MEANINGFUL USE - Greenway Health...Meaningful Use Reporting by Stage Overall, MU reporting (meaning...
48
MEANINGFUL USE Best Practices Guide MEANINGFUL USE
Transcript of MEANINGFUL USE - Greenway Health...Meaningful Use Reporting by Stage Overall, MU reporting (meaning...

MEANINGFULUSEBest Practices Guide
MEANINGFUL USE

INTRODUCTION

INTRODUCTIONThe Medicare and Medicaid Electronic Health Record (EHR) Incentive Programs, commonly known as meaningful use (MU), reward providers for delivering high-quality care — shifting American healthcare away from fee-for-service and toward pay-for-performance models to improve care and manage costs. Various quality programs — including accountable care organizations (ACOs) and the Physician Quality Reporting System (PQRS) — share the pay-for-performance goals of MU and continue to adopt its quality reporting objectives.
Public and private payer alignment will only increase as these quality initiatives evolve from adoption and functionality incentive programs into foundational elements of physicians’ reimbursements for care. Already, MU and related quality programs have sharpened their focus on patient outcomes and population health management. Multi-program performance initiatives in the 2016 Medicare physician fee schedule reflect this, as do proposals pending in Congress that would employ MU, PQRS and patient engagement strategies to help restructure the existing fee-for-service system.
To help ensure that you have the information you need to avoid financial penalties and plan for MU and its impact on other reimbursement programs, Greenway Health™ is delighted to present this guide to benefiting from MU and quality reporting. The guide:
• Walks you through registration, reporting choices, timelines, and attestation and payment cycles
• Details opportunities for bundling MU with other incentive programs — offering many benefits to practices, with little additional effort
• Includes insights and experiences shared by your peers, because one of the best ways to succeed in a program like MU is to familiarize yourself with what has worked for others
For your convenience, we’ve included at-a-glance charts and visual information, links to relevant Centers for Medicare & Medicaid Services (CMS) and Office of the National Coordinator for Health Information Technology (ONC) materials, and data examples to show the impact MU has on patient care and care coordination.
Three icons will be used next to section takeaways, indicating a classification for that particular bullet.
Great Resource Note Did You Know


Introduction ................................................................................................................................ 2Getting Started ........................................................................................................................... 6 Staging the Vision and Goals ................................................................................................. 7 Eligibility and Applicable Timelines ..................................................................................... 7 EPs in the Medicare Pathway ............................................................................................ 7 EPs in the Medicaid Pathway ............................................................................................ 7 Medicaid Eligibility Threshold Requirements .................................................................. 8 Meaningful Use Reporting by Stage ..................................................................................... 8Why Participate? ...................................................................................................................... 10 Incentive Fund Capture ....................................................................................................... 11 Medicare Pathway ............................................................................................................ 11 Medicaid Pathway ............................................................................................................ 12 Avoid Payment Adjustments ............................................................................................... 13 Ongoing Hardship Exceptions ......................................................................................... 13 Alignment With Quality Incentive Programs...................................................................... 14 Physician Quality Reporting System (PQRS) .................................................................. 14 Patient Care .......................................................................................................................... 14 Care Coordination, Safety and Outcomes ...................................................................... 14 Benefits of Patient Portals .............................................................................................. 15 Portals and MU Requirements ....................................................................................... 15How to Participate ................................................................................................................... 18 Implement and Verify a Meaningful Use-certified EHR ................................................ 19 Verify EHR Certification ................................................................................................... 19 Understanding Certification Editions ............................................................................. 19 Registering Per-provider for Meaningful Use Incentives ............................................. 20Assessing and Selecting Meaningful Use Measures ............................................................ 22 Changes for 2015 Through 2017.......................................................................................... 23 Summary of Care Objective ............................................................................................. 24 Clinical Quality Measures ................................................................................................ 25 Quality Measures and Incentive Programs ........................................................................ 25 What They Gauge .............................................................................................................. 25 Where the Data Comes From .......................................................................................... 25 How CMS Uses the Data .................................................................................................. 25Selection and Reporting .......................................................................................................... 26 Recommended Core Sets .................................................................................................... 27 Adult Recommended Core Measures ............................................................................. 27 Pediatric Recommended Core Measures ...................................................................... 27 Why These Specific Measures? ....................................................................................... 28 Choosing Appropriate CQMs for Your Practice ................................................................. 28 Reporting CQMs ............................................................................................................... 28What Are Your Colleagues Doing? .......................................................................................... 30 EPs’ Plans to Attest for Stage 2 .......................................................................................... 31 Providers Polled on Attestation .......................................................................................... 31 Top-ranked CQM Groups ..................................................................................................... 32 Preventive Care and Screening .......................................................................................... 32 Top-reported Pediatric Measures ...................................................................................... 33Capturing and Reporting (Attesting) Data ............................................................................. 34 Dashboard Technology ........................................................................................................ 35 Attestation ............................................................................................................................ 35 Attestation and CQMs .......................................................................................................... 35 Amending Submitted Attestations ...................................................................................... 35 Receiving Your Payment ...................................................................................................... 36 Meaningful Use Audits ........................................................................................................ 36 Appeals Process .............................................................................................................. 36What’s Next? ............................................................................................................................ 38 Meaningful Use Stage 3 ....................................................................................................... 39 Overview ........................................................................................................................... 39 Stage 3 Objectives and Measures ................................................................................... 39Now What? ............................................................................................................................... 42 Tools to Demonstrate Meaningful Use of HIT ................................................................43Glossary of Acronyms .............................................................................................................44Web Links ................................................................................................................................. 46
TABLE OF CONTENTS

GETTING STARTED

Getting Started | 7
GETTING STARTEDStaging the Vision and Goals
Understanding that EHR adoption has financial, workflow, installation and staffing implications, Congress supported funding the MU incentive program as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 to encourage widespread and accelerated adoption.
The HITECH Act charged CMS with determining program requirements in two categories:
• Objectives – Types of data to be captured
• Measures – Patient population levels, thresholds or percentages at which the data should be collected
The act also required CMS to create a set of clinical quality measures (CQMs). Provider groups and health information technology (HIT) organizations provided input used to shape the data-capture requirements.
The vision for MU is twofold:
1) To advance the functionality of EHRs and the corresponding documentation of clinical data over time
2) To use that data to advance evidence-based medicine by analyzing the impact of technology-driven or automated physician support tools on patient care, patient adherence to care plans and patient outcomes
MU intends to improve outcomes for at-risk elderly and low-income populations who represent the most clinically and financially challenging cases with respect to chronic disease management and access to care. On a larger scale, MU and related quality programs such as PQRS aim to improve clinical documentation and preventive care for better patient outcomes, improved population health and lower costs for all in the United States, regardless of age or income.1
To meet these goals, MU is organized into three stages, each with a unique area of emphasis as prescribed by CMS and ONC:
• Stage 1 – Data capture and reporting
• Stage 2 – Information exchange and care coordination
• Stage 3 – Improving outcomes
Later sections in this guide describe each stage — including requirements and goals — in more detail.
Eligibility and Applicable Timelines
MU defines eligible providers (EPs) as those who practice within the following categories, which include both primary care and specialty medicine.
EPS IN THE MEDICARE PATHWAY:
• Doctor of medicine or osteopathy
• Doctor of dental surgery or dental medicine
• Doctor of podiatry
• Doctor of optometry
• Chiropractor
EPS IN THE MEDICAID PATHWAY:
• Physicians (primarily, doctors of medicine and doctors of osteopathy)
• Nurse practitioner
• Certified nurse-midwife
• Dentist
• Physician assistant who furnishes services in a Federally Qualified Health Center (FQHC) or Rural Health Clinic (RHC) that is led by a physician assistant
MU timelines remain flexible as to when an EP can enter either program, which then determines how many payment years and maximum incentive funds can be pursued.
1Centers for Medicare and Medicaid Services. “Quality Initiatives — General Information.” http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/index.html?redirect=/QualityInitiativesGenInfo/01_Overview.asp

