MECHANISM RESISTANCEficacy in neurosyphilis andin gonorrhea is estab-lished beyond reasonable doubt...
19
FEVER AS A MECHANISM OF RESISTANCE IVAN L. BENNETT, JR., AND ANTHONY NICASTRI The Johns Hopkins University, School of Medicine, Baltimore, Maryland "Fever is a mighty engine which Nature brings into the world for the conquest of her enemies." This teleological pronouncement by Thomas Sydenham in the seventeenth century was a defi- nite enough expression of his opinion of fever as a mechanism of resistance (1). It was supported by no direct evidence at the time and, in large measure, it remains unsupported. That the febrile response to infectious disease is somehow beneficial has long been one of the tacit assumptions of medicine. As so often happens to traditional beliefs about commonplace natural phenomena, the view that fever is a staunch ally of the patient and his physician in the battle against microbial disease has achieved the status of a dogma. Thus insulated against serious chal- lenge or critical evaluation, it is easily overlooked as a problem meriting scientific scrutiny. Con- sequently, it is a subject considered less and less in the laboratory of the investigator, and more and more in the realm of the turner of neat phrases and composer of aphorisms. For example, Dr. Alan K. Done published recently an excellent article (2) in which he counseled his fellow pediatricians to employ moderation in prescribing antipyretic drugs. He based this advice on strong grounds other than interference with body defences but also quoted the following apt summary by the late Dr. Eugene Dubois: "Fever is merely a symptom and we are not sure that it is an enemy. It may be a friend." (3) Shortly thereafter, Dr. Done's article was sum- marized in a weekly news magazine under the eye-catching caption, "Friendly Fever?" (4). Perhaps a better illustration is to be found in a popular monthly magazine which recently pub- lished an article by a physician entitled, "Fever, the Heat that Heals," with the explanatory sub- heading, 'Your health can depend upon the body's built-in 'oven' which literally burns up disease germs." In it, an explanation of fever's role in resistance (5) is set forth in no uncertain terms: "Germ-damaged body cells are rapidly flushed out to make room for healthy new cell replace- ments and all one's hormones and cell enzymes, now heat activated, hasten the turnover of body chemicals in the struggle. Sometimes fever's nat- ural defending warmth overcomes disease germs simply by burning them out, since many germs cannot live above normal body temperature. Weakened by fever, disease germs become easy targets for the blood's heat-energized antibodies. Moreover, drugs like penicillin have been tested and found to work best against germs at fever warmth." The author concludes with this advice to the reader: "The next time you have a fever, it should be of some cooling comfort to know that your body is automatically on the job, hotly contending with whatever is ailing it. The best way to cooperate with nature and your physician's treatment is to 'play it cool'-take it easy in bed, relax and don't worry. You'll mend quicker that way." PRELIMINARY CONSIDERATIONS Our own investigations of the mechanism and diagnostic significance of fever and those of our associates have not borne directly upon the issue of the febrile response and resistance to infection. Therefore, the present discussion is based upon published reports of others and a few personal communications. From the enormous literature on specific fevers, pyrogens, changes in environ- mental temperature, fever therapy, antipyretic drugs, etc., references have been selected that best illustrate a specific point, that summarize and document in detail one aspect of the problem, or that form a basis for controlled speculation about avenues for further study. Whenever possi- ble, an anthropocentric effort has been made to interpret findings in terms of human disease. Early in the preparation of this review, it be- came obvious that the specific question of fever as a mechanism of resistance has often been con- fused and complicated by failure to separate it clearly from the much broader subject of the in- fluence of temperature upon biological systems in 16 on March 30, 2021 by guest http://mmbr.asm.org/ Downloaded from
Transcript of MECHANISM RESISTANCEficacy in neurosyphilis andin gonorrhea is estab-lished beyond reasonable doubt...
-
FEVER AS A MECHANISM OF RESISTANCE
IVAN L. BENNETT, JR., AND ANTHONY NICASTRI
The Johns Hopkins University, School of Medicine, Baltimore, Maryland
"Fever is a mighty engine which Nature bringsinto the world for the conquest of her enemies."
This teleological pronouncement by ThomasSydenham in the seventeenth century was a defi-nite enough expression of his opinion of fever asa mechanism of resistance (1). It was supportedby no direct evidence at the time and, in largemeasure, it remains unsupported.That the febrile response to infectious disease is
somehow beneficial has long been one of the tacitassumptions of medicine. As so often happens totraditional beliefs about commonplace naturalphenomena, the view that fever is a staunch allyof the patient and his physician in the battleagainst microbial disease has achieved the statusof a dogma. Thus insulated against serious chal-lenge or critical evaluation, it is easily overlookedas a problem meriting scientific scrutiny. Con-sequently, it is a subject considered less and lessin the laboratory of the investigator, and moreand more in the realm of the turner of neatphrases and composer of aphorisms.For example, Dr. Alan K. Done published
recently an excellent article (2) in which hecounseled his fellow pediatricians to employmoderation in prescribing antipyretic drugs. Hebased this advice on strong grounds other thaninterference with body defences but also quotedthe following apt summary by the late Dr. EugeneDubois:
"Fever is merely a symptom and we are not surethat it is an enemy. It may be a friend." (3)
Shortly thereafter, Dr. Done's article was sum-marized in a weekly news magazine under theeye-catching caption, "Friendly Fever?" (4).
Perhaps a better illustration is to be found in apopular monthly magazine which recently pub-lished an article by a physician entitled, "Fever,the Heat that Heals," with the explanatory sub-heading, 'Your health can depend upon thebody's built-in 'oven' which literally burns updisease germs." In it, an explanation of fever'srole in resistance (5) is set forth in no uncertainterms:
"Germ-damaged body cells are rapidly flushedout to make room for healthy new cell replace-ments and all one's hormones and cell enzymes,now heat activated, hasten the turnover of bodychemicals in the struggle. Sometimes fever's nat-ural defending warmth overcomes disease germssimply by burning them out, since many germscannot live above normal body temperature.Weakened by fever, disease germs become easytargets for the blood's heat-energized antibodies.Moreover, drugs like penicillin have been testedand found to work best against germs at feverwarmth."
The author concludes with this advice to thereader:
"The next time you have a fever, it should be ofsome cooling comfort to know that your body isautomatically on the job, hotly contending withwhatever is ailing it. The best way to cooperatewith nature and your physician's treatment is to'play it cool'-take it easy in bed, relax and don'tworry. You'll mend quicker that way."
PRELIMINARY CONSIDERATIONS
Our own investigations of the mechanism anddiagnostic significance of fever and those of ourassociates have not borne directly upon the issueof the febrile response and resistance to infection.Therefore, the present discussion is based uponpublished reports of others and a few personalcommunications. From the enormous literatureon specific fevers, pyrogens, changes in environ-mental temperature, fever therapy, antipyreticdrugs, etc., references have been selected thatbest illustrate a specific point, that summarizeand document in detail one aspect of the problem,or that form a basis for controlled speculationabout avenues for further study. Whenever possi-ble, an anthropocentric effort has been made tointerpret findings in terms of human disease.
Early in the preparation of this review, it be-came obvious that the specific question of feveras a mechanism of resistance has often been con-fused and complicated by failure to separate itclearly from the much broader subject of the in-fluence of temperature upon biological systems in
16
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
general. Therefore, it became desirable to formu-late a set of definitions and limiting conditions forthe inclusion of data purporting to bear uponfever. Although some of these "ground-rules"may seem arbitrary, they were intended and havebeen used only for general guidance of discussionand not as an excuse for caviling or casuistry.We have included in this preliminary discus-
sion several attempts to reason with phases ofthe problem. These "random reflections" (with-out benefit of specific data) may serve as prepara-tion for examining the experimental and clinicalevidence on fever's role in resistance.
1. Fever is defined as an elevation in body tem-perature resulting from disease.
2. The use of artificial fever in animals and inman has yielded important information about apossible role of natural fever in resistance. How-ever, the acceptability of conclusions from ex-periments with artificial fever is dependent uponthe method used to produce elevation of bodytemperature. Mechanical fever from radiantheat, hot baths, fever cabinets, etc., is apparentlyuncomplicated enough. Any supposed effect uponresistance of fever induced by injection of bac-terial endotoxins and related substances cannotbe taken at face value unless it clearly can beabolished by antipyretic drugs. The protectiveaction of endotoxins has been the subject of muchstudy and is independent of their pyrogenic ef-fects (6).
3. Fever might influence resistance to infectionin two ways: (a) By direct thermal effects uponmicroorganisms or their products, or (b) in-directly, by thermal alteration of one or more ofthe various cellular and humoral mechanismsthat are responsible for resistance to infection(and form the subject matter of this symposium).Therefore, we must look carefully at the knowneffects of fever temperatures upon microbes andupon cellular and biochemical activities of thehost.
4. The results of incubation in vitro of micro-organisms at temperatures in the febrile rangecannot alone serve as a basis for conclusions aboutphenomena in vivo in a febrile host. Effects in vivoattributed to elevated body temperature should,whenever possible, be checked by incubation ofthe infecting organism at increased tempera-tures in vitro.
5. The finding that artificial reduction in bodytemperature has an effect upon resistance to an
infecting agent does not justify the conclusionthat fever will have an opposite affect.
6. Normal body temperature is a determinantof host range for many parasites. Much informa-tion on this subject has come from studies ofamphibians, reptiles, and fish, which are con-veniently poikilothermic and do not becomefebrile in the usual sense. Normal body tempera-ture is not fever, however, and caution is neededin transferring observations in these lower formsto the question of fever as a mechanism of resist-ance in warm-blooded species. The range oftemperature change in febrile animals and man isnarrow. A generous scale in man would be 36 to42 C (96.8 to 107.6 F), granting rare exceptionsat either extreme. What conditions must wepostulate for fever to enhance significantly humanresistance to infection? We must first have amicroorganism that can multiply and producedisease, an agent that is pathogenic, at normalbody temperature, say 36 to 38 C (96.8 to 100.4F). Second, the disease must elicit a febrile re-sponse in man. Third, this fever, an elevation ofbody temperature of at most 5 to 6 C, must in-hibit, grievously injure, or destroy the parasite,or must "activate" secondary mechanisms withinthe host somehow capable of modifying the dis-ease process. Obviously, the microbial speciesthat fully meets these criteria is more likely to bethe exception than the rule.
