Measuring Landmine Incidents & Injuries Measuring ...
61
Measuring Landmine Incidents & Injuries and the Capacity to Provide Care Measuring Landmine Incidents & Injuries and the Capacity to Provide Care A Guide to Assist Governments and Non-governmental Organizations in Collecting Data about Landmine Victims, Hospitals and Orthopaedic Centers Physicians for Human Rights
Transcript of Measuring Landmine Incidents & Injuries Measuring ...

Measuring Landmine
Incidents & Injuries
and the Capacity to
Provide Care
Measuring Landmine
Incidents & Injuries
and the Capacity to
Provide Care
A Guide to Assist
Governments and
Non-governmental
Organizations in
Collecting Data about
Landmine Victims,
Hospitals and
Orthopaedic Centers
Physicians for Human Rights

Measuring Landmine Incidents &Injuries and the Capacity toProvide CareA Guide to Assist Governments and Non-governmental Organizations in Collecting Data about Landmine Victims,Hospitals and Orthopaedic Centers
March 2000

© 2000 Physicians for Human RightsAll rights reserved.Printed in the United States of America.ISBN 1-879707-32-2
Design: Glenn Ruga/Visual Communications Cover photos: Eric Stover

Physicians for Human Rights (PHR) mobilizes thehealth professions and enlists support from the generalpublic to protect and promote the human rights of allpeople.
Since 1986, PHR members have worked to stop tor-ture, disappearances, and political killings by govern-ments and opposition groups; to improve health andsanitary conditions in prisons and detention centers; toinvestigate the physical and psychological conse-quences of violations of humanitarian law in internaland international conflicts; to defend medical neutralityand the right of civilians and combatants to receivemedical care during times of war; to protect health pro-fessionals who are victims of violations of humanrights; and to prevent medical complicity in torture andother abuses.
PHR conducts educational and training projects forhealth professionals, members of the judiciary andhuman rights advocates on the application of medicaland forensic skills for the investigation of violations ofhuman rights. PHR bases its actions on the UniversalDeclaration of Human Rights and other internationalhuman rights and humanitarian agreements. The organ-
ization adheres to a policy of strict impartiality and isconcerned with the medical consequences of humansrights abuses regardless of the ideology of the offend-ing government or group.
As one of the founding members of the steeringcommittee of the International Campaign to Ban Land-mines, Physicians for Human Rights shared the 1997Nobel Peace Prize, awarded to the Campaign and itscoordinator Jody Williams. PHR currently serves ascoordinator of the US Campaign to Ban Landmines.
Leonard Rubenstein, J.D., is Executive Director andSusannah Sirkin is Deputy Director. Robert Lawrence,M.D., is President and Holly Atkinson, M.D., is VicePresident.
Physicians for Human Rights100 Boylston Street, Suite 702Boston. MA 02116 USATel. 617 695-0041Fax. 617 695-0307Email: [email protected]: www.phrusa.org
i i i
PHYSICIANS FOR HUMAN RIGHTS

CONTENTS
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . .vi
List of Acronyms . . . . . . . . . . . . . . . . . . . . . . . . . . .vi
1. Executive Summary . . . . . . . . . . . . . . . . . . . . . .1
2. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
3. Survey Tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
4. Pre-Implementation . . . . . . . . . . . . . . . . . . . . . .7
5. Implementation and Analysis . . . . . . . . . . . . . .11
6. Overview Tools . . . . . . . . . . . . . . . . . . . . . . . . .13Country Capacity ToolKey Informant Tool
7. Epidemiological Tools . . . . . . . . . . . . . . . . . . . .15Hospital Surveillance or Survey of
Landmines Injuries Tool Community Survey Tool
8. Capability and Social Reintegration Tools . . . .21Hospital Capability Survey ToolOrthopaedic/Rehab Center Capability
Survey Tool Social Reintegration and Rehabilitation
Survey Tool
9. Collecting Data . . . . . . . . . . . . . . . . . . . . . . . . . .31
Appendix A: Random Number Table . . . . . . . . . .34
Appendix B: Bibliography . . . . . . . . . . . . . . . . . . .35
Appendix C: Endnotes . . . . . . . . . . . . . . . . . . . . . .36
Appendix D: Blank Survey Tools . . . . . . . . . . . . .37
v
This manual was written by Adam Kushner, M.D.,M.P.H. and James Cobey, M.D., M.P.H., FACS withthe assistance of Ronald Waldman, M.D., M.P.H. ofthe Program on Forced Migration and Health, Centerfor Population and Family Health, Joseph L. MailmanSchool of Public Health, Columbia University; GilbertBurnham, M.D., Johns Hopkins University; and Etienne Krug, M.D., World Health Organization.
It was edited by Barbara Ayotte and SusannahSirkin of Physicians for Human Rights.
This project was funded with the assistance of theDepartment of Foreign Assistance and InternationalTrade (DFAIT) of the government of Canada and fromLandmine Monitor.
AP mines Antipersonnel mines
AT mines Antitank mines
ED Emergency department
ICBL International Campaign to Ban Landmines
ICRC International Committee of the RedCross
IDP Internally displaced person
IMSMA Information Management System forMine Action
NGO Non-governmental organization
OR Operating room
ORS Oral rehydration salts
PHR Physicians for Human Rights
UNMAS United Nations Mine Action Service
UNOCHA United Nations Office of Coordinationof Humanitarian Affairs
UXO Unexploded ordnance
WHO World Health Organization
v i
ACKNOWLEDGMENTS LIST OF ACRONYMS

Despite an international treaty banning the use of land-mines, tens of thousands of people are killed or injuredby these weapons every year. Epidemiological-basedsurveys are essential for properly quantifying the pub-lic health consequences. The results of such studiesfacilitate the allocation of resources and aid in evaluat-ing the impact of interventions. The development ofstandardized survey tools will help to ensure that datacollection proceeds according to appropriate scientificmethods and allow the comparison of data between dif-fering regions and countries. We hope you will usethese tools. They can be found in the back of this man-ual and are perforated so they can easily be removedand photocopied for repeated use.
An instrument for hospital-based surveillance and acommunity survey tool were developed by:
• World Health Organization (WHO)• Physicians for Human Rights (PHR)• International Committee of the Red Cross (ICRC)• Injury Center-Uganda• London School for Hygiene and Tropical Medicine
These core tools measure the morbidity and mortal-ity associated with landmine injuries and collect infor-mation on demographics, device type, pre-hospitalcare, transportation time and treatment. The first tool isan instrument for hospital -based surveillance that inte-grates into a broader WHO injury surveillance system.The second tool is a community survey undertakenwith WHO disease specific sampling techniques. Thedata collection tools can be used as part of an ongoingsurveillance system or as sample surveys that arerepeated over time. WHO is coordinating the pilot test-ing of these tools in collaboration with the above men-tioned organizations. We hope that these tools willidentify areas where landmine injuries are a significant
problem and thus target regions where more intensivesurveys should be undertaken.
Since the initial meetings, many groups, includingthe United Nations Mine Action Service (UNMAS)and the Information Management System for MineAction (IMSMA) have assisted with further refiningthe hospital data tool so that it is standardized and uni-versally accepted.
Physicians for Human Rights and other members ofthe International Campaign to Ban Landmines (ICBL)have developed an additional set of tools to measure:
• Pre-hospital care and hospital capabilities• Prosthetic capabilities• Rehabilitation and social reintegration of
landmine victims
We encourage Landmine Monitor, UNMAS andother governmental or non-governmental organizationsto use these tools or modify them as they see fit. Thesetools are different than “Level 1 Surveys”. Level 1 sur-veys are intensive, often year-long studies using focusgroups in villages to determine priorities for mineclearing. The tools contained in this manual can beused to supplement the findings of a Level 1 Survey or,more importantly, can easily provide data on areas thatrequire further humanitarian mine action assessment.These tools were designed to be easy to use, inexpen-sive to administer, and can be used either collectivelyor individually. Used as short surveys, they can be per-formed quickly to determine need and can be repeatedto measure change.
Our hope is that all parties concerned with theeffects of landmines on the public health of nations andcommunities may use these tools as a guide to targetdonor funding for future interventions.
1
1 EXECUTIVE SUMMARY

2 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

It is estimated that approximately sixty million land-mines are scattered in over 60 countries
1. On March 1,
1999, an international treaty banning the use, produc-tion, sale, transfer and stockpiling of antipersonnellandmines entered into force (the Mine Ban Treaty).Intensive efforts are still needed, however, to provideadequate care for the victims of these weapons.
The pain and suffering for countless victims of land-mines around the world is staggering. In Cambodia,one out of every 236 people is an amputee and inAfghanistan, nearly one out of every 50 Afghans is alandmine victim.
2Studies have shown that 48% of vic-
tims may die before receiving assistance and most willultimately need extensive rehabilitation.
3In many of
these countries the loss of a limb severely disables aperson and impedes their ability to function as a pro-ductive member of society.
TYPES OF LANDMINESMines vary in size, cost and destruction capacity. Gen-erally, it is the military, often under direct orders fromthe government, who determine what kinds of minesare to be used, where they will be placed and what kindof pattern will be used in laying them. Theoretically,the utilization of mines is determined by a specific,strategic policy designed to maximize defensive andoffensive military capabilities. However, in the actualpractice of warfare, such rules are usually ignored,resulting in the indiscriminate terrorization of civilianpopulations. The placement of landmines within or inclose proximity to non-military occupied areas has ledto both physical and psychological trauma.
A description of the various types of mines and theircommon uses listed below provides a clearer image ofthe insidious and pervasive threat caused by landmines.
Antipersonnel (AP) Landmines: These devices aredesigned to explode when a person walks on, or, insome cases, near them. They are often laid to protect
military installations from enemy approach. In somecountries, antipersonnel mines are used to preventenemy soldiers from removing antitank mines fromstrategically placed minefields. In addition to maimingenemy soldiers, AP mines may delay and inconven-ience enemy forces as soldiers are required to remove aseverely injured comrade from the field of battle. Typi-cally the worst scenario occurs when armies utilizeantipersonnel landmines indiscriminately to demoral-ize the civilian population by mining access routes todrinking water and firewood sources, grazing and agri-cultural lands, as well as travelling paths.
Antitank (AT) mines: These are larger devices thatexplode when vehicles drive over them. They are com-monly used to limit and deter the movement of enemytroops
Improvised Explosive Devices: Also referred to asBooby-Traps, these are designed to explode when aperson opens a door or picks up or handles a particularobject, such as a toy.
UXO (Unexploded Ordinance): Missiles, rockets,grenades and other explosives that fail to explode uponimpact, are referred to as Unexploded Ordinance, orUXOs. Most of these devices may still be “alive” oractive years, or even decades, after being deployed.
TYPES OF LANDMINE INJURIESLandmine injuries are frequently fatal with case fatalityrates estimated as high as 48%.
4Morbidity, including
high amputation rates in many mine-affected countries,increases the devastating effect of landmines. There arethree patterns of landmine injuries, as described by sur-geons from the International Committee of the RedCross.
5
Pattern I Injuries: Pattern I injuries are usually themost severe type and result when an individual steps ona buried landmine. Severe wounding of the legs, geni-
3
2 INTRODUCTION

talia, and arms often occurs and necessitates amputa-tion of legs and arms. Antipersonnel mines are the typeof landmines most responsible for Pattern I casualties.
Pattern II Injuries: These wounds result from detona-tion of fragmentation mines. Although frequently lethal,these injuries follow patterns similar to those caused byother fragmentation and shrapnel mechanisms such asUXO devices. Wounds of this type can effect any part ofthe body and patients frequently require abdominal sur-gery to repair bowel injuries. Injuries include extremity,abdominal, or facial injuries.
Pattern III Injuries: Wounds listed as Pattern IIIinjuries usually cause injury to the hands and face andfrequently lead to blindness. They are very often aresult of “mine tampering.” Mine tampering may resultfrom the handling of mines by a demining worker orchildren playing with small mines that look like toys.“Butterfly” mines, plastic mines with wings shapedlike a butterfly, are most often the perpetrators of thesetypes of injuries.
InterventionsThe World Health Organization describes landmines asa major worldwide public health problem.
6They have
outlined the need to:
• Determine the magnitude, scope and characteris-tics of the landmine problem;
• Study the factors that increase the risk of disease,injury or disability and determine which factors arepotentially modifiable;
• Assess what can be done to prevent the problem byusing the information about causes and risk factorsto design, pilot test and evaluate interventions;
• Implement the most promising interventions on abroad scale.
In following these principles, PHR, along withexperts from WHO and other organizations developedsurvey tools to measure the magnitude of landmineinjuries and the circumstances in which they occur.
To assess the validity of these tools, a pilot test wasconducted in June 1999 in Azerbaijan. A team fromPHR surveyed hospitals, rehabilitation centers, andcommunities and field-tested the ability of these toolsto quantify the public health consequences of landmineinjuries and the capacity of the medical infrastructure.Relief International, a non-governmental organizationthat has operated in Azerbaijan since 1992, assisted inthe logistics and recruitment of local health profession-als to administer the surveys.
4 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

Below is a summary of the tools contained in this manual:
I. OVERVIEW TOOLSTo Assist the Researcher in Preparing to Implementthe Tools
1. Country Capacity OverviewA tool to collect data on populations, health facili-
ties, and landmine-affected regions.
2. Key Informant SurveyA tool to collect data from interviews with commu-
nity or village leaders that is used to identify high-riskareas most affected by landmines and to help determinesample sites for the community survey.
II. EPIDEMIOLOGICAL TOOLS To Measure the Extent of the Landmine Problem
1. Hospital Surveillance or Survey of LandmineInjuries
A tool to record data on landmine victims at the timethey present to a hospital or, if proper records are avail-able, from operating room records and patient charts.The goal of this tool is to establish a global reportingsystem where injury data is collected and then trans-mitted either to centers in ministries of health or tointernational organizations responsible for the analysisand dissemination of the data. It integrates easily intothe WHO injury surveillance system with continuousdata collection. In addition, this tool can be used as ashort survey to establish baseline information thatallows for measuring trends over time.
2. Community Survey A tool to record data of mine-affected areas and pro-
vides information regarding the effect landmineinjuries have on communities. This tool is designed toassess the magnitude of the landmine problem in the
community and to create a profile of mine-affectedcommunities and individual landmine victims. It isspecifically designed to collect data on all individuals,including those who either did or did not seek hospitalcare or died before attaining care. By calculating thepercent of victims that were missed in the hospital data,the region’s true incidence of mine injuries can bedetermined. Data can be used to prioritize expenditureof resources, time, and money.
III. CAPABILITY AND SOCIAL REINTEGRATION TOOLSTo Assess the Effectiveness of the Resources of theHospitals and Orthopaedic/Rehabilitation Centers toTreat Mine Victims.
1. Hospital Capability SurveyA tool to assess the capacity of hospitals providing
surgical care in regions affected by landmines. Mea-surements provide information regarding hospital serv-ices necessary for performance of surgery. Theseinclude characteristics of the physical plant, personnel,surgical capabilities, and capacity of a hospital. Thedata collected will help in the allocation of donor fund-ing for specific projects or to individual facilities inneed of necessary equipment and supplies.
2. Orthopaedic/Rehabilitation Center CapabilitySurvey
A tool to assess the capability of orthopaedic andrehabilitation centers to treat landmine survivors inorder to determine where improvements and resourcesare needed. Functional capacity, health, educationaland social issues can be determined based upon theresults of this survey.
3. Social Reintegration and Rehabilitation Survey A tool to collect data that will allow agencies and
governments to determine the effectiveness ofresources that are available to landmine survivors andwhat steps can be done to insure that survivors receive
5
3 SURVEY TOOLS

adequate attention for successful reintegration intosociety. This survey will measure the extent to which avictim’s injuries are interfering with their ability to leadrelatively stable and self-sufficient lives and the degreeto which they are receiving aid from the government.
This tool should only be used where rehabilitationservices are available and administered carefully so asnot to raise expectations, which may not be possible tofulfill, of more assistance to a community.
6 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