8 | Getting Started
MEDICAID ELIGIBILITY THRESHOLD REQUIREMENTS
In addition to qualifying by clinician category, Medicaid EPs must:
• Have a 30% minimum Medicaid patient volume (20% for pediatricians), or
• Practice predominantly in an FQHC or RHC with a minimum 30% of patients meeting the definition of needing assistance
o CMS defines individuals “needing assistance” as those meeting any of the following three criteria:
1) Receiving medical assistance from Medicaid or the Children’s Health Insurance Program (CHIP)
2) Furnished uncompensated care by the provider
3) Furnished services at either no cost or reduced cost based on a sliding scale determined by the individual’s ability to pay
CHIP patients do not count toward patient volume criteria to industry performance benchmarks.
Meaningful Use Reporting by Stage
Overall, MU reporting (meaning the ongoing compilation and submission of required data to CMS) is accomplished by stage, and each stage extends over calendar years. How many calendar years depends on when an EP began reporting Stage 1. As a general rule, the program requires that EPs report at least two years of a given stage before advancing to the next.
For 2015 and beyond, CMS has merged Stage 1 and Stage 2 objectives into 10 total objectives, replacing the “core” and “menu” approach. While all EPs will report the same objectives, there are embedded exclusions for those still in Stage 1 in 2015.
Within current proposals and timelines, EPs can voluntarily begin Stage 3 in 2017. Currently, 2018 is set as the mandatory beginning of Stage 3 for all EPs.
Takeaways
Note
If an EP is brand new to MU in either 2015 or 2016, current proposals will also allow a 90-day reporting period for 2016.

Getting Started | 9
Reporting timelines
For 2015, EPs are only required to report and attest for any continuous 90-day period from within the 2015 calendar year.
According to current guidelines, however, recurring or returning EPs who participated in MU prior to 2015 will be required to report for the entire calendar year during 2016 and 2017.
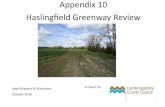
As described in the chart below, CMS is technically referring to program requirements as “Modified” Stage 2 or 3. This refers to the modification that eliminated
or lessened objectives and measures to be met in 2015 through 2017. In CMS language, this is a modification of the original Stage 2 final rule.
While all of the scenarios shown in the chart refer to Stage 2, EPs are still eligible to attest to Stage 1 objectives and measures if your first year of participation in the MU program was in either 2014 or 2015.
If you are in Stage 1 in 2015, there are specific exclusions to the modified objectives and measures, as detailed later in this guide.
Figure 1: Stages of Meaningful Use Modified
STAGE OF MEANIGFUL USE
FIRST YEAR AS A MEANINGFUL EHR USER 2015 2016 2017 2018
2011 Modified Stage 2 Modified Stage 2 Modified Stage 2 or Stage 3 Stage 3
2012 Modified Stage 2 Modified Stage 2 Modified Stage 2 or Stage 3 Stage 3
2013 Modified Stage 2 Modified Stage 2 Modified Stage 2 or Stage 3 Stage 3
2014 Modified Stage 2* Modified Stage 2 Modified Stage 2 or Stage 3 Stage 3
2015 Modified Stage 2* Modified Stage 2 Modified Stage 2 or Stage 3 Stage 3
2016 N/A Modified Stage 2 Modified Stage 2 or Stage 3 Stage 3
Notes*Eligible providers are still able to attest to Stage 1 objectives and measures if this is their first year of participation in the meaningful use program.

WHY PARTICIPATE?

Why Participate? | 11
WHY PARTICIPATE?
Incentive Fund CaptureMU rewards EHR adoption and continuous reporting through incentive funds granted per EP, no matter the size of a practice’s clinical staff.
This holds true whether EPs are pursuing the Medicare or Medicaid pathway, but there are fundamental differences between the two that have implications for:
• Total incentives received
• When an EP must begin a pathway to receive any funds
• When the funds run out
• Avoiding payment penalties, also known as “adjustments”
MEDICARE PATHWAY
In the Medicare pathway, incentive payments depend on when an EP enters the program. Payment amounts decrease over time, as detailed in Figure 2.
Important deadlines and incentive caps:
• 2016 is the last year that Medicare EPs can receive a payment (despite the overall program lasting through 2021 for Medicare or Medicaid EPs).
• Throughout a given EP’s Medicare timeline, an EP can miss an entire attestation year and then re-enter the program. For example, missing year two would mean then receiving the payment for year three. (A missed year’s payment cannot be made up, and missing a year would count against a maximum five-year cycle and payment).
Figure 2: Stages of Meaningful Use Modified
First Payment Received in 2011
First Payment Received in 2012
First Payment Received in 2013
First Payment Received in 2014
Payment Amount in 2011 $18,000
Payment Amount in 2012 $12,000 $18,000
Payment Amount in 2013
$7,840 Reduction ($160)
$11,760 Reduction ($240)
$14,700 Reduction ($300)
Payment Amount in 2014
$3,920 Reduction ($80)
$7,840 Reduction ($160)
$11,760 Reduction ($240)
$11,760 Reduction ($240)
Payment Amount in 2015
$1,960 Reduction ($40)
$3,920 Reduction ($80)
$7,840 Reduction ($160)
$7,840 Reduction ($160)
Payment Amount in 2016
$1,960 Reduction ($40)
$3,920 Reduction ($80)
$3,920 Reduction ($80)
TOTAL Incentive Payments $43,720 $43,480 $38,220 $23,520
Notes*As required by law, President Obama issued a sequestration order on March 1, 2013. Under mandatory reductions, Medicare EHR incentive payments made to eligible professionals and eligible hospitals will be reduced by 2%. This 2% reduction has been applied to any Medicare EHR incentive payment for a reporting period that ended on or after April 1, 2013. This reduction does not apply to Medicaid EHR incentive payments.

12 | Why Participate?
MEDICAID PATHWAY
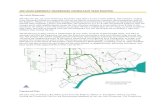
The Medicaid pathway is a maximum six-year funding program allowing a total, per-EP incentive payment of $63,750, as shown in Figure 3. Incentive payments in the Medicaid pathway remain the same over time and allow more flexible start dates to receive the maximum amount through 2021.
Important deadlines and notes
• 2016 is the last year a Medicaid EP can enter the program and receive maximum funds.
• The maximum participation of six years does not have to be completed during consecutive years, depending on start date.
• Funding is administered voluntarily by states and territories and can be subject to the participating state’s changes in funding or funding levels.
• The $21,250 one-time payment is for EPs who adopt, implement or upgrade (AIU) an EHR to one that is certified by ONC to satisfy MU functionality. This initial payment does not count as the first actual year of reporting and attestation.
Figure 3 Medicaid EHR Incentive Payment Schedule for Eligible Professionals First Payment
Received in 2011First Payment
Received in 2012First Payment
Received in 2013First Payment
Received in 2014First Payment
Received in 2015First Payment
Received in 2016
Payment Amount in 2011 $21,250 $0 $0 $0 $0 $0
Payment Amount in 2012 $8,500 $21,250 $0 $0 $0 $0
Payment Amount in 2013 $8,500 $8,500 $21,250 $0 $0 $0
Payment Amount in 2014 $8,500 $8,500 $8,500 $21,250 $0 $0
Payment Amount in 2015 $8,500 $8,500 $8,500 $8,500 $21,250 $0
Payment Amount in 2016 $8,500 $8,500 $8,500 $8,500 $8,500 $21,250
Payment Amount in 2017 $0 $8,500 $8,500 $8,500 $8,500 $8,500
Payment Amount in 2018 $0 $0 $8,500 $8,500 $8,500 $8,500
Payment Amount in 2019 $0 $0 $0 $8,500 $8,500 $8,500
Payment Amount in 2020 $0 $0 $0 $0 $8,500 $8,500
Payment Amount in 2021 $0 $0 $0 $0 $0 $8,500
TOTAL Incentive Payments $63,750 $63,750 $63,750 $63,750 $63,750 $63,750

