Maternal mortality
31
Why mother’s die??
-
Upload
chaimingcheng -
Category
Documents
-
view
169 -
download
3
Transcript of Maternal mortality

Why mother’s die??

THE REALITY….
One woman dies every minute
somewhere in the world because of
a complication related to pregnancy
or childbirth
80% of these death could be
prevented

MATERNAL MORTALITY
“The death of a woman while pregnant or within 42
days of termination of pregnancy, from any cause
related to or aggravated by the pregnancy or its
management, but not from accidental or
incidental causes”
- by FIGO

CLASSIFICATION
DirectDeaths resulting from obstetric
complications in pregnancy, labour and puerperium
IndirectDeaths resulting from previous existing
disease or diseases that developed during pregnancy and which was aggravated during pregnancy
FortuitousDeaths from other causes not related to
or influenced by pregnancy
LateDeath after 6 weeks until 1 year after
delivery

Classifiction Examples
Direct Thromboembolism
Haemorrhage
Ectopics
Hypertensive disease of pregnancy
Sepsis
Amniotic fluid embolism
Indirect Cardiac disease
Suicide
Epilepsy/CNS haemorrhage
Infections
Respiratory/gastrointestinal diseases

MMR
(Maternal mortality ratio)
Maternal mortality ratio (MMR) is the number of
women who die during pregnancy and childbirth, per
100,000 live births.
No of women dies
100,000 live births
National MMR have reached a plateau
between 28-30/100,000 LB the last 10 years

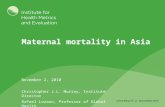
OUR STATE….
There is marked reduction in MMR in our state
YEAR MMR ( per 100,000 live
births)
2008 30.8
2009 26
2010 21.3
2011 21.7
2012 26.6
2013 9.3 (*** achieve MDG 5
target)
0
5
10
15
20
25
30
35
2008
2009
2010
2011
2012
2013
MMR
MMR

Causes of maternal death (malaysia)

4 MAIN CAUSES OF MATERNAL DEATH IN
SARAWAK
1. Post partum haemorrhage
2. Pulmonary embolism
3. Eclampsia
4. Cardiac disease

Maternal death according to
antenatal care

Phase of maternal death


MILLENIUM
DEVELEPMENTAL GOAL
(MDG)

MDG 5A: IMPROVE MATERNAL
HEALTH
TARGET Reduce maternal mortality ratio by
three quarters between 1990 and 2015
Indicators
- Maternal mortality ratio
- Proportion of birth attended by skilled health
MDG 5 target for state by 2015 – 11.08/100,000
LB

MDG 5B- IMPROVE MATERNAL
HEALTH
TARGET Universal access to
reproductive health by 2015
Indicators
- Contraceptive prevalence rate
- Adolescent birth rate
- Antenatal care coverage
- Unmet need for family planning


ISSUES & CHALLENGES….

HIGH RISK GROUPS
Remote communities
Illegal immigrants
High risk pregnancies
** SPECIAL ATTENTION
** CLOSE MONITORING

DEFICIENCIES NOTED FROM STATE
CEMD
Directives & guidelines not followed
Lack of blood & blood products in DH
Substandard management of PPH at DH
Delays in transferring ill patients to specialist hospitals
Obstetric patients only seen by MA in A&E or OPD
Unsafe clinical practices in LW
Inadequate post natal care
Failure to offer TOP in early pregnancy by physicians and cardiologists
More specialists & specialist hospitals!

Lessons from National CEMD
More than 60% of maternal deaths occurred
during the postnatal period
The risk of maternal deaths higher in women over
40 yrs and in mothers who already had 6 or more
children
Deaths due to obstetric embolism is rising
Unbooked cases have higher risk of mortality
Home deliveries is unsafe

WHAT SHOULD WE DO???

Plan of Action: 1 Hospital Directors should address individual hospital
needs in terms of manpower and O&G medical
equipment and ambulances
Monitoring & resuscitative equipments are old and
lacking
JKN to highlight & forward asset request to MOH
To make carboprost (haemabate), intrauterine
balloon (Bakri balloon) & magnesium sulphate
available in all DH and health centers that conducts
deliveries
Need for equipped ambulance and transport for
‘home visiting’

Plan of Action: 2
All previous and future directives from JKNS and
O&G guidelines MUST be implemented and
practiced
Staff should be briefed
Should be kept in a file and made easily
accessible in LW and A&E/OPD for reference
Perhaps LW nursing sister can be assigned?

Plan of Action: 3
All antenatal and postnatal mothers should be
considered as HIGH RISK when attending
OPD/A&E and MUST reviewed by a medical
officer
Low tolerance for admission
All repeat A&E visits for the same complaints
should be admitted for further monitoring and
management

Plan of Action: 4
Ensuring the level of blood and FFP in every
hospital is always at optimal level
Yellow alert should be at 70% optimum stock
Red alert should be at 50% optimum stock
Increase FFP stock by 20% if possible
A laboratory staff should be assigned to be in
charge
Stock level should be checked daily

Plan of Action: 5
Improving the management of PPH in district
hospitals:
1. Compulsory regular obstetric drills (3x/year)
2. ‘Red Alert’ system to be implemented
3. PPH box to be made available and regularly
checked
4. Carboprost at least 4 ampoules must be made
available in LW
5. BAKRI balloons once used have to be indented
6. ‘PPH management flowchart’ have to be on the
notice board
7. Ambulance driver should called once Red Alert is
activated

Plan of Action: 6
Reduce delays in transferring ill obstetric patients
Refer to specialist early!
Utilise the BUDDY SPECIALIST system
Discuss various scenarios and decide best way to
reduce transit time
All hospital directors to be well versed with SOP
on using medevac services

Plan of Action: 7
Improve O&G clinical services at the district
hospital level through:
1. CME activities (monthly)
2. Clinical audit of near misses and bad outcome
(monthly)
3. ‘Buddy Specialist’ to do supervisory visits (6
monthly)
4. Regular drills for obstetric emergencies

Plan of Action 8 Start Pre-pregnancy care & family planning services in all hospitals in 2011 (MDG 5)
Counseling for family planning for all postnatal patients compulsory
IUCD should be made an acceptable alternative to BTL, particularly in specialist hospitals where the waiting list for BTL is longer than 6 months
‘High risk patients’ needs to be identified and managed accordingly (inc. postnatal BTL)

Plan of Action 9
Audit
Audit activities for all ‘near misses’ &
complications should be carried out on weekly
basis
The only way to identify weaknesses and to
improve services
Feedback on audit activities by each hospital
should be made compulsory