Medical issue AUTUMN 2017 · 2 Medical issue AUTUmN 2017 New Osteoporosis Guidelines Released to...
6
New Osteoporosis Guidelines Released to Help Improve Australia’s Bone Health Research Bites: DXA Rates in Men Still Falling Significantly Behind Women Vitamin D and Bone Health News Update New Osteoporosis Guidelines MEDICAL ISSUE AUTUMN 2017
Transcript of Medical issue AUTUMN 2017 · 2 Medical issue AUTUmN 2017 New Osteoporosis Guidelines Released to...

New Osteoporosis Guidelines Released to Help Improve Australia’s Bone Health
Research Bites: DXA Rates in Men Still Falling Significantly Behind Women
Vitamin D and Bone Health
News Update
New Osteoporosis Guidelines
Medical issue AUTUMN 2017
Medical iSSUe autumn 20172
New Osteoporosis Guidelines Released to Help Improve Australia’s Bone HealthOsteoporosis Australia in collaboration with the Royal
Australian College of General Practitioners (RACGP) are
confident that new osteoporosis guidelines released in
March will assist general practitioners to improve the
bone health of Australian patients. The new clinical
guidelines update the previous edition and include
important developments over the past 6 years such as
progress in osteoporosis care, including the introduction
of a new medication, further clinical trial evidence for
existing medications and an expanded evidence base
for other interventions. The new guidelines will provide
general practitioners with the expert guidance needed
to help improve Australia’s bone health.
RACGP President Dr Bastian Seidel said “about
4.74 million Australians over the age of 50 have
osteoporosis or osteopenia and most of these patients
will turn to their GP for support. This is why the new
osteoporosis guidelines provide GPs with timely
and much needed expert guidance to better detect,
diagnose, and manage patients with osteoporosis.
It will take away the ambiguity that has previously been
associated with osteoporosis management.”
It is estimated there will be over 160,000 fractures due to poor bone health in 2017. Osteoporosis Australia CEO Greg Lyubomirsky said “once a patient has broken a bone from a minor incident there is no time to wait. The underlying cause of that break should be investigated urgently and the patient may require treatment to minimise the risk of the next fracture occurring. We also encourage people with risk factors for osteoporosis to speak to their doctor because being pro-active can help prevent that first broken bone.”
The clinical guidelines were updated as a working partnership between Osteoporosis Australia and the RACGP. Osteoporosis Australia project managed a working group of Australian bone health experts, led by Chair of the Osteoporosis Guideline Committee Professor Peter Ebeling AO. The committee reviewed the current evidence and made clear recommendations for the diagnosis, treatment and prevention of osteoporosis. The guideline was then critically reviewed, endorsed and then published by the RACGP.
“Too few people with important risk factors for
osteoporosis are investigated or treated. GPs play a
WelcOme This issue features the announcement of the first revision of the RACGP osteoporosis guidelines. With the rapid progress made in the field of osteoporosis, it was high time to update the old guidelines and provide medical practitioners with a current summary of the evidence. Apart from the useful executive summary and flow-chart, the new guidelines contain a number of evidence-based recommendations for osteoporosis diagnosis and treatment. Importantly, the guidelines now also provide information of how to deal with osteoporosis in patients with breast and prostate cancer, and advice on the use of fracture risk calculators. I encourage you to have a look at the revised guidelines, which are probably the most up-to-date worldwide (at least for the moment). I also urge you read Professor Mason’s brief and concise review on ‘Vitamin D and Bone Health,’ which summarises all you need to know about the ‘sunshine hormone.’
Prof Markus seibel
Medical iSSUe autumn 20173
front-line role in osteoporosis management and these new
guidelines create a real opportunity for improving detection
rates in general practice and reduce the burden of fractures.
Importantly, fewer than 20 percent of patients who sustain
a fracture due to osteoporosis are currently treated, despite
effective treatments being available. So we need to improve
this,” Professor Ebeling said.
