Medical education as an instance of situated learning Tim Dornan, Pim Teunissen, Preeti Shah.
60
Medical education as an instance of situated learning Tim Dornan, Pim Teunissen, Preeti Shah
-
Upload
jayson-tyler -
Category
Documents
-
view
229 -
download
0
Transcript of Medical education as an instance of situated learning Tim Dornan, Pim Teunissen, Preeti Shah.

Medical education as an instance of situated learning
Tim Dornan, Pim Teunissen, Preeti Shah

Outline
• Introductions,• Current trends in medical education,• Situated learning in the medical education
literature,• Two models that instantiate situated
learning within medicine:– Experience Based Learning (ExBL),– Teunissen’s Framework for Understanding
Learning (FUL).

Introductions
Stages of medical education
• Access education,• ‘Undergraduate education’; UG or PG
entry; theory followed by more or less workbased learning in the workplace,
• Postgraduate education; workbased with a more or less explicit instructional component,
• Continuing education/development; variably workbased vs instructional.

MMS: Some facts and figures
• Five major academic or NHS sites,• Staff:
• 27 academic staff, including 1 visiting chair,• 8 doctoral students; 10 medical student
researchers; 7 doctors in training,• 10 contract research staff, • Various affiliates.
• Embedded in:• Primary and secondary care,• UGE, PGE, and CPD.

TeachingEducationresearch
Clinical practice Administration

Communication education
MMSERG
Admission, progression, and achievement
UMAP
Emotional learning
Cultural integration
ReflectiveLearning
Personal & professional development
Cohort studies
Assessment
Technology enhanced enquiry learning
Workplacelearning
Problem/case based
learning

Programmatic research
• Conducting theory-based research,
• Judicious selection of research topics rather than isolated, disjointed research,
• Followed by long-term systematic investigations,
• A series of studies that build and test theories from multiple perspectives.
Bordage 2007

Current trends in medical education
Slowly moving from an individual perspective to a collective
perspective

Ottawa conference 2008
Collective competence– Rethinking the discourse of competence in
the context of teamwork; Lorelei Lingard– Implications for the assessment of doctors;
Paul Hager

Lingard 2008
Individual Cognition
Our dominant learning
theories (adult learning,
reflective learning,
experiential learning) take
the learner as ‘active
agent’ at the centre of the
activity of learning
Bleakley 2006
Collectivist discourse
Competence is
a constantly evolving set
of multiple,
interconnected behaviors
achieved through
participation and
enacted in time and
space

Lingard 2008
Social Learning Theory
The competence of a community emerges through social interaction, shared experience, development of tacit knowledge, and innovation in response to situated needs.
Lave and Wenger 1991; Eraut 2000; Mittendorf 2006

Hager 2008
Under the influence of the mind-as-container metaphor, knowledge is treated as consisting of objects contained in individual minds, something like the contents of mental filing cabinets.”
Bereiter 2002, p. 179

Hager 2008
Crucial assumptions of ‘common-sense’ story shapethinking about learning and assessment in educationalsystems and policy documentsAssumptions such as:• ‘What is learnt is an independent thing or substance’,• ‘Learning is a kind of thing inside of learners’,• ‘Application as movement of a thing (learning) from• place to place’,• ‘Learning as a thing independent of both the learner and
the contexts in which it is acquired and applied’.

Hager 2008
Participation metaphor• Learning through participation in human
practices,• What is learnt is a complex social construction
that subsumes the individual learner,• Learning is no longer independent of the learner,• Learning is inherently contextual; both learning
and the learner evolve as contexts change,• Communal learning important, i.e. learning by
teams or organisations that is not reducible to individual learning.

Hager 2008
Conclusions• Recognise multi-facetted nature of learning,• Learning as a process of becoming, involving
both individuals and groups,• Individual not always the right unit of analysis,• Team work and group practice as hot issues in
medical practice,• What structures facilitate and value both
individual and group learning?

Situated learning theory in the medical education literature

Reviews
Many publications; eg
• Wooliscroft – UG medical education,
• Mann and Kaufman – How theory can inform practice,
• Swanwick – Informal PG learning; ‘From Cognitivism to Culturism’,
• Bleakley – ‘The message from teamworking’.

Four SL research programmes
• Lyon – Sydney, Au. Two papers exploring UG medical students’ learning in operating theatres,
• Sheehan and Wilkinson - Christchurch NZ. Two papers developing a model of workbased PG learning through participation,
• Teunissen et al – Amsterdam and Maastricht, NL. Three papers using multiple theoretical perspectives to understanding PG learning through participation,
• Dornan et al – Manchester, Maastricht, Dalhousie, UK/NL/Ca. Five papers exploring UG workplace learning.

