Measurement of Neck Circumference and Its Correlation with Body Composition in a Sample of Students...
8
E-Mail [email protected] Original Paper Horm Res Paediatr 2014;82:179–186 DOI: 10.1159/000364823 Measurement of Neck Circumference and Its Correlation with Body Composition in a Sample of Students in São Paulo, Brazil Claudia Andrade Coutinho a Carlos Alberto Longui a Osmar Monte a Wolney Conde b Cristiane Kochi a a Pediatric Endocrinology Unit, Irmandade da Santa Casa de Misericórdia de São Paulo, Santa Casa de São Paulo Faculty of Medical Sciences, and b Department of Nutrition, School of Public Health, University of São Paulo, São Paulo, Brazil sity in childhood. There was a positive correlation between NC and BMI, WC and %BF. This study was the first to provide NC percentiles for children in Brazil. © 2014 S. Karger AG, Basel Introduction Obesity is a serious public health concern that affects both adults and children. It is a syndrome with multifac- torial etiology including polygenic inheritance [1, 2], and is associated with hypertension, dyslipidemia, insulin re- sistance, type 2 diabetes mellitus, and other comorbidities [1]. An obese adolescent has an 80% chance of remaining obese in adulthood and experiencing more serious health problems [3]. The prevalence of overweight is increasing worldwide [4]. In Brazil, data from a survey conducted in 2008–2009 showed that there was a significant increase in the preva- lence of overweight and obesity over the previous 35 years, especially in children aged <10 years [5]. The most effective method to combat the obesity pan- demic is prevention among children and adolescents using Key Words Neck circumference · Children · Adolescents · Obesity · Nutritional assessment Abstract Purpose: The purpose of this study was to verify the correlation between neck circumference (NC) and body mass index (BMI) in children, and to determine NC percentiles for Brazilian chil- dren. Methods: The subjects of this cross-sectional study were students between the ages of 6 and 19 years from five schools in São Paulo, Brazil. Clinical and anthropometric data were col- lected from the students from April 2011 to June 2012. NC was measured at the level of the cricoid cartilage. We calculated Pearson correlation coefficients between NC and other indices of obesity with Sigma Stat 3.5. NC percentiles were produced using the LMS (lambda, mu, and sigma) method (STATA 12.0). Results: Among 2,794 students, 49.9% were male. NC was sig- nificantly correlated with age, BMI, waist circumference (WC), and body fat percentage (%BF). The NC of boys was greater than that of girls. The NC curves of smoothed 3rd, 10th, 25th, 50th, 75th, 90th, and 97th percentiles were constructed by age and sex. Conclusions: NC can be used in the assessment of obe- Received: February 24, 2014 Accepted: May 26, 2014 Published online: August 12, 2014 HORMONE RESEARCH IN PÆDIATRICS Claudia Andrade Coutinho Pediatric Endocrinology Unit, Pediatric Department of Santa Casa de São Paulo Hospital Rua Dr Cesario Motta jr. 112, 5th floor São Paulo, SP 01221-020 (Brazil) E-Mail cau_coutinho @ yahoo.com.br © 2014 S. Karger AG, Basel 1663–2818/14/0823–0179$39.50/0 www.karger.com/hrp Downloaded by: University Toronto Libr. 142.150.190.39 - 11/19/2014 12:55:16 AM
Transcript of Measurement of Neck Circumference and Its Correlation with Body Composition in a Sample of Students...

E-Mail [email protected]
Original Paper
Horm Res Paediatr 2014;82:179–186 DOI: 10.1159/000364823
Measurement of Neck Circumference and Its Correlation with Body Composition in a Sample of Students in São Paulo, Brazil
Claudia Andrade Coutinho a Carlos Alberto Longui a Osmar Monte a
Wolney Conde b Cristiane Kochi a
a Pediatric Endocrinology Unit, Irmandade da Santa Casa de Misericórdia de São Paulo, Santa Casa de São Paulo Faculty of Medical Sciences, and b Department of Nutrition, School of Public Health, University of São Paulo, São Paulo , Brazil
sity in childhood. There was a positive correlation between NC and BMI, WC and %BF. This study was the first to provide NC percentiles for children in Brazil. © 2014 S. Karger AG, Basel
Introduction
Obesity is a serious public health concern that affects both adults and children. It is a syndrome with multifac-torial etiology including polygenic inheritance [1, 2] , and is associated with hypertension, dyslipidemia, insulin re-sistance, type 2 diabetes mellitus, and other comorbidities [1] . An obese adolescent has an 80% chance of remaining obese in adulthood and experiencing more serious health problems [3] .