7. If fever is often a significant factor in man'sresistance to microbial invasion, the fact is notimmediately evident from observation of patientswith common infectious diseases. Clinical im-pression, even in its documented form, clinicalinvestigation, offers seeming paradoxes. Milddisease (hence, high resistance) is usually char-acterized and is recognized by low fever. Loweredresistance and extensive disease elicit a higherand more protracted febrile response. Low orabsent fevers in moribund individuals with fulmi-nating infections are more reasonably lookedupon as resulting from rather than causing lowresistance. It is not necessary, of course, to ex-clude all other mechanisms of resistance in con-sidering a possible role of fever. It might be postu-lated that fever is a secondary defense that iscalled upon when other mechanisms falter andthen only in proportion to the body's needs. Ofsuch a suggestion, it can only be said that sup-porting evidence is not yet available. Despitemuch discussion of possible untoward effects upon
1960] 17
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
resistance, reduction of fever by drugs or othermeans has no obvious influence upon the courseor outcome of most infections. Consequently,antipyresis is widely used; indeed, it is more oftenprescribed than not. It seems justifiable to harbora strong suspicion that fever's role in man's resis-tance, if any, is trivial.
8. The results of fever therapy deserve examina-tion if for no other reason than that they are amajor factor in the tenacity of our belief in feveras a mechanism of resistance. The exorbitantand ill-founded claims that have been made fortherapeutic fever form a large, confusing, andentirely separate subject (6). However, its ef-ficacy in neurosyphilis and in gonorrhea is estab-lished beyond reasonable doubt (6-12). On thisbasis, can fever be regarded as a mechanism ofresistance to these two diseases which are ordi-narily accompanied by little or no fever? To doso seems as unreasonable as it would be to lookupon the prophylactic or therapeutic administra-tion of penicillin as a "mechanism of resistance"to group A streptococcal infection. One couldmake an attempt to assign fever a role in resist-ance by speculating that it might be an im-portant factor in the high rate of spontaneousarrest in syphilis (13, 14). Neurosyphilis or othertertiary stigmata perhaps occur only in those fewunfortunate individuals in whom the years of thelatent period are punctuated by an insufficientnumber of intercurrent febrile illnesses. This sug-gestion seems a trifle far-fetched, but it is a mildexample of the type of jumping to conclusionsthat the question of fever and resistance has in-spired for nearly 300 years.
Effects of Fever upon the Host
General elevation of body temperature is ac-companied by many changes, including an in-crease in metabolic rate of 7 per cent per degreeFahrenheit. Alterations that are difficult to relatedirectly to resistance have been summarized inmany reviews (6, 15) and include slight changesin carbohydrate metabolism (16-22) plasmaproteins (23, 24), iron absorption (25), vitaminrequirements (26-29), liver function tests (30),electrolyte balance (31, 32), sensitivity to drugs(33, 34), and others (35-38). The pathologicalchanges that have been described in fatal hyper-thermia (39-41) shed no light on the problem be-fore us.
There are certain alterations in circulating
leucocytes, usually mild leucopenia followed byleucocytosis, in artificial fever (42-47); that theseare of any particular significance in resistance isnot evident at present. Some claims for increasedphagocytic power of the leucocytes from febrileman or animals are based on trivial changes orare unfounded (48). An exception is the convinc-ing demonstration by Ellingson and Clark (49)that phagocytosis of staphylococci by guinea pigleucocytes in normal serum is maximal at 39 to41 C and by leucocytes in human blood at 38 to40 C. In both systems, the phagocytosis in vitroof this organism was lessened by temperaturesbelow or above these ranges. Acute phase proteinappears in human serum after induction of feverwith bacterial endotoxin but this is hardly at-tributable to the febrile response itself (50). De-scriptions of bactericidal substances for meningo-cocci and paratyphoid bacilli in the serum ofnormal and of febrile patients have been based onmethods so inexact that the interpretation of theirsignificance is not possible (51-53). Increasedtiters of these materials in afebrile patients withcirrhosis and malignant disease and low or absenttiters in patients febrile with brucellosis or in-fluenza suggest that fever alone is not an impor-tant determinant of serum levels (53).When the body temperature of dogs is raised,
an increase in adrenal vein and peripheral bloodlevels of 17-hydroxycorticosteroids occurs andhypophysectomy eliminates this reaction (54, 55).Without detouring into the extensive controversyover the role of adrenal steroid hormones in re-sistance to infection, it can be pointed out that apart of this increase is attributable to the increasein general metabolism of the fevered host. Whilethis may be desirable and beneficial, it is hardlyan argument for fever as a mechanism of resist-ance and will not be discussed further here.
HypersensitivityIt was shown by Gernez and Eloire (56) and
by Vallery-Radot et al. (57, 58) in 1936 thatelevation of body temperature by physical meansexerted a very definite but not absolute protectionagainst anaphylactic shock in sensitized guineapigs. This phenomenon has been rediscoveredseveral times (1, 59), but the importance of sup-pression of anaphylactic sensitivity in resistanceto infection is questionable. Induced fever willprevent the development of eezematoid skin sensi-tivity to turpentine in guinea pigs (60). Of more
18 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
interest is the observation that suppression oftuberculin skin reactivity in infected guinea pigssubjected to low temperatures is unaccompaniedby any change in the character and extent of thelesions of tuberculosis or survival time of theanimals (61).
It has been claimed that artificial feverpermitted the administration of large doses ofarsenicals to human patients who were hyper-sensitive to these agents (33). However, themaximal tolerated dose and minimal lethal doseof mapharsen for rabbits are actually reduced byartificial fever (62, 63).
Antibody Formation
There have been many claims and speculationsabout fever and the specific immune response (64,65). The effect of alterations of body temperatureupon antibody production actually has beendetermined for only a few systems. In rats, hypo-thermia amounting to a decrease in body tempera-ture of 5 C markedly reduced hemolysin produc-tion for sheep erythrocytes (66, 67). Animalswarmed to normal showed normal antibody pro-duction. Unfortunately, the effects of hyper-thermia on this system were not studied.
Rabbits submitted to artificial hyperpyrexiashowed a definite decrease in circulating comple-ment and in bacterial agglutinins; with prolongedor repeated fever, detectable agglutinins some-times disappeared entirely (68, 69). The detailedstudies of Ellingson and Clark (49) show clearlythat elevation of body temperature in rabbitsdoes not accelerate the immune response to sheeperythrocytes, egg albumin, or to typhoid bacilli.Indeed, very high fever impairs active immuniza-tion and accelerates the decline of antibody titersin passively immunized animals. No significanteffect of fever upon the complement content ofrabbit serum could be elicited by these investi-gators. However, a careful study of 15 patientssubjected to repeated fevers induced by physicalmeans showed no change in levels of circulatingcomplement or agglutinating and opsonizingantibodies (70). Koomen and Morgan (71) showedconclusively in man that fever per se elicitedno anamnestic response of serum antibodies forbacteria or influenza virus and that the recallphenomenon depended solely upon contact withhomologous or closely related antigens. There isgeneral agreement about the specificity of the
antigenic stimulus in anamnesia and fever aloneis not a factor in the reaction.We have been able to find only a single study
upon the influence of induced fever upon serologicresponse of man to inoculation of a standardantigenic stimulus. This report, by Hayashi (72),describes a potentiating effect of fever upon theproduction of neutralizing antibody by JapaneseB encephalitis vaccine. However, the pyrogenicstimulus employed was typhoid vaccine and,unfortunately, neutralizing antibody (or, at least,protective activity for mice against virus chal-lenge) appeared in some sera obtained from con-trol subjects given only typhoid vaccine. No suchactivity was detected in serum from controlsgiven neither the typhoid nor the viral vaccine.Although the subject of this symposium is non-
specific resistance, the effects of body tempera-ture and fever upon the specific immune responsefurnish such an excellent example of the dif-ficulties that accompany attempts to separatefactors in resistance to infection and the easewith which one may draw erroneous conclusionsthat a word about the matter seems appropriate.
Bisset (73) has called attention to a commonrelationship between body temperature and anti-body formation in amphibians, fish, and insects.For example, frogs immunized with killed bac-teria at 8 C do not produce serum agglutininsbut, when they are transferred to an ambienttemperature of 20 C, antibody formation com-mences normally. Frogs immunized at 20 C pro-duce agglutinins; transfer to 8 C is followed byreduction and disappearance of antibodies fromthe serum but rewarming immediately stimulatesfurther antibody production. Allen and McDaniel(74) noted the same train of events in frogs keptat 10 C or at room temperature after inoculationwith sheep erythrocytes. This relationship holdsin freshwater fish and in insects, and similar ob-servations have been made in bats with Trypano-soma equiperdum infection (75). Bisset's con-clusions, that the acquisition of the potential forantibody production is separable from the actualproduction of antibody and that in poikilothermsthe second stage is more affected by temperaturethan the first, seem wholly justified. Of greaterimportance is the explanation that these observa-tions offer for conflicting observations in naturaland experimental infections in amphibia and infish. In general, elevation of temperature in theseforms increases susceptibility to bacterial disease.
191960]
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
Therefore, if antibody production is increased byelevation of temperature and the offensive powerof the microbe is also enhanced, the outcome isdependent upon a delicate balance between thetwo. Factors of time and dose become very im-portant and similar experiments may show in-creased survival or increased mortality because ofpredominance of one of these two mechanisms.An illustration of the situation in warm-blooded
animals is offered by studies on tetanus. In 1907,Ritzmann (76) showed that white mice subjectedto an ambient temperature of 35 C would diewhen given an injection of tetanus spores thatproduced no mortality in mice at room tempera-ture. In 1951, Ipsen (77) showed that mice heldat 35 C were abnormally susceptible to tetanustoxin, dying after doses sublethal for normal miceand surviving for shorter periods than controlsgiven lethal doses. Elevation of temperature then,definitely decreases resistance of mice to chal-lenge with tetanus spores or toxin. However, in alater study, Ipsen (78) immunized mice with fluidtetanus toxoid and held them at 6, 25, or 35 C for2 weeks before challenge with tetanus toxin. Thehighest immunity was present in the group heldat hyperthermic levels, the lowest in the hypo-thermic group. These findings led Ipsen to pro-pose the term immunizability to describe theinherent properties of the host which determinethe intensity of the immune response as dis-tinguished from the factors of resistance whichdetermine the intensity of reaction to infection innonimmune animals.
In the few instances in which complete informa-tion is available, it is clear that any advantagethat fever might give a host in producing anti-body is likely to be offset by the enhanced patho-genicity of the infecting organism. The data aretoo sparse to permit generalization and are usefulonly as a signal to caution in drawing sweepingconclusions.
BACTERIAL INFECTIONS
Many early studies showed that animals main-tained at high ambient temperatures resisted in-fection by pneumococci (79-82), anthrax bacilli(83), staphylococci (81, 84), and other organisms(80, 81, 83). Ruata (85) found that elevatedtemperatures led to high mortality from variousgram-negative bacilli (typhoid, paratyphoid,dysentery, and colon bacilli; Vibrio comma). How-ever, none of these studies offers more than the
crudest indication of an importance of elevationof body temperature in resistance.
