Measurement of endogenous and exogenous alpha-granular platelet proteins in patients with immune and...
9
Measurement of endogenous and exogenous alpha-granular platelet proteins in patients with immune and nonimmune thrombocytopenia MARY H UGHES ,C ATHERINE P. M. HAY WA R D,P ETER H ORSEWOOD,² T HEODORE E. WARKENTIN AND J OHN G. K ELTON*² Departments of Pathology and *Medicine, Faculty of Health Sciences, McMaster University Division, Hamilton Health Sciences Corporation, and ²Canadian Red Cross Society, Hamilton, Ontario, Canada Received 22 January 1999; accepted for publication 9 June 1999 Summary. Idiopathic thrombocytopenic purpura (ITP) is caused by antiplatelet antibodies and is characterized by increased platelet destruction and elevated levels of IgG (platelet-associated IgG, PAIgG). Nonimmune thrombocyto- penic patients also have elevated levels of PAIgG. In this study we investigated two possible biological explanations for the increased levels of PAIgG in these patients. The first hypothesis suggests that a thrombocytopenic stress causes increased thrombocytopoiesis with increased numbers and content of the platelet alpha granules. The second hypothesis is that for uncertain reasons (immunological or cytokine) there is increased absorption of plasma proteins by either megakaryocytes or by the platelets themselves. To address this issue, we compared the level of megakaryocyte synthesized alpha granular proteins [platelet factor 4 (PF4) and beta-thromboglobulin (b-TG)] to plasma-absorbed alpha granular proteins (albumin, IgG and fibrinogen) in patients with immune (n 39) and nonimmune (n 60) thrombo- cytopenias. Plasma-absorbed alpha-granular proteins were elevated in both immune and nonimmune thrombocyto- penia with no increase in megakaryocyte synthesized alpha- granular proteins. These plasma-derived protein elevations were not attributable to elevated mean platelet volumes or elevated plasma concentrations of the respective protein. We hypothesize that the increased IgG in these platelets is not the result of production of larger platelets, but reflects a selective increase in the endocytosis of plasma-absorbed alpha-granular proteins at the megakaryocyte and/or platelet level. Keywords: platelet-associated IgG, idiopathic thrombocyto- penic purpura, endocytosis, plasma proteins, megakaryocyte. Idiopathic thrombocytopenic purpura (ITP) is a disorder characterized by increased platelet destruction through removal of antibody-coated platelets by phagocytic cells of the reticuloendothelial (RE) system (McMillan, 1981). This destructive process is mediated by antiplatelet autoantibodies (McMillan, 1981), directed against platelet surface glyco- proteins, with glycoproteins IIb/IIIa and Ib/IX being the most common targets (van Leeuwen et al, 1982; Woods et al, 1984a, b). It is not known what triggers the production of antiplatelet autoantibodies, nor is it possible to predict which patients are at an increased risk for developing life- threatening haemorrhages (Lightsey et al, 1976). For many years investigators have measured platelet- associated immunoglobulins (PAIgG) in patients with ITP. These studies led to two generally accepted observations. Firstly, platelets from patients with ITP have elevated levels of PAIgG (Kelton & Steeves, 1983; George, 1990; George et al, 1985; George & Saucerman, 1988). Secondly, elevated PAIgG is not specific for ITP and is observed in most thrombocytopenic disorders, including nonimmune disor- ders, such as aplastic anaemia and leukaemia (George & Saucerman, 1988; Kelton et al, 1989; Heaton et al, 1988; George, 1989; Mueller-Eckhardt et al, 1980). In this study we questioned the biological explanation for the increased levels of PAIgG in both immune and nonimmune thrombocytopenic disorders. The current explanation for increased PAIgG levels in patients with ITP is that elevated PAIgG levels are a reflection of the increased numbers of larger younger platelets circulating in these patients (George, 1990). Since larger platelets are thought to be more dense and since alpha-granule content is the primary determinant of platelet density, it would be expected British Journal of Haematology , 1999, 106, 762–770 762 q 1999 Blackwell Science Ltd Correspondence: Dr John G. Kelton, HSC 3W10, McMaster University Medical Center, 1200 Main Street West, Hamilton, Ontario, Canada L8N 3Z5.
-
Upload
mary-hughes -
Category
Documents
-
view
212 -
download
0
Transcript of Measurement of endogenous and exogenous alpha-granular platelet proteins in patients with immune and...

Measurement of endogenous and exogenous alpha-granular
platelet proteins in patients with immune and nonimmune
thrombocytopenia
MA RY HU G HE S, CATHERINE P. M. HAYWARD, PET ER HORSE WOOD,² THEODORE E. WARKENTIN AND JOHN G. KE LTON*²
Departments of Pathology and *Medicine, Faculty of Health Sciences, McMaster University Division,
Hamilton Health Sciences Corporation, and ²Canadian Red Cross Society, Hamilton, Ontario, Canada
Received 22 January 1999; accepted for publication 9 June 1999
Summary. Idiopathic thrombocytopenic purpura (ITP) iscaused by antiplatelet antibodies and is characterized byincreased platelet destruction and elevated levels of IgG(platelet-associated IgG, PAIgG). Nonimmune thrombocyto-penic patients also have elevated levels of PAIgG. In thisstudy we investigated two possible biological explanations forthe increased levels of PAIgG in these patients. The ®rsthypothesis suggests that a thrombocytopenic stress causesincreased thrombocytopoiesis with increased numbers andcontent of the platelet alpha granules. The second hypothesisis that for uncertain reasons (immunological or cytokine)there is increased absorption of plasma proteins by eithermegakaryocytes or by the platelets themselves. To addressthis issue, we compared the level of megakaryocytesynthesized alpha granular proteins [platelet factor 4 (PF4)and beta-thromboglobulin (b-TG)] to plasma-absorbed alpha
granular proteins (albumin, IgG and ®brinogen) in patientswith immune (n�39) and nonimmune (n�60) thrombo-cytopenias. Plasma-absorbed alpha-granular proteins wereelevated in both immune and nonimmune thrombocyto-penia with no increase in megakaryocyte synthesized alpha-granular proteins. These plasma-derived protein elevationswere not attributable to elevated mean platelet volumes orelevated plasma concentrations of the respective protein. Wehypothesize that the increased IgG in these platelets is notthe result of production of larger platelets, but re¯ects aselective increase in the endocytosis of plasma-absorbedalpha-granular proteins at the megakaryocyte and/orplatelet level.