The prevalence of overweight is increasing worldwide [4] . In Brazil, data from a survey conducted in 2008–2009 showed that there was a significant increase in the preva-lence of overweight and obesity over the previous 35 years, especially in children aged <10 years [5] .
The most effective method to combat the obesity pan-demic is prevention among children and adolescents using
Key Words
Neck circumference · Children · Adolescents · Obesity · Nutritional assessment
Abstract
Purpose: The purpose of this study was to verify the correlation between neck circumference (NC) and body mass index (BMI) in children, and to determine NC percentiles for Brazilian chil-dren. Methods: The subjects of this cross-sectional study were students between the ages of 6 and 19 years from five schools in São Paulo, Brazil. Clinical and anthropometric data were col-lected from the students from April 2011 to June 2012. NC was measured at the level of the cricoid cartilage. We calculated Pearson correlation coefficients between NC and other indices of obesity with Sigma Stat 3.5. NC percentiles were produced using the LMS (lambda, mu, and sigma) method (STATA 12.0). Results: Among 2,794 students, 49.9% were male. NC was sig-nificantly correlated with age, BMI, waist circumference (WC), and body fat percentage (%BF). The NC of boys was greater than that of girls. The NC curves of smoothed 3rd, 10th, 25th, 50th, 75th, 90th, and 97th percentiles were constructed by age and sex. Conclusions: NC can be used in the assessment of obe-
Received: February 24, 2014 Accepted: May 26, 2014 Published online: August 12, 2014
HORMONERESEARCH IN PÆDIATRICS
Claudia Andrade Coutinho Pediatric Endocrinology Unit, Pediatric Department of Santa Casa de São Paulo Hospital Rua Dr Cesario Motta jr. 112, 5th floor São Paulo, SP 01221-020 (Brazil) E-Mail cau_coutinho @ yahoo.com.br
© 2014 S. Karger AG, Basel1663–2818/14/0823–0179$39.50/0
www.karger.com/hrp
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Coutinho /Longui /Monte /Conde /Kochi Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
180
body composition assessments appropriate to the period of growth. The assessment most widely used is the body mass index (BMI) [1] , which is not a sensitive indicator of either the amount or the distribution of body fat in this age group [6–8] . Body fat distribution is important due to the known association between some diseases and a greater accumulation of abdominal fat, regardless of age and the amount of total body fat [9, 10] . It was reported by Katzmar-zyk et al. [11] that the most common metabolic disorders associated with childhood obesity are hypertension, insu-lin resistance and impaired glucose tolerance, and an ath-erogenic blood lipid profile. Measurement of waist cir-cumference (WC) is a safe and practical method for assess-ing abdominal fat in adults and children to identify individuals at risk for complications [12–14] . Maffeis et al. [15] describes after analysis of 818 children aged 3–11 years that WC measured at the midpoint between last rib and iliac crest is correlated with systolic and diastolic blood pressure, ratio of total cholesterol/HDL and inverse cor-relation with HDL. To avoid the need for different refer-ence values according to age and sex, WC-to-height ratio (WHtR) may be used; the normal cutoff value is <0.5 re-gardless of age and gender [16] . Another advantage about WHtR is to be one of the anthropometric indices most promising for predicting metabolic risk in children, par-ticularly at group overweight [11] . Browning et al. [17] demonstrated that WHtR and WC are more reliable than BMI at predicting the incidence of cardiovascular disease, diabetes, and other obesity-related conditions.
Measurement of neck circumference (NC) has recently been proposed as a new method for the assessment of over-weight and obesity in children and adults [18–23] . Correla-tions have been found between NC and risk factors such as dyslipidemia, altered glucose metabolism, and sleep apnea syndrome, both in adults [18] and in children [23] . The cut-off points to indicate overweight in adults are 34 cm for women and 37 cm for men, with good sensitivity (98%) and specificity (89%) [18] . These cutoff points are less defined in the pediatric population, since few studies to date have examined the association of NC with overweight and obe-sity in children and adolescents. Therefore, this study aimed to investigate the correlation between NC and BMI in Bra-zilian children, and to determine the cutoff points of NC for both sexes and in different age groups.
Methods
A cross-sectional study was performed following approval by the Ethics Committee in Research of the Faculty of Medical Sci-ences of the Santa Casa São Paulo (FCM-SCSP). We evaluated chil-
dren and adolescents aged 6–19 years, who were enrolled in one of five schools from April 2011 to June 2012 in the city of São Paulo, Brazil. The five schools were geographically spread out across the city; four were public schools and one was a private school. A con-venience sample of students was drawn for access and school avail-ability. The sample size required a clinical difference of 5% with a significance level of 5 and 80% power; therefore, 1,300 students of each sex were chosen for evaluation. There were 2,794 students included in our study.