Pneumococcal and Streptococcal InfectionsIn 1909, Strouse (86) demonstrated that the
native resistance of pigeons to infection bypneumococci is dependent upon normal bodytemperature. The average rectal temperature of30 pigeons was 41.5 C and this temperature in-hibited growth of most strains of pneumococcitested, killing a few outright. When the bodytemperature of the birds was reduced by ice andinjection of pyramidon (amidopyrine), they be-came susceptible to infection, disease, and death.Indeed, the course of pneumococcal infection insuch birds, according to Strouse, was preciselylike that in mice.
It was not until 1936 that this subject was ex-plored further. In that year, Enders, Shaffer, andtheir colleagues (87-90) studied the curious in-ability of many strains of type III pneumococcusto kill rabbits and found that the virulence ofthese pneumococci for this animal is paralleledby their ability to grow in cultures at 41 C.
In the same year, Rich and McKee (91), in apaper entitled, "The Mechanism of a HithertoUnexplained Form of Native Immunity to theType III Pneumococcus," described elegant ex-perimental observations which show clearly that,given the right set of circumstances, fever can bean important mechanism of resistance. Of theeight type III strains used, only one survived incultures at 41 C and only this strain producedfatal disease in rabbits. The seven "avirulent"strains elicited a consistent series of changes wheninoculated into the skin of the flank. For about24 hr, there was progressive inflammation,grossly and microscopically similar in everyrespect to lesions elicited by so-called virulentstrains. However, on the second day the lesionsbegan to subside and the animals invariably sur-vived. Reinoculation into the opposite flank atthis time was followed by little or no reaction.The rapidity of development of this almost com-plete resistance eliminated the usual mechanismsof specific immunity from consideration. The in-volution of the primary local lesion was found tocoincide with the onset of fever in the infectedanimal. Rabbits given artificial fever were foundto be completely immune to infection of the skinby type III pneumococci. Here then, was an ex-ample of a pathogenic organism which could
20 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
survive at normal body temperature but wasdestroyed in vivo by the temperatures reached inthe animal in which it had elicited febrile disease.
Neither Rich and McKee (91) nor Enders,Shaffer, et al. (87-90) conducted experiments inwhich elevation of body temperature was pre-vented in rabbits with type III pneumococcalinfection. Presumably, however, failure of thefebrile response to occur should convert thedisease into a fatal one. Curiously, in 1943,Muschenheim and his colleagues (92) carried outprecisely this study, although at the time ofpublication of their report, they did not mentionearlier work with the type III pneumococcus andwere apparently unaware of the probable explana-tion for their experimental results. These investi-gators infected rabbits by intradermal inoculationof "virulent" type I pneumococci or "relativelyavirulent" type III pneumococci. The latter wereso termed because they produced a local skinlesion in normal rabbits but never caused death.Infected animals were observed under three setsof conditions: at room temperature, at ambienttemperatures low enough to produce hypo-thermia, or after being given barbiturates in adosage sufficient to prevent or to inhibit greatlythe febrile response to the infection. All animalswith type I pneumococcal infections died. Amongthose inoculated with type III pneumococci,controls at room temperature survived and allsubjected to cooling died. Fever was variable inanimals given barbiturates and survival clearlyparalleled the height of the febrile response.From these observations, Muschenheim and
his coauthors were led to conclude that hypo-thermia's enhancement of lethality in infectionsproduced by "relatively avirulent" microorgan-isms might be a general biological phenomenon.Had they appreciated the crucial relationshipthat exists between body temperature of the rab-bit and "relative avirulence" of type III pneumo-cocci for this animal, it seems unlikely that thisgeneralization would have been implied.
Interestingly enough, the convenience of der-mal pneumococcal infection as an experimentaltool and the availability of the type III pneumo-coccus as the prototype of an avirulent agentled Sanders et al. in 1957 (93) to repeat theexperiments of Muschenheim, employing an un-typed virulent pneumococcus and an avirulenttype III strain inoculated intradermally in rab-bits. Again, prevention of fever by hypother-
mia converted the type III infection into alethal disease. Furthermore, in contrast to mor-tality rates of 40 per cent in rabbits given theuntyped virulent pneumococci and allowed torespond with fever, the institution of hypo-thermia rendered this infection uniformly fatal.While it is not the purpose of the present pa-per to discuss in detail the effects of hypother-mia upon resistance to infection, it must cer-tainly be pointed out that until organismsother than "avirulent" type III pneumococciare used, such experiments can be interpretedonly as confirming the importance of therange of body temperature in rabbits as a de-terminant of this "%virulence" of type III pneu-mococci. Eiseman and his colleagues (94-96) haveshown that prolonged hypothermia results in in-creased survival time and, under appropriate ex-perimental conditions, increased survival rate ofmice with type III pneumococcal peritonitis. Theselection of the type III pneumococcus for murineinfection by this group of investigators appearsto have been fortuitous. However, much of theirpuzzlement (96) over the "opposite effect" re-ported by Sanders et al. (93) is unquestionably aresult of failure to appreciate the role of bodytemperature in the rabbit in determining thecourse of infection by type III pneumococci.
Before leaving the subject of type III pneumo-coccal infection in rabbits, it should be empha-sized strongly that temperature is by no meansthe only determinant of resistance to this disease.The importance of phagocytosis was emphasizedby Rich and McKee (91) and, additionally, theypointed out that the rate of multiplication invivo of avirulent type III strains is slower thanthat of virulent type III strains even during thefirst few hours after inoculation before the onsetof fever. Although the experiments carried out byRich and McKee in benzolized leucopenic rab-bits were incomplete, the results suggest stronglythat in the absence of phagocytosis, fever alonemight not suffice to insure survival in type IIIinfection.
In this connection, unpublished experiments byC. M. MacLeod (personal communication) are rele-vant. Inoculation of the A/66 strain of "aviru-lent" type III pneumococcus intrapleurally wasfollowed regularly by suppurative pleuritis inrabbits. Despite fevers of 104.6 to 107.6 F, thisinfection often spread to the opposite pleura orpericardium. Moreover, cultures of blood and of
19601 21
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
pleural exudate were consistently positive forseveral days. In this circumstance, then, elevationof body temperature does not suffice to eliminatethe type III pneumococcus. Whether this out-come is attributable to the well-known ineffi-ciency of phagocytosis in serous cavities (97) orto decreased vulnerability to heat of microorgan-isms at suppurative foci similar, perhaps, to theirresistance to antibiotics in such areas (98), isspeculative but certainly worthy of additionalstudy.Have these findings any application to type III
pneumococcal infections in man? In 1938, theeffects of artificial fever in two patients with typeIII pneumococcal meningitis and of artificialfever and intrathecal antiserum in a third patientwere reported by Shaffer et al. (99). Although allthree patients eventually succumbed, the numberof organisms in the spinal fluid of one fell from225 million per ml to 200 per ml during 19 hr offever ranging from 105 to 107 F. In a secondcase, the spinal fluid count was 750 thousandpneumococci per ml and after 15 hr of hyper-thermia over 105 F, this had fallen to 5 thousandper ml. In the third patient, sterility of the spinalfluid was achieved and maintained for 36 hr by acombination of artificial fever and intrathecalinjection of antiserum. None of the pneumococcalstrains isolated from the patients in this studywas entirely susceptible to incubation in vitro at41 C and, of course, the almost uniformly fataloutcome of untreated pneumococcal infection ofthe meninges (99) makes this disease a most rigidand demanding test of any therapeutic regimen.To try to obtain some further information on
fever and type III pneumococcal infection in man,we obtained from the files of The Johns HopkinsHospital the records of 51 patients with untreatedlobar pneumonia in every instance shown to beproduced by type III organisms. There were 23recoveries and 28 fatalities in the series. Analysisof the temperature charts was carried out; when-ever a patient had maintained an oral tempera-ture of 104, 105, 106 or 107 F for at least 8 hrduring hospitalization, this was recorded. Table1 summarizes the incidence of these fevers in re-covered and fatal cases. It is readily apparentthat high fevers were far more frequent in pa-tients who died than in those who recovered. Itappears, then, that high fever simply indicatesincreased severity of infection in this disease andthat the febrile response is probably not an im
TABLE 1Incidence of high fevers in 51 patients with untreated
type III pneumococcal pneumonia
Incidence at Rectal Temperatureof:
Patients
104 F 105 F 106 F 107 F
%o % % %oRecovered (23 cases) 65 30 17 0Died (28 cases). 75 57 39 11
portant mechanism of recovery. The difficultiesencountered in trying to separate out any singlefactor influencing resistance in this type of retro-spective study of human disease are so obviousthat they need no discussion here. However, itcan be said that the two groups of patients wereentirely comparable in age, sex, color, and inci-dence of alcoholism (by history). One patient, a31-year-old Negro male, not an alcoholic, had 48hr of fever of 104 to 105 F, 24 hr of 105 to 106 F,and 24 hr of 106 to 107 F, yet succumbed to typeIII pneumococcal pneumonia. Information on theresistance in vitro to heat was lacking for allstrains isolated from these patients.Ritzmann (76), in 1907, found increased mor-
tality in mice kept at 35 C for 1 week and theninfected with streptococci. The studies of Calvinand Mills (100) showed that elevation of environ-mental temperatures increases the susceptibilityof mice to streptococcal disease. Using an inocu-lum that produced a mortality of 40 per centin animals at room temperature, these workersfound that 70 per cent of mice died at high tem-peratures but that all survived if kept in a coldroom. Larson et al. (101) reported that mice heldat high ambient temperature with resulting ele-vation of body temperatures by 3 to 4 F showedgreatly increased susceptibility to pneumococcalinfection. White and Parker (102) had shown thatsulfanilamide's bacteriostatic action against strep-tococei at 39 C became bactericidal when cultureswere incubated at 40 C. Blood levels of this drugare unaffected by fever (103). However, whenLarson and his colleagues (101) treated pneumo-coccal infection in mice with sulfanilamide atroom temperature and at incubator temperature,survival time was shortened by increased heat.In other words, elevation of body temperaturepromoted the infective process to a greater degreetban it did the protective effect of sulfanilamide.
292 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
In discussing or considering the febrile responseas a mechanism of resistance, it is important tonote that mice ordinarily react to bacterial in-fection (and to injection of bacterial pyrogens)with a drop, rather than a rise in body tempera-ture (6, 101, 104). This fact, of course, makes itextremely difficult to transfer experimental re-sults to other species.