COMMITMENT AND ACCESSBefore the administration of any of the tools, coopera-tion in the data collection should be obtained (if possi-ble) from all levels of the government in question, asissues of access are critical. At the very least, commit-ments of support and/or access to records should beobtained from those ministries that supervise healthcare/hospital records (such as the Ministry of Health).Data on landmine injuries may be considered by thecountry to be militarily sensitive and may also requireMinistry of Defense permission.
Ministries that provide access to mine-affected com-munities, such as the Ministry of Defense and/or Min-istry of Interior, may also be approached forpermission. Assurances should be obtained that com-munity surveys will not result in any form of retaliationor otherwise negative impact upon those surveyed.When possible, permits should be obtained beforeimplementation in order to facilitate actual administra-tion of the survey tools. All permits/assurances shouldbe provided in writing in order to assist with localadministration.
If expatriate consultation is required, written permis-sion from the Ministry of Health or other governmentalagency may be required for entry permits before arrivalin-country.
Military Landmine Victims/Access to GovernmentFacilities
Names and addresses of landmines victims injuredduring service with the military may be considered tobe confidential information, as would patient records ingovernment and/or military facilities. Prior to imple-mentation, the concerns of the Ministry of Defenseregarding this information should be obtained and per-mission received. However, in recognition of the sensi-tive nature of this information, staff should be preparedto maintain flexibility and may wish to train militarypersonnel to self-administer the survey of military
facilities/personnel for confidential distribution. Sur-veyors may then receive results (without identifiers)for analysis.
Similarly, military hospital capability may be of asensitive nature. However, all possible effort should bemade to obtain this information as many landmine vic-tims may be sent primarily to military hospitals andonly secondarily transferred to civilian hospitals onlyafter military hospitals reach full capacity.
Individual survey teams must then decide whetherthey consider the results accurate and complete enoughfor inclusion in the overall country report or whetheranalysis should be carried out separate from the inde-pendent evaluation.
Local OfficialsLocal officials may or may not maintain communi-
cations with the Ministries of Health and Defense.Therefore, contact should be made before arrival in dis-tricts to be surveyed. Approval from local officials tocollect data is valuable for political reasons as well asprevention of queries by local police agencies.
BACKGROUND INFORMATIONPopulation data (denominators) as well as detailedmaps should be gathered before implementation. Popu-lation data is essential to calculate rates, which areessential for comparison work and resource allocation.At times, this demographic information may be hard toobtain due to local or national political issues based onthat data. One may have to perform some quick cen-suses on a few villages to obtain more accurate esti-mates. (Note: The source of information must be citedin all reports.)
Previous surveys of landmine affected regions, pub-lic health consequences of landmines, and overallcountry capacity may already have been attempted.Careful research may reveal background incidencerates and/or health care facility capability. Such studies
7
4 PRE-IMPLEMENTATION

may prove useful as external validation of the tools aswell as introductory information regarding mine-affected regions. Again, care must be taken and allsources must be cited.
OTHER ORGANIZATIONSFrequently, countries with a high prevalence of land-mine injuries will already have organizations (govern-ment sponsored, non-governmental organizations,private foundations, etc.) in place to assist and docu-ment the effects of landmines. These agencies shouldbe contacted as far in advance as possible both as acourtesy and as a valuable resource for information,access and potential assistance. Methods to identifysuch agencies include contact with the government,World Health Organization, United Nations MineAction Service, members of the International Cam-paign to Ban Landmines, Save the Children countrydirectories, United Nations Office of Coordination ofHumanitarianAffairs country offices, local news organ-izations, and Internet searches.
LOGISTICSWhenever possible, logistics of the survey should beset-up before implementation; however, flexibilitymust be maintained as these considerations willundoubtedly change in the field as unexpected findingsand challenges are encountered.
STAFFINGStaffing needs will vary by country. In determining thespecific staffing needs of an individual country the fol-lowing staffing considerations may be of use:
• Expatriate consultants for training in administra-tion of the survey tools: Ideally this training willinclude a “Training of the Trainers” modulewhereby in-country staff will perform all aspects offuture surveys.
• In-country survey administrators including super-visors of surveys and locally recruited personnel toadminister the survey. Assistance in recruiting localpersonnel to conduct surveys may be facilitatedthrough contact with local, landmine-specificNGOs, village leaders, local rehabilitation centers,etc. Consideration should be taken concerning confi-
dentiality as local survey administrators may eitherelicit more information (due to greater trust by localcommunity members), or less (due to fears regard-ing confidentiality). Examples of local personnelwho may be recruited include teachers, administra-tors, and other respected members of the commu-nity. These people may be approached torecommend surveyors or requested to perform thesurveys themselves.
• Translators
• Drivers
TRANSPORTATIONThe number of vehicles necessary for staff members totravel to mine-affected regions should be determined.The physical terrain and accessibility of such areas isalso of high importance. Questions to address include:How good are the roads? Is there a particular seasonduring which roads are impassible? Are the roadsmined? For example, surveys may need to be post-poned until a dry season if annual rains prevent access.
LODGINGProvision should be made for lodging while in mine-
affected regions and, if necessary, while performinghospital and rehabilitation surveys.
TRANSLATION OF SURVEY TOOLSThe tools should be translated into the local language.An independent translator should translate them backinto English to validate the text.
DEFINITIONSThe time frame for sampling of records, i.e. one-monthinterval, six-month, one year, etc., should be specifiedprior to application, although flexibility may be main-tained as availability of records will dictate the out-come.
SECURITY/SAFETY MEASURESIssues of security and safety must be of the utmost con-cern. Under no circumstances are survey administra-tors to be placed in danger while obtaining data.Information regarding local conditions should be ascer-
8 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

tained from all available sources including local lead-ers and organizations, embassy staff and mediasources. It should be remembered that objectivesources of information may be most significant in thesecases.
MEMBERS OF THE SURVEY TEAMSeveral factors should be considered when choosingthe members of the survey team. As a whole the teamshould possess the following abilities, however, thesequalifications may overlap among team members anddo not constitute a strict requirement for each individ-ual member:
• Supervisory Experience (preferably of surveyadministrators)
• Medical and/or public health background
• Knowledge of local language and culture
Before the implementation phase, all members ofthe team should gather and discuss the questions, meth-ods for obtaining information, and division of duties.Team members may wish to assign groups to assesseach individual phase, i.e. hospital capability, rehabili-tation, community, or rotate through all surveys. Asthese assignments may change in the field, all membersof the team ought to familiarize themselves with allsurveys that are to be implemented.
It may be useful to discuss with all team members(expatriate or local) natural reactions they may havewhen first seeing or working with amputees or traumavictims. To some members of the team, this may beinsignificant, for others, the exposure may cause someinitial trauma and therefore a group discussion mayhelp mollify the experience.
P R E - I M P L E M E N TAT I O N 9

1 0 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

This section focuses on the specific needs for imple-menting each of the surveys. A description of all surveyquestions and analysis of what conclusions can bedrawn from each question is provided.
Depending on staffing and adequate supervision,multiple levels of the implementation phase may pro-ceed simultaneously; however, some surveys are neces-sary to complete in order to guide the implementation ofothers.
When deciding upon which surveys to implement, thetools can be divided into three groupings. The hospitalcapability and hospital surveillance or survey forms maybe implemented at the same time during a single visitwith a hospital director. Similarly the orthopaedic centersurvey may provide a list of names for random samplingfor the social reintegration survey. The key informantsurvey may provide overview information for either thecommunity or the social reintegration survey.
A basic timeline is on the following page and ismeant only as a rough guide. As some surveys morelogically precede others, surveyors may wish to admin-ister those tools sooner.
When implementing the surveys and during meet-ings, the following must be maintained:
• Agencies should understand that the information ispublic and will be available for wide distribution.
• All participants should be aware of the scope of thesurvey, including Ministry of Health and other agen-cies involved.
• The preliminary reports are to be available imme-diately upon completion of the survey.
All data may be immediately entered into Epi-Info forease of calculation, or preferably the UNMAS orIMSMA data base with preliminary frequencies and per-centages available at the end of the study for distributionto the Ministry of Health and interested local organiza-tions. All participating agencies must receive a copy of
the preliminary report, both as a courtesy and for dataverification. A letter requesting feedback from all partic-ipants should accompany the report. Such feedbackincludes suggestions for future studies/surveillance aswell as agencies’ perceptions of which areas need to betargeted for donor funding based on preliminary results.All suggestions should be examined and, if possibleincorporated into the secondary analysis.
1 1
5 IMPLEMENTATION AND ANALYSIS
The Country Capacity Overview Tool should always becompleted first.
GROUPING 1: OVERVIEW
GROUPING 2: EPIDEMIOLOGICAL
GROUPING 3: CAPABILITY AND SOCIAL REINTEGRATION
COUNTRY CAPACITYSURVEY
COMMUNITY AND KEY INFORMANT
HOSPITAL SURVEILLANCE OR
SURVEY
COMMUNITY SURVEY
HOSPITAL CAPABILITY
SOCIAL REINTEGRATION
SURVEY
HOSPITAL SURVEILLANCE OR
SURVEY
ORTHO/REHABSURVEY

TIMELINE
Hospital Capability Survey: 1-2 days
Hospital Surveillance or Survey: 1-2 weeks
Is adequate staffing available to complete theforms?
Will the hospital second staff to examine medicalrecords?
Will the data come from discharge records, operat-ing theatre logs, or emergency department forms?
Will training be required of those who will fill outthe forms?
Will a staff be motivated and able to implement thelong-term WHO Surveillance system or should onejust perform a simple one-time survey?
Key Informant Survey: 1-2 days
Community Survey: 1-3 weeks
Are adequate staff available to administer surveys?
How far apart are the villages to be surveyed?
Will there be training of trainers? How will they berecruited? (local, urban) How long will it take (1-2 days)?
Are any difficulties anticipated in locating those tobe surveyed?
Orthopaedic/Rehabilitation Capability: 1-2 days
Can also provide a list of names for the SocialReintegration Survey.
Social Reintegration Survey: 1-3 weeks
Is adequate staffing available to administer the survey?
How much time is allotted to train survey adminis-trators? 1-2 days?
How much time is required to travel between thosesurveyed? i.e. How far apart are villages in whichinformants live?
1 2 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

1. COUNTRY CAPACITY TOOLThis is a tool designed to collect background data onpopulations, health facilities, and landmine-affectedregions to guide the researcher. This includes basicinformation such as number of districts, number of hos-pitals with surgical capability, number of medical facili-ties without surgery, number of rehabilitation facilities,number of physicians and number of surgeons.
This tool should be completed first.See Appendix D for sample tool.
2. KEY INFORMANT SURVEY TOOL This tool is designed to collect background informationuseful in the completion of the community survey.Begin to collect this information as soon as possiblebefore starting the community survey. Initial data col-lection will preferably begin in the capital city and con-tinue throughout the mine-affected regions. From thisdata, a list of ‘sentinel’ villages can be gathered.
The key informant survey should be administered toanyone who may be of assistance in identifying vil-lages in which mines are an actual or a perceived prob-lem. Key informants should include (but not be limitedto): doctors/hospital administrators, governmentadministrators (e.g. Ministry of Health personnel, Dis-trict level administrators), heads of villages, staff oflocal mine-related NGOs, rehabilitation center work-ers, advocacy groups or mine victims.
If possible, information should be collected on thepopulation size and approximate area of any affecteddistricts. This information will be useful in the analysis
phase for approximating incidence and prevalencerates. Collect information on the number and locationof any hospitals (facilities with surgical capability) andmedical facilities (without surgical capability), as wellas prosthetic and rehabilitation centers, throughout theregion.
The following questions should be asked of localcommunity leaders:
• Are houses or buildings in the community cur-rently mined or booby trapped?
• Are fields or farmland currently mined?
• Have livestock been lost to mines in the previous12 months?
• Are water sources in the community currentlymined?
• Has the population been displaced because oflandmines in the previous 12 months?
From these questions, a general picture can besketched of which villages are affected by mines and inwhat capacity. Information may also be used to developa sense of the local perception of the problem; how-ever, bear in mind that analysis of other surveys mayindicate that the largest source of concern lies else-where (transport, hospital capability, etc.) This willlater be helpful in targeting financial and humanresources towards demining activities and mine aware-ness programs.
See Appendix D for sample of the Key InformantSurvey Tool.
1 3
6 OVERVIEW TOOLS

1 4 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

1. HOSPITAL SURVEILLANCE OR SURVEY OF LANDMINEINJURIES TOOL The Hospital Surveillance or Survey Tool may bepreferably used to set up an ongoing surveillance sys-tem. Alternatively, if permanent, reliable, affordablestaff are not available, it may be used as a one-time sur-vey and repeated periodically to measure change. Aswith other surveys, permission from the Ministry ofHealth for data collection, along with letters of intro-duction. should be obtained in advance. The data col-lection can lead the researcher to locations for thecommunity surveys.
Logistics
Request for AssistanceAt least one meeting with the director of the hospital
will be necessary to obtain data. Survey administratorsshould contact the director and request at least one hourto describe the survey in detail and seek assistance. Ifpossible, the survey and letters of introduction shouldbe forwarded before the meeting. The two purposes ofthis particular survey should be described.
First, the survey requires that hospital recordsregarding landmine victims be retrospectivelyreviewed for a specified period of time (one month, sixmonths, one year, etc). If hospital staff is unavailable tosearch through the records, locally recruited surveystaff should be hired, with the understanding that fullaccess to patient records will be given. The director ofthe hospital will be asked to contact surveyors oncemedical records have been examined, and an estimateof the amount of time necessary should be requested.The researcher must determine the ease of obtainingaccurate medical records and decide if discharge datashould be the primary source, the operating theatre logbook, or emergency room admission data.
If the tool is to be used for ongoing surveillance, theinstrument has been designed so that data collection on
the incidence of landmine injuries and the circum-stances in which these injuries occur can be collectedon a regular basis as patients present themselves forcare. This instrument can be used to collect data on theincidence of landmine injuries only, or can be usedwith other instruments to collect data on landmineinjuries and injuries due to other causes (traffic acci-dents, violence, etc.) The latter being more cost effec-tive. This ongoing data collection process will allowfor monitoring of trends over time, documenting inci-dence rates and evaluating prevention programs.
Quality controlRegarding cross-sectional information, quality con-
trol may be achieved through random selection ofpatient records for examination. After surveys are com-pleted, one or two may be selected through randomnumber generation and compared against the patientrecord in question. Similarly, sentinel site surveillance(studying locations in depth that have been shown tohave a high prevalence of the condition by either hospi-tal or community data) may be randomly checked byday of the month, number of surveys completed, etc.
Surveyors should be aware that much of the infor-mation being requested might not be available. If thehospital director/Ministry of Health agrees to allowsurveillance, hospital staff will need to be trained in theadministration of the surveys.
Survey QuestionsThe numbered questions on this tool are not in con-
secutive order because they coincide with the IMSMAMine UXO/ Incident/Accident Form. This tool isdesigned not to only assist in measuring injuries but toguide deminers to locations.
Questions 1.11-6.8 • Basic demographic data on the victim
1 5
7 EPIDEMIOLOGICAL TOOLS