Keywords: platelet-associated IgG, idiopathic thrombocyto-penic purpura, endocytosis, plasma proteins, megakaryocyte.
Idiopathic thrombocytopenic purpura (ITP) is a disordercharacterized by increased platelet destruction throughremoval of antibody-coated platelets by phagocytic cells ofthe reticuloendothelial (RE) system (McMillan, 1981). Thisdestructive process is mediated by antiplatelet autoantibodies(McMillan, 1981), directed against platelet surface glyco-proteins, with glycoproteins IIb/IIIa and Ib/IX being the mostcommon targets (van Leeuwen et al, 1982; Woods et al,1984a, b). It is not known what triggers the production ofantiplatelet autoantibodies, nor is it possible to predict whichpatients are at an increased risk for developing life-threatening haemorrhages (Lightsey et al, 1976).
For many years investigators have measured platelet-associated immunoglobulins (PAIgG) in patients with ITP.
These studies led to two generally accepted observations.Firstly, platelets from patients with ITP have elevated levels ofPAIgG (Kelton & Steeves, 1983; George, 1990; George et al,1985; George & Saucerman, 1988). Secondly, elevatedPAIgG is not speci®c for ITP and is observed in mostthrombocytopenic disorders, including nonimmune disor-ders, such as aplastic anaemia and leukaemia (George &Saucerman, 1988; Kelton et al, 1989; Heaton et al, 1988;George, 1989; Mueller-Eckhardt et al, 1980).
In this study we questioned the biological explanation forthe increased levels of PAIgG in both immune andnonimmune thrombocytopenic disorders. The currentexplanation for increased PAIgG levels in patients with ITPis that elevated PAIgG levels are a re¯ection of the increasednumbers of larger younger platelets circulating in thesepatients (George, 1990). Since larger platelets are thought tobe more dense and since alpha-granule content is theprimary determinant of platelet density, it would be expected
British Journal of Haematology, 1999, 106, 762±770
762 q 1999 Blackwell Science Ltd
Correspondence: Dr John G. Kelton, HSC 3W10, McMasterUniversity Medical Center, 1200 Main Street West, Hamilton,
Ontario, Canada L8N 3Z5.

763Measurement of Alpha-granular Platelet Protein in ITP
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
that platelets in ITP patients would contain more alpha-granule proteins such as IgG and albumin (George, 1990).
In this study we investigated this hypothesis directly bymeasuring several different alpha-granule proteins inpatients with ITP and nonimmune thrombocytopenias.The strategy we employed was to compare the amount ofmegakaryocyte-synthesized alpha-granule proteins (endo-genous platelet proteins; b-thromboglobulin and plateletfactor 4) to the amount of plasma-derived alpha-granuleproteins (exogenous platelet proteins; IgG, albumin and®brinogen). We postulated that by measuring both endo-genous and exogenous platelet proteins, and relating theseresults to platelet size (mean platelet volume), we coulddifferentiate whether the increased PAIgG in thrombocyto-penic patients was due to the production of larger platelets,a general overall increase in alpha-granular content, or aselective alteration in the pool of plasma-derived alpha-granular proteins.
MATERIALS AND METHODS
Patients and controls. The study was approved by aUniversity and Hospital Ethics Review Committee andsamples were collected with informed consent. We studied39 patients with ITP; 29 had active ITP and 10 patients werein remission. Patients were considered to have ITP if they metthe following criteria: thrombocytopenia (<150 ´ 109/l),a nonpalpable spleen, normal or increased numbers of
megakaryocytes in the bone marrow (if performed), and theabsence of secondary causes of thrombocytopenia (McMil-lan, 1981; Kelton & Gibbons, 1982). ITP patients weresubdivided into two groups, those with active disease(thrombocytopenia present) and those in remission. Patientswith a past history of ITP and normal platelet counts(>150 ´ 109/l), who were not on any immunosuppressivetherapy at the time of investigation, were classi®ed as havingITP in remission. The control patients (n�60) with otherhaematological disorders included patients with multiplemyeloma, aplastic anaemia, thrombotic thrombocytopenicpurpura, systemic lupus erythematosus, iron de®ciencyanaemia, myeloproliferative disorder, hypersplenism, spleno-megaly, leukaemia, lymphoma, alcoholic liver cirrhosis andincidental thrombocytopenia of pregnancy. These patientswere subdivided according to their platelet counts (throm-bocytopenic, n�26; normal platelet count, n�34). Thenormal controls (n�13) were a group of nonthrombocyto-penic, aspirin-free, healthy male and female laboratorypersonnel.