Why Participate? | 13
Avoid Payment Adjustments Like incentive payments, payment adjustments in the MU program were meant to motivate the adoption and meaningful use of EHRs.
Adjustments primarily affect EPs in the Medicare pathway.
Beginning on Jan. 1, 2015, payment adjustments started at 1 percent of EPs’ annual Medicare Part B claims of the Medicare Physician Fee Schedule. They will then accumulate over time to a currently projected 5 percent by 2019, depending on national attestation rates.
Generally, the adjustments are structured on an every-other-year basis. For example, if you did not attest in 2013, you will incur the 1 percent adjustment in 2015 and so on through the life of MU. CMS is currently projecting payment adjustments to occur through 2020.
Despite incentive payments in the Medicare pathway ending in 2016, Medicare EPs should continue with annual MU reporting and stage progression to avoid mounting payment adjustments.
ONGOING HARDSHIP EXCEPTIONS
Because payment adjustments can continue through the life of the MU program, hardship exceptions to the Medicare payment adjustments can likewise continue past the first payment adjustment in 2015.
Hardship categories providing exceptions from payment adjustments, according to CMS language, include:
• Lack of infrastructure — Insufficient Internet access to comply with related objectives and “insurmountable” barriers to obtaining connectivity
• Unforeseen/uncontrollable circumstances — Natural disaster, practice closure, financial reasons, EHR certification/ vendor issues
• Lack of “control” over availability of certified EHR technology — Natural disaster, practice closure, financial reasons, EHR certification/vendor issues
• Lack of face-to-face interaction with patients — When face-to- face interaction and follow-up with patients are outside of practice scope or when follow-up is “extremely rare”
Takeaways
Great Resource
• You can plan or estimate current and future payment cycles by using the charts in this guide. For more help planning your course of action, take advantage of CMS’s interactive online tool, My EHR Participation Timeline https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Participation-Timeline.html
Note
• Medicaid EPs in the MU program who do not bill Medicare are not subject to payment adjustments. But be careful to note that if you are in the Medicaid pathway and bill Medicare for patients who are Medicare beneficiaries, you will be subject to payment adjustments if you are not actively participating in MU or if you skip a reporting year.
Did You Know
• New for 2015 For 2015 attestations only, Congress and the president passed a law, Dec. 28, allowing for blanket hardship exceptions under the "Unforeseen/uncontrollable circumstances" hardship category. CMS says it will issue an application process early in January. To be granted, the law intends that EPs would only have to state they didn't have time to fully report in 2015, since the Stage 2 final rule was issued with less than 90 days left in calendar year 2015.

14 | Why Participate?
Alignment With Quality Incentive ProgramsMU provides a foundation for the workflows, clinical functionality, documentation and reporting not only to lower barriers for entering other quality programs, but also to align your practice’s quality reporting with other programs offering incentive capture.
PQRS — which predates MU — has increasingly aligned its electronic clinical quality measures (eCQMs) and EHR reporting requirements with those of MU.
This alignment of quality reporting requirements across programs will continue to expand with the development of advanced payment models (APMs) formed by CMS in collaboration with private payers (as detailed in the following sections).
PHYSICIAN QUALITY REPORTING SYSTEM (PQRS)
There are also many similarities between the MU and PQRS programs, in part because both are administered by CMS.
In PQRS, as in MU, providers and clinicians must meet eligibility criteria to participate. PQRS eligibility requirements can be found here: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/.
For example, EPs in both programs can select the same CQMs to satisfy both program requirements, provided that the measures are reported to CMS through EHRs certified to the MU program.
Payment penalties (adjustments) are part of the PQRS process. Adjustment rules differ depending on whether the reporting entity is an individual EP or a group practice:
• Overall, EPs who did not participate or report in 2014 are subject to a 2016 payment adjustment.
• Group reporting includes a requirement to register within the Group Practice Reporting Option (GPRO). Registering and then reporting nine CQMs through a certified EHR means avoiding a 2016 Medicare payment adjustment.
Patient CareCARE COORDINATION, SAFETY AND OUTCOMES Better documentation of patient care, improved tracking of outcomes and greater patient engagement represent major goals of MU. By following MU criteria, practices can advance patients’ access to their own health information, decrease adverse drug interactions and clinical errors,
Takeaways
Great Resource
• The CMS website, www.cms.gov, maintains a wealth of information on the PQRS program and its alignment with MU www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2014PQRS_EHR_Made_Simple_F12-20-2013.pdf

Why Participate? | 15
automate preventive and follow-up care processes, and streamline referrals for improved care coordination.
Progress toward those goals has already been made through several MU core objectives:2
• Electronic prescribing: More than 190 million electronic prescriptions have been transmitted since MU began. This, coupled with a separate required objective to utilize Computerized Physician Order Entry (CPOE) for medication orders, has been credited with reducing prescription and medication errors.
• Patient reminders: More than 13 million reminders have been sent for patients ages 65 and older or five and younger – which is driving adherence to care plans.
• Patient electronic access: More than 33 million patients have received electronic access to health information via patient portals.
BENEFITS OF PATIENT PORTALS
Every day, millions of people in the U.S. transact with banks, book airfare, reserve tables at restaurants and more using Internet and mobile applications or “apps.” They’ve grown to appreciate the convenience, access and speed with which apps enable them to accomplish these everyday tasks. It’s no wonder, then, that people have started to demand the same convenient access to their health information. When you couple that demand with the healthcare sector’s increased focus on patient engagement as a means to improve patient outcomes and population health, a spotlight falls on patient portals and the benefits they offer practices and patients.
Meeting MU reporting requirements for patient engagement presents a win-win situation: Through a patient portal on a practice’s website, patients can take an active role in their own healthcare, and practices acquire tools to boost office efficiency.
Through a portal, patients should be able to:
• Schedule appointments
• Request prescription refills
• Access financial tools, such as online statements and bill pay
• Review care and office visit summaries
• Access integrated personal health records (PHRs)
• Review test and lab results
• Access appointment reminders
• Contact the office through secure messaging
• Update insurance or contact information
Making these features available to patients can improve office efficiency by:
• Decreasing phone calls and mail
• Reducing time spent updating records and completing administrative tasks
• Minimizing waiting room paperwork
PORTALS AND MU REQUIREMENTS
Online patient portals can aid in meeting the following MU objectives for 2015-2017 Stages 1 and 2 reporting.
View, Download or Transmit
Stage 1
• 50% of patients are provided online access to their patient summary, with the ability to view, download or transmit
Stage 2
• At least 1 patient views, downloads or transmits his or her online health record during the reporting period in 2015/2016. (2017, more than 5%.)
• 50% of patients are provided online access to their patient summary, with the ability to view, download or transmit
2Tagalicod, Robert, Director, Office of E-Health Standards and Services, Centers for Medicare and Medicaid Services. “The Real World Impact of Meaningful Use.” Available at: http://www.cms.gov/eHealth/ListServ_RealWorldImpact_MeaningfulUse.html.