Students aged <6 years were not included in our study due to the belief that reliable measurements would be difficult to obtain as was demonstrated by LaBerge et al. [24] in children aged <5 years.
Children were excluded from the sample if they had a mass or cervical deformity that would interfere with the measurement of NC, a history of one or more chronic diseases, other conditions such as pregnancy, or and if they used medications that could af-fect growth.
Assessment of children was conducted at the school after pa-rental consent. The measurements were performed with the chil-dren wearing as little clothing as possible and no shoes.
The following data were collected by a single examiner using the same measurement methods and equipment: chronological age; weight as measured by an electronic scale with a capacity of 150 kg and 100 g precision; height as measured by a standard mobile stadi-ometer (Alturexata model and considering the nearest 0.1 cm) with the student standing erect, arms at sides, feet together, head facing in the Frankfurt plane parallel to the ground (head naturally straight, looking ahead); WC was measured to the nearest 0.1 cm at the end of normal expiration with the children standing using an inelastic and flexible tape at a point midway between the inferior margin of the lowest rib and the iliac crest [25] ; WHtR, and total body fat per-centage (%BF) measured to the nearest one tenth of a percent using a bioelectrical impedance analysis scale (Tanita model InnerScan 533 BC). Bioelectrical impedance analysis is only valid in children aged >7 years, so %BF was not determined for 6- and 7-year-old children. No preparatory instructions were provided to students with regard to hydration and physical activity. BMI was expressed in standard deviation scores and BMI SDS cutoff values used were according to WHO BMI references (WHO 2007), underweight is considered as BMI SDS <–2 SDS, normal weight between –2 and +1, overweight between +1 and +2, and obesity >+2 [26] . NC was measured using a flexible tape at the level of the cricoid cartilage with the student stand-ing and head held erect. We chose to measure NC at the level of the cricoid cartilage rather than the thyroid cartilage because the latter increases significantly in some, but not all, males during puberty. The cricoid cartilage is easy to palpate and does not exhibit variation dur-ing growth.
Statistical analysis was performed using Sigma Stat 3.5 to deter-mine the mean, standard deviation, median, and percentiles for age and anthropometric data collected (weight, height, BMI, WC, WHtR, %BF, and NC). The data were analyzed separately by sex and evaluated according to the following three age groups: <10 years, between 10 and 15 years, and >15 years. BMI SDS were used to classify subjects as normal weight (BMI SDS between –2 and +1) and overweight/obese (BMI SDS >+1), according to WHO. Pear-son correlation coefficients were calculated to explore the associa-tions between NC and other continuous variables such as age, weight, height, BMI, WC, and total %BF.
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Measurement of Neck Circumference in Brazilian Students
Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
181
Subsequently, for the construction of percentile curves with STATA 12.0 for Windows, we selected students with NC ±3 SD, stratified by sex and age, and calculated using the LMS method [27, 28] . The final percentile curves were generated by considering these three variables z-scores, corresponding to each percentile employing the formula: M (1 + LSz) 1/L . This method corrects for skewness in the data distributions: M stands for mean, S stands for a parameter, and L stands for the Box-Cox power scaling [27, 28] . That is required to transform the skewed data to normality, now employed by many modern references growth.
Results
Of 2,985 students initially identified for study inclusion, 48 were not present in school on the day of data collection and 143 were excluded for one or more of the exclusion reasons specified above. The final study sample of 2,794 stu-dents had 50.1% girls and 49.9% boys and the mean age was 11.1 ± 3.1 years. Based on the BMI SDS (WHO, 2007), 419 students in the sample (15%) were obese, 562 students (20%) were overweight, 1,776 (64%) were normal weight, and 37 (1%) were underweight. The highest percentage of obesity was among children aged <10 years. Table 1 shows the mean and standard deviation for height, total %BF, WC, NC and WHtR. The anthropometric indices for all age groups were significantly higher in the overweight/obese group than in the normal weight group.
Pearson correlation coefficients were calculated in groups, separated by age and sex, between NC and WC, BMI, and total %BF. NC was correlated with age (r = 0.71, p < 0.001), height (r = 0.81, p < 0.001), weight (r = 0.91, p < 0.001), BMI (r = 0.75, p < 0.001), total %BF (r = 0.22, p < 0.001), and WC (r = 0.81, p < 0.001). The same results were found when analysis was stratified by sex. The cor-relation with BMI and WC remained independent of age, as shown in table 2 . NC can be predicted from a linear combination of the age, BMI and height, without influ-ence of gender.