Platelet collection and preparation. Whole blood wascollected into acid citrate dextrose (ACD, pH 4´5, 6:1,vol:vol). Platelets were isolated by differential centrifugationand washed ®ve times in phosphate-buffered saline (PBS, pH6´5) with 10 mM ethylenediaminetetra-acetic acid disodium(EDTA). Washed platelets were resuspended to 1 ´ 108
platelets/ml in buffer (25 mM Tris, 100 mM NaCl, 0´02%bovine serum albumin (BSA), containing the protease
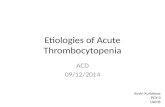
Fig 1. Measurement of PAIgG in immune and nonimmune patients and healthy controls. Each symbol represents a single patient or healthy
control. The mean (B) and standard deviation for each patient or healthy control group is indicated.

inhibitors leupeptin (50 mg/ml), 10 mM EDTA and phenyl-methylsulphonyl ¯uoride (0´25 mM). Platelets were lysed bythe addition of 0´5% Triton X-100 (Pierce, Rockford, Ill.).Following lysis (30 min at 228C), platelet lysates werecentrifuged (14 000 rpm for 20 min), and the supernatantswere used for all protein measurements.
Measurement of platelet-associated IgG (PAIgG). Platelet-associated IgG in lysed platelets was measured using animmunoradiometric assay. Anti-human IgG monoclonalantibody, CAG-2 (Warkentin et al, 1994), raised in ourlaboratory, was coated onto Immulon II (Dynatech, Chan-tilly, Va.) microtitre strip wells in 0´2 mol/l carbonate buffer(pH 9´5) overnight at 48C. This antibody recognized allsubclasses of IgG (Warkentin et al, 1994). The wells werewashed once with wash buffer (0´9% NaCl, 0´05% Tween-20) and blocked with 2% BSA/PBS for 2 h at roomtemperature. Platelet lysates were diluted (6´25±1´25 ´ 106 platelets/ml) in 2% BSA/PBS and duplicate100 ml samples were added to the wells. Plates wereincubated for 3 h at room temperature and then washed®ve times with wash buffer.
Monoclonal anti-human IgG, HB43 (American TypeCulture Collection, Rockville, Md.), was labelled with37 MBq Na125I per ml using the chloramine-T method andhad an average speci®c activity of 6´99 GBq/mg protein. The
125I-HB43 was diluted (1/1000) in 2% BSA/PBS and 100 mlwas added to each well. Following an incubation of 2 h atroom temperature, the wells were washed ®ve times withwash buffer and each well was transferred into 75 ´ 12 mmplastic tubes (Sarstedt, Newton, N.C.). An LKB 1275minigamma counter (Fisher Scienti®c, Nepean, Ont.) wasused to determine counts per minute per tube. Puri®edhuman IgG (Sigma-Aldrich, Oakville, Ont.) was diluted in2% BSA/PBS with 0´5% Triton X-100, and used to generatestandard curves. The results were expressed as mg IgG/109
platelets, which is equivalent to fg IgG/platelet.Measurement of platelet-associated albumin. Platelet-
associated albumin was measured using a similar method.ELISA plate wells were coated with monoclonal anti-humanalbumin (Clone HSA1/25.1.3; Cedarlane Laboratories,Hornby, Ont.) in 0´2 mol/l carbonate buffer (pH 9´5)overnight at 48C. Wells were washed once with washbuffer and blocked with 2% BSA/PBS for 2 h at roomtemperature. Platelet lysates were diluted (1´5±6´25 ´ 106
platelets/ml) in 2% BSA/PBS and duplicate 100 ml sampleswere added to plate wells. Plates were incubated for 3 h atroom temperature and then washed ®ve times with washbuffer. A second monoclonal anti-human albumin (Clone943127; Cortex Laboratories, San Leandro, Calif.) labelledwith 37 MBq Na125I per ml (average speci®c activity
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
764 Mary Hughes et al
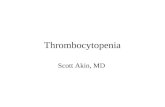
Fig 2. Measurement of platelet albumin in immune and nonimmune patients and healthy controls. Each symbol represents a single patient or
healthy control. The mean (B) and standard deviation for each patient or healthy control group is indicated.

765Measurement of Alpha-granular Platelet Protein in ITP
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
18´69 GBq/mg protein) was diluted (1/1000) in 2% BSA/PBS and 100 ml was added to each well. Following anincubation of 2 h at room temperature, plate wells werewashed ®ve times with wash buffer. Each well was placedinto 12 ´ 75 mm plastic tubes and counted in a gammacounter. The two monoclonal anti-human albumin anti-bodies used in this assay speci®cally recognized humanalbumin and did not recognize bovine serum albumin.Puri®ed human albumin (Sigma-Aldrich, Oakville, Ont.)diluted in 2% BSA/PBS, with 0´5% Triton X-100, was usedto generate standard curves. The results were expressed asmg/109 platelets.
Measurement of beta-thromboglobulin and platelet factor 4.Beta-thromboglobulin (b-TG) and platelet factor 4 (PF4)were measured on washed lysed platelets using commercialEIA kits obtained from Asserachrom (Murex Diagnostics,Guelph, Ont.), according to the manufacturer's speci®ca-tions. b-TG and PF4 concentrations were expressed as mg/109 platelets.
