Maxillary sinus and develoment
71
Dr V.RAMKUMAR Dr V.RAMKUMAR CONSULTANT CONSULTANT DENTAL&FACIOMAXILLARY SURGEON ENTAL&FACIOMAXILLARY SURGEON REG NO: 4118 –TAMILNADU- REG NO: 4118 –TAMILNADU- INDIA(ASIA) INDIA(ASIA) Maxillar y sinus
-
Upload
vasanramkumar -
Category
Documents
-
view
215 -
download
4
Transcript of Maxillary sinus and develoment

Dr V.RAMKUMARDr V.RAMKUMARCONSULTANT CONSULTANT
DENTAL&FACIOMAXILLARY DENTAL&FACIOMAXILLARY SURGEONSURGEON
REG NO: 4118 –TAMILNADU-REG NO: 4118 –TAMILNADU-INDIA(ASIA)INDIA(ASIA)
Maxillary sinus

Development and Anatomy

The maxillary sinus is the first of the paranasal sinuses to develop.
Appears as a lateral evagination or pouch of the mucous membrane of the middle meatus of the nose at about the third month of intra-uterine life.
The neck of the pouch remains small and forms the future ostium.

At birth, less than a cm in any direction Expands by pneumatization into the
developing alveolar process
Later on, extends anteriorly and inferiorly from skull base closely matching the growth rate of the maxilla and the developing dentition
Expansion ceases after eruption of the permanent teeth



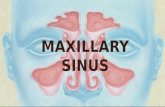
Paranasal sinuses in the adult and there communications

Largest of the paranasal sinuses, pyramidal shape, the base being the lateral nasal wall and the apex extends into the zygomatic process of the maxilla
The upper wall or the roof of the sinus is also the floor of the orbit
The floor of the sinus forms the base of the alveolar process

The posterior wall extends the length of the maxilla and dips into the maxillary tuberosity
Anterolaterally the sinus extends into the region of first bicuspid or cuspid teeth
Opens into the nasal cavity through the middle meatus
The average diameter would be from 30-34mm and volume being about 15cc

Blood supply –From small artery derived from the facial,
maxillary, infra-orbital, and greater palatine arteries.
Venous drainage –Accompany the arteries and drain into
anterior facial vein pterygoid plexus
Lymphatic drainage –Submandibular lymphatic glands

Physiology
Sinuses lined by respiratory epithelium – mucous-secreting pseudostratified ciliated columnar epithelium and periosteum.
Mucociliary mechanism provides the means for the removal of particulate matter and bacteria.
Mucous and other debris discharged into the middle meatus of the nose.

Functions
Impart resonance to the voice during speech.
Lighten the skull.
Warm the inspired air
Increases the surface area

Investigations

Radiological examination
Normal – Well defined radio opaque margins Normal – Well defined radio opaque margins with radiolucency throughout with radiolucency throughout

Common RadiographsCommon Radiographs
- Water’s View - Water’s View (15(15 Occipito Occipito – mental)– mental)
- Submentovertex view - Submentovertex view
- Lateral view of the - Lateral view of the sinuses sinuses
- IOPA radiograph- IOPA radiograph

Water’s View Water’s View (15(15 Occipito – Occipito – mental)mental)

Submentovertex viewSubmentovertex view

Lateral view of the sinusesLateral view of the sinuses

IOPA radiographIOPA radiograph

Infections Infections
Mucosal Lining thickensMucosal Lining thickens
( Radiolucency )( Radiolucency )
Radio opacityRadio opacity
Solid Masses Solid Masses
AntrolithAntrolith
OsteomaOsteoma
Fibro osseous lesions Fibro osseous lesions
Dense radio opacitiesDense radio opacities

Cysts
Round or oval radiolucency circumscribed by a sharp radio opaque margin

‘‘Y’ shaped line of EnnisY’ shaped line of Ennis
The line of junction of the lateral wall of the nose and the nasal floor is represented by the long leg of the letter ‘y’. A cyst in the area obliterates & modifies the typical pattern.

Relationship of the sinus Relationship of the sinus with with the Max. Molars the Max. Molars

Additional Investigations
CT
MRI
FESS Biopsy/FNAC
Trans-illumination

CT SCAN

Diseases of maxillary sinus

Maxillary Sinus
Inflammation
Benign lesions Malignancy
Fungal infectionsFibro osseous lesions

Sinusitis (acute / chronic)
Spread of infection from a dental abscess Facial fracture involving the maxillary sinus Tooth or root in the maxillary sinus Oro-antral fistulae Cysts Polyps Thickening of the sinus walls Dental prosthetic material (rear)
Commonly..
Causes:

Acute maxillary sinusitis
Symptoms:
Heavy felling in the face. Throbbing pain in the upper part of the
cheek or entire of the face which increases on bending the head.
Foul unilateral discharge Foul taste in the mouth Pyrexia Nocturnal coughing

Chronic maxillary sinusitis
Symptoms: History of repeated attacks of acute
mucopurulent rhinitis. Pain and tenderness are common. Diagnosis depends on long history of
standing nasal or post nasal discharge. Inspection of oropharynx frequently confirm
the existence of a descending pharyngeal exudate.
Pain is feature of chronic sinusitis of dental origin.
Lump on the gum

