Mechanisms of periodontal disease production
33
-
Upload
tago33347 -
Category
Health & Medicine
-
view
241 -
download
1
Transcript of Mechanisms of periodontal disease production


General Considerations
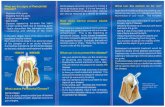
•Bacteria are the primary cause of periodontal disease, but are rarely found in the tissues in chronic periodontitis except during abscess formation.
•Intact Crevicular Epithelium is not permeable to bacteria, but it is permeable to bacterial antigens, metabolites and enzymes.

General Considerations
•In order to cause damage, bacteria must:Colonize the gingival crevice by evading host defences. Damage the crevicular epithelial barrierProduce substances that can either directly or indirectly cause tissue damage.

Evasion of host defences:
Direct damage to PMNS and macrophages ( leucotoxin produced by Actinobacillus actinomycetemcomitans )Reduced PMN chemotaxis ( Porphyromonas gingivalis )Degradation of immunoglobulins ( Capnocytophaga species ) and other anaerobes produce proteases which degrade IgG and IgA )Modulation of Cytokine function:
Cytokines are the major controlling factors of the inflammatory and immune systemsInterleukins ( IL1-10, IFN & TNF) are modulated to function in the favor of certain bacteria (Porphyromonas gingivalis ).

Degradation of fibrin:
Some bacteria possess fibrinolytic activity which reduces the trapping of bacteria by fibrin for surface phagocytosis.
Damage to Crevicular Epithelium:
Factors directly toxic to epithelium are produced by periodontal bacteria, which increases the permeability to bacterial products and eventually to bacteria themselves.
Oral thiols are all toxic by products of anaerobic bacterial metabolism of sulphur containing amino acids ( Cystine, Cysteine and methionine ) that are present in saliva, GCF,

The gingival and periodontal pockets and the tongue surface.
Volatile sulphur compounds comprise:
Hydrogen Sulphide
Methyl mercaptan
Dimethyl Sulphide
Dimethyle Disulphide
Porphyromonas gingivalis, Prevotella intermedia, Bacteroidesforsythus, Fusobacterium nucleatum and Treponema denticolaare all strict gram negative anaerobes that produce volatile sulphur compounds.

• Effects of volatile sulphur compounds in periodontal disease production:They increase the permeability of oral and crevicular epithelia. they impair oxygen utilization by host cells, react with cellular proteins, interfere with collagen maturation and increase collagen solubility, decrease DNA synthesis and proline transport and reduce total protein content of fibroblasts.

Methyl mercaptan incites the secretion of collagenase and prostaglandins from human fibroblasts, stimulates mononuclear cells to produce IL – 1, augment the activity of cathepsin B and converts mature collagen to a compound susceptible to enzymatic degradation.
They are related to the production of oral malodour or halitosis.

The subgingival gram- ve bacteria use proteins for their nutrition and therefore possess proteolytic enzymes to break down proteins to peptides and amino acids which they can absorb:
1- Proteolytic enzymes from putative periodontal pathogens.
Degradation of periodontal tissues by Bacterial enzymes :

Bacteria associated with periodontal disease produce a variety of proteolytic enzymes that participate to tissue breakdown, these include collagenases from P. gingivalis, Actinobacillusactinomycetemcomitans and spirochaetes, an elastase-like enzyme from spirochaetes, trypsin-like enzymes from P. gingivalis, Bacteroides forsythus and T. denticola.

These proteases can degrade all the elements of periodontal connective tissue including collagen types I & IV, elastinbasement membrane, proteoglycans and fibronectin.
they can also degrade components of the host defense systems( immunoglobulin and complement )
2- Hydrolytic enzymes from putative periodontal pathogens.These are produced by P. gingivalis, T. denticola and

F. Nucleatum and they could hydrolyze all the non-proteinaceouselements of the periodontal connective tissue(hyaluronidase & chondroitinase )
Strong acid and alkaline phosphatase activities are present in Porphyromonas, Prevotella and Bacteroides species , which contribute to alveolar bone breakdown.