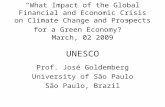
There were 2,783 students with NC of ±3 SD. The per-centile values, mean, and SD of NC for girls and boys in this group are shown in tables 3 and 4 , respectively. In figures 1 and 2 , the LMS curves for each gender are shown.
NC increased linearly with age for both sexes, an in-crease of 9.18 cm for boys and 5.4 cm for girls based on the values of the 50th percentile. The mean NC for each age was larger in boys than in girls. Figure 3 shows that this difference became more pronounced in subjects aged >11 years. In figure 3 the increase in the difference be-tween the NC values of boys and girls can be seen.
About the cutoff NC for each age and sex, we consid-ered ±2 SDS as normal. These values are available for cal-culation at www.clinicalcaselearning.com.
Table 1. Characteristics of students according to age, sex, and BMI
BMI SDS
<10 years 10 – 15 years >15 years
–2 to +1 >+1 –2 to +1 >+1 –2 to +1 >+1
BoysNumber 343 230 374 213 164 53Height 127.4 ± 8.0 131.9 ± 8.0* 151.2 ± 1.8 153.2 ± 10.9* 172.6 ± 6.6 174.9 ± 7.3*Height SDS –0.02 ± 0.9 0.64 ± 0.9* –0.02 ± 1.03 0.68 ± 1.0* –0.15 ± 0.9 0.15 ± 0.9BF% 16.6 ± 4.3 25.2 ± 8.3* 14.1 ± 4.7 26.4 ± 8.3* 11.5 ± 4.5 21.3 ± 7.5*WC 54.9 ± 3.5 66.8 ± 8.1* 62.2 ± 5.3 78.4 ± 10.3* 71.5 ± 4.5 87.6 ± 12.1*NC 26.2 ± 1.2 28.4 ± 1.6* 29.1 ± 2.3 31.7 ± 2.7* 34.0 ± 1.5 37.0 ± 1.8*WHtR 0.43 ± 0.02 0.50 ± 0.04* 0.41 ± 0.02 0.51 ± 0.05* 0.41 ± 0.02 0.50 ± 0.06*GirlsNumber 341 225 417 208 137 52Height 128.0 ± 8.4 133.6 ± 9.0* 150.5 ± 9.8 152.6 ± 7.6* 160.4 ± 6.1 161.8 ± 5.1Height SDS 0.07 ± 0.9 0.94 ± 1.0* –0.06 ± 1.0 0.41 ± 1.0* – 0.3 ± 0.9 – 0.1 ± 0.7BF% 18.8 ± 5.1 31.6 ± 6.5* 21.2 ± 4.9 33.0 ± 4.3* 23.2 ± 4.5 35.1 ± 4.7*WC 54.9 ± 3.9 69.1 ± 8.6* 62.0 ± 5.3 76.1 ± 8.2* 68.8 ± 5.2 83.7 ± 7.5*NC 25.6 ± 1.3 28.3 ± 2.0* 28.2 ± 1.6 30.7 ± 1.8* 30.3 ± 1.3 33.0 ± 2.0*WHtR 0.43 ± 0.02 0.51 ± 0.05* 0.41 ± 0.02 0.49 ± 0.05* 0.43 ± 0.03 0.51 ± 0.04* * p < 0.05 normal group (BMI SDS, –2 to +1 ) × overweight/obese (BMI SDS, >+2).