16 | Why Participate?
Takeaways
Did you know?
• Greenway Health provides practices with posters, brochures and more to help encourage patients to use the portal.
PROMOTE YOUR PORTAL
Simply having a portal doesn’t guarantee patients will use it, but you can maximize adoption rates — and eventually, results — with promotions including:
• Posters and pamphlets in waiting and exam rooms
• Promotion on paper billing statements
• Promotion during telephone conversations
• Take-home cards with login instructions
• Incentives such as preferred appointment times if requested through the portal
• Registration assistance during office visits
• Clear icons and prompts on practice website
• Regular external information flow to patient population
• Awareness campaigns
• Office hours
• Special events
• Physician buy-in and promotion directly to patients
Provide Patient-specific Education
Stage 1
• If chosen as a menu item, provide patient-specific education materials to more than 10% of all unique patients seen during the reporting period. Excluded if not chosen as a menu item
Stage 2
• Provide patient-specific education materials to more than 10% of all unique patients seen during the reporting period
Secure Messaging
Stage 1
• Excluded
Stage 2
• Attest that EHR is fully enabled to send/receive secure messages in 2015. For 2016, send for 1 patient. For 2017, send for more than 5% of patients


HOW TO PARTICIPATE

How to Participate | 19
HOW TO PARTICIPATE
Implement and Verify a Meaningful Use-certified EHRThe Office of the National Coordinator for Health Information Technology (ONC) oversees the certification process of EHRs to the specifications of MU objectives and measures. ONC has designated three organizations to carry out the testing and certification of EHRs, the names of which you should be familiar with when assessing EHR capabilities:
• Drummond Group www.drummondgroup.com/
• ICSA Labs www.icsalabs.com/
• InfoGard Laboratories, Inc www.infogard.com/
Verify EHR CertificationThe ONC maintains a detailed website that includes a list of all complete or modular EHRs that have been certified for MU. The site is searchable by vendor, product name or certification number.
Understanding Certification EditionsTo meet and report MU requirements from 2015 through 2017, EPs must use a 2014-certified edition of their EHR software.
After identifying MU certification and implementing a certified EHR, you are ready to register for the program.
Takeaways
Note
• Vendors must make available 2015-certified edition software by 2017 to accommodate EPs who wish to voluntarily begin MU Stage 3 in 2017. Stage 3 objectives and measures will require a 2015-certified software edition. EPs can also choose to report Stage 2 through 2017 — requiring the 2014 MU software edition only — before moving to Stage 3 in 2018, which will be mandatory for all EPs under current timelines.
Great Resource
• Additional information on the certification process can be found at www.healthit.gov/policy-researchers-implementers/onc-health-it-certification-program

20 | How to Participate
Takeaways
Did you know?
• CMS allows a third party — such as a group practice staff member — to register EPs for the program. Registering this way will create an Identity and Access Management System (I&A) web user account (User ID/Password), which will be associated to the eligible professional’s National Provider Identifier (NPI). To pursue this option, get started at https://nppes.cms.hhs.gov/IAWeb/login.do
Registering Per-provider for Meaningful Use IncentivesTo register for the Medicare or Medicaid incentive programs, there are a few basic things to know and elements to have ready:
• Registration is only required once during the life of the incentive program
• Registration is required for every individual EP within a practice
• Registration requires two types of identifying information:
o National Provider Identifier (NPI)
o National Plan and Provider Enumeration System (NPPES) web user account
- The NPPES user ID and password begins registration
- Providers may apply for and obtain an NPPES login at https://nppes.cms.hhs.gov/NPPES/Welcome.do
CMS REGISTRATION
CMS provides detailed online guides for the registration process, as well as an online registration portal:
• Registration Guide — Medicare Pathway: Registration User Guide for Medicare Eligible Professionals www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHRMedicareEP_RegistrationUserGuide.pdf
• Registration Guide— Medicaid Pathway: Registration User Guide for Medicaid Eligible Professionals www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHRMedicaidEP_RegistrationUserGuide.pdf
• Registration Portal: https://ehrincentives.cms.gov/hitech/login.action


ASSESSING AND SELECTING MEANINGFUL USE MEASURES

Assessing and Selecting MU Measures | 23
GETTING STARTEDChanges for 2015 Through 2017
For 2015 through 2017, CMS has reduced the number of objectives, measures and thresholds required to meet MU incentives and avoid payment adjustments.
To attest for Stages 1 and 2, EPs are now required to report 10 objectives. Nine are variations on traditional
MU core and menu sets, and one is a public health reporting objective.
The table below details these objectives, the exclusions available for EPs in Stage 1 and the options for public health reporting in Stages 1 and 2.
Figure 4: Meaningful Use Objectives and Measures 2015-17 Stage 1 and Stage 2 EPs
OBJECTIVE MEASURE(S) EXCLUSION(S)
1) Patient Electronic Access 1) More than 50% of patients are provided online access within 4 business days, with the ability to view, download or transmit to a third party.
2) 2015-2016: At least one patient seen during the reporting period views, download or transmits; 2017: more than 5% of patients view, download or transmit.
1) No exclusion.
2) EP does not create care plan/record information; area provides less than 4Mbps broadband.
(Stage 1: Exclude measure 2)
2) Secure Messaging 1) 2015: Provider attests “yes-no” that EHR is fully enabled to send/receive secure messages; 2016: Secure message sent for at least one patient; 2017: Secure message sent to more than 5% of patients.
EP conducts no office visits during reporting period, or practices in an area with less than 4Mbps broadband.
(Stage 1: Exclude objective)
3) CPOE Conduct CPOE on more than:
1) 60% of medication orders
2) 30% of lab orders
3) 30% of radiology orders
EP writes less than 100 of each (or all) order sets during the reporting period.
(Stage 1: Conduct CPOE on more than 30% of unique patients/at least one medication order; exclude lab and radiology thresholds.)
4) Clinical Decision Support 1) 5 CDS interventions related to 4 or more CQMs during the reporting period. If 4 not relevant, then related to “high priority” health conditions. Suggests 1 of 5 CDS interventions “be related to improving healthcare efficiency”.
2) Ability to conduct drug-drug and drug-allergy interaction checks.
1) No exclusion.
2) EP who writes less than 100 med orders within the reporting period.
(Stage 1: Implement 1 CDS relevant to specialty or clinical priority and track compliance with CDS rule.)
5) Electronic Prescribing More than 50% of prescriptions are queried for a drug formulary and sent electronically.
EP writes less than 100 prescriptions during reporting period; no pharmacies within 10 miles that accept electronic prescriptions.
(Stage 1 for 2015 only: More than 40% of prescriptions sent electronically; no formulary check required.)
ASSESSING AND SELECTING MEANINGFUL USE MEASURES

24 | Assessing and Selecting MU Measures
Figure 4 continued: Meaningful Use Objectives and Measures 2015-17 Stage 1 and Stage 2 EPs
OBJECTIVE MEASURE(S) EXCLUSION(S)
6) Protect Electronic Health Information
Conduct security risk analysis which includes encryption of PHI stored in EHR. Update and correct as necessary.
No exclusion.
7) Patient-specific Education Provided to more than 10% of all unique patients seen during the reporting period.
EP conducts no office visits during the reporting period.
(Stage 1: Exclude objective if not intended as a menu item.)
8) Medication Reconciliation Conducts med reconciliation on more than 50% of patients received during a transition of care (TOC).
EP is not the recipient of a TOC during the reporting period.
(Stage 1: Exclude objective if not intended as a menu item.)
9) Health Information Exchange
1) Create electronic summary of care for all referred or transitioned patients.
2) Transmit referrals for more than 10% of transitions of care.
1) No exclusion.
2) EP conducts less than 100 outbound referrals/TOCS during the reporting period.
(Stage 1 for 2015: Exclude)
10) Public Health Reporting Stage 1 for 2015: Select 1Stage 2 for 2015: Select 22016-2017: Select 2
1) Immunization registry
2) Syndromic surveillance
3) Specialized registry reporting
Attest to 1 of 3 levels of “active engagement” per selection: 1) Registered
2) In validation testing process
3) Electronically submitting
Registry cannot accept electronic information. Registry has not announced readiness to accept information.
1) EP does not clinically conduct the procedures or treat patients associated with registry categories.
2) Does not treat or diagnose disease or conditions associated with syndromic surveillance.
3) Does not diagnose or treat any disease or condition associated with or collect relevant data, as required by specialized reporting registry in their jurisdiction.
SUMMARY OF CARE OBJECTIVE
Different objectives and different required elements
The Summary of Care objective requires that a patient's summary of care be electronically exchanged during transitions of care and referrals. The data elements required within a summary of care include:
Summary of Care (16 elements)
1) Patient name
2) Referring or transitioning provider’s name and office contact information (EP only)
3) Procedures
4) Encounter diagnosis
5) Immunizations
6) Laboratory test results
7) Vital signs
8) Smoking status