• It has been proved that this anaerobic bacteria plays a major role in human periodontis.• It expresses tow major proteases : Arg- gingipain ( Arginine specific ) active on fibronectin and laminin Lys- gingipain ( Lysine specific ) active on fibrinogen.When both gingipains work in concert they activate Kallikrein to release the vasoactive Bradykinin, which results in increased GCF production and thus provide a continuous supply of nutrients to the bacterium.
Porphyromonas Gingivalis

Lys gingipain acts on fibrinogen and it thus increases local bleeding time, leading to gingival bleeding.Expression of Arg gingipain renders the P. gingivalis more resistant to phagocytosis by neutrophils due to it’s abilitity to degrade the major opsonin C3 .

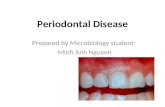
1- Subragingival plague.
2- Subgingival Flora:
- Attached to root surface
- Free within the pocket
- Within radicular cementum or dentin
- Attached to the lining of the pocket
- Within the soft tissue wall of the pocket
Sites of Periodontal Infection

Some bacteria invade cementum and radicular dentine ( p. gingivalis, previotella intermedia, Bacteroides spps ), which suggests that radicular dentine could act as a bacterial reservoir, from which pathogens can recolonize treated periodontal pockets and thus contribute to the recurrence of the disease.P. gingivalis and Actinobacillus actinomycetemcomitans are found most frequently at active sites.
Bacterial penetration

•Bacterial antigens penetrate the crevicular epithelium to enter the tissue and stimulate both arms of the immune system: Activation of the humoral immunity leads to an accumulation of plasma cells and the production of immunoglobulins with subsequent activation of the complement cascade resulting in inflammation and generation of prostaglandins.Stimulation of cellular immunity leads to production of lymphokines from activated T-lymphocytes, which modulate macrophage activity. Activated macrophages release cytokines ( IL-1,TNF & INF)
Role of the immune system in tissue degradation