Gonococcal InfectionsThe evidence for the efficacy of artificial fever
in the treatment of gonococcal urethritis, ar-thritis, and ophthalmia is excellent (9-12). Sincebefore the turn of the century, fever's benefit hadbeen attributed to thermal destruction of thegonococci. Carpenter and his colleagues (105) re-viewed the evidence for this mechanism of actionand carried out detailed studies of thermal deathtimes of recently isolated and older laboratorystrains of gonococci. The fresh isolates were moresusceptible than the older strains, more than halfof them being killed outright at 40 C for 30 hr.At 41 C, all gonococci were killed within 23 hrand 99 per cent of the organisms failed to survivefor 5 hr. At 41.5 C, 99 per cent were killed in 2hr although 20 hr were required to sterilize allcultures. These careful observations lend cre-dence to the idea of a direct thermal effect offever therapy in gonorrhea. Moreover, they sug-gest that sensitivity in vivo to heat may be greaterthan that of organisms outside the infected host.
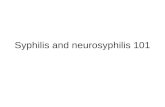
Gonorrheal urethritis and ophthalmia are us-ually afebrile diseases and even in gonorrhealarthritis fever is rarely high enough to be regardedas a mechanism of resistance. In considering thismatter, it occurred to us that high fever is aprominent manifestation of gonococcal infectionof the heart valves (106) but we were unable tofind any published study that would allow con-clusions about the effect of body temperatureupon resistance in this disease. A few cures ofgonococcal endocarditis by exposure in the fevercabinet are on record, but this method was notused in many cases while the disease was seenwith any frequency (107). It is, of course, rarelyencountered at present. However, it is of interestto note that there is a great deal of evidence forthe occasional occurrence of spontaneous recoveryin gonococcal endocarditis. Despite the very con-siderable difficulty of being absolutely certain ofthe diagnosis in any surviving patient, Thayer in1922 (108) and Williams in 1938 (109) analyzed
TABLE 2Febrile response in 48 fatal cases of
gonococcal endocarditis
No. of ResponsePatients Rsos
21 Oral temperatures of 104 F or more forat least 8 hr daily for 2 to 33 weeks.(Mean: 10.5 weeks.)
9 Oral temperatures of 105 F or more forat least 8 hr daily for 3 to 16 weeks.(Mean: 7 weeks.)
Despite an average of 588 hr ot fever above104 F and 392 hr over 105 F, all had positive cul-tures at autopsy.
the published reports and concluded that manyof them were indeed highly suggestive of spon-taneous remission. Because of the fact that pa-tients might undergo bacteriological remissionand still die of cardiac or renal damage, mortalityis a very strict criterion to apply to resistance inthis disease. We have been able to obtain detailedclinical records on 36 fatal cases of gonococcalendocarditis in which autopsy examination wascarried out at the Johns Hopkins Hospital andalso 12 from other sources, including publishedreports. In all of these, adequate bacteriologicalexamination was made at autopsy and, in everyinstance, gonococci were demonstrated in valvularvegetations (table 2). In 21 of the 48 cases, oraltemperature exceeded 104 F for an average of 8hr daily throughout a course ranging from 2 to 33weeks, the mean being 10.5 weeks. In 9 of the 48,oral temperatures averaged more than 105 F for8 hr daily for a mean course of 7 weeks, the rangebeing 3 to 16 weeks. In summary, among 48 fatalcases of gonococcal endocarditis, 21 patientsunderwent "spontaneous" fever therapy averag-ing 588 hr above 104 F and 9 averaged 392 hr offever exceeding 105 F without sterilization ofcultures. None of the infecting strains was testedby heating in vitro, of course. We have been un-able to obtain enough detailed information aboutcases in which spontaneous subsidence of gono-coccal endocarditis has supposedly occurred todraw any conclusion about the height of fever asa factor in them.The rarity of this infection at the present time
and the impossibility of observing patients with-out specific antibiotic treatment makes it doubt-
1960] 29"3
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
ful that this experiment of nature will ever becarried to completion prospectively. An extensivesurvey of past records from several institutionsmight conceivably give a retrospective answer.
Other Bacterial InfectionsAs a result of arguments with Colin, Pasteur
conceived the notion that the native immunity ofthe chicken to anthrax might be attributable tohigh body temperature (110). His demonstrationthat immersion in cold water overcomes the re-sistance of fowls to anthrax is often referred to asa classic example of the importance of tempera-ture in resistance. However, it is altogether prob-able that a proper explanation of Pasteur's resultswould be far more complex, particularly sinceBacillus anthracis, as pointed out by Wagner(111), flourishes in chicken blood or serum incu-bated at 43 C, a temperature higher than that ofthe living fowl.
It is neither feasible nor necessary to cataloguehere the numerous instances in which, on inade-quate grounds, body temperature has been as-sumed to play an important role in resistance tobacterial infection. However, the genetic resist-ance of chicks to fowl typhoid, a disease producedby Salmonella pullorum, illustrates clearly thenecessity for carefully controlled studies beforeaccepting the assumption that body temperatureand immunity are causally related. In 1942,Scholes and Hutt (112) noted that the averagebody temperature of chicks that were geneticallyresistant to S. pullorum was somewhat higherthan that of susceptible strains during the first 10days after hatching. This led to the conclusionthat body temperature was of major importancein the difference in susceptibility. Severens andhis co-workers (113) also noted higher body tem-peratures in resistant strains of chicks but wereunwilling, on the basis of this evidence alone, toaccord it much significance. The studies of Bellin 1947 (114) certainly settled the question. Uti-lizing resistant and susceptible inbred strains ofchicks, Bell first showed that there was no signifi-cant difference in body temperature betweenthem. The resistant chicks survived challengewith a number of bacilli 1000 times greater thanthe dose that produced a mortality rate of 90 percent in the susceptible chicks. Survival amongresistant chicks was unaccompanied by feverwhereas high fever was characteristic of the in-fection in the susceptible strain. Finally, the
febrile response of chicks which died within 10days after inoculation was consistently greaterthan that in chicks which expired after the 10thday. In other words, temperature played no partin the genetic resistance to S. pullorum and, insusceptible chicks, the height of fever was merelyindicative of severity of infection. These experi-ments by Bell are representative of the type ofstudy that is greatly needed before firm conclu-sions will be permissible about temperature andresistance for many other bacterial infections.
CRYPTOCOCCAL INFECTIONS
The experiments of Kuhn (115) showed thatCryptococcus hominis multiplied in vitro at 99 Fbut at 103 F decreased rapidly, some 85 per centof the inoculum dying within 5 days. Suggestingthat this difference might account for the uniformsusceptibility of mice and the relative resistanceof rabbits to experimental cryptococcosis, Kuhncarried out further studies (116, 117). He foundthat mice, whose rectal temperatures averaged99.1 F, died regularly after inoculation, whereasrabbits, whose rectal temperatures averaged 103.1F, were rarely affected. Furthermore, mice keptat ambient temperatures sufficient to raise rectaltemperature to more than 102 F lost their sus-ceptibility, living longer than controls or surviv-ing challenge inoculations completely. Theseexperiments were repeated by Kligman andWeidman in 1949 (118) and, of course, fevertherapy for the human disease was suggested,particularly since human cryptococcosis is oftenaccompanied by negligible fever. However, Mos-berg and Arnold (119) reported no benefit intwo patients with cryptococcosis treated with ar-tificial fever.Here the matter of fever as a mechanism of
resistance to mycotic disease rests at present.
MYCOBACTERIAL INFECTIONS
The probable role of high body temperature inthe natural resistance of birds to human strainsof tuberculosis was pointed out by Rich (120).Aronson (121) has reviewed in detail the nowfamiliar influence of body temperature upon thehost range of mycobacteria in amphibians, fish,and reptiles. We are unaware of any instance inwhich it has been shown that a change in bodytemperature resulting from fever has influencedresistance to mycobacterial infection in warm-blooded animals. However, Fermi and Salsano
24 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
reported in 1892 (122) that the resistance ofguinea pigs to an avian tubercle bacillus waslowered by maintaining the animals at high am-bient temperatures (91 to 95 F) for several weeks.Although it represents a digression from the
main topic, fever and resistance, a brief discussionof the influence of normal body temperature uponcertain mycobacterial diseases of man seemsworthwhile. In 1948, MacCallum et al. (123) andFenner and Leach (124) described the isolation,of Mycobacterium ulcerans from 6 patients withsevere ulcerations of exposed skin surfaces. Therewas no tendency for the infection to spread sys-temically and the lesions responded to total ex-cision, followed by grafting. This bacterium willnot grow in vitro at 25 C and grows poorly or notat all at temperatures of 37 C and above; theoptimal growth range is 30 to 33 C. It is alto-gether probable that the dermal localization ofdisease produced by this bacillus is directly at-tributable to its temperature requirement.A similar but clinically less severe ulceration of
the skin is produced by Mycobacterium balnei, the'swimming pool bacillus." The properties of thisorganism are well described by Linell and Nor-den, its discoverers (125). M. balnei can be culti-vated at 31 C, but fails to grow on most mediaat 37 C. Inoculation of cultures into several ani-mal species elicited results that seem to confirmcompletely the importance of temperature in de-termining the extent of disease produced. Theonly lesions observed in guinea pigs occurred inmales and consisted of scrotal ulcerations. Oc-casional skin lesions were noted in rabbits ofeither sex, but scrotal lesions characteristicallyfollowed parenteral inoculation of male rabbits.Chickens were unaffected. Intraperitoneal inocu-lation of mice or hamsters was followed by ulcera-tions of the tail, scrotum, nose, and footpads. Inmany animals, these healed after several weeks;rarely, small lesions were found in the lungs.Frogs and turtles developed generalized, fataldisease. In all of these species, the mycobacteriacould be demonstrated only in lesions, never fromnormal, uninvolved tissues.The range of mycobacterial disease in man,
then, can be looked upon as extending from super-ficial ulceration, produced by species which multi-ply best at slightly less than internal bodytemperature, to generalized tuberculosis. Thetendency to sparing of certain tissues in dissem-inated tuberculosis is not readily accounted for
by temperature alone (120). Both in the super-ficial and the generalized types of mycobacterialinfection, the organisms are localized to the le-sions.Taking advantage of the opportunity that a
symposium offers for speculation, we suggest theexistence of an influence of temperature uponmycobacterial infection in man that is intermedi-ate in type and is exemplified by leprosy. Thepossibility that temperature is an important de-terminant of tissue damage in leprosy was firstsuggested to one of us by Dr. Paul Brand, Pro-fessor of Orthopedics at the Christian MedicalCollege in Vellore, Madras State, South India.To our knowledge, Dr. Brand has not yet pub-lished a complete account of his extensive ob-servations on this subject; his name is mentionedhere only to make sure that he receives propercredit, and not to make him in any way responsi-ble for the speculations that follow.