Questions 2.4-6.11• Describe characteristics of the accident, includingplace of incident and general extent of the injuries(including death). This information is used to planmine clearance.
Questions 7.1-7.2• Provide details of the injuries which will helpassess the physical burden on the country to dealwith them.
Questions 9.1-9.5• Describe availability of first aid in the country oremergency medical services (ambulatory systems)to assess length of time before treatment . It also dis-cusses the location of the mine incident. This infor-mation is important for evaluation of the quality ofpre-hospital care which includes time taken to get toa hospital as well as availability of first aid.
Question 9.6• This information helps establish how mines areaffecting daily economic activity of a region.
Questions 9.9-end • These assess levels of mine awareness in a region.
See Appendix D for a sample of the tool.
2. COMMUNITY SURVEY OF LANDMINE INJURIES TOOLThe Community Survey is designed to assess mine-affected communities and determine which areas needto be targeted for demining activities and which sub-populations require greater mine awareness training.By interviewing community members who have beenvictims of landmines within the last 12 months, theoverall scope of the problem can be assessed in eachaffected community. This survey is not to be adminis-tered for injuries occurring greater than 12 monthsprior to the interview.
For example, if landmines are affecting herders inthe fields of one community, then that sub-populationshould specifically be identified for mine awarenesstraining. If in another community, mine accidents occurwhile driving, then the roads can be targeted for demi-ning operations.
The survey is to be administered to all recent (within
12 months) landmine victims in a group of sentinel vil-lages previously identified as being mine-affected(through the key informant survey). If upon completionof the survey in the sentinel villages, the number ofrecent mine victims is found to be too small to analyzeproperly, then, time and resources permitting, the sur-vey can be administered to recent landmine victims ineach village in the region.
Because the mine incidents have occurred within thelast 12 months, it may often be impossible to interviewthe victim directly. The victim may now be dead, at thehospital, or too traumatized to complete the survey. Inthese cases, the interview should be conducted with thehead of the victim’s household. If at any time itbecomes too difficult for the victim or family memberto continue, the interview should be halted immedi-ately and either continued with someone else from thefamily, delayed, or terminated.
Choosing the Sentinel VillagesBefore undertaking the Community Survey, inter-
views are conducted with key informants, (e.g. hospitaldirectors, rehabilitation center directors, other land-mine survivors, Ministry of Health or Ministry ofDefense personnel) to identify villages at high risk andwhere landmine injuries are known to have occurred.(See: Key Informant Survey Tool and/or Hospital Sur-veillance or Survey Tool). In selecting the number ofsentinel villages to visit, the total population of thesesentinel villages should approximate 10% of theregional population. If population figures are not avail-able, then 5-7 sentinel villages should be chosen. Inthese sentinel villages, the Community Surveys shouldbe administered along with the Social Reintegrationand Rehabilitation Survey to all landmine victimswithin the population parameters. If the number of sen-tinel villages identified through key informant inter-views is too numerous, then the villages can be placedin a randomized order and visited in the order chosen.
Identifying the VictimsThe Community Survey is designed to be adminis-
tered to those victims (or their families) whose land-mine encounter was within twelve months of surveyadministration.
1 6 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

Once the sentinel villages have been chosen, it isimportant to identify all landmine victims within eachvillage. This should not be a problem in smaller vil-lages. However, in larger villages or small cities manykey informants should be interviewed. Landmine vic-tims can be identified through speaking with villagechiefs, the village council, local doctors or social work-ers, disability activists, or through word of mouth. Inmid-size to large cities, identification of all landminevictims may prove to be impossible. In these cases, thesample population can be identified through keyinformant interviews, or through hospital or rehabilita-tion center records.
The names and ages of all landmine victims from thevillage should be recorded, as well as the approximatedate of the incident, location and the outcome (did thevictim die?). The families of those who were involvedin incidents over the last twelve months should beinterviewed using the community survey instrument,regardless of whether or not the victim died. To ensurean accurate yearly rate of incidence, this survey is notto be administered for injuries occurring greater than12 months prior to the interview.
Administration of the SurveyA complete list of villages in the area should be
obtained. It may be easier to break this list down bydistrict, region, county, etc. These villages should berandomized and visited in the order presented. In eachvillage, it should be determined whether or not thereare mine victims present. If so, administer the surveyto them; if not continue on to the next village on thelist. If the key informant surveys were done properly,then the mine victims should be concentrated in thesentinel villages.
Every effort should be made to train local commu-nity health workers to administer the surveys. Surveydata should be immediately analyzed and forwarded tothe local Ministry of Health and interested internationalorganizations. If a partnership with a local NGO can beestablished, then their staff members can be trained inthe administration of the survey. Once local NGOs areproperly trained, ongoing surveillance or repeat sur-veys can be easily implemented.
Survey QuestionsKey Informant Information
Questions 1-2: Household information• These questions are to determine a denominator forthe household and to determine the number of vic-tims.
Questions 3-4: Number of people killed/injured bylandmines in previous 12 months.
• A high number of recent deaths and injuries in thecommunity indicates the need for increased mineawareness and can also indicate recent mine layingactivities.
Questions 5-10: Village information• Responses will assess the level of mine awarenessin the community as well as the community’s per-ception of the mine problem. These data points canbe used to target mine awareness activities.
General Patient Information
Question 11: Name• This information is used to ensure that individualsare not interviewed more than once, and for spotchecking results.
Question 12: Victim number.• In the case that there is more than one landminevictim in a household, administer a separate ques-tionnaire for each victim and number each surveyconsecutively. If there is only one victim in thehousehold, this should be coded 1.
Questions 13- 14: Age of victim at time of injury; Sex ofvictim.
• Age of victim in years. If less than one year old,code as 01.• These questions provide demographics of thepatients surveyed. Are they primarily male andyoung? If so, they may be military personnel caughtin conflict or post-conflict situations. Are theyfemale and middle-aged? They may then be womentraveling away from home to gather food, fuel, orwater. Are they children? Landmines may be deto-nated while children play in affected areas.
E P I D E M I O L O G I C A L T O O L S 1 7

Question 15: Military status• Military status assists in demographic knowledgeand patient profiling. Has the country recently beenat war? If so, are civilians the ones primarily injuredby landmines or is it the military?
Question 16: Patient Status• Check all that apply. For example, an individualcan be a refugee as well as engaged in deminingactivities.• Useful in compiling a demographic profile of minevictims.
Question 17: Type of area.• The type of area indicates those locations mostlikely to result in injury. In addition, this questioncan be combined with others to create a more com-plete picture of the situation. If injuries primarilyoccur on roads or footpaths, travel may be the majorreason for injury. The results will indicate whethermines hinder resettlement (accidents occur in vil-lages), travel (roads and footpaths), cultivation(field), military/government activity (buildings), andother daily activity (riverbank). All answers providetargets for education efforts and mine awareness.
Question 18: Activity at time of injury• Handling a mine including taking the mine apartfor scrap metal or simply holding or moving a mine. • This question measures the effect of landmines onthe area’s economy. Do mines interfere with incomegenerating activity (farming, fishing, herding, hunt-ing), travel, or daily activity (collectingwood/water/food)? Are mine injuries occupational(demining)? Do they occur randomly (passing by)?If mines play a large role in daily or economic activ-ities, priority should be given to demining arableland or routes to water supply. Similarly, mineawareness and education should focus on theseareas. A large proportion of ‘handling mine’ victimsindicates a need for a more general mine safety andawareness training.
Question 19: Type of device• Types of mines: AP (antipersonnel) mines aresmaller mines designed to explode when a personwalks on them. AT (antitank) mines are largerdevices designed to explode only when vehicles
drive over them. UXOs (unexploded ordinances) areitems such as unexploded grenades, bullets, artilleryor ‘duds.’ Booby traps - also called “improvisedexplosive devices” - are designed to explode when aperson picks up or tampers with a particular object.• This question is useful in predicting types of injuryas well as site of incidents. If a large number ofinjuries are due to antitank mines, a greater numberof casualties and injuries while traveling might beexpected. High numbers of injuries due to UXOsoften indicate prior indiscriminate shelling, andinjuries are more likely to occur in a random fashion.
Clinical Outcome – Check all that apply.
Question 20: Amputation Upper Limb• Amputation of arms; includes loss of fingers.
Question 23: Deafness• Partial hearing loss is to be included
Question 24: Blindness• Partial vision impairment is to be included.
Questions 25-27: Head/neck injury; abdomen/thighinjury; limb injury
• Limb injury involves any damage to the arms orlegs not requiring amputation.
Question 28: Paraplegia• For this survey, paraplegia is defined as total orpartial loss of movement.• Questions 20-28 are used to classify the major typeof injury that has occurred. Type 1, the traumaticamputation of a lower extremity (questions 21-22),affects approximately 35% of the victims who sur-vive. Type 2 injuries include extremity, abdominal orfacial injuries (questions 25-27) resulting from frag-ments, blast or shrapnel. Type 3 injuries involve thehands or upper extremities (question 20). As victimsof Type 1 injuries almost always require a prosthesisalong with substantial rehabilitation in order to fullyreintegrate into society, a large number of Type 1injuries indicates a need to administer the socialreintegration and rehabilitation survey in order toensure adequate reintegration into society.• Information on other injuries (deafness, blindness,paraplegia, etc.) will also be useful in targeting inter-
1 8 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

ventions for landmine survivors. For example, alarge proportion of incidents resulting in deafnessrequires greater funding for assistance to the hear-ing-impaired.
Question 30: Other? • For example, injury to genitalia.
Incident Report
Question 31: Was the area known to be mined?• Responses will assess the level of mine awarenessin the community as well as the level of educationneeded to ensure adequate awareness.
Questions 32-34: Number of other victims; numberkilled; number injured.
• In order to be recorded, all other victims must havebeen physically injured. For example, people whowere in the same vehicle in a landmine incident butwere not physically injured should not be included.
Questions 32-34 assess the level of injury and deathassociated with the mine involved. If mines are causinga large number of injuries per mine, mine awarenessand demining efforts should be intensified.
Question 35: Did the victim go to the hospital?• ‘Hospital’ is defined as any medical facility withsurgical capabilities.
Question 36: Time to hospital• If the time to hospital is greater than three hours,then interventions should be made in transportingvictims.
Question 37: If the victim died, where did it occur?• Use only if the victim died as a result of landmine-related injuries. • This is a measure of the severity injuries as well asa potential target for intervention. For example, if ahigh proportion of victims die in transport, thenspeed of transportation to the hospital may need tobe improved.
Question 38: Did the victim receive rehabilitativecare?
• Rehabilitative care is defined as training or socialsupport.
Question 39: Did the victim receive a prosthesis?• It is important to realize that if the accident hap-pened recently, there may not have been enoughtime to receive a prosthesis. In the case of morerecent victims (i.e. within 3 months), the number ofvictims receiving prostheses is expected to be low.
Question 40: How often does/did the victim use a pros-thesis?
Questions 41-42: Did the victim work before theinjury? Does the victim currently work?
• Work can be either part time or full time, for pay ornot for pay. ‘Student’ is not included as work.• Military enrollment is considered employment.• Measures impact of landmine incident on eco-nomic activities and daily life events.
See Appendix D for a sample of this tool.
E P I D E M I O L O G I C A L T O O L S 1 9

2 0 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

1. HOSPITAL CAPABILITY SURVEY TOOLThis survey is designed to assess the ability of a hospi-tal to care for landmine victims needing surgical atten-tion. It is meant to provide a baseline analysis of thefacility and to be administered along with the HospitalSurveillance or Survey Tool. This information is essen-tial for donors who want to care for landmine victims.Helping build the infrastructure of a hospital may beone of the most important things that they can do.
LogisticsMeetings
While meeting with the director of the hospital tocollect data for the Hospital Surveillance or SurveyTool, the Hospital Capability Survey Tool can also becompleted. The director or a staff member should beable to provide the answers to the survey. The surveyorshould, however, take a thorough tour of the facilityand closely observe all the departments as they arefunctioning to get a true picture of the hospital. Staff,other than the administrator, should also be informallyinterviewed to obtain a sense of the capacity of thefacility. It may be necessary to schedule a second meet-ing to collect the survey form. At this time, it is usefulto review the responses and then obtain any furtherinformation the director may wish to convey to the sur-vey team or to potential donors. This information canbe included along with the final report.
This tool can only measure physical capability. It isextremely difficult to measure individual staff motiva-tion, which is often the most important determinant ofquality of care.
Survey QuestionsInitial information and questions 1-3 provide loca-
tion and contact information for the hospital in ques-tion. Many of the remaining questions require someone
on the team who has some knowledge of medical orhospital care.
Physical plantQuestions 4 through 17 provide information regard-
ing the physical capability of the hospital to supportsurgical procedures. Each question is designed to pro-vide insight concerning the essential equipment. Arough estimate of the quality and level of care the hos-pital can provide may be assessed through these ques-tions. In general, the following standards should apply:
• Possession of dedicated operating room, runningwater, electricity
• Sterilized equipment always available
• Laboratory with hematocrit capability
• Stored blood available within 30 minutes
• Stored blood on premises
• Laboratory available and working to test blood forHIV, malaria and syphilis
• Operating Room records kept
• Vital signs recorded daily
• X-ray facilities available
• Patient charts kept
• Anesthesia records kept
• Intact screens
Question 4: Is there a dedicated room for surgical pro-cedures?
• Is there a room specifically for surgical operations?Only one is necessary for a response of “yes.”• A dedicated room/operating room for surgical pro-cedures provides a measure of the size and capabil-ity of the facility to perform complex surgicalprocedures.
2 1
8 CAPABILITY AND SOCIAL REINTEGRATION TOOLS

