Medical Office Leases: Understanding the Regulatory ... · Medical Office Leases: Understanding the...
105
American Bar Association Section of Real Property, Trust and Estate Law 20 th Annual Spring Symposia Washington, D.C. April 30 – May 1, 2009 Medical Office Leases: Understanding the Regulatory Requirements Behind the Lease Terms Materials Prepared by: Andrew Dick, Esq. Hall, Render, Killian, Heath & Lyman, P.C. One American Square, Suite 2000 Indianapolis, Indiana 46282
Transcript of Medical Office Leases: Understanding the Regulatory ... · Medical Office Leases: Understanding the...

American Bar Association
Section of Real Property, Trust and Estate Law
20th Annual Spring Symposia
Washington, D.C.
April 30 – May 1, 2009
Medical Office Leases:
Understanding the Regulatory Requirements Behind the Lease Terms
Materials Prepared by:
Andrew Dick, Esq. Hall, Render, Killian, Heath & Lyman, P.C.
One American Square, Suite 2000 Indianapolis, Indiana 46282

BIOGRAPHICAL SKETCH
Andrew Dick Andrew is an attorney in the Indianapolis office of Hall, Render, Killian, Heath & Lyman, P.C., where his practice focuses on real estate transactions and environmental law. He advises hospitals, health systems and physician practice groups on matters relating to the purchase and sale of real estate, commercial space leasing arrangements, office condominium developments, zoning matters, easements and restrictive covenants. Andrew also advises clients on a broad range of environmental law matters, including compliance with regulations for the disposal of medical and hazardous waste, air and water permitting, regulatory programs for the clean-up of contaminated property and the negotiation of environmental insurance policies. Andrew is a graduate of the University of Southern Indiana (B.S. 2002), Michigan State University College of Law (J.D., magna cum laude 2005), and the University of Miami School of Law (LL.M., Real Property Development 2006).

TABLE OF CONTENTS INTRODUCTION TO HEALTH CARE REAL ESTATE ....................................................................... 1 HEALTH CARE FRAUD AND ABUSE LAWS................................................................................... 3
THE ANTI-KICKBACK LAW................................................................................................... 3 THE STARK LAW .................................................................................................................. 5 FAIR MARKET VALUE ASSESSMENTS ................................................................................... 6
TAX IMPLICATIONS OF HEALTH CARE LEASING ARRANGEMENTS .............................................. 6
PRIVATE INUREMENT............................................................................................................ 7 PRIVATE BENEFIT ................................................................................................................ 7 REV. PROC. 97-13................................................................................................................. 8
ENVIRONMENTAL ISSUES AFFECTING HEALTH CARE FACILITIES ............................................... 9 SAMPLE LEASE PROVISIONS ...................................................................................................... 11 REGULATORY AND COMPLIANCE ......................................................................................... 12 PERMITTED / PROHIBITED USE ............................................................................................. 21 ETHICAL AND RELIGIOUS DIRECTIVES ................................................................................. 25 ENVIRONMENTAL COMPLIANCE ........................................................................................... 27 ARTICLES OF INTEREST ETHICAL AND RELIGIOUS DIRECTIVES FOR CATHOLIC HEALTH CARE SERVICES
INTRODUCTION TO HEALTH CARE REAL ESTATE∗ Over the past decade, hospitals and healthcare real estate developers have been on a building spree. In fact, not since the 1940s and 1950s has the healthcare industry seen this type of building boom. Experts claim that healthcare real estate is the fastest growing construction sector behind Federal projects. Not only is the quantity of building projects growing, but the size of projects is on the rise. This trend is evident by the recent completion of several mega hospitals that have in excess of one million square feet and at an estimated cost of a whopping three hundred million dollars. The question that many in the real estate and construction industry ask is why is this sector experiencing such a boom and what is the end result to consumers? While there appears to be no simple answer, experts agree that several factors have resulted in this building boom. One factor is that many hospitals and health systems are selling or leasing their real estate holdings to private third party investors. Healthcare executives are realizing that their real estate can be turned into much needed capital. That capital, in turn, can be used to build newer inpatient facilities, add new technology or to invest in other ventures that yield a greater return. This also frees up capital to focus more attention on providing exemplary healthcare. Many hospitals and healthcare systems are beginning to recognize that owning real estate is costly and it requires sophisticated management personnel to operate efficiently. But management and maintenance of the facility is not the only concern. Healthcare executives realize that most of their holdings are leased or utilized by staff nurses and physicians that demand certain perks. One of the benefits to staff, and a struggle for hospitals and health systems, is the rate of rent being charged. While physician lease arrangements must pass various regulatory hurdles, most rental rates offered to staff physicians are less than the true fair market value. This means the hospital receives a smaller return on investment. The primary trend for large health systems is to sell their land and buildings that are either undeveloped or that are used for medical office buildings or outpatient clinics. While some sales occur outright and without limitations, most do not. Providers often convey the land and improvements to an investor under a long term ground lease for a term lasting anywhere from fifty to ninety-nine years. The ground leasing strategy provides the hospital with the best of both worlds. The hospital obtains substantial rental leases, although within the ground lease, the hospital limits the use of the facility so that the facility will not be used to compete with profitable hospital endeavors. One of the primary concerns that a hospital faces when selling or leasing their real estate is whether it could be used to harm their business. Selling or leasing of land should not occur until a full analysis of the facts are considered. Sometimes the unused land or building could be a potential site for expansion. The building might be more valuable and worth maintaining if the hospital is a major tenant in the building or if several leases are nearing expiration and the hospital plans to increase the current rate being charged. A professional accountant or financial consulting firm should be utilized during this process. ∗ A portion of this introduction is being reproduced from an article written by Andrew Dick for the November/December 2007 Edition of Practical Health Law.