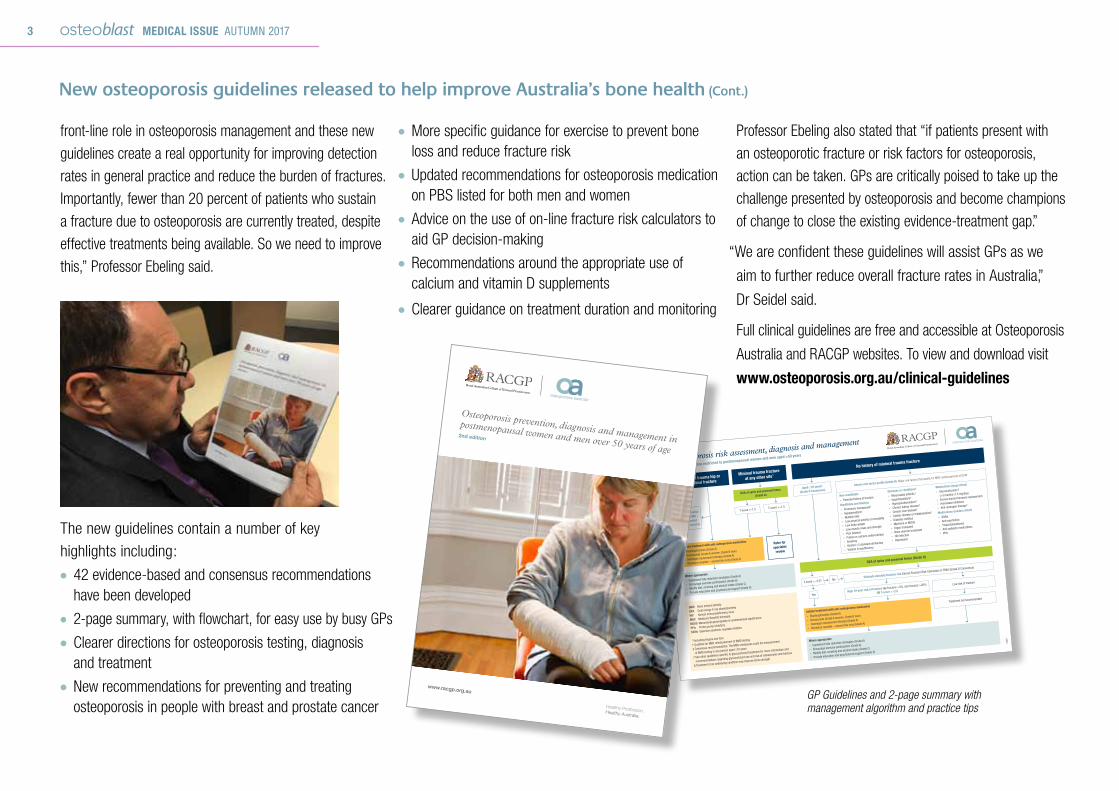
The new guidelines contain a number of key
highlights including: ● 42 evidence-based and consensus recommendations have been developed
● 2-page summary, with flowchart, for easy use by busy GPs ● Clearer directions for osteoporosis testing, diagnosis and treatment
● New recommendations for preventing and treating osteoporosis in people with breast and prostate cancer
● More specific guidance for exercise to prevent bone loss and reduce fracture risk
● Updated recommendations for osteoporosis medication on PBS listed for both men and women
● Advice on the use of on-line fracture risk calculators to aid GP decision-making
● Recommendations around the appropriate use of calcium and vitamin D supplements
● Clearer guidance on treatment duration and monitoring
New osteoporosis guidelines released to help improve Australia’s bone health (cont.)
