
Md flux dx4 week 10
21
Monitored & Fueled by MDflux Inspired by Science, Driven to Improve Patient Outcomes Team Dx4 # of interviews: 6+8/82 George Brooks | Christine Chu | Mike Horning | Robert Lee | Collin Williams Our innovative nutritional diagnostic allows dietitians and physicians to provide precise nutritional support to patients, resulting in faster recovery from injury and critical illness, and reduced hospital stay.
-
Upload
steve-blank -
Category
Education
-
view
1.032 -
download
0
Transcript of Md flux dx4 week 10

Monitored & Fueled by MDflux
Inspired by Science, Driven to Improve Patient Outcomes
Team Dx4 # of interviews: 6+8/82
George Brooks | Christine Chu | Mike Horning | Robert Lee | Collin Williams
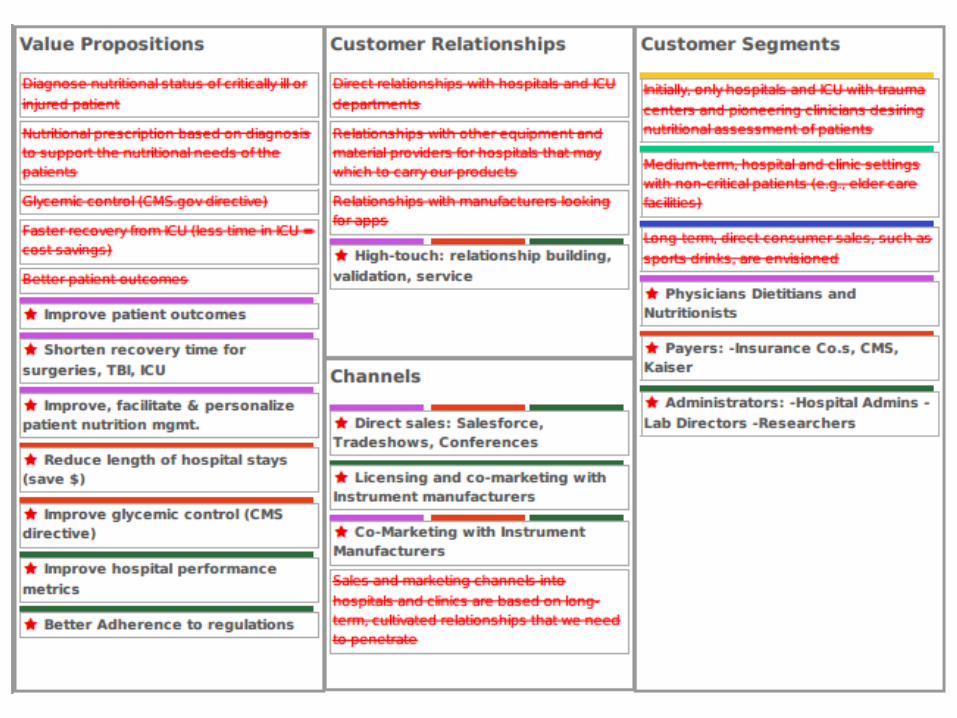
Our innovative nutritional diagnostic allows dietitians and physicians to provide precise nutritional support to patients, resulting in faster recovery from injury and critical illness, and reduced hospital stay.

ICUS lack accurate diagnostics to assess a patient’s nutritional state?
Here’s the Overlooked Problem
Overfed
Nourished
Starvation
Today’s Hospitalization Standard of Care

Standard of Hospital CareOur study shows near starvation state as maintained by standard of care for Traumatic Brain Injured Patients
Allowing for a body energy state supportive of healing and improved patient outcomes
Makes Diagnosis Possible Overfed
Nourished
Starvation
Actionable events with products already available
Traumatic Brain Injury
(TBI)
Product Market Fit – What we Thought
Neurologist

TBI
Etc….
OncologySurgeries
Short Gut
Preterm Infants
Product Market Fit – What we learned
Dietician
• Dietitians work across specialties• Dietitians will find Indications for Use• Dietitian will create demand for our products

