

May 2008, Vol 1, No 4
66
MAY 2008 VOLUME 1, NUMBER 4 ©2008 Engage Healthcare Communications, LLC www.AHDBonline.com THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN ™ Avoiding the Unthinkable: A Tale of 2 Triangles and the Process of Care They Govern Robert E. Henry The Unbearable Lightness of Mental Health Alberto Colombi, MD, MPH Schizophrenia: Current Concepts and Approaches to Patient Care Peter F. Buckley, MD; Adriana Foster, MD Trends in Pharmaceutical Expenditures: The Impact on Drug Benefit Design Joanne LaFleur, PharmD, MSPH; Leslie Fish, PharmD; Diana I. Brixner, RPh, PhD Medicare Coverage for Erythropoiesis-Stimulating Agents: The Perfect Storm Interview (Part 1) with Samuel M. Silver, MD, PhD ◆ Generic Drug Trends ◆ AACR Meeting Highlights ◆ FDA Watch ◆ Industry Trends CLINICAL BUSINESS REGULATORY EDITORIAL DEPARTMENTS ™ AMCP COVERAGE
-
Upload
dalia-buffery -
Category
Documents
-
view
270 -
download
4
description
American Health & Drug Benefits
Transcript of May 2008, Vol 1, No 4
MAY 2008 VOLUME 1, NUMBER 4
©2008 Engage Healthcare Communications, LLCwww.AHDBonline.com
THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN™
Avoiding the Unthinkable: A Tale of 2 Triangles and the Process of CareThey GovernRobert E. Henry
The Unbearable Lightness of Mental Health Alberto Colombi, MD, MPH
Schizophrenia: Current Concepts and Approaches to Patient CarePeter F. Buckley, MD; Adriana Foster, MD
Trends in Pharmaceutical Expenditures: The Impact on Drug Benefit DesignJoanne LaFleur, PharmD, MSPH; Leslie Fish, PharmD; Diana I. Brixner, RPh, PhD
Medicare Coverage for Erythropoiesis-Stimulating Agents: The Perfect StormInterview (Part 1) with Samuel M. Silver, MD, PhD
� Generic Drug Trends� AACR Meeting Highlights� FDA Watch� Industry Trends
CLINICAL
BUSINESS
REGULATORY
EDITORIAL
DEPARTMENTS
™
AMCP
COVERAGE

Help patients in your plan benefit from always-there patient care
Important Safety InformationBoxed Warning: Congestive Heart Failure
• Thiazolidinediones (TZDs), including ACTOS, cause or exacerbate congestive heart failure (CHF) in some patients. After initiation of ACTOSand after dose increases, observe patients carefully for signs and symptoms of heart failure (including excessive rapid weight gain, dyspnea,and/or edema). If these signs and symptoms develop, the heart failure should be managed according to current standards of care. Furthermore,discontinuation or dose reduction of ACTOS must be considered.1 • ACTOS is not recommended in patients with symptomatic heart failure.Initiation of ACTOS in patients with established NYHA Class III or IV heart failure is contraindicated.1
Cardiac considerations: Like other TZDs, ACTOS can cause fluid retention when used alone or in combination with other antidiabetic agents,including insulin. Fluid retention may lead to or exacerbate CHF. ACTOS should be used with caution in patients at risk for heart failure. Patientsshould be monitored for symptoms of heart failure or other adverse events related to fluid retention. In clinical trials, a small number of patientswith a history of previously existing cardiac disease were reported to develop CHF when treated with ACTOS in combination with insulin. Reportsof CHF have been received in postmarketing experience in patients with and without previously known heart disease.1 Hepatic safety: Reports ofhepatitis and of hepatic enzyme elevations to three or more times the upper limit of normal (ULN) have been received in postmarketingexperience with pioglitazone. Very rarely, these reports have involved hepatic failure with or without fatal outcome, although causality has notbeen established. Liver enzymes, including serum ALT, should be evaluated in all patients at initiation of therapy with ACTOS, and periodicallythereafter per the clinical judgment of the healthcare professional. If ALT >2.5X ULN at baseline or if the patient exhibits clinical evidence of activeliver disease, do not initiate therapy with ACTOS.1 Other considerations: ACTOS may also be associated with hypoglycemia, edema, anemia,weight gain, and/or ovulation in premenopausal, anovulatory women. Adequate contraception should be recommended for premenopausalwomen. Macular edema has been reported in some diabetic patients receiving TZD therapy, although a causal relationship is unknown. Personswith diabetes should have routine eye exams and be instructed to immediately report any visual changes to their healthcare provider. Anincreased incidence of bone fracture was noted in female patients taking ACTOS. The risk of fracture should be considered in the care of patientstreated with ACTOS, particularly females, and attention should be given to assessing and maintaining bone health according to current standardsof care.1 Well-tolerated therapy: In US placebo-controlled ACTOS monotherapy clinical trials, the most common adverse events (e5%) wereupper respiratory tract infection, headache, sinusitis, myalgia, tooth disorder, aggravated diabetes mellitus, and pharyngitis.1 Indications andusage: ACTOS is indicated as an adjunct to diet and exercise to improve glycemic control in patients with type 2 diabetes. ACTOS is approved foruse as monotherapy and in combination with sulfonylureas, metformin, or insulin when diet and exercise plus the single agent do not result in adequate glycemic control.1 • ACTOS should not be used in patients with type 1 diabetes. Management of type 2 diabetes should also includenutritional counseling, weight reduction as needed, and exercise.1 • The major metabolic defects in type 2 diabetes are peripheral insulinresistance in muscle and fat, decreased pancreatic insulin secretion, and increased hepatic glucoseoutput.2 Dyslipidemia in insulin resistance is represented by hypertriglyceridemia, decreased HDLlevels, and increased small dense LDL particles.3 Renal and gastrointestinal function are also clinicalconsiderations when prescribing an oral agent for type 2 diabetes.4
Indicated as an adjunct to diet and exercise to improveglycemic control in adultpatients with type 2 diabetes.
Please see Brief Summary of Prescribing Information on adjacent page.
References: 1. ACTOS package insert, Takeda Pharmaceuticals America, Inc. 2. Schinner S, Scherbaum WA, Bornstein SR, Barthel A.Molecular mechanisms of insulin resistance. Diabet Med. 2005;22:674-682. 3. American Diabetes Association. Dyslipidemiamanagement in adults with diabetes. Diabetes Care. 2004;27(suppl 1):S68-S71. 4. American Diabetes Association. Standardsof medical care in diabetes–2007. Diabetes Care. 2007;30(suppl 1):S4-S41.
ACTOS®
(pioglitazone hydrochloride) Tablets
Brief Summary of Prescribing Information. Please see package insert for Complete Prescribing Information.
WARNING: CONGESTIVE HEART FAILURE
• Thiazolidinediones, including ACTOS, cause or exacerbate congestive heart failure in some patients (see
WARNINGS). After initiation of ACTOS, and after dose increases, observe patients carefully for signs and
symptoms of heart failure (including excessive, rapid weight gain, dyspnea, and/or edema). If these
signs and symptoms develop, the heart failure should be managed according to the current standards
of care. Furthermore, discontinuation or dose reduction of ACTOS must be considered.
• ACTOS is not recommended in patients with symptomatic heart failure. Initiation of ACTOS in patients with
established NYHA Class III or IV heart failure is contraindicated (see CONTRAINDICATIONS and WARNINGS).
INDICATIONS AND USAGE
ACTOS is indicated as an adjunct to diet and exercise to improve glycemic control in patients with type 2 diabetes
(non-insulin-dependent diabetes mellitus, NIDDM). ACTOS is indicated for monotherapy. ACTOS is also indicated
for use in combination with a sulfonylurea, metformin, or insulin when diet and exercise plus the single agent
do not result in adequate glycemic control.
Management of type 2 diabetes should also include nutritional counseling, weight reduction as needed, and
exercise. These efforts are important not only in the primary treatment of type 2 diabetes, but also to maintain
the efficacy of drug therapy.
CONTRAINDICATIONS
Initiation of ACTOS in patients with established New York Heart Association (NYHA) Class III or IV heart failure is
contraindicated (see BOXED WARNING).
ACTOS is contraindicated in patients with known hypersensitivity to this product or any of its components.
WARNINGS
Cardiac Failure and Other Cardiac Effects
ACTOS, like other thiazolidinediones, can cause fluid retention when used alone or in combination with other
antidiabetic agents, including insulin. Fluid retention may lead to or exacerbate heart failure. Patients should be
observed for signs and symptoms of heart failure. If these signs and symptoms develop, the heart failure should
be managed according to current standards of care. Furthermore, discontinuation or dose reduction of ACTOS
must be considered (see BOXED WARNING). Patients with NYHA Class III and IV cardiac status were not studied
during pre-approval clinical trials and ACTOS is not recommended in these patients (see BOXED WARNING and
CONTRAINDICATIONS).
In one 16-week, U.S. double-blind, placebo-controlled clinical trial involving 566 patients with type 2 diabetes,
ACTOS at doses of 15 mg and 30 mg in combination with insulin was compared to insulin therapy alone. This
trial included patients with long-standing diabetes and a high prevalence of pre-existing medical conditions as
follows: arterial hypertension (57.2%), peripheral neuropathy (22.6%), coronary heart disease (19.6%), retinopathy
(13.1%), myocardial infarction (8.8%), vascular disease (6.4%), angina pectoris (4.4%), stroke and/or transient
ischemic attack (4.1%), and congestive heart failure (2.3%).
In this study, two of the 191 patients receiving 15 mg ACTOS plus insulin (1.1%) and two of the 188 patients
receiving 30 mg ACTOS plus insulin (1.1%) developed congestive heart failure compared with none of the
187 patients on insulin therapy alone. All four of these patients had previous histories of cardiovascular
conditions including coronary artery disease, previous CABG procedures, and myocardial infarction. In a
24-week, dose-controlled study in which ACTOS was coadministered with insulin, 0.3% of patients (1/345) on
30 mg and 0.9% (3/345) of patients on 45 mg reported CHF as a serious adverse event.
Analysis of data from these studies did not identify specific factors that predict increased risk of congestive
heart failure on combination therapy with insulin.
In type 2 diabetes and congestive heart failure (systolic dysfunction)A 24-week post-marketing safety study was performed to compare ACTOS (n=262) to glyburide (n=256) in
uncontrolled diabetic patients (mean HbA1c 8.8% at baseline) with NYHA Class II and III heart failure and
ejection fraction less than 40% (mean EF 30% at baseline). Over the course of the study, overnight hospitalization
for congestive heart failure was reported in 9.9% of patients on ACTOS compared to 4.7% of patients on
glyburide with a treatment difference observed from 6 weeks. This adverse event associated with ACTOS was
more marked in patients using insulin at baseline and in patients over 64 years of age. No difference in
cardiovascular mortality between the treatment groups was observed.
ACTOS should be initiated at the lowest approved dose if it is prescribed for patients with type 2 diabetes and
systolic heart failure (NYHA Class II). If subsequent dose escalation is necessary, the dose should be increased
gradually only after several months of treatment with careful monitoring for weight gain, edema, or signs and
symptoms of CHF exacerbation.
Prospective Pioglitazone Clinical Trial In Macrovascular Events (PROactive)In PROactive, 5238 patients with type 2 diabetes and a prior history of macrovascular disease were treated with
ACTOS (n=2605), force-titrated up to 45 mg once daily, or placebo (n=2633) (see ADVERSE REACTIONS). The
percentage of patients who had an event of serious heart failure was higher for patients treated with ACTOS
(5.7%, n=149) than for patients treated with placebo (4.1%, n=108). The incidence of death subsequent to a
report of serious heart failure was 1.5% (n=40) in patients treated with ACTOS and 1.4% (n=37) in placebo-
treated patients. In patients treated with an insulin-containing regimen at baseline, the incidence of serious
heart failure was 6.3% (n=54/864) with ACTOS and 5.2% (n=47/896) with placebo. For those patients treated
with a sulfonylurea-containing regimen at baseline, the incidence of serious heart failure was 5.8%
(n=94/1624) with ACTOS and 4.4% (n=71/1626) with placebo.
PRECAUTIONS
General
ACTOS exerts its antihyperglycemic effect only in the presence of insulin. Therefore, ACTOS should not be used
in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis.
Hypoglycemia: Patients receiving ACTOS in combination with insulin or oral hypoglycemic agents may be at risk
for hypoglycemia, and a reduction in the dose of the concomitant agent may be necessary.
Cardiovascular: In U.S. placebo-controlled clinical trials that excluded patients with New York Heart Association
(NYHA) Class III and IV cardiac status, the incidence of serious cardiac adverse events related to volume expansion
was not increased in patients treated with ACTOS as monotherapy or in combination with sulfonylureas or
metformin vs. placebo-treated patients. In insulin combination studies, a small number of patients with a history
of previously existing cardiac disease developed congestive heart failure when treated with ACTOS in combination
with insulin (see WARNINGS). Patients with NYHA Class III and IV cardiac status were not studied in these
ACTOS clinical trials. ACTOS is not indicated in patients with NYHA Class III or IV cardiac status.
In postmarketing experience with ACTOS, cases of congestive heart failure have been reported in patients
both with and without previously known heart disease.
Edema: ACTOS should be used with caution in patients with edema. In all U.S. clinical trials, edema was reported
more frequently in patients treated with ACTOS than in placebo-treated patients and appears to be dose related
(see ADVERSE REACTIONS). In postmarketing experience, reports of initiation or worsening of edema have
been received. Since thiazolidinediones, including ACTOS, can cause fluid retention, which can exacerbate or
lead to congestive heart failure, ACTOS should be used with caution in patients at risk for heart failure. Patients
should be monitored for signs and symptoms of heart failure (see BOXED WARNING, WARNINGS, and
PRECAUTIONS, Information for Patients).
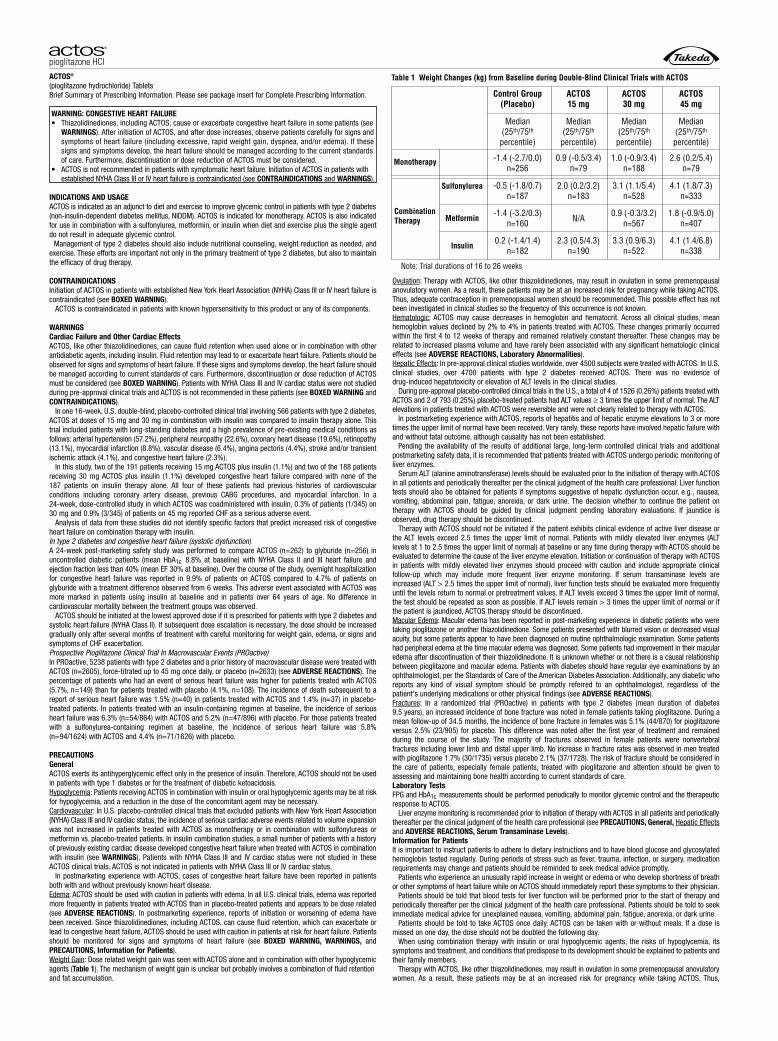
Weight Gain: Dose related weight gain was seen with ACTOS alone and in combination with other hypoglycemic
agents (Table 1). The mechanism of weight gain is unclear but probably involves a combination of fluid retention
and fat accumulation.
Ovulation: Therapy with ACTOS, like other thiazolidinediones, may result in ovulation in some premenopausal
anovulatory women. As a result, these patients may be at an increased risk for pregnancy while taking ACTOS.
Thus, adequate contraception in premenopausal women should be recommended. This possible effect has not
been investigated in clinical studies so the frequency of this occurrence is not known.
Hematologic: ACTOS may cause decreases in hemoglobin and hematocrit. Across all clinical studies, mean
hemoglobin values declined by 2% to 4% in patients treated with ACTOS. These changes primarily occurred
within the first 4 to 12 weeks of therapy and remained relatively constant thereafter. These changes may be
related to increased plasma volume and have rarely been associated with any significant hematologic clinical
effects (see ADVERSE REACTIONS, Laboratory Abnormalities).
Hepatic Effects: In pre-approval clinical studies worldwide, over 4500 subjects were treated with ACTOS. In U.S.
clinical studies, over 4700 patients with type 2 diabetes received ACTOS. There was no evidence of
drug-induced hepatotoxicity or elevation of ALT levels in the clinical studies.
During pre-approval placebo-controlled clinical trials in the U.S., a total of 4 of 1526 (0.26%) patients treated with
ACTOS and 2 of 793 (0.25%) placebo-treated patients had ALT values e 3 times the upper limit of normal. The ALT
elevations in patients treated with ACTOS were reversible and were not clearly related to therapy with ACTOS.
In postmarketing experience with ACTOS, reports of hepatitis and of hepatic enzyme elevations to 3 or more
times the upper limit of normal have been received. Very rarely, these reports have involved hepatic failure with
and without fatal outcome, although causality has not been established.
Pending the availability of the results of additional large, long-term controlled clinical trials and additional
postmarketing safety data, it is recommended that patients treated with ACTOS undergo periodic monitoring of
liver enzymes.
Serum ALT (alanine aminotransferase) levels should be evaluated prior to the initiation of therapy with ACTOS
in all patients and periodically thereafter per the clinical judgment of the health care professional. Liver function
tests should also be obtained for patients if symptoms suggestive of hepatic dysfunction occur, e.g., nausea,
vomiting, abdominal pain, fatigue, anorexia, or dark urine. The decision whether to continue the patient on
therapy with ACTOS should be guided by clinical judgment pending laboratory evaluations. If jaundice is
observed, drug therapy should be discontinued.
Therapy with ACTOS should not be initiated if the patient exhibits clinical evidence of active liver disease or
the ALT levels exceed 2.5 times the upper limit of normal. Patients with mildly elevated liver enzymes (ALT
levels at 1 to 2.5 times the upper limit of normal) at baseline or any time during therapy with ACTOS should be
evaluated to determine the cause of the liver enzyme elevation. Initiation or continuation of therapy with ACTOS
in patients with mildly elevated liver enzymes should proceed with caution and include appropriate clinical
follow-up which may include more frequent liver enzyme monitoring. If serum transaminase levels are
increased (ALT > 2.5 times the upper limit of normal), liver function tests should be evaluated more frequently
until the levels return to normal or pretreatment values. If ALT levels exceed 3 times the upper limit of normal,
the test should be repeated as soon as possible. If ALT levels remain > 3 times the upper limit of normal or if
the patient is jaundiced, ACTOS therapy should be discontinued.
Macular Edema: Macular edema has been reported in post-marketing experience in diabetic patients who were
taking pioglitazone or another thiazolidinedione. Some patients presented with blurred vision or decreased visual
acuity, but some patients appear to have been diagnosed on routine ophthalmologic examination. Some patients
had peripheral edema at the time macular edema was diagnosed. Some patients had improvement in their macular
edema after discontinuation of their thiazolidinedione. It is unknown whether or not there is a causal relationship
between pioglitazone and macular edema. Patients with diabetes should have regular eye examinations by an
ophthalmologist, per the Standards of Care of the American Diabetes Association. Additionally, any diabetic who
reports any kind of visual symptom should be promptly referred to an ophthalmologist, regardless of the
patient's underlying medications or other physical findings (see ADVERSE REACTIONS).
Fractures: In a randomized trial (PROactive) in patients with type 2 diabetes (mean duration of diabetes
9.5 years), an increased incidence of bone fracture was noted in female patients taking pioglitazone. During a
mean follow-up of 34.5 months, the incidence of bone fracture in females was 5.1% (44/870) for pioglitazone
versus 2.5% (23/905) for placebo. This difference was noted after the first year of treatment and remained
during the course of the study. The majority of fractures observed in female patients were nonvertebral
fractures including lower limb and distal upper limb. No increase in fracture rates was observed in men treated
with pioglitazone 1.7% (30/1735) versus placebo 2.1% (37/1728). The risk of fracture should be considered in
the care of patients, especially female patients, treated with pioglitazone and attention should be given to
assessing and maintaining bone health according to current standards of care.
Laboratory Tests
FPG and HbA1c measurements should be performed periodically to monitor glycemic control and the therapeutic
response to ACTOS.
Liver enzyme monitoring is recommended prior to initiation of therapy with ACTOS in all patients and periodically
thereafter per the clinical judgment of the health care professional (see PRECAUTIONS, General, Hepatic Effects
and ADVERSE REACTIONS, Serum Transaminase Levels).
Information for Patients
It is important to instruct patients to adhere to dietary instructions and to have blood glucose and glycosylated
hemoglobin tested regularly. During periods of stress such as fever, trauma, infection, or surgery, medication
requirements may change and patients should be reminded to seek medical advice promptly.
Patients who experience an unusually rapid increase in weight or edema or who develop shortness of breath
or other symptoms of heart failure while on ACTOS should immediately report these symptoms to their physician.
Patients should be told that blood tests for liver function will be performed prior to the start of therapy and
periodically thereafter per the clinical judgment of the health care professional. Patients should be told to seek
immediate medical advice for unexplained nausea, vomiting, abdominal pain, fatigue, anorexia, or dark urine.
Patients should be told to take ACTOS once daily. ACTOS can be taken with or without meals. If a dose is
missed on one day, the dose should not be doubled the following day.
When using combination therapy with insulin or oral hypoglycemic agents, the risks of hypoglycemia, its
symptoms and treatment, and conditions that predispose to its development should be explained to patients and
their family members.
Therapy with ACTOS, like other thiazolidinediones, may result in ovulation in some premenopausal anovulatory
women. As a result, these patients may be at an increased risk for pregnancy while taking ACTOS. Thus,
Table 1 Weight Changes (kg) from Baseline during Double-Blind Clinical Trials with ACTOS
Note: Trial durations of 16 to 26 weeks
Control Group(Placebo)
Median(25th/75th
percentile)
-1.4 (-2.7/0.0)n=256
-0.5 (-1.8/0.7)n=187
0.9 (-0.5/3.4)n=79
2.0 (0.2/3.2)n=183
3.1 (1.1/5.4)n=528
4.1 (1.8/7.3)n=333
0.9 (-0.3/3.2)n=567
1.8 (-0.9/5.0)n=407
3.3 (0.9/6.3)n=522
4.1 (1.4/6.8)n=338
N/A
2.3 (0.5/4.3)n=190
1.0 (-0.9/3.4)n=188
2.6 (0.2/5.4)n=79
Median(25th/75th
percentile)
Median(25th/75th
percentile)
Median(25th/75th
percentile)
ACTOS15 mg
ACTOS30 mg
ACTOS45 mg
Monotherapy
Sulfonylurea
-1.4 (-3.2/0.3)n=160
Metformin
0.2 (-1.4/1.4)n=182
Insulin
CombinationTherapy
©1999, 2008 Takeda Pharmaceuticals North America, Inc. PIO-00538 1/08 Printed in U.S.A.
adequate contraception in premenopausal women should be recommended. This possible effect has not been
investigated in clinical studies so the frequency of this occurrence is not known.
Drug Interactions
In vivo drug-drug interaction studies have suggested that pioglitazone may be a weak inducer of CYP 450 isoform
3A4 substrate.
An enzyme inhibitor of CYP2C8 (such as gemfibrozil) may significantly increase the AUC of pioglitazone and
an enzyme inducer of CYP2C8 (such as rifampin) may significantly decrease the AUC of pioglitazone. Therefore,
if an inhibitor or inducer of CYP2C8 is started or stopped during treatment with pioglitazone, changes in dia-
betes treatment may be needed based on clinical response.
Carcinogenesis, Mutagenesis, Impairment of Fertility
A two-year carcinogenicity study was conducted in male and female rats at oral doses up to 63 mg/kg (approximately
14 times the maximum recommended human oral dose of 45 mg based on mg/m2). Drug-induced tumors were not
observed in any organ except for the urinary bladder. Benign and/or malignant transitional cell neoplasms were
observed in male rats at 4 mg/kg/day and above (approximately equal to the maximum recommended human oral
dose based on mg/m2). A two-year carcinogenicity study was conducted in male and female mice at oral doses up
to 100 mg/kg/day (approximately 11 times the maximum recommended human oral dose based on mg/m2).
No drug-induced tumors were observed in any organ.
During prospective evaluation of urinary cytology involving more than 1800 patients receiving ACTOS in
clinical trials up to one year in duration, no new cases of bladder tumors were identified. In two 3-year studies
in which pioglitazone was compared to placebo or glyburide, there were 16/3656 (0.44%) reports of bladder
cancer in patients taking pioglitazone compared to 5/3679 (0.14%) in patients not taking pioglitazone. After
excluding patients in whom exposure to study drug was less than one year at the time of diagnosis of bladder
cancer, there were six (0.16%) cases on pioglitazone and two (0.05%) on placebo.
Pioglitazone HCl was not mutagenic in a battery of genetic toxicology studies, including the Ames bacterial
assay, a mammalian cell forward gene mutation assay (CHO/HPRT and AS52/XPRT), an in vitro cytogenetics
assay using CHL cells, an unscheduled DNA synthesis assay, and an in vivo micronucleus assay.
No adverse effects upon fertility were observed in male and female rats at oral doses up to 40 mg/kg pioglitazone
HCl daily prior to and throughout mating and gestation (approximately 9 times the maximum recommended
human oral dose based on mg/m2).
Animal Toxicology
Heart enlargement has been observed in mice (100 mg/kg), rats (4 mg/kg and above) and dogs (3 mg/kg) treated
orally with pioglitazone HCl (approximately 11, 1, and 2 times the maximum recommended human oral dose for
mice, rats, and dogs, respectively, based on mg/m2). In a one-year rat study, drug-related early death due to
apparent heart dysfunction occurred at an oral dose of 160 mg/kg/day (approximately 35 times the maximum
recommended human oral dose based on mg/m2). Heart enlargement was seen in a 13-week study in monkeys
at oral doses of 8.9 mg/kg and above (approximately 4 times the maximum recommended human oral dose
based on mg/m2), but not in a 52-week study at oral doses up to 32 mg/kg (approximately 13 times the maximum
recommended human oral dose based on mg/m2).
Pregnancy
Pregnancy Category C. Pioglitazone was not teratogenic in rats at oral doses up to 80 mg/kg or in rabbits given
up to 160 mg/kg during organogenesis (approximately 17 and 40 times the maximum recommended human
oral dose based on mg/m2, respectively). Delayed parturition and embryotoxicity (as evidenced by increased
postimplantation losses, delayed development and reduced fetal weights) were observed in rats at oral doses
of 40 mg/kg/day and above (approximately 10 times the maximum recommended human oral dose based on
mg/m2). No functional or behavioral toxicity was observed in offspring of rats. In rabbits, embryotoxicity was
observed at an oral dose of 160 mg/kg (approximately 40 times the maximum recommended human oral dose
based on mg/m2). Delayed postnatal development, attributed to decreased body weight, was observed in
offspring of rats at oral doses of 10 mg/kg and above during late gestation and lactation periods (approximately
2 times the maximum recommended human oral dose based on mg/m2).
There are no adequate and well-controlled studies in pregnant women. ACTOS should be used during pregnancy
only if the potential benefit justifies the potential risk to the fetus.
Because current information strongly suggests that abnormal blood glucose levels during pregnancy are
associated with a higher incidence of congenital anomalies, as well as increased neonatal morbidity and
mortality, most experts recommend that insulin be used during pregnancy to maintain blood glucose levels as
close to normal as possible.
Nursing Mothers
Pioglitazone is secreted in the milk of lactating rats. It is not known whether ACTOS is secreted in human milk.
Because many drugs are excreted in human milk, ACTOS should not be administered to a breastfeeding woman.
Pediatric Use
Safety and effectiveness of ACTOS in pediatric patients have not been established.
Elderly Use
Approximately 500 patients in placebo-controlled clinical trials of ACTOS were 65 and over. No significant
differences in effectiveness and safety were observed between these patients and younger patients.
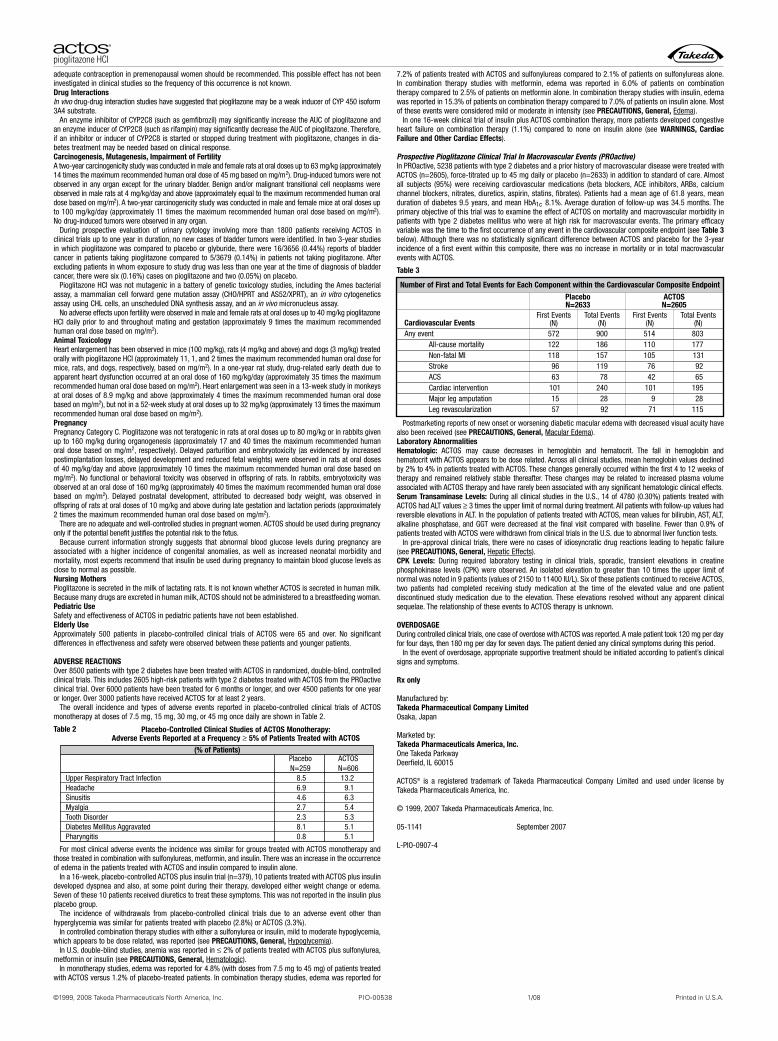
ADVERSE REACTIONS
Over 8500 patients with type 2 diabetes have been treated with ACTOS in randomized, double-blind, controlled
clinical trials. This includes 2605 high-risk patients with type 2 diabetes treated with ACTOS from the PROactive
clinical trial. Over 6000 patients have been treated for 6 months or longer, and over 4500 patients for one year
or longer. Over 3000 patients have received ACTOS for at least 2 years.
The overall incidence and types of adverse events reported in placebo-controlled clinical trials of ACTOS
monotherapy at doses of 7.5 mg, 15 mg, 30 mg, or 45 mg once daily are shown in Table 2.
Table 2
For most clinical adverse events the incidence was similar for groups treated with ACTOS monotherapy and
those treated in combination with sulfonylureas, metformin, and insulin. There was an increase in the occurrence
of edema in the patients treated with ACTOS and insulin compared to insulin alone.
In a 16-week, placebo-controlled ACTOS plus insulin trial (n=379), 10 patients treated with ACTOS plus insulin
developed dyspnea and also, at some point during their therapy, developed either weight change or edema.
Seven of these 10 patients received diuretics to treat these symptoms. This was not reported in the insulin plus
placebo group.
The incidence of withdrawals from placebo-controlled clinical trials due to an adverse event other than
hyperglycemia was similar for patients treated with placebo (2.8%) or ACTOS (3.3%).
In controlled combination therapy studies with either a sulfonylurea or insulin, mild to moderate hypoglycemia,
which appears to be dose related, was reported (see PRECAUTIONS, General, Hypoglycemia).
In U.S. double-blind studies, anemia was reported in � 2% of patients treated with ACTOS plus sulfonylurea,
metformin or insulin (see PRECAUTIONS, General, Hematologic).
In monotherapy studies, edema was reported for 4.8% (with doses from 7.5 mg to 45 mg) of patients treated
with ACTOS versus 1.2% of placebo-treated patients. In combination therapy studies, edema was reported for
7.2% of patients treated with ACTOS and sulfonylureas compared to 2.1% of patients on sulfonylureas alone.
In combination therapy studies with metformin, edema was reported in 6.0% of patients on combination
therapy compared to 2.5% of patients on metformin alone. In combination therapy studies with insulin, edema
was reported in 15.3% of patients on combination therapy compared to 7.0% of patients on insulin alone. Most
of these events were considered mild or moderate in intensity (see PRECAUTIONS, General, Edema).
In one 16-week clinical trial of insulin plus ACTOS combination therapy, more patients developed congestive
heart failure on combination therapy (1.1%) compared to none on insulin alone (see WARNINGS, Cardiac
Failure and Other Cardiac Effects).
Prospective Pioglitazone Clinical Trial In Macrovascular Events (PROactive)In PROactive, 5238 patients with type 2 diabetes and a prior history of macrovascular disease were treated with
ACTOS (n=2605), force-titrated up to 45 mg daily or placebo (n=2633) in addition to standard of care. Almost
all subjects (95%) were receiving cardiovascular medications (beta blockers, ACE inhibitors, ARBs, calcium
channel blockers, nitrates, diuretics, aspirin, statins, fibrates). Patients had a mean age of 61.8 years, mean
duration of diabetes 9.5 years, and mean HbA1c 8.1%. Average duration of follow-up was 34.5 months. The
primary objective of this trial was to examine the effect of ACTOS on mortality and macrovascular morbidity in
patients with type 2 diabetes mellitus who were at high risk for macrovascular events. The primary efficacy
variable was the time to the first occurrence of any event in the cardiovascular composite endpoint (see Table 3
below). Although there was no statistically significant difference between ACTOS and placebo for the 3-year
incidence of a first event within this composite, there was no increase in mortality or in total macrovascular
events with ACTOS.
Table 3
Postmarketing reports of new onset or worsening diabetic macular edema with decreased visual acuity have
also been received (see PRECAUTIONS, General, Macular Edema).
Laboratory Abnormalities
Hematologic: ACTOS may cause decreases in hemoglobin and hematocrit. The fall in hemoglobin and
hematocrit with ACTOS appears to be dose related. Across all clinical studies, mean hemoglobin values declined
by 2% to 4% in patients treated with ACTOS. These changes generally occurred within the first 4 to 12 weeks of
therapy and remained relatively stable thereafter. These changes may be related to increased plasma volume
associated with ACTOS therapy and have rarely been associated with any significant hematologic clinical effects.
Serum Transaminase Levels: During all clinical studies in the U.S., 14 of 4780 (0.30%) patients treated with
ACTOS had ALT values e 3 times the upper limit of normal during treatment. All patients with follow-up values had
reversible elevations in ALT. In the population of patients treated with ACTOS, mean values for bilirubin, AST, ALT,
alkaline phosphatase, and GGT were decreased at the final visit compared with baseline. Fewer than 0.9% of
patients treated with ACTOS were withdrawn from clinical trials in the U.S. due to abnormal liver function tests.
In pre-approval clinical trials, there were no cases of idiosyncratic drug reactions leading to hepatic failure
(see PRECAUTIONS, General, Hepatic Effects).
CPK Levels: During required laboratory testing in clinical trials, sporadic, transient elevations in creatine
phosphokinase levels (CPK) were observed. An isolated elevation to greater than 10 times the upper limit of
normal was noted in 9 patients (values of 2150 to 11400 IU/L). Six of these patients continued to receive ACTOS,
two patients had completed receiving study medication at the time of the elevated value and one patient
discontinued study medication due to the elevation. These elevations resolved without any apparent clinical
sequelae. The relationship of these events to ACTOS therapy is unknown.
OVERDOSAGE
During controlled clinical trials, one case of overdose with ACTOS was reported. A male patient took 120 mg per day
for four days, then 180 mg per day for seven days. The patient denied any clinical symptoms during this period.
In the event of overdosage, appropriate supportive treatment should be initiated according to patient’s clinical
signs and symptoms.
Rx only
Manufactured by:
Takeda Pharmaceutical Company Limited
Osaka, Japan
Marketed by:
Takeda Pharmaceuticals America, Inc.
One Takeda Parkway
Deerfield, IL 60015
ACTOS® is a registered trademark of Takeda Pharmaceutical Company Limited and used under license by
Takeda Pharmaceuticals America, Inc.
© 1999, 2007 Takeda Pharmaceuticals America, Inc.
05-1141 September 2007
L-PIO-0907-4
(% of Patients)Placebo ACTOS
N=259 N=606
Upper Respiratory Tract Infection 8.5 13.2
Headache 6.9 9.1
Sinusitis 4.6 6.3
Myalgia 2.7 5.4
Tooth Disorder 2.3 5.3
Diabetes Mellitus Aggravated 8.1 5.1
Pharyngitis 0.8 5.1
Placebo-Controlled Clinical Studies of ACTOS Monotherapy: Adverse Events Reported at a Frequency e 5% of Patients Treated with ACTOS
Number of First and Total Events for Each Component within the Cardiovascular Composite Endpoint
PlaceboN=2633
ACTOSN=2605
Cardiovascular Events
Any event
All-cause mortality
Non-fatal MI
Stroke
ACS
Cardiac intervention
Major leg amputation
Leg revascularization
First Events(N)
First Events(N)
Total Events(N)
Total Events(N)
572
122
118
96
63
101
15
57
900 514 803
186 110 177
157 105 131
119 76 92
78 42 65
240 101 195
28 9 28
92 71 115