2
If selling is a viable option, hospitals should choose their buyer carefully. The new landlord or owner will take over the delicate responsibility of managing the very physicians and staff that often work for or in the hospital. Hospital-staff relations are vital to the hospital's continued success. The hospital should also ensure that a declaration or ground lease contains limitations on the type of use. As mentioned earlier, the greatest concern is that the relinquished property will be used to compete with the hospital. The fear is that the physician group or another investor network will offer competing services next to the hospital. The hospital should also be concerned with maintaining control over the land after it's sold or leased. This means it should retain the right to amend the rules or enforce regulations against the new owner for the use of the facility or its maintenance. Certainly some of the new healthcare construction is the result of third party developers constructing new medical office buildings, but a large portion is dedicated to hospital facilities themselves. Since the year 2000, hospitals and health systems cite the following reasons for the building spree: (1) aging facilities; (2) new specialty services; (3) increasing competition; and (4) movement to underserved markets. Aging facilities is one of the primary reasons often cited for new development. The last building boom occurred in the late 1940s and early 1950s with financial support from the 1946 Hill-Burton Act. Since that time period, the healthcare industry has changed significantly. New technology is often difficult to add to old facilities. It's often cheaper to construct new facilities than to retrofit an old facility. Not only has the industry changed, but patients demand more, competition is fierce and studies show that hospital design can play an important role in the healing process. The days of shared rooms are becoming a thing of the past. Patients are demanding services akin to many hotels. Newer facilities offer single patient rooms with space for family members, and all the amenities can be controlled from the patient's bed, including the television, HVAC and lighting. Other reasons often cited for the building boom include a need to focus on expanding services and those that provide a greater return on investment. Hospitals realize that certain services are more profitable than others. Often coined "specialty services," these services include the following: cardiac care, neurology, orthopedics, women's and children's health and oncology. Insurance, Medicare and Medicaid pay more for these services and the healthcare industry wants to capitalize on this opportunity. Another often cited reason for the building activity is a move from inner-city facilities to suburban facilities. The phrase "following the rooftops" is often used by industry leaders when deciding where to build their newest expansion. These providers realize that suburban dwellers are often high quality patients with good insurance. Add the opportunity to build with low cost capital through traditional lending, bond financing and physician joint ventures and the present time looks appealing. Finally, patients demand new technology, new facilities and high quality staff. In the information age, consumers are well educated, seek out industry leaders and recognize that they have choices. It's also no surprise that new and high tech facilities attract highly qualified
3
physicians and their staff. Studies have shown that newer facilities that are designed using evidence based designs not only improve the healing process, but that hospital staff are happier, healthier and more efficient.
HEALTH CARE FRAUD AND ABUSE LAWS
One of the most important issues affecting health care leasing arrangements today is whether federal fraud and abuse laws are implicated. The federal government spends trillions of dollars on health care programs each year and it estimates that fraud accounts for up to 10% of those expenditures.
In recent years, federal governmental agencies have made prosecuting health care fraud a
priority. The two most common federal fraud and abuse laws used in this effort are laws commonly referred to as the Stark Law and Anti-Kickback Law, both of which have the potential to significantly influence leasing arrangements between health care providers.
THE ANTI-KICKBACK LAW
The Anti-Kickback Provision - Section 1128B(b), of the Social Security Act (42 U.S.C. § 1320a-7b(b)) or the "Anti-Kickback Law" as it is commonly known, was originally created in 1972 to prevent financial incentives from influencing where a beneficiary of a federal health care program receives medical treatment. Over the past three decades it has been amended and revised, although maintaining a common goal of prohibiting the payment or receipt of remuneration (kickbacks, bribes or rebates) in exchange for referring individuals to providers of designated health care services.
The scope of the Anti-Kickback Law covers a myriad of real estate transactions,
including leasing arrangements. If, for example, a physician rents office space from a hospital to which he or she refers patients, then the leasing arrangement will most likely be covered by the Anti-Kickback Law. If the leasing arrangement is regulated under this law, then one must be aware that penalties for non-compliance include fines up to $25,000, imprisonment and possibly being excluded from participation in government health care programs.
Leasing arrangements are not entirely prohibited. If the Anti-Kickback Law applies, then
the leasing arrangement is prohibited unless the arrangement meets one of the statutes safe harbors. A commonly used safe harbor for leasing arrangements is the space rental safe harbor. It says that remuneration (kickbacks, bribes or rebates) does not include any payment made by a lessee to a lessor for the use of premises, so long as the following five conditions are met: 1) the lease agreement is set out in writing and signed by the parties; 2) the lease agreement specifies the premises covered by the lease; 3) if the lease provides access to the premises for periodic intervals of time, rather than on a full-time basis, the lease must precisely specify the schedule of such intervals, including their exact length and rent for such interval; 4) the term of the lease is for not less than one (1) year; and 5) the aggregate rental charge is set in advance and is consistent with fair market value in arms-length transactions.
4
While all of the conditions within the space rental safe harbor should be followed, those related to the payment of rental should be reviewed carefully. The rental rate must be "set in advance" at the time the lease is executed. This requirement means that the rental rate must be established in the agreement at the commencement of the term, without taking into account the volume or value of any referrals or business otherwise generated between the lessor and lessee. Similarly, any rental escalators within the lease must also be "set in advance" with a formula for calculating how the rent will be increased throughout the term. Simply stating that the lessor may increase the rent after an initial period of time is insufficient. A set increase throughout the term or an adjustment using the consumer price index may be acceptable.
In addition to the rent being "set in advance," it must also be consistent with the fair
market value for the premises. For purposes of this statute, fair market value is defined as the value of the rental property for general commercial purposes, but should not be adjusted to reflect the additional value that one party (either the prospective lessee or lessor) would attribute to the premises as a result of its proximity or convenience to referral sources. The fair market value requirement becomes particularly important when analyzing health care leasing arrangements under the Anti-Kickback Law and the Stark Law (discussed below). Counsel for the lessor or lessee is not qualified to make a determination as to whether the rental rate meets the fair market value definition. Clients should be advised to engage an independent and qualified appraiser to make a written determination as to whether the rental rate meets the fair market value requirements defined in the Anti-Kickback Law.
To help identify the type of leasing arrangements that the federal government is attempting to prohibit with the Anti-Kickback Law, the Office of Inspector General (OIG), the investigatory body of the Department of Health and Human Services, issued a Special Fraud Alert identifying the following as "questionable" leasing arrangements:
• Rental amounts in excess of amounts paid for comparable property rented in arms-length
transactions between persons not in a position to refer business; • Rental amounts for subleases that exceed the rental amounts per square foot in the
primary lease; • Rental amounts that are subject to modification more often than annually; • Rental amounts that vary with the number of patients or referrals; • Rental arrangements that set a fixed rental fee per hour, but do not fix the number of
hours or the schedule of usage in advance (i.e., "as-needed" arrangements); • Rental amounts that are only paid if there are a certain number of Federal health care
program beneficiaries referred each month; and • Rental amounts that are conditioned upon the supplier's receipt of payments from a
Federal health care program.
5
THE STARK LAW
In 1988 federal legislators led by Congressman Pete Stark, again became concerned with the high costs of health care as a result of physicians referring Medicare and Medicaid patients to health care entities in which they had a financial interest. They were concerned that referral arrangements have the potential to influence physician decision-making, lead to kickbacks and cause the overutilization of health care services. In 1989, Congress passed legislation known as the "Stark Law" in response to these concerns.
The Stark Law has many similarities to the Anti-Kickback Law, in that it targets fraud
and abuse in government-run health care programs. However, the Stark Law focuses on physician referrals, whereas the Anti-Kickback Law regulates referrals between any person or entity. When the Stark Law was initially created, it only prohibited physicians from referring Medicare and Medicaid patients to a clinical laboratory in which the physician or physician's immediate family member had a financial relationship. It has since been revised to prohibit physicians from referring Medicare and Medicaid patients to any entity furnishing designated health services (beyond clinical laboratories, including imaging services, outpatient pharmacy services, occupational therapy services, etc.) in which a physician or its family member has a financial relationship. Unlike the Anti-Kickback Law, the Stark Law is a strict liability statute, meaning the parties intent to comply is irrelevant.
Like the Anti-Kickback Law, the Stark Law applies to most real estate transactions, including leasing arrangements. For example, the Stark Law would be triggered if a group of primary care physicians own a medical office building and they decide to lease space within their building to a group of physicians to whom they often refer patients. Due to the complexity of the Stark Law, it may be helpful to consider the following factors when reviewing health care leasing arrangements to determine if the Stark Law applies: 1) Is there a physician or an immediate family member of such physician involved in the leasing arrangement; 2) Does the physician or immediate family member have a financial relationship with the leasing entity; 3) Is there a referral or a referring physician; 4) Is there a referral to the leasing entity for the furnishing of designated health services; and 5) Is a claim being submitted for payment under Medicare or Medicaid? If the answer to all five inquiries is "yes," then an exception to the Stark Law must be found prior to entering into the leasing arrangement; otherwise, the arrangement is in violation of the law and civil penalties may be imposed. While there are a host of Stark Law exceptions, the rental of office space exemption may apply in real estate leasing arrangements. Failure to comply with the exemption may include penalties up to $100,000 in civil penalties. The exception allows payments for the use of office space made by a lessee to a lessor if the leasing arrangement meets the following requirements: 1) the agreement is in writing, signed by the parties and specifies the premises; 2) the lease term is at least one (1) year; 3) the space to be rented does not exceed that which is reasonable and necessary for the "legitimate business purposes" of the lessee and is used exclusively by the lessee; 4) the rental charge over the term of the agreement is "set in advance" and is consistent with the fair market value; 5) the rental charge over the term of the agreement is not determined

6
in a manner that takes into account the volume or value of referrals or other business generated between the parties; and 6) the agreement would be commercially reasonable even if no referrals were made between the lessee and the lessor.
Not unlike the fair market value requirement defined in the Anti-Kickback Law, the Stark equivalent provides that the leasing arrangement must be consistent with arms-length transactions, and the rental amount must be consistent with the general market value for the space. The rental amount cannot be adjusted to reflect the additional value that the prospective lessor or lessee would attribute to the proximity or convenience to the other where one party is a potential source of patient referrals to the lessee. Most importantly, the fair market rental rate cannot vary based upon volume or value of referrals. An independent, qualified appraiser should be consulted when determining whether the rental rate meets the Stark fair market value requirement. The Stark Law also restricts other lease terms. Leasing arrangements subject to Stark may be terminated with or without cause during the lease agreement's initial term, provided that the parties do not enter into an agreement for the same space during the first year of the original lease term. Similarly, a lessee cannot hold over beyond the term of the lease for a period longer than six (6) months. FAIR MARKET VALUE ASSESSMENTS
If the Stark Law and Anti-Kickback Law affect a leasing arrangement, then the parties should ensure that the rental amount is consistent with the fair market value for the space prior to executing the lease agreement. In most cases, an opinion from an independent and qualified appraiser will be adequate evidence to comply with both laws. However, in rural settings, the parties may not have access to an independent and qualified appraiser and may need to rely upon an independent and qualified real estate broker to form an opinion on the value of the space. In either event, a written report should be prepared indicating that the appraiser or broker considered comparable properties in the area when it arrived at the fair market rental rate.
TAX IMPLICATIONS OF HEALTH CARE LEASING ARRANGEMENTS
When tax-exempt health care organizations (hospitals and rural healthcare clinics) lease space to or from for-profit entities, they not only have to worry about the potential implications of the Stark and Anti-Kickback laws, but they must also concern themselves particularly with maintaining their tax-exempt status. Tax-exempt entities entering into leasing arrangements with for-profit entities should consider four issues that may ultimately jeopardize their tax-exempt status: 1) whether the leasing arrangement would result in private inurement to the lessor or lessee; 2) whether the leasing arrangement would confer a private benefit to the lessor or lessee; 3) if the leased spaced is financed with tax-exempt bond proceeds; and 4) whether the rules of Rev. Proc. 97-13 are met.
7
PRIVATE INUREMENT Section 501(c)(3) of the Internal Revenue Code ("Code") states that for an entity to receive and maintain its tax-exempt status, "no part of the net earnings of [the entity] may be to the benefit of any private shareholder or individual." This means that none of the income or assets of an exempt organization subject to the private inurement doctrine may be permitted to directly, or indirectly, unduly benefit an individual, person or other entity that has a close relationship with the organization, when he, she, or it is in a position to exercise a significant degree of control over the exempt entity. The doctrine was created to ensure that tax-exempt entities further their charitable purpose and not the private interests of its directors, trustees, officers or other interested persons - otherwise known as "insiders."1 Violations of the private inurement doctrine may result in the denial or revocation of an entity's exempt status. With that in mind, it's important to recognize that the private inurement doctrine would only apply to a tax-exempt entity leasing space to or from a person who qualifies as an insider, or a for-profit entity in which an insider has an interest. The doctrine does not necessarily prevent an exempt organization from leasing space to or from an insider; however, the rent and other terms would have to be reasonable, and the terms cannot favor the insider. The reasonableness standard requires an approximately equal exchange of benefits between the parties. Thus, a lease for fair market value to an insider would most likely avoid a violation of the private inurement doctrine as there would be no apparent indication of either party gaining an excess benefit from the transaction. When looking at potential violations of the private inurement doctrine in leasing arrangements, the IRS may consider the duration of the lease and the amount and frequency of the rent payments in relation to customs in the area.2 PRIVATE BENEFIT The second doctrine that may apply to exempt organizations leasing space to or from for-profit entities is the private benefit doctrine. The doctrine requires that an exempt entity operate exclusively for exempt purposes.3 An exempt organization will not be regarded as operating exclusively for its exempt purpose if more than an insubstantial part of its activities is not in furtherance of an exempt purpose.4 The private benefit doctrine differs from the private inurement doctrine in that it is broader and applies to transactions with individuals or entities that are not, or do not have members who are, insiders. Moreover, it tolerates some incidental benefit to private parties as long as that benefit is insubstantial. This determination is made by examining whether the private benefit is 1) quantitatively incidental – meaning it is insubstantial,
1 An insider is generally considered one who has a unique relationship with the exempt organization where the individual (or corporation) "can cause application of the organization's funds or assets for the private purposes of the person by reason of the" person's position to exercise and control over the organization. BRUCE R. HOPKINS, THE LAW OF TAX EXEMPT ORGANIZATIONS, 564 (9th ed. 2007)(citing American Campaign Academy v. Comm'r, 92 T.C. 1053 (1989). Insiders may include an organization's founders, trustees, directors, officers, key employees, members of the family of these individuals, and certain entities controlled by them. Id. 2 HOPKINS, supra note 1, at 580. 3 Treas.Reg.§1-501(c)(3)-1(c). 4 Id.

