Maternal & Fetal Safety in Labor & Delivery Laleh Eslamian MD. Associated Prof. Maternal Fetal...
27
-
Upload
eugene-claxon -
Category
Documents
-
view
222 -
download
0
Transcript of Maternal & Fetal Safety in Labor & Delivery Laleh Eslamian MD. Associated Prof. Maternal Fetal...

Maternal & Fetal Safety in
Labor & Delivery
Laleh Eslamian MD. Associated Prof.
Maternal Fetal Medicine, Shariati hospital, TUMS
Observational studies:
- Fecal incontinence in parous sisters> nulliparous sisters (2 – 3times)
- Urinary incontinence in parous sisters> nulliparous sisters (4 times)
- Among Pre menopausal women: SUI in parous > nulliparous.
- Among Post menopausal women: Hx of pregnancy & child birth: little
impact on SUI (Medications, age …)
- Among Post menopausal women: Hx of at least 1 delivery:
↑ 2 times prolapse – C/R – RVO than nulliparas
ASSOCIATION BETWEEN PFD
&
Pregnancy & Delivery
50% of incontinence, 75% of prolapse
Pregnancy & child birth → pelvic floor injury
Compression
Stretching
Tearing of nerves, muscles & connective tissue
Pelvic floor injury in pregnancy &child birth
are due to
Neural injury:
Anal sphincter injury: Medio lateral episiotomy
Injury to the lavator axis & coccygeus muscles
for occult injuries: Forceps delivery
Prolonged 2nd stage
Medio lateral epi
Neural injury:Descent of fetal head → stretch & compression of
pelvic floor & associated nerves
Risk factors for nerve damage: operative delivery
prolonged 2nd stage
↑ BW
Most resolve after 1st year, some remain >5yr
Denervation injury may accumulate with ↑ parity.
CAN OBTETRICAL CARE BE MODIFIED TO
REDUCE PFD?
1- C/S before labor: no RCT
weak evidence to support preventive role for C/S
(2006 National Institution of Health).
7 should undergo C/S to permit 1 woman from
developing PFD latter in life
2- Changes in labor management
*avoidance of episiotomy (anal sphincter trauma)
*avoidance of operative delivery (FI, pudendal neuropathy)
other factors? CPD – race.
*oxytocin use (no RCT)
*epidural anesthesia (no RCT)
*macrosomia: could influence → OB intervention
PFD
3- Prophylactic pelvic floor muscle exercises:
No effect (during pregnancy & post partum)
4- Limiting Parity:
Risk of prolapse doubles after 1st birth
↑ 10% with each additional delivery
5- Other strategies:
Age – race – smoking – obesity
(non modifiable)
Alternatives to operative vaginal deliveries (OVD)
C/S
Expectant management: delayed pushing
maternal rest
change in mat. position
emotional support
Augmentation with oxytocin
Selected Issues
SUI during pregnancy: The best delivery plan?
some observational studies: SUI are less after C/S
Some do not show this benefit
C/S →↓ SUI by 12% not affected by SUI during
pregnancy
Further studies are needed
Women who have undergone surgical repair.
The best delivery plan: no Consensus
Women with a prior anal sphincter laceration
secondary repair:
Carefully counseled about pregnancy & delivery
Recommendation of experts → planned C/S
Birth injuries of fetus - neonate
• Overall incidence: 2% NVD, 1.1% C/S
• ↑ Risk: macrosomia (>4000g), Mat. obesity, Breech, OVD,
Small mat. size & Mat. pelvic anomalies
• Most common: Soft tissue injuries (bruising – petechiae,
subcutaneous fat necrosis, lacerations)
• Lacerations are the most common injury associated with C/S.
Other Injuries
Extra cranial
Intra cranial
Facial
Fx
Neurologic
Intra abdominal
*Extra cranial: Caputsuccedaneum, cephalohematoma:
resolves spontaneously
*Intracranial: Subgaleal hemorrhage → massive blood
loss → not managed appropriately → shock & death
(4/10.000 NVD vs 59/10.000 vaccum)
ICH: 3.7, 16.2, 17/10.000
*Facial injuries: Nasal septal dislocation (3d)
Ocular injuries: (mild, resolves)
Fx:
Clavicle, humerus, femur, skull: resolve spontaneously
Immobilization (4w)
Neurologic injuries:
Brachial plexus & facial, phrenic & laryngeal nerves
resolve spontaneously
Spinal cord injuries: poor prognosis
Intra abdominal injuries
Rare, rupture & hemorrhage in to the liver,
spleen & adrenal gland.