Measurement of platelet-associated ®brinogen. Platelet-asso-ciated ®brinogen was measured using an enzyme-linkedimmunosorbent assay described previously (Hayward et al,1996). Puri®ed human ®brinogen (Alexis Biochemicals, SanDiego, Calif.), diluted in 2% BSA/PBS (with 0´5% Triton X-100) was used as the standard. The platelet ®brinogenresults were expressed as mg/109 platelets.
Mean platelet volume. Blood samples were collected intoEDTA anticoagulated tubes (Becton Dickinson, Mississauga,Ont.) and analysed on a Coulter S-Plus Counter (CoulterElectronics, Hialeah, Fla.), for determination of mean plateletvolumes (¯).
Serum IgG and serum albumin measurements. Serum IgGand albumin was measured using a Kallestad QM 300Protein Analysis System (Sano® Diagnostics Pasteur,Chaska, Min.).
Plasma ®brinogen measurements. Plasma ®brinogen levelswere measured using the Clauss ®brinogen assay and anMLA Electra 1600C Automatic Coagulation Analyzer(Medical Laboratory Automation, Montreal, Quebec).
Statistical analysis. Statistical analyses were performedusing the Corel Quattro Pro. (Version 7) data analysisprogram. Inferences about the corresponding measurementsof endogenous and exogenous alpha granular plateletproteins, total platelet protein and mean platelet volume,for each patient group, was made by calculating the meanand standard deviation for each data set. The quantitativeupper limit of normal for each platelet protein measured wasbased on the data set of the healthy control group (mean 62standard deviations). The Pearson product moment coef®-cient of correlation, r, was calculated to determine whetherdata sets were correlated. In addition, the calculated meanfor each data set was compared by using an analysis of
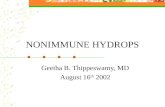
Fig 3. Measurement of platelet ®brinogen in immune and nonimmune patients and healthy controls. Each symbol represents a single patient or
healthy control. The mean (B) and standard deviation for each patient or healthy control group is indicated.

variance (ANOVA, one-way) to determine whether differencesamong the population means were signi®cant (P<0´05).
RESULTS
Plasma-derived platelet proteins were measured in healthycontrols, patients with active ITP (thrombocytopenic), andpatients with ITP in remission (normal platelet counts)(Figs 1±3). These assays were also performed in healthycontrols and patients with nonimmune thrombocytopeniaand nonimmune patients with normal platelet counts(Figs 1±3). The mean values and standard deviations forPAIgG, platelet albumin and platelet ®brinogen for thecontrol group and each patient group are summarized inTable I.
The mean values of the plasma-derived alpha-granularproteins, IgG, albumin and ®brinogen, were signi®cantlyhigher in platelets from thrombocytopenic patients, com-pared to the nonthrombocytopenic controls (P <0´05).These elevations were consistent and independent of themechanism responsible for the thrombocytopenia. With theexception of ®brinogen, these proteins were not signi®cantlyelevated in platelets from patients with normal plateletcounts (P >0´05). The one exception was observed innonthrombocytopenic patients with nonimmune haemato-logical disorders. The mean platelet ®brinogen for thispatient group was signi®cantly elevated, compared tonormal controls (P�0´0004). Patients with elevatedPAIgG, platelet-associated albumin, and/or platelet ®brino-gen, had normal levels of serum IgG, serum albumin, andplasma ®brinogen.
Megakaryocyte synthesized platelet proteins were mea-sured in healthy controls, patients with active ITP (throm-bocytopenic), and patients with ITP in remission (normalplatelet counts) (Fig 4). These assays were also performed inhealthy controls and patients with nonimmune thrombo-cytopenia and nonimmune patients with normal plateletcounts (Fig 4). The mean values and standard deviations forthe alpha-granular proteins, PF4 and b-TG, are summarizedin Table I. Whereas thrombocytopenic patients consistentlydemonstrated elevated plasma-derived platelet proteins, aparallel increase in megakaryocyte synthesized proteins wasnot observed in any patient. The mean values for theseproteins (b-TG and PF4) were not signi®cantly elevated inthrombocytopenic patients or any of the patient groups,compared to healthy controls (P >0´05).
To determine whether elevated plasma-derived plateletproteins re¯ected production of larger platelets in thrombo-cytopenic patients, we studied a parameter of platelet size;the mean platelet volume (MPV). The MPV for boththrombocytopenic and nonthrombocytopenic patientgroups were within the established normal range (Fig 5).Furthermore, there was no correlation between MPVelevation and the levels of PAIgG in the thrombocytopenicpatients with ITP (r�ÿ0´23), or in the thrombocytopenicpatients with nonimmune haematological disorders(r�ÿ0´26). Similarly, there was no correlation betweenMPV and elevated platelet albumin in these two patientgroups (r<0´15).
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
766 Mary Hughes et al
Ta
ble
I.M
easu
rem
ent
of
end
ogen
ou
sa
nd
exog
eno
us
alp
ha
-gra
nu
lar
pla
tele
tp
rote
ins,
an
dp
late
let
size
inth
rom
bo
cyto
pen
icp
ati
ents
an
dp
ati
ents
wit
hn
orm
al
pla
tele
tco
un
ts.