Although lepromatous leprosy is often referredto as a generalized disease, it has long been knownthat it is essentially a disease of the skin, theperipheral nerves, the eye, certain mucous mem-branes and, in males, the testes (126). Brand hasbeen concerned with surgical correction of ortho-pedic deformities in arrested leprosy; in hundredsof operations, he has noted that destructive le-sions are limited to the most superficial portionsof nerves and tendons. The classic physical find-ings of thickening of certain nerves, the posteriorauricular, ulnar at the elbow, superficial peroneal,radial, and median antebrachial (126, 127) haveusually been looked upon as representing areasin which the result of generalized involvement ofa nerve simply happens to be anatomically ac-cessible to palpation. Brand, however, has con-firmed what others have apparently suspected(126, 127), that these areas of palpable enlarge-ment in nerve trunks represent well-localizedsegmental disease and that the nerve is spared inall but its most superficial course. The distribu-tion of dermal lesions has long been noted to showpuzzling variations in different populations ofthe world (127) and, without going into detailhere, it can be stated that trauma can be elimi-nated as playing a significant part, and that theareas of skin least likely to be uncovered byclothing and hence least likely to be exposed,are invariably least likely to be diseased. Leprouslesions of the eye are notable for their anteriorlocalization; conjunctivitis, keratitis, and iritis
251960]
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
predominate and disease of the posterior globe isexceedingly rare, if, indeed, it occurs at all (126-129). The frequency with which leprosy involvesthe nasal mucosa is well known, and late diseaseof the buccal mucosa, pharynx, larynx, or uppertrachea is not unusual. The lungs and the gastro-intestinal tract from the upper esophagus downare spared. The only so-called internal organ inwhich destructive lesions occur is the testis. Thisfrequency of involvement of the male gonad fitswell with its "thermostatic" location and its usualtemperature of 92 to 94 F (130). Ovarian diseaseis exceedingly rare. The so-called lepromata thatcan be found as pinpoint-sized foci in liver, spleen,and, rarely, kidney consist of masses of macro-phages and do not progress to parenchymal de-struction.
Despite the striking restriction of tissue injuryto anatomical sites that appear to have in commona temperature somewhat lower than that of theinternal organs, leprosy bacilli are profusely dis-tributed throughout the body in lepromatouspatients and are by no means confined to de-structive lesions (126-129). It is not possible tostate unequivocally that the myriads of bacilliin lepra cells are viable because of present ina-bility to cultivate or to isolate them in animals.Morphologically, they do not differ from themicroorganisms in lesions. Conceivably, then,differences in temperature too slight to influencegrowth or survival of the infecting organism maydetermine the occurrence and extent of tissuedamage in leprosy. Finally, the consistent obser-vation that febrile crises or "lepra reactions" arefollowed by transient amelioration of symptomsand regression of lesions (126, 127, 129) and theapparently disappointing results of limited trialsof fever therapy (126) can be mentioned.
VIRAL DISEASES
Kassanis has reviewed in detail the effects ofchanges in temperature upon viral diseases ofplants (131). Information is also available on theinfluence of environmental temperature upon thepropagation of several animal viruses includingectromelia (132), vaccinia (133, 134), variola(134), herpes simplex (134-137), vesicular stoma-titis (138), poliomyelitis (139-143), Coxsackie B(144), infectious fibroma (145), myxoma (134,145), influenza (146-150), and avian bronchitis(151). Most of these studies on animal viruses,however, are limited in scope and have no direct
bearing upon the subject of fever and resistance.Therefore, this discussion will be limited to Cox-sackie B, poliomyelitis, and herpes simplex infec-tions.
Coxsackie B VirusWalker and Boring (144) have shown that in-
fection of adult mice with the Connecticut strainof Coxsackie B1 virus is strikingly influenced byenvironmental temperature. At 25 C, the diseaseis a pancreatitis and death is rare. At 4 C (whichproduces a decrease of 1 C in rectal temperature)a uniformly fatal disease is produced by this virusin adult mice. Inoculation of virus in mice keptat 36 C (producing a rise in rectal temperatureof 2 to 3 C) is followed by no illness and the viruscannot be recovered from these animals. If ani-mals are inoculated at 4 or 25 C and then trans-ferred to 36 C, virus disappears from the tissueswithin 24 hr. Incidentally, the poor weight gainof animals held at 36 C led Walker and Boringto conclude that this temperature was "moreadverse" in its effects than 4 C. It is clear thatvariations in adrenal cortical activity cannot ex-plain these results (144) and, for the present, itcan only be said that the matter remains to beexplored further. It is difficult to see how onecan speculate profitably about the applicabilityof these findings in mice to human infection withCoxsackie viruses.
Poliomyelitis VirusThe Squibb Centennial Lecture entitled, "Fac-
tors Influencing the Evolution of Viral Diseasesat the Cellular Level and in the Organism," whichDr. Andr6 Lwoff delivered at several institutionsin this country in the spring of 1959 (143),prompted the inclusion of poliomyelitis virus inthe present discussion.The important problem to which Lwoff ad-
dressed himself is that of the mechanism of re-covery from viral infections. Once viral multipli-cation has been initiated in a host, the sequenceof cell injury, appearance of lesions, damage toessential organs, and death is relatively easy tounderstand. However, the sudden cessation ofviral multiplication with restoration of health(or without impairment of health in the firstplace) that characterizes recovery before specificimmunity supervenes is an enigma. Another wayof stating the problem, perhaps, is to ask whyexposure of a nonimmune population to a virus
26 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
such as influenza or poliomyelitis fails to resultin infection of all, and why it is that frank diseasefails to appear in all of those in whom infectionis demonstrable by isolation of virus or by sero-logical procedures. Obviously, Lwoff concluded,if specific factors are not responsible, then non-specific factors deserve consideration, and he setout to examine the possible role of fever as anonspecific factor in resistance.To study this, he observed propagation of
poliomyelitis viruses in tissue cultures incubatedat temperatures between 37 and 40 C, well withinthe range of fevers in man. The yield of virus at37 C was 250 times greater than that at 40 C.By appropriate methods, this was shown to bean effect of temperature not upon the culturecells, but upon the virus itself, although the reac-tion was not simple thermal inactivation of viralparticles. It was also shown that repeated passageof virus in tissue culture at 41 C resulted in theselection of an extremely virulent, heat-resistantvariant. The virulence of a series of poliomyelitisstrains for mice was found to correlate well withtheir resistance to heat in tissue cultures.Having shown an effect of elevated temperature
upon development of poliomyelitis virus in this"introductory model," Lwoff next carried out ex-periments in mice similar to those of Walker andBoring (144) already referred to, employing polio-myelitis instead of Coxsackie B virus. Infectedmice kept at an ambient temperature of 36 Csurvived much longer than controls held at 20 Cafter infection.On the basis of these findings, Lwoff implied
that fever is an important nonspecific defensemechanism in poliomyelitis and probably otherviral infections. He suggested also that pyreto-therapy now may be reconsidered as somethingmore than a purely empirical procedure. Fever,a common response of the host to infection witha virus, may actually be beneficial, in the opinionof Lwoff, although, in his lecture, he apologizedfor producing such a "finalistic hypothesis" in acenturywhere purposivenesshas been so ridiculed.Because this concept is simple, he warned, it isnot necessarily wrong. However, the jump fromvirus propagation in tissue culture and incubatedmice to conclusions about fever and resistance inhuman poliomyelitis can hardly be looked uponas simple.How can failure of a virus to infect an individ-
ual be looked upon as resulting from fever as a
response to viral infection when infection and,consequently, fever did not occur? How can as-ymptomatic or subclinical infection, identified assuch by laboratory tests in the absence of feverand other manifestations of illness be attributedto fever which did not occur? More specifically,one might ask if there is any evidence that infec-tion of mice with poliomyelitis virus elicits afebrile response. If, as is true of other microbialintoxications and infections (6, 101, 104), polio-myelitis in mice is indeed an afebrile or evenhypothermic affliction, how can one concludethat fever which does not occur has any relation-ship to heat resistance of the infecting virus?The height and duration of fever parallel the
severity of the minor illness and of nonparalyticpoliomyelitis in man. In spinal paralytic disease,the end of progression in paralysis is signaled bydefervescence in about 90 per cent of cases. Howdo these characteristics of human poliomyelitisfit with the idea that fever is a mechanism ofresistance? To say that many other nonspecificfactors may be interacting in the host to deter-mine the severity of illness is merely to beg thequestion by stating a truism and to admit that acentral role of fever cannot be assumed on thebasis of present evidence.One possible answer, of course, might be to
look upon fever as capable of suppressing multi-plication of virus but at the same time offering amechanism for selection of heat-resistant, virulentparticles which are capable of propagation atfever temperatures. The outcome of the illnessmight then be said to depend upon this "balance,"a situation analogous to the "critical state"mentioned by Lwoff (143).When a scientist, even with apologies, produces
a purposive hypothesis on fever's beneficial rolein resistance to disease or indeed, any other phe-nomenon, and then, as Lwoff advocates, goesahead to "make abstraction of many aspects ofhis problem and decide that his approach is theonly important one," his interpretation of experi-mental findings is almost inevitably subject tobias, sometimes subtle, sometimes not so subtle.Almost any observation, be it experimental orclinical, is subject to two or more interpretations.The scientist who has decided that his approachis the "only important one" is, of course, ex-tremely likely to accept an interpretation thatwill support his own hypothesis to the exclusionof others. More important, he is likely to fail to
271960]
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
differentiate between direct proof of the hypothe-sis and failure to disprove it by utilizing phrasessuch as "in accord with,' ''not at variance with,"etc.Thus the available information permits the
statement that any amelioration of poliomyelitismight be attributable to the suppressive action offever and any intensification of the disease mightbe a result of fever's selective action for virulence.Proof is lacking.The real point, however, is not to find some
way in which fever can be blamed for the varia-tions in the clinical course of poliomyelitis, but,rather, to avoid the virtue of "simplicity" when itinvolves trying to explain the facts of clinicaldisease by disregarding them.
Herpes Simplex Virus
Latent infection with herpes simplex virus is,of course, very frequent in man (152). It is com-monly recognized that fever activates the infec-tion, producing typical "fever blisters." In otherwords, fever seems to lower resistance to the dis-ease. Because the effects of varying the tempera-ture of incubation of this virus in tissue cultureare somewhat controversial (135, 136), or morecorrectly, require further study, we will confineour remarks to disease in man.
Artificial fever induced by physical means(153, 154) or by injection of bacterial products(155, 156) is complicated by herpes labialis in40 to 70 per cent of cases.Among diseases in which fever blisters are a
frequent complication are malaria, relapsingfever, viral influenza, typhus and other rickett-sioses, and infections produced by pneumococci,meningococci, and streptococci (157-160). How-ever, herpes labialis is so unusual in the course oftuberculosis, smallpox, primary atypical pneumonia,brucellosis, and typhoid, that its presence arguesstrongly against the clinical diagnosis (157-160)of these diseases. The rarity of fever blisters intyphoid contrasts with their frequency in pa-tients given typhoid vaccine and raises an inter-esting question about the role of endotoxemia inthe pathogenesis of typhoid.