Assessing and Selecting MU Measures | 25
Figure 4 continued: Meaningful Use Objectives and Measures 2015-17 Stage 1 and Stage 2 EPs
OBJECTIVE MEASURE(S) EXCLUSION(S)
6) Protect Electronic Health Information
Conduct security risk analysis which includes encryption of PHI stored in EHR. Update and correct as necessary.
No exclusion.
7) Patient-specific Education Provided to more than 10% of all unique patients seen during the reporting period.
EP conducts no office visits during the reporting period.
(Stage 1: Exclude objective if not intended as a menu item.)
8) Medication Reconciliation Conducts med reconciliation on more than 50% of patients received during a transition of care (TOC).
EP is not the recipient of a TOC during the reporting period.
(Stage 1: Exclude objective if not intended as a menu item.)
9) Health Information Exchange
1) Create electronic summary of care for all referred or transitioned patients.
2) Transmit referrals for more than 10% of transitions of care.
1) No exclusion.
2) EP conducts less than 100 outbound referrals/TOCS during the reporting period.
(Stage 1 for 2015: Exclude)
10) Public Health Reporting Stage 1 for 2015: Select 1Stage 2 for 2015: Select 22016-2017: Select 2
1) Immunization registry
2) Syndromic surveillance
3) Specialized registry reporting
Attest to 1 of 3 levels of “active engagement” per selection: 1) Registered
2) In validation testing process
3) Electronically submitting
Registry cannot accept electronic information. Registry has not announced readiness to accept information.
1) EP does not clinically conduct the procedures or treat patients associated with registry categories.
2) Does not treat or diagnose disease or conditions associated with syndromic surveillance.
3) Does not diagnose or treat any disease or condition associated with or collect relevant data, as required by specialized reporting registry in their jurisdiction.
9) Functional status, including activities of daily living, cognitive and disability status
10) Demographic information, including preferred language
11) Care plan field, including goals and instructions
12 ) Care team, including the primary care provider of record and any additional known care team members beyond the referring or transitioning provider and the receiving provider
13) Reason for referral
14) Current problem list (and historical problems at discretion of EP)
16) Current medication list
17) Current medication allergy list
CLINICAL QUALITY MEASURES
In the past 10 years, CQMs have become an integral component in CMS’s drive to improve quality, reduce costs and expand access to healthcare for Medicare and Medicaid beneficiaries and, ultimately, for all patients in the U.S. Although quality reporting programs such as MU provide incentives to help providers implement and use EHRs to collect and report on clinical data, practices often need help deciding what data to collect, which measures to report on and how to best use their EHRs to do so.
The following provides you with the basic information you need to choose appropriate CQMs for your practice and offers tips on how to use your EHR to store the data in a structured format.
Quality Measures and Incentive Programs
As part of MU and other quality reporting programs, EPs must report on a selection of CQMs set forth by CMS.
Significant changes have been made to how CQMs are used under CMS quality reporting programs, including the Physician Quality Reporting System (PQRS) and the EHR Incentive Program (MU). CMS has worked hard to align the quality reporting requirements across the various programs. As a result, providers have the option to use the same set of quality measures to report CQMs for both PQRS and MU.
CQM reporting will continue to expand within the CMS MACRA program that will merge PQRS, MU and other quality measures as a new Medicare payment model set to begin in 2019.
IMPORTANT LINKS PQRS: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/index.html
EHR Incentive Program: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/ehrincentiveprograms/
WHAT THEY GAUGE• Health outcomes
• Clinical processes
• Patient safety
• Efficient use of healthcare resources
• Care coordination
• Patient engagement
• Population and public health
• Adherence to clinical guidelines
WHERE THE DATA COMES FROM
In the past, quality measures primarily used data from claims, but as technology has improved and become more prominent in the healthcare setting, many quality measures now use data from the provider’s EHR.
HOW CMS USES THE DATA
Think of CQMs as part of a system of care quality “checks and balances.” By requiring providers to track and record patient treatment via EHRs, CMS holds EPs accountable for providing safe, efficient and timely patient-centered care.
Some of the ways CMS uses CQM data include:
• To make policy decisions around quality
• To inform the public about the level of care provided within a given organization or by a particular provider
• To improve the quality of healthcare nationwide by focusing on programs designed to target significant weaknesses within our healthcare system

SELECTION AND REPORTING

Selection and Reporting | 27
SELECTION AND REPORTING
Recommended Core SetsEPs are encouraged to report from the recommended core set that best suits their scope of practice and patient population.
Additionally, all providers must select CQMs from at least three of the six key healthcare policy domains recommended by the Department of Health and Human Services’ National Quality Strategy:
• Patient and Family Engagement
• Patient Safety
• Care Coordination
• Population and Public Health
• Efficient Use of Healthcare Resources
• Clinical Processes/Effectiveness
A complete list of CQMs and their associated National Quality Strategy domains are posted on the recommended core set of CQMs (www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Recommended_Core_Set.html) for EPs — all focusing on high-priority clinical conditions.
A complete list of CQMs and their associated National Quality Strategy domains can be accessed, listed as recommended core sets of CQMs for EPs - all focusing on high-priority clinical conditions.
EPs must report on nine out of 64 total CQMs (https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EP_MeasuresTable_Posting_CQMs.pdf):
• 9 eCQMs for adult populations that meet all of the program requirements
• 9 eCQMs for pediatric populations that meet all of the program requirements
ADULT RECOMMENDED CORE MEASURES
• Controlling high blood pressure
• Use of high-risk medications in the elderly
• Preventive care and screening: Tobacco use: Screening and cessation intervention
• Use of imaging studies for low back pain
• Preventive care and screening: Screening for clinical depression and follow-up plan
• Documentation of current medications in the medical record
• Preventive care and screening: Body mass index (BMI) screening and follow-up
• Closing the referral loop: Receipt of specialist report
• Functional status assessment for complex chronic conditions
• Closing the referral loop: Receipt of specialist report
• Functional status assessment for complex chronic conditions
Full table of recommended adult measures can be found at https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014_CQM_AdultRecommend_CoreSetTable.pdf
PEDIATRIC RECOMMENDED CORE MEASURES
• Appropriate testing for children with pharyngitis
• Weight assessment and counseling for nutrition and physical activity for children and adolescents
• Chlamydia screening for women (16 to 24 years of age)
• Use of appropriate medications for asthma
• Childhood immunization status
• Appropriate treatment for children with upper respiratory infection (URI)
• ADHD: Follow-up care for children prescribed Attention-Deficit/Hyperactivity Disorder (ADHD) medication
• Preventive care and screening: Screening for clinical depression and follow-up plan
• Children who have dental decay or cavities