3www.AHDBonline.com
LETTER FROM THE EDITOR
Last month, 2 back-to-back meetingsbrought out some of the leadersdriving the transformation of health -
care into a value-based, patient-centeredsystem. The Academy of Managed CarePharmacy (AMCP) went first, celebratingits 20th anniversary, followed by the 5thAnnual World Health Care Congress(WHCC). Both sessions revealed just howdifferent, and better, healthcare is becom-ing. Even the warnings about the catastrophic conse-quences of not improving our healthcare system wereaccompanied by numerous remedies for it. Said onespeaker, “If you can’t imagine things getting that bad,they probably won’t.”
There is some truth to this. In the face of improvedevidence gathering, analysis, and application, it is get-ting harder to sit back and watch healthcare inefficien-cies—clinical or economic—get bad. There are simplytoo many constructive remedies being proposed. Weoutline some of the advances proposed at the AMCPmeeting in this issue of American Health & DrugBenefits (AHDB). Evidence-based medicine is finallymaking its appearance in value-based benefit designs.Data-gathering techniques are improving to the pointwhere healthcare providers and managers can track theeffects of shifts in formularies and benefit designs.Patient adherence is finally moving from a pipe dreamto a hard metric, fortified by a dizzying array of payor-generated tactics keeping patients connected withhealth “coaches.”
This is not your father’s healthcare system.And so, because reasonable people are seeing real
data showing what will happen to healthcare costs andoutcomes if new efficiencies are not instilled into thepractices of every stakeholder—from patient to pro -vider, payor to purchaser, manufacturer to regulatory—it is becoming sensible to conclude that things are notgoing to get that bad. We are not going to spend anunsupportable proportion of the US gross nationalproduct on healthcare midway through the century.We are not going to continue spending twice as muchfor identical healthcare outcomes in Miami as we do inMinnesota. And we will not apply population-baseddata on all patients as if everyone were an averagepatient. People are rational beings and, when con-
fronted by the unthinkable, will alter theircourse, not freeze like so many deer caughtin the headlights of spiraling costs andintractable local customs.
As we witness the transformation ofhealthcare from expert-based opinion toevidence-based, value-based, patient-cen-tered care, it becomes apparent that whileprocesses are changing, the principles thatsupport them are constant. The new
research presented at the 2 conferences locks in on theeternal triangle of value: cost, quality, and access. Sosaid Dr David Brailer, health information technology(HIT) expert, at his AMCP presentation. It is the bal-ancing of these 3 interlocking forces that drives value.
AHDB organizes information on the basis of thisand a second triangle: clinical, business, and regulato-ry. When value propositions are defined by a givenhealthcare intervention, that product or service mustbe delivered through formulary and benefit designs thatsatisfy a similar balance of clinical, business, and regu-latory criteria. Circumstances and resources are indynamic flux, but healthcare resource allocation isdriven by these unchanging principles.
At these meetings, presentations revealed stunningnew opportunities for value, with quality of researchthat was unthinkable even 5 years ago, and the trendcan be expected to continue indefinitely. Observa -tional data and HIT supplying it are bringing thepromise of evidence-based medicine to formulary andbenefit designs. Data were presented showing the dif-ferences in adherence rates across a range of medica-tions used for the same condition, and the differentoverall healthcare resources consumed by the differentpatient groups. The ability to track patient adherence,outcomes, and health care resource allocation withsuch granularity is making health benefits able to servethe patient and the healthcare system alike, empower-ing all stakeholders to know exponentially more aboutthe impact of healthcare interventions than was everpossible. This is good news for those caught in theglare of the headlights warning that spiraling health-care costs were about to overrun the entire system andeffectively wipe it out.
But back to that persistent value triangle of cost, qual-ity, and access: the impending “collision” is not just with
Avoiding the Unthinkable: A Tale of 2 Trianglesand the Process of Care They Govern

4 AMERICAN HEALTH & DRUG BENEFITS May 2008
LETTER FROM THE EDITOR
undesirable healthcare costs, but also with substandardquality of care and access to it. The new systems for gath-ering and analyzing data on the quality of care and theadherence (access) to treatment regimens are integral fordelivering best practices at best costs. Researchers areable to assign cost values to failing to provide optimaldrugs or devices or to perform appropriate diagnostictests. They can assess the impact on healthcare resourceutilization of poor patient adherence to optimal treat-ment regimens. The sentiment is old—C. Everett Coop’s
admonition that the least effective drug is the one nevertaken—but the ability to assign outcome metrics to it isnew, empowering all stakeholders to do something aboutit. This technology is not getting rid of expert opinionbut rather empowering experts to produce an evidence-based paradigm, armed with better facts than was everpossible before. Data are never self-explanatory, butexpert analysis will help unravel the huge disparities intreatment costs and outcomes of patients in differentparts of the United States—even in different areas of thestate of New Jersey, as Dr Uwe Reinhardt reported at therecent WHCC.
Thus, the quality of the Great Healthcare Debate onwhat benefits should be covered, and how, is increas-ing. Doomsday “chic” one hopes is on its way out,progress on its way in, as researchers replace a cost-cen-tered approach to managing spiraling costs with avalue-based approach: the cost-quality-access triangle.By putting these elements first—by putting thepatients’ needs, even the individual patient’s needs,first—costs will become manageable. Runaway health-care costs back in the 1990s were addressed by theHMO strategy, “just say low.” This cost-minimization,race-to-the-bottom strategy did not resonate withpatients or their providers. Evidence-based medicine
then began to emerge, but only as a gauge of clinicalquality. It became necessary to complete the triangula-tion of forces—cost, quality, access—by linking empir-ical quality care with access to care. This guides payorsand purchasers alike on the truly acceptable opportuni-ties to rein-in costs. Just how those models will takeshape is yet unknown. What is likely is that they willbe realistic, and that outcomes, health and economic,will be verifiable.
At the end of this scenario is the integration of stake-holder activities and agendas. Each party to the processof care is vitally interested in protecting its interests:patients, providers, payors, purchasers, manufacturers,regulatory, political, academia, evaluators, distributors,investors. Aligning the incentives of this multilateralgroup will require a collegial spirit currently absent fromthe Great Healthcare Debate. The quality of evidence-based outcomes should help make meaningful trans-parency possible, along with the redefining of responsi-bilities of each stakeholder group to the others, alwaysin support of the patient, the patient, the patient. Thefate of the 21st-century patient—which ultimately isus—will be determined in a more informed healthcareenvironment than ever existed.
The vitality of ideas expressed at this year’s health-care meetings and in the pages of this journal providesevidence of a resourcefulness that has never left health-care. For a time, the rush to progress seems drowned outby the glare of those frightful headlights warning ofimminent doom. But the unthinkable is providingample incentive to sidestep it. Experts are coming for-ward with propositions and systems for achievinghealthcare progress never before imagined, and withresults that are already taking root in our emerging newsystem of care. It is a good time to be alive, and becauseit is human nature not to accept the unthinkable, bet-ter times lie ahead. �
Robert E. HenryEditor-in-Chief
For editorial queries and submissions, please [email protected].
The quality of evidence-based outcomes shouldhelp make meaningful transparency possible,along with the redefining of responsibilities ofeach stakeholder group to the others, always insupport of the patient, the patient, the patient.
Open Access. Because different people
have different needs.
Bristol-Myers Squibb supports open and unrestricted access to mental health medications. For people with mental illness, having access to newer and potentially more effective medications can be a crucial component of treatment.
1 in 4 adults suffer from a diagnosable mental disorder
in any given year.1
Open access is especially important in the treatment of mental disorders because the response to therapy can vary greatly from individual to individual and from one medication to the next. Restrictions in the form of prior authorizations and preferred lists may have the unintended consequences of jeopardizing patient health while failing to reduce costs.
SUPPORT OPEN ACCESS AND GIVE PROVIDERS THE FREEDOM TO FIND THE MOST APPROPRIATE MEDICATION FOR EACH INDIVIDUAL.
1. National Institute of Mental Health. Available at: http://www.nimh.nih.gov/healthinformation/statisticsmenu.cfm. Accessed August 7, 2006.
D6-K0176Q October 2006 AA444678/10-06
,ISA�$OW������������������������
������������
0ETER�$RESSLER������������������������������
,AURA�$UCHARME���������������������������������������������������������������������������������������������
�����������������������
4ODD�$UNZELLO�������������������������
3COTT�$URFEE���������������������������������������������������������
�����������������������
+ATIE�%STEVES��������������������������������
���������������
#HARLES�%VANS����������������������
!URA�&ONG���������������������������������������������������������
THE MEDICATION PRESCRIBED FOR LAURA
MAY NOT WORK FOR SCOTT.

6 AMERICAN HEALTH & DRUG BENEFITS May 2008 www.AHDBonline.com
3 Avoiding the Unthinkable: A Tale of 2 Triangles and the Process of Care They GovernRobert E. Henry
10 The Unbearable Lightness of Mental Health Alberto Colombi, MD, MPH
50 Correction
13 Schizophrenia: Current Concepts and Approaches to Patient CarePeter F. Buckley, MD; Adriana Foster, MD
29 Trends in Pharmaceutical Expenditures: The Impact on Drug Benefit DesignJoanne LaFleur, PharmD, MSPH; Leslie Fish, PharmD; Diana I. Brixner, RPh, PhD
46 Medicare Coverage for Erythropoiesis-Stimulating Agents: The Perfect StormInterview (Part 1) with Samuel M. Silver, MD, PhD
Continued on page 8
MAY 2008 VOLUME 1, NUMBER 4
BUSINESS
EDITORIAL
REGULATORY
™ ™
PublisherNicholas [email protected]
Associate PublisherMaurice [email protected]
Editorial DirectorDalia [email protected]
Contributing EditorSandy Paton
Senior Production ManagerAlaina Pede
Director of Human ResourcesBlanche Marchitto
PresidentBrian F. [email protected]
Editor-in-ChiefRobert E. [email protected]
American Health & Drug Benefits is found-ed on the concept that health and drugbenefits have undergone a transforma-tion: the econometric value of a drug is ofequal importance to clinical outcomes asit is to serving as the basis for securingcoverage in formularies and drug benefitdesigns. Benefit designs are greatly affect-ed by numerous clinical, business, andpolicy conditions.
This publication provides benefit designdecision makers the integrated industryinformation they require to devise formu-laries and drug benefit designs that standup to today’s special healthcare deliveryand business needs.
Contact Information:For reprints, subscription information, andeditorial queries, please contact:[email protected]
Mission Statement
CLINICAL
AMCP COVERAGE
38 Economic Trends Influencing Healthcare ReformKeynote address delivered by Robert B. Reich
40 Technology in Healthcare: The Wave of the FuturePresented by David Brailer, MD, PhD
42 Medication Therapy Management Project—The Latest Information for Managed Care PharmacyPresented by Marissa Schlaifer, RPh; Linda Baggett, RPh, CGP; and Kimberly Vernachio, PharmD
44 Responding to FDA Alerts: How to Reduce Risks and LiabilityPresented by Kathleen Orrico, PharmD

©2008 Abbott Laboratories Abbott Park, IL 60064 306-78502 March 2008 Printed in U.S.A.
Now Available
Please visit www.simcortablets.com

8 AMERICAN HEALTH & DRUG BENEFITS May 2008 www.AHDBonline.com
Clinical EditorThomas McCarter, MD, FACPChief Clinical OfficerExecutive Health Resources [email protected]
Business/Government EditorKip Piper, MA, CHEPresident, Health Results [email protected]
Editorial BoardPharmacy Reimbursement PolicyMichael R. Schaffer, PharmD, MBAArthur F. Shinn, PharmD, FASCP
EmployersF. Randy Vogenberg, RPh, PhDAlberto M. Colombi, MD, MPH
Specialty PharmacyRebecca M. Shanahan, Esq.
Managed Care Pharmacy PolicyCynthia J. Pigg, BSPharm, MHA
Managed Markets MarketingJeffrey A. Bourret, RPh, MS, FASHPCharles E. Collins, Jr, MS, MBA
Clinical ResearchNirav R. Shah, MD, MPHSamuel M. Silver, MD, PhDMichael A. Weber, MD
Managed Care & Government AffairsSharad Mansukani, MD
Research & DevelopmentMichael F. Murphy, MD, PhDWayne A. Rosenkrans, Jr, PhD
Healthcare OutcomesGary M. Owens, MD
Outcomes ResearchGordon M. Cummins, MSTimothy S. Regan, BPharm, RPh
Pharmacy & Specialty ProductsJames T. Kenney, RPh, MBA
Pharmacy Benefit DesignJoel V. Brill, MDScott R. Taylor, RPh, MBA
PharmacoeconomicsJeff Jianfei Guo, BPharm, MS, PhD
Policy & Public HealthAlex Hathaway, MD, MPH, FACPMJoseph R. Antos, PhD
ActuaryDavid Williams
24 Generic Drug TrendsGary M. Owens, MD
34 Information for Authors
52 AACR Meeting HighlightsBy Caroline Helwick
53 Letter
54 FDA WatchMark Senak, JD
56 Industry TrendsGordon M. Cummins, MS
59 Executive Summaries
MAY 2008 VOLUME 1, NUMBER 4
DEPARTMENTS
American Health & Drug Benefits, ISSN 1942-2962 (print); ISSN 1942-2970 (online), is published 9 times a year by Engage HealthcareCommunications, LLC, 241 Forsgate Drive, Suite 205B, Jamesburg, NJ 08831. Copyright © 2008 by Engage Healthcare Communications,LLC. All rights reserved. American Health & Drug Benefits and The Peer-Reviewed Forum for Evidence in Benefit Design are trademarks of EngageHealthcare Communications, LLC. No part of this publication may be reproduced or transmitted in any form or by any means now or here-after known, electronic or mechanical, including photocopy, recording, or any informational storage and retrieval system, without written per-mission from the Publisher. Printed in the United States of America. Address all editorial correspondence to: [email protected],Telephone: 732-992-1889. Fax: 732-992-1881. American Health & Drug Benefits, 241 Forsgate Drive, Suite 205B, Jamesburg, NJ 08831.
POSTMASTER: CORRESPONDENCE REGARDING SUBSCRIPTIONS OR CHANGE OF ADDRESS should be directed to CIRCU-LATION DIRECTOR, American Health & Drug Benefits, 241 Forsgate Drive, Suite 205B, Jamesburg, NJ 08831. Fax: 732-992-1881. YEAR-LY SUBSCRIPTION RATES: One year: $99.00 USD; Two years: $149.00 USD; Three years: $199.00 USD.
Permission requests to reprint all or part of any article published in this journal should be addressed to REPRINT PERMISSIONS DEPART-MENT, Engage Healthcare Communications LLC, 241 Forsgate Drive, Suite 205B, Jamesburg, NJ 08831. The ideas and opinions expressedin American Health & Drug Benefits do not necessarily reflect those of the Editorial Board, the Editors, or the Publisher. Publication of an adver-tisement or other product mentioned in American Health & Drug Benefits should not be construed as an endorsement of the product or themanufacturer’s claims. Readers are encouraged to contact the manufacturers about any features or limitations of products mentioned. Neitherthe Editors nor the Publisher assume any responsibility for any injury and/or damage to persons or property arising out of or related to any useof the material mentioned in this publication.
™ ™
26 58 60
UNMANAGED MOMENTS

The only complete line of strengths for dosing flexibility
Stock OXYCODONE HCI from Ethex today and be ready for prescription requests!
• Generically priced
• Supported by an awareness campaignto prescribers
• Patient Sample Vouchers, redeemable atthe pharmacy, offer a free trial of 10 mg or20 mg tablets (with a valid prescription,void where prohibited by law)
NDC 58177-625-04 5 mg 100’s
NDC 58177-625-11 5 mg 10x10 UD
NDC 58177-461-04 10 mg 100’s
NDC 58177-445-04 15 mg 100’s
NDC 58177-462-04 20 mg 100’s
NDC 58177-446-04 30 mg 100’s
For more information log on towww.ethex.com or call 1-888-567-9176.
10 AMERICAN HEALTH & DRUG BENEFITS May 2008
Is wellness just a physical matter? Is theburden of disease just a matter of costs?These are obviously rhetorical ques-
tions. No one would challenge the notionthat health is more than the absence of dis-ease and is at the very least a state of men-tal and physical well-being. But how oftendo we try to understand “mental wellness”?How often do we look into screening, diag-nosis, intervention, and referral of mentalissues in a fragmented mental healthcare system?
Similarly, no one would deny that the total burdenof disease on work and on society is more than just itsdirect healthcare cost. Most of us recognize that indi-rect healthcare costs should be factored in, and theseinclude absenteeism and presenteeism. Nevertheless,how often do we truly try to quantify health-related lossof function, hindered performance, and, ultimately,productivity loss? Compounding mental health andproductivity loss, how well do we do in weighing in theintangible loss of function associated with mental stressand disease?
From prevention to treatment, there is an unin-tended but actual difference in how matters of physi-cal and mental wellness are being addressed—one withempathy, the other with stigma. For instance, shouldan injury occur, a legion of good healthcare and safetycolleagues will investigate, intervene, and discuss cor-rective actions. Should a heart attack happen—a per-sonal matter, mind you—emergency response wouldbe activated, people trained in CPR would come for-ward, defibrillators would be made available, and well-ness teams would address risk prevention—from bloodpressure to cholesterol level—and, in the back end,coronary artery disease claims utilization and costswould be analyzed.
But what about stress or depression, let alone a fatalcase, as in suicide? A hallway murmur would followperhaps, but no one will ask: • Could it have been prevented? • Are our health programs adequate? • Did our wellness team raise awareness?
• Do we facilitate access to treatmentand to prevention of mental discomfortand disease?• Are our employee assistance programsproactive?
It is “personal,” we have no right “tointerfere,” and we do not mean to. Butwould you let a personal heart attack takeplace without questioning if the ambu-lance arrives on time? Without activating
the emergency response system, without even tryingCPR, and without questioning if appropriate cardio-vascular health-promotion programs are in place? Twopersonal matters that are nevertheless being treatedvery differently.
One argument for such disparity is that mentalhealth is light, evanescent, elusive. Even excluding thepersonal suffering, if we look at economic figures only,that alone should be a compelling reason to betterunderstand the whole “weight” of the issue.
Let us look at some preliminary figures. In our com-pany, during a period of 7 years or so, some 28,000employees filled out a self-reported Health RiskAssessment (HRA) Questionnaire online. Of these,about 19,000 were US employees, of whom about 1800voluntarily filled out the validated depression screen-ing instrument Patient Health Questionnaire (PHQ)-91
and responded to the Work Limitations Questionnaire(WLQ), which assesses limitations in performing nor-mal job functions that result from physical or emotion-al matters.2 The WLQ calculates a Productivity LossIndex and a Time Loss Index. The approximately 1800employees also completed a Stress Satisfaction OffsetScore, which explores demand, control, effort, andreward of their job situation.3
Thus unassumingly, imperfectly, and while attend-ing to the usual center-stage physical wellness charac-ters—cardiovascular disease, diabetes, and metabolicsyndrome prevention—we found ourselves looking at arespectable sample of our own employees who weresending us a message about mental wellness. Such amessage cannot be ignored—our own people telling usthat stress is the most important risk factor for them(69%), but the one which they are least ready tochange (11%), either because they are not interested in
The Unbearable Lightness of Mental Health Alberto Colombi, MD, MPH
GUEST EDITORIAL
Dr Colombi is Corporate Medical Director, PPG Industries,Inc, Pittsburgh, PA.
Continued on page 12

Healthcare may be a numbers game,
but we’re only interested in one number.
At Lilly, helping you manage your
patients requires a shared commitment to
delivering initiatives, ideas, and
positive outcomes. So we keep our focus
on those who count on our medicines.
From diabetes and mental health
education, to patient adherence efforts, to
simply offering the best answers we can,
Lilly is working towards one focus...
one patient at a time.
1happier,healthier, more compliantpatient
All numbers current as of December 2006. MG45572 COPYRIGHT © 2007 ELI LILLY AND COMPANY.
550thousand patients
enrolled in pharmacy
adherence programs
10medicines for
diabetes and
mental health