Situated learning within MMS groupUnderstanding contexts, processes, and
outcomes within COPs to strengthen them• Lown, Carroll, Braidman and others; Medical students’ personal and
professional development within a COP,• Sanders, Vaughan, Wass; Cultural integration into a COP,• Pearson, Warren, Lown, Bundy; Emotional learning within COP,• Smithies, Capelli, Boggis and others; How a COP can define ILOs, • Graham, Dornan; Closing the loop between learners’ experiences of
community and teachers’ construction of community,• Shah, Dexter, Dornan; Mapping learning processes within COP in
order to reify and strengthen them,• Woolley, Isba; On-line case discussion within COP,• Regan, Braidman; Facilitated on-line learning within COP,• Shacklady, Smithson; Transitions along developmental trajectories,• Illingworth, Hart and others; Transferring competence within COP,• ExBL ..

Model 1: Undergraduate medical education – in the workplace but
not necessarily workbasedExperience based learning

The 19th century and earlier
The likely youth .. destined for a medical career .. was indentured to some reputable practitioner to whom his service was successively menial, pharmaceutical, and professional
He ran his master’s errands washed the bottles, mixed the drugs, spread the plasters, and finally, as the stipulated term drew towards its close, actually took part in the daily practice of his preceptor – bleeding his patients, pulling their teeth, and obeying a hurried summons in the night.
Abraham Flexner 1910

An academical system without the personal influence of teachers upon pupils, is an Arctic winter; it will create an ice-bound, petrified, cast-iron University, and nothing else
Sir William Osler 1906

Why is situated learning attractive?
• “Our original intention .. was to rescue the idea of apprenticeship”,
• “Learning .. concerns the whole person acting in the world”,
• “LPP does not take intentional instruction to be in itself the source or cause of learning”,
• “LPP is an analytical perspective”,
Lave and Wenger 1991

Why is situated learning attractive?
• “Newcomers (need) broad access to arenas of mature practice”,
• “Deeper sense of the value of participation .. lies in becoming part of the community”,
• Tension between self-replicating social community and one in a constant state of “learning, transformation, and change”,
Lave and Wenger 1991

The practicality of theory
A perspective is not a recipe; it does not tell you just what to do. Rather, it acts as a guide about what to pay attention to, what difficulties to expect, and how to approach problems
Wenger 1998

Expectations of a theory
1. Predict which approaches will be effective,
2. Create a framework for evaluating current practice,
3. Create a framework for new, untested theories,
4. Promote consistency in practice.
Mann 2004 quoting Laidley and Braddock

“Make a difference”
Med
ical
sch
ool e
ntra
nt
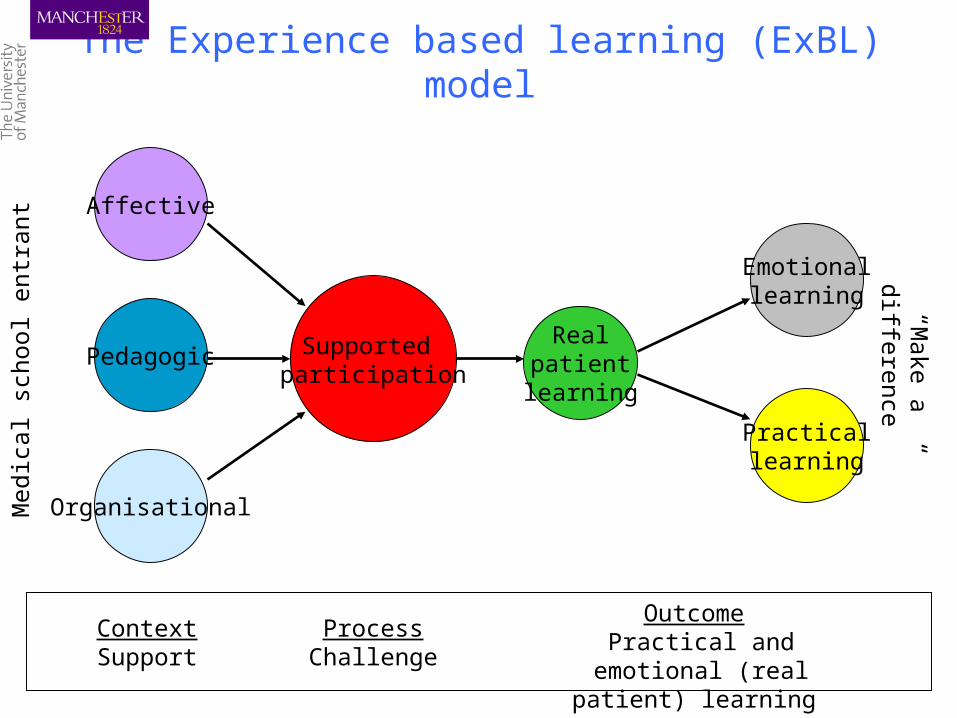
The Experience based learning (ExBL) model

