Measurement of neutrophil membrane CD64 and HLA-Dr in a patient with abdominal sepsis
4
CASE REPORT Measurement of neutrophil membrane CD64 and HLA-Dr in a patient with abdominal sepsis Wim van der Meer a, * , Colin Stephen Scott b , Carin Verlaat c , Jacqueline Klein Gunnewiek a , Adilia Warris d a Department of Clinical Chemistry, Radboud University Nijmegen Medical Center, P.O. Box 9101, 6500 HB Nijmegen, The Netherlands b Abbott GmbH and Co. KG, Diagnostics Division, Wiesbaden-Delkenheim, Germany c Intensive Care Department, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands d Department of Pediatrics and Medical Microbiology, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands Accepted 7 September 2005 Available online 25 October 2005 KEYWORDS Bacteraemia; Neutrophils; CD64; HLA-Dr Summary A patient with abdominal sepsis, had both intra and extracellular bacteria in a blood smear, and high levels of neutrophil membrane CD64 and HLA-Dr. Intracellular bacteria are only observed in the terminal phase of a sepsis. Our patient recovered, suggesting that a high expression of neutrophil CD64 is indicative for a good prognosis. Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. Case report and methods A 3-year-old boy, treated for acute lymphoblastic leukemia, developed a perforation of the distal esophagus during chemotherapy. He developed severe esophageal stenosis and a tracheo-esopha- geal fistula. Associated feeding difficulties and recurrent lower respiratory tract infections required surgical correction by esophagectomy and insertion of a gastric tube. Seven days later he developed severe pancolitis, which was treated with total parenteral feeding and metronidazole. On day 14, while in intensive care, he developed septic shock and respiratory insufficiency. Haema- tological investigations revealed anaemia (Hb 4.9 mmol/L) with normal platelet (347!10 9 /L) and white blood cell (9.9!10 9 /L) counts. The leukocyte differential comprised 5% metamyelo- cytes, 20% non-segmented (band) neutrophils, 58% segmented neutrophils, 13% lymphocytes and 4% monocytes. Intra-neutrophilic and extracellular bacteria as well as neutrophil toxic changes (Fig. 1) were also noted. Other laboratory findings included a C-reactive protein of 229 mg/L (normal !5 mg/L), fibrinogen 5910 mg/L (normal 1500– 3500 mg/L) and D-dimer 15 970 ng/mL (normal ! 500 ng/mL). A diagnosis of bacterial septicemia with secondary disseminated intravascular coagu- lation (DIC) was made and broad-spectrum Journal of Infection (2006) 53, e43–e46 www.elsevierhealth.com/journals/jinf 0163-4453/$30.00 Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.jinf.2005.09.003 * Corresponding author. Tel.: C31 24 3610611; fax: C31 24 3541743. E-mail address: [email protected] (W. van der Meer).
-
Upload
wim-van-der-meer -
Category
Documents
-
view
213 -
download
0
Transcript of Measurement of neutrophil membrane CD64 and HLA-Dr in a patient with abdominal sepsis

CASE REPORT
Measurement of neutrophil membrane CD64and HLA-Dr in a patient with abdominal sepsis
Wim van der Meera,*, Colin Stephen Scottb, Carin Verlaatc,Jacqueline Klein Gunnewieka, Adilia Warrisd
aDepartment of Clinical Chemistry, Radboud University Nijmegen Medical Center, P.O. Box 9101,6500 HB Nijmegen, The NetherlandsbAbbott GmbH and Co. KG, Diagnostics Division, Wiesbaden-Delkenheim, GermanycIntensive Care Department, Radboud University Nijmegen Medical Center, Nijmegen, The NetherlandsdDepartment of Pediatrics and Medical Microbiology, Radboud University Nijmegen Medical Center,Nijmegen, The Netherlands
Accepted 7 September 2005Available online 25 October 2005
01do
35
Me
KEYWORDSBacteraemia;Neutrophils;CD64;HLA-Dr
63-4453/$30.00 Q 2005 The Britishi:10.1016/j.jinf.2005.09.003
* Corresponding author. Tel.: C3141743.E-mail address: w.vandermeer@aer).