Question 5: Is running water available for surgerygreater than (>)12 hours per day?
• Is water available for washing and sterilization ofequipment? The term “>12 hours” is to preventoccasional (e.g. 15 minutes/day) water availabilityfor constituting an answer of “yes” to this question. Running water measures the ability of the hospital toclean equipment, irrigate and clean wounds.
Question 6: Is electricity always available for surgicalprocedures?
• Can lighting be maintained for surgical proce-dures? Is a generator present on the premises?• Electricity indicates the capacity for continuouslighting and ability to use more sophisticated equip-ment and to perform surgery at all hours.
Question 7: Are there intact screens on the windowsand doors of the operating room?
• Are screens kept to prevent flies and other pestsfrom entering the OR?• Intact screens measure the cleanliness of the roomas well as the ability to keep flies and pests out of thehospital.
Question 8: Can X-rays be taken? (Is there film, devel-oper, and technical support?)
• Are X-rays available for use with operating roomprocedures? Are they available off-site?• X-rays measure the support facilities of the hospi-tal and the equipment available to assess woundsand fractures.
Question 9: Is sterilization equipment always avail-able/working? (For drapes and instruments)
• Can equipment be sterilized prior to use or reuse?• Sterilization equipment allows for surgical proce-dures to be done under sterile conditions, limitingpossible infectious complications and also indicatessome level of support facilities available.
Question 10: Is blood available within 30 minutes?• Availability of blood may be associated with a phle-botomist available within 30 minutes to draw bloodfor use, or an off-site storage/blood transfer facility.• If blood is not stored on premises, blood may beavailable through other means. Landmine victimsfrequently require blood transfusions and the abilityto store blood may reduce complications.
Question 11: Is stored blood available?• Stored blood in hospital should measure whetheror not blood is available immediately upon demand(check with Question 10)• The response is “yes” if stored blood is availableon the premises and indicates whether or not refrig-eration is available on-site.• A walking blood bank near local staff or commu-nity that has been typed so they can donate bloodrapidly may also be a solution.
Question 12: Is a laboratory available and working tomeasure hematocrit or hemoglobin?
• The “laboratory” may consist of the ability to cen-trifuge/spin blood to obtain hematocrit levels. Theselevels would be used to diagnose anemia and to deter-mine whether or not blood transfusion is necessary. • The ability to measure Hct/Hgb should used as asurrogate for a very basic laboratory facility. The abil-ity to test blood indicates a slightly higher standard.
Question 13: Is a laboratory available and working totest blood for viruses?
• Can blood be tested for infections such as HIV,Hepatitis B and C, malaria and syphilis?
Question 14: Are patient charts kept?• Is the patient monitored for the entire period ofhospitalization?• Patient charts indicate the level of follow-up care.If patient charts are kept, the patient was followedfor the duration of hospitalization and the facilitywould probably be able to institute a surveillancesystem.
Question 15: Is an operating room log kept?• Are types of procedures performed in the OR mon-itored? Is usage of the OR monitored?• Presence of operating room logs indicate that thetypes of procedures in the operating room are fol-lowed, that the usage of the OR is measured, andthat more complicated procedures are probably per-formed. These records can also be accessed for hos-pital surveillance or survey patients or socialreintegration patients.
Question 16: Are Anesthesia records kept?• Are intra-operative vital signs continuously moni-tored?
2 2 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

• Anesthesia records indicate that intra-operativevital signs are measured and recorded. Anesthesiarecords provide another measure of the level ofpatient management.
Question 17: Are vital signs recorded on a daily basis?• Are temperature, heart rate, respiratory rate, andblood pressure measured on a daily basis?• A daily record of vital signs indicates post-opera-tive care and the presence of some staff qualified (bycurrent hospital standards) to follow the patient andmeasure progress or identify complications.
Operating RoomA hospital that can easily care for landmine victims
can be expected to answer “yes” to all questions. Sucha facility can provide for complex surgery and has ade-quate supplies for the performance of these procedures.Such a hospital most likely acts as a referral center andis the final facility usually encountered by landminevictims.
Basic abilities/capacities include cement floor/tileand operating lights. Mid-level technical expertiseincludes suction, circuit anesthesia. Supplies for 2abdominal cases per day, circuit anesthesia, and endo-tracheal intubation would be functions of moreadvanced, referral hospitals.
Question 18: Is the operating room floor cement or tile?• Can the floor be cleaned? Is this a permanent facility?• Cement or tile flooring measures the cleanliness of theoperating room and the permanence of the structure.
Question 19: Are operating lights available and working?• Operating room lights, with the presence of elec-tricity (Question 6) measures the ability to providecontinuous care.
Question 20: Are enough surgical supplies availablefor 2 abdominal cases per day?
• Supplies for 2 abdominal cases per day indicatesthat major operations may be performed and thatsterilized equipment and personnel are available. • An answer of “yes,” to this question assumes ade-quate personnel and sterilized equipment. RecheckQuestion 9 (Is sterilization equipment available?) Asthis question should then also be affirmative asshould questions 4, 5, and 10.
Question 21: Is suction available and working?• Suction should be considered as mid-level techni-cal expertise.
Question 22: Is circuit anesthesia available and work-ing for 2 abdominal cases per day?
• Circuit anesthesia indicates continuous anesthesiawith the ability to intubate the patient. (Question 23)
Question 23. Are supplies for endotracheal intubationavailable and working?
• Endotracheal intubation allows artificial respiration. • Circuit anesthesia allows for more complex proce-dures.• Endotracheal intubation requires anesthesia forlarger procedures and is used in more complex pro-cedures.
Personnel
Question 24: Is a medical officer available 24 hours aday?
• Is a general physician (family practice, internalmedicine, etc) available at all times of the day?• The presence of a medical officer twenty-fourhours per day equates with a higher level of care.
Question 25: Is the hospital open for surgery 24 hoursa day?
• Surgery may be inclusive of less technical opera-tions (lacerations, c-sections, etc.) and does notrequire that a surgeon be on the premises or on staff;however, some physician presence is necessary foran answer of “yes.”
Question 26: Is a trained surgeon available 24 hours aday? (Trained for closed chest trauma, abdominalexploration and amputations)
• Can a trained surgeon be called for immediate sur-gery in case of an emergency?• Twenty-four hour surgery and the presence of atrained surgeon provides for the highest level ofcare.
Question 27: Is anesthesia available 24 hours a day?(Including ET intubation)
• An answer of “yes” would only be possible if Ques-tion 23 (ET ability) is answered in the affirmative. • Presence of anesthesia 24-hours per day indicatesthat more technical procedures may be performed
C A PA B I L I T Y A N D S O C I A L R E I N T E G R AT I O N T O O L S 2 3

Question 28: Are nursing staff available 24 hours a dayfor intravenous infusions?
• Are nursing staff trained to administer intravenousfluid and antibiotics for seriously ill patients? • Presence of nursing staff indicates that post-operativevital signs and potential complications are monitored.
Question 29: Is there staff to help feed and take care ofpatients post-op?
• Do hospital staff follow patients for the duration oftheir hospital stay? Are patients fed or do familymembers stay in the hospital to care for the patient?• Hospital staff to feed and care for patients helps toprovide an estimate of the size of the facility and thestaffing capabilities.
Question 30: Number of hospital beds• This number indicates the size of the hospital.• The number of hospital beds along with the num-ber of in-patient admissions per year help to providean estimate of facility utilization.
Question 31: Number of patients hospitalized in previ-ous 12 months
• Check annual report. Approximations can be usedif actual records are unavailable. This numbershould be in-patient admissions only. • These questions allow for calculation of an overallmortality rate per hospital (deaths/# hospitalized).
Question 32: Number of surgical procedures in previ-ous 12 months
• Check annual report. Approximations can be usedif actual records are unavailable.• Calculation of a surgical mortality rate (surgicaldeaths/procedures)
Question 33: Number of abdominal operations per year• Check annual report. Approximations can be usedif actual records are unavailable.• Abdominal operations are considered more com-plex surgery (more so than amputations) and meas-ure the ability of the hospital to perform larger cases.
Question 34: Number of cesarean sections per year• Check annual report. Approximations can be usedif actual records are unavailable.• Cesarean sections per year measures the ability ofthe hospital to perform more technical but not com-plex surgery.
Question 35: Number of landmine victims treated inprevious 12 months
• Check annual report. Approximations can be usedif actual records are unavailable. • Number of landmine victims treated in previous 12months allows a measurement to be compared fromcommunity data. Also names of victims can be col-lected for social reintegration surveys. It is impera-tive to note that this number does not necessarilyindicate the number of landmine victims peryear, as it will not include those with minorinjuries or those who died and were never takento a hospital.
Question 36: Number of amputations performed onlandmine victims in previous 12 months
• Check annual report. Approximations can be usedif actual records are unavailable. • Amputation rate: Number of amputations/numbertreated (level of severity of patients treated in hospital)
Question 37: Number of landmine victims who died inthe hospital in previous 12 months
• Check annual report. Approximations can be usedif actual records are unavailable.• Mortality of those treated: number of victims whodied/number treated
Question 38: Number of operations for landmine vic-tims in previous 12 months
• Check annual report. Approximations can be usedif actual records are unavailable.• Operation rate: number operated on/number treated(level of severity of patients arriving in hospital
2. ORTHOPAEDIC CENTER CAPABILITY SURVEY TOOL
Initial Meeting: Request for AssistanceAt least one meeting at the orthopaedic center will
be necessary to obtain the required data. Survey admin-istrators should contact the orthopaedic center directorand request at least one hour to describe the survey indetail. If possible, the survey and letters of introductionshould be forwarded before the meeting. Two purposesfor the meeting should be identified.
1. The survey will highlight the capability of thefacility in providing assistance for landmine victims. Ifpossible, the director should complete the survey at the
2 4 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

initial meeting. However, it may be necessary to returnfor a second meeting.
2. A random list of names can be useful for institut-ing the social reintegration survey tool. If such a list isto be used, a complete list of names and addresses of alllandmine victims seen at the facility within the timeframe specified should be requested. Surveyors willthen randomly select names for patients to interviewaccording to the methods detailed below.
Second Meeting: Data CollectionA second meeting with the director of the center may
be necessary to retrieve the completed survey form orcollect the list of landmine victims. At this time, thedirector should be informed and reassured that resultswill be made available as they are generated.
Survey Questions
Question 1: Type of Center• An orthopaedic center refers to a facility that man-ufactures and/or provides prosthesis, wheelchairs orcrutches to amputees and persons with disabilities. Arehabilitation center employs physical therapists andprovides long term rehabilitation and physical ther-apy. A center may be one or both.• The type of center and the number of each type(orthopaedic and/or rehabilitation) indicates thecapability of the country to fit prosthesis and pro-vide rehabilitation. One can then ask the question,are more orthopaedic centers necessary? More reha-bilitation centers?
Question 2: Affiliation• Record major affiliation of the facility. “Public”refers to governmental, non-military facility.• Affiliation indicates sources of funding. If most ofthe facilities are military, do civilians receive ade-quate care? If most are public, is there an opportu-nity for private funding?
Question 3 and Question 4: Are there established refer-ral patterns and where do referrals come from?
• “Hospitals” refer to a standardized method ofreferral from hospitals to orthopaedic centers. • Location of referral indicates the pattern of the sys-tem. Is there a formal hospital referral system? Theimplementation of one might be necessary in order
to ensure adequate follow-up care. Is the communityaware of the center? Community education efforts(brochures, media, etc.) may be required to increaseknowledge of health facilities available.
Question 5: Number of patients fitted with prosthesisper year
• Information from annual report, preferably mostrecent year.• This number indicates the demand for services andmay be used as a numerator for Questions 6-8, i.e. # ofpatients/prosthetists, # of patients/physical therapists
Question 6: Number of prosthetists employed.• This should refer to paid and fully trained staffonly. • These figures provide a quantitative assessment ofthe adequacy of staff. Is there a small number ofprosthetists or physical therapists per patient? If so,more personnel may need to be hired. Is a small per-centage certified? More training may be required toassist the facility.
Question 7: Number of prosthetists ISPO certified• How many of the prosthetists are trained and meetthe standards or the International Society of Pros-thetists and Orthothists?
Question 8: Number of physical therapists employed• If the center is not a rehab center (Question 1), thisanswer should be zero. If this is not the case, verifywith the source.
Question 9: Do you have enough personnel?• Ask the source to define what is meant by enoughpersonnel, e.g “no waiting list” might be used as aguide for adequacy of personnel.
Question 9 provides a qualitative follow-up to Ques-tions 5-8.
• An administrator may feel that inadequate staffingis present, yet the patient load per personnel mayindicate that resources need to be targeted else-where. Conversely, the patient load may be largerthan expected, yet the administrator answers thatstaffing is adequate. Such situations would requirefollow-up and re-interview for further assessment.
Questions 10-14: Number of artificial limbs, primarylimbs, replacement limbs, wheelchairs, and crutchesmade per year.
C A PA B I L I T Y A N D S O C I A L R E I N T E G R AT I O N T O O L S 2 5

• Primary limbs are those fitted for a patient for thefirst time.• Replacement limbs are fitted for patients when aprimary limb is broken or inadequate.• These numbers present the capability of the facilityto provide mobility equipment to amputee and per-sons with disabilities.• The number of primary limbs compared to thenumber of replacement limbs can give a rough indi-cation of the number of amputations occurring dur-ing a given year and the longevity of prostheses.
Type of Prosthesis Used
Questions 15-18: Polypropylene, leather/wood, alu-minum, polyester/fiberglass
• If an answer of “yes” is given to any of these ques-tions, Questions 10-12 should have a value (i.e. If atype of prosthesis is made, then a certain numbershould be made per year). If this is not the case,query the source for verification.• On-site capability to make a prosthesis is measured.
Question 19: Do you have a polypropylene press andmould?
• If the answer to Question 19 is “yes,” and Question15 (polypropylene prosthesis made) is “no,” querythe source as to why.
Question 20: Do you charge for a prosthesis?• Does someone outside the facility (patient, govern-ment, etc.) pay for a prosthesis, or is it give free ofcharge? Whether or not the facility charges for pros-thesis indicates the access to care by the patient andalso the resources available to the facility. • Do they have inadequate staff because they pro-vide care to the indigent whereas another facilityrequires payment yet have adequate staffing? Dothey charge yet have inadequate supplies?
Question 21: Do you have adequate supplies for manu-facturing prostheses?
• Is material available for manufacturing prostheses?• Adequate supplies for manufacture points to theability of the facility to provide enough prostheses tokeep up with patient demand, especially if patientload/year is high and no charge is assessed.
Question 22: Is there standardized manufacturing ofprostheses?
• Is a singular and simple format used every time inthe manufacture of prostheses? This question is mostapplicable to those with a polypropylene press(Question 19) and other who manufacture their ownprostheses (Questions 10-12) • Is a simple format used for the manufacture of aprosthesis? Standard manufacture indicates a for-malized method for training. If no standard is main-tained, quality control and training efforts might bedirected towards manufacture.
Question 23: Is there centralized manufacturing ofprostheses?
• Does the country possess a central site for the man-ufacture of prostheses? • Central distribution points to a country’s ability toprovide prostheses. If no standard is maintained(Question 22) and there is no centralized distributionpoint, the quality of the prosthesis might be inade-quate to meet patient needs. If central distribution isabsent, local capacity building through training pro-grams in the manufacture of prosthesis might offermore value.
Question 24: Are there other ortho/rehab centers near by?• Are centers located close enough for easy referralof patients in case one center receives too manypatients at once? • If the patient load of the facility is high, cananother center meet the increased demand?
Question 25: Are there local training programs fortechnicians?
• Does the center itself provide training programs fortechnicians? • Is the program sustainable? For example, if a non-governmental organization is funding the facility(Question 2: Affiliation), do they provide a mecha-nism for continuation after the NGO leaves thecountry or turns over the facility?
Question 26: Are there outreach programs?• Does the center itself provide outreach? Outreachshould be described as entering into the communityto provide information regarding rehabilitation andassistance to patients who may not be able to reachthe clinic/center on their own accord.
2 6 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