There is relatively little interest in such clini-cal trivia as fever blisters in this antibiotic age.Their presence or absence is not often recordedin clinical charts and retrospective reviews ofhospital records will not often yield reliable in-formation. We are therefore greatly indebted to
Dr. Maxwell Finland for data acquired from hiscareful personal observations of patients. In con-trast to the frequency of herpes labialis as a com-plication of pneumococcal and streptococcalpneumonias, Dr. Finland tells us that it is ex-tremely rare in staphylococcal pneumonia if, in-deed, it occurs at all (personal communication).That elevation of body temperature enhances
susceptibility to herpes simplex can hardly bedoubted. However, these consistent variations inthe incidence of fever blisters deserve furtherstudy. Is fever itself the activating mechanism forthe virus, or is resistance lowered by anotherfactor that accompanies some fevers and is ab-sent in others? Or is there produced a factor thatprotects the host against the virus in febrile dis-eases which are rarely complicated by feverblisters?
REFERENCES1. DE KRUIF, P. AND SIMPSON, W. M. 1940
Possible significance of the inhibitory effectof fever on anaphylactic phenomena. J.Lab. Clin. Med., 26, 125-130.
2. DONE, A. K. 1959 Uses and abuses of anti-pyretic therapy. Pediatrics, 23, 774-780.
3. DuiBois, E. F. 1946 Fever and the regula-tion of body temperature. Charles CThomas, Springfield, Ill.
4. Anonymous 1959 Friendly fever? Time,LXXIII, 73.
5. BENJAMIN, H. S. 1959 Fever, the heat thatheals. Coronet, 45, 132-138.
6. BENNETT, I. L., JR., AND CLUFF, L. E. 1957Bacterial pyrogens. Pharmacol. Revs.,9, 427-475.
7. V. WAGNER-JAUREGG, J. 1918 tber dieEiniwirkung der Malaria aud die pro-gressive Paralyse. Psychiat.-Neurol.Wochschr., 20, 132-251.
8. BOAK, R. A., CARPENTER, C. M., AND WAR-REN, S. L. 1932 Studies on the physio-logical effects of fever temperatures. III.The thermal death time of Treponema palli-dum in vitro with special reference to fevertemperatures. J. Exptl. Med., 56, 741-750.
9. FINGER, E., GHON, A., AND SCHLAGENHAU-FER, F. 1894 Beitrage zur Biologie desGonococcus und zur pathologischen Ana-tomie des gonorrhoischen Processes.Arch. Dermatol. u. Syphilis, 28, 3-24.
10. CULVER, H. 1917 The treatment of gonor-rheal infections by the intravenous injec-tion of killed gonococci, meningococci, andcolon bacilli. J. Am. Med. Assoc., 68,362-366.
28 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
11. HENCH, P. S. 1935 Clinical notes on theresults of fever therapy in different dis-eases. Proc. Staff Meetings Mayo Clinic,10, 662-666.
12. HASLER, W. T. AND SPEKTER, L. 1936 Arti-ficial fever in the treatment of gonorrhealophthalmia. J. Am. Med. Assoc., 107,102-104.
13. MOORE, J. E. 1944 The modern treatment ofsyphilis, 2nd ed. Charles C Thomas,Springfield, Ill.
14. STOKES, J. H., BEERMAN, H., AND INGRAHAM,N. R., JR. 1945 Modern clinical syphilol-ogy, 3rd ed. W. B. Saunders Co., Phila-delphia.
15. WAKINI, K. G. 1948 The physiologic effectsof heat. J. Am. Med. Asoc., 138, 1091-1097.
16. WIEN, R. 1937 Fever and insulin resist-ance. Quart. J. Pharm. and Pharmacol.,10, 621-648.
17. WIEN, R. 1938 Glucose tolerance and lac-tate utilization during fever. Quart. J.Pharm. and Pharmacol., 11, 34-35.
18. KIRSTEIN, M. B. AND BROMBERG, L. 1939The effect of fever therapy upon carbohy-drate metabolism. J. Lab. Clin. Med.,25, 7-10.
19. OHTAKE, I. 1939 Studies on the changes inblood sugar content during fever. JapanJ. Exptl. Med., 17, 249-267.
20. SOMOGYI, M. AND KIRSTEIN, M. B. 1940Changes in blood ketone acids during arti-ficial fever. Proc. Soc. Exptl. Biol. Med.,45, 640-644.
21. LoSEKI, L. AND GUNDERSON, M. F. 1941The effect of artificial fever upon liverglycogen. Arch. Phys. Therapy, 22, 171-174.
22. GALL, E. A. AND STEINBERG, A. 1947 Bio-chemical studies during malarial and arti-ficial fevers. J. Lab. Clin. Med., 32, 508-525.
23. REIMANN, H. 1932 The significance of feverand blood protein changes in regard todefense against infection. Ann. InternalMed., 6, 362-374.
24. Kopp, I. 1942 Plasma proteins in thera-peutic fever. J. Lab. Clin. Med., 27, 1054-1062.
25. DUBACH, R., CALLENDER, S. J. E., ANDMOORE, C. V. 1948 Studies in iron trans-portation and metabolism. IV. Adsorptionof radioactive iron in patients with feverand anemias of varied etiology. Blood, 3,526-540.
26. ZOOK, J. AND SHARPLESS, G. R. 1938 Vita-
min C nutrition in artificial fever. Proc.Soc. Exptl. Biol. Med., 39, 233-236.
27. DAUM, K., BOYD, K., AND PAUL, W. D. 1939Influence of fever therapy on blood levelsand urinary excretion of ascorbic acid.Proc. Soc. Exptl. Biol. Med., 40, 129-132.
28. OSHOME, S. L. AND FARMER, C. J. 1942 In-fluence of hyperpyrexia on ascorbic acidconcentration in the blood. Proc. Soc.Exptl. Biol. Med., 49, 575-578.
29. ARON, H. C. S., CRAIG, R. M., FARMER, C. J.,KENDELL, H. W., AND SCHWEMLEIN, G. X.1946 Effect of elevated body temperatureon plasma vitamin A and carotene. Proc.Soc. Exptl. Biol. Med., 61, 271-276.
30. HICKS, M. H., HOLT, H. P., GUERRANT, J. L.,AND LEAVELL, B. S. 1948 The effect ofspontaneous and artificially induced feveron liver function. J. Clin. Invest., 27,580-587.
31. PIJOAN, M. 1939 Certain biologic effectsduring artificial fever. Arch. Phys. Ther-apy, 20, 170-174.
32. GORDON, E. E., DARLING, R. C., AND SHEA,E. 1949 Effects of physical hyperthermiaupon blood gas equilibria in man. J.Appl. Physiol., 1, 496-511.
33. KENDELL, H. W. AND SIMPSON, W. M. 1937Experimental treatment of early syphiliswith artificial fever combined with chemo-therapy. Am. J. Syphilis, Gonorrhea,Venereal Diseases, 21, 526-543.
34. McGUIGAN, R. A. 1938 The effect of tem-perature on digitalis action. J. Lab. Clin.Med., 23, 999-1006.
35. KiSSERI, M. AND BIERMAN, W. 1933 In-fluence of hyperpyrexia on velocity ofblood flow. Proc. Soc. Exptl. Biol. Med.,30, 527-530.
36. MCCARRELL, J. D. 1940 The effects of hy-perthermia and hypothermia on cervicallymph flow. Am. J. Physiol., 130, 34-42.
37. SUGUIRA, K. 1941 The effect of high andlow body temperature upon the growth ofirradiated mouse sarcoma 180. Radiology37, 85-93.
38. HADDY, F. J., CAMPBELL, G. S., AND VIS-SCHER, M. B. 1949 Effects of changes inbody temperature and inspired air humid-ity on lung edema and hemorrhage. Am.J. Physiol., 58, 429-432.
39. WILBUR, E. L. AND STEVENS, J. B. 1937Morbid anatomic changes following artifi-cial fever with report of autopsies. South.Med. J., 30, 286-290.
40. GORE, I. AND ISAACSON, N. H. 1949 Thepathology of hyperpyrexia. Am. J. Path-ol., 25, 1029-1059.
1960] 29
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NTICASTRI
41. DOHN, N. R., NEYMANN, C. A., AND OSBORNE,S. L. 1949 Pathologic changes in thecentral nervous system resulting from ex-perimentally produced hyperpyrexia. J.Neuropathol. Exptl. Neurol., 8, 295-304.
42. BIERMAN, W. 1934 Effect of hyperpyrexiainduced by radiation upon leukocyte count.Am. J. Med. Sci., 187, 545-552.
43. COHEN, P. AND WARREN, S. L. 1935 Astudy of the leukocytosis produced in manby artificial fever. J. Clin. Invest., 14,423-433.
44. SIMON, J. F. 1936 Effects of hyperpyrexiaon the human blood count, blood chem-istry, and urine. J. Lab. Clin. Med., 21,400-404.
45. DOAN, C. A. 1938 Peripheral blood phe-nomena and differential response of bonemarrow and lymph nodes to hyperpyrexia.Radiology, 30, 382-389.
46. LATTA, J. S. AND NELSON, W. W. 1948 Theeffects of experimental hyperpyrexia andrestraint on the blood and hemopoieticorgans of the albino rat. Am. J. Anat.,82, 321-351.
47. HABLER, W. L., HIGGINS, G. M., AND HER-RICK, J. F. 1952 Certain endocrine in-fluences governing the leukocytic responseto fever. Blood, 7, 326-336.
48. LEDINGHAM, J. C. G. 1908 The influence oftemperature on phagocytosis. Proc. Roy.Soc. (London), B, 80, 188-195.
49. ELLINGSON, H. V. AND CLARK, P. F. 1942The influence of artificial fever on mech-anisms of resistance. J. Immunol., 43,65-83.
50. HEDLUND, P., FRISK, A. R., AND BUCHT, H.1948 The appearance of acute phase pro-tein after induced fever in man. ActaMed. Scand., 131, 417-421.
51. WULFF, F. 1935 Recherches sur les sub-stances bactericides du serum humainparticulierment pendant la fievre. Compt.rend. soc. biol., 119, 424-426.
52. WULFF, F. 1937 On the bactericidal sub-stances against paratyphoid bacilli demon-strated in human serum, especially in theserum of fever patients. Acta. Pathol.Microbiol. Scand., 14, 530-537.