8
measured in the context of the overall tax-exempt benefit conferred by the activity, and 2) qualitatively incidental, meaning the private benefit to certain individuals is necessary to achieving the tax-exempt purposes of the organization.5 Regardless, exempt entities should be especially wary of the application of the doctrine as the IRS has used it increasingly in recent years to deny or revoke organizations exempt status.6 Where a tax-exempt organization desires to lease space to or from a for-profit entity, the private benefit doctrine will most likely apply. Therefore, the parties involved must look at whether the agreement is quantitatively and qualitatively incidental so that the transaction does not jeopardize the exempt entity's exempt status. Specifically, the exempt organization's purposes should not be to provide such leases to private parties. Rather, if an exempt organization operates for charitable purposes, the majority of its activities/benefits should be dedicated to its charitable purpose and the private benefit the lease confers should be insignificant in comparison. The exempt organization should also look at the lease terms to make sure that it is agreeing to what could be considered "necessary" to effect its exempt purpose and that the terms and the price do not provide any unnecessary benefit to the for-profit party. For example, where a hospital leases space to a for-profit entity for necessary services at fair market value, and for as long as those services are needed for the hospital to effect its charitable purposes, the terms and rent should not be in violation of the private benefit doctrine. REV. PROC. 97-13 Most exempt health care organizations are allowed to issue tax-exempt bonds to finance land acquisitions and building projects. However, Rev. Rul. 97-13 ("Ruling") places limitations on the contracts exempt entities make with other entities that involve property financed by the proceeds of the tax-exempt bonds. The Ruling's purpose is to "set forth conditions under which a management contract does not result in private business use under § 141(b) of the Code."7 Specifically, it limits the use of "management contracts," (service or incentive payment contracts) between an exempt user and a service provider which is not a "qualified user."8 Under the ruling, a qualified user is considered a state or local government unit or any instrumentality thereof and any 501(c)(3) organizations if the financed property is not used in an unrelated trade or business under § 513 of the Code.9 The Ruling also states that "private business can arise by ownership, actual beneficial use of property pursuant to a lease, a management or incentive payment contract, or any other arrangement such as a take or pay or other output type contract."10
5 Rev. Rul. 70-186, 1970-1 C.B. 128. 6 Bruce R. Hopkins, Nonprofit Law Insights: Beware the Private Benefit Doctrine, http://www.bizonline-content.com/pkfnan/article.asp?cid=52&nid=9&pid=607532835&aid=375 (last visited January 15, 2008). 7 Rev. Proc. 97-13 § 1. 8 Jones Day, Memorandum Re: Rev. Proc. 97-13, http://www.nchffa.com/Dan%20Bacastow%20handout.pdf (last visited January 18, 2008). 9 Rev. Proc. 97-13 § 3.07. 10 Rev. Proc. 97-13 § 2.01(3).

9
The Ruling lays out operating guidelines for management contracts,11 but more importantly it provides for several safe harbors under which these contracts would not be in violation of § 141(b) of the Code.12 Exempt organizations will only have to meet the safe harbors of the Ruling if they (1) enter into "management contracts" as defined by the Ruling, which (2) involve property financed by the proceeds of the tax-exempt bonds the exempt organizations issued, and (3) that property is not used in an unrelated trade or business. Thus, if an exempt entity executes a management contract with a for-profit service provider (an unqualified user), giving that provider a leasehold interest in financed property,13 which property is used in the exempt entity's related trade or business, it will trigger the provisions of the Ruling. The Ruling would then require the exempt and for-profit parties involved in the transaction to meet the safe harbors of the Ruling or the bonds the exempt organization issued will no longer be tax-exempt, which will remove the tax-exempt benefit for those who have invested in those bonds.
ENVIRONMENTAL ISSUES AFFECTING HEALTH CARE FACILITIES Over the past seven years, the U.S. Environmental Protection Agency (the "EPA") has taken great interest in whether hospitals and healthcare providers are in compliance with environmental regulations. In 2002, Region 2 of the EPA started the Hospital and Healthcare Environmental Compliance Initiative (the "Initiative") in response to the growing number of environmental violations within the healthcare sector. According to the EPA, most hospitals and healthcare providers are simply not aware of their responsibility under federal environmental guidelines and have failed to implement effective compliance strategies. Through this Initiative, the EPA is taking a closer look at the hospital and healthcare facilities, stepping up inspections and enforcement activities. The goal of the Initiative is to ensure that these facilities are in compliance with all federal environmental laws and regulations, although the EPA is specifically focusing on those dealing with hazardous wastes, waste water discharges, air emissions, and storage tanks. Since the Initiative began, Region 2 of the EPA has inspected 44 healthcare facilities that have resulted in 22 enforcement actions and $911,018 in penalties. In 2003, the EPA aggressively sought fines against Nassau University Medical Center in East Meadow, New York for $279,900 and Mountainside Hospital in Montclair, New Jersey for $64,349. Both fines were sought for violations of the Resource Conservation and Recovery Act (RCRA) relating to the improper designation, storage, and labeling of hazardous wastes. The EPA also noted that neither hospital had a permit to store hazardous wastes. From 2004 through 2006 the EPA has continued to focus enforcement efforts towards hospitals and healthcare facilities by issuing more fines for noncompliance.
11 Rev. Proc. 97-13 §§ 5.01(1)-(5). 12 Rev. Proc. 97-13 §§ 5.03(1)-(6). 13 Rev. Proc. 97-13 § 2.01(4).