• Outreach programs and employment of disabledpersons provide a measure of the facilities’ efforts toreintegrate the victim into society.
Question 27: Are there appropriate facilities and sur-geons available to do stump revisions?
• “Appropriate facilities” include hospital servicesand personnel for stump revision. These do not needto be in the center itself.• This question provides a qualitative assessment bythe facility director of the hospital’s ability to dostump revisions, i.e. If stump revision percentagesare high, does the problem lie with the surgeon’sability to perform a primary amputation, thepatient’s ability to care for the amputation or accessto secondary surgery?
Question 28: Can you estimate the number of patientswho need stump revisions?
• A stump revision indicates the need for additional sur-gery on the stump in order to properly fit a prosthesis.• The source should be asked to provide as close anapproximation as possible, but it should be stressedthat only an approximation (not an exact figure) isnecessary. • Stump revisions point to either the quality of theamputation itself (use with hospital capability sur-vey) or the care and management of the stump. If thenumber is large, training might be required in one ofthese two areas or there may be inadequate access tosurgical interventions.
3. SOCIAL REINTEGRATION AND REHABILITATION SURVEY TOOL
RationaleThis is one of the most important tools in this manual.It measures the effectiveness of the rehabilitativeefforts—whether they be from hospitals, rehabilitationcenters, governmental or non-governmental efforts.This data will assist in helping these resources finetunetheir efforts.
The purpose for the Social Reintegration and Reha-bilitation Survey Tool is to determine the extent towhich the needs of landmine victims are satisfied. It isdesigned to provide a multidimensional measure of avictim’s return to society after experiencing physicaltrauma associated with a landmine injury. These
dimensions of social reintegration measured by the sur-vey fall under the following categories:
I. Informational AccessDoes the victim have access to information andknowledge concerning the injury
II. Disability DiscriminationDiscrimination based upon disability (Has the injuryaffected the victim’s ability to gain employment,schooling, training, etc.)
III. Social SupportPersonal social support structures indicate the levelto which the victim is cared for and receives help, beit informational, emotional, financial or physicalsupport.
Access to medical facilities, which includes boththe provision of information concerning the victim’sinjuries as well as the surgical processes required fora prosthesis, i.e. does the victim understand the needfor stump revisions?
IV. Institutional ResourcesWhat kind of systems are in place to provide efficientand reliable assistance to mine victims, i.e. is there ahospital or clinic close to mine-infected villages?
MeetingsThis survey is to be used for all surviving victims oflandmine injuries who sustained their injuries morethan 12 months ago, thereby insuring that they haveundergone some kind of reintegration and/or rehabilita-tion process which is now being evaluated. To mosteffectively accomplish the goals of this survey, meet-ings must be set up with officials from the local hospi-tals, rehab/orthopaedic centers and village keyinformants. Due to the sensitive nature of speakingwith mine victims, meetings should also be arrangedwith representatives of the local Ministries of Healthand Social Welfare.
ImplementationLists of victims to survey can be obtained either fromregistries at hospitals and orthopaedic centers or directlyfrom local villages and districts. The decision on groupof patients to survey depends upon who will use the dataand the availability of initial information. Either random
C A PA B I L I T Y A N D S O C I A L R E I N T E G R AT I O N T O O L S 2 7

sampling or cluster sampling of landmine survivors (seenext chapter) can accomplish to desired goal of obtain-ing a representative sample of rehabilitation and socialreintegration in a defined community.
While administering the survey, if there are ques-tions which prove to be emotionally difficult for thevictim, it is advisable to either move on to the nextquestion or end the survey depending on the situation,i.e. “Refused to Answer” is a completely acceptableanswer and should not be pressed further. The benefitsof this survey include its straightforward but compre-hensive construction and the potential for interventionsbased upon the collected data. Note: One significantdifference between this and the Community SurveyTool is that this survey must be done with the victim asopposed to the head of their household.
Survey Questions
Questions 1–3: Source of Sample• By knowing where the victim population is beingsampled from, you can compare and contrast infor-mation gained from the sample with the other sur-veys that may have utilized the same source, therebycreating a general picture of each sample source’sresource profile.• This profile can then guide future interventionsaimed at increasing resources within respective sam-ple sources such as a specific rehabilitation center orvillage.
Questions 4-8: Personal Data• During the analysis stage, it will be important todetermine the relative age, gender and year of injuryof landmine survivors for purposes of intervention.
Questions 9-17: Types of Injuries• Gaining an understanding of the types of injuriesexperienced by landmine survivors will help deter-mine which medical resources need to be targetedtowards specific disabilities. For example, the needsof someone who has been blinded are different thanthe needs of someone who has lost both their legs.
Question 18: Where did you receive medical care?• Information on the type of medical care receivedwill allow for targeting of specific facilities forimprovement or possible interventions.
Question 19: Physical Therapy Upon Leaving the Hos-pital
• Identifying the number of survivors receivingrehab or physical therapy will allow for evaluationof access and current standards of care.
Question 20: Did you have an amputation?• This section is to evaluate survivors with amputa-tions and the care they receive.
Question 21: How many orthopaedic/rehab centerhave you visited?
• This question provides insight into whether sur-vivors obtain proper care or must seek equipmentand care from varying sources.
Questions 22-25: Mobility Equipment• It is just as important to know that survivors areusing some kind of mobility equipment as well whatkind of equipment they are using. If a large propor-tion of survivors are not using mobility equipmentthen this must be further investigated. • Survivors who are waiting for a long time for theirmobility equipment are experiencing a high degreeof frustration and discomfort in their daily lives.
Question 26: How many surgeries did you need beforeyou could wear a prosthesis?
• The number of surgeries needed in order to wear aprosthesis will help illustrate the effectiveness ofmedical therapy.
Question 27: Do you think you need additional surgeryor a stump revision?
• This question represents the survey’s first attemptto measure survivor’s perceptions of their injuriesand the services they receive. If you find a differ-ence between what is perceived and what the needsare, interventions can then be sought. For example,if you find that a large number of survivors thinkthey need a stump revision when in fact their pros-thesis is at fault and therefore not being used, theneducation of survivors may be a priority.
Questions 28-35: Prostheses• These questions will provide basic informationconcerning a survivor’s use of prostheses. It will bevital to know if survivors do not have a prosthesis orif they have not had one in some time. You will beable to determine how durable and comfortable their
2 8 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

prostheses are, why they may not be wearing theirprostheses and their perceptions on whether or nottheir prostheses are fully functional or in need ofrepair. This will allow you to know if the survivorshave been given proper instructions on the care oftheir prostheses, how often the prostheses should bereplaced, and if they possess a basic understandingof the mechanics of their prosthetic.
Questions 36-42: Employment Information• These series of questions provide a measure of theimpact of a survivor’s injuries upon their ability tobe employed, whether it be as a soldier in the army,a government administrator, or a farmer. The beforeand after nature of the questions will allow you toknow to what extent their injury has affected theirpotential as a productive member of society. Youwill be able to figure out what injuries have providedthe most amount of harm in limiting the potential ofwhere and for how long a survivor works.
Question 43-44: Legal issues concerning disabilities• Policies and laws concerning persons with disabil-ities will vary greatly from country to country, butthe extent to which a survivor knows of the laws oftheir nation may impact their well-being. Forinstance, if a survivor is unaware that there arenational laws concerning mine-disabled survivors,then they are also likely to be unaware that they areeligible for a pension due to their injury stemming
from a landmine. In addition, if aid agencies caninsure that survivors are made aware of national aswell as international laws governing the rights ofmine survivors, then they may become empoweredto both pursue their entitlement as disabled and asglobal citizens.
Questions 45-47: The accessibility of health careresources
• The information collected in this section enablesyou to pinpoint the inadequacies in medical care formine survivors. As well, if a rehab center is locatedfar away it will limit a victim’s desire and ability totravel for physical therapy and medical follow-ups.
Questions 48-49: Social Support Capability• These question outline the support network of aparticular community. In countries where there is lit-tle community support, government institutions orother groups may be necessary to provide the carewhich is needed for landmine injury survivors.
Questions 50-51: Injury Discrimination and Limita-tions
• This information, when viewed in relation toemployment status and injury, can help to give anindication of the effectiveness of rehabilitation andsocial reintegration. survivors who are able to func-tion in society are less likely to feel that they aretreated differently from others or suffer limits totheir education or work.
C A PA B I L I T Y A N D S O C I A L R E I N T E G R AT I O N T O O L S 2 9

3 0 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

Whatever method of data collection or sampling isused, it is imperative to get national and local popula-tion figures. The number of victims is only of value ifrelated to a reliable denominator (population data).Accurate population data may be difficult to obtain as itmay have political value. Check as many sources aspossible in order to assure the validity of the results.These data are crucial in developing ratios and trackingdifferences between various regions and countries.
Sampling enables us to conduct a scientificallysound study without visiting all members of the popu-lation at risk. Sampling should only become an issuewhen conducting either the Community Survey or theSocial Rehabilitation Survey. The Hospital and KeyInformant Surveys can guide the researcher to regionsreported to have landmine victims. The CommunitySurvey allows the calculation of rates, since the hospi-tal data alone misses those who may have neverreceived documented medical care. In completing thetwo capability surveys, it should be feasible to visiteach and every facility to administer the survey, ensur-ing 100% coverage (in theory). However, in countrieswith large numbers of landmine victims, it will proveto be impossible to administer a survey to every sur-vivor; even if one had the time and financial resourcesto visit thousands of survivors, it would prove to beimpossible to locate every one.
There are essentially four sampling methods that canbe used for the landmine project: simple random sam-pling, systematic sampling, two-stage cluster samplingand sentinel site sampling. In general, one should startat the hospitals to identify where survivors are comingfrom and then visit these districts. The Key Informanttool will then be useful in determining the villages thatare most affected. Households within these villagesshould then be visited and family members or survivorsinterviewed.
In situations where there is social collapse and keyinformants such as chiefs, mayors, or priests do notexist then one of three methods is necessary to obtain a
sample. First, if all houses in the village or affectedareas are known then a random survey can be under-taken. If the number of households is not too large andthere are adequate resources, a systematic sample,every nth house, can be sampled, providing the entirevillage is covered. Lastly, if only rough estimates of thevillage populations in a region exist, a two-stage, 30-cluster survey should be undertaken. This last methodshould be undertaken as a last resort, because it isreally only valid if the prevalence is high and it usesconsiderable resources.
CALCULATING A SAMPLE SIZEThis discussion of sample size may seem compli-
cated at first glance, but it is simpler than you think ifyou try it. If you are having trouble, contact peoplewho have done previous statistical work for assistance.
Simply put, the sample size is the number of inter-views necessary to administer before the data can beconsidered to be statistically sound. The sample sizedepends on both the prevalence rate of landmineinjuries in the population and the investigator’s desiredprecision of the data. In most cases, the precision canbe assigned to be either ±5% or ±10% (using 5% willresult in a larger sample size). The sample size can thenbe calculated as:
Sample size = (1.962x prevalence %)x(100 – prevalence %)
(Precision %)2
Therefore, with an estimated landmine victim preva-lence rate of 10%, and a precision of ±5%, the samplesize can be calculated to be (1.96
2x 10 x 90)/5
2= 138.
One would need to conduct 138 interviews to ensurequality of data.
However, it is important to note that:
•This formula is not valid if the prevalence rate iseither very low (<5%) or very high (>95%).
C O L L E C T I N G D ATA 3 1
9 COLLECTING DATA

•If the prevalence rate is in doubt, then it is best touse 50% as this will lead to a larger sample size.
•This formula is only valid for a large populationsize. As a general rule, this formula holds when thecalculated sample size represents less than about10% of the total population.
Simple Random SamplingSimple random sampling is a method that ensures thatevery member of the population has an equal chance ofbeing included in the sample. For example, once acomplete list of landmine victims is obtained from arehabilitation center in preparation for the Social Reha-bilitation Survey, this method is used to choose whichvictims should be surveyed, and how many surveyswill be necessary. If the number of recent landmine vic-tims is very large, this method can also be used tochoose to whom to administer the Community Survey.
• Obtain a complete, numbered list of landmine vic-tims that meet the criteria for the social rehabilita-tion survey (e.g. victim more than 12 months ago,still alive). This is your sampling frame. (for exam-ple, 1,200 victims) Each victim is assigned a numberstarting with 0001, 0002 and so forth.
• Using the random number table in Appendix A,choose any single digit number on the page as anarbitrary starting place (see sample 1 circled on ran-dom number table).
• Read down the column of numbers from this point,looking at groupings of four numbers across (sincethe sampling frame is four digits). Ignore the spacebetween columns, if necessary. All numbers whichare less than or equal to the sampling frame (1,200in this case) are selected as members of the sample.For example, 0233 would be the first sample fromthis list. Going down from the circled number 1,5029 would be too large, same with 1,332. The num-ber 0233 would be victim number 233. This personis included as the first in your random sample. Thenext number for this sample would be 0733 or victimnumber 733.
• If any numbers are repeated, ignore them aftertheir first appearance. When you reach the bottom ofthe page, move to top of next column starting at
same relative position as original first number.(Example 4887). Proceed down this row. Continuefinding appropriate victim numbers until samplesize has been reached (138 in this case). If you reachthe end of the page before this is obtained, beginagain in first column of top of page to the left.
Systematic SamplingThis is an alternative to simple random sampling usedwhen it is difficult to obtain a sampling frame. Samplehouseholds are chosen systematically as they appear intime or space. For example, one household out of every15 households as field health workers walk systemi-cally around a village.
• Estimate the total number of households in the vil-lage.
• Calculate the sampling interval (s) by dividing thenumber of households by the required sample size(see above).
• Choose a random number less than or equal to thesampling interval. This is the number of the firstmember of your sample.
• Proceed in sequence to select one in every s mem-bers of the population for the sample until therequired sample size has been achieved
Two-Stage Cluster SamplingCluster sampling has been popularized by WHO’sExpanded Program on Immunization. It has becomepopular for making rapid assessments of large popula-tions because it is quicker and more convenient to organ-ize than simple random sampling. The basic idea is that,first, villages are chosen at random and, secondly, clus-ters of individuals or households are chosen within eachvillage. This method should only be used in a very largepopulation in which the number of landmine victims islarge and fairly uniformly distributed. These conditionsmay be rarely met for mine victim data.
To calculate cluster size, use the formula for samplesize given above and double the result. For example, inthe example given above, the sample size would be 138x 2 or 276. Then divide the sample size by the numberof clusters you require (usually 30) and round up to the
3 2 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