Neonatal Complications due to OVD:
Short term → head compression.
traction on fetal intracranial structures,
face, scalp
Most serious: ICH
Bruises abrasions, lacerations, facial nerve palsy,
cephalohematoma, retinal hemorrhage, subgaleal
hemorrhage, skull fx.
Most of these occurs in the course of a spontaneous vag.
delivery.
presentation: 10hr
(Continued)
Long term: ICH
(subdural, subarachnoid, IV, intraparencyhmal
& neuromuscular injury)
Vacuum <34w
Vacuum: ↑ neonatal cephalohematoma, ↑ retinal
hemorrhage VS. forceps or spontaneous vag. delivery
Developmental outcomes = equivalant for forceps &
vaccum
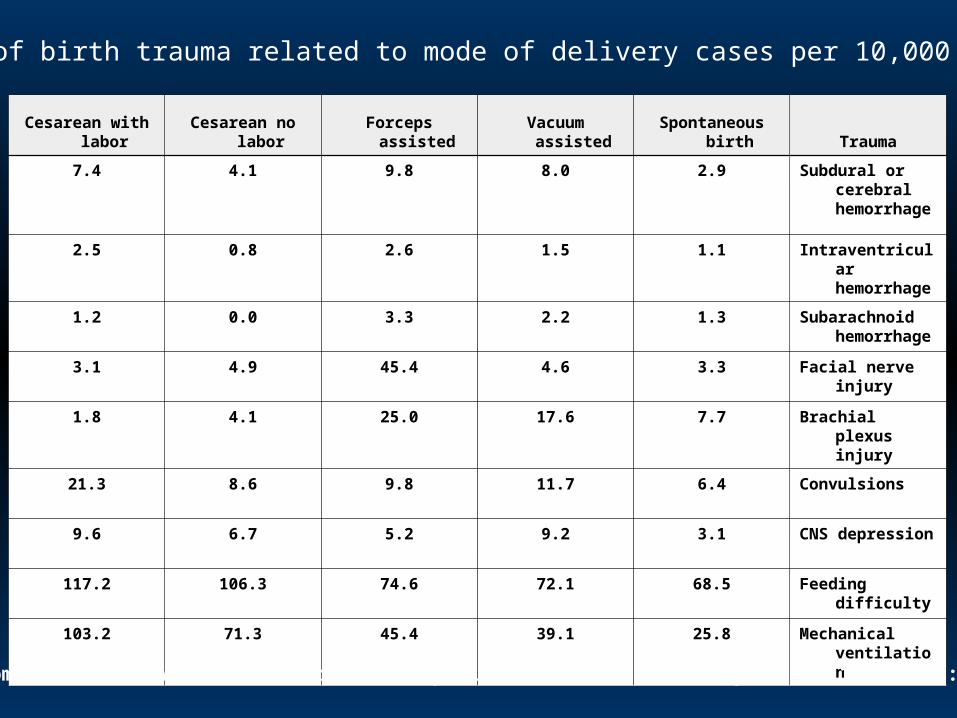
Frequency of birth trauma related to mode of delivery cases per 10,000 births
TraumaSpontaneous birthVacuum assistedForceps assistedCesarean no laborCesarean with
labor
Subdural or cerebral hemorrhage
2.98.09.84.17.4
Intraventricular hemorrhage
1.11.52.60.82.5
Subarachnoid hemorrhage
1.32.23.30.01.2
Facial nerve injury3.34.645.44.93.1
Brachial plexus injury
7.717.625.04.11.8
Convulsions6.411.79.88.621.3
CNS depression3.19.25.26.79.6
Feeding difficulty68.572.174.6106.3117.2
Mechanical ventilation
25.839.145.471.3103.2
Adapted from: data in Towner, D, Castro, MA, Eby-Wilkens, E, et al. N Engl J Med 1999; 341:1709.