Summary A patient with abdominal sepsis, had both intra and extracellularbacteria in a blood smear, and high levels of neutrophil membrane CD64 and HLA-Dr.Intracellular bacteria are only observed in the terminal phase of a sepsis. Our patientrecovered, suggesting that a high expression of neutrophil CD64 is indicative for agood prognosis.Q 2005 The British Infection Society. Published by Elsevier Ltd. All rights reserved.
Case report and methods
A 3-year-old boy, treated for acute lymphoblasticleukemia, developed a perforation of the distalesophagus during chemotherapy. He developedsevere esophageal stenosis and a tracheo-esopha-geal fistula. Associated feeding difficulties andrecurrent lower respiratory tract infectionsrequired surgical correction by esophagectomyand insertion of a gastric tube. Seven days laterhe developed severe pancolitis, which was treatedwith total parenteral feeding and metronidazole.
Infection Society. Published by
24 3610611; fax: C31 24
kc.umcn.nl (W. van der
On day 14, while in intensive care, he developedseptic shock and respiratory insufficiency. Haema-tological investigations revealed anaemia (Hb4.9 mmol/L) with normal platelet (347!109/L)and white blood cell (9.9!109/L) counts. Theleukocyte differential comprised 5% metamyelo-cytes, 20% non-segmented (band) neutrophils, 58%segmented neutrophils, 13% lymphocytes and 4%monocytes. Intra-neutrophilic and extracellularbacteria as well as neutrophil toxic changes(Fig. 1) were also noted. Other laboratory findingsincluded a C-reactive protein of 229 mg/L (normal!5 mg/L), fibrinogen 5910 mg/L (normal 1500–3500 mg/L) and D-dimer 15 970 ng/mL (normal !500 ng/mL). A diagnosis of bacterial septicemiawith secondary disseminated intravascular coagu-lation (DIC) was made and broad-spectrum
Journal of Infection (2006) 53, e43–e46
www.elsevierhealth.com/journals/jinf
Elsevier Ltd. All rights reserved.

Figure 1 Peripheral blood smear of our patient stainedaccording May-Grunwald Giemsa showing both intra-neutrophilic and extracellular bacteria.
W. van der Meer et al.e44
antibiotics (meropenem and tobramycin) werestarted after collection of blood, urine and trachealsecretions for culture. He was intubated because ofrespiratory failure and the port-a-cath was removedas it was considered the likely source of thebacteraemia. A laparotomy was also performedbecause of suspected intestinal perforation andlarge amounts of ascites were removed. The smallintestines were vital with no abnormalities, and thecolon showed signs of pancolitis without a perfor-ation. The abdomen was left open to ensureefficient drainage. Blood cultures from the port-a-cath and from peripheral veins revealed Entero-bacter aerogenes and Enterococcus faecalis. Thefollowing day, renal failure and liver functionabnormalities developed together with persistentlactic acidosis, hyperglycemia and hypertension.High ventilation pressures were required to induceadequate oxygenation. Further haematologicalinvestigations showed a slight increase in thegranulocyte count (to 9.0!109/L) and moderatethrombocytopenia (97!109/L). Four days afterlaparotomy, his clinical condition improved andenteral feeding by jejunostomy was started. Renaland liver function improved, CRP (C-reactiveprotein) decreased to normal levels, plateletcount and DIC recovered, and the fever disap-peared. Extubation followed after 7 days ofartificially ventilation. He was treated for 2 weekswith meropenem and teicoplanin. Three weekslater, a Ramirez abdominoplasty was performedand a perforation of the colon found and attributedas the focus of his poly-microbial septicemia. Atpresent, the boy is doing relatively well.
In addition to standard laboratory investigations,an analysis of neutrophil membrane CD64 and HLA-Dr (Ia) expression was undertaken in a blood sampletaken at the initial sepsis work-up at the moment of
clinical presentation of bacteraemia. Measurementof neutrophil membrane CD64 (PMN-CD64) has beenthe subject of recent reports1,2 and is consideredpotentially useful for the diagnostic assessment ofsepsis for patients when conventional haematolo-gical parameters may be uninformative.3 The CD64antigen is a high-affinity receptor (FcgRI) expressedby monocytes but not by normal neutrophils.However, upregulated and detectable expressionof PMN-CD64 is mediated by lipopolysaccharides,g-interferon and granulocyte colony-forming factor(G-CSF),4 and is also characteristically seen inpatients with infection. In contrast, constitutivelyexpressed membrane Ia by immature granulocytesis effectively lost with neutrophil differentiationfrom the myelocyte.