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Coutinho /Longui /Monte /Conde /Kochi Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
182
Table 2. Pearson correlation coefficients between NC and BMI, WC, total BF% by age and sex
Age Girls Boys
n BMI WC BF% p n BMI WC BF% p
6 104 0.66 0.76 – <0.001 111 0.63 0.72 – <0.0017 148 0.82 0.87 0.64 <0.001 152 0.77 0.79 0.44 <0.0018 138 0.84 0.86 0.77 <0.001 161 0.75 0.77 0.55 <0.0019 181 0.81 0.85 0.72 <0.001 154 0.80 0.81 0.53 <0.001
10 172 0.80 0.82 0.73 <0.001 179 0.83 0.86 0.61 <0.00111 154 0.86 0.85 0.83 <0.001 125 0.83 0.79 0.62 <0.00112 142 0.80 0.79 0.76 <0.001 108 0.81 0.79 0.63 <0.00113 89 0.86 0.82 0.77 <0.001 100 0.79 0.77 0.61 <0.00114 80 0.72 0.72 0.69 <0.001 87 0.76 0.73 0.67 <0.00115 190 0.74 0.73 0.67 <0.001 218 0.74 0.72 0.53 <0.001
Table 3. Values of L, M, S and NC percentiles for girls by age
Age n Mean SD L S M P3 P10 P25 P50 P75 P90 P97
6 104 25.8 1.73 –2.877 0.062 25.80 23.3 23.9 24.8 25.8 27.0 28.3 29.87 146 26.1 1.72 –2.531 0.069 26.21 23.4 24.2 25.1 26.2 27.5 28.9 30.78 138 26.9 2.08 –2.118 0.072 26.73 23.7 24.5 25.5 26.7 28.1 29.6 31.89 181 27.5 2.27 –1.684 0.072 27.34 24.1 25.0 26.0 27.3 28.7 30.2 31.9
10 172 27.8 2.03 –1.274 0.071 27.99 24.7 25.6 26.7 27.9 29.4 30.8 32.411 153 28.8 2.08 –0.931 0.068 28.66 25.3 26.3 27.3 28.6 30.0 31.4 32.812 142 29.3 1.86 –0.702 0.065 29.32 26.0 27.0 28.0 29.3 30.6 31.9 33.313 88 30.0 1.94 –0.630 0.061 29.93 26.7 27.7 28.7 29.9 31.2 32.4 33.714 79 30.1 1.44 –0.761 0.057 30.47 27.4 28.3 29.3 30.4 31.7 32.8 34.115 70 30.8 1.87 –1.140 0.054 30.9 28.0 28.8 29.8 30.9 32.1 33.2 34.516 65 31.0 1.81 –1.811 0.053 31.20 28.4 29.2 30.1 31.2 32.4 33.5 34.817 35 31.4 2.10 –2.819 0.054 31.34 28.6 29.4 30.2 31.3 32.5 33.8 35.318 19 30.8 1.71 –4.209 0.057 31.27 28.6 29.3 30.1 31.2 32.6 34.1 36.0
Table 4. Values of L, M, S and NC percentiles for boys by age
Age n Mean SD L S M P3 P10 P25 P50 P75 P90 P97
6 110 26.1 1.31 –1.870 0.048 26.44 24.3 24.9 25.6 26.4 27.3 28.2 29.27 152 26.7 1.71 –1.964 0.057 26.50 24.0 24.7 25.5 26.5 27.6 28.7 29.98 161 27.1 1.67 –1.988 0.064 26.89 24.1 24.8 25.7 26.8 28.1 29.4 30.99 154 28.1 1.80 –1.969 0.069 27.54 24.5 25.3 26.3 27.5 28.9 30.4 32.0
10 178 28.7 2.22 –1.934 0.073 28.41 25.1 26.0 27.1 28.4 29.3 31.5 33.311 124 29.0 1.93 –1.910 0.074 29.42 25.9 26.9 28.0 29.4 31.0 32.7 34.612 108 29.9 2.58 –1.924 0.075 30.52 26.9 27.9 29.0 30.5 32.2 33.9 35.913 100 31.1 2.74 –2.004 0.073 31.65 28.0 29.0 30.1 31.6 33.3 35.1 37.214 87 32.7 2.56 –2.176 0.071 32.75 29.0 30.1 31.2 32.7 34.4 36.2 38.415 66 34.2 2.22 –2.469 0.068 33.75 30.1 31.1 32.3 33.7 35.4 37.2 39.416 63 34.7 1.87 –2.907 0.064 34.61 31.1 32.1 33.2 34.6 36.2 38.0 40.217 64 35.1 2.03 –3.520 0.060 35.25 32.0 32.9 33.9 35.2 36.8 38.5 40.718 24 34.9 2.29 –4.334 0.055 35.62 32.6 33.4 34.4 35.6 37.1 38.7 40.9
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Measurement of Neck Circumference in Brazilian Students
Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
183
Discussion
Obesity is currently one of the most serious health problems today, with a progressive increase in childhood, especially in younger age groups. Because of the comor-bid conditions associated with obesity, early diagnosis is important for more effective intervention. New, more re-liable and practical assessment methods are needed due to the disadvantages of methods in current use. There is a discussion about using NC as parameter for evaluation overweight in childhood. In the study of Nafiu et al. [29] it was possible to demonstrate a correlation between NC
and BMI and high blood pressure in a sample of 1,058 children aged 6–18 years, who had an incidence of over-weight and obesity was 19.0 and 18.7%, respectively. Katz et al. [30] also described NC as a risk factor for obstructive sleep apnea for boys >12 years.