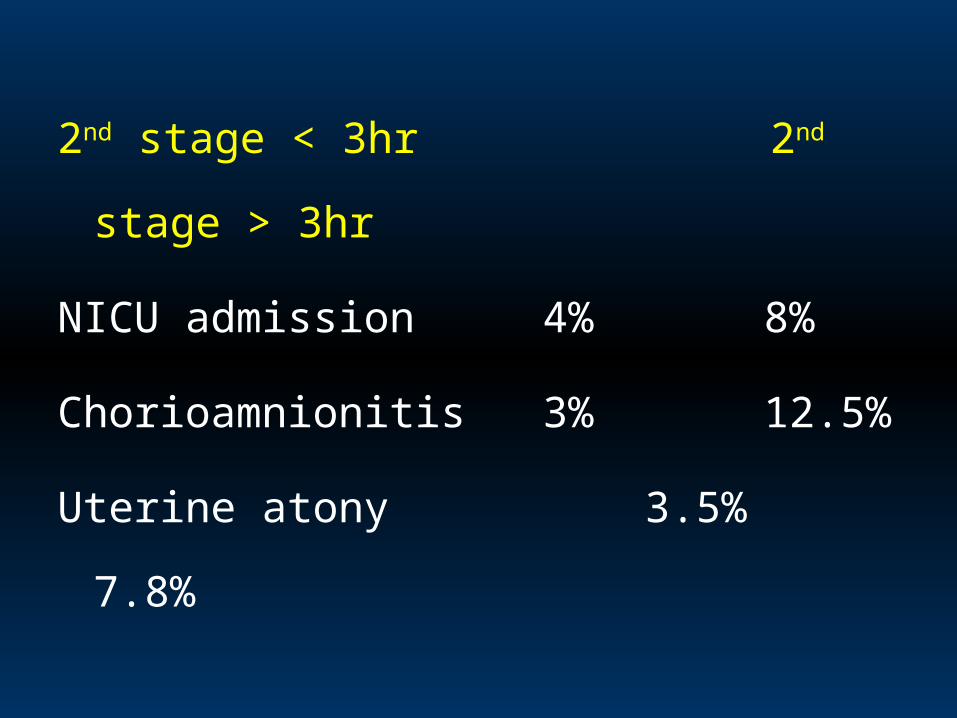
2nd stage < 3hr 2nd stage > 3hr
NICU admission 4% 8%
Chorioamnionitis 3% 12.5%
Uterine atony 3.5% 7.8%
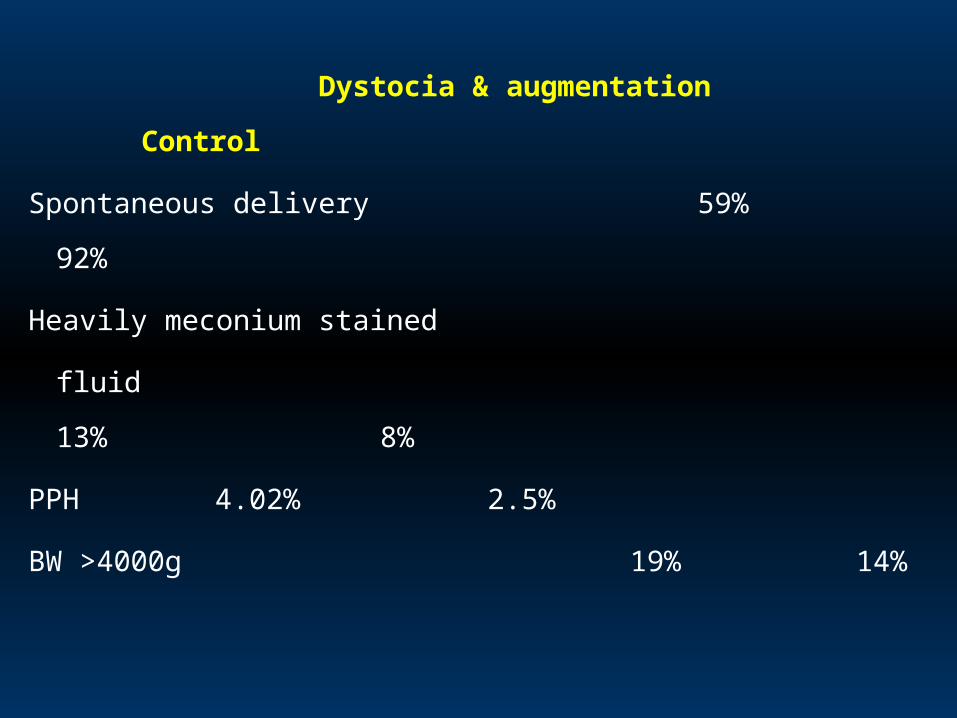
Dystocia & augmentation Control
Spontaneous delivery 59% 92%
Heavily meconium stained
fluid 13% 8%
PPH 4.02% 2.5%
BW >4000g 19% 14%
Patient safety:
Minimizing error & preventing harm
Reason for errors: Human fallibility
Medical complexity
System deficiencies
Defensive barriers
Strategies to reduce errors:
& subsequent adverse out comes
1- Team & individual training
2- Simulation & drills
3- Development of protocols, guidelines, checklists.
4- Use of informative technology
5- Education.