12 AMERICAN HEALTH & DRUG BENEFITS May 2008
GUEST EDITORIAL
change, or possibly because they do not believe thatchange is possible.
We are trained to interpret self-reported chronicconditions, predisease predictors, and lifestyle risk fac-tor stratification, but we are unprepared to readthrough a message about stress, let alone depression.We wonder what this all means: Is there an unrecog-nized issue of adapting organizations to human psy-chology—“orgonomics”—as much as there is a recog-nized need of adapting tools to human physiology, as intraditional ergonomics? While we wonder about orga-nizational stressors and the possibility of prevention,we also ask ourselves what will be the treatment expe-rience for those who might have screened positive forclinically relevant depression.
Although their triage ends with the recommenda-tion to consult with their personal physician—who isreally taking care of them, and how? What will be theirrehabilitation and early and safe return to work experi-ence in a fragmented healthcare system, where stigmafor mental disease does not facilitate early identifica-tion, screening, referral, and return to function?
Can we at least make the business case that mentalwellness deserves as much attention as physical well-ness does? Let us take another look at the productivityloss associated with these preliminary data.
Our company’s preliminary self-reported HRAdata show that besides the expected impact of aller-gies and bronchitis, stress and depression are ofutmost importance for preventing productivity loss.Stress is one of the most relevant factors for loss ofproductivity on a population basis. According to ourdata, about $2 million are estimated lost per 1000employees each year due to sub-par performanceresulting from what is defined as “stress.” These data
give equal importance to stress at work and at home,stress about parental care as much as about care foran elderly relative. Similarly, our data indicate thatdepression is another critical area for loss of engage-ment and productivity.
In addition, our data show that not only the fewsevere, untreated depression cases result in very highindividual productivity loss, but that the moderate andmild depression cases, which are more common, add upto the overall population burden of disease whenprevalence is considered. In fact, moderate and mildunaddressed depression may account for two thirds ofthe burden of depression on overall productivity loss.This, in our data, is estimated to translate to about $1million per 1000 employees annually. Accordingly, wewould estimate that each year, for every 1000 employ-ees, possibly $3 million is lost in absenteeism or pre-senteeism because of stress and depression combined.Even if these estimates need further critical refinement,this entire issue carries substantial weight on financialgrounds alone.
Let me conclude with the obvious: Economics is notthe only consideration. In the initial days of occupa-tional safety many decades ago, the seeds of good safe-ty programs were rooted in the moral unwillingness toaccept the “normalcy” of preventable disease, disabili-ty, and loss of life. Similarly, I am confident that men-tal well-being has to start with our nonacceptance ofstigma and avoidable, crippling disability—let aloneloss of life—from mental illness.
Although mental distress requires the respect thatis due to personal matters, it also deserves supportiveenvironments, relationships that respect employees’dignity, and practical ways of balancing work and life.Keeping employees healthy, productive, and engagedis arguably a good business proposition. And al -though mental health seems “soft,” its unbearablelightness does measure up in the ability of health togenerate wealth. �
References1. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a briefdepression measure. J Gen Intern Med. 2001;16:606-613.2. Lerner D, Amick BC III, Rogers WH, et al. The Work LimitationsQuestionnaire. Med Care. 2001;39:72-85. 3. Shain M. Stress Satisfaction Offset Score (SSOS): best advice onstress risk management in the workplace. 2000. Publication prepared forHealth Canada; available through Dr Martin Shain, at [email protected].
Keeping employees healthy, productive, and engaged is arguably a good businessproposition. And although mental healthseems “soft,” it does measure up in the ability of health to generate wealth.
Continued from page 10
2.5 mg, 5 mg and 10 mg Tablets
Brief Summary: For complete details please see full Prescribing Information for BYSTOLIC.
INDICATIONS AND USAGEBYSTOLIC is indicated for the treatment of hypertension. BYSTOLIC may be usedalone or in combination with other antihypertensive agents.
CONTRAINDICATIONSBYSTOLIC is contraindicated in patients with severe bradycardia, heart blockgreater than first degree, cardiogenic shock, decompensated cardiac failure, sicksinus syndrome (unless a permanent pacemaker is in place), or severe hepaticimpairment (Child-Pugh >B), and in patients who are hypersensitive to any compo-nent of this product.
WARNINGSAbrupt Cessation of Therapy Patients with coronary artery disease treated with BYSTOLIC should be advisedagainst abrupt discontinuation of therapy. Severe exacerbation of angina and theoccurrence of myocardial infarction and ventricular arrhythmias have been reportedin patients with coronary artery disease following the abrupt discontinuation of ther-apy with β-blockers. Myocardial infarction and ventricular arrhythmias may occurwith or without preceding exacerbation of the angina pectoris. Even patients withoutovert coronary artery disease should be cautioned against interruption or abrupt dis-continuation of therapy. As with other β-blockers, when discontinuation of BYSTOLICis planned, patients should be carefully observed and advised to minimize physicalactivity. BYSTOLIC should be tapered over 1 to 2 weeks when possible. If the anginaworsens or acute coronary insufficiency develops, it is recommended that BYSTOLICbe promptly reinstituted, at least temporarily.Cardiac FailureSympathetic stimulation is a vital component supporting circulatory function in thesetting of congestive heart failure, and β-blockade may result in further depression ofmyocardial contractility and precipitate more severe failure. In patients who havecompensated congestive heart failure, BYSTOLIC should be administered cautiously.If heart failure worsens, discontinuation of BYSTOLIC should be considered. Angina and Acute Myocardial InfarctionBYSTOLIC was not studied in patients with angina pectoris or who had a recent MI.Bronchospastic DiseasesIn general, patients with bronchospastic diseases should not receive β-blockers.Anesthesia and Major SurgeryIf BYSTOLIC is to be continued perioperatively, patients should be closely moni-tored when anesthetic agents which depress myocardial function, such as ether,cyclopropane, and trichloroethylene, are used. If β-blocking therapy is withdrawnprior to major surgery, the impaired ability of the heart to respond to reflex adren-ergic stimuli may augment the risks of general anesthesia and surgical procedures.The β-blocking effects of BYSTOLIC can be reversed by β-agonists, e.g., dobutamineor isoproterenol. However, such patients may be subject to protracted severehypotension. Additionally, difficulty in restarting and maintaining the heartbeat hasbeen reported with β-blockers.Diabetes and Hypoglycemiaβ-blockers may mask some of the manifestations of hypoglycemia, particularlytachycardia. Nonselective β-blockers may potentiate insulin-induced hypoglycemiaand delay recovery of serum glucose levels. It is not known whether nebivolol hasthese effects. Patients subject to spontaneous hypoglycemia, or diabetic patientsreceiving insulin or oral hypoglycemic agents, should be advised about these possibilities and nebivolol should be used with caution.Thyrotoxicosisβ-blockers may mask clinical signs of hyperthyroidism, such as tachycardia.Abrupt withdrawal of β-blockers may be followed by an exacerbation of the symp-toms of hyperthyroidism or may precipitate a thyroid storm.Peripheral Vascular Diseaseβ-blockers can precipitate or aggravate symptoms of arterial insufficiency in patientswith peripheral vascular disease. Caution should be exercised in these patients.Non-dihydropyridine Calcium Channel BlockersBecause of significant negative inotropic and chronotropic effects in patients treatedwith β-blockers and calcium channel blockers of the verapamil and diltiazem type,caution should be used in patients treated concomitantly with these agents and ECGand blood pressure should be monitored.
PRECAUTIONSUse with CYP2D6 inhibitorsNebivolol exposure increases with inhibition of CYP2D6 (see Drug Interactions).The dose of BYSTOLIC may need to be reduced.Impaired Renal FunctionBYSTOLIC should be used with caution in patients with severe renal impairmentbecause of decreased renal clearance. BYSTOLIC has not been studied in patientsreceiving dialysis.Impaired Hepatic FunctionBYSTOLIC should be used with caution in patients with moderate hepatic impair-ment because of decreased metabolism. Since BYSTOLIC has not been studied in patients with severe hepatic impairment, BYSTOLIC is contraindicated in thispopulation (see CLINICAL PHARMACOLOGY, Special Populations and DOSAGEAND ADMINISTRATION).Risk of Anaphylactic Reactions While taking β-blockers, patients with a history of severe anaphylactic reactions toa variety of allergens may be more reactive to repeated challenge either accidental,diagnostic, or therapeutic. Such patients may be unresponsive to the usual dosesof epinephrine used to treat allergic reactions.In patients with known or suspected pheochromocytoma, an alpha-blocker shouldbe initiated prior to the use of any β-blocker.Information for PatientsPatients should be advised to take BYSTOLIC regularly and continuously, as directed. BYSTOLIC can be taken with or without food. If a dose is missed, thepatient should take the next scheduled dose only (without doubling it). Patientsshould not interrupt or discontinue BYSTOLIC without consulting the physician.Patients should know how they react to this medicine before they operate automo-biles, use machinery, or engage in other tasks requiring alertness.Patients should be advised to consult a physician if any difficulty in breathingoccurs, or if they develop signs or symptoms of worsening congestive heart failuresuch as weight gain or increasing shortness of breath, or excessive bradycardia.
Patients subject to spontaneous hypoglycemia, or diabetic patients receiving insulinor oral hypoglycemic agents, should be cautioned that β-blockers may mask someof the manifestations of hypoglycemia, particularly tachycardia. Nebivolol should beused with caution in these patients.Drug InteractionsBYSTOLIC should be used with care when myocardial depressants or inhibitors ofAV conduction, such as certain calcium antagonists (particularly of the phenylalky-lamine [verapamil] and benzothiazepine [diltiazem] classes), or antiarrhythmicagents, such as disopyramide, are used concurrently. Both digitalis glycosides andβ-blockers slow atrioventricular conduction and decrease heart rate. Concomitantuse can increase the risk of bradycardia.BYSTOLIC should not be combined with other β-blockers. Patients receiving catecholamine-depleting drugs, such as reserpine or guanethidine, should beclosely monitored, because the added β-blocking action of BYSTOLIC may produceexcessive reduction of sympathetic activity. In patients who are receivingBYSTOLIC and clonidine, BYSTOLIC should be discontinued for several days beforethe gradual tapering of clonidine.CYP2D6 Inhibitors: Use caution when BYSTOLIC is co-administered with CYP2D6inhibitors (quinidine, propafenone, fluoxetine, paroxetine, etc.) (see CLINICALPHARMACOLOGY, Drug Interactions).Carcinogenesis, Mutagenesis, Impairment of FertilityIn a two-year study of nebivolol in mice, a statistically significant increase in theincidence of testicular Leydig cell hyperplasia and adenomas was observed at 40 mg/kg/day (5 times the maximally recommended human dose of 40 mg on amg/m2 basis). Similar findings were not reported in mice administered doses equalto approximately 0.3 or 1.2 times the maximum recommended human dose. Noevidence of a tumorigenic effect was observed in a 24-month study in Wistar ratsreceiving doses of nebivolol of 2.5, 10 and 40 mg/kg/day (equivalent to 0.6, 2.4,and 10 times the maximally recommended human dose). Co-administration ofdihydrotestosterone reduced blood LH levels and prevented the Leydig cell hyper-plasia, consistent with an indirect LH-mediated effect of nebivolol in mice and notthought to be clinically relevant in man. A randomized, double-blind, placebo- and active-controlled, parallel-group study inhealthy male volunteers was conducted to determine the effects of nebivolol onadrenal function, luteinizing hormone, and testosterone levels. This study demon-strated that 6 weeks of daily dosing with 10 mg of nebivolol had no significant effecton ACTH-stimulated mean serum cortisol AUC0-120 min, serum LH, or serum totaltestosterone.Effects on spermatogenesis were seen in male rats and mice at ≥40 mg/kg/day (10 and 5 times the MRHD, respectively). For rats, the effects on spermatogenesiswere not reversed and may have worsened during a four week recovery period. Theeffects of nebivolol on sperm in mice, however, were partially reversible. Mutagenesis: Nebivolol was not genotoxic when tested in a battery of assays(Ames, in vitro mouse lymphoma TK+/-, in vitro human peripheral lymphocyte chro-mosome aberration, in vivo Drosophila melanogaster sex-linked recessive lethal,and in vivo mouse bone marrow micronucleus tests).Pregnancy: Teratogenic Effects. Pregnancy Category C:Decreased pup body weights occurred at 1.25 and 2.5 mg/kg in rats, when exposedduring the perinatal period (late gestation, parturition and lactation). At 5 mg/kg andhigher doses (1.2 times the MRHD), prolonged gestation, dystocia and reducedmaternal care were produced with corresponding increases in late fetal deaths andstillbirths and decreased birth weight, live litter size and pup survival. Insufficientnumbers of pups survived at 5 mg/kg to evaluate the offspring for reproductive performance. In studies in which pregnant rats were given nebivolol during organogenesis,reduced fetal body weights were observed at maternally toxic doses of 20 and 40 mg/kg/day (5 and 10 times the MRHD), and small reversible delays in sternaland thoracic ossification associated with the reduced fetal body weights and a smallincrease in resorption occurred at 40 mg/kg/day (10 times the MRHD). No adverseeffects on embryo-fetal viability, sex, weight or morphology were observed in studies in which nebivolol was given to pregnant rabbits at doses as high as 20 mg/kg/day (10 times the MRHD).Labor and DeliveryNebivolol caused prolonged gestation and dystocia at doses ≥5 mg/kg in rats (1.2 times the MRHD). These effects were associated with increased fetal deathsand stillborn pups, and decreased birth weight, live litter size and pup survival rate,events that occurred only when nebivolol was given during the perinatal period (lategestation, parturition and lactation). No studies of nebivolol were conducted in pregnant women. BYSTOLIC should beused during pregnancy only if the potential benefit justifies the potential risk to thefetus.Nursing MothersStudies in rats have shown that nebivolol or its metabolites cross the placental barrier and are excreted in breast milk. It is not known whether this drug is excretedin human milk.Because of the potential for β-blockers to produce serious adverse reactions innursing infants, especially bradycardia, BYSTOLIC is not recommended duringnursing.Geriatric UseOf the 2800 patients in the U.S.-sponsored placebo-controlled clinical hypertensionstudies, 478 patients were 65 years of age or older. No overall differences in efficacyor in the incidence of adverse events were observed between older and youngerpatients.Pediatric UseSafety and effectiveness in pediatric patients have not been established. Pediatricstudies in ages newborn to 18 years old have not been conducted because ofincomplete characterization of developmental toxicity and possible adverse effectson long-term fertility (see Carcinogenesis, Mutagenesis and Impairment ofInfertility).
ADVERSE REACTIONSThe data described below reflect worldwide clinical trial exposure to BYSTOLIC in6545 patients, including 5038 patients treated for hypertension and the remaining1507 subjects treated for other cardiovascular diseases. Doses ranged from 0.5 mgto 40 mg. Patients received BYSTOLIC for up to 24 months, with over 1900 patientstreated for at least 6 months, and approximately 1300 patients for more than oneyear. In placebo-controlled clinical trials comparing BYSTOLIC with placebo, dis-continuation of therapy due to adverse events was reported in 2.8% of patientstreated with nebivolol and 2.2% of patients given placebo. The most commonadverse events that led to discontinuation of BYSTOLIC were headache (0.4%),nausea (0.2%) and bradycardia (0.2%).Adverse Reactions in Controlled TrialsTable 1 lists treatment-emergent signs and symptoms that were reported in three 12-week, placebo-controlled monotherapy trials involving 1597 hypertensive patientstreated with either 5 mg, 10 mg or 20-40 mg of BYSTOLIC and 205 patients given placebo and for which the rate of occurrence was at least 1% of patients treated with nebivolol and greater than the rate for those treated with placebo in atleast one dose group.
Table 1. Treatment-Emergent Adverse Events with an Incidence (over 6 weeks)≥1% in BYSTOLIC-treated Patients and at a Higher Frequency than Placebo-Treated Patients
Placebo Nebivolol Nebivolol Nebivolol 5 mg 10 mg 20-40 mg
(n = 205) (n = 459) (n = 461) (n = 677)(%) (%) (%) (%)
Headache 6 9 6 7Fatigue 1 2 2 5Dizziness 2 2 3 4Diarrhea 2 2 2 3Nausea 0 1 3 2Insomnia 0 1 1 1Chest pain 0 0 1 1Bradycardia 0 0 0 1Dyspnea 0 0 1 1Rash 0 0 1 1Peripheral edema 0 1 1 1
Other Adverse Events Observed During Worldwide Clinical TrialsListed below are other reported adverse events with an incidence of at least 1% inthe more than 5300 patients treated with BYSTOLIC in controlled or open-label trials, whether or not attributed to treatment, except for those already appearing inTable 1, terms too general to be informative, minor symptoms, or events unlikelyto be attributable to drug because they are common in the population. Theseadverse events were in most cases observed at a similar frequency in placebo-treated patients in the controlled studies.Body as a whole: asthenia.Gastrointestinal System Disorders: abdominal pain Metabolic and Nutritional Disorders: hypercholesterolemia and hyperuricemia Nervous System Disorders: paraesthesiaLaboratoryIn controlled monotherapy trials, BYSTOLIC was associated with an increase inBUN, uric acid, triglycerides and a decrease in HDL cholesterol and platelet count. Events Identified from Spontaneous Reports of BYSTOLIC Received Worldwide.The following adverse events have been identified from spontaneous reports ofBYSTOLIC received worldwide and have not been listed elsewhere. These adverseevents have been chosen for inclusion due to a combination of seriousness, frequency of reporting or potential causal connection to BYSTOLIC. Events commonin the population have generally been omitted. Because these events were reportedvoluntarily from a population of uncertain size, it is not possible to estimate their fre-quency or establish a causal relationship to BYSTOLIC exposure: abnormal hepaticfunction (including increased AST, ALT and bilirubin), acute pulmonary edema, acuterenal failure, atrioventricular block (both second and third degree), bronchospasm,erectile dysfunction, hypersensitivity (including urticaria, allergic vasculitis and rarereports of angioedema), myocardial infarction, pruritus, psoriasis, Raynaud’s phenomenon, peripheral ischemia/claudication, somnolence, syncope, thrombocy-topenia, various rashes and skin disorders, vertigo, and vomiting.
OVERDOSAGEIn clinical trials and worldwide postmarketing experience there were reports ofBYSTOLIC overdose. The most common signs and symptoms associated withBYSTOLIC overdosage are bradycardia and hypotension. Other important adverseevents reported with BYSTOLIC overdose include cardiac failure, dizziness, hypo-glycemia, fatigue and vomiting. Other adverse events associated with β-blockeroverdose include bronchospasm and heart block.The largest known ingestion of BYSTOLIC worldwide involved a patient who ingested up to 500 mg of BYSTOLIC along with several 100 mg tablets of acetylsali-cylic acid in a suicide attempt. The patient experienced hyperhidrosis, pallor,depressed level of consciousness, hypokinesia, hypotension, sinus bradycardia,hypoglycemia, hypokalemia, respiratory failure and vomiting. The patient recovered.Due to extensive drug binding to plasma proteins, hemodialysis is not expected toenhance nebivolol clearance.If overdose occurs, BYSTOLIC should be stopped and general supportive and specific symptomatic treatment should be provided. Based on expected pharmaco-logic actions and recommendations for other β-blockers, the following generalmeasures should be considered when clinically warranted:Bradycardia: Administer IV atropine. If the response is inadequate, isoproterenol oranother agent with positive chronotropic properties may be given cautiously. Undersome circumstances, transthoracic or transvenous pacemaker placement may benecessary.Hypotension: Administer IV fluids and vasopressors. Intravenous glucagon may beuseful.Heart Block (second or third degree): Patients should be carefully monitored andtreated with isoproterenol infusion. Under some circumstances, transthoracic ortransvenous pacemaker placement may be necessary.Congestive Heart Failure: Initiate therapy with digitalis glycoside and diuretics. In certain cases, consideration should be given to the use of inotropic and vaso-dilating agents. Bronchospasm: Administer bronchodilator therapy such as a short-acting inhaledβ2-agonist and/or aminophylline.Hypoglycemia: Administer IV glucose. Repeated doses of IV glucose or possiblyglucagon may be required.In the event of intoxication where there are symptoms of shock, treatment must becontinued for a sufficiently long period consistent with the 12-19 hour effectivehalf-life of BYSTOLIC. Supportive measures should continue until clinical stabilityis achieved.Call the National Poison Control Center (800-222-1222) for the most current infor-mation on β-blocker overdose treatment.
Forest Pharmaceuticals, Inc.Subsidiary of Forest Laboratories, Inc.
St. Louis, MO 63045, USALicensed from Mylan Laboratories, Inc.
Under license from JanssenPharmaceutica N.V., Beerse, Belgium
Rev. 12/07© 2007 Forest Laboratories, Inc.
Rx Only
For the treatment of hypertension
Please see brief summary of full Prescribing Information on adjacent page.
For full Prescribing Information visit www.BYSTOLIC.com.
Important Safety InformationPatients being treated with BYSTOLIC should be advised against abrupt discontinuation of therapy. Severe exacerbation of anginaand the occurrence of myocardial infarction and ventricular arrhythmias have been reported following the abrupt cessation oftherapy with beta blockers. When discontinuation is planned, the dosage should be reduced gradually over a 1- to 2-week periodand the patient carefully monitored.BYSTOLIC is contraindicated in severe bradycardia, heart block greater than first degree, cardiogenic shock, decompensatedcardiac failure, sick sinus syndrome (unless a permanent pacemaker is in place), severe hepatic impairment (Child-Pugh >B), and in patients who are hypersensitive to any component of this product.BYSTOLIC should be used with caution in patients with peripheral vascular disease, thyrotoxicosis, in patients treated concomitantlywith beta blockers and calcium channel blockers of the verapamil and diltiazem type (ECG and blood pressure should be monitored),severe renal impairment, and any degree of hepatic impairment or in patients undergoing major surgery. Caution should also beused in diabetic patients as beta blockers may mask some of the manifestations of hypoglycemia, particularly tachycardia.In general, patients with bronchospastic disease should not receive beta blockers. BYSTOLIC should not be combined with other beta blockers.The most common adverse events with BYSTOLIC versus placebo (approximately >1% and greater than placebo) were headache, fatigue, dizziness, diarrhea, nausea, insomnia, chest pain, bradycardia, dyspnea, rash, and peripheral edema.
*In extensive metabolizers (most of the population) and at doses <10 mg, BYSTOLIC is preferentially �1 selective. The mechanism of action of the antihypertensive response of BYSTOLIC hasnot been definitively established. Possible factors that may be involved include: (1) decreased heart rate, (2) decreased myocardial contractility, (3) diminution of tonic sympathetic outflow to theperiphery from cerebral vasomotor centers, (4) suppression of renin activity, and (5) vasodilation and decreased peripheral vascular resistance.
References: 1. BYSTOLIC [package insert]. St. Louis, Mo: Forest Pharmaceuticals, Inc.; 2007. 2. Data on file. Forest Laboratories, Inc. 3. Saunders E, Smith WB, DeSalvo KB, Sullivan WA.The efficacy and tolerability of nebivolol in hypertensive African American patients. J Clin Hypertens. 2007;9:866-875.
Introducing BYSTOLIC.A novel beta blocker with efficacy and favorable tolerability across a broad range of patients.1-3
n Unique mechanism of action includes cardioselective beta blockade and vasodilation1*
n Once-daily antihypertensive, with efficacy maintained over 24 hours1
©2008 Forest Laboratories, Inc. 44-1012269R1 02/08
13www.AHDBonline.com
CLINICAL
Schizophrenia is a poorly understood condition.Despite several recent documentaries and moviesdepicting the course and disability of this illness,
the lay public remains largely confused about schizo-phrenia and continues to harbor notions that it is a“split personality” or a “Jekyll and Hyde” phenomenon.Regrettably, efforts to articulate a clear account of whatschizophrenia really is and what causes it have beenhampered by a lack of compelling evidence as to its eti-ology. Despite the many clues to the cause(s) of schizo-phrenia, definitive evidence is still lacking. In manyways, we can be more dogmatic about what is not rele-vant to schizophrenia (Table 1). This is importantbecause stigma, which is fueled by a lack of knowledge,is a major obstacle in managing schizophrenia. Severalbooks provide comprehensive information about schiz-ophrenia.1-4 This article offers a current overview ofschizophrenia and its treatment.
DiagnosisSchizophrenia is a complicated diagnosis. The con-
dition is characterized by delusions (fixed, false beliefs),hallucinations (typically “hearing voices” when no oneis around), disturbances of speech (illogicality, nonlin-earity of thought and conversation), restricted affectand emotionality, and impairments of thinking (mem-ory, attention, reasoning, awareness).
Schizophrenia: Current Conceptsand Approaches to Patient CarePeter F. Buckley, MDAdriana Foster, MD
Schizophrenia is the most serious of all mental conditions. It is typically a long-lastingcondition characterized by repeated relapses and by marked functional impairment.Genetic and environmental factors are important. Exactly which factors and how thesecombine to cause schizophrenia is still unclear. Antipsychotic medications form thebedrock for treatment. These drugs are effective, but not entirely so, and are associatedwith negative side effects. Individual differences among the available medications suggestthat trials with a different medication may be appropriate when one agent fails or is notappropriate for the specific patient. Monitoring for side effects is important to ensure effi-cacy and compliance. Often, patients choose to stop taking their medications for a vari-
ety of reasons, which invariably will lead most patients to a relapse of illness. Beyond medications, patients needconsiderable support and specialized services. Families are a key resource. The recent focus on personal determi-nation has led to recovery-based services, including the incorporation of peer support into patient care. [AHDB.2008;1(4):13-22.]
Dr Buckley is Professor and Chair, and Dr Foster is AssistantProfessor, Department of Psychiatry and Health Behavior,Medical College of Georgia, Atlanta.
Peter F. Buckley, MD
Table 1 Dispelling Common Myths about Schizophrenia
1. Despite common belief, schizophrenia is NOT causedby: • “Difficult” parents• Diet• Stress• The left side of the brain dominating the right side
2. It is not a split personality3. Not all patients are violent4. Patients are not “inventing” unusual ideas or lying,
they believe these
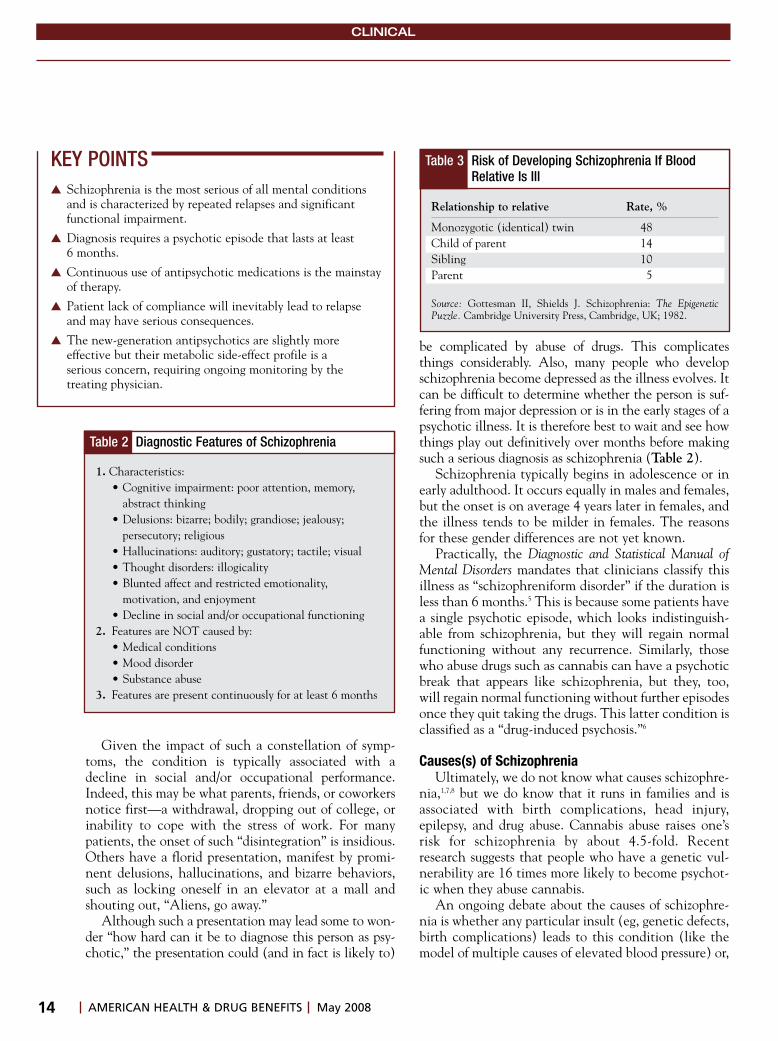
14 AMERICAN HEALTH & DRUG BENEFITS May 2008
CLINICAL
Given the impact of such a constellation of symp-toms, the condition is typically associated with adecline in social and/or occupational performance.Indeed, this may be what parents, friends, or coworkersnotice first—a withdrawal, dropping out of college, orinability to cope with the stress of work. For manypatients, the onset of such “disintegration” is insidious.Others have a florid presentation, manifest by promi-nent delusions, hallucinations, and bizarre behaviors,such as locking oneself in an elevator at a mall andshouting out, “Aliens, go away.”
Although such a presentation may lead some to won-der “how hard can it be to diagnose this person as psy-chotic,” the presentation could (and in fact is likely to)
be complicated by abuse of drugs. This complicatesthings considerably. Also, many people who developschizophrenia become depressed as the illness evolves. Itcan be difficult to determine whether the person is suf-fering from major depression or is in the early stages of apsychotic illness. It is therefore best to wait and see howthings play out definitively over months before makingsuch a serious diagnosis as schizophrenia (Table 2).
Schizophrenia typically begins in adolescence or inearly adulthood. It occurs equally in males and females,but the onset is on average 4 years later in females, andthe illness tends to be milder in females. The reasonsfor these gender differences are not yet known.
Practically, the Diagnostic and Statistical Manual ofMental Disorders mandates that clinicians classify thisillness as “schizophreniform disorder” if the duration isless than 6 months.5 This is because some patients havea single psychotic episode, which looks indistinguish-able from schizophrenia, but they will regain normalfunctioning without any recurrence. Similarly, thosewho abuse drugs such as cannabis can have a psychoticbreak that appears like schizophrenia, but they, too,will regain normal functioning without further episodesonce they quit taking the drugs. This latter condition isclassified as a “drug-induced psychosis.”6
Causes(s) of SchizophreniaUltimately, we do not know what causes schizophre-
nia,1,7,8 but we do know that it runs in families and isassociated with birth complications, head injury,epilepsy, and drug abuse. Cannabis abuse raises one’srisk for schizophrenia by about 4.5-fold. Recentresearch suggests that people who have a genetic vul-nerability are 16 times more likely to become psychot-ic when they abuse cannabis.
An ongoing debate about the causes of schizophre-nia is whether any particular insult (eg, genetic defects,birth complications) leads to this condition (like themodel of multiple causes of elevated blood pressure) or,
KEY POINTS� Schizophrenia is the most serious of all mental conditions
and is characterized by repeated relapses and significantfunctional impairment.
� Diagnosis requires a psychotic episode that lasts at least 6 months.
� Continuous use of antipsychotic medications is the mainstayof therapy.
� Patient lack of compliance will inevitably lead to relapseand may have serious consequences.
� The new-generation antipsychotics are slightly more effective but their metabolic side-effect profile is a serious concern, requiring ongoing monitoring by the treating physician.
Table 2 Diagnostic Features of Schizophrenia
1. Characteristics:• Cognitive impairment: poor attention, memory,
abstract thinking• Delusions: bizarre; bodily; grandiose; jealousy;
persecutory; religious• Hallucinations: auditory; gustatory; tactile; visual • Thought disorders: illogicality• Blunted affect and restricted emotionality,
motivation, and enjoyment• Decline in social and/or occupational functioning
2. Features are NOT caused by: • Medical conditions • Mood disorder• Substance abuse
3. Features are present continuously for at least 6 months
Table 3 Risk of Developing Schizophrenia If BloodRelative Is Ill
Relationship to relative Rate, %
Monozygotic (identical) twin 48Child of parent 14Sibling 10Parent 5
Source: Gottesman II, Shields J. Schizophrenia: The EpigeneticPuzzle. Cambridge University Press, Cambridge, UK; 1982.
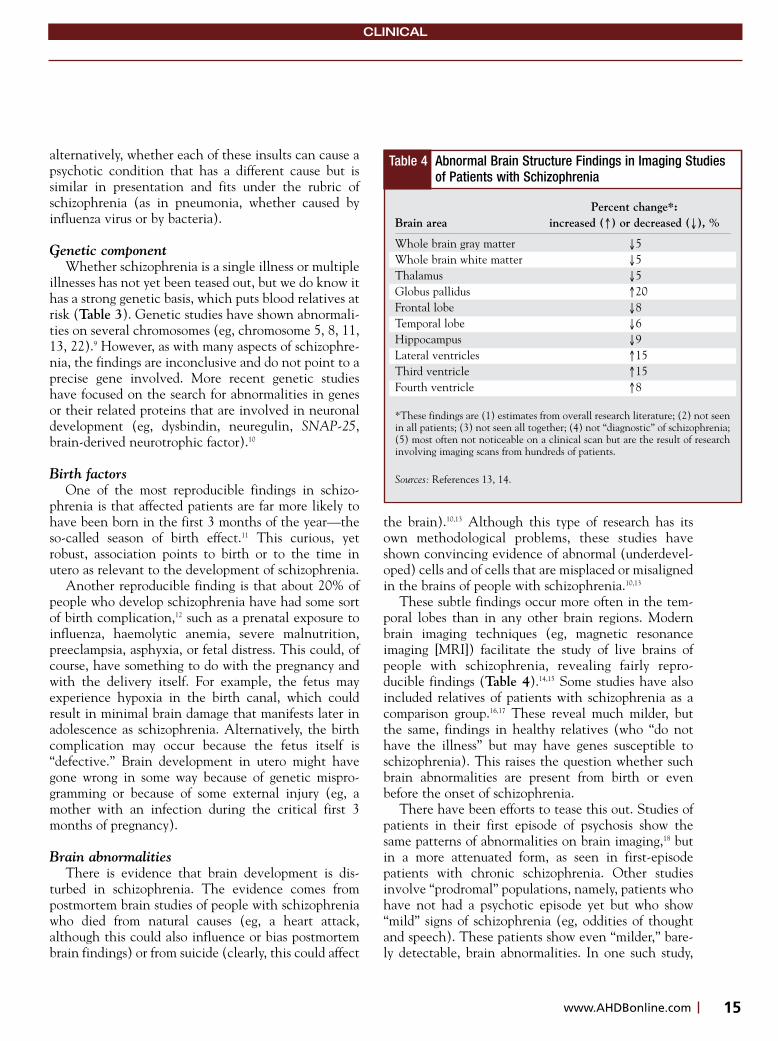
15www.AHDBonline.com
CLINICAL
alternatively, whether each of these insults can cause apsychotic condition that has a different cause but issimilar in presentation and fits under the rubric ofschizophrenia (as in pneumonia, whether caused byinfluenza virus or by bacteria).
Genetic componentWhether schizophrenia is a single illness or multiple
illnesses has not yet been teased out, but we do know ithas a strong genetic basis, which puts blood relatives atrisk (Table 3). Genetic studies have shown abnormali-ties on several chromosomes (eg, chromosome 5, 8, 11,13, 22).9 However, as with many aspects of schizophre-nia, the findings are inconclusive and do not point to aprecise gene involved. More recent genetic studieshave focused on the search for abnormalities in genesor their related proteins that are involved in neuronaldevelopment (eg, dysbindin, neuregulin, SNAP-25,brain-derived neurotrophic factor).10
Birth factors One of the most reproducible findings in schizo-
phrenia is that affected patients are far more likely tohave been born in the first 3 months of the year—theso-called season of birth effect.11 This curious, yetrobust, association points to birth or to the time inutero as relevant to the development of schizophrenia.
Another reproducible finding is that about 20% ofpeople who develop schizophrenia have had some sortof birth complication,12 such as a prenatal exposure toinfluenza, haemolytic anemia, severe malnutrition,preeclampsia, asphyxia, or fetal distress. This could, ofcourse, have something to do with the pregnancy andwith the delivery itself. For example, the fetus mayexperience hypoxia in the birth canal, which couldresult in minimal brain damage that manifests later inadolescence as schizophrenia. Alternatively, the birthcomplication may occur because the fetus itself is“defective.” Brain development in utero might havegone wrong in some way because of genetic mispro-gramming or because of some external injury (eg, amother with an infection during the critical first 3months of pregnancy).
Brain abnormalitiesThere is evidence that brain development is dis-
turbed in schizophrenia. The evidence comes frompostmortem brain studies of people with schizophreniawho died from natural causes (eg, a heart attack,although this could also influence or bias postmortembrain findings) or from suicide (clearly, this could affect
the brain).10,13 Although this type of research has itsown methodological problems, these studies haveshown convincing evidence of abnormal (underdevel-oped) cells and of cells that are misplaced or misalignedin the brains of people with schizophrenia.10,13
These subtle findings occur more often in the tem-poral lobes than in any other brain regions. Modernbrain imaging techniques (eg, magnetic resonanceimaging [MRI]) facilitate the study of live brains ofpeople with schizophrenia, revealing fairly repro-ducible findings (Table 4).14,15 Some studies have alsoincluded relatives of patients with schizophrenia as acomparison group.16,17 These reveal much milder, butthe same, findings in healthy relatives (who “do nothave the illness” but may have genes susceptible toschizophrenia). This raises the question whether suchbrain abnormalities are present from birth or evenbefore the onset of schizophrenia.
There have been efforts to tease this out. Studies ofpatients in their first episode of psychosis show thesame patterns of abnormalities on brain imaging,18 butin a more attenuated form, as seen in first-episodepatients with chronic schizophrenia. Other studiesinvolve “prodromal” populations, namely, patients whohave not had a psychotic episode yet but who show“mild” signs of schizophrenia (eg, oddities of thoughtand speech). These patients show even “milder,” bare-ly detectable, brain abnormalities. In one such study,
Table 4 Abnormal Brain Structure Findings in Imaging Studiesof Patients with Schizophrenia
Percent change*:Brain area increased (�) or decreased (�), %
Whole brain gray matter �5Whole brain white matter �5Thalamus �5Globus pallidus �20Frontal lobe �8Temporal lobe �6Hippocampus �9Lateral ventricles �15Third ventricle �15Fourth ventricle �8
*These findings are (1) estimates from overall research literature; (2) not seenin all patients; (3) not seen all together; (4) not “diagnostic” of schizophrenia;(5) most often not noticeable on a clinical scan but are the result of researchinvolving imaging scans from hundreds of patients.
Sources: References 13, 14.

16 AMERICAN HEALTH & DRUG BENEFITS May 2008
CLINICAL
the prodromal patients who went on to have a psy-chotic break had more temporal lobe abnormalities onMRI than patients who did not progress to psychosis.19
Collectively, these findings, which point to faultyearly brain development, have led many to consider thatschizophrenia may be a neurodevelopmental disorder(Table 5).1,7,20 That is, people with schizophrenia mayhave an aberrant development of brain “hardwire” (eg,misplaced, misaligned, or immature cells; faulty neuralcommunication tracks). It is postulated that as time goesby, these cortical vulnerabilities become exposed as thepatient progresses toward psychosis. Some have suggest-
ed that the reason for the onset of psychosis at adoles-cence is a clue. This is a time of brain “rewiring” andplasticity. With these changes, the otherwise “dormant”brain abnormalities are now exposed. Others have pos-tulated that given this brain vulnerability from birth,other events (eg, drug abuse, stress) during adolescencemay also push the person (ie, brain) “over the edge” tocause psychosis. This “2-hit” notion is also an intuitive-ly appealing hypothesis. All these reflect the notion thatschizophrenia is a neurodevelopmental disorder, and aswith other such disorders (eg, cerebral palsy), the causesmay be genetic, environmental, or both.
Kraepelin, the German psychiatrist who firstdescribed schizophrenia in 1896, considers this to be adementing condition. He describes how schizophreniaevolves in adolescence and progresses inexorably into achronic state (which he called “dementia praecox,”dementia of youth).
Seemingly in direct opposition to the brain-imagingevidence that supports the neurodevelopmentalhypothesis in schizophrenia, other, long-term imagingstudies report a progressive loss of brain tissue.21,22 Thiswould favor a neurodegenerative hypothesis of schizo-phrenia (like Huntington’s disease). Some have sug-gested that schizophrenia may have both neurodevel-opmental and neurodegenerative processes at work.Under such a parsimonious scheme, it is proposed thatthe underlying neurodevelopmental brain vulnerabilitypredisposes to a more progressive brain loss.23 A prece-dent for this viewpoint is Down syndrome (DS), whichis a prototypical neurodevelopmental disorder causedby chromosomal abnormalities. Patients with DS showa variety of neurodevelopmental features clinically (seeTable 5), and they also have mental retardation.Patients with DS develop Alzheimer’s-like dementiavery early on, typically in their 40s. Therefore, somehave suggested that a 2-process model may also explainschizophrenia. But as elegant as each of these hypo -theses are, they are also very difficult to prove or refute.
The weight of evidence currently favors a neurodevel-opmental basis for schizophrenia. It is plausible that somepatients could have a neurodevelopmental form of schiz-ophrenia, while others may have a neurodegenerativeschizophrenia.20 The complexity of the process involvedand the lack of a clear understanding lessen our ability togive a clear picture about schizophrenia to the public.
Brain Chemistry and Schizophrenia Overactivity of the dopamine neurotransmitter sys-
tem is the most compelling neurochemical abnormalityin schizophrenia.24 This is also the most easily explained
Table 5 Evidence for Schizophrenia as a NeurodevelopmentalDisorder
1. Genes that code for neurodevelopment have been implicated2. High rates of birth complications3. Season of birth phenomenon4. Many patients have minor physical anomalies*
• Abnormal or fused webs at toes• Abnormal palmar creases• Low-set ears• Shortened faces• Widened eyes
5. Many patients have abnormal fingerprints*6. Type and pattern of structural brain abnormalities seen in
brain-imaging studies7. Type and pattern of brain changes in postmortem studies
*Subtle skin “blemishes” that relate in timing to maturation of the skin andthe central nervous system in utero.
Table 6 Elements of Comprehensive Care for Patients with Schizophrenia
Access to coordinated substance abuse servicesAppropriate medication treatmentCounseling: supportive psychotherapyGood medical careMore specialized counseling/support:
Cognitive behavioral therapyPeer support services
Psychoeducation (illness education)Social skills training and community reintegration support servicesFinancial aidHousing supportSheltered and “regular” employment opportunitiesSupport and educational opportunities
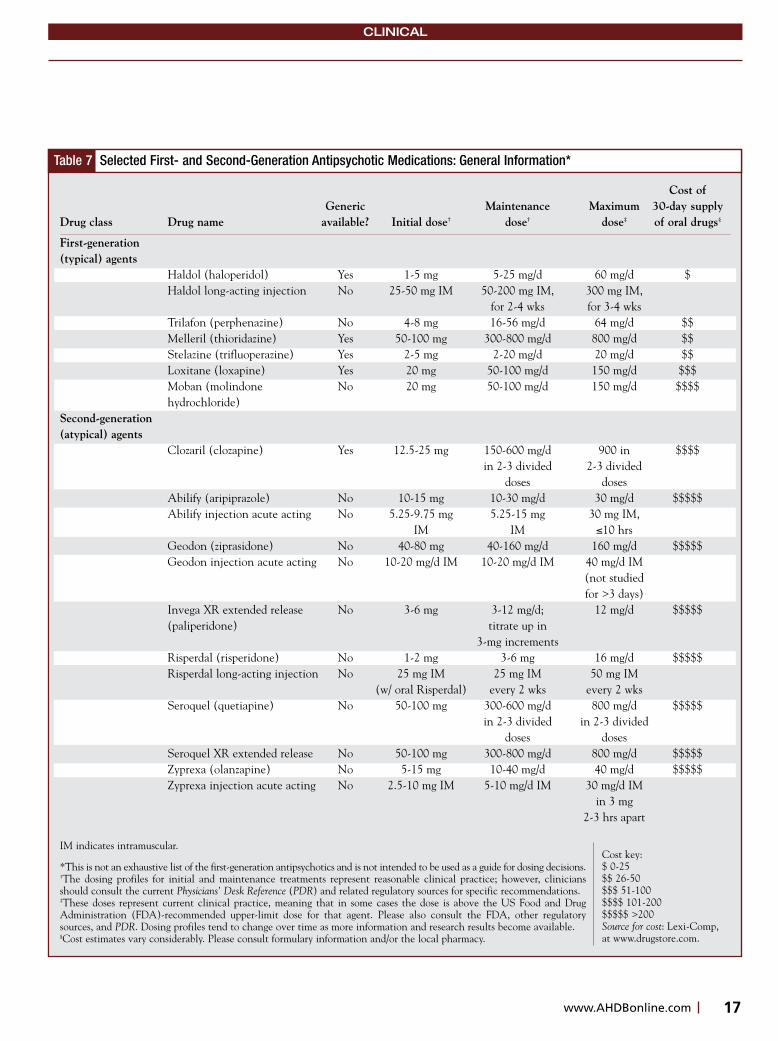
17www.AHDBonline.com
CLINICAL
Table 7 Selected First- and Second-Generation Antipsychotic Medications: General Information*
Cost ofGeneric Maintenance Maximum 30-day supply
Drug class Drug name available? Initial dose† dose† dose‡ of oral drugs§
First-generation(typical) agents
Haldol (haloperidol) Yes 1-5 mg 5-25 mg/d 60 mg/d $Haldol long-acting injection No 25-50 mg IM 50-200 mg IM, 300 mg IM,
for 2-4 wks for 3-4 wksTrilafon (perphenazine) No 4-8 mg 16-56 mg/d 64 mg/d $$Melleril (thioridazine) Yes 50-100 mg 300-800 mg/d 800 mg/d $$Stelazine (trifluoperazine) Yes 2-5 mg 2-20 mg/d 20 mg/d $$Loxitane (loxapine) Yes 20 mg 50-100 mg/d 150 mg/d $$$Moban (molindone No 20 mg 50-100 mg/d 150 mg/d $$$$hydrochloride)
Second-generation(atypical) agents
Clozaril (clozapine) Yes 12.5-25 mg 150-600 mg/d 900 in $$$$in 2-3 divided 2-3 divided
doses dosesAbilify (aripiprazole) No 10-15 mg 10-30 mg/d 30 mg/d $$$$$Abilify injection acute acting No 5.25-9.75 mg 5.25-15 mg 30 mg IM,
IM IM �10 hrsGeodon (ziprasidone) No 40-80 mg 40-160 mg/d 160 mg/d $$$$$Geodon injection acute acting No 10-20 mg/d IM 10-20 mg/d IM 40 mg/d IM
(not studiedfor >3 days)
Invega XR extended release No 3-6 mg 3-12 mg/d; 12 mg/d $$$$$(paliperidone) titrate up in
3-mg incrementsRisperdal (risperidone) No 1-2 mg 3-6 mg 16 mg/d $$$$$Risperdal long-acting injection No 25 mg IM 25 mg IM 50 mg IM
(w/ oral Risperdal) every 2 wks every 2 wksSeroquel (quetiapine) No 50-100 mg 300-600 mg/d 800 mg/d $$$$$
in 2-3 divided in 2-3 divided doses doses
Seroquel XR extended release No 50-100 mg 300-800 mg/d 800 mg/d $$$$$Zyprexa (olanzapine) No 5-15 mg 10-40 mg/d 40 mg/d $$$$$Zyprexa injection acute acting No 2.5-10 mg IM 5-10 mg/d IM 30 mg/d IM
in 3 mg2-3 hrs apart
IM indicates intramuscular.
*This is not an exhaustive list of the first-generation antipsychotics and is not intended to be used as a guide for dosing decisions.†The dosing profiles for initial and maintenance treatments represent reasonable clinical practice; however, cliniciansshould consult the current Physicians’ Desk Reference (PDR) and related regulatory sources for specific recommendations. ‡These doses represent current clinical practice, meaning that in some cases the dose is above the US Food and DrugAdministration (FDA)-recommended upper-limit dose for that agent. Please also consult the FDA, other regulatorysources, and PDR. Dosing profiles tend to change over time as more information and research results become available.§Cost estimates vary considerably. Please consult formulary information and/or the local pharmacy.
Cost key: $ 0-25$$ 26-50$$$ 51-100$$$$ 101-200$$$$$ >200Source for cost: Lexi-Comp,at www.drugstore.com.
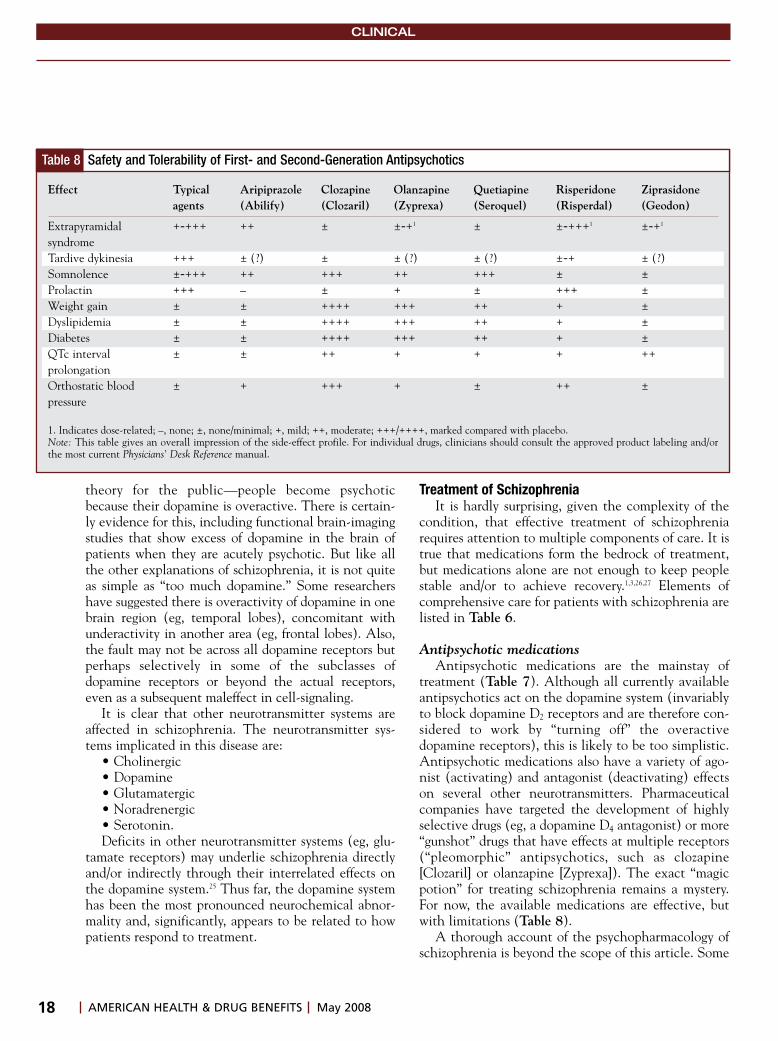
18 AMERICAN HEALTH & DRUG BENEFITS May 2008
CLINICAL
theory for the public—people become psychoticbecause their dopamine is overactive. There is certain-ly evidence for this, including functional brain-imagingstudies that show excess of dopamine in the brain ofpatients when they are acutely psychotic. But like allthe other explanations of schizophrenia, it is not quiteas simple as “too much dopamine.” Some researchershave suggested there is overactivity of dopamine in onebrain region (eg, temporal lobes), concomitant withunderactivity in another area (eg, frontal lobes). Also,the fault may not be across all dopamine receptors butperhaps selectively in some of the subclasses ofdopamine receptors or beyond the actual receptors,even as a subsequent maleffect in cell-signaling.
It is clear that other neurotransmitter systems areaffected in schizophrenia. The neurotransmitter sys-tems implicated in this disease are:
• Cholinergic• Dopamine• Glutamatergic• Noradrenergic• Serotonin.Deficits in other neurotransmitter systems (eg, glu-
tamate receptors) may underlie schizophrenia directlyand/or indirectly through their interrelated effects onthe dopamine system.25 Thus far, the dopamine systemhas been the most pronounced neurochemical abnor-mality and, significantly, appears to be related to howpatients respond to treatment.
Treatment of SchizophreniaIt is hardly surprising, given the complexity of the
condition, that effective treatment of schizophreniarequires attention to multiple components of care. It istrue that medications form the bedrock of treatment,but medications alone are not enough to keep peoplestable and/or to achieve recovery.1,3,26,27 Elements ofcomprehensive care for patients with schizophrenia arelisted in Table 6.
Antipsychotic medicationsAntipsychotic medications are the mainstay of
treatment (Table 7). Although all currently availableantipsychotics act on the dopamine system (invariablyto block dopamine D2 receptors and are therefore con-sidered to work by “turning off” the overactivedopamine receptors), this is likely to be too simplistic.Antipsychotic medications also have a variety of ago-nist (activating) and antagonist (deactivating) effectson several other neurotransmitters. Pharmaceuticalcompanies have targeted the development of highlyselective drugs (eg, a dopamine D4 antagonist) or more“gunshot” drugs that have effects at multiple receptors(“pleomorphic” antipsychotics, such as clozapine[Clozaril] or olanzapine [Zyprexa]). The exact “magicpotion” for treating schizophrenia remains a mystery.For now, the available medications are effective, butwith limitations (Table 8).
A thorough account of the psychopharmacology ofschizophrenia is beyond the scope of this article. Some
Table 8 Safety and Tolerability of First- and Second-Generation Antipsychotics
Effect Typical Aripiprazole Clozapine Olanzapine Quetiapine Risperidone Ziprasidoneagents (Abilify) (Clozaril) (Zyprexa) (Seroquel) (Risperdal) (Geodon)
Extrapyramidal +-+++ ++ ± ±-+1 ± ±-+++1 ±-+1
syndromeTardive dykinesia +++ ± (?) ± ± (?) ± (?) ±-+ ± (?)Somnolence ±-+++ ++ +++ ++ +++ ± ±Prolactin +++ – ± + ± +++ ±Weight gain ± ± ++++ +++ ++ + ±Dyslipidemia ± ± ++++ +++ ++ + ±Diabetes ± ± ++++ +++ ++ + ±QTc interval ± ± ++ + + + ++prolongation Orthostatic blood ± + +++ + ± ++ ±pressure
1. Indicates dose-related; –, none; ±, none/minimal; +, mild; ++, moderate; +++/++++, marked compared with placebo.Note: This table gives an overall impression of the side-effect profile. For individual drugs, clinicians should consult the approved product labeling and/orthe most current Physicians’ Desk Reference manual.