28 | Selection and Reporting
Full table of recommended adult measures can be found at https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014_CQM_PrediatricRecommended_CoreSetTable.pdf
WHY THESE SPECIFIC MEASURES?
CMS selected the recommended core sets of CQMs based on the following factors:
• Conditions that contribute to the morbidity and mortality of the most Medicare and Medicaid beneficiaries
• Conditions that represent national public health priorities
• Conditions that are common to health disparities
• Conditions that disproportionately drive healthcare costs and could improve with better quality measurement
• Measures that would enable CMS, states and the provider community to measure quality of care in new dimensions, with a stronger focus on sparing measurement
• Measures that include patient and/or caregiver engagement
For more detailed information on 2015 and 2016 CQMs and electronic reporting options, view the eCQM Library at www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/eCQM_Library.html.
Choosing Appropriate CQMs for Your PracticeThe following questions can help providers understand where opportunities for quality improvement exist and which measures are appropriate for tracking that improvement.
• Is the measure’s population reflected in your patient mix?
For example, a pediatrician should not choose a measure that excludes children.
• Does the measure correlate with specific diseases that are more prevalent or harder to control among your patients?
For example, the practice may have many patients with diabetes but few with asthma.
• Are you already using the measure for other quality measurement or reporting activities?
Consider what the practice does for commercial payers, the state and other initiatives. Take advantage of overlaps to streamline your data collection and reporting activities
Choosing CQMs to report on for MU can be a daunting task. It’s suggested that you begin this process by looking at your patient population as a whole and pulling out the top 10 to 20 diagnoses that you typically see. From there, you can match those diagnoses against the listing of CQMs available, identify the best candidates that align with the most-common diagnoses among your patients and work with your vendor to ensure that your EHR system has the ability to track the measures you select.
A HELPFUL HINT FROM THE FIELD “The key to choosing the best clinical quality measures for your practice to report against is to step back and look at your patient population as a whole.”
—Barbara Tergis, RN, BSNOffice Manager, Family Practice Hastings on Hudson, New York
Source: www.healthit.gov
REPORTING CQMS
CMS recognizes the need for program alignment and offers several ways to report CQMs based on the EPs involvement in other quality programs.
Options that only apply for the EHR Incentive Program:
• Attest to CQMs through the EHR Registration & Attestation System
• eReport CQMs through the PQRS Portal

Selection and Reporting | 29
Options that align with other quality programs:
• Report individual EPs’ CQMs through PQRS Portal
• Report group’s CQMs through PQRS Portal
• Report group’s CQMs through Pioneer ACO participation or Comprehensive Primary Care Initiative participation
To assess providers’ compliance and progress, most programs require that CQM data be reported. To capture and share patient data efficiently, providers need an EHR that stores data in a structured format. This structured data allows patient information to be easily retrieved and transferred and enables the provider to use the EHR in ways that can aid patient care.
Some of the EHR functions listed below can help improve the performance of this data:
• Confirm that the patient’s problem list is up to date
o Determine if patient meets exclusion or exception criteria for the measure
o Determine if patient is encountering specific barriers to treatment adherence
o Review any changes in vital signs
o Use clinical decision support to highlight missing services (for example, reminders for age-appropriate vaccinations or cancer screenings)
• Review the patient’s medications, if applicable
o Use ePrescribing to obtain prescription and refill history
o Determine if there are any drug-drug or drug-allergy interactions
o Confirm that the patient’s active medication and active medication allergy lists are up to date
o Perform a medication reconciliation, if necessary
o Determine if there are barriers to medication adherence for the patient
• Engage the patient
o Be sure to provide updated clinical summaries at each visit
- Ensure information on the clinical summary is accurate for the patient (for example, a mammogram reminder for a double mastectomy patient would not be appropriate)
o Provide patient with patient-specific education resources
o Send reminders for follow-up or preventive care using the patient’s preferred method
Figure 5: Provider Reporting of Clinical Quality Measures
QUALITY INITIATIVE WHO REPORTS CQMS? SOURCE OF DATA PROVIDER REPORTING MECHANISM PURPOSE OF REPORTING
EHR Incentive Program Eligible providers Electronic health record Attestation or Group Practice Reporting Option (GPRO)
Determine eligibility for EHR incentive
Physician Quality Reporting System Eligible Medicare physicians Medical records Group Practice Reporting
Option (GPRO)Determine eligibility for PQRS incentive payment
Accountable Care Organizations Medicare-approved ACOs Medical records, surveys
& claims Group Practice Reporting
Option (GPRO)Determine eligibility to
share in savings
Million Hearts Campaign Provider volunteers Provider-determined Optional Prevent cardiac- related deaths
Children’s Health Insurance Program Medicaid & CHIP agencies Claims N/A - State-reported
Monitor and improve quality for Medicaid & CHIP
beneficiaries
Medicare Advantage Part C Medicare Health Plans
Medical records, surveys & claims
Determined by health plan where applicable
Provide pubilicly available quality ratings for Medicare
Advantage Plans

WHAT ARE YOUR COLLEAGUES DOING?

What Are Your Colleagues Doing? | 31
WHAT ARE YOUR COLLEAGUES DOING?Greenway surveyed providers to learn more about which CQMs they use to attest for MU. The survey results offered great insight into the most-used CQM groups and the specific measures within each group.
Figure 6: EPs’ Plans to Attest for Stage 2
YES NO, but PLAN TO attest
NO, with NO plans to attest DON’T KNOW
STA
GE
1
STA
GE
284%
2%10%
4%
YES NO, but PLAN TO attest
NO, with NO plans to attest DON’T KNOW
20%
5%17%
58%
Figure 7: Providers Polled on Attestation84% of EPs have attested for MU Stage 1
78% have already attested or plan to attest for MU Stage 2
EPs have attested for MU Stage 1
EPs have already attested or plan to attest for MU Stage 2
84%
78%

32 | What Are Your Colleagues Doing?
Figure 8: Top-ranked CQM Groups• Preventive Care and Screening (78%)
• Hypertension (55%)
• Diabetes (52%)
According to the Centers for Disease Control and Prevention (CDC), more than one-third of U.S. adults (34.9 percent) are obese. With a rising obesity rate and related health conditions, it’s no surprise that these have become providers’ top CQM choices.
Preventive Care and Screening – 78%Hypertension – 55%
Diabetes – 52%
Others Include:Cancer Screening | 45%Care Coordination/Patient Safety Measures | 45%Asthma Measures | 31%Elderly Care | 31%Pediatric Measures | 28%Heart Failure, CAD, Atrial Fibrillation Measures | 28%
Mental Illness/Substance Abuse Measures | 21%Low Back Pain/Knee or Hip Replacement Measures | 17%Oncology Measures | 8%IVD Measures | 7%HIV/AIDS Measures | 5%Cataracts/POAG Measures | 2%
Figure 9: Preventive Care and ScreeningAmericans are living longer but with more chronic illness. This calls for more and more preventive care and places smoking, obesity and high blood pressure at the top of the CQMs on which providers choose to report.
Tobacco Use: Screening and Cessation Intervention – 83%
BMI: Screening and Follow-up – 76%
Preventive Care & Screening: Influenza Immunization – 67%
Others Include:Screening for High Blood Pressure and Follow-up Documented | 64%Cholesterol : Fasting Low-Density Lipoprotein (LDL-C) Testing | 56%Screening for Clinical Depression & Follow-up | 43%
Chlamydia Screening for Women | 42%Risk-Satisfied Cholesterol - Fasting Low-Density Lipoprotein (LDL-C) | 37%Pregnant Women that had HBsAG Testing | 30%