Our study also demonstrated that NC could be used as an indicator of overweight and obesity in children and adolescents, showing strong correlation with BMI and WC.
In our study of students in São Paulo, prevalence of overweight and obesity was 20 and 15%, respectively. These percentages are considerably higher than those re-
p97
p90
p75
p50p25p10p3
38
36
34
32
30
28
26
24
22N
eck
circ
umfe
renc
e (c
m)
6.0
6.6
7.0
7.6
8.0
8.6
9.0
9.6
10.0
10.6
11.0
11.6
12.0
12.6
13.0
13.6
14.0
14.6
15.0
15.6
16.0
16.6
17.0
17.6
18.0
Age (years)
p97
p90
p75p50p25p10p3
42
37
32
27
22
Nec
k ci
rcum
fere
nce
(cm
)
6.0
6.6
7.0
7.6
8.0
8.6
9.0
9.6
10.0
10.6
11.0
11.6
12.0
12.6
13.0
13.6
14.0
14.6
15.0
15.6
16.0
16.6
17.0
17.6
18.0
Age (years)
Fig. 1. NC percentiles for girls.
Fig. 2. NC percentiles for boys.
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Coutinho /Longui /Monte /Conde /Kochi Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
184
ported in population studies performed in our country in 2010 by the Survey of Family Budgets [5] . The significant increase in overweight and obesity found in children aged <10 years has been observed by other researchers as well [4, 25, 31, 32] .
With regard to measurement of NC, LaBerge et al. [24] observed a good intra- and inter-observer reliability in children aged >6 years, finding it necessary to perform only one measurement. In their research, children were divided into three groups according to age (2–5, 6–10, and 11–16 years), and each child was measured twice by each of the three examiners. Our data showed that the overweight/obese group had higher values of NC, WC, and WHtR. These results are similar to those reported by Hatipoglu et al. [33] for Turkish children and adolescents aged between 6 and 18 years. Our study also found simi-lar results to others with regard to differences in NC based on sex, that is, boys have larger NC than girls [34, 35] . In our study, the difference became more pro-nounced at age >11 years, ranging from a 0.63-cm differ-ence between boys and girls at the age of 6 years, and a 4.3-cm difference at the age of 18 years. Mazicioglu et al. [36] evaluated 4,581 children and adolescents (6–18 years) and found that NC was larger in boys than in girls across all age groups. The difference became more pro-nounced at age >12 years, ranging from a 0.58-cm differ-ence between boys and girls at the age of 6 years, and a
5-cm difference at the age of 18 years. This observed dif-ference between males and females keeps in adulthood, as described by Stabe et al. [37] in a study with Brazilian adults that described a cutoff higher for men. We believe that the increase in NC in boys is because of the greater increase in muscular mass in this area, comparing to girls.
Similar to other previous publications, NC in our study was correlated with other measures of body com-position regardless of age [18–23, 33–36, 38–40] .
We describe NC SDS, considering ±2 SDS as normal, and these cutoff are similar to those published in adult cohorts. Our study can also be related to that described by Ben-Noun et al. [18] which assessed 979 patients in Israel to determine cutoff points for classification of over-weight/obesity in adults. In that study, men with NC <37 cm and women with NC <34 cm were classified as normal weight (i.e. not overweight or obese). Stabe et al. [37] , af-ter analyzing 1,053 adults in Brazil, described as cutoff to identify metabolic syndrome 40 cm for men and 36 cm for women. These cutoff points are similar to those found in our study as +2 SDS for the group >15 years old, 34.8 cm for girls and 38.9 cm for boys.
Further research is needed regarding the correlation between NC with laboratory indices such as dyslipidemia, fasting glucose, and insulin levels, as well as other clinical parameters such as blood pressure, to better define cutoff
37
35
33
31
29
27
25N
eck
circ
umfe
renc
e (c
m)
6.0
6.6
7.0
7.6
8.0
8.6
9.0
9.6
10.0
10.6
11.0
11.6
12.0
12.6
13.0
13.6
14.0
14.6
15.0
15.6
16.0
16.6
17.0
17.6
18.0
Age (years)
Boys
Girls
Fig. 3. Comparison of the 50th percentile of NC between boys and girls aged 6–18 years.
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Measurement of Neck Circumference in Brazilian Students
Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
185
points associated with these comorbidities in our popula-tion.
In conclusion, measurement of NC is shown to be a practical, accessible method for assessing overweight and obesity in children and adolescents. It strongly correlates with other anthropometric measures such as BMI, WC, and total %BF. This study was the first to provide NC per-centiles for children in Brazil. The study validated the use of NC in the assessment of childhood obesity, a vital step in primary prevention of obesity-related comorbid condi-tions.