19www.AHDBonline.com
CLINICAL
general comments on the treatment of schizophreniaare more appropriate.
1. With the exception of clozapine, the otherantipsychotics are more similar than different in theirability to control the symptoms of schizophrenia.28,29 Allof them are effective in relieving acute symptoms—anxiety, agitation, delusions, and hallucinations. Somemay act a bit quicker (or perhaps are easier to getquicker to an effective dose) and some may be morepowerful in their effect on symptoms (again, dosingmay play a big role here).
The older (also known as conventional, typical, orfirst-generation) antipsychotic medications haveproved efficacy and work best against positive symp-toms, with little benefit for negative, depressive, orcognitive symptoms (they may even worsen theseaspects of the illness). Their major adverse side effectsare related to their antagonism of the dopamine system.These drugs cause acute and chronic muscle(extrapyramidal) side effects that are distressing anddisfiguring. Because they have been around for a longtime, they are relatively inexpensive.
The new antipsychotics, also known as atypical orsecond-generation antipsychotics, show similar orslightly better efficacy compared with the first-genera-tion agents in treating positive symptoms. They havevariable, but generally only modest, benefits in treatingnegative, depressive, and cognitive symptoms.Although these medications generally have a lower riskfor extrapyramidal side effects than the first-generationagents, they have other serious side effects, as reflectedin Table 8.
More so than the first-generation antipsychotics, thenewer agents cause weight gain and metabolic distur-bances of glucose, insulin, cholesterol, and lipids.29,30 Thisis a major drawback, which has substantially complicat-ed the treatment of schizophrenia and is currently thenumber-one issue in the psychopharmacology of schizo-phrenia. Treating physicians are monitoring patientscarefully to detect such disturbances and are also con-cerned about switching medications and seeking relief inanother antipsychotic when these problems emerge.
These drugs are also remarkably expensive, whichlimits access and imposes high financial burden on analready overburdened mental healthcare system. Incontrast, if these (or any particular) drugs keep apatient from relapsing and avoiding hospitalization,then the medication is cost-effective.
2. Although antipsychotics are generally effective(better in acute care and for positive symptoms), a sub-stantial group of patients remains unwell. Some
patients relapse frequently over time; some are chroni-cally psychotic, and the medications barely work forthem. Efforts to help these patients include:• Trials of high doses of an antipsychotic• A trial of 2 antipsychotics together • Trials of add-on drugs (eg, antidepressants, stimu-
lants) that may boost the effect of the antipsychotics• Use of clozapine (the most powerful of all antipsy-
chotics but with a high side-effect burden)• For intractable situations, as well as for severe depres-
sion or catatonia, a trial of electroconvulsive therapy. There is also a particular interest at present in find-
ing ways to reduce the cognitive deficits of schizophre-nia, which are rate-limiting obstacles to recovery.31
3. The side-effects burden of the antipsychotics issubstantial. Clinicians engage in a trial-and-errorprocess with patients in an effort to find the drug thatwill work best and will result in fewer side effects. Thesensitivity of each patient is unique—both in terms ofthe ability to respond to one drug (but perhaps not toanother) as well as to experience the side effects.
The response and tolerability of each patient is indi-vidualized. We can make general predictions about theoverall risk-benefit profile of any given drug, but how apatient will fare in practice is the true test. In addition,the dose of the medication strongly influences bothresponse and tolerability. At present, the selection,dosing, and use of antipsychotics in clinical practice aremore art than science. Efforts toward personalized med-icine and toward the emergent strategy of pharmacoge-netics (the genetics of medication response and side-effect prediction) offer future hope.
4. Regardless of the benefits and drawbacks of themedications themselves, our ability to treat schizophre-nia is curtailed even more by the patient’s reluctance totake antipsychotic drugs and to continue using medica-tions.32 Estimates differ by each study, but approximate-ly 50% of patients are noncompliant with their pre-scribed antipsychotic medication regimen.33 Most arepartially noncompliant, missing medications “here andthere.” Some patients are noncompliant and “learn thehard way,” by having recurrent relapses of illness. Somepatients remain noncompliant with treatment and, as aresult, are extremely difficult to treat.
When at imminent risk to themselves or others,patients can be hospitalized against their will and beforcibly medicated until their illness is stabilized. Theproblem then recurs, however, when they are dis-charged from the hospital. To combat medication non-compliance, patients can receive their antipsychoticmedication in an injectable form that provides contin-

20 AMERICAN HEALTH & DRUG BENEFITS May 2008
CLINICAL
uous treatment over weeks, usually 2 to 4 weeks. Someclinicians believe that this strategy is underutilized andshould become more mainstream rather than be con-fined to patients who refuse their medications.
Comorbidities complicate treatment In addition to the complexity of the illness itself,
patients with schizophrenia are likely to have otherpsychiatric and/or medical comorbidities over thecourse of their illness, as outlined in Table 9.
Social aspects of treating mental illness Beyond medications, patients need a huge amount of
support.34 The greatest support patients can get—and doget—is from their families. Relatives provide love, emo-tional support, housing, and financial assistance. Theyare also the people who know the patient best and canbe watchful for signs of relapse. However, the emotion-al strain of caring and living with someone who is suf-fering from schizophrenia can be overwhelming.Relatives also need support. They need education onthe latest treatments, as well as tips on how to managedifficult situations. Organizations such as the NationalAlliance for Mental Illness are an invaluable resource.
Patients also need psychological support from men-tal health professionals. Patients benefit from counsel-ing and supportive psychotherapy. There are also pro-grams that focus on social skills training, helpingpatients to make friends and to reintegrate into thecommunity. Most patients do not work; if they do, it isoften at a low-paying job. Although it is clear thatactive psychosis and cognitive deficits reduce thecapacity of people to hold down jobs (especially stress-ful jobs), it is also evident that having a job is a power-ful motivator for healthy living and boosts self-esteem.
There are now efforts to train people and to enhance
their cognitive abilities so that they will be able to sus-tain in employment.35 Our system is poorly constructedto help people get, and hold jobs. Sometimes patientsare faced with the painful decision of taking a job andlosing their Medicaid support, because they now earn awage. These situations expose some of the many waysthat our society discriminates against people with men-tal illness.
Similar to the role of sponsors in AlcoholicsAnonymous, patients with serious mental illness arenow also helping other patients to recover.36 These“peer-support specialists” can be powerful catalysts forchange, for individual patients and for systems of carethrough their roles as advocates. This is a powerfulapproach that broadens the focus of care toward moremeaningful, life-attainment goals. It also instills per-sonal responsibility and hope in patients.
Hope is a powerful catalyst in coping with illness.The notion that some people can recover from seriousillnesses like schizophrenia is powerful.37 Importantcomponents of recovery for people with serious mentalillness include hope, spirituality, and empowerment.37
Patients with more severe illness require continuoussupport to help them live in the community. This serv-ice is delivered by a community psychiatric team com-prised of case managers, with each team serving just afew patients. This labor-intensive approach, called“assertive community treatment” (ACT), works well tomaintain patients in the community. Although itsstaffing costs are high, it is still cost-effective, becauseACT dramatically reduces days spent in a hospital.
Conclusion Schizophrenia is a challenging condition to diag-
nose and to treat. The lack of insight that is so commonwith the condition could undermine (through treat-ment nonadherence) the efforts of family and mentalhealth professionals to provide comprehensive care.The potential for comorbidities further adds to thecomplexity of the illness and will require additionalpsychiatric and/or medical treatment. These furthercomplicate already arduous clinical circumstances.Patients with schizophrenia need comprehensive care,compassion, and support. They deserve this. �
Disclosure Statement Dr Buckley receives grant/research support from AstraZeneca,
National Institute of Mental Health, Pfizer, Solvay, and Wyeth; is aconsultant to AstraZeneca, Bristol-Myers Squibb, Eli Lilly, JanssenPharmaceutica, Lundbeck, Pfizer, Solvay, and Wyeth; and receiveshonoraria from Bristol-Myers Squibb, Janssen Pharmaceutica,Lundbeck, and Pfizer.
Table 9 Psychiatric and Medical Conditions Associated with Schizophrenia
Anxiety and (less commonly) obsessions/compulsionCardiovascular disordersDepressionMetabolic disturbancesObesitySexual behavior associated with HIV, hepatitis C infection SmokingSubstance abuseSuicidality Violence

21www.AHDBonline.com
CLINICAL
References1. Lieberman J, Stoup S, Perkins DO. Textbook of Schizophrenia.Washington, DC: American Psychiatric Press; 2006.2. Jones PB, Buckley PF. Schizophrenia. London: Elsevier; 2006.3. Castle DJ, Copolov D, Wykes T, Mueser K, eds. Pharmacological andPsychosocial Treatments for Schizophrenia. 2nd ed. London: Informa; 2008.4. Torrey EF. Surviving Schizophrenia: A Manual for Families, Patients, andProviders. Collins: New York; 2006 [1983].5. American Psychiatric Association. Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition, Text Revised. Washington, DC:American Psychiatric Association; 2000.6. Castle DJ, Murray RM, eds. Marijuana and Madness. Cambridge,England: Cambridge University Press; 2004.7. Lieberman JA, Perkins D, Belger A, et al. The early stages of schizo-phrenia: speculation on the pathogenesis, pathophysiology, and thera-peutic approaches. Biol Psychiatry. 2001;50:884-897.8. Buckley PF. Update on the treatment of schizophrenia and bipolar dis-order. CNS Spectr. 2008;13(suppl):1-10. 9. McClellan JM, Susser E, King MC. Schizophrenia: a common diseasecaused by multiple rare alleles. Br J Psychiatry. 2007;190:194-199.10. Harrison PJ, Weinberger DR. Schizophrenia genes, gene expression,and neuropathology: on the matter of their convergence. Mol Psychiatry.2005;10(1):40-68.11. McGrath JJ, Murray RM. Risk factors for schizophrenia: from con-ception to birth. Hirsch SR, Weinberger DR, eds. In: Schizophrenia.Oxford: Blackwell Press; 2003.12. Cannon M, Clarke MC. Risk for schizophrenia—broadening theconcepts, pushing back the boundaries. Schizophr Res. 2005;79:5-13.13. Iritani S. Neuropathology of schizophrenia: a mini review.Neuropathology. 2007;27(6):604-608.14. Pearlson GD, Calhoun V. Structural and functional magnetic reso-nance imaging in psychiatric disorders. Can J Psychiatry. 2007;52:158-166.15. Wright IC, Rabe-Hesketh S, Woodruff PW, et al. Meta-analysis ofregional brain volumes in schizophrenia. Am J Psychiatry. 2000;57:16-25.16. Boos HB, Aleman A, Cahn W, et al. Brain volumes in relatives ofpatients with schizophrenia: a meta-analysis. Arch Gen Psychiatry.2007;64:297-304. 17. Harms MP, Wang L, Mamah D, et al Thalamic shape abnormalitiesin individuals with schizophrenia and their nonpsychotic siblings. JNeuroscie. 2007;27:13835-13842. 18. Weiden PJ, Buckley PF, Grody M. Understanding and treating “first-episode” schizophrenia. Psychiatr Clin North Am. 2007;30:481-510.19. Pantelis C, Velakoulis D, McGorry PD. Neuroanatomical abnormal-ities before and after onset of psychosis: a cross-sectional and longitudi-nal MRI comparison. Lancet. 2003;361:281-288.20. Murray RM, O’Callaghan E, Castle DJ, Lewis SW. A neurodevelop-mental approach to the classification of schizophrenia. Schizophr Bull.1992;18:319-332.21. Malaspina D. Schizophrenia: a neurodevelopmental or a neurode-generative disorder. J Clin Psychiatry. 2006;67:e07.22. Molina V, Reig S, Sanz J, et al. Association between relative tempo-ral and prefrontal sulcal cerebrospinal fluid and illness duration in schiz-ophrenia. Schizophr Res. 2002;58:305-312. 23. Waddington JL. Neuroimaging and other neurobiological indices inschizophrenia: relationship to measurement of functional outcome. Br JPsychiatry. 2007;50(suppl):s52-s57.24. Kapur S, Remmington G. Dopamine D2 receptors and their role inatypical antipsychotic action: still necessary and may even be sufficient.Biol Psychiatry. 2001;50:873-883.25. Meador-Woodruff J, Klienman J. Neurochemistry of schizophrenia:glutamate abnormalities. In: Davis KL, Charey D, Coyle JT, Nemeroff C,eds. Neuropsychopharmacology: Fifth Generation of Progress. Lippincott,Williams and Wilkins: Philadelphia, PA; 2002. 26. Lehman AF, Lieberman JA, Dixon LB, et al. Practice guidelines forthe management of patients with schizophrenia, second edition. Am JPsychiatry. 2004;161(2 suppl):1-56.
27. Buckley PF. Factors that influence treatment success in schizophre-nia. J Clin Psychiatry. 2008;69:4-10 (in press). 28. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsy-chotic drugs in patients with chronic schizophrenia. N Engl J Med.2005;353:1209-1223.29. Meyer JM. Cardiovascular illness and hyperlipidemia in patientswith schizophrenia. In: Meyer JM, Nasrallah HA, eds. Medical Illness andSchizophrenia. Washington, DC: American Psychiatric Publishing;2003:53-80. 30. Newcomer JW. Antipsychotic medications: metabolic and cardio-vascular risk. J Clin Psychiatry. 2007;68(suppl 4):8-13.31. Moore TA, Buchanan B, Buckley P, et al. The Texas MedicationAlgorithm Project antipsychotic algorithm for schizophrenia: 2006update. J Clin Psychiatry. 2007;68:1751-1762. 32. Harvey PD, Cornblatt B. Pharmacological treatment of cognition inschizophrenia: an idea whose time has come. Am J Psychiatry.2008;165:163-165.33. Dolder CR, Lacro JP, Dunn LB, Jeste DV. Antipsychotic medicationadherence: is there a difference between typical and atypical agents? AmJ Psychiatry. 2002;159:103-108.34. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factorsfor medication non-adherence in patients with schizophrenia. J ClinPsychiatry. 2002;63:892-909.35. Lauriello J, Bustillo J, Keith SJ. A critical review of research on psy-chosocial treatment of schizophrenia. Biol Psychiatry. 1999;46:1409-1417.36. Davidson L, Chinman M, Sells D, et al. Peer support among adults withmental illness: a report from the field. Schizophr Bull. 2006;32:443-450.37. Substance Abuse and Mental Health Services Administration.National consensus statement on mental health recovery. Rockville,MD: US Department of Health and Human Services; 2006. http://mentalhealth.samhsa.gov/publications/allpubs/sma05-4129/. AccessedDecember 20, 2006.
AHDB Stakeholder Perspective
The Approach to SchizophreniaPAYORS: Payors have had a difficult time
understanding how to approach schizophrenia. Inthe private sector, payors are accustomed to takingaction when possible. Employers expect contract-ed insurance companies to take action on theirbehalf whenever it makes sense. This disease state,however, does not lend itself to such a direct treat-ment approach. Patients with schizophrenia-relat-ed disorders are often reluctant to adhere to med-ication regimens. The results are often viewed inone of two ways: The sick member who avoidsmedication, or the sick member who takes expen-sive medications in a nonadherent manner—bothof which result in less-than-optimal health.
The major payors in this arena are state Medicaidagencies. Medicaid dollars pay for a substantialamount, perhaps half, of all prescriptions for schizo-phrenia, and must then pay for all related healthcare
Continued on page 22

costs. So what are the goals of these state agencies? Thestates seek to ensure that people have access to care.Unfortunately, effectiveness is secondary to access.
This theme seems to be consistent regardless ofwho the payor is—private or public. As we do forother disease states, the payor community shouldpush for a metric that demonstrates effective care forthe patient with schizophrenia. Granting access to arandom assortment of nonadherent monotherapiesand combination therapies is not the answer. Weshould strive to ensure that patients and theirproviders make valiant attempts at treatment proto-cols before abandoning them in favor of the nexthorse on the schizophrenia drug carousel.
In the 1970s, advocates fought against the use of“depo-products” (eg, injected haloperidol) on thebasis that some patients were overmedicated, andthat one did not have the ability to immediately
reverse the course of treatment if desired when usingsuch extended-release products. Over the past 35years, reverting to daily oral medications as standardtreatment has witnessed the reemergence of patientnonadherence. A call for a return to forced medica-tion has now been heard to redress the situation.Where shall it go from here?
PATIENTS: Ultimately, the direction should bedetermined by what is best for the patient. Neitherlegal advocates interested in outlawing extended-release medications as a civil rights infringement, norstate agencies willing to throw the entire medicinecabinet at patients without regard to medicationeffectiveness, should be making this decision.
Michael Schaffer, PharmDDirector of PharmacyHealthMarkets, Philadelphia, PA
Prior Authorization for AntipsychoticsComplicates Adherence
BENEFIT MANAGERS: The question of openversus restrictive access to the newer (atypical)antipsychotic medications lingers, as prior authoriza-tion (PA) and step-edit policies are being used tocontrol costs,1 and nonadherence remains a majorconcern. In his article, Dr Buckley notes that schizo-phrenia is the most serious mental condition, whichrequires optimal therapy.
Findings from a study just published in HealthAffairs and led by Dr Steven B. Soumerai of HarvardMedical School’s Department of Ambulatory Care andPrevention “provide strong evidence of both intendedand unintended consequences of the Maine PA poli-cy”2 implemented in a Medicaid program from July2003 through March 2004. Dr Soumerai and col-leagues compared antipsychotics use in the Maine pro-gram pre- and postimplementation of the PA policy;an open access Medicaid program in New Hampshirewas used as control. The Maine PA policy resulted ina 29% greater risk of treatment discontinuation com-pared with the period before implementing the PApolicy.2 No differences in discontinuation risk werefound in the New Hampshire program.
The authors concluded that “the most adverse clin-ical outcome was treatment discontinuation, which is
a strong predictor of acute psychotic episode, hospi-talization, and other negative clinical and economicoutcomes. Pharmacy savings were minimal.”2 Theyadmit that restrictive policies may control costs whenapplied to more homogeneous drug classes (eg, non -steroidal anti-inflammatory drugs or angiotensin-converting enzyme inhibitors), but because of markeddifferences in patients’ response to antipsychotics,such tools are not productive and can be harmfulwhen used for antipsychotics the authors say. In aninterview with Newswire, Dr Soumerai said, “Giventhe tremendous variation in individual responses tothese drugs as well as the devastating impact of treat-ment disruption on schizophrenic patients, a policythat pushes all patients toward a limited number ofpreferred drugs may do more harm than good.”3
More than 30% of Medicare Part D and Medicaidprograms have PA policies for antipsychotics.1,2
References1. Polinki JM, Wang PS, Fischer MA. Medicaid’s prior authorizationprogram and access to atypical antipsychotic medications. Health Aff.2007;26:750-760.2. Soumerai SB, Zhang F, Ross-Deganan D, et al. Use of atypicalantipsychotic drugs for schizophrenia in Maine Medicaid following apolicy change. Health Aff. 2008;27:w185-w195; DOI 10.1377/hlthaff.27.3.w185.3. Plasso A. Restrictive drug policies often cause schizophrenicpatients to discontinue medications. Newswire; April 1, 2008. www.PharmExec.findpharma.com. Accessed April 6, 2008.
AHDB Stakeholder Perspective Continued from page 21
CLINICAL
AMERICAN HEALTH & DRUG BENEFITS May 200822
Soaring healthcare
costs are only
the symptoms.
You’ve got
to start treating
the disease.
3RD Law of Healthonomics:
������������������������������������������������������������������������� ������� ����� �� ��� ���������� �������� ��������� ���� ���� ���������������������������������������������������������������������������������������������������������������������������������������������������������� ��������������������������������������������������������� ��� ��������������� ������ ������������ ������������ ��������������������������������������������������������������������������������������������������������������������������
����������������������������������www.CenterVBHM.com
Reference: 1.���������������������������������������������������������������������������������������������������������������������������������������������
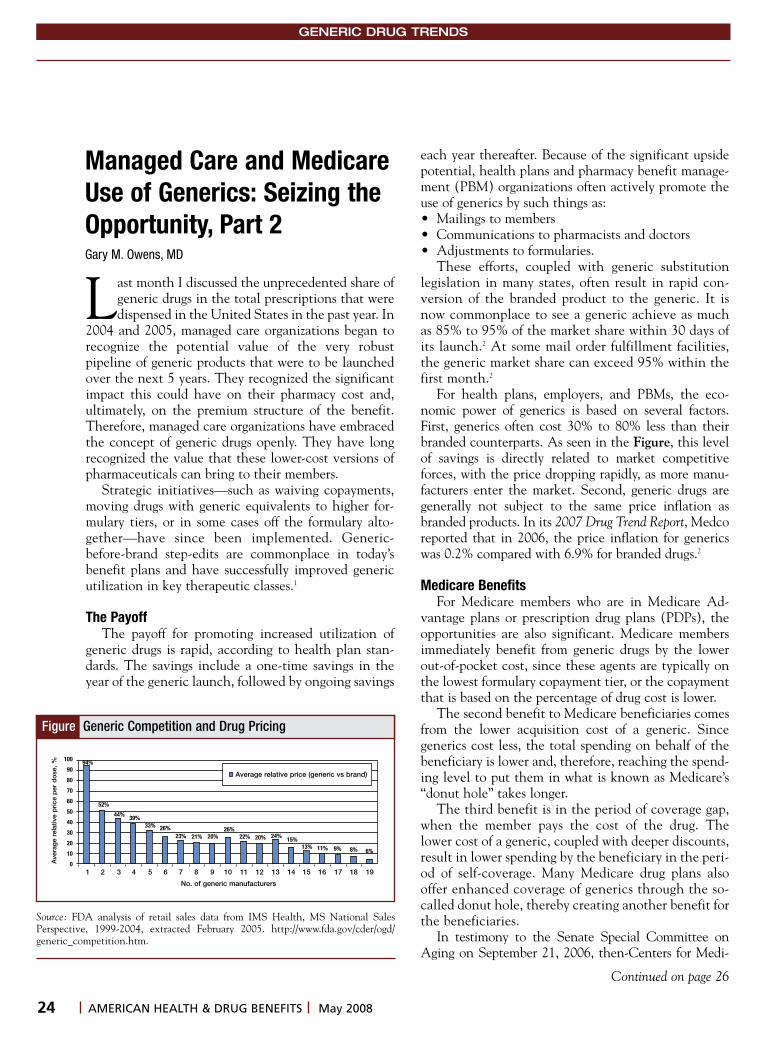
24 AMERICAN HEALTH & DRUG BENEFITS May 2008
GENERIC DRUG TRENDS
Managed Care and MedicareUse of Generics: Seizing theOpportunity, Part 2Gary M. Owens, MD
Last month I discussed the unprecedented share ofgeneric drugs in the total prescriptions that weredispensed in the United States in the past year. In
2004 and 2005, managed care organizations began torecognize the potential value of the very robustpipeline of generic products that were to be launchedover the next 5 years. They recognized the significantimpact this could have on their pharmacy cost and,ultimately, on the premium structure of the benefit.Therefore, managed care organizations have embracedthe concept of generic drugs openly. They have longrecognized the value that these lower-cost versions ofpharmaceuticals can bring to their members.
Strategic initiatives—such as waiving copayments,moving drugs with generic equivalents to higher for-mulary tiers, or in some cases off the formulary alto-gether—have since been implemented. Generic-before-brand step-edits are commonplace in today’sbenefit plans and have successfully improved genericutilization in key therapeutic classes.1
The PayoffThe payoff for promoting increased utilization of
generic drugs is rapid, according to health plan stan-dards. The savings include a one-time savings in theyear of the generic launch, followed by ongoing savings
each year thereafter. Because of the significant upsidepotential, health plans and pharmacy benefit manage-ment (PBM) organizations often actively promote theuse of generics by such things as: • Mailings to members• Communications to pharmacists and doctors• Adjustments to formularies.
These efforts, coupled with generic substitutionlegislation in many states, often result in rapid con-version of the branded product to the generic. It isnow commonplace to see a generic achieve as muchas 85% to 95% of the market share within 30 days ofits launch.2 At some mail order fulfillment facilities,the generic market share can exceed 95% within thefirst month.2
For health plans, employers, and PBMs, the eco-nomic power of generics is based on several factors.First, generics often cost 30% to 80% less than theirbranded counterparts. As seen in the Figure, this levelof savings is directly related to market competitiveforces, with the price dropping rapidly, as more manu-facturers enter the market. Second, generic drugs aregenerally not subject to the same price inflation asbranded products. In its 2007 Drug Trend Report, Medcoreported that in 2006, the price inflation for genericswas 0.2% compared with 6.9% for branded drugs.2
Medicare BenefitsFor Medicare members who are in Medicare Ad -
vantage plans or prescription drug plans (PDPs), theopportunities are also significant. Medicare membersimmediately benefit from generic drugs by the lowerout-of-pocket cost, since these agents are typically onthe lowest formulary copayment tier, or the copaymentthat is based on the percentage of drug cost is lower.
The second benefit to Medicare beneficiaries comesfrom the lower acquisition cost of a generic. Sincegenerics cost less, the total spending on behalf of thebeneficiary is lower and, therefore, reaching the spend-ing level to put them in what is known as Medicare’s“donut hole” takes longer.
The third benefit is in the period of coverage gap,when the member pays the cost of the drug. Thelower cost of a generic, coupled with deeper discounts,result in lower spending by the beneficiary in the peri-od of self-coverage. Many Medicare drug plans alsooffer enhanced coverage of generics through the so-called donut hole, thereby creating another benefit forthe beneficiaries.
In testimony to the Senate Special Committee onAging on September 21, 2006, then-Centers for Medi -
Figure Generic Competition and Drug Pricing
Source: FDA analysis of retail sales data from IMS Health, MS National SalesPerspective, 1999-2004, extracted February 2005. http://www.fda.gov/cder/ogd/generic_competition.htm.
No. of generic manufacturers
Ave
rag
e re
lativ
e p
rice
per
do
se, %
100
90
80
70
60
50
40
30
20
10
01 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
94%
6%8%9%11%13%15%
24%20%22%26%
20%21%23%26%33%
39%44%
52%
Average relative price (generic vs brand)
Continued on page 26

Global Resources.Uncompromising Standards.
800-RX-MYLAN
www.mylan.com
©2008 Mylan Inc. MYNMKT202
Over the past year, Mylan has
blossomed into one of the largest
generic companies in the world—
with operations in more than 90
countries. By acquiring the Generics
Business of Merck KGaA, we have
dramatically diversified our product
portfolio into new therapeutic areas,
dosage forms and delivery systems.
As we expand beyond our shores,
we take with us knowledge and
expertise gained for more than 45
years. We recognize the trust that
pharmacists place in Mylan Products,
that’s why we will continue to do
what we do best . . . make proven
medicine more affordable for the
patients who need them.

26 AMERICAN HEALTH & DRUG BENEFITS May 2008
GENERIC DRUG TRENDS
care & Medicaid Administrator, Mark B. McClellan,MD, PhD, testified that, “There are early indicationsthat Medicare beneficiaries enrolled in Part D are rely-ing on generics to a greater extent than the U.S. pop-ulation as a whole. We would expect this utilizationtrend to continue, as more and more beneficiaries real-ize the significant savings available by switching togeneric drugs.”3 Dr McClellan added, “The ConsumersUnion found that beneficiaries with common chronicconditions who switch to generic or other therapeuti-cally equivalent medications can save between $2300and $5300 a year.”3
Generics in Benefit Design: Potential Consequences Less than 25 years ago the use of generic drugs was
relatively uncommon, with fewer than 20% of allprescriptions being filled with a generic product.4
Barriers to entry of the generic market were signifi-cantly altered in 1984, with the passage of theHatch-Waxman Act (see AHDB, April 2008, pages52-55). The past 10 years have seen significant real-ization of the benefits of this legislation, as billions ofdollars in sales of branded drugs have been convert-ed to generics. The public has benefited from moreavailability of these low-cost alternatives to brandeddrugs by seeing a significant decrease in the rate ofpharmaceutical-spending increase. In addition,Medicare beneficiaries who are enrolled in MedicareAdvantage plans or PDPs have taken full advantageof the savings that generics have to offer. One poten-tial consequence of this, however, may have been thedemise of the blockbuster small-molecule model inthe pharmaceutical industry.
The consequences of this development are stillunclear, but 2007 did witness the fewest US Food andDrug Administration approvals of new drugs since1983. In contrast, consumers in both commercial andMedicare plans have seen significant savings accrue tothem by switching to lower-cost generics. As noted lastmonth, in 2007 generic drugs accounted for 63% of allprescriptions written in this country.4 But this repre-sents only about 20% of the total pharmacy spendingon drugs5; therefore, there are still many opportunitiesfor savings using generic medications.
It is reasonable to expect continued emphasis, edu-cational efforts, and PBMs designed to encourage theuse of generic drugs in 2008 and beyond as a growingportion of the pharmacy market converts to generics. Itis also reasonable to expect continued pressure onpharmacy cost and continued efforts to help controlthis cost by the use of generics.
Conclusion: Specialty PharmacyOne large, untapped area of generic potential is the
biologic and specialty pharmacy area. The debate overthis issue will certainly intensify in the future. In themeantime, we can expect continued emphasis byhealth plans, PBMs, and benefit managers on the valueof generic medications in the pharmacy benefit. �
Disclosure StatementDr Owens is a consultant to Amgen, Genzyme, Novartis, and
Wyeth, and received an honorarium from Encysive.
References1. Atlantic Information Services [AIS]. Health plans try new tactics tospur generic drug utilization. Reprinted from the August 7, 2006, issueof Health Plan Week. http://www.aishealth.com/ManagedCare/GenBus/MCW_health_plans_tactics_generics.html. Accesssed January 21, 2008. 2. Medco Health Solutions. 2007 Drug Trend Report. 2007, vol 9. http://www.medco.com/art/pdf/Drug_Trend_2007.pdf. Accessed February 3, 2008.3. McClellan MB. Generic drug utilization in the Medicare prescriptiondrug benefit. Senate Special Committee on Aging, Washington, DC.September 21, 2006. http://www.hhs.gov/asl/testify/t060921.html.Accessed March 18, 2008.4. Frank RG. The ongoing regulation of generic drugs. N Engl J Med.2007;357(20):1993-1996.5. IMS Health. Generics market expected to soar to $80 billion by 2008.http://www.imshealth.com/ims/portal/front/articleC/0,2777,6599_40183881_52651243,00.html. Accessed February 3, 2008.
Dr Owens is President, Gary Owens Associates and formerchair of Pharmacy & Therapeutic Committees, IndependenceBlue Cross.
Unmanaged Moment
“He’s losing it. He just told the truth,the whole truth and nothing but the truth.”
Continued from page 24

29www.AHDBonline.com
BUSINESS
In the latter part of the 1990s, the annual increaserate in national spending for pharmaceutical med-ications ranged from 11% to 17%, overtaking the
growth rates for hospital care (3%-6%) and physicianservices (4%-7%), which had dominated the health-care industry in the 1970s.1 At the turn of the 21st cen-tury, this rate was expected to continue to climb butinstead had reached a peak by 2001-2002. And by2005, the increased spending rate fell to 6%—the low-est it had been since the 1970s.2 For the first 9 monthsof 2007, the increase rate was only 4.7%—slightlylower than the expected range between 5% and 7%.3
Current projections of increased prescription drugspending rate for 2008 are3:
• 5% to 7% in the outpatient setting• 12% to 14% in clinic-administered drugs• 4% to 6% for hospital drug expenditures.
This recent leveling-off can be attributed to severalfactors (many of them a direct result of opposite trendsin the previous decade), including4,5:• A smaller number of new drugs entering the market• Expirations of patents for several blockbuster drugs
in 2002-2003• Reductions in the use of several high-cost agents
because of safety concerns• Switching to nonprescription status for some fre-
quently used drugs• Lower price inflation for prescription drugs• Higher cost-sharing by consumers• The introduction of a Medicare prescription drug
benefit (Part D) in 2005.
Reasons for Shift in Prescription Drug SpendingTrends
The high rates of growth in the late 1990s are attrib-uted to 3 main factors—(1) increased overall utilization,
Trends in PharmaceuticalExpenditures: The Impact onDrug Benefit DesignJoanne LaFleur, PharmD, MSPHLeslie Fish, PharmDDiana I. Brixner, RPh, PhD
Annual national spending for pharmaceutical agents was increasing at a rapid paceduring the late 1990s and early part of the 21st century, outpacing increases in spendingon hospital care and on physician services, which had dominated the industry in the1970s. In the past few years, however, this trend has shifted, resulting in a lower growthrate in 2005. The reasons for these trends of increases and subsequent declines areexplained in this article, including the slower pace of increase in generics and the increas-ing role of biologic agents in the rate of pharmaceutical price inflation. The sharp increas-es in drug spending led to changes in prescription drug benefit designs that have not beenfully tested. The recent decline creates an opportunity for health plans to evaluate thevalue of current and new strategies and implement value-based benefit designs in accor-
dance with the shifting focus in healthcare toward value-based patient care. [AHDB, 2008;1(4):29-34.]
Dr LaFleur is Research Assistant Professor, University ofUtah Pharmacotherapy Outcomes Research Center, SaltLake City, UT; Dr Fish is Senior Director of PharmacyServices, Fallon Community Health Plan, Worcester, MA;and Dr Brixner is Associate Professor and Director,University of Utah Pharmacotherapy Outcomes ResearchCenter, Salt Lake City, UT.
Joanne LaFleur, PharmD,MSPH

30 AMERICAN HEALTH & DRUG BENEFITS May 2008
BUSINESS
(2) increased prescription drug prices, and (3) increaseduse of new and expensive drugs. The first factor, in -creased overall utilization, reflects both an increase inthe total US population and an increase in the per-capi-ta number of prescriptions consumed on an annual basis.From 1993 to 2000, the US population increased from256 million to 276 million.1 This population expansionhas continued and, according to the most recent Censusestimates, has just crossed the 300-million mark.6
During the same period, the average number of pre-scriptions per person also rose—from 7.3 to 10.4.1 Thisincrease in utilization per capita is the result of severalfactors, including an average annual increase of 14% inpromotional spending by pharmaceutical manufactur-ers between 1996 and 2000, as well as an increase inthe proportion of all consumers who are older than age65 years.1 The elderly are by far the largest consumersof prescription drugs, spending 2.7% of their income onprescriptions, compared to only 1% for the generalpopulation.1 This may also be partly explained by alower overall income for the elderly. Nonetheless, forthe period from 1993 to 2000, utilization changesaccounted for about one half of the overall increase inpharmaceutical spending.1
A second contributor to the high rates of increase inpharmaceutical spending has been the increase in pricesfor prescription drugs, which was clearly evident through-out the 1990s (Figure 1) and continued into the newcentury. In 1990, the average price for a prescription drugat a retail pharmacy was $22; by 2000 it had increased to$46.1 Hidden in this number is a striking increase in retailprices for brand-name drugs. The average retail price forgeneric drugs increased from $10 in 1990 to $19 in 1999,roughly a 90% increase, compared with the averageincrease in the retail price for brand-name drugs from $27in 1990 to $65 in 1999—an increase of 140%.1
From 1994 to 2005, prices in creased by an average of8.3% annually—more than triple the average annualinflation rate of 2.5% during that period.1 Over the pastseveral years, the increased availability and use of bio-logic drugs has been one cause of pharmaceutical priceinflation; biologics are used by only 0.2% of patients in
the United States but account for 8% oftotal medical costs in an insured pop-ulation.4 More recently, since theintroduction of Medicare Part D, thecost of medications used by theMedicare population has increasedfaster than inflation and cost-of-liv-ing adjustment for social security—by9.2%, which is nearly 4 times higherthan the average inflation rate overpast years.7
Between April 2006 and April2007, the cost increases for some ofthe most frequently prescribed Part Ddrugs were1: • 15% for escitalopram (Lexapro) • 5% for calcipotriene ointment
(Dovonex)
KEY POINTS� The annual increase rate in drug spending has been declin-
ing since 2005. Current projections suggest this trend willcontinue in 2008.
� People older than 65 are the largest consumers of prescrip-tion drugs—spending 2.7% of their income compared with1% in the general population.
� The growing use of biologics has contributed to pharma -ceutical price inflation; biologics are used by 0.2% ofpatients but account for 8% of total medical costs in aninsured population.
� The increase in prescription drug spending by private insur-ance in the late 1990s led to the targeting of prescriptiondrugs for managed plans to rein in costs, primarily by shift-ing costs to the patient.
� The decreased pressure on health plans to contain costs inthe coming years provides a great opportunity to evaluate for the first time the impact of cost-saving strategies onpatient outcomes and long-term costs.
� Value-based drug benefit design should lead to overall cost-efficiencies.
Used with permission from Kaiser Family Foundation.1,2 All rights reserved.
Figure 1 Average Retail Prescription Drug Prices, 1990-2000
Cost
, $
70
60
50
40
30
20
10
01990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000Generic Rx Brand-name Rx All Rx
10
27
22
11
30
24
12
34
26
13
35
27
14
37
29
15
40
30
16
45
33
17
50
36
17
54
38
18
61
42
19
65
46
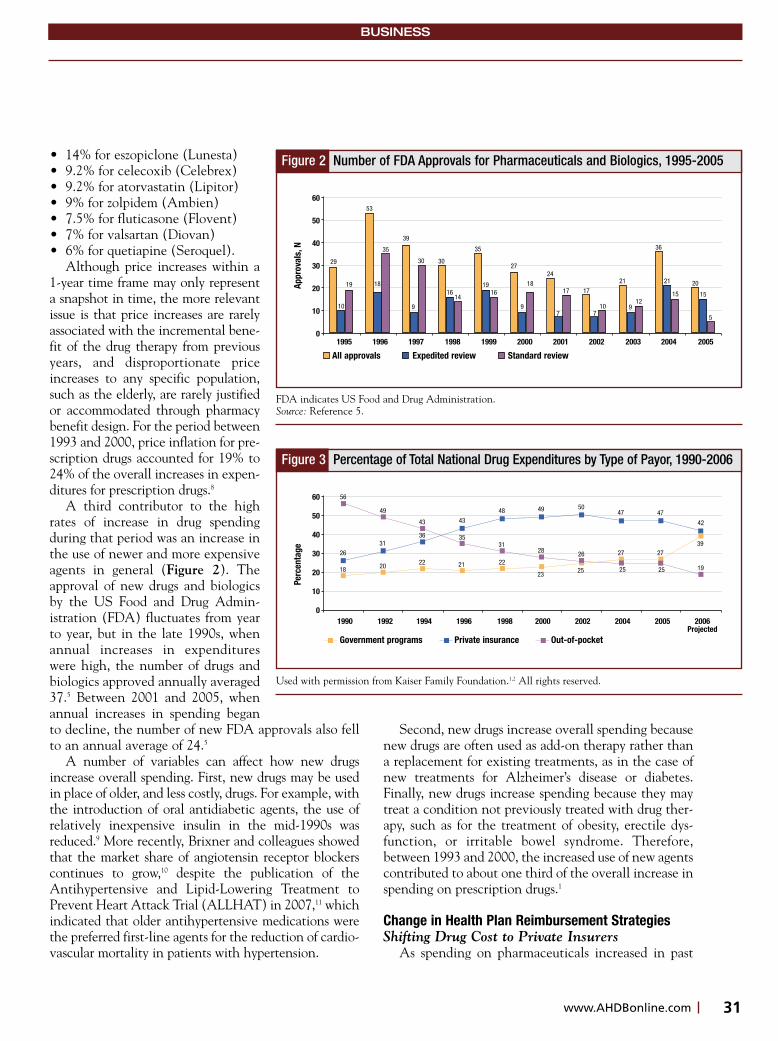
31www.AHDBonline.com
BUSINESS
• 14% for eszopiclone (Lunesta)• 9.2% for celecoxib (Celebrex)• 9.2% for atorvastatin (Lipitor) • 9% for zolpidem (Ambien)• 7.5% for fluticasone (Flovent)• 7% for valsartan (Diovan)• 6% for quetiapine (Seroquel).
Although price increases within a1-year time frame may only representa snapshot in time, the more relevantissue is that price increases are rarelyassociated with the incremental bene-fit of the drug therapy from previousyears, and disproportionate priceincreases to any specific population,such as the elderly, are rarely justifiedor accommodated through pharmacybenefit design. For the period between1993 and 2000, price inflation for pre-scription drugs accounted for 19% to24% of the overall in creases in expen-ditures for prescription drugs.8
A third contributor to the highrates of increase in drug spendingduring that period was an increase inthe use of newer and more expensiveagents in general (Figure 2). Theapproval of new drugs and biologicsby the US Food and Drug Admin -istration (FDA) fluctuates from yearto year, but in the late 1990s, whenannual increases in expenditureswere high, the number of drugs andbiologics approved annually averaged37.5 Between 2001 and 2005, whenannual increases in spending beganto decline, the number of new FDA approvals also fellto an annual average of 24.5
A number of variables can affect how new drugsincrease overall spending. First, new drugs may be usedin place of older, and less costly, drugs. For example, withthe introduction of oral antidiabetic agents, the use ofrelatively inexpensive insulin in the mid-1990s wasreduced.9 More recently, Brixner and colleagues showedthat the market share of angiotensin receptor blockerscontinues to grow,10 despite the publication of theAntihypertensive and Lipid-Lowering Treatment toPrevent Heart Attack Trial (ALLHAT) in 2007,11 whichindicated that older antihypertensive medications werethe preferred first-line agents for the reduction of cardio-vascular mortality in patients with hypertension.
Second, new drugs increase overall spending becausenew drugs are often used as add-on therapy rather thana replacement for existing treatments, as in the case ofnew treatments for Alzheimer’s disease or diabetes.Finally, new drugs increase spending because they maytreat a condition not previously treated with drug ther-apy, such as for the treatment of obesity, erectile dys-function, or irritable bowel syndrome. Therefore,between 1993 and 2000, the increased use of new agentscontributed to about one third of the overall increase inspending on prescription drugs.1
Change in Health Plan Reimbursement StrategiesShifting Drug Cost to Private Insurers
As spending on pharmaceuticals increased in past
Used with permission from Kaiser Family Foundation.1,2 All rights reserved.
Figure 3 Percentage of Total National Drug Expenditures by Type of Payor, 1990-2006
Perc
enta
ge
60
50
40
30
20
10
01990 1992 1994 1996 1998 2000 2002 2004 2005 2006
ProjectedGovernment programs Private insurance Out-of-pocket
56
49
26
18
31
20
43
36
22
43
35
21
48
31
22
49
28
23
50
26
25
47
27
25
47
27
25
42
39
19
FDA indicates US Food and Drug Administration.Source: Reference 5.
Figure 2 Number of FDA Approvals for Pharmaceuticals and Biologics, 1995-2005
Appr
oval
s, N
60
50
40
30
20
10
01995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
All approvals Expedited review Standard review
29
10
19 18
9
1614
1916
9
18
7
17
710 9
12
21
15 15
5
53
35
39
30 30
35
2724
17
21
36
20
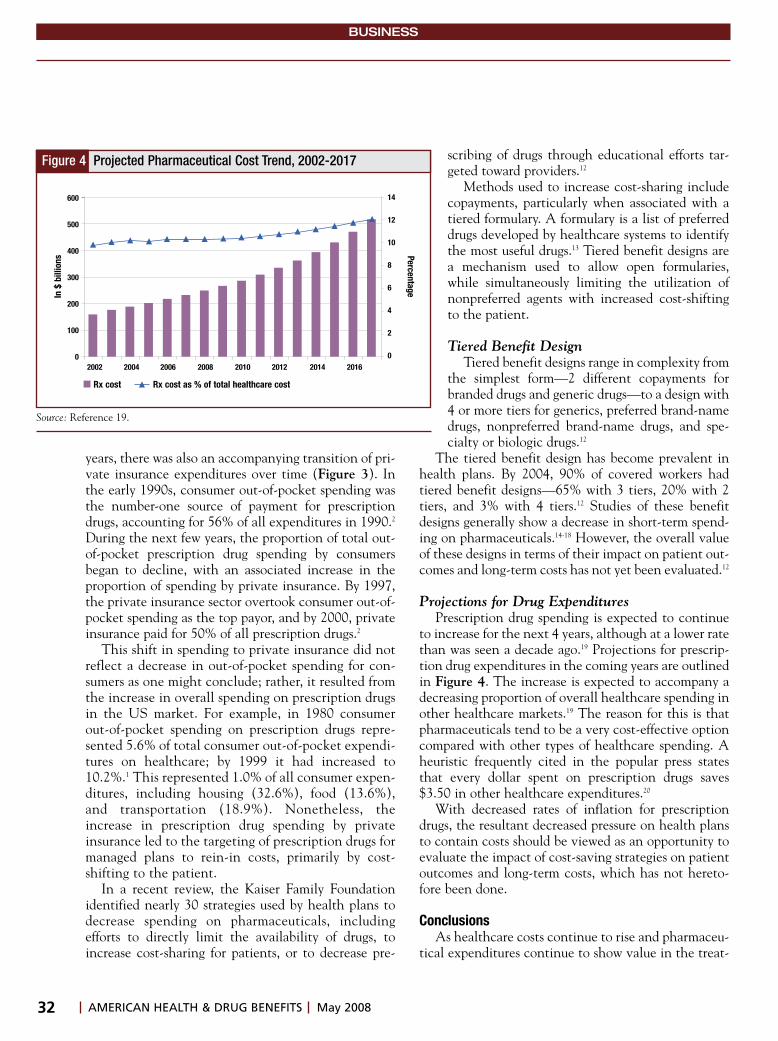
32 AMERICAN HEALTH & DRUG BENEFITS May 2008
BUSINESS
years, there was also an accompanying transition of pri-vate insurance expenditures over time (Figure 3). Inthe early 1990s, consumer out-of-pocket spending wasthe number-one source of payment for prescriptiondrugs, accounting for 56% of all expenditures in 1990.2
During the next few years, the proportion of total out-of-pocket prescription drug spending by consumersbegan to decline, with an associated increase in theproportion of spending by private insurance. By 1997,the private insurance sector overtook consumer out-of-pocket spending as the top payor, and by 2000, privateinsurance paid for 50% of all prescription drugs.2
This shift in spending to private insurance did notreflect a decrease in out-of-pocket spending for con-sumers as one might conclude; rather, it resulted fromthe increase in overall spending on prescription drugsin the US market. For example, in 1980 consumerout-of-pocket spending on prescription drugs repre-sented 5.6% of total consumer out-of-pocket expendi-tures on healthcare; by 1999 it had increased to10.2%.1 This represented 1.0% of all consumer expen-ditures, including housing (32.6%), food (13.6%),and transportation (18.9%). Nonetheless, theincrease in prescription drug spending by privateinsurance led to the targeting of prescription drugs formanaged plans to rein-in costs, primarily by cost-shifting to the patient.
In a recent review, the Kaiser Family Foundationidentified nearly 30 strategies used by health plans todecrease spending on pharmaceuticals, includingefforts to directly limit the availability of drugs, toincrease cost-sharing for patients, or to decrease pre-
scribing of drugs through educational efforts tar-geted toward providers.12
Methods used to increase cost-sharing includecopayments, particularly when associated with atiered formulary. A formulary is a list of preferreddrugs developed by healthcare systems to identifythe most useful drugs.13 Tiered benefit designs area mechanism used to allow open formularies,while simultaneously limiting the utilization ofnonpreferred agents with increased cost-shiftingto the patient.
Tiered Benefit DesignTiered benefit designs range in complexity from
the simplest form—2 different copayments forbranded drugs and generic drugs—to a design with4 or more tiers for generics, preferred brand-namedrugs, nonpreferred brand-name drugs, and spe-cialty or biologic drugs.12
The tiered benefit design has become prevalent inhealth plans. By 2004, 90% of covered workers hadtiered benefit designs—65% with 3 tiers, 20% with 2tiers, and 3% with 4 tiers.12 Studies of these benefitdesigns generally show a decrease in short-term spend-ing on pharmaceuticals.14-18 However, the overall valueof these designs in terms of their impact on patient out-comes and long-term costs has not yet been evaluated.12
Projections for Drug Expenditures Prescription drug spending is expected to continue
to increase for the next 4 years, although at a lower ratethan was seen a decade ago.19 Projections for prescrip-tion drug expenditures in the coming years are outlinedin Figure 4. The increase is expected to accompany adecreasing proportion of overall healthcare spending inother healthcare markets.19 The reason for this is thatpharmaceuticals tend to be a very cost-effective optioncompared with other types of healthcare spending. Aheuristic frequently cited in the popular press statesthat every dollar spent on prescription drugs saves$3.50 in other healthcare expenditures.20
With decreased rates of inflation for prescriptiondrugs, the resultant decreased pressure on health plansto contain costs should be viewed as an opportunity toevaluate the impact of cost-saving strategies on patientoutcomes and long-term costs, which has not hereto-fore been done.
ConclusionsAs healthcare costs continue to rise and pharmaceu-
tical expenditures continue to show value in the treat-
Source: Reference 19.
Figure 4 Projected Pharmaceutical Cost Trend, 2002-2017
In $
bill
ions
600
500
400
300
200
100
02002 2004 2006 2008 2010 2012 2014 2016
Rx cost Rx cost as % of total healthcare cost
14
12
10
8
6
4
2
0Percentage