Assess risk factor profile (Grade B) Major risk factors that qualify for MBS reimbursement of DXA†
Minimal trauma hip or
vertebral fracture
Minimal trauma fracture
at any other site*
No history of minimal trauma fracture
DXA of spine and proximal femur (Grade A)
Osteoporosis risk assessment, diagnosis and management
Recommendations restricted to postmenopausal women and men aged >50 years
Initiate treatment with anti-osteoporosis medication
» Bisphosphonates (Grade A)
» Denosumab (Grade A women, Grade B men)
» Oestrogen replacement therapy (Grade A)
» Strontium ranelate – second line only (Grade A)
Initiate treatment with anti-osteoporosis medication
» Bisphosphonates (Grade A)
» Denosumab (Grade A women, Grade B men)
» Oestrogen replacement therapy (Grade A)
» Strontium ranelate – second line only (Grade A)
Refer for
specialist
review
DXA to establish
baseline BMD –
recommended
but not essential
BMD Bone mineral density
DXA Dual energy X-ray absorptiometry
HIV Human immunodeficiency virus
MBS Medicare Benefits Schedule
MGUS Monoclonal gammopathy of undetermined significance
PPIs Proton pump inhibitors
SSRIs Selective serotonin reuptake inhibitor
* Excluding fingers and toes
† Qualifies for MBS reimbursement of BMD testing
‡ Consensus recommendation. The MBS reimburses costs for measurement
of BMD testing in any person aged ≥70 years
|| See other guidelines specific to glucocorticoid treatment for more information and
recommendations regarding glucocorticoid use and risk of osteoporosis and fracture
§ Treatment of an underlying condition may improve bone strength
DXA of spine and proximal femur
(Grade A) Non-modifiable
» Parental history of fracture
Modifiable and lifestyle
» Premature menopause†
» Hypogonadism†
» Multiple falls
» Low physical activity or immobility
» Low body weight
» Low muscle mass and strength
» Poor balance
» Protein or calcium undernutrition
» Smoking
» Alcohol >2 standard drinks/day
» Vitamin D insufficiency
Estimate absolute fracture risk Garvan Fracture Risk Calculator or FRAX (Grade D Consensus)
Aged ≥70 years‡
(Grade D Consensus) Diseases or conditions§
» Rheumatoid arthritis†
» Hyperthyroidism†
» Hyperparathyroidism†
» Chronic kidney disease†
» Chronic liver disease†
» Coeliac disease or malabsorption†
» Diabetes mellitus
» Myeloma or MGUS
» Organ transplant
» Bone marrow transplant
» HIV infection
» Depression
Medications (large effect)
» Glucocorticoids†||
(>3 months≥7.5 mg/day)
» Excess thyroid hormone replacement
» Aromatase inhibitors
» Anti-androgen therapy†
Medications (modest effect)
» SSRIs
» Anti-psychotics
» Thiazolidenediones
» Anti-epileptic medications
» PPIs
T-score ≤–1.5
T-score ≤–2.5?
T-score >–1.5
No
Yes
Where appropriate
» Implement falls reduction strategies (Grade A)
» Encourage exercise participation (Grade A)
» Modify diet, smoking and alcohol intake (Grade C)
» Provide education and psychosocial support (Grade D)
Where appropriate
» Implement falls reduction strategies (Grade A)
» Encourage exercise participation (Grade A)
» Modify diet, smoking and alcohol intake (Grade C)
» Provide education and psychosocial support (Grade D)
High 10-year risk of fracture Hip fracture >3%, any fracture >20%
OR T-score ≤–2.5
Low risk of fracture
Treatment not recommended
4428
www.racgp.org.au
Healthy Profession.Healthy Australia.
Osteoporosis prevention, diagnosis and management in
postmenopausal women and men over 50 years of age
2nd edition
GP Guidelines and 2-page summary with management algorithm and practice tips
Professor Ebeling also stated that “if patients present with
an osteoporotic fracture or risk factors for osteoporosis,
action can be taken. GPs are critically poised to take up the
challenge presented by osteoporosis and become champions
of change to close the existing evidence-treatment gap.”
“We are confident these guidelines will assist GPs as we
aim to further reduce overall fracture rates in Australia,”
Dr Seidel said.
Full clinical guidelines are free and accessible at Osteoporosis
Australia and RACGP websites. To view and download visit
www.osteoporosis.org.au/clinical-guidelines
Medical iSSUe autumn 20174
dXa Rates in Men still Falling significantly Behind WomenA new analysis of Medicare data has revealed a worrying lack of awareness of fracture
risk in Australian men. Publishing in the December 2016 issue of the Journal of Clinical
Densitometry (doi: 10.1016/j.jocd.2016.10.008), researchers from Sydney’s Garvan
Institute of Medical Research and St Vincent’s Hospital analysed Medicare Item Statistic
reports of DXA scans in males and females between 1995 and 2015, broken down by
age group. In general, the picture is encouraging, with DXA claims increasing steadily in
both men and women over the 20-year period. A jump in claims in 2007 for the over 65s
reflects improvements in Medicare provision – it was in 2007 that all individuals over the
age of 70 became eligible for subsidised DXA. However, the research has highlighted
the continued disparity in bone health management between men and women. Although
male DXA rates have improved over the past 20 years, men are still not being tested
in the same numbers as women. From 2007, more than twice as many women in the
75-84 age group were tested than men of the same age, and in the 65-74 age group,
three times more women were tested.