10
In light of the EPA's Initiative, attorneys representing healthcare providers should review their the environmental compliance language within their lease agreements. According to the EPA, the most common concerns for a hospital or healthcare facility are as follows: Clean Air compliance -Incinerators have all permits -Labs have any necessary permits -Asbestos removed properly -Paint booths have all permits Hazardous waste (HW) compliance -Proper labeling of HW -Inspection of HW storage sites to ensure storage areas don't exceed storage requirements -Proper HW determinations -Train employees on HW disposal and segregation -Underground Storage Tanks are in compliance and properly maintained Clean Water compliance -Permit obtained for wastewater discharges -Not disposing of HW through floor drains -Spill prevention control measures are in place Other laws that should be reviewed: -OSHA regulations -State environmental regulations -JCAHO guidance 812400v3

11
Sample Healthcare Lease Provisions
12
Sample Regulatory and Compliance Lease Provisions Example 1
22.12. Regulatory Matters.
(a) Landlord and Tenant enter into this Lease with the intent of conducting their relationship and implementing the agreements contained herein in full compliance with applicable federal, state and local law, including without limitation, the Medicare/Medicaid Anti-Kickback statute (the "Anti-Kickback Law") and Section 1877 of the Social Security Act (the "Stark Law"), as amended. Notwithstanding any unanticipated effect of any of the provisions of this Lease, neither party will intentionally conduct itself under the terms of this Lease in a manner that would constitute a violation of the Anti-Kickback Law or the Stark Law. Without limiting the generality of the foregoing, Landlord and Tenant expressly agree that nothing contained in this Lease shall require either party to refer any patients to the other, or to any affiliate or subsidiary of the other.
(b) If any legislation, regulation or government policy is passed or adopted,
the effect of which would cause either party to be in violation of such laws due to the existence of any provision of this Lease, then Landlord and Tenant agree to negotiate in good faith for a period of 90 days to modify the terms of this Lease to comply with applicable law. Should the parties hereto fail to agree upon modified terms to this Lease within this time, either Landlord or Tenant may immediately terminate this Agreement by giving written notice to the other party.
(c) For purposes of this Section of this Lease, "protected health information",
or PHI, shall have the meaning defined by the Standards for Privacy of Individually Identifiable Health Information, 45 C.F.R. Part 160 and Subparts A and E of Part 164 (the "Privacy Standards"), as promulgated by the Department of Health and Human Services ("HHS") pursuant to the Administrative Simplification provisions of the Health Insurance Portability and Accountability Act of 1996 ("HIPAA"). Tenant agrees to reasonably safeguard PHI from any intentional or unintentional disclosure in violation of the Privacy Standards by implementing appropriate administrative, technical and physical safeguards to protect the privacy of PHI. Tenant further agrees to implement appropriate administrative, technical and physical safeguards to limit incidental disclosures of PHI, including disclosures to Landlord, its subcontractors and agents. The parties agree that neither the Landlord nor its contractors, subcontractors or agents shall need access to, nor shall they use or disclose, any PHI of Tenant. However, in the event PHI is disclosed by Tenant or its agents to Landlord, its, contractors, subcontractors or agents, regardless as to whether the disclosure is inadvertent or otherwise, Landlord agrees to take reasonable steps to maintain, and to require its contractors, subcontractors and agents to maintain, the privacy and confidentiality of such PHI. The parties agree that the foregoing does not create, and is not intended to create, a "business associate" relationship between the parties as that term is defined by the Privacy Standards.

13
Example 2
Section 17.6 Fraud and Abuse / Stark Act. It is the intent and good faith belief of the parties hereto that this Lease complies with the Medicare/Medicaid Anti-Fraud and Abuse Statute ("Statute") and the regulations promulgated thereunder. It is also the intent and good faith belief that this Lease complies with the provisions of the Stark Act (the "Act") and does not in any manner violate the Act. Subsequent to the execution of this Lease, should any provision of this Lease be deemed by either party to be contrary to the provisions of said Statute, Act, regulations thereunder, or the "Safe Harbor" guidelines, then the parties agree to attempt in good faith to renegotiate the problematic provision to the mutual satisfaction of the parties. In the event the parties are not able to mutually agree on modification of the problematic provision, then either party may terminate this Lease upon thirty (30) days written notice to the other party if the terminating party has a good faith belief that the problematic provision creates an unfavorable exposure under said Statute, Act, regulations or "Safe Harbor" provisions thereunder.
Example 3 22. Regulatory Compliance. Lessor represents to Lessee that Lessor or individuals with an ownership interest in Lessor are considered to be a "referring physician" or a "referral source" as to Lessee for services paid for by Medicare or a state health care program, as the terms are defined under any federal or state health care anti-referral or anti-kickback, regulation, interpretation or opinion ("Referral Source").
22.1 Referral Source. Lessor and Lessee hereby acknowledge and agree that it is not a purpose of this Lease or any of the transactions contemplated herein to exert influence in any manner over the reason or judgment of any party with respect to the referral of patients or business of any nature whatsoever. It is the intent of the parties hereto that any referrals that may be made directly or indirectly by Lessor to Lessee’s business, shall be based solely upon the medical judgment and discretion of a patient’s physician while acting in the best interests of the patient. Lessor and Lessee hereby agree that the Rent and any increases in the Rent are intended to reflect fair market value and do not take into account the volume or value of referrals or business that may otherwise be generated between the parties for which payment may be made in whole or in part under Medicare, Medicaid or other Federal health care programs.
22.2 Termination Due to Legislative or Administrative Changes. In the event
that there shall be a change in applicable health care law or the interpretation thereof, including, without limitation, Medicare or Medicaid, statutes, regulations, or general instructions, (or the application thereof), the adoption of new legislation or regulations applicable to this Lease, the implementation of a change in payment methodology in any material third party payor reimbursement system, or the initiation of an enforcement action with respect to any applicable health care law, any of
14
which affects the continuing legality of this Lease, then either party may, by notice, propose an amendment to conform this Lease to applicable laws. If notice of such proposed change is given and the parties hereto are unable to agree within ninety (90) days upon an amendment, then either party may terminate this Lease by ten (10) days' advance written notice to the other party, unless a sooner termination is required under applicable law or circumstances.
22.3 Exclusions. During the term of this Lease, Lessor shall notify Lessee of
any exclusion of Lessor or its affiliates, employees, contractors, or agents from participation in any federal health care program, as defined under 42 U.S.C. §1320a-7b (f), for the provision of items or services for which payment may be made under such federal health care programs ("Exclusion") within two (2) business days of learning of any such Exclusion or any basis therefore. Lessee shall have the right to immediately terminate this Lease upon learning of any Exclusion.
22.4 Medicare Access to Books and Records. In the event, and only in the
event, that Section 952 of P.L. 96-499 (42 U.S.C. Section 1395x(v)(1)(I)) is applicable to this Lease, Lessee and Lessor agree as follows: (i) until the expiration of four years after the termination of this Lease, Lessor shall make available, upon written request by the Secretary of the federal Department of Health and Human Services or upon request by the Comptroller General of the United States, or any of their duly authorized representatives, this Lease, and books, documents and records of Lessor that are necessary to certify the nature and extent of the costs incurred pursuant to this Lease; (ii) if Lessor carries out any of the duties of this Lease or other contract between the parties through a subcontract, with a value or cost of $10,000 or more over a twelve-month period, with a related organization, such subcontract shall contain a clause to the effect that until the expiration of four years after the furnishing of such services pursuant to such subcontract, the related organization shall make available, upon written request to the Secretary of the federal Department of Health and Human Services or upon request to the Comptroller General of the United States, or any of their duly authorized representatives, the subcontract, and books, documents and records of such organization that are necessary to verify the nature and extent of the costs incurred pursuant to such subcontract; and (iii) Lessor shall notify Lessee immediately of the nature and scope of any request for access to books and records described above and shall provide copies of any books, records or documents to Lessee prior to the provision of same to any governmental agent to give Lessee an opportunity to lawfully oppose such production of documents if Lessee believes such opposition is warranted. In addition, Lessor shall indemnify and hold Lessee harmless from any liability arising out of any refusal by Lessor to grant access to books and records as
15
required above. Nothing herein shall be deemed to be a waiver of any applicable privilege (such as attorney client privilege) by Lessee.
22.5. Representations and Warranties of Lessee. Lessee represents and warrants to Lessor as follows:
(a) Non-Exclusion. Neither Lessee nor any of its affiliates are excluded from participation in any federal health care program, as defined under 42 U.S.C. §1320a-7b (f), for the provision of items or services for which payment may be made under such federal health care programs. Lessee shall notify Lessor of any exclusion of Lessee or its affiliates from participation in any federal health care program, as defined under 42 U.S.C. §1320a-7b (f), for the provision of items or services for which payment may be made under such federal health care programs ("Exclusion") within two (2) business days of learning of any such Exclusion or any basis therefore. Lessor shall have the right to immediately terminate this Lease upon learning of any Exclusion; and
(b) Business Terms. To Lessee's knowledge and belief: (a) the
Premises do not exceed that which is reasonable and necessary for the legitimate business of Lessee; (b) Lessee's Proportionate Share does not exceed Lessee's pro-rata share of expenses for the Premises and common areas based upon the total Building Rentable Area; and (c) the rental charges: (i) are set in advance, (ii) are consistent with fair market value, (iii) do not take into account the volume or value of any referrals or other business generated between the parties, nor do they include any additional charges attributable to the proximity or convenience of Lessor as a potential referral source; and (iv) would be commercially reasonable even if no referrals were made between Lessee and Lessor or their respective affiliates.
22.6. Representations and Warranties of Lessor. Lessor represents and warrants
to Lessee as follows:
(a) Non-Exclusion. Neither Lessor nor any of its affiliates (i) are excluded from participation in any federal health care program, as defined under 42 U.S.C. §1320a-7b (f), for the provision of items or services for which payment may be made under such federal health care programs; or (ii) have arranged or contracted (by employment or otherwise) with any employee, contractor or agent that Lessor or its affiliates know or should know are excluded from participation in any federal health care program;