33www.AHDBonline.com
BUSINESS
ment and prevention of disease, drug benefit designshould be expected to transition from a cost-manage-ment approach to a value-based approach. Patientsshould be expected to pay more when preference drivestheir decision. However, when legitimate health con-cerns, such as lack of efficacy or adverse events, can bedocumented, that evidence should support access toalternative medication choice, without financial bur-den to the patient. If access to drugs is determined bythe drugs’ value to defined populations, then value-based drug benefit design should lead to overall cost-efficiencies, by defining patient-target populations fordrug access and not by defining this access by cost. �
Disclosure Statement Dr Brixner received honoraria from Pfizer for the preparation of
this article.
References1. Henry J. Kaiser Family Foundation. Prescription Drug Trends—AChartbook Update. Kaiser Family Foundation. http://www.kff.org/rxdrugs/loader.cfm?url=/commonspot/security/getfile.cfm&PageID=13796. November 2001. Accessed March 22, 2008. 2. Henry J. Kaiser Family Foundation. Prescription Drug Trends. KaiserFamily Foundation. http://www.kff.org/rxdrugs/upload/3057_06.pdf.Updated May 2007. Accessed March 22, 2008.3. Hoffman JM, Shah ND, Vermeulen LC, et al. Projecting future drugexpenditures—2008. Am J Health Syst Pharm. 2008;65:234-253.4. Hoffman JM, Shah ND, Vermeulen LC, et al. Projecting future drugexpenditures—2006. Am J Health-Syst Pharm. 2006;63:123-138.5. US Food and Drug Administration. Center for Drug Evaluation andResearch Report to the Nation: 2005. Improving Public Health ThroughHuman Drugs. http://www.fda.gov/cder/reports/rtn/2005/rtn2005.PPT.Updated August 2006. Accessed March 22, 2008. 6. CNN.com. US population now 300 million and growing. CNN.com.http://www.cnn.com/2006/US/10/17/300.million.over/index.html.Updated October 17, 2006. Accessed March 22, 2008.7. Families USA. No Bargain: Medicare Drug Plans Deliver High Prices.Families USA Publication No. 07-101. http://www.familiesusa.org/assets/pdfs/no-bargain-medicare-drug.pdf. Accessed April 25, 2008.8. Hoffman JM, Shah ND, Vermeaulen LC, et al. Projecting future drugexpenditures—2007. Am J Health Syst Pharm. 2007;64:298-314.9. Hauber A, Gale EA. The market in diabetes. Diabetologia.2006;49:247-252.10. Brixner DI, Ghate SR, McAdam-Marx C, Maio V. Analysis of pri-mary care prescribing patterns of antihypertensive agents (AAs) beforeand after publication of the Antihypertensive and Lipid-LoweringTreatment to Prevent Heart Attack Trial (ALLHAT). Poster presentedat the International Society for Pharmacoeconomics and OutcomesResearch (ISPOR) 9th Annual European Congress, October 28-31,2006, Copenhagen, Denmark.11. Einhorn PT, Davis BR, Massie BM, et al, for the ALLHATCollaborative Research Group. The Antihypertensive and Lipid LoweringTreatment to Prevent Heart Attack Trial (ALLHAT) heart failure valida-tion study: diagnosis and prognosis. Am Heart J. 2007;153:42-53. 12. Henry J. Kaiser Family Foundation. Cost-containment strategies forprescription drugs: assessing the evidence in the literature.http://www.kff.org/rxdrugs/upload/Cost-Containment-Strategies-for-Prescription-Drugs-Assessing-The-Evidence-in-the-Literature-Report.pdf.Updated March, 2005. Accessed March 22, 2008. 13. American Society of Health-System Pharmacists. ASHP guidelines onformulary system management. Am J Health Syst Pharm. 1992;49:648-652.
14. Huskamp HA, Deverka PA, Epstein AM, et al. The effect of incen-tive-based formularies on prescription-drug utilization and spending. NEngl J Med. 2003;349:2224-2232.15. Joyce GF, Escarce JJ, Solomon MD, Goldman DP. Employer drugbenefit plans and spending on prescription drugs. JAMA. 2002;288:1733-1739.16. Kamal-Bahl S, Briesacher B. How do incentive-based formulariesinfluence drug selection and spending for hypertension? Health Aff(Millwood). 2004;23:227-236.17. Motheral B, Fairman KA. Effect of a three-tier prescription copay onpharmaceutical and other medical utilization. Med Care. 2001;39:1293-1304.18. Rector TS, Finch MD, Danzon PM, et al. Effect of tiered prescrip-tion copayments on the use of preferred brand medications. Med Care.2003;41:398-406.19. Keehan S, Sisko A, Truffer C, et al. Health spending projectionsthrough 2017: the baby boom generation is coming to Medicare. HealthAff. 2008;27:w145-w155.20. Pear R. Future bleak for bill to keep health records confidential. NewYork Times; 1999:A12.
For inquiries or comments, please [email protected].
AHDB Stakeholder Perspective
Drug Expenditures’ Impact on Benefit Design
HEALTH PLANS: Commercially sponsoredhealth plans remain focused on aggressive cost-management strategies for healthcare services thatmake sense to all stakeholders. As a premise forfacilitating change, the authors may be naïve aboutthe window of opportunity to introduce new solu-tions for healthcare expenditures, including phar-maceuticals. Although there may some respite incost escalation as a result of brand blockbustersgoing generic, overall costs have not truly flattenedfrom a health plan sponsor’s perspective.
Current drug trends remain a concern, and alter-natives, such as value-based strategies, are increas-ing from an interest perspective but not from theperspective of adoption across the greater market-place. Some of the many issues associated with theconcept of value-based benefit design is a lack ofconsensus on what constitutes such value, as wellas what works for both the employee and theemployer; how to implement a value-based plan;and what program design is the best for optimaleconomic outcomes for any specific plan sponsor.
Employers and other plan sponsors are facing arecessionlike economy in the United States, along
Continued on page 34
with a multivariate set of factors that affect health-care costs, including the presidential election cycle.Furthermore, the impact of biologic drugs followedby nanotechnology will likely exert greater pressureon an existing pharmacy benefit system that does notappear to work for drug products, with cost of prod-uct expenditures 10- to 100-fold greater than the tra-ditional oral or topical pharmaceuticals used in themarket today.
BENEFIT MANAGERS: It is important for allstakeholders to address fundamental issues in thehealthcare market. A review of value-based drugbenefit design is reasonable and needs to be replicat-ed beyond a few success stories. Furthermore, thebasic premise of increased cost-efficiency throughefforts such as value-based plans or patient-segmenttargeting needs to be better understood. For example,some believe that patient segmentation throughmedical/scientific means, such as personalized
healthcare, could increase health spending and exac-erbate drug trends for the short-term, which canthreaten business survival. Another question is howcan we achieve appropriate patient segmentationthrough existing benefit programs or designs to pro-vide the needed cost-efficiencies in health plans thatwill include the value of pharmaceuticals?
Commenting or reporting on current trends andbenefit design can be a challenge for academicresearchers, as well as for healthcare benefit man-agers. Being aware of all the information and per-spectives available about medical or pharmacy pro-gram benefit performance, however, can only help alldecision makers in making better informed healthbenefit plan decisions.
F. Randy Vogenberg, RPh, PhDChief Strategic OfficerEmployer-based Pharmaceutical Strategies, LLC
AHDB Stakeholder Perspective Continued from page 33
Information for Authors
Manuscripts submitted to American Health & Drug Benefits(AHDB) must be original and must not have been published previ-ously, either in print or in electronic form. Manuscripts cannot besubmitted elsewhere while under consideration by AHDB.
To be considered for publication, manuscripts must adhere tothe format described in this document. All manuscripts are subjectto peer review, and acceptance is based on that review. If accept-ed, authors will be notified of any recommended revisions. Therevised manuscript should be resubmitted in its entirety, with allchanges made.
Routine editorial changes will be made to conform to housestyle, following the AMA Manual of Style, 10th ed. (New York, NY:Oxford University Press, 2007). The edited manuscript is sent tothe author for a final review and approval. Time from submission topublication is generally 3 to 5 months.
COPYRIGHT/DISCLOSUREAuthors are required to sign a Copyright Transfer Form, assign-
ing all copyrights to Engage Healthcare Communications, LLC,publisher of AHDB, as well as a Financial Disclosure Form, disclos-ing any financial interests or potential conflict of interest involvingthe materials discussed in the manuscript.
MANUSCRIPT FORMAT• Title page should have a proper title for the article and list the
names, titles, and affiliations of all authors. Also list the name,
address, telephone number, and e-mail address of the correspon-ding author
• A 200-word Abstract• Conclusion • Double space the entire manuscript and number pages • Cite all Tables and Figures in the text, but place the actual
graphic elements at the end of the article; type all figure headsand captions in a Word format
• References: use 25-30 current, post-1990 references, cited in thetext but listed at the end of the manuscript. Avoid automaticnumbering or footnote/endnote features
• Length of article: 2500-3000 words, plus tables and figures • Save all Figures or images as individual files, at high resolution
(300 dpi), as jpg, tiff, or eps. Images not saved appropriately orsaved within the Word document will delay the peer-reviewprocess significantly.
PERMISSIONS Authors must secure a written permission from the original pub-
lisher for any previously published (online or in print) Table orFigure. Provide the source with each element.
HOW TO SUBMIT Save the manuscripts as a Word file and attach individual files for
each image used in the article, saved as an image file (eg, jpeg, tif, eps).Submit the manuscript electronically to: [email protected]. For assistance with submission, call 732-992-1892.
BUSINESS
AMERICAN HEALTH & DRUG BENEFITS May 200834
For many patients with schizophrenia
Gaps in medication can compromise their progress …
RISPERDAL CONSTA helps to keep them on solid footingRISPERDAL CONSTA, while not guaranteeing adherence, allows you to recognize and intervene when a patient misses a dose
© Ortho-McNeil-Janssen Pharmaceuticals, Inc. 2008
March 2008 01CS851R101CS921
RISPERDAL® CONSTA® (risperidone) long-acting injection is indicated for the treatment of schizophrenia.
IMPORTANT SAFETY INFORMATION FOR RISPERDAL CONSTA
Increased Mortality in Elderly Patients with Dementia-Related Psychosis
Elderly patients with dementia-related psychosis treated with atypical antipsychotic drugs are at an increased risk of death compared to placebo. Analyses of 17 placebo-controlled trials (modal duration of 10 weeks) in these patients revealed a risk of death in the drug-treated patients of between 1.6 to 1.7 times that seen in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. RISPERDAL® CONSTA® (risperidone) is not approved for the treatment of patients with dementia-related psychosis.
Commonly Observed Adverse Events for RISPERDAL CONSTA: Treatment-emergent adverse events with an incidence of 5% or greater in at least one of the RISPERDAL CONSTA groups (25 mg or 50 mg) and at least twice that of placebo were: somnolence, akathisia, Parkinsonism, dyspepsia, constipation, dry mouth, fatigue, and weight increase.
Hyperglycemia and Diabetes: Hyperglycemia, some cases extreme and associated with ketoacidosis, hyperosmolar coma or death has been reported in patients treated with atypical antipsychotics (APS), including RISPERDAL CONSTA. Patients starting treatment with APS who have or are at risk for diabetes should undergo fasting blood glucose testing at the beginning of and during treatment. Patients who develop symptoms of
hyperglycemia should also undergo fasting blood glucose testing.
Tardive Dyskinesia (TD): TD is a syndrome of potentially irreversible, involuntary, dyskinetic movements that may develop in patients treated with antipsychotic medications. The risk of developing TD and the likelihood that dyskinetic movements will become irreversible are believed to increase with duration of treatment and total cumulative dose. Elderly patients appeared to be at increased risk for TD. Prescribing should be consistent with the need to minimize the risk of TD. The syndrome may remit, partially or completely, if antipsychotic treatment is withdrawn.
Neuroleptic Malignant Syndrome (NMS): NMS, a potentially fatal symptom complex, has been reported with the use of antipsychotic medications, including RISPERDAL CONSTA. Clinical manifestations include muscle rigidity, fever, altered mental status and evidence of autonomic instability (see full Prescribing Information). Management should include immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy, intensive symptomatic treatment and medical monitoring, and treatment of any concomitant serious medical problems.
Cerebrovascular Adverse Events (CAEs): CAEs, including fatalities, have been reported in elderly patients with dementia-related psychosis taking oral risperidone in clinical trials. The incidence of CAEs with risperidone was significantly higher than with placebo. RISPERDAL CONSTA is not approved for treating these patients.
Extrapyramidal Symptoms (EPS): The overall incidence of EPS-related adverse events in patients treated with 25 mg and 50 mg of RISPERDAL CONSTA and placebo, respectively, were akathisia (2%, 9%, 4%), Parkinsonism* (4%, 10%, 3%) and tremor (0%, 3%, 0%). *Bradykinesia, extrapyramidal disorder, and hypokinesia.
Weight Gain: In a 12-week trial, the percentage
of patients experiencing weight gain (>7% of baseline body weight) was 6% placebo versus 9%RISPERDAL CONSTA.
Orthostatic Hypotension: RISPERDAL CONSTA may induce orthostatic hypotension associated with dizziness, tachycardia, and in some patients, syncope, especially during the initial dose-titration period. Monitoring should be considered in patients for whom this may be of concern. RISPERDAL CONSTA should be used with caution in patients with known cardiovascular disease, and conditions that would predispose patients to hypotension.
Potential for Cognitive and Motor Impairment: RISPERDAL CONSTA has the potential to impair judgment, thinking, or motor skills. Patients should be cautioned about operating hazardous machinery, including motor vehicles, until they are reasonably certain that RISPERDAL CONSTA does not affect them adversely.
Maintenance Treatment: Patients should be periodically reassessed to determine the need for continued treatment.
Please see accompanying brief summary of full Prescribing Information, including Boxed Warning, for RISPERDAL CONSTA.
Visit our Web site at risperdalconsta.com
IN M
E N TA L H E A
LT
H
CELE
BRATING 50 YEAR
S
TM
INDICATIONS AND USAGE: RISPERDAL® CONSTA® (risperidone) is indicated for the treatment ofschizophrenia.CONTRAINDICATIONS: RISPERDAL® CONSTA® (risperidone) is contraindicated in patients with aknown hypersensitivity to the product or any of its components.WARNINGS: Increased Mortality in Elderly Patients with Dementia-Related Psychosis: Elderlypatients with dementia-related psychosis treated with atypical antipsychotic drugs are at anincreased risk of death compared to placebo. RISPERDAL® CONSTA® (risperidone) is notapproved for the treatment of dementia-related psychosis (see Boxed Warning). NeurolepticMalignant Syndrome (NMS): A potentially fatal symptom complex sometimes referred to asNeuroleptic Malignant Syndrome (NMS) has been reported with antipsychotic drugs. Clinicalmanifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, and evidence ofautonomic instability. Other signs may include elevated creatinine phosphokinase, myoglobinuria(rhabdomyolysis), and acute renal failure. Management should include: discontinuation of theantipsychotic and other drugs not essential to therapy; intensive symptomatic treatment and medicalmonitoring; and treatment of other serious medical problems. If a patient requires antipsychotic drugsafter recovery from NMS, the reintroduction of drug therapy should be carefully considered. Thepatient should be carefully monitored, since recurrences have been reported. Tardive Dyskinesia: Asyndrome of potentially irreversible, involuntary, dyskinetic movements may develop in patients treatedwith antipsychotic drugs. The risk of developing and likelihood that it will become irreversible arebelieved to increase with the duration of treatment and the total cumulative dose. However, tardivedyskinesia can develop, after brief treatment periods at low doses. There is no known treatment forestablished cases of tardive dyskinesia, although it may remit, partially or completely, if theantipsychotic is withdrawn. Prescribing should be in a manner to minimize the occurrence. In patientswho require chronic treatment, the smallest dose and the shortest duration of treatment producing asatisfactory clinical response should be sought. The need for continued treatment should bereassessed periodically. If signs and symptoms should appear drug discontinuation should beconsidered. Cerebrovascular Adverse Events, Including Stroke, in Elderly Patients withDementia-Related Psychosis: Cerebrovascular adverse events (e.g., stroke, transient ischemicattack), including fatalities, were reported in patients (mean age 85 years; range 73-97) in trials of oralrisperidone in elderly patients with dementia-related psychosis. In placebo-controlled trials, there wasa significantly higher incidence of cerebrovascular adverse events in patients treated with oralrisperidone compared to patients treated with placebo. RISPERDAL® CONSTA® is not approved forthe treatment of patients with dementia-related psychosis. (See also Boxed WARNING, WARNINGS:Increased Mortality in Elderly Patients with Dementia-Related Psychosis.) Hyperglycemia andDiabetes Mellitus: Hyperglycemia, in some cases extreme and associated with ketoacidosis orhyperosmolar coma or death, has been reported in patients treated with atypical antipsychoticsincluding RISPERDAL®. Patients with an established diagnosis of diabetes mellitus who are startedon atypical antipsychotics should be monitored regularly for worsening of glucose control. Patientswith risk factors for diabetes mellitus who are starting treatment with atypical antipsychotics shouldundergo fasting blood glucose testing at the beginning of treatment and periodically during treatment.PRECAUTIONS: General: Administration: RISPERDAL® CONSTA® should be injected into thegluteal muscle, and care must be taken to avoid inadvertent injection into a blood vessel. (SeeDOSAGE AND ADMINISTRATION in full PI, and ADVERSE REACTIONS – Postintroduction Reports[retinal artery occlusion].) Orthostatic Hypotension: RISPERDAL® CONSTA® (risperidone) mayinduce orthostatic hypotension associated with dizziness, tachycardia, and in some patients, syncope,probably reflecting its alpha-adrenergic antagonistic properties. Syncope was reported in 0.8%(12/1499 patients) of patients treated with RISPERDAL® CONSTA® in multiple-dose studies. Patientsshould be instructed in nonpharmacologic interventions that help to reduce the occurrence oforthostatic hypotension (e.g., sitting on the edge of the bed for several minutes before attempting tostand in the morning and slowly rising from a seated position). RISPERDAL® CONSTA® should beused with particular caution in (1) patients with known cardiovascular disease (history of myocardialinfarction or ischemia, heart failure, or conduction abnormalities), cerebrovascular disease, andconditions which would predispose patients to hypotension, e.g., dehydration and hypovolemia, and(2) in the elderly and patients with renal or hepatic impairment. Monitoring of orthostatic vital signsshould be considered in all such patients, and a dose reduction should be considered if hypotensionoccurs. Clinically significant hypotension has been observed with concomitant use of oralRISPERDAL® and antihypertensive medication. Seizures: During premarketing testing, seizuresoccurred in 0.3% (5/1499 patients) of patients treated with RISPERDAL® CONSTA®. Therefore,RISPERDAL® CONSTA® should be used cautiously in patients with a history of seizures. Dysphagia:Esophageal dysmotility and aspiration have been associated with antipsychotic drug use. Aspirationpneumonia is a common cause of morbidity and mortality in patients with advanced Alzheimer’sdementia. RISPERDAL® CONSTA® and other antipsychotic drugs should be used cautiously inpatients at risk for aspiration pneumonia. (See also Boxed WARNING, WARNINGS: IncreasedMortality in Elderly Patients with Dementia-Related Psychosis.) Osteodystrophy and Tumors inAnimals: RISPERDAL® CONSTA® produced osteodystrophy in male and female rats in a 1-yeartoxicity study and a 2-year carcinogenicity study at a dose of 40 mg/kg administered IM every 2weeks. RISPERDAL® CONSTA® produced renal tubular tumors (adenoma, adenocarcinoma) andadrenomedullary pheochromocytomas in male rats in the 2-year carcinogenicity study at 40 mg/kgadministered IM every 2 weeks. In addition, RISPERDAL® CONSTA® produced an increase in amarker of cellular proliferation in renal tissue in males in the 1-year toxicity study and in renal tumor-bearing males in the 2-year carcinogenicity study at 40 mg/kg administered IM every 2 weeks.Neither the renal or adrenal tumors, nor osteodystrophy, were seen in studies of orallyadministered risperidone. Osteodystrophy was not observed in dogs at doses up to 14 times (basedon AUC) the IM MRHD in a 1-year toxicity study. The renal tubular and adrenomedullary tumors inmale rats and other tumor findings are described in more detail under PRECAUTIONS,Carcinogenicity, Mutagenesis, Impairment of Fertility. The relevance of these findings to human risk isunknown. Hyperprolactinemia: As with other drugs that antagonize dopamine D2 receptors,risperidone elevates prolactin levels and the elevation persists during chronic administration. Neitherclinical studies nor epidemiologic studies conducted to date have shown an association betweenchronic administration of this class of drugs and tumorigenesis in humans; the available evidence isconsidered too limited to be conclusive at this time. Potential for Cognitive and Motor Impairment:Somnolence was reported by 5% of patients treated with RISPERDAL® CONSTA® in multiple-dosetrials. Patients should be cautioned about operating hazardous machinery, including automobiles, untilthey are reasonably certain that treatment with RISPERDAL® CONSTA® does not affect them
adversely. Priapism: Rare cases of priapism have been reported in patients treated withRISPERDAL® CONSTA®. Thrombotic Thrombocytopenic Purpura (TTP): A single case of TTP wasreported in a 28 year-old female patient receiving oral RISPERDAL® in a large, open premarketingexperience (approximately 1300 patients). She experienced jaundice, fever, and bruising, buteventually recovered after receiving plasmapheresis. The relationship to RISPERDAL® therapy isunknown. Antiemetic Effect: Risperidone has an antiemetic effect in animals; this effect may alsooccur in humans, and may mask signs and symptoms of overdosage with certain drugs or ofconditions such as intestinal obstruction, Reye’s syndrome, and brain tumor. Body TemperatureRegulation: Disruption of body temperature regulation has been attributed to antipsychotic agents.Suicide: The possibility of a suicide attempt is inherent in schizophrenia, and close supervision ofhigh-risk patients should accompany drug therapy. Use in Patients with Concomitant Illness:Clinical experience with RISPERDAL® CONSTA® in patients with certain concomitant systemicillnesses is limited. Patients with Parkinson's Disease or Dementia with Lewy Bodies who receiveantipsychotics, including RISPERDAL® CONSTA®, are reported to have an increased sensitivity toantipsychotic medications. Manifestations of this increased sensitivity have been reported to includeconfusion, obtundation, postural instability with frequent falls, extrapyramidal symptoms, and clinicalfeatures consistent with the neuroleptic malignant syndrome. Caution is advisable when usingRISPERDAL® CONSTA® in patients with diseases or conditions that could affect metabolism orhemodynamic responses. Increased plasma concentrations of risperidone and 9–hydroxyrisperidoneoccur in patients with severe renal impairment. Patients with renal or hepatic impairment should becarefully titrated on oral RISPERDAL® before treatment with RISPERDAL® CONSTA® is initiated at adose of 25 mg. A lower initial dose of 12.5 mg may be appropriate when clinical factors warrant doseadjustment, such as in patients with renal or hepatic impairment (see DOSAGE AND ADMINISTRATION– Dosage in Special Populations in full PI). Information for Patients: Physicians are advised todiscuss the following issues with patients for whom they prescribe RISPERDAL® CONSTA®.Orthostatic Hypotension: Patients should be advised of the risk of orthostatic hypotension andinstructed in nonpharmacologic interventions that help to reduce the occurrence of orthostatichypotension (e.g., sitting on the edge of the bed for several minutes before attempting to stand in themorning and slowly rising from a seated position). Interference With Cognitive and MotorPerformance: Because RISPERDAL® CONSTA® has the potential to impair judgment, thinking, ormotor skills, patients should be cautioned about operating hazardous machinery, includingautomobiles, until they are reasonably certain that treatment with RISPERDAL® CONSTA® does notaffect them adversely. Pregnancy: Patients should be advised to notify their physician if they becomepregnant or intend to become pregnant during therapy and for at least 12 weeks after the last injectionof RISPERDAL® CONSTA®. Nursing: Patients should be advised not to breast-feed an infant duringtreatment and for at least 12 weeks after the last injection of RISPERDAL® CONSTA®. ConcomitantMedication: Patients should be advised to inform their physicians if they are taking, or plan to take,any prescription or over-the-counter drugs, since there is a potential for interactions. Alcohol: Patientsshould be advised to avoid alcohol during treatment with RISPERDAL® CONSTA®. DrugInteractions: The interactions of RISPERDAL® CONSTA® and other drugs have not beensystematically evaluated. Given the primary CNS effects of risperidone, caution should be used whenRISPERDAL® CONSTA® is administered in combination with other centrally-acting drugs or alcohol.Because of its potential for inducing hypotension, RISPERDAL® CONSTA® may enhance thehypotensive effects of other therapeutic agents with this potential. RISPERDAL® CONSTA® mayantagonize the effects of levodopa and dopamine agonists. Amitriptyline did not affect thepharmacokinetics of risperidone or the active moiety. Cimetidine and ranitidine increased thebioavailability of risperidone by 64% and 26%, respectively. However, cimetidine did not affect theAUC of the active moiety, whereas ranitidine increased the AUC of the active moiety by 20%. Chronicadministration of clozapine with risperidone may decrease the clearance of risperidone.Carbamazepine and Other CYP 3A4 Enzyme Inducers: In a drug interaction study in schizophrenicpatients, 11 subjects received oral risperidone titrated to 6 mg/day for 3 weeks, followed by concurrentadministration of carbamazepine for an additional 3 weeks. During co-administration, the plasmaconcentrations of risperidone and its pharmacologically active metabolite, 9-hydroxyrisperidone, weredecreased by about 50%. Plasma concentrations of carbamazepine did not appear to be affected. Co-administration of other known CYP 3A4 enzyme inducers (e.g., phenytoin, rifampin, andphenobarbital) with risperidone may cause similar decreases in the combined plasma concentrationsof risperidone and 9-hydroxyrisperidone, which could lead to decreased efficacy of RISPERDAL® CONSTA®
treatment. At the initiation of therapy with carbamazepine or other known CYP 3A4 hepatic enzymeinducers, patients should be closely monitored during the first 4-8 weeks, since the dose ofRISPERDAL® CONSTA® may need to be adjusted. A dose increase, or additional oral RISPERDAL®,may need to be considered. On discontinuation of carbamazepine or other CYP 3A4 hepatic enzymeinducers, the dosage of RISPERDAL® CONSTA® should be re-evaluated and, if necessary,decreased. Patients may be placed on a lower dose of RISPERDAL® CONSTA® between 2 to 4 weeksbefore the planned discontinuation of carbamazepine or other CYP 3A4 enzyme inducers to adjust forthe expected increase in plasma concentrations of risperidone plus 9-hydroxyrisperidone. For patientstreated with the recommended dose of 25 mg RISPERDAL® CONSTA® and discontinuing fromcarbamazepine or other CYP 3A4 enzyme inducers, it is recommended to continue treatment with the25 mg dose unless clinical judgment necessitates lowering the RISPERDAL® CONSTA® dose to12.5 mg or necessitates interruption of RISPERDAL® CONSTA® treatment. (See also DOSAGE ANDADMINISTRATION in full PI.) The efficacy of the 12.5 mg dose has not been investigated in clinicaltrials. Fluoxetine and Paroxetine: Fluoxetine (20 mg QD) and paroxetine (20 mg QD), CYP 2D6inhibitors, have been shown to increase the plasma concentration of risperidone 2.5-2.8 fold and 3-9fold, respectively. Fluoxetine did not affect the plasma concentration of 9-hydroxyrisperidone.Paroxetine lowered the concentration of 9-hydroxyrisperidone by about 10%. When either concomitantfluoxetine or paroxetine is initiated or discontinued, the physician should re-evaluate the dose ofRISPERDAL® CONSTA®. When initiation of fluoxetine or paroxetine is considered, patients may beplaced on a lower dose of RISPERDAL® CONSTA® between 2 to 4 weeks before the planned start offluoxetine or paroxetine therapy to adjust for the expected increase in plasma concentrations ofrisperidone. When fluoxetine or paroxetine is initiated in patients receiving the recommended dose of25 mg RISPERDAL® CONSTA®, it is recommended to continue treatment with the 25 mg dose unlessclinical judgment necessitates lowering the RISPERDAL® CONSTA® dose to 12.5 mg or necessitatesinterruption of RISPERDAL® CONSTA® treatment. When RISPERDAL® CONSTA® is initiated inpatients already receiving fluoxetine or paroxetine, a starting dose of 12.5 mg can be considered. Theefficacy of the 12.5 mg dose has not been investigated in clinical trials. (See also DOSAGE ANDADMINISTRATION in full PI.) The effects of discontinuation of concomitant fluoxetine or paroxetinetherapy on the pharmacokinetics of risperidone and 9-hydroxyrisperidone have not been studied.Lithium: Repeated oral doses of risperidone (3 mg BID) did not affect the exposure (AUC) or peakplasma concentrations (Cmax) of lithium (n=13). Valproate: Repeated oral doses of risperidone (4 mgQD) did not affect the pre-dose or average plasma concentrations and exposure (AUC) of valproate(1000 mg/day in three divided doses) compared to placebo (n=21). However, there was a 20%increase in valproate peak plasma concentration (Cmax) after concomitant administration ofrisperidone. Digoxin: RISPERDAL® (0.25 mg BID) did not show a clinically relevant effect on thepharmacokinetics of digoxin. Drugs that Inhibit CYP 2D6 and Other CYP Isozymes: Risperidone ismetabolized to 9–hydroxyrisperidone by CYP 2D6, an enzyme that is polymorphic in the populationand that can be inhibited by a variety of psychotropic and other drugs (see CLINICALPHARMACOLOGY in full PI). Drug interactions that reduce the metabolism of risperidone to9–hydroxyrisperidone would increase the plasma concentrations of risperidone and lower theconcentrations of 9–hydroxyrisperidone. Analysis of clinical studies involving a modest number of poormetabolizers (n�;70 patients) does not suggest that poor and extensive metabolizers have differentrates of adverse effects. No comparison of effectiveness in the two groups has been made. In vitrostudies showed that drugs metabolized by other CYP isozymes, including 1A1, 1A2, 2C9, 2C19, and3A4, are only weak inhibitors of risperidone metabolism. There were no significant interactionsbetween risperidone and erythromycin (see CLINICAL PHARMACOLOGY in full PI). DrugsMetabolized by CYP 2D6: In vitro studies indicate that risperidone is a relatively weak inhibitor of
Increased Mortality in Elderly Patients with Dementia–Related PsychosisElderly patients with dementia-related psychosis treated with atypical antipsychotic drugsare at an increased risk of death compared to placebo. Analyses of seventeen placebocontrolled trials (modal duration of 10 weeks) in these patients revealed a risk of death in thedrug-treated patients of between 1.6 to 1.7 times that seen in placebo-treated patients. Overthe course of a typical 10 week controlled trial, the rate of death in drug-treated patients wasabout 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes ofdeath were varied, most of the deaths appeared to be either cardiovascular (e.g., heartfailure, sudden death) or infectious (e.g., pneumonia) in nature. RISPERDAL® CONSTA®
(risperidone) is not approved for the treatment of patients with Dementia-Related Psychosis.
BEFORE PRESCRIBING, PLEASE CONSULT COMPLETE PRESCRIBING INFORMATION OFWHICH THE FOLLOWING IS A BRIEF SUMMARY.