What Are Your Colleagues Doing? | 33
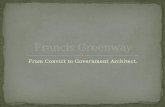
Figure 10: Top-reported Pediatric Measures Weight assessment and ADHD top the list of the reported pediatric clinical measures. Over the past three decades, childhood obesity rates in America have tripled, and today, nearly one in three children in America are overweight or obese. And an estimated 6.4 million children ages four through 17 had received a diagnosis of attention deficit hyperactivity disorder (ADHD) at some point in their lives. About two-thirds of those with a current diagnosis receive prescriptions for stimulants such as Ritalin or Adderall.
Childhood Immunization Status (NQF 0038)
Weight Assessment & Counseling for Nutrition and Physical Activity
for Children and Adolescents (NQF 024)
ADHD: Follow-Up Care for Children Prescribed Medication (NQF 0108)
Appropriate Treatment for Children with Upper Respiratory
infection (URI) (NQF 0069)
Appropriate Testing for Childrenwith Pharyngitis (NQF 0002)
Primary Caries Prevention and Intervention as Offered by Primary
Care Providers, including Dentists
Hemoglobin A1c Test (NQF 0060)
Maternal DepressionScreening (NQF 1401)
Children Who have DentalDecay or Cavities
79%
67%
46%
54%
33%
33%
26%
33%
21%

CAPTURING AND REPORTING (ATTESTING) DATA

Getting Started | 35
CAPTURING AND REPORTING (ATTESTING) DATADashboard Technology
To capture required clinical data — core objectives, menu objectives and CQMs — to be reported (attested) to CMS, choose certified EHR technology that offers a dashboard feature. Best practice MU dashboards in EHRs capture objective and CQM data for each attesting EP. By collecting data over time, these dashboards allow practices to view and assess each EP’s progress on the measures well before it is time to attest.
Attestation
Medicare EPs attest for MU via the same CMS online portal (https://ehrincentives.cms.gov/hitech/login.action) used to register for the program.
• The attestation process for both Medicare and Medicaid EPs requires the NPI number and logins, whether the attestation is through the national CMS portal or state Medicaid sites
• A third party may complete the attestation process on behalf of an EP
See more about the NPI and third-part attestation requirements in the Registration section of this guide.
Attestation and CQMsCQMs may be submitted along with core and menu objectives during attestation. EPs may also choose to submit one set of CQMs to satisfy requirements of both MU and other programs requiring CQMs data, such as PQRS.
Be aware that programs such as PQRS require a full calendar year of CQM reporting, which can delay your MU incentive payment until the CQM submission is processed, even if your MU attestation was for a 90-day period.
See the CQMs section of this guide for more information on CQMs.
Amending Submitted Attestations
Medicare EPs who wish to change or amend information after they have attested or believe an error has occurred may contact the CMS Information Center by telephone at 1-888-734-6433.
Takeaways
Note
• While both Medicare and Medicaid EPs register through the CMS portal, Medicaid EPs attest through their individual states’ Medicaid agency websites.
• MU attestation is not complete until the EP submits CQMs. Medicare EPs submit CQMs data to CMS. Medicaid EPs submit CQMs data to their state Medicaid agencies.
Capturing and Reporting (Attesting) Data | 35

36 | Capturing and Reporting (Attesting) Data
Receiving Your Payment
• Medicare EPs receive annual incentive payments in one lump sum, generally within the calendar quarter following the date of attestation
• Medicare EPs eligible for an additional payment by practicing in a Health Professional Shortage Area (HPSA) receive that payment separately from the main MU incentive payment
• Medicaid payments are subject to variations depending on how each state handles incentive payments
• Payments are matched to EPs through the same NPI or Taxpayer Identification Number (TIN) selected during registration
Meaningful Use Audits
Pre- and post-payment audits began in 2013 and remain in effect.
Resources available from the CMS website, www.cms.gov,include an overview of the audit program, details about supporting documentation checklists and examples of documentation (www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHR_SupportingDocumentation_Audits.pdf) used to support data objectives.
APPEALS PROCESS
For Medicare EPs, CMS maintains an appeals process for a variety of issues, such as audit findings, EHR certification, CQM electronic reporting, program eligibility and other topics pursued by an EP.
An overview of this process and sample submission forms can be found at www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Appeal_EP_FilingRequest-.pdf.
Takeaways
Note
• Retain data from each attestation for six years to cover the timeline for a potential MU audit.


WHAT’S NEXT?

What’s Next? | 39
WHAT’S NEXT?
Meaningful Use Stage 3OVERVIEW
• Stage 3 is currently scheduled to begin in 2018 for all Medicare and Medicaid EPs
• EPs who have successfully completed two years of Stage 2 can voluntarily begin Stage 3 in 2017 or submit an additional year of Stage 2 and begin Stage 3 in 2018
• To successfully report to Stage 3, EPs must use a 2015 edition of certified MU software
• EPs are required to report MU data for the entire calendar year for their first year of Stage 3
• For Stage 3, EPs will have to receive data as well as send — a new requirement for MU
o One major way that is being done is through the intake of patient-generated health data (PGHD)
- Data is to be received by practices and the EHR via Application Programming Interface (API) technology, which will allow patients to send data from third-party apps and will allow other practitioners to send patient data
- Portals will still be viable for Stage 3, as many APIs will be placed on existing portals as a gateway
- The traditional view, download and transmit functions remain for Stage 3 but in a more limited capacity within the overall Coordination of Care objective
STAGE 3 OBJECTIVES AND MEASURES
Stage 3 is proposed to include a set of eight objectives, similar to those established for MU Stage 2 reporting in 2015 through 2017. This demonstrates the goal of CMS to streamline and simplify the MU reporting process,
while aligning measures with other incentive and quality programs.
8 basic objectives (See accompanying chart for full objectives, measures and exclusions)
1) Protect Patient Health Information
2) Electronic Prescribing (eRx)
3) Clinical Decision Support
4) Computerized Physician Order Entry (CPOE)
5) Patient Electronic Access to Health Information
6) Coordination of Care through Patient Engagement
7) Health Information Exchange
8) Public Health and Clinical Data Registry Reporting
Stage 3 Measure and Threshold expansion examples:
• Electronic Prescribing
o More than 60% of all permissible prescriptions written by the EP are queried for a drug formulary and transmitted electronically
o Option for ePrescribing controlled substances in states allowing electronic prescriptions
• Computerized Physician Order Entry (CPOE)
o Used to record at least 60% of medication orders
o Used to record at least 60% of lab orders
o Used to record at least 60% of diagnostic imaging orders
• VDT/Patient Access to Information
o Provide more than 80% of patients with access to view, download or transmit their health information, through a portal or certified API
o Provide more than 35% of patients with access to patient-specific educational material

40 | What’s Next?
• Health Information Exchange
o Electronic summary of care is sent for more than 50% of referral and transition-of-care patients
o Electronic summary of care is received for more than 40% of referral and new patients coming into the practice
o Perform clinical reconciliation on more than 80% of TOCs received, two of three ways:
- Medications
- Medication allergies
- Problem list
• Public Health Reporting
o Select two of five measures:
- Immunizations (bidirectional)
- Syndromic surveillance (from urgent care settings only)
- Electronic case reporting (begins in 2018)
- Public health registries
- Clinical data registries
Figure 11: Meaningful Use Stage 3 Objectives and Measures
OBJECTIVE MEASURE(S) EXCLUSION(S)
1) Protect Patient Health Information
Conduct and update an annual security risk analysis. No exclusion.
2) Electronic Prescribing More than 60% of prescriptions are queried for a drug formulary and sent electronically.
EP writes less than 100 prescriptions during reporting period; no pharmacies within 10 miles that accept electronic prescriptions.
3) Clinical Decision Support 1) 5 CDS interventions related to 4 or more CQMs during the reporting period. If 4 not relevant, then related to “high priority” health conditions. Suggests 1 of 5 CDS interventions “be related to improving healthcare efficiency”.
2) Ability to conduct drug-drug and drug-allergy interaction checks.
1) No exclusion.2) EP writes less than 100 med orders during the reporting period.
4) CPOE 1) 60% of med orders
2) 60% of lab orders
3) 60% of imaging orders
EP writes less than 100 of each (or all) order sets during the reporting period.