Acknowledgements
The authors are grateful to students and staff of the participat-ing schools: Escola Municipal de Ensino Fundamental Antônio Carlos de Andrada e Silva, Escola Estadual Professor Roldão Lopes de Barros, Escola Estadual Arthur Guimarães, Colégio Claretiano, and Escola Estadual Professora Marina Cintra.
Disclosure Statement
The authors have no conflicts of interest to disclose.
References
1 Daniels SR, Jacobson MS, McCrindle BW, Eckel RH, Sanner BM: American Heart As-sociation Childhood Obesity Research Sum-mit: executive summary. Circulation 2009; 119: 2114–2123.
2 Snyder EE, Walts B, Pérusse L, Chagnon YC, Weisnagel SJ, Rankinen T, Bouchard C: The human obesity gene map: the 2003 update. Obes Res 2004; 12: 369–439.
3 Travers SH, Jeffers BW, Eckel RH: Insulin re-sistance during puberty and future fat accu-mulation. J Clin Endocrinol Metab 2002; 87: 3814–3818.
4 De Onis M, Blössner M, Borghi E: Global prevalence and trends of overweight and obe-sity among preschool children. Am J Clin Nutr 2010; 92: 1257–1264.
5 Pesquisa de Orçamentos Familiares: Antrop-ometria e estado nutricional de crianças, ado-lescentes e adultos no Brasil. Available from http://www.ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009_encaa/ (accessed September 15, 2010).
6 Daniels SR: The use of BMI in the clinical set-ting. Pediatrics 2009; 124:S35–S41.
7 Reilly JJ, Dorosty AR, Emmett P: Identifica-tion of the obese child: adequacy of the body mass index for clinical practice and epidemi-ology. Int J Obes Relat Metab Disord 2000; 24: 1623–1627.
8 Prentice AM, Jebb SA: Beyond body mass in-dex. Obes Rev 2001; 2: 141–147.
9 Kissebah AH, Krakower GR: Regional adi-posity and morbidity. Physiol Ver 1994; 74: 761–811.
10 Bouchard C, Johnson FE: Fat distribution during growth and late healthy outcomes. Clin Nutr Insight 1989; 15: 6.
11 Katzmarzyk PT, Shen W, Baxter-Jones A, Bell JD, Butte NF, Demerath EW, Gilsanz V, Go-ran MI, Hirschler V, Hu HH, Maffeis C, Ma-lina RM, Muller MJ, Pietrobelli A, Wells JCK: Adiposity in children and adolescents: corre-lates and clinical consequences of fat stored in specific body depots. Pediatr Obes 2012; 7:e42–e61.
12 Taylor RW, Jones IE, Williams SM, Goulding A: Evaluation of waist circumference, waist-to-hip ratio and the conicity index as screen-ing tools for high trunk fat mass, as measured by dual energy X-ray absorptiometry, in chil-dren aged 3–19 years. Am J Clin Nutr 2000; 72: 490–495.
13 Botton J, Heude B, Kettaneh A, Borys JM, Lommez A, Bresson JL, Ducimetiere P, Charles M: Cardiovascular risk factor levels and their relationship with overweight and fat distribution in children. Metabolism 2007; 56: 614–622.
14 Hirschler V, Aranda C, Calcagno MDL, Mac-calini G, Jadzinsky M: Can waist circumfer-ence identify children with the metabolic syn-drome? Arch Pediatr Adolesc Med 2005; 159: 740.
15 Maffeis C, Pietrobelli A, Grezzani A, Provera S, Tato L: Waist circumference and Cardio-vascular risk factors in prepubertal children. Obes Res 2001; 9: 179–187.
16 Ashwell M, Hsieh SD: Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr 2005; 56: 303–307.
17 Browning LM, Hsieh SD, Ashwell M: A sys-tematic review of waist-to-height ratio as a screening tool for the prediction of cardiovas-cular disease and diabetes: 0: 5 could be a suit-able global boundary value. Nutr Res Rev 2010; 23: 247–269.
18 Ben-Noun L, Sohar E, Laor A: Neck circum-ference as a simple screening measure for identifying overweight and obese patients. Obes Res 2001; 9: 470–477.
19 Laakso M, Matilainen V, Keinänen-Kiukaan-niemi S: Association of neck circumference with insulin resistance-related factors. Int J Obes Relat Metab Disord 2002; 26: 873–875.