PMNs:Contain 4 distinct cytoplasmic bodies:-Azurophlic granules contain neutral proteinases ( elastase & cathepsin G )- Specific granules contain (MMP-8 & 9)- C granules contain acid hydrolases (cathepsin B & D )- Secretory vacoules contain plasminogen Activator .
Infammatory cells
Infammatory cells
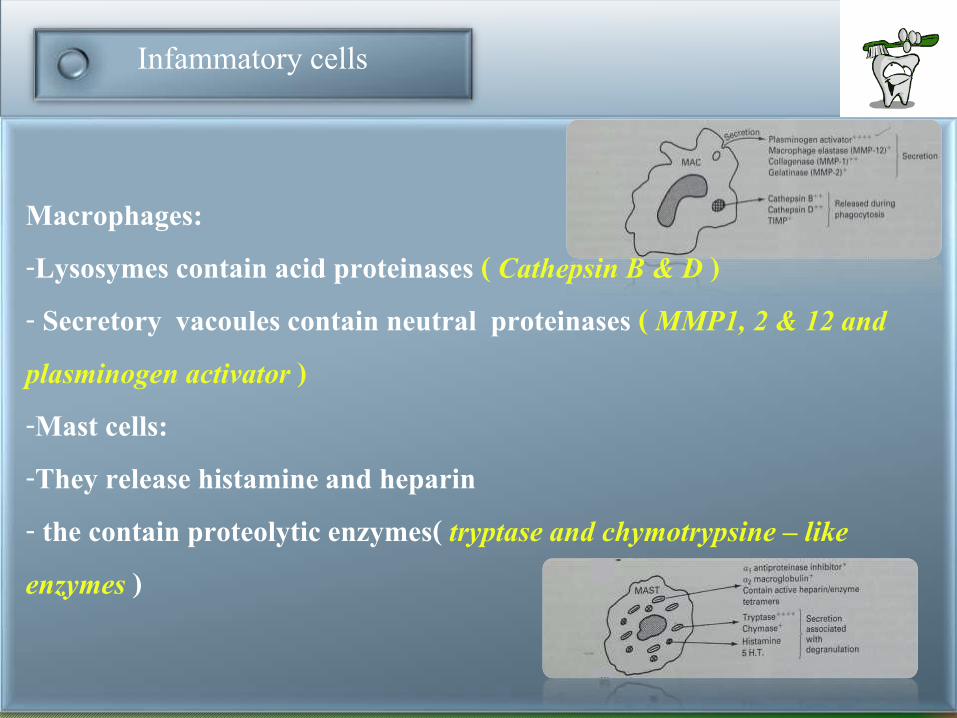
Macrophages:-Lysosymes contain acid proteinases ( Cathepsin B & D )- Secretory vacoules contain neutral proteinases ( MMP1, 2 & 12 and plasminogen activator )-Mast cells:-They release histamine and heparin- the contain proteolytic enzymes( tryptase and chymotrypsine – like enzymes )
Collagen degradation
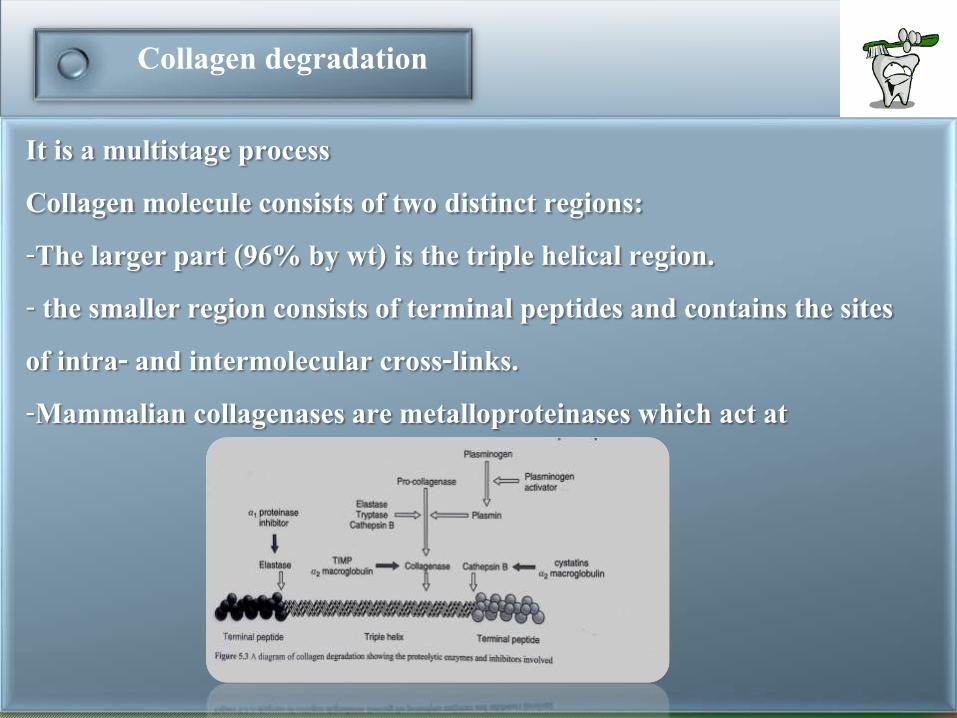
It is a multistage processCollagen molecule consists of two distinct regions:-The larger part (96% by wt) is the triple helical region.- the smaller region consists of terminal peptides and contains the sites of intra- and intermolecular cross-links.-Mammalian collagenases are metalloproteinases which act at

Collagen degradation
neutral PH in the presence of metal ions to cleave the triple helix into two fragments.MMPs 1 & 8 are present in many cells ( inflammatory )and tissues as latent enzymes either as pro-enzymes or enzyme inhibitor complexes.PMNs play major roles in MMPs – mediated destructive lesions.

Bone Resorption
Fibroblasts are found throughout the connective tissue and are the main cells secreting and degrading collagen.Larger amounts of collagen are extracellularly degraded by fibroblasts as a result MMPs secretion.Bone resorption is probably the most critical factor in periodontal attachment deterioration leading to eventual tooth loss.

Bone Resorption
•Substances that can induce resorption in periodontal disease come from two sources:Subgingival bacteriaPeriodontal tissues.Substances from bacteria include lipopolysacchrides, lipoteichoic acid ( actiobacillus) and surface associated material SAM ( g+ve bacteria ).SAM can stimulate the production of prostaglandin E2 and collagenase from bone cells, by first releasing IL1 which then stimulates the release of PGF2 and collagenase.