Pla
tele
tsi
zeP
lasm
a-d
eriv
edp
late
let
pro
tein
sM
ega
ka
ryo
cyte
syn
thes
ized
pro
tein
s
Pla
tele
tM
PV
IgG
Alb
um
inF
ibri
no
gen
bT
GP
F4
cou
nt
(¯)
(mg
/10
9p
late
lets
)(m
g/1
09
pla
tele
ts)
(mg
/10
9p
late
lets
)(m
g/1
09
pla
tele
ts)
(mg
/10
9p
late
lets
)
Act
ive
ITP
62
´86
32
´61
0´1
61
´37
66
´1a
21
´96
18
´3b
54
76
64
4c
67
´76
32
´43
´16
1´3
(th
rom
bo
cyto
pen
ic)
(n�
29
)
ITP
rem
issi
on
22
76
64
´78
´96
0´7
3´1
61
´21
0´5
63
´41
55
61
43
55
´66
26
´22
´66
1´1
(no
rma
lp
late
let
cou
nt)
(n�
10
)
No
nim
mu
ne
ha
ema
tolo
gic
al
dis
ord
ers
58
´26
38
´68
´36
1´5
10
´36
13
´8d
36
´26
46
´8e
42
06
49
4f
51
´46
28
´62
´56
1´3
(th
rom
bo
cyto
pen
ic)
(n�
26
)
No
nim
mu
ne
ha
ema
tolo
gic
al
dis
ord
ers
32
46
21
´78
´66
1´8
3´4
62
´49
´16
9´3
33
66
38
7g
68
´96
63
´13
´46
2´2
(no
rma
lp
late
let
cou
nt)
(n�
34
)
Hea
lth
yco
ntr
ols
33
06
25
´29
´76
0´7
2´4
60
´96
´46
1´6
13
06
52
35
´66
23
´22
´36
1´2
(no
rma
lp
late
let
cou
nt)
(n�
13
)
De®
ned
up
per
lim
its
of
no
rma
l1
1´1
4´3
9´6
23
4´8
82
4´7
(ba
sed
on
hea
lth
yco
ntr
ols
)(m
ean�
2S
D)
Da
taa
rere
po
rted
as
mea
ns
6st
an
da
rdd
evia
tio
ns:
n�
nu
mb
ero
fsa
mp
les.
Ita
lici
zed
va
lues
are
tho
sew
hic
hw
ere
sig
ni®
can
tly
hig
her
tha
tth
ed
e®n
edu
pp
erli
mit
of
no
rma
lfo
rth
at
pro
tein
.IT
P:
idio
pa
thic
thro
mb
ocy
top
enic
pu
rpu
ra;b
TG
:b
-th
rom
bog
lob
uli
n;
PF
4:
pla
tele
tfa
cto
r4
;M
PV
:m
ean
pla
tele
tvo
lum
e.a
P�
0´0
00
07
,b
P�
0´0
01
7,
cP�
0´0
02
9,
dP�
0´0
02
6,
eP�
0´0
03
8,
fP�
0´0
02
6,
gP�
0´0
00
4.

767Measurement of Alpha-granular Platelet Protein in ITP
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
Fig
4.
Mea
sure
men
to
fp
late
let
fact
or
4(P
F4
)a
nd
bet
a-t
hro
mb
oglo
bu
lin
(BT
G)
inim
mu
ne
an
dn
on
imm
un
ep
ati
ents
an
dh
ealt
hy
con
tro
ls.
Ea
chsy
mb
ol
rep
rese
nts
asi
ng
lep
ati
ent
or
hea
lth
yco
ntr
ol.
Th
em
ean
(B)
an
dst
an
da
rdd
evia
tio
nfo
rea
chp
ati
ent
or
hea
lth
yco
ntr
ol
gro
up
isin
dic
ate
d.

DISCUSSION
Platelet populations from ITP patients have been shown tohave a greater size heterogeneity as re¯ected by an increasedpercentage of megathrombocytes (Karpatkin, 1985; Khanet al, 1975; Zucker-Franklin & Karpatkin, 1977; Garg et al,1972). It has been hypothesized that this altered largerplatelet population may be responsible for the elevated PAIgGlevels observed in ITP patients (Shulman et al, 1982; Pfuelleret al, 1981, 1986). Indeed, Corash et al (1977) demonstratedthat large-heavier platelets contained more alpha granules.Based on these observations, the purpose of our study was todetermine if platelets from ITP patients, who presumablyhave `larger and heavier' platelets containing more alphagranules, do in fact have an increased alpha-granule proteincontent.
For this report we measured two types of alpha-granuleprotein based on their origin of synthesis. These proteinsincluded several megakaryocyte synthesized (endogenousalpha-granular platelet proteins; bTG and PF4) as well asseveral plasma-derived alpha-granular proteins (exogenousalpha-granular platelet proteins; IgG, albumin and ®brino-gen) in platelets from patients with a variety of thrombocyto-penic and nonthromboctyopenic disorders. We postulatedthat if the explanation for elevated PAIgG was megakaryo-cytic stimulated production of larger heavier platelets thenthere would be an increase in mean platelet volume, with anincrease in all components of the alpha granule. In thismodel, levels of plasma-derived alpha-granular proteins maybe normal or increased. However, if the stimulus occurred atthe circulating platelet level, then one would expect plateletswith normal levels of endogenous alpha-granular proteins,but elevated levels of plasma-derived alpha-granularproteins.