nearest whole number. This provides the number ofindividuals per cluster. In this example, the sample size276 is divided by the number of clusters 30 to get 9.2,which is rounded up to get 10 individuals per cluster.
• Make a list of all villages in the region togetherwith their population size.
• Calculate the cumulative population size as you godown the list.
• Calculate the sampling interval by dividing thetotal population by the number of clusters to beselected (usually 30).
• Select a random number which is less than or equalto your sampling interval, and using the cumulativepopulation total, find the village it represents.
• The next village is obtained by adding the sam-pling interval to this starting number and locatingthe village which it represents. It may be that thesame village, especially if it has a proportionallyhigh population, will be chosen more than onceusing this method. If that is the case, then conductmore than one cluster survey in those villages.
• Continue to add the sampling interval to the previ-ous number obtained until the correct number ofclusters has been obtained.
Once the list of villages to be surveyed is deter-mined, then for each village:
• Go to a central place in the village.
• Spin a bottle and mark the direction in which itpoints.
• Walk to the edge of the village in this direction andcount the number of households on the route.
• Choose a random number to identify one of thehouseholds on the route.
• Start with this house and select the individuals liv-ing in the house who belong to the population beingsampled. If no one fits the criteria, continue to thenext house.
• Continue visiting neighboring households until thenumber of individuals per cluster is obtained.
• If a village is to have more than one cluster, thenrepeat all the steps for each cluster.
Sentinel Site SurveillanceBecause landmine victims are often grouped around
affected villages and not evenly distributed throughouta region, two-stage cluster sampling is usually not aneffective means of measuring the impact of landminesin the region. If by chance, the clusters that the investi-gators chose do not correspond with where the land-mine victims are, then the data will subsequently beunder-reported. If by chance, one does choose the cor-rect villages, then the data will be over-reported.Because of this fact, sentinel site surveillance is usuallythe most accurate means of reporting data on landminevictims.
Sentinel sites are chosen because they are known tobe affected by landmines, and therefore have a greaterchance of having a large number of victims. While thisdata cannot be extrapolated to the greater area as awhole, it does give an accurate picture of the affectedregions.
In order to perform sentinel site surveillance, a num-ber of key informant interviews should be administeredto identify as many mine-affected villages in the regionas possible. When enough interviews have been com-pleted a list of all the villages mentioned should becompiled. These villages can then be put into a randomorder, using a random number table. If time andresources permit, then the rest of the villages in theregion can also be put into a random order, and thesevillages can be visited after completion of all the sen-tinel sites.
Upon arrival in each of the sentinel villages, if acomplete list of landmine victims is unavailable, thenindividual households can be chosen for sampling pur-poses using either one of the three previously describedmethods.
C O L L E C T I N G D ATA 3 3

3 4 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E
APPENDIX A: RANDOM NUMBER TABLE
Start
See page 32for instructionson how to usethis table. Themarkings onthis table arean exampledescribed onpage 32.

We recommend the following journal articles for back-ground reading.
Bennett S, Woods T, Liyanage WM, Smith DL. A sim-plified general method for cluster-sample surveys ofhealth in developing countries. World Health Statis-tics Quarterly,44: 98-106 (1991). A good explana-tion of conducting a cluster-sample survey. A bitmore technical than the other articles cited, but stilluseful for the field health worker.
Ledogar RJ, Andersson N. Impact estimation throughsentinel community surveillance. Third World Plan-ning Review. 15(3): 263-272, (1993). This excellentoverview of sentinel site surveillance is designed foruse in urban planning, but can be adapted to the pub-lic health sector. The article includes sections onselection of sites, constraints of the method andmeasuring impact.
Macfarlane SBJ. Conducting a descriptive survey: 1.planning the survey. Tropical Doctor. 26: 161-164,(1996).
Macfarlane SBJ. Conducting a descriptive survey: 2.choosing a sampling strategy. Tropical Doctor. 27:14-21, (1997).
Macfarlane SBJ. Conducting a descriptive survey: 3.summarizing and presenting data. Tropical Doctor.28: 18-28, (1998).
This three-part series offers an excellent presentationof how to conduct descriptive surveys, such as thelandmine community survey. Explanations on how toplan the survey, calculating sample size, choosing asampling method, calculating cluster size and differentmethods of presenting the data. The series should bemust reading for anyone conducting this type of publichealth surveillance.
3 5
APPENDIX B: BIBLIOGRAPHY

APPENDIX C: ENDNOTES1
International Campaign to Ban Landmines, Land-mine Monitor Report 1999: Toward a Mine-FreeWorld, 1999. www.icbl.org
2Humanitarian Demining, “Direct and Indirect Con-
sequences of Landmines on Public Health,”www.brtrc.com, October 7, 1998.
3-4 Ascherio A, Biellik R, Epstein A, Deaths andInjuries Caused by Landmines in Mozambique, Lancet,1995; 346: 721-724.
5 Krug E, Ikeda R, Qualls M, Anderson M, Rosen-berg M, Jackson R, “Preventing Land Mine-RelatedInjury and Disability: A Public Health Perspective,”Journal of the American Medical Association (JAMA),1998; 280 (5) 465-6.
3 6 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

Overview Tools Country Capacity ToolKey Informant Tool
Epidemiological ToolsHospital Surveillance or Survey of
Landmines Injuries Tool Community Survey Tool
Capability and Social Reintegration ToolsHospital Capability Survey ToolOrthopaedic/Rehab Center Capability Survey Tool Social Reintegration and Rehabilitation Survey Tool
B L A N K S U RV E Y T O O L S 3 7
APPENDIX D: BLANK SURVEY TOOLS

3 8 M E A S U R I N G L A N D M I N E I N C I D E N T S & I N J U R I E S A N D T H E C A PA C I T Y T O P R O V I D E C A R E

Cou
ntry
Cap
acity
Too
l / P
age
1 of
1
OV
ER
VIE
W T
OO
L 1
Cou
ntry
Cap
acit
y T
ool
Dat
e of
Sur
vey:
____
____
____
____
____
____
____
____
____
___
1.C
ount
ry:_
____
____
____
____
____
____
____
____
____
_
Sour
ce o
f D
ata:
____
____
____
____
____
____
____
____
_
2.Po
pula
tion:
____
____
____
____
____
____
____
____
____
3.G
eogr
aphi
c A
rea(
sq.k
m.)
:___
____
____
____
____
____
_
4.N
umbe
r of
Dis
tric
ts:_
____
____
____
____
____
____
____
5.N
umbe
r of
Hos
pita
ls w
ith S
urgi
cal C
apab
ility
:
(Lis
t Sep
arat
ely)
____
____
____
____
____
____
____
____
6.N
umbe
r of
Med
ical
Fac
ilitie
s (N
o Su
rger
y)
(Lis
t Sep
arat
ely)
____
____
____
____
____
____
____
____
7.N
umbe
r of
Pro
sthe
tic/R
ehab
Fac
ilitie
s:
(Lis
t Sep
arat
ely)
____
____
____
____
____
____
____
____
8.N
umbe
r of
Phy
sici
ans:
____
____
____
____
____
____
___
9.N
umbe
r of
Sur
geon
s:__
____
____
____
____
____
____
__
10.
Nat
iona
l or
Reg
iona
l Fir
st A
id C
ertif
icat
ion:
0.N
o1.
Yes
9.U
nkno
wn
11.
Nat
iona
l or
Reg
iona
l Em
erge
ncy
Med
ical
Ser
vice
s Sy
stem
:(B
CL
S, A
CL
S, A
TL
S)0.
No
1.Y
es9.
Unk
now
n
12.
Law
s or
dec
rees
for
per
sons
with
dis
abili
ties?
0.N
o1.
Yes
9.U
nkno
wn
13.
Law
s or
dec
rees
des
igna
ted
for
acce
ss to
pub
lic b
uild
ings
for
min
e vi
ctim
s or
dis
able
d pe
rson
s?0.
No
1.Y
es9.
Unk
now
n

OV
ER
VIE
W T
OO
L #
2 Key
Inf
orm
ant
Too
l
Inte
rvie
wer
Nam
e:__
____
____
____
____
____
____
____
____
____
Dat
e of
Sur
vey:
____
____
____
____
____
____
____
____
____
____
Cou
ntry
:___
____
____
____
____
____
____
____
____
____
____
___
Dis
tric
t:___
____
____
____
____
____
____
____
____
____
____
____
Sour
ce o
f D
ata:
____
____
____
____
____
____
____
____
____
____
_
Dis
tric
t Pop
ulat
ion:
____
____
____
____
____
____
____
____
____
__
Dis
tric
t Are
a (s
q. k
m.)
:___
____
____
____
____
____
____
____
____
Com
mun
ity L
eade
r N
ame:
____
____
____
____
____
____
____
____
Add
ress
:___
____
____
____
____
____
____
____
____
____
____
___
Num
ber
of H
ospi
tals
in D
istr
ict (
Surg
ery)
:
(Lis
t Sep
arat
ely)
____
____
____
____
____
__
Num
ber
of M
edic
al F
acili
ties
in D
istr
ict (
No
Surg
ery)
:
(Lis
t Sep
arat
ely)
____
____
____
____
____
__
Num
ber
of P
rost
hetic
/Reh
ab C
ente
rs:
(Lis
t Sep
arat
ely)
____
____
____
____
____
__
Are
hou
ses
or b
uild
ings
in th
e co
mm
unity
cur
rent
ly m
ined
or
boob
ytr
appe
d?0.
No
1.Y
es
Are
fie
lds
or f
arm
land
cur
rent
ly m
ined
?0.
No
1.Y
es
Hav
e liv
esto
ck b
een
lost
to m
ines
in th
e pr
evio
us 1
2 m
onth
s?0.
No
1.Y
es
Are
wat
er s
ourc
es in
the
com
mun
ity c
urre
ntly
min
ed?
0.N
o1.
Yes
Has
the
popu
latio
n be
en d
ispl
aced
bec
ause
of
land
min
es in
the
prev
ious
12 m
onth
s? 0.N
o1.
Yes
Lis
t vill
ages
whe
re th
ere
are
land
min
e vi
ctim
s:
1.__
____
____
____
____
____
____
____
____
__
2.__
____
____
____
____
____
____
____
____
__
3.__
____
____
____
____
____
____
____
____
__
4.__
____
____
____
____
____
____
____
____
__
5. _
____
____
____
____
____
____
____
____
___
Key
Inf
orm
ant T
ool /
Pag
e 1
of 1

Hos
pita
l Sur
veill
ance
or
Surv
ey o
f L
andm
ine
Inju
ries
Too
l / P
age
1 of
2
EPIDEMIOLOGICAL TOOL #1

Hos
pita
l Sur
veill
ance
or
Surv
ey o
f L
andm
ine
Inju
ries
Too
l / P
age
2 of
2

EP
IDE
MIO
LOG
ICA
L T
OO
L #1
Com
mun
ity
Surv
ey T
ool
Inte
rvie
wer
Nam
e:__
____
____
____
____
____
____
____
____
____
_
Dat
e of
Int
ervi
ew: (
DD
/MM
/YE
AR
)
Vill
age/
Clu
ster
Num
ber:
Hou
seho
ld N
umbe
r:
Fam
ily L
eade
r N
ame:
____
____
____
____
____
____
____
____
____
_
Add
ress
:___
____
____
____
____
____
____
____
____
____
____
____
Dis
tric
t:___
____
____
____
____
____
____
____
____
____
____
____
_
1.N
umbe
r of
peo
ple
livin
g in
hou
seho
ld 1
2 m
onth
s ag
o:
2.N
umbe
r of
peo
ple
livin
g in
hou
seho
ld n
ow:
3.N
umbe
r of
peo
ple
kille
d by
land
min
es in
pre
viou
s 12
mon
ths:
(Lis
t eac
h se
para
tely
)N
ame:
____
____
____
____
____
____
____
____
____
____
_D
ate
of in
jury
:___
____
____
____
____
____
____
____
____
Loc
atio
n:__
____
____
____
____
____
____
____
____
____
_N
ame:
____
____
____
____
____
____
____
____
____
____
_D
ate
of in
jury
:___
____
____
____
____
____
____
____
____
Loc
atio
n:__
____
____
____
____
____
____
____
____
____
_N
ame:
____
____
____
____
____
____
____
____
____
____
_D
ate
of in
jury
:___
____
____
____
____
____
____
____
____
Loc
atio
n:__
____
____
____
____
____
____
____
____
____
_
4.N
umbe
r of
peo
ple
inju
red
by la
ndm
ines
in p
revi
ous
12 m
onth
s:(L
ist e
ach
sepa
rate
ly)
Nam
e:__
____
____
____
____
____
____
____
____
____
___
Dat
e of
inju
ry:_
____
____
____
____
____
____
____
____
__L
ocat
ion:
____
____
____
____
____
____
____
____
____
___
Nam
e:__
____
____
____
____
____
____
____
____
____
___
Dat
e of
inju
ry:_
____
____
____
____
____
____
____
____
__
Loc
atio
n:__
____
____
____
____
____
____
____
____
____
_N
ame:
____
____
____
____
____
____
____
____
____
____
_D
ate
of in
jury
:___
____
____
____
____
____
____
____
____
Loc
atio
n:__
____
____
____
____
____
____
____
____
____
_
5.H
ave
hous
es o
r bu
ildin
gs in
you
r vi
llage
bee
n m
ined
or
boob
ytr
appe
d?0.
No
1.Y
es9.
Unk
now
n
6.A
re y
our
fiel
ds o
r fa
rmla
nds
curr
ently
min
ed?
0.N
o1.
Yes
9.U
nkno
wn
7.A
re y
our
wat
er s
ourc
es c
urre
ntly
min
ed?
0.N
o.1.
Yes
9.U
nkno
wn
8.H
ave
you
lost
live
stoc
k du
e to
land
min
es in
the
prev
ious
12
mon
ths?
0.N
o.1.
Yes
.
9.H
ave
you
had
to c
hang
e ho
uses
bec
ause
of
land
min
es in
the
perv
ious
12
mon
ths?
0.N
o.1.
Yes
.
10.
Hav
e yo
u ha
d to
mov
e to
a d
iffe
rent
are
a be
caus
e of
land
min
esin
the
prev
ious
12
mon
ths:
0.N
o1.
Yes
If a
ny h
ouse
hold
mem
bers
wer
e ki
lled
or in
jure
d by
ala
ndm
ine
cont
inue
wit
h se
para
te in
terv
iew
s fo
r ea
ch v
icti
m.
Com
mun
ity S
urve
y To
ol /
Page
1 o
f 4
EP
IDE
MIO
LOG
ICA
LT
OO
L#2