CYP 2D6. Therefore, RISPERDAL® CONSTA® is not expected to substantially inhibit the clearance ofdrugs that are metabolized by this enzymatic pathway. In drug interaction studies, oral risperidone didnot significantly affect the pharmacokinetics of donepezil and galantamine, which are metabolized byCYP 2D6. Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis - Oral:Carcinogenicity studies were conducted in Swiss albino mice and Wistar rats. Risperidone wasadministered in the diet at doses of 0.63, 2.5, and 10 mg/kg for 18 months to mice and for 25 monthsto rats. These doses are equivalent to 2.4, 9.4, and 37.5 times the oral maximum recommendedhuman dose (MRHD) for schizophrenia (16 mg/day) on a mg/kg basis, or 0.2, 0.75, and 3 times theoral MRHD (mice) or 0.4, 1.5, and 6 times the oral MRHD (rats) on a mg/m2 basis. A maximumtolerated dose was not achieved in male mice. There was a significant increase in pituitary glandadenomas in female mice at doses 0.75 and 3 times the oral MRHD on a mg/m2 basis. There was asignificant increase in endocrine pancreatic adenomas in male rats at doses 1.5 and 6 times the oralMRHD on a mg/m2 basis. Mammary gland adenocarcinomas were significantly increased in femalemice at all doses tested (0.2, 0.75, and 3 times the oral MRHD on a mg/m2 basis), in female rats at alldoses tested (0.4, 1.5, and 6 times the oral MRHD on a mg/m2 basis), and in male rats at a dose 6times the oral MRHD on a mg/m2 basis. Carcinogenesis - IM: RISPERDAL® CONSTA® wasevaluated in a 24-month carcinogenicity study in which SPF Wistar rats were treated every 2 weekswith IM injections of either 5 mg/kg or 40 mg/kg of risperidone. These doses are 1 and 8 times theMRHD (50 mg) on a mg/m2 basis. A control group received injections of 0.9% NaCl, and a vehiclecontrol group was injected with placebo microspheres. There was a significant increase in pituitarygland adenomas, endocrine pancreas adenomas, and adrenomedullary pheochromocytomas at 8times the IM MRHD on a mg/m2 basis. The incidence of mammary gland adenocarcinomas wassignificantly increased in female rats at both doses (1 and 8 times the IM MRHD on a mg/m2 basis). Asignificant increase in renal tubular tumors (adenoma, adenocarcinomas) was observed in male ratsat 8 times the IM MRHD on a mg/m2 basis. Plasma exposures (AUC) in rats were 0.3 and 2 times (at5 and 40 mg/kg, respectively) the expected plasma exposure (AUC) at the IM MRHD. The relevancefor human risk of the findings of prolactin-mediated endocrine tumors in rodents is unknown (seePRECAUTIONS - Hyperprolactinemia). Mutagenesis: No evidence of mutagenic potential for oralrisperidone was found. In addition, no evidence of mutagenic potential was found in the in vitro Amesreverse mutation test for RISPERDAL® CONSTA®. Impairment of Fertility: Oral risperidone (0.16 to5 mg/kg) was shown to impair mating, but not fertility, in Wistar rats in three reproductive studies atdoses 0.1 to 3 times the oral maximum recommended human dose. No mating and fertility studieswere conducted with RISPERDAL® CONSTA®. Pregnancy: Pregnancy Category C: The teratogenicpotential of oral risperidone was studied in three embryofetal development studies in Sprague-Dawleyand Wistar rats (0.63-10 mg/kg or 0.4 to 6 times the oral maximum recommended human dose[MRHD] on a mg/m2 basis) and in one embryofetal development study in New Zealand rabbits (0.31-5 mg/kg or 0.4 to 6 times the oral MRHD on a mg/m2 basis). The incidence of malformations was notincreased compared to control in offspring of rats or rabbits given 0.4 to 6 times the oral MRHD on amg/m2 basis. In three reproductive studies in rats (two peri/post-natal development studies and amultigenerational study), there was an increase in pup deaths during the first 4 days of lactation atdoses of 0.16-5 mg/kg or 0.1 to 3 times the oral MRHD on a mg/m2 basis. It is not known whetherthese deaths were due to a direct effect on the fetuses or pups or to effects on the dams. There wasno no-effect dose for increased rat pup mortality. In one peri/post-natal development study, there wasan increase in stillborn rat pups at a dose of 2.5 mg/kg or 1.5 times the oral MRHD on a mg/m2 basis.In a cross-fostering study in Wistar rats, toxic effects on the fetus or pups, as evidenced by a decreasein the number of live pups and an increase in the number of dead pups at birth (Day 0), and adecrease in birth weight in pups of drug-treated dams were observed. In addition, there was anincrease in deaths by Day 1 among pups of drug-treated dams, regardless of whether or not the pupswere cross-fostered. Risperidone also appeared to impair maternal behavior in that pup body weightgain and survival (from Days 1 to 4 of lactation) were reduced in pups born to control but reared bydrug-treated dams. These effects were all noted at the one dose of risperidone tested, i.e., 5 mg/kg or3 times the oral MRHD on a mg/m2 basis. No studies were conducted with RISPERDAL® CONSTA®.Placental transfer of risperidone occurs in rat pups. There are no adequate and well-controlled studiesin pregnant women. However, there was one report of a case of agenesis of the corpus callosum inan infant exposed to risperidone in utero. The causal relationship to oral RISPERDAL® therapy isunknown. Reversible extrapyramidal symptoms in the neonate were observed following postmarketinguse of risperidone during the last trimester of pregnancy. RISPERDAL® CONSTA® should be usedduring pregnancy only if the potential benefit justifies the potential risk to the fetus. Labor andDelivery: The effect of RISPERDAL® CONSTA® on labor and delivery in humans is unknown.Nursing Mothers: In animal studies, risperidone and 9–hydroxyrisperidone are excreted in milk.Risperidone and 9–hydroxyrisperidone are also excreted in human breast milk. Therefore, womenshould not breast-feed during treatment with RISPERDAL® CONSTA® and for at least 12 weeks afterthe last injection. Pediatric Use: RISPERDAL® CONSTA® has not been studied in children youngerthan 18 years old. Geriatric Use: In an open-label study, 57 clinically stable, elderly patients (e65years old) with schizophrenia or schizoaffective disorder received RISPERDAL® CONSTA® every 2weeks for up to 12 months. In general, no differences in the tolerability of RISPERDAL® CONSTA®
were observed between otherwise healthy elderly and nonelderly patients. Therefore, dosingrecommendations for otherwise healthy elderly patients are the same as for nonelderly patients.Because elderly patients exhibit a greater tendency to orthostatic hypotension than nonelderlypatients, elderly patients should be instructed in nonpharmacologic interventions that help to reducethe occurrence of orthostatic hypotension (e.g., sitting on the edge of the bed for several minutesbefore attempting to stand in the morning and slowly rising from a seated position). In addition,monitoring of orthostatic vital signs should be considered in elderly patients for whom orthostatichypotension is of concern (see PRECAUTIONS, DOSAGE AND ADMINISTRATION and CLINICALPHARMACOLOGY in full PI). Concomitant use with Furosemide in Elderly Patients withDementia-Related Psychosis: In placebo-controlled trials in elderly patients with dementia-relatedpsychosis, a higher incidence of mortality was observed in patients treated with furosemide plus oralrisperidone when compared to patients treated with oral risperidone alone or with oral placebo plusfurosemide. No pathological mechanism has been identified to explain this finding, and no consistentpattern for cause of death was observed. An increase of mortality in elderly patients with dementia-related psychosis was seen with the use of oral risperidone regardless of concomitant use withfurosemide. RISPERDAL® CONSTA® is not approved for the treatment of patients with dementia-related psychosis. (See Boxed WARNING, WARNINGS: Increased Mortality in Elderly Patientswith Dementia-Related Psychosis.)ADVERSE REACTIONS: Associated with Discontinuation of Treatment: In the 12-week, placebo-controlled trial, the incidence of schizophrenic patients who discontinued treatment due to an adverseevent was lower with RISPERDAL® CONSTA® (11%; 22/202 patients) than with placebo (13%; 13/98patients). Incidence in Controlled Trials: Commonly Observed Adverse Events in ControlledClinical Trials: Spontaneously reported, treatment-emergent adverse events with an incidence of 5%or greater in at least one of the RISPERDAL® CONSTA® groups (25 mg or 50 mg) and at least twicethat of placebo were: somnolence, akathisia, parkinsonism, dyspepsia, constipation, dry mouth,fatigue, weight increase. Dose Dependency of Adverse Events: Extrapyramidal Symptoms: Theoverall incidence of EPS-related adverse events (akathisia, dystonia, parkinsonism, and tremor) inpatients treated with 25 mg RISPERDAL® CONSTA® was comparable to that of patients treated withplacebo; the incidence of EPS-related adverse events was higher in patients treated with 50 mgRISPERDAL® CONSTA®. Dystonia: Class Effect: Symptoms of dystonia, prolonged abnormalcontractions of muscle groups, may occur in susceptible individuals during the first few days oftreatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing totightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. Whilethese symptoms can occur at low doses, they occur more frequently and with greater severity withhigh potency and at higher doses of first generation antipsychotic drugs. An elevated risk of acutedystonia is observed in males and younger age groups. Vital Sign Changes: RISPERDAL® isassociated with orthostatic hypotension and tachycardia (see PRECAUTIONS). In the placebo-controlled
trial, orthostatic hypotension was observed in 2% of patients treated with 25 mg or 50 mgRISPERDAL® CONSTA® (see PRECAUTIONS). Weight Changes: In the 12-week, placebo-controlledtrial, 9% of patients treated with RISPERDAL® CONSTA®, compared with 6% of patients treated withplacebo, experienced a weight gain of >7% of body weight at endpoint. Laboratory Changes: Thepercentage of patients treated with RISPERDAL® CONSTA® who experienced potentially importantchanges in routine serum chemistry, hematology, or urinalysis parameters was similar to or less thanthat of placebo patients. Additionally, no patients discontinued treatment due to changes in serumchemistry, hematology, or urinalysis parameters. ECG Changes: The electrocardiograms of 202schizophrenic patients treated with 25 mg or 50 mg RISPERDAL® CONSTA® and 98 schizophrenicpatients treated with placebo in a 12-week, double-blind, placebo-controlled trial were evaluated.Compared with placebo, there were no statistically significant differences in QTc intervals (usingFridericia’s and linear correction factors) during treatment with RISPERDAL® CONSTA®. PainAssessment and Local Injection Site Reactions: The mean intensity of injection pain reported bypatients using a visual analog scale (0 = no pain to 100 = unbearably painful) decreased in alltreatment groups from the first to the last injection (placebo: 16.7 to 12.6; 25 mg: 12.0 to 9.0; 50 mg:18.2 to 11.8). After the sixth injection (Week 10), investigator ratings indicated that 1% of patientstreated with 25 mg or 50 mg RISPERDAL® CONSTA® experienced redness, swelling, or induration atthe injection site. Other Events Observed During the Premarketing Evaluation ofRISPERDAL® CONSTA®: During its premarketing assessment, RISPERDAL® CONSTA® wasadministered to 1499 patients in multiple-dose studies. The conditions and duration of exposure toRISPERDAL® CONSTA® varied greatly, and included (in overlapping categories) open-label anddouble-blind studies, uncontrolled and controlled studies, inpatient and outpatient studies, fixed-doseand titration studies, and short-term and long-term exposure studies. The following reactions werereported: (Note: frequent adverse events are those occurring in at least 1/100 patients; infrequentadverse events are those occurring in 1/100 to 1/1000 patients; rare events are those occurring infewer than 1/1000 patients. It is important to emphasize that, although the reported events occurredduring treatment with RISPERDAL® CONSTA®, they were not necessarily caused by it.) PsychiatricDisorders: Frequent: anxiety, psychosis, depression, agitation, nervousness, paranoid reaction,delusion, apathy. Infrequent: anorexia, impaired concentration, impotence, emotional lability, manicreaction, decreased libido, increased appetite, amnesia, confusion, euphoria, depersonalization,paroniria, delirium, psychotic depression. Central and Peripheral Nervous System Disorders:Frequent: hypertonia, dystonia. Infrequent: dyskinesia, vertigo, leg cramps, tardive dyskinesiaa,involuntary muscle contractions, paraesthesia, abnormal gait, bradykinesia, convulsions, hypokinesia,ataxia, fecal incontinence, oculogyric crisis, tetany, apraxia, dementia, migraine. Rare: neurolepticmalignant syndrome. aIn the integrated database of multiple-dose studies (1499 patients withschizophrenia or schizoaffective disorder), 9 patients (0.6%) treated with RISPERDAL® CONSTA® (alldosages combined) experienced an adverse event of tardive dyskinesia. Body as a Whole/GeneralDisorders: Frequent: back pain, chest pain, asthenia. Infrequent: malaise, choking. GastrointestinalDisorders: Frequent: nausea, vomiting, abdominal pain. Infrequent: gastritis, gastroesophagealreflux, flatulence, hemorrhoids, melena, dysphagia, rectal hemorrhage, stomatitis, colitis, gastric ulcer,gingivitis, irritable bowel syndrome, ulcerative stomatitis. Respiratory System Disorders: Frequent:dyspnea. Infrequent: pneumonia, stridor, hemoptysis. Rare: pulmonary edema. Skin and AppendageDisorders: Frequent: rash. Infrequent: eczema, pruritus, erythematous rash, dermatitis, alopecia,seborrhea, photosensitivity reaction, increased sweating. Metabolic and Nutritional Disorders:Infrequent: hyperur icemia, hyperglycemia, hyperlipemia, hypokalemia, glycosuria,hypercholesterolemia, obesity, dehydration, diabetes mellitus, hyponatremia. Musculo-SkeletalSystem Disorders: Frequent: arthralgia, skeletal pain. Infrequent: torticollis, arthrosis, muscleweakness, tendinitis, arthritis, arthropathy. Heart Rate and Rhythm Disorders: Frequent:tachycardia. Infrequent: bradycardia, AV block, palpitation, bundle branch block. Rare: T-waveinversion. Cardiovascular Disorders: Frequent: hypotension. Infrequent: postural hypotension.Urinary System Disorders: Frequent: urinary incontinence. Infrequent: hematuria, micturitionfrequency, renal pain, urinary retention. Vision Disorders: Infrequent: conjunctivitis, eye pain,abnormal accommodation. Reproductive Disorders, Female: Frequent: amenorrhea. Infrequent:nonpuerperal lactation, vaginitis, dysmenorrhea, breast pain, leukorrhea. Resistance MechanismDisorders: Infrequent: abscess. Liver and Biliary System Disorders: Frequent: increased hepaticenzymes. Infrequent: hepatomegaly, increased SGPT. Rare: bilirubinemia, increased GGT, hepatitis,hepatocellular damage, jaundice, fatty liver, increased SGOT. Reproductive Disorders, Male:Infrequent: ejaculation failure. Application Site Disorders: Frequent: injection site pain. Infrequent:injection site reaction. Hearing and Vestibular Disorders: Infrequent: earache, deafness, hearingdecreased. Red Blood Cell Disorders: Frequent: anemia. White Cell and Resistance Disorders:Infrequent: lymphadenopathy, leucopenia, cervical lymphadenopathy. Rare: granulocytopenia,leukocytosis, lymphopenia. Endocrine Disorders: Infrequent: hyperprolactinemia, gynecomastia,hypothyroidism. Platelet, Bleeding and Clotting Disorders: Infrequent: purpura, epistaxis. Rare:pulmonary embolism, hematoma, thrombocytopenia. Myo-, Endo-, and Pericardial and ValveDisorders: Infrequent: myocardial ischemia, angina pectoris, myocardial infarction. Vascular(Extracardiac) Disorders: Infrequent: phlebitis. Rare: intermittent claudication, flushing,thrombophlebitis. Postintroduction Reports: The following adverse drug reactions have beenidentified during postapproval use of risperidone: agranulocytosis, anaphylactic reaction, angioedema,atrial fibrillation, diabetic ketoacidosis in patients with impaired glucose metabolism, hypothermia,inappropriate antidiuretic hormone secretion, intestinal obstruction, jaundice, mania, pancreatitis,priapism, QT prolongation, sleep apnea syndrome, and water intoxication. Adverse events reportedsince market introduction which were temporally (but not necessarily causally) related to oralRISPERDAL® therapy include the following: apnea, cerebrovascular disorder, includingcerebrovascular accident, diabetes mellitus aggravated, hyperglycemia, Parkinson’s diseaseaggravated, and pituitary adenomas. There have been rare reports of sudden death and/orcardiopulmonary arrest in patients receiving oral RISPERDAL®. A causal relationship with oralRISPERDAL® has not been established. It is important to note that sudden and unexpected deathmay occur in psychotic patients whether they remain untreated or whether they are treated with otherantipsychotic drugs. Retinal artery occlusion after injection of RISPERDAL® CONSTA® has beenreported during postmarketing surveillance. This has been reported in the presence of abnormalarteriovenous anastomosis.DRUG ABUSE AND DEPENDENCEControlled Substance Class: RISPERDAL® CONSTA® (risperidone) is not a controlled substance.For more information on symptoms and treatment of overdosage, see full PrescribingInformation.7519511B - US Patent 4,804,663 Revised February 2008
©Ortho-McNeil-Janssen Pharmaceuticals, Inc. 2008 01CS947B

38 AMERICAN HEALTH & DRUG BENEFITS May 2008
AMCP HIGHLIGHTS
The US economy is in a consumer-driven recessionthat is likely to be long and deep and that is usher-ing in dramatic changes in consumer spending pat-
terns. This will inevitably translate into healthcarechanges as well, according to Robert B. Reich. The 3major trends underlying current economic changes aredemographics, globalization, and technology.
Economic TrendsDemographics
The changing demographics of the US populationinfluence our healthcare. “The biggest problem we facein terms of the demographic time bomb is healthcare.Healthcare expenses are going up by double digits…and there is a grave, grave necessity and a groundswellfor some kind of reform,” Mr Reich points out. Unlikein 1994, when the Clinton administration attemptedto gain support for universal healthcare, health-relatedexpenditures are now rising faster with increasingcopayments and deductibles, and a much larger per-centage of the population is without health insurance.“This is the time, this is the hour, that people are real-ly ready for healthcare reform,” he says.
Changing demographics and healthcare costs com-prise only a portion of the set of circumstances leadingto the current recession, which is making the economythe number one issue in the upcoming presidentialelection. The previous 3 recessions were brought aboutbecause the Federal Reserve Board raised interest ratestoo high in an effort to fight inflation or becauseinvestors and businesses had overinvested in equip-ment and then pulled back on their spending.
In contrast, this recession is led by consumers whoare pulling back on spending. “The economy requirespeople to spend money to buy all the goods and servic-es that the economy produces,” Mr Reich notes. “AndAmerican consumers are deep in debt, deeper in debtthan we have ever seen before in the history of keepingdata on debt. They had been getting money out of theirhomes, treating their homes as piggy banks, refinancingthrough home equity loans. They can’t do that any-more” because of declining home prices and rising fueland food prices, as well as continued job loss.
The current median wage adjusted for inflation isjust slightly above where it was in 1970. The averageAmerican is already working 450 hours annually morethan the average European. All of the coping mecha-nisms to deal with low median wages have disappeared.“There really is no way in which people can keep onspending at the rate at which we are producing goodsand services,” Mr Reich explains. And healthcare costsare increasing.
The impending retirement of the baby boomersposes great challenges to social security, retirementplans, and to Medicare. Demographics interlock withglobalization and technology to shape the currenteconomy and our future healthcare.
Globalization“When most people think about globalization, they
think about trade, they think about ‘our’ companies ver-sus ‘their’ companies,” Mr Reich says. “Every big com-pany is becoming a global company, with suppliers com-ing from all over the world. American companies andeven American products have dissolved.” Even prod-ucts with an American nameplate are global products.
“Where things are made in the supply chain, wherecomponents come from, and where particular thingsare done” depend more and more on worldwide wagesand expertise. His own hip replacements were de -signed in France, manufactured in Germany, andinstalled with the expertise of American physicians.Expertise is crucial, and this is what Americans needto worry about.
Americans are very concerned that globalization isdirecting jobs to China, Southeast Asia, and other low-
Economic Trends Influencing Healthcare ReformBy Maude Campbell
Based on a keynote address by Robert B. Reich delivered at the Academy of Managed Care Pharmacy, April 17,2008, San Francisco, CA.
Robert B. Reich is Professor of Public Policy at the Universityof California at Berkeley, CA, and former Secretary of Laborunder President Clinton.
“There is a grave, grave necessity and agroundswell for some kind of reform.”

39www.AHDBonline.com
wage nations, but in reality “jobs are not all going tothe low-wage nations. If that is where jobs were going,Bangladesh would be the center of the world economyand it is not.” High-wage nations such as Germanycontinue to be major exporters even though theirwages are high. This is because “they have expertise,they have knowledge, they have skills. If we want toremain a high-wage economy, we have to educate our-selves, our children, and our grandchildren to makesure they have the productivity and the skill and theinnovative potential to actually justify a high standardof living in this global economy,” he emphasizes.
TechnologyTechnology is responsible for displacing more
Americans than globalization, according to Mr Reich.“The reason we are losing all the manufacturing jobs,the primary reason, is not because they are going toChina. The primary reason is that manufacturing isbecoming so efficient. In a factory in the United Statesthere are no people.” Although governors like toattract factories to their states, with tax abatementsand subsidies, the old assembly lines are gone. “The fac-tories are full to capacity, they are humming, but thereare only 10 people in the factory and they are techni-cians behind computer consoles controlling themachine tools and robots. We are not going to get a lotof new jobs out of factories.”
In the early 1900s more than half of Americansworked in agriculture; today, only 5% of Americans do.Mr Reich explains that this is “not because farming wasa big disaster, but because farming was a big success. Itis the same with manufacturing…. Even in China, thefactories that used to be inefficient—the state-run fac-tories are getting new technologies and they need fewerpeople.”
Most Americans are not unemployed, but their jobsdo not pay well. Jobs are in the local service economyand are sheltered from globalization, because they mustbe done in person. Again, the solution is education.“Globalization and technology are your friends if youare well educated, because globalization means youhave a greater and greater market for your insights, foryour knowledge, for your applications…. Globalizationand technology are your enemies if you don’t have ade-quate education,” Mr Reich suggests.
“Companies are going to be even more intenselycompeting for talented people and there is going to beeven greater pressure for immigration,” Mr Reichpoints out. “A debate on immigration has alreadyoccurred and it is only going to get louder.”
Healthcare ReformHealthcare consumers are experiencing dramatic
changes in the economy that present growing chal-lenges to delivering quality healthcare and pharmaceu-ticals. “There is going to be a change, and it won’t bedramatic, it will be incremental,” Mr Reich predicts.“The question is, will it be sensible?”
Because the aging population and rising healthcarecosts will put substantial change on Medicare, it is pre-dicted that there will be a change in law affectingMedicare and other health programs. “There is going tobe a change in law that enables government to use thisleverage with pharmaceutical companies to reduce theprice in bulk discounts of pharmaceuticals,” Mr Reichsays, adding that this will reduce the research anddevelopment incentives to the pharmaceutical indus-try. “Behind a lot of reform in healthcare are thesekinds of diabolical trade-offs in terms of how much weare, as a society, prepared to pay for new drugs, new pro-cedures, new equipment, and life-saving advances.”
Healthcare reform will also have to address preven-tion. “Prevention is a big part of it. Disease manage-ment is a big part of it. Using information technologybetter than we are using it to cut down on paperworktoday is a big part of it,” Mr Reich notes.
“The American healthcare system is the onlyhealthcare system in the world that I know of designedto avoid sick people.” He notes the pressure on someinsurers to cover only people who are low risk and lowexpense “and to try and avoid people with preexistingconditions or who are more expensive. There is also agreat deal spent on advertising, marketing, and on con-testing claims.” The question is how to get rid of allthese “reverse incentives,” he adds.
Mr Reich suggests that, “We are not going to go to sin-gle payer, but I do believe that giving people the backdoor to a low-cost kind of Chevrolet model healthcaresystem, because it is cheap, gathers enough people into itthat they have some bargaining leverage to get betterdeals. That might be the way we tiptoe toward whatmight ultimately be somewhat of a single payer system.” �
AMCP HIGHLIGHTS
“The American healthcare system is the onlyhealthcare system in the world...designed toavoid sick people.”
40 AMERICAN HEALTH & DRUG BENEFITS May 2008
AMCP HIGHLIGHTS
The 3 main areas fueling healthcare reform initia-tives are cost, access, and quality; these areashave given resonance to the progress of health-
care information technology (HIT), because cost,access, and quality cannot be fixed without an infor-mation infrastructure in place, David Brailer, MD, PhDtold the meeting attendees. “It is not so much that HITinfrastructure is so special or magic, it is because allthese areas need very specific, clinically valid, timely,patient-specific, actionable information.”
Progress has been made since the Bush administra-tion announced in 2004 that HIT would be a majoragenda item. Whereas in 2004 only 20% of hospitalshad electronic medical records (EMR) and 5% had sys-tems underway, today about 65% of US hospitals eitherhave an EMR system or are putting one in place.Physicians’ offices have progressed more slowly, withabout 20% to 25% having EMR compared with only10% in 2004. About 10% of physicians now use elec-tronic prescribing. A huge standards initiative is under-way to coordinate HIT across the different practices andhospitals to ensure system compatibility, said Dr Brailer,who predicts that in the next presidency, Medicare maymake EMR use a condition of participation.
A 2007 poll of Medicare beneficiaries showed that90% would prefer electronic prescriptions, allowingphysicians to check their coverage and review theirmedical history. “The American public really under-
stands that it is important that your information fol-lows you,” Dr Brailer observed.
But while the basic building blocks are comingtogether, enormous challenges remain before an effi-cient HIT infrastructure is created in which everyonehas an EMR that is connected to a central system. Theprimary issue is who will pay for it. The cost is estimat-ed to be $100 billion over a decade, but this pales whenwe think of total healthcare expenditures. The problemis that the doctors and hospitals who are paying for itare not the people who benefit from it, because ofMedicare’s obsolete reimbursement policies and fee-for-service medicine. “If you use a tool to improve efficien-cy and quality, your cost of care is lower, because youare seeing patients less frequently, they are beingadmitted less frequently, they are less likely to need labtests, and less imaging is being done…. All that [sav-ings] accrues to the payer.” It is clear, Dr Brailer says,that the federal government will not pay for it.
Privacy is another key challenge. Online EMRrepositories, such as Google Health and MicrosoftHealth Vault, are not coverage entities under theHealth Insurance Probability and Accountability Act(HIPAA) and, therefore, are not subject to state pri-vacy rules. Such entities could choose to make theinformation available to a pharmaceutical companydirectly or sell it for insurance underwriting use.“Privacy challenges are going to flare up in the nextcouple of years,” says Dr Brailer. “HIPAA was neverdesigned for a digital era.”
Americans understand that person-based portabilityof their health records has great benefits, and thatevery time they enter an emergency room they will notbe asked the same questions about what lab tests theyhave had or what imaging studies they have had done,but 3 aspects of HIPAA make this impossible, he says. 1. Patients cannot require to send their medical infor-
mation to a third party. Under HIPAA, the infor-mation can only be given to the patient. Many doc-tors or hospitals will not send it on the patient’sbehalf, even when the patient asks for it.
2. Providers have 120 days from the time of thepatient’s request to send the information, which
Technology in Healthcare: The Wave of the FutureBy Maude Campbell
Based on a presentation by David Brailer, MD, PhD, at the Academy of Managed Care Pharmacy AnnualMeeting, April 18, 2008, in San Francisco, CA.
Dr Brailer is founder and chairman of Health EvolutionPartners, a private equity fund focused on transforming thehealthcare industry. He served as the National Coordinator forHealth Information Technology under the Bush administration.
A 2007 poll of Medicare beneficiaries showedthat 90% would prefer electronic prescriptions.

41www.AHDBonline.com
makes this useless. “120 minutes is okay maybe,depending on what it is; 120 seconds is perfect.”
3. Information can be sent in whatever format pro -viders deem efficient; they do not have to put it inan electronic format. HIT would become if andwhen there is an economic and regulatory pathwayto portability, but this will require a comprehensiveredo of the old HIPAA policies, suggests Dr Brailer.
The HIT Revolution The transition into HIT is not only going to result
in people having an electronic record. “This chal-lenge that we have of trying to get the HIT revolutionstarted is going to turn around and become a key dis-ruptor of the brands we trust in healthcare, whetherthey are pharma, hospital, physician, or payor brands.It happens in every industry,” Dr Brailer says. “Look atwhat’s happened with retail. Most of the top levelretail brands in American of 15 years ago don’t exist.”He outlines some of the advantages and consequencesof HIT:
Remote monitoring. HIT will likely shift primarycare to the home. There is clear evidence that remotemonitoring systems using an array of very inexpensive,passive sensors can help keep patients out of nursinghomes for basic, low-skill care. Such systems monitorwhether someone is up and around, and whether theyhave done certain activities of daily living. These tech-nologies are now available for about $200. “The abilityto monitor compliance, utilization, and functional sta-tus anywhere we go is one of the key attributes of mov-ing forward,” he says.
Formulaic prescribing. The incorporation of EMRand HIT architecture will create a new class of prescrip-tions. For example, a patient with a urinary tract infec-tion with an EMR containing lab results, culture results,known medication allergies, and current medicationswill be able to walk up to a kiosk and walk away withthe appropriate treatment. “About 25% of prescriptionsare formulaic, they follow an automated thought processthat is driven by factual data, where subjective datahave some roll but not very much,” Dr Brailer says.“There may be regulatory barriers and people may beshocked if this happens, but they were shocked whenyou could walk up to a machine and take $200 out.”
Geographic control. HIT “will disrupt geographiccartels,” Dr Brailer says. “If I could describe healthcarein any way I’d say it is an industry comprised of geo-graphic cartels.” Hospital systems, payors, radiologygroups, and other specialty groups try to control theirgeographic markets. HIT will make it possible, for
example, to send radiology views remotely so that aradiologist in another location can read the results fora more competitive price. “This will start generating atremendous amount of increased radiology utilization,”he predicts. Dermatology and pathology are other like-ly areas that will be subject to similar disruption.
Super-consumers. Overall, 5% to 10% of consumersshape the market place. In healthcare, it is estimatedthat about 2% of Americans are active consumers, real-ly paying attention to their options and treatments ortreatment alternatives. Websites for specific chronicillnesses already exist where patients can talk to othersimilar patients and find out what they are being treat-ed with. The Internet induces a level of highlyinformed user, but not expert-mediated information. “
Globalization. “I think you will see globalization ofmedical services,” Dr Brailer says. “I’ve seen evidence ofpeople in other countries beginning to develop tools…todevelop and manage the medical operations of a healthplan, to be able to handle all the basic primary care dis-cussion with patients and the follow up, to be the peopleto respond to patient e-mails and help hammer out theirproblems….Much of it is happening in Asia from oneAsian country to another. The United States is not thecenterpiece of the global healthcare system.”
Improved care, reduced cost. Dr Brailer believesthat these innovations will “flip” healthcare on its headand form new ways “to deliver better care, morepatient-focused care, more integrated and cost-effec-tive care.” This will shift the power to patients “in wayswe haven’t even begun to imagine,” and generate newtypes of competition and decision making. One newfocus will be toward prevention.
“You will see two kinds of organizations. The onesthat stick their heads in the sand and say it is not goingto happen, and in my view, get torn asunder by it. Andyou’re going to see people who get it and are out aheadof it.” Some of the best health systems and physicianorganizations are already living this revolution in realtime and understand that it is not theory, but that it iswell underway, he concluded. �
AMCP HIGHLIGHTS
“The ability to monitor compliance, utilization,and functional status anywhere we go is oneof the key attributes of moving forward.”

42 AMERICAN HEALTH & DRUG BENEFITS May 2008
AMCP HIGHLIGHTS
Marisa Schlaifer, RPh, Director of PharmacyAffairs at the Academy of Managed CarePharmacy (AMCP) described a new medica-
tion therapy management (MTM) program that wasdeveloped by the AMCP to serve as a guide for MTMprograms for those designing and those purchasing anMTM program.
There are differences between MTM programs andMTM services, Dr Schlaifer explains. MTM programsare developed by health plans or other healthcaregroups and focus on optimizing therapeutic outcomes,whereas MTM services describe the components ofMTM programs delivered by healthcare professionals.MTM programs that implement effective MTM serv -ices enhance patient care and lead to better health,while decreasing healthcare system costs.
Drug therapy management programs are designed toensure that medications provided to eligible beneficiar-ies are used appropriately, thus reducing adverse eventsand optimizing therapeutic outcomes through im -proved medication use.
The MTM Validation ProjectThis new MTM initiative was intended to guide all
purchases of MTM programs, whether they are underMedicare Part D, commercial, or other settings. TheNational Committee for Quality Assurance (NCQA)was contracted to conduct the validation study. TheNCQA surveyed 20 representative Medicare Part D
and non–Medicare Part D programs and conducted in-depth site visits with 5 of the programs. Phase 1 con-sisted of telephone surveys with purchasers, pharma-cies, physicians, and consumer advocacy organizationsand regulators.
The NCQA found great variety among the pro-grams. Technology played a great role in all aspects ofthe MTM programs. In addition to regular mail andpersonal communications and interventions, they usedfax, the Internet, and e-mail. The features and opera-tional aspects were confirmed as realistic and valuableas a general direction for MTM programs. Among the20 programs surveyed, pharmacists were identified asthe primary deliverers and managers.
All the information gathered was then presented tothe AMCP Advisory Panel, which reviewed it andmade recommendations on how to modify the originaldocument. The MTM consensus document was pulledtogether by a broad array of stakeholders, includingrepresentatives from the American Association ofRetired Persons, AMCP, American Academy of FamilyPhysicians, American Geriatric Society, AmericanPharmacists Association, Veterans Administration,and National Business Coalition on Health, and repre-sentatives from health plans, pharmacy benefit man-agers, integrated health systems, and stand-alone MTMprograms. Many of the details of the program are con-tained in a January 2008 AMCP supplement.
Features of a Successful MTM Program Linda Baggett, RPh, CGP, and Kimberly Vernachio,
PharmD, Pharmacotherapy Specialists at Aetna,described the qualities of a Medicare MTM program atAetna that can serve as a model for implementing suc-cessful MTM programs. They began by noting that asignificant proportion of medical errors are related toadverse events, and hospitalizations are significantlyattributed to adverse events. The Institute of Medicinereported that as of January 2000, 44,000 to 98,000deaths occurred annually as a result of medical errors.Of these, approximately 7000 deaths annually are relat-
Medication Therapy Management Project—TheLatest Information for Managed Care PharmacyBy Sandy Paton
Based on a presentation by Marissa Schlaifer, RPh; Linda Baggett, RPh, CGP; and Kimberly Vernachio, PharmD,at the Academy of Managed Care Pharmacy Annual Meeting, April 17, 2008, San Francisco, CA.
Ms Schlaifer is Director of Pharmacy Affairs at the Academyof Managed Care Pharmacy; Ms Baggett and Dr Vernachioare Medicare Pharmacotherapy Specialists at Aetna, Inc.
Technology played a great role in all aspectsof the MTM programs.