Previously, we have postulated that elevated levels of PAIgGmight suggest that immune mechanisms could contribute tothe thrombocytopenia in patients with historically classi®ed`nonimmune' thrombocytopenic disorders (Sinha & Kelton,
1990). Indeed, Hymes et al (1979) reported that some patientswith thrombocytopenia in disorders other than ITP havecirculating anti-platelet antibody. In our study we attempted toexclude `nonimmune' thrombocytopenic patients who testedpositive for the most commonly detected anti-platelet anti-bodies in ITP (anti-glycoprotein IIb/IIIa and anti-glycoproteinIb/IX), by screening platelet lysate samples from each patientin an antigen capture assay according to Warner et al (1999).Based on the results of this assay (not shown), all patientscategorized with ITP demonstrated detectable anti-glycopro-tein IIb/IIIa or anti-glycoprotein Ib/IX antibody, whereas allpatients categorized with nonimmune thrombocytopeniafailed to demonstrate anti-platelet antibodies in this assay.Although this screening approach does not rule out thepossibility that patients categorized with `nonimmune' throm-bocytopenia may still have an anti-platelet immune compo-nent with speci®cities other than glycoprotein IIb/IIIa orglycoprotein Ib/IX, it is clear that the `immune mechanisms'responsible for the thrombocytopenia in ITP versus `non-immune' thrombocytopenic disorders, are distinct.
Our de®ned quantitative upper limit of normal for eachplatelet protein measured was based on values obtained froma group of healthy controls (n�13). The results we obtainedwere similar to those obtained by other investigators usingdifferent techniques. Together these studies indicate that thenormal amounts of protein from solubilized platelets as<5 mg PAIgG/109 platelets (Kelton & Steeves, 1983; Keltonet al, 1989), <15 mg albumin/109 platelets (Kelton & Steeves,1983), 80±140 mg ®brinogen/109 platelets (Colman et al,1994; McKeown et al, 1993), 30±80 mg b-TG/109 platelets(Colman et al, 1994; McKeown et al, 1993; Bellon et al,1993; Kerry & Curtis, 1985) and <5±14 mg PF4/109
platelets (Colman et al, 1994; McKeown et al, 1993; Bellonet al, 1993; Kerry & Curtis, 1985).
When platelets from groups of immune and nonimmunethrombocytopenic patients were studied we observed aconsistent increase in plasma-derived platelet proteins,with no parallel increase in megakaryocyte synthesized
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
768 Mary Hughes et al
Fig 5. Measurement of mean platelet volume (MPV) in immune and nonimmune patients and healthy controls. Each symbol represents a singlepatient or healthy control. The mean (B) and standard deviation for each patient or healthy control group is indicated.

769Measurement of Alpha-granular Platelet Protein in ITP
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
proteins (Figs 1±4). In this study not all individual patientswith immune and nonimmune thrombocytopenia demon-strated increased PAIgG levels. These ®ndings suggest thatthere may be two subsets of thrombocytopenic patients:those with increased PAIgG levels and those with noincrease. In our study we focused on whether there was adifference in the overall average level of measured alpha-granule proteins between different patient groups, ratherthan individual patients. Although it remains debatable as towhich assay measures the true amount of IgG on washedplatelets, it is clear that the overall mean PAIgG value fromthe group of patients with ITP and the group of patients withnonimmune thrombocytopenia both have a signi®cantincrease in PAIgG compared to normal controls whenassayed by the same technique. We suggest that thesedifferences are not a re¯ection of the platelet preparation orassay techniques, but rather a re¯ection of the patientpopulation as a whole.
The results of our study failed to demonstrate an increasein the level of megakaryocyte synthesized proteins in eitherimmune or nonimmune thrombocytopenic patients. These®ndings support earlier studies where no difference wasfound in platelet density between normal controls, ITPpatients and patients with nonimmune thrombocytopenicdisorders (Illes et al, 1987). Furthermore, studies by Pfuelleret al (1986), in contrast to Corash et al (1977), found thatPAIgG of both controls and patients with immune andnonimmune thrombocytopenia is preferentially located inthe lightest platelets rather than in heavier platelets. Wesuggest that elevated levels of PAIgG observed amongthrombocytopenic patients are not due to the presence of agreater percentage of megathrombocytes found among thesepatients, but is a re¯ection of an altered process of IgGaccumulation by platelets and/or megakaryocytes.
It is well accepted that the mean platelet volume inthrombocytopenic patients is generally elevated in compar-ison to patients with normal platelet counts (Garg et al,1971; Branehog et al, 1975). However, in our study we failedto observe an increase in overall mean platelet volumebetween patient groups in comparison to normal controls.Although some individual thrombocytopenic patients hadincreased mean platelet volumes, because of the greatvariation within the patient groups, the differences did notreach statistical signi®cance for the group as a whole. In ourstudy we focused on whether there was a difference in theoverall mean platelet volume between different patientgroups, rather than individual patients. Our results agreewith earlier studies by Kelton et al (1979) and Holme et al(1988) who also found no relationship between increasedlevels of platelet associated IgG and any particular size classof platelets.
The observation that IgG is elevated in parallel with otherplasma proteins (albumin and ®brinogen) in thrombocyto-penic patients provides further information about PAIgG.Firstly, not only are measurements of PAIgG of no diagnosticusefulness, but measurements of platelet albumin, or anyother plasma-derived alpha-granule protein, will yield thesame information as IgG measurements. Secondly, anisolated increase in the exogenous alpha-granule protein
content in platelets from thrombocytopenic patients suggeststhat the mechanism of internalization of IgG and otherplasma proteins is altered in platelets and/or megakaryo-cytes in these patients. Thirdly, the observation that elevatedPAIgG measurements are observed in patients with diverseclinical aetiologies (both immune and nonimmune), sug-gests that increased PAIgG measurements may be unrelatedto platelet clearance.