11.
Nam
e:__
____
____
____
____
____
____
___
12.
Vic
tim n
umbe
r:
13.
Age
of
vict
im a
t tim
e of
inju
ry:
14.
Sex
of v
ictim
:0.
Mal
e1.
Fem
ale
15.
Mili
tary
sta
tus
1.M
ilita
ry2.
Civ
ilian
16.
Vic
tim s
tatu
s1.
Loc
al c
ivili
an2.
Inte
rnal
ly d
ispl
aced
per
son
3.R
efug
ee4.
Ret
urne
e5
Dem
iner
8.O
ther
:___
____
____
___
9.U
nkno
wn
17.
Typ
e of
are
a:1.
Vill
age
2.R
oad/
road
side
3.R
iver
bank
4.Fi
eld
5.Fo
otpa
th6.
Surr
ound
ing
mili
tary
bui
ldin
g7.
Surr
ound
ing
gove
rnm
ent b
uild
ing
8.O
ther
____
____
____
____
____
9.U
nkno
wn
18.
Act
ivity
at t
ime
of in
jury
1.Fa
rmin
g2.
Dem
inin
g3.
Han
dlin
g M
ine
4.Fi
shin
g5.
Her
ding
6.H
untin
g7.
Col
lect
ing
woo
d/w
ater
/foo
d8.
Tra
velin
g in
veh
icle
/ on
anim
al9.
Pass
ing
by10
.Pl
ayin
g w
ith m
ine
11.
Uns
peci
fied
/unk
now
n12
.O
ther
:___
____
____
____
____
__
19.
Typ
e of
dev
ice:
1.A
P m
ine
2.A
T m
ine
3.U
XO
4.B
ooby
Tra
p9.
Unk
now
n
Clin
ical
Out
com
e
20.
Am
puta
tion
Upp
er L
imb
0.N
one
1.U
nila
tera
l2.
Bila
tera
l
21.
Am
puta
tion
Bel
ow K
nee
0.N
one
1.U
nila
tera
l2.
Bila
tera
l
22.
Am
puta
tion
Abo
ve K
nee
0.N
one
1.U
nila
tera
l2.
Bila
tera
l
Com
mun
ity S
urve
y To
ol /
Page
2 o
f 4

23.
Dea
fnes
s0.
Non
e1.
Uni
late
ral
2.B
ilate
ral
24.
Blin
dnes
s0.
Non
e1
Uni
late
ral
2.B
ilate
ral
25.
Hea
d/N
eck
Inju
ry0.
No
1.Y
es
26.
Abd
omen
/Tho
rax
Inju
ry0.
No
1.Y
es
27.
Lim
b In
jury
0.N
o1.
Yes
28.
Para
pleg
ia0.
No
1.Y
es
29.
Die
d0.
No
1.Y
es
30.
Oth
er:_
____
____
____
____
____
____
____
____
31.
Was
the
area
kno
wn
to b
e m
ined
?0.
No
1.Y
es9.
Unk
now
n
32.
Wer
e th
ere
othe
r vi
ctim
s in
sam
e bl
ast?
0.N
o1.
Yes
9.U
nkno
wn
33.
Num
ber
of o
ther
peo
ple
kille
d in
sam
e bl
ast:
34.
Num
ber
of o
ther
peo
ple
inju
red
in s
ame
blas
t:
35.
Did
the
vict
im g
o to
a h
ospi
tal?
0.N
o (G
o to
37)
1.Y
es9.
Unk
now
n
36.
Tim
e to
hos
pita
l.1.
Les
s th
an 3
hou
rs2.
3 to
6 h
ours
3.7
to 2
3 ho
urs
4.1
to 3
day
s6.
G
reat
er th
an 3
day
s.9.
Unk
now
n
37.
If th
e vi
ctim
die
d, w
here
did
it o
ccur
?1.
Site
of
inju
ry2.
Dur
ing
tran
spor
t3.
At h
ospi
tal
4.A
t hom
e9.
Unk
now
n
38.
Did
the
vict
im r
ecei
ve r
ehab
ilita
tive
care
?0.
No
1.Y
es9.
U
nkno
wn
39.
Did
the
vict
im r
ecei
ve a
pro
sthe
sis?
0.N
o (G
o to
41)
1.Y
es9.
U
nkno
wn
Com
mun
ity S
urve
y To
ol /
Page
3 o
f 4

40.
How
oft
en d
oes/
did
the
vict
im u
se a
pro
sthe
sis?
0.N
ever
1.L
ess
than
1 h
our
daily
2.1-
5 ho
urs
daily
3.6
hour
s or
mor
e da
ily9.
U
nkno
wn
41.
Did
the
vict
im w
ork
befo
re th
e in
jury
?0.
No
1.Y
es9.
U
nkno
wn
42.
If a
live,
doe
s th
e vi
ctim
cur
rent
ly w
ork?
0.N
o1.
Yes
Com
mun
ity S
urve
y To
ol /
Page
4 o
f 4

CA
PA
BIL
ITY
AN
D S
OC
IAL
RE
INT
EG
RA
TIO
N T
OO
L #
1
Hos
pita
l Cap
abili
ty S
urve
y T
ool
Inte
rvie
wer
Nam
e:__
____
____
____
____
____
____
__D
ate
of S
urve
y:__
____
____
____
____
____
____
___
Cou
ntry
:__
____
____
____
____
____
____
___
Sour
ce o
f D
ata:
____
____
____
____
____
____
____
_
Cat
chm
ent A
rea
Popu
latio
n:__
____
____
____
____
____
Cat
chm
ent A
rea
(sq.
km
.)__
____
____
____
____
____
1.H
ospi
tal N
ame:
____
____
____
____
____
____
____
_
2.A
ddre
ss:
____
____
____
____
____
____
____
_
3. A
ffili
atio
n:1.
Gov
ernm
ent
2.M
issi
onar
y3.
Publ
ic4.
Inte
rnat
iona
l NG
O5.
Priv
ate
6.M
ilita
ry7.
Oth
er
Phy
sica
l Pla
nt:
4. I
s th
ere
a de
dica
ted
room
for
sur
gica
l pro
cedu
res?
0)
No
1)
Yes
9)U
nkno
wn
5. I
s ru
nnin
g w
ater
ava
ilabl
e fo
r su
rger
y >
12
hour
s pe
r da
y?0)
N
o1)
Y
es9)
Unk
now
n
6. I
s el
ectr
icity
alw
ays
avai
labl
e fo
r su
rgic
al p
roce
dure
s?0)
N
o1)
Y
es9)
Unk
now
n
7. C
an s
teri
lity
alw
ays
be m
aint
aine
d in
the
oper
atin
g ro
om?
(Are
ther
ein
tact
scr
eens
on
the
win
dow
s an
d do
ors?
)0)
N
o1)
Y
es9)
Unk
now
n
8. C
an x
-ray
s be
take
n? (
Is th
ere
film
, dev
elop
er, a
nd te
chni
cal
supp
ort?
)0)
N
o1)
Y
es9)
Unk
now
n
9. I
s st
erili
zatio
n eq
uipm
ent a
lway
s av
aila
ble
and
wor
king
?
(Fo
r dr
apes
and
inst
rum
ents
)0)
N
o1)
Y
es9)
Unk
now
n
10.
Is b
lood
ava
ilabl
e w
ithin
30
min
utes
?0)
N
o1)
Y
es9)
Unk
now
n
11.
Is s
tore
d bl
ood
avai
labl
e?0)
N
o1)
Y
es2)
W
alki
ng B
lood
Ban
k9)
Unk
now
n
Hos
pita
l Cap
abili
ty S
urve
y To
ol /
Page
1 o
f 3
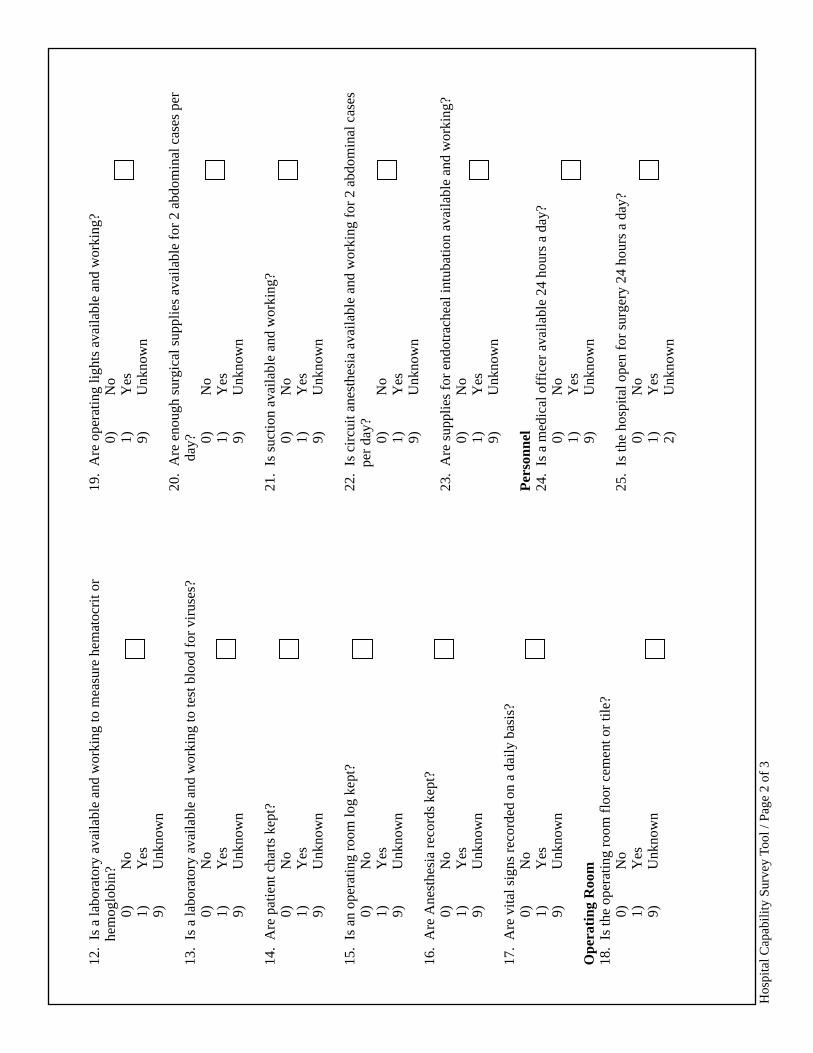
12.
Is a
labo
rato
ry a
vaila
ble
and
wor
king
to m
easu
re h
emat
ocri
t or
hem
oglo
bin?
0)
No
1)
Yes
9)U
nkno
wn
13.
Is a
labo
rato
ry a
vaila
ble
and
wor
king
to te
st b
lood
for
vir
uses
?0)
N
o1)
Y
es9)
Unk
now
n
14.
Are
pat
ient
cha
rts
kept
?0)
N
o1)
Y
es9)
Unk
now
n
15.
Is a
n op
erat
ing
room
log
kept
?0)
N
o1)
Y
es9)
Unk
now
n
16.
Are
Ane
sthe
sia
reco
rds
kept
?0)
N
o1)
Y
es9)
Unk
now
n
17.
Are
vita
l sig
ns r
ecor
ded
on a
dai
ly b
asis
?0)
N
o1)
Y
es9)
Unk
now
n
Ope
rati
ng R
oom
18.
Is th
e op
erat
ing
room
flo
or c
emen
t or
tile?
0)
No
1)
Yes
9)U
nkno
wn
19.
Are
ope
ratin
g lig
hts
avai
labl
e an
d w
orki
ng?
0)
No
1)
Yes
9)U
nkno
wn
20.
Are
eno
ugh
surg
ical
sup
plie
s av
aila
ble
for
2 ab
dom
inal
cas
es p
erda
y? 0)
No
1)
Yes
9)U
nkno
wn
21.
Is s
uctio
n av
aila
ble
and
wor
king
?0)
N
o1)
Y
es9)
Unk
now
n
22.
Is c
ircu
it an
esth
esia
ava
ilabl
e an
d w
orki
ng f
or 2
abd
omin
al c
ases
per
day?
0)
No
1)
Yes
9)U
nkno
wn
23.
Are
sup
plie
s fo
r en
dotr
ache
al in
tuba
tion
avai
labl
e an
d w
orki
ng?
0)
No
1)
Yes
9)U
nkno
wn
Per
sonn
el24
. Is
a m
edic
al o
ffic
er a
vaila
ble
24 h
ours
a d
ay?
0)
No
1)
Yes
9)U
nkno
wn
25.
Is th
e ho
spita
l ope
n fo
r su
rger
y 24
hou
rs a
day
?0)
N
o1)
Y
es2)
Unk
now
n
Hos
pita
l Cap
abili
ty S
urve
y To
ol /
Page
2 o
f 3

26.
Is a
trai
ned
surg
eon
avai
labl
e 24
hou
rs a
day
? (T
rain
ed f
or c
lose
dch
est t
raum
a, a
bdom
inal
exp
lora
tion
and
ampu
tatio
ns)
0)
No
1)
Yes
9)U
nkno
wn
27.
Is a
nest
hesi
a av
aila
ble
24 h
ours
a d
ay?
(Inc
ludi
ng E
T in
tuba
tion)
0)
No
1)
Yes
9)U
nkno
wn
28.
Are
nur
sing
sta
ff a
vaila
ble
24 h
ours
a d
ay f
or in
trav
enou
sin
fusi
ons?
0)
No
1)
Yes
9)U
nkno
wn
29.
Is th
ere
hosp
ital s
taff
to h
elp
feed
and
take
car
e of
pat
ient
s po
st-o
p?0)
N
o1)
Y
es9)
Unk
now
n
30.
Num
ber
of h
ospi
tal b
eds
31.
Num
ber
of in
-pat
ient
adm
issi
ons
in p
revi
ous
12 m
onth
s:
32.
Num
ber
of s
urgi
cal p
roce
dure
s in
pre
viou
s 12
mon
ths:
33.
Num
ber
of a
bdom
inal
ope
ratio
ns p
er y
ear:
34.
Num
ber
of c
esar
ean
sect
ions
per
yea
r:
35.
Num
ber
of la
ndm
ine
vict
ims
trea
ted
in p
revi
ous
12 m
onth
s:
36.
Num
ber
of a
mpu
tatio
ns p
erfo
rmed
on
land
min
e vi
ctim
s in
pre
viou
s12
mon
ths:
37.
Num
ber
of la
ndm
ine
vict
ims
who
die
d in
the
hosp
ital i
n pr
evio
us12
mon
ths:
38.
Num
ber
of o
pera
tions
for
land
min
e vi
ctim
s in
pre
viou
s 12
mon
ths:
Hos
pita
l Cap
abili
ty S
urve
y To
ol /
Page
3 o
f 3