Interestingly, testing in men aged 85 and over appears to be responsible for a large
proportion of the rise in male testing rates since 1995. This finding is important,
because although men over 85 are at higher individual risk of fracture (as are women),
the bulk of fractures in the male population actually occur in the 65-84 age group,
reflecting male demographic age distribution in Australia. The authors suggest that
increased testing in this very elderly population reflects increasing awareness of high
fracture risk in this age group by health care professionals.
The reasons for the persistently poor DXA overall testing rates in men remain
unclear. The report’s authors suggest a perception by health care professionals that
osteoporosis is uncommon in men, despite data demonstrating that a man of 60 has
a 29% chance of a fracture in his remaining lifetime. Other contributory factors may
be mens’ lower interest in their personal health, social isolation or depression. Specific
educational strategies to target the 65-84 age group – where fracture prevalence is
greatest – may improve osteoporosis awareness and result in better outcomes for men.
researchbitesResearch Review by Dr lisa croucher (OA Scientific Advisor)
Medical iSSUe autumn 20175
With increasing uptake of effective treatments for osteoporosis, it is easy to forget the importance of ‘lifestyle interventions’ – vitamin D, calcium and weight-bearing exercise – in optimising bone health throughout life as well as optimising responses to specific osteoporosis treatments. This article will focus on vitamin D. The basic physiology indicates that vitamin D, actually the hormone made from vitamin D, 1,25-dihydroxvitamin D, is important for active absorption of calcium from the gut. The calcium, of course, has to be ingested in the first place. Dietary calcium, absorbed through the actions of vitamin D metabolites, helps to replace calcium lost each day in the urine, gut and sweat. If this process works well, it means that bone, which is the major store of calcium in the body, does not need to be raided to maintain blood calcium, despite these daily losses.
As people get older, renal losses of calcium become larger and efficiency of calcium absorption in the gut is reduced. At the same time, frail older people and people who need to live in institutions where care is provided, do not get out in the sun much to make vitamin D in skin (there is not much vitamin D in most unfortified foods) and mostly cannot be persuaded to do so, even with assistance.1 They often have a poor appetite, resulting in less than optimal calcium intake (1300mg/day in older people)2 and poor intake of protein, which is also important for bone health. Vitamin D is also a key factor in optimal muscle function, which affects propensity to fall.3
There have been numerous meta-analyses of randomised controlled trials of patients given vitamin D with or without calcium with fractures as the outcome. The consensus views are that the combination of vitamin D and calcium (see physiology above) does have a modest, but significant effect to reduce fractures in older, susceptible people (4-7). Trials involving vitamin D are difficult to do well, since vitamin D is already present in the body. If the person has enough vitamin D, whatever ‘enough’ is, and a target of a minimum of 50nmol/L, higher at end of summer to allow for winter drop is recommended,8 giving more vitamin D will not produce any benefit. Not surprisingly therefore, the best evidence of efficacy in fracture reduction, for vitamin D with calcium come from studies in markedly vitamin D-deficient patients at high risk of fracture.9 There is also evidence that some of the more specific treatments for osteoporosis do not work as well if patients are vitamin D deficient.10 Most of the clinical trials of osteoporosis treatments are undertaken in patients given vitamin D and calcium supplements. Low vitamin D status may increase incidence of hypocalcemia in patients given intravenous bisphosphonate or denosumab, though usually for conditions such as metastatic malignancy, where high doses of these agents are used.11,12
Guidance on vitamin D testing has stressed that only groups at-risk of vitamin D deficiency require investigation, for example: severe lack of sun exposure for cultural, medical or occupational reasons, malabsorption, signs or symptoms of osteoporosis or osteomalacia, hyperparathyroidism, very
dark skin, taking medication known to impact D levels (eg: anticonvulsants) or infants of vitamin D deficient mothers.