43www.AHDBonline.com
ed to adverse drug reactions.1 Statistics point to adversedrug reactions as a serious problem, occurring in 1 of 5patient injuries or death per year.2
Drug-related issues are responsible for 33% of hospi-tal admissions in older patients, including misuse (eg,nonadherence, wrong indication, and contraindica-tion) and adverse drug reactions (eg, electrolyte imbal-ances from changes in cardiovascular medications).3
Aetna’s MTM program has been a work in progresssince 2006. Aetna has identified the following 7 keyfeatures that characterize a successful MTM program.Such a program should: • Be patient-centered• Use an interdisciplinary approach and be team-
based• Have effective communication among team mem-
bers • Clearly define the perspective on each issue regard-
ing population-based or individual perspective• Be flexible in design• Use an evidence-based medical approach• Promote its services; a good program does no good
unless others know about it.
From the start, Aetna assumed that the number ofdrugs a patient was taking would provide a strategy forintervention. This approach led to the development ofa screening algorithm. The number of prescriptionsquantitated the number of drug-related opportunitiesfor intervention. Members taking 14 or more drugswere considered the most complex members; however,polypharmacy turned out not to be the first issuerequiring attention. The number of drugs was not nec-essarily supportive of meaningful opportunities forintervention.
Identifying Risk GroupsProgram coordinators eventually differentiated clin-
ical risk groups based on medication (eg, anticoagulantuse, diabetes mellitus, congestive heart failure, demen-tia, asthma and chronic obstructive pulmonary disease,end-stage renal disease, and rheumatoid arthritis).
The highest risk group was patients older than age80, the frail elderly. These patients were at highestrisk and received direct care from pharmacists. Thevast majority of their members were between ages 71and 80 years. Aetna expected to find most of theirdrug-related issues in this group. They also expectedthat the frail elderly would have more medical issues,which did not turn out to be the case. Instead theyfound that drug-related issues in patients younger
than age 60 years were just as great as those inpatients older than age 80. The proportions wereidentical across the ages.
Another finding was that most of their patients had3 physicians. They then reached out to all these physi-cians, who needed to be a part of their effort in coordi-nating care.
Postintervention follow-up by letters to patients(low touch) and letters plus critical calls (high touch)served to reduce events and, therefore, costs. Costavoidance occurred whether the intervention was lowtouch ($476 per member annually) or high touch($2506 per member annually). Getting to the mostoptimal outcome in a cost-effective manner was thenext problem to solve. It was once again broughthome that any intervention would reduce events andthus costs.
Focus for the Future?A pharmacy-based intervention program is critical
to the success of future program expansions. The focusshould remain on opportunities to expand clinical andsafety issues in medication therapy, as well as meetingthe educational needs of physicians about drug-relatedissues and coordinating this information with members.
The focus should be on pill burden (ie, the numberof medications a patient takes each day). Therapy mustbe streamlined to facilitate successful patient imple-mentation. Aetna is currently looking at alternativestrategies for compliance and persistence. The data arebeginning to suggest that there is a finite longevity toany intervention, which may very well vary by the typeof intervention. �
References1. Committee on Quality of Health Care in America: Institute ofMedicine. To Err is Human: Building a Safer Health System. Washington,DC: National Academy Press; 2000.2. Leape LL, Brennan TA, Laird N, et al. The nature of adverse eventsin hospitalized patients. Results of the Harvard Medical Practice StudyII. N Engl J Med. 1991;324:377-384. 3. Cooper JW Jr, Burfield AH. Medication therapy management strate-gies for geriatric patient interventions: Medicare Part D implemen -tation. Ann Long Term Care. 2007;15:33-38.
AMCP HIGHLIGHTS
Drug-related issues are responsible for 33% ofhospital admissions in older patients, includingmisuse and adverse drug reactions.
44 AMERICAN HEALTH & DRUG BENEFITS May 2008
AMCP HIGHLIGHTS
Snafu, a common term used to describe a situationmarked by error or confusion, has been adoptedby the Palo Alto Medical Foundation as the title
of a committee dedicated to reducing risks and liabilityby providing prompt response to US Food and DrugAdministration (FDA) drug safety warnings, medicalproduct recalls, and other drug and device safety issues.Through their Safety, Notification, and Follow-up(SNAFU) Committee, the Palo Alto Medical Founda -tion serves as a conduit for these FDA alerts to phar-macists, physicians, and patients.
The SNAFU Committee is made up of pharmacists,physicians, directors of materials management andclinical services, nursing and patient safety officers, andpublic relations department to address toxicity issues(both possible and probable) and device warnings. Theselection of committee members was based on con-structing a global view of safety activities.
The process begins by reviewing the FDA MedWatchalerts to determine how and where to disseminate infor-mation that will contribute to patient safety. Only alertsworthy of notice are sent to avoid unnecessary noise. E-mail conversations are initiated as soon as an alert isidentified. A plan can then be quickly developed and anaction voted on. For example, when the MedWatchPublic Health Advisory posted a problem concerningliver toxicity associated with telithromycin (Paxil) in2006, the SNAFU Committee had first to determine the
extent of risk to the patient population, which pre-scribers and patients to notify, whether specialists shouldbe involved, and what materials should be developed.The time to implement these tasks was an importantpart of the picture, including whether preventive actionshould be taken. The chosen plan of action included ane-mail alert to member physicians, who could thendecide the next course of action based on their patientbase. In matters of pressing issues, phone call follow-upsare also conducted, alerting physicians to check theirwebsites and Outlook postings. In this case, a follow-upe-mail further recommended avoiding use of the drug.After the 2 warnings, alerts were issued. Only 4 patientsmet Palo Alto’s internal guidelines for antibiotic failureand multi-drug resistance. Of 21 patients who receivedtelithromycin, 13 had received it as a sample.
This finding prompted further scrutiny into why abroad-spectrum antibiotic was being sampled in thefirst place. The SNAFU Committee recommendedthat such samples be disallowed and requested that thePharmacy & Therapeutics (P&T) Committee add thisprohibition to the sample policy.
Provider, Patient NotificationInformation imparted to providers must be concise,
offer important facts, and suggest a course of action andsupport tools. In addition, it must be determined “whoneeds to know.” The Committee is rarely hampered byprivacy concerns based on Health Insurance Portabilityand Accountability Act compliance issues. Thus, whenpatients need to know, patients are notified. At times,however, there are areas of sensitivity. For example,when paroxetine was contraindicated in pregnantwomen, notification was sent to all women of possiblechildbearing age (12 to 55 years). They attempted tocast a wide net to patients but a narrow net to pro -viders. Patients were advised to self-monitor for signsand symptoms. Only 1 pregnant woman was takingparoxetine. The overall goal was to reduce the possibil-ity of harm to a patient and lessen the risk of liabilityto the medical group.
Responding to FDA Alerts: How to Reduce Risksand LiabilityBy Sandy Paton
Based on a presentation by Kathleen Orrico, PharmD, at the Academy of Managed Care Pharmacy AnnualMeeting, April 17, 2008, San Francisco, CA.
Kathleen Orrico, PharmD, is Health Sciences AssistantClinical Professor, University of California at San Francisco.
Information imparted to providers must beconcise, offer important facts, and suggest acourse of action and support tools.
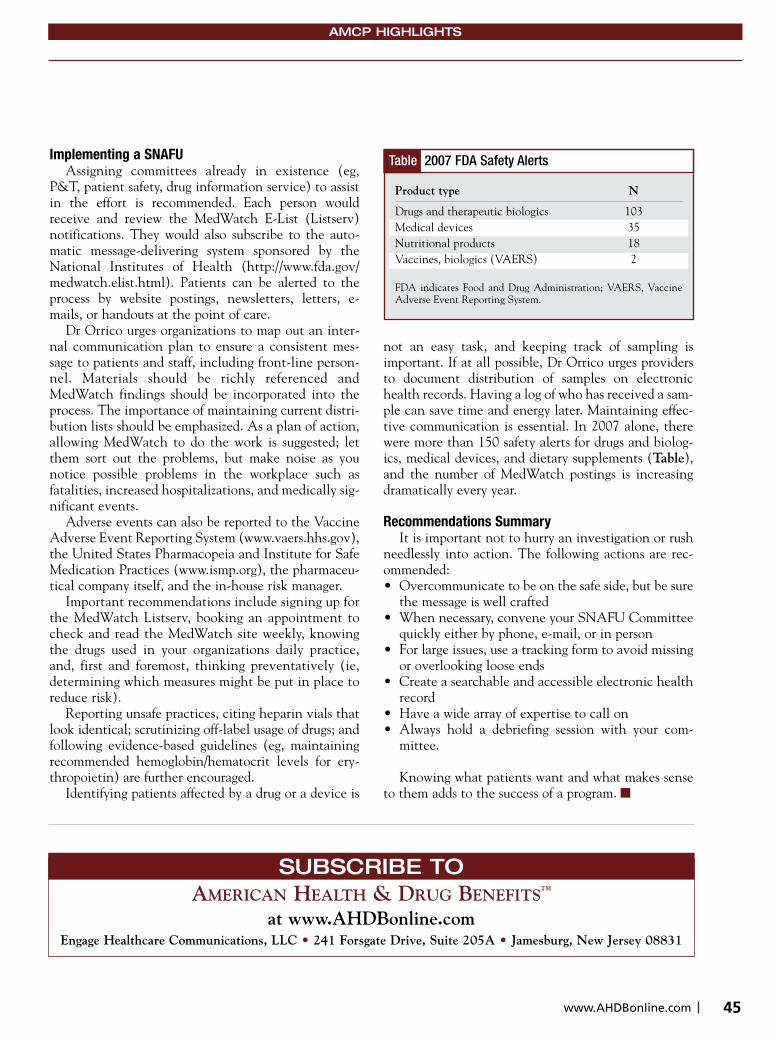
45www.AHDBonline.com
Implementing a SNAFUAssigning committees already in existence (eg,
P&T, patient safety, drug information service) to assistin the effort is recommended. Each person wouldreceive and review the MedWatch E-List (Listserv)notifications. They would also subscribe to the auto-matic message-delivering system sponsored by theNational Institutes of Health (http://www.fda.gov/medwatch.elist.html). Patients can be alerted to theprocess by website postings, newsletters, letters, e-mails, or handouts at the point of care.
Dr Orrico urges organizations to map out an inter-nal communication plan to ensure a consistent mes-sage to patients and staff, including front-line person-nel. Materials should be richly referenced andMedWatch findings should be incorporated into theprocess. The importance of maintaining current distri-bution lists should be emphasized. As a plan of action,allowing MedWatch to do the work is suggested; letthem sort out the problems, but make noise as younotice possible problems in the workplace such asfatalities, increased hospitalizations, and medically sig-nificant events.
Adverse events can also be reported to the VaccineAdverse Event Reporting System (www.vaers.hhs.gov),the United States Pharmacopeia and Institute for SafeMedication Practices (www.ismp.org), the pharmaceu-tical company itself, and the in-house risk manager.
Important recommendations include signing up forthe MedWatch Listserv, booking an appointment tocheck and read the MedWatch site weekly, knowingthe drugs used in your organizations daily practice,and, first and foremost, thinking preventatively (ie,determining which measures might be put in place toreduce risk).
Reporting unsafe practices, citing heparin vials thatlook identical; scrutinizing off-label usage of drugs; andfollowing evidence-based guidelines (eg, maintainingrecommended hemoglobin/hematocrit levels for ery-thropoietin) are further encouraged.
Identifying patients affected by a drug or a device is
not an easy task, and keeping track of sampling isimportant. If at all possible, Dr Orrico urges providersto document distribution of samples on electronichealth records. Having a log of who has received a sam-ple can save time and energy later. Maintaining effec-tive communication is essential. In 2007 alone, therewere more than 150 safety alerts for drugs and biolog-ics, medical devices, and dietary supplements (Table),and the number of MedWatch postings is increasingdramatically every year.
Recommendations SummaryIt is important not to hurry an investigation or rush
needlessly into action. The following actions are rec-ommended:• Overcommunicate to be on the safe side, but be sure
the message is well crafted• When necessary, convene your SNAFU Committee
quickly either by phone, e-mail, or in person• For large issues, use a tracking form to avoid missing
or overlooking loose ends• Create a searchable and accessible electronic health
record• Have a wide array of expertise to call on• Always hold a debriefing session with your com -
mittee.
Knowing what patients want and what makes senseto them adds to the success of a program. �
AMCP HIGHLIGHTS
Table 2007 FDA Safety Alerts
Product type N
Drugs and therapeutic biologics 103Medical devices 35Nutritional products 18Vaccines, biologics (VAERS) 2
FDA indicates Food and Drug Administration; VAERS, VaccineAdverse Event Reporting System.
SUBSCRIBE TOAMERICAN HEALTH & DRUG BENEFITS™
at www.AHDBonline.comEngage Healthcare Communications, LLC • 241 Forsgate Drive, Suite 205A • Jamesburg, New Jersey 08831

46 AMERICAN HEALTH & DRUG BENEFITS May 2008
REGULATORY
Robert Henry: Medicare’s recommendations for erythropoiesis-stimulating agents (ESAs) revolvesaround several key stakeholders with diverse agen-
das—those of the US Food and Drug Administration(FDA), the American Society of Hematology (ASH), theAmerican Society of Clinical Oncology (ASCO), andpharmaceutical companies. What are the coverage issues forthese various stakeholders?
Sam Silver: This is a very sensitive issue. Articlespublished in the New York Times were quite negativewith regard to perverse economic incentives for physi-cians’ prescribing of ESAs. Oncologists are seekingflexibility in determining how to use the ESA medica-tions based on a hemoglobin level cut-off of less than12 g/dL. Professional medical societies value evidence-based findings. Practicing oncologists can be made to
look like the “bad guys” interested only in profit mar-gins and not in the patient; but this issue is far morecomplicated than that. Physicians do try to do the bestfor their patients, and yet financial incentives can bean inappropriate driver.
Henry: Dr Randy Vogenberg will be leading the discus-sion to explore the issue from the different stakeholders’ per-spectives.
F. Randy Vogenberg: I am a pharmacist by training,with a PhD in healthcare administration, and I have beeninvolved in employer-related benefit issues. I also work withpharmacy benefit managers, health plans, benefit consult-ants, and brokers, so I see this issue from a variety of per-spectives in terms of the financial and clinical implications inthe marketplace.
Silver: During my 10 years of being the director ofBone Marrow Transplantation at the University ofMichigan, I got interested in reimbursement issues forclinical trials, especially with regard to bone marrow
Medicare Coverage forErythropoiesis-StimulatingAgents: The Perfect StormInterview (Part 1) with Samuel M. Silver, MD, PhD
Medicare policy changes have an immediate impact on health plans with regard to set-ting payment policy for providers. So when Medicare tightened payment guidelines for alucrative class of anemia drugs—erythropoiesis-stimulating agents—an ambitious set ofrules was put into effect. Health plans often follow suit in short order, enforcing publicguidelines on private payors, even when saving money is not a consideration. However,when Medicare takes an unreasonably hard line, plans tend to focus on members andphysicians more fervently, attempting to soften the hard line. In this first part of the inter-view, Dr Silver examines the coverage decisions set by the Centers for Medicare &
Medicaid Services for the use of erythropoiesis-stimulating agents and discusses the issues surrounding their adop-tion, indications versus off-label use, as well as lingering questions about their role in tumor progression and otherrisk factors. [AHDB. 2008;1(4):46-50.]
Dr Silver is Professor of Internal Medicine, Director, CancerCenter Network, Division of Hematology/Oncology, andDirector, Medical Management Center, University ofMichigan Health Systems, Ann Arbor, MI.

47www.AHDBonline.com
REGULATORY
transplantations for breast cancer in the 1990s. I even-tually became active at ASH and chaired several com-mittees, including their Reimbursement Sub committee,and I am finishing my term on their ExecutiveCommittee. I was also a member of the Board of theAmerican Society of Blood and Marrow Transplantationand currently serve on several committees of ASCO. Inaddition, I am still practicing hematology/oncology,while remaining involved in reimbursement.
Hematologists and oncologists have been lookingfor the Holy Grail—how to avoid transfusions—forquite some time, and thought they had found it inESAs. We all had concerns about blood products sincethe arrival of HIV, particularly in the hemophilic pop-ulation. Red blood cell transfusions are fraught withpossible complications, including hepatitis and otherside effects, such as transfusion-associated lung injury.Consequently, we allowed patients to run low hemo-globin counts secondary to their underlying malignan-cies and chemotherapy, but this negatively affectedtheir quality of life (QOL). Today many of us use trans-fusions as needed, without a particular target in mind,and we tend to focus on symptomatology rather thanon any target hemoglobin level that signals the needfor transfusion.
Vogenberg: Could you discuss the evolution of the usesand concerns regarding ESAs?
Silver: When ESAs came on the market, they werewell embraced. The FDA-labeled indication was todecrease the number of transfusions or avoid them alto-gether, but in time, studies implied that increasinghemoglobin levels also improved patients’ QOL. Thepharmaceutical industry embraced and publicized thesestudies to physicians and through direct marketing topatients. And so, years after the original FDA indica-tion, these agents became associated with QOL issues.With all the off-label uses common today, we forgotthat these drugs were actually indicated to avoid trans-fusions, and the focus shifted to QOL.
Around 2004, it became apparent that patients withend-stage renal disease (ESRD) and chemotherapy-induced anemia were having thromboembolic eventsas a result of treatment with ESAs, especially inpatients whose hemoglobin levels were driven to morethan 12 g/dL. The Oncology Drug Advisory Com -mittee (ODAC) noted that appropriate studies werenot being conducted to examine the effects of thesedrugs on ESRD patients or on tumor progression.1
Rather, existing studies examined transfusion-avoid-
ance and QOL issues associated with hemoglobin lev-els higher than 12 g/dL.
ODAC asked Johnson & Johnson and Amgen toundertake appropriate studies on potential risks withthese agents. Studies continued to accumulate during2006 and 2007 from patients with renal insufficien-cy–associated anemia and from those with chemother-apy-induced anemia, raising concerns about the risks ofearly death, tumor progression, and serious cardiovas-cular events.
In 2007, ESAs had the highest drug expenditures inMedicare Part B,2,3 and safety issues became a seriousconcern. Alarming findings were emerging from sever-al studies.
In a European study, Henke and colleagues usederythropoietin-beta (not available in the UnitedStates) for locally advanced head and neck cancerwith target hemoglobin levels ranging from 12 g/dLto 13 g/dL.4 The study’s findings showed a significanthazard ratio for localized progression of head andneck cancer. There were concerns regarding thestudy’s validity, however, because this study did notinclude a systematic review of tumor progression byuse of radiologic data.
Leyland-Jones and colleagues examined the use ofESAs in patients with metastatic breast cancer, show-ing decreased survival at 12 months.5 Another study byWright and colleagues on metastatic non–small-celllung cancer also demonstrated reduced survival withESAs compared with placebo.6
KEY POINTS� ESAs are indicated for treating patients as a way to avoid
transfusions, but the focus in practice has since shifted tooff-label use for quality-of-life concerns.
� Safety issues have become a serious concern with ESAs, as findings of early death, tumor progression, and serious cardiovascular events linger.
� In 2007, ESAs had the highest drug expenditures inMedicare Part B.
� In November 2007, the FDA strengthened its “black box”warning for the use of ESAs, because of increased evidence of tumor progression and reduced survival.
� In March 2008, the Oncology Drug Advisory Committeerecommended limiting the use of these agents in the cancersetting to circumstances where chemotherapy is not givenfor curative purposes, and not to exclude their use inpatients with head and neck cancer or breast cancer.

48 AMERICAN HEALTH & DRUG BENEFITS May 2008
REGULATORY
Finally, there was an Amgen study conducted inEastern Europe.7 It was conducted on patients withmultiple types of cancer who had not receivedchemotherapy or radiation. These patients were ran-domized to receive transfusions alone or ESAs.Survival was shortened in patients who were notreceiving chemotherapy. This finding caused particularconcern at the FDA, because this use of ESAs was com-pletely off-label: This was not chemotherapy-inducedanemia but rather it was the anemia associated withcancer itself. We do not know whether the shorter sur-vival was from the tumor progression or whether it wasrelated to the thromboembolic events, but there cer-tainly appeared to be a shortened survival in the ESAarm of the study.7
The findings from these studies led to the first blackbox warning for ESAs, issued by the FDA in March2007.8 The FDA announced that physicians shouldonly use the lowest dose of an ESA necessary to avoidthe need for blood transfusions caused by anemia.Based on the Henke study,4 the FDA also noted thatthere was a reduced time to tumor progression inpatients with advanced head and neck cancer with theuse of these agents. This study, as well as the Europeanstudy which showed a decreased survival in patientswith cancer-related anemia who received ESAs,7 ledthe FDA to determine that ESAs are not indicated inpatients whose hemoglobin levels are more than 12g/dL or in patients who are not receiving chemothera-py or radiation.
In May 2007, the New York Times published a front-page story titled, “Doctors Reaping Millions for Use ofAnemia Drugs.”9 The article described how 2 of theworld’s largest drug companies are paying hundreds ofmillions of dollars to doctors every year in return forgiving their patients “anemia medications” and indoses that regulators now say may be unsafe. It wasnoted that the doses were legal, but that very few peo-ple apart from the doctors were aware of the high doses
used. Critics, including prominent cancer and renalexperts, said that the payments gave physicians anincentive to prescribe the medications at levels thatmay increase patients’ risks of heart attacks or strokes.We thus have what I call, “ESAs—the perfect storm.”
The ESAs are supportive-care drugs, but providingthem in doses higher than indicated by the FDAappears to result in an increased incidence of throm-boembolic events, early death, and possibly tumorprogression.
Vogenberg: Was there a marketing issue surrounding allthis?
Silver: When ASH/ASCO issued their guidelinesin 2003, they reviewed QOL issues in the literature andwere not impressed by the evidence. Apparently therewas a very high dropout rate of patients in the involvedstudies. The scales used in the studies did not makeclear what a clinically significant benefit meant from aQOL point of view. Perhaps if they had compared dif-ferences in QOL in patients with hemoglobin levels of8 g/dL versus 11 g/dL (instead of higher levels), theQOL issues could have been clearer.
The marketing issue revolved around the QOLissue. If one could show conclusively that QOLincreased when hemoglobin levels increased above theindicated level, it would have provided sufficient evi-dence to raise hemoglobin levels.
Vogenberg: There are many issues surrounding QOLfrom a payor perspective, including a strong bias againstit. I think that might have contributed to this perfect stormsituation.
Silver: True. But, as you know, marketing andresearch go hand in hand. This is nothing new, but itcertainly is an issue, especially when dealing with QOLand survival.
The day after the New York Times article appeared,ODAC reviewed the clinical trials data. The compa-nies released a lot of data on QOL, which did not con-vince ODAC. The companies did agree that there wasan increased incidence of thromboembolic events, butthey tried to dismiss the issue of tumor progression. Ithink the issue of tumor progression is something wereally do not understand, and it has not been welldemonstrated. In December 2007, the National CancerInstitute convened a meeting of investigators who con-cluded that there were compelling in vitro data to con-tinue investigations on ESAs and tumor progression.
This finding caused particular concern at theFDA, because this use of ESAs was completelyoff-label: This was not chemotherapy-inducedanemia but rather it was the anemia associated with cancer itself.

49www.AHDBonline.com
REGULATORY
The ODAC review indicated that the FDA shouldconsider adding to the product labeling further restric-tions on the use of ESAs in patients with the types oftumors implicated in available trials, which the FDAdid in November 2007.10 Because the issue of tumorprogression had not been sorted out, it was suggestedthat additional trials should be conducted.
Vogenberg: Have there been any data regarding thelong-term use of ESAs in patients?
Silver: There is a wealth of data that show that usingESAs in inpatients with low-grade myelodysplastic syn-drome (MDS) could lower their transfusion require-ments. MDS is a chronic disease, and thus therapy maybe required for many years. Using ESAs in cancerchemotherapy is very short-term—6 to 9 months atmost. But this discussion is premature, because there isno FDA indication for its use in MDS, and it is unlike-ly that an indication would be added soon, given thecurrent atmosphere.
The Centers for Medicare & Medicaid Services(CMS) recently issued a National Coverage Deter -mination (NCD) on ESAs for non–renal disease indi-cations. CMS remains mute on the use of ESAs for thetreatment of anemia associated with myelodysplasia,since they stated it was a premalignant condition, andthe Medicare NCD was for the chemotherapy-inducedanemia in cancer patients. This is a major issue for meas a hematologist, because there are good data for theuse of ESAs in low-grade MDS. Based on this NCD,Medicare has now placed its coverage of ESAs for MDSat the hands of Part B carrier medical directors and PartA fiscal intermediaries.
But the NCD stated that CMS still did not thinkthat ESAs work for MDS, which could bias local carri-ers against it. CMS remained silent on differentiatingtypes of tumors, but from the point of view of ASH,one of the things we considered most onerous in theNCD was that the trigger point was defined as a hemo-globin level of 10 g/dL. If a patient’s level was above 10g/dL, you were to avoid ESA therapy.
So, initiation of therapy was at a hemoglobin levelof less than 10 g/dL, and maintenance was also at lessthan 10 g/dL. This is a serious paradigm shift from howESAs had been used, and yet there was no evidence tosupport it. This ruling requires significant and frequenttesting of patients to ensure that their hemoglobin lev-els did not exceed the new 10-g/dL threshold.
Vogenberg: Did anyone challenge CMS on this?
Silver: Several societies challenged this. The FDAsaid that there were no new data available that wouldallow them to change their minds. ASH/ASCO thenissued guidelines about ESA use in late 2007, sayingthat starting with hemoglobin levels of less than 10g/dL was very reasonable, but the maintenance rangeshould be between 10 g/dL and 12 g/dL. The recom-mendation was also concordant with FDA labelingthat if a patient’s hemoglobin rose above 11 g/dL, youshould start to cut back on the ESA dose. So essential-ly, they were looking at the midrange hemoglobin levelbetween 10 g/dL and 12 g/dL.
Vogenberg: As a clinician, how do you determine howto proceed, because it may take a couple of days before yousee a response?
Silver: That’s very true. It remains to be seen howthis will affect transfusions. I have suggested to CMSand to members of Congress that we should use claim-based data to look retrospectively and prospectively atthe transfusion requirements of Medicare beneficiarieswho are and those who are not receiving ESAs for che -motherapy-induced anemia, to determine transfusionuse before and after the new NCD. It may now bemore difficult to compare these time periods withclaim-based data, because physicians will allow hemo-globin levels to get lower than they have allowed inthe past. �
Disclosure StatementDr Silver is a consultant to Bear Stearns, Lehman Brothers, and
the Gerson Lehrman Group, and receives grant/research supportfrom Blue Cross Blue Shield of New Jersey.
References 1. The Oncology Drug Advisory Committee. Safety concerns associatedwith Aranesp (darbepoetin alfa) Amgen, Inc. and Procrit (epoetin alfa)Ortho Biotech, LP, for the treatment of anemia associated with cancerchemotherapy. May 4, 2004. http://www.fda.gov/ohrms/dockets/ac/04/briefing/4037B2_04_FDA-Aranesp-Procrit.htm#_ednref45. AccessedApril 29, 2008.
So, initiation of therapy was at a hemoglobinlevel of less than 10 g/dL, and maintenancewas also at less than 10 g/dL. This is a seriousparadigm shift from how ESAs had been used,and yet there was no evidence to support it.
50 AMERICAN HEALTH & DRUG BENEFITS May 2008
REGULATORY
2. Steinbrook R. Erythropoietin, the FDA, and oncology. N Engl J Med.2007;356:2448-2451.3. Duh MD, Weiner JR, White LA, et al. Management of anaemia: acritical and systematic review of the cost effectiveness of erythropoiesis-stimulating agents. Pharmacoeconomics. 2008;26:99-120. 4. Henke M, Laszig R, Rübe C, et al. Erythropoietin to treat head andneck cancer patients with anaemia undergoing radiotherapy: randomised,double-blind, placebo-controlled trial. Lancet. 2003;362:1255-1260.5. Leyland-Jones B, Semiglazov V, Pawlicki M, et al. Maintaining nor-mal hemoglobin levels with epoetin alfa in mainly nonanemic patientswith metastatic breast cancer receiving first-line chemotherapy: a sur-vival study. J Clin Oncol. 2005;23:5960-5972.6. Wright JR, Ung YC, Julian JA, et al. Randomized, double-blind,placebo-controlled trial of erythropoietin in non–small-cell lung cancerwith disease-related anemia. J Clin Oncol. 2007;25:1027-1032.7. Glaspy J, Smith R, Aapro M, et al. Results from a phase 3, randomized,
double-blind, placebo-controlled study of darbepoetin alfa for the treat-ment of anemia in patients not receiving chemotherapy or radiotherapy.Paper presented at the American Association for Cancer ResearchAnnual Meeting Proceedings; April 14-18, 2007; Los Angeles, CA.8. FDA Alert. Information for healthcare professionals: erythropoiesis-stimulating agents (ESA) [Aranesp (darbepoetin), Epogen (epoetin alfa),and Procrit (epoetin alfa)]. Rockville, MD: US Food and DrugAdministration; March 9, 2007. http://www.fda.gov/cder/drug/InfoSheets/HCP/RHE2007HCP.htm. Accessed April 6, 2008. 9. Berenson A, Pollack A. Doctors reaping millions for use of anemiadrugs. New York Times. May 9, 2007:A1.10. New FDA warnings: communication about an ongoing safety review.Erythropoiesis-stimulating agents (ESAs) epoetin alfa (marketed asProcrit, Epogen) darbepoetin alfa (marketed as Aranesp). November 8,2007. http://www.fda.gov/cder/drug/early_comm/ESA.htm. AccessedApril 6, 2008.
AHDB Stakeholder Perspective
UnitedHealthcare’s Response to the ESA Debate
PAYORS: It is important to remember whyUnitedHealthcare became interested in the issue ofthe erythropoiesis-stimulating agents (ESAs).Following the US Food and Drug Administration(FDA) warning about potential problems withESAs, UnitedHealthcare launched a pilot study inNew York, New Jersey, and Connecticut, requiringprecertification for any ESA injection. We used theguidelines issued by professional cancer societies toset our maximum hemoglobin coverage limit at12 g/dL. Higher hemoglobin levels were not cov-ered. This 6-month pilot study revealed a 35%reduction in the use of ESAs, indicating that 1 of 3doses that were being administered could havepotentially harmed the patient.
Physicians and patients have become confusedabout the purpose of these medications. As Dr Silverstates in his article, ESAs were originally created toavoid transfusions—a dangerous procedure even withcurrent sophisticated screening. The quality-of-life(QOL) marketing, misaligned economic incentives,and the erroneously perceived safety profile made it
easy to become lax about the actual FDA indicationsfor this therapy. Even now, the ESA problem is stillnot resolved.
Every therapy has a potential for toxicity.Transfusion medicine has improved substantiallysince the emergence of the HIV epidemic in the1970s, but Dr Silver aptly summarizes the significantrisks that still exist. If oncologists use transfusion forQOL reasons rather than for physiologic problems,such as angina, orthostatic hypotension, or restingdyspnea, we will simply be trading one set of prob-lems for another.
RESEARCH: We can expect a rush of studiesthat will examine rates of transfusions before and asa result of the recent coverage changes for ESAs, butif these studies do not examine the hemoglobin lev-els and the medical indications for those transfu-sions, these studies will be worthless. The unan-swered question that needs to be examined is: Is itworth any toxicity at all to treat patients with ahemoglobin level above 10 g/dL?
HEALTH PLANS: So while that debate goeson, UnitedHealthcare will continue its present pol-icy of simply asking professionals to adhere to theirown guidelines.
Lee Newcomer, MDUnitedHealthcare, Minneapolis, MN
CorrectionIn Table 2 in the article “Not waiting for Godot: the evolution of health promotion at PPG industries” (April 2008,
page 31), STD indicates short-term disability, not sexually transmitted disease, as is incorrectly noted there.
Do you measure resource
utilization and costs associated
with depression?
Managing quality and cost is the foundation of today’s
managed care structure. Wyeth recognizes that balancing
quality and cost is a formidable challenge for managed health
care professionals. We also recognize that success, in part,
hinges on tools and resources that can aid in the evaluation
of care management and may lead to reinforcing solutions. As
part of our continuing efforts to improve the quality of care for
patients with depression, we are proud to sponsor this
comprehensive claims-based review to promote ongoing
clinical and financial assessments that improve care in this
patient population.
To learn more about this exclusive program,
please contact your Wyeth Pharmaceuticals
Account Manager today!
N e w E d i t i o n N o w A v a i l a b l e
Award-winningDepression Benchmarks!
Gold AwardAster Awards, May 2007
Merit Awards (2)Healthcare Advertising Awards,
April 2007
A comprehensive, claims-based analysis of more than 600,000
patient episodes of depression (1 episode = 1 year)
highlighting direct costs and utilization of
resources across 5 domains of care:
� Inpatient care
� Outpatient care
� Ancillary care (labs, tests, procedures)
� Emergency department
� Pharmaceuticals
“Depression Benchmarks” and “TRU Benchmarks” are trademarks owned by Managed Care Measures, LLC. Depression BenchmarksTM
publication cover design, photograph, and color scheme (except for Total Resource
UtilizationTM
blue banner): © 2008, Wyeth Pharmaceuticals Inc., Philadelphia, PA 19101. Total Resource UtilizationTM
blue banner: © 1999-2008 Managed Care Measures, LLC. The remainder of this advertisement:
© 2008, Wyeth Pharmaceuticals Inc., Philadelphia, PA 19101. 223008-01
DepressionBenchmarks
TM

52 AMERICAN HEALTH & DRUG BENEFITS May 2008
AACR MEETING HIGHLIGHTS
Anticancer DrugDevelopment Trends:Translational MedicineBy Caroline Helwick
More than 17,000 of the world’s best cancerscientists convened in April in San Diegofor the annual meeting of the American
Association for Cancer Research (AACR). Break -throughs in molecular targeting of the seemingly limit-less tumor-cell–signaling pathways were highlighted inmany of the 6000 abstracts presented.
Eileen P. White, PhD, Chair of the AACR 2008program committee, noted, “This meeting is�a show-case for�the best science that is happening every -where: the best molecular biology, cell biology, drugdevelopment.”
The common goal of these research efforts is tobring drugs to the pharmacy sooner, to save lives, the“bench to bedside” approach. “We now know thatcancer is not just one disease but hundreds of differentdiseases. The challenge is to identify the characteris-tics of a patient’s particular tumor and tailor treatmentto those characteristics. Personalized medicine is crit-ical to this process and is the aim of the future,” DrWhite said.
Laboratory research is moving rapidly into the clin-ical setting, she noted. “Basic and clinical sciences aremerging, and this interface is what we call translation-al medicine.”
New Pathways and TherapiesA remarkable increase is evident in our under-
standing of the genomic drivers of malignancy and thecellular pathways that are highjacked to support onco-genesis. Inhibitors of the epidermal growth factorreceptor and vascular endothelial growth factor soundmundane now that the molecular lexicon contains somany new members. Researchers are rapidly expand-ing the range of tumor targets that are “druggable” bysmall-molecule and antibody-based technologies.
Control of translation—namely, genetic factors—isalso important in the regulation of cell growth and pro-liferation. A number of translation initiation factorsare overexpressed or deregulated in tumors or causemalignant transformation. Genes and gene complexesbelieved to be important in tumor formation have beenrecently targeted for cancer therapy.
You will be hearing more about these:
• The protein p53 is a transcription factor activated bymany stresses that impinge upon cells as they progressfrom normalcy to malignancy. Activation is good, butp53 is mutated in 50% of cancers (to facilitategrowth) and inactivated in the other 50%. Regulationof p53 offers immense therapeutic opportunities.
• Mutations in the phosphoinositide-3 kinase (PI3K)pathway occur in many solid tumors, and most can-cers have elevated PI3K signaling. PI3K, therefore,has become a promising therapeutic target.
• The mammalian target of rapamycin (mTOR) sig-naling pathway is a conserved serine/threoninekinase that helps integrate growth factor and envi-ronmental signals (hypoxia, nutrients) and regulatethe cell cycle, hence mTOR inhibitor has become afocus of drug development.
• The serine/threonine kinase Akt serves as a conver-gence point for many molecular alterations in cancerand controls cellular processes that contribute to can-cer development. Akt activation confers resistance tomany cancer therapies and is a poor prognostic factor.
• The insulinlike growth factor (IGF) system is alinked network of growth factors, binding proteins,and receptors that are involved in normal growthand metabolism.
• Inhibitors of c-MET and its ligand, hepatocytegrowth factor/scatter factor (HGF/SF), have beenleading therapeutic targets. Inappropriate c-METsignaling occurs in virtually all types of solid tumorsand can participate in all stages of cancer develop-ment. Biologics and small-molecule inhibitorsdirected against this pair are promising therapeutics.
• Blockade of transforming growth factor-� (TGF-�)is expected to impede growth, progression, andmetastatic potential of malignant disease. Increasedexpression and production of TGF-� occurs in manyneoplasms and is associated with reduced survival.
• Ras proteins play a key role in mediating signalingevents involved in many cellular responses; there-fore, critical elements of the Ras pathways arepotential targets for therapeutic intervention.
• Histone deacetylase (HDAC) is a family of 11enzymes that help regulate cancer through their rolein the control of gene expression. HDAC inhibitorsselectively switch on tumor suppressor genes.
• Heat shock protein 90 (HSP90) is a cellular chap-erone protein required for the activation of severalprotein kinases. HSP90 inhibitors have been shownto have antiproliferative and antitumor activities.