SAM from A. actinomycetemcomitans is most potent in stimulating bone resorption and it produces this effect by releasing IL6 instead, which directly stimulates osteoclsts.SAM from A. actinomycetemcomitans contains:
Chaperonin: Protein with potent osteolytic activity Gapstatin: Protein with potent anti-mitotic activityPotent cytokine-inducing peptide which act by stimulating IL6
The actions of these proteins are important in the pathogenesis of chronic and juvenile periodontitis, by inducing alveolar bone resorption and inhibiting bone and periodontal ligament regeneration and repair.

Host factors:Eicosanoids: prostaglandins, hydroxyeicosatetraenoic acids (HETES ) and leukotrienes are infammatory mediators derived from cell membrane phospholipids by the action of cyclo-oxygenase or lipo-oxygenase on arachadonic acid.PGS were the first mediators of local bone resorption to be discovered, PGE1,PGE2 and prostcyclin (PGI2 ) all stimulate bone resorptionOther products like Heparin ( from mast cells ) can enhance bone resorption when it works in concert with LPS and Lipoteichoic acid.Out of all cytokines, IL-1 and TNF are the most potent stimulators of bone resorption and are the only ones implicated in perodontitis.

Mechanism of Bone Resorption
-The bone loss in periodontal disease occur at local sites , but is regulated by both local and systemic factors.- Osteoclasts are the main effector cells in the restorative process, but this process couldn’t occur without the presence of both osteoclasts and osteoblasts.-Osteoblasts are involved in the regulation of osteoclasts function at several levels.
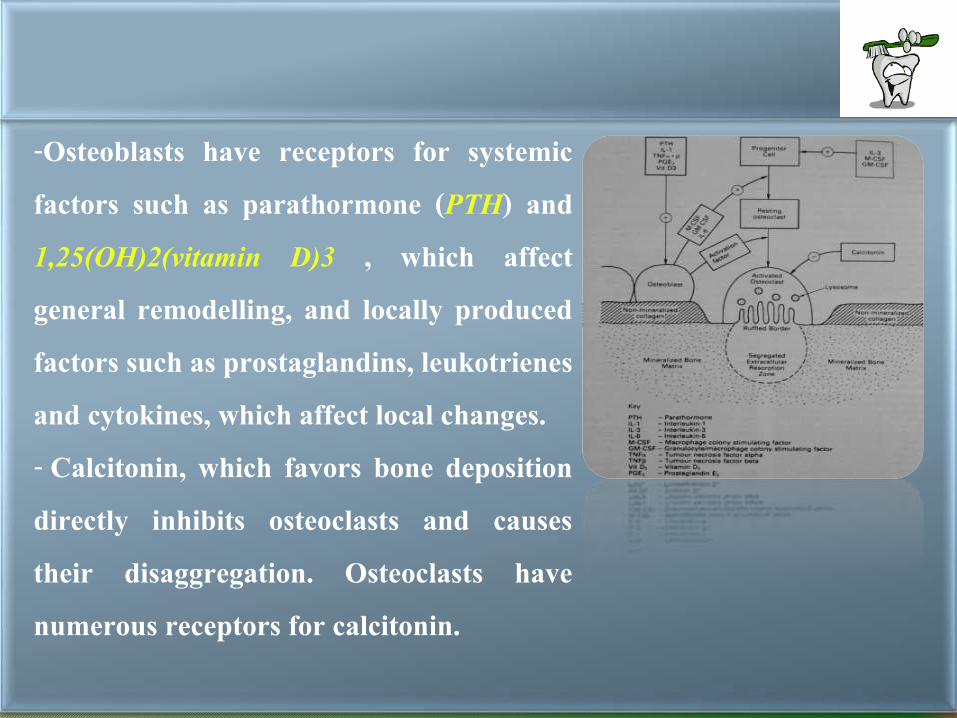
-Osteoblasts have receptors for systemic factors such as parathormone (PTH) and 1,25(OH)2(vitamin D)3 , which affect general remodelling, and locally produced factors such as prostaglandins, leukotrienes and cytokines, which affect local changes.- Calcitonin, which favors bone deposition directly inhibits osteoclasts and causes their disaggregation. Osteoclasts have numerous receptors for calcitonin.