16
(b) Advisory Opinion. Lessor shall not, directly or indirectly, request or cause an Advisory Opinion to be requested regarding or relating to the legality of this Lease or the transactions contemplated hereunder or substantially similar circumstances from any governmental body, including without limitation the U.S. Department of Health and Human Services Office of Inspector General or the Centers for Medicare and Medicaid Services without the prior written concurrence of Lessee, whether pursuant to this Section or otherwise. All submissions of any nature in connection with an Advisory Opinion request shall be approved in writing by Lessee prior to submission; and
(c) Business Terms. To Lessor's knowledge and belief: (a) the
Premises do not exceed that which is reasonable and necessary for the legitimate business of Lessee; (b) Lessee's Proportionate Share does not exceed Lessee's pro-rata share of expenses for the Premises and common areas based upon the total Building Rentable Area; and (c) the rental charges: (i) are set in advance, (ii) are consistent with fair market value, (iii) do not take into account the volume or value of any referrals or other business generated between the parties, nor do they include any additional charges attributable to the proximity or convenience of Lessee as a potential referral source, and (iv) would be commercially reasonable even if no referrals were made between Lessee and Lessor or their respective affiliates.
22.7. Corporate Integrity Agreement.
(a) Lessor acknowledges that Lessee is under a Corporate Integrity
Agreement with the Office of the Inspector General of the Federal Department of Health and Human Services (the "CIA"), and that such CIA imposes various reporting and operational compliance related obligations on Lessee. To the extent not otherwise set forth herein, Lessor agrees to cooperate with Lessee in compliance with the requirements of such CIA, as such requirements may apply to Lessor’s performance pursuant to this Lease.
(b) Lessor hereby certifies that Lessor will (i) comply with Lessee’s
Compliance Plan, including the training related to compliance with 42 U.S.C. § 1320a- 7b(b) (the "Anti-Kickback Statute") as it pertains to Lessor , and (ii) comply with Lessee’s Compliance Critical Concepts and policies and procedures related to compliance with the Anti-Kickback Statute, a copy of each of which has been provided to Lessor hereunder, and in each case solely as applicable to performance of Services under this Lease.

17
(c) Lessor certifies that it will comply with Lessee’s Compliance Plan and with the terms of the Anti-Kickback Statute in all matters involving Lessee.
(d) Lessor and Lessee certify that the agreement is not intended to
generate referrals for services or supplies for which payment may be made in whole or in part under any Federal health care program.
(e) If this Lease is terminated for any reason within one (1) year
following the Commencement Date, then Lessor and Lessee will not enter into any similar agreement with each other for the Premises before the first anniversary of the Commencement Date.
Example 4
Section 10. Representations and Warranties.
A. Tenant represents and warrants that at the time of its signing this Lease, it has obtained all licenses, certifications, and permits required under applicable law for the delivery of healthcare services at the applicable Leased Premises.
B. Tenant represents and warrants that all persons performing medical and healthcare services in a Leased Premises under this Agreement are licensed, certified, or permitted, under applicable state law of the state in which such services are to be provided, to perform the medical or healthcare services provided in the Leased Premises. Tenant shall adopt and implement a credentialing program consistent with the industry standards covering all licensed practitioners performing health care services at the Leased Premises.
C. Tenant represents and warrants that all persons performing medical or healthcare services in a Leased Premises under this Agreement will maintain, at no cost to Landlord, any license, certification, or permit required under the applicable state law for each state in which such person performs medical and healthcare services.
D. Tenant represents and warrants that all personnel performing services in the Leased Premises under this Agreement will provide services within the scope of their applicable license, certification, or as permitted by applicable state law. Tenant further represents and warrants that physicians licensed under applicable state law for each state in which any non-physician personnel will perform services in the applicable Leased Premises will be supervising the non-physician personnel where such supervision is required by applicable state law.
E. Tenant covenants that any health care provider performing medical and related services in the Leased Premises under this Agreement will fully and properly disclose to their patients, to the extent required by applicable state law, any financial interest that the health care provider has in an entity to which that health care provider refers the patient.
F. Tenant covenants to maintain any books, records, patient charts, patient files, or any other document containing protected health information as defined in regulations to the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), at 45 C.F. R.

18
§164.501, as amended, in accordance with all applicable laws, regulations, ordinances, statutes, and rules.
G. Tenant warrants that each agent, employee, and representative performing medical and related services under this Agreement understands the requirements and obligations required of Tenant and each agent, employee, and representative performing medical and related services under this Agreement under the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) and under all applicable federal and state healthcare fraud and abuse laws including, but not limited to, the federal Antikickback Statute and the Stark law. Tenant’s agents, employees, and representatives performing medical and related services under this Agreement shall use reasonable efforts to maintain any protected health information orally conveyed by a patient while in the Leased Premises. Tenant further covenants that each agent, employee, and representative performing medical and related services under this Agreement undergoes training or education on the requirements and obligations of Tenant and each agent, employee, and representative performing medical and related services under this Agreement under HIPAA and under all applicable federal and state healthcare fraud and abuse laws including, but not limited to, the federal Antikickback Statute and the Stark law prior to beginning an assignment at the applicable Leased Premises and periodically thereafter.
H. Tenant represents and warrants that neither it, nor its agents, employees, or representatives, is currently excluded, debarred, suspended, or otherwise ineligible to participate in Medicare, Medicaid, or any other federal health care program. Further, Tenant covenants not to act, or permit its agents, employees, and representatives to act, in any way that will reasonably result in the exclusion, debarment, suspension, or other action making Tenant, or any agent, employee, or representative of Tenant, ineligible to participate in Medicare, Medicaid, or any other federal health care program. Tenant covenants to notify Landlord immediately of any threatened, proposed, or actual exclusion from Medicare, Medicaid, or any other federal health care program.
I. Tenant covenants to notify Landlord, in writing within thirty (30) days, of the receipt of any letter, notice, correspondence or pleading that asserts or makes any Claim against the Tenant or its agents, employees, and representatives, whether sounding in liability or medical malpractice, arising out of or related to the operations or provision of services in the Leased Premises. Tenant further covenants to notify Landlord, in writing within fifteen (15) days of the receipt of any letter, notice, correspondence or pleading that informs Tenant, or its agent, employees, or representatives, of any pending matter to take action against, suspend or revoke, whether permanently or temporarily, any license, certification, permit or other authorization required of the Tenant, its agents, employees or representatives to conduct operations or provide services in the Leased Premises.
J. Tenant represents and warrants that Landlord, in its capacity under this Agreement, is not Tenant’s “Business Associate,” as that term is defined in HIPAA regulations.
K. Tenant represents that the space rented does not exceed that which is reasonably necessary to accomplish the commercially reasonable business purpose of this Agreement.
L. Tenant shall ensure that the prices it charges to customers for all health care services do not exceed the prices for such services that Tenant posts at the Leased Premises.

19
Tenant shall also ensure that the prices it charges to third-party payors are consistent with the terms of Tenant’s agreements with such payors and applicable law.
M. Tenant shall not operate Leased Premises as an out-patient facility of a hospital.
Example 5 Section 25. Fair Market Value.
A. Landlord and Tenant agree that no charge or payment owed by either party to the other party under this Agreement has been determined in a manner that takes into account the volume or value of any referral or other business generated between the parties. Landlord and Tenant further agree that it is their intention that this Agreement fully comply with the terms of the Space Rental Safe Harbor to the federal Anti-Kickback Statute, 42 C.F.R. § 1001.952 (b). In the event any study of the fair market value of the Leased Premises conducted on behalf of Landlord by an independent valuation consultant at any time during the Lease Term concludes that the Rent charged under this Agreement is inconsistent with fair market value then, upon the provision of written notice by Landlord to Tenant of such conclusion, the Rent automatically adjusts effective as of the date thirty (30) days after the date of such notice, without the need for further action by the parties, unless Tenant provides written notice to Landlord during such thirty (30)-day period of its intent to terminate this Agreement as to the affected Leased Premises. Any such termination is effective thirty (30) days after the date of Tenant’s notice.
B. Each and every time that this Agreement as to a particular Leased Premises is renewed and only upon such renewal, the Base Rent for the renewed lease term will adjust upward by a percentage amount equal to the CPI Adjustment Factor (defined next). The “CPI Adjustment Factor” means the percentage change, if any, in the CPI (defined next) from the actual Rent Commencement Date of the prior applicable period to the applicable date on which the CPI Adjustment Factor is measured. “CPI” means the United States Department of Labor, Bureau of Labor Statistics, Consumer Price Index for all Urban Consumers (U.S. city average, base 1982-1984 = 100). For example, the first adjustment to the Base Rent will increase by the CPI Adjustment Factor determined by the increase in the CPI between the Rent Commencement Date of the applicable Leased Premises and the first day of the renewal term. If the CPI is discontinued during the Lease Term of the applicable Leased Premises or published less frequently during the Lease Term of the applicable Leased Premises than it is during the six (6) months preceding the date the parties entered into the Agreement as to the applicable Leased Premises, Landlord and Tenant will either substitute an official index that is nearly equivalent to the CPI and is published by the Bureau of Labor Statistics, or a successor governmental agency, or use a substitute procedure that reasonably reflects and monitors consumer prices, the base year (1982-84 =100), or another base year. If another base year is used in computing the CPI, the CPI as changed or the figures used in making the applicable adjustments will accordingly change so that all changes in the CPI are taken into account despite the change in the base year.