Management of sinusitis

Non – Surgical
Surgical
Management of sinusitis

Medical (non-surgical)…
Analgesics (for acute form) Anti-histamines Topical intranasal steroid Antibiotics Remove source of infection If no improvement…surgical intervention Decongestants Steam inhalation

Surgical options…
Caldwell-Luc antrostomy
Needle sinusotomy
Functional Endoscopic Sinus Surgery (FESS)
Maxillectomy = malignancy

Trouble-shooting Areas Of Dental Interest
Displacement of root into the sinus
Fracture of the maxillary tuberosity
Oro-antral Fistula

Root displacement into the antrum
Sudden disappearance of the root from the socket during extraction
Accompanied by a) Unilateral epistaxisb) Escape of fluids from the mouth into the
nosec) Passage of air into the mouth when the
patient sucks or swallows

Alteration in vocal resonance
Difficulty in blowing out the cheeks or drawing on a cigarette

Delayed clinical disturbances
Unilateral nasal discharge of pus
Foul or salty taste Facial pain
Sinusitis

Radiological examination
Periapical view positioned well apically
True occlusal radiograph

Indications for removal
Small fragments - probably unnecessary surgery
Secondary infection, severe sinusitis

Surgery for removal
Caldwell-Luc Operation

CAUSES:
Invasion of tuberosity by the antrum
Common in isolated maxillary molars
Divergent or hypercementosed roots

If fracture occurs…
Bony fragment and the tooth should be freed from the soft tissues followed by
apposition of soft tissue by mattress sutures

Oro-antral fistulaOro-antral fistula
It is a pathological or unnatural communication between the oral cavity and maxillary sinus
Fistula always lined by epithelium and is long standing

Contd..
Acute form is oro-antral communication
If oro-antral communication does not heal or is untreated, epithelial tract forms

Predisposing factors
When apices of the upper teeth and the lining of the maxillary sinus are intimately related
Chronic apical or advanced periodontal disease replaces apical bone with granulation tissue
In suspected cases traumatizing the socket

When the sinus is infected, the infection destroys the clot in the socket
Excessive damage to the bone of the socket the loss of the clot
Upper first molar- risky

On examination..
An obvious large opening leading into the sinus
Symptoms as per root in antrum
Small perforation - difficult to detect
Never probe or abuse a socket

Pinch nose and blow gently
Whistling noise may be heard as air escapes from the fistula

Large Oro-antral fistula – good drainage, seldom sinusitis
Pin hole fistula- no drainage, chances of sinusitis

Treatment
Suture socket , antibiotics, nasal decongesants, preserve and protect clot, overdenture obturator- normally heal

Primary closurePrimary closure

2-3 days delay… same treatment

Late presentation…
After a week
Formation of fistulous tract - to be excised
Maxillary sinusitis – if present to be treated
Attempt surgical closure

Approaches
Simple suturesSimple sutures ( Primary ( Primary
closure)closure)
FlapsLocal Distant

Local Flaps
Buccal approach= von Reherman’s flap
Palatal approach= Ashley’s flap
Combination of buccal and palatal flaps


Buccal approach
Local anaesthesiaA) Excision of epithelial tract
B) Buccal flap, von Reherman’s flap- divergent incision into the buccal sulcus-
3- 4 mm from each side of the resulting alveolar defect
horizontal incision in taut periosteum to mobilize the mucoperiosteal flap

Contd..
.. the free margin of the buccal flap rests on
the palatal mucoperiosteum on sound bone where it is sutured covering the Oro-antral fistula


2nd approach
Palatal transposition flap (Ashley’s flap)
- based on greater palatine artery - thicker flap - longitudinal incision about 4-5 mms
above the gingival margin

Contd…
Followed by a parallel incision
Almost along the midline of the palate
Both incisions connected anteriorly with a U shaped cut
The thick palatal flap is rotated to cover the alveolar orifice with edges resting on sound bone for healing


TUMOURS INVADING THE TUMOURS INVADING THE SINUSSINUS
Ohngren’s lineOhngren’s lineImaginary plane Imaginary plane
depicted by a line depicted by a line joining the medial joining the medial canthus of the eye canthus of the eye to the angle of the to the angle of the mandible, dividing mandible, dividing the nasal cavity and the nasal cavity and the antrum into two the antrum into two halves halves

Infrastructure – Anterior and InferiorInfrastructure – Anterior and Inferior
– – Readily amenable to Readily amenable to surgery surgery with fair with fair prognosis prognosis
Supra Structure – Posterior and SuperiorSupra Structure – Posterior and Superior – – Not Readily amenable to Not Readily amenable to surgery, poor prognosis surgery, poor prognosis

Clinical Features
Ulcer, Swelling, Mobile Teeth & Pain (Nerve Involvement)
Management - Maxillectomy
• Partial/Limited
• Subtotal
• Total

Subtotal MaxillectomyLarger lesions of the gums, palate or the antrum which extend to the superior aspects or beyond the confines of the antrum
Proposed Bony cuts

Total MaxillectomyPrimary Tumours filling the entire antrum In some cases infra orbital rim is preserved


SINUS LIFTSINUS LIFT
Posterior Maxillary Height Posterior Maxillary Height Deficiencies while placing Deficiencies while placing implantsimplants
Closed or open method Closed or open method Osteotomes used to in-fracture Osteotomes used to in-fracture
the antral floor the antral floor Bone GraftsBone Grafts

Thank You