20 Ben-Noun L, Laor A: Relationship of neck cir-cumference to cardiovascular risk factors. Obes Res 2003; 11: 226–231.
21 Ben-Noun L, Laor A: Relationship between changes in neck circumference and cardio-vascular risk factors. Exp Clin Cardiol 2006; 11: 14–20.
22 Hingorjo MR, Qureshi MA, Mehdi A: Neck circumference as a useful marker of obesity: a comparison with body mass index and waist circumference. J Pak Med Assoc 2012; 62: 36.
23 Kurtoglu S, Hatipoglu N, Mazicioglu MM, Kondolot M: Neck circumference as a novel parameter to determine metabolic risk factors in obese children. Eur J Clin Invest 2012; 42: 623–630.
24 LaBerge RC, Vaccani JP, Gow RM, Gaboury I, Hoey L, Katz SL: Inter- and intra-rater reli-ability of neck circumference measurements in children. Pediatr Pulmonol 2009; 44: 64–69.
25 World Health Organization (WHO): Obesity: Preventing and Managing the Global Epi-demic. Report of a WHO Consultation. Ge-neva, WHO, 2000.
26 World Health Organization: Growth reference data for 5–19 years, WHO reference 2007. Available at http://www.who.int/growthref/en/ (accessed June 20, 2008).
27 Cole TJ: Fitting smoothed centile curves to reference data. J R Stat Soc 1988; 151: 385–418.
28 Cole TJ, Green PJ: Smoothing reference cen-tile curves: the LMS method and penalized likelihood. Stat Med 1992; 11: 1305–1319.
29 Nafiu OO, Zepeda A, Curcio C, Prasad Y: As-sociation of neck circumference and obesity status with elevated blood pressure in chil-dren. J Hum Hypertens 2014; 28: 263–268.
30 Katz S, Murto K, Barrowman N, Clarke J, Hoey L, Momoli F, Vaccani JP: Neck circum-ference percentile: a screening tool for pediat-ric obstructive sleep apnea. Pediatr Pulmonol 2014, Epub ahead of print.
31 Kimm SY, Obarzanek E: Childhood obesity: a new pandemic of the new millennium. Pedi-atrics 2002; 110: 1003–1007.
32 Lobstein T, Baur L, Uauy R: IASO interna-tional obesity task force. Obesity in children and young people: a crisis in public health. Obes Rev 2004; 5: 4–85.
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM

Coutinho /Longui /Monte /Conde /Kochi Horm Res Paediatr 2014;82:179–186DOI: 10.1159/000364823
186
33 Hatipoglu N, Mazicioglu MM, Kurtoglu S, Kendirci M: Neck circumference: an addition-al tool of screening overweight and obesity in childhood. Eur J Pediatr 2010; 169: 733–739.
34 Nafiu OO, Burke C, Lee J, Voepel-Lewis T, Malviya S, Tremper KK: Neck circumference as a screening measure for identifying chil-dren with high body mass index. Pediatrics 2010; 126:e306–e310.
35 Lou DH, Yin FZ, Wang R, Ma CM, Liu XL, Lu Q: Neck circumference is an accurate and simple index for evaluating overweight and obesity in Han children. Ann Hum Biol 2012; 39: 161–165.
36 Mazicioglu MM, Kurtoglu S, Ozturk A, Hati-poglu N, Cicek B, Ustunbas HB: Percentiles and mean values for neck circumference in Turkish children aged 6–18 years. Acted Pae-diatr 2010; 99: 1847–1853.
37 Stabe C, Vasques ACJ, Lima MMO, Tambas-cia MA, Pareja JC, Yamanaka A, Geloneze B: Neck circumference as a simple tool for iden-tifying the metabolic syndrome and insulin resistance: results from the Brazilian Meta-bolic Syndrome Study. Clin Endocrinol 2013; 78: 874–881.
38 Androutsos O, Grammatikaki E, Moschonis G, Roma-Giannikou E, Chrousos GP, Manios Y, Kanaka-Gantenbein C: Neck cir-cumference: a useful screening tool of car-diovascular risk in children. Pediatr Obes 2012; 7: 187–195.
39 Gonçalves VSS, Faria E: Perímetro do pescoço como preditor de excesso de gordura corporal no início da adolescência. Rev Nutr 2014;27:161–171.
40 Atwa HA, Fiala LEM, Handoka NM: Neck circumference as an additional tool for detect-ing children with high body mass index. J Am Sci 2012; 8: 442–446.
Dow
nloa
ded
by:
Uni
vers
ity T
oron
to L
ibr.
142.
150.
190.
39 -
11/
19/2
014
12:5
5:16
AM