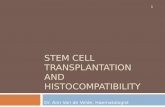
The immunofluorescent detection and quanti-tation of neutrophil CD64 and Ia was performedusing the Cell-Dyn CD4000 haematology analyser(Abbott Diagnostics, Santa Clara, CA, U.S.A.) aspreviously described.5 Patient expression of neu-trophil CD64 and Ia was compared to a series of 10healthy individuals (4 males, 6 females; mean age21, range 18–24 years, without febrile illness ormedication in the 2 weeks preceding the study).These studies revealed that granulocytes in ourpatient had a markedly increased medianexpression of CD64 of 750 AFU (Arbitrary Fluor-escent Units) compared to a normal median of 98AFU (SD 8.7) (Fig. 2(a)). Expression of membrane Ia(Fig. 2(b)) was also significantly increased (26.4AFU) compared to normal (median 10.7, SD 0.6)although this level of expression is relatively lowcompared to monocyte expression which is typicallyin excess of 260 AFU.5
Discussion
The expression of neutrophil CD64 was very high inour patient at the time of clinical presentation withbacteraemia. In a previous study of 117 patients,comprising patients with and without knowninfections, using the same assay procedure,5 onlysix were found with a neutrophil CD64 levelexceeding 700 AFU, with the mean CRP values forthese being 260 mg/L (range 176–360 mg/L), indi-cating that a high CRP value is associated with ahigh CD64 level. Determination of neutrophilmembrane Ia expression has not been system-atically looked at previously although one reportfound that increased Ia expression could be inducedin some patients treated with g-interferon.6 Wetook the opportunity to analyse this in our patientand found a modest but nevertheless significant

Figure 2 Quantitative staining intensities for neutrophil membrane CD64 and HLA-Dr (Ia) expression. Neutrophilswere gated according to optical scatter characteristics (0 vs. 78), and post-acquisition fluorescent channelcompensation was then applied. The histogram displays of FL1 (CD64) or FL2 (Ia) staining for our patient (shaded)are compared to those obtained from 10 normal control samples. Neutrophil CD64 staining profiles were normallydistributed while Ia expression was typically non-normal. Note the markedly increased CD64 and the weakly increased Iaexpression. The minor population of granulocytes in our patient (arrow) with higher Ia staining may correspond to thesmall proportion of immature granulocytes (metamyelocytes) noted in the morphological differential.
Neutrophil activation in bacteraemia e45
increase compared to normal. To establish whetherthis could be a consistent phenomenon, neutrophilIa expression was retrospectively determined forthe six previously investigated samples with highneutrophil CD64. The mean neutrophil Ia level forthese was 21.7 AFU (observed 18.4–25.4 AFU) andthus similar in magnitude to that seen with ourpatient. While these higher values could reflect the
presence of immature components, as our patientindeed had a leukocyte differential that included 5%metamyelocytes and 20% band cells, this is con-sidered unlikely as only three of these six patientsamples did show immature granulocytes.5 Disor-dered granulopoiesis, such as cellular asynchrony,might also be proposed as a reason for highneutrophil CD64 expression in patients with

W. van der Meer et al.e46
leukaemia although again unlikely as the primarymalignancy in our patient was lymphoid in natureand at the time of this episode of bacteraemia theleukaemia was in remission.
Excluding samples with post-venesection con-tamination, intracellular bacteria are only observedin blood smears in the terminal phase of sepsis.7–9
Earlier reports suggest that neutrophil CD64expression can be used for diagnostic assessmentof sepsis,2,10 and that a poor prognosis is associatedwith a lower neutrophil CD64 (and monocyte Ia)expression.11,12
With regards to monocyte Ia, significantreductions are characteristically seen in patientswith sepsis11,13,14 with reversion to normal levels ofexpression as sepsis-associated transient immuno-suppression is overcome.15 However, this measure-ment can be problematic in patients when severemonocytopenia occurs during the acute stages ofsepsis. Analysis of neutrophils in such circum-stances thus offers a number of advantages. Wetherefore, evaluated a new and simple approach formeasuring these cellular antigens with a routinehaematology analyser and confirmed markedlyelevated CD64 expression in our patient, andadditional evidence for mildly upregulated mem-brane Ia. While the diagnosis in our patient was notin doubt, these observations nevertheless suggestthat such measurements could be useful in inves-tigating patients where a suspicion of sepsis is moreequivocal.