There are few precedents for cells acquiring proteinscontained within regulated secretory granules by endocy-tosis. In platelets, speci®c receptors such as GP IIb/IIIa andFcgRII may be responsible for the internalization of®brinogen and IgG in a receptor-speci®c manner (George1990; George et al, 1985; George & Saucerman, 1988;Harrison et al, 1989). However, a speci®c receptor has notbeen identi®ed for albumin. Presently, there are no reportedstudies on the quantitation of platelet receptors in ITPpatients versus normal controls. However, the observationthat increased levels of PAIgG are not con®ned to anyparticular size class of platelets (Kelton et al, 1979; Holmeet al, 1988) suggests that there may not be a quantitativedifference in the number of IgG platelet receptors in ITPpatients, but rather a difference in the presence of astimulating factor for IgG internalization.
Based on the results of our study, we hypothesize thatstimuli associated with thrombocytopenia may be respon-sible for the altered uptake of plasma-derived alpha-granularproteins in thrombocytopenic patients. Our data suggest thatthis stimulus may be independent of the mechanism ofthrombocytopenia. We hypothesize that stimuli in thrombo-cytopenic patients leads to increased endocytosis by mega-karyocytes and/or platelets, resulting in platelets withelevated levels of plasma proteins.
ACKNOWLEDGMENTS
This work was supported by a grant from the MedicalResearch Council of Canada and the Heart and StrokeFoundation of Ontario to J. G. Kelton and a Bayer/CanadianRed Cross Society Research Studentship to M. Hughes. C. P.M. Hayward is a Research Scholar of the Heart and StrokeFoundation of Ontario.
REFERENCES
Bellon, J.L., Castellanos, C., Acevedo, L. & Amiral, J. (1993)
Measurement of beta-thromboglobulin and platelet factor 4 tofollow up patients with arti®cial heart valves. Seminars in
Thrombosis and Hemostasis, 19, (Suppl. 1), 178±182.
Branehog, I., Kutti, J., Ridell, B., Swolin, B. & Weinfeld, A. (1975)
The relation of thrombokinetics to bone marrow megakaryocytesin idiopathic thrombocytopenic purpura (ITP). Blood, 45, 551±
562.
Colman, R.W., Hirsh, J., Marder, V.J. & Salzman, E.W. (1994)
Hemostasis and Thrombosis: Basic Principles and Clinical Practice, 3rdedn. Lippincott, Philadelphia.
Corash, L., Tan, H. & Gralnick, H.R. (1977) Heterogeneity of human
whole blood platelet subpopulations. I. Relationship betweenbuoyant density, cell volume, and ultrastructure. Blood, 49, 71±87.
Garg, S.K., Amorosi, E.L. & Karpatkin, S. (1971) Use of the

megathrombocyte as an index of megakaryocyte number. New
England Journal of Medicine, 284, 11±17.
Garg, S.K., Lachner, H. & Karpatkin, S. (1972) The increased
percentage of megathrombocytes in various clinical disorders.Annals of Internal Medicine, 77, 361±369.
George, J.N. (1989) The origin and signi®cance of platelet IgG.
Platelet Immunobiology: Molecular and Clinical Aspects (ed. by T. J.
Kunicki and J. N. George), pp. 305±336. Lippincott, Philadelphia.George, J.N. (1990) Platelet immunoglobulin G: its signi®cance for
the evaluation of thrombocytopenia and for understanding the
origin of a-granule proteins. Blood, 76, 859±870.George, J.N., Saucerman, S., Levine, S.P., Knieriem, L.K. &
Bainton, D.F. (1985) Immunoglobulin G is a platelet alpha
granule-secreted protein. Journal of Clinical Investigation, 76,
2020±2025.Harrison, P., Wilbourn, B., Debili, N., Vainchenker, W., Breton-
Gorius, J., Lawrie, A.S., Masse, J-M., Savidge, G.F. & Cramer, E.M.
(1989) Uptake of plasma ®brinogen into the alpha granules of
human megakaryocytes and platelets. Journal of Clinical Investiga-tion, 84, 1320±1324.
Hayward, C.P., Rivard, G.E., Kane, W.H., Drouin, J., Zheng, S.,
Moore, J.C. & Kelton, J.G. (1996) An autosomal dominantqualitative platelet disorder associated with multimerin de®ciency,
abnormalities in platelet factor V, thrombospondin, von Wille-
brand factor, and ®brinogen and an epinephrine aggregation
defect. Blood, 87, 4967±4978.Heaton, W.A., Holme, S. & Hartman, P. (1988) Elevated levels of
PAIgG in thrombocytopenic patients are not related to the
presence of microthrombocytes or megathrombocytes. American
Journal of Clinical Pathology, 89, 88±94.Holme, S., Heaton, A., Kunchuba, A. & Hartman, P. (1988)
Increased levels of platelet associated IgG in patients with
thrombocytopenia are not con®ned to any particular size class
of platelets. British Journal of Haematology, 68, 431±436.Hymes, K., Shulman, S. & Karpatkin, S. (1979) A solid-phase
radioimmunoassay for bound anti-platelet antibody. Journal of
Laboratory and Clinical Medicine, 94, 639±648.Illes, I., Pfueller, S.L., Hussein, S., Chesterman, C.N. & Martin, J.F.