Cap
abil
ity
and
Soci
al R
eint
egra
tion
Sur
vey
Too
l #2
Ort
hopa
edic
/Reh
ab C
ente
r C
apab
ility
Sur
vey
Inte
rvie
wer
Nam
e:__
____
____
____
____
____
___
Faci
lity
Nam
e:__
____
____
____
____
____
___
Add
ress
:__
____
____
____
____
____
___
Dat
e of
Int
ervi
ew:
____
____
____
____
____
____
_
1. T
ype
of C
ente
r1.
Hos
pita
l2.
Ort
hope
dic
Cen
ter
3.R
ehab
Cen
ter
4.O
ther
2. A
ffili
atio
n1.
Mili
tary
2.M
issi
onar
y3.
Inte
rnat
iona
l/Non
-gov
ernm
enta
l4.
Priv
ate
5.Pu
blic
6.O
ther
3.A
re th
ere
esta
blis
hed
refe
rral
pat
tern
s?0.
No
1.Y
es
4. W
hat i
s th
e pr
imar
y so
urce
of
ref
erra
ls?
1.H
ospi
tals
2.C
omm
unity
hea
lth w
orke
rs3.
Patie
nts
4.W
ord
of m
outh
9.U
nkno
wn
5. N
umbe
r of
pat
ient
s fi
tted
with
pro
sthe
sis
per
year
.
6. N
umbe
r of
pro
sthe
tists
em
ploy
ed.
7.
Num
ber
of p
rost
hetis
ts I
SPO
cer
tifie
d.
8.
Num
ber
of p
hysi
cal t
hera
pist
s em
ploy
ed.
9.
Do
you
have
eno
ugh
pers
onne
l?0.
No
1.Y
es
10.
Num
ber
of a
rtif
icia
l lim
bs m
ade
per
year
:
11.
Num
ber
of p
rim
ary
limbs
mad
e pe
r ye
ar:
12.
Num
ber
of r
epla
cem
ent l
imbs
per
yea
r:
13.
Num
ber
of w
heel
chai
rs m
ade
per
year
:
14.
Num
ber
of c
rutc
hes
mad
e pe
r ye
ar:
Typ
e of
pro
sthe
sis
mad
e: (
0-N
o, 1
-Yes
)
15.
Pol
ypro
pyle
ne
16.
Lea
ther
/woo
d
17.
Alu
min
um
18.
Poly
este
r/fi
berg
lass
19.
Do
you
have
a p
olyp
ropy
lene
pre
ss a
nd m
ould
?0.
No
1.Y
es
20.
Do
you
char
ge f
or a
pro
sthe
sis?
0.N
o1.
Yes
Ort
hopa
edic
/Reh
ab C
ente
r C
apab
ility
Sur
vey
Tool
/ Pa
ge 1
of
2

21.
Do
you
have
ade
quat
e su
pplie
s fo
r m
anuf
actu
ring
pro
sthe
ses?
0.N
o1.
Yes
22.
Is th
ere
stan
dard
ized
man
ufac
turi
ng o
f pr
osth
eses
?0.
No
1.Y
es
23.
Is th
ere
cent
raliz
ed m
anuf
actu
ring
of
pros
thes
es?
0.N
o1.
Yes
24.
Are
ther
e ot
her
orth
o/re
hab
cent
ers
near
by?
0.N
o1.
Yes
25.
Are
ther
e lo
cal t
rain
ing
prog
ram
s fo
r te
chni
cian
s?0.
No
1.Y
es
26.
Are
ther
e ou
trea
ch p
rogr
ams?
0.N
o1.
Yes
27.
Do
you
empl
oy d
isab
led
pers
ons?
0.N
o1.
Yes
28.
Are
ther
e ap
prop
riat
e fa
cilit
ies
and
surg
eons
ava
ilabl
e to
do
stum
pre
visi
ons?
0.N
o1.
Yes
29.
Can
you
est
imat
e th
e nu
mbe
r of
pat
ient
s w
ho n
eed
stum
p re
visi
ons?
1.1%
2.1-
5%3.
6-10
%4
11-2
5%5
Gre
ater
than
25%
Ort
hopa
edic
/Reh
ab C
ente
r C
apab
ility
Sur
vey
Tool
/ Pa
ge 2
of
2

CA
PA
BIL
ITY
AN
D S
OC
IAL
RE
INT
EG
RA
TIO
N S
UR
VE
Y T
OO
L #
3So
cial
Rei
nteg
rati
on a
nd R
ehab
ilita
tion
Sur
vey
Too
l
Inte
rvie
wer
Nam
e:__
____
____
____
____
____
____
____
____
____
Dat
e of
Int
ervi
ew:_
____
____
____
____
____
____
____
_
1.So
urce
of
Sam
ple:
1.H
ospi
tal
2.
Reh
ab C
ente
r3.
N
atio
nal D
ata
Bas
e4.
V
illag
e5.
Pr
ivat
e:__
____
____
____
____
____
____
____
____
_
2.H
ospi
tal o
r R
ehab
Cen
ter
Nam
e:__
____
____
____
____
____
____
____
__
3.A
ddre
ss:
____
____
____
____
____
____
____
____
____
____
____
____
__
4.N
ame
of V
ictim
:__
____
____
____
____
____
____
____
____
____
____
____
____
5.A
ddre
ss:
____
____
____
____
____
____
____
____
____
____
____
____
__
6.Se
x of
vic
tim:
0.M
ale
1.Fe
mal
e
7.
Cur
rent
Age
of
vict
im
8.Y
ear
of I
njur
y
9.A
mpu
tatio
n U
pper
Lim
b0.
Non
e1.
Uni
late
ral
2.B
ilate
ral
10.
Am
puta
tion
Bel
ow K
nee
0.N
one
1.U
nila
tera
l2.
Bila
tera
l
11.
Am
puta
tion
Abo
ve K
nee
0.N
one
1.U
nila
tera
l2.
B
ilate
ral
12.
Dea
fnes
s0.
Non
e1.
Uni
late
ral
2.B
ilate
ral
13.
Blin
dnes
s0.
Non
e1
Uni
late
ral
2.B
ilate
ral
14.
Hea
d/N
eck
Inju
ry0.
No
1.Y
es
15.
Abd
omen
/Tho
rax
Inju
ry0.
No
1.Y
es
16.
Lim
b In
jury
(B
urns
, Cut
s, e
tc.)
0.N
o1.
Yes
17.
Para
pleg
ia (
Los
s of
Mov
emen
t)0.
No
1.Y
es
Soci
al R
eint
egra
tion
and
Reh
abili
tatio
n To
ol /
Page
1 o
f 4

18.
Whe
re d
id y
ou r
ecei
ve m
edic
al c
are?
[R
ead
Cho
ices
]1.
Tra
ditio
nal h
eale
r2.
Hea
lth C
ente
r/Po
st3.
Publ
ic H
ospi
tal
4.M
issi
onar
y H
ospi
tal
5.In
tern
atio
nal/N
GO
Hos
pita
l6.
Priv
ate
Hos
pita
l7.
M
ilita
ry H
ospi
tal
9O
ther
19.
Aft
er le
avin
g th
e ho
spita
l, di
d yo
u re
ceiv
e re
hab/
phys
ical
ther
apy?
0.N
o1.
Yes
20.
Did
you
hav
e an
am
puta
tion?
0.N
o (G
o to
Que
stio
n 36
)1.
Yes
21.
How
man
y or
thop
aedi
c/re
hab
cent
ers
have
you
vis
ited?
0.N
one
1.O
ne2.
Tw
o3.
Gre
ater
than
two
22.
Wha
t mob
ility
equ
ipm
ent d
o yo
u us
e? [
Rea
d ch
oice
s]1.
Pros
thes
is2.
Whe
elch
air
3.C
rutc
hes
4.N
othi
ng (
Go
to q
uest
ion
36)
5.O
ther
____
____
____
____
____
____
____
_
23.
Whe
re d
id y
ou g
et th
e m
obili
ty e
quip
men
t?1.
Hos
pita
l2.
Ort
hopa
edic
Cen
ter
3.R
ehab
. Cen
ter
4.C
omm
unity
Out
reac
h5.
Oth
er
24.
Aft
er y
our
firs
t inj
ury,
how
man
y m
onth
s pa
ssed
bef
ore
you
got
mob
ility
equ
ipm
ent?
0.L
ess
than
6 m
onth
s1.
6 –
12 m
onth
s2.
Mor
e th
an 1
2 m
onth
s
25.
Did
you
pay
for
the
mob
ility
equ
ipm
ent?
0.N
o1.
Yes
2.R
efus
ed to
ans
wer
26.
How
man
y tim
es d
id y
ou n
eed
surg
ery
befo
re y
ou c
ould
use
apr
osth
esis
?:0.
Non
e1.
12.
2
3.
Mor
e th
an 2
27.
Do
you
thin
k yo
u cu
rren
tly n
eed
addi
tiona
l sur
gery
or
a st
ump
revi
sion
?0.
No
1.Y
es2.
I
do n
ot k
now
28.
How
man
y pr
osth
esis
hav
e yo
u ha
d?0.
Non
e [G
o to
Que
stio
n 36
]1.
12.
23.
34.
4 or
mor
e
29.
How
man
y m
onth
s do
es a
pro
sthe
sis
last
?0.
Les
s th
an 6
mon
ths
1.6
– 12
mon
ths
2.M
ore
than
12
mon
ths
Soci
al R
eint
egra
tion
and
Reh
abili
tatio
n To
ol /
Page
2 o
f 4

30.
Whe
n di
d yo
u la
st w
ear
a pr
osth
esis
?0.
N
ever
(G
o to
que
stio
n 33
)1.
Dur
ing
the
past
wee
k2.
Dur
ing
the
past
mon
th3.
Mor
e th
an a
mon
th a
go4.
Can
Not
Rem
embe
r9.
Ref
used
to A
nsw
er
31.
For
how
long
do
you
usua
lly w
ear
a pr
osth
esis
?0.
Nev
er (
Go
to q
uest
ion
33)
1.L
ess
than
1 h
our
daily
2.1
to 5
hou
rs d
aily
3.6
hour
s or
mor
e da
ily9.
Ref
used
to A
nsw
er
32.
Whe
re d
o yo
u us
e th
e pr
osth
esis
?1.
At h
ome
only
2.O
utsi
de o
nly
3.A
t hom
e an
d ou
tsid
e4.
Do
not u
se p
rost
hesi
s
33.
Why
do
you
not u
se a
pro
sthe
sis?
1.Pa
in2.
Bro
ken
3.Sa
ve f
or lo
nger
use
4.
Not
use
ful
5.
Dis
com
fort
6.O
ther
34.
Doe
s yo
ur p
rost
hesi
s ne
ed r
epai
r no
w?
0.N
o (G
o to
Que
stio
n 36
)1.
Yes
2.I
do n
ot k
now
35.
Pros
thes
is n
eeds
rep
airs
of:
1.So
cket
2.H
inge
3.Fe
et4.
Oth
er
EM
PL
OY
ME
NT
36.
Wer
e yo
u em
ploy
ed b
efor
e in
jury
?0.
No
(Go
to Q
uest
ion
39)
1.Y
es9.
Ref
used
37.
Did
you
wor
k:1.
Full
time
(>8
hour
s/da
y, 5
day
s/w
k)2.
Part
-tim
e (<
8 ho
urs/
day,
5 d
ays/
wk)
3.Sp
orad
ical
ly (
one
day
per
wee
k)4.
Occ
asio
nally
(fe
w d
ays/
mon
th)
9.R
efus
ed
38.
Whe
re d
id y
ou w
ork?
(Rea
d lis
t)1.
At h
ome
2.O
ffic
e/In
dust
ry/F
acto
ry3.
On
a fa
rm4.
In d
iffe
rent
pla
ces
(mob
ile)
5.O
ther
39.
Are
you
cur
rent
ly e
mpl
oyed
?0.
No
(G
o to
que
stio
n 42
)1.
Yes
9.R
efus
ed
40.
Do
you
wor
k? (
Rea
d lis
t)1.
Full
time
(>8
hour
s/da
y, 5
day
s/w
k)2.
Part
-tim
e (<
8 ho
urs/
day,
5 d
ays/
wk)
3.Sp
orad
ical
ly (
one
day
per
wee
k)4.
Occ
asio
nally
(fe
w d
ays/
mon
th)
9.R
efus
ed
41.
Whe
re d
o yo
u w
ork?
(R
ead
list)
1.A
t hom
e2.
Off
ice/
Indu
stry
/Fac
tory
3.O
n a
farm
4.In
dif
fere
nt p
lace
s (m
obile
)5.
Oth
er
Soci
al R
eint
egra
tion
and
Reh
abili
tatio
n To
ol /
Page
3 o
f 4

42.
Do
you
rece
ive
any
pens
ion/
soci
al s
ecur
ity f
rom
the
gove
rnm
ent
or f
orm
er e
mpl
oyer
?0.
No
1.Y
es9.
Ref
used
LE
GA
L I
SSU
ES
43.
Are
you
aw
are
of la
ws
for
min
e vi
ctim
s an
d th
e di
sabl
ed?
0.N
o [G
o to
Que
stio
n 45
]1.
Yes
9.R
efus
ed
44.
Wha
t do
thes
e la
ws
do?
1.Fi
nanc
ially
sup
port
min
e vi
ctim
s/ d
isab
led
to a
ttend
sch
ool
or
trai
ning
.2.
Ass
ist v
ictim
s/di
sabl
ed to
get
ben
efits
or
empl
oym
ent.
3.D
o no
thin
g di
ffer
ent f
or v
ictim
s.4.
Oth
er__
____
____
____
____
__5.
I do
not
kno
w9.
Ref
used
HE
AL
TH
AN
D H
EA
LT
H C
AR
E
45.
Are
ther
e ou
trea
ch p
rogr
ams
for
reha
b or
phy
sica
l the
rapy
in y
our
com
mun
ity?
0.N
o1.
Yes
2.I
do n
ot k
now
46.
How
far
is th
e ne
ares
t reh
ab/o
rtho
pedi
c ce
nter
?1.
L
ess
than
1 k
m2.
L
ess
than
5 k
m3.
L
ess
than
20
km4.
M
ore
than
20
km
47.
How
long
doe
s it
take
you
to r
each
the
near
est r
ehab
/ort
hope
dic
cent
er?
1.L
ess
than
1 h
our
2.L
ess
than
3 h
ours
3.L
ess
than
6 h
ours
4.L
ess
than
24
hour
s5.
G
reat
er th
an 2
4 ho
urs
SOC
IAL
SU
PP
OR
T A
ND
CO
MM
UN
ITY
PA
RT
ICIP
AT
ION
48.
H
ow m
any
peop
le li
ve w
ith y
ou?
1.1
pers
on2.
2-4
peop
le3.
5-10
peo
ple
4.M
ore
than
10
peop
le
49.
Doe
s an
yone
take
car
e of
you
?1.
No,
I ta
ke c
are
of m
ysel
f 2.
Yes
, my
Mot
her/
fath
er3.
Yes
, the
chi
ldre
n in
the
hous
ehol
d4.
Yes
, fri
ends
, nei
ghbo
rs, o
r re
lativ
es5.
Yes
, wif
e9.
Ref
used
50.
Do
you
feel
that
peo
ple
trea
t you
dif
fere
ntly
bec
ause
of
your
inju
ry?
0.N
o1.
Yes
2.I
do n
ot k
now
9.
R
efus
ed
51.
Do
you
feel
that
you
r in
jury
has
lim
ited
your
abi
lity
to g
ain
trai
ning
, atte
nd s
choo
l or
to w
ork?
0.N
o1.
Yes
9.R
efus
ed
Soci
al R
eint
egra
tion
and
Reh
abili
tatio
n To
ol /
Page
4 o
f 4