Acknowledgements
The authors like to thank Ms Jacqueline Dinnissenfor interpretation of blood smears.
References
1. Davis BH, Bigelow NC, Curnutte JT, Ornvold K. NeutrophilCD64 expression. Potential diagnostic indicator of acuteinflammation and therapeutic monitor of interferon-gtherapy. Lab Hematol 1995;1:3–12.
2. Ng PC, Li G, Chui KM, Chu WCW, Li K, Wong RPO, et al.Neutrophil CD64 is a sensitive diagnostic marker for early-onset neonatal infection. Pediatr Res 2004;5:796–803.
3. Shapiro MF, Greenfield S. The complete blood count andleukocyte differential count. An approach to their rationalapplication. Ann Intern Med 1987;106:65–74.
4. Schiff DE, Rae J, Martin TR, Davis BH, Curnette JT. Increasedphagocyte Fc gammaR1 expression and improved Fc gamma-receptor-mediated phagocytosis after in vivo recombinanthuman interferon-gamma treatment of normal humansubjects. Blood 1997;90:3187–94.
5. Van der Meer W, van Dun L, Klein Gunnewiek J, Roemer B,Scott CS. Simultaneous determination of membrane CD64and HLA-DR expression by blood neutrophils and monocytesusing the monoclonal antibody fluorescence capability of aroutine haematology analyser, submitted.
6. Reinisch W, Lichtenberger C, Steger G, Tillinger W,Scheiner O, Gangl A, et al. Donor dependent, interferon-ginduced HLA-DR expression on human neutrophils in vivo.Clin Exp Immunol 2003;133:476–84.
7. Lehmann LS, Spivak JL. Rapid and definitive diagnosis ofinfectious diseases using peripheral blood smears.J Intensive Care Med 1992;1:36–47.
8. van der Meer W, Verwiel JMM, Gidding CEM, de Metz M, deKeijzer MH. Bacteria in blood smears: overwhelming sepsisor trivial contamination. Acta Haematol 2002;107:220–3.
9. Blot F, Nitenberg G, Chachaty E, Raynard B, Germann N,Antoun S, et al. Diagnosis of catheter-related bacteraemia: aprospective comparison of the time to positivity of hub-blood versus peripheral-blood cultures. Lancet 1999;354:1071–7.
10. Hodge G, Hodge S, Han P, Haslam R. Multiple leukocyteactivation markers to detect neonatal infection. Clin ExpImmunol 2004;135:125–9.
11. Kobold ACM, Tulliken JE, Zijlstra JG, Sluiter W, Hermans J,Kallenberg CGM, et al. Leukocyte activation in sepsis;correlations with disease state and mortality. IntensiveCare Med 2000;26:883–92.
12. Volk HD, Reinke P, Krausch D, Zuckermann H, Asadullah K,Muller JM, et al. Monocyte deactivation—rationale for a newtherapeutic strategy in sepsis. Intensive Care Med 1996;22:S474–S81.
13. Le Tulzo Y, Pangault C, Amiot L, Guilloux V, Arvieux C,Camus C, et al. Monocyte human leukocyte antigen-DRtranscriptional downregulation by cortisol during septicshock. Am J Respir Crit Care Med 2004;169:1144–52.
14. Sedlackova L, Prucha M, Dostal A. Immunological monitoringof sepsis using flow cytometry—quantitation of monocyteHLA-DR expression and granulocyte CD64 expression.Epidemiol Mikrobiol Imunol 2005;54:54–61.
15. Drossou-Agakidou V, Kanakoudi-Tsakalidou F, Sarafidis K,Tzimouli V, Parakou A, Kremenopoulos G, et al. In vivo effectof rhGM-CSF and rhG-CSF on monocyte HLA-DR expression ofseptic neonates. Cytokine 2002;18:260–8.