Customer Archetype•Jill Redgate, Critical Dietitian, VA Hospital – West LA•Certified Clinician – Manages critical care•Orders nutritional support directly or consults with
physician
“[MDflux] could revolutionize nutrition and change standard of care”
Current Standard of Hospital Care
Time Honored equations based on height/weight/age
Personalized measurement of nutritional needs
Actionable data around the needs of each patient
Continuous monitoring of
progress

“This could replace the finger prick glucose test”Dr. Neil MartinChair of Neurosurgery at Ronald Reagan UCLA Medical Center
“You have to do this!”Susan MooreDirector of Strategy and Business Development, Children's Hospital & Research Center Oakland
“Nutrition is the ticket out of there.”Dr. Elizabeth Thilo, M.D.Clinical Neonatologist, University of Colorado, Denver 10/28/13Referring to premies leaving the NICU

PathologistLDT
Submits code:CPT 82544
Current Channel: In-Hospital LDT
Hospital Reimbursement
CMS / InsuranceUsing inpatient
DRG code
$185per test
*LDT = Laboratory Developed Test
Sales & Marketing
Dietitian & Physician order
test
What We Learned - Where to Start

Future Strategic Partnership
ReimbursementCMS / Insurance
Using New CPT/DRG Code
PathologistSubmits
UsingNew MDflux
Code
Sales & MarketScale CPT 82544
ResourcesAssistance with
Regulatory Approvals
What We Learned – Way Forward
$TBD

Overfed
Nourished
Starvation
6 Demo

What We Learned
1. Dietitian key stakeholder2. Indication for use in neonatal care3. Partnering with a multi-
national partner to scale and achieve FDA and international approvals.

Appendix

1. 14 TBI patients & 6 Controls, dual tracer Completed
Two JCI articles currently under review
2. 40 TBI patients, dual tracerConfirms the results of (1)
Will submit multiple publications
3. Started trial for TBI with single tracer plus Alternative FuelsDiscussing Surgery Application
Ongoing contract discussions and future publications
5. Pursuing Neonatologist KOL for Preterm Infant Care Application
4. Ongoing animal studies and research & development, Rutgers Univ.
Clinical Trials – UCLA & Others

Pricing Based on CPT Code 82544
What We Learned from the Course
Net Sales (at $150 or $200 per)Gross Margin at ~ 63% of Net SalesOperating Margin ~ 50% of Gross Margin
(Depending on R&D expense and co-marketing expenses).
EBITDA at 17-33% of Total (Depending on Operational Expenses)

• Equals all US hospital patients• 36M US inpatient hospitalizations per year• Average length of stay equals 5 days• Assuming $250 per patient yields $9B TAM
Total Addressable Market (TAM)
•ICU cases•4M cases per year @$250 each = $1B•Because ICU stays are much more expensive (>$10K per day) value-based pricing may yield higher revenue
Target Market
What We Learned from the Course
$ = The power to do good

Pro
duct
Lau
nch
2012
Clin
ical
M
ilest
ones
Start
Mile
ston
esR
egul
ator
y/ IP
M
ilest
ones
Q1 Q2 Q3 Q4
2013Q1 Q2 Q3 Q4
2014Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2015 2016
SystemSystem
2017Q1 Q2Q1 Q2 Q3 Q4
2018Q3
17 12/4/2009
Proof of Concept
Provisional Patent
Minimal Viable Product
Laboratory Prototype
Strategy
Continue Pilot Studies
FDA Submission & Clearance Post market activities
PUBS
SafetyTrials
PivotalTrials
Timeline
What we Learned Financial / Operations
$10M
$15M
Cas
h R
eser
ve
$5M
$20M Self funding Seed funding Series A funding Series B funding
8 US Patents & PCT counterpart
PUBS
CLIALDT
Pre-IDE IVD- Partnership PMA submission & approval



HospitalHospital pays MDflux based on procedure-specific CPT codeCPT 82544 =$185
Company Reimbursement
CMS & Private InsuranceCMS/Insurance pays the hospital based on condition-specific DRGActual $ amount varies by hospital
$185% of total per test

CONFIRM Source: FDA.gov
Pursuing pre-market approval (PMA) by:FDA Office of In Vitro Diagnostics (IVD) and Radiological Health (OIR)
Pathway through FDA RegulationsPre-Market Approval


















