Medical Microbiology Haemophilus and Bordetella · Bordetella pertussis, the cause of whooping...
31
Medical Microbiology Haemophilus and Bordetella Chapter 31 551-564
Transcript of Medical Microbiology Haemophilus and Bordetella · Bordetella pertussis, the cause of whooping...
-
Medical Microbiology
Haemophilus and Bordetella
Chapter 31
551-564
-
Haemophilus and Bordetella Small, Gram-negative coccobacillary shape.
Exclusively found in humans
The major species are Haemophilus influenzae, the cause of acute purulent meningitis
Bordetella pertussis, the cause of whooping cough.
-
BordetellaGeneral Characteristics
Gram –negative coccobaccili (rod-shaped) single or paired
Obligate aerobe – Requires O2 to live
Colonizes the respiratory tract
Specific to human hosts
7 species, The main species
1. B. pertussis: Whooping Cough (Pertussis)
1. B. parapertussis
2. B. bronchiseptica
-
EPIDEMIOLOGY Pertussis is a major health problem worldwide,
Bordetella pertussis is spread by airborne droplet nuclei and remains localized to the trachobronchial tree.
It is highly contagious, infecting more than 90% of exposed susceptible persons.
-
Virulence Factors Adhesions
1. Filamentous hemagglutinin
(FHA)
2. Pertactin
3. Agglutinogen
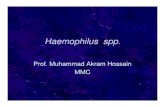
Anchor Bordetella to epithelium
Colonization of tracheal epithelial
cells by Bordetella pertussis
-
Virulence Factors Toxins
1. Tracheal Cytotoxin (TCT)
Direct toxicity to tracheal epithelium
Paralysis of the cilli…mucous build up….trigger violent cough reflex to clear airway
Although considerable local inflammation
and exudate are produced in the bronchi, B pertussis does not directly
invade the cells of the
respiratory tract or spread to deeper tissue sites
-
Virulence Factors Toxins
1. Pertussis Toxin (PTX)
Anchoring it to epithelial surface
Increase level of lymphocytes in blood (T-cells)
Stimulate T cell to divide and inhibit it from leaving
the blood
Increase sensitivity of respiratory tissue to
histamine…. Fluid enter airway
tissue…swelling….hard to breath….classic
whooping sound
-
Virulence Factors Toxins
1. Adenylate Cyclase Toxin (CYA)
Invasive toxin
Activated by host cell calmodulin
Apoptosis, inhibit cell signal, inhibit immune cells
Inhibit phagocytes to get to site of infection and kill
bacteria
-
Pathogenesis Attached to tracheal epithelium
After attachment: bacteria immobilize cilia: destroy ciliated cell
Produce epithelium devoid the ciliary blanket
Persistent coughing
-
Clinical Presentation:
Whooping Cough
Incubation period 4-21 days
3 Stages
1. Catarrhal Stage 1-2 weeks
2. Paroxysmal Stage 1-6 weeks
3. Covalescent Stage weeks-months
-
Clinical Presentation:
Whooping Cough
Catarrhal Stage 1-2 weeks nose, sneezing, low fever, and a mild cough (common mistaken for cold)
Runny nose
Nasal congestion
Red, watery eyes
Fever
Cough
The disease is most communicable at this stage
because large numbers of organisms are present in the
nasopharynx and the mucoid secretions.
-
Clinical Presentation:
2. Paroxysmal Stage 1-6 weeks
whooping cough, which consists of uninterrupted fit of
coughing followed by an inspiratory whooping noise
End with a high-pitched "whoop" sound during the next
breath of air (closed swollen epiglottis)
up to 50 times
a day for 2 to 4 weeks
Severe and prolonged coughing attacks may:
Provoke vomiting
Collapsed lung
Tiny petechial in the face
Hernias
Cause extreme fatigue
-
Children
In infants — especially those under 6 months of age — complications from
whooping cough are more severe and may include:
Pneumonia (superinfecting
organism such as Streptococcus pneumoniae)
Slowed or stopped breathing
Dehydration or weight loss due to feeding difficulties
Seizures
Brain damage
related to the venous pressure effects of
the paroxysmal
coughing and the anoxia produced by
inadequate ventilation and apneic spells.