20
Example 6 Section 18.10 Regulatory Compliance. The parties agree that this Lease is intended to
comply with all state and federal laws, regulations, and policies including, but not limited to the Anti-Kickback Statute (42 U.S.C. Section 1320a-7b(b)) and the regulations promulgated thereunder, and the Ethics in Patient Referrals Act (42 U.S.C. Section 1395nn) (also known as "Stark") and the regulations promulgated thereunder (collectively, the "Health Care Laws"). If any provision of this Lease is believed by either party in good faith to be materially in violation of the Health Care Laws, the parties shall attempt in good faith to amend this Lease, if possible, to conform to the Laws. If the parties are unable to agree on any such amendment, or if it is not possible to amend the Lease to comply with the Laws, then either party may terminate this Lease. Example 7 35. Protected Health Information.
(a) Lessor acknowledges and agrees that from time to time during the Term, Lessor, its representatives or assigns may be exposed to, or have access to, Protected Health Information ("PHI"), as defined by HIPAA, 45 CFR Parts 160 and 164. Lessor agrees that it will not use or disclose PHI for any purpose unless required by a court of competent jurisdiction or by any governmental authority in accordance will the requirements or HIPAA and all other applicable medical privacy laws.
(b) Lessor shall preserve any "Confidential Information" of or pertaining to
Lessee and shall not, without first obtaining Lessee’s prior written consent, disclose to any person or organization, or use for its own benefit, any Confidential Information of or pertaining to Lessee during and after the Lease Term, unless such Confidential Information is required to be disclosed by a court of competent jurisdiction or by any governmental authority. As used herein, the term "Confidential Information" shall mean any business, financial, personal or technical information relating to the business or other activities of Lessee that Lessor obtains in connection with this Lease.

21
Sample Permitted / Prohibited Use Language
Example 1
ARTICLE III USE AND OCCUPANCY
Section 3.1 Use; Compliance; Operation. (A) Permitted Use. The Leased Premises shall be used for only for the Permitted Uses and for no other purpose. Landlord does not guarantee that Tenant shall be the exclusive provider of any medical service or procedure. All such physician offices shall be exclusively used and occupied by physicians and staff necessary to support such physicians in the practice of medicine. All such physicians shall be members of the active medical staff of the Hospital or the Hospital Parties. (B) Prohibited Use. Tenant shall not use or permit the Leased Premises to be used or occupied: (i) to provide health care services that are at any time provided to inpatients or outpatients of the Hospital (collectively, the "Restricted Services") or (ii) to provide any of the following services: antenatal diagnostics; audio and vestibular testing; brain stem evoked potentials; CAT scans; DCG (Holter Monitor); durable medical equipment products; ECG (Electrocardiogram); EEG (Electroencephalogram); evoked potentials; fluoroscopy; angiography; general laboratory tests; general radiology studies; infusion; mammography; positron emission tomography (PET) scans; operating rooms; pharmacy; pulmonary function tests; renal services; sleep lab; thallium stress test; ultrasound; magnetic resonance imaging ("MRI"), computerized tomography ("CT"), invasive and/or intravascular procedures (other than endoscopy and colonoscopy procedures), osteoporosis screening services, digital radiology, physical therapy, speech therapy or occupational therapy, or any procedure involving the administration of a radiopharmaceutical for diagnosis, therapy or research (nuclear medicine); any procedure requiring anesthesia which must be administered by an anesthesiologist or certified registered nurse anesthetist ("CRNA") or other trained anesthetist, hospice, hospital, medical oncology, radiation oncology, urgent care center, respiratory therapy, home health services, or use of one or more hyperbaric oxygen chambers (the "Prohibited Services"); provided, however, that the restrictions with respect to Restricted Services shall not prohibit Tenant from providing Restricted Services that are not Prohibited Services to Tenant’s "own patients." The term "own patients," as used herein shall mean persons who specifically seek out and request the professional services of Tenant because of Tenant’s medical specialty (and not solely because Tenant provides Restricted Services), or who are referred for professional services because of Tenant’s medical specialty (and not solely because Tenant provides the Restricted Services). Tenant shall not market or promote the provision of Restricted Services in the Building to any person. In the event that there is any disagreement between the Hospital and Tenant regarding whether services are Restricted Services, or whether a person seeks out or is referred to an occupant for purposes unrelated to the provision of Restricted Services, such disagreement shall be resolved by the Hospital in its reasonable discretion and the same shall be binding on Tenant. In addition, the Hospital may from time to time add to, delete from or

22
otherwise modify the services constituting Prohibited Services and Tenant shall not use the Leased Premises to provide such Prohibited Services; provided, however: (1) Tenant shall not be charged with knowledge of any modification to the Prohibited Services until a copy of the same shall have been provided to Tenant; and (2) if Hospital adds a service to the list of Prohibited Services (a "New Prohibited Service"), and Tenant was, prior to Hospital giving such notice of such New Prohibited Service, already providing the New Prohibited Service, Tenant shall be permitted to continue to provide such New Prohibited Service throughout the Term including expansions of the rentable area thereunder and including all renewals thereof. (C) Third Party Beneficiary. The Hospital Parties as well as any other operator of the Hospital are third party beneficiaries of the provisions of this Section 3.1 and shall be entitled to enforce breaches of such provisions directly against Tenant. Example 2 SECTION 4. USE OF PREMISES
4.1 Prohibited Uses.
(a) The Premises shall continuously and at all times during the Term be used
and occupied by Tenant for general office use and medical office use ("Physicians") to engage in the practice of pulmonary and/or polysomnography medicine services, including testing and interpretation and other related activities incidental thereto ("Permitted Use"), and for no other purposes. Landlord acknowledges and agrees that Tenant and its patients will be occupying the Premises on a twenty-four (24) hour basis, Monday through Sunday, including legal holidays ("Normal Business Hours"), in order to perform those services described as Permitted Uses. Notwithstanding the foregoing, the provision or operation of any of the following services or facilities shall not be permitted in the Premises:
(i) the provision of any medical or related service to or for any person
that is in addition to the examination and diagnosis of patients performed directly by a Physician or by other health care professionals either independently licensed or under the direct supervision of a Physician, or a facility operated for the provision of any such service(s);
(ii) a laboratory (including, without limitation, a pathology laboratory
or a clinical laboratory); and (iii) diagnostic or therapeutic testing services, including without
limitation, all diagnostic imaging services, including without limitation, the following:
A. fluoroscopy; B. x-ray;
23
C. plane film radiography; D. computerized tomography (CT); E. ultrasound; F. radiation therapy; G. mammography and breast diagnostics; H. nuclear medicine testing; and I. magnetic resonance imaging.
(b) Notwithstanding the foregoing, nothing herein shall prevent Physicians who conduct a medical practice on the Premises from performing outpatient surgeries that do not require general anesthesia, intravenous sedation or the presence of an anesthesiologist or from rendering pathological laboratory or x-ray services for which Tenant has obtained Landlord’s consent pursuant to paragraph 4.1(c); provided that such surgery services, pathological laboratory or x-ray services are the kind usually and customarily provided in a physician’s office, are provided to such Physician’s own patients who are not referred to such Physician for the sole purpose of receiving the same, and are merely ancillary and incidental to such Physician’s primary medical practice and do not constitute the Physician’s primary medical practice or specialty or constitute the predominant services rendered by the Physician to the Physician’s patients.
(c) Prior to providing pathological laboratory or x-ray services, Tenant shall have
submitted to Landlord a detailed description of the laboratory or x-ray services Tenant desires to provide or perform and Landlord shall have consented in writing to the provision or performance of such services, which consent may be denied in Landlord’s reasonable discretion (the provision of such services and procedures shall be strictly limited to those services and procedures to which Landlord has expressly consented in writing and the terms of this paragraph shall be strictly construed to prohibit any expansion or addition to such services or procedures without Landlord’s written consent); provided, however, Tenant shall be permitted to provide pulmonary and/or polysomnography diagnostic or therapeutic testing services, including, but not limited to the use of Continuous Positive airway pressure (CPAP) testing services, Electroencephalography (EEG) and Polysomnogram (PSG) testing services. Tenant shall not dispense any drugs or medicines to persons other than Tenant’s own patients. Prior to the installation of any diagnostic, laboratory or radiology equipment, Tenant shall provide Landlord with a list of such equipment; a list of any hazardous substances, wastes or materials, as hereinafter defined, which will be used or generated in connection with the use of such diagnostic, laboratory or radiology equipment; and Tenant’s proposed procedures for the use, storage and disposal of any hazardous substances, wastes or materials, including but not limited to the procedure for silver recovery for any radiology equipment.