53. HJORTH, P. 1937 Investigations of a ther-mostabile bactericidal substance in humanserum, demonstrated particularly in theserum of fever patients. Acta. Pathol.Microbiol. Scand., 14, 412-426.
54. BARLOW, G., AGERSBORG, H. P., JR., ANDKEYS, H. E. 1956 Blood levels of 17-hydroxycorticosteroids in hyperthermic
dogs. Proc. Soc. Exptl. Biol. Med., 93,280-284.
55. RICHARDS, J. B. AND EGDAHL, R. H. 1956Effect of acute hyperthermia on adrenal17-hydroxycorticosteroid secretion in dogs.Am. J. Physiol., 186, 435-439.
56. GERNEZ, C. AND ELOIRE, F. 1937 Influencede l'hyperthermie provoquee sur les phe-nomenes anaphylactiques chez le cobaye.Compt. rend. soc. biol., 124, 682-684.
57. VALLERY-RADOT, P., MAURIC, G., AND LE-MANT, J. 1936 Etude des reactions vaso-motrices des vaisseaux cutanes chezl'homme au cours de l'hyperthermie pro-voqu6e. Compt. rend. soc. biol., 123, 572-574.
58. VALLERY-RADOT, P., MAURIC, G., AND LE-MANT, J. 1936 Etudes des reactions vaso-motrices des gros vaisseaux chez l'hommeau cours de l'hyrperthemie provoquee.Compt. rend. soc. biol., 123, 574-575.
59. GOTTSCHALL, R. Y., DE KRUIF, P., COPE, H.E., AND LAURENT, D. 1944 The effect ofartificially induced fever on anaphylacticshock in actively sensitized guinea pigs.J. Lab. Clin. Med., 29, 614-623.
60. GOLDMEN, L. 1939 The effect of fever arti-ficially induced on the skin sensitivity ofguinea pigs to turpentine. J. Invest.Dermatol., 2, 281-287.
61. DUERSCHNER, D. R., MUSCHENHEIM, C., ANDHARDY, J. D. 1943 Hypothermia in ex-perimental infections. II. The effect ofhypothermia on tuberculin sensitivity inguinea pigs. J. Infectious Diseases, 72,183-186.
62. BOAK, R. A., DORN, F. L., AND CARPENTER,C. M. 1945 The effect of fever on thetoxicity of mapharsen for rabbits. Am. J.Syphilis, Gonorrhea, Venereal Diseases,29, 428-431.
63. STOKINGER, H. E., DORN, F. L., BOAK, R. A.,AND CARPENTER, C. M. 1944 The effectof fever on the distribution of arsenic inthe tissues of rabbits injected intravenouslywith mapharsen. Am. J. Syphilis, Gonor-rhea, Venereal Diseases, 28, 465-470.
64. TIDY, H. L. 1916 Influence of febrile con-ditions on inoculation agglutinins. Lan-cet, 94(1), 241-242, 1058.
65. DREYER, G., GIBSON, A. G., AND WALKER, E.W. A. 1916 Further remarks on agglutin-ation tests in inoculated persons and theinfluence of febrile conditions on inocula-tion agglutinins. Lancet, 94, 766-768.
66. STANTON, A. H., MEUNNING, L., KOPELOFF,L. M., AND KOPELOFF, N. 1942 Spinal
30 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
1FEVER AS MECHANISM OF RESISTANCE
cord section and hemolysin production inthe rat. J. Immunol., 44, 237-246.
67. KOPELOFF, L. M. AND STANTON, A. H. 1942The effect of body temperature upon hemo-lysin production in the rat. J. Immunol.,44, 247-250.
68. ECKER, E. E. AND O'NEAL, N. 1932 Effectsof hyperpyrexia induced by an ultra-highfrequency current on B. typhosus agglu-tinin and complement. Am. J. PublicHealth, 22, 1050-1054.
69. HADJOPOULOS, L. G. AND BIERMAN, W. 1934Effects of hyperpyrexia induced by physicalmeans upon complement-fixing antibodies.J. Lab. Clin. Med., 20, 227-230.
70. JUNG, R. W. 1935 Immunologic studies inhyperpyrexia. Arch. Phys. Therapy, 16,397-404.
71. KOOMEN, J., JR., AND MORGAN, H. R. 1954An evaluation of the anamnestic serumreaction in certain febrile illnesses. Am.J. Med. Sci., 228, 520-524.
72. HAYASHI, H. 1952 On the influence offevering upon the serological response inhuman beings vaccinated against JapaneseB encephalitis. Kitasato Arch. Exptl.Med., 25, 23-24.
73. BISSET, K. A. 1948 The effect of tempera-ture upon antibody production in cold-blooded vertebrates. J. Pathol. Bacteriol.,60, 87-92.
74. ALLEN, F. W. AND MCDANIEL, E. C. 1937A study of the relation of temperature toantibody formation in cold-blooded ani-mals. J. Immunol., 32, 143-152.
75. KALABUCHOV, N. AND LEVINSON, L. 1935Effect of low temperature upon trypano-somes (Trypanosoma equiperdum) in mam-mals. Nature, 136, 553.
76. RITZMANN, 0. 1907 t'ber den Einfluss dererhohten Aussentemperatur auf denVerlauf der experimentellen Tetanus- undStreptokokken-Infektion. Arch. Hyg., 61,355-382.
77. IPSEN, J., JR. 1951 The effect of environ-mental temperature on the reaction ofmice to tetanus toxin. J. Immunol., 66,687-694.
78. IPSEN, J. 1952 The effect of environmentaltemperature on the immune response ofmice to tetanus toxoid. J. Immunol., 69,273-283.
79. WALTHER, P. 1891 Die Einwirkung derkunstlichen Erhohung der Korpertempera-tur auf den Verlauf der Infektion durchPneumonie Diplokokken. Arch. Hyg., 12,329-350.
80. LOEWY, A. AND RICHTER, P. F. 1896 Expe-rimentelle Untersuchungen uber die Heil-kraft des Fiebers. Arch. pathol. Anat. u.Physiol., 145, 49-77.
81. ROLLY, FR. AND MELTZER 1908 Experi-mentale Untersuchungen uber der Be-dentung der Hyperthermie. Deut. Arch.klin. Med., 94, 335-364.
82. McDOWELL, C. 1923 The effect of differenttemperatures and humidities on the re-sistance of rats to pneumococcus infection.Am. J. Hyg., 3, 521-546.
83. RoVIGHI, A. 1892 tJber den Einfluss derkunstlichen Erhohung der Korpertempera-tur auf der Verlauf einiger infektiosenProcesse. Prager Med. Wochschr., 17,291-293.
84. ENGELHARDT, G. 1898 Einwirkung erhoh-ter Temperaturen auf die Staphylomyko-sen. Z. Hyg. Infektionskrank., 28, 239-260.
85. RUATA, G. Q. 1909 L'influenza del caldoumido sulle infezioni. Bull. sci. med., 9,59-110.
86. STROUSE, S. 1909 Experimental studies onpneumococcus infections. J. Exptl. Med.,11, 743-761.
87. ENDERS, J. F. AND SHAFFER, M. F. 1936Studies on natural immunity to-pneumo-coccus type III. I. The- capacity of strainsof pneumococcus type III to grow at 41°C.and their virulence for rabbits. J. Exptl.Med., 64, 7-18.
88. SHAFFER, M. F., ENDERS, J. F., AND WU, C.J. 1936 II. Certain distinguishing prop-erties of two strains of pneumococcus typeIII varying in their virulence for rabbitsand the reappearance of these propertiesfollowing R -k S reconversion of theirrespective rough derivative. J. Exptl.Med., 64, 281-305.
89. ENDERS, J. F., SHAFFER, M. F., AND WU, C.J. 1936 III. Correlation of the behaviorin vivo of pneumococci type III varying intheir virulence for rabbits with certaindifferences observed in vitro. J. Exptl.Med., 64, 307-331.
90. ENDERS, J. F., Wu, C. J., AND SHAFFER, M.F. 1936 IV. Observations on a non-typespecific humoral factor involved in resist-ance to pneumococcus type III. J. Exptl.Med., 64, 425-438.
91. RICH, A. R. AND MCKEE, C. M. 1936 Themechanism of a hitherto unexplained formof native immunity to the type III pneumo-coccus. Bull. Johns Hopkins Hosp., 59,171-207.
19601 31
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
92. MUSCHENHEIM, C., DUERSCHRER, D. R.,HARDY, J. D., AND STOLL, A. M. 1943Hypothermia in experimental infections.III. The effect of hypothermia on resistanceto experimental pneumococcus infection.J. Infectious Diseases, 72, 187-196.
93. SANDERS, F., CRAWFORD, E. S., AND DEBA-KEY, M. E. 1957 Effects of hypothermiaon experimental intracutaneous pneumo-coccal infection in rabbits. Surg. Forum,8, 92-97.
94. EISEMAN, B., MALETTE, W. G., WATKYNS, R.S., SUMMERS, W. B., AND TONG, J. L. 1956Prolonged hypothermia in experimentalpneumococcal peritonitis. J. Clin. Invest.,35, 940-946.
95. WATKYNS, R. S., HIROSE, H., AND EISEMAN,B. 1957 Prolonged hypothermia in exper-imental pneumococcal peritonitis. Surg.Forum, 8, 88-92.
96. WATKYNS, R. S., HIROSE, H., AND EISEMAN,B. 1958 Prolonged hypothermia in exper-imental pneumococcal peritonitis. Surg..Gynecol. Obstet., 107, 363-369.
97. WOOD, W. B., JR. 1951-52 Studies on thecellular immunology of acute bacterialinfections. Harvey Lectures, 47, 72-98.
98. SMITH, M. R. AND WOOD, W. B., JR. 1956An experimental analysis of the curativeaction of penicillin in acute bacterial in-fections. III. The effect of suppurationupon the antibacterial action of the drug.J. Exptl. Med., 103, 509-522.
99. SHAFFER, M. F., ENDERS, J. F., AND WILSON,J. 1938 The effect of artificial fever andspecific antiserum on the organisms presentin cases of type III pneumococcus menin-gitis. J. Clin. Invest., 17, 133-145.
100. CALVIN, J. W. AND MILLS, C. A. 1939 Easeof body heat loss and resistance to infec-tion. Science, 90, 275-276.
101. LARSON, W. P., BIETER, R. N., LEVINE, M.,AND McLIMANS, W. F. 1939 Temperaturereactions in mice infected with pneumo-cocci. Proc. Soc. Exptl. Biol. Med., 42,649651.
102. WHITE, H. J. AND PARKER, J. M. 1938 Thebactericidal effect of sulfanilamide upon,3-hemolytic streptococci in vitro. J. Bac-teriol., 36, 481-498.