-
Clinical Presentation:
Whooping Cough
1. Covalescent Stage weeks-months
Gradual recovery starts
Airway heal
-
Laboratory Diagnosis
Gram stain
Isolation by culture
(nasopharyngeal specimens)
Regan-Lowe Agar
charcoal agar incubated at 35/37 °C
for at least 3 days
Growth required special medium with supplement nicotinamide ,additive charcoal to Slow growth 3-7 days
Throat swabs are not suitable because the
cilia to which the organism attaches are not
found there
Specimens collected early in the course of disease
(during the catarrhal or early paroxysmal stage) provide the greatest chance of
successful isolation.
-
Laboratory Diagnosis
Polymerase Chain Reaction (PCR)
Direct fluorescent antibody (DFA)
Bordettela antibodies detection by
ELISA
-
Treatment Once the paroxysmal coughing stage has been reached, the treatment of
pertussis is primarily
supportive.
Antimicrobial therapy is useful at earlier stages
macrolides are preferred for both treatment and prophylaxis.
-
Treatment and Prevention
Antibiotic Therapy
Erythromycin
Azithromycin
Clarithromycin
Pertussis vaccine
Diphtheria, Tetanus, and Pertussis
(DTP) vaccine as early as 6 weeks
but no later than 6 y/o
-
Haemophilus - General Characteristics
Short (1.0-1.5 m) coccobacilli
Aerobic
Non motile
During late 19th century believed to cause influenza
Severe bacterial infection, particularly among infants
Major pathogens for which humans are natural hosts
1. Haemophilus influenzae
2. Haemophilus ducreyi-
-
H ducreyi Induce sexually transmitted diseases (chancroid)
Africa and southeast Asia
Tender papule in the external genetalia that erode and cause painful ulcer
-
Haemophilus influenzae
H. influenza has a polysaccharide capsule
Six different serotypes (a-f) of polysaccharide capsule
95% of invasive disease caused by type b (Hib) which contain polyribose-ribitol phosphate (PRP) capsule
-
Require to use the culture media enriched with blood or blood product
Need exogenous hematin (X factor)
Need nicotinamide adenine dinucleotide NAD (V factors)
-
Epidemiology Transmitted via respiratory droplets, or direct contact
with contaminated secretions.
Normal flora of the human respiratory tract and oral cavity, nasphyarunx (20-80%) non tybable Hi,capsulated strai are not rare
Incidence of invasive disease in children
-
0
5
10
15
20
25
1990 1992 1994 1996 1998 2000 2002 2004
Inc
ide
nc
e
Incidence of Invasive Hib Disease
*Rate per 100,000 children
-
Virulent Factors
Antiphagocytic polysaccharide capsule is the major
pathogenesis factor
Lipopolysaccharide lipid A component from the cell
wall (major role in non capsule strains) ntiphagocytic
effect
All virulent strains produce neuraminidase and an
IgA protease
Lipooligosaccharide (LOS) : toxic to cilli and
respiratory epi
No exotoxins
-
Pathogenesis
Organism colonizes nasopharynx followed by:
1. Local invasion: otitis media and sinusitis (90% NTHi)(OM, sinusitis, chronic bronchitis)
2. Systemic invasion: blood – bacteremia –meningitis, bone, joint
-
Cellulitis
6%
Arthritis
8% Bacteremia
2%
Meningitis
50%
Epiglottitis
17%
Pneumonia
15%
Osteomyelitis
2%
*prevaccination era
Hib Clinical Presentations Pre-vaccination
-
Meningitis
Accounted for approximately
50%-65% of cases in the prevaccine era
Hearing impairment or neurological sequelae in
15%-30%
Case-fatality rate 2%-5% despite of effective
antimicrobial therapy
-
Laboratory Diagnosis Gram stain
Requires 2 erythrocyte factors for growth:
X (hemin) and V (NAD). X & V factors
are released following lysis of RBCs
Culture:
IsoVitaleX-enriched chocolate agar
Small cooci-bacilli gram negative grow on
chocolate agar but not in blood agar
that grow on chocolate agar but not blood agar strongly suggest Haemophilus
-
Laboratory Diagnosis Biochemical tests:
Catalase, oxidase, nitrate reduction
and glucose fermentation all positive
Serological tests for serotyping (anti-a, b..)
-
Treatment and Prevention
Hospitalization required
Treatment with an effective 3rd generation
cephalosporin, or chloramphenicol plus
ampicillin
Prevention by vaccination and reduce risk
factors