24
4.2. Practice Group Restrictions. In order to preserve the optimum tenant mix within the Building, Landlord and Tenant have agreed to the restrictions set forth in Schedule 4.2 attached to this Lease and made a part hereof.
4.3. Physician Qualifications. All Physicians who conduct a medical practice and
related activities in the Premises must be and remain appropriately licensed and in good standing with the state licensing board and any applicable federal, state or local certification or licensing agency or office. Example 3
Section 18.9 Staff Privileges. Tenant represents that all of the physicians of Tenant occupying the Premises enjoy staff privileges at the Hospital. If, at any time during the Lease Term, all of the physicians of Tenant occupying the Premises cease to enjoy staff privileges at said Hospital at the same time, Landlord may, at its option in addition to any other remedies Landlord may have, cancel this Lease by giving 60 days’ written notice of its intention to do so, and this Lease shall then terminate at the expiration of said 60-day period. The Hospital Parties as well as any other operator of the Hospital are third party beneficiaries of the provisions of this Section 18.9 and shall be entitled to enforce breaches of such provisions directly against Tenant.

25
Sample Ethical and Religious Directive Language Example 1 COMPLIANCE WITH ETHICAL AND RELIGIOUS DIRECTIVES: The parties recognize that Tenant is a member of Ascension Health and that the operation of Tenant's business in accordance with the Ethical and Religious Directives for Catholic Health Care Services, as promulgated by the United States Conference of Catholic Bishops, Washington, D.C., of the Roman Catholic Church or its successor (the "Directives") and the principles and beliefs of the Roman Catholic Church is a matter of conscience to Tenant. Accordingly, no part of the Building or Shopping Center shall be used in a manner that is inconsistent with the Directives. Moreover, it is the intent and agreement of the parties that neither this Lease nor any part hereof shall be construed to require Tenant to violate said Directives and all parts of this Lease must be interpreted in a manner that is consistent with said Directives. [Alternatively] Under no circumstances shall any occupant of any unit owned by Landlord in the building in which the Premises are located perform direct abortion (as hereinafter defined), euthanasia or assisted suicide services. For purposes hereof, "direct abortion" refers to any procedure, device and/or medication whose sole immediate effect or directly intended purpose is the termination of pregnancy by : (i) destroying the developing human embryo or fetus at any stage after conception; (ii) expelling the embryo or fetus before viability; or (iii) preventing the embryo from implanting. "Direct abortion" includes, in the context of assisted reproductive techniques, the creation of more embryos than could be implanted at once. For purposes of this definition, the term "embryo" shall include the stage of development beginning at conception and continuing through the eighth week of gestation. The term "fetus" shall include the stage of development beginning with the ninth week of gestation and continuing through the remainder of the pregnancy. "Direct abortion" does not refer to an operation, treatment or medication that: (i) has as its intended purpose and direct effect the cure of a proportionately serious pathological condition of a pregnant woman; (ii) cannot be safely postponed until the fetus is viable; and (iii) may result in the unintended but foreseen death of the embryo or fetus (the death of the embryo or fetus under the circumstances described in clause (i), (ii) and (iii) would constitute an "indirect abortion"). In addition, Landlord covenants that it will not consent to the performance of direct abortion (as defined above), euthanasia or assisted suicide in or at any portion of the building in which the Premises are located and that performance of such acts is not permitted under leases of any portion of the building in which the Premises are located.

26
Example 2 Section 16. ETHICAL CONSIDERATIONS. Unless otherwise required by law, Lessee will require physicians under its jurisdiction, in respect to such physicians’ medical practice in the leased premises, to observe the ethical directives of the Roman Catholic Church required of members of the medical staff of Hospital in their practice in said hospital. Example 3
Section 1.1 Ethical and Religious Directives. The Leased Premises shall not be used in a manner that is inconsistent with the Ethical and Religious Directives for Catholic Health Care Services as approved, issued and amended from time to time by the United States Conference of Catholic Bishops, Washington, D.C., of the Roman Catholic Church or its successor.

27
Sample Environmental Compliance Language
Example 1
Section 15. Hazardous Materials.
(a) Generally. Tenant shall comply with all environmental laws, regulations and ordinances and shall not, except as hereinafter provided, cause or permit substances or materials defined as hazardous, toxic or environmentally unsafe under any governmental law, regulation or ordinance ("Hazardous Materials") to be brought upon, kept or used in, on, or under or about the Premises or the Real Property, without the prior written consent of Landlord, except that Landlord's consent shall be unnecessary for those items constituting Hazardous Materials stored, sold or used by Tenant in the ordinary course of Tenant's business. Tenant shall cause the use and storage of such Hazardous Materials brought upon, kept or used by Tenant in or about the Premises to comply with all environmental laws, regulations and ordinances. Without limiting the foregoing, if the presence of any Hazardous Materials on the Premises brought upon, kept or used by Tenant results in any contamination of the Real Property, Building or the Premises, Tenant shall promptly take all actions, at Tenant's sole expense, that are necessary to comply with all environmental laws, regulations and ordinances. If Tenant breaches the obligations stated in this Section 15 or if the presence of Hazardous Materials brought upon, kept or used in the Premises by Tenant results in contamination of the Real Property, Building or the Premises, then Tenant shall indemnify, defend and hold harmless Landlord from and against any and all claims, demands, losses, expenses, damages, liabilities, fines, penalties, charges, administrative and judicial proceedings and orders, judgments, remedial action requirements, enforcement actions of any kind, and all costs and expenses incurred in connection therewith which arise (prior, during or after the Term) as a result of Tenant's breach of this paragraph or such contamination. Tenant's obligations hereunder shall survive the termination or expiration of this Lease.
(b) Potentially Infectious Medical Waste. Tenant, shall be responsible, at
Tenant's sole cost and expenses, for the proper handling, storage and removal of potentially infectious medical waste generated in the Premises, and Tenant shall provide incineration or other proper disposal. Tenant's failure to properly dispose of such waste or failure to comply with environmental laws, regulations and ordinances shall be deemed a default hereunder. Tenant hereby agrees to indemnify, defend and hold harmless Landlord from and against any claims, liabilities, damages and suits arising in connection with potentially infectious medical waste used or generated in Tenant's medical practice. Tenant's obligations hereunder shall survive the termination or expiration of this Lease. Additional terms are set forth in Rider 1 Infectious and Hazardous Waste attached hereto and made part hereof.
28
RIDER 1
INFECTIOUS AND HAZARDOUS WASTE
1. Hazardous Material is defined as any solid; liquid or gas that is capable of producing
harmful affects on humans or the environment. This material can be ignitable, corrosive, reactive or toxic. Hazardous materials become hazardous waste after they have been used. Used needles and syringes are hazardous waste.
2. Infectious waste is defined as any waste that contains pathogen or is capable of
producing an infectious disease. This definition requires a consideration of the factors necessary for induction of disease which include:
A. Adequate dose B. Resistance of host C. Portal of entry D. Presence of a pathogen and virulence
Therefore, for a waste to be infectious, it must contain pathogens with sufficient virulence and quantity so that exposure to the waste by a susceptible host could result in an infectious disease.
3. Infectious medical wastes are those wastes capable of causing disease. The categories
of medical waste include the following:
A. Cultures and Stocks - Cultures and stocks of agents infectious to humans, and associated biologicals. For example: cultures from medical laboratories; waste from the production of biologicals; discarded live and attenuated vaccines, and culture dishes and devices used to transfer, inoculate and mix cultures.
B. Pathological Wastes - Human pathological wastes. For example: tissue, organs and body parts (except teeth and the contiguous structures of bone and gum), and body fluids that are removed during medical procedures and specimens of body fluids and their containers.
C. Blood and Body Products - Discarded waste human blood and blood components (e.g. serum and plasma) and saturated material containing free flowing blood and blood components.
D. Sharps - Discarded sharps used in human patient care, medical research or clinical or pharmaceutical laboratories. For example: hypodermic, I.V., and other medical needles; hypodermic and I.V. syringes; Pasteur pipettes; scalpel blades; blood vials; and broken or unbroken glassware in contact with infectious agents, including slides or cover slips.
E. Unused Sharps - Discarded hypodermic, I.V. and other medical needles, hypodermic, I.V., syringes, and scalpel blades. Unused sharps should be considered part of infectious medical wastes as it is often difficult to determine if they have been used.