53www.AHDBonline.com
AACR MEETING HIGHLIGHTS
• The pathways of cell death and cell survival providemany opportunities for therapeutic targeting in can-cer, such as with drugs targeting the B-cell leuke -mia/lymphoma 2 (Bcl-2) family and the tissue dis-turbance of the death ligand (TRAIL) receptors.
• Proteins with specific functions in mitosis are thetarget of novel agents known as mitotic kinase andkinesin inhibitors, such as the epothilone class ofagents (eg, ixabepilone).
• Proteosomes have enzymatic activity and regulatoryfunctions with respect to cellular protein turnover.Second-generation proteosome inhibitors are nowin clinical development, following the success withbortezomib.
• A host of pro- and antiangiogenic factors regulatean “angiogenic switch” that, when turned on, allowsfor blood vessel growth and tumor aggressiveness.Angiogenesis inhibitors targeting this switch are inclinical trials.
A Scientist Perspective “Probably the most interesting pathway is the sig-
naling cascade involving PI3K, Akt, and mTOR, withIGF at the receptor level. A number of compoundshave been developed to block each of these compo-nents,” said Alex A. Adjei, MD, PhD, senior vice pres-ident of clinical research and the Katherine AnneGioia Chair in Cancer Medicine at Roswell ParkCancer Institute, Rochester, NY.
In addition, cancer processes, such as the traffickingof proteins or regulation of gene expression, are alsoimportant. Many inhibitors of these processes are indevelopment, such as HSP90 and HDAC inhibitors.
“The number of compounds directed at any one tar-get or process reflects the fact that science has becomeegalitarian,” he observed. “Gone are the days when wefound one drug hitting a target and that one drug gotto market 5 years later. Now, when the target is identi-fied, you see 5 to 6 compounds come out of the gate atthe same time. We are now in the position of having alot more drugs than targets.”
“As we understand the different molecular aberra-tions in cancer, the defects in different kinds of cells,we will be able to give different drugs to differentpatients. We will be thinking about these numerousmolecular targeted agents the way we think aboutantibiotics today: some work for one infection and notthe other.” �
Continue to Focus on Broader Issues, Not Juston Drug Benefits
To the Editor: I wanted to let you know how much Ienjoyed reading the inaugural (February) issue ofAmerican Health & Drug Benefits. All the articles are ontarget as far as addressing important issues, and therange of different perspectives is impressive.
I must admit that I am a little confused aboutwhether the primary focus is going to be on drug ther-apy as opposed to a broader range of subjects. Fromyour mission statement it appears that the focus isclearly on pharmacotherapy and drug benefits, butthe articles, especially the one by Gingrich andDesmond, address the much broader issue of health-care reform. As a physician and a medical directorwhose focus—while including pharmacotherapy—ison the broader issues of care, I certainly hope thatyou will continue to highlight issues other than justdrug benefits and pharmacotherapy.
This is a “different” type of journal, which is not easyto accomplish in a crowded field of competitors. Mycongratulations to you, and I will look forward to futureissues, which I hope will be made available.
Stephen Gorshow, MD, FACPVice President and Senior Medical DirectorEmerging Technology and Clinical PolicyGreenwood Village, CO
Letter to the Editor
LettersWe welcome your letters and comments aboutarticles published in American Health & DrugBenefits. Please limit your responses to about400 words. If using references, please providecomplete information. All letters are minimallyedited for clarity and style, and if published, willappear in the print and the online versions of thejournal. Please provide your name, any degree,and affiliation.Submit letters to [email protected].
LETTERS
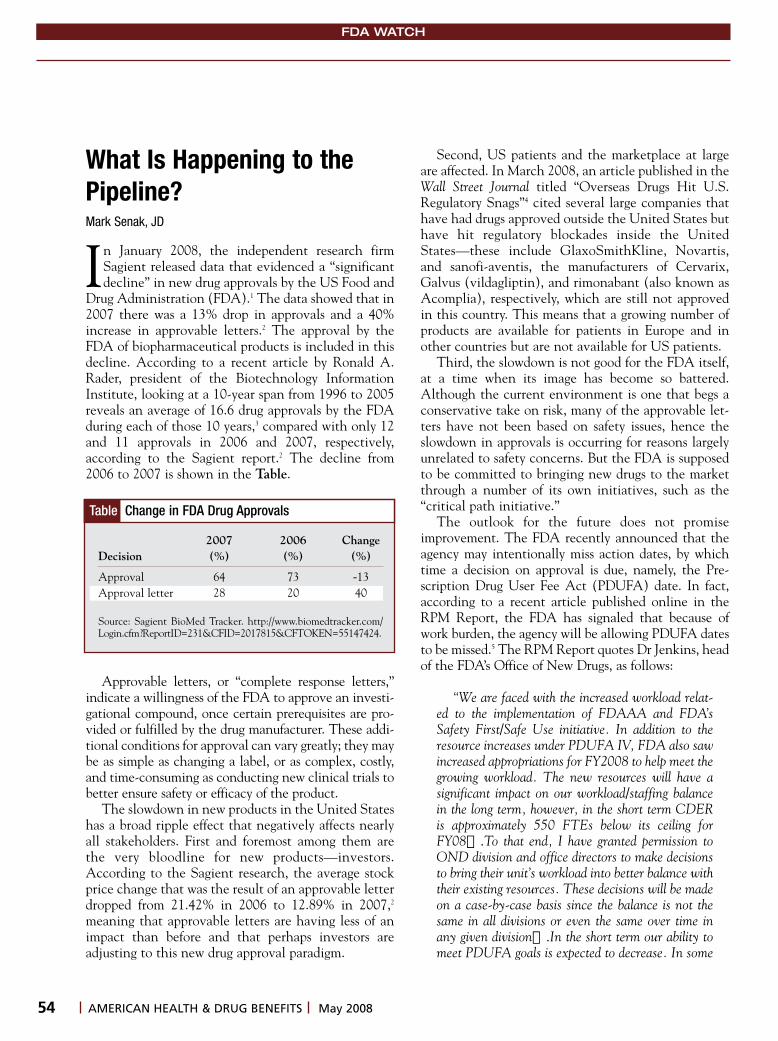
54 AMERICAN HEALTH & DRUG BENEFITS May 2008
FDA WATCH
What Is Happening to thePipeline?Mark Senak, JD
In January 2008, the independent research firmSagient released data that evidenced a “significantdecline” in new drug approvals by the US Food and
Drug Administration (FDA).1 The data showed that in2007 there was a 13% drop in approvals and a 40%increase in approvable letters.2 The approval by theFDA of biopharmaceutical products is included in thisdecline. According to a recent article by Ronald A.Rader, president of the Bio technology InformationInstitute, looking at a 10-year span from 1996 to 2005reveals an average of 16.6 drug approvals by the FDAduring each of those 10 years,3 compared with only 12and 11 approvals in 2006 and 2007, respectively,according to the Sagient report.2 The decline from2006 to 2007 is shown in the Table.
Approvable letters, or “complete response letters,”indicate a willingness of the FDA to approve an investi-gational compound, once certain prerequisites are pro-vided or fulfilled by the drug manufacturer. These addi-tional conditions for approval can vary greatly; they maybe as simple as changing a label, or as complex, costly,and time-consuming as conducting new clinical trials tobetter ensure safety or efficacy of the product.
The slowdown in new products in the United Stateshas a broad ripple effect that negatively affects nearlyall stakeholders. First and foremost among them arethe very bloodline for new products—investors.According to the Sagient research, the average stockprice change that was the result of an approvable letterdropped from 21.42% in 2006 to 12.89% in 2007,2
meaning that approvable letters are having less of animpact than before and that perhaps investors areadjusting to this new drug approval paradigm.
Second, US patients and the marketplace at largeare affected. In March 2008, an article published in theWall Street Journal titled “Overseas Drugs Hit U.S.Regulatory Snags”4 cited several large companies thathave had drugs approved outside the United States buthave hit regulatory blockades inside the UnitedStates—these include GlaxoSmithKline, Novartis,and sanofi-aventis, the manufacturers of Cervarix,Galvus (vildagliptin), and rimonabant (also known asAcomplia), respectively, which are still not approvedin this country. This means that a growing number ofproducts are available for patients in Europe and inother countries but are not available for US patients.
Third, the slowdown is not good for the FDA itself,at a time when its image has become so battered.Although the current environment is one that begs aconservative take on risk, many of the approvable let-ters have not been based on safety issues, hence theslowdown in approvals is occurring for reasons largelyunrelated to safety concerns. But the FDA is supposedto be committed to bringing new drugs to the marketthrough a number of its own initiatives, such as the“critical path initiative.”
The outlook for the future does not promiseimprovement. The FDA recently announced that theagency may intentionally miss action dates, by whichtime a decision on approval is due, namely, the Pre -scription Drug User Fee Act (PDUFA) date. In fact,according to a recent article published online in theRPM Report, the FDA has signaled that because ofwork burden, the agency will be allowing PDUFA datesto be missed.5 The RPM Report quotes Dr Jenkins, headof the FDA’s Office of New Drugs, as follows:
“We are faced with the increased workload relat-ed to the implementation of FDAAA and FDA’sSafety First/Safe Use initiative. In addition to theresource increases under PDUFA IV, FDA also sawincreased appropriations for FY2008 to help meet thegrowing workload. The new resources will have asignificant impact on our workload/staffing balancein the long term, however, in the short term CDERis approximately 550 FTEs below its ceiling forFY08….To that end, I have granted permission toOND division and office directors to make decisionsto bring their unit’s workload into better balance withtheir existing resources. These decisions will be madeon a case-by-case basis since the balance is not thesame in all divisions or even the same over time inany given division….In the short term our ability tomeet PDUFA goals is expected to decrease. In some
2007 2006 ChangeDecision (%) (%) (%)
Approval 64 73 -13Approval letter 28 20 40
Source: Sagient BioMed Tracker. http://www.biomedtracker.com/Login.cfm?ReportID=231&CFID=2017815&CFTOKEN=55147424.
Table Change in FDA Drug Approvals

55www.AHDBonline.com
FDA WATCH
cases we may have to cut back on work by decliningrequests from sponsors for guidance (e.g., meetings,multiple cycle SPA reviews) and in other cases wemay decide to go past the PDUFA goal date forreview of an application. In cases where we decide togo past the PDUFA goal date the sponsor will benotified by the division management of that plan.”5
It is difficult to discern from the “increased work-load” when the rate of fees that come to the FDA asuser fees under PDUFA has increased substantially. Inother words, the pharmaceutical industry is beingcharged more money for fewer outcomes.
Finally, the delay in product approvals resultingfrom approvable letters or from deadlines missed by theFDA means that once approved, a product has lesstime on the market to recover research costs and tosupply a profit for the investors. The logical conse-quence is that prices of the product, once approved,will have to be higher over a shorter period of time.
The United States is by far the largest market forpharmaceutical products, and the current situation isnot likely to change that. But, according to theEuropean Federation of Pharmaceutical Industries andAssociations, the United States represents nearly twicethe sales of pharmaceutical products compared withEurope. In addition, between 1990 and 2006, invest-
Mr Senak is Senior Vice President at Fleishman-Hillard inWashington, DC, and author of Eye on FDA blog,www.eyeonfda.com.
ment in new research in the United States grew 5times compared with only 2.9 times in Europe. Thatmeans that for all the potential market and all theinvestment there are fewer products. The slowdown indrug approvals by the FDA may address the currentenvironment, but in the long-run it has a negativeimpact on nearly everyone. �
References1. Sagient BioMed Tracker. http://www.biomedtracker.com/Login.cfm?ReportID=231&CFID=2017815&CFTOKEN=55147424. AccessedApril 15, 2008.2. Reuters. Sagient research reports significant decline in FDA drugapproval rate. http://www.reuters.com/article/pressRelease/idUS130687+09-Jan-2008+PNW20080109. Accessed April 15, 2008.3. Rader RA. Paucity of biopharma approvals raises alarm: lower num-bers, novelty, and economic impact indicate problems. Genet EngBiotechnol News. 2008;28(6):10. http://www.biopharma.com/approvals_GEN.html. Accessed April 15, 2008.4. Whalen J. Overseas drugs hit U.S. regulatory snags. WSJ. March 26,2008; page B4. http://online.wsj.com/article/SB120648160360663519.html?mod=googlenews_wsj. Accessed April 15, 2008.5. The RPM Report. FDA’s outlook on the drug approval drought.February 1, 2008. http://therpmreport.com. Accessed April 15, 2008[article fee].
Call for PapersThe editors of American Health & Drug Benefits (AHDB) are pleased to invite readers to submit articles for
publication on topics examining advances in clinical, business, and regulatory developments relevant to attainingvalue—a balance of cost, quality, and access—in formulary and benefit design strategies. AHDB offers an open forumfor all healthcare stakeholders to present their needs, initiatives, and data, with the goal of achieving patient-cen-tered health and drug benefits that meet the needs of all stakeholders—patients, providers, payors, purchasers, dis-tributors, regulatory, manufacturers, evaluators, and researchers.
Articles should discuss key issues that can improve the quality and efficiency of our healthcare delivery system ingeneral and of formulary and drug benefit strategies in particular. Types of articles and topics sought include:
• Original research• Review articles• Expert opinions• Diagnosis/treatment guidelines• Drug updates• Government reports• Foundation reports• Off-label use/misuse
All papers will undergo a peer-review process. Please submit your manuscript electronically [email protected], or mail to AHDB, 241 Forsgate Drive, Suite 205A, Jamesburg, NJ 08831.
• Clinical topics: � Alzheimer’s/dementia� Asthma/allergies� Cholesterol management � Diabetes� Depression
� Hypertension� Infectious diseases� Pain management� Schizophrenia� Cancer therapy

56 AMERICAN HEALTH & DRUG BENEFITS May 2008
INDUSTRY TRENDS
Since 2000, there have been approximately 822compounds for the treatment of depression that arecurrently in various stages of development (Table 1).
More than 70% of all of the depression compoundscurrently in clinical development are sponsored by aselect number of organizations. The top organizationssponsoring such trials are listed in Table 2. Of these,approximately 28% of the compounds are sponsored bythe National Institute of Mental Health in collabora-tion with other organizations.
INDUSTRY TRENDS—CLINICALGordon M. Cummins, MS
Table 1 Depression Compounds in Development
Source: http://www.clinicaltrials.gov/ct2/results?cond=depression&cntry1=NA%3AUS&rcv_s=01%2F01%2F2000&rcv_e=03%2F17%2F2008&show_down=Y#down. Accessed March 21, 2008
Phase Compounds, N Total, %
Preclinical 2 0.2Phase 1 36 4.4Phase 1/2 28 3.4Phase 2 114 13.9Phase 2/3 20 2.4Phase 3 174 21.2Phase 4 168 20.4Unknown 280 34.1Total 822 100.00
Table 2 Organizations Sponsoring DepressionCompounds in Clinical Development
Source: http://www.clinicaltrials.gov/ct2/results?cond=depression&cntry1=NA%3AUS&rcv_s=01%2F01%2F2000&rcv_e=03%2F17%2F2008&show_down=Y#down. Accessed March 21, 2008.
Sponsor Total N %
National Institute of Mental Health 231 28.1Department of Veterans Affairs 42 5.1Eli Lilly 22 2.7Massachusetts General Hospital 20 2.4National Center for Complementaryand Alternative Medicine 19 2.3Stanford University 19 2.3GlaxoSmithKline 18 2.2New York State Psychiatric Institute 16 1.9AstraZeneca 14 1.7National Institute on Drug Abuse 14 1.7Sanofi-aventis 13 1.6University of Pittsburgh 13 1.6Duke University 12 1.5Emory University 12 1.5Yale University 11 1.3Wyeth 10 1.2Merck 9 1.1University of Texas SouthwesternMedical Center 9 1.1Indiana University School of Medicine 8 1.0McLean Hospital 8 1.0Weill Medical College of CornellUniversity 8 1.0Medical University of South Carolina 7 0.9National Institute of Diabetes andDigestive and Kidney Diseases 7 0.9National Institute on Alcohol Abuseand Alcoholism 7 0.9Pfizer 7 0.9
Depression frequently presents in association with achronic illness in the general population. The presenceof comorbid depression has been shown to be predic-tive of worse outcomes of the medical illness and ofincreased mortality.1 Major depressive disorder affectsapproximately 14.8 million (6.7%) of the adult USpopulation (18 or older) in any given year.2
INDUSTRY TRENDS—BUSINESS Depression has been associated with the followingmedical conditions: • 85% of patients with depression experience signifi-
cant symptoms of anxiety3
• About 75% of patients with obsessive-compulsivedisorder report that they have suffered from symp-toms of depression4
• Chronic major depression increases the risk of can-cer by 88% over 3.8 years of follow-up5
Continued on page 58
SELF-ADMINISTERED VERSUS PROVIDER-ADMINISTERED
�������������������������������������������������
�������������������������������������������
����������������������������������������������������������������������������
�����������������������������������������������������������������������������
���������������������������������������������������������������������������
�������������������������������������������������������������������������������
��������������������������������������������������������������������������������
����������������������������������������������������������������������������������
���������������������������������������������������������������������������������
���������������������������������������������������������������������������
���������������������������������������������������������������������������������
���������������������������������������������������������
New research from Xcenda provides answers to strategic questions facing
the oncology market:
�� ����������������������������������������������������������������������
�� ��������������������������������������������������������������������������
���������������������������������
�� ��������������������������������������������������������������������������
�������������������������
�� ������������������������������������������������������������������������
�� ������������������������������������������������������������������
������������������������
������������������������������������������������
����������������������������������������������������
[email protected] or 800-320-6497
�������������������������������������������������������������
�������������������������������������������������������
����������������������������������������������������������
������������������������������������������������������
www.xcenda.com
Route of Administration Impacts Payer Coverage – Learn How & Why
58 AMERICAN HEALTH & DRUG BENEFITS May 2008
INDUSTRY TRENDS
• Patients with cancer have a high rate of psychiatriccomorbidity; approximately 50% of those with can-cer have emotional difficulties6
• Nearly 50% of women diagnosed with early breastcancer had depression, anxiety, or both in the yearafter diagnosis7
• About 33% of patients with acute post–myocardialinfarction are depressed; depression is a strong inde-pendent predictor of negative outcomes in patientswith coronary artery disease8
• The prevalence for major depression among patientswith HIV or AIDS has been estimated to bebetween 15% and 40%, far exceeding that seen inthe general population9
• 40% of patients with Parkinson’s disease havecomorbid depression.10
Not surprisingly, depression plays a major role inoverall costs of healthcare services:
• Annual economic consequences of depression havebeen estimated at 11.5 billion euros in the UnitedKingdom and $83 billion in the United States
• The economic burden is staggering, with estimatesrunning as much as $51.5 billion a year in lost pro-ductivity.11 An additional $26.1 billion is spent formedical treatment11
• More than 70% of people diagnosed with depres-sion are employed, and depression results in 400million lost work days annually, according toKeith Dixon, PhD, president of Cigna BehavioralHealth. In the private sector, Dr Dixon notes,depressed employees use, on average, more than$4000/year in medical services compared with lessthan $1000/year used by employees withoutdepression, making depression a significant com-ponent of healthcare costs12
• Employers pay almost 75% of the $80-billion price tagfor treatment of depressive disorders each year.13 �
References1. Goodnick PJ, Hernandez M. Treatment of depression in comorbidmedical illness. Expert Opin Pharmacother. 2000;1(17):1367-1384. 2. Kessler RC, Chiu WT, Demier O, et al. Prevalence, severity, andcomorbidity of 12-month DSM-IV disorders in the National ComorbiditySurvey Replication. Arch Gen Psychiatry. 2005;62(6):617-627.3. Gorman JM. Comorbid depression and anxiety disorders. DepressAnxiety. 1996-1997;4:160-168. 4. The University of Florida Obsessive-Compulsive Disorder Program.http://www.ufocd.org/OtherConditions.htm. Accessed February 20, 2006.5. Penninx BW, Guralnik JM, Pahor M, et al. Chronically depressedmood and cancer risk in older persons. J Natl Cancer Inst. 1998;90(24):1888-1893.6. Derogatis LR, Morrow GR, Fetting J, et al. The prevalence of psychi-atric disorders among cancer patients. JAMA. 1983;249(6):751-757.7. Burgess C, Corneliu V, Love S, et al. Depression and anxiety in
women with early breast cancer: five year observational cohort study.BMJ. 2005;330(7493):702. 8. Vaccarino V, Karl SV, Abramson J, Krumholz HM. Depressive symp-toms and risk of functional decline and death in patients with heart fail-ure. J Am Coll Cardiol. 2001;38(1):199-205. 9. Angelino AF, Treisman GJ. Management of psychiatric disorders inpatients infected with human immunodeficiency virus. Clin Infect Dis.2001;33(6):847-856. 10. McDonald WM, Richard IH, DeLong MR. Prevalence, etiology, andtreatment of depression in Parkinson’s disease. Biol Psychiatry. 2003;54(3):363-375.11. Lerner D, Adler DA, Chang H, et al. Unemployment, job retention,and productivity loss among employees with depression. Psychiatr Serv.2004;55(12):1371-1378.12. Dixon K. Direct costs of depression in the workplace are tip of the ice-berg; employers have huge stake in promoting depression treatment.PRNewswire. October 13, 2005. http://www.prnewswire.com/cgibin/stories.pl?acct=104&story=/www/story/10-13-2005/0004167764&edate. Accessed February 20, 2006.13. Durso KA. Depression in the workplace: prevalence, cost and pro-ductivity impact. Employee Benefit News. December 2004. http://www.benefitnews.com/detail.cfm?id=6776&terms=%7Cpresenteeism%7C. Accessed February 20, 2006.
Unmanaged Moment
“From January to May I work for the governmentto pay for my income tax, and from May to October
to pay for my malpractice insurance.”
Continued from page 56
59www.AHDBonline.com
Executive SummariesThe UnbearableLightness ofMental Health By Alberto Colombi, MD, MPH
In his guest editorial, Dr AlbertoColombi, Medical Director at PPGIndustries, Pittsburgh, PA, points agentle finger at different stakehold-ers—employers, health insuranceplans, benefit design managers, aswell as the American public—charging all of us to consider mental“wellness” as important a concept asphysical well-being. Making thecase that mental health translatesinto wealth for employers, for healthplans, and for society at large, heurges decision makers in healthcareand all of those involved in thedelivery of patient care to placescreening, diagnosis, intervention,and referral of mental issues on thesame footing as the cardinal physicalconditions—diabetes, heart disease,and the metabolic syndrome. Usingself-reported data from his compa-ny’s employees, Dr Colombi makesthe business case that mental well-ness deserves as much attention as
physical wellness from an economicpoint of view, as well as from thevantage point of employees’ overallhealth and well-being and finallyfrom the perspective of the UShealthcare system in general.
Schizophrenia:Current Conceptsand Approachesto Patient CareBy Peter F. Buckley, MD, and AdrianaFoster, MD
Schizophrenia, the most seriousmental illness, is still poorly under-stood by scientists, and the lay pub-lic remains largely confused aboutthis condition and continues to har-bor notions that it is a “split person-ality” or a “Jekyll and Hyde” phe-nomenon. Dr Peter F. Buckley, aworld expert on schizophrenia andthe author of many books and arti-cles on the subject, is Professor andChair, Department of Psychiatryand Health Behavior, MedicalCollege of Georgia, Atlanta. He andDr Foster outline what is known
today about this serious conditionand why correct treatment is soimportant. Stigma, which is fueledby a lack of knowledge, is a majorobstacle in the management ofschizophrenia, Dr Buckley pointsout. Antipsychotic medications,both the older, so-called typicalagents, and the second-generation,atypical medications, form thebedrock for treatment. These drugsare effective, but patients vary intheir response to each drug and theirside-effect profile. Individual differ-ences among the available medica-tions suggest that trials with a differ-ent medication may be appropriatewhen one agent fails or is not appro-priate for the specific patient.Therefore, allowing physicians toprescribe the drug that is best suitedfor the individual patient, regardlessof cost, is crucial. Just as importantis monitoring for side effects, toensure efficacy and compliance.Patients often stop taking their med-ications for a variety of reasons,which invariably will lead mostpatients to a relapse of illness. DrBuckley emphasizes the need forappropriate and individualized man-agement of each patient with thebest available treatments.
SUBSCRIBE TO
at www.AHDBonline.comEngage Healthcare Communications, LLC • 241 Forsgate Drive-Suite 205A • Jamesburg, New Jersey 08831
Continued on page 60

Trends inPharmaceuticalExpenditures:The Impact onDrug BenefitDesignBy Joanne LaFleur, PharmD, MSPH;Leslie Fish, PharmD; and Diana I. Brixner, RPh, PhD
In the 1990s, national spendingon pharmaceuticals increased at arapid pace, outpacing increases onhospital and physician services,which had dominated the industryin the years before. However, thistrend has shifted in the past fewyears, as is evident from currentnational data. Dr Joanne LaFleur,Research Assistant Professor, Uni -versity of Utah PharmacotherapyOutcomes Research Center, SaltLake City, and colleagues describethe new declining spending trendsand offer the reasons for thesetrends. Among the forces pushingtraditional pharmaceuticals downare the increasing use of genericsand the growing role of biologicagents. Dr LaFleur and colleaguespropose that this new drug trendpresents an opportunity for healthplans to evaluate the value of cur-rent and new drug benefit strategiesand implement value-based benefitdesigns in accordance with theshifting focus in healthcare towardpersonalized patient care. They fur-ther suggest that value-based drugbenefit design should lead to over-all cost-efficiencies by designingaccess according to patient popula-tions rather than by cost.
MedicareCoverage forErythropoiesis-StimulatingAgents: ThePerfect Storm Part 1 of an interview with Samuel M.Silver, MD, PhD
In 2007, Medicare changed theirpolicy regarding payment for erythro-poiesis-stimulating agents (ESAs), alucrative class of anemia drugs, thusexerting an almost immediate influ-ence on carriers and limiting the useof these agents. Although somestates have mandates that preventhealth plans from taking the actionprescribed by Medicare, the agency
still wields a great influence. DrSamuel Silver, Director of theCancer Center Network, Division ofHema tology/Oncology, Universityof Michigan Health Systems, AnnArbor, is finishing his term on theAmerican Society of HematologyExecutive Committee and alsoserves on several committees at theAmerican Society of ClinicalOncology. Dr Silver describes theevolution of the clinical use of ESAsfrom a way to avoid transfusion to aquality-of-life issue and the implica-tions of this shift in practice. He alsoelaborates on the effect ofMedicare’s reimbursement policieson health plans and clinicians andhas suggested to members ofCongress and to the Centers forMedicare & Medicaid Services toreview the current database prospec-tively to assess the use of transfusionin cancer patients in relation to therecent policy changes. �
60 AMERICAN HEALTH & DRUG BENEFITS May 2008
EXECUTIVE SUMMARIES
Unmanaged Moment
“There’s a placebo among us!”

Brief Summary of Prescribing Information
USE IN PREGNANCYWhen used in pregnancy during the second and third trimesters, drugs that act directly on therenin-angiotensin system can cause injury and even death to the developing fetus. When pregnancy is detected, MICARDIS® tablets should be discontinued as soon as possible.See WARNINGS: Fetal/Neonatal Morbidity and Mortality
INDICATIONSMICARDIS is indicated for the treatment of hypertension. It may be used alone or in combination with otherantihypertensive agents.
CONTRAINDICATIONSMICARDIS (telmisartan) is contraindicated in patients who are hypersensitive to any component of this product.
WARNINGSFetal/Neonatal Morbidity and Mortality Drugs that act directly on the renin-angiotensin system can causefetal and neonatal morbidity and death when administered to pregnant women. Several dozen cases have beenreported in the world literature in patients who were taking angiotensin converting enzyme inhibitors. Whenpregnancy is detected, MICARDIS (telmisartan) tablets should be discontinued as soon as possible. The use ofdrugs that act directly on the renin-angiotensin system during the second and third trimesters of pregnancyhas been associated with fetal and neonatal injury, including hypotension, neonatal skull hypoplasia, anuria,reversible or irreversible renal failure, and death. Oligohydramnios has also been reported, presumablyresulting from decreased fetal renal function; oligohydramnios in this setting has been associated with fetallimb contractures, craniofacial deformation, and hypoplastic lung development. Prematurity, intrauterinegrowth retardation, and patent ductus arteriosus have also been reported, although it is not clear whetherthese occurrences were due to exposure to the drug. These adverse effects do not appear to have resultedfrom intrauterine drug exposure that has been limited to the first trimester. Mothers whose embryos andfetuses are exposed to an angiotensin II receptor antagonist only during the first trimester should be soinformed. Nonetheless, when patients become pregnant, physicians should have the patient discontinue theuse of MICARDIS tablets as soon as possible. Rarely (probably less often than once in every thousandpregnancies), no alternative to an angiotensin II receptor antagonist will be found. In these rare cases, the mothersshould be apprised of the potential hazards to their fetuses, and serial ultrasound examinations should beperformed to assess the intra-amniotic environment. If oligohydramnios is observed, MICARDIS tablets shouldbe discontinued unless they are considered life-saving for the mother. Contraction stress testing (CST), anon-stress test (NST), or biophysical profiling (BPP) may be appropriate, depending upon the week ofpregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear untilafter the fetus has sustained irreversible injury. Infants with histories of in utero exposure to an angiotensinII receptor antagonist should be closely observed for hypotension, oliguria, and hyperkalemia. If oliguriaoccurs, attention should be directed toward support of blood pressure and renal perfusion. Exchangetransfusion or dialysis may be required as a means of reversing hypotension and/or substituting fordisordered renal function. There is no clinical experience with the use of MICARDIS tablets in pregnantwomen. No teratogenic effects were observed when telmisartan was administered to pregnant rats at oraldoses of up to 50 mg/kg/day and to pregnant rabbits at oral doses up to 45 mg/kg/day. In rabbits,embryolethality associated with maternal toxicity (reduced body weight gain and food consumption) wasobserved at 45 mg/kg/day [about 12 times the maximum recommended human dose (MRHD) of 80 mg on amg/m2 basis]. In rats, maternally toxic (reduction in body weight gain and food consumption) telmisartandoses of 15 mg/kg/day (about 1.9 times the MRHD on a mg/m2 basis), administered during late gestation andlactation, were observed to produce adverse effects in neonates, including reduced viability, low birth weight,delayed maturation, and decreased weight gain. Telmisartan has been shown to be present in rat fetusesduring late gestation and in rat milk. The no observed effect doses for developmental toxicity in rats andrabbits, 5 and 15 mg/kg/day, respectively, are about 0.64 and 3.7 times, on a mg/m2 basis, the maximumrecommended human dose of telmisartan (80 mg/day). Hypotension in Volume-Depleted Patients Inpatients with an activated renin-angiotensin system, such as volume- and/or salt-depleted patients (e.g., those being treated with high doses of diuretics), symptomatic hypotension may occur after initiation oftherapy with MICARDIS® tablets. This condition should be corrected prior to administration of MICARDIS tablets,or treatment should start under close medical supervision with a reduced dose. If hypotension does occur, thepatient should be placed in the supine position and, if necessary, given an intravenous infusion of normalsaline. A transient hypotensive response is not a contraindication to further treatment, which usually can becontinued without difficulty once the blood pressure has stabilized.PRECAUTIONSGeneral. Impaired Hepatic Function: As the majority of telmisartan is eliminated by biliary excretion, patientswith biliary obstructive disorders or hepatic insufficiency can be expected to have reduced clearance. MICARDIS(telmisartan) tablets should be used with caution in these patients. Impaired Renal Function: As a consequenceof inhibiting the renin-angiotensin-aldosterone system, changes in renal function may be anticipated insusceptible individuals. In patients whose renal function may depend on the activity of the renin-angiotensin-aldosterone system (e.g., patients with severe congestive heart failure), treatment with angiotensin-converting enzyme inhibitors and angiotensin receptor antagonists has been associated with oliguria and/orprogressive azotemia and (rarely) with acute renal failure and/or death. Similar results may be anticipatedin patients treated with MICARDIS tablets. In studies of ACE inhibitors in patients with unilateral or bilateralrenal artery stenosis, increases in serum creatinine or blood urea nitrogen were observed. There has beenno long term use of MICARDIS tablets in patients with unilateral or bilateral renal artery stenosis but an effectsimilar to that seen with ACE inhibitors should be anticipated. Information for Patients. Pregnancy: Femalepatients of childbearing age should be told about the consequences of second- and third-trimester exposureto drugs that act on the renin-angiotensin system, and they should also be told that these consequences donot appear to have resulted from intrauterine drug exposure that has been limited to the first trimester. Thesepatients should be asked to report pregnancies to their physicians as soon as possible. Drug Interactions.Digoxin: When telmisartan was coadministered with digoxin, median increases in digoxin peak plasmaconcentration (49%) and in trough concentration (20%) were observed. It is, therefore, recommended thatdigoxin levels be monitored when initiating, adjusting, and discontinuing telmisartan to avoid possible over-or under-digitalization. Warfarin: Telmisartan administered for 10 days slightly decreased the mean warfarintrough plasma concentration; this decrease did not result in a change in International Normalized Ratio (INR).Other Drugs: Coadministration of telmisartan did not result in a clinically significant interaction withacetaminophen, amlodipine, glibenclamide, simvastatin, hydrochlorothiazide or ibuprofen. Telmisartan is notmetabolized by the cytochrome P450 system and had no effects in vitro on cytochrome P450 enzymes,except for some inhibition of CYP2C19. Telmisartan is not expected to interact with drugs that inhibitcytochrome P450 enzymes; it is also not expected to interact with drugs metabolized by cytochrome P450enzymes, except for possible inhibition of the metabolism of drugs metabolized by CYP2C19.Carcinogenesis, Mutagenesis, Impairment of Fertility There was no evidence of carcinogenicity whentelmisartan was administered in the diet to mice and rats for up to 2 years. The highest doses administered tomice (1000 mg/kg/day) and rats (100 mg/kg/day) are, on a mg/m2 basis, about 59 and 13 times, respectively,the maximum recommended human dose (MRHD) of telmisartan. These same doses have been shown toprovide average systemic exposures to telmisartan >100 times and >25 times, respectively, the systemicexposure in humans receiving the MRHD (80 mg/day). Genotoxicity assays did not reveal any telmisartan-related effects at either the gene or chromosome level. These assays included bacterial mutagenicity testswith Salmonella and E. coli (Ames), a gene mutation test with Chinese hamster V79 cells, a cytogenetic testwith human lymphocytes, and a mouse micronucleus test. No drug-related effects on the reproductiveperformance of male and female rats were noted at 100 mg/kg/day (the highest dose administered), about 13times, on a mg/m2 basis, the MRHD of telmisartan. This dose in the rat resulted in an average systemic exposure(telmisartan AUC as determined on day 6 of pregnancy) at least 50 times the average systemic exposure inhumans at the MRHD (80 mg/day). Pregnancy Pregnancy Categories C (first trimester) and D (second andthird trimesters). See WARNINGS, Fetal/Neonatal Morbidity and Mortality. Nursing Mothers It is notknown whether telmisartan is excreted in human milk, but telmisartan was shown to be present in the milk oflactating rats. Because of the potential for adverse effects on the nursing infant, a decision should be made whetherto discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.Pediatric Use Safety and effectiveness in pediatric patients have not been established. Geriatric Use Of thetotal number of patients receiving MICARDIS in clinical studies, 551 (18.6%) were 65 to 74 years of age and 130(4.4%) were 75 years or older. No overall differences in effectiveness and safety were observed in these patientscompared to younger patients and other reported clinical experience has not identified differences in responsesbetween the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
ADVERSE REACTIONSMICARDIS (telmisartan) has been evaluated for safety in more than 3700 patients, including 1900 treated for
over six months and more than 1300 for over one year. Adverse experiences have generally been mild andtransient in nature and have only infrequently required discontinuation of therapy. In placebo-controlled trialsinvolving 1041 patients treated with various doses of telmisartan (20-160mg) monotherapy for up to 12 weeks,an overall incidence of adverse events similar to that of placebo was observed. Adverse events occurring at anincidence of 1% or more in patients treated with telmisartan and at a greater rate than in patients treated withplacebo, irrespective of their causal association, are presented as follows: The most common adverse eventsoccurring with MICARDIS Tablets monotherapy at a rate of e1% and greater than placebo, respectively, were:upper respiratory tract infection (URTI) (7%, 6%), back pain (3%, 1%), sinusitis (3%, 2%), diarrhea (3%, 2%), andpharyngitis (1%, 0%). In addition to the adverse events, the following events occurred at a rate of 1% but wereat least as frequent in the placebo group: influenza-like symptoms, dyspepsia, myalgia, urinary tract infection,abdominal pain, headache, dizziness, pain, fatigue, coughing, hypertension, chest pain, nausea and peripheraledema. Discontinuation of therapy due to adverse events was required in 2.8% of 1455 patients treated withMICARDIS tablets and 6.1% of 380 placebo patients in placebo-controlled clinical trials. The incidence of adverseevents was not dose-related and did not correlate with gender, age, or race of patients. The incidence of coughoccurring with telmisartan in six placebo-controlled trials was identical to that noted for placebo-treatedpatients (1.6%). In addition to those listed above, adverse events that occurred in more than 0.3% of 3500patients treated with MICARDIS monotherapy in controlled or open trials are listed below. It cannot bedetermined whether these events were causally related to MICARDIS tablets: Autonomic Nervous System:impotence, increased sweating, flushing; Body as a Whole: allergy, fever, leg pain, malaise; Cardiovascular:palpitation, dependent edema, angina pectoris, tachycardia, leg edema, abnormal ECG; CNS: insomnia,somnolence, migraine, vertigo, paresthesia, involuntary muscle contractions, hypoaesthesia; Gastrointestinal:flatulence, constipation, gastritis, vomiting, dry mouth, hemorrhoids, gastroenteritis, enteritis, gastroesophageal reflux,toothache, non-specific gastrointestinal disorders; Metabolic: gout, hypercholesterolemia, diabetes mellitus;Musculoskeletal: arthritis, arthralgia, leg cramps; Psychiatric: anxiety, depression, nervousness; ResistanceMechanism: infection, fungal infection, abscess, otitis media; Respiratory: asthma, bronchitis, rhinitis, dyspnea,epistaxis; Skin: dermatitis, rash, eczema, pruritus; Urinary: micturition frequency, cystitis; Vascular:cerebrovascular disorder; and Special Senses: abnormal vision, conjunctivitis, tinnitus, earache. During initialclinical studies, a single case of angioedema was reported (among a total of 3781 patients treated withtelmisartan). Clinical Laboratory Findings In placebo-controlled clinical trials, clinically relevant changes instandard laboratory test parameters were rarely associated with administration of MICARDIS tablets.Hemoglobin: A greater than 2 g/dL decrease in hemoglobin was observed in 0.8% telmisartan patientscompared with 0.3% placebo patients. No patients discontinued therapy due to anemia. Creatinine: A 0.5 mg/dLrise or greater in creatinine was observed in 0.4% telmisartan patients compared with 0.3% placebopatients. One telmisartan-treated patient discontinued therapy due to increases in creatinine and blood ureanitrogen. Liver Enzymes: Occasional elevations of liver chemistries occurred in patients treated withtelmisartan; all marked elevations occurred at a higher frequency with placebo. No telmisartan-treatedpatients discontinued therapy due to abnormal hepatic function. Post-Marketing Experience The followingadverse reactions have been identified during post-approval use of MICARDIS tablets. Because these reactionsare reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate theirfrequency or establish a causal relationship to drug exposure. Decisions to include these reactions in labelingare typically based on one or more of the following factors: (1) seriousness of the reaction, (2) frequency ofreporting, or (3) strength of causal connection to MICARDIS tablets. The most frequently spontaneously reportedevents include: headache, dizziness, asthenia, coughing, nausea, fatigue, weakness, edema, face edema, lowerlimb edema, angioneurotic edema, urticaria, hypersensitivity, sweating increased, erythema, chest pain, atrialfibrillation, congestive heart failure, myocardial infarction, blood pressure increased, hypertension aggravated,hypotension (including postural hypotension), hyperkalemia, syncope, dyspepsia, diarrhea, pain, urinary tractinfection, erectile dysfunction, back pain, abdominal pain, muscle cramps (including leg cramps), myalgia,bradycardia, eosinophilia, thrombocytopenia, uric acid increased, abnormal hepatic function/liver disorder, renalimpairment including acute renal failure, anemia, and increased CPK. Rare cases of rhabdomyolysis have beenreported in patients receiving angiotensin II receptor blockers, including MICARDIS.
OVERDOSAGELimited data are available with regard to overdosage in humans. The most likely manifestation of overdosagewith MICARDIS (telmisartan) tablets would be hypotension, dizziness and tachycardia; bradycardia couldoccur from parasympathetic (vagal) stimulation. If symptomatic hypotension should occur, supportive treatment should be instituted. Telmisartan is not removed by hemodialysis.
DOSAGE AND ADMINISTRATIONDosage must be individualized.The usual starting dose of MICARDIS (telmisartan) tablets is 40 mg once a day. Bloodpressure response is dose related over the range of 20-80 mg. Special Populations:Patients with depletion ofintravascular volume should have the condition corrected or MICARDIS tablets should be initiated underclose medical supervision (see WARNINGS, Hypotension in Volume-Depleted Patients). Patients withbiliary obstructive disorders or hepatic insufficiency should have treatment started under close medicalsupervision (see PRECAUTIONS, General, Impaired Hepatic Function, and Impaired Renal Function). Mostof the antihypertensive effect is apparent within two weeks and maximal reduction is generally attained afterfour weeks. When additional blood pressure reduction beyond that achieved with 80 mg MICARDIS isrequired, a diuretic may be added. No initial dosing adjustment is necessary for elderly patients or patientswith mild-to-moderate renal impairment, including those on hemodialysis. Patients on dialysis may developorthostatic hypotension; their blood pressure should be closely monitored. MICARDIS tablets may beadministered with other antihypertensive agents. MICARDIS tablets may be administered with or without food.
Rx only
MC-BS (03/07)
Copyright © 2007, Boehringer Ingelheim Pharmaceuticals, Inc. All rights reserved.
Printed in U.S.A. (10/07) MC48827
MICARDIS is indicated for the treatment of hypertension. It may be used alone or in combination with other antihypertensive agents.
MICARDIS is contraindicated in patients who are hypersensitive to any component of this product. The most common adverse events occurring withMICARDIS Tablets monotherapy at a rate of e1% and greater than placebo, respectively, were: upper respiratory tract infection (URTI) (7%, 6%), back pain(3%, 1%), sinusitis (3%, 2%), diarrhea (3%, 2%), and pharyngitis (1%, 0%).
Please see Brief Summary of Product Information on adjacent page.
USE IN PREGNANCYWhen used in pregnancy during the second and third trimesters, drugs that act directly on the renin-angiotensin system can causeinjury and even death to the developing fetus. When pregnancy is detected, MICARDIS Tablets should be discontinued as soon as possible(see WARNINGS, Fetal/Neonatal Morbidity and Mortality).
Copyright © 2007, Boehringer Ingelheim Pharmaceuticals, Inc. All rights reserved. Printed in U.S.A. (10/07) MC48828
����������������������������������������������������������1
��������� More than ������������������� in the early morning2
References: 1. Weber MA,White WB, Giles TD, et al. An effectiveness study comparing algorithm-based antihypertensivetherapy with previous treatments using conventional and ambulatory blood pressure measurements. J Clin Hypertens.2006;8:241-250. 2. White WB, Giles T, Bakris GL, et al. Measuring the efficacy of antihypertensive therapy by ambulatoryblood pressure monitoring in the primary care setting. Am Heart J. 2006;151:176-184.
Please visit www. micardis.com for more information, including Prescribing Information.


