When dealing with older or frail people, where advice to go into the sun for brief periods, most days,8 is unlikely to be heeded or practical,1 vitamin D supplements are an alternative. A baseline vitamin D status measurement (actually measuring 25-hydroxyvitamin D (25(OH)D), the major circulating vitamin D metabolite), in at risk patients, may be helpful in monitoring the effect of therapy. Daily treatment with around 1000IU (25mcg) of vitamin D3 (cholecalciferol , the same compound made in skin and the form of vitamin D in nearly all supplements now available in Australia) should be enough to raise 25(OH)D levels to above 50nmol/L, but higher doses may be needed in some patients.8 It takes over 3 months for 25OHD to reach a new steady state in blood after starting supplements or after a change in dose, so there is little point in ordering a follow-up vitamin D assay earlier than this.8
Compliance with vitamin D supplementation, even in clinical trials, is poor.5 For this reason, alternatives to daily vitamin D treatment have been tested. Once yearly high doses of 500,000IU (12,500mcg) did not cause hypercalcaemia, but actually increased the risk of falls with a non-significant increase in fractures, for reasons that are unclear.13 If vitamin D supplements are required and daily dosing is impractical, weekly doses of vitamin D are an option that may enhance the patient compliance. These formulations are now available in Australia.
References available upon request.
Vitamin D and Bone Health Professor Rebecca Mason Head of Physiology, School of Medical Sciences, Sydney Medical School Deputy Director, Bosch Institute
Medical iSSUe autumn 20176
NeWS UPDATe
Resources for General Practice Information and resources for general practice can be accessed online in the GP section of the Osteoporosis Australia website, located under the Healthcare Professional section. www.osteoporosis.org.au
Medical issue AUTUMN 2017
Medical editor: Prof Markus Seibel
editorial: Melita Daru Ainslie Bishop
advertising: Melita Daru
Osteoblast is a publication of: Osteoporosis Australia ABN 45 098 570 515
PO Box 550 Broadway NSW 2007
National office 02 9518 8140 National hotline 1800 242 141
www.osteoporosis.org.au
Copyright © Osteoporosis Australia 2017. Except as provided by the Copyright Act 1968, no part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means without the prior written permission of the publisher.
Reaching General Practice
The start of the new triennium in 2017 and the release of new clinical guidelines for osteoporosis management means the topic of osteoporosis will feature in the scientific programs of large GP conferences around Australia. In particular the HealthEd Women and Children’s Health Update, GPCE Conferences and the RACGP annual conference.
update regarding treatment
Servier are alerting GPs about the change in availability of strontium ranelate (trade name Protos) in Australia. The product will be discontinued permanently and only limited stock will be available worldwide beyond August 2017. The notification recommends that no new patients should be initiated on the treatment. Servier states the decision is not related to a quality of safety issue in Australia or internationally, it is due to a significant reduction in global demand for the treatment (Protos).
World congress breaks record
The World Congress on Osteoporosis, Osteoarthritis and Musculoskeletal Diseases was hosted by the IOF and ESCEO on 23-27 March in Florence. The congress attracted a record number of abstracts and over 4,000 delegates. As part of the congress Professor John Kanis, President of the International Osteoporosis Foundation, presented awards to seven individual members for their dedication to the work of IOF and commitment to advancing education and awareness in their countries and region. The Asia – Pacific award was presented to Professor Kerrie Sanders – team leader of musculoskeletal science, health economics and nutrition at the Institute for Health and Ageing, Melbourne; Honorary position as Principal Fellow at the University of Melbourne and member of the Medical and Scientific Advisory committee of Osteoporosis Australia and the IOF Committee of Scientific Advisors.
The congress was preceded by the bi-annual Worldwide Conference of Osteoporosis Patient Societies representing over 30 countries from all regions and including Osteoporosis Australia. The Know Your Bones consumer program launched by Osteoporosis Australia was featured among other success stories from patient societies. Greg Lyubomirsky, CEO of Osteoporosis Australia said “it is encouraging to see the programs being introduced in other parts of the world and share ideas from what has worked.” Professor Kerrie Sanders
do your patients need information?Direct patients to the Osteoporosis Australia website or tollfree patient info number
www.osteoporosis.org.au1800 242 141