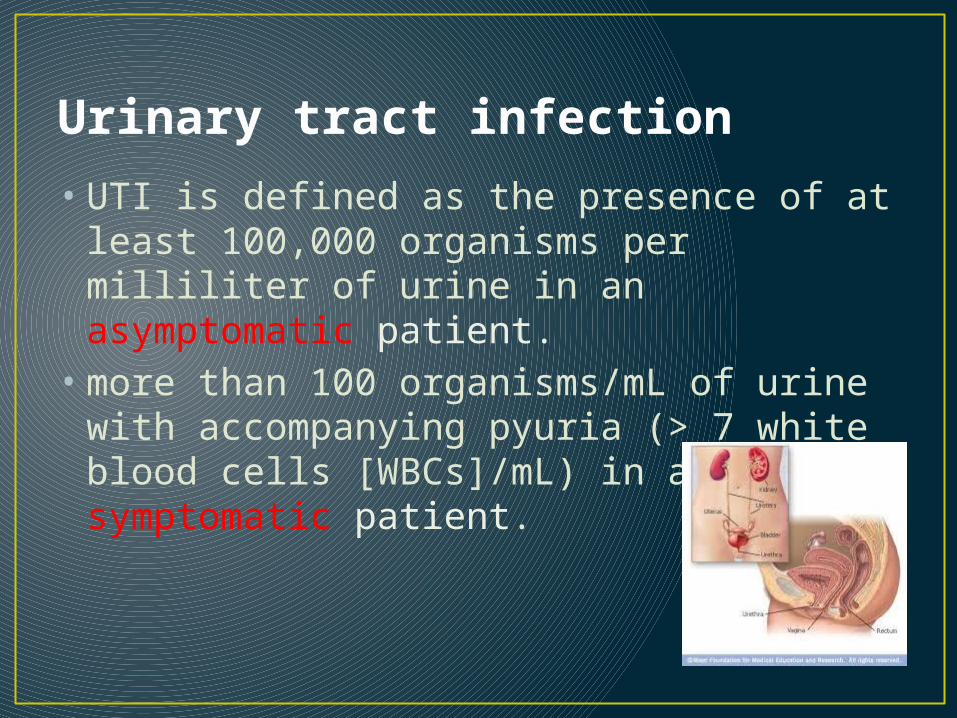
Urinary tract infection
• UTI is defined as the presence of at least 100,000 organisms per milliliter of urine in an asymptomatic patient.
• more than 100 organisms/mL of urine with accompanying pyuria (> 7 white blood cells [WBCs]/mL) in a symptomatic patient.

Pathophysiology• Infections result from ascending
colonization of the urinary tract, primarily by existing vaginal, perineal, and fecal flora.
• urinary retention caused by the weight of the enlarging uterus
• urinary stasis due to progesterone-induced ureteral smooth muscle relaxation.
• Blood-volume expansion is accompanied by increases in the glomerular filtration rate and urinary output
• Loss of ureteral tone combined with increased urinary tract volume results in urinary stasis, which can lead to dilatation of the ureters, renal pelvis, and calyces.
• Urinary stasis and the presence of vesicoureteral reflux predispose some women to upper urinary tract infections (UTIs) and acute pyelonephritis.

Causes
• E.coli is the most common cause of urinary tract infection (UTI).
• Cesarean delivery• Preeclampsia
Presentation
• Cystitis(1%)- suprapubic pain, frequency,dysuria,urgency,haematuria, proteinuria.
• Pyelonephritis(2%)- fever,rigor ,tachycardia, loin pain ,vomiting
Management• The urine should be cultured at the booking visit,
and asymptomatic bacteriuria is treated.• In pyelonephritis, treat with intravenous
antibiotics.

Chronic renal disease
• Affect 0.2% of pregnant women.• Dependent on the degree of hypertension
and renal impairment.• Creatinine level is more than 200 mmol/L.• Occurs in late pregnancy
• Aetiology:• 1. reflux nephropathy • 2. diabetes• 3. systemic lupus erythromatosus (SLE) • 4.Glomerulonephritis.• 5. polycystic kidney disease.
• Classification: • mild, moderate or severe depending on the serum
creatinine.• creatinine depends on the muscle mass i.e. a
figure representing moderate impairment in an 85-kg may represent severe impairment for a 50-kg woman.
Effect of pregnancy on renal impairment:
• - mild impairment (creatinine < 125 μmol/l): tolerate pregnancy well with no renal function deterioration.
• - severe renal impairment (creatinine > 250 μmol/l): at increased risk of permanent loss of function during and after pregnancy and even end stage of renal failure.

Effect of renal impairment on pregnancy :
• 1. PET, IUGR, spontaneous and iatrogenic premature delivery.
• - severe renal impairment + hypertension have < 50 % chance of successful pregnancy because of severe, early-onset of PET with severe IUGR.
• - premature delivery is justified in rapidly worsening renal function to avoid dialysis even in the absence of PET.
• 2. severe renal impairment → polyhydramnios and risk of cord prolapse due to fetal polyuria in response to high osmotic load from increased maternal urea.
• 3. nephrotic syndrome and heavy protienuria → severe hypoalbuminria with associated risks of pulmonary oedema and thrombosis.

MANAGEMENT
• Ultrasound for fetal growth
• Measurement of renal function
• Screening for urinary infection
• Control of hypertension
• Dialysis (severe)
PRESENTATION
• tiredness• swollen ankles, feet or
hands (due to water retention)
• shortness of breath• nausea• blood in the urine
VENOUS THROMBOEMBOLIC DISEASE
• Pregnancy increases the risk of venous thromboembolism (VTE) 4- to 5-fold over that in the nonpregnant state.
• The 2 manifestations of VTE are deep venous thrombosis (DVT) and pulmonary embolus (PE).
• Blood clotting factors are increased,fibrinolytic activity is reduced and blood flow is altered by mechanical obstuction and immobility.
• Women with inherited prothrombotic conditions and those with a family or personal history are prone to thromboses.
• Pulmonary embolus is important cause of maternal death.
Presentation
• DVT: leg pain and discomfort (the left is more commonly affected), swelling, tenderness, oedema, increased temperature and a raised white cell count. There may also be abdominal pain.
• PE: dyspnoea, pleuritic chest pain, haemoptysis, faintness, collapse.

DIAGNOSIS• In non-pregnant
womenChest x-rayArterial blood gas
analysisComputed tomographyVQ scanningurgent compression
duplex ultrasound scan.
MANAGEMENT
• Treated with subcuatneous LMWH.
• Doses are adjusted according to the anti-Factor 10a.
• Treatment should be stop before labour and restarted and continued into the puerperium.