29
4. Infectious waste will be separated from other waste by containing it in disposable red
plastic bags/containers which are impervious to moisture. 5. Needles and sharps must be contained in disposable rigid containers which can be
sealed with a tight fitting lid. 6. All spills of infectious waste should be wiped up immediately, using the Spill Kit.
Specific instructions are included in the Spill Kit package. 7. Any spillage, or injury from handling infectious wastes must be reported to the
Landlord and an incident report will be filed. 8 . Specific Disposal Instructions: Tenant shall, at Tenant's cost and expense, be solely responsible for proper containment and disposal of all infectious and/or biomedical waste. Tenant shall be responsible to contract for licensed services to handle and dispose of infectious and/or biomedical waste. Such services shall comply with all applicable Federal, State, or Municipal laws, regulations and guidelines. Example 2
6.3. Medical and Hazardous Waste. (a) Any Hazardous, toxic, infectious or dangerous substances lawfully permitted and generally recognized as necessary and appropriate for healthcare or medical use may be stored and used on the Premises so long as (i) such storage and use is in the ordinary course of Tenant's business permitted under this Lease; and (ii) such storage and use is performed in compliance with all applicable laws and in compliance with commercially reasonable standards prevailing in the industry for storage and use of such materials. Tenant, at Tenant’s sole cost and expense, shall be responsible for Hazardous, toxic or infectious waste removal for the Premises and the maintenance and storage thereof pending removal, all in accordance with all applicable laws, regulations and orders. Tenant shall not cause or permit the release or disposal of any Hazardous substances, wastes or materials, or any medical, special or infectious wastes, on or about the Premises or the Building. "Hazardous substances" as such term is used in this Agreement means any Hazardous or toxic substance, material or waste, regulated or listed pursuant to any federal, state or local environmental law, including without limitation, the Clean Air Act, the Clean Water Act, the Toxic Substances Control Act, the Comprehensive Environmental Response Compensation and Liability Act, the Resource Conservation and Recovery Act, the Federal Insecticide, Fungicide, Rodenticide Act, the Safe Drinking Water Act and the Occupational Safety and Health Act. Tenant shall comply with all rules and policies set by Landlord, and with all federal, state and local laws, regulations and ordinances which govern the use, storage, handling and disposal of Hazardous substances, wastes or materials and medical, special or infectious wastes. Tenant shall indemnify, defend and hold Landlord harmless from and against any claims or liability arising out of or connected with Tenant’s failure to comply with the terms of this Section 6.3, which terms shall survive the
30
expiration or earlier termination of this Lease. If Landlord decides to provide medical, special and infectious waste removal services for its tenants (which decision may be made in Landlord’s sole discretion), Tenant may elect to contract separately with Landlord for such services; provided that Tenant shall pay Landlord a reasonable fee for the provision of such service, the amount of which shall be determined by Landlord.
(b) Tenant shall not permit undue accumulations of garbage, trash, rubbish or
other refuse within the Premises and shall keep all refuse in proper containers until disposal of such refuse. Tenant shall not permit the mixing or disposal of any Hazardous substances, wastes or materials or any medical, special or infectious waste with the general office refuse and Landlord shall have no duty or obligation to remove any Hazardous substances, wastes or materials or any medical, special or infectious waste from the Premises (except as provided by separate contract as set forth above in Section 6.3(a)). Example 3
ARTICLE VI HAZARDOUS MATERIALS
Section 6.1 Hazardous Materials. Tenant shall not in any manner use, maintain or
allow the use or maintenance of the Leased Premises in violation of any Laws. Tenant shall not use, maintain or allow the use or maintenance of the Leased Premises or any part thereof to treat, store, dispose of, transfer, release, convey or recover hazardous, toxic or infectious waste nor shall Tenant otherwise, in any manner, possess or allow the possession of any hazardous, toxic or infectious waste on or about the Leased Premises; provided, however, any hazardous, toxic or infectious waste lawfully permitted and generally recognized as necessary and appropriate for medical office use may be stored and used on the Leased Premises so long as (i) such storage and use is in the ordinary course of Tenant's business permitted under this Lease; (ii) such storage and use is performed in compliance with all applicable Laws and in compliance with commercially reasonable standards prevailing in the industry for storage and use of such materials; (iii) Tenant delivers prior written notice to Landlord of the identity of and information regarding such materials as Landlord may require; and (iv) Landlord consents thereto. Hazardous, toxic or infectious waste shall mean any solid, liquid or gaseous waste, substance or emission or any combination thereof which may (according to generally accepted scientific and medical opinion) (i) cause or significantly contribute to an increase in mortality or in serious illness, or (ii) pose the risk of a substantial present or potential hazard to human health, to the environment or otherwise to animal or plant life, and shall include without limitation hazardous substances and materials described in the Comprehensive Environmental Response, Compensation and Liability Act of 1980, as amended; the Resource Conservation and Recovery Act, as amended; and any other applicable federal, state or local Laws. Tenant shall immediately notify Landlord of the presence or suspected presence of any hazardous, toxic or infectious waste on or about the Leased Premises and shall deliver to Landlord any notice received by Tenant relating thereto. The provisions of this Section 6.1 shall, likewise, apply to Landlord with respect to the Building (other than the Leased Premises) and the Common Areas. Each party hereto shall indemnify and hold the other harmless from any and all claims, loss, liability, costs,

31
expenses or damage, including attorneys' fees and costs of remediation, incurred by the other in connection with any breach of the obligations under this Section 6.1. The covenants and obligations of the parties under this Section 6.1 shall survive the expiration or earlier termination of this Lease.
Example 4
10. Environmental. Lessee shall not cause or permit any hazardous or toxic
substances, materials or waste, including, without limitation, medical waste and asbestos ("Hazardous Substances") to be used, generated, stored or disposed of in, on or under, or transported to or from the Premises unless such Hazardous Substances are reasonably necessary for Lessee's business conducted in the Premises; provided, however, Lessee shall at all times and in all material respects comply with all local, state, and federal laws, ordinances, rules, regulations and orders, whether now in existence or hereafter adopted relating to Hazardous Substances or otherwise pertaining to the environment (the "Environmental Laws") and further provided that Lessee shall periodically cause to be removed from the Premises at Lessee's sole cost and expense such Hazardous Substances placed thereon by Lessee or Lessee's agents, servants, employees, guests, invitees and/or independent contractors in accordance with good business practices, such removal to be performed by persons or entities duly qualified to handle and dispose of Hazardous Substances. Without limiting the generality of the foregoing, Lessor acknowledges that the following Hazardous Substances, among others, are required for Lessee's business operations: bleach, cidex, hibiclena, metrocide, hydrogen peroxide, and formaldahyde. Upon the expiration or earlier termination of this Lease, Lessee shall cause all Hazardous Substances placed on the Premises by Lessee to be removed, at Lessee's cost and expense, from the Premises and disposed of in strict accordance with the Environmental Laws.
Articles of Interest












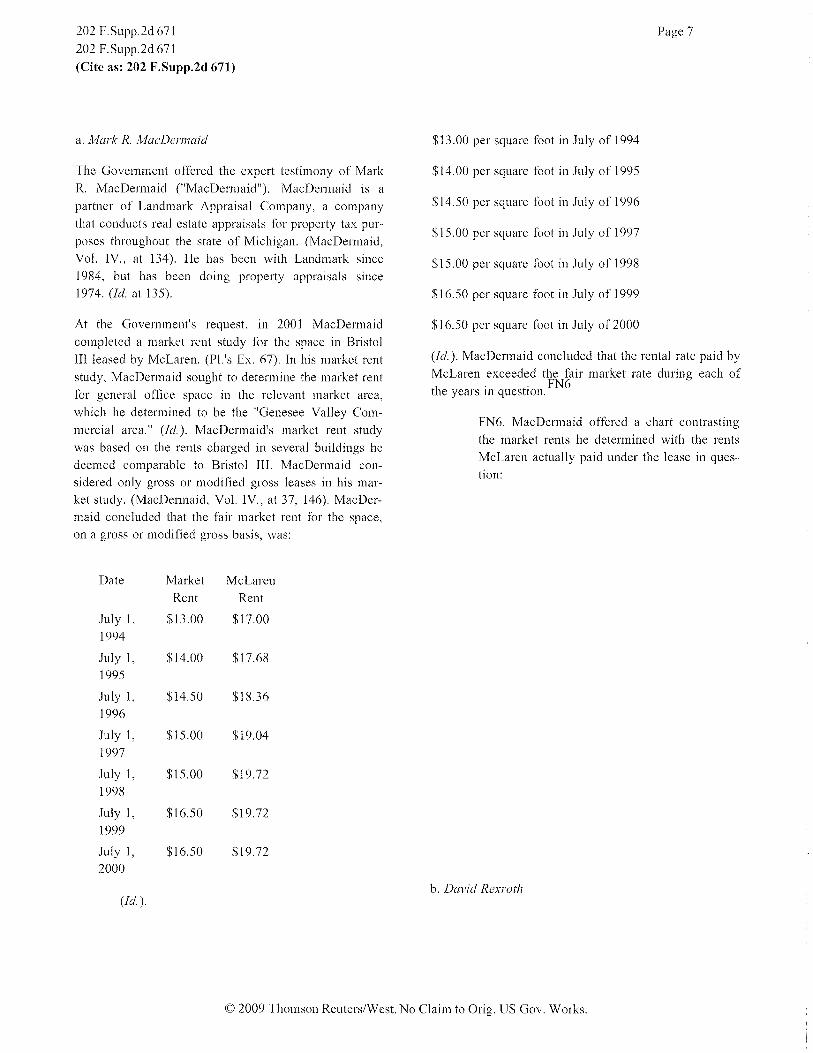












































![Understanding Intellectual Property Law · Understanding Sales and Leases of Goods, Third Edition William H. Henning, William H. Lawrence, ... New Uses of Old Products 57 [d] ...](https://static.fdocuments.us/doc/165x107/5f986df4e300de7e7f00ce00/understanding-intellectual-property-law-understanding-sales-and-leases-of-goods.jpg)