-Stimulated osteoblasts secrete factors that both prepare the bone surface for osteoclastic resorption and stimulate the development of function osteoclasts. -Osteoclast production involves the formation from precursor stem cells in the bone marrow and the migration to
the bone surface, where they remain as pre-osteoclasts until they
receive the appropriate stimulus
-Osteblasts stimulate osteoclasts formation by the secretion of
cytokine and cell-to-cell contact.

- Osteoblasts secrete (GM-CSF) , (M-CSF) and IL-6. IL-6 secretion is stimulated by the attachment of IL-1 to its osteoblast receptor.-IL-6, (GM-CSF), (M-CSF) in concert with IL-3 stimulate the development of precursor cells in the bone marrow.
-The pre- osteoclast divide and fuse into multinucleated osteoclasts, and spread over the bone surface prior to resoprption.- Stimulated osteoblast also secrete pro- collegenase and plasminogenactivator.
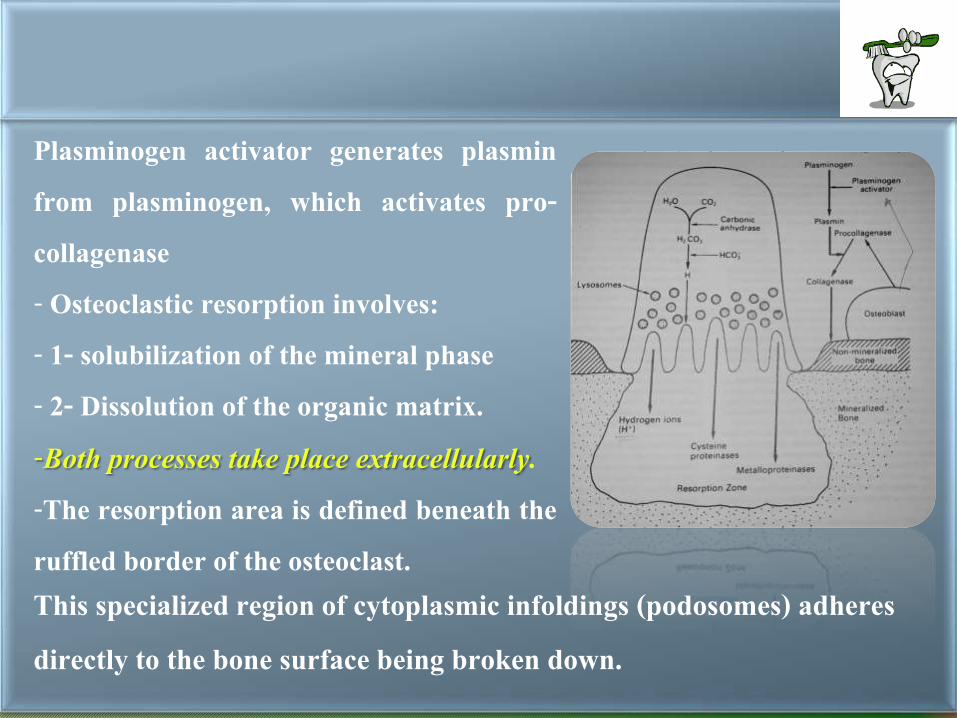
Plasminogen activator generates plasmin from plasminogen, which activates pro-collagenase- Osteoclastic resorption involves:- 1- solubilization of the mineral phase- 2- Dissolution of the organic matrix.-Both processes take place extracellularly.-The resorption area is defined beneath the ruffled border of the osteoclast. This specialized region of cytoplasmic infoldings (podosomes) adheres directly to the bone surface being broken down.

the mineral is dissolved by acid secretion and intracellular PH regulation is achieved by carbonic anhydrase abundant in the osteoclastic cytoplasm.-Bicarbonate, generated by carbonic anhydrase, is secreted from the basal outer membrane via HCO3/CL- exchange.-The hydrogen ions are released into the functionally extracellular lysosomal compartment, where they solubilize the mineral.

-Osteoclasts also produce reactive oxygen species (ROS).-Hydrogen ions and ROS creates a suitable PH for the lysosomal cysteine proteinases(cathepsin B,L & N) which degrade
proteoglycans of the bone matrix and attack the non helical terminal portions of collagen mollecule.-As the PH increases, MMPS become functional and attack the helical portion of the collagen molecule.