(1987) Platelets in idiopathic thrombocytopenic purpura are
increased in size but are of normal density. British Journal of
Haematology, 67, 173±176.Karpatkin, S. (1985) Autoimmune thrombocytopenic purpura.
Seminars in Hematology, 22, 260±288.
Kelton, J.G. & Gibbons, S. (1982) Autoimmune platelet destruction:
idiopathic thrombocytopenic purpura. Seminars in Thrombosis andHaemostasis, 8, 83±104.
Kelton, J.G., Murphy, W.G., Lucarelli, A., Garvey-Williams, J.,
Santos, A., Meyer, R. & Powers, P. (1989) A prospectivecomparison of four techniques for measuring platelet-associated
IgG. British Journal of Haematology, 71, 97±105.
Kelton, J.G., Neame, P.B., Bishop, J., Ali, M., Gauldie, J. & Hirsh, J.
(1979) The direct assay for platelet-associated IgG (PAIgG): lack ofassociation between antibody level and platelet size. Blood, 53,
73±80.
Kelton, J.G. & Steeves, K. (1983) The amount of platelet-bound
albumin parallels the amount of IgG on washed platelets frompatients with immune thrombocytopenia. Blood, 62, 924±927.
Kerry, P.J. & Curtis, A.D. (1985) Standardization of b-thromboglo-
bulin (b-TG) and platelet factor 4 (PF4): a collaborative study to
establish international standards for b-TG and PF4. Thrombosis
and Haemostasis, 53, 51±55.
Khan, I., Zucker-Franklin, D. & Karpatkin, S. (1975) Microthrom-
bocytosis and platelet fragmentation associated with idiopathic/autoimmune thrombocytopenic purpura. British Journal of Hae-
matology, 31, 449±460.
Lightsey, A.L., McMillan, R., Koenig, H.M., Schanberger, J.E. &
Lang, J.E. (1976) In vitro production of platelet-binding IgG inchildhood idiopathic thrombocytopenic purpura. Journal of
Pediatrics, 88, 414±418.
McKeown, L.P., Williams, S.B., Shafer, B., Murray, N. & Grainick, H.R.(1993) Alpha granule proteins in type I von Willebrand's disease.
American Journal of Hematology, 42, 158±161.
McMillan, R. (1981) Chronic idiopathic thrombocytopenic purpura.
New England Journal of Medicine, 304, 1135±1147.Mueller-Eckhardt, C., Kayser, W., Mersch-Baumert, K., Mueller-
Eckhardt, G., Breidenbach, M., Kugel, H.G. & Graubner, M. (1980)
The clinical signi®cance of platelet associated IgG: a study of 298
patients with various disorders. British Journal of Haematology, 46,123±131.
Pfueller, S.L., Chesterman, I., Illes, S., Hussein, S. & Martin, T.F.
(1986) Relationship of platelet-associated immunoglobulin G andplatelet protein to platelet size and density in normal individuals
and patients with thrombocytopenia. Journal of Laboratory and
Clinical Medicine, 107, 299±305.
Pfueller, S.L., Cosgrove, L., Firkin, B.G. & Tew, D. (1981) Relationshipof raised platelet IgG in thrombocytopenia to total platelet protein
content. British Journal of Haematology, 49, 293±302.
Shulman, N.R., Leissinger, C.A., Hotchkiss, A.J. & Kautz, C.A. (1982)
The nonspeci®c nature of platelet associated IgG. Transactions ofthe Association of American Physicians, 95, 213±226.
Sinha, R.K. & Kelton, J.G. (1990) Current controversies concerning
the measurement of platelet-associated IgG. Transfusion Medicine
Reviews, 4, 121±135.van Leeuwen, E.F., van der Ven, J.T.H., Engelfriet, C.P. & von dem
Borne, A.E.G. (1982) Speci®city of autoantibodies in autoimmune
thrombocytopenia. Blood, 59, 23±26.Warkentin, T.E., Hayward, C.P.M., Boshkov, L.K, Santos, A.V.,
Sheppard, J-A.I., Bode, A.P. & Kelton, J.G. (1994) Sera from patients
with heparin-induced thrombocytopenia generate platelet-derived
microparticles with procoagulant activity: an explanation for thethrombotic complications of heparin-induced thrombocytopenia.
Blood, 84, 3691±3699.
Warner, M.N., Moore, J.C., Warkentin, T.E., Santos, A.V. & Kelton, J.G.
(1999) A prospective study of protein-speci®c assays used toinvestigate idiopathic thrombocytopenic purpura. British Journal
of Haematology, 104, 442±447.
Woods, V.L., Kurata, Y., Montgomery, R.R., Tani, P., Mason, D.,Oh, E.H. & McMillan, R. (1984a) Autoantibodies against platelet
glycoprotein Ib in patients with chronic idiopathic thrombocyto-
penic purpura. Blood, 64, 156±160.
Woods, V.L., Oh, E.H., Mason, D. & McMillan, R. (1984b)Autoantibodies against the platelet glycoprotein IIb/IIIa complex
in patients with chronic ITP. Blood, 63, 368±375.
Zucker-Franklin, D. & Karpatkin, S. (1977) Red cell and platelet
fragmentation in idiopathic autoimmune thrombocytopenicpurpura. New England Journal of Medicine, 297, 517±526.
q 1999 Blackwell Science Ltd, British Journal of Haematology 106: 762±770
770 Mary Hughes et al