What’s Next? | 41
Figure 11 Continued: Meaningful Use Stage 3 Objectives and Measures
OBJECTIVE MEASURE(S) EXCLUSION(S)
5) Patient Electronic Access to Health Information
1) More than 80% of patients given access to view, download, transmit and access to the API, within 48 hours of availability.
2) The patient is provided access to patient-specific education resources for more than 35% of patients.
EP conducts no office visits during the reporting period.
EP conducts 50% of patient encounters in county that does not have 50% of housing units with 4 Mbps broadband.
6) Coordination of Care Attest to all 3 measures, meet 2 of 3 measure thresholds1) More than 10% of patients engage with the EHR made
accessible by provider. This can be met by patient either:
A) Using VDT health information to a 3rd party, Or
B) Access health information via API, Or
C) Combination of both pathways
2) A secure message must be sent or received for more than 25% of patients (2017 only, more than 5%).
3) Patient-generated health data or from non-clinical setting received for more than 5% of patients.
EP conducts no office visits during the reporting period.
EP conducts 50% of patient encounters in county that does not have 50% of housing units with 4 Mbps broadband.
7) Health Information Exchange (Summary of Care/Transitions of Care)
Attest to all 3 measures, meet 2 of 3 measure thresholds.
1) Create and electronically send SOC for more than 50% of TOCs.
2) Create and add to SOC for more than 40% of TOCs received/new patient encounters.
3) Perform clinical information reconciliation on more than 80% of TOCs received/new patient encounters, 2 of 3 ways: meds, med allergies, problem list.
1) Less than 100 TOCs conducted during reporting period, or 50% of encounters occur in households without 4Mbps broadband.
2) Less than 100 TOCs/new patients received during the reporting period, or 50% of encounters occur in households without 4Mbps of broadband.
3) Less than 100 TOCs/new patients received during the reporting period.
8) Active Engagement of Public Health Reporting
Select 2 of 5
Show active engagement: Registered, within validation testing process, electronically submitting.
1) Immunization Registry (bi-directional)2) Syndromic Surveillance (urgent care only)3) Electronic Case Reporting (begins 2018)4) Public Health Registry5) Clinical Data Registry
Can report twice to 4 or 5 to meet objective.
1) EP does not give immunization, registry cannot accept electronic data, registry is not ready to accept 6 months prior to reporting period.
2) EP does not practice in category of providers used by registry, registry cannot accept, registry is not ready to accept 6 months prior to reporting period.
3) EP does not treat or diagnose disease being collected by reportable disease system, registry cannot accept, registry not ready to accept 6 months prior to reporting period.
4) EP does not diagnose or treat disease/condition matching registry, registry cannot accept, registry not ready to accept 6 months prior to reporting.
5) EP does not diagnose or treat conditions associated with clinical data registry, registry cannot accept, registry not ready to accept 6 months prior to reporting.

NOW WHAT?

Now What? | 43
NOW WHAT?
Tools to Demonstrate Meaningful Use of HITUnderstanding present and future MU requirements is the first step to preparing your practice for a smooth, successful attestation. Equally important, though, is choosing the right tools to track and report your progress toward meeting core and menu objectives. In order to participate in MU, practices need integrated practice management, EHR and data reporting solutions with the ability to exchange data with state registries.
To aid selection, begin looking for ONC-certified complete solutions. But keep in mind that as MU and other incentive programs become increasingly demanding, practices will benefit most from true healthcare IT partners who are dedicated to helping them stay compliant and profitable.
Greenway Health has partnered with more than 10,000 practices to provide award-winning clinical, operational and financial software solutions used to increase care quality, efficiency and patient safety and successfully attest for MU and other value-based programs.
Choose GreenwayEach physician and practice is different. Choose a partner that treats you that way. To see why thousands of your peers have selected Greenway Health as their EHR and health information solutions partner, greenwayhealth.com or call 877-446-3840.

GLOSSARY OF ACRONYMS

Getting Started | 45Glossary of Acronyms | 45
IT’S HEALTHCARE, SO YOU NEED THIS:
Glossary of AcronymsACO: Accountable Care Organization
AIU: Adopt, Implement or Upgrade
APM: Advanced Payment Model
CCHIT: the Certification Commission for Health Information Technology
CDS: Clinical Decision Support
CQMs: Clinical Quality Measures
CMS: Centers for Medicare & Medicaid Services
CPCi: Comprehensive Primary Care Initiative
EHR: Electronic Health Record
EHRA: Electronic Health Record Association
EP: Eligible Professional
FQHC: Federally Qualified Health Center
GPRO: Group Practice Reporting Option
HIT: Heath Information Technology
HITECH Act: Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009
MU: Meaningful use
NCQA: National Committee for Quality Assurance
NPI: National Provider Identifier
NPPES: National Plan and Provider Enumeration System
ONC: Office of the National Coordinator
PECOS: Medicare Provider Enrollment, Chain and Ownership System
PHR: Personal Health Record
PQRS: Physician Quality Reporting System
RHC: Rural Health Clinic
VDT: View, Download and Transmit

WEB LINKS

Web Links | 47
COMPREHENSIVE LIST OF LINKS:
CMS website: www.cms.gov
Centers for Medicare and Medicaid Services. Quality Initiatives — General Information: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/index.html?redirect=/QualityInitiativesGenInfo/01_Overview.asp
EHR Participation Timeline: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Participation-Timeline.html
The Real World Impact of Meaningful Use: www.cms.gov/eHealth/ListServ_RealWorldImpact_MeaningfulUse.html.
PQRS eligibility requirements can be found here: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/
PQRS program and its alignment with MU: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/Downloads/2014PQRS_EHR_Made_Simple_F12-20-2013.pdf
Information on the certification process: www.healthit.gov/policy-researchers-implementers/onc-health-it-certification-program
Registration User Guide for Medicare Eligible Professionals: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHRMedicareEP_RegistrationUserGuide.pdf
MU Registration Guide— Medicaid Pathway: Registration User Guide for Medicaid Eligible Professionals: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHRMedicaidEP_RegistrationUserGuide.pdf
MU Registration Portal: https://ehrincentives.cms.gov/hitech/login.action
NPPES login: https://nppes.cms.hhs.gov/NPPES/Welcome.do
National Provider Identifier (NPI): https://nppes.cms.hhs.gov/IAWeb/login.do
Full table of recommended pediatric measures: https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014_CQM_PrediatricRecommended_CoreSetTable.pdf
PQRS: www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/index.html
EHR Incentive Program: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/index.html?redirect=/ehrincentiveprograms/
Recommended core set of CQMs: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Recommended_Core_Set.html
EPs must report on nine out of 64 total CQMs: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EP_MeasuresTable_Posting_CQMs.pdf)
Full table of recommended adult measures: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014_CQM_AdultRecommend_CoreSetTable.pdf
eCQM Library: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/eCQM_Library.html
Audit program: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/EHR_SupportingDocumentation_Audits.pdf
Appeals process and sample submission forms: www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Appeal_EP_FilingRequest-.pdf
EHR and health information solutions partner: greenwayhealth.com
Drummond Group: www.drummondgroup.com/
ICSA Labs: www.icsalabs.com/
InfoGard Laboratories, Inc: www.infogard.com
HealthIT.gov: www.healthit.gov