103. LEWIS, M. D. AND GUNDERSON, M. F. 1939The effect of artificial fever on the bloodsulfonamide level in rabbits. Arch. Phys.Therapy, 20, 432-436.
104. WEIR, J. A. 1947 The temperature of themouse in health and disease. Proc. IowaAcad. Sci., 54, 383.
105. CARPENTER, C. M., BOAK, R. A., MUCCI, L.A., AND WARREN, S. L. 1933 Studies onthe physiologic effects of fever tempera-tures. The thermal death time of Neisseriagonorrhoeae in vitro with special referenceto fever temperatures. J. Lab. Clin. Med.,18, 981-990.
106. FUTCHER, P. H. 1940 The double quotidiantemperature curve of gonococcal endocar-ditis. A diagnostic aid. Am. J. Med. Sci..199, 23-27.
107. WILLIAMS, R. H. 1937 Gonococcal endo-carditis treated with artificial fever (Ket-tering Hypertherm). Ann. Internal Med.,10, 1766-1774.
108. THAYER, W. S. 1922 On the cardiac com-plications of gonorrhea. Bull. Johns Hop-kins Hosp., 33, 361-372.
109. WILLIAMS, R. H. 1938 Gonococcic endo-carditis. Arch. Internal Med., 61, 26-38.
110. VALLERY-RADOT, R. 1923 The life of Pas-teur, pp. 268-270. Doubleday & Co., Inc.,New York.
111. WAGNER, K. E. 1890 Contribution al'6tude de l'immunit6. Le charbon despoules. Ann. inst. Pasteur, 4, 570-602.
112. SCHOLES, J. C. AND HUTT, F. B. 1942 Therelationship between body temperature andgenetic resistance to S. pullorum in thefowl. Cornell Univ. Agr. Expt. Sta.Memoir No. 244.
113. SEVERENS, J. M., ROBERTS, E., AND CARD,L. E. 1944 A study of the defense mech-anism involved in hereditary resistance topullorum disease of the domestic fowl. J.Infectious Diseases, 75, 33-46.
114. BELL, A. E. 1947 Temperature changes inthe chick during the course of fowl typhoid.Proc. Iowa Acad. Sci., 54, 303-308.
115. KUHN, L. R. 1939 Growth and viability ofCryptococcus hominis at mouse and rabbitbody temperatures. Proc. Soc. Exptl.Biol. Med., 41, 573-574.
116. KUHN, L. R. 1939 Experimental crypto-coccic infection. Arch. Pathol., 27, 803.
117. KUHN, L. R. 1949 Effect of elevated bodytemperature on cryptococcosis in mice.Proc. Soc. Exptl. Biol. Med., 71, 341-343.
118. KLIGMAN, A. M. AND WEIDMAN, F. D. 1949Experimental studies on treatment of hu-man torulosis. Arch. Dermatol. u. Syphi-lis, 60, 726-741.
119. MOSBERG, W. H. AND ARNOLD, J. G., JR.1950 Torulosis of the central nervoussystem. Review of literature and reportof five cases. Arch. Internal Med., 32,1153-1183.
32 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
FEVER AS MECHANISM OF RESISTANCE
120. RICH, A. R. 1951 The pathogenesis of tu-berculosis, 2nd ed. Charles C Thomas,Springfield, Ill.
121. ARONSON, J. D. 1938 Tuberculosis of cold-blooded animals. In Tuberculosis andleprosy. The Mycobacterial Diseases Sym-posium I. Am. Assoc. Advance. Sci.,Washington, D. C.
122. FERMI AND SALSANO 1892 tber die Pra-disposition fur Tuberculose. Centr. Bak-teriol. Parasitenk., 12, 750-752.
123. MACCALLUM, P., TOLHURST, J. C., BUCKLE,G., AND SISSONS, H. A. 1948 A new myo-bacterial infection in man. J. Pathol.Bacterial., 60, 93-122.
124. FENNER, F. AND LEACH, R. H. 1952 Stud-ies on Mycobacterium ulcerans. I. Serologicrelationship to other Mycobacteria. Aus-tralian J. Exptl. Biol. Med. Sci., 30, 1-10.
125. LINELL, F. AND NORDEN, A. 1954 Myco-bacterium balnei: a new acid-fast bacillusoccurring in swimming pools and capable ofproducing skin lesions in humans. ActaTuberc. Scand., Suppl. No. 33.
126. MUIR, E. 1948 Manual of leprosy. Wil-liams & Wilkins Co., Baltimore.
127. ROGERS, L. AND MUIR, E. 1925 Leprosy.William Wood and Co., New York.
128. BLACK, S. H. 1938 The pathology of lep-rosy. In Tuberculosis and leprosy. Themycobacterial diseases Symposium I. Am.Assoc. Advance. Sci., 1938.
129. MITSUDA, K. 1952 Atlas of leprosy. Cho-tokai Foundation, Okayama, Japan.
130. NEWMAN, H. F. AND WILHELM, S. F. 1950Testicular temperature in man. J. Urol.,63, 349-352.
131. KASSANIS, B. 1957 Effects of changingtemperature on plant virus diseases. Ad-vances in Virus Research, 4, 221-241.
132. BURNET, F. M. AND LUSH, D. 1936 Thepropagation of the virus of infectious ec-tromelia of mice in the developing egg. J.Pathol. Bacteriol., 43, 105-120.
133. NELSON, J. B. 1940 Development of vac-cinia and variola viruses in embryonatedeggs at 280C. Proc. Soc. Exptl. Biol.Med., 43, 110-112.
134. THOMPSON, R. L. AND COATES, M. S. 1942The effect of temperature upon the growthand survival of myxoma, herpes, and vac-cinia viruses in tissue culture. J. Infec-tious Diseases, 71, 83-85.
135. WHULER, C. E. 1958 The effect of tempera-ture upon the production of herpes simplexvirus in tissue culture. J. Immunol., 81,98-106.
136. HOGGAN, M. D. AND ROIZMAN, B. 1959The effect of the temperature of incubationon the formation and release of herpes sim-plex virus in infected FL cells. Virology,8, 508-524.
137. ARMSTRONG, C. 1942 Some recent researchin the field of neurotropic viruses withespecial reference to lymphocytic chorio-meningitis and herpes simplex. MilitarySurgeon, 91, 129-145.
138. SIGURDSSON, B. 1943 The influence of ageof host and temperature of incubation ininfection of the chick embryo with vesicularstomatitis virus. J. Exptl. Med., 78,17-26.
139. WOLF, H. F. 1934-35 Prevention of polio-myelitis in monkeys by means of hyper-pyrexia. Proc. Soc. Exptl. Biol. Med., 32,1083-1087.
140. SCHERER, W. R. 1954 Studies on the pro-pagation in vitro of poliomyelitis viruses.VI. Effect on virus yield of cell population,virus inoculum, and temperature of incu-bation. J. Immunol., 73, 331-336.
141. LIKAR, M. AND WILSON, D. C. 1958 Ob-servations on the interaction of poliovirus'and host cells in vitro. I. The effect ofenvironmental temperature. Brit. J.Exptl. Pathol., 39, 674-678.
142. LWOFF, A., TOURNIER, P., AND CARTEAUD,J. P. 1959 Influence de l'hyperthermieexperimentale sur la poliomyelite de lasouris. Compt. rend., 248, 1876-1878.
143. LWOFF, A. 1959 Factors influencing theevolution of viral diseases at the cellularlevel and in the organism. Bacteriol.Revs., 23, 109-124.
144. WALKER, D. L. AND BORING, W. D. 1958Factors influencing host-virus interactions.III. Further studies on the alteration ofCoxsackie virus infection in adult mice byenvironmental temperature. J. Immunol.,80, 39-44.
145. THOMPSON, R. L. 1938 The influence oftemperature upon proliferation of infec-tious fibroma and infectious myxoma vir-uses in vivo. J. Infectious Diseases, 62,307-312.
146. BURNET, F. M. 1936 The use of the de-veloping egg in virus research. Med. Re-search Council (Brit.), Spec. Rept. Ser.No. 220.
147. ENDERS, J. F. AND PEARSON, H. E. 1941Resistance of chicks to infection with in-fluenza A virus. Proc. Soc. Exptl. Biol.Med., 48, 143-146.
148. SULKIN, S. E. 1945. The effect of environ-
1960] 33
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/
-
BENNETT AND NICASTRI
mental temperature on experimental in-fluenza in mice. J. Immunol., 51, 291-300.
149. VON MAGNUS, P. 1951 Propagation of thePR 8 strain of influenza A virus in chickembryos. I. The influence of various ex-perimental conditions on virus multiplica-tion. Acta Pathol. Microbiol. Scand., 28,250-277.
150. BRIODY, B. A., CASSEL, W. A., LYTLE, J.,AND FEARING, M. 1953 Adaptation ofinfluenza virus to mice. I. Genetic andenvironmental factors affecting an A primestrain of influenza virus. Yale J. Biol.and Med., 25, 391-400.
151. SIMPSON, R.W. AND GROUPP, V. 1959 Tem-perature of incubation as a critical factorin the behavior of avian bronchitis virus inchicken embryos. Virology, 8, 456-469.
152. SCOTT, T. F. McN. 1954 Infection with thevirus of herpes simplex. New Engl. J.Med., 250, 183-188.
153. WARREN, S. L., CARPENTER, C. M., ANDBOAK, R. A. 1940 Symptomatic herpes,
a sequela of artificially induced fever. J.Exptl. Med., 71, 155-168.
154. SUTTON, R. L. 1944 Herpes following fevertherapy. Bull. U. S. Army Med. Dept.No. 78, 115-116.
155. KROMAYER, E. 1931 tVber Fieberbehand-lung mit Pyrifer. Dermatol. Wochschr.,93, 1547-1550.
156. SPEIRER, C. 1931 Die unspezifische Be-handlung der Gonorrhoe mit Pyrifer.Dermatol. Wochschr., 92, 13-17.
157. ROLLESTON, J. D. 1907 Herpes -facialis indiphtheria. Brit. J. Dermatol., 19, 375-378.
158. ROLLESTON, J. D. 1910 Herpes facialis inscarlet fever. Brit. J. Dermatol., 19, 309-312.
159. WRIGHT, F. J., COOKE, E. R. N., AND ST. A.M. D'Sauza, J. 1953 Observations onbrucellosis in Kenya. Trans. Roy. Soc.Trop. Med. Hyg., 47, 117-129.
160. BENNETT, I. L., JR., AND HOOK, E. W. 1957.Fever of unknown origin. Disease-a-Month, November, 1957.
34 [VOL. 24
on March 30, 2021 by guest
http://mm
br.asm.org/
Dow
nloaded from
http://mmbr.asm.org/