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Participation
The Experience based learning (ExBL) model

“Make a difference”
Med
ical
sch
ool e
ntra
nt
The Experience based learning (ExBL) model
Student
Participation
Doctor
Patient

“Make a difference”
Med
ical
sch
ool e
ntra
nt
The Experience based learning (ExBL) model
Student
Participation
Doctor
Patient
Passive observerActive observer
Actor in rehearsalActor in performance

“Make a difference”
Med
ical
sch
ool e
ntra
nt
The Experience based learning (ExBL) model
Student
Participation
Doctor
Patient
Passive observerActive observer
Actor in rehearsalActor in performance
Stu
de
nt se
nio
rity Ca
se c
om
ple
xity

Doctor
Student Patient
Participation as:Passive observerActive observer
Actor in rehearsalActor in performance

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Participation
The Experience based learning (ExBL) model
Process Challenge

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Participation
The Experience based learning (ExBL) model
Process Challenge
Affective
Pedagogic
Organisational
Context Support

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Interacting positively with students:
Making them welcomeHaving a warm team climate
Drawing students into the teamEncouraging reticent students
Stopping students being “spare wheels”
Not belittlingSharing
The Experience based learning (ExBL) model
Affective support

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Participation
The Experience based learning (ExBL) model
Process Challenge
Affective
Pedagogic
Organisational
Context Support

“Make a difference”
Med
ical
sch
ool e
ntra
nt Making participation possibleFamiliarity with the curriculum
Answering questions despite PBL!Suggesting objectives
Not letting “risk” stand in the way“Teaching” knowledge and skills
Creating tasks
The Experience based learning (ExBL) model
Pedagogic support

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Participation
The Experience based learning (ExBL) model
Process Challenge
Affective
Pedagogic
Organisational
Context Support

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Making placements workCurriculum structure &
sequence Placements that maximise
participationContinuity of attachment
Group sizePlacement timetable
The Experience based learning (ExBL) model
Organisational support

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
The Experience based learning (ExBL) model
Process Challenge
Context Support
Affective
Pedagogic
Organisational

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
The Experience based learning (ExBL) model
Process Challenge
Context Support
Affective
Pedagogic
Organisational
Realpatientlearning

“Make a difference”
Med
ical
sch
ool e
ntra
nt
The Experience based learning (ExBL) model
Real patient learning
Experiencing .. reality
•“Why we’re here”
•“Best way to learn”
•“Seeing things for real”
•“Medicine in action
rather than theory”
•“Linking"
Gaining ..
•Positive feelings
and identity
•Cognitive structuring
and strengthening
•Reality
•(Social) competence

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
The Experience based learning (ExBL) model
Process Challenge
Context Support
Affective
Pedagogic
Organisational
Realpatientlearning
Practicallearning

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Acquiring skillsApplying knowledge
Learning to learn
The Experience based learning (ExBL) model
Practical learning

“Make a difference”
Med
ical
sch
ool e
ntra
nt Learning to learnHow to manage time
How to behave in workplacesWhat to expect from clinical staff
How to handle difficult situationsHow to make sensible choices
How to learn reflectively
The Experience based learning (ExBL) model
Practical learning

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
The Experience based learning (ExBL) model
Process Challenge
Context Support
Affective
Pedagogic
Organisational
Realpatientlearning
Practicallearning
Emotionallearning

“Make a difference”
Med
ical
sch
ool e
ntra
nt
State of mind: Developing a sense of identity
Building confidenceSustaining motivation
Feeling rewarded
The Experience based learning (ExBL) model
Emotional learning
“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
The Experience based learning (ExBL) model
Process Challenge
Context Support
Outcome Practical and emotional (real
patient) learning
Affective
Pedagogic
Organisational
Realpatientlearning
Practicallearning
Emotionallearning

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
Process Challenge
Context Support
Outcome Practical and emotional (real
patient) learning
Affective
Pedagogic
Organisational
Realpatientlearning
Practicallearning
Emotionallearning
The Experience based learning (ExBL) model

“Make a difference”
Med
ical
sch
ool e
ntra
nt
Supported participation
Process Challenge
Context Support
Outcome Practical and emotional (real
patient) learning
Affective
Pedagogic
Organisational
Realpatientlearning
Practicallearning
Emotionallearning
The Experience based learning (ExBL) model

Model 2: Postgraduate medical education – workbased


Perspectives on learning
Blueprints of a building

Towards a conceptual framework
• Research on learning in PME
• Insights from various disciplines
– Legitimate peripheral participation– Communities of Practice– Cognitive Load Theory– Social psychology

Model 2: Workbased postgraduate medical education

From activity to social practices and culture

Individual understanding


Discussion …